buddy newton, md facp medical ... - apa.memberclicks.net · medical director of antimicrobial...
TRANSCRIPT

Buddy Newton, MD FACPMedical Director of Antimicrobial Stewardship
Washington Regional Medical CenterFayetteville, AR


I do not have any financial or commercial disclosures
I have prescribed and taken antibiotics

“On the whole, the position of antimicrobial agents in medical therapy is highly satisfactory. The majority of bacterial infections can be cured simply, effectively, and cheaply. The mortality and morbidity from bacterial diseases has fallen so low that they are no longer among the important unsolved problems of medicine. These accomplishments are widely known and appreciated…”
Ernest Jawetz, noted microbiologist. 1956

“The war against infectious disease has been won”
Dr. Willam Stuart, US Surgeon General. 1969

80% of all ABX in the USA are used in animal/food industry
25 million pounds of ABX are produced for human consumption annually
160 million courses of ABX in NONhospitalized pts annually
30%-50% of all hospitalized pts receive a course of ABX
50%-99% of antimicrobial use is inappropriate

Treatment duration too long Treatment of noninfectious entities◦ Colonization◦ “Lasix-responsive” pneumonia◦ “CYA”
Ineffective therapy when pathogen is ID’d ◦ Wrong choice◦ Wrong dose

Improve patient care Reduce unwanted consequences of ABX
overuse or misuse Reduction in emergence of MDROs Preservation of antimicrobial activity for
future use Reduction in healthcare costs

By the end of 2017, CMS should have Federal regulations (Conditions of Participation) in place that will require U.S. hospitals, critical access hospitals, and long‐term care and nursing home facilities to have in place robust antibiotic stewardship programs that adhere to best practices, such as those contained in the CDC Core Elements for Hospital Antibiotic Stewardship Program recommendations. Similar requirements should be phased in rapidly for other settings including long‐term acute care hospitals, other post‐acute facilities, ambulatory, surgery centers, and dialysis centers.

We don’t but there are some clues based on currently available data

Summary of Core Elements of Hospital Antibiotic Stewardship Programs
Leadership Commitment: Dedicating necessary human, financial and information technology resources Accountability: Appointing a single leader responsible for program outcomes. Experience with successful programs show that a physician leader is effectiveDrug Expertise: Appointing a single pharmacist leader responsible for working to improve antibiotic use.Action: Implementing at least one recommended action, such as systemic evaluation of ongoing treatment need after a set period of initial treatment (i.e. “antibiotic time out” after 48 hours)Tracking: Monitoring antibiotic prescribing and resistance patternsReporting: Regular reporting information on antibiotic use and resistance to doctors, nurses and relevant staffEducation: Educating clinicians about resistance and optimal prescribing
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html

Checklist for Core Elements of Hospital Antibiotic Stewardship Programs
The following checklist is a companion to Core Elements of Hospital Antibiotic Stewardship Programs.
This checklist should be used to systematically assess key elements and actions to ensure optimal antibiotic prescribing and limit overuse and misuse of antibiotics in hospitals. CDC recommends that all hospitals implement an Antibiotic Stewardship Program. Facilities using this checklist should involve one or more knowledgeable staff to determine if the following principles and actions to improve antibiotic use are in place. The elements in this checklist have been shown in previous studies to be helpful in improving antibiotic use though not all of the elements might be feasible in all hospitals.
http://www.cdc.gov/nhsn/forms/57.103_PSHospSurv_BLANK.pdf

LEADERSHIP SUPPORT ESTABLISHED AT FACILITY
A. Does your facility have a formal, written statement of support from leadership that supports efforts to improve antibiotic use (antibiotic stewardship)?
❑ Yes ❑ No
B. Does your facility receive any budgeted financial support for antibiotic stewardship activities (e.g., support for salary, training, or IT support)?
❑ Yes ❑ No

ACCOUNTABILITY
A. Is there a physician leader responsible for program outcomes of stewardship activities at your facility?
❑ Yes ❑ No
DRUG EXPERTISE
A. Is there a pharmacist leader responsible for working to improve antibiotic use at your facility?
❑ Yes ❑ No

KEY SUPPORT FOR THE ANTIBIOTIC STEWARDSHIP PROGRAMDoes any of the staff below work with the stewardship leaders to improve antibiotic use?
B. Clinicians❑ Yes ❑ No
C. Infection Prevention and Healthcare Epidemiology❑ Yes ❑ No
D. Quality Improvement❑ Yes ❑ No
E. Microbiology (Laboratory)❑ Yes ❑ No
F. Information Technology (IT) ❑ Yes ❑ No
G. Nursing❑ Yes ❑ No

ACTIONS TO SUPPORT OPTIMAL ANTIBIOTIC USE
POLICIES POLICY ESTABLISHED
A. Does your facility have a policy that requires prescribers to document in the medical record or during order entry a dose, duration, and indication for all antibiotic prescriptions?
❑ Yes ❑ No
B. Does your facility have facility-specific treatment recommendations, based on national guidelines and local susceptibility, to assist with antibiotic selection for common clinical conditions?
❑ Yes ❑ No

SPECIFIC INTERVENTIONS TO IMPROVE ANTIBIOTIC USEAre the following actions to improve antibiotic prescribing conducted in your facility?
BROAD INTERVENTIONS
C. Is there a formal procedure for all clinicians to review the appropriateness of all antibiotics 48 hours after the initial orders (e.g. antibiotic time out)?
❑ Yes ❑ No
D. Do specified antibiotic agents need to be approved by a physician or pharmacist prior to dispensing (i.e., pre-authorization) at your facility?
❑ Yes ❑ No
E. Does a physician or pharmacist review courses of therapy for specified antibiotic agents (i.e., prospective audit with feedback) at your facility?
❑ Yes ❑ No

PHARMACY-DRIVEN INTERVENTIONSAre the following actions implemented in your facility?
F. Automatic changes from intravenous to oral antibiotic therapy in appropriate situations?
❑ Yes ❑ No
G. Dose adjustments in cases of organ dysfunction?❑ Yes ❑ No
H. Dose optimization (pharmacokinetics/pharmacodynamics) to optimize the treatment of organisms with reduced susceptibility?
❑ Yes ❑ No
I. Automatic alerts in situations where therapy might be unnecessarily duplicative?
❑ Yes ❑ No
J. Time-sensitive automatic stop orders for specified antibiotic prescriptions?
❑ Yes ❑ No

DIAGNOSIS AND INFECTIONS SPECIFIC INTERVENTIONSDoes your facility have specific interventions in place to ensure optimal use of antibiotics to treat the following common infections?
K. Community-acquired pneumonia ❑ Yes ❑ No
L. Urinary tract infection❑ Yes ❑ No
M. Skin and soft tissue infections❑ Yes ❑ No
N. Surgical prophylaxis❑ Yes ❑ No
O. Empiric treatment of Methicillin-resistant Staphylococcus aureus (MRSA)
❑ Yes ❑ No

P. Non-C. Difficile infection (CDI) antibiotics in new cases of CDI❑ Yes ❑ No
Q. Culture-proven invasive (e.g., blood stream) infections❑ Yes ❑ No
DIAGNOSIS AND INFECTIONS SPECIFIC INTERVENTIONS (con’t)

TRACKING: MONITORING ANTIBIOTIC PRESCRIBING, USE, AND RESISTANCE
PROCESS MEASURES
A. Does your stewardship program monitor adherence to a documentation policy (dose, duration, and indication)?
❑ Yes ❑ No
B. Does your stewardship program monitor adherence to facility-specific treatment recommendations?
❑ Yes ❑ No
C. Does your stewardship program monitor compliance with one of more of the specific interventions in place?
❑ Yes ❑ No

ANTIBIOTIC USE AND OUTCOME MEASURES
D. Does your facility track rates of C. difficile infection?❑ Yes ❑ No
E. Does your facility produce an antibiogram (cumulative antibiotic susceptibility report?
❑ Yes ❑ No

Does your facility monitor antibiotic use (consumption) at the unit and/or facility wide level by one of the following metrics:
F. By counts of antibiotic(s) administered to patients per day (Days of Therapy; DOT)?
❑ Yes ❑ No
G. By number of grams of antibiotics used (Defined Daily Dose, DDD)? ❑ Yes ❑ No
H. By direct expenditure for antibiotics (purchasing costs)?❑ Yes ❑ No

REPORTING INFORMATION TO STAFF ON IMPROVING ANTIBIOTIC USE AND RESISTANCE
A. Does you stewardship program share facility-specific reports on antibiotic use with prescribers?
❑ Yes ❑ No
B. Has a current antibiogram been distributed to prescribers at your facility?
❑ Yes ❑ No
C. Do prescribers ever receive direct, personalized communication about how they can improve their antibiotic prescribing?
❑ Yes ❑ No

EDUCATION
A. Does your stewardship program provide education to clinicians and other relevant staff on improving antibiotic prescribing?
❑ Yes ❑ No

Established- Jan 2012

0%10%20%30%40%50%60%70%80%90%
Surgery
Medicine
Total

02468
1012141618
13-J
an
13-M
ar
13-M
ay
13-J
ul
13-S
ep
13-N
ov Jan
14-M
ar
14-M
ay
14-J
ul
14-S
ep
14-N
ov
15-J
an
15-M
ar
15-M
ay
15-J
ul
Started distributing notes personally

Recs taken
Recs not taken
LOT Reduction
(d)
% reduction
Mean 2012
2.26 3.24 -0.98 -30.2%
Mean 2013
2.43 3.44 -1.01 -29.4%
Mean 2014
2.51 3.92 -1.41 -36.0%

1.771.8
2.081.91
1.61.79
1.61.69
0
0.5
1
1.5
2
2.5
Q1 Q2 Q3 Q4
2010
2011
2012
2013
2014
2015
1.691.86


Simple blood test specific for bacterial infection
In healthy people, PCT concentration are found <0.05ng/ml
Concentrations >0.5ng/ml can be interpreted as abnormal
During severe bacterial infections and sepsis, blood levels rise rapidly (up to x100K) – no elevation from viral infections
Standard of Care for much of Europe in the management of infection and sepsis

Healthy Sepsis
In relevant bacterial infection, PCT is produced and released into circulation from the entire body
Müller B. et al., JCEM 2001

Alternative synthesis of PCTBacterial toxins (gram+/-) and cytokines stimulate production of PCT in all parenchymal tissuesPCT is immediately released into bloodstreamThis process can be blocked during viral infections
Adapted from Christ-Crain et al. 2005

Three elements are required to the induction process◦ Stimulus – bacterial toxin or trauma◦ Differentiated parenchymal cells◦ Adhering monocytes
PCT plasma concentrations◦ Significant after 6 hours◦ Peak values – 12 to 24 hours◦ Half-life - about 24 hours◦ Not impaired by neutropenia or other immunocomprised states

Healthy Individuals
Local Infections
Systemic Infections (Sepsis)
Severe Sepsis
Septic Shock
0.05 ng/ml
0.5 ng/ml
2 ng/ml
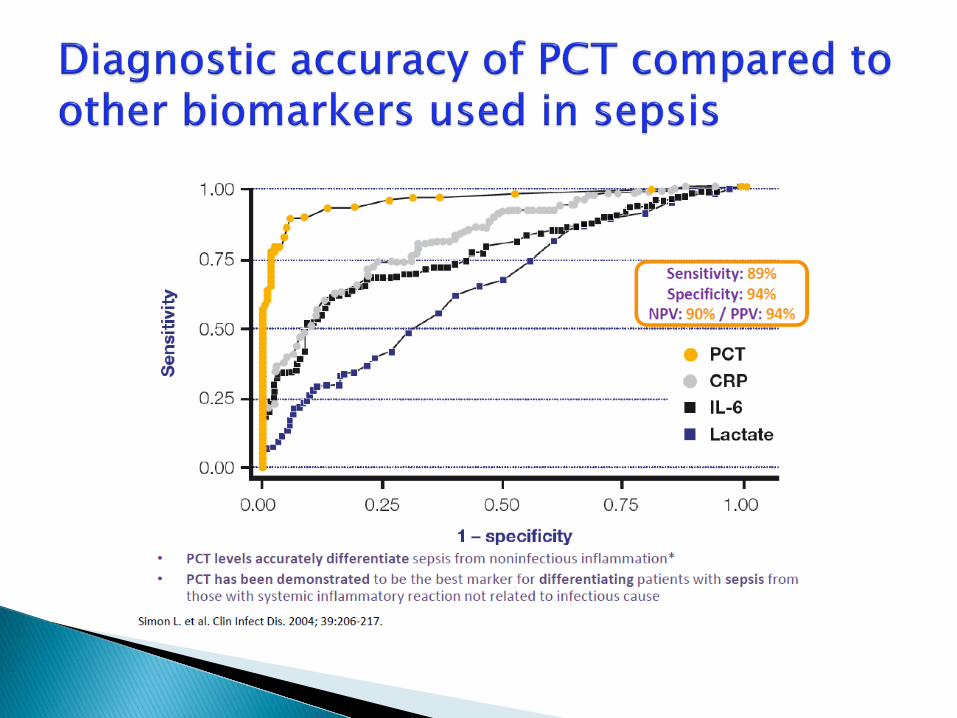
•In critically ill patients, PCT levels elevate in correlation to the severity of bacterial infection. Also excellent prognostic marker.•Integrating PCT in sepsis management can lead to improved patient outcomes

Diagnosis of bacteremia/sepsis in adults and neonates (>72 hours old)
Differentiating bacterial vs nonbacterial pneumonia
Differentiating bacterial vs aseptic meningitis Diagnosis of bacterial infection in febrile
neutropenia Diagnosis of septic arthritis

Newborn <48hr-increased PCT values (physiological peak)
Primary inflammation syndrome following extensive trauma: extensive burns, major surgery (cardiac, transplant, abdominal)
Medullary C-cell cancers of the thyroid, pulmonary small-cell carcinoma
Prolonged circulatory failure (cardiogenicshock, hemorrhagic shock, thermal shock)
Malaria & some fungal infections

Consider the clinical context-(pts in septic shock should not have ABX withheld if PCT is normal)
Serial measurements are preferred and may be very helpful
Consider the dynamics of the disease-(PCT levels fall after trauma if no infection present. If PCT levels are rising after ABX, consider changing ABX or looking for drainable source of infection)
Keep in mind conditions that will cause PCT levels to rise

Evidence-basedCriterion
RCTs Observational Studies
Strong evidence for PCT URICOPD exacerbationPneumoniaSevere sepsis/septic shock
Good evidence for PCT VAPPostop infxnsMeningitis
BacteremiaPyelo/UTIs
Moderate evidence for PCT
Postop feverSeptic arthritisNeutropenia
Weak evidence for PCT EndocarditisIntra-abd abscessPancreatitis
Riedel S. Diagn Microbiol Infect Dis. 73 (2012); 221-7.

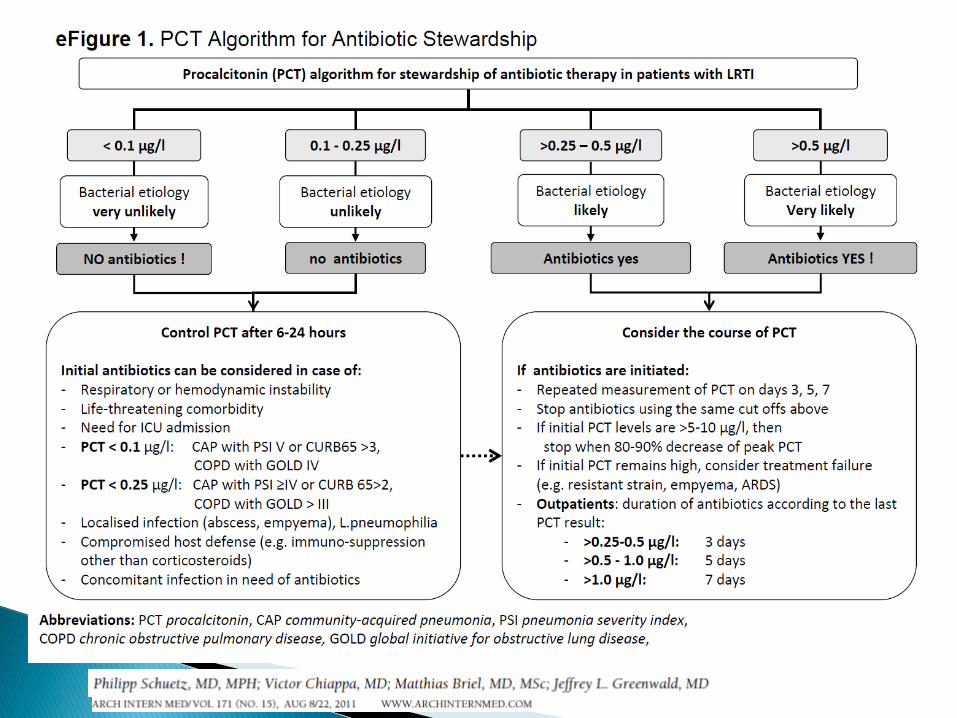
May be general or disease specific Simple or more involved Assist in:◦ Should antibiotic therapy be initiated◦ Initial antibiotic intensity◦ Repeat PCT◦ Course adjustment◦ De-escalation of therapy◦ Discontinuation of therapy

Meta-analysis (4221 pts, 14 RCTs) PCT-guided vs standard Rx (control)◦ No change in mortality (5.7% vs 6.3%) or in Rx
failure (19.1% vs 21.9%) in any clinical setting◦ Total ABX exposure reduced by 3.47 days across all
clinical settings [outpt (-3.06), ED (-2.96), ICU (-3.21)]◦ PC setting-lower prescription rates for resp illness◦ ED & ICU settings-shorter duration of ABX therapy
Schuetz P, Briel M, Christ-Cain M, et al. Clin Infect Dis 2012;55:651-62.


0.950.42
0.92 1.19 1.141.98
1.311.68
2.10
0.57
0123456789
1Q 13 2Q 13 3Q13 4Q 13 1Q 14 2Q 14 3Q 14 4Q 14 1Q 15 2Q 15(YTD)
Delta
Abnl or no PCT
Nl or normalized PCT
Linear (Delta)
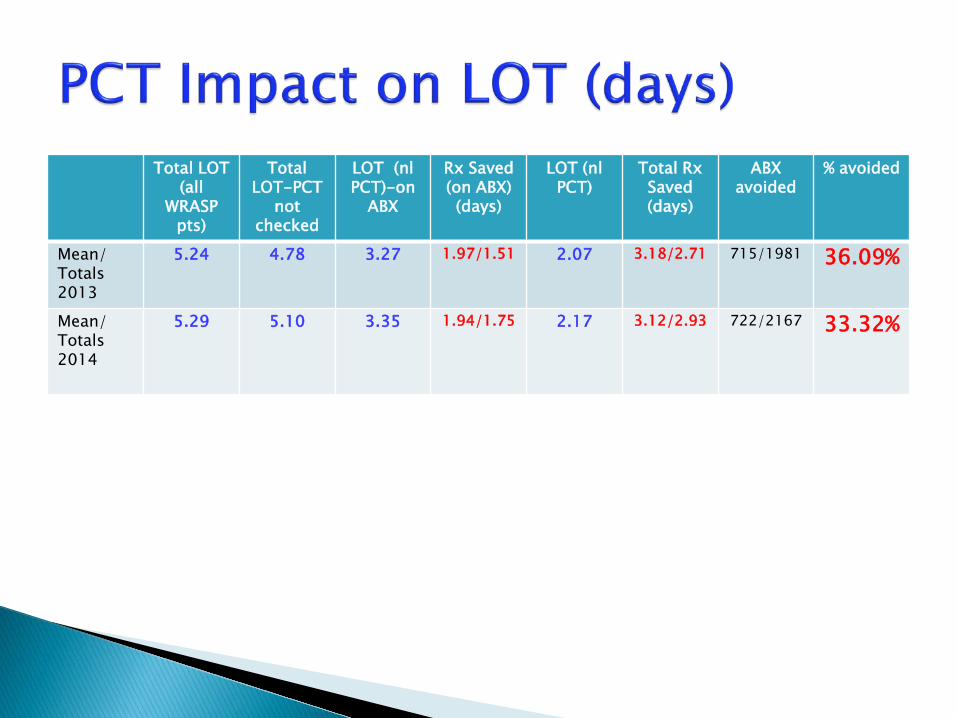
Total LOT (all
WRASP pts)
Total LOT-PCT
not checked
LOT (nlPCT)-on
ABX
Rx Saved (on ABX)(days)
LOT (nlPCT)
Total Rx Saved (days)
ABX avoided
% avoided
Mean/ Totals 2013
5.24 4.78 3.27 1.97/1.51 2.07 3.18/2.71 715/1981 36.09%
Mean/ Totals 2014
5.29 5.10 3.35 1.94/1.75 2.17 3.12/2.93 722/2167 33.32%

Total LOT (all
WRASP pts)
Total LOT-PCT
not checked
LOT (nlPCT)-on
ABX
Rx Saved (on ABX)(days)
LOT (nlPCT)
Total Rx Saved (days)
ABX avoided
% avoided
Mean/ Totals 2014
5.29 5.10 3.35 1.94/1.75 2.17 3.12/2.93 722/2167 33.32%
Jan 15 6.14 5.79 3.49 2.65/2.30 2.37 3.72/3.42 73/223 32.74%
Feb 15 5.81 6.03 3.71 2.10/2.32 2.27 3.49/3.76 81/205 39.51%Mar 15 6.10 5.62 3.95 2.15/1.67 2.53 3.50/3.09 72/196 36.73%Apr 15 4.53 4.15 3.31 1.22/0.84 2.31 2.21/1.84 61/200 30.50%May 15 5.18 4.76 3.76 1.42/1.00 2.29 2.80/2.47 75/183 40.98%Jun 15Jul 15Aug 15
Sep 15Oct 15
Nov 15
Dec 15

857 cases from 5/13-4/14 Compared LOS and LOT in all ASP patients with
PCT data◦ Total LOS (nl PCT vs abnl PCT)-8.5d vs 8.2d; p=0.2001◦ LOT after ASP advice (compliers vs noncompliers)- 2.5d
vs 3.9d, P<0.0001◦ Total LOT (compliers vs noncompliers)-5.1d vs 6.6d,
P<0.001-No difference in any clinical outcomes
PCT-guided ASP can result in a significant reduction in antibiotic use
ID Week 2015-Poster #1507

Highly specific biomarker for bacterial infxn (best data is in resp infxn & sepsis)
Excellent correlation with severity of illness thus an excellent prognostic marker
Excellent decision tool for initiating ABX and de-escalation/discontinuation of therapy
Serial measures are key to clinical success for inpatients.


Strikes more than 750,000 people annually in the United States
Mortality remains at 18% or higher Clinical diagnosis remains challenging Severe sepsis accounts for $16 billion hospital inpatient costs

6.5
11.2
4.2
7.2
0
2
4
6
8
10
12
ICU LOS Hospital LOS
Leng
th o
f Sta
y (d
ays)
Severe SepsisPatients

31%
2%0%
5%
10%
15%
20%
25%
30%
35%
Top Ten DRG Totals (avg)
Vent
ilato
r Use
(%
)
Severe SepsisPatients

23
12
-
5
10
15
20
25
Top Ten DRG Totals (avg)
Cost
per
Cas
e (T
hous
ands
of D
olla
rs)
Severe SepsisPatients


Bacterial Components
Activators of Inflammation
and Coagulation
Inflammation and
Coagulation
Hypotension and Organ
Dysfunction
SIRS Sepsis Severe Sepsis
Septic Shock
2 or More
• > 38◦C or < 36◦C. • >90 bpm.• >20
breaths/min.• paCO2 < 32 mm
Hg.• WBC >
12,000/mm3, < 4,000/mm3, or >10% bands
• SIRS resulting frominfection.
• Organ dysfunction.
• Hypoperfusion.• Hypotension.
• Sepsis-induced hypotension.
• Perfusion abnormabilites.

Ist step is RECOGNITION of SEPSIS!! Early intervention is critical Appropriate antibiotic therapy within one
hour of hypotension Resuscitation/re-establish perfusion
within six hours
It is hard to treat something that you do not know exists….
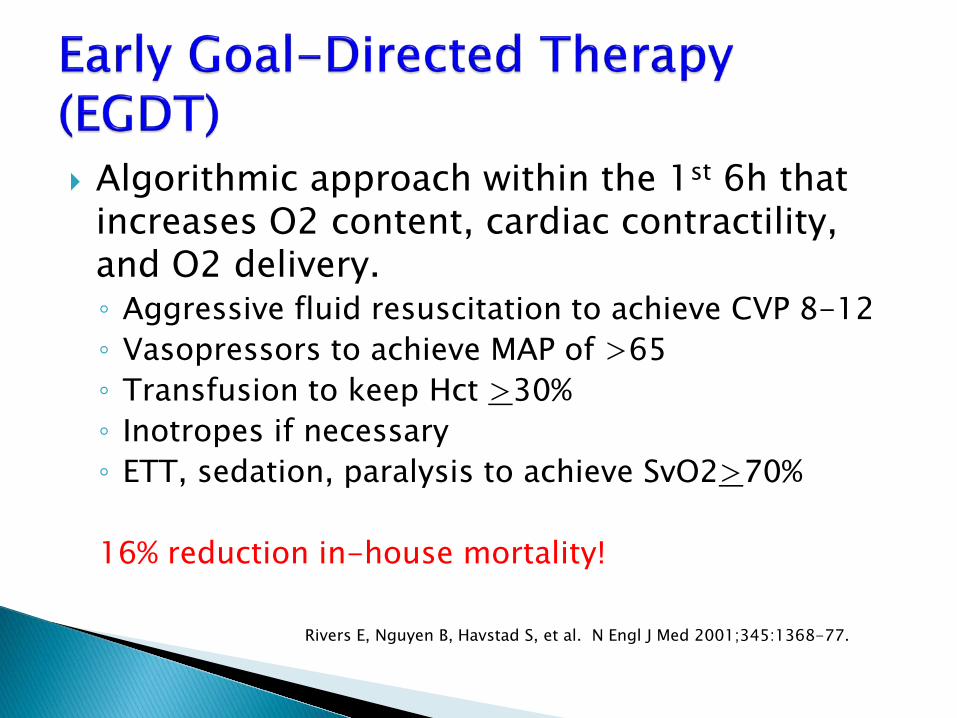
Algorithmic approach within the 1st 6h that increases O2 content, cardiac contractility, and O2 delivery.◦ Aggressive fluid resuscitation to achieve CVP 8-12◦ Vasopressors to achieve MAP of >65◦ Transfusion to keep Hct >30%◦ Inotropes if necessary◦ ETT, sedation, paralysis to achieve SvO2>70%
16% reduction in-house mortality!
Rivers E, Nguyen B, Havstad S, et al. N Engl J Med 2001;345:1368-77.
Decreases mortality (23% vs 43%) Decreases ICU LOS (5d vs 8 d) Decreases time in ED (thus increases
throughput)-(201 mins vs 180 mins)
Only initiated in 57% of eligible patients◦ Lack of recognition◦ Inexperience in junior medical staff◦ Lack of senior nursing staff
Sivayoham N, Rhodes A, Jaiganesh T, et al. Eur J Emerg Med. 2012;19:235-40.

7.6% increase in mortality for every hour that ABX not given!You do the math!!
Kumar A, Roberts D, Wood KE, et al. Crit Care Med 2006;34:1589-96.

261 patients undergoing EGDT Triage to ABX <1h (mortality 19.5% vs 33.2%) Qualification for EGDT to ABX <1h (mortality
25.0% vs 38.5%)
Gaieski DF, Mikkelsen ME, Band RA, et al. Crit Care Med 2010;38:1045-53.

Recognition◦ Automated sepsis alerts in Cerner and PICIS◦ Immediate evaluation followed by 2L fluid bolus
(within 1h)◦ POC lactate◦ STAT procalcitonin (TAT <1h)
If lactate >4.0; PCT>1.0 or MAP<65 or SBP<90 after above fluid bolus then proceed to Phase 1 of the Sepsis Powerplan.

Continue fluid boluses until MAP>65 or SBP>90
Draw BCx’s (always 2 sets) Meropenem-1 gm IVP over 3-5 mins Levaquin-750 mg IV over 0.5-1h Vancomycin-1 g IVPB over 45mins-1h
Place CVL if possible

CVL must be in place Fluid management per defined CVP criteria Vasopressors dictated by MAP criteria Transfusions dictated by SvO2 criteria Predefined empiric antibiotic management
directed by presumed source of infection CMS Core Measures addressed in powerplan.

4% 8% 3%
95%
59%
73%
0%10%20%30%40%50%60%70%80%90%
100%
3Q/4Q2013
1Q 2014 2Q 2014 1Q 2015 2Q 2015 3Q 2015

0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
2012 2013 2014 2015 (thru6/15)
MS-DRG 871
MS-DRG 871
Order Set developed
Major pushvia ED MDs
Nat’l Mortality Rate

Huge impact on society, financially, and patient outcomes (mortality, LOS, etc)
Must recognize and initiate treatment severe sepsis very early to impact survival
Modifiable determinants of mortality are aggressive fluid resuscitation and ABX initiation
EGDT has the most significant impact on patient outcomes for sepsis in the last 25 years

