bringing health care online: the role of information
TRANSCRIPT

Bringing Health Care Online: The Role ofInformation Technologies
September 1995
OTA-ITC-624
GPO stock #052-003-01433-5
Recommended Citation: U.S. Congress, Office of Technology Assessment, BringingHealth Care Online: The Role of Information Technologies, OTA-ITC-624 (Washington,DC: U.S. Government Printing Office, September 1995).

iii
oreword
nformation technologies are transforming the way health care is de-livered. Innovations such as computer-based patient records, hospi-tal information systems, computer-based decision support tools,community health information networks, telemedicine, and new
ways of distributing health information to consumers are beginning toaffect the cost, quality, and accessibility of health care. Changes in thehealth care delivery system, including the emergence of managed healthcare and integrated delivery systems, are breaking down the organiza-tional barriers that have stood between care providers, insurers, medicalresearchers, and public health professionals. Old distinctions betweenclinical health information and administrative health information aregradually eroding as new health care delivery patterns emerge that aresupported by, and in some cases reliant on, the widespread use of net-worked computers and telecommunications.
Bringing Health Care Online: The Role of Information Technologiesdiscusses the synergy between information technologies and new trendsin the health care delivery system as health care is brought online. It iden-tifies some of the opportunities to improve health care delivery throughincreased use of information technology, and discusses some of the con-ceptual, organizational, and technical barriers that have made its adop-tion so uneven. The report identifies key technologies and shows howthey are being used to communicate clinical information, simplify ad-ministration of health care delivery, assess the quality of health care, in-form the decisionmaking of providers and administrators, and supportdelivery of health care at a distance.
OTA appreciates the assistance of the project advisory panelists,workshop participants, and contractors, as well as the many other indi-viduals who participated in the study. OTA values their perspectives andcomments; the report is, however, solely the responsibility of OTA.
ROGER C. HERDMANDirector

iv
dvisory Panel
Clement McDonald(Chair)Distinguished Professor of
MedicineIndiana University School of
MedicineIndianapolis, IN
June AbbeyDirector of ResearchInstitute of InnovationShadyside HospitalPittsburgh, PA
Stephen DeutschProfessorLabor Education and Research
CenterUniversity of OregonEugene, OR
Elliott FisherAssociate Professor of MedicineDartmouth Medical SchoolHanover, NH
Bonnie Guiton HillDeanMcIntire School of CommerceUniversity of VirginiaCharlottesville, VA
James HazelrigsExecutive DirectorMedical Database CommissionState of North CarolinaRaleigh, NC
Susan HornSenior ScientistInstitute for Health Care Delivery
ResearchIntermountain Health CareSalt Lake City, UT
James HuntDistinguished ProfessorHealth Sciences CenterUniversity of TennesseeMemphis, TN
Nancy MilioProfessor of Health Policy &
AdministrationUniversity of North CarolinaChapel Hill, NC
Lori Muhlstein*Market Manager, Health CareBell Atlantic Corp.Falls Church, VA
John NymanAssociate ProfessorInstitute for Health Services
ResearchUniversity of MinnesotaMinneapolis, MN
Madison PowersSenior Research ScholarKennedy Institute of EthicsGeorgetown UniversityWashington, DC
Jane PrestonPresidentAmerican Telemedicine
AssociationAustin, TX
Marsha RadajVice President, OperationsWisconsin Health Information
NetworkBrookfield, WI
William ReedQuantum Health Resources, Inc.Indianapolis, IN
Bert TobinExecutive Vice PresidentBenton InternationalNew York, NY
Bradley WareFairfax, VA
________________
*Until December 1994
Note: OTA appreciates the valuable assistance and thoughtful comments provided by the advisory panelists. The panel does not,however, necessarily approve, disapprove, or endorse this report. OTA assumes full responsibility for the report and the accuracy of itscontents.

v
roject Staff
Peter D. BlairAssistant Director, OTAIndustry, Commerce, and
International Security Division
Clyde BehneyAssistant Director, OTAHealth, Education, and
Environment Division
Andrew W. WyckoffProgram DirectorIndustry, Telecommunications,
and Commerce Program
James W. CurlinProgram Director1
Industry, Telecommunications,and Commerce Program
Sean TunisProgram DirectorHealth Program
Karen G. BandyProject Director
Jean E. SmithAssistant Project Director
William CreagerContractor/Congressional Fellow
David KlingmanSenior Analyst
Laura StrickerResearch Analyst2
ADMINISTRATIVE STAFF
Liz EmanuelOffice Administrator
Karry FornshillSecretary
Diane JacksonAdministrative Secretary
Karolyn St. ClairPC Specialist
PUBLISHING STAFF
Mary Lou HiggsManager
Chip MooreProduction Editor
Bonnie SparksElectronic Publishing Specialist
Chris OnrubiaSenior Graphic Designer
CONTRACTORSAspden AssociatesCollin CanrightHealth Economics Research, Inc.The Orkand Corp.Phoenix Planning & Evaluation,
Ltd.Project HOPE, Center for Health
Affairs
________________
1Through September 19942Through June 1994

vi
1 Introduction, Summary, and Options 1Challenges and Opportunities for Information
Technologies 2Trends in the Health Care System5Congressional Interest9Report Summary 10Other Applications 23
2 Information Technologies forTransforming Health Care 29Islands of Automation 30The Life Cycle of Health Information34Key Technologies for the Emerging Health Information
Infrastructure 42Sharing the Common Pool of Data68Policy Issues and Options73
3 Networks for Health Information 79Administrative Simplification 80Administrative Activities in Health Care83Provider Administrative Activities 83Exchanging Information Between Providers
and Payers 84Linking Health Care Providers With Suppliers93Pharmaceutical Industry EDI94Community and Regional Networking95Costs and Cost-Effectiveness103Policy Implications of Electronic Health
Information 109Policy Considerations for Congress118
4 Using Information Technology to Improvethe Quality of Health Care 123Clinical Decision Support 124Performance Assessment142Conclusions 152
ontents

vii
5 Telemedicine: Remote Access to HealthServices and Information 159Telemedicine’s Potential Effects160Telemedicine Applications 165Telemedicine Issues177Telemedicine Policy Options187
APPENDICES
A Workshop Participants 193
B Reviewers and Contributors 195
C Applications of Clinical Decision SupportSystems 197
D Executive Branch TelemedicineActivities 201
E Electronic Health InformationSources 207
F Boxes, Figures, and Tables 213
G Abbreviations and Glossary 215

Introduction,Summary,
andOptions
nformation technologies are transforming the way healthcare is delivered. Innovations such as computer-based pa-tient records, hospital information systems, computer-baseddecision support tools, community health information net-
works, telemedicine, and new ways of distributing health in-formation to consumers are beginning to affect the cost, quality,and accessibility of health care. The technologies that supportthese applications—relational databases, network communica-tions, distributed processing architectures, optical disk storage,and others—are used today by some health care providers andpayers. Yet information technology is often found in isolated“islands of automation” in health care provider and payer institu-tions. Despite the incorporation of high technology into almostevery other aspect of clinical practice, information technologieshave not been fully embraced.
Meanwhile, transformations in the way health care is deliveredare creating new opportunities for innovative applications of in-formation technologies. The health care delivery system is cur-rently undergoing many changes, including the emergence ofmanaged health care and integrated delivery systems that arebreaking down the organizational barriers that have stood be-tween care providers, insurers, medical researchers, and publichealth professionals. These barriers have supported a clear de-marcation between clinical health information and administrativehealth information and reinforced a long-standing distinction be-tween treatment of disease and preservation of health. These dis-tinctions are gradually eroding as new health care deliverypatterns emerge that are supported by, and in some cases relianton, the widespread use of networked computers and telecommu-nications. | 1

2 | Bringing Health Care Online: The Role of Information Technologies
This report discusses the synergy between in-formation technologies and new trends in thehealth care delivery system as health care isbrought online. It identifies some of the opportu-nities to improve health care delivery through in-creased use of information technology, anddiscusses some of the conceptual, organizational,and technical barriers that have made its adoptionso uneven. The report identifies key technologiesand shows how they are being used to communi-cate clinical information, simplify administrationof health care delivery, assess the quality of healthcare, inform the decisionmaking of providers andadministrators, and support delivery of health careat a distance.
CHALLENGES AND OPPORTUNITIES FORINFORMATION TECHNOLOGIESThe technologies used for collecting, distilling,storing, protecting, and communicating data arewidely used throughout American industry. In thehealth care industry, however, their applicationhas been limited to scattered islands of automa-tion, usually limited to discrete departments with-in hospitals. Computers are widely deployed, butnot widely connected. Clinical and administrativehealth information are rarely commingled. Bothtypes of health information are still stored andconveyed primarily in paper form. Health in-formation is rarely converted to digital form andshared among the clinics and primary care officeswhere most health care occurs, the hospitals andcritical care units where most health care dollarsare spent, or the population-based health servicesthat address community-wide health issues. Com-puters are typically used to organize and adminis-ter specific, limited types of health information,but are not linked into an infrastructure that mightallow broader efficiencies or higher quality healthcare.
Figure 1-1 shows the level of adoption of someselected information technology applications asreported by chief information officers (CIOs) of
primarily large health care institutions. As thefigure indicates, almost 70 percent of those re-sponding have introduced electronic systems forsubmitting insurance claims, and more are in theprocess of adopting them. Technologies that allowcommunication between computers at disparatelocations, for example physician-hospital datanetworks or enterprise-wide networks, are beingadopted or planned by a substantial number ofthese institutions as well. Computer-based patientrecord (CPR) systems, which are difficult to im-plement because they require such close integra-tion between many different systems, are at leastin the planning process, according to 50 percent ofresponding CIOs, but so far only about 20 percentconsider that they have CPRs operating at leastat an experimental level. When asked whichtechnologies they were currently evaluating con-ceptually for future implementation, the two mostfrequently mentioned by CIOs were communityhealth information networks and telemedicine.1
The health care delivery system has severalunique characteristics that discourage the spreadof information technologies. Health professionalsperform a wide variety of tasks including rapidlychanging combinations of “hands-on” care, in-ductive and diagnostic thinking, detailed record-keeping, patient education, and communicationwith colleagues. Most of the hardware and soft-ware approaches that address one of these aspectsof medical practice intrude unacceptably on someother aspect: computers are not yet as useful, ubiq-uitous, and handy as the stethoscope and othercommon medical technologies. In addition, medi-cal practice is extraordinarily complex and itchanges rapidly. Systematizing even the processof performing medical procedures, much less ra-tionalizing the language and scientific knowledgeunderlying those procedures, is an almost intrac-table problem. Despite the ongoing efforts of stan-dards-setting bodies, no unified conceptual modelexists that is powerful enough to construct themapping between the information that must be
1 College of Healthcare Information Management, Telecommunications in Health Care Survey, 1994 (Ann Arbor, MI: 1994), pp. 20-21.

Chapter 1 Introduction, Summary, and Options 3
Electronic claims submissionVoice mail for staff/physicians
Physician/hospital data networksGeneral telecom services
Ask-a-nurse/referral serviceEnterprise networks
Answering servicesAlpha pagers
Data processing servicesHome emergency alert
Telecommuting
Interactive voice response
Computer-based patient record
Teleradiology
Distance learning (satellite)Handheld computer devices
PCs
Community health information networksPicture archiving & communication
Home monitoring
Distance learning (video)Telemedicine
Voice mail for patients
Telepathology
,■ A d o p t e d
❏ Planning to adoptI I I
0 20 40 60 80 100
Percent
SOURCE: Center for Healthcare Management Information, Telecommunications in Healthcare Survey, 1994 (Ann Arbor, Ml. 1994)
stored in computer databases and medicine as it ispracticed. In a sense, there is not yet a consensusabout what information should be kept in comput-er-based patient records or how it should be de-scribed, organized, and indexed.
Apart from the complexity of clinical knowl-edge and practice, there are structural reasons thatdiscourage implementation of informationtechnologies in health care settings. In addition,many communities have only a few hospitals ormajor insurers. The cooperation necessary to in-terconnect medical information within a horizon-tal layer of the health care system may be seen asanticompetitive and subject to antitrust regula-tion, or it may be hindered by organizations thatregard their internal information systems as com-
petitive advantages and accumulated patient re-cords as corporate assets.
Information technologies tend to flatten orga-nizations and may not mesh well with the rigidlydefined job roles and hierarchical structure of cur-rent medical practice (see box l-l). Many types oforganizational changes will emerge throughoutthe health care system if information technologiesare widely adopted. In other industries, changesassociated with the introduction of informationtechnologies have included large reductions in thedemand for some types of workers (e.g., mid-levelmanagers and bank tellers), increased responsibi-lities for workers in jobs that traditionally in-volved little decisionmaking (line workers inmanufacturing industries), and an increase in
4

4 Bringing Health Care Online: The Role of Information Technologies
Increased use of information technology will continue to affect the jobs of the 10 million Americans
who work in health care. This workforce is currently growing at about 3.9 percent per year. Changes in
the structure of health care delivery are affecting the composition of the workforce. For example, hospi-
tal employment, while it still represents half of people employed in health care, is the slowest growing
sector at 1.7 percent per year. Home health care however, is growing at about 18 percent annually,
although it still accounts for only a small portion of the workforce.1
This report does not analyze the changes that information technology might bring to jobs in health
care, or the effects that these changes might have on the quality of the work environment. These would
be fruitful areas for future research. In general, it appears that information technology applications
could reduce the need for some types of work and could redefine some job roles.
For example, electronic data Interchange (EDI), defined as the application-to-application exchange
of business documents, is increasingly being used to carry out medical payments and other administra-
tive transactions between health care providers and insurance payers. Application-to-application
means that computer programs at different firms exchange information and complete transactions di-
rectly, without human intervention. Physicians’ office staffs, for example, often notice a decrease in the
number of telephone calls they make and letters they write after being linked with Insurers through on-
line systems. Much of the potential savings foreseen through “administrate simplification” of the health
care payments process comes from reduced personnel costs.2 The systems currently being implement-
ed do not totally eliminate human intervention, and within many provider and payer organizations some
of the employee time saved by automated payment systems will be spent on other tasks. Nevertheless,
a Iikely outcome of widespread use of electronic medical payments IS the elimination of some jobs in
both provider and payer organizations.(continued,)
1 U S Department of Commerce, U.S. Industrial Outlook, 1994 (Washington, DC: 1994), pp. 42-1 to 42-62 See, for example, Workgroup on Electronic Data Interchange, 1993 Report (Hartford, CT and Chicago, IL October 1993),
p 7-30
competition for local experts from nonlocal health care reflect the ability of computer net-sources (discount stockbrokers, for instance).Similar changes are likely to occur for health pro-fessionals, along with a redistribution of status,responsibilities, and remuneration associatedwith the various health disciplines.
Information technologies not only redefinejobs, but they may have more subtle ramificationsas well. The widespread adoption of integrated in-formation systems will challenge the legal sys-tem. Information technologies facilitate alliancesbetween geographically separate parties. Thus,they may challenge the existing structure of statemedical licensing and malpractice laws, as well as“pen and quill” laws that require paper-basedmedical recordkeeping. Consolidations and merg-ers among the many companies offering managed
works and digital telecommunications to act as anervous system that can connect previously inde-pendent parts of the health care delivery and ad-ministrative systems, forming new bodies knownas integrated delivery systems. These new corpo-rate structures may pose antitrust questions asthey challenge traditional providers of health carein isolated markets.
Information technologies diffuse decisionmak-ing and responsibility y because they are developed,maintained, and employed by a variety of people.Physicians—who have held unique positions ofstatus and compensation, as well as legal respon-sibility and risk, under the traditional systems oflicensure and malpractice law—may be put in theuncomfortable position of being solely responsi-

Chapter 1 Introduction, Summary, and Options 5
Information technology also can change job roles. For example, when physicians place medication
orders at a computer terminal, they take on a data entry task that might previously have been done by a
ward clerk, a pharmacist, or a pharmacy clerk. With proper design, the technology can help integrate
this task with others the physician performs—retrieving information about the patient’s condition, look-
ing up the proper dosage and use of medications, or making judgments and decisions about additional
tests and treatments. Whether data entry is an additional burden, or an integral part of an improved and
more efficient process for rendering care, depends on a wide variety of personal, institutional, hard-
ware, software, and interface design factors.
In some cases, role changes are induced by other organizational changes in which information
technology IS a facilitator. For example, one way that health care organizations are reducing costs IS by
redesigning work so that tasks once done by high-cost personnel are now done by lower cost person-
nel. For example, much primary health care previously done by physicians is now being done by physi-
cian extenders like physician assistants and nurse practitioners. In some hospitals, work previously
done by licensed and registered nurses is now done by nursing aides—sometimes labeled patient care
technicians, 3 while nurses take on the role of managing a team of caregivers.4 This trend IS typical of a
“reengineering” movement in hospital management known as patient-centered care or patient-focused
care—as opposed to department-focused care. Computer technologies—including computer-based
decision support tools and treatment protocols, online patient information systems, patient monitoring
devices, and teleconferencing systems—can support and assist people giving care in these new ways.
SOURCE: Office of Technology Assessment, 1995.
3 Wall Street Journal, Feb. 10, 1995, p. 61.4 M.L. Parsons and C.L. Murdaugh, Patient-Centered Care, A Model for Restructuring (Gaithersburg, MD Aspen Publishers,
1994)
ble for implementing complex policies resultingfrom a mix of research findings, technicalconstraints, and business priorities. Networkedinformation technologies may pose new chal-lenges to the traditional legal assumption that con-sumers are adequately protected against poorquality of care through the ability to file lawsuitsagainst their providers, and alternate guarantees ofhigh-quality care may need to be designed to re-place the current legal remedies.
Finally, information technologies are expen-sive to implement and their benefits may be diffi-cult to directly measure, even when all parties arehappy with the results. This may delay their de-
ployment in an industry whose sophisticated tech-nological base is seen by some to be a drivingforce in making health care more expensive.
TRENDS IN THE HEALTH CARE SYSTEM
❚ Aggressive Cost ManagementA major concern for providers, payers, policy-makers, and consumers alike is the rising costs ofdelivering care. Health care expenditures in-creased from 5.9 percent of gross domestic prod-uct in 1965 to 13.9 percent in 1993.2 Totalexpenditures for health care in 1993 were $884.2billion. Government sources pay for about 43 per-
2 Katharine R. Levit et al., “National Health Expenditures, 1993,” Health Care Financing Review, vol. 16, No. 1, fall 1994, pp. 247-294.

6 | Bringing Health Care Online: The Role of Information Technologies
cent of this total; the federal government alonepays nearly 32 percent. Health care is also a majorsegment of the economy, employing approxi-mately 10 million people, about 2.6 million ofwhom do primarily administrative work.3
As the costs of health care have continued torise, there have been concerns in government andin the industry itself about how to contain and re-verse the increase. In the 1990s, particularly in the103d Congress, a number of proposals were madefor far-reaching reforms in the health care indus-try. At the same time, within the health care andinsurance industries, many initiatives to controlcosts are already under way. In fact, perhaps due inpart to these efforts, the growth rate of health carecosts appears to have slowed during the 1990-93period.
One of the major influences in the health careindustry has been the growth of managed healthcare. “Managed care” is a somewhat nebulousterm, but generally refers to a “system of manag-ing and financing health care delivery to ensurethat services provided to managed care plan mem-bers are necessary, efficiently provided, and ap-propriately priced.”4 Managed care organizationsuse a number of techniques to control access toproviders, contain costs, manage utilization of re-sources, and ensure favorable outcomes for pa-tients.
The number of people enrolled in managed careplans has increased dramatically in the past 20years. By 1992, enrollment had grown to over halfof all employees covered by employer grouphealth insurance.5 As shown in box 1-2, the con-cept of managed care has expanded to includemany types of health plans and delivery systems.Many traditional fee-for-service health insuranceplans (those that reimburse members for health
care payments) are also using at least some caremanagement techniques to manage their costs.
❚ Integration of Health ServicesHealth care has historically been a very frag-mented industry. Routine medical care, crisismedical care, medical insurance, medical re-search, and management of public health typicallyhave been handled by entirely separate organiza-tions in business, government, and universities,and a large number of intermediary institutions aswell. There are more than 1.2 million health careproviders—ranging from solo practitioners to1,000-bed hospitals—and they are often isolatedin separate corporate entities from the more than3,000 private insurance payers that distribute pay-ments for health care services. The providers andinsurance companies are further isolated from themedical research community, government healthcare agencies, and public health organizations. Anetwork of private-sector intermediaries hasformed to facilitate the complicated relationshipsbetween the various organizations. It is unlikelythat any of these entities will be willing to collector organize data that save money or effort for someother organization, but deliver the intermediary noimmediate benefit; systemic savings may be irrel-evant in a vertically fractured industry.
Some of this fragmentation may be reducedwith the current trend toward vertical and horizon-tal integration of providers and payers into sys-tems that offer the full “continuum of care” tocovered populations. An integrated delivery sys-tem is one that brings together hospitals, primarycare providers, nursing homes, home health careproviders, pharmacies, and other services into asingle system through purchase, merger, jointventure, contract, or other means. As hospital ad-
3 U.S. Congress, Office of Technology Assessment, International Comparisons of Administrative Costs in Health Care, OTA-BP-H-135
(Washington, DC: U.S. Government Printing Office), September 1994.
4 Marrianne F. Fazen, Managed Care Desk Reference (Dallas, TX: HCS Publications, 1994), p. 149.5 U.S. Congress, General Accounting Office, Managed Health Care: Effect on Employers’ Costs Difficult To Measure, GAO/HRD-94-3
(Washington, DC: U.S. Government Printing Office), October 1993.

Chapter 1 Introduction, Summary, and Options 7
Managed care can refer to both the elements of managing care and the institutional structures within
which care is managed, To some, managed care means the use of management tools such as pread-
mission certification (for ensuring that only members who need hospital care are admitted to the hospi-
tal), concurrent review (ensuring that necessary and appropriate care is delivered during a hospitaliza-
tion), or financial Incentives or penalties for both providers and plan members. To others the term is
equated with alternative delivery systems that are variously known by names such as health mainte-
nance organization (HMO) or preferred provider organization (PPO).
In contrast to traditional fee-for-service or indemnity insurance plans where the insurer simply reim-
burses the insured individual for incurred health expenses and has no direct relationship with the pro-
viders of care, managed care organizations create a direct relationship between the insurer and the
provider of care, Whether physicians are salaried employees or contractors, they have a relationship
with the managed care plan wherein they give up some clinical and financial autonomy to that organiza-
tion. The consumer who joins a managed care plan also surrenders some freedom of choice. The HMO
or PPO in turn takes on a managerial role with the hope of containing costs and enhancing the quality of
care.
One concept used in certain forms of managed care is cavitation. Under capitated payment sys-
tems, providers receive a set payment per patient per period, regardless of the amount of services they
provide Providers who exceed their budgets will suffer losses. A second concept common to managed
care is the limitation on the patients’ choice of providers. Some plans only allow patients to choose from
a panel of providers associated with the plan (“closed panel”). Others permit patients greater flexibility,
but require patients to pay a higher share of costs when using outside providers. While the concepts of
capitation and Iimitations on the patient’s choice originated with early HMOs, they are now pervading
the whole health care industry, and many insurance plans, including traditional indemnity plans, may
include these features to some degree. Some managed care organizations have tighter controls—both
over payments and over patient-provider relationships; others maintain looser controls. Closed-panel
HMOs are generally the most restrictive, while independent practice associations (IPAs)—HMOs where
physicians work under nonexclusive contracts and may also have fee-for-service patients—are less so,
as are PPOs.
Managed Care and Cost SavingsAccording to recent studies, care management techniques reduce health care costs, primarily
through the reduced use of services. For example, the Congressional Budget Office (CBO) reports that,
compared to indemnity plans, closed-panel HMOs reduce the use of medical services by about 196
percent and IPAs reduce use by about 0.8 percent. The combined average effect of all HMOs is a re-
duction in services of 7.8 percent when compared with the current mix of indemnity plans. 1 Less restric-
tive types of managed care have not shown such significant reductions, according to CBO.
SOURCE: Adapted from U.S. Congress, Office of Technology Assessment, Understanding Estimates of National Health Expenditures
Under Health Reform, OTA-H-594 (Washington DC: U.S. Government Printing Office, May 1994), p. 76
1 U.S. Congress, Congressional Budget Office, The Effects of Managed Care and Managed Competition (Washington, DC Con-gressional Budget Office, 1995)

8 | Bringing Health Care Online: The Role of Information Technologies
missions and inpatient days have declined be-cause of cost control efforts begun in the 1980s,many hospitals have entered these other lines ofbusiness. Some integrated delivery systems arebeing organized by insurers or managed care orga-nizations.
❚ Increasing Value of Digital InformationNew patterns in health care delivery are enhancingthe value of clinical health data and creating in-centives for collecting and disseminating healthinformation electronically within and between or-ganizations. As managed care organizations growand fee-for-service care wanes, doctors and otherpractitioners have both a financial interest in de-livering low-cost care and incentives for docu-menting and analyzing their care practices.Administrators in Health Maintenance Organiza-tions (HMOs) and integrated delivery systemshave long sought to reduce transaction costs (afteran initial investment in equipment and software)by computerizing internal communications andautomating communications with suppliers andother business partners. In addition, they have avested interest in understanding the clinical de-tails of how care is delivered in order to efficientlymanage resources.
For example, it is possible to use administrativerecords alone to limit overuse of optometry ser-vices by approving eye examinations purely onthe basis of elapsed time since the last exam. How-ever, care can be more prudently and perhaps com-passionately managed by considering not only thetime of the last billing, but also the clinical recordof that visit and other health information about thepatient. Were the previous results normal, or didthey indicate a problem? Does the patient haveany other conditions that might warrant frequenteye examinations? Could the current complaint bedue to an adverse reaction to a prescribed medica-tion and, hence, warrant a visit to the prescribingphysician rather than an optometrist? This fine-grained analysis of clinical records is contingenton standardization and digitization of clinical re-cords because paper records are generally inade-quate for these purposes.
Finally, the government has a stake in helpingto develop inexpensive, standardized approachesto information exchange so it can effectively fundmedical research, manage widespread publichealth problems, reduce its administrative costs,and reduce the cost of the health care it purchasesand provides through Medicare, Medicaid, veter-ans’ care, and employee insurance programs. Anindication of the magnitude of this interest is thedesignation of health care applications as a keycomponent of the National Information Infra-structure (NII) by the Administration’s Informa-tion Infrastructure Task Force (IITF). Appointedby the President, the IITF is comprised of high-level representatives of the federal agencies thatplay a role in developing and applying informa-tion and telecommunications technologies. TheIITF’s Committee on Applications and Technolo-gy coordinates efforts to develop, demonstrate,and promote applications of the NII and developsand recommends technology strategy and policyto accelerate its implementation. One part of thiscommittee is the Health Information and Applica-tions Working Group. This group is again dividedinto subgroups in the categories of telemedicine,consumer health information, standards, andemergency medicine.
These private and governmental interests indigitizing health information in order to managecosts and integrate delivery of health services aremanifest in a slow but perceptible trend towardstandardization of health care information and op-timization of care delivery. These processes areoccurring on many levels. The medical and com-puting communities are slowly developing: a)lexicons for consistently describing medical care,b) consensus standards for exchanging medicaldata between computers, and c) models for how tocollect and organize medical information digital-ly. Protocols for standardizing delivery of care andmetrics for measuring the quality of health careservices are being developed, as well as decisionsupport systems that may increase the efficacy ofmedical decisions. And throughout the health caredelivery system, innovative applications of in-

Chapter 1 Introduction, Summary, and Options | 9
formation technologies are being studied, tested,and implemented.
CONGRESSIONAL INTERESTRecognizing the changes occurring in both healthcare and telecommunication technology and theirrelevance to the congressional agenda, the Chair-man of the Senate Committee on Labor and Hu-man Resources asked the Office of TechnologyAssessment (OTA) to conduct a study on the im-pacts of information technology on the health caresystem. The request was supported by the Chair-man of the House Committee on Energy andCommerce.6
Recently, there have been numerous legislativeinitiatives addressing aspects of incorporating in-formation technologies into the delivery of healthcare. In the 103d Congress, several comprehen-sive health care reform bills were introduced,7 andthis pattern has continued in the 104th Congress.These bills seek to restructure various aspects ofthe payment and insurance framework of thehealth care industry, but, in addition, they oftenspecify procedures for simplifying administrationof health care delivery through the use of informa-tion technologies. For example, several recentbills direct the Secretary of the Department ofHealth and Human Services (DHHS) to adopt uni-form standards for various medical data, based onthe work of standards committees accredited bythe American National Standards Institute and onthe advice of groups such as the Workgroup forElectronic Data Interchange and the Computer-Based Patient Records Institute.8
The bills call for standards for:
1. defining common sets of data elements to bestored electronically in patient records,
2. performing administrative transactions,3. assigning uniform patient and provider identi-
fication numbers,4. assigning codes to medical procedures and de-
scriptions,5. applying electronic signatures, and6. ensuring patient privacy and data security.
Most bills specify the adoption of the standardsby DHHS within two years or less, and, followingthe adoption, provide various measures designedto encourage rapid adoption of the standards bynearly all health care providers. These measuresmay include direct incentives, such as require-ments that all health plans implement the stan-dards for all transactions, or indirect incentives,such as requirements that all transactions regard-ing Medicare patients be filed electronically. Theincentives may also be provisional: they may di-rect the Secretary to assess whether sufficientnumbers of health plans are utilizing the standardsand to require full participation, should it prove tobe cost-effective. Most bills include exceptionsfor small hospitals and those that can show theyare in the process of installing an adequate in-formation system. Some of the bills override statelaws requiring the maintenance of paper-based pa-tient records.
Several bills seek to establish national or statedatabases of health information for quality assess-ment purposes, control of fraud, or tracking dis-ease patterns.9 Other bills would authorize grants
6 This committee is now known as the House Committee on Commerce.7 Two examples are U.S. Congress, Senate, S. 1757, Health Security Act, and S. 1494, Health Care Information Modernization and Security
Act of 1994 (Washington, DC: U.S. Government Printing Office, 1994).
8 U.S. Congress, House of Representatives, H.R. 1200, American Health Security Act of 1995 and H.R. 1234, Basic Health Care Reform Actof 1995 (Washington, DC: U.S. Government Printing Office, 1995); and U.S. Congress, Senate, S. 7, Family Health Insurance Protection Act(Washington, DC: U.S. Government Printing Office, 1995).
9 U.S. Congress, House of Representatives, H.R. 798, Veterans’ Benefits, Title 38 U.S.C., Amendment (Washington, DC: U.S. Government
Printing Office, 1995), and H.R. 1200 and S. 7, ibid.

10 | Bringing Health Care Online: The Role of Information Technologies
for rural telemedicine efforts10 or establish a tele-medicine commission to formulate plans forwidespread implementation of telemedicine.11
Finally, there have been efforts in both the 103dand 104th Congresses to reform and deregulatetelecommunications.12 Such reforms may affectthe price of telecommunications services and,therefore, help determine the feasibility of incor-porating telecommunications into health care de-livery on a large scale. In addition, current billshave certain direct influences on health care, in-cluding a requirement that prices for telecommu-nications service to rural health care providers becomparable to those for urban providers.13
REPORT SUMMARY
❚ Scope of the AnalysisIn chapters 2 through 5, this report discusses someof the challenges and opportunities for using in-formation technology to improve the health caresystem. First, it addresses the potential impact ofinformation technologies on health care deliveryand introduces a variety of technologies that arebeing used to collect, organize, and share clinicalinformation needed for providing patient care.The report then explores the exchange of healthinformation for administrative purposes amongthe many stakeholders including providers, payers,employers, consumers, and government agencies.It discusses how the quality of health care mightbe improved by providing health care profession-als with high-quality information and decisionsupport tools at the point of care. Finally, the re-port explores the potential for addressing the
needs of those in rural or other underserved areasthrough telemedicine.
Advanced information technologies offer anarray of other possibilities for influencing deliv-ery of health care services. It was impossible to ad-dress all applications in this report. Those selectedwere viewed as having the most potential for de-creasing costs and improving quality and access inhealth care. Particular emphasis is placed on ad-ministrative simplification, quality assessment,and telemedicine, as specified by the congression-al committee requesting the report. The report alsobriefly mentions the potential for telecommunica-tions to assist consumers in becoming better in-formed and more involved in decisions affectingtheir health care, and points to the need for addi-tional study. Emerging applications of informa-tion technology, including remote surgery andvirtual reality applications, were not considered,nor were issues related to the reform of medicaleducation to include greater use of informationtechnology. These are, however, fertile areas forfuture research.
Before computers were introduced into thehealth care delivery system, clinical and adminis-trative records were kept separately in paper form,patient utilization of services was rarely scruti-nized systematically, and clinical information wasseldom exchanged between business organiza-tions (or even among the various clinicians an in-dividual might see). Thus, paper-based technolo-gies and common organizational policies workedalong with various state laws to provide an ad hoclevel of protection for individual privacy that isclearly inadequate in the emerging world of com-
10 U.S. Congress, House of Representatives, H.R. 851, Rural Telemedicine Act of 1995 (Washington, DC: U.S. Government Printing Office,
1995), and U.S. Congress, Senate, S. 7, op. cit., footnote 8.
11 U.S. Congress, House of Representatives, H.R. 426, National Committee on Telemedicine Act (Washington, DC: U.S. Government Print-
ing Office, 1995).
12 U.S. Congress, House of Representatives, H.R. 3626, Antitrust and Communications Reform Act of 1994; Antitrust Reform Act of 1994(Washington, DC: U.S. Government Printing Office, 1994), and U.S. Congress, Senate, S. 1822, Communications Act of 1994; Telecommunica-tions Equipment Research and Manufacturing Competition Act of 1994, and S. 2111, Telecommunications Services Enhancement Act of 1994(Washington, DC: U.S. Government Printing Office, 1994).
13 U.S. Congress, Senate, S. 652, Telecommunications Competition and Deregulation Act of 1995 (Washington, DC: U.S. Government
Printing Office, 1995).

Chapter 1 Introduction, Summary, and Options | 11
puterized patient records, integrated delivery ser-vices that operate on a nationwide basis, andinstant electronic messaging. New combinationsof legislative protections and technical safeguardswill be necessary to protect individual privacy ashealth care information is computerized and stan-dardized. These issues are discussed brieflythroughout this report, but were discussed in de-tail in the OTA report Protecting Privacy in Com-puterized Medical Information.14
The issues and policy options that emerge fromeach chapter of this report are briefly summarizedin the sections that follow. First, however, two keythemes are introduced that echo throughout thechapters. These are cost containment and stan-dards development, and they reflect congressionalconcerns about containing health care costs andenabling administrative simplification that aremanifest in the bills of the 103d and 104th Con-gresses.
❚ Cost ContainmentReducing the cost of delivering health care is per-haps the prime motivation for congressional inter-est in exploring the use of information technology.Anticipated cost savings are based on analogousreductions in transaction costs for industries suchas banking—which built information infrastruc-tures supporting automated teller machines andpoint-of-purchase credit card verification—andon the increase in productivity and product qualityin domestic manufacturing industries associatedwith just-in-time inventory control, continuousquality improvement, and other techniques thatare highly dependent on information technolo-gies. Although similar efficiencies and improve-ments may be possible within the health care
system, the magnitude of the savings is very diffi-cult to predict for several reasons.
Most cost containment predictions maintainthe traditional fault line between administrativeinformation and clinical information. Administra-tive processes include activities such as transmit-ting and processing claims, utilization review,purchasing supplies and tracking inventory, pay-ing bills, managing internal finances, negotiatingcontracts, complying with regulations, and con-trolling quality. Administrative costs of providinghealth care have been estimated at between $108billion and $135.1 billion per year in 1991,15 orbetween 12 and 15 percent of the health care bill.Estimates of annual savings that could be realizedthrough increased use of information technologyin administrative functions have ranged from $5billion to $36 billion,16 or enough to reduce ad-ministrative costs between 0.5 and 3.6 percent.
These estimates, discussed in more detail inchapter 3, may be somewhat optimistic becausethey assume rapid adoption of electronic data in-terchange and high rates of market penetrationthat do not appear to be materializing. The deeperproblem with such predictions is that they areoften based on merely converting all transactionswithin the existing system of fee-for-servicehealth care to electronic form. However, the shift-ing landscape of health care delivery patterns can-not be treated as a perturbation within a more rapidprocess of digitizing health information. Suchdigitization did not happen over the past two de-cades despite the availability of increasingly capa-ble computer and telecommunication systems;indeed, several organizational and technologicalimpediments (discussed in chapter 2) make it like-ly that widespread digitization will happen only in
14 U.S. Congress, Office of Technology Assessment, Protecting Privacy in Computerized Medical Information, OTA-TCT-576 (Washing-
ton, DC: U.S. Government Printing Office, September 1993).
15 Allen Doubloon and Matthew Bergheiser, “Reducing Administrative Costs in a Pluralistic Delivery System Through Automation,” pre-
pared by Lewin-VHI for the Healthcare Financial Management Association, Apr. 30, 1993.
16 Project HOPE, Center for Health Affairs, “Estimating the Cost-Effectiveness of Selected Information Technology Applications,” unpub-
lished contractor report prepared for the Office of Technology Assessment, March 1995.

12 | Bringing Health Care Online: The Role of Information Technologies
synergy with the progressive adoption of man-aged health care practices and development of in-tegrated service delivery systems.
A second class of economic considerationsconcerns the effectiveness of encouraging specificinformation technology implementations. Theseare of concern to Congress for purposes of guidingprocurement decisions and research priorities. Inrecent years, the field of economic evaluation ofmedical technologies has expanded rapidly. Ris-ing spending on health care has stimulated the useof formal techniques such as cost-effectivenessanalysis and cost-benefit analysis to assess thecost and health effects of using particular medicaltechnologies.
Cost-effectiveness analysis (CEA) has emergedas the most popular technique for economic evalu-ations. CEA involves a structured, comparativeevaluation of two or more health care interven-tions. Analyses are designed to show the relation-ship between resources used (costs) and healthbenefits achieved (effects) for given technologiesor programs. In CEA, the cost per specified healtheffect, such as lives saved or quality-adjusted life-years saved, is calculated for particular technolo-gies or programs. If the ratio is measured similarlyfor different technologies or programs, the costper effect can be compared. Formal CEA involvesa number of explicit steps, including:
1. identifying the perspective of the study,2. identifying the competing interventions,3. defining costs,4. defining effects,5. discounting future costs and effects to their
present value,6. adjusting for quality-of-life factors,7. analyzing the incremental costs and conse-
quences of one option over another, and8. examining uncertainties underlying
the analysis.
In cost-benefit analysis (CBA), the net costs ofan intervention are compared with the net savings:the benefits of a program or technology are ex-pressed entirely in monetary terms. Because thebenefit of medical technology generally involveshealth effects such as life-years saved, CBA re-
quires that these effects be valued in monetaryterms. One of two techniques—the human capitalapproach or the willingness-to-pay approach—isgenerally used to measure benefits. The humancapital approach considers the value of a humanlife by estimating an individual’s projected futureearnings. The willingness-to-pay approach con-siders how much individuals are willing to pay fora reduction in the risk of death or illness.
Applying the formal techniques of CEA andCBA to information technology applications inhealth care is difficult for a number of reasons.Some of the difficulties are general to all medicaltechnologies: the competing alternatives for atechnology are not always known; a technologymay be cost-effective in some patient groups andnot in others; technologies constantly undergochange; there are no standards on how to definecosts (e.g., whether and how to consider indirectcosts such as productivity losses, or intangiblecosts such as pain and suffering); there are no stan-dards regarding the length of patient followuptime to consider; analysts differ in their use ofmethodologies by which to adjust health effectsfor quality-of-life factors; and there are many un-certainties underlying such analyses. A generalproblem with CBA involves trying to place amonetary value on reductions in mortality or mor-bidity.
Beyond these general difficulties, evaluatinginformation technologies presents some uniqueproblems. It is difficult to conduct comparativestudies because system features and levels of ser-vice vary widely across institutions and users. Inaddition, many applications have been in exis-tence only a short time. Information technologiesand applications change frequently, making anal-yses difficult—and making even some well-con-ducted analyses quickly obsolete. In general, it isdifficult to identify and quantify appropriatecosts, savings, and health effects. For most evalu-ations of information technology, direct costswould include equipment and operating costs, thevalue of the technician’s time, and the cost ofmaintaining equipment. However, it is hard to ac-curately identify and quantify indirect costs such

Chapter 1 Introduction, Summary, and Options | 13
as productivity gains or losses. In general, it isvery difficult to tie the use of information technol-ogies to health consequences.
As a result of these limitations, most existingeconomic evaluations do not constitute formalcost-effectiveness or cost-benefit analyses. Instead,most have attempted to estimate savings in termsof productivity gains to the system. Some havealso speculated about how various applicationswill ultimately influence patient care. The designand scope of such analyses vary widely acrossstudies, as does the level of rigor.
Congressional OptionsRecognizing that implementation of informationtechnologies will bean incremental process, Con-gress may wish to attempt to evaluate the possiblesystemic savings associated with implementationof information technologies in a way that recog-nizes the shifting patterns of health care delivery.Alternatively, Congress could evaluate, for ad-ministrative purposes, the costs and benefits ofimplementing various specific technologies orsets of technologies. These are difficult chal-lenges. However, should Congress wish to pursuesuch analyses, it could direct agencies or congres-sional support services to implement one or moreof the following options:
Analyze systemic savings that mightbe associated with implementation of informationtechnologies and related changes in health care deliv-ery systems using realistic estimates for the pace of im-plementation.
Conduct or fund research to evaluatethe costs and effectiveness of individual informationtechnologies, such as order-entry systems, clinical pro-tocols, and electronic interchange of claim and pay-ment information.
Evaluate the potential for synergies be-tween information technologies by funding research inthe implementation of multiple simultaneous applica-tions in test and control facilities.
Establish baseline data for the costs ofcurrent information structures in the health care deliverysystem so that future implementations can be objec-tively evaluated.
Given these possibilities for cost-benefit analy-ses and systemic cost analyses, it should be notedthat some stakeholders who contributed to this as-sessment indicated that rigorous cost-benefit orcost-effectiveness analyses would not play a ma-jor role in their decisions to implement informa-tion technologies. Rather, these technologies andsystems of technologies were considered by manystakeholders to be as fundamental and as immuneto cost-benefit analysis as the telephone: adoptionof the technologies would be necessary to remaincompetitive in the health care industry.
■ Standards DevelopmentThe second major theme that recurs throughoutthis report is the central role of standards develop-ment for systematizing the compilation and ex-change of health care information. One value ofdigitized health information is that it can be ma-nipulated quickly and accurately by computerswithout human intervention. The accuracy, speed,and cost of machine-processing are adversely af-fected by novelty, diversity, and frequent changesin the rules. Until standards are in place and com-pliance is widespread, costly activities—such asmaintaining multiple formats for health care in-formation, dealing with exceptions, and develop-ing new interface software as new proprietaryapproaches to managing health information be-come fashionable—will continue to offset somepotential savings of processing health care recordsand transactions electronically.
Standards development is an ongoing process.A number of organizations are working on stan-dards for the content and format of electronichealth information. Standards for the format ofbilling and core insurance transactions are welldeveloped, and the Health Care Financing Ad-ministration (HCFA) has adopted some of them.Another area of standardization that could facili-tate electronic transactions is a system of unique

14 | Bringing Health Care Online: The Role of Information Technologies
identifiers for individuals, providers, and sites ofcare. At present, each provider uses its own num-bering system, which can create confusion whenhealth information is exchanged between differ-ent institutions.
The development of technical standards is pri-marily a private-sector activity. However, it couldbe accelerated through federal participation in de-veloping standards that would encourage in-formation exchange and protect the privacy ofparticipants in the health care system, and throughexpeditious implementation of such standards inall federal health care matters as a catalyst fortheir adoption by the private sector. This shouldnot be construed as a call for federal agencies toindependently establish standards for implement-ing information technologies—such efforts wouldalmost certainly fail to meet the needs of variousstakeholders. Rather, federal agency participationin existing standards activities would preempt du-plicative development of federal regulations andrequirements. Further discussion of standards ap-pears in individual chapters of this report.
❚ Information Technologies forTransforming Health Care
The potential for new computing and telecommu-nications technologies to reduce the cost of deliv-ering health care, while facilitating broad structur-al changes in the health care industry, may presagea rapid expansion in the application of informa-tion technologies to the health care system. Chap-ter 2 charts the technological and organizationalfactors that will help guide the path of that expan-sion should it occur.
Policy IssuesMany of the practical frustrations encountered byparticipants in the health care system can be tracedto the inability of current information systems toprovide accurate, timely information where it isneeded in the health care process. Poor informa-tion mobility has become an impediment to effi-cient delivery of high-quality health care. Thisimpediment becomes more prominent, expen-sive, and problematic for health care delivery or-
ganizations as they grow larger and morecomplex. One approach to solving this problem isto liberate health information from its traditionalpaper medium by creating, transmitting, and proc-essing it through more flexible electronic means.Electronic information can be used again andagain, in different forms for different purposes. Itcan be reformatted easily and transmitted cheaplyonce the infrastructure to do so is in place.
Chapter 2 identifies the broad currents of in-formation flowing within the health care system,and then describes various approaches to comput-erizing clinical information within hospital andambulatory care units. One portion of this clinicalinformation is the patient’s medical record, whichhas conventionally been kept as a thick folder ofpaper forms and films. The chapter describes thedesign of paper recordkeeping systems and thereasons they are inadequate for documenting carein an integrated health care delivery organization.It discusses ways that this information might bedigitized and then disseminated (with appropriatesecurity measures) through standardized commu-nications protocols.
A diverse suite of key computer and commu-nication technologies supports the digitizationand dissemination of clinical records. The chapterdescribes technologies for: a) capturing data asit is generated by caregivers and the machinesthey use to monitor and treat the patient; b) com-pressing, storing, securing, and retrieving data;c) networking and telecommunications technolo-gies sharing information; and d) refining data andcomparing data streams so computers can supportmedical decisionmaking. Insight and wisdommust somehow be culled from an overwhelmingflood of bits and bytes.
This suite of advanced information technolo-gies is also the context for discussions in subse-quent chapters of the report that addressadministrative health data management, qualityassessment and decision support, and deliveringhealth care services and information at a distance.
Congressional OptionsMany of these core technologies have been devel-oped by the private sector for nonmedical pur-

Chapter 1 Introduction, Summary, and Options | 15
poses and will be adopted within the health caresystem as needed. Nonetheless, Congress maywish to consider certain policy options that couldencourage harmony in how that adoption pro-ceeds.
Support standards-setting activities.
Congress could direct relevant agencies to sup-ply personnel to actively participate in standards-setting meetings. This would proactively obviateany federal regulatory activity that might be atodds with consensus standards by making surethat government interests are represented withinthe standards-setting process. Congress couldalso provide financial support for the process, in-cluding funding research support to help resolveany technological roadblocks that impede stan-dards development. Congress could also directfederal agencies to set aggressive schedules forimplementation of consensus standards in theirown health care delivery and administrative acti-vities as a catalyst for similar private-sector ac-tion.
Fund and coordinate research efforts toovercome specific technological barriers.
These efforts could include research into hu-man-computer interface technologies for use inhealth care settings and research into large-scale,open architecture implementations of informationtechnologies in health care settings.
Coordinate federal efforts to implementhealth care information technologies.
The agencies or committees charged with thiscoordination could:
1. establish procedures for expediting approvaland distribution of medical software;
2. establish mechanisms (or support similar pri-vate-sector efforts) for reviewing and dissemi-nating clinical protocols;
■
advise Congress on specific needs of the medi-cal, technical, and consumer communities withrespect to legislation establishing regulationsand policies pertinent to information technolo-gies; andset national standards for patient and institu-tional identification numbers and security pro-cedures to be used with patient records.
Networks for Health AdministrationChapter 3 explores the exchange of healthinformation among the many stakeholders—pro-viders, payers, employers, consumers, and govern-ment agencies—particularly for administrativepurposes.
Policy IssuesAs part of a larger effort to reduce costs, improvequality of care, and improve access to health care,efforts to effect administrative efficiency throughgreater use of electronic commerce in health careare an important component. Today, about 75 per-cent of hospital claims are submitted electronical-ly, the vast majority of these being Medicareclaims submitted to HCFA. Physicians submitsome 47 percent of their Medicare claims elec-tronically, but only about 16 percent of totalclaims. 17 Between some payers and providers, the.process of billing and being paid has been totallyautomated, with the organizations exchangingelectronic claims, remittance advice (documentsthat explain how much of the claim is paid), andelectronic funds transfers. However, such levelsof automation are still unusual. Electronic claimservices help providers deal with the multitude ofdifferent formats and requirements of payers.They offer software and services for translatingand reformatting claims and other electronictransactions among the 400 or so different sys-tems in use.
Compared with a paper-based system, it ap-pears that electronic information reduces costs forsome users. Most of the estimates for savings re-
17 “Automated Medical Payments Statistical Overview,” Automated Medical Payments News, Feb. 8, 1993, p. 3.

16 | Bringing Health Care Online: The Role of Information Technologies
sulting from the use of information technology arebased on cost reductions in payer-provider trans-actions resulting from automation in a fee-for-ser-vice environment. Managed care organizationscan have equivalent transactions that presumablywill cost less using information technology. How-ever, the major savings that are expected to accruefrom managed care come from better managementof both resources and patient and clinician behav-ior—for example, reduction of unnecessary ser-vices. Information technology should assist in thisas well. For example, having up-to-date patient re-cords available at the point of service should re-duce duplicate testing or the provision ofnonallowed treatments. While it has been arguedthat information technology fosters better man-agement, actual evidence of its contributions tocost reduction in this area is difficult to find.
Community health information networks(CHINs) facilitate exchanges of clinical or admin-istrative data among providers and payers in a par-ticular community or region. CHINs can helpoffset the lack of standardization by providingtranslations and interfaces between incompatiblecomputer systems used by different network sub-scribers. Some networks, often called CHMISs(Community Health Management InformationSystems), may also maintain a repository of ad-ministrative information for use in performingoutcome research and quality assessments of pro-viders and insurance plans in the community. Atthis point it is not clear whether community net-works, which offer service to competing providersin the community, will survive as more verticallyintegrated health care organizations build propri-etary information networks.
While exchanging health information electron-ically offers advantages, it also raises fears thatprivacy and confidentiality of health informationmay not be protected. Many consumers alreadyfear that too many people have access to theirhealth information. Most information needed forhealth care administrative transactions comesultimately from the patient record. Clinical in-formation in coded, abstracted form becomes ad-ministrative information. The provider attemptsto capture, either through manual or automated
means, everything that is done for the patient dur-ing a stay or visit, and to document informationabout resource utilization and costs in order toprepare an appropriate bill. Electronic patient re-cords are under development in many locationsthroughout the country. In addition to technologi-cal and organizational barriers, there are a numberof regulatory and legal barriers to complete imple-mentation of electronic patient records, includingconflicting state laws and regulations about howpatient records must be maintained and the wayprivacy and confidentiality of records should beprotected.
Health information is not limited to the patientrecord. Rights of patient access and procedures forprotection of privacy and confidentiality are notclearly defined for secondary and tertiary users ofhealth information (e.g., payers, researchers, andorganizations maintaining health data reposito-ries) under federal or most state laws. While mosthealth care is local, in that people usually see care-givers in their own communities, health informa-tion often needs to cross state lines because thepayer, provider, patient, and/or employer may bein different states.
Congressional OptionsSavings may be available to the health care systemas a whole as a result of universal implementationof electronic medical payments. However, at cur-rent implementation rates, universal compliancemay not be achieved for some time, if ever. Get-ting started with electronic commerce requires asolid organizational commitment and a signifi-cant investment in equipment, software, processredesign, and education, but some organizationshave weak financial incentives to make the invest-ments needed to institute electronic payments.Others are forging ahead, unwilling to wait forstandards. The health care industry in the UnitedStates is not organized as a “system” with a centralfocus or consensus on how to deal with system-wide problems. The different parts of the frag-mented system have diverse incentives, andefforts by participants to control costs in their ownarea can tend to increase costs elsewhere. How-ever, these shifted costs are so subtle and spread

Chapter 1 Introduction, Summary, and Options | 17
over so many participants in a complex systemthat they are difficult to quantify.
The federal government has provided someleadership in helping the health care industrymove toward greater use of electronic informa-tion, and may wish to continue this leadershiprole. There are three major areas in which govern-ment action might be considered: 1) providingleadership in the adoption of standards for elec-tronic medical payments and other transactionsand exchanges of health information; 2) establish-ing a system of unique identifiers for people, pro-viders, and payers; and 3) establishing a moreconsistent regulatory environment for interstateexchanges of health information.
Continue to influence the standardiza-tion of health care information primarily through the fed-eral government role as a major insurer.
The Health Care Financing Administration’s(HCFA’s) adoption of claims submission stan-dards, along with incentives such as faster pay-ment of electronic claims, has already beeninstrumental in encouraging some payers and pro-viders to begin use of electronic payment systems.
Require the adoption of industry-devel-oped standards for core electronic transactions, in-cluding minimum and maximum data sets, and settimetables for their implementation.
If it is believed that HCFA’s influence alonewill not ensure high enough levels of participationin a standardized electronic health payment sys-tem, then a more active federal role may be con-sidered. A corollary to this option may be:
Charge a government agency with re-sponsibility and authority to set standards and data def-initions for administrative transactions in consultationwith industry groups, and to manage changes to stan-dards over time; alternatively create an agency or com-mission for this purpose.
Establish a system of unique identifiersfor patients, providers, and sites of care.
A national system of electronic commerce forhealth information will operate more smoothly ifthere is a better system for uniquely identifyingparticipants in that system, both to prevent du-plication and loss of information and to facilitatecoordination of benefits when multiple providersand payers are involved in a patient’s care. Be-cause of its national reach, the federal governmentmay be in the best position to establish systems ofidentifiers.
In order to create a consistent legal and regula-tory environment for electronic health informa-tion, Congress may wish to consider the followingoptions:
Encourage the passage of uniformstate legislation with regard to privacy and confidential-ity allowable storage media, and standards for healthinformation.
A number of industry groups have been work-ing with state governments to encourage adoptionof uniform legislation, and the Department ofHealth and Human Services has been assigned thelead role in designing model state privacy laws.An alternative or supplement to this option maybe:
Establish federal legislation and regula-tion regarding privacy and confidentiality of medical in-formation, storage media for patient records, andstandards for storage and transmission of medical in-formation.
Additional federal legislation may be neces-sary as a framework for state legislation, or to re-place state laws, if the process of revisinglegislation on a state-by-state basis is seen as inef-fective or too time-consuming.
Charge a government agency with re-sponsibility to oversee the protection of health caredata; provide ongoing review of privacy issues; keepabreast of developments in technology security mea-sures, and information flow; and advise Congressabout privacy matters in the area of health care informa-tion.

18 | Bringing Health Care Online: The Role of Information Technologies
Because of the importance of privacy and con-fidentiality to the public, the continually changinguses for health information, and the constantlychanging nature of threats to privacy and confi-dentiality, it may be necessary to establish one or-ganization as an ongoing locus of responsibility.
❚ Improving the Quality of Health CareChapter 4 finds that advanced informationtechnologies—computer-based patient records,structured data entry, advanced human-computerinterface technologies, portable computers, auto-mated data capture, online query, knowledge-based information systems, and computernetworks—can potentially improve the quality ofhealth care by enhancing clinical decision sup-port, and by improving data for assessing both theeffectiveness of health services and the perfor-mance of health care providers and insuranceplans.
Information technologies could facilitate fasterand easier collection of information about the pa-tient and the health problem at hand. Portions ofthat information could be entered by clinicians ator near the point of care, captured directly fromdiagnostic and monitoring equipment, or enteredby the patient prior to care. Technologies such asrelational databases with online query could sup-port faster and easier search and retrieval of pre-viously collected information about the patient, aswell as information from local or remote knowl-edge bases. Development of computer-based clin-ical protocols and other forms of clinical decisionsupport systems (CDSSs) that apply decisionrules and other knowledge-based approaches toinformation about the patient and health problemat hand could recommend diagnoses, tests, treat-ments, and preventive care. They could also leadto more rigorous construction and analysis ofmeasures of service effectiveness and perfor-mance of providers and plans. Computer net-works, high capacity telecommunications,advanced human-computer interface technolo-gies, and improved graphics software could leadto more flexible organization and display of thisinformation as appropriate for individual clini-
cians, and more rapid and widespread dissemina-tion of the results of performance measures tovarious parties.
Empirical evidence demonstrating the abilityof these technologies to achieve these goals is lim-ited, mixed, or incomplete. Moreover, concernshave been raised about possible adverse effects onthe quality of health care arising from thesetechnologies, including:
1. incorrect parameters or criteria, or omitted oraltered steps, in CDSSs that could lead to inap-propriate care;
2. excessive reliance on monitoring equipmentand CDSSs, which could undermine the abilityof clinicians to exercise professional judgmentin nonroutine cases and reduce the interperson-al aspects of patient care (the “quality of car-ing”); and
3. the temptation to use readily available adminis-trative data for assessing the effectiveness ofspecific health services or the performance ofproviders or insurance plans.
If the data are incomplete or inaccurate, the re-sults could be misleading.
Policy IssuesThe private sector has been largely responsible forthe development and application of informationtechnologies in clinical decision support and per-formance assessment of health care providers andinsurance plans. The federal government’s rolehas mainly involved:
1. developing information systems and perfor-mance measures for its own health insuranceand health care delivery programs, most nota-bly Medicare;
2. funding of intramural and extramural researchand demonstration projects; and
3. participating in voluntary standards-setting ac-tivities with private-sector organizations.
All of these activities in both the private andpublic sectors are likely to continue, with some in-creasing and others decreasing. In an era of bud-getary and regulatory restraints, however, majornew government initiatives, such as funding for

Chapter 1 Introduction, Summary, and Options | 19
technology development or mandated regulationof clinical information systems, are unlikely. Itcan be argued that this is appropriate—in otherwords, that the federal government should not in-terfere in private market decisions regarding theselection of new technologies or their applica-tions.
On the other hand, the federal government—specifically HCFA—is responsible for ensuringtight the quality of health care rendered to Medi-care and Medicaid beneficiaries.18 Recent effortsto move more beneficiaries into managed carehave underscored quality concerns, given the ex-pectation that cavitation creates an incentive forunderservice. 19 Several policy issues regardingthe potential impact of information technology onthe quality of care delivered to Medicare and Med-icaid beneficiaries deserve the attention of federalpolicymakers.
The foremost issue is the extent to which clini-cal information systems actually change clinicalpractice patterns and patient outcomes, and wheth-er those changes are beneficial to providers andpatients. Empirical research on this issue remainslimited, mixed, or incomplete, and more solid evi-dence regarding these impacts needs to be ob-tained. To pursue such research, Congress couldconsider the following options.
Congressional Options
Maintain or increase funding for intra-mural research and extramural grants and contracts toprivate-sector organizations for research and demon-stration projects designed to:
develop and test the reliability and validity ofvarious methods of measuring and assessing(with risk adjustment) the performance of pro-viders and health plans;develop, implement, and evaluate specific sys-tems of risk-adjusted performance indicators;
■ evaluate the effectiveness and safety of clinicalinformation systems, including CDSSs.
Maintain or increase funding for HCFAto develop and evaluate performance assessmentmethods and systems suitable for Medicare and Med-icaid enrollees, using intramural research and extramu-ral grants and contracts to private sector organizationsfor research and demonstration projects as needed.
Assign the task of coordinating the de-velopment and evaluation of performance assessmentmethods and systems and clinical information systemsto a single federal agency.
Reduce funding for development andevaluation of performance assessment methods andsystems and clinical information systems, and directHCFA to employ performance assessment methodsand systems developed and evaluated in the privatesector with minimal adaptation.
Until more solid evidence is available regard-ing the effectiveness and safety of existing clinicalinformation systems and the reliability and validi-ty of performance assessment systems, more dras-tic action—such as mandating the testing andcertification of ail such systems—is probably notjustified. Legal questions regarding who shouldbe held liable in situations in which such systemslead clinicians to make decisions that harm pa-tients are probably best left to the courts to re-solve.
Assuming that clinical information systems arefound to be effective and safe in terms of their im-pacts on practice patterns and patient outcomes,the next set of issues focuses on the most efficientmeans of developing and implementing those sys-tems.
One issue regarding government involvementin the development of standards and technologyconcerns the classification and coding of healthservices. Many major payers currently employ
18 The state governments share responsibility for the Medicaid Program with the federal government.19 Given a fixed payment per plan member, providers may be tempted to minimize the volume and/or intensity of services rendered for each
patient.

20 | Bringing Health Care Online: The Role of Information Technologies
two separate systems for coding health services:ICD-9-CM 20 for billing by inpatient hospitals andother institutional providers, and CPT-421 for“professional” billing by clinicians and other non-institutional providers and suppliers.
For payment and other purposes, services ren-dered by a clinician in an inpatient setting must becoded using both of these systems, creating addi-tional costs for providers. For many services,however, the codes in ICD-9-CM cannot beequated (“crosswalked”) with those in CPT-4 be-cause of substantial structural differences betweenthe two coding systems. Moreover, bothICD-9-CM (Vol. 3) and CPT-4 have serious tech-nical limitations, such as overlapping and duplica-tive codes and inconsistent and noncurrent use ofterminology. Most importantly, neither has ade-quate room for expansion, so both are running outof codes as new services are created or differentuses of existing services are distinguished. In ad-dition, neither system provides sufficient clinicaldetail to support the creation of the kinds of data-bases required to accurately assess patient out-comes using advanced information technologies.
Citing these and other problems, the NationalCommittee on Vital and Health Statistics, an advi-sory body to the Secretary of Health and HumanServices, has recommended developing a unifiedclassification and coding system for health careservices. 22 However, in 1994, even HCFA reaf-firmed its intention to continue this dual codingsystem policy in its Medicare and Medicaid pro-grams, despite the substantial barriers this posesto efficient information processing and analysis.
Provide additional funding for intramu-ral and extramural research on the feasibility of devel-oping a single classification and coding system that
could be applied to all health care services performedby all providers in all settings.
Establish a new executive branch pro-gram to develop a unified service classification andcoding system.
Once a unified service classificationand coding system is developed, mandate that all fed-era/ agencies that manage health insurance and healthcare delivery programs use that system in those pro-grams.
Provide minimal funding for monitoringand facilitating private sector development of a unifiedservice classification and coding system.
■ Telemedicine: Remote Access to HealthServices and Information
Telemedicine can be broadly defined as the use ofinformation technology to deliver medical ser-vices and information from one location to anoth-er. The use of telecommunications to deliverhealth care services and exchange information isnot new. Chapter 5 discusses how recent techno-logical advances—such as fiber optics, integratedservices digital networks, and compressed video—have eliminated or minimized some of theproblems (e.g., poor quality images and slowtransmission speeds) that limited earlier applica-tions.
Currently, there is much interest in the potentialof telemedicine to lower costs, improve quality,and increase access to health care, especially forthose who live in remote or underserved areas. Pi-lot tests are also under way to test the feasibility ofdelivering a variety of services directly to con-sumers in their homes.
20 Practice Management Information Corp., International Classification of Diseases, 9th Revision, Clinical Modification, Fourth Edition,
1993 (Los Angeles, CA: 1993).21 American Medical Association, Physicians’ Curreny Procedural Terminology, 1994 (Chicago, IL: September 1993).22 U.S. Department of Health and Human Services, Public Health Service, National Committee on Vital and Health Statistics, The National
Committee on Vital and Health Statistics, 1993 (Washington, DC: May 1994), pp. 8-10,54-75.

Chapter 1 Introduction, Summary, and Options | 21
Although there are no studies that prove thecost-effectiveness of telemedicine, in some casesit would seem to have the potential to reduce costsfor some participants. For example, telemedicinecan eliminate the time and wages lost at work andtraveling expenses incurred when specialists and/or patients have to travel for consultations. In ad-dition, keeping patients in their own communitiescan increase revenues for local hospitals and de-crease the cost to patients. The cost of a bed in acommunity hospital is considerably less than in alarge medical center. Costs might also be reducedby staffing hospitals and clinics with allied healthprofessionals, such as nurse practitioners and phy-sician assistants, who would deliver serviceswhere there is no resident physician. Overall costsalso could be lower using telemedicine if it allowspatients to be seen earlier, thus preventing theneed for later, more costly care. Using telecom-munications to deliver services directly to thehome would also reduce the costs of travel, as wellas the pressures on clinics, emergency rooms, anddoctors’ offices.
In the short term, however, costs could in-crease. Telemedicine could add an extra step to theprocess if the patient still requires referral to alarger medical center. If it improves access to care,there may be increased use of health services asmore people take advantage of their availability. Ifreimbursement for telemedicine services becomeswidespread, the system may be vulnerable toabuse through overuse or fraudulent claims. Costis not the only criterion, however. It is important toconsider the “value” of delivering services tothose who might otherwise not get them at all be-cause of their physical location.
Telemedicine can increase access to health carefor populations in rural or inner city areas. It cando so by making these areas more attractive tohealth care providers by giving them immediateelectronic access to up-to-date information and re-sources, specialists for consultative purposes,continuing medical education, and other col-leagues. Enabling local hospitals to remain eco-nomically viable by keeping patients in their owncommunities is another benefit for access, as wellas for the economic stability of the community.
Telemedicine appears to have the potential toimprove the quality of care, but this has not yetbeen proven. It can provide faster, more conve-nient treatment and minimize the disruption of thepatient’s life. By reducing the need for referrals,the continuity of patient care is ensured. The qual-ity of care may be better for a patient who has thebenefit of family support in the local area. For pro-viders, ready access to information to help themmake more informed decisions will improve thequality of the care they deliver. Electronic accesswill help them stay up to date and enable them toreceive continuing medical education creditswithout leaving their communities. Some believethat the establishment of clinical practice guide-lines for telemedicine could help to provide amore consistent level of care.
While telemedicine has been practiced for 30years, its current iteration is still in the early stagesof development. It will take a number of years be-fore it is used widely enough and evaluated suffi-ciently in terms of its effectiveness and efficiencyfor definitive statements to be made about itsoverall value and recommended uses. Like all newtechnologies, there will be impacts that cannot beanticipated in advance. Rigorous evaluation stud-ies are needed to determine telemedicine’s poten-tial benefits, and such research is currently beingsupported by a number of federal agencies. The re-sults should provide policymakers with the datathey need to make decisions about the efficacy oftelemedicine. Proposed federal budget cuts, how-ever, are likely to have a negative impact on tele-medicine research efforts.
Policy IssuesWhile the use of telecommunications in deliver-ing health services has great potential, it alsoraises a number of issues that need to be resolvedif telemedicine is to thrive. In general, patient con-sultations using telemedicine are not reimburs-able (except for teleradiology and telepathology).This will have a negative effect on its diffusion un-til HCFA promulgates a national policy. One ofthe reasons for HCFA’s reluctance is the fact thatthere is a lack of research available to support the

22 | Bringing Health Care Online: The Role of Information Technologies
safety, efficacy, clinical utility, and cost-effective-ness of telemedicine.
Another issue is the cost of the telecommunica-tions links required for telemedicine. In many ru-ral areas, the communication infrastructure isunable to support the bandwidth necessary tocarry the signals for telemedicine using two-wayinteractive video. In addition, the costs of connec-tions between local and long-distance telecom-munication carriers can pose a significant barrierto telemedicine projects. Under the existing tariffstructures, telephone calls placed to locations in-side the local access transport area boundaries areoften more expensive than those placed outsidethe same service area.
Telemedicine raises some difficult legal andregulatory issues as well. Remote diagnosis andtreatment across state lines could bring differentlaws and regulations into play. A previous OTAreport found that the present legal scheme does notprovide consistent, comprehensive protection ofprivacy in health care information, whether it ex-ists in a paper or computerized environment.Clearly the privacy implications for telemedicinewill continue to receive careful scrutiny. Physi-cian licensing becomes an issue because telemedi-cine facilitates consultations without respect tostate borders and could conceivably require con-sultants to be licensed in a number of states. Thiswould be impractical and is likely to constrain thediffusion of telemedicine projects. Telemedicinemay, in fact, decrease the threat of malpracticesuits through improved recordkeeping and data-bases, and the fact that taping the consultationswill automatically provide proof of the encounter.However, it may also raise other liability issues,such as the lack of a “hands-on” examination bythe consultant.
Congressional OptionsResponsibility for telemedicine policy is sharedamong federal, state, and local lawmakers, andmany of the decisions affecting the diffusion oftelemedicine are influenced largely by the privatesector. Federal efforts to reform both the healthcare and telecommunications systems, each trav-
eling its separate path, will have an effect on tele-medicine’s progress.
Implementation of telemedicine is likely toproceed with or without federal support as provid-ers recognize its benefits to their practices. How-ever, federal government support will be requiredif it is to benefit those who need it the most—people living in rural and inner-city areas wheremarket forces are unlikely to provide the servicesneeded. In a time of tight fiscal constraints andshrinking research budgets, federal funding pro-vided will need to be carefully monitored to en-sure it is being used wisely. If Congress wishes toencourage the diffusion of telemedicine to helpsolve the disparities in health care availability, itcan have the most impact in the areas of researchfunding and reimbursement for telemedicine con-sultations. The two are closely connected, in thatformulating a standard reimbursement policy isdependent on obtaining satisfactory answers tomany of the questions raised about telemedicine’sefficacy and cost-effectiveness. Congress maywish to:
Continue to support demonstration andevaluation projects.
The research currently under way is crucial toanswering many of the questions about the bene-fits of telemedicine. To ensure that projects aresustainable when funding ends, agencies need tobuild in certain requirements. This is currentlyachieved by requiring that grantees make a finan-cial investment in the project, often throughmatching funds. Many of the current funding op-portunities for telemedicine projects focus on ru-ral areas. Telemedicine also offers potential forsolving some of the problems of inner-city healthfacilities. After assessing these needs, Congresscould target support for depressed areas where theneeds are great and a limited investment might behighly leveraged.
Because the data that would support a uniformreimbursement policy for telemedicine consulta-tions are not yet available, HCFA is moving slow-ly and deliberately in accumulating the necessaryinformation on which to base a sound decision.

Chapter 1 Introduction, Summary, and Options | 23
This seems a prudent strategy. Experimentingwith reimbursement in a small number of demon-stration sites will provide valuable insights thatwill eventually enable the agency to craft a carefulpolicy based on actual results. Congress may wishto ensure that adequate finding is provided tosupport those experiments. As the results becomeavailable, Congress may wish to provide oversightand conduct hearings to determine what furtheraction may be warranted.
Until recently, there was a lack of coordinationof federal efforts in research, policymaking, andimplementation of distance care. This has been re-medied considerably by the creation of the teleme-dicine working group of the Administration’sInformation Infrastructure Task Force.
The costs of implementing telemedicine can bea barrier to its diffusion, especially for small com-munities and facilities. To address this barrier,Congress may wish to:
Create incentives for cooperative effortsand consortia.
In many small communities, it makes econom-ic sense for groups to share the costs of imple-menting, operating, and maintaining atelecommunications network. For example,schools, medical clinics, libraries, social services,and others who would benefit from improved in-formation services may need to join forces to getstarted. The Department of Defense and the Na-tional Aeronautics and Space Administration(NASA) have been leaders in research related totelemedicine applications, and the military hashealth facilities in a number of locations. In somesites the military has cooperated with civilianhealth care personnel to deliver services usingtelecommunications. Where possible, the exper-tise that exists in the military and NASA should beshared with the civilian sector. Agencies such asthe Department of Veterans Affairs could also beinvolved in cooperative efforts with the civiliansector.
Ensure that information about telemedi-cine is widely disseminated.
In many cases, those who might benefit mostfrom telemedicine applications know very littleabout them. While information dissemination isincreasing in a variety of formats, there is a needfor a centralized, online database of telemedicineinformation. Such coordination might includecreating an electronic clearinghouse that wouldprovide a range of information about telemedicineprojects, including funding opportunities, currentprojects, and people to contact for assistance andadvice. Congress might wish to ensure that mech-anisms exist, either in the public or private sectors,to widely disseminate research results and otherinformation about telemedicine.
One of the goals of the IITF telemedicine work-ing group is to investigate the feasibility of settingup an online database of telemedicine activities,and work is continuing to determine the best wayto achieve this. Such a clearinghouse could be es-tablished in a designated federal agency withinDHHS, such as the National Library of Medicineor the Office of Rural Health Policy. Alternatively,Congress could provide support for a private-sec-tor group, such as the Telemedicine InformationExchange network at the Telemedicine ResearchCenter, Oregon Health Sciences University. Thisoption would avoid duplication of effort and pro-vide a single site where telemedicine informationcould be maintained and obtained. However, itwould also require careful consideration concern-ing the content of the database and how informa-tion would be structured and formatted. Anytelemedicine clearinghouse would only be usefulif kept up to date, and support for qualified staffwould needed to be assured.
OTHER APPLICATIONSThe applications of information technology de-tailed in chapters 2 through 5 and summarizedabove were selected because of their potential toimprove access to health care, improve the qualityof care, and reduce the costs of delivering care.These were of particular interest to the study’s re-questers. OTA was unable to undertake an in-depth analysis of a number of other applicationsof information technology that also have potential

24 | Bringing Health Care Online: The Role of Information Technologies
for improving health care. Two are mentionedhere—consumer health informatics and commu-nity networking.
❚ Consumer Health InformaticsConsumer health informatics has been defined as“the study, development, and implementation ofcomputer and telecommunications applicationsand interfaces designed to be used by health con-sumers.”23 The basic principle is that of empower-ing people to play a greater role in their own healthcare and to be active participants in decisions af-fecting their health.24 Information technology canbe used to provide more health-related informa-tion to consumers, “the largest untapped resourcefor health care.”25 Taking measures to prevent ill-ness and disease, by adjusting lifestyles or takingsafety precautions, for example, could have a pos-itive impact on the health care delivery system andallow people to lead healthier lives.
Shared decision support systems are designedto inform patient/provider decisions regardingprevention, diagnosis, management, and treat-ment, and ultimately to improve the quality ofcare and reduce costs. Choices are made collabo-ratively by patients and their caregivers. An exam-ple is the interactive video disk system developedat Dartmouth Medical School that allows menwith benign prostatic hyperplasia and early stageprostatic cancer to share in decisions on theircourse of treatment.26 Some regard these comput-
er-based systems as transforming the culture ofthe health care system to one in which patients,physicians, and other providers play equal roles indecisionmaking. 27
Information technology also could play an im-portant role in reducing a consumer’s need forhealth care services. Demand management can bedefined as the “the support of individuals so thatthey can make rational health and medical deci-sions based on a consideration of the benefits andrisks of the options available.”28 Current exam-ples include health risk appraisals, written and au-diovisual media, telephone counseling services,and community resources. Although a compre-hensive demand management system does not yetexist, information technologies can make inter-ventions more available and effective, and pro-vide a sophisticated, multipurpose informationsystem based on a new concept of the individualhealth record. When developed, these comprehen-sive services will allow consumers to understand,choose, and evaluate health services in new ways,and could have a positive impact on health carecosts and quality.29
Information technology also fosters commu-nication among people who can provide supportand encouragement to those dealing with chronicillnesses or a medical crisis. There is a large andgrowing community of people using computers toprovide help and support to one another to addressa variety of concerns. For example, as of early
23 Tom Ferguson (ed.), “Consumer Health Informatics: Bringing the Patient Into the Loop,” Proceedings of the First National Conferenceon Consumer Health Informatics, July 1993, p. 2. The Administration’s Information Infrastructure Task Force, Consumer Information Sub-group, defines consumer health informatics as “any information that enables individuals to understand their health and make health-relateddecisions for themselves or their families.”
24 John Wennberg, “Shared Decision Making and Multimedia,” Health and the New Media: Technologies Transforming Personal and Pub-
lic Health, Linda M. Harris (ed.) (Hillsdale, NJ: Lawrence Erlbaum Associates, Inc., 1995).
25 Vergil Slee and Deborah Deatrick, “Reengineering Health Care Decision Making,” Health Commons Update, vol. 2, winter 1995, p. 6.26 Wennberg, op. cit., footnote 24.27 Deborah Deatrick, Executive Director, Health Commons Institute, personal communication, June 9, 1995. See also Slee and Deatrick, op.
cit., footnote 25, p. 1.
28 D.M. Vickery, “Demand Management, Self-Care, and the New Media,” Linda M. Harris (ed.), op. cit., footnote 24.29 Ibid.

Chapter 1 Introduction, Summary, and Options | 25
May 1995, America Online reported it had 148scheduled self-help groups.30 Some of thesegroups address health-related concerns, such asdiabetes, stroke, AIDS, cancer, or disabilities.Others support the caregivers of people sufferingfrom Alzheimer’s disease or other debilitating ill-nesses. Nonprofit groups, such as the AmericanSelf-Help Clearinghouse, provide assistance andinformation to those wishing to set up an electron-ic support group or find out about such groups.31
Information on a variety of online health resourcescan be obtained from the National Health In-formation Center.32
The CHESS system is an example of one thatallows consumers to access information abouttheir illnesses and to support one another usinghome terminals.33 Another is the Connect Sys-tem, a computer and voice-mail system used tomonitor inner city drug-using pregnant women inCleveland, Ohio. At Case Western Reserve Uni-versity, ComputerLink was a demonstration proj-ect that supported the caregivers of persons withAlzheimer’s disease and AIDS by delivering in-formation, communication, and decision support,accessed through home terminals.34 (See ch. 5 formore complete discussion of these systems.) Fu-ture systems geared to the needs of consumers arelikely to include interactive video to the home.
Participants in an OTA workshop in July 1994had a number of suggestions regarding what ac-
tions are needed to foster greater electronic healthresources for consumers. These included:
1. support research and development;2. support wide access to the NII as it develops;3. insist on good needs assessment for consumer
applications;4. incorporate medical informatics into the med-
ical education curriculum;5. support clinical trials of different ways of shar-
ing health data;6. reduce the cost of telephone links to electronic
bulletin boards;7. subsidize premarket development of tools that
private corporations can use and resell;8. facilitate the use of technology by managed
care organizations;9. educate, support, and train users; and
10. provide grassroots technology “set-asides.”
The Administration’s Information Infrastruc-ture Task Force has a subgroup of representativesfrom federal agencies who are addressing con-sumer health information and the NII. This com-mittee has coordinated the development of a draftwhite paper outlining key policy issues for thefederal government to consider as the public in-creasingly relies on electronic means of informa-tion access and exchange.35 This paper wasreleased for public comment at a federally spon-sored national conference on networked consum-
30 Todd Woodward, Self-Help Information Center, America Online, personal communication, May 8, 1995.31 Barbara J. White and Edward J. Madara (eds.), The Self-Help Sourcebook: Finding and Forming Mutual Aid Self-Help Groups, 4th ed.
(Denville, NJ: St. Clares-Riverside Medical Center, 1992).
32 NHIC’s home page on the World Wide Web is located at <URL: http://hic-nt.health.org/ >. NHIC is a service of the Office of DiseasePrevention and Health Promotion, Public Health Service, U.S. Department of Health and Human Services, and the George Washington Univer-sity Himmelfarb Medical Library.
33 F.M. McTavish et al., “CHESS: An Interactive Computer System for Women with Breast Cancer Piloted with an Under-Served Popula-tion,” n.d.
34 Patricia F. Brennan, “Differential Use of Computer Network Services,” American Medical Informatics Association, Proceedings,
Seventh Annual Symposium on Computer Applications in Medicine, Oct. 30-Nov. 3, 1993, Washington, DC, p. 27.
35 Kevin Patrick and Shannah Koss, “Consumer Information ‘White Paper,’” Consumer Health Information Subgroup, Health Informationand Application Working Group, Committee on Applications and Technology, Information Infrastructure Task Force, working draft, May 15,1995.

26 | Bringing Health Care Online: The Role of Information Technologies
er health information in May 1995. It will serve asthe cornerstone for Administration policy in ap-plications technology development and use.
Key policy issues for the federal governmentidentified in the paper include:
� the need to coordinate federal consumer healthinformation dissemination efforts both withinthe government (federal, state, and local) andwith private providers;
� assurance of privacy and confidentiality;� assurance of the availability of information
critical for public health;� the need for research and evaluation of the im-
pact of consumer health information;� the role of standards in vocabularies and data
transmission;� information validity and integrity;� assurance of telecommunications infrastruc-
ture for adequate information delivery; and� education and training.
❚ Community NetworkingHuman services, including health care, are oftendelivered in a fragmented fashion, leading to du-plication of effort on the part of providers and con-sumers. Telecommunications could be used tocoordinate and streamline these services throughcommunity networking,36 enabling the providersof a wide variety of social services to share in-
formation and communicate with one another. Anearlier OTA report discussed the role of the localcommunity infrastructure—schools, libraries, se-nior centers, and town halls—in delivering federalservices to citizens electronically, especially thosein rural areas, small towns, inner cities, and peoplewith special needs37 (see box 1-3). The difficultiesof building an infrastructure can be a barrier, how-ever. One group of researchers commented:
Although there is widespread endorsement ofsuch proposed efforts as managed care and one-stop shop service delivery, the more difficulttask in most communities is to build an infra-structure that supports such coordination with aholistic approach to service and care.38
One example of a project using telecommu-nication and computer technologies to supportand coordinate health and human services at thecommunity level is the Community Services Net-work (CSN) in Washington, DC. This is a joint ef-fort of the U.S. Public Health Service, HowardUniversity School of Social Work, Rice Universi-ty and Baylor College of Medicine, MacroInternational, Inc., United Seniors Health Cooperative, and Bell Atlantic Corp. Several communitiesacross the country are currently exploring the de-velopment of CSNs. The Lawrence LivermoreLab in California is helping Macro and other part-ners develop test-beds to move CSNs from pilot toearly operational status.39
36 For a discussion of the role of information technology in strengthening community action, see Nancy Milio, Engines of Empowerment
(Ann Arbor, MI: Health Administration Press, 1995).
37 U.S. Congress, Office of Technology Assessment, Making Government Work: Electronic Delivery of Federal Services, OTA-TCT-578(Washington, DC: Government Printing Office, September 1993), ch. 5. See also U.S. Congress, Office of Technology Assessment, Telecom-munications Technology and Native Americans: Opportunities and Challenges, OTA-ITC-621 (Washington, DC: U.S. Government PrintingOffice, August 1995).
38 G.A. Gorry et al., “Health Care as Teamwork: The Internet Collaboratory,” in Health and the New Media, op. cit., footnote 24, p. 97.39 Kevin Patrick, Department of Health and Human Services, personal communication, May 10, 1995.

Chapter 1 Introduction, Summary, and Options 27
OTA commissioned two grassroots computer networks to conduct computer conferences on the topic of
electronic service delivery. Big Sky Telegraph (BST), headquartered in Dillon, MT, and the National Public Tele-
computing Network (NPTN), headquartered in Cleveland, OH, conducted the conferences during late summer
and fall of 1992. Lessons learned include:
1. The costs to users of grassroots computer networking can be minimized. Almost any personal computer
(PC) and modem wiII suffice, high-end, high-speed equipment is not necessary. Online telecommunication
charges can be reduced by copying messages to a PC and preparing responses with the telecommunications
line turned off, and by using fractional rates and bulk purchase discounts. Use of equipment that transmits
messages faster will reduce online charges further.
2 Any local community can have a community computer bulletin board. BST has, in effect, created six
“Little Skys” where people can dial in with a local call—further reducing online costs. BST IS a rural equivalent
of the NPTN’s network of “Freeness. ” BST is a rural FreeNet. All you need is a PC, modem, telephone line, and
inexpensive bulletin board software, And to further reduce costs, the “Little Sky” or “FreeNet” can dial up a
host computer once a night at off-peak rates to copy or add bulletin board items.
3. Community computer bulletin boards really extend a sense of community. BST and NPTN, Iike Compu-
Serve and Minitel, found that users participate as much for sociability as for content. Users seek a comfort
level and degree of intimacy that is not always prevalent in the community-at-large. Computer conferencing
also greatly reduces any biases due to sex, physique, disabilities, speaking ability, etc. It is a leveling technol-
ogy in this sense.
4. Community computer networks usually get only limited support from the established government and
business community. The BST and NPTN approach is low-cost and decentralized; the state and federal bu-
reaucracies tend to favor higher cost, more centralized, or at least more controllable, approaches Also the
“not invented here” syndrome IS evident. Each organization has a tendency to invent its own solution or ap-
proach,
5. Grassroots computer network utilities like BST and NPTN can facilitate local access to national computer
networks that might not be otherwise technically feasible or affordable. If local residents find computer net-
works such as the Internet expensive or difficult to access directly, computer utilities can provide low-cost,
user-friendly connections.
6. Grassroots computer conferencing works for children. Children as young as the third grade can use
computer conferencing to learn keyboarding, e-mail, and the concept of communicating among a group elec-
tronically (even some first-graders can handle it).
7. Grassroots computer conferencing has significant potential for government service delivery For exam-
ple: a) agricultural extension services, b) small business assistance, c) International trade—global trade net-
works offer tremendous potential for locally based global entrepreneurial networking, d) Indian reservation ser-
vices, especially for the Indian schools and hospitals, e) vocational education for displaced homemakers, f)
job opportunities—potential for computerized catalogs of jobs and skill requirements, and g) public access to
the Iegislative process.
8. Training is essential to computer conferencing success. It is Important for first experiences to be positive
in order to develop self-confidence. Help lines work, rather than forcing users to struggle through manuals. As
confidence builds, users can do more themselves and handle more complex functions. Initially many people
are not ready for searching databases; but eventually users will want to and can do searches.
9. federal programs largely miss the potential of grassroots computing. The government does not have
good mechanisms to support small, local innovators who lack a major Institutional affiliation. Suggestions
mini-grants of up to $5,000 or so to local innovators; more flexibility in the National Science Foundation and
other federal grant programs to support individuals and small, grassroots organizations, inclusion of grass-
roots representatives on federal advisory and peer review panels; technology showcases and demonstrations
(e.g., fiber-to-the-school demonstrations in rural, economically disadvantaged areas).
SOURCE: Big Sky Telegraph, National Public Telecomputing Network, and Office of Technology Assessment, 1993 ‘ -— .
I
I
I
I

InformationTechnologies for
TransformingHealth
Care
he central event of successful health care is the preserva-tion of health or the healing of an infirmity through em-ployment of medical expertise for the benefit of a patient.This can be deeply satisfying for all parties, but it often
occurs within a complicated and frustrating health care deliverysystem. Working from dimly remembered medical facts and per-haps a few consumer health information brochures or a thinguidebook published by an insurance company, individuals mustdecide which doctor to select, pay for their care, negotiate reim-bursement, evaluate the care they receive, and choose healthylifestyles. But if patients and consumers have too little informa-tion, doctors and other health care practitioners generally havetoo much. They must keep abreast of a burgeoning medical re-search literature, gather information from bulging but inadequatepaper record systems, diagnose and treat diseases, educate pa-tients, and extend or limit patient access to specialists. Adminis-trators and insurance companies must work within informationsystems that are often poorly organized to answer complex ques-tions as they compete for customers, comply with shifting regula-tory policy, optimize use of resources, provide high-qualityhealth care, and meet investor demands for profitability. And thefederal government, in its role as a provider and purchaser ofhealth care, must find ways to minimize the cost of providinghealth care.
Many of the frustrations encountered by participants in thehealth care system can be traced to the inability of current in-formation systems to provide adequate, accurate, timely, and ap-propriate information. Poor information flow has become animpediment to efficient delivery of high-quality health care.
| 29

30 | Bringing Health Care Online: The Role of Information Technologies
ISLANDS OF AUTOMATIONThere is a long history of attempts to solve theproblems of inadequate health information sys-tems by using computers. When the first general-purpose laboratory computer was introduced tothe market, it was immediately used in a projectto compile computer-based medical histories.40
Today, many hospitals spend a large portionof their budgets on computers and recordkeeping.An entire academic field called medical in-formatics has developed around the study of ad-ministrative, clinical, demographic, research, andeducational information generated in the processof delivering health care services. Many healthprofessionals believe that delivery and coordina-tion of care might be greatly improved if all rele-vant information were collected in a standarddigital form and broadly connected in a health datasystem. This would enable authorized persons torapidly access and modify data when necessary.
No such system currently exists.Thirty years of academic, commercial, and
government research have produced successfulpilot programs and commercial implementationsof parts of a comprehensive digital health in-formation system. Many hospitals have comput-erized their administrative or clinical records,many insurance claims and orders for supplies aresubmitted electronically, many research materialsare distributed over computer networks, and elec-tronic distribution of consumer health informa-tion has begun. However, there is still no systemthat comprehensively facilitates the flow of alltypes of health information and symmetrically ad-dresses the needs of clinicians, administrators,policymakers, patients, and consumers. The fullpotential of digital health information will only be
realized when it begins to flow beyond the con-fines of single departments, institutions, or com-munities.
The current situation is often characterized as aseries of islands of automation. This report pro-vides a tour of that digital archipelago; it surveysthe history and terrain of the existing islands of au-tomation and offers potential options for possiblefederal roles in enlarging and connecting the is-lands. This chapter begins, as it were, with theocean: it provides an overview of the organizationand flow of information within the broad healthcare system. It then describes information systemswithin hospitals and clinics. By focusing on thesubset of clinical information that has been storedconventionally as paper-based clinical patient re-cords, the discussion illustrates some of the prob-lems and challenges confronted in the effort todigitize health information. The chapter also de-scribes several key technologies that underlie ef-forts to build an interconnected health datasystem. Subsequent chapters describe ways thesetechnologies are being used in administrative sys-tems, clinical decision support and care evalua-tion systems, and systems for delivering healthcare to a scattered and diverse population throughtelemedicine and other techniques.
The story begins with a glimpse of the imag-ined mainland: the following scenario illustratessome of the many ways that health care might bedifferent should information technology achieveits full potential as a medical tool. The scenario isfictional, but not utopian: it explores how the ex-periences of consumers, clinical teams, adminis-trators, and policymakers might change in a worldwhere health information flows freely.41 It implic-itly illustrates some of the problematic aspects of
40 W.V. Slack et al., “A Computer-Based Medical History System,” New England Journal of Medicine, vol. 274, 1966, pp. 194-198. Slackused LINC, one of the first general purpose laboratory computers and an ancestor of the desktop computers now spreading throughout thehealth care delivery system.
41 In the scenario, information “flows freely” in that structural and technological impediments to exchanging information have been mini-mized, but it only flows within prescribed channels. This qualification will need to be applied to any comprehensive health data system thatmight develop. There must be adequate security and confidentiality mechanisms in place so that all participants are willing to trust the systemand put their information into it. In addition, the legal, regulatory, and technological standards that define the channels must be stable and ratio-nal enough for businesses and institutions to depend on them.

Chapter 2 Information Technologies for Transforming Health Care | 31
the digital revolution in health care, along with themany possible opportunities and advantages.Consider, then, a fictional scenario of health carein a fully digital world.
❚ Simplified AdministrationEmilia finished her reply to the clinic’s e-mailmessage and launched her web browser. Thee-mail had been a reminder confirming her ap-pointment later that day at the maternity clinic atthe medical school; with only a month remaininguntil her due date, she was well acquainted withthe routine of arriving at the clinic, having thenurse practitioner check the baby’s size and heart-beat, and returning home with a fresh stock of vi-tamins and increasingly real expectations for thefuture. Emilia chose the medical school’s homepage from her browser’s list of recently visitedsites and typed her name and password into thescheduling inquiry form. In a moment, the re-sponse to her query appeared: appointments in thematernity clinic were running about 20 minuteslate. She had plenty of time for lunch before thevisit.
For the past few years, Emilia had received pri-mary health care through the student health ser-vice at her college, but when she became pregnantall that changed. She was referred to the maternityclinic at a teaching hospital associated with theuniversity and had received all her prenatal visitsand screening there. From her first visit, it hadbeen apparent that things were done differently atthe hospital than at any doctor’s office or clinic shehad visited. Emilia and her husband John had ar-rived well before their scheduled appointment, ex-pecting to have to complete a pile of paper forms.Instead, they were directed to one of a set of kiosksin the reception area where they sat down and be-gan interacting with a computer program. Thecomputer asked Emilia to swipe the magnetic-stripe card from the student health service throughthe reader next to the machine, and then the ma-chine began asking them questions. Most of thequestions were the usual ones—“Do you have ahistory of heart trouble?” for example—but atleast she didn’t have to fill out all those tedious ad-
dresses—her own, her next of kin, and the like.The computer had already read them from themagnetic card. It took only five minutes to com-plete the program’s questions because it didn’t askfor the same information in many different wayslike paper forms often do. When she clicked on thebutton indicating that she was an only child, theprogram didn’t ask any further questions about thehealth history of her siblings. The program had afew sections for John to fill out about his own fam-ily history.
The kiosk then provided a curious sectionabout granting the hospital permission to use theinformation generated during her care. Emilia hadseen similar language in small type at the bottomof paper forms and had always initialed the boxesindicating her agreement, but she had never paidmuch attention to it. This program made the in-formation permission seem almost as important asthe health history itself: it requested specific per-mission to use all her medical information withinthe hospital, it asked for separate permission to re-lease her record of care anonymously to state orfederal authorities for research purposes, it askedfor permission to automatically compare her pro-file with those sought for various clinical trials inthe hospital, and on and on. In the end, the pro-gram summarized all the permissions she had giv-en and asked her once more to approve the wholeset. Emilia realized she didn’t fully understandwhat sorts of clinical trials the questionnairemight be referring to, and so she changed her ap-proval of that item to a request for more informa-tion.
After completing the program, she returned tothe desk and the receptionist gave her a new plas-tic card. “It’s a smart card,” he said, “try not tobend it.” Emilia asked why the program had beenso annoyingly thorough in asking for permissionto use her health information. “If we don’t annoyyou now, someone else might annoy you later,”the receptionist explained. “We keep digital re-cords instead of paper records in this hospital, sowe can’t control where our information goes justby locking the drawer of a filing cabinet. Ofcourse, we use passwords, encryption, and othersecurity measures to control who can read and al-

32 | Bringing Health Care Online: The Role of Information Technologies
ter your records in the hospital, but some of yourhealth information goes elsewhere as well. We billyour insurance company electronically so all youever have to worry about is the copayment, and weabstract information from your records for reportsrequested by our management and those requiredby the government. The permission form you’vejust completed provides another layer of securitythat helps ensure that whenever your records areused for purposes other than directly providingcare to you, you know about it and have approvedit. It’s a little like giving us a digital power of attor-ney—anyone who has your health informationand wants to release it to someone else for a differ-ent purpose has to check for your permissionagainst the file you’ve just created. That’s the rule,even if everything directly identifying you hasbeen removed from the record. You’re not givingus blanket permission to use your health data—that’s why the form is broken into so many separatequestions covering different aspects of informa-tion sharing. And it’s fine to decline permission onthis form—that just means we’ll need to ask yourpermission on a case-by-case basis later.”
Emilia thought for a moment. “So I own myhealth records?” The receptionist smiled, “No,and you certainly couldn’t reassemble all the in-formation once it is released, but you can help de-termine where that information goes. I see thatyou’ve asked for more information about enroll-ment in clinical trials. The computer has put a re-minder on your nurse practitioner’s schedule todiscuss that with you. She’ll tell you about someof our ongoing research and discuss how your caremight be affected by your decision to share orwithhold information from the system thatmatches eligible patients with clinical trials.”
❚ Informed Patients and ConsumersEmilia and John had many more experiences withthe kiosk following that initial visit. Each timethey came to the clinic, they checked in by insert-ing the smart card and charging the copayment totheir credit card, then used their spare momentsbefore the nurse practitioner was available to learn
more about their baby. The computer referred toinformation in Emilia’s electronic patient recordand then presented multimedia modules tied to thegestational age of the baby. When ultrasoundscans were taken early in the pregnancy, theycould review them on the screen in full motion,and Emilia was able to change the contrast andcolor schemes so that even John could recognizethe baby’s face. They still got the little snapshotthat most parents take home, but they could alsoe-mail their parents a minute or so of digitized vid-eo as well.
There were modules about the risks and bene-fits of alpha-fetal protein screening, genetic test-ing, pain medication during delivery, and themany other decisions they had to make. WhenJohn couldn’t go with her to the prenatal visits, hewould work through the same educational mod-ules at home using a web browser over the Inter-net. Emilia liked being able to find the answers tosome of her questions without having to ask theclinician directly—not only did she avoid havingto play telephone tag with the clinic or call in atcertain hours of the day, but she could get informa-tion on her own so that she was more confident inasking questions face-to-face.
Emilia collected information from several dif-ferent electronic information sources besides themedical school. She borrowed a health informa-tion CD-ROM from a friend and found severalmore disks and videos at the city library. She sub-scribed to a free Internet mailing list about preg-nancy and childbirth experiences and participatedin a chat forum with other women on a commer-cial online service. And she made a point of regu-larly exchanging e-mail with some of the otherwomen in her birthing classes at the hospital. Thatclass was definitely not a place for high-tech mul-timedia programs, but for hand-holding andeducation from a nurse who had seen many, manybirths. Nonetheless, the scheduling for the classwas set up through the hospital computer system,and the women kept in touch electronically witheach other and their teacher between classes.

Chapter 2 Information Technologies for Transforming Health Care | 33
❚ Paperless MedicineWhen Emilia arrived at the clinic, she answered afew questions that the kiosk had for her and thenwent into a room where a nurse recorded herweight and vital signs and measured her belly be-fore the nurse practitioner arrived. The nurse in-serted Emilia’s smart card into a computer in theexamination room and typed the weight and sizemeasurements into a form that appeared on thescreen; the blood pressure machine and thermom-eter were hooked directly into the computer sys-tem and their measurements appeared on the sameform automatically. Computers in the teachinghospital certainly weren’t limited to multimediakiosks in the reception area. Every doctor, nurse,receptionist, and treatment room had one, and allthe computers were interconnected by cables, ra-dio, or infrared links. When the nurse practitionerentered the room, she was invariably holding asmall computer in her hand and noting the new da-tapoint on the graph showing Emilia’s weightthroughout her pregnancy. A summary of Emilia’sprevious visits and her responses to the screeningquestions today were also provided. The nursepractitioner’s computer didn’t have a keyboard,but that didn’t seem to matter because there waslittle writing or typing involved. If the NP wantedto order a laboratory test, for instance, she selectedthe proper form from a menu on the screen andmost of the information would already be filled inby the computer. She used a stylus to check offboxes indicating what she wanted done and thendispatched the order by tapping out her passwordon a little keyboard displayed on the screen. Dur-ing most of the encounter, the NP simply set thecomputer aside and concentrated on the patient.Today, she had a concerned look on her face.
“Emilia, I’m worried that your baby’s sizeseems to be reaching a plateau rather than sharplyincreasing in the usual way for the last few weeksof pregnancy.” She showed her the screen of herhandheld computer, which had a plot of the se-quence of Emilia’s measurements along with anormative size development chart. “The dashedlines represent the limits for a standard distribu-tion of women. You’re still within those bound-
aries, and so your baby may well be developingnormally, but I’d like to order a few tests, begin-ning with another ultrasound. I can see that the ul-trasound technician has an opening at 2:20, andI’d like you to get the test done as soon as pos-sible.”
Emilia’s heart fell. It would be her third ultra-sound so far. The first one had been exhilarating,and the second one less so. It had produced the ex-pected pictures, but hadn’t really been mentionedby her doctor after it was completed. It seemedthat the clinicians were willing to order tests veryreadily, given that there wasn’t any paperwork in-volved and the results appeared very quickly ontheir screens. How did they know that ordering somany tests helped ensure healthier deliveries? Itcertainly wasn’t cheap. At this point, though, shewasn’t worried that the ultrasound was unneces-sary but that it would be a harbinger of bad news.As she refocused her thoughts, she could hear thenurse practitioner saying, “You have an hour. Whydon’t you spend the time looking at our Deliveryand Birth CD-ROM just in case you don’t havethe opportunity to finish those classes?”
❚ Empowered Clinical TeamsIn the staff conference room, Dr. Conway’s pagervibrated and the digital assistant on the table infront of her simultaneously awoke from its elec-tronic slumber. The doctor felt a little sleepy her-self, but at least she was getting continuingmedical education credits for these lunchtimeseminars utilizing the satellite link to Boston. Sheglanced at the incoming e-mail, which indicatedthat an obstetrics resident wanted her help with adecision about a potential c-section. The doctorleft the seminar quietly and read the case précisthat the digital assistant displayed as she walkeddown the hall.
Emilia’s ultrasound technician had used imag-ing software to measure pockets of amniotic fluidaround the baby and had recognized that the vol-ume of the pockets was critically low for this stageof pregnancy. One of the hospital’s decision sup-port systems had come to the same conclusion bycomparing the numbers in the technician’s sum-

34 I Bringing Health Care Online: The Role of Information Technologies
mary to the predictions of the OB-GYN expertsystem. After asking the technician to confirm itsfinding, the computer issued an alert to the resi-dent on call. The resident’s online work history in-dicated that he hadn’t had direct experience withthis type of case, so the system prepared a one-page summary of similar cases from the last yearand a set of hyperlinks to the abstracts of relevantresearch literature. The resident skimmed the in-formation as it appeared on his clipboard-shapedcomputer, talked to Emilia, and came to a quickdecision to admit her to the hospital. With thetouch of several on-screen buttons, he dispatchedsoftware agents that silently scheduled a room forEmilia, requisitioned a suite of monitoring equip-ment, ordered IV bags and Pitocin from the phar-macy, altered nursing assignments, and summonedDr. Conway.
Emilia had entered the clinic that morningthinking it would be a normal day, but now shefound herself in the labor and delivery room with-out so much as a suitcase . . . the baby needed tocome out, labor would be induced, and the onlyquestion was whether a c-section could beavoided. She longed for the sort of uncomplicatedbirth described in her classes, but it was not to be.As she was calling John on her bedside phone andasking him to drive faster, a nurse wheeled in sev-eral monitors and an IV pump and quickly at-tached them to a bedside computer. The nurseopened a panel on the IV pump and inserted a bar-coded bottle; PITOCIN-FLOW OFF began glowingon the computer screen. Now the monitorshummed all around Emilia, measuring her pulseand blood oxygenation and the baby “s as well, andready to measure the contractions that wouldcome. Emilia was attached to so many wires thatshe felt her body itself was a part of the informa-tion superhighway. She felt disoriented, but at leastthe nurse had sufficient time to sit with her for afew minutes and explain what was happening.
Dr. Conway walked in with the resident andintroduced herself. “We’ve been watching the fe-tal monitor data as we discussed your case in thenext room—there’s no indication that the baby isin distress, so we’re going to induce labor as soonas your husband arrives and see how it goes.
Please try to relax-chances are you’ll be homewith your baby in 24 hours. Do you have any aller-gies to medications I should know about?” Emiliaalmost replied that there wasn’t anything particu-larly relaxing about being sent home less than 24hours after delivery, but she sighed and simplysaid, “No, no allergies. ” Dr. Conway already knewthat—the pharmacy alert system had cross-checked Emilia’s history for potential problemswith the pain-management drugs that might beused in the delivery and posted the results alongwith the drug prices on her digital assistant—butshe always asked again, just to be sure. She chosethe medications she wanted from the displayedformulary and dispatched a software agent thatwould arrange for delivery of the drugs to Emiliabedside and update the pharmacy’s inventory andreordering system. She performed a quick physi-cal exam and then sat at a console in the corner todictate her findings into Emilia’s patient record.As Dr. Conway spoke into the microphone, thecomputer recognized her words and inserted theminto forms on the screen in front of her much fasterthan she could have typed them. She filled out thecare plan and entered nursing and laboratory or-ders with a few touches of a stylus on the screen ofher digital assistant. Finally, she used a passwordto attach a digital signature and time stamp to theorders and the findings and then turned in herchair. “Emilia, when your husband arrives, youshould start discussing names for the baby. Thatone decision our computers can ‘t help you make!”
THE LIFE CYCLE OF HEALTHINFORMATIONEmilia’s story describes some of the ways that ap-plications of information technologies couldchange the delivery of health care. The scenariofocuses on the experiences of a patient in a special-ized clinical setting titan urban hospital. However,similar opportunities, difficulties, and changeswill arise as information technologies are incorpo-rated into the jobs of health care workers and intohome health care, rural health care, medicaleducation, population-based public health ser-vices, and other types of health care delivery. The

Chapter 2 Information Technologies for Transforming Health Care | 35
first step in this process is the digitization of healthinformation and the creation of an infrastructurethat allows health information to flow seamlesslyamong the various parts of the delivery system.
Although the experiences described in Emilia’sstory depend on the use of information from manydifferent sources and on communication betweennetworks administered by many different types ofinstitutions, they are sometimes said to be prod-ucts of an electronic, digital, or computer-basedpatient record. This report will use the term com-puter-based patient record in a more limitedsense: it is a compilation in digital form of all theclinical and administrative information relating tothe care of a single individual. Computer-basedpatient records serve as repositories for clinical in-formation and as records of communications andtransactions; their analogs in traditional health in-formation systems are paper-based patient recordsor charts, usually kept in folders along with filmsat each site of care. Although computer-based pa-tient records may be localized in a single data file,they might also be widely distributed in comput-ers throughout an institution or among severalinstitutions. In either case, the perceived locationof the record is on a computer screen in front of theperson using it at any particular moment.
It is possible to design stand-alone computer-based patient record systems and some are in use,but much of the advantage of computerizinghealth information is lost if other systems andprocesses within the provider institution are un-able to interact with information in the record.Maintaining a stand-alone patient record, for ex-ample, could require caregivers or clerical person-nel to retype test results that were produced by acomputerized lab analyzer in order to get theminto the record, or to retype administrative in-formation from the record for use in creating fi-nancial statements. To avoid these inefficiencies,computer-based patient records are usually em-bedded in various other information systems.
These systems include not only computer hard-ware and software and networks, but also the“people, data, rules, procedures, processing andstorage devices—and communication and sup-port facilities” involved in managing the recordsystem and distributing data and informationthroughout the provider organization.42 For hos-pital patients, computer-based patient records aretypically linked to clinical information systemsthat track clinician-patient encounters, and theymay be linked to administrative, laboratory, nurs-ing, and pharmacy information systems as well.However, most health care encounters occur out-side of hospitals. The large amount of health in-formation generated in primary care and homecare settings could be captured in computerizedpatient record systems embedded in informationsystems appropriate for private and group practicedoctors and public health workers.
Ideally, within a single institution, the distinc-tions between these various information systemsshould be transparent to users so they becomeparts of a seamless enterprise information system.In practice, however, the components for eachtype of information system are usually procuredseparately, and their integration can be plagued bya lack of design coordination and technical stan-dards. New departmental computer systems maybe incompatible with each other and with pre-viously installed legacy systems. Although thediscussion in this chapter primarily encompassesclinical information systems in hospitals, most ofthe benefits described in the scenario will comefrom the synergistic interaction between comput-er-based patient records and broader sources of in-formation assembled from a variety of networkedinformation systems. The next section illustrateshow information flows within clinical informa-tion systems and discusses the content, utility,strengths, and weaknesses of paper and computer-based patient records.
42 Richard S. Dick and Elaine B. Steen (eds.), The Computer-Based Patient Record: An Essential Technology for Health Care (Washington,
DC: National Academy Press, 1991), p. 12.

36 | Bringing Health Care Online: The Role of Information Technologies
❚ Clinical Information SystemsFigure 2-1 shows some of the ways that informa-tion flows between patient records and the variousinformation systems inside and surrounding alarge health care organization.43 The informationmight be contained in a mixture of paper and com-puterized records and transferred via computernetworks, fax, modem, mail, or courier. The fig-ure indicates general sources and destinations ofinformation, but is not intended to reflect the spe-cific architectures or communication pathways ina particular setting. For instance, the institution’sdata repositories are shown near the center of thefigure, but they may be implemented as a singlecentralized record system or distributed amongvarious departments in the hospital. The data re-positories include administrative and clinical pa-tient records representing information aboutindividual patients. They also include financialand other management-oriented databases that in-corporate data gleaned from records of the entirepatient population. Information such as sched-ules, personnel records, internal communications,and regulatory policies that support the operationof the institution are also included. One of the keyadvantages of shifting to computer-based patientrecords is the opportunity to strengthen the linkbetween clinical records and management in-formation systems so that resource use and qualityof care can be analyzed using clinical data.
Clinical patient records contain encounterinformation, bedside data and nursing notes gen-erated in the wards, laboratory reports, pharma-ceutical receipts, images, and specialized reportsfrom various institutional departments. The ad-ministrative departments exchange informationwith various external health care providers andpractitioners and with the patient. They also gen-
erate information about the patient’s demograph-ics and movements within the hospital andcompile bills using information from the clinicalrecords. The bills and orders for new supplies arepassed to logistics departments, which generatepurchase orders for medical supplies and pharma-ceuticals. They also send out bills to insurancecompanies and request (through intermediaries)reimbursement from the Health Care FinancingAdministration (HCFA) and state agencies forcare provided through the Medicare and Medicaidprograms. Caregivers may use clinical researchliterature, public knowledge bases, and other ex-ternal information resources. Federal and stategovernments indirectly shape the flow of healthcare information by funding clinical research andaspects of communication infrastructure develop-ment, and through the regulatory activities of theFood and Drug Administration, HCFA, state li-censing authorities, and other bodies.
One example of a comprehensive clinical in-formation system is the Regenstrief Medical Re-cord System developed by the Indiana UniversityMedical Center.44 This system is used for bothhospital and outpatient care in a network of threehospitals and 30 clinics, several health mainte-nance organization (HMO) offices, and care sitesfor the homeless and elderly. The system capturesdata from clinicians through an order-entry sys-tem and through links to administrative, laborato-ry, and pharmacy information systems. Inaddition, it captures nursing notes and some of thedata generated by bedside monitors and electro-cardiogram carts. It automatically reviews eachpatient chart for completeness and uses a set ofmore than a thousand rules to generate noticesabout allergies, potential drug-diagnosis interac-tions, treatment suggestions, preventive care, and
43 The figure gives a central role to the hospital as a reflection of this chapter’s emphasis on information systems in hospitals. Of course, mostindividuals receive very little of their care at hospitals, and while hospitals generate an enormous amount of medical and administrative in-formation, they are only one part of the overall health information complex. Chapters 1, 3, and 5 address this larger context and discuss primaryhealth care, integrated health maintenance organizations, consumer health information, and other generators and users of health information.
44 C.J. McDonald et al., “The Regenstrief Medical Record System—Experience with MD Order Entry and Community-Wide Extensions,”
Proceedings of the Eighteenth Annual Symposium on Computer Applications in Medical Care, vol. 18, 1994, p. 1059.
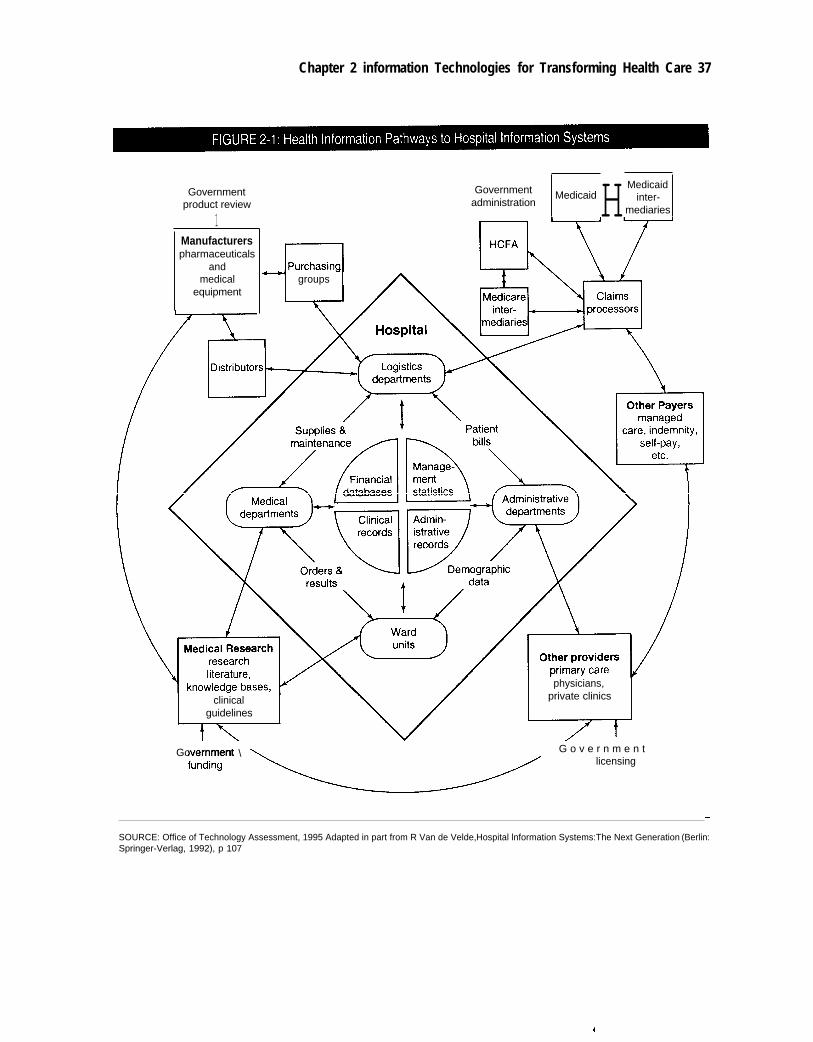
Chapter 2 information Technologies for Transforming Health Care 37
Governmentproduct review
1Manufacturerspharmaceuticals
andmedical
equipment
Government H MedicaidMedicaid
administration inter-mediaries
groups
physicians,
clinical private clinics
guidelines
Government \ G o v e r n m e n tlicensing
SOURCE: Office of Technology Assessment, 1995 Adapted in part from R Van de Velde, Hospital lnformation Systems:The Next Generation (Berlin:Springer-Verlag, 1992), p 107

38 | Bringing Health Care Online: The Role of Information Technologies
compliance with institutional guidelines. En-sembles of patient records meeting specific crite-ria can be assembled by scanning a databasedescribing more than 800,000 patients and 80 mil-lion separate clinical observations. Administra-tors use this capability for quality-controlpurposes and medical researchers use it to as-semble cohorts of eligible patients for clinicaltrials. The Regenstrief system is a hybrid of paper-based and computer-based information manage-ment: some information is captured anddisseminated electronically, but the system alsoprints reports of rounds made by physicians and aset of reminders, alerts, and customized encounterforms on paper prior to each patient’s visit. Clerkstranscribe and code the handwritten notes on theseforms after the encounter.45
Some of the institutional capabilities describedin this section are also available for individual orgroup medical practices through software thatadds the capability for clinical recordkeeping toadministrative practice management systems.
❚ Paper-Based Patient RecordsMost of the clinical and administrative informa-tion that flows throughout the health care systemis still recorded on paper. Over 10 billion pages ofpatient records are produced in the United Stateseach year,46 each of them a masterpiece of idio-syncratic functionality. In order to receive accredi-tation, hospitals must ensure that their recordsmeet certain minimum content standards estab-lished by the Joint Commission on Accreditationof Healthcare Organizations, as well as any con-tent requirements mandated by state regula-tions.47 In general, however, health careorganizations are free to determine how the in-formation is arranged. Institutions design theirown filing and communications systems to meet
internally determined information needs, and in-dividual departments often design forms to reflectinformation generated in self-contained proc-esses. To some extent, paper records are individu-alistic even to the level of single sentencesbecause much of the information is handwrittenand clinicians may phrase entries using their ownterms and conventions.
Box 2-1 lists some of the many types of in-formation that usually appear in a hospital’s paperrecords. Different types of providers might as-semble records with different content; for exam-ple, ambulatory care records generally have fewercategories of information than hospital records,but they may span a much greater time period be-cause they are historical records documentingmany encounters. Patient records also incorporateadministrative records such as letters, insuranceclaims, and bills, although these may be storedseparately from clinical records.
Paper records within a single folder have tradi-tionally been kept either in the chronologicalorder of collection or in source-oriented or pro-blem-oriented formats. Source-oriented recordsare organized with forms from nurses, physicians,labs, and other sources in separate sections. Prob-lem-oriented records organize the various notesinto a brief database of information identifying thepatient, a problem list of the aspects of the pa-tient’s condition that require treatment, an initialplan for treating the problems, and progress notesdetailing actions engendered by the problems andplans.
This nonstandardization of patient records isnot necessarily a symptom of poor design;instead, it is a reflection of the main task that pa-tient records once served. They were a highly de-tailed, patient-centered documentation of the careprocess and a record of everything that happened
45 C.J. McDonald and G.O. Barnett, “Medical Record Systems,” Medical Informatics: Computer Applications in Health Care, E.H. Short-
liffe and L.E. Perrealt (eds.), G. Wiederhold and L.M. Fagan (assoc. eds.) (Reading, MA: Addison-Wesley, 1990).
46 U.S. Congress, General Accounting Office, Automated Medical Records: Leadership Needed To Expedite Standards Development
(Washington, DC: General Accounting Office, 1993).
47 Some examples of state legal requirements for medical records are discussed in ch. 3.

Chapter 2 information Technologies for Transforming Health Care 39
The admission/discharge record provides a synopsis of the overall patient record. It contains basic
identifying and financial information about the patient, along with certain clinical information such as the
admitting and final diagnoses, a summary of the procedures performed and medical consultations, and
a description of the disposition of the patient. This record is typically organized on a sheet attached to
the face of the other paper records, which contain two broad categories of information:
Administrative data:■ Attestation statements certify that the diagnoses and procedures performed are accurately and com-
pletely documented to meet the requirements of Medicare and other payers.■ Conditions of admission record the patient’s consent to be admitted and receive routine services,
diagnostic procedures, and medical treatment.■ Consents for release of information allow the hospital to release health information to insurers or oth-
ers.■ Special consents authorize nonroutine diagnostic or therapeutic procedures.
Medical or clinical data:■ The medical history includes descriptions of the chief complaint, present illness, past medical history,
psychosocial history, family history, review of physiological systems, and physical examination of thepatient.
■ Physicians orders specify tests, medications, and regimens of care.■ Progress notes detail the course of the patient illness, response to treatment, and status at dis-
charge.■ Departmental reports record the contributions of the pathology, radiology, laboratory, physical thera-
py, respiratory therapy, and social service departments to the care of the patient.■ Nursing data include notes with detailed observations of the patient and descriptions of the nursing
care regime, a sheet recording the patient’s vital signs and fluid intake and output, and a sheet docu-menting the time and dosage of each medication the patient receives.
● Operative reports include an anesthesia report, description of the surgical event, and a recovery roomrecord.
= Discharge summaries concisely recapitulate the patient’s treatment in the hospital and its results
Coronary care, intensive care, psychiatric, and other special care units typically contribute their own
special forms to patient records. Obstetrics and gynecology units usually have specific forms that in
include a patient’s antepartum records and medical history, her labor and delivery records, postpartum
records, and a newborn record describing the baby’s care.
SOURCE: Adapted from Jonathan P Tomes, Compliance Guide for Electronic Health Records (New York, NY Faulkner & Gray, 1994)
pp. 31-32
with respect to a patient during a particular epi- The problem is that the functionality requiredsode of care. In ambulatory care settings, theywere also repositories of historical informationabout an individual’s previous care. The recordsmediated communications and conveyed instruc-tions and responsibilities among members of themedical team. In this context, designing a stan-dard format for documenting patient-clinician en-counters made about as much sense as trying toenforce a standard format for phone conversationsor diary entries.
of patient records has grown far beyond thebounds of recordkeeping and communicationwithin a limited team because of changes to boththe delivery system and clinical practice. Patientrecords are now widely used for legal, administra-tive, and research purposes. They have becomesources of information for determining eligibilityfor insurance payments and for documenting theextent of injuries or the quality of care for use inlegal proceedings. They may be used to provide

40 | Bringing Health Care Online: The Role of Information Technologies
data for evaluating the quality and appropriate-ness of care for peer review, accreditation, or otherquality assurance programs and for reportingcommunicable diseases and other required data tocivil authorities. With the advent of integratedmanaged care organizations, clinical records havebecome information sources for analyzing the re-source requirements, outcomes, and profitabilityof health care practices.
In response to these broader functions, patientrecords now have at least two phases. In the activephase, clinicians and administrators insert andedit information. As legal documents, patient re-cords are treated like other business records thatmight be needed in a trial. Recorded entries mustbe made by people with first-hand knowledge ofthe events, acting in their ordinary capacity, andthe time and date of each entry must be shown.When errors are found and corrected, the recordmust show clearly both the original entry and thecorrection, along with the name of the personmaking the correction. In the passive, permanentphase the patient record serves as an unalterablelegal record.48 Its contents are occasionally ex-amined, usually by users far removed from theclinical setting. At this point, information may beabstracted from the record for research or manage-ment purposes, and all links identifying the in-formation with a particular individual removed.
Even with this adaptation, paper records maynot be adequate for the information demandsof modern health care delivery systems. A num-ber of weaknesses of paper records have beenidentified:49
� Paper-based patient records document thecaregiving process inadequately. Medical re-cordkeeping is a hurried, ancillary activity inthe encounter room. Clinicians may not haveenough time to completely and accurately fillout the forms comprising the paper records, and
the required health information is sometimesunavailable or of questionable accuracy as thenotes are written. Physicians’ and nurses’ notesmay be illegible if handwritten, or inaccurate ifdictated and then transcribed. Detailed descrip-tions of the patient’s health problem and thereasoning behind diagnoses and choices of ser-vices may be left out or abbreviated becausethey are hard to summarize and tedious to re-cord. The voluminous data from physiologicalmonitors are difficult to record accurately byhand. Other components, such as laboratoryand radiological reports, may be missing be-cause of filing or communication errors.
� Paper-based patient records hinder informa-tion flow. Once information has been recordedwithin a set of bulky paper records, it may notbe readily accessible later. Efforts to compile amore complete paper record are likely to exac-erbate this problem. The data are bound to thepaper itself and individual pieces cannot besorted for relevance, making the record diffi-cult to use when dealing with multiple prob-lems or extended treatments. Collecting andaggregating data from multiple records for pur-poses of quality monitoring or clinical researchinvolves an expensive and time-consumingmanual search. Paper records can be in only oneplace at a time. Short of laboriously photocopy-ing and then shipping them by courier, recordsmay frequently be unavailable to a caregiverwho needs them. When the record is unavail-able, new data cannot be entered in a timelymanner; entries must often be made frommemory or copied from other forms or informalnotes. This can lead to the creation of “shadowrecords” that are difficult to coordinate with theprimary record set and which may contain con-flicting or anachronistic data. Finally, the data
48 J.P. Tomes, Compliance Guide to Electronic Health Records (New York, NY: Faulkner and Gray, 1994), pp. 9-11.49 Dick and Steen, op. cit., footnote 3; and M.L. McHugh, “Nurses’ Needs for Computer-Based Patient Records,” in M.J. Ball and M.F.
Collen, Aspects of the Computer-Based Patient Record (New York, NY: Springer-Verlag, 1992), pp. 16-29.

Chapter 2 Information Technologies for Transforming Health Care | 41
are only as secure as the paper itself, and entirerecords, or individual pages within a record,can easily be misplaced, damaged, lost, orstolen.
� Paper records impede the integration of healthcare delivery, research, and administration.The wide variety of formats, styles, and orga-nizational systems for paper records frustratesthe coordination of care between differentproviders, or even between departments orpractitioners in the same institution. The im-penetrability of the record means that there arefew tools that can use information in the paperrecords to generate reminders, decision aids,and other supports for work.
❚ Computer-Based Patient RecordsIf all the information in paper-based records weredigitized and embedded within information sys-tems that provide rapid, contextualized access tothe data and links to other information in the insti-tution, some of the shortcomings of paper record-keeping could be addressed:
� The health care delivery process could be fullydocumented. Information could be gathered asit is generated using a variety of conventionaland handheld computers equipped with key-boards, pen-based structured data entry, andvoice or handwriting recognition. Illegible orinconsistent entries could be caught and cor-rected as they are entered. Physiological moni-tors could collect data and insert themautomatically into the record after checking forerrors, noise, and inappropriate values. Con-flicting data from disparate sources could bereconciled and cross-checked for accuracy.Medical orders, their results, and all other inter-nal transactions could be tracked automatically.
� Health information could be unfettered. Itcould be stored as individually indexed itemsof information that could be abstracted into re-ports and compared among patients. Recordscould be accessed simultaneously by multipleusers and easily duplicated when necessary. In-formation anywhere in the record could be ac-cessed with minimal delay. Data could be
liberated from any one delivery medium anddigital devices that access them could be de-signed with a wide variety of capabilities andcapacities.
� Caregiving, research, and administrationcould be knit together. Data from digital re-cords could be extracted and exchanged ac-cording to consensus standards. Their contentcould be enriched through the development ofdecision support tools. Patient records could beshared within and across institutions, thusavoiding delays.
Not all approaches to collecting health in-formation meet these objectives equally well.Most of the benefits of computerizing the patientrecord are realized when information is deliveredto the caregiver or patient, but most of the expenseand problems of computerizing the patient recordare realized when the information is collected. Ingeneral, converting raw data into electronic in-formation that can be shared requires that caregiv-ers spend extra time and lose some flexibility intheir recordkeeping—at least initially—and it re-quires institutional investments for training,maintenance of standards, and redesigning workprocesses. The costs and benefits of electronic pa-tient records are proportional to the effort in-volved in collecting, organizing, and distillingdata into useful information.
For example, a page from a paper patient recordcould be stored electronically in many differentways. The information could be simply scannedand stored as an image (much like a fax) that is apicture of the paper form, but is not searchable oreditable. Document imaging systems are widelyavailable that use computers and optical disks tostore such images and make them available to cli-nicians on workstations with graphics terminals.These systems reduce the amount of physical stor-age space required for patient records, and they al-low the records to be shared by clinicians andadministrative offices without physically trans-porting the records. Preparing to implement animage-based system can help institutions stream-line their recordkeeping system by forcing them toanalyze the paper forms in use and eliminate re-

42 | Bringing Health Care Online: The Role of Information Technologies
dundant ones.50 Some systems allow clinicians touse electronic signatures to approve documentimages at the workstations, and others allow in-formation from laboratory instruments or othercomputerized processes to be captured as textalong with the images. While document imagingsystems can mitigate some of the problems of thepatient record, they are not really a step toward de-veloping a true computer-based patient record orprovider information system. They have the dis-tinct disadvantage of being primarily a collectionof images rather than a collection of separately ad-dressable facts about each patient, and the in-formation in those images cannot be easilyextracted or manipulated for reporting purposes orfor integration with decision support systems. Pa-tient records from document imaging systemscannot be easily shared with other departments orinstitutions using different record systems.
Additional effort can be expended as the dataare collected and stored to make the health in-formation in the records more useful. Documentimages can be converted to textual form either byapplying secondary processing techniques such asoptical character recognition or by manually re-typing the data using word-processing software.Paper documents and document images can besidestepped entirely by entering the data directlyinto computers through on-screen forms. Once in-formation is stored as text rather than images oftext, it becomes much more mobile because it canbe exchanged electronically as files or e-mail withother information systems. Free-text data is stillproblematic, however, because it is unstruc-tured—there is no set placement or format for theinformation it contains—and because the termsused in the text may have ambiguous or inconsis-tent definitions. These problems can be addressedby using databases that store data as discrete ele-ments that are separately addressable and edit-able—rather than as long, unstructured textfiles—and by the adoption of various standards toconsistently define the structure and content of
electronic messages between information sys-tems. Although the existence of various standardsmay be transparent to the clinician, the use of suchstandards is often facilitated through the use ofstructured data entry, where the organization ofdocumentation and the choices of terminology arepredefined and standardized.
Implementation of an information system withdatabases, structured data entry, and messagestandardization requires more sweeping changesin documentation practices than adoption of animage-based system, but the resulting patient re-cords are far more flexible and harness more of thecomputer’s power as an analytical tool. Becauseeach fact about the patient is stored discretely andcan be retrieved separately, information can be or-ganized and presented in different ways, depend-ing on the needs of the user. The records can easilyincorporate information from laboratory and ad-ministrative systems and the information systemsof outside providers, and they can be supplement-ed by decision support systems. On the otherhand, collecting such information in usable formfrom all the different sources can present a pletho-ra of organizational and technical hurdles. Be-cause of the costs involved, in terms of investmentin hardware and software, professional effort, andchanges in work process, organizations take thesehurdles a few at a time. Today, few, if any, providerorganizations have a completely electronic patientrecord. Most providers who are working towarddeveloping computer-stored records find them-selves somewhere along an evolutionary continu-um, using a hybrid system encompassing bothcomputer and paper records.
KEY TECHNOLOGIES FOR THEEMERGING HEALTH INFORMATIONINFRASTRUCTUREEmilia’s scenario at the beginning of this chapteris fictional; it portrays a suite of information toolsand resources harmoniously communicating with
50 “Case Study: The Toledo Hospital Turns to Document Imaging To Automate Emergency Center Medical Records,” Healthcare Telecom
Report, Sept. 26, 1994, vol. 2, No. 20, pp. 1, 5-7.

Chapter 2 Information Technologies for Transforming Health Care | 43
each other and integrated into health care deliveryin a way that is not available anywhere today.However, while the synergy between the tools isfictional, the tools themselves are readily avail-able. Information technologies have been used formany years in academic, governmental, and pri-vate research, in pilot projects, and in commercialproducts, and consensus is emerging on whichones will form the basis for an advanced health in-formation infrastructure. This section introducesseveral important communications and computertechnologies, including computerized data cap-ture and distillation, high-capacity digital storage,broadband telecommunications, and advancedhuman-computer interface techniques.
There are several reasons why the technologiesand standards underlying applications must be un-derstood for purposes of setting public policy.First, technological changes are challenging therelevance and enforceability of the existing bodyof state and federal law. Several states virtuallypreclude the development of computer-based pa-tient records by specifying in pen and quill legis-lation the required storage media for patientrecords.51 These laws were no doubt meant to en-sure the singularity and permanence of patient re-cords, but they were probably written without anappreciation of the compactness, duplicability,and durability of optical disks. While it is true thatoptical disks have only become available relative-ly recently, their features have been described andexpected for at least 20 years. To avoid inflexibleand inappropriate laws, it is important to considertechnological trends well in advance of their im-plementation.52
Second, technologies have inherent affor-dances53—they make some activities very easyand others more difficult, and they imposeconstraints on the behavior of users. For example,Canada has a telecommunications infrastructurethat ensures cheap, reliable data transfer usingmodems, and France has an infrastructure thatsupports the widespread use of smart cards, whichcan hold several pages of data and be carried in awallet. One result of the different affordances ofthese two technologies is that the experience ofprocuring health care and transferring patient re-cords in Canada is very different from that inFrance. In Canada, smart cards are being used totransfer data in small, special purpose situations,but the bulk of the flow of health information oc-curs over integrated data networks.54 In France,the extensive smart card infrastructure and theability of individuals to choose their own doctors,health care establishments, and pharmacies havegiven rise to over 70 different card systems. Basichealth information and the specific details relatedto a single treatment or prescription are encodedon a card and later accessed by the appropriatehealth care provider, government services agency,or pharmacy. The cards make patient records moreaccurate and mobile than paper records, but theydo not to contain a person’s entire health history.55
Legislative action that encourages specific tech-nological approaches, such as broadband commu-nications, inevitably affords some conveniences,some problems, and many striking changes inhow health care can be delivered. It is importantthat such consequences be anticipated before leg-islation is crafted.
51 The laws, which usually specify paper or microfilm records, are explained more fully in chapter 3.52 This caveat applies to legislation that might endorse any particular storage medium or other specific technology, including optical media.
For instance, the equipment to read optical disks is often obsolescent long before the disks themselves.
53 D.A. Norman, Things That Make Us Smart: Defending Human Attributes in the Age of the Machine (Reading, MA: Addison-Wesley,
1993), p. 106.
54 R. Alvarez, “Canadian Policies and Strategies for Health Cards,” unpublished paper presented at Cartes Santes conference, Marseilles,
France, September 1993.
55 Phoenix Planning and Evaluation, Ltd., “Potential Card Applications in the Health Care Industry,” unpublished contractor report pre-
pared for the Office of Technology Assessment, U.S. Congress, Washington, DC, January 1994.

44 Bringing Health Care Online: The Role of Information Technologies
Finally, despite the evanescent nature of high-technology products in an entrepreneurial society,successful technologies and standards have endur-ing influence. Each new generation of informationtechnologies forms a legacy that future genera-tions must support. At the cusp of what may be amajor expansion in the purchase of computers andtelecommunications equipment for health carepurposes, it is important that technologicalchoices embodied in legislative policy and gov-ernment procurements be consistent with long-range congressional goals for public health,medical research, and personal privacy. Thetechnologies described in the following sectionsare shown in table 2-1.
❚ Capturing Data at the Point of CareClinical records document brief encounters be-tween health care professionals and the patientthrough descriptive text, diagnoses, treatmentprotocols, and nurses’ notes typed or written byhand on charts and forms. Measurements of physi-ological variables are a second major source ofclinical data. Nurses, respiratory therapists, andother practitioners read these measurements frommedical monitors periodically and transfer themto the patient record. Although clinicians and oth-er end-users of patient records are most likely tobe held legally responsible for their quality, re-sponsibility for entering the data is often eitherdelegated to a transcriptionist or delayed until theend of the shift. Whenever the responsibility forinserting these types of data into the record is dele-gated or postponed, the possibility of incorporat-ing errors is increased.
Several new technologies may address thisproblem by capturing clinical data as they are gen-erated at the site of care. This generally improvesdata quality because that quality is best verified bythose who rely on it most frequently.56 These data
Human-computer interactionhandheld computershandwriting recognitionpersonal digital assistantsspeech recognitionautomated data collectionstructured data entry
Storage, processing, and compressioncomputer-based patient recordsmagnetic stripe cardssmart cardspicture archiving and communications systemsmedical imagingoptical storageimage compressiondigital signal processorsobject-oriented software design
Connectivityclinical information systemscabled, optical, and wireless networksInternet and electronic mailWorld Wide WebIntegrated Services Digital Network (ISDN)frame relayAsynchronous Transfer Mode (ATM)client-server computingmessaging and coding standardsproprietary and consensus standardsMedical Information Bus
Securitypasswordsfault tolerant computersredundant disk (RAID) systemsauthenticatorsencryptionfirewalls
Data distillationdecision support systemspattern recognitionartificial neural networksknowledge-based systemsrelational databasesknowledge discoverynatural language processingencoders and groupers
SOURCE: Office of Technology Assessment, 1995
56 S. Henderson et al., “Computerized Clinical Protocols in an Intensive Care Unit: How Well Are They Followed?” Proceedings of the
Fourteenth Annual Symposium on Computer Applications in Medical Care, vol. 14, 1990, pp. 284-288.

Chapter 2 Information Technologies for Transforming Health Care | 45
collection technologies include portable comput-ers, digital assistants, speech and handwriting rec-ognition, and the standardization of automateddata collection from medical monitors.
Portable computers may be either small ver-sions of desktop computers or they may incorpo-rate entirely new hardware, operating systems,and data organization paradigms. Laptop comput-ers are not widely used in hospital rooms becausethere is rarely a flat spot on which to rest them.Instead, tablet computers that can be operatedwhile being cradled in one arm are used. They usu-ally contain small hard drives, backlit screens, andbatteries that last a few hours before recharging.They may contain small PC cards (also known asPCMCIA cards) that allow them to communicatevia wireless modem or with short-range radio orinfrared receivers attached to the computer net-work in the hospital.57 They resemble laptop com-puters in size and weight, but their keyboards areeither missing entirely or folded behind the dis-play screen. The screen itself is a digitizer as wellas a display, which means that it can detect thepresence and position of a nearby stylus. The sty-lus is used like a mouse on a desktop computer topull down menus, activate icons, and press “but-tons.” Numbers and letters can be entered with thestylus via an image of a conventional keyboard,but medical applications for tablet computers typ-ically avoid ersatz typing as much as possible.Instead, the user chooses from a branching set ofpossible actions. For instance, to write a prescrip-tion, the doctor might use the stylus to pull down amenu to initiate the process and then choose “anti-biotic” from a short list of drug types that appears.A list of antibiotics in the hospital’s formulary ap-pears, and when one is chosen a list of appropriatedosages appears, and soon. However, if this proc-ess is poorly designed, the clinician is trapped in asingle mode of communication-Prescriptionwriting-until entirely finished. It may be diffi-
The Moto ro la Marco , a persona l d ig i ta l ass is tan t w i th hand-wr i t ing and ges tu re recogn i t ion and w i re less ne twork ing ca-pability Digital assistants and other handheld computersallow clinical data to be collected at the time and place ofcare.
cult to navigate through the series of lists and toback up and correct errors.
Personal digital assistants (PDAs) area differ-ent type of portable computer. As shown in thephoto, they fit in the pocket of a medical lab coat.They have smaller displays than laptop comput-ers, and their batteries last much longer. PDAsmay have wireless communications capabilities,and while they lack hard drives, they typicallyemploy high-performance computer processors.The extra processing power allows them to ad-dress some of the shortcomings of mobilecomputing without keyboards by using human-computer interface designs not found on desktopcomputers. One approach is to use a social inter-
57 PC cards are not limited to communications devices; they can contain more exotic equipment such as miniature hard drives, encryption
chips, or even atomic clocks.

46 | Bringing Health Care Online: The Role of Information Technologies
face such as that presented by devices employingGeneral Magic’s Magic Cap operating system.Different capabilities of the computer are repre-sented by different physical objects in a room por-trayed on the display. To write prescriptions, theclinician might tap on a picture of a notepad; shecould also tap on a medical reference book to lookup a drug’s description even as she works on theprescription.
Other PDAs use handwriting recognition ornovel data storage strategies, such as those facili-tated by Apple Computer’s Newton operating sys-tem. A wide variety of clinical applications havebeen written for Newton PDAs, including chart-ing and patient management software, medicalreference texts, applications for accessing drug in-formation and writing prescriptions, and calcula-tors for determining drug dosages, IV drip rates,and other common medical computations. Oneexample is the Constellation Project at Brighamand Women’s Hospital and Massachusetts Gener-al Hospital in Boston that equipped medical resi-dents with PDAs containing the AmericanCollege of Physicians’ Medical Knowledge Self-Assessment Program, an ICU/CCU Drug Refer-ence Book, the hospitals’ Medical ResidentHandbooks, a medical calculator, and several oth-er medical reference texts.58
Handwriting recognition attempts to recognizewords and letters within handwritten script. Opti-cal character recognition is a related technologyused with desktop computers and optical scannersthat attempts to recognize printed or neatly writtenblock letters on paper forms. Speech recognitionis yet another pattern-matching technology that
facilitates entry of textual notes into a computerwithout using a keyboard. The technologies un-derlying handwriting recognition and speech rec-ognition are briefly surveyed in box 2-2. Speechrecognition systems capable of recognizing spe-cialized medical vocabularies have been availablefor several years. They typically cost several thou-sand dollars per computer workstation. None ofthe current implementations of speech recogni-tion for clinical use is portable; they are usuallydeployed to reduce the delay and potential for er-ror involved in transcribing recorded notes, ratherthan as data collection devices at the point of care.Speech recognition systems are also useful in situ-ations where notes need to be taken, but the clini-cian’s hands are not free.
Another approach to making data collectionimmediate and accurate involves gathering all thedata generated by the suite of medical monitorsand therapeutic devices at the bedside without hu-man intervention. Automated data collectionhelps reduce the number of errors introduced andpropagated by end-of-shift recordkeeping59 andreduces the 40 to 60 percent of nurses’ time that isspent taking and organizing notes and charting pa-tient care.60 It supports vigilant care by employingcomputers to constantly monitor critical physio-logical variables and call attention to dangerousconditions, and by allowing caregivers to checkon current patient status and developing trendsfrom afar. By providing accurate and timely de-pictions of patient status, automated data collec-tion affords greater assurance that computer-based decision support tools will provide correctinformation on which to base a clinical decision.61
58 S.E. Labkoff et al., “The Constellation Project: Access to Medical Reference Information Using Personal Digital Assistants,” Proceed-
ings of the Eighteenth Annual Symposium on Computer Applications in Medical Care, vol. 18, 1994, p. 1024.
59 R.M. Gardner et al., “Real Time Data Acquisition: Experience with the Medical Information Bus (MIB),” Proceedings of the Fifteenth
Annual Symposium on Computer Applications in Medical Care, vol. 15, 1991, pp. 813-817.
60 B.W. Childs, “Bedside Terminals: One of the Answers to the Nursing Shortage,” Healthcare Informatics, vol. 7, No. 12, 1990, p. 37.61 T.P. Clemmer and R.M. Gardner, “Medical Informatics in the Intensive Care Unit: State of the Art 1991,” International Journal of Clinical
Monitoring and Computing, vol. 8, No. 4, 1992, pp. 237-250.

BOX 2-2: Speech and Handwriting Recognition
Doctors may someday consider pocket information tools to be as indispensable as stethoscopesand prescription pads. However, while they may be willing to carry some sort of small computer around,it is unlikely that they will carry a computer keyboard as well. Speech recognition and handwritingrecognition are two technologies that seek to liberate computers from keyboards by transferring di-rectly into the patient record any notes spoken into a tiny pocket computer or written on its face.
The diagram here shows a highly simpli-fied illustration of the speech recognition pro-cess. The computer digitizes the electrical sig-nal from the microphone and breaks it into sepa-rate utterances by identifying short pauses inthe speaker’s voice. The computer then usesFourier analysis to determine the frequenciesor pitches present in the utterance as a func-tion of time. A lower resolution signature is de-rived from this spectrum by slicing it into fre-quency bands and time segments and averag-ing the spectrum within each cell. Finally, thecomputer identifies the utterance by selectingthe best match for its signature from a library ofknown speech patterns. Searching for a matchwithin a library containing all possible humanutterances would be hopelessly difficult; in-stead, searches are usually constrained. Natu-ral language processing uses the syntax of pre-viously recognized words to limit the range ofpossible matches for the current utterance sig-nature, and the words in the library typically arefurther restricted to a certain domain of knowl-edge, such as radiology. Most of the calcula-tions in current speech-recognition systems aredelegated by the computer processor to spe-cialized chips called digital signal processors(DSPs).
Discrete speech recognition systems re-quire speakers to insert short pauses betweenwords. Continuous speech recognition systemsattempt the much more difficult task of recogniz-ing normal speech, which has pauses for punc-tuation but no natural silences between words.In this case, dividing the flow of speech into chunks is much more difficult and the utterances corre-spond more closely to phonemes than to words. Matching the utterance signature to a pattern in the
"defective heart valve"
"heart" waveform
"heart" spectrum
"heart" signature
"short" "heart" "smart"Pattern Library
Separate utterances
Calculate spectrum
Calculate average spectrum in cells
Recorded speech
Find best match in library
"heart"
• • • •
Constrain search
Previous results
(continued)
Chapter 2 Information Technologies for Transforming Health Care | 47

48 Bringing Health Care Online: The Role of Information Technologies
library is more difficult as well because phonemes can be legitimately combined in many more ways
than words, and syntax constraints are difficult to apply until the phonemes have been assembled into
potential words. The pattern library itself can be built in two ways. Speaker-dependent recognition sys-
tems require the user to build a database of his or her own voice samples. Speaker-independent rec-
ognition systems use a preassembled library assembled from averages of the voices of many speak-
ers. Adaptive systems customize a speaker-independent library to a user’s voice patterns over time.
Currently, discrete speaker-independent voice recognition systems are available for desktop com-
puters, but continuous voice recognition is limited to very brief phrases. Continuous, speaker-indepen-
dent speech recognition has been demonstrated in research laboratories on computers with 256 DSPs
operating in parallel.1 Most clinical applications employ adaptive or speaker-dependent technology
that typically must be trained for a few hours a day over a period of weeks by each clinician. Handwrit-
ing recognition is conceptually similar to speech recognition. The input variable is not the loudness of
the voice as a function of time, but the position of the pen’s tip as a function of time. Commercial hand-
writing recognition systems have been developed that focus on either block printing or cursive script.
Block printing, with well-formed, separated letters, is analogous to discrete speech; smoothly-con-
nected cursive script is analogous to continuous speech. The recognition accuracy of all these technol-
ogies is somewhere between 80 percent and 95 percent, which is to say that the text contained in this
box would have at least 40 mistakes.
Many experts have questioned the wisdom of using technologies that require either extensive train-
ing or the power of hundreds of desktop computers to enter “the patient complains of nausea” in the
patient record with 95 percent accuracy. It is likely that successful implementations of these technolo-
gies will be a hybrid of recognition technologies with other human-computer interface approaches. One
example of this is the PEN-ivory system.2 “The computer displays an encounter form with groups of
descriptive terms on it. When a term is chosen, PEN-ivory guides the clinician through progressively
deeper levels of description by displaying additional terms appropriate for the original choice. For
instance, circling “cough” brings up a display with “severity,” followed by choices of “mild, moderate,
severe” and similar sets of choices for “onset, “ “frequency,” and other criteria. The system must recog-
nize gestures such as circling of terms or crossing them out, but it need not directly recognize handwrit-
ing, The program compiles a paragraph of plain English text from content determined by the clinician’s
choices and transfers it to the patient record. Similar structured data entry approaches have been
employed in speech recognition systems, and they have an added benefit of helping to standardize
medical terminologies and descriptions in the patient record. The success of such an approach de-
pends on the details of its design and the preferences of its users. Some hybrid recognition systems are
constraining and inflexible, while others are developing into fast, reliable transcription systems.
In any system that transforms ideas or words into permanent records, there is a tradeoff between
two different conveniences: users want perfectly accurate transcriptions of their ideas, but they also
want perfect flexibility to structure or amend the ideas as they choose. The competition for speech and
handwriting recognition systems is provided by pens, pencils, and paper, which have achieved both of
these goals admirably for many years.
SOURCE: Office of Technology Assessment, 1995
1 R.C. Johnson, “Speech Recognition Popping Up All Over,” Electronic Engineering Times, Feb. 6, 1995, P. 35.2A.D. Poon and L.M. Fagan, “PEN-lvory: The Design and Evaluation of Pen-Based Computer System for Structured Data Entry,”
Proceedings of the Annual Symposium on Computer Applications in Medical Care, vol. 18, 1994, pp. 447-451.

Chapter 2 Information Technologies for Transforming Health Care | 49
Unfortunately, gathering data from medical mon-itors is not a straightforward task because differentdevices use different communication protocolsand physical connections. Box 2-3 describes theMedical Information Bus standard that is a pro-posed solution to this problem.
❚ Data Distillation ToolsCollecting clinical data as they are generated isonly the first aspect of the difficult problem of as-sembling digital patient records. As health careprofessionals manually enter data in conventionalpaper records, they perform several crucial but im-plicit tasks. They make judgments about the valid-ity of the data, often mentally filtering a rapidlychanging display or perhaps reconciling readingsfrom one instrument with those of other instru-ments measuring the same quantity. They certifydata as relevant by entering them in the record andreject aberrant observations, such as heart ratemeasurements made on a patient having a fit ofcoughing. They convert the data into a standardformat, with the physical layout of paper formsserving as an interface that structures the informa-tion and highlights its important parts for doctorsand other clinicians. Professionals think aboutwhat the data they are recording indicate about thepatient’s condition. Finally, they alert other care-givers if their observations suggest a criticalcondition.
Data distillation is an informal label for the ap-plication of a set of diverse information technolo-gies in the attempt to automate these secondaryfunctions traditionally performed as rapid, skilledhuman judgments. One expert has observed:
The great mass of useful numbers we gener-ate by computer has got to be tamed and con-trolled. We have learned how to make themeasurements. Now we must learn how to han-
dle the resulting data and present them in under-standable terms. Used right, automation canintegrate these data, simplify them, scan andevaluate them. Automation is not a cold-blooded monster-machine between us and thepatient. It is a tool to expand our medical power,to let us get closer to the patient, and take bettercare of him.62
Concerns about how to extract meaning from aperceived flood of health data are not new. Theywere mounting even in the early 1900s whenHarvey Cushing began arguing for the necessityof regular monitoring of blood pressure.63 Datadistillation technologies can help refine problem-atic medical data and inform clinical decision-making. In administrative and research contexts,they can also be used to discover patterns and cor-relations within massive compilations of healthinformation, an undertaking less tractable tomanual human effort.
Early computerized attempts to distill clinicaldata sometimes tried to fully automate the diag-nostic process. The programs asked the clinician aset of questions about a patient and then used theanswers to navigate among a branching set ofmutually exclusive alternative diagnoses. Theythen delivered the conclusion in oracular fashion;unfortunately, the conclusions were sometimeswrong, and few doctors suffer oracles gladly.These logical decision-tree systems overlookednot only the complexity, but the subtlety of medi-cal decisionmaking.
More recent systems attempt to support clini-cians’ thought processes, rather than supplantthem. Three types of data distillation systems incommon use are pattern recognition systems, neu-ral networks, and knowledge-based expert sys-tems. Pattern recognition is frequently used inmedical monitors to recognize emerging trends.
62 J.J. Osborne, “Computers in Critical Care Medicine: Promises and Pitfalls,” Critical Care Medicine, vol. 10, 1982, pp. 808-810.63 H. Cushing, “On Routine Determination of Arterial Tension in Operating Room and Clinic,” Boston Medical Surgical Journal, vol. 148,
1903, p. 250, as cited in R.M. Gardner, “Medical Data: Their Acquisition, Storage, and Use,” Medical Informatics: Computer Applications inHealth Care, E.H. Shortliffe and L.E. Perrealt (eds.), G. Wiederhold and L.M. Fagan (assoc. eds.) (Reading, MA: Addison-Wesley, 1990), p.369.

50 Bringing Health Care Online: The Role of Information Technologies
One of the challenges of assembling a fully digital patient record is finding ways to transfer into it the
wealth of physiological information generated at the bedside by sophisticated medical monitors, One
solution is to let the pulse oximeters, ventilators, IV pumps, and other devices do the job themselves. In
fact, most monitors could already do so if they could communicate with the hospital’s computers: many
bedside monitoring and therapeutic devices have, hidden (and forgotten) on their back panel, tiny
communications ports that can transmit in digital form the values displayed as numbers, lights, and bar
graphs on the front panel of the instrument, What is missing is agreement among manufacturers about
how that port should be designed and how it should exchange data with other machines. Such agree-
ments are difficult because different types of medical devices generate data in widely varying amounts,
qualities, and formats, and the communications interface must be implemented inexpensively so that it
represents only a small portion of the overall cost of the least expensive instruments.
Vendors of clinical data management systems often design proprietary adapters and software mod-
ules to Iink their computers to individual medical devices. When new monitoring devices are acquired in
an intensive care unit, the interface software and hardware must usually be procured from the computer
vendor. While this may be an adequate solution for some settings, one director of clinical computing at
a major hospital has said, “What happens to us as users is that: 1 ) we pay a premium price for compat-
ible devices that we are forced to buy from the primary manufacturer, 2) we do not get the monitoring or
measuring device at all, and 3) we are not able to Integrate the data from multiple devices convenient-ly." 1 While this grim assessment may not reflect everyone’s viewpoint, it is clear that the lack of industry-
wide Interface standards for medical devices has held back wide-scale connection of bedside devices
to the broader hospital information Infrastructure.
Consensus messaging standards such as HL7 (see box 2-8) and the IEEE P1073 Medical Informa-
tion Bus (MIB) standard may be one solution to this problem. The MIB committee is a group of doctors,
vendors, medical engineers, and Information system specialists that is seeking to address the problems
Inherent in proprietary and custom-device networking approaches by establishing a common standardfor the hardware and software used to communicate between medical devices. The MIB standard is
conceptually similar to standards that have been developed for communication among electronic de-
vices in airplanes, and it Incorporates many existing standards from other areas of communications and
computer design. The standard describes three types of “controllers” that comprise a medical device
network, Every medical monitoring device is associated with a device communications controller
(continued)
Electrocardiogram monitors, for instance, often cording to their shapes and a library assembled ofaverage the shape of a patient’s ECG trace for arrhythmia specific to the patient. Further tracesabout 20 heartbeats in order to build a profile of a are then compared to the patient own customized“normal trace.” Subsequent traces are then library of heart problems, and the urgency of ancompared to the normal trace; if they differ signif- alarm matched to the severity of the abnormali-icantly, they are classified as aberrations and an ty.64
alarm can be passed on to a caregiver. Moreover, Another type of pattern recognition can be im-the aberrant signals can themselves be sorted ac- plemented using arrays of interconnected simple
64 Gardner, “Patient-Monitoring Systems,” Medical Informatics: Computer Applications in Health Care, ibid., p. 382.

Chapter 2 information Technologies for Transforming Health Care 51
housed in an external adapter connected to an existing communications port or incorporated Internally,
perhaps on a single special-purpose integrated circuit. Every patient is associated with a bedside
communications controller located in a bedside computer. Caregivers can quickly connect multiple
medical devices to the bedside computer in a star topology and then disconnect or Interchange them
without turning off the power, Each device identifies itself unambiguously to the bedside controller and
automatically establishes communication when it is plugged in. The cables and modular connectors are
standardized so that medical devices can be redeployed rapidly much like telephones, modems, and
answering machines in the home.
A master communications controller connects the various bedside communications controllers with
each other and with the rest of the hospital information infrastructure through standard Ethernet or To-
ken Ring networks. Two-way communications among these three controllers provide the means for au-
tomatic transfer of data from bedside devices into the patient record and allow device settings to be
adjusted remotely. They also facilitate full integration of bedside data with data from other sources in the
institution and enable cooperation between devices and systems. Additionally, future devices wiII Iikely
Incorporate lights on the front panel that indicate whether reliable communication has been established,
and textual messages such as the name of the medication in an IV pump.
Software applications running on device, bedside, and master communications controllers will com-
municate among themselves by sending messages whose syntax is specified by a new object-oriented
Medical Data Device Language (MDDL) defined by the IEEE PI 073 standard. The MDDL is one of
many consensus messaging standards discussed elsewhere in this report that are used to mediate in-
formation flows within health care institutions,
KEY: IEEE = Institute of Electrical and Electronics Engineers
SOURCES: M.M. Shabot, “Standardized Acquisition of Bedside Data: The IEEE P1073 Medical Information Bus, ” International Jour-nal of Clinical Monitoring and Computing, vol. 6, No 4, 1989, pp. 197-204, R M Gardner et al , “Real Time Data Acquistion: Experi-
ence with the Medical Information Bus (MIB), ” Proceedings of the Fifteenth Annual Symposium on Computer Applications in Medical
Care, vol 15, 1991, pp. 813-817, and J. Wittenber and M.M. Shabot, “The Medical Device Data Language for the PI 073 MedicalInformation Bus Standard, ” International Journal of Clinical Monitoring and Computing, vol 7, No 2, 1990, pp. 91-98.
1 R.M. Gardner, “Federal Medical Device Regulations What Are the Implications for Respiratory Care?” Respiratory Care, vol. 33,
NO 4, 1988, pp. 258-263
processors 65 called artificial neural networks.Each processor makes a simple calculation basedon the values of a small number of input variablesthat might be physiological measurements for apatient. The output of the calculation for eachprocessor serves as the input for other processorsin the network. The network can be trained by us-ing its overall output to adjust the strengths of theconnections between various processors. Ideally,a neural network might be exposed to comprehen-
sive sets of physiological data gathered frommany patients who died from sudden pulmonaryembolisms, and then trained through the feedbackprocess until its output is consistent for all the pa-tients. If that feat could be accomplished, the net-work would then have “learned” which features inthe data set reliably indicate imminent pulmonaryembolisms, and it could then be used to monitorother patients. One problem is that comprehen-sive, comparable data sets covering multiple pa-
65 The processors are usually simulated in software rather than being discrete electronic chips.

52 | Bringing Health Care Online: The Role of Information Technologies
tients are very rare. One of the benefits of digitalrecordkeeping might be the compilation of datasets that could be used to train artificial neural net-works for clinical decision support.
Most of the decision support systems that issuealerts and warnings based on clinical data areknowledge-based systems, which attempt to inter-pret information about a patient using expertisecaptured in a computerized database known as aknowledge base. In a simple implementation, ap-propriate actions or diagnoses for a patient couldbe identified by matching words used by doctorsin their written encounter records with termsfound in a library of disease descriptions or knownpatient cases. More typically, expertise is capturedas a large set of heuristics (rules of thumb) ratherthan as textual descriptions. Knowledge engineersdesign these rule-based expert systems by inter-viewing medical experts and constructing rulesets based on the experts’ practical experiencesand insights, institutional policies, and the medi-cal research literature. A typical rule used with aventilator might read, “If a patient’s spontaneousbreathing rate changes by more than 10 percentand the change is larger than five breaths per min-ute and the breathing rate is between 0.5 and 70breaths per minute and the ventilator mode waschanged within the last minute, then bring thechange to the attending physician’s attention.”66
An inference engine coordinates the process of ob-taining information from the patient record or cli-nician, finding applicable rules, and reconcilingthe conclusions of multiple rules if the clinicaldata match more than one. Expert systems workwell in narrow application areas such as determin-ing appropriate antibiotic treatments. They areless successful in supporting decisions in broadly
defined application areas because it is difficult todefine and maintain a complete, up-to-date set ofrules. One implementation of a rule-based expertsystem in a hospital setting is the HELP system,profiled in box 2-4.
Distillation tools are also important for healthadministration and research after clinical and ad-ministrative data have been abstracted from indi-vidual records and stored in large institutionaldatabases. Relational databases organize datainto sets of two-dimensional tables and allow us-ers to retrieve information from specific rows andcolumns in the tables using brief requests in aquery language. While a relational databasemight be used to store the clinical and administra-tive data for the patients in an HMO, the data real-ly represent a complex multidimensional data set.It might be very difficult, for instance, to assemblewith a query all the data necessary for a cost-of-care analysis of a set of interventions using severaldifferent measures of resource consumption overtime in different units of the HMO. Online analyt-ical processing is a database query technique thatis optimized to support decisionmaking using in-formation from complex, multidimensional datasets.67 Querying techniques find sets of recordswithin a database that fit a desired pattern. Knowl-edge discovery techniques address the oppositeproblem: they attempt to identify patterns usefulfor describing a specified data set. For instance, atypical medical research data set generated in amulticlinic randomized trial designed to studysurgical interventions to control lipids contribut-ing to atherosclerosis included 1,400 variablesmeasured on 838 patients for 7 to 14 years.68
Knowledge discovery techniques can be used to
66 T.D. East, W.H. Young, and R.M. Gardner, “Digital Electronic Communication Between ICU Ventilators and Computers and Printers,”
Respiratory Care, vol. 37. No. 9, 1992, pp. 1113-1123.
67 A. Radding, “Blue Cross Climbs Mountain of Data with OLAP,” Infoworld, Jan. 30, 1995, p. 64.68 H. Buchwals et al., “The Program on the Surgical Control of the Hyperlipidemias,” Surgery, vol. 92, No. 4, 1982, p. 654.

Chapter 2 information Technologies for Transforming Health Care | 53
Clinical information systems built around computer-based patient records have the potential to im-prove the quality of health care. They can help clinicians manage complicated medical situations andmake informed decisions Involving many variables and complex calculations. Such systems can helpInstitutions evaluate and standardize the way clinicians deliver care. They also can facilitate the devel-opment and evolution of clinical policies and procedures based on the latest research results, on mea-sured links between clinical outcomes and practices, and on considerations, such as local pathogentrends, that may be unique to a particular institution. One example of a clinical information system thatachieves some of these benefits is the HELP (Health Evaluation through Logical Processing) systemHELP consists of several logical modules that support data collection and delivery at the point of careand provide a rich system of reminders, alerts, and prompts based on clinical protocols for care of spe-cific disease conditions.
The primary installation of HELP is at LDS Hospital in Salt Lake City, Utah, a private, 520-bed, tertia-ry-care hospital and teaching center associated with the University of Utah School of Medicine. TheHELP system was developed at LDS over a long period of time with direct Involvement of clinicians(Including nurses and therapists as well as physicians), researchers, and administrators in the design ofthe system. LDS Hospital is part of the nonprofit Intermountain Health Care, Inc., chain of hospitals andoutpatient clinics in Utah, Idaho, and Wyoming. The HELP system IS being installed at numerous loca-tions within the Intermountain system and at several other hospitals around the nation. It IS distributedcommercially by 3M Health Information Systems of St. Paul, Minnesota.
The HELP system at LDS is installed on a centralized group of twelve fault-tolerant processors linkedthrough other computers to over 1,000 terminals at patient bedsides and other sites throughout the hos-pital. Nurses, physicians, respiratory therapists, and others enter data manually through keyboards as acombination of multiple choice selections, number entry, and some free text entry. In the intensive careunit, many of the medical devices, such as ventilators and pulse oximeters, are Iinked directly to theHELP system. Patient information is stored in a central patient database connected to the medical re-cords department, radiology and surgical units, and many of the laboratories and other departments.The system processes an enormous amount of information, including over 18,000 data entry items perday for respiratory care alone.
Each data entry is screened by a decisionmaking processor against a series of protocols stored in aseparate medical knowledge base. The protocols are derived from the published literature and fromconsensus opinions of experts at LDS and at other institutions. They are also derived from analysis ofthe clinical results for selected groups of LDS patients. The protocols may be simply algorithms for cal-culating derived quantities from measured variables in order to save time and reduce errors. They mayalso be decision criteria that recognize and alert clinicians to potential drug allergies, drug-drug inter-actions, drug selection and dosing problems, organ dysfunction, or critical changes in laboratory orphysiologic parameters. Costs and charges for clinical care are routinely computed and displayed forall chargeable items and for all nonphysician personnel time.
Managing a complex clinical situation such as ventilator support of respiration can involve consider-ation of hundreds of potential variables and sources of information. HELP protocols rationalize and sys-tematize that process. They are developed by small working groups, first as flow diagrams on paperand later as software code. Protocol calculations and recommendations are displayed on bedside ter-minals and incorporated into printed documentation including shift reports, daily rounds reports, weeklyreports, daily administrative and management reports, and final reports when patients are discharged.Clinicians may deviate from the recommendations of the protocols, but typically they must justify their
(continued)

54 Bringing Health Care Online: The Role of Information Technologies
decisions with defensible reasons apart from personal style preferences. The quality and efficacy of the
protocols are continuously monitored through daily log reviews, on-call reports, and personal feedback
from clinicians to the working group.
One application of HELP protocols has been the empiric design of antibiotic therapies. Antibiotics
can be targeted to a patient’s specific pathogens once they have been identified through microbiologi-
cal tests, but it is often impractical to wait for the results of laboratory cultures before beginning antibiot-
ic therapy. Broad-spectrum antibiotics (which are more expensive than single-agent antibiotics) are
often prescribed in this situation, and HELP protocols have been developed that recommend one or
more antibiotics effective against the most probable pathogens at the lowest possible cost. They use
data from the computer-based patient record and infection-specific Information and identify the most
likely pathogens on the basis of those Identified in patients with similar characteristics during the pre-
vious five years and the most recent six months. The recommendations are tailored to the infection site
and to the patient’s allergies and renal problems. The data are updated every month to provide trend
analysis of pathogens and antibiotic resistance patterns within the hospital. Clinical trials have shown
that physicians using the protocols prescribe regimens that cost less, utilize fewer antibiotics, and cov-
er a broader range of pathogens than those recommended by physicians in the absence of decision
support.
HELP protocols have also been used to contribute to the quality of clinical research through stan-
dardization of the care process one example involves randomized clinical trials at LDS comparing two
therapies for patients with adult respiratory distress syndrome (ARDS). Mechanical ventilators are used
to support the breathing of ARDS patients. Since their lungs are severely dysfunctional, high pressures
and volumes of air are sometimes required to maintain sufficient oxygenation levels, but the vigorous
ventilation can itself cause further lung injury. One alternative therapy revolves ventilation at lower fre-
quencies and pressures and removal of C02 outside the body. Each ventilation technique is compli-
cated and involves numerous adjustments of ventilator parameters throughout a month of care, com-
parison of the two therapies is extremely problematic unless the criteria for controlling the ventilators are
standardized for a suite of patients. HELP protocols were developed that assured equivalent intensity of
care for patients in trials of the two therapies. All the patients under protocol-guided care showed high-
er survival rates than expected from historical patterns, and the uniformity of care afforded by the proto-
cols allowed direct comparison of the two ventilation therapies.
SOURCE: R.S. Evans et al., “lmproving Empiric Antibiotic Selection Using Computer Decision Support, ” Archives of Internal Medi-cine, voI. 154, 1994, pp. 878-884, A.H. Morris, “Protocol Management of Adult Respiratory Distress Syndrome, ” New Horizons, vol.1, No. 4, 1993, pp. 593-602
find useful correlations or causal connections ❚ Storage and Compression Technologiesamong the variables in such large databases; the Clinical monitoring and imaging devices spawncorrelations that are found can then serve as a copious amounts of data. For example, pulse oxi-knowledge base for a rule-based expert system.69 meters report with every heartbeat the con-
69 J.M. Long et al., “Automating the Discovery of Causal Relationships in a Medical Records Database, " in Knowledge Discovery in Data-
bases, G. Piatetsky-Shapiro and W.J. Frawley (eds.) (Menlo Park, CA: AAAI Press/The MIT Press, 1991 ), pp. 465-476.

Chapter 2 information Technologies for Transforming Health Care 55
Average number Average storageDynamic range of images requirement
Modality Image size (pixels) (bits) per exam per exam (MBytes)—Computed tomography
.— —512 X 512 12 30 – 15.0
Magnetic resonance imaging 256 X 256 12 50 6 5
Digital subtraction angiography 1,000x1,000 8 20 200
Digital fluorography 1,000x1,000 8 15 150
Ultrasound imaging 512 X512 6 36 9 0
Nuclear medicine 128 X 128 8 26 0 4
Computed radiography 2,000 x 2,000 10 4 32.0
Digitized film 4,000 x 4,000 12 4 128,0
SOURCE: Adapted from K.G. Baxter et al.,“Wide Area Networks for Teleradiology,” Journal of Digital Imaging, vol. 4, No. 1, 1991, pp. 51-59
centration of dissolved gases in the blood. Trans-ferring this oxygenation data directly into the re-cord would generate about 1.5 million bytes ofinformation per day per patient---equivalent toabout 400 pages of numbers—and the majority ofthe data would never be accessed again.70 Institu-tions that develop systems for rapidly collectingand distilling large quantities of health informa-tion will need to judiciously moderate their appe-tites for information and refine their skills fordetermining which data can be safely discarded.Nonetheless, the demand for permanent storage ofpatient records is growing rapidly.
Some storage technologies make selected por-tions of patient records portable. Many institu-tions issue the ubiquitous magnetic stripe card totheir patients for identification purposes. Thesecan store about 250 text characters, enough to holda patient’s name, address, identification number,date of birth, copayment information, and a briefpassword. They are widely used in combinationwith low-speed modem networks to verify pa-tients’ eligibility for insurance benefits. Smartcards are the same size as credit cards, but theyhave embedded computer chips and enough staticmemory to hold several pages of textual informa-
tion. Laser optical cards have an even greater stor-age capacity, although once information is writtenonto the cards it typically cannot be altered or sup-plemented. None of these card technologies canreplace computer-based patient records becausethey are vulnerable to loss and fail to provide con-tinuous access to an individual’s health data. Theymay be widely employed, however, to carry emer-gency medical information and the demographicinformation necessary to coordinate a patient ac-cess to services at multiple sites. Smart cards havebeen used in several states to coordinate deliveryof multiple social programs, such as Medicaid andthe Women, Infants, and Children nutritional pro-gram (WIC), and to replace paper vouchers andfood stamps.
71 They are widely used in Europeanhealth care systems. An infrastructure of smartcard readers has not developed yet in the UnitedStates, largely because the existence of a reliableand relatively cheap telecommunications systemhas made modem communications and magneticstripe cards a more attractive way to exchangesmall amounts of data.72
The storage requirements for textual and nu-merical data in patient records are dwarfed by thestorage space requirements shown in table 2-2 for
70 East et al., op. cit., footnote 27.71 Phoenix Planning and Evaluation, Ltd., op. cit., footnote 16.72 Card technologies are discussed more fully in chapter 3, box 3-4.

BOX 2-5: Digital Image Compression
Image compression technologies play a crucial role in enabling the efficient storage and inexpensivedissemination of medical images. The digital images shown in this box are representations of dental x-rays (for illustrative purposes, they have been digitized with a far lower resolution than usual radiographicimages). The top image occupies approximately 96,000 bytes of storage space on a computer disk. Thesecond image occupies only 21,000 bytes of storage space; it has been compressed using a compres-sion standard known as JPEG (Joint Photographic Experts Group). The two images are virtually indistin-guishable, but subtracting one image from the other (and enhancing the contrast of the result) revealsthe information that was lost in the compression, asshown in the bottom image. This difference image wouldbe a uniform white if the compression were lossless.Instead, the image contains delicate grey patterns thatrepresent some of the subtle details present in the origi-nal image but missing from the compressed image.
The apparent similarity of the top two images is largelyan artifact of the printing technology used in this report:the differences would be more noticeable had the filmsbeen reproduced on a high-resolution image setter. Simi-larly, the appropriateness of compression in hospital set-tings depends on the display technology used to presentthe image. To reproduce the enormous dynamic rangeand spatial resolution of traditional photographic films,radiological images used for interpretive diagnosis aretypically sampled 2,000 times per inch and displayedon expensive high-resolution monitors. Compressiontechniques that result in any loss of detail may be inap-propriate for display of such images. Medical imagesare used in many other less demanding contexts, how-ever. For instance, the referring physician may wish todiscuss the image with the radiologist over the telephonewhile viewing it on a desktop computer monitor that is in-capable of displaying the subtleties of the image, even ifthey were present in the file. JPEG or other compressiontechnologies are often used in situations like this to reduce
(continued)
56 | Chapter 2 Information Technologies for Transforming Health Care
medical images such as x-rays, magnetic reso-nance images, and computed tomography scans.These new imaging technologies challenge theability of information systems to store and pro-cess data, but they enable the development of newgenerations of highly localized surgical and radia-tion therapies that otherwise would not be pos-sible. The computational resources necessary formedical imaging will continue to grow with theincreasing use of high-resolution spatial imaging,in which multiple images are assembled into a
Original Image 96kBytes�
Compressed Image 21kBytes
Difference (contrast enhanced)
three-dimensional model, and with the develop-ment of functional imaging, where processes suchas the rate of oxygen metabolism in a particularbody structure are studied by assembling multiplecopies of the same image over time.
Conventional films from x-ray and nuclearmedicine images are converted to electronic formusing laser digitizers, but many other imaging tech-nologies produce digital images from the outset.In some cases, images are compressed using tech-nologies like those described in box 2-5 to re-

Chapter 2 information Technologies for Transforming Health Care 57
the size of an image file by a factor of 10 or more. Minimizing the size of image files is even more impor-
tant when they are to be transmitted to a remote site over a telemedicine link or modem because com-
pression can drastically reduce the cost and the elapsed time necessary to transmit the image
Compression technologies work by eliminating redundant information in images. Natural images
contain coherent patterns: colors and tones usually change slowly across the width of an image. When
an image is relatively free of noise (like the “snow” on a television screen), the intensity of each tiny area
@xc/) in the image is often related to the intensity of its neighboring pixels. For instance, if the numbers
1 to 9 are used to represent the tones from black to white, then a series of pixels in the dental x-rays
above that cross the boundary of the tooth might be represented by the string of numbers:
11111111133399999999. A simplistic method for compressing the sequence of greys is run-length en-
coding, in which the string could be replaced by the much shorter string: 91 ’33 ’89, that is, “nine 1‘s,
followed by three 3’s, followed by eight 9’s.”
Practical schemes for image compression are much more sophisticated. The JPEG compression
used for the dental images divides the image into cells containing 64 pixels. Within each cell, the com-
ponents of the picture that vary quickly across the cell are separated from those that vary slowly. The
high-frequency components are suppressed or discarded; they appear as the rapidly varying grey and
white pattern in the bottom image above. Remnants-of the 64-pixel cells are also visible in the bottom
dental image.
Compression technologies are used extensively to store and transmit digital medical images. They
have become very fast and inexpensive as a result of the intensive development efforts by computer
and communications companies seeking ways to efficiently transmit digitized images and video for
publishing and broadcasting.
SOURCE: Office of Technology Assessment, 1995.
duce transmission times and storage space re- machines. The imaging machines can share thequirements. Medical images are typically storedand manipulated on large hard drives, similar tothose in desktop computers, and then transferredto digital tape, magneto-optical disks, recordableCD-ROMs, or COLDS (Computer Output to LaserDisks) for archival storage. The latter threetechnologies use light beams to store and recordinformation on durable plastic or magnetic disks.Although the disks themselves are likely to last formany decades, it is not clear that the equipmentnecessary to read the disks will be manufacturedthroughout the life of the medical information.
Medical imaging is an ideal domain for integra-tion of information technologies. The variousimaging machines are expensive and so highlyspecialized that no single vendor can impose pro-prietary standards on vendors of different types of
same type of displays and data manipulation com-puters, however, and this has encouraged the de-velopment of broad data exchange standards.Radiology and nuclear medicine are consultativedisciplines, but since the images need not be inter-preted at the site where they are collected, con-sultations can be carried out at a distance or evenover telemedicine links. Radiologists usually ex-amine images displayed with the highest possibleresolution, but primary care physicians who relyon their interpretations may also wish to have ac-cess to lower resolution copies of images in orderto explain the interpretations to patients. Finally,an economic incentive exists for developing fullydigital image storage: medical images are amongthe most commonly misplaced or unavailable re-cords. Some 40 percent of all x-ray films are unre-

58 | Bringing Health Care Online: The Role of Information Technologies
trievable, making it necessary to repeat imagingprocedures and extend hospital stays.73
Information systems that manipulate, store,and share digital medical images are called PACS,or picture archiving and communications systems.PACS typically capture data directly from animager or a laser film digitizer, and then allow us-ers to share and modify them using a computer, acommunications network, a large storage system,and a high-resolution display. The communica-tions between hardware components are governedby a mature standard for PACS developed by acommittee of the American College of Radiologyand the National Electrical ManufacturersAssociation.74 The DICOM (Digital Imaging andCommunications in Medicine) standard is one ex-ample of a communications standard. It definescommon formats for data generated by imagingequipment and standard actions that can be per-formed on the images. It specifies how messagesabout the data and the processing actions can beexchanged among machines.
The DICOM standard also specifies ap-proaches to compliance reporting and testing.Vendors that sell machines purporting to adhereto the DICOM standard must publish compliancestatements indicating which portions of the stan-dard are implemented. Hospitals can then comparecompliance statements for all the equipment theypurchase and build a functional PACS system us-ing equipment from a variety of vendors. This isone example of how the development of industry-specific voluntary standards can help remove bar-riers to technology implementation.
The character of radiological practice is chang-ing as PACS develop. PACS make it easier for pri-mary doctors to consult radiologists, but they also
enable doctors to examine radiological imagesfirsthand and make their own interpretations.75
The development of PACS may eventually helptransform radiology into more of a laboratory ser-vice than an independent medical discipline inhospitals.
❚ Display and Retrieval of DataMost hospital information systems use the normalgraphical and textual interfaces found on desktopcomputers, thus exposing their legacy as primari-ly administrative information systems. It is notclear, however, that interfaces developed for ad-ministrative and business applications will be ad-equate for conveying the huge amount of clinicalinformation that will become available if patientrecords are fully digitized. The stakes are high be-cause floods of new data make it increasingly like-ly that people will overlook important parametersand make faulty judgments.
Consider the difficulties in presenting all thetypes of information in the patient record on asingle computer display. One candidate for such alocus of information might be bedside patientdata management systems, which are dedicatedcomputers connected to various physiologicalmonitors for a patient in an intensive care unit.Currently, they need to display physiological datafrom up to 10 monitors, either as text or wave-forms. If those data are to be entered automaticallyinto electronic records rather than summarized onpaper forms, the interface must provide ways forusers to attach vocal or textual annotations to thedata.76 If the bedside computer is to be linked tothe broader hospital information systems, the in-terface must then be able to cluster associated data
73 S.C. Horii et al., “A Comparison of Case Retrieval Times: Film Versus Picture Archiving and Communications Systems,” Journal of
Digital Imaging, vol. 5, No. 3, 1992, pp. 138-143.
74 American College of Radiology, National Electrical Manufacturers Association, “Digital Imaging and Communications in Medicine
(DICOM): Version 3.0,” Draft Standard, ACR-NEMA Committee, Working Group VI, Washington, DC, 1993.
75 H.L. Kundel, S.B. Seshadri, and R.L. Arenson, “Clinical Experience with PACS at the University of Pennsylvania,” Computers and Medi-
cal Imaging Graphics, vol. 15, No. 3, 1992, pp. 197-200.
76 E.H. Shortliffe and G.O. Barnett, “Medical Data: Their Acquisition, Storage, and Use,” Medical Informatics: Computer Applications in
Health Care, E.H. Shortliffe and L.E. Perrealt (eds.), G. Wiederhold and L.M. Fagan (assoc. eds.) (Reading, MA: Addison-Wesley, 1990).

Chapter 2 Information Technologies for Transforming Health Care | 59
from a broad variety of sources according to pa-tient status: if a patient has an electrolyte imbal-ance, for instance, all the relevant laboratoryresults, dietary information, and treatment ordersshould be displayed alongside blood chemistrydata from a bedside analyzer. Because medical de-cisions are usually made with information from awide variety of sources, including laboratoriesand radiology departments, the display must ac-commodate textual notes and display high-resolu-tion images77 and video.
By now, the display is getting a bit cluttered,but there is more. Clinical decision support mightbe implemented at the bedside so clinicians can bealerted to potentially dangerous situations, such asdrug-drug interactions and critical changes in lab-oratory and physiological parameters. If so, thenthe screen must not only display the alerts, butprovide contextual information so they can beevaluated; it will need to show an appropriateamount of historical data along with the currentdata. To enable clinicians to act on whatever deci-sions they make, the display must provide chart-ing and order-entry forms. If administrativefunctions are integrated as well, the display willneed to notify clinicians of the prices of the medi-cations and lab tests they order, and displaye-mail, calendars, and scheduling information. Itmust do all these jobs without the aid of the manytools and customizations that help users cope withdesktop computers because bedside computersneed a standardized interface to accommodatemultiple users.78 And on top of all that, the inter-face should provide for easy editing and annota-tion of all the types of information mentioned thus
far, as well as robust security and methods for cli-nicians to disavow data that they do not trust ordeem irrelevant.
All of these objectives have to be accomplishedon video monitors smaller than a standard pieceof paper. In fact, the standard piece of paper re-mains the main competitor to video displays formost of the information tasks listed above, andmany institutions that have implemented the mostcomprehensive computer-based patient recordsincorporate high-volume printing as their in-formation distribution medium.79 Printed pagescan display up to 20 times more information in agiven area than standard computer monitors.80
Even computer displays with high-resolutiongraphic monitors often sacrifice much of the avail-able display area to a plethora of semi-permanent“buttons” and other interface elements designedto receive information from users rather than con-vey information to them.
It is not clear that the display techniques suit-able for desktop computers or current-generationpatient data management systems are appropriatefor high-bandwidth display of clinical informa-tion. Interface designers have developed very ef-fective techniques for conveying complicateddata to users (in aircraft cockpits, for example) andfor receiving complicated data from users (viaspreadsheets and word processors), and even forletting users browse within complicated data sets(through hypertext and graphical database front-ends). The medical environment is a curious mixof those three situations. Design approaches thatare sufficiently capable may not yet haveemerged. Many of the frustrations evinced in pilot
77 Current monitors used at the bedside have neither the spatial resolution nor the dynamic range to display diagnostic-quality radiologicalimages.
78 This consideration is less critical for long-term users who might design customized presentation configurations to be displayed accordingto their preferences whenever they use a computer. Nonetheless, the basic functionality of the health information system and the accessibilityand interpretability of data it presents must not rely on such customizations because the systems are often used by a rapidly changing ensembleof users with little time for training.
79 C.J. McDonald et al., “The Regenstrief Medical Record: 1991 A Campus-Wide System,” Proceedings of the Fifteenth Annual Symposium
on Computer Applications in Medical Care, vol. 15, 1991, pp. 925-928.
80 This is a conservative estimate. For a discussion of high-density information display, see E.R. Tufte, Envisioning Information (Cheshire,
CT: Graphics Press, 1990), pp. 37-51.

60 Bringing Health Care Online: The Role of Information Technologies
projects are due to inadequate solutions to human-computer interface problems. In the absence ofnew developments, the displays at the patient’sbedside, the nursing station, and the physician’sdesktop are potentially “choke points” throughwhich most of the benefits of a fully computerizedpatient record may fit only awkwardly. The ad-vantages of the computer-based patient recordmay be elusive, if only because they cannot be en-visioned.
❚ Data SecurityPeople reveal highly sensitive information tohealth professionals. If clinicians or institutionsmisuse or misrecord the confidential information,it might be used to restrict or revoke a person’shealth insurance or revise judgments of their suit-ability for a job or a loan. When such mistakes aremade, it is often difficult for the individual to cor-rect them or hold anyone accountable. Any newhealth data recordkeeping system must ensure thatinformation is used appropriately or people willavoid using it. In a 1993 Harris-Equifax poll, 27
percent of those responding indicated that theirpersonal health care information had already beenimproperly disclosed and 71 percent indicatedthat they felt that use of computers would need tobe restricted in order for privacy to be protected.81
Several issues are involved. First, health in-formation needs to be confidential: it should beused only for approved purposes and shared onlyamong authorized people typically associatedwith the patient by a special relationship, such asthe physician-patient relationship. Second, an ap-propriate level of privacy for the information mustbe established: some balance must be struck be-tween an individual’s right to keep informationconfidential and the benefits that can accrue to so-ciety if the information is shared more broadly. Fi-nally, the records must have adequate security:administrative and technical measures must pro-tect them from unwarranted loss, modification, ordissemination. Several technological approachesto securing electronic patient records by restrict-ing access are discussed in box 2-6. Maintainingthe privacy, confidentiality, and security of patientrecords presents organizational and political
Appropriate use of health information can only be ensured if those trusted to use the information
merit that trust. However, there are technological approaches to ensuring that the data cannot be inad-
vertently lost, damaged, or erased, and that they are only available to a defined community of users.
If a computerized patient record system is to operate without a paper backup system, it must func-
tion reliably all of the time. To ensure data integrity, computer systems often store critical data on redun-
dant arrays of independent disks (RAIDs). These arrays write data onto two or more hard disks simulta-
neously, In addition to providing a backup copy of the data, RAIDs also speed up the system, making
data accessible from the disk that can retrieve them the quickest. One of the disks is taken offline for a
few minutes once each day, and a copy of its contents can be transferred to a backup tape while the
other disk continues to function, after the backup is completed, the disks are desynchronized. The data
on the tapes are often transferred to magneto-optical or CD-ROM disks for longer term storage. Multi-
ple copies may be made, with one copy remaining offsite. Redundancy is also used for the central
processing units and other hardware components of fault-tolerant computer systems so that faulty compo-
(continued)
81 Louis Harris and Associates, A.F. Westin, The Equifax Report on Consumers in the Information Age (Atlanta, GA: Equifax, 1990).

Chapter 2 information Technologies for Transforming Health Care 61
nents can often be identified and replaced without turning off the computers. Using these techniques,
patient record systems have been designed that are available for use 99.5 percent of the time.1
To restrict access to records to authorized personnel only, clinical personnel must enter their name
and a personal password before accessing computer files. This restriction only works if the password
cannot be overheard or easily guessed. Some systems either assign complex passwords or require that
they be periodically changed, but this raises the possibility that the passwords will be forgotten or mis-
Iaid because they are more difficult to remember. More robust techniques require that authorized users
possess some physical device in addition to a password. One such device is a handheld authenticator,
which encrypts a user’s password using a short string of text issued as a challenge by the host comput-
er. The challenge text, and hence the expected response, can change with each attempted access to
the computer. Alternatively, security systems might require that a device such as a smart card be in-
serted in the computer while files are being accessed. Finally, biometric identifiers such as a retinal
scans or fingerprints can Identify authorized computer users, although these techniques are rarely
employed in health care institutions because they require expensive equipment.
Maintaining a usage log of all documents accessed and changed helps discourage improper use of
records by unauthorized (or even authorized) personnel, The log can be scanned manually or automati-
cally to detect attempts to log onto the system or change files, and its presence discourages such at-
tempts. The integrity of a document and responsibility for its contents might be additionally certified by
the use of digital signatures.
In principle, a hospital might choose to protect its patient records by using encryption techniques as
well, making the information uninterpretable. It could encrypt data using symmetric encryption, where
all users of the data would need to know a particular decoding password, or it might use asymmetric
encryption, where the documents for a particular user are encoded with a well-known public key and
decoded using a private key known only to the intended user. In practice, clinical documents and mes-
sages are intended for rapid access by multiple users; they are rarely encrypted because it slows down
the processing and because an adequate public key infrastructure has not been established.
Health care institutions often connect their computers to broader networks of computers so their
members can communicate via e-mail and have access to remote databases and internet resources.
Separate computer networks are sometimes maintained to isolate patient records from these commu-
nications needs. Alternatively, firewalls may be put in place that stand between computer networks in-
ternal and external to the health care institution; firewalls are systems of computers and switches that
restrict to approved locations the destination or source of data packets entering or leaving the hospital’s
network.
SOURCE: Office of Technology Assessment, 1995 Adapted in part from U S Congress, Office of Technology Assessment, Informa-tion Security and Privacy in Network Environment, OTA-TCT-606 (Washington, DC: U.S. Government Printing Office, September
1994)
40 Institute of Medicine, The Computer-Based Patient Record: An Essential Technology for Health Care (Washington, DC: Nation-
al Academy Press, 1991), p 74

62 | Bringing Health Care Online: The Role of Information Technologies
challenges as well as technical challenges; theseissues have been discussed in detail in an earlierOTA report.82
When institutional security standards govern-ing the handling of paper-based patient records areinadequate, the records can easily be lost orviewed and copied without leaving any trace ofthe action. Still, while the confidentiality of paper-based records is easily compromised by autho-rized people who misuse their access to patientinformation, the sheer bulk of paper records helpskeep them private: information is not easily ab-stracted from paper records. The fluidity of com-puter-based patient records, however, makessecuring their confidentiality more problematic.
One of the benefits of computer-based recordsis that information can be used for multiple pur-poses. The effectiveness of a certain AIDS treat-ment might be evaluated, for instance, bycomparing the outcomes of various treatments fora panel of individuals enrolled in a controlledstudy. Unfortunately, even if patients’ names areremoved from copies of the relevant informationextracted from their records, their identities canoften be determined by correlating the data withinformation in other publicly available electronicdatabases. One challenge is to develop identi-fiers for patients and providers that will allowmedical data to be exchanged among various in-formation systems without compromising the pa-tients’ privacy.
In addition to developing unique identifiers, aset of privacy principles need to be establishedthat govern who can access health information andhow they may use it. Many private and public sec-tor groups have developed strategies and policiesfor protecting the privacy of health information.For example, the Privacy Working Group of theInformation Policy Committee, Information In-frastructure Task Force has published a set of draft
principles for providing and using personal in-formation in all contexts, including health care ap-plications.83 Among other provisions, theseprinciples direct those who plan to collect person-al information to assess the impact of those planson individual privacy and to limit the amount ofinformation collected to that necessary for theirimmediate use. In addition, they should inform in-dividuals why their information is being col-lected, how it will be protected, and how it will beused, and they should take reasonable steps to pre-vent the disclosure or improper alteration of per-sonal information. The principles also chargeindividuals with the responsibility to understandthe consequences of releasing personal informa-tion and to discern how and why their informationis being collected. The working group’s principlesencourage both education about the uses of per-sonal information and the establishment of rightsof redress for privacy abuse. Legislative actionmay eventually be appropriate to guarantee theprivacy of health information as consensus devel-ops on appropriate policies.
❚ High-Bandwidth CommunicationsWithout telecommunications and networkingtechnologies, information is confined to the com-puter in which it is created. In addition to the tradi-tional uses of telecommunications for phoneconversations and paging, there is an increasingneed for remote communications to transfer digi-tal health information. Physicians might wish touse computers at home to track the status of pa-tients or receive notification of important lab re-sults. Group practices might submit batches ofinsurance claims to data-processing intermedi-aries electronically and remind patients of up-coming appointments using automated phonesystems. The term “house call” might reenter the
82 U.S. Congress, Office of Technology Assessment, Protecting Privacy in Computerized Medical Information, OTA-TCT-576 (Washing-
ton, DC: U.S. Government Printing Office, September 1993).
83 Office of Management and Budget, “National Information Infrastructure: Draft Principles for Providing and Using Personal Information
and Commentary,” Federal Register, vol. 60, No. 13, Jan. 20, 1994, pp. 4362-4370.

Chapter 2 information Technologies for Transforming Health
medical lexicon with the advent of in-home medi-cal monitoring devices for elderly or chronicallyill patients, devices that can deliver basic physio-logical information to doctors via modem. Hospi-tals might link their information systems toremote medical databases or support videoconfer-encing and telemedicine applications to broadentheir base of patients in the community. Integratedhealth delivery institutions might link computersat various sites into a single wide area network.Community health information networks (CHINS)might link various clinical institutions, compo-nents of the public health system, private medicalpractices, payers, data repositories, and academicinstitutions so that health information can beshared on a regional basis. The telecommunica-tions and networking technologies underlyingthese new health information applications are sur-veyed in box 2-7.
Individuals are also beginning to use telecom-munications and networking technologies to gainaccess to medical information. One of the mostprominent applications of broadband commu-
nications is the delivery of educational
Care 63
materialsvia the international network of computers knownas the Internet. Individuals can learn about healthissues and correspond with others who share com-mon interests by joining electronic mailing listsdedicated to discussions of specific medicalconditions. Many health care providers now pro-vide educational materials for patients, consum-ers, and doctors through World Wide Web pages,which are collections of pictures, text, sound, andvideo along with links to related information onother computers. The OncoLink Multimedia Can-cer Resource web page at the University of Penn-sylvania is shown in figure 2-2. From this page,computer users can navigate to many other pagesthat give them information about cancer terminol-ogy, ongoing clinical trials, how to prepare for ahospital visit, and many other topics.84 There is noincremental charge to access this or any of thehundreds of other web sites offering medical andhealth information on the Internet. However, ahome computer and modem are required, as wellas access to the network through an account pur-
How can computers in different parts of the country be connected to each other so they can share
health Information? One way to answer this question is to start with an understanding of how ordinary
telephone calls work. When a caller speaks into a phone mouthpiece, a microphone converts the
sounds into smoothly varying analog voltages, which then propagate along wires to the earpiece in the
distant phone where they are reconverted to sound. The wires from the two phones are connected by a
series of switches. If the two phones are within a hospital, the call will probably pass through just one
switch, within the private branch exchange (PBX) owned by the hospital. If the call’s destination is out-
side the hospital, the PBX wiII pass it on to an external switch owned by a local exchange carrier (LEC),
which is typically a regional Bell operating company. If the receiving phone is connected to the same
switch, the call goes through. Otherwise, it IS passed to other switches owned by the same LEC within a
LATA (Local Access Transport Area) region. The United States is divided into 137 LATAs of various
sizes; to go beyond the boundaries of a single LATA, the call must be passed to an interexchange carri-
er, such as AT&T, MCI, Sprint, WilTel, or others. At the far end, the call must again pass through the
series of switches owned by a different LEC until it arrives at its destination.
(continued)
84“OncoI.ink,’” University of Pennsylvania, April 1995. <URL:http://oncolink.upenn.edu>

64 Bringing Health Care Online: The Role of Information Technologies
LECs and interexchange carriers would have to maintain millions of sets of wires if all phone calls
were passed along as analog signals. Instead, the signal is usually digitized shortly after it leaves the
originating phone, often before it reaches the first switch. Many digitized signals can be easily mixed
together or multiplexed, carried on a single set of wires, and then separated at the destination. More-
over, the signals needn’t travel along wires: they can also be carried as pulses of light along fiberoptic
cables or as microwave signals between land stations or satellites. Digital communication links are
more robust than analog ones—they are more immune to noise and require less frequent reamplification
of the signals. If a hospital has a digital PBX or it wants to connect computers at different sites, its ad-
ministrators might choose to bring a digital line right into the facility. The capacity or bandwidth of such
a connection is typically measured by the number of normal voice connections it can carry: a DS-0
connection (64 thousand bits per second) can carry a single voice connection; a DS-1 or T1 connec-
tion (1 .544 million bits per second) can carry 24 phone conversations; a DS-3 or T3 connection (45
million bits per second) can carry 672 voice conversations, and so on. Various fractional levels between
these capacities can be ordered as well. A typical x-ray image could be transferred over a DS-O con-
nection in about eight minutes, over a DS-1 connection in about 20 seconds, over a DS-3 connection in
about 0.7 seconds, and over the high-capacity cross-continent “backbones” in a few milliseconds, The
bottleneck in telecommunications is the slowest connection.
A caller Initiates a connection by lifting the telephone handset from its cradle. The phone sends an
“off-the-hook” message to the nearest switch, which responds with a dial tone. The caller then presses
a sequence of touch-tone buttons, and the switch listens to the tones and figures out how to route the
call. This is called in-band switching because the caller can hear the dial tone, dialing, and pauses on
the same connection that will later carry the voice conversation. Some types of digital connections have
out-of-band switching, where separate connections carry the switching information. For instance, a ba-
sic rate integrated services digital network (ISDN) line contains two DS-0 channels for the messages
and an additional lower capacity channel for the switching signals. When the handset is lifted, the con-
nection to the receiving party is established almost immediately, The familiar whistle and rasp of mo-
dems may become rare as basic rate ISDN lines become more common in homes and businesses,
Currently, ISDN modems can transfer digital data onto the wider telecommunications system about six
times as fast as a typical modem. ISDN services cost only a little more than normal phone lines on a
monthly basis, but they are less convenient to set up and require more expensive equipment. ISDN
lines with capacities up to DS-1 are also available, again with separate switching and data (or voice)
channels.
All the connections discussed so far link remote phones or computers through a series of switches.
Often a facility doesn’t need that switching capability, however. It may have a pair of computers or PBXs
at two sites that it wants to connect without allowing any other outside connections. In that case, it may
choose to have a dedicated or leased line installed between the two sites.
Normal telephone calls carrying voices typically occupy an entire channel for the duration of the
conversation-other users wanting to contact the recipient get a busy signal. Voice calls are usually
connection-oriented because momentary disconnections or imperfections in a conversation are annoy-
ing. However, it is not easy to annoy a computer; communications between computers are often inter-
mittent or even connectionless, which means that no constant link between a particular set of originat-
ing and receiving computers is maintained. Digital data exchanges often consist of bursts of intense
activity surrounded by periods of silence. Packet-based communications exploit this pattern by inter-
(continued)

Chapter 2 information Technologies for Transforming Health Care 65
leaving the communications of whole sets of computers at once. Data streams are broken up into pack-
ets, and each packet contains a destination address indicating where it should go. Packet-based com-
munications are commonly used within local area networks (LAN), which connect a limited number of
computers within an institution in a loop or branching structure. Digital signals on LANs may pass along
copper wires resembling phone wires or cable-TV cables, or through the air as radio or infrared signals
on wireless LAN connections. Often several LANs within an institution are connected into an enterprise
network by a high-speed backbone that sometimes utilizes fiberoptic cables.
Packet-based communications can be used for telecommunications as well as for computer net-
working, especially when data rather than voices are being conveyed. A long message might be bro-
ken up into a huge number of packets. Each packet wends its way through the telecommunications
network, guided by routers along the way. Computers prepare the packets according to networking pro-
tocols published by network vendors or by standards committees. Depending on the protocol, packets
can be guided along predefine routes, or they may take different routes to the destination and experi-
ence different delays along the way, but be reassembled by the receiving computer into the correct
order.
Different computer networks utilize different packet formats and protocols; the packets on different
networks might be different sizes or have different addressing schemes. It is inconvenient for a comput-
er launching a packet to have to know what sort of packet is expected by the receiving computer,
which might be thousands of miles away. Sometimes this problem is solved by having all parties on the
network agree on a common standard such as the TCP/IP protocol (Transmission Control Protocol/lnter-
net Protocol) used for communication among computers in the worldwide Internet. Still, it is often nec-
essary to transfer packets from one network to a different network with a different protocol. One way to
do this is to employ a sort of diplomatic pouch called frame relay: packets traveling on the high-capac-
ity telecommunications network are wrapped in standard envelopes or frames and then unwrapped at
the receiving end into whatever packet format is required. The frames may have various lengths de-
pending on the size of the packet inside. Frame relay communications work well for transferring data
files such as x-ray images, but they are less effective for transferring video streams because unpredict-
able delays experienced by different-sized frames can lead to pauses and jumps in the video play-
back. A different and faster approach is to reformat all packets into minimalist cells that are a kind of
least common denominator. That is the approach behind asynchronous transfer mode communications
(ATM). Because all ATM cells are exactly alike, the routing equipment that shuttles them around the
world can be designed to be extremely fast, and the transmission delays for a series of cells will be
relatively constant. Video streams can be reassembled from ATM cells with few noticeable delays
High-speed frame relay and ATM communications will be necessary for any large-scale networking
that involves sharing large amounts of health information.
SOURCE: Office of Technology Assessment, 1995, and “The Telecommunications Glossary, ” Wiltel Communications Corp. , April
1995. <URL:http://www.wiltel.com/glossary/glossary.html>
chased from an Internet service provider or a com- industry. Already, demand management systemsmercial online service. are in place within some integrated HMOs nurses
High-bandwidth communications may have a in centralized locations use telephones to give ad-profound effect on the structure and process of vice for managing particular health problems tohealth care services analogous to the changes that patients located throughout the HMO’s serviceautomated teller machines brought to the banking area. Consultative practices such as radiology and

Figure 2-2: Health Information on the Internet
66 | Chapter 2 Information Technologies for Transforming Health Care
dermatology are slowly beginning to use high-bandwidth communications over dedicatedphone lines to practice telemedicine. Asswitched high-bandwidth connections becomewidely available, a dramatic change could oc-cur in which the hub-and-spoke topology ofmost telemedicine networks (with an academichospital at the hub of most consultations) maydissolve into a more dynamic network, and acompetitive market for health advice mayemerge. Individuals may eventually be able toget expert information about their health inmore convenient ways than from their doctors.
■ Distributed Computing andObject-Oriented Software
Health care information systems, like mostother large computer applications, were de-
signed for many years around the capabilitiesof powerful mainframe computers. Usersgained access to information stored in the largedatabases of a central computer using relativelyslow, text-based terminals. Although the cen-tral computer might be very fast, it had to per-form many duties. Its performance in respond-ing to a user's request for a patient's admissionrecords, for instance, might be slow if it wereoccupied with another calculation-intensivetask, such as preparing a monthly payroll.
As the speed and capabilities of desktopcomputers and networks have increased, thecentralized, hierarchical structure associatedwith mainframe computers is being replaced inmany instances with distributed computing us-ing a client-server architecture. The many tasksperformed by a monolithic central computer are
SOURCE: Oncolink, University of Pennsylvania, April 1995. URL: http://Oncolink.upenn.edu/

Chapter 2 Information Technologies for Transforming Health Care | 67
decoupled, and the workload dispersed among aseries of programs running on a set of smallercomputers, or servers. Each server handles a spe-cific task, according to requests made by otherprograms, or clients, on the network.
Typically, users interact with client programsrunning on desktop computers with relatively so-phisticated graphics capabilities. A client pro-gram for scheduling patient surgery, for instance,might issue requests for information to serversthroughout the institution. A request might be fora discrete piece of information, such as the pa-tient’s admission date, which could be retrievedfrom the admissions database. The request couldalso be more complicated: it could spawn a so-phisticated scheduling calculation on an adminis-trative server that itself required informationevoked from other servers. The client programmelds the information from the various sourcesand displays it to the user. The data and the com-putational resources of the information system aredistributed throughout the institution rather thanbeing localized in a centralized computer. Thefailure of any one computer is unlikely to compro-mise the entire system. In addition, if the admis-sions server were heavily used, the departmentmight maintain a number of different servers, withthe load being passed to the server that is least bur-dened at a given moment. Thus, capacity can beadded incrementally to a client-server network.
Client-server computing replaces large, centralcomputers with interacting networks of servers,each accomplishing specific tasks and communi-cating with standardized messages. A similartrend known as object-oriented design is affectingthe internal structure of computer software. In-creasingly, developers are decoupling large, mul-tipurpose software applications into sets ofinteracting objects. For instance, a common taskfor a software designer might be to change thetype of information in a record—perhaps makingroom for nine-digit zip codes instead of five-digit
zip codes. With traditional software design, thistype of change might require changing all of theroutines that ever manipulate zip codes, includingprinting routines, file storage routines, sortingroutines, and so on. These routines could be scat-tered throughout the code, and finding and alter-ing them is a difficult and time-consumingproject. Moreover, changing any of the routinescould have unintended consequences elsewhere inthe program for other data that use the same rou-tines. Object-oriented design bundles all of theseroutines along with the zip code itself into an en-capsulated object. Thus, all the zip code routinescan be easily changed and tested, without affect-ing any of the rest of the software in the project.
Ideally, object-oriented design can lead to soft-ware code that is modular and reusable. Compli-cated software applications can be built rapidlyfrom standardized libraries of classes of objects.This new software paradigm may pose significantchallenges for regulatory structures governingdistribution of medical software. Currently, medi-cal software is regulated by the Food and DrugAdministration (FDA) under the same systemused for medical devices. Before marketing theirproducts, vendors must register their medical soft-ware with the FDA and obtain official approval ofits safety and effectiveness. Vendors must docu-ment their design process and demonstrate thatpotential safety hazards associated with softwarecomponents have been identified and addressed.
Several categories of software are exempt fromthis process, including general-purpose softwaresuch as word processors, software designed foruse in teaching, nonclinical research, or privatepractice, and knowledge-based systems that re-quire human intervention before any impact onhuman health could occur.85 This policy may beadequate for medical software embedded in physi-cal devices or distributed through conventionalchannels, but it may prove cumbersome as moreresearch institutes become linked by the Internet.
85 Office of Device Evaluation, Center for Devices and Radiological Health, Food and Drug Administration, “Reviewer Guidance for Com-
puter Controlled Medical Devices Undergoing 510(K) Review” (Washington, DC: 1991).

68 | Bringing Health Care Online: The Role of Information Technologies
Software developed for academic research pur-poses is commonly distributed at no charge to oth-er researchers using a procedure known as ftp, orfile transfer protocol. In the absence of a clearFDA policy regarding electronic distribution ofmedical software, concerns that the FDA maytreat distributors of free software as medical ven-dors have delayed the ftp distribution of at leastone product intended for calculation of radiothera-py treatment doses.86
In addition, the policies deal inadequately withsoftware developed using object-oriented designand perhaps assembled from components writtenby a variety of sources and only assembled by thefinal vendor. The exemption from regulation forgeneral-purpose software raises the possibilitythat vendors could avoid FDA oversight of theirproducts by selling a general-purpose “shell” pro-gram that could then link together modules withmedical functionality that had been distributed viaftp at no charge.
Finally, the distinction between source codeand object code for a computer program is becom-ing a key issue—source code is written in a com-puter language such as C++ or FORTRAN andcan be altered by any competent programmer,whereas object code is a translation of the sourcecode into a form executable by a particular ma-chine. To ensure uniformity of approved software,the FDA has typically allowed vendors to distrib-ute only the object code for their computer pro-grams because it cannot be easily altered by theend-user. A similar restriction on electronicallydistributed software is problematic, however. Dis-tribution of source code may be protected by thefirst amendment, and such a restriction wouldhave a burdensome effect on academic researchand prevent cross-verification of the soundness ofcode design by independent groups. The FDA is
currently reviewing and revising its policies onregulation of medical software.
SHARING THE COMMON POOL OF DATA
❚ StandardsStandards are agreements on how to implementtechnologies. They allow buyers to choose com-patible medical equipment and software from avariety of vendors, and thus encourage both in-novation and price competition. Sometimes defacto proprietary standards emerge when a singlevendor controls a large share of the market for aparticular item. Consensus standards are devel-oped by committees with representatives frommany different stakeholders. The committees caninclude representatives of vendors, the medicalcommunity, the government, unions, and any oth-er interested individuals who choose to participatein the laborious process of writing and agreeing onstandards. Standards committees are accreditedby organizations such as the American Society forTesting and Materials (ASTM), the American Na-tional Standards Institute (ANSI), or by other na-tional or international organizations.87 They meetover a period of years and develop drafts thatmembers of the committee vote on after extendedrevisions and public review. Standards bodies oc-casionally have problems reaching decisions asrapidly as new technologies are developed.
Understanding consensus standards is compli-cated in that the name of an individual standard isusually an acronym that reflects the identity of thestandards committee, rather than the function ofthe standard. Figure 2-3 shows the alphabet soupof interrelated messaging standards for exchang-ing data among various parts of a hospital: stan-dards written by ASTM Subcommittee E31.15specify the format for messages traveling to and
86 “Council on Competitiveness Identifies Telemedicine Barriers in Report Summarizing Fall Conference,” Healthcare Telecom Report,vol. 3, No. 1, Jan. 2, 1995; and Edward L. Chaney, Professor, North Carolina Clinical Cancer Center, University of North Carolina, personalcommunication, May 1, 1995.
87 A complete description of the standards-setting process can be found in , U.S. Congress, Office of Technology Assessment, Global Stan-
dards: Building Blocks for the Future, OTA-TCT-512 (Washington, DC: U.S. Government Printing Office, March 1992).
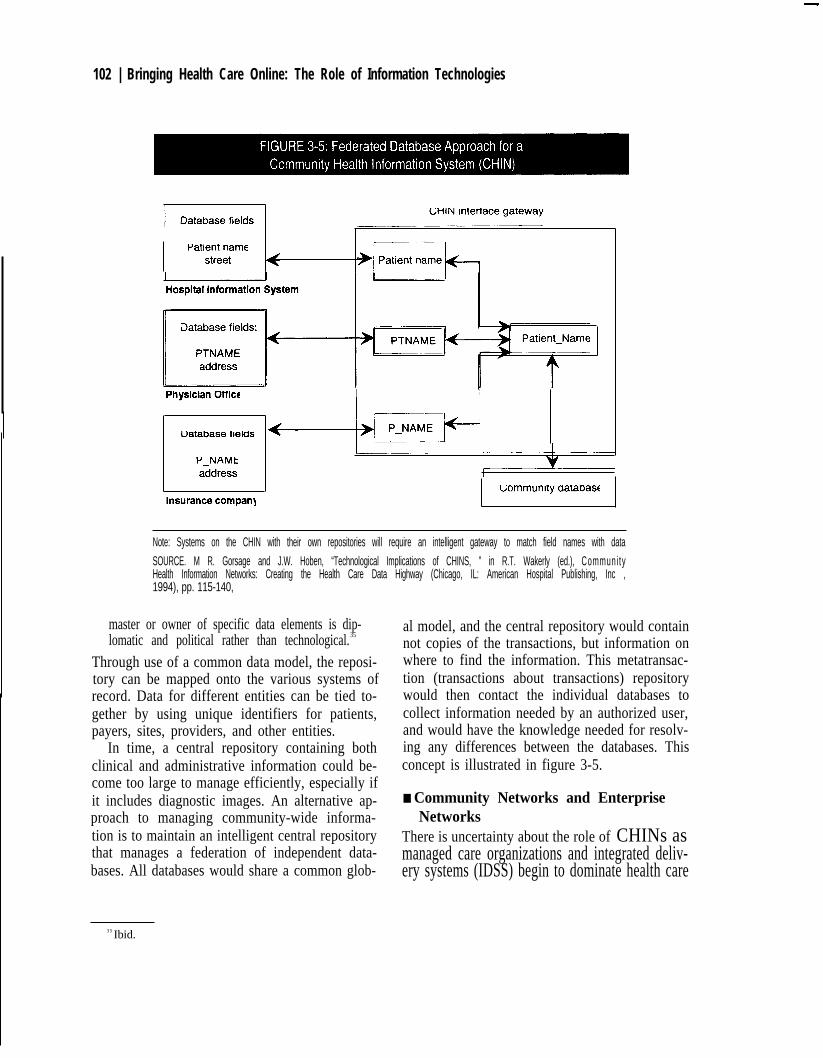
102 | Bringing Health Care Online: The Role of Information Technologies
Note: Systems on the CHIN with their own repositories will require an intelligent gateway to match field names with data
SOURCE. M R. Gorsage and J.W. Hoben, “Technological Implications of CHINS, ” in R.T. Wakerly (ed.), Communi tyHealth Information Networks: Creating the Health Care Data Highway (Chicago, IL: American Hospital Publishing, Inc ,1994), pp. 115-140,
master or owner of specific data elements is dip-lomatic and political rather than technological.35
Through use of a common data model, the reposi-tory can be mapped onto the various systems ofrecord. Data for different entities can be tied to-gether by using unique identifiers for patients,payers, sites, providers, and other entities.
In time, a central repository containing bothclinical and administrative information could be-come too large to manage efficiently, especially ifit includes diagnostic images. An alternative ap-proach to managing community-wide informa-tion is to maintain an intelligent central repositorythat manages a federation of independent data-bases. All databases would share a common glob-
al model, and the central repository would containnot copies of the transactions, but information onwhere to find the information. This metatransac-tion (transactions about transactions) repositorywould then contact the individual databases tocollect information needed by an authorized user,and would have the knowledge needed for resolv-ing any differences between the databases. Thisconcept is illustrated in figure 3-5.
■ Community Networks and EnterpriseNetworks
There is uncertainty about the role of CHINs asmanaged care organizations and integrated deliv-ery systems (IDSS) begin to dominate health care
35 Ibid.

70 | Bringing Health Care Online: The Role of Information Technologies
from knowledge bases, ANSI X12 standards gov-ern communication of financial data to insurersand others outside the health care institution, theNCPDP standard developed by the NationalCouncil of Prescription Drug Pharmacies speci-fies the format for messages containing pharma-ceutical information, and so on. Purchasers ofhealth care equipment and software can more easi-ly build extensible systems by buying items thatstore and exchange information according to oneor more of these consensus standards rather thanproprietary standards.
A model of communications published by theInternational Standards Organization describesseven different levels of computer communica-tions, beginning with physical interconnectionsand ending with the standards that specify howmessages are passed between software applica-tions (the seventh level). One of the most widelyused messaging standards is the HL7 (Health Lev-el Seven) standard for electronic interchange ofhealth data.
HL7 is explained in more detail in box 2-8.Most of the standards in figure 2-3 are conceptual-ly similar to HL7 and closely related to it. Forinstance, standards written by ASTM Subcom-mittee E31.16 specify the format for messagescontaining neurophysiological data. These mes-sages use the same syntax, and most of the samesegments, as HL7 messages, but they include datastructures for continuous waveforms such as elec-troencephalogram traces.88 HL7 was originally astandard for communicating laboratory data andother clinical observation data between softwareapplications, but it now includes structures forcommunicating clinical orders, billing informa-tion, and patient admission, discharge, transfer,
and registration information within single institu-tions.
This suite of standards has brought a modicumof order to the varied approaches to sending mes-sages within and among health care institutions.Each standard defines the structure of messageswithin a certain jurisdiction. But what happenswhen a measurement generated by a laboratoryinstrument and formatted according to the ASTME1394 standard needs to be passed to a bedsidemonitor that normally formats information ac-cording to the P1073 standard? Individual stan-dard-to-standard translation schemes could bedesigned, but they would necessarily be inconstant flux as the various standards evolve. Toaddress these types of problems, ANSI created aHealth Informatics Standards Planning Panel(HISPP) in 1993 to coordinate standards develop-ment efforts. A number of working groups haveformed under the aegis of HISPP, each made up ofrepresentatives from organizations involved indeveloping health messaging standards. Oneworking group, for instance, is developing aframework for a common data model that willserve as an evolving guide and resource for all thevarious messaging standards. The framework willincorporate the innovations of the various stan-dards committees and harmonize their efforts overthe long term using an iterative process.89
The messaging standards in figure 2-3 definehow messages are communicated, but the contentof the messages is set by an entirely different set ofstandards. Some of these were developed in indus-trial or scientific settings, such as the “metric sys-tem” or Systemé Internationale that defines unitsof measurement. Others are specific to medicalcontexts. Standards are necessary for coding and
88 Moreover, the chair of the group working on automated data within the HL7 committee has agreed to include these same messageconstructs for transmitting wave forms in HL7 messages, and the same is true for other standards committees. Despite the diversity and multi-plicity of committees and working groups, the emerging standards are generally complementary.
89 T.E. Rutt, “Work of the IEEE P1157 Medical Data Interchange Committee,” International Journal of Clinical Monitoring and Comput-ing, vol. 6, 1989, pp. 45-57, and Trial-Use Standard for Health Care Data Interchange-Information Model Methods, Data Model Framework,P1157.1 Draft 1 (Piscataway, NJ: IEEE Standards Department, 1994).

70 Bringing Health Care Online: The Role of Information Technologies
Standards for interchanging health data and assigning codes to medical concepts underlie all ef-
forts to make patient records electronically accessible. This box presents one of the major messaging
standards (HL7—Health Level 7) and one of the major coding standards (ICD-9-CM—International
Classification of Diseases, 9th Revision, Clinical Modification). These are representative examples, but
HL7 is only one of the many messaging standards used to convey health data, and ICD-9-CM is one of
the two major coding systems used in the United States.
Messaging standards specify the syntax of an electronic message and coding standards specify its
semantics. A similar distinction exists for more familiar messages, such as postcards. The syntax of a
postcard corresponds to the arrangement of its elements: the addressee’s name appears in a standard
posit! on, the city in another, the message is placed in a box on the left half and the stamp in the upper
right, and so on. The arrangement IS set by international postal conventions. The meaning of the letters
appearing within a given element (its semantics) is determined by an entirely different set of conven-
tions, namely the language employed by the correspondent. Similarly, HL7 and other messaging stan-
dards specify the order of the many discrete elements that make up a message and indicate which
elements are required and which are optional. ICD-9-CM and other coding systems assign meaning to
the characters in the message.
Electronic MessagesHL7 messages are streams of text that are relatively simple to interpret, As an example, the portion
of the message that carries the patient’s address might be represented as “...1432 Hosteler Street ‘Apt
232ˆChlcagoˆILˆ60603ˆUSA... ” In addition to demographic information identifying the patient, an HL7
message delivering the results of a laboratory test might include hundreds of other data elements con-
taining numerical values for the measured parameters, the measurement units, and portions of the mes-
sage that bore the initial request so that the request and response can be matched and reconciled. The
data elements contain internal indications of the coding standards to be used. For instance, one small
portion of the standard message defined by HL7 contains the patient’s diagnosis. This slot might be
filled with the characters “410.1ˆI9C. ” The software application receiving this message knows from the
position of the characters within the message that this is a diagnosis, and it simply has to assign mean-
ing to the character by looking up diagnosis number 410,1 in the set of codes published by the
ICD-9-CM Committee. The table would indicate that the diagnosis is ‘(anterior myocardial infarction. ”
Alternatively, the same diagnosis could be conveyed in a different coding scheme employing an entire-
Iy different code set, but still using the same HL7-defined structure. This allows the software application
sending a message to choose whatever coding scheme is most appropriate for the data it processes.
Libraries of disease and procedure descriptions can evolve without necessitating any changes in the
software governing how messages are sent.
(continued)
A model of communications published by the el Seven) standard for electronic interchange ofInternational Standards Organization describes health data.seven different levels of computer communica- HL7 is explained in more detail in box 2-8.tions, beginning with physical interconnections Most of the standards in figure 2-3 are conceptual-and ending with the standards that specify how ly similar to HL7 and closely related to it. Formessages are passed between software applica- instance, standards written by ASTM Subcom-tions (the seventh level). One of the most widely mittee E31. 16 specify the format for messagesused messaging standards is the HL7 (Health Lev- containing neurophysiological data. These mes-

Chapter 2 information Technologies for Transforming Health Care 71
Clinical Coding SystemsCodes are an attempt to standardize the description of clinical practice so that diagnoses or proce-
dures relevant to different patients can be compared side-by-side. They are used for both research
purposes and reimbursement of claims. ICD-9-CM codes are widely used to describe inpatient treat-
ments in hospitals, and CPT-4 codes (Physicians’ Current Procedural Terminology, 4th Edition) are
used by physicians and other health care professionals for billing purposes. The ICD-9-CM codes are
a combination of the ICD-9 diagnostic code set maintained by the World Health Organization for de-
scribing diseases and a set of codes for medical procedures maintained by the Health Care Financing
Administration (HCFA). HCFA requires that ICD-9-CM diagnostic codes be used for itemized Medicare
inpatient and ambulatory care claims, and it determines payment levels based on the grouping of treat-
ments, according to the procedure codes, into Diagnosis Related Groups (DRGs).
Medical coders are employed in hospitals to assign codes to the procedures described in patient
records following guidelines published by the American Hospital Association. It is a very complex and
sophisticated task. Although there are some aspirations to automate the coding process by assigning
codes through computer analysis of clinical orders, it is Iikely that information technologies will be more
commonly used to assist medical coders rather than to replace them. Decision-support systems known
as encoders are commercially available starting from an initial suggested code, they prompt the coder
to investigate related codes and check to make sure that the group of codes ultimately assigned is
internally consistent. Groupers are software applications that deduce from the final set of assigned
codes a DRG, which is the basis for Medicare or other Insurance reimbursement Finally, many coders
use online libraries of coding reference manuals.
Current coding systems have been criticized as too Imprecise to describe some aspects of clinical
practice. Another common criticism is that the terminology used in various codes IS inconsistent Cur-
rently, Medicare reimbursements depend only on the primary DRG without regard for the significant ex-
tra expense involved in caring for a patient with a complicated secondary diagnosis. Future revisions of
ICD-9-CM may address these problems to some extent. The 10th revision will attempt to Incorporate
standard clinical definitions used throughout its specifications, and DRGs wiII be severity refined so that
reimbursements can more accurately reflect the cost of treating the patient. In recognition of the in-
creasing importance of ambulatory care as managed care institutions seek to minimize the number of
hospital admissions, HCFA is also developing a new set of codes for use in outpatient care.
SOURCES: C.J. McDonald, D K Martin, and J.M. Overhage, “Standards for the Electronic Transfer of Clinical Data Progress andPromises,” Topics in Health Records Management, vol. 11, No. 4, 1991, pp. 1-16, B. Siwicki,“Coding Changes on the Horizon Health
Data Management, vol 3, No. 1, 1994, pp. 42-43
— .
sages use the same syntax, and most of the same standard for communicating laboratory data andsegments, as HL7 messages, but they include data other clinical observation data between softwarestructures for continuous waveforms such as elec- applications, but it now includes structures fortroencephalogram traces.
88 HL7 was originally a communicating clinical orders, billing informa-
88 Moreover, the chair of the group working on automated data within the HL7 committee has agreed to include these same message
constructs for transmitting wave forms in HL7 messages, and the same is true for other standards committees. Despite the diversity and multi-plicity of committees and working groups, the emerging standards are generally complementary.

Chapter 2 Information Technologies for Transforming Health Care | 73
der way to facilitate that expansion. One exampleis the nonprofit Healthcare Open Systems andTrials (HOST) consortium.90 HOST is establish-ing test sites for deployment of new informationtechnologies at medical institutions and an OpenSystems Laboratory where the compatibility ofvarious technologies can be demonstrated. TheHOST consortium has recently received a grantthrough the Advanced Technology Program(ATP) at the National Institute of Standards andTechnology, which is also funding several otherprojects that develop or implement novel informa-tion technologies for use in the health care sys-tem.91
Integration of the various technologies andstandards into working systems is also one focusof the High-Performance Computing and Com-munications (HPCC) program. This multiagencyfederal effort was initiated by the President’s Of-fice of Science and Technology Policy during theBush Administration and expanded by legislationintroduced by then-Senator Albert Gore. The Na-tional Science Foundation (NSF), National Aero-nautics and Space Administration (NASA),National Institutes of Health (NIH), and otheragencies participating in the HPCC program sup-port the development of the underlying technolo-gies essential for telemedicine and other healthcare applications of the National Information In-frastructure, including the National Research andEducation Network (NREN), pilot implementa-tions of advanced information technologies inhealth care settings, and supercomputer centers.92
Recent HPCC grants through NLM have fundedresearch leading to implementation of computer-based patient records in the Indianapolis metro-
politan area,93 creation of a statewide digitalnetwork to support telemedicine and rural healthcare providers in Iowa,94 development of ad-vanced computer simulations of human anatomicstructure to support surgical planning and medicaleducation, and numerous other projects.
Population-based public health services mayalso benefit from the development of standardsand technologies that will enable health informa-tion to flow freely. Advanced techniques forknowledge discovery in databases may be appliedto help automate the identification of public healththreats, such as the recent Hantavirus outbreakthat was identified through a medical examinersurveillance database maintained by the Centersfor Disease Control and Prevention (CDC). Asmall number of grants supporting the develop-ment of public health applications have beenawarded by the National Telecommunications andInformation Administration, and other integrativework is proceeding with support from CDC,AHCPR, the U.S. Public Health Service, and oth-er agencies.
POLICY ISSUES AND OPTIONSThe technologies for collecting, distilling, stor-ing, securing, and communicating data are widelyused throughout American industry. They areused in health care organizations as well, but theirapplication has been limited to scattered islands ofautomation. Despite the incorporation of hightechnology into almost every other aspect of clini-cal practice, information technologies have notbeen fully embraced.
The health care delivery system has severalunique characteristics that discourage the spread
90 The HOST consortium has over 30 corporate and academic partners. It was co-developed in 1994 by the Microelectronics and Computer
Technology Corporation (MCC) and the Computer-based Patient Records Institute.
91 B. Deming, “Launching a High-Profile Automation Mission,” Health Data Management, vol. 3, No. 5, May 1995, pp. 15-19.92 D.A.B. Lindberg and B.L. Humphreys, “The High-Performance Computing and Communications Program, the National Information
Infrastructure, and Health Care,” Journal of the American Medical Informatics Association, vol. 2, No. 3, 1995, pp. 156-159.
93 J.M. Overhage, W.M. Tierney, and C.J. McDonald, “Design and Implementation of the Indianapolis Network for Patient Care and Re-
search,” Bulletin of the Medical Library Association, vol. 83, No. 1, 1995, pp. 48-56.
94 M. Kienzle et al., “Iowa’s National Laboratory for the Study of Rural Telemedicine: A Description of Work in Progress,” Bulletin of the
Medical Library Association, vol. 83, No. 1, 1995, pp. 37-41.

74 | Bringing Health Care Online: The Role of Information Technologies
of information technologies. Clinical practice isextremely complex, and despite the efforts ofstandards committees, no unified conceptualmodel exists that is powerful enough to guide thecreation of computer databases that adequatelyrepresent medicine as it is practiced. No consen-sus has emerged on what information should bekept in electronic patient records, how detailed itshould be, or how it should be described and in-dexed.
It is not a lack of appropriate hardware that lim-its or impedes productive computing in healthcare services. Rather, it is a failure to understandthe intricacies of health care delivery as related tocapture and use of medical data, and the ways inwhich they must be manipulated. Hence, what isput into software, and thus the software itself,does not adequately reflect the real needs of healthcare providers or the ways in which they conducttheir activities.95
Experience gained in solving problems in onearea of medical practice may not be applicable toother areas. A clear example of this occurs withdecision support systems. Self-contained, rule-based systems are widely used in well-definedareas such as infection diagnosis and in somemedical equipment, but attempts to extend thescale of decision support to broader areas of medi-cal expertise have been frustrated. This resemblesthe general pattern of medical research: narrowproblems are solved on a local basis. The result isan idiosyncratic vocabulary and nonuniform clin-ical practice. Perhaps medical informatics worksbest at solving a large number of microproblems.If so, efforts should turn toward smoothly inte-grating all the microsolutions.
In addition to the complexity of clinical knowl-edge, the structure of the health care industrydiscourages implementation of information tech-nologies. Providers of health care services areoften isolated in separate corporate entities from
the insurance companies that pay them for theirservices. Providers and payers are further isolatedfrom the medical research community, govern-ment health care agencies, and public healthorganizations. A network of private sector inter-mediaries has formed to facilitate the complicatedrelationships between the various organizations.None of these entities is likely to be willing to col-lect or organize data that saves money or effort forsome other organization, but delivers it no im-mediately useful benefit; systemic savings may beirrelevant in a vertically fractured industry. In ad-dition, many communities have only a few hospi-tals or major insurers. The cooperation necessaryto interconnect medical information within a hori-zontal layer of the health care system may be seenas anticompetitive and subject to antitrust regula-tion, or it may be hindered by organizations thatregard their internal information systems as com-petitive advantages and accumulated patient re-cords as corporate assets.
Information technologies tend to flatten orga-nizations and may not mesh well with the rigidlydefined job roles and hierarchical structure of cur-rent clinical practice. As an example, a patient re-cords system was installed at the University ofVirginia Medical Center that required clinicians toenter medical orders on computers. This had anunexpected effect on the education of fourth-yearmedical students who are often allowed to placeorders for a patient’s care with the approval of aresident physician. With paper records, this hadbeen a simple matter that saved time for the resi-dent and gave satisfying responsibility to the stu-dents: the student drew up a list of potentialorders, consulted the resident, and had the list ap-proved. With computerized order entry, the proc-ess was much more cumbersome. Each order wasissued separately and needed to be approved sepa-rately. This meant either calling a resident multi-ple times to approve individual orders or placing
95 T.L. Lincoln, D.J. Essin, and W.H. Ware, “The Electronic Medical Record: A Challenge for Computer Science To Develop Clinically andSocially Relevant Computer Systems To Coordinate Information for Patient Care and Analysis,” The Information Society, vol. 9, 1995, pp.157-158.

Chapter 2 Information Technologies for Transforming Health Care | 75
orders in suspension one by one and then findingways to reassemble them for a single consultationwith the resident.96
It might be argued that changes to the design ofthe system, or implementation of a records systemmore carefully tailored to support desired workpatterns, could alleviate this specific problem.Nonetheless, the deeper issue is that completionof every detail of order entry is a new and perhapsunwelcome task for physicians. To some extent,all information systems that deliver informationto a clinician at the point of care also require si-multaneous collection of information by the clini-cian at the point of care. Job descriptions willchange as decisionmaking, authorizing actions,and entering data become more tightly linked:
In contradistinction to the retail sector, whichcan assign relatively inexperienced employeesto data-entry positions [and create competitiveadvantages by capturing data at the point ofsale], the health care sector places the mosthighly trained professional personnel with thegreatest opportunity cost in the data-entryrole.97
Changes in job roles will occur throughout thehealth care system, should information technolo-gies be widely adopted. These changes will beaccompanied by redistributions in health profes-sionals’ time and by shifts in the responsibilitiesand status associated with the various health disci-plines.
Information technologies may have more sub-tle ramifications as well. The widespread adop-tion of integrated information systems willchallenge the legal system. Patients are the con-sumers of health services, and their traditionalprotection against poor-quality care has been theability to file lawsuits against their providers. In-formation technologies are tools for providinghealth care, but they are maintained and employedby a variety of people who may be geographically
separated. Who is responsible if a treatment proto-col recommended by a decision support systemturns out to be injurious? Is it the academicianwho designed the protocol, the reviewers who ap-proved its publication, the insurance companythat insisted it be implemented, the hospital boardthat approved its use, the interface designer whofailed to provide contextual information thatcould have contraindicated its use, or the primaryphysician who employed the protocol, but mayhave had no knowledge of its deficiencies? And ifno one can be held directly accountable, what al-ternative system of quality control must be de-signed to replace the current legal remedies?Information technologies diffuse responsibility,and changes in the hierarchical way that medicalcare is practiced may be necessary before they arefully embraced.
Finally, information technologies are expen-sive to implement and their benefits may be diffi-cult to measure directly, even when all parties arehappy with the results. This may help delay theirdeployment in an industry whose sophisticatedtechnological base is seen by some to be a drivingforce in making health care more expensive.
❚ Opportunities and ChallengesGiven these obstacles, installation and efficientutilization of information technologies in healthcare will continue to be incremental and difficult.However, there are a number of reasons why Con-gress may wish to actively support this process.
First, implementation of information technolo-gies could lead to reductions in federal healthcare expenditures. The federal government is amajor purchaser of health care through Medicareand Medicaid, and a major integrated provider andpayer through its health care programs for militarypersonnel, veterans, and Native Americans.While individual private sector organizations par-
96 T.A. Massaro, “Introducing Physician Order Entry at a Major Academic Medical Center: II. Impact on Medical Education,” Academic
Medicine, vol. 68, No. 1, 1993, pp. 25-30.
97 T.A. Massaro, “Introducing Physician Order Entry at a Major Academic Medical Center: I. Impact on Organizational Culture and Behav-
ior,” Academic Medicine, vol. 68, No. 1, 1993, pp. 20-25.

76 | Bringing Health Care Online: The Role of Information Technologies
ticipating in health care delivery may find it diffi-cult to realize financial benefits from systemicchanges, the federal government is ideally si-tuated to recoup whatever costs might be incurredin encouraging adoption of information technolo-gies at all levels of health care delivery by substan-tially reducing its own health care costs.Researchers and others have suggested that multi-billion-dollar annual savings might be possiblewith increased use of information technologies inhealth care. Chapter 3 discusses these projectionsfor administrative savings.
Information technologies may also foster com-petition in the health care industry. Chapter 4discusses ways that advanced information tech-nologies can be used to evaluate the effectivenessof health care procedures and the efficiency ofhealth care organizations. Although these tech-niques for quality assessment are highly problem-atic, they may represent an unprecedented metricby which organizations and practices can becompared and contrasted, thereby enabling con-sumers and managers to make more informedchoices concerning their health care.
Implementation of information technologiesmay help increase access to health care throughprivate sector activities. Chapter 5 discusses waysthat information technologies may allow healthcare providers to extend their reach in the commu-nities they serve through telemedicine or othermeans for electronic delivery of services. In addi-tion, new technologies may help decentralizehealth care by increasing the flow of useful in-formation to primary care doctors so that morepeople can have access to state-of-the-art healthcare without resorting to hospital or emergencyroom care. This consideration is especially impor-tant in rural communities and inner-city commu-nities where the viability of large health careinstitutions is uncertain.
Finally, information technologies could lead tosystemic changes and opportunities that will en-
able the American health care system to betterserve its citizens through more convenient andperhaps less expensive delivery of health services.Some of the benefits and conveniences (as well assome of the drawbacks) of health care enhancedby information technology were envisioned in thefictional scenario at the beginning of this chapter.Many others will only become apparent once abroad information infrastructure is in place. Everynew tool contains embedded ideas that go beyondthe function of the tool itself.98 When personalcomputers were developed, there was little indica-tion or intention that they would rapidly developinto tools for individuals to publish and access in-formation across the globe; the federal govern-ment played an important role in that developmentthrough its support of the development of the In-ternet’s predecessors.
There are indications that similar dynamicswill emerge as the health information infrastruc-ture continues to evolve. One example of this ap-pears in the area of pharmaceuticals. The volumeof pharmacy claims is much greater than the num-ber of claims for clinical procedures, and pharma-cy claims are also much simpler to process thanother claims. Two crucial enabling standards ex-ist: the National Council of Prescription DrugPharmacies (NCPDP) has developed a widely ac-cepted standard for communication between com-munity pharmacies and claims processors, and theFDA has defined the National Drug Code thatspecifies a unique code for each drug. As a result,pharmacy claims were one of the earliest areas tobe computerized. Today, over 90 percent of com-munity pharmacies are connected online to at leastone third-party pharmaceutical claims proces-sor.99 This connectivity led to the expected ad-ministrative savings due to elimination ofpaperwork and automation of eligibility verifica-tion and inventory replenishment, but it also hadthe relatively unforeseen benefit of making avail-
98 N. Postman, Amusing Ourselves to Death: Public Discourse in the Age of Show Business (New York, NY: Viking Press, 1985), p. 30.99 C.J. McDonald, “News on U.S. Health Informatics Standards” (letter), M.D. Computing, vol. 12, No. 3, 1995, pp. 180-186.

Chapter 2 information Technologies for Transforming Health Care | 77
to savings in pharmacy expenditures for manyproviders using PBMs, although some studieshave shown that savings are sometimes offset byincreased use of other, more expensive servicessuch as hospital outpatient, inpatient, or emergen-cy services.100 Information technologies have ledto significant changes in the distribution and pur-chasing of pharmaceuticals, such as the develop-ment of formularies, or lists of preferred drugs,and the widespread use of generic drugs and drugsdiscounted by manufacturers. The implementa-tion of information systems has had a broadimpact even on pharmaceutical research and de-velopment because it has encouraged develop-ment of novel drugs and generic drugs, but made itless attractive to develop new entries for drugcategories with numerous existing products.l01
Computerization of pharmacy transactions pre-sents an opportunity for addressing more compre-hensive health maintenance issues, such as patientcompliance with drug therapies, because physi-cians could be informed when their patients fail torenew prescriptions or when they obtain addition-al drugs prescribed by other caregivers. Freelyflowing health information may have large im-plications for both the creativity and the competi-tiveness of the health care industry.
■ Policy OptionsIf Congress wishes to support and affect the diffu-sion of information technology in health care set-tings, it could consider a number of options.
Support standards-setting activities
Congress may wish to participate in or monitorefforts to set standards for implementation of in-formation technologies in the health care system.Congress could:
■ support the development and adoption of con-sensus standards for electronic messaging andclinical coding. This could be achieved by di-recting agencies to supply personnel to activelyparticipate in standards-setting meetings and todevelop aggressive timetables for governmentimplementations of consensus standards. Taxcredits could also be extended to encourage thepurchase of information systems that imple-ment consensus standards.
■ support the development of coding systems andnomenclatures necessary for communicatingthe content of patient records. This could bedone by continuing to fund the development ofthe Unified Medical Language System and re-lated efforts at the National Library of Medi-cine.
■ ensure that technical standards for the contentof patient records and for minimum levels ofprivacy and confidentiality meet privacy policygoals. This mission could be delegated to: 1 ) aspecial task force made up of technology, priva-cy, and health information experts; 2) a com-mittee charged with an ongoing review ofhealth information privacy issues; ’02 or 3) anexisting committee, such as the Health In-formation and Applications Working Group ofthe Information Infrastructure Task Force(IITF).
Fund and coordinate research efforts toovercome specific technological barriers.
Most of the technologies discussed in thischapter have been developed through corporate oracademic research that was not connected directlyto health applications. As a result, some areas,such as human-computer interface design for usein medical contexts, are not well developed and
100 C.M. Kozma et al., PharmacoEconomics, VOl. 4, 1993, pp. 92-103, 187-202.101 Judith L. Wagner, Senior Associate, Health Program, Office of Technology Assessment, testimony presented before the Committee on
Finance, U.S. Senate, hearing on Long-Term Care and Drug Benefits Under Health Care Reform, Apr. 19, 1994.102 U.S. Congress, Office of Technology Assessment, op. cit., footnote 43, p. 2O.

78 | Bringing Health Care Online: The Role of Information Technologies
may pose difficult problems in the implementa-tion of integrated systems. Congress could en-courage research into these areas by creatingfocused programs administered by the NationalScience Foundation, the National Institutes ofHealth, or other agencies providing traditionalpeer-reviewed research grants. In addition, Con-gress could support research into large-scale im-plementation of information technologies inhealth care settings through pilot programs andtesting centers.
Coordinate federal efforts to implementhealth care information technologies.
This coordination could be achieved throughexisting agencies and committees or through theestablishment of a special committee or commis-sion. In particular, the relevant bodies might becharged to:
■ establish procedures for expediting approvaland distribution of medical software. Faultysoftware is as dangerous and worthy of regula-tion as poorly designed medical hardware, butsoftware has the unique feature that it can be de-veloped incrementally and distributed elec-tronically.
■ establish mechanisms (or support similar pri-vate sector efforts) for reviewing and dissemi-nating clinical protocols. 1 0 3
■ advise Congress on specific needs of the clini-cal community with respect to legislation es-tablishing regulations and policies pertinent toinformation technologies. Current issues thatfall under this rubric are liability reform andtelecommunications deregulation legislation.
■ establish policies consistent with privacypolicy goals for implementation of uniform pa-tient and provider identifiers for use in federalagencies.
103 For further discussion, see chapter 4.
Networksfor
HealthInformation
nformation technology can be used to automate many ad-ministrative processes in the health care system, includingtransactions between those who provide health care servicesand those who pay for them. The general term electronic
commerce is used in the chapter to describe the automation ofbusiness transactions and the direct computer-to-computer ex-change of information, business documents, and money.
This chapter examines electronic communications betweenproviders and payers (including interactions with electronic med-ical claims companies, value-added networks, clearinghouses,and others that facilitate this communication). It also discusseselectronic commerce between health care providers and medical/surgical manufacturers and distributors, as well as between phar-macies and both pharmaceutical distributors and claims payers.The role of communication networks in facilitating the exchangeof health information among health care providers, payers, andothers on a community-wide or regional basis is examined. Fig-ure 3-1 illustrates some of the directions in which informationneeds to be exchanged, or transactions need to be effected, amongthe various components of the health care delivery system.
Electronic communications can free administrative informa-tion from paper, allow it to be processed automatically (withouthuman intervention), and permit it to be readily reused for a num-ber of related purposes. In many cases, it appears that electroniccommerce can provide some cost savings to health care systemparticipants and to the system as a whole. Realizing those savingsrequires investment in equipment and training, as well as indus-trywide agreement on and compliance with standards for the for-mat and content of messages. The chapter reviews some of theresearch on costs and cost-effectiveness of various uses of elec- | 79

80 Bringing Health Care Online: The Role of Information Technologies
I I I
Medical/surgicalproduct
manufacturers
Medicare fiscalintermediariesand carriers
I I
Medical/surgicaldistributors
I
/
I HEALTH CARE I
I
Wholesale drugdistributors
Health CareFinancing
Administration(Medicare)
I I
SOURCE: J. Moynihan and K Norman
I
LClaims payers■ Indemnity■ Managed care■ Self-insured
Medicaidprocessors
I Medicaid IL . I
Self-pay
“Health Care EDI: An Overview, ” EDI Forum, voI. 6, No 2, 1991, p 11
tronic commerce and regional networks in healthcare. In addition, it outlines some of the overarch-ing issues that affect the adoption of the technolo-gy by participants-industry fragmentation, theslow development of standards, the fragmentedregulatory and policy environment, as well as con-cerns about privacy, confidentiality, and securityof health information in a networked environ-ment.
ADMINISTRATIVE SIMPLIFICATIONAdministrative simplification has come to meanstreamlining and standardizing the transactionsbetween health care providers and payers to re-duce costs. The administrative costs of providinghealth care have been estimated at between $108billion and $135.1 billion per year in 1991,1 or be-tween 12 and 15 percent of the health care bill. Es-
1 Lewin-VHI, “Reducing Administrative Costs in a Pluralistic Delivery System Through Automation,” prepared by A. Dobson and M.
Bergheiser for the Healthcare Financial Management Association, Apr. 30, 1993.

Chapter 3 Networks for Health Information | 81
timates of annual savings that could be realizedthrough increased use of information technologyto streamline administrative functions haveranged from $5 billion to $36 billion,2 or enoughto reduce administrative costs between 0.5 and 3.6percent.
Administrative simplification generally meansnot only standardizing forms, procedures, and in-formation requirements, but also moving to elec-tronic technologies from paper-based transactionsand recordkeeping. This chapter will review someof the technological, legal, and economic issuesinvolved in administrative simplification. It alsodiscusses more generally the concept of “electron-ic commerce,” the exchange of business informa-tion and money through computer networks, andspecific tools for electronic commerce such aselectronic data interchange (EDI). (See boxes 3-1and 3-2.)
In the traditional “fee-for-service” health caredelivery system, the health care provider performsservices for the patient and then submits a bill tothe patient. If the patient is insured, either the pro-vider or the patient will submit a claim to the payer(insurer) to reimburse the patient or to pay the pro-vider directly on the patient’s behalf. The informa-tion exchanged between care providers and payers(insurers) can be very complex. The informationthat a payer requires a health care provider to fur-nish in order to get a claim paid depends not onlyon the payer’s policies, but on the laws of thestates in which the payer, provider, and patient arelocated. In addition, because many patients arecovered by more than one insurance plan, theremay be secondary or tertiary payers involved inpaying a single bill. From the provider’s point ofview, getting that bill paid may be quite burden-some. The various payers may not only requiredifferent information, in different forms, but may
also require the provider to furnish informationabout the other payers in order to coordinate bene-fits for the patient.
Several studies of health care administrativecosts have suggested that the large number of dif-ferent payer institutions (over 6,000) and the vari-ety of formats in which they request claiminformation are factors in making the cost ofhealth care administration much higher for theUnited States than for other industrialized coun-tries.3 A government-mandated change to asingle-payer system might reduce these costs, butsuch an action appears unlikely. Administrativesimplification, through the introduction of elec-tronic transactions and through standardization oftransactions and processes, may offer a way toachieve more modest savings.
Many managed care companies now performthe functions of both payer and provider. How-ever, this does not necessarily reduce the numberof transactions or ensure that administrative sim-plification will be achieved simply by enrollingmost of the population in health maintenance or-ganizations (HMOs) or other managed care sys-tems.4 While some interorganizational transac-tions are eliminated, they are often replaced byanalogous exchanges of information within themanaged care company. In addition, managedcare organizations are “information hungry” andare creating new management information ex-changes between their “provider” and “payer”components.
In some HMOs, where patients are served onlyby providers employed by the HMO and where allfinancial risks (the insurance functions) are as-sumed by the HMO itself, there is usually littleneed to submit claims to payers, except for occa-sional referrals to outside specialists. However,managed care is coming to have forms. Managed
2 Project HOPE Center for Health Affairs, Bethesda, MD, “Estimating the Cost-Effectiveness of Selected Information Technology Applica-
tions,” unpublished contractor report prepared for the Office of Technology Assessment, U.S. Congress, Washington, DC, March 1995.
3 U.S. Congress, Office of Technology Assessment, International Comparisons of Administrative Costs in Health Care, OTA-BP-H-135
(Washington, DC: U.S. Government Printing Office, spring 1994).
4 For more description of managed care, see box 1.1.

82 Bringing Health Care Online: The Role of Information Technologies
Electronic Data Interchange (EDI) IS defined as the application-to-application interchange of busi-
ness data between organizations using a standard data format. 1 A computer application is a software
system that performs work Information IS routed through telecommunications networks, received by an
organization’s EDI system, and processed by its computer applications—all without human intervention.
Redundant data entry IS thus eliminated, which increases the accuracy of information and reduces ad-
ministrative costs.
Organizations doing business with one another are called trading partners. Companies have used
EDI to reduce the costs of exchanging and processing documents for more than 25 years. In the last
several years, however, companies and consultants have placed EDI into a larger context called elec-
tronic commerce
Electronic commerce IS a management concept in which all information flows between and within
organizations through networked computer systems Work can be done in ways that differ from a paper-
based system. In electronic commerce, for Instance, a process made up of discrete tasks may be per-
formed as a series of parallel tasks. Only one person can work on a paper document at a time. When
the Information contained on that document is freed from the constraints of paper and ink and is avail-
able in electronic form, several people can access, use, and transform the information at the same
time.
EDI is not a concept like electronic commerce, it is a technology consisting of rules and standards
programmed into computers One could say that EDI is to electronic commerce as statistical process
control IS to total quality management, that is, EDI is one of the tools required to put the management
concept of electronic commerce into action.2
Standardization is the key to EDI. Computers cannot process the Information that moves between
organizations electronically unless it is encoded in a manner that the computers at both organizations
can recognize. In other words, both computers must be able to speak the same language. In Iinguistic
terms, they must follow standard usage. EDI provides a set of rules, grammar, and syntax that forms the
basis of standard usage in the electronic exchange of business data. EDI is both the means and the
language that computers use to “talk business.”3
SOURCE: C. Canright, “Electronic Commerce and Networking in Health Care, ” unpublished contractor report prepared for the Off Iceof Technology Assessment, U S Congress, Washington, DC, Jan 31, 1995
1 C. Canright, “The Problem of Data Mapping, " EDI Executive, voI. 4, No. 6, June 1989, p 12 G. Gerson, Sr., “lnterview with Captain Bruce Bennett, USN, Executive Agent for Electronic Commerce, United States Depart-
ment of Defense, ” EDI Forum, vol. 6, No 3, 1993, p 423 R.W. Notto, “EDI Standards: A Historical Perspective, " EDI Forum, vol. 1, No. 1, 1988, p. 120.
care organizations can have a variety of relation- Managed care organizations also exchange ad-ships with providers (e.g., they may be em-ployees, or they may accept patients underexclusive or nonexclusive contracts). They mayalso have a variety of relations with payers, as-suming some financial risk internally, while stillsubmitting claims to other payers. Thus, these or-ganizational arrangements still involve transac-tions between provider and insurer organizations.
ministrative or clinical information internally andwith their contract providers. In order to be profit-able under flat-rate capitated contracts, managedcare organizations must reduce duplicativeservices and manage each patient’s utilization ofservices. This means that each clinician in the sys-tem who encounters a patient should ideally haveaccess to a fairly complete medical record in order

Chapter 3 Networks for Health Information 83
IValue-added networks (VANS) are the means most companies use to exchange electronic data inter-
change (EDI) transactions. VANS are the electronic equivalent of a package delivery service Rather
than make a direct computer connection with trading partners, companies send their data to a VAN It
receives a bundle of EDI transactions—representing many types of business documents and bound for
many different trading partners—and routes the individual transactions to the appropriate trading part-
ner’s electronic mailbox, When the trading partner connects with the network, the EDI transactions are
transmitted to its computer. VANS make EDI easier because they eliminate the scheduling problems
that arise when making direct computer connections. They can also be more secure than direct com-
puter connections because trading partners are isolated from each other’s systems.
SOURCE: C. Canright, “Electronic Commerce and Networking in Health Care, ’ unpublished contractor report prepared for the Officeof Technology Assessment, U S Congress, Washington DC, Jan 31, 1995
to know what has been done by others. It alsomeans that management should know what re-sources are expended on that patient, even whenthere is no need to actually generate a bill. Manymanaged care organizations are finding the needfor “encounter reports” that contain much of thesame information that is currently included in in-surance claim forms in a fee-for-service system.While the encounter report could be considered aninternal communication within the managed carecompany, in some cases delivering it will takevery much the same technology and pose many ofthe same problems as the delivery of claim in-formation between a provider and payer.
ADMINISTRATIVE ACTIVITIES IN HEALTHCAREAdministrative activities related to health care oc-cur at all levels of the health care system, includ-ing health care providers, payers, and local, state,and federal government agencies. These activitiesinclude:■ Health care providers (individual and institu-
tional): Calculating bills and billing payers;transmitting records to outside providers orpayers; internal financial management; regula-tory compliance; utilization review; quality as-
in
●
in
■
surance; and acquisition, distribution, andstorage of equipment and supplies.Payers: Claims processing; coordinating bene-fits with other payers; claims payment; manag-ing plan enrollment and eligibility; statisticalanalyses and quality assurance; and regulatorycompliance.Employers and other large purchasers ofhealth care services: Comparing and selectingplans; and managing enrollment of employeesor members.Consumers (patients): Submitting claims:tracking eligible expenses; and paying copay-ments and uncovered bills.Government agencies: All of the above activi-ties in roles as providers, payers, and employ-ers; data collection for vital statistics; healthcare financing data; and regulatory oversight.
A fuller description of administrative activitiesand costs is available in a previous Office of Tech-nology Assessment report, International Com-parisons of Administrative Costs in Health Care. -s
PROVIDER ADMINISTRATIVE ACTIVITIESMany information exchanges that take place with-in a single provider’s organization (e.g., admis-s ion-discharge-transfer messages or billing
5 Office of Technology Assessment, op. cit., footnote 3.

84 | Bringing Health Care Online: The Role of Information Technologies
information) are automated. Use of the HealthLevel 7 (HL7) standard, discussed in chapter 2,which is used for exchange of clinical informa-tion, is also growing for administrative and patientmanagement information. Most vendors of bothadministrative and clinical information systemsare supporting the HL7 standard. Use of comput-ers in administration and patient management isnot limited to hospitals or large clinics. Althoughmany doctors’ offices still rely on paper patient re-cords and billing systems, a growing number arecomputerizing at least some of their business andadministrative functions. Computerized practicemanagement systems (PMSs) automate functionssuch as accounts receivable, insurance, billing,and appointments; they also record the patient’sdiagnoses, procedures, medical history, and finan-cial history. PMSs offer a wide range of function-ality and very little standardization; some systemswere developed on an ad hoc basis by their usersand others were purchased from one of more than400 vendors. Some PMSs also help physiciansdeal with the complexities of managed care con-tracts, for example, by maintaining member lists,posting capitation payments from plans, trackingthe number of visits or services provided for eachpatient, and providing reports on the profitabilityof the relationship with each plan.
Typically, providers only have informationabout their own contribution to a patient’s care—for example, hospitals maintain records of inpa-tient stays and doctors’ offices keep track of officevisits. But to manage patients’ use of resources ef-fectively, managed care organizations want totrack patient care over several years and integratedifferent services that were performed at variouslocations. Integration of financial and clinical in-formation is also important to managed care.6
Integrated Delivery Systems (IDSs) are emerg-ing to meet the need of health care organizations todeliver a full range of health care services to theircovered populations. An IDS, either through own-
ership, partnership, joint venture, strategic al-liance, or contract, brings together hospitals,ambulatory care facilities, affiliated physicians’offices, nursing homes, home care services, labo-ratories, wellness programs, and so on. IDSs havebeen springing up rapidly as managed care com-panies position themselves to compete; the resultis a conglomeration of provider organizationswith different levels and types of automation anduses of information technology. Some IDSs aremaking the investments needed to develop “enter-prise-wide” information systems to allow ex-change of clinical and administrative informationamong their various components.
Health care providers perform a variety of ad-ministrative activities associated with each ad-mission, visit, or episode of care. These activitiesbegin well before the face-to-face encounter withthe patient and last long after the patient has leftthe institution or professional’s office. Preadmis-sion and preregistration cover a variety of logisti-cal, clinical, and financial activities, includingeligibility confirmations, certifications, and au-thorizations for care, which generally requirecommunication with the patient’s payer.
EXCHANGING INFORMATION BETWEENPROVIDERS AND PAYERSDuring the course of treatment or admission, addi-tional transactions flow between the provider andpayer or care manager, including reauthorizations,recertifications, interim billing, and a variety ofreview activities. Due to the limits on some healthcare coverage, the provider might also have toredo the eligibility function as well. Figure 3-2 il-lustrates some of the information flows betweenpayer and provider at various stages in the proc-ess.7
At some point during or after treatment, theprovider will issue a bill and/or a claim. Copies ofthe bill might go to the patient, as well as to one or
6 D. S. Kolb and J. L. Horowitz, “Managing the Transition to Capitation,” Healthcare Financial Management, February 1995.7 The following description of administrative information exchanges is based on information from D. Rode, immediate past co-chairman,
ASC X12 Insurance Subcommittee, Healthcare Task Group, personal communication, May 12, 1995.

Chapter 3 Networks for Health Information 185
Health care provider
Pre-admission,registration, andtreatment period
Admission or registration
Inpatient treatment
- - - - - - - -Discharge
Billing period
- - - - - - - - - -
Followupcollection period
Payer or primary providercommunications
Eligibility verification request
<—Eligibility confirmation or denial-----------------------------------—Primary provider,
benefits department, or
Coverage data request---------------------------------------> eligibility department
<----Coverage data reply
Precertification and/or authorization request->
<—precertification and/or authorization approvalUtilization
Recertification request review
<-Recer t i f i ca t ion approva l
Claim submission (interim bill and/or medical data)-->
<-- - In ter im payment
Claim submission (final bill and/or medical data)--->
<—Claim status inquiryI
Claimsprocessing
Claim status inquiry response
! J
transfer
SOURCE: Adapted from D Rode, “EDI Holds Potential for Cutting Receivables Processing Costs,” Healthcare Financial Management Association,March 1990, p 15
more payers. When more than one payer is in-volved, the provider may send a bill to all partiesand work through a very complicated process tocoordinate billing (and payment). Even patientswho belong to managed care entities that capitatepayments or use other reimbursement methodsmight need to have all or parts of their bill or claimsent for management information purposes.
After the initial claim or billing, the providermay have several followup steps, such as provid-ing additional information to a payer inquiringabout the status of a claim previously sent to oneor more payers. Because more than one provider
may be billing for services rendered during thesame episode of care, both providers and payersmay have to coordinate and track their informa-tion. Many institutions and some individual pro-viders are also required to send additionalinformation as attachments to the claim. Amongthe required documents are discharge abstracts,surgical reports, first reports of injury, and attesta-tion reports. Late submission of these reportsmight also delay the payment of the originalclaim.
Finally, the provider receives a payment or re-jection from the payer. This is a two-step process

86 I Bringing Healthcare Online: The Role of Information Technologies
Information systems allow many caregivers to share clinicaland administrative information.
because the provider must reconcile the paymentto the original claim, as well as to the posting proc-ess at its financial institution. The information re-ceived with the payment or rejection (usuallycalled remittance advice) can be as simple as acheck number or it may include pages of informa-tion responding to each line of the original claim.If the patient has health care coverage from a sec-ondary payer, the provider may then have to repeatthe process, submitting a secondary billing claimto that payer, and including with the claim in-formation about what was and was not paid by theprimary payer (some institutions bill the patientwho is then responsible for collecting from sec-ondary payers). On average, most institutions donot see payment on a claim for well over twomonths. Individual and professional paymentsoften take longer.8
During the course of these provider-payertransactions there can be many telephone contactsand letters exchanged among the parties. In an in-patient environment, which is relatively stable,the cost of carrying out these transactions is rela-tively low compared to the amount of the claim.However, the opposite is true in an outpatient orambulatory-care setting. The provider’s costs forprocessing each transaction, claim, or eligibility
verification is about the same as in an inpatientsetting, but the resulting revenue is much less. Themove of health care toward more outpatient carewill accentuate this problem.
The traditional model for health payments hasbeen that the provider charges the patient a fee forthe services provided. The patient (or the provideron the patient’s behalf) files a claim with the pa-tient’s insurer (payer) for payment of the coveredportion of this fee. There are several types of trans-actions in the fee-for-service environment whereelectronic communications could be applied.These transactions are: 1) claims submission, 2)remittance advice, 3) claims inquiry, 4) enroll-ment, and 5) eligibility inquiry.
Claims submission is the process of preparingand submitting documents to a payer on behalf ofa patient. Nearly all claims for hospital servicesare submitted by the provider. Claims for servicesin a physician’s office may be prepared by eitherthe patient or the provider; in preferred providernetworks, the physician usually files the claim. In-formation required to complete the claim formmay have entered the provider’s accounting sys-tem through either a direct interface with other in-formation systems in the provider organization, orthrough keyboard input by a data-entry clerk whoreads the various paper documents about the pa-tient and enters the data into the patient-account-ing system. This system, whether paper-based orcomputer-based, must prepare a claim documentin a form that is acceptable to the payer.
Remittance advice is a document returned tothe provider by the payer along with payment afterthe claim is processed. The remittance advice ex-plains what the payment covers and how the claimwas adjudicated by the payer. The providercompares the payment with the original claim todetermine whether the amounts match. If theclaim and payment do not match, the clerk checksthe remittance advice to determine where the dif-ferences lie. When the claim and the various pay-ments match, either immediately or after a process
8 A review of quarterly analyses by Zimmerman& Associates, Hales Comer, WI, shows receivables always exceed 60 days. Ibid.

Chapter 3 Networks for Health Information | 87
of negotiating discrepancies, the claim is recon-ciled with its associated payments and closed. Re-mittance advice can be a paper document thataccompanies a check; an electronic document thataccompanies an electronic funds transfer; or anelectronic document that is separate from, but re-lated to, an electronic funds transfer sent by othermeans.
Claims inquiry is a process that providers useeither to determine when payment will be made orto negotiate discrepancies in a claim that has beenpartially paid. Often, inquiries are telephone con-versations, but some vendors are beginning to of-fer online inquiries.
Enrollment is a process that involves the payerand the patient’s employer (or sponsor of thehealth care plan in which the patient enrolls). En-rollment transactions occur when people join ahealth plan, change their family status, move,change plans, and so on.
Eligibility inquiries are transactions betweenproviders and payers to determine what benefitsthe patient is entitled to. Patients arriving at thedoctor’s office, hospital, pharmacy, or other pro-vider location are asked what kind of coveragethey have and from whom. This information isconfirmed by an inquiry to the payer by mail, tele-phone call, or an electronic process. Having thisconfirmation quickly is useful to the provider: itmeans that correct copayment amounts can be col-lected right away, for example, or that certain ser-vices will not be offered to people who are notentitled to them. EDI standards have been devel-oped for the above transactions. (See box 3-3.)
In a managed care environment, some of thesetransactions are different. For example, in anHMO, where members are charged a fixed fee perperson (capitation) and are not billed for individu-al services, the traditional insurance claim is un-necessary. In some cases, however, HMOs areusing an encounter report to provide managementinformation about services provided, and these
could be considered surrogates for insuranceclaims. Enrollment transactions and inquiriesabout a member’s eligibility for services are as im-portant in a managed care environment as in a fee-for-service system; in some cases, they may beinternal transactions between parts of the same or-ganization (perhaps at different locations) ratherthan between different organizations.
❚ Status of Electronic InsuranceTransactions9
Health Care Financing AdministrationAs the largest payer of health care claims in thecountry, the federal government for years has en-couraged providers and insurers to do businesselectronically, especially the submission of Medi-care claims. The Medicare program (and the fed-eral portion of the Medicaid program) isadministered by the Health Care Financing Ad-ministration (HCFA) which, beginning in the1970s, established electronic links between hos-pitals and fiscal intermediaries—the insurancecompanies that process Medicare claims undercontract with the government. Currently, 80 dif-ferent insurance companies process some 730million Medicare claims annually.10
Initially, the shift away from paper involvedhospitals submitting bills by either direct-dataentry (DDE) terminal, linked directly by leasedphone lines to the mainframe computer of the fis-cal intermediary, or by computer tape. In eithercase, clerical personnel would key in the neces-sary information. For computer tape transactions,they would format the information on computertape, which was then sent to the fiscal intermedi-ary. For the fiscal intermediary, the volume of in-formation received on tape—and thus the reducedcosts of processing as compared with paper sub-missions—justified writing separate computer in-terfaces to translate the different tape formats asrequired.
9 This section is based on C. Canright, “Electronic Commerce and Networking in Health Care,” unpublished contractor report prepared for
the Office of Technology Assessment, U.S. Congress, Washington, DC, January 1995.
10 “Implementing EDI on a Colossal Scale: An Interview with HCFA’s Carol Walton,” EDI Forum, vol. 6, No. 2, 1993, p. 47.

88 I Bringing Health Care Online: The Role of Information Technologies
T h e k e y t o t h e c o n c e p t o f a d m i n i s t r a t i v e s i m p l i f i c a t i o n l i e s i n d a t a s t a n d a r
throughout this report. Indeed, the one thing that nearly everyone involved in health care automation
agrees on IS that uniform data standards are required to control health care administration costs.
Roughly speaking, data-processing standards have two components: content and transmission.
Data-content standards specify how meaning should be represented. Data-transmission (or messag-
ing) standards specify how information encoded as strings of binary digits should be structured for
transmission over wires or through the air.
Data TransmissionEDI standards for business documents structure information in such a way that computers at differ-
ent organizations can process it. Computers do not process documents like humans read documents.
Computers process data. To the computer, EDI is not a facsimile of a document that a computer stores;
it is a stream of data that actually causes a computer application to perform a specific action. 1
Data, however, are not quite enough. Data may be two-character codes that represent an idea or a
string of characters that represent, for instance, a Social Security number (SSN). Because all data are
represented as strings of 0s and 1s, computers need a means of distinguishing data denoting one idea
from data denoting another.
Computers distinguish one bit of data from another through positional relationships. If a health care
claim were written as a single line, then the computer would need to know what part of the Iine repre-
sented an SSN and what part represented a patient’s name. By cutting that Iine of characters up into
data elements, a computer can recognize one type of reformation from another. The first data element
might represent a patient’s name and address, while the second represents the line items on a claim.
EDI standards provide that type of structure. They provide a common way for computers to structure
the data that represent business documents.
The standards for moving the data that appear on common business documents between organiza-
tions are called the ASC Xl 2 standards for electronic data interchange, named after the American Na-
tional Standards Institute’s Accredited Standards Committee Xl 2, which develops them. ASC Xl 2 stan-
dards define a syntax and provide a structure for moving data between organizations. In that way, EDI
standards are external data-transmission standards. The structure that represents a business document
is ca l led a t r a n s a c t i o n s e t ; t r a n s a c t i o n s e t s a r e t h e e l e c t r o n i c e q u i v a l e n t s o f p a p e r b u s i n e s s d o c u m e n t s .
Transaction sets, then, are composed of an ordered series of data segments. Data segments are
analogous to the groups of data that perform specific functions within a business document, such as
Iine items on a purchase order, terms of payment on an invoice, or the identification (name and ad-
dress) sections that appear on any business document. Segments, in turn, are constructed of an or-
dered series of Iogically related data elements. Data elements specify such things as unit of measure,
price, quantity, and currency.
Data ContentThe content of standards comes to the fore at the data-element level of the X12 standards. Much of
the content of a transaction set consists of codes used by a company or an industry to represent the
1E.J. Bass, “lntroduction to EDI,” unpublished paper presented to Accredited Standards Committee X12, St
Charles, IL, May 16, 1988
(continued)

Chapter 3 Networks for Health Information 189
specifics of its business. As much as possible, the Xl 2 committee seeks to standardize content across
industries. The segment and data elements used in transaction sets to represent a name and address,
for Instance, are the same for transportation concerns as for health care concerns.
Just because two organizations support the Xl 2 standards, however, does not mean that commu-
nication between them is seamless. On a technical level, both systems are compatible because they
are communicating using a common language. On a content level, however, compatibility is nowhere
near guaranteed, particularly in health care. The data content of ASC Xl 2 standards comes from indus-
try- and company-specific codes. In health care, for instance, the ASC Xl 2 health care remittance ad-
vice standard uses Adjustment Reason Codes maintained by the Blue Cross and Blue Shield Associa-
tion and Current Procedural Terminology (CPT) Codes maintained by the American Medical
Association. In fact, any organization can petition the ASC Xl 2 committee to include its codes into the
standard. As long as those codes meet the test of business necessity and perform functions that exist-
ing codes cannot perform, the codes are incorporated into the standard,
As a result, ASC Xl 2 standards accommodate a huge amount of data content and they can perform
the same business function in many different ways. Most Industries have Iimited this variability by pub-
lishing Implementation manuals specifying how a particular transaction set should be used to conduct
business with companies in that Industry.
The data content used in the ASC Xl 2 health care transaction sets IS still too broadly defined, Nearly
everyone revolved in EDI in the health care Industry agrees that widespread EDI implementation wiII
require greater uniformity in data content. As the WEDI committee puts it, “A significant barrier to the
Implementation of EDI IS the fact that implementation guides have not been developed that Incorporate
standard requirements and content across large segments of the health care industry It IS critical that
private payers and government programs, including Medicare and Medicaid, use a common set of for-
mats to achieve the highest level of administrative cost savings and accelerate the implementation of
EDI.” 2
The health care industry needs a business model that specifies the data required in each transaction
and how they should be encoded and structured within the standards. Efficient standards require that
all participants in the industry agree on. 1 ) what data to collect, 2) when to collect it, and 3) how to
collect it.3
In the absence of industrywide implementation manuals, many in the industry are relying on imple-
mentation guidelines created by the Health Care Financing Administration (HCFA), the first payer to
Implement the health care claim payment and advice (ASC Xl 2.835) transaction set and the claim sub-
mission (ASC Xl 2.837) transaction set,
SOURCE: C. Canright, “Electronic Commerce and Networking In Health Care, ” unpublished contractor report prepared for the Off Ice
of Technology Assessment, Jan 31, 1995

90 | Bringing Health Care Online: The Role of Information Technologies
But as large chain-affiliated hospitals foundthat they were dealing with many different for-mats, they asked HCFA to establish a standardtape format, which it did in the late 1970s. Thestandard tape format allowed hospitals and otherlarge institutions to introduce a degree of stan-dardization into their claims submissions process.However, they still faced different data require-ments from different fiscal intermediaries in dif-ferent states.
During the 1980s, with the growing use of per-sonal computers, HCFA also began to encouragephysicians to do business electronically. In themid-1980s, HCFA aggressively put pressure onproviders to convert to electronic billing, and by1985, HCFA received about two-thirds of Part Ahospital claims and one-third of Part B supple-mental insurance claims electronically.11 Part Aclaims are submitted by hospitals and other largeinstitutions for inpatient care. Part B claims aresubmitted by physicians and clinics.
HCFA’s push for electronic claims processingcame to a standstill in the late 1980s. Congress, aspart of an attempt to balance the federal budget,mandated an extended timeframe for paying allMedicare claims. HCFA, however, had used expe-dited payment as an incentive for providers to sub-mit bills electronically. Without the incentive offaster payment, many providers saw no reason tomake the investments needed to submit claimselectronically.
HCFA started to promote electronic billingagain in 1991 as part of a short-term strategy to re-duce administrative costs. Until then, HCFA hadconcerned itself solely with automating claims. In1991, however, the agency turned its attention toautomating the remittance advice document,which accompanies a claim payment and explainswhat the payment covers. Rather than develop itsown remittance format, HCFA adopted the EDI
format for health care remittance advices that hadjust been approved by Accredited Standards Com-mittee X12. HCFA became the first organizationto test the new EDI remittance advice format andremains its largest user.
In 1992, HCFA established a uniform paymentpolicy and procedures for making electronic pay-ments to medical providers for Medicare claims.Providers who submit at least 90 percent of theirMedicare claims electronically can receive claimspayments electronically through the banking in-dustry’s automated clearinghouse network andtheir local banks, rather than through paper checksmailed to their offices. HCFA again had a fasterpayment incentive to encourage electronic claimssubmissions. Since then, HCFA has adopted theEDI-based claims form as its standard and man-dated that all Medicare processors adopt it by July1, 1996. The agency’s long-term goal is to have allMedicare claims handled electronically by theyear 2000.
Private InsurersBecause many Medicare beneficiaries also carryprivate insurance policies that cover deductiblesand copayment obligations under Medicare,HCFA’s EDI projects also affect the administra-tion of payments by private insurers. In manystates, the fiscal intermediary for the Medicareprogram obtains its own private insurance claimselectronically through the same linkages used forMedicare. With Medicare moving toward 100 per-cent electronic claim submission, “it seems likelythat private firms will be making use of thetechnology as well.”12
Some large insurers accept and process nearly80 percent of claims by computer.13 However,there are many small insurers that are only begin-ning to accept electronic claims. Today, about 75percent of hospital claims are submitted electroni-
11 M. Buffington, Director of Claims Processing, Health Care Financing Administration, personal communication, Sept. 7, 1994.
12 D. Fularczyk, Manager, Blue Cross and Blue Shield United of Wisconsin’s Proservices subsidiary, quoted in T. Higgins, “Setting Stan-
dard for Electronic Claims Could Lead to Paperless Providers,” The Business Journal-Milwaukee, February 1993, pp. S3-S5.
13 B. Politzer, “Claims of Excellence,” HMO Magazine, vol. 32, No. 6, November-December 1991, p. 39.

Chapter 3 Networks for Health Information | 91
cally, but the vast majority of these are Medicareclaims submitted to HCFA rather than to privateinsurers. Physicians submit some 16 percent oftheir claims electronically in total; however, theysubmit 47 percent of their Medicare claims elec-tronically.14
Electronic Medical Claims ServicesOne of the difficulties of connecting providers andpayers is the different data and networking for-mats that exist in the health care industry. Conven-tional wisdom, for instance, holds that electronicclaims are structured in some 400 different ways.Electronic medical claims companies, includingvalue-added networks and clearinghouses, pro-vide services that connect providers with manypayers using a single system.15
These services give providers a single point ofelectronic contact to many payers. In addition torouting information between a provider and itspayers, they edit and reformat claims data. Thisfrees providers from the burden of programmingtheir systems to handle the wide variety of elec-tronic formats. For example, a physician’s officewanting to send claims electronically generallyuses personal computer software that communi-cates with the service via telephone lines. Physi-cians using practice management systems canoften integrate this software with their systems.This requires that the processing service cooperatewith the vendor of the practice management sys-tem (there are several hundred in the country) towrite the necessary interfaces. For physicians whodo not use practice management systems, the ser-vice provides software that allows clerical person-nel to enter claims data directly into forms thatappear on a PC screen.
Provider-specific edits are needed on eachclaim. Because health care claims are not univer-sally standardized, different payers require data tobe presented differently in their claims. One payer
may also require data that another payer does not.The software checks the claims that are keyed in orreceived from a practice management system tomake sure they conform to the data requirementsof the designated payer.
If the claims meet all requirements, the PC soft-ware sends them to the electronic claims service.The service performs further editing and thentransmits the claims to payers, in some casesthrough direct network connections to the payerand in others through a claims clearinghouse thathas such a connection.
Many electronic medical claims services canperform some or all of the following transactiontypes: electronic claims filing; claims-status in-quiry and online claims correction; eligibility andbenefits inquiry; electronic remittance advicedata; automated electronic remittance posting,along with supplemental and secondary billing;and electronic funds transfer. The services avail-able to a provider vary by payer and depend onpayer capabilities. Not all payers, for instance, canprovide remittance advice data electronically.
Most of the transactions processed by electron-ic medical claims services are currently not basedon EDI standards, particularly the nonclaimstransactions. However, use of standard EDIclaims may increase as HCFA mandates them.Until then, however, many payers are not accept-ing standard EDI claims. Nonclaims transactions,such as eligibility verification, are not based onEDI standards because the standards are eitherbrand new or do not exist. Many of these servicesintend to support EDI standards, but place moreemphasis on making transactions electronically,whatever the format. They believe that it is betterto begin electronic processing now than to wait forthe often slow standards-development cycle.
The initial cost of getting a physician startedwith an electronic claims service is between$1,500 and $2,500, depending on the size of the
14 “Automated Medical Payments Statistical Overview,” Automated Medical Payments News, Feb. 8, 1993, p. 3.15 B. Dodge, Vice President, HCS, Inc., personal communication, Aug. 26, 1994.

92 | Bringing Health Care Online: The Role of Information Technologies
practice. Staff training may be an additional ex-pense. There is also a per-transaction fee, whichcould be on the order of $0.35 to $0.85, dependingon the type of transaction. Claims fall toward theupper end of the range because they are more com-plex documents and contain more data, whiletransactions such as eligibility inquiries costless.16
In the early years of EDI development in otherindustries, value-added networks (VANs) offeredsimilar translation services for companies that didnot want to develop or install their own EDI man-agement systems. Over time, companies pur-chased their own EDI systems, rather than paytranslation fees to the VANs. A similar develop-ment is unlikely in health care. Only larger institu-tions are likely to have the financial and staffresources to manage an EDI system. For smallermedical practices, claims services and VANs maycontinue to provide a way to transact businesselectronically.
Financial InstitutionsCompletely automating the health care paymentprocess means involving the trading partners’ fi-nancial institutions. In the 1970s, the banking in-dustry established its own formats for electronicfunds transfer (EFT) through the National Auto-mated Clearing House Association (NACHA).NACHA governs the automated clearinghouse(ACH), a network of computer-based check-clear-ing and settlement facilities for the interchange ofelectronic debits and credits among financialinstitutions (note that bank clearinghouses are dif-ferent entities from the insurance clearinghousesmentioned above).
The banking industry designed its original EFTformats to move money between financial institu-tions. In the 1980s, NACHA worked with corpo-rations to set ACH formats for corporate-to-corporate payments. At that point, the NACHAformats for EFT began to conflict with, and then
migrate toward, industry’s formats for EDI. Thehybrid of EFT, whose purpose is to move moneybetween financial institutions electronically, andEDI, whose purpose is to move business data be-tween corporations electronically, became knownas financial EDI (or EFT/EDI).
Since the development of financial EDI for-mats in the mid 1980s, the number of corporationsusing the ACH to make payments has steadily ris-en, showing an average annual growth of between25 and 30 percent per year for the past severalyears. In terms of total payment volume, however,financial EDI volume statistics are less impres-sive. Last year, the estimated 13 million paymentsmade through financial EDI represented onlyabout 0.1 percent of the total estimated volume of11.7 billion payments.17
Financial EDI payments, in all industries, con-sist of two parts: the payment and the remittanceadvice. One difficulty faced by the banking indus-try is that few banks are capable of processing allof the information contained in financial EDI pay-ments. ACH formats themselves are not compat-ible with the information-laden EDI formats. Tomove native EDI data through the ACH requireswrapping an EDI transaction in a NACHA enve-lope. The financial institution then unwraps andprocesses the EDI payment transaction. The en-veloping process puts some limitations on theamount of data an EDI transaction can carry—apotential problem given the amount of data in ahealth care remittance advice document.
As a result, many companies are sending EDIpayment orders and remittance advices throughseparate paths—the payment itself as a simpleEFT transfer through the ACH and the remittanceadvice as an EDI transmission through a VAN. Inthat case, companies receive the payment-depositinformation from their banks and reconcile it withthe remittance data received from the VAN.
However, some banks that specialize in finan-cial EDI are moving into the health care market.
16 Ibid.17 National Automated Clearing House Association figures reported in Canright, op. cit., footnote 9.

Chapter 3 Networks for Health Information | 93
BankAmerica, San Francisco, CA; Chase Man-hattan, New York, NY; Huntington Bancshares,Columbus, OH; PNC Bank Corp., Pittsburgh, PA;and National City Corp., Cleveland, OH, areamong the national and regional banks that nowprocess medical bill payments electronically forhospitals, clinics, and other health care providerswho are their banking customers. Some of them,in addition to handling EFT payments, are also of-fering the services of a processing service.
❚ Standardized FormsThe federal government has played a major role instandardizing electronic forms in the health careindustry. For instance, institutional providers areencouraged to submit Medicare and Medicaidclaims using the UB-92 form, which was createdby the National Uniform Billing Committee(NUBC). The difficulty is that each state adds itsown requirements to the UB-92 form, whichmeans that some payers and nearly all softwarevendors have to support nearly 50 different ver-sions of the UB-92.18 Moreover, the EDI standardfor transmitting claims, ASC X12.837 (healthcare claim), can structure data contained in theUB-92 in several different ways, all of which arecorrect insofar as the standard is concerned.19 Theresult is that the health care industry’s standardsare not yet standard enough for easy implementa-tion of electronic commerce.
HCFA has developed implementation guidesfor health care claim and remittance advice trans-actions. By July 1, 1996, all electronic claims willbe submitted to HCFA using the standard forms.20
The HCFA requirement is expected to stimulateEDI use throughout the industry. To ensure thatthe health care industry uses a single EDI version
of the UB-92, the Workgroup for Electronic DataInterchange (WEDI) and the NUBC are develop-ing EDI implementation guidelines based on theHCFA guide, which is becoming the de facto in-dustry standard.
LINKING HEALTH CARE PROVIDERSWITH SUPPLIERS21
In contrast with health care payments, the use ofelectronic commerce between large health careproviders and hospital suppliers has a longer his-tory, dating back to the mid-1970s when theAmerican Hospital Supply Corp. (AHSC)introduced the first electronic order-entry (EOE)system called Analytic Systems Automated Pur-chasing (ASAP). ASAP initially allowed hospi-tals to place orders using a touch-tone telephone.As ASAP evolved, hospital purchasing managerscould enter orders into terminals connected toAHSC’s mainframe computer, which automati-cally reserved inventory and generated a packinglist. The system was so convenient that purchas-ing managers placed orders with AHSC at the ex-pense of its competitors.22 Hospitals achievedbenefits by: 1) eliminating manual order writing;2) reducing transcription errors that result whenorders are written manually or taken over thephone; and 3) increasing the accuracy and timeli-ness of order, delivery, and cost information.
The proliferation of other EOE systems becamea problem to major hospitals, especially chainsand large purchasing groups. Those organizationspurchased supplies from several vendors, whichmeant they had to use several different EOE sys-tems. They faced the same problems that have ledto the development of EDI in other industries:higher costs from having to support multiple pro-
18 D. Rode, “UB-92, HCFA 1500: The Genesis of EDI?” Health Care Financial Management, vol. 47, No. 1, January 1993, pp. 82-83.19 D. Hodges, Integrating Computer-Based Technologies Into HMOs (Washington, DC: Group Health Association of America, Inc., 1993),
p. 41.
20 M. Buffington, op. cit., footnote 11.
21 This section is based on Canright, op. cit., footnote 9.22 R. Forester, “A History of ASAP at Baxter Health Care: The Journey from Proprietary to X12 Standards,” EDI Forum, vol. 4, No. 1, 1991,
p. 96. (Baxter acquired the ASAP system when it merged with American Hospital Supply Corp. in 1984.)

94 | Bringing Health Care Online: The Role of Information Technologies
prietary systems,23 including additional space forthe terminals and additional training for purchas-ing personnel. Today, most hospital-supply com-panies are making a transition to EDI and offerEDI-based alternatives to their proprietary elec-tronic order-entry systems.
In addition to the companies that directly sup-ply hospitals and other providers, the companiesthat manufacture health care supplies and equip-ment are beginning to use EDI to connect with thesmaller companies that they rely on to distributetheir products to hospitals, physicians, and otherhealth care providers. For the manufacturers, EDIconnections result in cost savings because they nolonger need to key purchasing information intotheir systems. By automating business with alltheir distributors, the relatively small benefits thatcome from automating each trading relationshipare multiplied over a large base. For distributors, itis not clear whether the conversion to EDI resultsin net savings or net costs.
When the process of purchasing and paying forsupplies is automated through EDI, it can be inte-grated with a larger automated materials manage-ment information system that can includeinventory control, automatic replenishment,tracking of chargeable suppliers and equipment,invoicing, and patient cost accounting. Greateruse of information systems for these purposes hasbeen shown to improve inventory control and re-duce the costs of materials management in otherindustries. Currently, only a few hospitals andhealth care groups are using this technology to itsfull potential.24
The movement to electronic systems in hospi-tal materials management has not been pervasiveamong hospitals. By 1990, hospitals used EDI toplace some 24 percent of orders to suppliers.25
Purchase orders and confirmations still representthe bulk of EDI transactions in hospitals; hospitalshave been slow to use EDI for other purchasingfunctions, such as electronic invoicing and pay-ment.26 WEDI, for instance, estimated that some6,000 of 6,138 acute care hospitals require EDIupgrades.27
Overall, the health care supply portion of thehealth care industry has made a good start in auto-mating trading relationships. As suppliers offerand providers adopt more sophisticated materials-management strategies, EDI will become increas-ingly necessary as well as commonplace.
PHARMACEUTICAL INDUSTRY EDIThe drug distribution chain has been an early andsuccessful adopter of electronic commerce. Asearly as 1972, a major drug wholesaler began a pi-lot project to transmit purchase orders directly tothe computers of major manufacturers. Industryorganizations, such as the National WholesaleDruggists Association and the American SurgicalTrade Association, actively supported these acti-vities and encouraged the development of indus-try-wide standards. Use of electronic ordering wasfound to reduce order lead-times, which reducedinventory requirements. Some industry analystsbelieve that adopting electronic ordering is a ma-jor factor in alleviating and reversing economic
23 The terms “proprietary system” and “proprietary data format” refer to electronic business communications systems that work for a singlecompany—the one that provided the system or software. The terms “standard system” or “standard data format,” in contrast, refer to EDI sys-tems that are designed to ease communications with any organization that supports EDI standards.
24 ECRI, “Computer Information Systems, Materials Management,” ECRI Special Reports, 202765 424-008 (Butler Meeting, PA: 1995),p. 3.
25 Arthur Andersen & Co., Stockless Materials Management: How It Fits Into the Health Care Cost Puzzle (Alexandria, VA: HIDA Educa-
tional Foundation, 1990), p. 56.
26 J.J. Moynihan and K. Norman, “Health Care EDI: An Overview,” EDI Forum, vol. 6, No. 2, 1993, p. 11.27 Workgroup for Electronic Data Interchange, Report (Hartford, CT, and Chicago, IL: October 1993), p. 9-34.

Chapter 3 Networks for Health Information | 95
hardships that drug wholesalers had been experi-encing in the early 1980s.28 By 1986, 96 percentof drug wholesalers were using EDI, as were 90percent of pharmaceutical manufacturers—one ofthe highest penetration rates of any industry at thattime.
Today, electronic commerce has also expandedrapidly to independent drugstores and drugchains. About 95 percent of drugstores are com-puterized. Many of them order from distributorsusing either proprietary systems or EDI standardsand guidelines developed by the American Soci-ety of Automation in Pharmacy.
Because many prescription drugs are paid foror reimbursed by insurance plans, electronic linkshave also been established between pharmaciesand payers. A standard format for communicationbetween pharmacies and insurers is in widespreaduse. Online eligibility systems have helped tospeed processing and payments by enabling phar-macies to check a patient’s benefits before fillingthe prescription. After a physician or patient sub-mits a prescription (either by phone or in writing),the pharmacy enters the information from the pa-tient’s prescription benefit card (issued by the in-surer, health plan, or employer) and theinformation from the prescription into an onlinesystem using the National Counter PrescriptionDrug Plan’s (NCPDP) standards for real-timetransactions. Through this system, the pharmacycontacts a database where it can confirm the pa-tient’s eligibility status, find out whether the payerwill pay for this drug, determine the copaymentamount, and ascertain whether the payer allows orrequires generic substitutions.
Pharmacy claims are much less complex thanother health care claims, and a much larger per-centage of them are submitted electronically. In1993, over half of the prescription claims reim-
bursed by insurance payers were submitted elec-tronically and that percentage continues togrow.29 NCPDP recently introduced a paper-based claim form based on the electronic format tosimplify reimbursement for patients whose payersare not yet using electronic pharmacy claim sub-mission.30
The existence of large databases of prescrip-tion-related information in a standard format is of-fering new tools to both the pharmaceutical andinsurance industries. Databases are being used toanalyze the patterns of drug purchase, to developformularies or lists of preferred drugs, to comparecosts of alternative drugs, and to compare the cost-effectiveness of drugs to alternative treatments.
COMMUNITY AND REGIONALNETWORKING
❚ Community Health InformationNetworks
A community health information network (CHIN)can be either a proper or a generic name for a typeof information system that is still undergoing de-velopment and definition. Another term used iscommunity health management information sys-tem (CHMIS), which can also be both a commonor proper name. Both of these networks are envi-sioned as systems that allow the seamless ex-change of clinical or administrative informationamong health care providers, payers, and other au-thorized users. Currently, there are between 75and 100 community networks in early stages ofstartup or implementation that roughly corre-spond to the CHIN or CHMIS descriptions be-low.31 (This report will use the term CHIN asgeneric and will use CHMIS only when distin-guishing features of the CHMIS model).
28 P.K. Sokol, From EDI to Electronic Commerce (New York, NY: McGraw-Hill, Inc., 1995), pp. 212-219.29 Ibid.
30 G. Muirhead, “Stake Your Rx Claim: NCPDP Issues Standard Paper Form for Reimbursement,” Drug Topics, Nov. 7, 1994, p. 106.31 R. T. Wakerly, remarks at CHINs and CHMISs: Networks for Community Health Information and Management, meeting of the National
Health Policy Forum, Washington, DC, Oct. 25, 1994.

96 I Bringing Health Care Online: The Role of Information Technologies
Small clinics and individual health care providers arebeg inn ing to use compute r -based sys tems fo r p rac t i cemanagement , recordkeep ing , and communica t ion w i thlabora to r ies , hosp i ta l s , and insure rs .
At their most basic, CHINs are electronic sys-tems whereby claims filing, eligibility verifica-tion, and other transactions can be performed by aprovider (whether a single physician or a majorhealth care organization) and an insurance clear-inghouse; or whereby a physician’s office can con-tact a hospital’s information system to obtainclinical or administrative information on a patient.However, CHIN developers envision them as ex-panding into systems that link all participants inthe health care system—providers, payers, banks,pharmacies, public health agencies, employers,and others. Moreover, a fully developed CHINmight allow a physician to assemble a single pa-tient’s information across different institutionsand databases to produce a complete medical re-cord; or it could permit a researcher to aggregatethe data for many patients to compare perfor-mance of different plans and providers. In future,CHINs might also be a means for sharing access tomedical knowledge, remote diagnostic applica-tions, and expert advice based on outcome and ef-fectiveness analyses.32
The difference between a CHIN and a CHMISis primarily one of initial priorities. All of these
systems start with some initial features and ser-vices and add others as they grow. CHINs, for themost part, were developed to provide connectivityand transport of data among the users. Some ofthem are concentrating first on linking physiciansand clinics with hospitals and labs to access clini-cal data, and secondarily are providing claim fil-ing and other insurance-related services. SomeCHINs have a long-term goal of building a com-munity-wide data repository for outcomes re-search and for comparing the performance ofplans and providers, but they have not yet startedthat phase of their development. Other CHINshave no plans for building a centralized data re-pository, but envision that the standardizationthey provide will eventually allow authorized us-ers to transparently aggregate data across manydatabases, thus accomplishing the same purpose.
CHMISs, on the other hand, have started withthe concept of building a data repository for use inassessing the performance of health care providersand plans. Collection and analysis of managementinformation is a priority. Although there is varia-tion among the CHMISs started so far, most arefocusing on providing insurance transaction ser-vices (that is, connectivity and services linkingproviders and payers) and on capturing data fromthose transactions into the data repository. Ser-vices linking providers with providers to ex-change clinical data are also planned in ‘manycases.
Issues associated with CHINs include owner-ship and control, and network design and datamanagement.
■ Ownership and ControlThere are several possible ownership models forCHINs. One is a joint venture between a healthcare provider and an information system vendor.This is likely to be a for-profit organization, offer-ing community-wide service, with the goal of pro-viding easier communications among the various
32 D.L. Zimmerman, CHINs and CHMISs: Networks for Community Health Information and Management. Issue Brief No. 657 (Washing-
ton, DC: National Health Policy Forum, 1994).

Chapter 3 Networks for Health Information | 97
users. The vendor may first implement servicesfor the partner or lead sponsor and then attempt tocontract with other users based on demonstrationsof the usefulness of the service. An example ofthis ownership model is the Wisconsin Health In-formation Network (WHIN), developed by Auro-ra Health Care Corp. and Ameritech HealthConnections (a subsidiary of Ameritech, the re-gional telephone provider). Initially, WHIN pro-vided physicians with access to laboratory results,patient census data, and other information in thedatabases of the hospitals where they are affili-ated. In addition, the network now offers an elec-tronic claims service for filing claims andperforming some other insurance transactions.Besides the Aurora-owned hospitals, 11 otherhospitals and their affiliated physicians are nowon the system. One difficulty with this ownershipmodel is that the system may be viewed with somesuspicion by competing hospitals who may worrythat the provider that owns the system is giving it-self some advantage. Even in cases where a ven-dor is sole owner, late adopters may view thesystem as “belonging” to the early adopters. Thereare 45 to 50 communities with vendor-ownedCHINs.
An alternative model used by some CHINs is toform an understanding among a broad group ofpotential users before the system is built andcreate an ownership structure that will be viewedas more neutral by all participants. Although theirorganization varies, systems under developmentin Vermont, New York, Washington State, Chica-go, Cincinnati, and other locations have attemptedto develop a broad coalition of communitygroups—providers, payers, and employers—be-fore the network is built. These groups then jointlysponsor the creation of a not-for-profit organiza-tion to operate the system. This model also hasdifficulties. Developing community consensusabout the goals and operation of the system cantake a great deal of time, so systems opting for thismodel come to market much more slowly. Agree-
ments between stakeholder groups may becomefragile when it becomes necessary for participantsto actually commit money to the major project. Itis not yet clear who should make the biggest in-vestments in community networks because no oneknows who will accrue the most benefit fromthem.
Other ownership patterns, including variationsand hybrids of the above, ownership by a consor-tium of vendors, or ownership by a state or localgovernment agency, are possible, and are beingtried in some locations.33
❚ Network Design and Data ManagementCHINs vary widely in their approach to the func-tion of the network, the content of the informationcarried on it, and the standards to be used by or im-posed on participants. One basic decision facingall CHINs is whether or not the network willmaintain a central database of health information.Although creating a central repository is a funda-mental goal of some networks, others have active-ly rejected the idea and use the fact that eachparticipant maintains its own proprietary data as aselling point.
Technology decisions related to designing aCHIN are complex because their goal is to bringtogether a diverse set of information suppliers andusers who are operating incompatible systems.The network must establish “rules of the road” sothat participants can share information usefully.This means standardizing formats for data contentand structure and creating interfaces so that differ-ent computers and different people can use them.In the absence of clear national standards, differ-ent CHINs are developing their own ways of do-ing this.
Figure 3-3 outlines the high-level architectureof a CHIN. The network must interact with a vari-ety of different application systems in the partici-pants’ information systems. For the most part,network participants will not be willing or able to
33 Ibid.

98 I Bringing Health Care Online: The Role of Information Technologies
Admission, discharge,and transfer
Laboratory
CHIN
Radiology gateway
Pharmacy
Other
Hospital
<-- ‘ - -
Membership
--->CHIN Claims system
gateway
OtherL
Payer
(Optional)CHIN host system—
Switch functions Support functions
Help deskSession management Reporting
II
CommunityDatabase
Patient dataPayer dataProvider dataEmployer dataMedical costs
ICHIN user interface CHIN user/host interfaces CHIN host interfaces
Financial Medical journals
Physician’s office Clinic Medical information service
SOURCE: M R Gorsage and J W Hoben, “Technological Implications of CHINS, ” in R T Wakerly (ed.), Community Health Information Networks,Creating the Health Care Data Highway (Chicago, IL American Hospital Publishing, Inc.,1994), pp.115-140

Chapter 3 Networks for HeaIth Information 199
change their own operations substantially in orderto participate, so the network must develop inter-faces to diverse systems as well as gateways(sometimes called application interface gatewaysor translators) to convert messages from one stan-dard to another (e.g., from a proprietary system toHL7 or to a standard EDI format). The networkprovides a number of value-added services to par-ticipants, including switching functions like rout-ing (delivering data between trading partners),security (maintaining passwords and access con-trols; encryption), session management (e.g.,creating audit trails), and messaging (harmonizi-ng disparate e-mail systems and providing accessto external databases or networks). Generally thenetwork also provides support functions for userorganizations, including a help desk and billingand administrative information on system use.
User interface and point-of-service mecha-nisms, such as card readers and other devices, canprovide access to the network and initiate transac-tions. For example, scanning a patient’s identifi-cation card can initiate a verification of thepatient’s eligibility for benefits. For more in-formation on cards as access and identification de-vices, see box 3-4.
User interfaces can be customized to allow eachuser to see data in the form that is most convenientfor that user, as shown in figure 3-4. When a physi-cian’s office contacts different hospitals for pa-tient information, the user will see the informationin that office preferred format, despite the differ-ences in hospital information systems. Similarly,any data from the hospital that need to be down-loaded into the physician’s practice managementsystem are formatted to be acceptable to that sys-
Smart cards, magnetic stripe cards, and other small portable devices may offer a low-cost way to
store and transfer electronic health information. Cards can be used as identification and authorization
tools or as actual storage media. Cards currently play a role in the health care system, predominantly as
a means of patient identification and association with a particular health plan.
Types of cards include:■
in
■
●
Paper cards, usually with printed data and perhaps with a barcode or magnetic stripe; these are usu-
ally issued by health plans as a means of identification.
Magnetic stripe cards, such as those widely used in the financial industry (e.g., credit and automated
teller machine—ATM—cards). The magnetic stripe on the back can carry a limited amount of informa-
tion—226 characters in the case of a typical three-track card. They are typically used with online sys-
tems for accessing a database.
Smart cards have an integrated circuit chip with a range of capabilities. They can support securityfeatures such as encryption and differential access for different parts of the card. They can be used
to interact with online systems or to store varying amounts of data; the typical 24-kilobit card stores
one full page of text. A backup copy of stored data may be kept on a provider’s computer to protect
against loss.
Laser optical cards carry a wide stripe on the back that contains information that is “burned” into the
card with a laser. Once written, data cannot be modified, although new data can be added to some
types of laser optical cards. They can carry 2.5 megabytes of digital information (about 1,200 pages
of text). They typically do not have security features unless an integrated circuit chip is added to the
card for this purpose.
(continued)

100 I Bringing Health Care Online: The Role of Information Technologies
In the health care system, cards could be used to: streamline various administrative functions (e.g.,claims processing); automate functions that tend to be repetitive in nature (e.g., filling out medical histo-ry forms); and improve the quality of care by reducing the likelihood of duplicative testing or possibledrug interactions. Potential applications of card technology include:
■ Patient Identification, enrollment verification, and eligibility verification■ Emergency Information■ Payments and claim processing■ Prescriptions■ Medical history
Magnetic stripe cards have wide use in health care in the United States, perhaps because of thelarge installed base of cards and card readers already in use by the financial industry and the public’sfamiliarity with these cards. A number of U.S. health plans use plastic magnetic stripe cards, and atleast 22 states use them to identify people eligible for Medicaid benefits. The patient presents the cardwhen entering the hospital, provider’s office, or other location. When the card is scanned, Informationthat already exists about the patient can be linked with newly entered data in an automated fashion.Eligibility for service, the amount of the copayment, and other payment reformation can also be ob-tained quickly so that accounts can be settled before the patient leaves. Although magnetic stripecards carry only a small amount of information, they are useful as access devices to Iink with the pro-vider’s or payer’s online databases, and the U.S. telecommunications infrastructure is adequate to pro-vide these linkages in almost any location.
A number of health plans in the United States are testing the use of smart cards. Currently, stan-dards for the data format, encryption, and security features are only beginning to emerge. This meansthat cards are only being used within closed systems. The Department of Defense is conducting a mul-timedia (magnetic stripe, bar code, integrated circuit chip, and photograph) identification card pilotprogram, which wiII test the viability of deploying smart cards for multifunctional purposes with a prima-ry focus on health care. Canada, Great Britain, and Japan are also looking into smart cards for healthcare informatlon.
Smart cards are used more widely in Europe than in the United States, but even in Europe, their usein health care is primarily for identification and for limited amounts of clinical and administrate informa-tion. In Germany, smart cards generally contain only administrative information. In France, cards typi-cally contain some clinical information, but there is no attempt to store a complete medical record; rath-er, basic information is placed on the card and may be accessed by providers or pharmacies to reduceerrors or to speed data processing. The storage capacity of many cards currently in use is usually notsufficient to maintain a complete medical history, although higher capacity cards are becoming avail-able. Widespread use of portable electronic patient records in card form wiII depend on the availabilityof standardized patient record systems in the computers of all providers who will interact with and up-date the cards. Such systems are not currently available in Europe or the United States.
Laser optical cards are still an emerging technology and are not widely used. In one pilot project, theTexas Department of Human Resources has issued 2,500 cards containing demographic informationand Immunization records. Equipment to read the cards is available at only a few locations, but theproject is expected to expand. Experiments with laser optical health cards are also under way in Scot-land.
SOURCE: Adapted from Phoenix Planning and Evaluation, Ltd , “Potential Card Applications in the Health Care Industry, ” unpub-lished contractor report prepared for the Off Ice of Technology Assessment, January 1994

Chapter 3 Networks for Health Information 101
Ourtown General Hospitalinformation system
Ourtown General HospitalAdmission/discharge/transfer (ADT)
Name IDOption:1. Review2. Register3. Reports
PC in hospital department
General Hospital ADT
PC in physician’s office
Note Common user systems sign-on allows for a custom screen (regardless of application) for users according to their profiles
SOURCE Adapted from M R Gorsage and J W Hoben, “Technological Implications of CHINS, ” in R.T. Wakerly (ed.), Community Health InformationNetworks: Creating the Health Care Data Highway (Chicago, IL American Hospital Publishing, Inc., 1994), pp. 115-140
tern. The network system maintains a profile ofeach user and the way that information must bepresented. Similarly, data for claims filing or othertransactions can be entered by the physician’s of-fice in a single format, regardless of payer. Thenetwork, through the application integration gate-way function, can then take responsibility fortranslating or reformatting the information to suitthe requirements of each payer. This approachshould reduce a participant’s training costs be-cause employees only have to learn one set ofmenus and navigational tools.
While the user’s view of data appears inte-grated through the use of common user interfacemechanisms, actually integrating data across mul-
tiple databases is another problem entirely.CHINs that include a central data repository areaddressing this problem now. A repository is a“central database populated by transactions fromseveral disparate departmental and organizationalsystems.” 34 T h e r e p o s i t o r y c o n t a i n s c o p i e s o ftransaction data carried out by various tradingpartners; it is not the original or sole source of in-formation. Management of information from dis-parate sources can be a complex task:
To ensure data integrity, the [application in-tegration gateway] should have data audit andcontrol mechanisms to synchronize replicateddata with its various storage locations. The taskof determining which transaction system is the
34 M.R. Gorsage and J.W. Hoben, “Technological Implications of CHINs," in R. T. Wakerly (cd.), Community Health Information Net-
works: Creating the Health Care Data Highway (Chicago, IL: American Hospital Publishing, Inc., 1994), pp. 115-140.

102 | Bringing Health Care Online: The Role of Information Technologies
Note: Systems on the CHIN with their own repositories will require an intelligent gateway to match field names with data
SOURCE. M R. Gorsage and J.W. Hoben, “Technological Implications of CHINS, ” in R.T. Wakerly (ed.), Communi tyHealth Information Networks: Creating the Health Care Data Highway (Chicago, IL: American Hospital Publishing, Inc ,1994), pp. 115-140,
master or owner of specific data elements is dip-lomatic and political rather than technological.35
Through use of a common data model, the reposi-tory can be mapped onto the various systems ofrecord. Data for different entities can be tied to-gether by using unique identifiers for patients,payers, sites, providers, and other entities.
In time, a central repository containing bothclinical and administrative information could be-come too large to manage efficiently, especially ifit includes diagnostic images. An alternative ap-proach to managing community-wide informa-tion is to maintain an intelligent central repositorythat manages a federation of independent data-bases. All databases would share a common glob-
al model, and the central repository would containnot copies of the transactions, but information onwhere to find the information. This metatransac-tion (transactions about transactions) repositorywould then contact the individual databases tocollect information needed by an authorized user,and would have the knowledge needed for resolv-ing any differences between the databases. Thisconcept is illustrated in figure 3-5.
■ Community Networks and EnterpriseNetworks
There is uncertainty about the role of CHINs asmanaged care organizations and integrated deliv-ery systems (IDSS) begin to dominate health care
35 Ibid.

Chapter 3 Networks for Health Information | 103
delivery. CHIN development takes time and, inthe meantime, some IDSs may build their ownproprietary enterprise-wide networks. IDSs willcarry out most of their data communication on theirown enterprise networks because many of theiradministrative functions will be internal, and theymay not need to join a community-wide network.
There are two schools of thought on the pos-sible interactions of CHINs and IDS networks.One holds that IDSs have no need for CHINs, andthat CHINs are a short-term or limited phenome-non that will fade as markets become dominatedby two or three competing managed care organiza-tions. Because the IDSs are competitors, they willhave no incentive to share information, and thusconnectivity between them will not be needed.
The other school of thought says that IDSs needCHINs because even in a managed care environ-ment there will still be out-of-plan referrals, pro-viders with multiple affiliations, and mobility ofproviders and patients among plans. In order to betotally electronic in processing administrative in-formation, IDSs will need access to a community-wide or regional network infrastructure. Further,even though IDSs will want to keep private theirown data on outcomes, utilization, and costs, it islikely that large purchasers of health care (and per-haps regulatory agencies) will insist on seeing atleast some of this information on a community-wide basis, and CHINs will offer a mechanism.36
There is even the view that some IDSs will eventu-ally become CHINs, perhaps setting up subsid-iaries to offer CHIN services to their competitorsand unaffiliated providers in their communities.37
❚ Networking and Public HealthThe usefulness of community and regional net-works increases if they are also able to interactwith public health agencies at the local, state, orfederal levels. The Department of Health and Hu-
man Services has been tasked by the Administra-tion to act as the lead agency in coordinatingfederal government activities related to health in-formation systems.38 Among the long-term goalsto be pursued is the creation of a national forum forcollaboration on standards development forhealth information. Health information networks,automated payment systems, and other systemsare part of the national information infrastructure(NII) where public- and private-sector activitiesneed to be coordinated.
The Public Health Practice Program Office atthe Centers for Disease Control (CDC) is develop-ing an Information Network for Public Health Of-ficials (INPHO) that provides state and localpublic health officials with access to timely in-formation on disease prevention and healthpromotion, including: 1) local and national dis-ease and injury rates and associated risk factorsand prevention measures; 2) preventive healthdata, guidelines, regulations, training materials,and emergency notices; and 3) reports of epide-miological investigations. The system will initial-ly employ CDC’s personal computer software(WONDER) as well as voice and fax technolo-gies, but will eventually use Internet tools. It willprovide an electronic mail service for federal,state, and local public health officials, startingwith local area networks and building towardwide area networks. The INPHO system is beingpilot-tested in Georgia through a $5.2 milliongrant from the Robert W. Woodruff Foundation toEmory University in Atlanta, teamed with severalother academic and state government organiza-tions in Georgia.
COSTS AND COST-EFFECTIVENESS
❚ System CostsHigh system costs often pose a barrier for a busi-ness wanting to embrace EDI. Hardware, soft-
36 F. Bazzoli, “Will CHINs Be Able To Mesh with Enterprise Networks?” Health Data Management, March 1995, pp. 47-52.
37 R.T. Wakerly, “Models of CHIN Ownership,” in Wakerly, op cit., footnote 34, pp. 53-71.38 A. Gore, Vice President, Washington, DC, memorandum to D. Shalala, Secretary of Health and Human Services, Washington, DC, Mar. 8,
1995.

104 | Bringing Health Care Online: The Role of Information Technologies
ware, installation, and staff training are allexpensive. If an organization opts to work throughan electronic claims company or a VAN, it mustpay per-transaction charges. If it creates a directline to its trading partners, it will incur costs fornetwork setup and telecommunications equip-ment. Staff will be required to manage the system,adapt it to changing standards, and act as a liaisonwith new trading partners.
One estimate puts the total average, per-compa-ny EDI investment at between $200,000 and$700,000.39 The lower figure is for a suppliercompany, while the higher is for a large companyseeking to connect all its suppliers. For the healthcare industry, WEDI estimates implementationcosts at $7,500 to $15,000 for individual profes-sionals and $25,000 to $500,000 for institu-tions.40 Costs include hardware, software,consulting, and VAN charges. Most companies donot perform a break-even analysis, according tothe EDI Group, a firm that studies EDI use gener-ally. Those that do, however, report that they reachthe break-even point within two years.41
There are relatively weak near-term incentivesfor some users in the health care industry to as-sume the high initial costs of EDI. Although thereare promises of administrative savings, these willbe spread out among most sectors of the industry.Further, it is likely that savings will not be fullyrealized until all transactions are electronic. Abusiness that has some trading partners using EDIand some using paper has the expense of maintain-ing both systems. This is often the case in healthcare at this time.
❚ National Estimates of AdministrativeCost Savings
A number of key studies focus on national esti-mates of potential savings from using informationtechnology for health care administrative func-tions. These include studies by WEDI, the TiberGroup, Arthur D. Little, Inc. (ADL), HCFA, andLewin-VHI.42 The findings of these studies aresummarized in table 3-1. It is important to notethat comparisons across studies should be madewith caution: the definitions used for the variousadministrative transactions vary widely, as do themethodologies for estimating costs and savings.Still, it is instructive to examine the findings fromthese studies in clarifying possible savings frominformation technologies in health care.
The studies on national administrative savingsproject that information technology applicationscould save in the range of $5 billion to $36 billionper year in total health costs, which translates intoapproximately 0.5 to 3.6 percent of total nationalhealth spending. The Tiber Group study (whichwas commissioned as part of the WEDI Report)attempted to differentiate the savings per transac-tion for payers and for providers. It found that thegreatest savings for both would be in the areas ofclaims inquiry and claims submission—which arevery information-intensive. With the exception ofthe ADL report (which included some clinical aswell as administrative functions), the magnitudeof the projected annual savings was quite similaracross studies.
There is some reason to believe that these esti-mates may be overly optimistic. For example, ex-
39 D. M. Ferguson and D. J. Masson, “The State of EDI in the U.S. in 1993,” EDI Forum, vol. 6, No. 4, 1993, p. 10.40 R.L. Schaich, “Health Care Reform Costs and Benefits,” EDI World, vol. 3, No. 12, December 1993, p. 51.41 Ibid.42 WEDI estimates and Tiber Group estimates are reported in WEDI, op. cit., footnote 27; Arthur D. Little, Inc., Telecommunications: Can It
Help Solve America’s Health Care Problems? No. 91810-98 (Cambridge, MA: July 1992); U.S. Department of Health and Human Services,Health Care Financing Administration, White Paper on Financial Implications of Information Technology, 1991; Lewin-VHI, Reducing Ad-ministrative Costs in a Pluralistic Delivery System, report prepared for the Healthcare Financial Management Association, Apr. 30, 1993).

Study Application/function Claims Enrollment Payment & Eligibility Claims Totalsubmission remittance inquiry net savings
Workgroup for Electronic Data $45 to$13 1 billion $21 to $43 billion $1 1 to $1 3 billion $25 to $ 49 billion $28 to $ 40 billion $42 billionlnterchange (WEDI) annually
Key assumptions1
2
3
A comprehensive, standardized ElectronicData Interchange capability is establishedthroughout the health care system accordingto an aggressive Implementation scheduleover the next three years
Standard formats wiII be adhered to verysoon
Employer automation costs only reflect thecosts required to automate the transfer ofenrollment data for companies with over 50employees
4
5
6
annually annually annually annually (over SIX years)
For enrollment, 171,722 employers with more than 50 7. Implementation schedule assumes costs are amortizedemployees wiII save 0.5 to 1.0 FTE or $12,000 to over three years$24,000 per year, minus annual transaction costs of $78 - 30% implementation occurs in year 1($1.50 times 52 transactions) - 70% Implementation occurs in year 2
-100 % Implementation occurs in year 3For eligibility, there wiII be an elimination of nearly 6,000institutions to maintain enrollment or eligibility lists sup-plied by payers
For payment and remittance, on average, there are 15claims per remittance advice.
Sources: Previous WEDI findings, Health Care Financial Administration reports, A.D. Little report, Lewin-VHl report, proprietary data, and Tiber Group study, which was part of WEDI report
Tiber Group study
Key assumptions
1. Startup costs and fixed costs used in the 3study were assumed to be sufficient for100% EDI.
2. Surveys were completed by only 14 physi-cians, nine hospitals, and SIX payers There- 4fore, the data are assumed to be externallyvalid in order to project national savings
$064,$110
(savings per transaction for insurer, then hospital) (over 5 years)
Broad definitions for the applications (or transactions)were necessary due to definitional issues at many dem-onstration sites
Even though price competition in the computer industryis quite high, costs were held constant for the study
Source: Surveys at each of three demonstration sites.
Arthur D. Little $6 billionannually
$36 billion
Key assumptions annually
1. The $30 billion in savings not due to claims 3 Implementation costs are not included in the economic modelsubmission wiII come from electronic man-agement and transportation of patient in-formation, including the use of home healthterminals to reduce discussions with provid-ers; reduction in emergency room visits; ear-ly intervention: and Improved creation, trans-port, storage, and retrieval of computer-based patient records
2 Legal issues regarding liability wiII havebeen resolved
Sources: Data were gathered from available research and pilot studies when available, otherwise determined by panel of experts at Arthur D Little.
(continued)

Study Application/function Claims Enrollment Payment & Eligibility Claims Totalsubmission remittance inquiry net savings— — — — —
Health Care Financing Administration $58 billion $04 billion $24 billion $0.8 billion $0.1 billion $436 to $74 billionKey assumptions annually
1 For claims subbmission, payers and provld- 4ers wiII each save 50 cents per claim for anestimated three billion paper claims
52. For eligibility, assumed 75 million transac-
tions and savings of $140 per transaction.
3 For claims inquiry, assumed provider sav-ings would be one-half as much as payersavings estimated by WEDI
Source: WEDI report provided most of the information
annually annually
Administrative costs assumed to be growing at the rateof total health care expenditures
Each visit, test, or procedure performed by a provider IScounted as a separate “claim “
annually annually (over SIX years)
Lewin-VHl $1,9 to $4.5 billion $2.6 to $52 billionKey assumptions annually net in 1993
1 The entire medical bill (all tests and pro-cedures) is counted as one claim.
2. For claims submission, providers willsave $1 30 per claim and payers willsave 60 cents per claim
Sources: Cost estimates from Congressional Budget Office and General Accounting Office, industry sources, including The Medical Group Management Association; calculations by Lewin-VHI experts
o
SOURCE. Project HOPE Center for Health Affairs, Bethesda, MD, “Estimating the Cost-Effectiveness of Selected Information Technology Applications,” unpublished contrac-tor report prepared for the Office of Technology Assessment, U.S. Congress, Washington, DC, May 9, 1995.

Chapter 3 Networks for Health Information | 107
perts interviewed by OTA note that theassumption by both WEDI and the Tiber Groupthat EDI will be rapidly implemented by a highpercentage of providers and payers is unrealistic.However, the WEDI Report’s other assumptionson savings from specific administrative transac-tions, which were based on industry surveys andcase studies, seem to be more reasonable.43 Poten-tial savings noted in the ADL report also seemgenerous for a number of reasons. The report didnot include the costs of implementing new sys-tems, for example. The authors defended thisomission by pointing to the variability of pricing,and the fact that the cost of implementation wouldbe widely shared with other industry applications.Another problem was that some of the categoriesof cost savings were vague and the data used tosupport the claims were not always well justified.Finally, the results include some clinical applica-tions as well as administrative applications, socomparisons with other national estimates are dif-ficult to make.
The HCFA results, which relied heavily on theWEDI methodology, may also be optimistic forreasons noted above. In addition, the report wasnot explicit about how some of the calculationswere made. The Lewin-VHI report was also vagueabout some of the assumptions underlying theircalculations.
Despite limitations, however, it is interesting tonote that the studies taken together suggest that in-formation technology applications in health careadministration will produce important, but not in-ordinate, savings to the health care system. In lightof some claims made about the potential reductionin administrative costs that would arise from in-formation technology, the actual savings pro-jected appear rather modest. This generalprediction seemed to be shared by experts inter-viewed by OTA. They also emphasized that thefact that existing studies do not show large savingsdoes not diminish the potential importance oftechnology applications in increasing system effi-
ciencies (which may be difficult to capture in anevaluation) or in improving patient care.
❚ Savings from Reducing Errors andDetecting Fraud
Creating a health care bill or claim is a very com-plex process, and there are many opportunities forunintentional error or deliberate fraud. An impor-tant part of developing the bill is to describe theprocedures performed for the patient. This in-formation must be transferred from the patient re-cord to the administrative system and, ultimately,into the bill or claim. Many payers, includingHCFA, use one of several diagnostic and proce-dural coding languages, such as ICD-9-CM, as thebasis of their payment formula. Many providerstry to capture coding information as close to thesource as possible, for example, by listing thecode along with the procedure name on paperforms physicians use for ordering tests and proce-dures, or by having a computer-based system au-tomatically record the code whenever a procedureis ordered by name. When diagnoses and proce-dures are not captured in coded form (e.g., if theyare written in free-hand notes), then trained codersmust read through the record to find informationto be put in the bill.
The coding systems are far from perfect. Deci-sions about which code to use are not always clearand can be the subject of negotiation betweenpayer and provider while a complex claim is adju-dicated. Misreading, miskeying, and other mis-takes can cause bills to have incorrect codes. Inaddition, some providers deliberately engage infraudulent practices such as upcoding (describingthe procedure performed with the code for a morecomplex one) and unbundling (billing for two ormore procedures when a single comprehensivecode exists that describes the procedure per-formed) in an attempt to get a higher level of com-pensation from the payer.
A number of software products have been de-veloped to check claims for inconsistent, erro-
43 Project HOPE Center for Health Affairs, op. cit., footnote 2.

108 | Bringing Health Care Online: The Role of Information Technologies
neous, or suspicious coding. Some payers havetheir own proprietary systems to check claims be-fore paying.44 In addition, a number of commer-cial products are available for payers, providers,or other firms that prepare claims on a provider’sbehalf. Detecting obvious errors in bills saves pro-viders the trouble and expense of submittingclaims that will be rejected; such software issometimes available in practice management sys-tems and other administrative software for provid-ers.
A recent study by the General Accounting Of-fice (GAO) tested several commercial fraud-de-tecting software packages on samples of Medicareclaims and found them very effective in detectingerrors and flagging possible fraud. GAO sug-gested that use of such software could have savedHCFA about $603 million in 1993 and $640 mil-lion in 1994. These savings, amounting to about1.8 percent of Medicare reimbursements for sup-plies and services, are in line with the savings re-ported by private insurers using the samesoftware. GAO also notes that Medicare benefi-ciaries would have saved money as well—$134million in 1993 and $142 million in 1994.45
❚ Economic Justification of CHINsNo one has demonstrated whether of not CHINsare cost-effective. Those that exist have only beenin operation for a few years and their data have notbeen publicly analyzed. However, the large in-vestments made by vendors suggest that their ownproprietary estimates show a profitable future forCHINs. On the other hand, a number of vendorshave dropped out of this market already. In addi-tion to the large investments involved, many ofthem have perceived the possibility, or experi-
enced the reality, of failing to develop communityconsensus about the role of the CHIN and servicesthat need to be provided. Even if a project is initi-ated by a vendor rather than a coalition of commu-nity groups, it is necessary to have the interest andcommitment of a minimum number of potentialcustomers from the relevant user groups; other-wise the project is too risky.46
The investment required to build a communitynetwork is large. Estimates for WHIN suggest thatthe partners invested $4 million to $6 million inhardware, software, sales, and operations teamsbefore recouping any costs. Costs for WHIN sub-scribers depend on their size and the level of ser-vice they desire. A hospital might make aone-time investment of $50,000 to $125,000 (de-pending on its current level of automation, thenumber of custom interfaces that must be built,etc.). Ongoing costs are determined by an algo-rithm that includes the number of physicians onstaff, number of beds, and annual patient visits.Other ongoing costs include a per-transaction costfor insurance transactions. Physicians’ offices paya $450 installation and training fee, an ongoingcharge of $30 per physician per month, and a per-transaction charge for insurance services.47
Projected savings from participating in WHINcould be $750,000 to $1.5 million per year for a300-bed hospital. The actual savings might de-pend on how effectively the hospital was using in-formation technology and EDI before joining thecommunity network. Before implementing theWHIN, the Aurora Health Care Corp. operated aproprietary network for communicating with phy-sician offices. That system had required a $1 mil-lion initial investment and operating costs of$250,000 to $350,000 per year. Aurora estimates
44 J. Newall and B. Colbert, “Using Automated Bundling, Unbundling, and Rebundling Processes Before Paying Claims,” in Health In-
formation Networks, proceedings of a conference sponsored by the Health Care and Insurance Institute, Sept. 28-29, 1993, Philadelphia, PA.
45 U.S. Congress, General Accounting Office, Medicare Claims: Commercial Technology Could Save Billions Lost to Billing Abuse, GAO/
IMD-95-135 (Washington, DC: May 1995).
46 J. Sanders, remarks at CHINs and CHMISs: Networks for Community Health Information and Management, meeting of the National
Health Policy Forum, Washington, DC, Oct. 25, 1994.
47 M. Radaj, Vice President, Operations, Wisconsin Health Information Network, personal communication, July 8, 1994.

Chapter 3 Networks for Health Information | 109
that participation in WHIN will provide greaterfunctionality for half that cost per year. Annualsavings for physicians’ practices might be in the$2,500 to $5,000 range.48 WHIN is currentlyworking with the University of Wisconsin to con-duct a cost-effectiveness study.
Cost savings to participants could accrue froma CHIN’s ability to: 1) link participants; 2) delivermanagement information at the point of service;and 3) standardize electronic transactions. Link-ing participants electronically can reduce the needfor telephone calls, travel, postage, and use of de-livery services. For example, enabling physiciansto check test results, sign attestations, or viewimages online presumably saves professionaltime by eliminating some trips to the hospital. Re-ducing phone calls can be difficult to quantify as acost savings, but many office administrators havecited it as an immediate and welcome benefit ofonline systems.
Delivering management information at thepoint of service can facilitate the process of regis-tering patients, checking their eligibility, and giv-ing them care. Having management informationavailable before treatment begins can reduce thenumber of rejected claims and other costs of work-ing without complete information. In addition,user software at the provider’s location can checkthe accuracy of entered data (e.g., in claim filing)and put data into a format preferred by the payer—all before it leaves the provider’s premises. Thiscould reduce personnel and staff training costs forboth providers and payers, and reduce the costs ofcorrecting rejected claims for both providers andpayers. Of course, services like these do not neces-sarily have to be delivered over a community-wide network. A large number of insuranceclearinghouses and other electronic medicalclaims services offer these services directly to pro-viders. The possible advantage of a CHIN is to
combine both clinical and insurance informationprocessing in a single system
Community networks offer providers of allsizes the opportunity to move toward more uni-form, standardized electronic communicationwithout having the immediate need to changetheir existing systems. More information can becaptured automatically and used in additionalways, which should reduce costs to participants.Use of common interfaces and elimination orstandardization of some key entry tasks (such asfiling insurance claims) could also reduce person-nel and training costs.
POLICY IMPLICATIONS OF ELECTRONICHEALTH INFORMATIONAmong the issues affecting the health care indus-try’s adoption of information technology are: 1)industry fragmentation; 2) complexity of in-formation needs; 3) standards; 4) standard identi-fiers; 5) an inconsistent legislative and policyenvironment; and 6) privacy, confidentiality, andsecurity concerns.
❚ Industry Fragmentation49
The industries that have implemented electroniccommerce most completely have been led by asingle industry group devoted to implementingdata standards. Examples include the Transporta-tion Data Coordinating Committee that devel-oped EDI standards for the transportation industryin the mid-1970s or the banking industry’s Na-tional Automated Clearinghouse Association.The health care industry has no single focus forEDI activities. WEDI believes that implementa-tion has been hampered as a result and will notproceed quickly unless a central entity is formedto coordinate implementation and education.50
An even more critical factor, however, is thefragmented nature of the health care industry in
48 Ibid.49 This section is based on Canright, op. cit., footnote 9.50 Workgroup for Electronic Data Interchange, op. cit., footnote 27, p. 1-9.

110 | Bringing Health Care Online: The Role of Information Technologies
general. In most industries where EDI has beensuccessful (e.g., utilities, banking, transportation,and auto manufacturing), a few large organiza-tions—called hubs in the language of electroniccommerce—made EDI an explicit requirementfor continuing a business relationship. Thus, forthe smaller spoke companies, the decision was notwhether to adopt EDI, but how quickly. Onehealth care EDI consultant describes health care inthe United States as a $900 billion “cottage indus-try.”51 There are over 1.2 million health care pro-viders, ranging from single practitioners to1,000-bed hospitals and more than 3,000 privatepayers. The effective number of different providerorganizations may decline somewhat with the cur-rent trend toward hospital mergers, the purchaseof clinics and medical practices by integrated de-livery systems, and the continuing affiliation ofphysicians into independent practice associationsand other arrangements. But the structure of thehealth care industry is unlikely to approach the rel-ative simplicity of banking or air transportation.In health care, the industry hubs are providers, andmost providers are small organizations withoutthe time, finances, or staff resources to prepare im-plementation guidelines, set standards, and im-plement systems. They must rely on the guidanceof vendors that provide software, claims process-ing, and networking services.
HCFA has been the successful organization inmoving the health care industry toward EDI be-cause of its financial reach. For many health careorganizations, it was HCFA’s development of theMedicare Transaction System (MTS) and its in-centives to submit Medicare claims electronicallythat prompted initial interest in EDI. These incen-tives have included: 1) faster payment for cleanclaims (14 days for electronic, 27 for paper); 2)electronic funds transfer; and 3) free or at-costbilling software. Private sector payers are unlikelyto offer many of these incentives to providers. For
example, payers have an incentive to delay pay-ment as long as possible in order to maximize theirown use of the funds; they would be unlikely to of-fer providers quick payment as an incentive to be-gin an EDI relationship unless it could be clearlydemonstrated that EDI reduces their own costs(not the provider’s costs or the costs of the systemas a whole) enough to offset this advantage. How-ever, because many providers and payers are be-ginning to use EDI to deal with HCFA, theinfrastructure is being created that they can alsouse to deal with one another.
❚ Complexity of Information NeedsIn banking and financial services, most electronictransactions are simple and highly standardized.Consumers and businesses benefit from the easeof using the automated teller machines and creditcard transactions made possible by that standard-ization. Health care payment requires a number ofdifferent types of transactions, and often largeamounts of data have to be exchanged. In addi-tion, the procedures, information needs, paymentarrangements, and authorization procedures foreach type of transaction can vary, depending onthe characteristics of the payer, patient, patient’semployer, and sometimes the diagnosis or proce-dure involved.52 This complexity has slowed thediffusion of electronic commerce into the healthcare arena.
❚ StandardsThe key to the functionality and growth of elec-tronic medical payment lies in the establishmentof standards. As discussed in chapter 2, standards-setting and acceptance are moving slowly. Currentestimates put the number of proprietary claimsformats in use at 400—too many even for softwareto translate between sender and receiver.
51 J. J. Moynihan, “More Payers Should Convert to EDI,” Healthcare Financial Management, vol. 48, No. 5, May 1994, p. 66.52 Faulkner and Gray Health Information Center, Health Care and the Electronic Superhighway: A Provider Perspective on Electronic Data
Interchange and Automated Medical Payment (Washington, DC: Faulkner & Gray, 1992), p. 21.

Chapter 3 Networks for Health Information | 111
The standards-setting process is voluntary andcompliance with the standards will be voluntaryas well. Yet administrative savings may not actu-ally be realized unless standards are more strin-gent and compliance with them is nearlyuniversal. As mentioned earlier, there are nearly50 different implementations of the standardUB-92 form, requiring providers and payers withinterstate business to use several versions of it. Astandard claim form will not truly be standard, forexample, as long as each payer can demand addi-tional documentation to accompany it. Whilepayers usually request additional information inan effort to reduce their own costs, the difficultyand expense of maintaining different forms pres-umably raises costs for the industry as a whole.
❚ Standard Identifiers for Individuals,Providers, and Payers
Interstate electronic commerce for health in-formation would be facilitated by a system ofstandard identifiers. Because each provider orprovider group (as well as payers and other usersof health information) maintains its own identifi-cation number scheme and assigns its own num-bers, patient records are not uniquely identifiedonce they leave the institutions where they havebeen created. This can create confusion in themulti-institutional sharing of clinical or adminis-trative information. Unique identification can beaccomplished by combining several differentidentifiers—for example, a file number, plusmiddle initial, plus address—but it is generallyagreed that a system of standard identifiers wouldbe more stable over time.
Some argue that the benefits of fully electronicrecords are more easily obtained if each individualcould be uniquely identified. If each person had auniversal patient identifier it would be easier tolink the health information maintained at differentinstitutions, for example. In addition to identify-
ing patients, health care providers and specificsites of care also need to be identified. While thereare a number of recommendations for developingnumbering schemes de novo, some industry orga-nizations recommend modifying or expanding ex-isting identification number schemes in order toget unique identifiers in place more quickly.53
Universal identifiers are common in some Eu-ropean countries where they are assigned topeople at birth. The United States has been slow toadopt a universal numbering system and manygroups have actively opposed such a system basedon privacy concerns.
The Social Security Number (SSN), or anothernumber based on it, has been recommended foruse as the universal patient identifier. Because thisnumbering system is already in place, somegroups argue that it would be the fastest and leastcostly method of instituting a universal number-ing system.54 The ubiquity and convenience of theSSN make it a tempting candidate for a universalhealth identifier.
However, privacy advocates have opposed theuse of the SSN as a health identifier precisely be-cause it has had so many other uses. The SSN isthe key to a lot of nonhealth-related informationabout a person—including financial, tax, credit,educational, and other information on file withgovernment agencies and private firms. It is veryeasy, with access to the SSN, to quickly developdetailed dossiers on anyone. In addition, some in-dividuals, primarily infants and noncitizens, donot have SSNs. Some people have multiple SSNs.The system has been in operation for 60 years, andthere is a long history of invalid and fraudulentlyacquired numbers. Because the form of the SSNdates from the precomputer era, it also lacks acheck digit (an extra digit added to a computer-based number that aids in error detection andcorrection).
53 For example, see American Medical Informatics Association, “Position Paper on Standards for Medical Identifiers, Codes and Messages
Needed To Create an Efficient Computer-Stored Medical Record” (Bethesda, MD: Apr. 20, 1993).
54 Ibid., p. 2.

112 | Bringing Health Care Online: The Role of Information Technologies
It can be argued that many of the privacy-basedobjections to the SSN—fraudulent numbers, link-ages to other databases, and so on—will also ap-ply to any new numbering scheme that could beadopted. While there is merit in this argument,there is also the possibility that a new numberingsystem would be safer because, for example, itwould have legal protections from the outset toprevent its use for other purposes.
Alternative schemes for developing uniqueidentifiers have been proposed. Some would in-clude segments of the patient’s name, latitude andlongitude coordinates of the place of birth, date ofbirth, and perhaps parts of the SSN. Some systemsalso involve encrypting the number, or convertingit to an alphanumeric identifier, in order to eitherprotect privacy or to make the number shorter andeasier to remember.55
One system that is now being put into place toidentify providers is the National Provider Identi-fier (NPI), which will be implemented by HCFAin 1996. In its present form, the NPI system is notuniversal—it will apply only to Medicare partici-pants. It will provide unique identification num-bers for physicians, other providers, and the siteswhere they provide care. In developing the NPIsystem, HCFA worked with a number of federal,state, and private-sector organizations. The NPIwill consist of a seven-character alphanumericidentifier with a one-character check digit. NPInumbers can be encrypted to protect privacy andconfidentiality.
By design, there will be no intelligence im-bedded in the NPI number; that is, analysis of thenumber itself will not yield useful informationabout the provider it identifies. Rather, the num-ber points to a location in a database called the Na-tional Provider File that will contain descriptivedata about the provider. Thus, numbers will nothave to be reissued when provider characteristics(address, number of locations, or types of special-ty) change. The numbering format has the poten-
tial to provide 10 million all-numeric identifiersor up to 27 billion alphanumeric identifiers, mak-ing it sufficiently large to serve as a national sys-tem for identifying all providers, includingnonparticipants in Medicare. Should such a na-tional system be desired, authorizing legislationwould be needed to allow HCFA to open the sys-tem.
HCFA is also in the process of developing aregistry and identifier system for payers. This sys-tem would identify and maintain information onthe payers who offer secondary coverage forMedicare participants. The process of coordinat-ing benefits is complex for Medicare as it is in theprivate sector. A primary payer, such as Medicare,is often not aware that a patient has secondary cov-erage, or may not have complete information onthe benefits for which the patient is eligible andthe rules for calculating reimbursement. Withoutthis information, the primary payer can some-times pay inappropriately (that is, pay more thanthe patient is entitled to). In addition, the processof filing a claim with the secondary payer is com-plex; the provider or patient must often file a sepa-rate claim based on remittance informationprovided by the primary payer. By incorporating aregistry of secondary payers and a complete set ofrules for coordination of benefits into its MedicareTransaction System, HCFA hopes to be able tomore accurately calculate reimbursement basedon all the benefits available to a patient. At thesame time, it could automatically send a bill to thesecondary payer, simplifying the claim processfor patients and providers.
❚ Inconsistent Regulatory Environmentfor Health Information
State government regulations concerning elec-tronic health information and patient records, aswell as privacy, vary widely. This creates a diffi-cult environment in which to implement standard-
55 For example, see P.C. Carpenter et al., “The Universal Patient Identifier: A Discussion and Proposal,” Patient Centered Computing: 17th
Annual Symposium on Computer Applications in Medical Care (New York, NY: McGraw Hill, Inc., 1993).

Chapter 3 Networks for Health Information | 113
ized processes. There are four areas in which statelegislation and regulation impact on electronichealth information. They include laws on: 1) stor-age media for medical records; 2) use of electronicsignatures; 3) privacy and confidentiality ofhealth information; and 4) patient access to healthrecords.
Storage Media for Medical RecordsState governments generally have licensing au-thority over health care providers and requirethem to maintain medical records. Nearly everystate regulates what media are permissible forstoring medical records. In many states, the lan-guage is reasonably “technology neutral” and theuse of catchall phrases such as “other useableforms” or “other appropriate processes” has beentaken to mean that computerized record storage ispermitted. In some states, however, legislationhas served as a barrier to the development of auto-mated patient records by specifying the permittedmedia (e.g., microfilm or paper) and excludingdisks, tapes, and other computerized storage me-dia. Other states require clinicians’ signatures inink on particular forms, implying a paper originalto which the signature can be affixed. Some statesspecifically permit the use of computers for somefunctions but forbid it for others, thus hinderingthe development of a complete computer-basedrecord. There are other paradoxes and inconsisten-cies in legislation as well, with some states per-mitting electronic signatures for some purposesbut requiring retention of a paper or microfilmedrecord.56
Only a few states specifically authorize com-puterized medical records. Indiana statutes, forexample, authorize the use of “computerized re-cords that maintain confidentiality.” They specifi-cally state that the recording of hospital medicalrecords by the data-processing system is “an origi-nal written record” and authorize the courts to
treat information retrieved from such systems asoriginals for purposes of admissibility into evi-dence.57
Some of the states whose statutes posed barri-ers to electronic patient records are making prog-ress toward changing the statutes. For example,North Dakota is considering legislation thatwould make the recording of a medical record on acomputerized system the equivalent of aphotographic process, thus making printouts andother items retrieved from the system admissiblein court.
Recordkeeping rules for nonhospital provid-ers—nursing homes and physicians’ offices, forexample—are often covered by different statestatutes or regulations and can be very differentfrom those that apply to hospitals in the samestate. Implementing a complete electronic patientrecord in a multisite provider organization, thatmight include hospitals and nursing homes, can becomplicated if these requirements differ widely.
The absence of state legislative or regulatorysupport for electronic patient records does notnecessarily mean that providers in that state areforgoing development of information systems orelectronic record systems. It does mean, however,that the providers face certain legal risks if they donot maintain the paper record system as well, andthey must bear the costs of operating both sys-tems. Currently, most providers are not techno-logically capable of creating a “complete”electronic record in any case. They maintain amixed paper and electronic system for practical,as well as regulatory, reasons. The regulatory in-consistencies among states can create difficultiesfor health care organizations that are attempting todevelop common patient record systems for sitesin more than one state.
Federal legislation governing business records(which includes medical records) implies thatcomputerized records are permitted (once again
56 J. P. Tomes, Compliance Guide to Electronic Health Records” (New York, NY: Faulkner and Gray, 1994), pp. 14-19.57 Burns Ind. Code Ann. sec. 34-3-15.5-2.

114 | Bringing Health Care Online: The Role of Information Technologies
using language about “other processes”).58 In ad-dition, HCFA, which administers the Medicareprogram, authorizes the use of computerized med-ical records if they are maintained in a form thatcan be reproduced legally, and if the system meetsMedicare’s conditions for participation. Theseconditions basically state that the system mustprotect the security of the records and ensure thatonly the authorized persons are able to sign them.The Department of Health and Human Services,in an effort to encourage the development of com-puterized patient records, had legislationintroduced in the 103d Congress to require pro-viders to maintain outpatient data in electronicform as a condition of participation in Medicare.59
Electronic SignaturesSignatures are necessary to attest to the complete-ness and authenticity of a medical record. Gener-ally, each entry in a record is signed orauthenticated by the person responsible for thatentry. An electronic record can be signed electron-ically, and this is permitted in many states; onceagain, however, electronic signatures are treateddifferently from state to state. Some states are si-lent about the specific means or technology to beused for the signature, or they say that industryand professional standards should dictate the formof the signature. This would seem to permit theuse of electronic signatures in those states becausethe Joint Commission on Accreditation of Health-care Organizations, American Hospital Associa-tion, and other industry groups have publishedguidelines related to electronic signatures. Somestates (like Pennsylvania, Alaska, and California)specifically authorize the use of an electronic sig-nature activated by a computer key that is knownonly to the authorized user.
HCFA accepts electronic signatures on admis-sion data sheets, attestations, and other documentsused to reimburse providers treating Medicare pa-tients. Providers must demonstrate that their com-puter systems meet HCFA guidelines.
Privacy and Confidentiality of HealthInformationBoth federal and state legislation cover the priva-cy of patient records. Records held by the federalgovernment are protected under the PrivacyAct,60 which governs federal disclosure of confi-dential information. At the state level there is a va-riety of approaches to privacy protection, and anumber of states have privacy laws that covermedical information. Other states have sections intheir Medical Practice Acts that prohibit physi-cians from revealing information obtained in con-fidence from a patient during treatment. TheAmerican Medical Association has publishedstandards for hospitals to protect the privacy of pa-tient information. Some courts have enforcedthese standards under state contract law as impliedconditions of the contractual relationship betweenphysicians and patients.
Even among the states that have well-definedlaws on the privacy of medical records, few ad-dress the flow of information to secondary users,such as insurance payers, researchers, and soforth. Further, because states are so inconsistentin how they deal with electronic informationgenerally, few of them confront issues directly re-lated to protecting privacy in computerized patientrecords. For a more detailed discussion, see theprevious OTA report, Protecting Privacy in Com-puterized Medical Information.61
58 28 U.S.C. 1732.59 Tomes, op. cit., footnote 56, p. 14.
60 5 U.S.C. sec. 552a.61 U.S. Congress, Office of Technology Assessment, Protecting Privacy in Computerized Medical Information, OTA-TCT-576 (Washing-
ton, DC: U.S. Government Printing Office, September 1993), pp. 41-45.

Chapter 3 Networks for Health Information | 115
Patient Access to Health RecordsBecause patients have a property right in their re-cords, it seems reasonable that they should be ableto inspect or copy them. Access to medical recordsheld by the federal government (e.g., Departmentof Veterans Affairs or other hospitals operated bythe federal government) is governed by the Priva-cy Act. The Privacy Act requires agencies to es-tablish procedures under which individuals canview or receive copies of their own records. It alsoauthorizes the establishment of special proceduresfor handling information that might, in the judg-ment of the agency, have an adverse effect on theindividual. These procedures have generally in-volved designating a third party to examine therecords and releasing them to a physician desig-nated by the patient.62
For private sector hospitals and other provid-ers, state laws and regulations govern patient ac-cess to medical records. Thirty-seven states havestatutory provisions for allowing a patient to re-view and/or copy his or her medical records. In afew additional states, the patient’s right to accessis not specifically stated, but can be inferred fromother language.63 In addition, some courts haveruled that providers have a common-law duty toallow a patient to access his or her records, absentlegislation.64 In 22 states, the patient may becharged reasonable copying fees, and 19 requirethat the patient apply for the records in writing.Twelve states permit physicians to deny patientaccess to a record if something in the record wouldhave an adverse affect on the patient; in most of
these cases, however, the record must be releasedto an attorney, physician, or other representativedesignated by the patient.65
A patient’s right of access to informationderived from the medical record, but housed in thedatabase of an insurer or other third party, is un-clear in many states. Only 14 states have legisla-tion giving patients access to insurance databasesand limiting redisclosure of medical informationheld by nonproviders.66
❚ Privacy, Confidentiality, and Security ofHealth Information
Privacy, confidentiality, and security of electronicdata are areas of great concern because of the sen-sitivity of health information. Privacy is essential-ly the right of an individual to limit access toinformation regarding that individual. Confiden-tiality is a form of informational privacy charac-terized by a special relationship between people,such as the relationship between doctor and pa-tient. Security refers to technical and organiza-tional procedures that protect electronicinformation and data-processing systems fromunauthorized access, modification, destruction, ormisuse.67
The appropriate levels of privacy, confidential-ity, and security, as well as the techniques forachieving them, may vary depending on the insti-tutional context and the use of the information.Tradeoffs are often necessary. For example, with-in a single hospital, confidentiality might be bestserved by allowing a patient’s record to be seen
62 U.S. Congress, Congressional Research Service, Access to Medical Records Under Federal Law, No. 93-708A (Washington, DC: Aug. 3,
1993), p. 16.
63 U.S. Congress, Congressional Research Service, Patient Access to Medical Records: A Statutory Survey of the United States, No.92-896A (Washington, DC: Nov. 17, 1992), and Medical Records: State Laws and Regulations Regarding Ownership and Patient Access, No.93-519A (Washington, DC: May 20, 1993).
64 R. S. Dick and E.B. Steen (eds.), The Computer-Based Patient Record: An Essential Technology for Health Care (Washington, DC: Na-
tional Academy Press, 1991), p. 166.
65 U.S., Congressional Research Service, Patient Access, op. cit., footnote 63.
66 Dick and Steen, op. cit., footnote 64.67 L. O. Gostin et al., “Privacy and Security of Personal Information in a New Health Care System,” The Journal of the American Medical
Association, vol. 270, No. 20, Nov. 24, 1993, p. 2487.

116 | Bringing Health Care Online: The Role of Information Technologies
only by the attending physician and the nurse as-signed to that patient. However, such a policywould affect the quality of patient care—it wouldunduly inconvenience and slow the work of sub-stitute nurses, consulting physicians, intensivecare personnel, or other caregivers who mightneed the record on short notice. Thus, a balancebetween confidentiality and convenience must befound. Most hospitals allow fairly broad access topatient records by authorized caregivers, and theyusually have security systems to keep track ofeach access. In some cases, this feature is used reg-ularly to keep caregivers aware that they are ac-countable for their use of the information system.At one hospital, for example, users are regularlynotified on-screen that each instance of access to apatient record is automatically recorded and thatpatients have the right to see a list of those wholooked at their records.68
When information moves out of the single pro-vider institution, priorities may change. The EDIindustry has focused most of its concern on the se-curity of information. Companies engaged intransmitting business information electronical-ly—financial institutions in particular—haveadopted technical solutions to two problems. Thefirst is that information transmitted over phonelines might be read by unauthorized persons. Onetechnique for addressing this is encryption. A sec-ond problem is that people sending or receivinginformation may not, in fact, be who they say theyare. Authentication techniques—the use of pass-words, keys, and other automated identifiers—areused to verify the identity of the person sending orreceiving information.69
Thus far, the EDI industry has a good securityrecord, according to the Workgroup on ElectronicData Interchange (WEDI), which says “there havebeen no reported incidents of the confidentialityof EDI messages being compromised.”70 Indeed,the risk of data leakage to outside computer hack-ers can be minimized in an online system. Securi-ty measures such as encryption procedures,password access, and audit logs help to discouragedata theft. With electronic information, systemadministrators have more numerous and powerfultools for monitoring and protecting informationthan they do with paper-based records.71
Privacy and confidentiality—the main focus ofconcern for the health care industry—are provingmore difficult to protect. As health care informa-tion increasingly moves over electronic networks,it becomes accessible to more people at widelyscattered institutions with different policies andprocedures in place. The potential for abuse in-creases accordingly. Unauthorized uses of in-formation by authorized users can be a majorproblem that is difficult to stop by technologicalmeans. Because of a plethora of conflicting statelaws regarding confidentiality, it is difficult to es-tablish legally defensible policies on proper ac-cess to records; people handling records oftenhave no clear guidelines for acceptable release ofinformation. A 1993 OTA report on privacy andconfidentiality of health information notes:
The present system of protection for healthcare information offers a patchwork of codes;State laws of varying scope; and Federal lawsapplicable to only limited kinds of information,or information maintained specifically by the
68 C. Safran et al., “Protection of Confidentiality in the Computer-Based Patient Record,” M.D. Computing, vol. 12, No. 3, 1995.69 For further information on network security issues and technologies, see U.S. Congress, Office of Technology Assessment, Information
Security and Privacy in Network Environments, OTA-TCT-606 (Washington, DC: U.S. Government Printing Office, September 1994) and Is-sue Update On Information Security and Privacy in Network Environments, OTA-BP-TCT-147 (Washington, DC: Government Printing Office,June 1995).
70 Quoted in Benjamin Wright, “Health Care and Privacy Law in Electronic Commerce,” Health Care Financial Management, vol. 48, No.
1, January 1994.
71 Ibid.

Chapter 3 Networks for Health Information | 117
Federal Government. The present legal schemedoes not provide consistent, comprehensiveprotection for privacy in health care informa-tion, whether it exists in a paper or computerizedenvironment.72
The situation has not changed appreciably sincethis report was published.
Without uniform privacy and confidentialitylaws, it is extremely difficult to expedite the de-velopment of interstate health records transfer.Accordingly, WEDI called on Congress to ensurethe uniform, confidential treatment of identifiableinformation in electronic environments. As elec-tronic interstate transfer of medical data increases,policies concerning the access to medical in-formation by secondary users of medical data, theuse of medical data for nontreatment purposes,and the redress of privacy violations must be madeconsistent in all state. Privacy legislation shouldalso address the requirements for informed con-sent of patients. Patients are often unaware of howtheir medical information will be used, to whom itmay be released, and what rights they may have toaccess or correct it once it is in the hands of a sec-ondary user.
Whether information is stored in a computer oron a piece of paper, the public fears the abuse ofmedical information by both authorized and unau-thorized parties. In a 1993 health privacy poll, 80percent of all respondents believed that consum-ers had lost all control over the circulation and useof health care information.73 These concerns canlead (and have led) to physicians withholding in-formation from patient records at the patient’s re-quest in order to protect his or her privacy.74 Tocreate an inaccurate or incomplete patient record,even with beneficial intent, could ultimately haveserious effects on the patient; in addition, such ac-
tions render records less useful for outcomes re-search and other statistical purposes.
Improved patient education about privacyrights may decrease the lack of control patientsfeel over the spread of medical information. Untilnational, uniform privacy legislation is enacted,WEDI suggests steps to protect privacy in its 1992report.75 Providers should:
� ensure that the patient has authorized release ofhealth information to an insurer by signing therelease contained on the insurance form,
� ensure that they release information in strictcompliance with the written release,
� ensure that they have complied with any rele-vant laws governing disclosure to insurers,
� establish security policies for employees whohave access to and process patient health in-formation, and
� establish security protocols for computer sys-tems used to process claims.
The WEDI guidelines were not intended to re-place the need for federal legislation or to absolvesystem operators from responsibility to designand maintain secure computing environments.
Although solutions to the networking problemsof privacy, confidentiality, and security remainunclear, the questions they embody do not: Whatpotential benefits of increased access to healthcare information will materialize, and will theyoutweigh the reduction in individual privacy thatincreased access to information inevitably brings?These questions must receive considered answers.“Opportunities for using electronic networks maybe lost if there is serious mistrust of their safety.”76
The concept of fair information practices setforth in the federal Privacy Act is fundamental to anumber of existing privacy laws and proposed ini-
72 Office of Technology Assessment, op. cit., footnote 60, p. 13.
73 Gostin et al., op. cit., footnote 67.74 Office of Technology Assessment, op. cit., footnote 60, p. 6.75 Workgroup for Electronic Data Interchange, 1992 Report (Hartford, CT, and Chicago, IL: September 1992).76 Gostin et al., op. cit., footnote 67.

118 | Bringing Health Care Online: The Role of Information Technologies
tiatives to protect medical information. Commoncharacteristics are:
1. Records pertain to medical information on in-dividuals.
2. Individuals are given the right to access muchof the personal information kept on them.
3. Limits are placed on the disclosure of certainpersonal information to third parties.
4. Health care personnel are required to requestinformation directly from the individual towhom it pertains, whenever possible.
5. When a government entity requests personalinformation from an individual, laws requirethe individual to be notified of the authority forthe collection of data, whether the disclosure ismandatory or voluntary.
6. The individual may contest the accuracy, com-pleteness, and timeliness of his or her personalinformation and request an amendment.
7. Health care personnel must decide whether toamend the information within a fixed time,usually 30 days after receiving a request.
8. The individual whose request for change is de-nied may file a statement of disagreement,which must be included in the record and dis-closed along with it thereafter.
9. The individual can seek review of a denied re-quest.
Protecting Privacy in Computerized MedicalRecords77 noted that basing new protection formedical information solely on the Privacy Act andon principles of fair information practices will failto consider the complexity of today’s informationenvironment, with its distributed processing,sophisticated database management systems, com-puter networks, and widespread use of microcom-puters.
It is apparent that protecting personal in-formation in a computerized environment in-volves, at a minimum, access to records,
security of information flows, and new methodsof informing individuals where information isstored, where it has been sent, and how it is beingused.78
POLICY CONSIDERATIONS FORCONGRESSAttempts to improve administrative efficiency byincreased use of electronic commerce in healthcare are an important component of a larger effortto reduce costs, improve quality of care, and im-prove access. Compared with a paper-based sys-tem, electronic information systems do appear toreduce costs for some users. The industry is mov-ing in this direction. Standards development acti-vities are under way.
However, getting started with electronic com-merce is expensive. Some organizations haveweak financial incentives to make the necessaryinvestments to institute electronic payments,while others are forging ahead without waiting forstandards to be set. Some experts interviewed byOTA commented that the complexities of dealingwith paper records and paper-based transactions,particularly as health care organizations growlarger and enter new lines of business, are forcingsome organizations to implement electronic sys-tems, even if they have no way to measure the ac-tual cost-effectiveness of a particular system. Thecomputer network, like the telephone, is becom-ing a part of the way business is conducted; a firmsimply has to have one to compete in the market,whether it makes economic sense or not.79
There may be some savings for the health caresystem as a whole if electronic medical payments,for example, are implemented on a near-universalscale. However, at current rates of implementa-tion, high levels of use of electronic payments orcompliance with standards may not be achievedfor some time. The health care industry in the
77 Office of Technology Assessment, op. cit., footnote 60.78 Ibid., p. 79.79 Project HOPE Center for Health Affairs, op. cit., footnote 2.

Chapter 3 Networks for Health Information | 119
United States is not organized as a “system” with acentral focus or consensus on how to deal withsystemwide problems. The different parts of thesystem have diverse incentives, and efforts to con-trol costs in one area may increase costs in another.However, these shifted costs are so subtle andspread over so many participants in a complexsystem that they are hard to quantify. For example,a major payer, in an effort to reduce its own costs,may begin to request additional data and docu-mentation (beyond what is on the standard forms)when providers submit large claims. All providerswho deal with that payer then incur additionalcosts to resubmit rejected claims, develop andmaintain different versions of the standard form,or provide the additional data with all claims toavoid the problem of deciding when to send it andwhen not to. Situations like these make it difficultfor the industry to establish truly uniform proce-dures.
The trend toward managed care reduces this di-versity of interest to some extent. The percentageof people covered by traditional indemnity insur-ance in the fee-for-service sector can be expectedto decrease, thus reducing the number of transac-tions between providers and payers as well. Somemanaged care organizations, like staff modelHMOs, will internalize these transactions, andwill presumably perform them efficiently out ofsheer corporate self-interest. But managed care istaking many forms, including independent prac-tice associations and other arrangements forwhich transactions will remain external between anetwork of different provider and payer organiza-tions. For the near future, absent a far-reachinggovernment-imposed restructuring of the system,many private insurers and health care providerswill continue to do business as independent firmswhose interests do not coincide.
There are three major areas in which govern-ment action might be considered: 1) providingleadership in the adoption of standards for elec-tronic medical payments and other transactionsand exchanges of health information; 2) establish-ing a system of unique identifiers for people,providers, and payers; and 3) establishing a more
consistent regulatory environment for interstateexchanges of health information.
❚ StandardsThe federal government has already played a ma-jor role in establishing the current level of stan-dardization. For example, in the area of electronicmedical payments, HCFA’s commitment to elec-tronic claims-filing and its adoption of EDI stan-dards have caused many providers and privatepayers to use these technologies. Further steps byHCFA—for example, offering truly expeditedpayment to providers who file electronically(instead of making delayed payment to those whomake paper claims, as is currently the case)—could encourage more providers to make thenecessary investments needed to comply. HCFA’searly adoption of EDI standards for other formsand transactions could also inspire other payers tomake use of them. HCFA’s ongoing plans to estab-lish a national payer file and to automate second-ary payments should also serve as an example ofhow to simplify the complex process of coordina-tion of benefits. Thus, one option for federal ac-tion is to continue to influence the standardizationof health care information transactions throughthe federal government’s role as a major insurer.
However, even HCFA’s leadership will not en-sure universal compliance with standards amongall payers and providers, and it is likely that wide-spread compliance is needed in order to realize no-ticeable savings. As long as some set ofparticipants does not comply, many others willhave to maintain separate systems or multiple ver-sions in order to do business with them. The in-formation involved is very complex, and certainclasses of participants—payers, state govern-ments, and others—will continue to create theneed for new types of data for their own purposes,but not necessarily those of their trading partnersor the system as a whole. If they have either moneyor licensing authority on their side, their tradingpartners will have to comply with their demandsin addition to the standard.
Given that near-universal compliance seems tobe important, but is not being achieved as yet,

120 | Bringing Health Care Online: The Role of Information Technologies
Congress may want government to take a more ac-tive role in administrative simplification. Thus, amore active approach would be for Congress toconsider requiring the adoption of industry-devel-oped standards for core electronic transactions,including maximum data sets, and setting timeta-bles for their implementation.
This option suggests the adoption of standardsfor a small set of core transactions within the nearfuture. It assumes that the transition from a fee-for-service environment to a managed care envi-ronment is going to be a gradual one, and that for anumber of years it will be worthwhile to make thebasic fee-for-service transactions as efficient aspossible. This option is also limited in that its aimis not to mandate sweeping requirements for im-plementing electronic transactions, but rather tofocus on a small set of transactions. Core transac-tions include: claims and billing, payment and re-mittance advice, eligibility inquiry, enrollment,and coordination of benefits. Standard forms formanaged care transactions, such as the encounterreport, could also be considered in this group.These are areas where the voluntary standardsprocess is well advanced. Requiring adoption ofstandards for other transactions might be consid-ered in the future.
The option includes a requirement for maxi-mum data sets for each transaction. It will be nec-essary to obtain consensus from providers andpayers about what information is needed for thetransactions, and then ensure that participantsmay not unilaterally increase information require-ments that would lead to the proliferation of non-standard forms.
A requirement for universal compliance withan electronic transaction system would necessari-ly create problems for some providers and payers,particularly small ones. Clearly not all providersand payers will be able to handle electronic trans-actions or modify their proprietary systems tomeet standards within any given timeframe; how-ever, they should be able to contract with commu-nity health information networks, clearinghouses,electronic medical claims services, or other firmswho can provide these services for them.
Unfortunately, a government-imposed stan-dards-setting process would require some centralfocus of authority to set timetables and to ensurecompliance. Therefore, a necessary corollary tothe option discussed above would be to charge agovernment agency with responsibility and au-thority to set standards and data definitions foradministrative transactions in consultation withindustry groups, and to manage changes to stan-dards over time; or create an agency or commis-sion for this purpose.
Establishing a central authority, whether withinan existing agency or in a new commission, is alsoa cost—one that would be shifted from the healthcare system as a whole to the government. How-ever, it is unlikely that standards and timetableswill be adhered to unless someone is in charge.
Possible disadvantages of requiring standard-ization and creating an authority—for example,locking into a standard too soon—do not appear tobe problems for electronic medical payments atthis time, at least for core transactions. Industrygroups have made progress with standards for thebasic core transactions and preliminary versionsare available for many. There is a need, however,to ensure that the standards are implemented in thesame way so their use is uniform. Industry input,from both payers and providers, is definitely need-ed for this. Clearly, if the agency or commissionattempted to develop standards de novo, many un-necessary costs could be incurred; therefore itwould have to work closely with industry groupsalready in existence. A number of industry groupshave voiced support for greater government in-volvement, including actions to speed the stan-dards-setting process.
❚ Standard Identifiers for Individuals,Providers, and Payers
Consistent with the above options, another areafor nationwide action would be to establish a sys-tem of unique identifiers for patients, providers,and payers.
Controversy continues about the particular sys-tem of identifiers to be used for individuals. In the

Chapter 3 Networks for Health Information | 121
past, OTA has cautioned against use of the SSN asa national identification number of any kind,largely on privacy grounds. OTA has suggested inearlier work that a new numbering system, withlegal protections against misuse built in from thebeginning, would be more appropriate. Support-ers of the SSN argue, with some merit, that the dis-advantages cited for the SSN are bound to afflictany numbering system eventually, even one that isdeveloped from scratch. With modifications, suchas a check digit or other additional digits, the SSNmay be the fastest and possibly the lowest-cost op-tion for establishing a numbering system.
Identifier systems that meet the needs of bothprivate sector and government users would bemost useful. HCFA has made efforts to include avariety of public and private stakeholders in thedevelopment of its national provider identifier(NPI). That system, which HCFA proposes to im-plement for Medicare providers in 1996, has thepotential to be expanded into a universal system.Expanding the NPI to include non-Medicare pro-viders would require congressional action to al-low HCFA to open up the system and to establishwhich agency should administer it. Similarly,HCFA’s efforts toward developing a payer registryand automating the secondary payment processcould serve as the basis for establishing a national,automated coordination-of-benefits system forprivate payers.
❚ Consistent Regulatory EnvironmentSome state governments, under the influence ofindustry associations and other groups, are at-tempting to change state legislation that limits thedevelopment of computer-based patient records.However, the variety of state legislation that af-fects electronic health information is still bewil-dering and poses a barrier to the efficientdevelopment of interstate electronic commerce inhealth care. One option is to encourage the pas-sage of uniform state legislation with regard toprivacy and confidentiality, allowable storagemedia, and standards for health information. Anumber of industry groups are already working
with legislatures to enact uniform legislation. Inaddition, the Department of Health and HumanServices has recently been tasked by the Adminis-tration to take the lead in developing model stateprivacy laws and model institutional privacy poli-cies for health information. Such leadership by afederal agency may be useful in speeding theadoption of new information laws.
Privacy and confidentiality are particularly im-portant areas in dealing with health information; ifthere is little confidence that an electronic medicalinformation system will protect them, then pro-viders and patients will be unwilling to use it. Ifthe process of revising legislation on a state-by-state basis is seen as too time-consuming, or notsufficiently effective, then some additional feder-al intervention may be necessary either to supportuniform legislation or to provide federal legisla-tion. In this case, Congress may wish to establishfederal legislation and regulation with regard toprivacy and confidentiality of medical informa-tion, as well as storage media for medical recordsand electronic data standards for storage andtransmission of medical information. A corollaryto this option is to charge a government agency,or create a committee or commission, to overseethe protection of health care data; to provide on-going review of privacy issues; to keep abreast ofdevelopments in technology, security measures,and information flow; and to advise Congressabout privacy matters in the area of health careinformation.
The purpose of these options is to create a na-tional environment where electronic commerceand the development of computer-based patientrecords is not discouraged by local differences inregulation. This would establish a minimum floorso that interstate commerce and information ex-change can be maintained. There is still a need forconsiderable research on the computer-based pa-tient record and other kinds of health information.Detailed standards about the computer-based pa-tient record within a particular provider organiza-tion cannot be legislated or established byregulation at this time, and, in fact, such regula-

122 | Bringing Health Care Online: The Role of Information Technologies
tion may never be desirable. However, minimumstandards for the storage and protection of healthinformation, and for its exchange among institu-tions, may now be in order.
Many violations of security, privacy, or confi-dentiality are caused by insiders—trusted individ-uals who exceed their authority or put informationthey are authorized to have to an unauthorizeduse.80 Establishing clear and uniform law to pro-tect privacy and confidentiality, along with civiland criminal penalties for violations, would en-courage organizations that handle electronichealth care information to establish strong internalpolicies and procedures, which will be as impor-tant as technological protections for information.With regard to privacy and confidentiality, an ear-lier OTA report cited seven provisions to be con-sidered in any federal legislation affecting healthinformation:1. Define the subject matter of the legislation,
health care information, to encompass the fullrange of medical information collected, stored,and transmitted about individuals, not simplythe patient record.
2. Define the elements comprising invasion ofprivacy of health care information and provide
criminal and civil sanctions for improper pos-session, brokering, disclosure, or sale of healthcare information, with penalties sufficient todeter perpetrators.
3. Establish requirements for informed consent.4. Establish rules for educating patients about in-
formation practices; access to information;amendment, correction, and deletion of in-formation; and creation of databases.
5. Establish protocols for access to informationby secondary users, and determine their rightsand responsibilities in the information they ac-cess.
6. Structure the law to track the information flow,incorporating the ability of computer securitysystems to monitor and warn of leaks and im-proper access to information so the law can beapplied to the information at the point of abuse,not to one “home” institution.
7. Establish a committee, commission, or panel tooversee privacy in health care information.81
These principles will continue to be useful indesigning uniform state or federal regulation withregard to health information security, privacy, andconfidentiality.
80 Office of Technology Assessment, op. cit., footnote 69.81 Office of Technology Assessment, op. cit., footnote 60, p. 87

Using InformationTechnology To Improve
the Quality ofHealth Care
he quality of health care is ultimately judged by the impactof specific health services on the patient’s health status.1
Improving quality involves identifying and using healthservices that, when properly executed, produce the great-
est improvement in health status. The most direct contributionthat information technology can make to improving the quality ofhealth care is to provide the clinician with better informationabout the patient and health problem at hand, and alternative testsand treatments for that problem, preferably at the point of care.This would enable clinicians to choose more effective servicesmore quickly2 and help them avoid potentially tragic errors.3
This chapter discusses the potential for advanced informationtechnologies to improve the quality of health care—as indicated
1 Institute of Medicine, Medicare: A Strategy for Quality Assurance, K.N. Lohr (ed.)
(Washington, DC: National Academy Press, 1990), pp. 20-25.
2 K.L. Coltin and D.B. Aronow, “Quality Assurance and Quality Improvement in theInformation Age,” Putting Research to Work in Quality Improvement and Quality Assur-ance, M.L. Grady, J. Bernstein, and S. Robinson (eds.), Agency for Health Care Policy andResearch, Pub. No. 93-0034 (Rockville, MD: July 1993), pp. 51-54; S.D. Horn and D.S.P.Hopkins, “Introduction,” Clinical Practice Improvement: A New Technology for Devel-oping Cost-Effective Quality Health Care, S.D. Horn and D.S.P. Hopkins (eds.)(NewYork, NY: Faulkner & Gray, 1994), pp. 1-5.
3 L.L. Leape, “Error in Medicine,” Journal of the American Medical Association, vol.272, No. 23, Dec. 21, 1994, pp. 1851-1857; L.L. Leape et al., “Systems Analysis of Ad-verse Drug Events,”Journal of the American Medical Association, vol. 274, No.1, July 5,1995, pp. 35-43; D.W. Bates et al., “Incidence of Adverse Drug Events and Potential Ad-verse Drug Events: Implications for Prevention,” Journal of the American MedicalAssociation, vol. 274, No.1, July 5, 1995, pp. 29-34.
| 123

124 | Bringing Health Care Online: The Role of Information Technologies
by the effectiveness of clinical decisionmak-ing4—and the potential role of the federal govern-ment in that process. The most relevanttechnologies5 include:
� electronic patient records,� structured data entry,� advanced human-computer interface technolo-
gies,� portable computers,� automated capture of data from diagnostic and
monitoring equipment,� relational databases with online query (key-
word search and retrieval),� knowledge-based computing, and� computer networks.
This chapter first reviews the clinical decisionsupport approach to improving health care, andthe ways in which information technology couldenhance clinical decisionmaking. It then ex-amines the performance assessment approach toimproving health care, which involves evaluatingspecific health services, providers,6 and insuranceplans.7 Ways in which some of the problems con-fronting both approaches might be resolved by us-ing information technology are explored. Thechapter concludes with a discussion of policy is-sues and options regarding potential governmen-tal roles in those developments.
CLINICAL DECISION SUPPORTClinical decision support can be broadly and sim-ply defined as the use of information to help a cli-nician diagnose and/or treat a patient’s healthproblem. Two kinds of information are involved:
1) information about the patient; and 2) informa-tion about the kind of health problem afflicting thepatient and alternative tests and treatments for it.Clinical decision support is by no means a newphenomenon—such information traditionally hasbeen available from several sources. However,those sources have limitations that often diminishtheir reliability or their accessibility at the point ofcare.
The time pressures of clinical practice do notallow clinicians to study the patient’s entire healthhistory or review the latest clinical knowledge onevery nonroutine health problem they encounter.Consequently, one major goal of clinical decisionsupport is to locate needed information and makeit available to the clinician in readily usable format the point of care as quickly as possible, and in amanner that minimally interferes with the careprocess. Moreover, the potentially severe conse-quences of incorrect clinical decisions for both thepatient and the clinician require that the informa-tion retrieved be as accurate as possible.
❚ Limitations of Traditional InformationSources
Information About the PatientThe specific kinds of information about the pa-tient that are useful in clinical decisionmaking fallinto two broad categories:
1. Health problems, both current (signs andsymptoms, physical findings, diagnostic testresults, functional status, etc.) and previous(medical history, including previous servicesfor each health problem); and
4 This approach focuses on the effectiveness of the health services delivered by providers and insurance plans (see footnotes 6 and 7). Therole of the patient in clinical decisionmaking and self-care, and ways in which information technology can enhance that role, were discussed inchapter 1.
5 See chapter 2 for details on these technologies.
6 Throughout this chapter, the term providers includes both individual clinicians and institutional providers such as hospitals. Cliniciansinclude physicians and other licensed practitioners, such as nurses. Physicians include allopathic medical doctors, osteopaths, chiropractors,podiatrists, etc. In discussing clinicians who diagnose and treat health problems, this report includes nurse practitioners, physician assistants,and other physician extenders who are licensed to prescribe medications.
7 The term health insurance plan here includes traditional indemnity plans and managed care organizations (health maintenance organiza-
tions, preferred provider organizations, etc.).

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 125
2. Background, including demographic traits(age, sex, ethnicity, and socioeconomic status),risky behaviors (substance abuse and hazard-ous occupations, sports, hobbies, or sexualpractices), exposures (occupational and environ-mental hazards), allergies, and family history.
Information about the patient traditionally hasbeen drawn from the paper-based patient recordand direct clinical examination of the patient.Briefly, the major difficulties with the paper-based patient record8 include:
� indecipherable content,� lack of comprehensiveness,� lack of completeness,� inaccuracy,� inaccessibility,� lack of uniformity and standards,� slow and cumbersome transmission,� lack of security, and� sheer physical volume.
These problems make it difficult to quickly lo-cate accurate and readily usable information aboutthe patient at the point of care.
Problems with the clinical examination9 in-clude:
� unsystematic methods in obtaining thepatient’s health history,
� unsystematic methods in observing thepatient’s signs and symptoms,
� faulty reasoning and inference in using thecollected information, and
� the amount of time required to obtain andrecord all of this information.
These drawbacks jeopardize the completenessand accuracy of new information about the pa-tient’s current health problems.
Information About the Health ProblemThe most efficient source of information about aspecific health problem is the clinician’s ownknowledge and experience with similar cases.Such information can usually be retrieved almostinstantaneously from the clinician’s memory andcan be readily applied to a health problem in termsthat the clinician understands. Indeed, between 80and 90 percent of clinical actions are based onsuch information.10 However, it is impossible forclinicians to remember all available informationabout all of the health problems they are likely toencounter, or all of the alternative tests and treat-ments for those problems. Even experts on a givenhealth problem are likely to have only selected in-formation on that problem—information that maybe unsystematic, unrepresentative, and biased.Most clinicians need to consult other sources ofclinical knowledge and experience, at least on oc-casion.
A clinician may seek the advice of other clini-cians and researchers who have special knowl-edge or experience regarding the health problemat hand. However, the patients usually seen by theconsultant may differ from the referring clini-cian’s patients in important ways. In addition, anyindividual clinician’s patients may not be typicalof all patients with the health problem at hand, andthe consultant’s knowledge and experience couldalso be highly selective. Finally, consultants sim-
8 Institute of Medicine, The Computer-Based Patient Record: An Essential Technology for Health Care, R.S. Dick and E.B. Steen (eds.)(Washington, DC: National Academy Press, 1991), pp. 12-19; P.C. Tang, D. Fafchamps, and E.H. Shortliffe, “Traditional Medical Records as aSource of Clinical Data in the Outpatient Setting,” Proceedings of the Eighteenth Annual Symposium on Computer Applications in MedicalCare, J.G. Ozbolt (ed.) (Philadelphia, PA: Hanley & Belfus, 1994), pp. 575-579; J.C. Wyatt, “Clinical Data Systems, Part 1: Data and MedicalRecords,” Lancet, vol. 344, No. 8936, Dec. 3, 1994, pp. 1543-1547. For further discussion of problems with paper-based patient records, seechapter 2.
9 See C. Selby et al., “Set Up and Run an Objective Structured Clinical Exam,” British Medical Journal, vol. 310, No. 6988, May 6, 1995, pp.
1187-1190.
10 B.C. James, “Advances in Computer-Based Patient Records for Health Services Research,” presentation at the 12th Annual Meeting of
the Association for Health Services Research, Chicago, IL, June 4-6, 1995.

126 | Bringing Health Care Online: The Role of Information Technologies
ply may not be available when needed in urgentcases.
A related source of clinical guidance for practi-tioners is legal standards of care, which specifythe levels of care provided by the majority of phy-sicians in particular clinical situations. Thesestandards are determined by the courts, largely onthe basis of testimony by expert witnesses duringmalpractice lawsuits. The widely conflictingopinions expressed by different experts in manysuch contexts illustrate the extent to which legalstandards of care can be vague, inconsistent, andincomplete.11 Extensive variation in practice pat-terns among clinicians within and across localitieshas been thoroughly documented. This variationreflects, in part, the lack of consensus regardingthe most effective ways to treat most health prob-lems.12
To extend the individual knowledge and expe-rience of individual clinicians, institutional pro-viders or multifacility enterprises with largenumbers of patients sometimes conduct localclinical research on those patients over time. Suchefforts can generate information that is useful inthose providers’ own clinical decisionmaking, aswell as for publication. (Providers with fewer pa-tients often conduct such research as well, but thenumber of cases may be too small to support sta-tistically reliable comparison among treatmentgroups.) However, local research may be usefulonly in that setting if the institution’s patients orpractice patterns are atypical. In any case, exten-sive local research is not that common, evenamong large institutions.
Information published in printed clinical liter-ature (reference books, textbooks, research stud-ies, and professional periodicals) is anotherwell-established source of information for clinicaldecisionmaking. However, it can be difficult to lo-cate such information quickly because of inade-quate indexing and the problem of keeping papermaterials organized. In addition, a considerableamount of time can elapse before new informationgets published; and once published, it quickly be-comes outdated. Maintaining large amounts ofprinted information in accurate, up-to-date, andreadily accessible form can be expensive.
As with clinician knowledge and experience,clinical literature also may sometimes harborbiases resulting from the use of unsystematicmethods in generating the information. Even peer-reviewed research literature is hampered by publi-cation bias stemming from the preference ofauthors, journal editors, and reviewers for statisti-cally significant results supporting specific hy-potheses, particularly if those results areperceived as being important.13 To be consideredworthy of publication, articles whose results failto support an hypothesis must strongly challengewidely held theories and assumptions. On the oth-er hand, published research findings are oftenwidely and uncritically accepted without carefulconsideration of the soundness of the methodolo-gies used.
Despite decades of clinical and epidemiologic-al research, systematic evidence is still lacking re-garding “what works” in diagnosing, treating, and
11 U.S. Congress, Office of Technology Assessment, Defensive Medicine and Medical Malpractice, OTA-H-602 (Washington, DC: U.S.
Government Printing Office, July 1994), pp. 30-31, 164.
12 H. Krakauer et al., “The Systematic Assessment of Variations in Medical Practices and Their Outcomes,” Public Health Reports, vol. 110,No. 1, Jan.-Feb., 1995, pp. 2-12; U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work: Searching forEvidence, OTA-H-608 (Washington, DC: U.S. Government Printing Office, Sept. 1994), pp. 26-34.
13 K. Dickersin and Y.I. Min, “Publication Bias: The Problem That Won’t Go Away,” Doing More Harm Than Good: The Evaluation ofHealth Care Interventions, K.S. Warren and F. Mosteller (eds.) (New York, NY: New York Academy of Sciences, 1993); P.J. Easterbrook et al.,“Publication Bias in Clinical Research,” Lancet, vol. 337, No. 8746, Apr. 13, 1991, pp. 867-872.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 127
preventing most health problems—much lesswhich methods are most cost-effective.14 In addi-tion, even the evidence that does exist is not al-ways put to use in clinical practice. To rephrase anearlier statement, only between 10 and 20 percentof clinical actions are based on published scientif-ic research.15
❚ Practice Guidelines and ProtocolsEven when solid experiential or research-basedevidence is available, human beings are inherentlyfallible processors of that information.16 They cantrack no more than four variables simultaneously,compared with the hundreds of variables thatcharacterize even a single health condition.17 It isimpossible for clinicians to remember all avail-able information about all of the health problemsthey are likely to encounter, or all of the alterna-tive tests and treatments for those problems, or allrelevant characteristics and histories of all of theirpatients. Moreover, recall is biased toward thingsthat are considered to be more important, that tendto confirm one’s prejudices, and that are more re-cently experienced.18 Indeed, one researcher hasreferred to clinical decision support as “uncertain-ty management.”19
In an effort to reduce this uncertainty, clinicalpractice guidelines20 have been developed overthe past few decades by numerous medical spe-cialty societies, insurance companies, utilizationreview organizations, managed care organiza-tions, and government agencies. Guidelines focuson a given health problem or procedure, and areusually developed through a group consensusprocess among selected clinical experts on thatproblem or procedure. The intent is to providebroad parameters within which clinicians contin-ue to exercise judgment, rather than to dictate ex-act steps to follow.21 Figure 4-1 reproduces analgorithm that depicts a clinical practice guidelinefor management of patients with heart failure, de-veloped by the federal government’s Agency forHealth Care Policy and Research (AHCPR). Evenwhen practice guidelines are available, however,evidence suggests that clinicians often forget tofollow them, or deviate from them without clearcause, especially in high-stress situations.22 Re-search also shows that it is difficult to change cli-nician behavior simply by providing them withinformation, even in the form of guidelines.23
Formal clinical protocols are more rigorousmodels of the process of care for a given
14 U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12; P.J. Neumann and M.
Johannesson, “From Principle to Public Policy: Using Cost-Effectiveness Analysis,” Health Affairs, vol. 13, No. 3, summer 1994, pp. 206-214.
15 James, op. cit., footnote 10.16 C.J. McDonald, “Protocol-Based Computer Reminders, The Quality of Care and the Non-Perfectability of Man,” New England Journal
of Medicine, vol. 295, No. 24, Dec. 9, 1976, pp. 1351-1355; Leape, op. cit., footnote 3.
17 A.H. Morris, “Protocol Management of Adult Respiratory Distress Syndrome,” New Horizons, vol. 1, No. 4, Nov. 1993, p. 594.18 Ibid., p. 593.19 E.H. Shortliffe, “Medical Informatics and Clinical Decision Making: The Science and the Pragmatics,” Medical Decision Making, vol.
11, No. 4, Oct.-Dec. Supplement, 1991, pp. S2-S4.
20 Clinical practice guidelines are sometimes called practice parameters or some variation of clinical paths or critical pathways—terminol-
ogy adapted from critical path analysis in manufacturing and other industries.
21 U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12, ch. 7.
22 E. Coiera, “Medical Informatics,” British Medical Journal, vol. 310, No. 6991, May 27, 1995, p. 1383.23 T.H. Lee. et al., “Failure of Information as an Intervention To Modify Clinical Management,” Annals of Internal Medicine, vol. 122, No. 6,
Mar. 15, 1995, p. 436; U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12, ch. 8.

128 Bringing Health Care Online: The Role of Information Technologies

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 129
health problem. They are composed of highly spe-cific steps and decision parameters regardingdiagnosis, treatment, or prevention of a problem.The inputs and outputs of a given step can be ei-ther deterministic (involving a fixed value or ac-tion) or probabilistic (involving a range ofpossible values or actions). Clinicians may stillexercise judgment and override any particular stepin a protocol, but having a clear sequence of spe-cific steps to follow can help ensure that none willbe inadvertently forgotten or altered.24
Many clinicians view practice guidelines andprotocols skeptically as being “cookbook medi-cine,”25 concocted largely by clinically unin-formed researchers and bureaucrats. Some arealso concerned that guidelines may be usedagainst clinicians in malpractice suits,26 althoughevidence indicates that they are used by bothplaintiffs’ and defendants’ attorneys.27 Other cli-nicians criticize guidelines that are based more onjudgmental consensus than on scientific evidence.These guidelines are seen as being vague and sub-jective, lacking in specificity and testability, andbased on incomplete and inaccurate informa-tion—drawbacks that make it difficult to derivecase-specific advice.28
For example, nurses at LDS Hospital in SaltLake City, Utah, found that the AHCPR guidelinefor treating pressure ulcers was too vague to use inclinical practice. Most importantly, the guidelinedid not specify the treatment options for variouscombinations of scores on six components of a
measure of risk for developing pressure ulcers. Ateam of nurses, physicians, and researchers con-verted the guideline into a more formal clinicalprotocol by developing exact specifications forthose treatment options through an iterative groupconsensus process and monitoring of patient out-comes.29 This illustrates how local research canbe used to inform the development and refinementof clinical practice guidelines and protocols. Italso emphasizes the need for careful testing andscreening of these kinds of clinical decision sup-port.
❚ Potential Contributions of InformationTechnology
The basic question in this area is whether ad-vanced information technologies can 1) improvethe accuracy of the information needed in clinicaldecisionmaking, 2) reduce the amount of time re-quired to retrieve that information, and 3) makethat information accessible at the point of care.This section highlights some of the potential con-tributions these technologies can make to clinicaldecision support. A later section summarizessome of the limited and mixed evidence bearingon these questions.
Entering and Retrieving Patient InformationThe key technology for improving patient in-formation is the electronic patient record thatstores comprehensive information on the patient
24 Coiera, op. cit., footnote 22.25 W.W. Parmley, “Clinical Practice Guidelines: Does the Cookbook Have Enough Recipes?” Journal of the American Medical Associa-
tion, vol. 272, No. 17, Nov. 2, 1994, pp. 1374-1375.
26 F. Bazzoli, “Computerized Records Will Play a Key Role in the Implementation of Clinical Guidelines,” Health Data Management, Feb-
ruary 1995, p. 32.
27 A.L. Hyams et al., “Practice Guidelines and Malpractice Litigation: A Two-Way Street,” Annals of Internal Medicine, vol. 122, No. 6,
Mar. 15, 1995, pp. 450-455.
28 C.J. McDonald and J.M. Overhage, “Guidelines You Can Follow and Can Trust: An Ideal and an Example,” Journal of the American
Medical Association, vol. 271, No. 11, Mar. 16, 1994, pp. 872-873.
29 S. D. Horn, C. Ashton, and D.M. Tracy, “Prevention and Treatment of Pressure Ulcers by Protocol,” Clinical Practice Improvement: ANew Technology for Developing Cost-Effective Quality Health Care, S.D. Horn and D.S.P. Hopkins (eds.)(New York, NY: Faulkner & Gray,1994), pp. 253-262; “LDS Nurses Reduce Pressure Ulcer Incidence with Retooled Guidelines,” Report on Medical Guidelines & OutcomesResearch, Feb. 23, 1995, pp. 10-11.

130 | Bringing Health Care Online: The Role of Information Technologies
from a variety of sources (clinic, laboratory, phar-macy, etc.).30 Other technologies for handling pa-tient information operate in conjunction with theelectronic patient record. Overall, these technolo-gies could permit faster, easier, and more accuratecollection of information about the patient.31
Clinical examination results can be entered by cli-nicians at or near the point of care, particularlywith the aid of portable computers. Structureddata entry, such as on-screen forms and menus andprepared blocks of text, can encourage completedata collection and reduce keying errors, particu-larly when pen-based computing is used ratherthan keyboards. Automatic date- and time-stamp-ing of entries facilitates documentation and track-ing of patient care and outcomes over time.
Some patient data can be captured directly fromdiagnostic and monitoring equipment, bypassinghuman data entry altogether. Radiographicimages, full-motion videos, and sound recordingscan be digitized, stored, and transmitted electroni-cally, often with resolution approaching that ofanalog technologies. Patient background in-formation and risk factors32 can be entered intocomputers by patients themselves, again with theaid of structured data entry and advanced human-computer interface technologies. One example ofsuch a system is HealthQuiz33 (see appendix C).Basic demographic traits can be obtained fromother computer databases (e.g., insurance eligibil-ity files) through computer networks, again by-passing human data entry.
Using relational databases with online query,information technologies can also permit faster,easier, and better targeted search and retrieval ofpreviously collected information about the pa-
tient—even at the point of care. Portable comput-ers and advanced human-computer interfacetechnologies can also be helpful here. Electronicstorage of digitized radiographic images, full-mo-tion videos, and sound recordings can make themeasier to locate, although retrieving them can beslow if the computers, telecommunications equip-ment, or transmission lines used have insufficientcapacity. Increasingly powerful and flexiblegraphics software and higher resolution displayscan offer flexibility in the ways information is or-ganized and displayed to suit the individual needsof clinicians.
Retrieving Information About the HealthProblemComputer and telecommunications networks, inconjunction with online query, portable comput-ers, and advanced human-computer interfaces,can make information about various health prob-lems more readily accessible from either local orremote knowledge bases. Many research librariesprovide online access to their computerized cata-logs (e.g., the Library of Congress’s SCORPIO)and bibliographic databases (e.g., The NationalLibrary of Medicine’s MEDLINE) that can bequeried online. Documents can be ordered elec-tronically (even during an online literature search)from one of the more than 4,000 member librariesof the National Network of Libraries of Medicine.Documents can be shipped in hard-copy form ortransmitted electronically via the Internet or fax.Unfortunately, these databases do not cover all ofthe clinical literature, and it can be difficult toidentify all studies of a certain kind, such as ran-domized controlled trials.34
30 Although the computer-based patient record is usually conceptualized as being a centralized repository, in reality different components of
the record may be stored in separate but seamlessly linked computer systems.
31 J.C. Wyatt, “Clinical Data Systems, Part 2: Components and Techniques,” Lancet, vol. 344, No. 8937, Dec. 10, 1994, pp. 1609-1614.32 Risk factors are key health problems and background characteristics that can affect the patient’s outcome, independent of the specific
kinds of services received.
33 “ ‘HealthQuiz’ Makes Preventive Care Guidelines Easy To Apply,” Report on Medical Guidelines & Outcomes Research, Jan. 26, 1995,
pp. 5-6.
34 U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12, p. 81.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 131
The National Cancer Institute (NCI) maintainsa Physician Data Query (PDQ) system that pro-vides online information via the Internet (Cancer-Net) and by fax (CancerFax) regarding variouscancers, ongoing clinical trials, and individualsand organizations involved in cancer care. TheUniversity of Pennsylvania also maintains a mul-timedia cancer information resource on the Inter-net called OncoLink. The Centers for DiseaseControl and Prevention provide online access tothe full text of Morbidity and Mortality WeeklyReport, and has recently launched an online jour-nal called Emerging Infectious Diseases. Severalbiomedical journals are also available online.35
Some periodicals, and even complete booksand reports, are becoming available on CD-ROMsthat can be purchased or obtained through manylibraries. (In their current form, however, CD-ROMs cannot be updated, and must be replaced asknowledge changes.) Both CD-ROMs and the In-ternet permit inclusion of graphics, videos, andsound in textual documents. This helps offset thecomplaint that it is not only less pleasant to readdocuments on a video screen than on paper, but ac-tually slower.36
Information technology is also making practiceguidelines more readily accessible. The NationalLibrary of Medicine (NLM) offers online accessto practice guidelines developed by AHCPR, andNCI’s PDQ system includes information on can-cer treatment protocols. Private organizationssuch as the American Medical Association are
also distributing their practice guidelines on CD-ROMs and computer diskettes.
In recent years, an international movementamong researchers and clinicians has developedan approach to clinical problem-solving called ev-idence-based medicine.37 It involves systematicsearching and critical appraisal of the research lit-erature to identify findings that can be applied to aclearly defined clinical problem. This approachgoes beyond the narrative review articles occa-sionally published in leading clinical journals. Itemploys systematic review of the literature, inwhich specific items of information are extractedfrom each work and compared across works, us-ing structured methods. The most sophisticatedform of systematic review is meta-analysis, orquantitative synthesis of the statistical results of anumber of studies on a given topic.38 Special jour-nals have been established to summarize and eval-uate the vast literature on selected healthproblems.39 The Cochrane Collaboration, an in-ternational network of researchers, distributesresults of systematic reviews of randomized con-trolled trials—or the most reliable evidence fromother sources—on selected health problems (be-ginning with pregnancy and childbirth) in un-copyrighted form via the Internet, as well as oncomputer diskettes and CD-ROMs.40 However, itis unclear how these results will get incorporatedsystematically into clinical practice guidelinesand protocols.41
35 H.F. Judson, “Structural Transformations of the Sciences and the End of Peer Review,” Journal of the American Medical Association, vol.
272, No. 2, July 13, 1994, p. 93.
36 J.C. Wyatt, op. cit., footnote 31, p. 1613.37 W. Rosenberg and A. Donald, “Evidence Based Medicine: An Approach to Clinical Problem-Solving,” British Medical Journal, vol. 310,
No. 6987, Apr. 29, 1995, pp. 1122-1126.
38 U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12, pp. 59-65.39 F. Davidoff et al., “Evidence Based Medicine: A New Journal To Help Doctors Identify the Information They Need,” British Medical
Journal, vol. 310, No. 6987, Apr. 29, 1995, pp. 1085-1086.
40 Cochrane Collaboration, “The Cochrane Collaboration: Preparing, Maintaining, and Disseminating Systematic Reviews of the Effects of
Health Care,” Oxford, England, brochure, n.d.
41 J.C. Wyatt, “Clinical Data Systems, Part 3: Development and Evaluation,” Lancet, vol. 344, No. 8938, Dec. 17, 1994, p. 1687.

132 | Bringing Health Care Online: The Role of Information Technologies
The prospect of making information such as re-search results readily and inexpensively availablefor online query through the Internet has spawnedvisions of electronic (online) publishing.42 Notonly are certain peer-reviewed journals alreadyavailable online, but in some disciplines, such asphysics, preprints containing preliminary resultsare often distributed over the Internet prior toprinted publication.43 At first glance, this mightappear to reduce the problem of publication bias.However, in addition to the fact that much ofthat bias rests with authors themselves, there areseveral other concerns about this prospect. Mostimportant is the absence of online screeningmechanisms to replace the process of scientificpeer review that seeks to ensure the quality of pub-lished research.44 Without such mechanisms forscreening documents for scientific rigor as well asrelevance to one’s interests,45 the increasing prob-lem of information overload could worsen. More-over, public access to unrefereed preprints ofmedical research could lead some people to mis-use medications.46 On the other hand, online ac-cess to the full text of commercially publishedbooks and journal articles is likely to remain lim-ited until electronic subscription and paymentmechanisms become established and issues re-
garding intellectual property rights and electroniccopying are resolved.47
Computer-Based Clinical Decision SupportSystemsIncreasingly, the traditional sources of clinical de-cision support are being supplemented by clinicalinformation systems, mainly at large academicmedical centers. The most rudimentary of theseare library systems or simple data systems48 thatmerely display information about the patient and/or the health problem to the clinician without of-fering advice based on analysis of thatinformation. However, some clinical informationsystems contain expert systems or knowledge-based systems that do offer advice to the clinicianregarding diagnosis, testing, or treatment.49 Thegoal of either simple or knowledge-based decisionsupport systems is to provide more complete andaccurate information more quickly to the clini-cian—preferably at the point of care—thereby im-proving clinical decisionmaking in terms ofpatient outcome measures. These benefits to theclinician presumably outweigh the added burdenof more extensive data collection and entry. Clini-cal information systems may also contain otherapplications besides decision support, such as on-
42 R.E. LaPorte et al., “The Death of Biomedical Journals,” British Medical Journal, vol. 310, No. 6991, 1387-1390, May 27, 1995, pp.
1085-1086; Judson, op. cit., footnote 35.
43 J.P. Kassirer and M. Angell, “The Internet and the Journal,” Journal of the American Medical Association, vol. 332, No. 25, June 22,
1995, p 1709.
44 Both Judson and LaPorte et al, op. cit., footnote 42, propose an online peer review system in which all readers of a document wouldcomment on it. LaPorte et al. go further in proposing that readers give each document ratings in various categories. These comments and sum-mary ratings would subsequently be attached to the document for other readers to use in screening. One potential problem with this scenario isthat readers willing to take time to evaluate all documents that they read might well be a small, self-selected, hence unrepresentative group; andthere would be no way to ensure that they were qualified to evaluate the document. Kassirer and Angell discuss the perils of “majority rule”compared to peer review. Op. cit., footnote 43.
45 LaPorte et al. suggest that software agents could be used to select only documents that meet certain user-specified content criteria. Op. cit.,
footnote 42.
46 Kassirer and Angell, op. cit., footnote 43.47 U.S. Congress, Office of Technology Assessment, Information Security and Privacy in Network Environments, OTA-TCT-606 (Wash-
ington, DC: U.S. Government Printing Office, September 1994), pp. 96-110.
48 Wyatt, op. cit., footnote 41.49 Wyatt refers to these as advisory systems. Ibid.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 133
line order entry, that allows the clinician to submitorders for tests and treatments (including pharma-ceuticals).
A knowledge-based system designed for clini-cal use, sometimes called a clinical decision sup-port system (CDSS), usually involves three basiccomponents:50
1. Data on the patient being diagnosed or treatedare either entered into the system manually,captured automatically from diagnostic ormonitoring equipment, or drawn from an elec-tronic patient record.
2. A knowledge base contains rules and decisionalgorithms that incorporate knowledge andjudgment about the health problem at hand andalternative tests and treatments for it, mainly inthe form of “if-then” statements, such as “if thepatient’s potassium is less than 3.0 mEq/dl andthe patient is on digoxin, then warn the clini-cian to consider potassium supplementa-tion.”51
3. An inference engine combines informationfrom both the patient data and the knowledgebase to perform specified tasks, outlined in ap-pendix C.
Some CDSSs—usually those developed more re-cently—employ probabilistic and adaptive ap-proaches, such as fuzzy logic, Bayesian networks,or neural networks. Others—usually those devel-oped earlier—employ rule-based systems, deci-sion trees, and other deterministic methods,although probabilistic decision nodes are some-times employed.52
Many of the major applications of CDSSs wereimplemented over the past 15 to 20 years in twopioneer systems:
� the Health Evaluation through Logical Proc-essing (HELP) system developed by Inter-mountain Health Care (IHC) and its flagshipinstitution, LDS Hospital and the University ofUtah in Salt Lake City;53 and
� the Regenstrief Medical Record System(RMRS), developed by the Regenstrief Insti-tute and Indiana University, initially at WishardMemorial Hospital in Indianapolis.54
Components of both of these systems are mar-keted commercially: HELP by the 3M Co., withabout five installations outside of Utah; andRMRS by Shared Medical Systems, Inc. (SMS),with about 10 installations outside of Indiana.Several other CDSSs, or some of their particularapplications, are also commercially available.However, most are implemented by clinical re-searchers in the form of highly specialized, local-ized, and experimental systems that vary widelyin their levels of development.
Computer-Based Clinical ProtocolsThe most advanced CDSSs integrate several ofthe applications outlined in appendix C into for-mal clinical protocols. Again, some are based ondeterministic models, while others employ proba-bilistic and adaptive approaches. Converting aclinical protocol into computer-based algorithmsforces the developer to use unambiguous ter-minology, examine the logic of all linkages
50 See D.P. Connelly and S.T. Bennett, “Expert Systems and the Clinical Laboratory Information System,” Clinics in Laboratory Medicine,
vol. 11, No. 1, March 1991, p. 136.
51 R.F. Gibson and B. Middleton, “Health Care Information Management Systems To Support CQI,” Clinical Practice Improvement: A NewTechnology for Developing Cost-Effective Quality Health Care, S.D. Horn and D.S.P. Hopkins (eds.)(New York, NY: Faulkner & Gray, 1994),p. 109.
52 R.A. Miller, “Medical Diagnositc Decision Support Systems—Past, Present, and Future,” Journal of the American Medical Informatics
Association, vol. 1, No. 1, Jan./Feb. 1994, pp. 11-16.
53 See chapter 2 and G.J. Kuperman, R.M. Gardner, and T.A. Pryor, HELP: A Dynamic Hospital Information System, Computers and Medi-
cine Series (New York, NY: Springer-Verlag, 1991).
54 See C.J. McDonald et al., “The Regenstrief Medical Record System: 20 Years of Experience in Hospitals, Clinics, and Neighborhood
Health Centers,” M.D. Computing, vol. 9, No. 4, July/August 1992, pp. 206-217.

134 | Bringing Health Care Online: The Role of Information Technologies
among steps, and—in deterministic models—specify exact parameters. It also facilitates refine-ment and updating of the protocol over time,based on any of the traditional sources of clinicaldecision support outlined earlier, plus feedbackfrom clinicians who use the protocol—particular-ly the reasons they document for overriding itsrecommendations—and from local research onpatient outcomes.
Researchers at Intermountain Health Care55
have developed an approach to quality improve-ment, called clinical practice improvement, thatessentially combines computer-based protocols,local research, and the principles of continuousquality improvement (CQI).56 A protocol is devel-oped for a selected health problem (e.g., acute re-spiratory distress syndrome) based on review ofrelevant literature, clinician judgment, and retro-spective analysis of data from the electronic pa-tient record system. The protocol is refinedthrough discussion and consensus among clini-cians, and serves to guide diagnosis and treatmentfor the selected health problem. In addition, ran-domized controlled trials of various alternativediagnostic and therapeutic procedures for thatproblem are conducted, and the protocol is furtherrefined in light of the results of those trials.
Computer-based clinical protocols may alsoprove valuable in a more indirect way. The full po-tential of CDSSs is constrained by the limitationsof electronic storage devices. Storing complete,full-text information on all possible health prob-
lems and alternative tests and treatments for themin a manner that permits rapid retrieval of that in-formation at the point of care is prohibitively ex-pensive. However, by distilling selected elementsof full-text information on a particular healthproblem and its alternative tests and treatmentsinto explicit steps, criteria, and parameters, clini-cal protocols can greatly reduce storage require-ments.
Other Potential Benefits of InformationTechnologyBoth clinical protocol development and local re-search can benefit from advanced informationtechnologies. Most patients receive care frommore than one provider, and within a given pro-vider organization there are usually several sepa-rate information systems, often one for eachdepartment (inpatient, laboratory, pharmacy,etc.). Electronic patient record systems and com-puter networks within and across provider orga-nizations can facilitate the tracking of all care andoutcomes of individual patients over time. Thesesystems make it easier and more efficient to linkthe separate records for a given patient across alldepartments and providers, particularly if a com-mon, unique patient identifier is used in all re-cords. The value of assembling patient data acrossseveral departments is illustrated by local researchthat used the HELP system at LDS Hospital toidentify specific causes of adverse drug events57
and hospital-acquired infections.58 Computer net-
55 S.D. Horn and D.S.P. Hopkins (eds.), Clinical Practice Improvement: A New Technology for Developing Cost-Effective Quality Health
Care (New York, NY: Faulkner & Gray, 1994).
56 CQI (also known as total quality management, or TQM) was originally developed in the field of manufacturing and was subsequentlyadapted to health care. See W.E. Deming, Common Causes and Special Causes of Improvement: Stable System, Out of Crisis (Cambridge, MA:MIT Center for Advanced Engineering Study, 1986); D.M. Berwick, “Continuous Improvement as an Ideal in Health Care,” New England Jour-nal of Medicine, vol. 320, No. 1, Jan. 5, 1989, pp. 53-56; Institute of Medicine, Medicare: A Strategy for Quality Assurance, K.N. Lohr (ed.)(Washington, DC: National Academy Press, 1990), pp. 58-64; S.B. Kritchevsky and B.P. Simmons, “Continuous Quality Improvement: Con-cepts and Applications for Physician Care,” Journal of the American Medical Association, vol. 266, No. 13, Oct. 2, 1991, pp. 1817-1823; Leape,op. cit., footnote 3; Leape et al., op. cit., footnote 3.
57 R.S. Evans et al., “Preventing Adverse Drug Events in Hospitalized Patients,” The Annals of Pharmacotherapy, vol. 28, No. 4, April 1994,
pp. 523-527.
58 D.C. Classen et al., “Prophylactic Antibiotics Used To Prevent Surgical Wound Infections,” Horn and Hopkins, op. cit., footnote 55, pp.
217-221.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 135
works across provider organizations could alsopermit wider and faster dissemination of clinicalprotocols and the results of generalizable local re-search, particularly to remote sites.
An indirect but important way for advanced in-formation technologies to enhance the quality ofhealth care could be improving the outcomes dataused in research on the effectiveness of specifichealth services. Electronic patient records, struc-tured data entry, advanced human-computer inter-faces, portable computers, and automated datacapture from diagnostic and monitoring equip-ment could make the collection of patient data notonly faster and easier, but also more complete andaccurate. This could permit more valid and reli-able measurement of patient risk factors, clinicalprocesses, and outcomes. Records or results forpatients with a given health problem but treated indifferent ways could be pooled across providers,creating very large databases for assessing the ef-fectiveness of specific health services. This wouldrequire using health problems, process and out-come measures, and analytical methodologiesthat were as similar as possible across providers.Research based on these improved data could en-hance the medical knowledge on which clinicaldecision support is based.
From the perspective of physicians, one directbenefit of using advanced information technologyin medical practice recently became readily appar-ent: Two malpractice insurance companies beganoffering reduced premiums to physicians who usespecific commercial electronic patient record sys-tems.59 This development mainly reflects the im-proved patient information and documentation ofcare that electronic patient records offer, com-pared with paper-based records.
❚ Continuing Problems in ClinicalDecision Support
Technology DevelopmentAs impressive as their applications are, the useful-ness of clinical decision support systems can stillbe hampered by incomplete, inaccurate, or inac-cessible information—problems that advancedinformation technologies could help overcome.As discussed in chapter 2, however, the capabili-ties of many of the information technologiesemployed in CDSSs remain limited and theircosts remain high, posing substantial barriers totheir widespread use. Several technological ad-vances are needed for faster, easier, and more ac-curate collection, entry, and retrieval of patientinformation, and more readily accessible informa-tion about the health problem. The needed ad-vances include:
� advanced human-computer interface technolo-gies, particularly voice recognition, for easierand possibly hands-free input and retrieval ofinformation;
� more extensive use of structured data entry,such as on-screen forms and menus and pre-pared blocks of text, to ensure complete datacollection and reduce keying errors;
� smaller, more portable computers that can linkinto larger computer networks, either throughwireless technologies or docking stations;
� improved wireless technologies that minimizesuch limitations as the restricted range andplacement of infrared technologies that useline-of-sight transmission, or the electromag-netic interference generated by radio-wavetransmission;
59 “Malpractice Insurers Offer Discounts for Doctors Using Electronic Records,” Health Data Management, February 1995, p. 14.

136 | Bringing Health Care Online: The Role of Information Technologies
� more efficient methods of filtering and summa-rizing the enormous quantities of data captureddirectly from diagnostic and monitoring equip-ment, such as focusing on abnormal data valuesand trends;
� higher capacity and more flexible electronicstorage devices, such as updatable CD-ROMs;
� higher resolution computer displays;� more powerful and flexible graphics software;� improved technologies for capturing and stor-
ing digitized radiographic images, full-motionvideos, and sound recordings, and faster meth-ods of retrieving such information;
� faster and more flexible methods of onlinequery using relational databases;
� higher capacity telecommunications equip-ment and transmission lines; and
� more complete coverage of the research litera-ture by online bibliographic databases.
As one researcher put it:
[Clinicians] need a system that is easy to use:computer terminals must be ubiquitous, systemresponse must be immediate (not seconds), nec-essary data should always be on-line, accessible,and confidential, and very little training shouldbe required.60
In addition, system down time must be at an ab-solute minimum, and data should be retained foras long as possible without diminishing system re-sponse times. Systems that meet all the needs ofclinicians may have to be developed in-houserather than adapted from commercial products.61
Standards DevelopmentThe issues regarding standards development dis-cussed in chapters 2 and 3 apply here as well.However, some additional aspects of these topicsand issues that apply to clinical decision supportrequire further discussion.
Messaging standardsAt first glance, it might appear that the develop-ment of messaging standards for electronic ex-change of information among disparate computersystems is less important in clinical decision sup-port than in other health care applications of ad-vanced information technologies, such aselectronic claims payment. Clinical decision sup-port is inherently localized—that is, specific to in-dividual providers—whereas electronic commerceinvolves transactions among providers and be-tween providers and other parties. Nevertheless,most patients receive care from more than oneprovider and from several departments within agiven organization. Thus, messaging standardsand common, unique patient and provider identi-fiers could facilitate patient record linkagethrough computer networks. (At the same time,standards for protecting patient and provider pri-vacy would need to be developed and enforced—see chapter 3.) Such standards could alsoencourage wider and faster dissemination of clini-cal protocols and local research results, and couldenable providers with different types of computersystems to access various central repositories ofmedical knowledge.
Clinical information contentIn theory, clinical decision support could alsobenefit from further development of standards forclinical information content—mainly commonmedical nomenclatures and uniform coding sys-tems for diagnoses, procedures, and test results—to help ensure that all needed information ispresent and accurate. Some analysts believe thedevelopment of a universal clinical nomenclatureand coding system is critical to the effective use ofinformation technology to improve the quality ofhealth care.62 However, developing a truly univer-
60 Wyatt, op. cit., footnote 41, p. 1682.
61 Ibid., p. 1685.62 M. Ackerman et al., “Standards for Medical Identifiers, Codes, and Messages Needed To Create an Efficient Computer-Stored Medical
Record,” Journal of the American Medical Informatics Association, vol. 1, No. 1, January./February 1994, pp. 1-7.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 137
sal system is a difficult task, given the wide varia-tion in existing systems and the intensity ofinstitutional commitment to those systems. In-deed, some analysts question whether a truly uni-versal system can ever be developed, contendingthat “terminology evolves in a context of use” thatcannot be supplanted.63 Instead, “vocabulariesneed to be constructed in a manner that preservesthe context of each discipline and ensures transla-tion between disciplines.”64 An alternative tocompiling enumerative systems that attempt tolist all possible terms in advance is a composition-al approach. Such systems use basic terms asbuilding blocks that can be combined in variousways to form higher level terms tailored to partic-ular applications and specialties.65
NLM has already made some progress in thisarea through the ongoing development of its Uni-fied Medical Language System (UMLS), which isbeing tested at about 500 sites.66 (Institutions andindividuals receive the software free of charge inexchange for testing it and commenting on it.) De-spite its name, UMLS is not in itself a unified clin-ical language; rather, it is more a means oftranslating among disparate clinical nomencla-tures. Its major purpose is to facilitate the retrievaland integration of biomedical information fromdisparate machine-readable sources by mappingand interpreting over 200,000 specific conceptsacross different classification systems, codingsystems, and controlled vocabularies (in which
only one term denotes each concept). The centralcomponent of the UMLS is a Metathesaurus thatessentially links synonyms from disparate vocab-ularies to a common term.
A separately developed Unified Nursing Lan-guage System (UNLS) is being incorporated intothe UMLS.67 A related NLM project is the Inte-grated Academic Information Management Sys-tem, which provides grants to academic medicalcenters for investigating communications and in-formation processing technologies. Thesetechnologies are designed to facilitate exchangeand interpretation of data among different com-puter systems, with the ultimate goal of develop-ing integrated health care information systems.68
One such effort is the Arden Syntax, a languagefor encoding and sharing medical knowledgebased largely on the HELP and RMRS systemsdescribed earlier.69 The syntax is organized intoseparate Medical Logic Modules (MLMs) thatcontain sufficient logic to make a single medicaldecision, running automatically in conjunctionwith a program known as an event monitor. Thesyntax offers the ability to query clinical data-bases, many of which have been found to be com-patible with the syntax. Six institutions areactively using the syntax, and three others are re-viewing it. MLMs have been used to generatealerts, interpretations, diagnoses, screening forclinical research, quality assurance functions, andadministrative support. However, they have not
63 Coiera, op. cit., footnote 22, p. 1384.64 P.F. Brennan, “On the Relevance of Discipline to Informatics,” Journal of the American Medical Informatics Association, vol. 1, No. 2,
Mar./Apr. 1994, p. 200.
65 Coiera, op. cit., footnote 22, p. 1385.66 D.A. Lindberg, B.L. Humphreys, and A.T. McCray, “The Unified Medical Language System,” Methods of Information in Medicine, vol.
32, No. 4, August 1993, pp. 281-291; A.T. McCray, Chief, Cognitive Sciences Branch, National Library of Medicine, personal communication,June 8, 1995.
67 K.A. McCormick et al., “Toward Standard Classification Schemes for Nursing Language: Recommendations of the American NursesAssociation Steering Committee on Databases To Support Clinical Nursing Practice,” Journal of the American Medical Informatics Associa-tion, vol. 1, No. 6, November/December 1994, pp. 421-427.
68 Coltin and Aronow, op. cit., footnote 2.69 Columbia-Presbyterian Medical Center, Arden Syntax home page on the World Wide Web <URL:http://www.cpmc.columbia.edu/ar-
den/>, 1995; T.A. Pryor and G. Hripcsak, “The Arden Syntax for Medical Logic Modules,” International Journal of Clinical Monitoring andComputing, vol. 10, No. 4, November 1993, pp. 215-224.

138 | Bringing Health Care Online: The Role of Information Technologies
been fully validated for clinical use, and not all ofthe ones developed are in active use. Nonetheless,the Arden Syntax has been adopted as a standardby the American Society for Testing and Materials(ASTM document E 1460).
Effectiveness and Safety of Clinical DecisionSupport Systems
EffectivenessEvidence regarding the effectiveness of CDSSs inimproving clinical processes and patient outcom-es is limited and mixed.70 One review of the de-velopment and evaluation of clinical data systemsfocused on “simple data systems” that do not offerclinical advice, but rather simply display informa-tion on the patient and/or the health problem.71 Itconcluded that these systems improve some clini-cal processes (accuracy of predictions of patientprogress, number or types of diagnostic tests or-dered, and completeness of data collection), butthat there is little evidence of improvement in pa-tient outcomes. Regarding data accuracy, the re-viewer noted:
If the system is not interactive, if data are col-lected largely for billing or administrative pur-poses, if coding staff are poorly instructed andtrained, and if clinicians are unaware of the sys-tem and do not monitor the data, inaccuracy willbe the rule. Reasons for data inaccuracy areoften organisational, not technical.72
Data completeness is improved when the sys-tem prompts the clinician or clerk for specific data
items. However, it is less clear whether paymentincentives improve data completeness, or whetherdata are more complete when a clinician entersthem directly rather than using encounter forms. Itis also unclear whether using computers saves cli-nician time; but even if it doesn’t, it will likely im-prove the quality of data.73
A recent review of systematic studies of the im-pact of CDSSs on clinician behavior and patientoutcomes found generally positive effects on cli-nician behavior, although this effect varied ac-cording to the type of application performed bythe CDSS.74 Three of four studies of CDSSs fordetermining the dose of toxic drugs reportedstatistically significant improvements in achiev-ing therapeutic levels. Four of six studies of pre-ventive care reminder systems found significantincreases in the performance of specific immu-nizations or screening tests. Seven of nine studiesof the impact of CDSSs on active medical care(e.g., adherence to a protocol for management ofhypertension) found significant positive effects.On the other hand, only one of five studies of com-puter-aided diagnosis found a significant im-provement in diagnostic accuracy. Moreover,only three of ten studies of the impact of CDSSson patient outcomes found significant effects fa-voring the use of a CDSS.
More recent studies also demonstrate themixed potential of CDSSs. One study found thatcomputer-based alerts of rising creatinine levels inhospitalized patients enabled clinicians to changemedications or dosages earlier, thereby decreas-
70 Wyatt, op. cit., footnote 41; M.E. Johnston et al., “Effects of Computer-based Clinical Decision Support Systems on Clinician Perfor-mance and Patient Outcome: A Critical Appraisal of Research,” Annals of Internal Medicine, vol. 120, No. 2, Jan. 15, 1994, pp. 135-142; D.M.Rind et al., “Effect of Computer-Based Alerts on the Treatment and Outcomes of Hospitalized Patients,” Archives of Internal Medicine, vol. 154,No. 13, July 11, 1994, pp. 1511-1517; E.S. Berner et al., “Performance of Four Computer-Based Diagnostic Systems,” New England Journal ofMedicine, vol. 330, No. 25, June 23, 1994, pp. 1792-1796; W.A. Knaus et al., “The SUPPORT Prognostic Model: Objective Estimates of Surviv-al for Seriously Ill Hospitalized Adults,” Annals of Internal Medicine, vol. 122, No. 3, Feb. 1, 1995, pp. 191-203.
71 Wyatt, op. cit., footnote 41, p. 1686.72 Ibid., p. 1684.73 Wyatt, op. cit., footnote 41, pp. 1684-1686.74 Johnston et al., op. cit., footnote 70.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 139
ing the risk of serious renal impairment by morethan half.75 The SUPPORT prognostic model (seeappendix C) predicted survival as well as did agroup of clinicians. However, incorporating theclinicians’ subjective estimates as predictors inthe model improved both its predictive accuracyand its ability to identify patients with high proba-bilities of survival or death.76
Using data describing 105 actual cases that dif-fered in their degree of diagnostic difficulty,another study evaluated the performance of fourgeneral diagnostic CDSSs: Dxplain, Iliad, Medi-tel, and QMR (see appendix C). The performanceof these systems on several measures of diagnos-tic accuracy was compared to diagnoses deter-mined by group consensus among 10 clinicalexperts. No single system consistently scored bet-ter than the others on all performance measures. Amajority of the diagnoses that the systems listedwere correct (or closely related to the correct diag-nosis), but the correct diagnosis usually did notappear in the top five diagnoses listed by the sys-tems. Moreover, far less than a majority of thediagnoses they listed were considered relevant.On average, they listed less than half of the diag-noses identified by the expert clinicians, but theylisted about two additional relevant diagnoses notoriginally identified by the clinicians. These re-sults emphasize the potential usefulness ofCDSSs in reminding clinicians of overlooked al-ternatives, but also the importance of clinician ex-perience and judgment in interpreting andfiltering information.77
SafetyCDSSs, particularly computer-based clinical pro-tocols, may reduce inappropriate practice varia-tions and improve patient outcomes. Yet it ispossible that the most successful CDSSs could be-come viewed as rigid sets of rules for diagnosingand/or treating particular health problems. Clini-cians might then become overly dependent onthem, adhering to the recommended steps withoutquestion or independent investigation, and allow-ing their own knowledge, skill, and judgment toerode as a result.78 Alternatively, systems thatprovide too many simultaneous streams of in-formation could cause information overload,prompting clinicians either to focus on certainitems and neglect other important tasks, or to shunall such information .79
Any of these developments could adversely af-fect the quality of patient care and undermine theinterpersonal aspects of patient care (the “qualityof caring”).80 Indeed, there are indications that pa-tients find clinicians less communicative whenusing computers to enter patient data. Cliniciansthemselves mainly fear that computers mightthreaten patient and provider privacy, create legalor ethical problems, increase government controlof health care, or rely on out-of-date knowledge.81
CDSSs are only as good as the medical knowl-edge on which they are based. Due to methodolog-ical errors in the research underlying a CDSS or tosubstantive misinterpretation of research results, aCDSS may contain incorrect parameters or deci-sion criteria or may overlook crucial steps in the
75 Rind et al., op. cit., footnote 70.
76 Knaus et al., op. cit., footnote 70.77 Berner et al., op. cit., footnote 70.78 D. DeMoro, Director, Health Care Professions Council, Service Employees International Union Local 250, Oakland, CA, personal com-
munication, Mar. 29, 1995.
79 D.M. Rind, R. Davis, and C. Safran, “Designing Studies of Computer-Based Alerts and Reminders,” M.D. Computing, vol. 12, No. 2,
Mar.-Apr. 1995, p. 125.
80 DeMoro, op. cit., footnote 78.81 Wyatt, op. cit., footnote 41, p. 1684

140 | Bringing Health Care Online: The Role of Information Technologies
A patient in the Intensive Care Unit at IDS Hospital in Salt Lake City Utah, is monitored by computer-controlled devices that helpclinicians observe the patient's condition and alert them to unfavorable trends.
diagnosis or treatment of a given health problem.It could thus mislead a clinician into making deci-sions that harm patients. One observer points outthat the vast amounts of information that comput-ers can process at lightning speed can make itvirtually impossible for humans to verify that theresults are correct. He recommends that:■ clinicians have substantial input into the design
and development of a clinical information sys-tem,
■ the limitations of the system be clearly spelledout to the user, and
■ the system itself be designed to explain to theuser exactly what it is doing as it is beingused.82
Assessing Clinical Decision Support SystemsSome analysts have called for rigorous evaluationof the effectiveness and safety of clinical informa-tion systems.83 However, there seems to be littlesentiment for mandatory testing and certificationof such systems by government authorities. Re-gardless, CDSSs should be used with caution, andthey should be carefully assessed regarding their
82 M.F. Smith, "Are Clinical Information Systems Safe? Clinicians Should Give More Attention to Possible Failures in Their Computer
Systems,” British Medical Journal, vol. 308, No. 6929, Mar. 5, 1994, p. 612.83 Wyatt, op. cit., footnote 41; Rind, Davis, and Safran, op. cit., footnote 79; R. Wall, “Computer Rx: More Harm Than Good?” Journal of
Medical Systems, vol. 15, Nos. 5/6, December 1991, pp. 321-334; L.I.. Iezzoni, “ ‘Black Box’ Medical Information Systems: A Technology
Needing Assessment,’’ Journal of the American Medical Association, vol. 265, No. 22, June 12, 1991, pp. 3006-3007.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 141
effectiveness and safety—by their developers andusers, and perhaps by payers and accrediting bod-ies, if not by the government. As one researcherput it:
Clinicians should try to judge the claims ofthese newcomers in the same cautious way thatthey would examine claims about a new drug.84
As pointed out in chapter 2, the U.S. Food andDrug Administration (FDA) already regulatesmedical software as medical devices. Currentpolicy85 exempts from regulation any softwarethat is either:
1. general in purpose (e.g., database managementsystems or library systems for storing, retriev-ing, or disseminating health care information);
2. used in education or nonclinical research, oronly in the practice of the provider (practitioneror institution) that developed it (i.e., withoutbeing disseminated further); or
3. a knowledge-based decision support systemthat is “intended to involve competent humanintervention before any impact on humanhealth occurs (e.g., where clinical judgmentand experience can be used to check and inter-pret a system’s output).”86
In its definition of research software, the FDAintends to include software that is distributed freeof charge in source-code form so that it can be ex-amined by other researchers.87 (Commercial soft-ware must be distributed as object code that is
designed to be read only by particular computers,and is thus very difficult for humans to alter.)
In the case of “home-grown” software that isnot distributed beyond the originating institution,and if the institution conducts research using fed-eral government funds, then the use of such soft-ware on human subjects is regulated by the localInstitutional Review Board.88 There are apparent-ly no restrictions on the development and use ofhome-grown software in institutions that do notconduct federally sponsored research, or amongpractitioners in private practice. Yet these sys-tems, too, could mislead clinicians into makingdecisions that might harm patients. The issue iswhether the FDA should review and/or repeal anyof the exemptions listed above.
It can be argued that regulation of clinical deci-sionmaking is not within the FDA’s purview, andthat other public and private sector mechanisms,such as the malpractice system and managed care,can adequately perform that function. Further, theeffectiveness and safety of clinical informationsystems could be assessed by private sector orga-nizations, such as payers or professional societies.On the other hand, those organizations may not becapable of performing such assessments, or ofconducting research on the best methods of doingso.
Assessment of CDSSs can include randomizedcontrolled trials in which the health outcomes ofpatients treated with the aid of a CDSS are
84 Coiera, op. cit., footnote 22, p. 1381.85 This policy is based on a draft statement published on Nov. 13, 1989 (see footnote 86) that has yet to be formally implemented. The FDA
has used this draft statement as a basis for determining the applicability of the medical device regulations to specific software products on acase-by-case basis. The agency is in the process of developing formal regulations in this area. H. Rudolph, Acting Director, Office of Scienceand Technology, Center for Devices and Radiological Health, U.S. Food and Drug Administration, personal communication, June 30, 1995.
86 U.S. Department of Health and Human Services, Food and Drug Administration, Center for Devices and Radiological Health, Office ofDevice Evaluation, “Reviewer Guidance for Computer Controlled Medical Devices Undergoing 510(k) Review” (Rockville, MD: Aug. 29,1991), pp. 37-40.
87 This new criterion for identifying research software was adopted partly in response to the case involving a radiotherapy dosing product
(see chapter 2, footnote 47). Rudolph, op. cit., footnote 85.
88 Ibid. Each provider institution that conducts research using federal government funds is required to establish an Institutional Review
Board, largely to ensure that required procedures regarding treatment of human subjects—mainly informed consent—are followed.

142 | Bringing Health Care Online: The Role of Information Technologies
compared with those treated by conventionalmethods.89 However, numerous complicationscan hamper such trials.90 In particular, imple-menting a CDSS may engender other changes inpractice patterns (e.g., teamwork, consultation,training, and altered role relationships) that aremore directly responsible for any observedchanges in patient outcomes than is the CDSS it-self.
Moreover, random assignment of patients orclinical staff to comparison groups may not be fea-sible here.91 If only patients are randomized intothe comparison groups (with the CDSS beingused in one group and not in the other), then clini-cal staff may carry over CDSS-induced changes inpractice patterns from the treatment group to thecontrol group. Yet randomizing staff into the com-parison groups can disrupt teamwork and alienateone staff group or the other (e.g., new burdens forthe treatment-group staff or feelings of exclusionfor the control-group staff). Another approach isto randomize entire staff teams or departments, al-though such clustering requires much larger sam-ples to maintain precision of estimates. Thisapproach is similar to the method of the firms trialin clinical research in which patients are randomlyassigned to similar (parallel) providers who usedifferent treatments, rather than to differentgroups that receive different treatments from thesame provider.92
At a minimum, CDSSs appear to help preventclinicians from neglecting or altering basic stepsin specific processes of care. However, it will be along time before CDSSs cover every contingencyin those processes, even for highly specific healthproblems. Despite the vagaries of clinician experi-ence, memory, and judgment, these will continue
to be essential elements of clinical decisionmak-ing. As randomized controlled trials and otherforms of effectiveness research increase knowl-edge regarding which health services truly “work”for a given health problem, marked deviationsfrom established standards of practice will be-come less justifiable. However, there will contin-ue to be room for variation in the judgmentalapplication of those standards to individual pa-tients in particular settings and locations. CDSSsmust continue to be viewed as aids to clinician ex-perience and judgment, rather than as substitutesfor them; and clinicians must retain the ability tooverride the recommendations of CDSSs. At thesame time, clinicians should also be required todocument the reasons for those decisions so thatthe CDSSs can be improved over time.
PERFORMANCE ASSESSMENT
❚ Comparison to Clinical DecisionSupport
A less direct approach to improving the quality ofhealth care is assessing the performance of provid-ers and health insurance plans.93 This approachseeks to:
� evaluate the performance of providers or plansin delivering health services to patients,
� give providers or plans feedback on their per-formance to help them improve, and
� give performance information to payers, pur-chasers, and consumers to help them select pro-viders and plans.
Performance measures can focus on several as-pects of patient care. Two of the more importantones are: 1) the use of specific services that areconsidered to be appropriate for a given health
89 Johnston et al., op. cit., footnote 70; Smith, op. cit., footnote 82; Wall, op. cit., footnote 83; J. Wyatt and D. Spiegelhalter, “Evaluating
Medical Expert Systems: What To Test and How?” Medical Informatics, vol. 15, No. 3, July-Sept. 1990, pp. 205-217.
90 Wyatt, op. cit., footnote 41; Rind, Davis, and Safran, op. cit., footnote 79.91 Ibid.
92 U.S. Congress, Office of Technology Assessment, Identifying Health Technologies That Work, op. cit., footnote 12, pp. 57-58.93 This approach focuses mainly on providers. Even assessing the performance of insurance plans involves, in part, assessing the perfor-
mance of the providers employed or contracted by those plans.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 143
problem, and 2) patient outcomes of those ser-vices, usually measured by adverse events such asdeaths, complications, and readmissions. In thisrespect, the kinds of information needed to assessproviders or plans are similar to those needed forclinical decision support: detailed informationabout individual patients and their health prob-lems, and the specific health services that individ-ual providers (clinicians or institutions) use todiagnose, treat, or prevent those problems. Thekinds of technologies required to generate and uti-lize that information are also similar.
Although, in theory, they should have no bear-ing on clinical decisionmaking, certain additionalfactors (beyond those minimally needed for clini-cal decision support) may also influence clini-cians’ choices of services and affect patientoutcomes.94 These include the patient’s socioeco-nomic status, social supports (marital status, liv-ing arrangements, etc.), and type of healthinsurance (e.g., indemnity, prepaid, public, oruninsured). These factors need to be considered inassessing provider and plan performance, and per-haps in clinical decision support as well. In addi-tion, the more subjective aspects of the careprocess, such as patient satisfaction with thehealth services they receive or with various fea-tures of insurance plans, are apparently of greaterinterest in performance assessment than in clinicaldecision support—at least at present.
In examining the link between processes andoutcomes, performance assessment usually fo-cuses on adverse outcomes that result from ser-vices already rendered, thus helping to identify
processes that need correcting. In contrast, clini-cal decision support focuses on selecting servicesin advance that are likely to maximize favorableoutcomes and minimize adverse ones. In both ap-proaches, patient risk factors condition the rela-tionship between processes and outcomes.
❚ Relationship to Other Recent TrendsThe performance assessment approach to qualityimprovement fits with recent trends toward man-aged care and increased competition amongproviders and insurance plans.95 Traditional in-demnity insurance and fee-for-service reimburse-ment are seen as creating incentives for providersto overuse health services in order to maximize in-come. Thus, one goal of performance assessmentis to reduce “unnecessary” services, thereby re-straining the escalation of health care costs.
On the other hand, managed care—particularlyprepayment for health services—is seen as creat-ing incentives for providers to keep costs lowerthan the prepayment amount. One way to do this isto reduce the volume and intensity of services de-livered to patients. If this leads to underuse of ser-vices that are “necessary” for the diagnosis,treatment, or prevention of a given health prob-lem, then patients’ health status could be adverse-ly affected. Thus, another goal of performanceassessment is to monitor patient outcomes andrates of use of services that are presumed to im-prove those outcomes.
The performance assessment approach as-sumes that giving providers feedback on their per-
94 J.S. Feinstein, “The Relationship Between Socioeconomic Status and Health: A Review of the Literature,” The Milbank Quarterly, vol.71, No. 2, 1993, pp. 279-322; N.E. Adler et al., “Socioeconomic Inequalities in Health: No Easy Solution,” Journal of the American MedicalAssociation, vol. 269, No. 24, June 23/30, 1993, pp. 3140-3145; H.R. Burstin, S.R. Lipsitz, and T.A. Brennan, “Socioeconomic Status and Riskfor Substandard Medical Care,” Journal of the American Medical Association, vol. 268, No. 17, Nov. 4, 1992, pp. 2383-2387; J. Hadley, E.P.Steinberg, and J. Feder, “Comparison of Uninsured and Privately Insured Hospital Patients: Condition on Admission, Resource Use, and Out-come,” Journal of the American Medical Association, vol. 265, No. 3, Jan. 16, 1991, pp. 374-379.
95 See R. Lavizzo-Mourey, “Measuring Quality in Health Care Reform,” Journal of Health Care for the Poor and Underserved, vol. 5, No.3, 1994, pp. 202-211; J.E. Sisk and S.A. Glied, “Innovation Under Federal Health Care Reform,” Health Affairs, vol. 13, No. 3, summer 1994,pp. 82-97; Health Care Quality Alliance, Quality Considerations: An Analysis of Federal Health Care Reform Plans (Washington, DC: HealthCare Quality Alliance, July 1994); C. Anderson, “Measuring What Works in Health Care,” Science, vol. 263, No. 25, Feb. 25, 1994, pp.1080-1082.

144 | Bringing Health Care Online: The Role of Information Technologies
formance in terms of patient outcomes encouragesthem to improve their processes of care by select-ing the most effective services for a given healthproblem. Identification and correction of prob-lems in production processes is one major compo-nent of CQI in manufacturing, an approach thatwas subsequently adapted to the health care indus-try. More recently, managed care organizationsand even pharmaceutical companies have soughtto adapt the CQI approach to the management ofspecific chronic, costly health problems, such asdiabetes, asthma, and high blood pressure, acrossall care settings. In part, this approach, known asdisease management, involves practice guide-lines, outcomes measurement, and feedback toproviders and insurance plans.96 At the same time,employers and health plans have sought to dealwith the rising cost of pharmaceuticals throughpharmacy benefit management, which employstechniques of disease management as well aspharmacy networks, negotiated discounts and re-bates, lists of preferred drugs, and online utiliza-tion review.97
All of these related approaches rest on the fol-lowing series of assumptions. The most effectiveservices also tend to be the most cost-effectiveones because, even if they cost more to provide,their positive impact on patient health status leadsto reduced use and cost of services in the long run.Thus, giving providers feedback on their perfor-mance both improves the quality and reduces thecost of health care. In addition, distributing per-formance information to payers, purchasers, andconsumers helps them choose providers that
employ the most cost-effective services for a giv-en health problem. Moreover, if sufficient num-bers of payers, purchasers, and consumers useonly those providers that employ the most cost-ef-fective services, then this forces all providers touse those services and to reduce the prices of thoseservices. This increased competition among pro-viders induces further improvements in the quali-ty of health care and reductions in its cost.
❚ Performance Indicator Projects (ReportCards)
In recent years, various groups have sought to de-velop summary sets of performance indicatorscommonly called report cards.98 Assessments us-ing such indicators are designed to:
1. help consumers, payers, and self-insured pur-chasers compare and select among providers;
2. help consumers and purchasers select amonginsurance plans; or
3. give performance information to accreditationbodies for providers or insurance plans.
They can also be used to provide feedback toproviders for quality improvement purposes, andto assist public policy makers in regulating plansand formulating health policy.99 In addition, pro-viders and insurance plans often tout performanceindicator projects or favorable results in their mar-keting efforts; others respond by trying to makeprocess changes that will improve their scores onperformance indicators.100 However, systematicevidence regarding the impact of performance in-
96 K. Terry, “Disease Management: Continuous Health-Care Improvement,” Business and Health, April 1995, pp. 64-72; G. Anders, “Drug
Makers Help Manage Patient Care,” Wall Street Journal, May 17, 1995, p. B1.
97 L. Etheredge, Pharmacy Benefit Management: The Right Rx? Briefing Paper, Health Insurance Project, The George Washington Univer-
sity, April 1995.
98 For a critical appraisal of performance indicator projects, see A. Epstein, “Performance Reports on Quality—Prototypes, Problems, and
Prospects,” Journal of the American Medical Association, vol. 333, No. 1, July 6, 1995, pp. 57-61.
99 U.S. Congress, General Accounting Office, Health Care Reform: “Report Cards” Are Useful but Significant Issues Need To Be Ad-dressed, GAO/HEHS-94-219 (Washington, DC: September 1994); J. Mangano, “Report Cards Come of Age,” 1995 Medical Quality Manage-ment Sourcebook, K.J. Migdail and M. Youngs (eds.) (New York, NY: Faulkner & Gray, 1994), pp. 1-21.
100 L. Oberman, “How Do Health Plans Perform?” American Medical News, Mar. 20, 1995, pp. 1, 30.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 145
dicator projects on provider or plan behavior islacking.
Perhaps the earliest and best-known perfor-mance indicator project was the effort by HCFA toassess mortality rates among Medicare patients inevery hospital in the nation. Reports were releasedannually to the public beginning in 1986, but weresuspended in 1993 due, in part, to criticism ofHCFA’s methodology,101 particularly regardingrisk adjustment.102 As a supplement to its PeerReview Organization program of quality assur-ance, HCFA is developing a new set of perfor-mance indicators for ambulatory care, known asDeveloping and Evaluating Methods to PromoteAmbulatory Care Quality (DEMPAQ).103 Anoth-er government project is the U.S. Public HealthService’s Year 2000 Health Objectives for the Na-tion, comprised of population-based measures ofhealth promotion and disease prevention, such asinfant mortality rates.104
In the private sector, the National Committeefor Quality Assurance (NCQA) developed theHealth Plan Employer Data and Information Set(HEDIS) as part of its oversight of health insur-ance plans (largely managed care organiza-tions).105 Box 4-1 summarizes the measures usedin HEDIS. Like many performance indicator proj-ects, the HEDIS measures focus on processes of
care, that is, utilization of presumably appropriateservices among certain groups of plan members,and the accessibility or availability of those ser-vices. Of the HEDIS “quality of care” measures,only hospitalization for asthma and low birthweight represent patient outcomes. Moreover,none of the HEDIS measures is adjusted for mem-ber or patient risk factors. HCFA is in the processof adapting the HEDIS model to its Medicare andMedicaid programs.106
In 1994, NCQA conducted a one-year pilottest of 28 of the HEDIS measures using datafrom 21 health plans throughout the United States.(The pilot study also included a survey of enrolleesatisfaction with health plan performance.) TheHEDIS pilot data from each participating planwere audited for reliability and comparability byan independent firm. Each audit involved a reviewof the overall structure of the plan’s data collectionand processing procedures; a site visit to the planby an audit team; verification of the plan’s sourcecode and specifications; and validation of theplan’s measures and data. The pilot study identi-fied needs for additional quality measures in keyclinical areas (e.g., mental health), risk adjust-ment, field testing, improved standardization ofdata collection procedures, investment in en-hanced clinical information systems, refinement
101 U.S. Congress, General Accounting Office, op. cit., footnote 99; S.T. Fleming, L.L. Hicks, and R.C. Bailey, “Interpreting the Health Care
Financing Administration’s Mortality Statistics,” Medical Care, vol. 33, No. 2, February 1995, pp. 186-201.
102 Risk adjustment is statistical control of patient risk factors in the analysis of the utilization and outcomes of health services. The term alsorefers to control of financial risk factors faced by insurance companies. See L.I. Iezzoni, “Risk Adjustment for Medical Outcome Studies,”Medical Effectiveness Research Data Methods, M.L. Grady, and H.A. Schwartz (eds.), Agency for Health Care Policy and Research, AHCPRPub. No. 92-0056 (Rockville, MD: July 1992), pp. 83-97.
103 Delmarva Foundation for Medical Care, Inc., Developing and Evaluating Methods to Promote Ambulatory Care Quality, Final Report
(Washington, DC: August 1994), pp. 1-6.
104 U.S. Department of Health and Human Services, Public Health Service, Healthy People 2000: National Health Promotion and Disease
Prevention Objectives, DHHS Pub. No. (PHS) 91-50212 (Washington, DC: U.S. Government Printing Office, 1991).
105 National Committee for Quality Assurance, Health Employer Data and Information Set and Users’ Manual, Version 2.0 (Washington,
DC: 1993); National Committee for Quality Assurance, HEDIS 2.5: Updated Specifications for HEDIS 2.0 (Washington, DC: January 1995).
106 “HCFA, Outside Groups to Adapt HEDIS for Use in Medicare, Medicaid Programs,” BNA’s Health Care Policy Report, Mar. 27, 1995,
pp. 479-480.

146 Bringing Health Care Online: The Role of Information Technologies
QUALITY OF CARE
Childhood Immunization Rate: Proportion of children who had received specified Immunizations as of
their second birthday.
Cholesterol Screening: Proportion of adults aged 40 to 64 who received a cholesterol test during the
past five years.
Mammography Screening: Proportion of women aged 52 to 64 who received one or more mammo-
grams during the past two years
Cervical Cancer Screening: Proportion of women aged 21 to 64 who received one or more Pap tests
for cervical cancer during the past three years
Low Birthweight: Proportion of all Iive births that were low birthweight (under 2,500 grams) or very low
birthweight (under 1,500 grams) during the past year.
Prenatal Care in First Trimester: Proportion of women with one or more Iive births during the past year
who had one or more prenatal care visits 26 to 44 weeks prior to delivery,
Asthma Inpatient Admission Rate: Proportion of members aged 2 to 19 (or 20 to 39) who had one ormore inpatient discharges with a principal diagnosis of asthma within the past year, also, of those mem-
bers with such discharges, the proportion who had more than one such discharge.
Diabetic Retinal Exam: Proportion of members aged 31 to 64 with diabetes (i.e., who were dispensed
insulin or oral hypoglycemics) who received a retinal ophthalmoscopic examination during the past
year.
Ambulatory Follow-Up After Hospitalization for Major Affective Disorder: Proportion of members
aged 18 to 64 with an Inpatient discharge for major affective disorder during the past year who had one
or more ambulatory mental health encounters or day/night treatments within 30 days of discharge.
1 The listed measures are used in the set of performance measures for health insurance plans known as the Health Plan Employer
Data and Information Set (HEDIS), Version 25 HEDIS was developed by the National Committee for Quality Assurance (NCQA) as
part of its oversight of managed care plans The categories and titles of the measures are drawn from the NCQA manual, HED/S25
Updated Specifications for HEDIS 20 (Washington, DC January 1995) The descriptions of the measures are OTA summaries of the
detailed specifications presented in that manual. All measures are based on plan members who were continuously enrolled in the plan
during the specified time period. A plan IS a health insurance plan, a member IS a person who is enrolled in the plan
(continued)
of audit procedures, and more research on the crediting hospitals and other institutionalkinds of information consumers need. 107 providers. Implementation of the IMSystem be-
Another performance indicator project is the gan in 1994, starting with voluntary participationIndicator Measurement System (IMSystem) de- by hospitals that could generate the necessaryveloped by the Joint Commission on Accredita- data. 108 Box 4-2 summarizes the measures used intion of Healthcare Organizations, as part of its the IMSystem, which are about equally divided“Agenda for Change” to adopt specific outcome- between process and outcome measures.oriented measures to support the process of ac-
107 National Committee for Quality Assurance, Executive Summary for Report Card Pilot Project (Washington, DC: 1995), PP. 1-6.108 Joint Commission on Accreditation of Healthcare Organizations, IMSystem General Information (Oakbrook Terrace, IL: 1994), PP. 3-6.

Chapter 4 Using Information Technology To Improve the Quality of Health Care 1147
OTHER MEASURES2
Access to Health Services: The proportion of adult members who had one or more provider visits dur-ing the past three years, the proportion of primary care physicians accepting additional members, and
average waiting time for a primary care provider appointment.
Member Satisfaction: The proportion of members who are satisfied with the plan, and the percentage
of members of who rate the plan as good, very good, or excellent
Membership: Total number of member years, and the proportion of members who disenroll from theplan (including those who die), by type of plan health maintenance organization, preferred provider
organization, or point of service/other.
Utilization: Average length of inpatient stay, the number inpatient discharges per 1,000 member years
and the number of inpatient days per 1,000 member years.
Finance: Average revenue per member per month, the percentage change in average revenue, theloss ratio (percentage of total premiums devoted to expenses), the number of years in business, net
income (revenue minus expenses), and net worth (assets minus Iiabilities).
Health Plan Management and Activities: The percentage of primary care physicians who are board
certified, the percentage of specialist physicians who are board certified, and the percentage of prima-ry care physicians who left the plan
SOURCE: U S Congress, Office of Technology Assessment, 1995, based on National Committee for Quality Assurance, HEDIS 25Updated Specifications for HEDIS 20 (Washington DC January 1995)
2These are examples of measures Iisted under categories other than Quality of Care in the HEDIS 25 manual
The IMSystem also adjusts for patient risk fac-tors (demographic traits, complicating healthproblems, etc.) by developing an outcome predic-tion model for each performance measure. Eachmodel is based on risk factors that contribute sig-nificantly to the prediction of that performancemeasure. Using a given model, each institution’sactual sore on the performance measure iscompared to its predicted score. 109 Institutionsthat score “worse” than predicted can then investi-gate the reasons behind those results. IMSystemreports are available to consumers for $30 per hos -pital. l10
109 Ibid., pp. 16-18.
Performance indicator projects are also beingconducted by several managed care organizations.employer coalitions, and state governments, someusing the HEDIS model. Examples include:United HealthCare Corp. (a national managedcare organization); the Massachusetts HealthcarePurchaser Group (an employer coalition); and thestates of California, Florida, New York, and Penn-sylvania. l11 Moreover, several legislative propos-
als for national health reform, including theClinton Administration’s 1994 plan, have con-tained mandates for the development of such indi -
110 “JCAHO Releases Data, Gets Blasted by AHA and AMA,” Business and Health, January 1995, p. 16.111 U.S. Congress, General Accounting Office, op. cit., footnote 99; S. Vibbert et al. (eds. ), The Medical Outcomes & Guidelines Sourcebook
(New York, NY: Faulkner& Gray, 1994); K.J. Migdail and M. Youngs (eds.), 1995 Medical Quality Management Sourcebook (New York, NY.Faulkner & Gray, 1994).
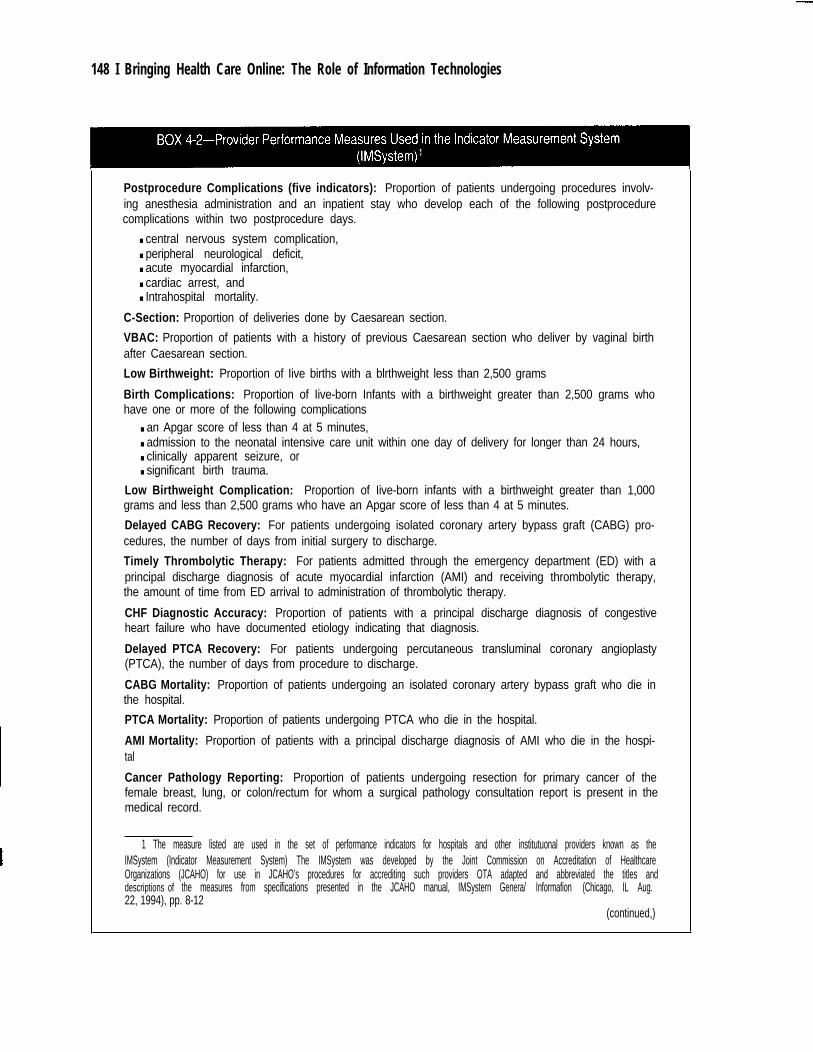
148 I Bringing Health Care Online: The Role of Information Technologies
Postprocedure Complications (five indicators): Proportion of patients undergoing procedures involv-ing anesthesia administration and an inpatient stay who develop each of the following postprocedurecomplications within two postprocedure days.
■ central nervous system complication,■ peripheral neurological deficit,■ acute myocardial infarction,■ cardiac arrest, and■ Intrahospital mortality.
C-Section: Proportion of deliveries done by Caesarean section.
VBAC: Proportion of patients with a history of previous Caesarean section who deliver by vaginal birthafter Caesarean section.
Low Birthweight: Proportion of Iive births with a blrthweight less than 2,500 grams
Birth Complications: Proportion of Iive-born Infants with a birthweight greater than 2,500 grams whohave one or more of the following complications
■ an Apgar score of less than 4 at 5 minutes,■ admission to the neonatal intensive care unit within one day of delivery for longer than 24 hours,■ clinically apparent seizure, or■ significant birth trauma.
Low Birthweight Complication: Proportion of Iive-born infants with a birthweight greater than 1,000grams and less than 2,500 grams who have an Apgar score of less than 4 at 5 minutes.
Delayed CABG Recovery: For patients undergoing isolated coronary artery bypass graft (CABG) pro-cedures, the number of days from initial surgery to discharge.
Timely Thrombolytic Therapy: For patients admitted through the emergency department (ED) with aprincipal discharge diagnosis of acute myocardial infarction (AMI) and receiving thrombolytic therapy,the amount of time from ED arrival to administration of thrombolytic therapy.
CHF Diagnostic Accuracy: Proportion of patients with a principal discharge diagnosis of congestiveheart failure who have documented etiology indicating that diagnosis.
Delayed PTCA Recovery: For patients undergoing percutaneous transluminal coronary angioplasty(PTCA), the number of days from procedure to discharge.
CABG Mortality: Proportion of patients undergoing an isolated coronary artery bypass graft who die inthe hospital.
PTCA Mortality: Proportion of patients undergoing PTCA who die in the hospital.
AMI Mortality: Proportion of patients with a principal discharge diagnosis of AMI who die in the hospi-tal
Cancer Pathology Reporting: Proportion of patients undergoing resection for primary cancer of thefemale breast, lung, or colon/rectum for whom a surgical pathology consultation report is present in themedical record.
1 The measure listed are used in the set of performance indicators for hospitals and other institutuonal providers known as theIMSystem (Indicator Measurement System) The IMSystem was developed by the Joint Commission on Accreditation of HealthcareOrganizations (JCAHO) for use in JCAHO’s procedures for accrediting such providers OTA adapted and abbreviated the titles anddescriptions of the measures from specifications presented in the JCAHO manual, IMSystern Genera/ Informafion (Chicago, IL Aug.22, 1994), pp. 8-12
(continued,)

Chapter 4 Using Information Technology To Improve the Quality of Health Care 1149
Tumor Staging: Proportion of patients undergoing resection for primary cancer of the female breast,
lung, or colon/rectum who have stage of tumor designated by a managing physician.
Breast Cancer Testing: Proportion of female patients with Stage I or greater primary breast cancer
undergoing initial biopsy or resection who have estrogen receptor analysts results in the medical re-
cord
Lung Cancer Diagnosis/Staging: Proportion of patients with non-small cell primary lung cancer under-
going thoracotomy who have complete surgical resection of tumor.
Colon/Rectum Cancer Preoperative Evaluation: Proportion of patients undergoing resection for pri-mary cancer of the colon/rectum whose preoperative evaluation by a managing physician included ex-
amination of the entire colon.
Trauma Monitoring: Proportion of trauma patients with systolic blood pressure, pulse rate, and respira-
tory rate documented on arrival in the ED and at least hourly for three hours or until ED disposition,whichever IS earner
Head Trauma Monitoring: Proportion of trauma patients with selected intracranial injuries who have a
Glasgow coma scale score documented on arrival in the ED and at least hourly for three hours or untilED disposition, whichever IS earner.
Airway Management for Comatose Trauma: Proportion of ED comatose trauma patients with selectedIntracranial Injuries who are discharged from the ED prior to endotracheal intubation or cricothyrotomy
Timely CT Scans: For patients undergoing computerized tomography (CT) scan of the head, the
amount of time from emergency department arrival to initial CT scan.
Timely Neurological Procedures: For patients undergoing selected neurosurgical procedures, the
amount of time from emergency department arrival to procedure.
Timely Orthopedic Procedures: For patients undergoing selected orthopedic procedures, the amount
of time from emergency department arrival to procedure.
Timely Abdominal Procedures: For trauma patients undergoing selected abdominal surgical proce-
dures, the amount of time from emergency department arrival to procedure.
Preventable Death from Pneumothorax/Hemothorax: Proportion of patients who die in the hospital
with a diagnosis of pneumothorax or hemothorax who did not undergo a thoracostomy or thoracotomy.
Preventable Death among Trauma Patients: Proportion of trauma patients with a systolic blood pres-
sure of less than 70 mm Hg within two hours of ED arrival who die in the hospital without undergoing a
Iaparotomy or thoracotomy.
SOURCE: U.S. Congress, Office of Technology Assessment, 1995, based on Joint Commission on Accreditation of Healthcare Orga-nizations, IMSystem General Information (Chicago, IL Aug 22, 1994)
caters to be used in assessing all providers and magazine called Health Pages that reports on theinsurance plans. Private, for-profit companies services and prices of physicians, hospitals, andhave also entered the market for performance in- managed care plans in several cities for $3.95 performation, producing reports for sale to the gener- issue. 112
al public. A prominent example is a consumer

150 | Bringing Health Care Online: The Role of Information Technologies
In January 1995, a private, for-profit data anal-ysis firm published a performance report on 10hospitals in Orange County, California, using raw,unadjusted Medicare billing data to measuremortality rates for coronary artery bypass graftsurgery. The $10 purchase price of the report waspartially subsidized by an undisclosed subscrip-tion fee from the study’s top-ranking hospital,which used the results in newspaper advertising.While this case prompted some observers to callfor regulation of performance measurement meth-ods and reporting—by the industry itself, if not bythe government—others expressed confidencethat “the market will eventually sort itself out.”113
❚ Information Technology andPerformance Assessment
Advanced information technologies could con-tribute to performance assessment in health carein two main ways. One is improving the measuresand data on which those assessments are based.The second is making the results of those assess-ments, and the measures and data on which theyare based, more readily accessible to payers, pur-chasers, consumers, and researchers.
By its very nature, performance assessment re-views past performance, and thus cannot feasiblyemploy clinical trials and other forms of prospec-tive analysis. Performance assessment thus em-ploys retrospective analysis that involves eitherprimary data collection or secondary analysis ofavailable administrative data, or both (as with theHEDIS and IMSystem measures). Primary dataare collected mainly through: 1) clinician reviewsof paper-based patient records, and 2) surveys ofpatients and providers. Administrative data in-clude hospital discharge abstracts, and health in-surance claims or encounter records andenrollment records. Each of these data sources has
certain limitations that advanced informationtechnologies might help overcome.
Given current information technologies andanalytic methods, tradeoffs exist between primaryand secondary data for assessing provider andplan performance. A balance must be soughtamong several considerations: 1) the clinical de-tail of the information that can be gathered, 2) thenumber of patients that can be included, 3) the costper unit of information gathered, and 4) theamount of time required to obtain and clean thedata. Larger numbers of patients enhance the pre-cision of statistical estimates, and clinical detail isessential in statistical control for confoundingvariables—particularly patient risk factors—thatcould affect the provider’s choice of services orthe patient’s outcome.
In general, administrative data can cover verylarge numbers of patients at very low cost to theanalyst and can be obtained relatively quickly.(The time and expense of collecting such datahave already been absorbed by administrativeprocesses.) However, they can cover only themore objective measures of care processes (e.g.,the proportion of diabetics receiving an annual ret-inal examination) and patient outcomes (e.g., theproportion of births with low birth weight). More-over, administrative data contain very little clini-cal detail to support process and outcomemeasures.114
In contrast, primary data collection can covermore subjective measures (e.g., appropriatenessof a procedure, patient satisfaction with the carereceived, patient self-perception of health statusand quality of life, etc.) as well as several of themore objective ones. Moreover, it can obtain richdetail on those measures: clinical detail, in thecase of patient record review; and perceptual/atti-tudinal detail, in the case of surveys. However,
113 “Bypass Surgery Report Ignites Uproar Among Calif. Hospitals,” Report on Medical Guidelines & Outcomes Research, Jan. 26, 1995,
pp. 1, 2, and 12.
114 J.G. Jollis et al., “Discordance of Databases Designed for Claims Payment versus Clinical Information Systems: Implications for Out-
comes Research,” Annals of Internal Medicine, vol. 119, No. 8, Oct. 15, 1993, pp. 844-850.

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 151
such data are collected at much greater cost in bothtime and money; so they are usually gathered onfar fewer patients, thereby reducing the precisionof statistical estimates. Ideally, all measureswould be obtained in complete clinical detail onvery large numbers of patients very quickly and atvery low cost. This is precisely the vision offeredby advanced information technologies.
A major limitation of readily available admin-istrative data is the absence of measures of variousconfounding factors that may affect a provider’schoice of services or a patient’s outcome, and thusdistort the true effects of the processes of care be-ing evaluated. The most important confoundingvariables are patient risk factors (demographictraits, complicating health problems, etc.). Failingto adjust adequately for such factors could mis-lead payers, purchasers, and consumers regardingprovider or plan performance,115 as illustrated bythe recent case involving a private report card onhospitals in Orange County, California.
Many of the most important patient risk factorsare best measured using detailed clinical data,such as physical findings and diagnostic test re-sults. Computerization of such clinical informa-tion should make it easier to obtain and use inperformance assessments. One approach wouldbe to require that more clinical information be in-cluded in administrative data. In recent years,payers and government agencies have mandatedincreased numbers of diagnosis and procedurecodes and other clinical data elements included inclaims and discharge abstracts. This has greatlyincreased the information burden on providers;116
yet it still does not yield the kinds of clinical detailrequired for valid performance assessment. More-
over, accuracy problems in diagnosis and proce-dure coding render those data suspect.117
The more promising approach to providingneeded clinical information is to computerize thepatient record. Rather than having clinicallytrained personnel read, interpret, and code the in-formation contained in paper-based patient re-cords, most of the relevant information could beprecoded in the electronic patient record andreadily extracted for analysis. Alternatively, un-coded information (free text) contained in theelectronic patient record could be processedthrough advanced methods of pattern recognition,such as natural language processing (see chapter2). The usefulness of these capabilities greatly de-pends on three other aspects of advanced informa-tion technologies: input, storage, and retrieval.That is, to be useful for performance assessmentpurposes, the information in the electronic patientrecord must be accurately and easily entered (pre-ferably at the point of care) and extracted (usuallyat sites other than the point of care, e.g., an ana-lyst’s office). Moreover, storage capacities mustbe adequate to handle the huge quantities of in-formation involved.
As stated earlier, computer networks couldmake it easier to track the care and outcomes of in-dividual patients by facilitating record linkageacross all providers and departments. Networkscould also make it easier to share patient data, per-formance measurement algorithms, and assess-ment results among providers, payers, purchasers,and researchers to compare the performance ofproviders or plans. Like assessing the effective-ness of specific health services, such comparisonswould require using health problems, process and
115 Epstein, op. cit., footnote 98, pp. 58, 60; S. Salem-Schatz et al., “The Case for Case-Mix Adjustment in Practice Profiling: When Good
Apples Look Bad,” Journal of the American Medical Association, vol. 272, No. 11, Sept. 21, 1994, pp. 871-874.
116 D.R. Longo et al., Inventory of External Data Demands Placed on Hospitals (Chicago, IL: The Hospital Research and Educational Trust
of the American Hospital Association, 1990).
117 See L.I. Iezzoni, Risk Adjustment for Measuring Health Care Outcomes (Ann Arbor, MI: Health Administration Press, 1994), pp.142-167; R.A. Bright, J. Avorn, and D.E. Everitt, “Medicaid Data as a Resource for Epidemiologic Studies: Strengths and Limitations,” Journalof Clinical Epidemiology, vol. 42, No. 10, 1989, pp. 941-943; J. Whittle, “Large Administrative Database Analysis,” Tools for EvaluatingHealth Technologies: Five Background Papers, U.S. Congress, Office of Technology Assessment, OTA-BP-H-142 (Washington, DC: U.S.Government Printing Office, February 1995), pp. 33-35.

152 | Bringing Health Care Online: The Role of Information Technologies
outcome measures, and analytical methodologiesthat are as similar as possible across providers.These efforts would also be facilitated by messag-ing standards for electronic exchange of informa-tion among different computer systems, and bymethods of translating among disparate clinicalnomenclatures and coding systems.
CONCLUSIONS
❚ Summary of FindingsAdvanced information technologies—electronicpatient records, structured data entry, new human-computer interface technologies, portable com-puters, automated data capture, relationaldatabases with online query, knowledge-basedcomputing, and computer networks—can poten-tially improve the quality of health care. Theycould do so by enhancing clinical decision supportand by improving data for assessing the effective-ness of health services and the performance ofhealth care providers and insurance plans. Specifi-cally, they could facilitate:
� faster and easier collection and entry of in-formation about the patient’s health problemand background, with portions of that informa-tion being:
—entered by clinicians at or near the point ofcare;
—captured directly from diagnostic and moni-toring equipment (including digitized radio-graphic images, full-motion videos, andsound recordings); or
—entered by the patient prior to care;
� faster, easier, and better targeted search and re-trieval (possibly at the point of care) of:
—previously collected information about thepatient; and
—information about the kind of health problemafflicting the patient and alternative tests andtreatments for it, drawn from local or remoteknowledge bases;
� more flexible organization and display of thisinformation as appropriate for particular clini-cians;
� development of computer-based clinical proto-cols and other forms of CDSSs that apply deci-sion rules and other knowledge-basedapproaches to information about the patientand the health problem;
� more rigorous construction and analysis ofmeasures of service effectiveness and providerand plan performance; and
� more rapid and widespread dissemination ofnot only the results of these measures and localclinical research using CDSSs, but also the pa-tient data, measurement algorithms, andCDSSs on which those results are based.
Currently, empirical evidence demonstratingthe ability of these technologies to achieve thesegoals is limited, mixed, or incomplete. Moreover,concerns have been raised about possible adverseeffects on the quality of health care arising fromthese applications, including:
� incorrect parameters or criteria, or omitted oraltered steps, in clinical decision support sys-tems that could lead to inappropriate care;
� excessive reliance on clinical decision supportsystems, which could undermine the ability ofclinicians to exercise professional judgment innonroutine cases and reduce the interpersonalaspects of patient care (“ the quality of caring”);and
� the temptation to use readily available adminis-trative data for assessing the effectiveness ofspecific health services or the performance ofproviders or insurance plans. If the data are in-complete or inaccurate, the results could bemisleading.
❚ Policy OptionsThe private sector has been largely responsible forthe development and application of informationtechnologies in clinical decision support and per-formance assessment of health care providers andinsurance plans. The federal government’s rolehas mainly involved:
� developing information systems and perfor-mance measures for its own health insuranceand health care delivery programs, most nota-bly Medicare;

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 153
� funding of intramural and extramural researchand demonstration projects; and
� participating in consensus standards-develop-ment processes along with private sector orga-nizations.
All of these activities in both the private and pub-lic sectors are likely to continue, with some in-creasing and others decreasing. In an era ofbudgetary and regulatory restraints, however,major new government initiatives, such as fund-ing for technology development or mandated reg-ulation of clinical information systems, areunlikely. It can be argued that this is appropriate—in other words, that the federal government shouldnot interfere in private market decisions regardingthe selection of new technologies or their applica-tions.
On the other hand, the federal government—specifically HCFA—is responsible for ensuringthe quality of health care rendered to Medicare andMedicaid beneficiaries.118 Recent efforts to movemore beneficiaries into managed care have under-scored quality concerns, given the expectationthat capitation creates an incentive for underser-vice.119 Several policy issues regarding the poten-tial impact of information technology on thequality of care delivered to Medicare and Medic-aid beneficiaries deserve the attention of federalpolicymakers.
Effectiveness and SafetyThe foremost issue is the extent to which clinicalinformation systems actually change clinicalpractice patterns and patient outcomes, andwhether those changes are beneficial to providersand patients. Empirical research on this issue re-mains limited, mixed, or incomplete, and moresolid evidence regarding these impacts needs to beobtained. If these systems do indeed improve thequality of care, then the next set of issues can be
addressed: What are the most efficient means ofdeveloping and implementing such systems?
Much of the research supporting the develop-ment and evaluation of clinical information sys-tems (including CDSSs) has been conducted byacademic institutions and other private sector or-ganizations. Many of these projects have receivedgrant or contract funding from federal executivebranch agencies, mainly NLM and AHCPR (or itspredecessor, the National Center for Health Ser-vices Research, NCHSR). However, there hasbeen little coordination among these privately andpublicly funded projects in terms of their methodsof evaluating the effectiveness and safety of clini-cal information systems. The focus of these evalu-ations should be on the impacts of these systemson clinical practice patterns and patient outcomes.Where possible, these evaluations should be con-ducted prospectively, including randomized con-trolled trials.
Given its methodological shortcomings, asses-sing the performance of providers and insuranceplans and disseminating information regardingthat performance to various parties may prove tobe an ineffective approach to improving the quali-ty of health care.120 At present, however, there isgreat demand for performance information in boththe public and private sectors; and if such informa-tion is going to be produced and used, it should beas valid and reliable as possible. Advanced in-formation technologies—primarily electronic pa-tient records—promise to improve performanceassessment by making more information on pa-tients, providers, services, and outcomes morereadily available in a more detailed, accurate, andusable form. Most importantly, such informationcould improve methods of risk adjustment for per-formance indicators that are based on health careprocesses and outcomes. Conversely, the devel-opment of reliable and valid performance assess-
118 The state governments share responsibility for the Medicaid program with the federal government.
119 Given a fixed payment per plan member, providers may be tempted to minimize the volume and/or intensity of services rendered for
each patient.
120 Epstein, op cit., footnote 98.
154 | Bringing Health Care Online: The Role of Information Technologies
ment indicators could improve the application ofinformation technology to health care by identify-ing the most important data elements to include inelectronic patient records.
Like clinical information systems, much of theresearch and development work on performanceassessment and risk adjustment has been con-ducted by private sector organizations, often withfunding from federal agencies, mainly AHCPR(or NCHSR) and HCFA. Working with privatesector organizations, HCFA has begun develop-ing the DEMPAQ indicators for ambulatory careamong Medicare beneficiaries and adapting theprivately developed HEDIS system to the Medi-caid managed care population. Nonetheless, therehas been little coordination among all of these pri-vately and publicly funded projects on perfor-mance assessment and risk adjustment, orbetween these projects and those evaluating theeffectiveness and safety of clinical informationsystems. The basic issue is whether all of thesefederal efforts should continue as they are, orwhether more or less funding and/or coordinationwould be appropriate.
Maintain or increase funding for intra-mural research and extramural grants and contracts toprivate sector organizations for research and demon-stration projects designed to:
■
■
■
develop and test the reliability and validity ofvarious methods of measuring and assessing(with risk adjustment) the performance of pro-viders and health plans;develop, implement, and evaluate specific sys-tems of risk-adjusted performance indicators;evaluate the effectiveness and safety of clinicalinformation systems, including CDSSs.The FDA could employ the results of the evalu-
ations of clinical information systems in formulat-ing regulations for that class of medical software,and HCFA could adapt the most promising perfor-mance assessment systems for use in its Medicareand Medicaid programs—as it is now doing withthe Medicaid HEDIS indicators (which are not yetrisk-adjusted). This option would maintain thecurrent approach of funding research, develop-
ment, and evaluation programs through severalgovernment agencies, with little coordinationamong them. It would thus preserve the autonomyin program direction currently enjoyed by the var-ious agencies and the consequent diversity in thetypes of programs and their results. On the otherhand, HCFA would have to: 1) wait for the neededperformance assessment systems to be developedand evaluated; and 2) use performance indicatorsthat still may not be truly appropriate for theMedicare or Medicaid populations.
Maintain or increase funding for HCFAto develop and evaluate performance assessmentmethods and systems suitable for Medicare and Med-icaid enrollees, using intramural research and extramu-ral grants and contracts to private sector organizationsfor research and demonstration projects as needed.
This is HCFA’s current approach in developingthe DEMPAQ indicators for ambulatory careamong Medicare beneficiaries. Given that HCFAis also adapting privately developed indicators(Medicaid HEDIS), options la and lb are notmutually exclusive. However, option 1 a would bemore costly than option lb because, under option1a, development and evaluation funding would bespread over a broader array of performance assess-ment systems as well as clinical information sys-tems. From another perspective, more effort couldbe concentrated on the information needs of theMedicare and Medicaid programs for a givenamount of funding. On the other hand, option lbwould sacrifice federal direction of evaluations ofclinical information systems that could be usefulto the FDA in formulating regulations.
Assign the task of coordinating the de-velopment and evaluation of performance assessmentmethods and systems and clinical information systemsto a single agency
This option could be adopted regardless ofwhether option la, option lb, or both were pur-sued. The designated agency—such as HCFA orAHCPR—would ensure that all federally fundedprojects employ rigorous and uniform methods toenhance the soundness and comparability of their

Chapter 4 Using Information Technology To Improve the Quality of Health Care | 155
results. In addition, agency personnel would meetwith representatives of private sector corpora-tions, foundations, and research organizationsthat also fund or conduct such projects to discussthe most promising approaches to research, devel-opment, and evaluation. This option would re-quire only small additional costs for personnel,travel, and meetings; yet it could greatly increasethe value and timeliness of project results. On theother hand, it would diminish the autonomy inprogram direction currently enjoyed by the vari-ous agencies and the consequent diversity in thetypes of programs and their results.
Reduce funding for development andevaluation of performance assessment methods andsystems and clinical information systems, and directHCFA to employ performance assessment methodsand systems developed and evaluated in the privatesector with minimal adaptation.
This option would capitalize on the diversearray of performance assessment methods andsystems being developed in the private sector. Itwould reduce government expenditures, depend-ing on the amount of work needed to adapt pri-vately developed performance assessmentsystems to the Medicare or Medicaid popula-tions—which in turn would depend on the initialsuitability of those systems’ indicators. However,to an even greater extent than with option la,HCFA would have to: 1) wait for the needed per-formance assessment systems to be developed andevaluated in the private sector; and 2) use perfor-mance indicators that still may not be trulyappropriate for the Medicare or Medicaid popula-tions.
Until more solid evidence is available regard-ing the effectiveness and safety of existing clinicalinformation systems and the reliability and validi-ty of performance assessment systems, more dras-tic action—such as mandating the testing andcertification of all such systems—is probably notjustified. Legal questions regarding who should
be held liable in situations in which such systemslead clinicians to make decisions that harm pa-tients are probably best left to the courts to re-solve.
Standards and TechnologyAssuming that clinical information systems arefound to be effective and safe in terms of their im-pacts on practice patterns and patient outcomes,the next set of issues focuses on the most efficientmeans of developing and implementing those sys-tems. Three options regarding government in-volvement in the development of standards andtechnology that were presented in chapter 2 war-rant additional emphasis here. One is continuedgovernment participation (along with private sec-tor organizations) in the voluntary, cooperative,public- private process of developing consensusstandards for electronic messaging (exchange ofinformation among disparate computer systems).The second is funding and coordinating researchto overcome specific technological barriers (e.g.,limitations of electronic storage devices). Theseactions would not only facilitate the developmentand testing of clinical information systems andperformance assessment systems, but would alsoenhance the clinical knowledge on which they arebased.
The third option concerns continuation of fund-ing for NLM to develop the Unified MedicalLanguage System (UMLS). A major problemconfronting the UMLS project is that one of themost widely used systems for classifying and cod-ing health care services, called the Physicians’Current Procedural Terminology, Fourth Edition(CPT-4), is copyrighted by the American MedicalAssociation (AMA). Thus, the more recent ver-sions of CPT-4 cannot be incorporated intoUMLS. 121 Many major payers currently employCPT-4 for “professional” billing by clinicians andother noninstitutional providers and suppliers, butalso use the International Classification of Dis -
121 McCray, op. cit., footnote 66.

156 | Bringing Health Care Online: The Role of Information Technologies
eases, Ninth Edition, Clinical Modification (ICD-9-CM), Volume 3 (Procedures), for billing by in-patient hospitals and other institutional providers.
For payment and other purposes, services ren-dered by a clinician in an inpatient setting must becoded using both of these systems, creating addi-tional costs for providers. For many services,however, the codes in ICD-9-CM cannot beequated (”crosswalked”) with those in CPT-4 be-cause of substantial structural differences betweenthe two coding systems.122 Moreover, bothICD-9-CM (Vol. 3) and CPT-4 have serious tech-nical limitations, such as overlapping and duplica-tive codes and inconsistent and noncurrent use ofterminology. Most importantly, neither has ade-quate room for expansion, so both are running outof codes as new services are created or differentuses of existing services are distinguished. In ad-dition, neither system provides sufficient clinicaldetail to support the creation of the kinds of data-bases required to accurately assess patient out-comes using advanced information technol-ogies.123
Citing these and other problems, the NationalCommittee on Vital and Health Statistics(NCVHS), an advisory body to the Secretary ofHealth and Human Services, has recommendedthe development of a single, unified classificationand coding system that covers all health care ser-
vices rendered by all providers in all settings, andthat can be used for multiple purposes (reimburse-ment, research, etc.).124 The NCVHS maintainedthat, although implementing such a system wouldinitially be costly (particularly in the conversionof computer systems, databases, reimbursementsystems, and documentation), it would savemoney in the long run through administrative sim-plification; more accurate coding and documenta-tion; encouragement of automation and uniformterminology, data collection, and data processing;better monitoring and detection of errors, fraud,and ineffective procedures; and reduced trainingcosts.125
Legislation that would have required the devel-opment of such a system was introduced in the103d Congress (H.R. 1255), but was tabled in fa-vor of incorporation into broader health care re-form legislation that subsequently did not pass.126
A survey of users of ICD-9-CM (Vol. 3) andCPT-4 found extensive dissatisfaction with themand widespread support for the concept of asingle, unified system. Opposition to this conceptwas expressed mainly by physicians and represen-tatives of medical organizations.127 On the otherhand, concern has been expressed about the pro-prietary nature of CPT-4 and the AMA’s role inmaintaining a system that is widely used for pub-lic purposes.128
122 For example, in CPT-4 the code for total abdominal hysterectomy (58150) includes procedures performed with or without removal ofovaries or fallopian tubes, whereas ICD-9-CM (Vol. 3) has separate codes for total abdominal hysterectomy (68.4) and removal of ovaries and/or tubes (65.3 through 65.6). Thus, the CPT-4 code cannot be used to identify patients who had undergone only a total abdominal hysterectomy(without removal of ovaries or fallopian tubes). See American Medical Association, Physicians’ Current Procedural Terminology, 1994 (Chi-cago, IL: September 1993), p. 355, and Practice Management Information Corp., International Classification of Diseases, 9th Revision, Clini-cal Modification, Fourth Edition, 1993 (Los Angeles, CA: 1993), pp. 935, 937.
123 Iezzoni, Risk Adjustment for Measuring Health Care Outcomes, op. cit., footnote 117, pp. 164-167; Whittle, op. cit., footnote 117; U.S.Department of Health and Human Services, Public Health Service, National Committee on Vital and Health Statistics, The National Committeeon Vital and Health Statistics, 1993 (Washington, DC: May 1994), pp. 8-10, 54-75.
124 U.S. Department of Health and Human Services, Public Health Service, National Committee on Vital and Health Statistics, op. cit., foot-
note 123, pp. 54-55.
125 Ibid., pp. 59-62.126 Ibid., p. 56.127 Ibid., pp. 56-58.128 Ibid., p. 60.

Chapter 4 Using Information Technology To lmprove the Quality of Health Care | 157
The NCVHS concluded that existing serviceclassification and coding systems “are structural-ly flawed and wastefully redundant,” and that nei-ther ICD-9-CM (Vol. 3) nor CPT-4 “can be ‘fixed’without a complete overhaul (that is, creating anew classification).”] 29 Yet in 1994, even HCFAreaffirmed its intention to continue this dual cod-ing system policy in its Medicare and Medicaidprograms, despite the substantial barriers thisposes to efficient information processing andanalysis. l30 Although the agency intends to con-duct a pilot study on the feasibility of modifyingor replacing ICD-9-CM (Vol. 3), and will remainopen to ideas regarding a unified system, HCFAintends to continue its use of CPT-4 and its “coop-erative relationship with the AMA.”l31
Provide additional funding for intramu-ral and extramural research on the feasibility of devel-oping a single classification and coding system thatcould be applied to all health care services performedby all providers in all settings.
Although this research could be conducted ordirected by a single agency (such as NLM, HCFA,or AHCPR), extensive involvement by and coop-eration with other agencies, private sector orga-nizations (providers, payers, research associa-tions, and particularly the AMA), and the WorldHealth Organization (WHO) would be essential.If such a classification system were developed,NLM could then incorporate it into UMLS. Thisresearch would incur modest additional cost, andwould further delay development of a unified ser-vice classification and coding system.
Establish a new executive branch pro-gram to develop a unified service classification andcoding system.
This option would bypass research on the feasi-bility of developing such a system (option 2a).Again, the program to develop a new system couldbe conducted by one or more executive branchagencies, with extensive input from other agen-cies, private sector organizations, and WHO. Thisoption would also incur larger additional coststhan option 2a; however, it could expedite devel-opment of the new system. On the other hand, itwould be more objectionable to parties that arecommitted to the current dual coding systempolicy.
Once a unified service classificationand coding system is developed, mandate that all fed-eral agencies that manage health insurance and healthcare delivery programs use that system in those pro-grams.
In addition to HCFA, these agencies include theDepartment of Defense, the Department of Veter-ans Affairs, and the Indian Health Service. Pro-moting efficient information processing andanalysis in these programs would seem warranted,considering the government’s enormous invest-ment in them. Given the magnitude of these pro-grams in the health care marketplace, most privatepayers would probably soon adopt the new unifiedservice classification and coding system, just asthey began using the ICD-9-CM system afterHCFA implemented it. On the other hand, such a
129 Ibid., p. 54.130 U.S. Deparment Health and Human Services, Public Health Service, National Committee on Vital and Health Statistics, Subcommit-
tee on Medical Classification Systems, Meeting Minutes, Washington, DC, Apr. 18, 1994, pp. 5-7, 9-10, For physician and supplier billing,HCFA actually uses its own system, called the HCFA Common Procedure Coding System (HCPCS), that incorporates CPT-4 but also containsadditional codes.
131 Ibid., p. 5. In another manifestation of this relationship, HCFA and the AMA recently formed the National Uniform Claim committee,
“designed to give physicians more of a say in the creation and implementation of standards for electronic claims processing.” This move hasbeen harshly criticized by some participants in the existing voluntary, cooperative, public-private process of consensus standards development.“Yet Another Group Prepares To Work on Claims Standards,” Health Data Management, May 1995, p. 14.

158 I Bringing Health Care Online: The Role of Information Technologies
mandatory approach would probably be the mostobjectionable option to parties that are committedto the current dual coding system policy.
Provide minimal funding for monitoringand facilitating private sector development of a unifiedservice classification and coding system.
Rather than mandating and/or funding the de-velopment of a unified service classification andcoding system, Congress could continue to leavethe development of such a system to the privatesector. Minimal funding could be provided for ex-isting agencies (e.g., NLM) and committees (e.g.,
NCVHS) to monitor private sector activities andto facilitate those activities—for example, bysponsoring meetings among interested parties.This option would capitalize on the existing vol-untary, cooperative, public-private process of de-veloping consensus standards. It would also be theleast objectionable option to parties that are com-mitted to the current dual coding system policy,and it would only marginally increase governmentexpenditures. Its major drawback would be thelong period of time that would probably be re-quired for the consensus standards-developmentprocess to produce the needed system.
Telemedicine:Remote Access to
Health Services and Information
elemedicine can be broadly defined as the use of informa-tion technology to deliver medical services and informa-tion from one location to another. Since the 1960s,telecommunication has been used to exchange medical
information between sites in both rural and urban areas. One ofthe earliest applications of telemedicine was at the University ofNebraska where two-way, closed-circuit microwave televisionwas used for psychiatric consultations. Another was in Boston,where a video link was established between a health clinic at Lo-gan Airport and the Massachusetts General Hospital. The Nation-al Aeronautics and Space Administration (NASA) also was apioneer in the 1960s with its satellite support of a telemedicineproject, conducted by the National Library of Medicine (NLM),that provided health services to the Appalachian and RockyMountain regions and Alaska. In the 1970s, NASA also spon-sored the STARPAHC (Space Technology Applied to Rural Pa-pago Advanced Health Care) project, implemented with theIndian Health Service and the Department of Health, Educationand Welfare on the Papago Indian Reservation in Arizona.
Early expansion of telemedicine was affected, however, by thecost and limitations of the technology. Recent technological ad-vances—such as fiber optics, integrated services digital networks(ISDN), and compressed video—have eliminated or minimizedmany of these problems, fostering a resurgence of private- andpublic-sector interest in the potential of telemedicine to lowercosts, improve quality, and increase access to health care, espe-cially for those who live in remote or underserved areas. Thetechnology is not only better; it is also becoming cheaper.
While telemedicine has been practiced for more than 30 years,its current iteration is still in the early stages of development. One | 159

160 | Bringing Health Care Online: The Role of Information Technologies
recent journal article remarked that: “Telemedi-cine is on its way (although it has not yet ar-rived).”1 Others believe that telemedicine has nowcome into its own.
Having now come of age, telemedicine hasthe potential of having a greater impact on thefuture of medicine than any other modal-ity . . . Telemedicine is, in the final analysis,bringing reality to the vision of an enhanced ac-cessibility of medical care and a global networkof health care.2
It may be a number of years before telemedi-cine is used widely enough and evaluated suffi-ciently in terms of its effectiveness and efficiencyfor definitive statements to be made about itsoverall value and recommended uses. Like all newtechnologies, there will be impacts that cannot beanticipated in advance. Rigorous evaluation stud-ies are needed to determine telemedicine’s poten-tial benefits, and such research is beginning totake place.
With Congress, the Administration, the healthcare industry, and consumers all searching forways to reduce the costs of delivering health care,the potential of telemedicine has been receivingcareful scrutiny. A number of bills directly relatedto telemedicine were introduced in the 103d Con-gress; so far in the 104th Congress, four bills havebeen introduced that refer to telemedicine. TheAdministration’s Information Infrastructure TaskForce is considering the role that informationtechnology can play in delivering health servicesmore efficiently and effectively as part of theNational Information Infrastructure (NII) initia-tive. A task force subgroup of representatives
from federal agencies is addressing the currentstatus and potential of telemedicine. Telemedicinealso has important international implications, andorganizations like the World Health Organizationand the European Commission are exploring itspotential as well.
TELEMEDICINE’S POTENTIAL EFFECTSParts of the United States that are sparsely popu-lated continue to have difficulty attracting and re-taining health professionals, as well as supportinglocal hospitals and clinics. An earlier OTA reportoutlined the ongoing problems of delivering ade-quate, high-quality health care to people who livein rural areas.3 Since the report was released in1990, the problems rural residents face in acces-sing health care have not changed substantially,although there have been some selected improve-ments. Although access to physicians continues tobe limited and rural hospitals continue to close,the financial picture for rural hospitals that remainopen has improved somewhat.4
One physician, discussing the potential bene-fits of telemedicine, described the problems fac-ing rural health care this way:
What do you call a place the size of New YorkState with almost no medical, surgical, or pe-diatric subspecialists? . . . Western Kansas. Thisarea has been medically underserved for genera-tions. Subspecialty access has not been the onlydifficulty. There are also serious problems withthe retention of primary care physicians, theprovision of nursing education and emergencyroom coverage, and the financial health of ruralhospitals. The primary challenge has been geo-graphic—and until recently there did not seem
1 E.A. Franken et al., “Telemedicine and Teleradiology: A Tale of Two Cultures,” Telemedicine Journal, vol. 1, No. 1, spring 1995, p. 7.2 Michael E. DeBakey, “Telemedicine Has Now Come of Age,” Telemedicine Journal, vol. 1, No. 1, spring 1995, p. 43 U.S. Congress, Office of Technology Assessment, Health Care in Rural America, OTA-H-434 (Washington, DC: U.S. Government Print-
ing Office, September 1990).
4 “Health Care in Rural America,” statement of the Office of Technology Assessment at a hearing of the Senate Committee on Agriculture,Nutrition, and Forestry, June 9, 1994.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 161
to be any way adequately to confront the chal-lenge.5
There are a number of reasons why isolatedareas have difficulty attracting and retaininghealth care professionals. Medical practice isoften more demanding and less lucrative than inlarger centers. Providers may also feel isolatedfrom mentors, colleagues, and the information re-sources necessary to support them personally andprofessionally. Equipment may be less up to dateand facilities less than adequate. Similar problemsoften plague the delivery of health care to large in-ner-city populations. Telemedicine is a tool thatmay help address the problem of provider dis-tribution by improving communication capabili-ties and providing convenient access to up-to-dateinformation, consultations, and other forms ofsupport.6
The use of telecommunications to deliverhealth services has the potential to reduce costs,improve quality, and improve access to care in ru-ral and other underserved areas of the country. Al-though the extent of this potential is largelyspeculative at this time, researchers are beginningto address telemedicine’s impacts. According toone researcher:
. . . telemedicine may be unique in having thepotential for introducing low-cost, high-effi-ciency components that may, under certainconditions, increase access to care while possi-bly limiting increases in cost by enhancinghealth outcomes.7
If research results prove to be largely positive,telemedicine is likely to become fairly routineover the next 10 to 20 years.8
One thing is certain—no single technologicalsolution will work for all communities. Each loca-tion is unique, and systems designed to addressaccess problems must be tailored to meet the par-ticular needs and culture of each community,whether rural or urban. As noted in an earlier OTAreport, communities are endowed differently withrespect to their cultures, locations, landscapes,and natural and human resources, as well as theiraccess to information technologies.9
❚ Costs of Delivering Health CareDetermining the costs of delivering medical ser-vices is a difficult task under any circumstances.It is even more complicated when dealing with atechnical application like telemedicine where somany aspects of its practice are still unknown.Comparing the cost of telemedicine with the de-livery of conventional medical services is one ap-proach. However, it is important to keep in mindthat, in reality, the practice of telemedicine will as-sume its own characteristics and may ultimatelybe quite different from previous models. Anotherapproach might be to compare telemedicine toother ways of increasing access to specialist care(i.e., visiting consultant clinics or satellite clin-ics).10 The cost of telemedicine needs to be con-sidered in relation to how it contributes to
5 Ace Allen, “Telemedicine in Kansas: Introduction,” Kansas Medicine, vol. 93, No. 12, December 1992, p. 322.6 See Daniel McCarthy, “The Virtual Health Economy: Telemedicine and the Supply of Primary Care Physicians in Rural America,” Ameri-
can Journal of Law & Medicine, vol. 21, No. 1, 1995.7 R.L. Bashshur, “On the Definition and Evaluation of Telemedicine,” Telemedicine Journal, vol. 1, No. 1, spring 1995, p. 23.
8 Jim Grigsby et al., “Analysis of Expansion of Access to Care Through Use of Telemedicine, Report 4: Study Summary and Recommenda-tions for Further Research,” Center for Health Policy Research, Denver, CO, December 1994, p. 3.2.
9 U.S. Congress, Office of Technology Assessment, Rural America at the Crossroads: Networking for the Future, OTA-TCT-471 (Washing-ton, DC: U.S. Government Printing Office, April 1991), p. 7.
10 Michael G. Kienzle, Project Director, University of Iowa National Laboratory for the Study of Rural Telemedicine, Iowa City, IA, person-al communication, May 10, 1995.

162 | Bringing Health Care Online: The Role of Information Technologies
improving the health of the population by prevent-ing disease, treating illness, and ameliorating painand suffering, and how it compares with alterna-tive systems.11
A recent report prepared for the Health Care Fi-nancing Administration (HCFA) that included anextensive literature review of telemedicine re-search found no studies that provided an adequateoverview of its cost-effectiveness.12 Although itis too soon to know whether the use of telecom-munications to deliver health care services will ac-tually lower costs, it would seem to have thepotential to do so for some participants. For exam-ple, telemedicine can eliminate time and wageslost at work and traveling expenses incurred whenspecialists and/or patients have to travel for con-sultations. In addition, keeping patients in theirown communities can increase local hospital rev-enues and decrease the cost to patients. The cost ofa bed in a community hospital is considerably lessthan in a large medical center. Costs might also bereduced by staffing hospitals and clinics with al-lied health professionals, such as nurse practitio-ners and physician assistants, who would deliverservices where there is no resident physician.These providers could be assisted and monitoredremotely by physicians using a telecommunica-tions link. In some cases, overall costs might alsobe lowered using telemedicine if patients aretreated sooner when their illnesses are less severe.However, if earlier diagnosis leads to an expen-sive course of treatment that would otherwise nothave been provided, costs could increase.
An earlier OTA report noted that one of thegreatest problems rural hospitals face is the out-
migration of residents to urban areas for care.13
Many hospitals in small communities have beenforced to close because their bed census droppedso low they became uneconomical to operate. Theeconomic impact on a small community when itshospital closes is enormous. In addition to reduc-ing access to care, such closures have a major im-pact on employment opportunities. The viabilityof small hospitals might improve if telemedicineallowed more patients to receive consultative ser-vices locally, rather than being referred to largemedical centers.
In addition to cost considerations, it is impor-tant not to lose sight of the value of telemedicine indelivering services or ensuring health care jobs.Communities suffer when people do not receiveneeded care or become unemployed when a hospi-tal closes because it is no longer economically vi-able. These societal costs are important, butextremely difficult to measure. As one recent re-port stated:
. . . improved access and quality, benefits frompreventive care, and rural economic develop-ment are difficult to quantify and are likely to beleft out of the cost-effectiveness equation. Whenthis occurs, the cost-effectiveness analysis willmisrepresent telemedicine’s true benefits andlead to sub-optimal decisions on whether andhow to invest in these systems.14
While telemedicine might reduce costs in cer-tain cases, there is also the potential that costs mayincrease, at least in the short term. A consultationcould represent an additional cost when used for apatient who would not have been seen by a spe-cialist at all without the availability of telemedi-
11 For a discussion of cost-benefit analysis and cost-effectiveness analysis, see R.L. Bashshur, “Telemedicine Effects: Cost, Quality andAccess,” Journal of Medical Systems, April 1995.
12 Jim Grigsby et al., “Analysis of Expansion of Access to Care Through Use of Telemedicine and Mobile Health Services, Report 1: Litera-ture Review and Analytic Framework,” December 1993, p. 2.3. The lack of cost-effectiveness data on the use of information technology inhealth care delivery is not unusual. An OTA contractor report reviewing such studies as they apply to administrative simplification found little inthe literature. “Estimating the Cost-Effectiveness of Selected Information Technology Applications,” Project HOPE, Center for Health Affairs,unpublished contractor report prepared for the Office of Technology Assessment, March 1995.
13 U.S. Congress, Office of Technology Assessment, op. cit., footnote 3, p. 12.14 Office of Rural Health Policy, Health Resources and Services Administration, Public Health Service, Department of Health and Human
Services, Reaching Rural, (Washington, DC: 1994), p. 11.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 163
cine.15 However, the advantage of early diagnosisand treatment using telemedicine may offset later,more expensive episodes, thereby reducing theoverall costs of care. Concerns have also beenraised about the potential for overutilization or
- fraud if third-party reimbursement for telemedi-cine consultations becomes widespread, thusdriving up costs. There is also the possibility thattelemedicine might lower costs to patients, but in-crease costs for Medicare because more people areprovided access to health care.l6 What is notknown is whether real improvements in health sta-tus would offset the increase in demand for care,should either occur.17
■ Access to Health ServicesAccess to health services is a function of demo-graphic factors such as geography, education, eco-nomic status, and age. For patients to have access,there must be health care providers and adequatefacilities and services to deliver care. In a June1994 hearing, the Chair of the Congressional Ru-ral Caucus testified:
. . . the primary discussion in rural areas abouthealth care reform is not focused on the structureof alliances or the composition of the standardbenefits package, but is concerned about the fi-nancial stability of the local hospital or recruit-ment of a new town doctor.1 8
Rural and remote areas face special problemswhen it comes to delivering health care. For exam-ple, the rural population is disproportionately old-er and poorer. They have more chronic illnesses
For prac t i t ioners in rura l o r o ther underserved areas,telemedicine can improve communication capabilities byprov id ing conven ien t access to consu l tan ts , up - to -da tein format ion, and o ther forms o f suppor t
and more work-related accidents. A large percent-age of general physicians are within five years ofretirement.l9
Geography is a critical factor because, tradi-tionally, there has been a shortage of care in areaswhere medical providers are less likely to want topractice, such as rural and inner city locations.20 Itis difficult to recruit and retain health care provid-ers because this type of practice tends to be less lu-crative, fails to provide professional interactionand support, and places high demands on practi-tioners. Although the number of physicians prac-ticing in rural areas is increasing overall, ruralresidents continue to be more than twice as likely
15 Jim Grigsby et al., “Analysis of Expansion of Access to Care Through Use of Telemedicine and Mobile Health Services, Report 2: Case
Studies and Current Status of Telemedicine;” May 1994, p. 3.2.16 Grigsby er al., Report 4, op. cit., footnote 8, p. 7.6.
17 R.L. Bashshur, School of Public Health, University of Michigan, personal communication, May 15, 1995.18 Congresswoman Jill Long, Chair, Congressional Rural Caucus, testimony before the Senate Committee on Agriculture, Nutrition and
Forestry, June 9, 1994.19 Ibid.
20 Ibid.

164 | Bringing Health Care Online: The Role of Information Technologies
as the nation as a whole to face shortages of prima-ry care physicians.21 To help attract and keep phy-sicians, it seems clear that a community’s accessto health services may increasingly depend onproviding practitioners with electronic access toinformation, continuing medical education, andpeer support. This may be particularly true for anew generation of practitioners who are accus-tomed to using computers in their work.
The availability of telemedicine services mayhelp rural and other underserved communitiessolve some of their problems in accessing healthcare by making rural practice more attractive. On-line access to information and expert advice mayhelp rural health care professionals overcometheir sense of isolation from other colleagues andthe lack of access to the up-to-date informationthey need to practice effectively. Telemedicineservices also increase the access of rural physi-cians to medical specialists and vice versa, provid-ing a two-way educational experience. Teachers inacademic medical centers learn about the prob-lems physicians face in a rural practice, which willhelp them better prepare medical students for therealities of practice. Rural physicians gain in twoways—from the educational experience of inter-acting with and learning from specialists, and byhaving access to formal continuing medicaleducation courses.22 Some people caution, how-ever, that improving telecommunication linksshould not be viewed as a substitute for improvedphysician availability in rural areas.23 Citizensmay take the view that they are receiving second-class medical services if the role of telemedicine is
perceived as a substitute for a health care providerin their community.
❚ Quality of CareExperts who assess the quality of conventionalmedical care use complicated measures of struc-ture, process, and outcome.24 Structure refers tostaff, equipment, and organization; process refersto measures of appropriateness, necessity, andtechnical quality; and outcome refers to measuresof effectiveness, as well as the patient’s functionalstatus, health status, and satisfaction and qualityof life.
Because telemedicine is an electronic means todeliver care, not a specific medical procedure, itcannot be compared with conventional care in thesame way that individual procedures can be mea-sured.25 Clinical effectiveness has not been dem-onstrated for all clinical functions using all typesof technology. However, a scale of clinical effec-tiveness can be constructed to differentiate thoseservices that have been assessed from those thatare still experimental. Grigsby et al. have sug-gested one way of demonstrating how the qualityof care delivered using telemedicine could be as-sessed, based on a number of applications. Theirreport suggests four categories of current teleme-dicine applications:
1. Applications that are plainly effective.2. Applications that are likely to be effective, but
the implications of implementing them are un-clear. They would require further research tounderstand their effects.
21 S.M. Korczyk, “Health Care Needs, Resources and Access in Rural America,” a report for the National Rural Electric CooperativeAssociation (Washington, DC: National Rural Electric Cooperative Association’s Retirement, Safety and Insurance Department, spring 1994),p. 14.
22 For a relevant discussion related to education, see U.S. Congress, Office of Technology Assessment, Teachers and Technology: Makingthe Connection, OTA-EHR-616 (Washington, DC: U.S. Government Printing Office, April 1995).
23 Korczyk, op. cit., footnote 21, p. 19.
24 For a more complete discussion of quality assessment, see ch. 4, “Information Technologies and the Quality of Health Care.”25 Grigsby et al., “Analysis of Expansion of Access to Care Through Use of Telemedicine and Mobile Health Services, Report 3: Telemedi-
cine Policy: Quality Assurance, Utilization Reviews, and Coverage,” Center for Health Policy Research, Denver, CO, August 1994, p. 3.3.

Chapter 5 Telemedicine: Remote Access to Health Services and Information 1165
3.
4.
Applications for which the safety and effective-ness are currently unknown, or for which basicresearch is required to specify requisite techni-cal parameters.Applications that are entirely experimental, orwhich anticipate the integration of different ex-isting advanced technologies.26
Whether and how telemedicine affects the qual-ity of care delivered has not yet been proven.However, it is possible to speculate that some as-pects of the electronic medical encounter mightprovide better care from the patient perspective.Telemedicine could provide faster, more conve-
27 The ability to receive the ser-nient treatment.vices of a specialist without having to leave one’scommunity also provides better continuity ofcare. Similarly, allowing a patient to remain in thelocal hospital with family and friends for supportcould improve the quality of the experience for thepatient and could, in fact, contribute to a faster re-covery. These benefits would minimize the dis-ruption of the patient’s life and reduce the amountof working time lost. Followup care seems wellsuited to telemedicine, and might be carried outmore effectively and efficiently by electronicmeans, thereby avoiding the costs of time andtravel for an office visit.
For the health care provider, telemedicine canoffer tools to assist in providing high-quality ser-vices. Having timely, convenient access to themost up-to-date information, continuing medicaleducation programs, decision support systems,and consultations with specialists in large medicalcenters should increase the provider’s options andimprove his or her ability to accurately diagnoseand effectively treat patients. The development ofclinical practice guidelines for telemedicine couldenable providers to deliver better care. However,
26 Ibid., p. 3.4.
whether or not telemedicine consultations im-prove the quality of care will only be known whenthe research has been done to determine patientoutcomes.
TELEMEDICINE APPLICATIONSTelemedicine is broadly defined as the use of in-formation technology to deliver medical servicesand information from one location to another.However, there are differences of opinion regard-ing what the definition should include.28 Mostagree that it includes applications in areas such aspathology and radiology, as well as consultations
CLOSE TO HOME JOHN McPHERSON
©1995 John McPherson/Dist by Universal Press Syndicate
8-10
“Mrs. Nortman just sent in this fax of a rash thatshe’s got on her stomach.”
27 Norwegian researchers have found that—assessed by criteria for delivering health services in a timely fashion and as close to the patient
residence as possible-telemedicine maintains a higher level of quality than traditional medical services. U. Holand and S. Pedersen. “’QualityRequirements for Telemedical Services,” Telemedicine, Telektronikk, vol. 89, No. 1, 1993, p. 52.
28 For a discussion of telemedicine definitions, see Bashshur, Op. Ch., footnote 7. pp. 20-22.

166 I Bringing Health Care Online: The Role of Information Technologies
■ Initial urgent evaluation of patients, triage decisions, and pretransfer arrangements.■ Medical and surgical followup and medication checks.■ Supervision and consultation for primary care encounters in sites where a physician is not available.■ Routine consultations and second opinions based on history, physical exam findings, and available test data.■ Transmission of diagnostic Images.■ Extended diagnostic work-ups or short-term management of self-limited conditions.■ Management of chronic diseases and conditions requiring a specialist not available locally.■ Transmission of medical data.■ Public health, preventive medicine, and patient education
SOURCE: Grigsby et al., “Analysis of Expansion of Access to Care Through Telemedicine, Report 4, Study Summary and Recommen-dations for Further Research, ” Center for Health Policy Research, Denver, CO, December 1994, p 43
in specialties such as neurology, dermatology, car-diology, and general medicine. While some con-sider certain forms of medical education withinthe definition, others would exclude the use ofvideo to transmit purely didactic classroom lec -tures where there is no direct interaction betweenstudent and teacher. Whatever the definition, tele-medicine implies a closer link between the tele-communications infrastructure and the health caresystem that includes the entire range of teleser-vices. 79
Telemedicine can be used for a variety of pur-poses (see table 5-1 ).30 Some applications of tele-communications in the health field have been inuse longer than others. Teleradiology, for exam-ple, has about 30 years’ experience and a literaturedating from the early 1970s. Other applicationsare newer, and as yet have produced few researchresults. Current telemedicine projects vary withrespect to goals, organization, funding, andtechnology. This diversity is shown in brief de-scriptions of some current telemedicine programs.
■ Teleconsultations
Medical College of Georgia TelemedicineSystemThe Telemedicine System was initiated by theMedical College of Georgia (MCG) in November1991 when it connected with Dodge County Hos-pital in Eastman, Georgia, 130 miles away. Thesystem’s overall goal is to ensure that everyone inthe state has immediate access to quality healthcare. 31 The director envisions a telemedicine net-work that would spread out from a medical centercomplex to a number of satellite sites, such as ru-ral hospitals, correctional facilities, and even mili-tary bases (see figure 5-1 ). Although the system iscurrently used largely for cardiology and neurolo-gy consultations, it can be adapted for a variety ofspecialties, such as dermatology, ophthalmology,or gastroenterology through the use of a variety ofcamera adapters. In addition to consultations, thesystem can also be used to guide certain proce-dures, such as a endoscopy or laparoscopy. MCG’s
29 Birger J. Nymo, “Telemedicine,” Telektronikk, vol. 89, No. 1, 1993, p. 4.30 A recent study prepared for HCFA reported findings on the current status of telemedicine in the United states. Grigsby et al., Report 3, op.
cit., footnote 25, pp. 3.1-3.5.31 J.H. Sanders and F.J. Tedesco, “Telemedicine: Bringing Medical Care to Isolated Communities,”. . Journal of the Medical Association of
Georgia, May 1993, pp. 237-241.
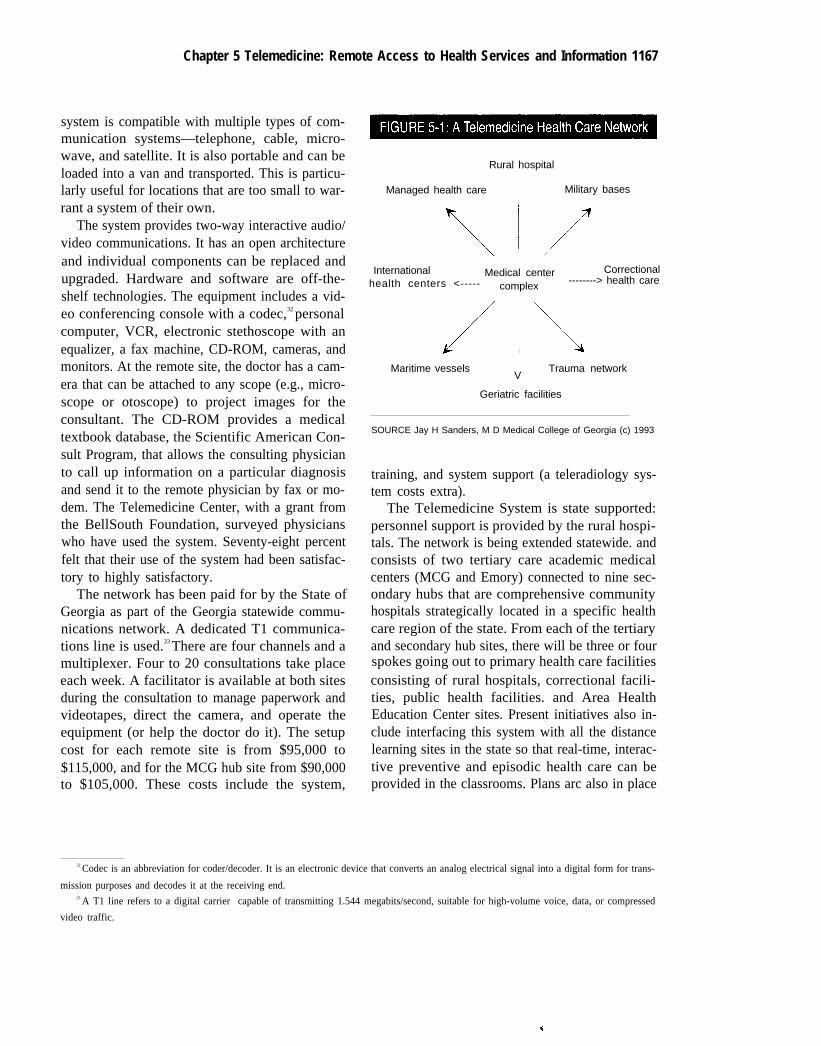
Chapter 5 Telemedicine: Remote Access to Health Services and Information 1167
system is compatible with multiple types of com-munication systems—telephone, cable, micro-wave, and satellite. It is also portable and can beloaded into a van and transported. This is particu-larly useful for locations that are too small to war-rant a system of their own.
The system provides two-way interactive audio/video communications. It has an open architectureand individual components can be replaced andupgraded. Hardware and software are off-the-shelf technologies. The equipment includes a vid-eo conferencing console with a codec,32 personalcomputer, VCR, electronic stethoscope with anequalizer, a fax machine, CD-ROM, cameras, andmonitors. At the remote site, the doctor has a cam-era that can be attached to any scope (e.g., micro-scope or otoscope) to project images for theconsultant. The CD-ROM provides a medicaltextbook database, the Scientific American Con-sult Program, that allows the consulting physicianto call up information on a particular diagnosisand send it to the remote physician by fax or mo-dem. The Telemedicine Center, with a grant fromthe BellSouth Foundation, surveyed physicianswho have used the system. Seventy-eight percentfelt that their use of the system had been satisfac-tory to highly satisfactory.
The network has been paid for by the State ofGeorgia as part of the Georgia statewide commu-nications network. A dedicated T1 communica-tions line is used.33 There are four channels and amultiplexer. Four to 20 consultations take placeeach week. A facilitator is available at both sitesduring the consultation to manage paperwork andvideotapes, direct the camera, and operate theequipment (or help the doctor do it). The setupcost for each remote site is from $95,000 to$115,000, and for the MCG hub site from $90,000to $105,000. These costs include the system,
Rural hospital
Managed health care Military bases
International Medical center Correctionalhealth centers <----- --------> health carecomplex
Maritime vesselsV
Trauma network
Geriatric facilities
SOURCE Jay H Sanders, M D Medical College of Georgia (c) 1993
training, and system support (a teleradiology sys-tem costs extra).
The Telemedicine System is state supported:personnel support is provided by the rural hospi-tals. The network is being extended statewide. andconsists of two tertiary care academic medicalcenters (MCG and Emory) connected to nine sec-ondary hubs that are comprehensive communityhospitals strategically located in a specific healthcare region of the state. From each of the tertiaryand secondary hub sites, there will be three or fourspokes going out to primary health care facilitiesconsisting of rural hospitals, correctional facili-ties, public health facilities. and Area HealthEducation Center sites. Present initiatives also in-clude interfacing this system with all the distancelearning sites in the state so that real-time, interac-tive preventive and episodic health care can beprovided in the classrooms. Plans arc also in place
32 Codec is an abbreviation for coder/decoder. It is an electronic device that converts an analog electrical signal into a digital form for trans-
mission purposes and decodes it at the receiving end.33 A T1 line refers to a digital carrier capable of transmitting 1.544 megabits/second, suitable for high-volume voice, data, or compressed
video traffic.

168 | Bringing Health Care Online: The Role of Information Technologies
to interface military health care needs with the ci-vilian hospital backbone. Based on the telecom-munication infrastructure put into place to supportthe telemedicine system, a patient at any site canbe examined by a physician at any other site. Dis-tance is totally transparent and seamless. MCGalso has plans for a demonstration project that willmonitor certain patients in their homes, the so-called electronic house call, as well as for a desk-top telemedicine system for the physicians’ offices.
Medicaid and Medicare are currently reimburs-ing the consultant and the referring physician atDodge County Hospital, and Medicaid pays therural hospital a facility fee. This reimbursementwas granted by the Medicare carrier (Aetna), andapplies only to the original sites in Georgia andnot to new ones. Blue Cross/Blue Shield reim-burses only the consultant. MCG has estimatedthat approximately 86 percent of patients who pre-viously would have been transported to MCG noware kept at the remote sites. The daily cost of a hos-pital bed in a rural area is placed at approximately$800, compared with $1,300 at MCG, and thecosts of transportation, increased time away fromwork, and delay in therapy represent additionalexpenses.
Physicians in remote areas who use the MCGsystem for consultations are given credit hours to-ward meeting their continuing medical education(CME) requirements, which are necessary for li-cense renewals. They do not have to interrupt theirpractice to attend classroom lectures in a differentlocation. This educational activity becomes di-rectly relevant to their day-to-day practice andmore meaningful than a lecture format.
Texas Telemedicine ProjectWith funding provided by foundations and ven-dors, the Texas Telemedicine Project began opera-tions in April 1991. It was established as a
research project to study viability factors poten-tially operative in a national health care deliverysystem. The project uses interactive two-way au-dio and video to connect sites in Austin with sitesin Giddings, a small town with fewer than 4,000people.34 The sites in Austin are the Austin StateHospital, the state headquarters of the TexasYouth Commission, the Austin Diagnostic Clinic,and the Texas Telemedicine project office. In Gid-dings, the Lee Memorial Hospital, a Texas YouthCommission maximum-security unit, the Gid-dings Regional Dialysis Clinic, and the Commu-nity Mental Health Clinic are connected. Each sitehas a unit with video, audio, and high-speed datatransfer channels; ports for a fax and laser printer;and two 20-inch color monitors, two video camer-as, two microphones, and a speaker. T1 telecom-munication circuits are provided in part bySouthwestern Bell, GTE, and LDDS. Economiesof scale are produced by scheduled sharing of tele-communication lines.
At night, when emergency triage may be need-ed for auto accident victims, the system connectsthe Giddings Hospital with the Austin DiagnosticClinic. In the morning, the Austin DiagnosticClinic is connected to the Giddings Dialysis Cen-ter to monitor patients coming off and going ondialysis. Management rounds of each site aremade electronically by Telemedicine InteractiveConsultative Services each day. The Texas Tele-medicine Project used a questionnaire for patientsand providers to document problems and satisfac-tion with the system. Results over the first twoyears documented a 99.35 percent satisfactionrate.
Kansas University Medical CenterTelemedicine in Kansas is a cooperative effort in-volving the Kansas City and Wichita campuses ofthe Kansas University Medical Center (KUMC),
34 Description taken from J. Preston, F.W. Brown, and B. Hartley, “Using Telemedicine To Improve Health Care in Distance Areas,” Hospi-tal and Community Psychiatry, vol. 43, No. 1, January 1992, pp. 29-30; also J. Preston, Director, Texas Telemedicine Project, personal commu-nication, May 14, 1995.

Chapter 5 Telemedicine: Remote Access to Health Services and lnformation| 169
I n 1991 , be fo re te lemed ic ine was ava i l ab le , phys ic ians f romThe University of Kansas Medical Center in Kansas CityKansas, traveled 270 miles to Hays, Kansas, to visit patients.
the state government, the Northwest Kansas AreaHealth Education Center, and nine rural hospi-tals.35 The system is designed to provide real-timemedical consultations involving a patient andpractitioner (physician, nurse practitioner, or phy-sician assistant) at the distant end and a specialistat the medical center. Full-motion, compressedtwo-way video is used, and there are facilities forinterfacing imaging equipment, using an electron-ic stethoscope, for example. Continuing educa-tion courses (including courses that provide CMEcredit for physicians) are offered over the sameequipment. The system is currently used 20 to 25percent for clinical applications, 30 percent forcontinuing education (nonphysicians), 20 percentcontinuing medical education (physicians), and20 to 25 percent for administrative functions.
Teleconsultations are mainly used to determinethe need for face-to-face treatment or for regularfollowup after a face-to-face visit. In 1993, 180consultations were conducted in 931 hours of totaloperations (including continuing education andadministrative uses). In 1994, there were 189 con-sultations. KUMC estimates that, while telemedi-cine does not completely replace the need for
In 1995, an oncologist at The University of Kansas MedicalCenter in Kansas City, Kansas, consults with a nurseprac t i t i oner a t the Hayes Med ica l Cen te r v ia an in te rac t i vev ideocon fe rence w i thou t l eav ing the med ica l cen te r .
transportation, it can eliminate a significantamount of travel for patients and specialists.
Use of T1 telecommunications lines in theState of Kansas network costs $35 per hour for on-peak use and $20 per hour for off-peak; but localaccess is expensive, especially if the transmissionhas to cross local access transport area (LATA)boundaries. Hospitals in the telemedicine pro-gram are paying between $421 and $1,318 permonth for local access to the nearest point-of-presence of the State network. Local accesscharges for T1 lines are mileage-sensitive.
A telemedicine suite includes one or two35-inch, 650-line digital monitors, one or two vid-eo cameras, graphics stand, slide converter(35mm to video interface), VCRs, microphones,and auscultation equipment (wireless stetho-scope). The camera at the distant site can be con-trolled remotely by the physician at the centralsite. Any medical imaging equipment that putsout an NTSC (television) signal can be interfaceddirectly, or a videotape made by that equipmentcan be played. Radiographic images are trans-mitted via video camera (use of a digitizing scan-
35 Description based on site vitie, descriptive material provided; A. Allen, R. Cox, and C. Thomas, “Telemedicine in Kansas,’’ Kansas Medi-
cine, December 1992, pp. 323-325; and A. Allen, Oncologist Telemedicine Project, University of Kansas, personal communication, July 6,1995.

170 | Bringing Health Care Online: The Role of Information Technologies
ner is far more expensive). All inputs are sent to acodec, which converts analog signals to digitalones for transmission. When purchased, the costof a basic equipment suite was about $90,000, andnow has dropped closer to $50,000.
The State of Kansas permits educational, medi-cal, county government, and other such organiza-tions to connect to the KANS-A-N state-owneddigital telephone network. The network does notyet extend to every county, and T1 lines are not yetavailable for local access in all counties. The tele-medicine application usually uses one-quarter of aT1 line (384 kb). Compression to this bandwidthgives some “ghosting” and “tiling” on fast mo-tion, but is acceptable for viewing normal, medi-cally significant motions such as a patient’s gait.KUMC’s experience is that picture quality formedical images such as ultrasound, computerizedaxial tomography (CT) scans, magnetic resonanceimaging (MRI), or some x-rays is not perceptiblyimpaired; however, quality is not good enough fora mammogram. Picture quality on fast motion isreportedly better using one-half T1 bandwidth.
The Mayo ClinicThe Mayo Clinic in Rochester, Minnesota, be-came a major developer of telemedicine in 1987when it expanded to sites in Scottsdale, Arizona,and Jacksonville, Florida. Today, Mayo uses tele-medicine for clinical care, education, and admin-istrative coordination to integrate the three sites.Current projects include the use of satellite com-munications to deliver consultative care to theMiddle East and the use of compressed video andland lines to deliver a wide range of services to af-filiated entities within Iowa, Wisconsin, and Min-
nesota. Mayo Clinic also provides services for theAmman Diagnostic Clinic in Jordan. During 12weeks in 1994, Mayo joined with the Pine RidgeIndian Reservation and NASA in an experiment toprovide professional education and clinical con-sulting services to professionals at Pine Ridge.Based on questionnaires completed by all the par-ticipants, it was determined that the project wasboth feasible and useful.36
Mayo is collaborating with NASA and the Ad-vanced Research Projects Agency (ARPA) on aproject to use the Advanced Communications andTechnology Satellite (ACTS) to deliver servicesto small communities in remote environments.37
In November 1993, Mayo sponsored a telemedi-cine symposium, and in April 1995 hosted theSecond International Conference on the MedicalAspects of Telemedicine and Second AnnualMayo Telemedicine Symposium.
East Carolina University School of MedicineEast Carolina University (ECU) performs teleme-dicine consultations to the largest prison in NorthCarolina and two rural hospitals.38 Physicians seeand talk to the patients via the telemedicine linkand then diagnose and prescribe medicationswhen necessary. A digital stethoscope, a graphicscamera, and a miniature, handheld dermatologycamera are used to aid in patient examinations.The working model developed for the prison sys-tem is now being expanded to six rural hospitalsand a large naval hospital (see figure 5-2). Aunique aspect of the ECU program is the hybridcommunications network and hardware that havebeen integrated. With the addition of an asynchro-nous transfer mode (ATM) network, this will be
36 T.E. Kottke and M.A. Trapp, “The Pine Ridge Indian Reservation/Mayo Clinic/NASA Telemedicine Project: A Feasibility Study,” pres-ented at the Second International Conference on the Medical Aspects of Telemedicine and Second Annual Mayo Telemedicine Symposium,Rochester, MN, Apr. 6-9, 1995. See also U.S. Congress, Office of Technology Assessment, Telecommunications Technology and Native Ameri-cans: Opportunities and Challenges, OTA-ITC-621 (Washington, DC: U.S. Government Printing Office, August 1995).
37 E.G. Tangalos, Mayo Clinic/Mayo Foundation, Rochester, MN, “Hearing on Telemedicine: An Information Highway To Save Lives,”held by the Subcommittee on Investigations and Oversight, Committee on Science, Space, and Technology, U.S. House of Representatives,May 2, 1994, pp. 12-13.
38 Information from East Carolina University School of Medicine, “Telemedicine,” brochure, August 1995; and David Balch, Director,Rural Eastern Carolina Health Network, personal communication, Aug. 15, 1995.

Chapter 5 Telemedicine: Remote Access to Health Services and Information 1171
ElizabethAhoskie City
●
. Sites linked to ECU
◆ Major NCIH sites
CoastalCommunity
SOURCE: East Carolina University, Greenville, NC, 1995
the only telemedicine program in the world oper-ating integrated T1 line microwave and ATMlinks. Current Federal support includes grantsfrom HCFA, the National Telecommunicationsand Information Administration (NTIA), and theOffice of Rural Health Policy (ORHP).
ECU recently conducted a demonstration clinicat a conference in California in which 84 peoplewere seen in three days via a live ATM link toECU. Conference participants were given the op-portunity to have a consulting specialist at ECUlisten to their heart beat, examine their ears, lookat a skin lesion, or explore some other medicalproblem of interest. Two-way video, audio, anddata were transmitted between the sites.
The Rural Eastern Carolina Health Network(REACH-TV) (consisting of the ECU School ofMedicine, Pitt County Memorial Hospital, East-ern AHEC, and the Center for Health SciencesCommunication) focuses on telemedicine, tele-conferencing/distance learning, and applied re-search interactive information environments.
RODEO NET ProjectThe mission of RODEO NET (Rural Options forDevelopment and Educational Opportunities Net-work) is “to pioneer advances in improving the de-livery of human services by connecting peopleusing appropriate communication technolo-

172 | Bringing Health Care Online: The Role of Information Technologies
gies.”39 In 1991, the Eastern Oregon Human Ser-vices Consortium was awarded a three-year grantof approximately $700,000 by the Rural HealthOutreach Grant Program of the Office of RuralHealth Policy (Health Resources and ServicesAdministration) for the purpose of demonstratingan innovative model of mental health care in a ru-ral area. RODEO NET uses three networks of Ore-gon ED-NET, which was created by the State ofOregon in 1989. Network I provides live, interac-tive one-way video, two-way audio services to 45“receive” sites in eastern Oregon. Network II pro-vides two-way video, audio, and data services us-ing digitally compressed video technology in 10studios. COMPASS is a local “dial-up” computerdata network that provides a variety of informa-tion services. These include user-friendly accessto local, national, and international databases andthe Internet; government and academic libraries;bulletin boards; electronic mail; and computer-conferencing services.
RODEO NET currently uses all three networksto train mental health providers in eastern Oregon.For example, both professional and paraprofes-sional staff who work with children and adoles-cents who have severe emotional disturbances andtheir families participate in a certificate programto upgrade staff qualifications. Individual trainingis also provided.
In addition to training, RODEO NET providescrisis response using Network II to enable person-nel to access the on-call psychiatrist at the EasternOregon Psychiatric Center in Pendleton to helpdeal with persons suffering extreme emotional orbehavioral turmoil. Such a response system oftensaves the time and money required to transport anindividual and keeps that person in the communi-ty. RODEO NET provides ongoing clinics for
medication management and case consultationson an ongoing or as needed basis, reducing thenumber of admissions to acute care facilities. In-terviews for preadmission, predischarge, andtransfers are now accomplished via Network II,and precommitment and psychiatric review boardhearings are conducted using interactive TV. Theproject also plans to work with consumer groupsto help them create their own computer network-ing conferences within the COMPASS system.
❚ Teleradiology and TelepathologyThe use of telecommunications to transmit medi-cal images is quite well developed and widespread.A teleradiology system acquires radiographicimages at one location and transmits them to oneor more remote sites, where they are displayed onan interactive display system and/or converted tohard copy.40 Transmissions might include CATscans, MRIs, or x-ray images. CAT scans andMRIs originate in digital form, but a film digitizermust be used to convert conventional radiographsfrom film to digital form. Teleradiology systemsoften employ a wide area network.
Teleradiology systems transmit images fromone hospital to another, from an imaging center toa hospital, or from an imaging center or hospital toa radiologist’s office or home. Each requires dif-ferent technologies and communication links andeach site has different requirements.41 For exam-ple, a radiologist who is on call may review animage in his or her office or at home, but at a latertime will also review the original image beforemaking a final diagnosis. In this instance, a lowerimage resolution, requiring less expensive equip-ment, may be acceptable. A higher quality imageis required if the radiologist is making a final in-terpretation without seeing the original image, as
39 Description taken from “RODEO NET Project Summary,” Oct. 25, 1993; and Cathy Britain, Program Manager, RODEO NET, personalcommunication, June 1995.
40 For an in-depth description of teleradiology, see S. Batnitzky et al., “Teleradiology: An Assessment,” Radiology, vol. 177, 1990.41 S.J. Dwyer, III, et al., “Wide Area Network Strategies for Teleradiology Systems,” RadioGraphics, vol. 12, No. 3, May 1993, p. 569.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 173
in the case of a request for a second opinion or ahospital that contracts for its radiological inter-pretations.42
In its study for HCFA, the Center for HealthPolicy Research found that, with some excep-tions, radiology using telecommunications is fea-sible.43 For providers, training in the use of theequipment appears to be a critical component, par-ticularly learning to manipulate and interpretimages using a video image on a monitor. Prelimi-nary research suggests, however, that in mostcases radiologists prefer conventional films andview boxes to teleradiology because reading themis less time-consuming and perhaps because theyare more familiar with them.44 The American Col-lege of Radiologists is currently evaluating equip-ment standards and practice parameters.
The field of medical imaging offers one of themost fertile grounds for the application of ad-vanced computer and communications technolo-gies. All-digital systems, known as picturearchiving and communications systems (PACS),now offer imaging of sufficient quality for prima-ry diagnosis in radiology, although their highcosts are a barrier to diffusion. The University ofVirginia operates a PACS system that it plans tohook into two remote sites, at distances of four and10 miles, using a T1 telecommunications line.Further expansion is planned based on the experi-ence with the two sites.45
The use of telecommunications for telepatholo-gy is also well established. Because of the needfor high-quality imaging, the requirements of
pathology call for equipment that is more sophis-ticated than is required for other telemedicine ap-plications.46 Early research findings suggest thattelemedicine allows frozen sections of tissuespecimens to be analyzed accurately.47 An exam-ple of a telepathology program is the Arizona-International Telemedicine Network (AITN), es-tablished at the University of Arizona in 1993. Itsgoals are to provide consultation services, usetelepathology in quality assurance programs, par-ticipate in research on the development of tele-pathology systems, and examine the impact oftelepathology services on the practice of medi-cine, including patient outcomes. The network in-volves five locations in Arizona and one each inMexico and China.48
❚ Home-Based Health ServicesIn addition to using telecommunications to deliv-er health services from one medical facility toanother, there is also the potential to use it to deliv-er services to people in their homes.49 In someways, electronic “house calls” represent a moveback to a health care system that is more home-centered rather than hospital-centered.50 Using avariety of technologies—including telephone,computers, monitoring devices, and interactivevideo—telemedicine could reduce or eliminatepatient travel, resulting in lower costs for the pa-tient and perhaps making a hospital or clinic visitunnecessary. This could be particularly helpful topeople whose mobility is limited or who may notbe well enough to travel. The elderly face particu-
42 Batnitzky, op. cit., footnote 40, p. 15.43 Grigsby et al., Report 1, op. cit., footnote 12, p. 2.13.44 Grigsby et al., Report 4, op. cit., 8, p. 2.3.45 Healthcare Telecom Report, Sept. 12, 1994, pp. 5-6.
46 Grigsby et al., Report 1, op. cit., footnote 12, p. 2.6.47 Grigsby et al., Report 4, op. cit., footnote 8, p. 2.3.48 A.K. Bhattacharyya et al., “Case Triage Model for the Practice of Telepathology,” Telemedicine Journal, vol. 1, No. 1, spring 1995, pp.
9-17.
49 See also the section on consumer health informatics in ch. 1.50 Mary Gardiner Jones, “Electronic House Calls: 21st Century Healthcare Services for Consumers,” Proceedings of the Mayo Telemedi-
cine Symposium, Oct. 1-3, 1993, p. 39.

174 | Bringing Health Care Online: The Role of Information Technologies
lar challenges in meeting their need for services,and advanced telecommunications—particularlytwo-way video to the home—could ultimatelyprovide them a full range of services.51
Home-based telemedicine could be particular-ly effective for followup care and for monitoringchronic illnesses, such as asthma or diabetes.Monitoring allows preventive measures to be tak-en before problems get so severe that hospitaliza-tion becomes necessary. Telemetry devices athome that connect to a computer—to provideelectrocardiograms or blood-pressure readings,for example—could alert the patient’s physicianthat treatment is necessary. Such a system couldprovide a more cost-effective method of care byreducing medical visits for conditions that are notsevere.
Several demonstrations are currently underway related to home delivery of services. For ex-ample, in several months, Eastern Carolina Uni-versity (ECU) will begin home trials for about sixpatients (initially) for remote cardiac rehabilita-tion using telephone, cable TV, and telemetryunits. Using one-way video and two-way audio, aphysician will monitor a patient at home while thepatient rides a stationary bicycle. Patients will seethe physician on their cable TV and will be able toconverse with him or her.52 This will permit real-time monitoring of their vital signs by the medicalcenter. In addition, ECU and Economic GrowthStrategies, Inc., in conjunction with Smart House,has created a health demonstration house. HealthHouse will use interactive communications toprovide monitoring, diagnosis, and informationproducts and services.
In collaboration with the Center for Total Ac-cess at Fort Gordon and the Georgia Tech Re-search Institute, the Medical College of Georgia
also is planning to place equipment in 25 homes tomonitor patients who have frequent hospitaliza-tions or emergency room visits. A similar systemwill be placed in a large nursing home, and into thehome of the nursing home’s medical director, toavoid unnecessary admissions to the hospital. TheHarvard Community Health Plan in Burlington,Massachusetts, operated a Triage and EducationSystem by placing computer terminals in 150homes. Patients used the system to get customizedhealth information and guidance based on re-sponses to a questionnaire they completed on thescreen. It enabled patients to manage common ill-nesses or injuries and monitor chronic healthconditions. The project was deemed a success, butwas discontinued because funds were unavailableto finance it when the demonstration ended.53
The Comprehensive Health Enhancement Sup-port System (CHESS) uses an interactive comput-er system to provide information, social support,and problem-solving tools for people living withAIDS and HIV infection. CHESS was developedat the University of Wisconsin-Madison under agrant from the W.K. Kellogg Foundation. Thesystem provides information, referrals to serviceproviders, patient support in making difficult de-cisions, and networking with experts and othersfacing the same concerns. When computers wereplaced in homes for three to six months, their usewas extremely heavy. Subjects who used CHESSreported a significantly higher quality of life inseveral dimensions, including social support andcognitive functioning. Users also reported signifi-cant reductions in some types of health carecosts.54 CHESS has also been used in a study ofeight African-American women with breast can-cer who lived in impoverished areas of inner-city
51 Mary Gardiner Jones, “Meeting the Home Health Care Needs of the Elderly in the 21st Century Through Telecommunications: Reportand Recommendations,” Consumer Interest Research Institute, Washington, DC, Mar. 10, 1995, p. 6.
52 Healthcare Telecom Report, vol. 2, No. 7, Mar. 28, 1994, p. 1.
53 Site visit, Harvard Community Health Plan, 1994. Most users liked the system, and HCHP noted a 15 percent increase in the use of self-care to treat health problems, a 14 percent increase in appropriate level of care decisions, and a 5 percent reduction in health center visits.
54 D.H. Gustafson et al., “The Use and Impact of a Computer-Based Support System for People Living with AIDS and HIV Infection,” n.d.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 175
Chicago. It was very well received, extensivelyused, and produced feelings of acceptance, mo-tivation, understanding, and relief among partici-pants.55
Delivering health services directly or providingneeded information does not always require theuser to have sophisticated equipment. The Con-nect System at Cleveland State University uses acomputer and voice mail system to monitor drug-using pregnant patients, patients in drug treat-ment, and mothers of newborns. This system is fornonemergencies, and patients access it using atouchtone telephone and a password. It is used tocommunicate with caregivers, and the computercalls the patient if there is a message waiting.Those without a telephone can call in on a regularbasis to collect messages. There is also a Commu-nity Health Rap line that will find an expert to an-swer questions. Telephone Pals will connectpatients with others who share a common healthcondition. Home Monitoring allows a clinician tocall a child’s parent at regular intervals to ask a se-ries of questions. Answers are sent directly to theclinician, who will contact the parents if there is aneed for action. Appointment and medication re-minders are also sent. Research showed that send-ing reminders for immunizations resulted in 82percent of patients in the experimental groupkeeping their appointments, compared with 69percent for the control group. The resulting immu-nization rates were 68 percent for the experimen-tal group, compared with 45.5 percent for thecontrol group. This is in a community in whichonly 4 percent graduated high school and 40 per-
cent owned their own telephone (12 percent wereboth homeless and phoneless).56
❚ Other SitesTelemedicine offers safety, security, and cost ad-vantages in delivering services to correctional fa-cilities. For example, since 1992, the EastCarolina University (ECU) School of Medicinehas provided consulting services to the CentralPrison in Raleigh, North Carolina, a top-securityprison.57 The prison doctor is able to consult viatelecommunications with specialists at ECU, thusavoiding the need to transport inmates or bring inspecialists. Consultants were reluctant to visit theprison, and the cost of transporting an inmate tothe hospital ranged from $700 to $5,000, depend-ing on the amount of security required.
In Texas, the University of Texas MedicalBranch at Galveston has seen 40 to 62 patients aweek from the prison population in Phase 1 of aprogram that began in October 1994. Their goal is100 patients per week by the end of 1995.58 Pa-tients are usually presented by physician assis-tants. The Texas prison system is looking attelemedicine as a way to reduce referrals to thestate’s tertiary care centers, such as the one at Gal-veston, which are overburdened with inmate re-ferrals. The Medical College of Georgia also isconnected to correctional facilities, and inmateswho previously needed to be transported forhealth care can now be treated at the prison usingtelemedicine.59
It seems clear that the delivery of health ser-vices using telecommunications is possible in any
55 F.M. McTavish et al., “CHESS: An Interactive Computer System for Women with Breast Cancer Piloted with an Under-served Popula-tion,” n.d.
56 F. Alemi, Health Administration Program, Cleveland State University, Cleveland, Ohio, personal communication, May 11, 1995.
57 East Carolina University School of Medicine and the Center for Health Sciences Communication, World Wide Web site home page:<URL: http://www.telemed.med.ecu.edu/>.
58 R.M. Brecht, “Implementation of Telemedicine Into the Texas Prison System,” presented at the Second International Conference on theMedical Aspects of Telemedicine and Second Mayo Telemedicine Symposium, Rochester, MN, Apr. 7, 1995.
59 J. Sanders, testimony, hearing of the House Committee on Science, Space, and Technology, Subcommittee on Investigations and Over-sight, May 2, 1994.

176 | Bringing Health Care Online: The Role of Information Technologies
number of settings, including school clinics andnursing homes. In addition to rural areas, experi-ments are taking place in urban areas as well. Anexample is at Stanford University in California,where a pilot project is under way to connect an ur-ban clinic serving the poor, a large multispecialtygroup practice, and a nursing home.60 Telemedi-cine’s potential to respond in emergency situa-tions, such as natural disasters or militarydeployments, has already been demonstrated.61
Decisions concerning potential applicationsclearly will be based on the usual criteria of howthey affect health care costs, access, and quality.
❚ Telemedicine Projects in OtherCountries
A number of other countries, particularly thosewith remote or isolated areas, currently use tele-communications to deliver health services. Thecharacteristics of these programs tend to reflectboth the health care and telecommunications poli-cies of the individual country.
For example, in Norway, the health sector hasbeen chosen by the government as one of the mainareas for the national plan for information technol-ogy.62 Remote areas and severe winter weatherconditions make the delivery of health care diffi-cult. The University Hospital of Tromso, with thesupport of Norwegian Telecom Research, hasbeen using telemedicine since 1988 for remotediagnosis in Northern Norway for radiology;pathology; dermatology; cardiology; ear, noseand throat; and psychiatry. The system is also usedextensively for distance education for physiciansand nurses, as well as training in use of the
technology. This is a coordinated research and de-velopment project with an interdisciplinary re-search group based in Tromso. Cooperation withinstitutions and personnel in the regional healthservice is encouraged. Local research institutionsparticipate and local industry is involved in devel-oping the technology.63 The telemedicine net-work is expected eventually to expand to Oslo andadditional remote areas of Norway. Plans are alsounder way to link up with the Mayo Clinic andJohns Hopkins University Hospital in Baltimore,Maryland, for consultations.64
In Canada, the oldest and best-known use oftelemedicine is at the Memorial University ofNewfoundland where its Telemedicine Centre hasoperated since 1975. The Centre operates a dedi-cated audio network with 54 sites in health centersand the remainder in community colleges, highschools, university campuses, and governmentbuildings. It provides both health programs (con-tinuing health education, medical data transfer,community health education programs, andhealth professional meetings) and a wide range ofdistance education programs and administrativemeetings for government and others.65 Anothertelemedicine program in Western Canada linksDrumheller Regional Health Complex with theUniversity of Calgary and adjoining FoothillsHospital. This program was developed in partner-ship with Alberta Government Telephones andCalgary-based Hughes Aircraft, which is provid-ing the hardware and software.66
South Australia established a TelemedicineProject in June 1991 to examine the potential roleof telemedicine in health services delivery. It is a
60 Bob Holmes, “Medicine Cruises the Infobahn,” Stanford Medicine, spring 1995, pp. 20-23.61 J.B. Crowther and R. Poropatich, “Telemedicine in the U.S. Army: Case Reports from Somalia and Croatia,” Telemedicine Journal, vol. 1,
No. 1, spring 1995, pp. 73-80.
62 B.J. Nymo and B. Engum, “Telemedicine To Improve the Quality, Availability and Effectiveness of the Health Service in Rural Regions,”paper presented at “Seminar on the Regional Impact of Advanced Telecommunication Services,” Kiruna, June 19-21, 1990, p. 1.
63 Ibid., p. 4.64 Healthcare Telecom Report, July 18, 1994, p. 8.65 Memorial University of Newfoundland, Telemedicine Centre, Information Sheet, 1993.66 Calgary Herald, “Long-Distance Healing,” June 27, 1993, p. A1.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 177
collaborative effort of the Economic Develop-ment Authority of South Australia, the SouthAustralian Health Commission, MFP Australia,and Telecom Australia.67 The project was estab-lished between the Royal Adelaide Hospital,South Australia’s largest teaching hospital withmore than 800 beds and a full range of specialistservices, and South Australia’s largest countryhospital in Whyalla, situated 400 kilometresnorthwest of Adelaide. The Whyalla Hospital has150 beds, services a town of 27,000 people, andhas a limited range of specialist services. FromSeptember 1992 to June 1993, a total of 190 tele-medicine sessions were held, divided betweeneducation, clinical, administration, and demon-stration and training sessions. A study of the proj-ect reported that clinical use was most successfulfor psychiatry, dermatology, and geriatric assess-ment. Postgraduate medical education and admin-istrative education were also very successful. Theproject proved less successful for physiotherapy,occupational therapy, speech pathology, and den-tistry. The study also concluded that telemedicineservices will be most successful where they com-plement and enhance existing health services.
TELEMEDICINE ISSUESLike all applications of new technologies, thereare barriers to widespread diffusion of telemedi-cine.68 Some of the problems are related to thetechnology, but most can be attributed to otherfactors.
❚ Reimbursement for ServicesA critical issue for telemedicine is whether andhow it will be reimbursed by Medicare/Medicaid
and other third-party payers. In rural areas, up to40 percent of physicians’ patient base consists ofMedicare/Medicaid patients.69 As one congress-man testified at a 1994 hearing on rural healthcare:
Telemedicine is particularly important to ru-ral health delivery systems. . . However, with-out the assurance of payment for telemedicineservices, the full potential of telemedicaltechnology will never be realized. . . This ad-ministrative roadblock prevents the develop-ment and expansion of these systems in ruralAmerica.70
HCFA, the federal agency responsible forMedicare/Medicaid reimbursement of services,has been under pressure to reimburse for servicesdelivered using telemedicine, and is consideringwhat its policy should be. Traditionally, physi-cians have not been reimbursed for consultationsusing telecommunications (i.e., the telephone).Current rules for reimbursement require face-to-face contact (defined as in the same room) be-tween physician and patient. Services that do notinvolve direct interaction with the patient, such asteleradiology, telepathology, or EKG testing, arealso reimbursed;71 however, consultations inwhich there is interaction between patient andconsultant using videoconferencing are not.72
Aetna, the Medicare carrier in Georgia, currentlycovers telemedicine consults at the Dodge CountyHospital, part of the Medical College of Georgia’stelemedicine system. This policy does not applyto new sites in Georgia.
To assist HCFA in its decisionmaking, theagency commissioned a study of the primary fac-tors to consider in any reimbursement policy. Theresearchers outlined three principal consider-
67 “South Australian Pilot Telemedicine Project,” Project Team Evaluation Report, November 1993, p. 2.
68 For a discussion of barriers to implementation, see J.H. Sanders and R.L. Bashshur, “Challenges to the Implementation of Telemedicine,”Telemedicine Journal, vol. 1, No. 2, summer 1995.
69 BNA’s Health Care Policy Report, vol. 2, Feb. 28, 1994, p. 418.70 Pat Roberts, (R-KS), hearing before the Committee on Ways and Means, Subcommittee on Health, House of Representatives, U.S. Con-
gress, Feb. 7, 1994.
71 Office of Rural Health Policy, op. cit., footnote 14, p. 6.72 Ibid.

178 | Bringing Health Care Online: The Role of Information Technologies
ations: 1) the adequacy of the technology, 2) medi-cal effectiveness, and 3) the appropriateness of theapplications.73 The report concluded that it wouldbe reasonable to proceed with reimbursement forsome telemedicine services—those that are wide-ly accepted as effective; those that are probably ef-fective, but with unknown effects on the healthcare system (with some restrictions placed on re-imbursement); and applications that require basicresearch (evaluated for reimbursement on a case-by-case basis).74 Coverage might also be re-stricted to certain geographic areas, institutions,or applications. In addition to this recently com-pleted project, HCFA is currently supporting sev-eral demonstration projects that will help in itsdecision process. The agency also has funded atelemedicine evaluation project, to be conductedby researchers at the University of Michigan, anda data collection project at the Telemedicine Re-search Center in Portland, Oregon.
At a May 1994 hearing on “Telemedicine: AnInformation Highway To Save Lives,” a HCFAofficial testified:
Because of our limited experience with de-livery of telemedical services in the real world,we would like to proceed with caution. How-ever, I can say with confidence, that through theuse of pilot projects undertaken by both the Gov-ernment and private industry, we will be able tolearn the best approach to provide effective andefficient health care services for our beneficia-ries. HCFA envisions accessible health care be-ing provided through the use of telemedicineand other emerging technologies but it must bebased on solid data so that the quality of healthcare provided is not compromised.75
It is unlikely that HCFA will move ahead with-out a clearer understanding of all the issues. Re-search currently under way should address someof the questions that the agency would want an-swered before proposing a uniform reimburse-
ment policy for telemedicine. In the meantime,some experiments could be tried that would fur-ther the decisionmaking process, particularly withrespect to costs. HCFA is currently seeking aMedicare waiver from the Office of Managementand Budget that would allow the agency to pro-vide reimbursement for physician services ren-dered via telemedicine for pilot projects in Iowa,Georgia, West Virginia, and North Carolina.
HCFA will continue to be concerned about tele-medicine’s safety and effectiveness, quality ofcare, practice standards, and the impact on physi-cian distribution. However, the agency will alsobe concerned about any increase in Medicarespending that could result from reimbursement fortelemedicine services. At a time when reductionsin the growth of Medicare are being proposed,there will be reluctance to initiate policies thatcould increase costs by increasing access to ser-vices.
❚ Lack of Research/ExperienceAnother barrier to telemedicine is the lack of re-search demonstrating its safety and efficacy, clini-cal utility, and cost-effectiveness. This is aproblem for potential users, payers, and policy-makers. No one knows for certain which medicalconditions are best suited to the use of telemedi-cine. For example, believing that the “hands-on”experience is critical for initial patient examina-tions, some providers feel that telemedicine worksbetter for followup care than for an initial visit.Clearly, some procedures are better suited to theuse of interactive video than others in terms of thepatient’s comfort level. Research on patient satis-faction with telemedicine is limited, but results in-dicate that in general they like it.
Early experiments in telemedicine were termi-nated before they produced answers concerningits cost, impact on access, and effects on quality of
73 Grigsby et al., Report 1, op. cit., footnote 12, p. i.
74 Grigsby et al., Report 4, op. cit., footnote 8, p. 5.175 Helen L. Smits, Deputy Administrator, Health Care Financing Administration, statement at a hearing at the National Institutes of Health
before the Committee on Science, Space and Technology, U.S. House of Representatives, May 2, 1994, p. 13.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 179
care.76 Those projects did not end because theyfailed to achieve their objectives. Instead, the rea-sons included: 1) lack of familiarity and limitedexperience with the systems, 2) lack of institution-al commitments to sustain them when outsidefunding ran out, 3) lack of incentives for physi-cians to use the systems, 4) limitations of thetechnology, and 5) poor system planning and de-sign.77
In its request for proposals for an exploratoryevaluation of telemedicine, the Office of RuralHealth Policy listed four primary objectives:
1. to determine the current status of telemedicinein rural health with respect to the number andtypes of systems in operation, levels of technol-ogy employed, types of specialty services pro-vided, utilization of services, costs, and patientand provider acceptance;
2. to explore the effects of telemedicine on accessto care, practitioner isolation, and the develop-ment of health care networks;
3. to explore the organizational factors (at facility,network, community, and state levels) that aidor impede the successful development and im-plementation of telemedicine systems; and
4. to develop, test, and refine data collectioninstruments that may be used in subsequentevaluation efforts.78
The results of this exploratory evaluation andother research under way should lay the ground-work for future research projects designed toanswer the many questions concerning the effec-tiveness of telemedicine. Evaluation tools will
clarify what telemedicine technologies are mostappropriate and which health care services are bestsuited to remote consultation.79 The National Li-brary of Medicine, with some support also fromHCFA and the Department of Veterans Affairs, iscurrently sponsoring a study by the Institute ofMedicine that will try to establish clear evaluationcriteria by which the appropriateness, effective-ness, acceptability, and other aspects of telemedi-cine might be rigorously measured and assessed.(See also appendix D.)
Several organizations have formed to promoteand coordinate telemedicine research activitiesand share research strategies. Examples are theNational Consortium for Telemedicine Evalua-tion (see box 5-1) and the Clinical TelemedicineCooperative Group (see box 5-2). The AmericanTelemedicine Association also promotes researchas part of a comprehensive agenda for telemedi-cine.
❚ Telecommunications InfrastructureThe technology exists to provide a wide variety oftelemedicine services over regular telephonelines. For example, the teledermatology programat the Oregon Health Sciences University (sup-ported by NLM’s High Performance Computingand Communications initiative) uses still imagesover standard phone lines to transmit skin images.In many rural areas, however, the telecommunica-tions infrastructure does not provide a medical fa-cility with sufficient bandwidth to carry thenecessary signals for interactive video telecon-
76 Bashshur, op. cit., footnote 11.77 Ibid., p. 6.
78 Office of Rural Health Policy, Health Resources and Services Administration, Public Health Service, Department of Health & HumanServices, Request for Proposal No. HRSA 240-OA-22(4) for “Exploratory Evaluation of the Rural Application of Telemedicine,” 1995, p. 9.
79 D.A. Perednia, “Evaluating the Use of Telemedicine for Mental Health Applications,” June 1994, pp. 8-9.

180 I Bringing Health Care Online: The Role of Information Technologies
The National Consortium for Telemedicine Evaluation (NCTE) was organized in 1993 at the University
of Michigan, School of Public Health, Department of Health Management and Policy for the purpose of
conducting multistate, multisite evaluation of telemedicine systems The evaluation IS focused on ac-
cessibility, cost, and quality, The consortium serves two specific objectives: 1) to assist in the evaluation
of individual telemedicine programs/projects as prototype systems of care involving specific configura-
tions of technology (high end, low end), manpower (MD and non-MD providers), organization (orga-
nized and unorganized, Integrated networks), and clinical applications (specific diagnostic services, full
service, full-time service) To date, participants in the Consortium include NASA, Medical College of
Georgia, University of West Virginia, MD-TM University of Kentucky, Louisiana Health Care Authority,
and Mid-Nebraska Telemedicine System, The Consortium is developing detailed methodologies for
telemedicine evaluation, including sample design and data collection protocols
SOURCE: National Consortium for Telemedicine Evaluation, Department of Health Management and Policy School of Pubic Health,University of Michigan, Ann Arbor, Ml
sultations. 80 The cost of the telecommunicationslinks required for telemedicine represents a majorbarrier to its broader use. Often new lines must belaid and new tariffs developed. If a single facilityhas to absorb the full costs of the transmission ser-vices. the costs may be prohibitive. In addition tolaying a new line for broadband service, it mayalso be necessary for the communications carrierto install a digital switch to ensure that the qualityof the compressed video signals is acceptable.
Boundaries were established after the breakupof AT&T that made telephone calls placed outsidethe local access transport area much cheaper thanthose placed within the same service area.81 Thehigh cost of connectivity between local and long-
distance carriers is a difficult hurdle for telemedi-cine systems to overcome.82 To lower trans-mission costs, some have suggested that an essen-tial service rate be set for local governments, hos-pitals, and educational facilities that wouldprovide a basic level of service at guaranteedprices that are not based on distance.83 In somecases, cooperative efforts among telemedicineproviders, state agencies, and telephone compa-nies have resulted in negotiated rates that are moreaffordable for the providers .84 Implementing tele-medicine projects generally is easier in states likePennsylvania, North Carolina. Georgia, Kansas,and Iowa where statewide networks already exist.As the number of statewide networks increases,
80 For an in-depth discussion of the rural communication infrastructure, see U.S. Congress, Office of Technology Assessment, op. cit., foot-note 9. For further discussion of the communication infrastructure, see U.S. Congress, Office of Technology Assessment. Critical Connections.”Communication for the Future, OTA-CIT-407 (Washington, DC: U.S. Government Printing Office, January 1990). For a description of broad-band network technology, see U.S. Congress, Office of Technology Assessment, Advanced Network Technology, OTA-BP-TCT-101 (Washing-ton. DC: U.S. Government Printing Office, June 1993), ch. 3. For an in-depth discussion of the role wireless technologies will play in the emerg-ing Nil, see U.S. Congress, Office of Technology Assessment, Wireless Technologies and the National Information Infrastructure, OTA-ITC-622 (Washington, DC: U.S. Government Printing Office, July 1995).
81 Office of Rural Health Policy, op. cit., footnote 14, pp. 4-5. The report cited the example of the Texas MedNet Project, whose 1992 month-
ly transmission costs were $27 per mile within the same local telephone service area, and $5 per mile between service areas.82E.G. Tangalos, ‘“Telemedicine Outcomes: What We Know and What We Don’t,” paper presented at the Rural Telemedicine Workshop.
Office of Rural Health Policy, Washington, DC, Nov. 3-5, 1993, p. 4.83 Office of Rural Health Policy, op. cit., footnote 14, P. 17.84 Dena S. Puskin and Jay H. Sanders, “Telemedicine Infrastructure Development, ’’. Journal of Medical Systems, vol. 19, No. 2, 1995, p. 2.

Chapter 5 Telemedicine: Remote Access to Health Services and Information 1181
The Clinical Telemedicine Cooperative Group (CTCG) IS a not-for-profit, independent medical re-
search corporation with offices in Portland, Oregon, and Kansas City, Kansas CTCG members share
common telemedicine research protocols, data collection instruments, and testing methodologies, By
coordinating research efforts, members are able to perform statistically valid telemedicine research
faster, and at a lower cost, than would otherwise be possible, Expertise in computer systems, research
design, imaging, statistical analysis, engineering, and specific medical expertise IS available to CTCG
members through TRC staff and affiliates The CTCG network IS based on successful community-based
research cooperatives---models that demonstrate the advantages and validity of large-scale, multi-
centered trials in clinical research. Pilot funding for the CTCG was provided by the Health Care Financ-
ing Administration.
SOURCES: D.A. Perednia, “Telemedicine System Evaluation and a Collaborative Model for Multi-centered Research, Journal of Medi-cal Systems, vol. 19, No 3, 1995, and J Kadel, Member Information Coordinator, CTCG, Oregon Health Sciences University, Port-land, OR personal communication, July 11, 1994
more and more uses will be found for telemedicine are interoperable, technology standards will be es-in both rural and urban areas.
In rural areas, hospitals, schools, government,and other community groups can aggregate de-mand and share a network to help spread the sys-tem costs. This can only be accomplished, however,when residents are involved in planning and de-veloping a system and have a sense of ownershipin it. In an earlier study, OTA suggested that RuralArea Networks would allow rural communities tocustomize networks to their own needs, whileachieving economies of scale and scope85 (see fig-ure 5-3). By sharing in the creation of such a net-work, rural communities would be able to enjoysome of the benefits of their urban counterparts. Asystem of “bandwidth on demand”, in which userspay only for the time they use on the system,would greatly reduce the costs of telemedicine andobviate the need for a dedicated communicationsline. Such service could be provided using an ad-vanced switching technology such as asynchro-nous transfer mode, which can support manydifferent kinds of services. To ensure that systems
sential for communication providers. 86 Many ofthese issues are currently being addressed in thecontext of the Administration’s NII initiative, par-ticularly by members of the Information Infra-structure Task Force (IITF).
Delivering health care to the home is increas-ingly important for people who need convalescentor chronic care. A public network that can providetwo-way video, high speed data transfer, andgraphics is required before a wide range of healthservices can be delivered directly to the home.Some telephone companies are beginning to re-spond to this recognized need by devising strate-gies to implement such advanced services, andhome services are figuring prominently in NII dis-cussions.
❚ Legal/RegulatoryRemote diagnosis and treatment across state linescould bring differing laws and regulations intoconflict. Telemedicine raises a number of legal is-sues related to privacy/confidentiality, licensing
85U.S. Congress, Office of Technology Assessment, op. cit.. footnote 9, p. 59.86 For discussions of technology standards, see chs. 1 and 2. See also U.S. Congress, Office of Technology Assessment, Global Standards:
Building Blocks for the Future, TCT-512 (Washington, DC: U.S. Government Printing Office, March 1992).
d
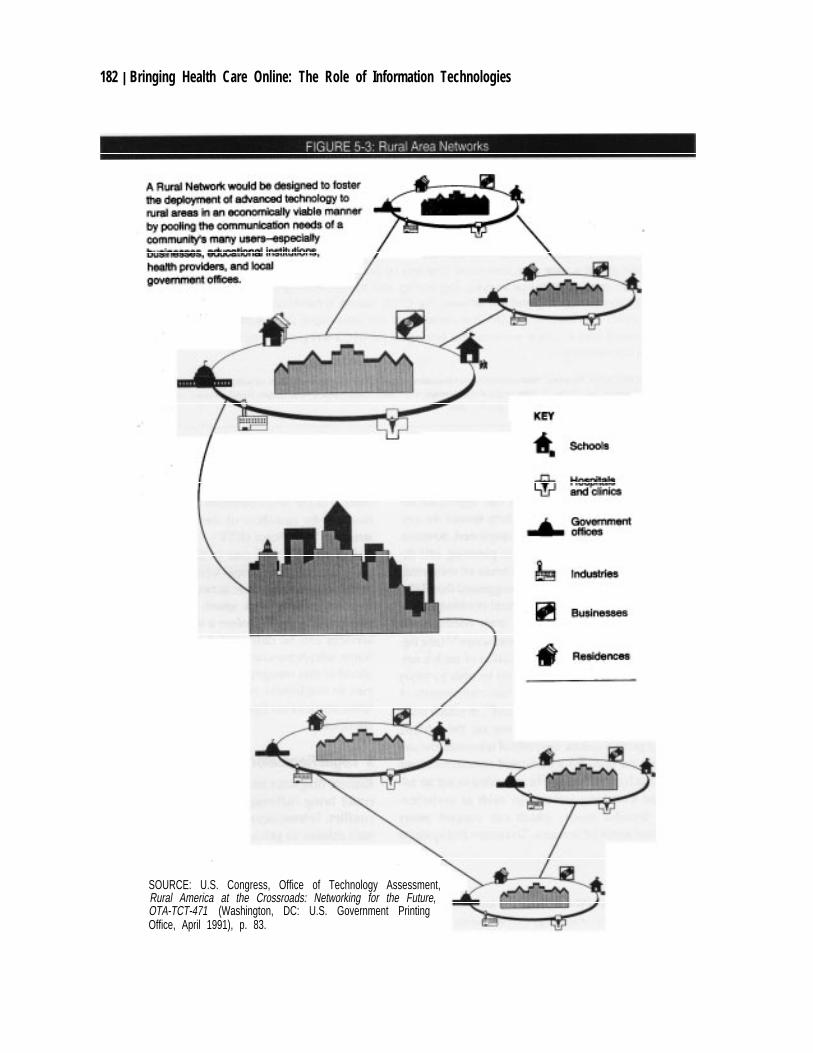
182 | Bringing Health Care Online: The Role of Information Technologies
SOURCE: U.S. Congress, Office of Technology Assessment,Rural America at the Crossroads: Networking for the Future,OTA-TCT-471 (Washington, DC: U.S. Government PrintingOffice, April 1991), p. 83.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 183
and credentialing, and liability that could repre-sent significant barriers to its broader diffusion.
Privacy and ConfidentialityPrivacy in health care information has been pro-tected in two ways: 1) in the historical ethical ob-ligations of the health care provider to maintainthe confidentiality of medical information, and 2)in a legal right to privacy, both generally and spe-cifically, in health information. Confidentialityinvolves control over who has access to informa-tion. Other terms frequently used in privacyprotection discussions are integrity and security.Integrity assures that information and programsare changed only in a specified and authorizedmanner, that computer resources operate correct-ly, and that the data in them are not subject to un-authorized changes. A system meeting standardsfor access allows authorized users access to in-formation resources on an ongoing basis.87 Secu-rity refers to the framework within which anorganization establishes needed levels of informa-tion security to achieve, among other things, theconfidentiality goals.88
The use of telecommunications to deliver med-ical care may pose additional risks to the privacyof patients and their records. For example, the cre-ation of a videotape of a consultation might pose anew privacy threat for the patient unless appropri-ate safeguards to control access to it are built intothe process. The issue of who has access to this in-formation will need to be considered and resolvedin advance. Depending on the nature of the ex-amination, the patient may also have privacy con-cerns in terms of who is actually present in eachlocation during the consultation. Nonmedical per-sonnel, such as a technician or facilitator, may beneeded to assist in the consultation.
If a videotaped consultation becomes part ofthe patient’s medical record, it would be treatedlike other videotaped information on the patient(e.g., an angiographic procedure, for example). Inthese cases, the usual privacy laws would apply.State laws governing the transmission and retriev-al of patient medical records vary, and officials areconcerned about user verification and access, au-thentication, security, and data integrity.
A previous OTA study found that the presentsystem of protecting health care information of-fers a patchwork of codes; state laws of varyingscope; and federal laws applicable to only limitedkinds of information, or information maintainedspecifically by the federal government.89 Thepresent legal scheme does not provide consistent,comprehensive protection for privacy in healthcare information, whether it exists in a paper orcomputerized environment. Clearly the privacyimplications for telemedicine will continue to re-ceive careful scrutiny. Vice President Gore has re-cently asked the Department of Health and HumanServices (DHHS) to develop model institu- tionalprivacy policies and model state laws for healthinformation in the context of the NII.90 This activ-ity is to be coordinated with the activities of theIITF in the privacy area.
Physician LicensingPhysicians must be licensed by the states in whichthey practice. Telecommunication facilitates con-sultations without respect to state borders andcould conceivably require consultants to be li-censed in a number of states. This would be im-practical and is likely to constrain the broaderdiffusion of telemedicine programs. In July 1994,the State of Kansas passed legislation requiring
87 C.P. Pfleeger, Security in Computing (Englewood Cliffs, NJ: Prentice Hall, Inc. 1989), pp. 5-6.88Ibid., p. 90.
89 U.S. Congress, Office of Technology Assessment, Protecting Privacy in Computerized Medical Information, OTA-TCT-576 (Washing-ton, DC: U.S. Government Printing Office, September 1993), pp. 12-13.
90 Vice President Al Gore, memorandum to Donna Shalala, Secretary of Health and Human Services, Mar. 8, 1995.

184 | Bringing Health Care Online: The Role of Information Technologies
that out-of-state physicians who provide consulta-tions using telemedicine be licensed in Kansas.
The licensing problem for telemedicine couldbe addressed by the implementation of national li-censing standards or the classification of physi-cians practicing telemedicine as consultingphysicians, thereby circumventing state rules. Fora start, such a national license could be provided tophysicians who provide consultations to under-served populations. A precedent exists for physi-cians serving in the military, the Department ofVeterans Affairs, the Indian Health Service, andthe Public Health Service.91 Another way to ad-dress the problem of licensing is to place the over-all responsibility for the patient’s care in the handsof the referring physician and view a consultant ina different state as making recommendations only.A novel approach unique to telemedicine wouldbe to consider that the patient is being “trans-ported” electronically to the consultant, thus ob-viating the need for the specialist to be licensed inthe patient’s home state.92
The issue of credentialing arises with telemedi-cine in terms of the use of consultants. In the Med-ical College of Georgia program, the JointCommission on Accreditation of Hospitals (JCA-HO) has determined that hospital credentials arenot a problem for the consulting physician as longas all physician orders are written by the referringphysician. The Federation of Boards of StateMedical Examiners has established a task force todeal with the problem of providing interstate tele-health care, while preserving state licensure, cre-dentialing, and monitoring of health careprofessionals.93
LiabilityThe liability implications of telemedicine are un-clear. At least two aspects of telemedicine couldpose liability problems. One is the fact that, in aremote consultation, the specialist does not per-form a hands-on examination, which could be re-garded as delivering less than adequate care. Thesecond aspect is that the use of compressed video,in which repetitious information is eliminated asthe data are converted from analog to digital andback, may raise the issue of diagnosing with lessthan complete information.94 On the other hand,telemedicine may, in fact, decrease the threat ofmalpractice suits by providing better recordkeep-ing and databases, and the fact that taping the con-sultations will automatically provide proof of theencounter. Tapes could also help to prove the in-nocence of providers who are falsely accused.
Consulting physicians could reduce their li-ability by adhering to practice guidelines for vari-ous telemedicine applications. Such guidelineswould need to be established by national healthprofessional associations.95 Another way of limit-ing liability would be to protect physicians andmedical centers that provide telemedicine con-sultations to the underserved under the doctrine ofsovereign immunity, which might take the form ofa cap on economic damages or some other hold-harmless protection.96 Liability considerationsfor telemedicine must, of course, be viewed in thecontext of ensuring the patient adequate recoursein cases of actual negligence.
91 Sanders and Bashshur, op. cit., footnote 68.92 Ibid.
93 J. Preston, M.D., President, American Telemedicine Association, personal communication, May 14, 1995.94 Office of Rural Health Policy, op. cit., footnote 14, pp. 8-9.95 Ibid., p. 9.96 Ibid.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 185
❚ Development Costs/FinancingThe costs of developing a telemedicine project canbe high. These costs include telecommunicationcharges, equipment costs, technical support, train-ing, and administrative support. Many small com-munities operating on their own will be unable toafford these costs. Telemedicine lends itself tocost-sharing as a way of financing projects as wellas assembling the expertise necessary to make itsuccessful. For example, the Medical College ofGeorgia project is a partnership that includes pri-vate industry, the state government, the Gover-nor’s office, academia, and, most importantly, theprimary health care facilities. There are many oth-er examples of groups working together to sharethe expense of building a system. Within commu-nities, systems that are too costly for health ap-plications alone can be shared with educational,local government, social, and community servicesto make the investment feasible.
One suggestion for small rural health care faci-lities is to lease a system for three to five years.The revenue generated by the anticipated increasein bed census and ambulatory care activity couldbe used to offset the leasing costs. Some facilitiesmay still need government support in the form of aloan for start-up purposes before they could as-sume the costs of leasing a system.97
❚ Technological and ImplementationIssues
In implementing a telemedicine project, it is im-portant to first define its objectives, and then se-lect the appropriate technology to meet thoseneeds.98 The focus should be on how telemedicinecan contribute to better clinical decisionmakingand patient care. Depending on what the project isdesigned to achieve, the technology might rangefrom a touchtone telephone to a sophisticatedmultimedia system. This points to the need for
careful planning in advance and a clear under-standing of the project goals. Experience suggeststhe need for a flexible, open system that can easilybe adapted to advances in technology. The com-plexity and sophistication of the technology se-lected will depend on what it is required to do.Transmission speed, image resolution, storage ca-pacity, mobility, and ease of use are importantconsiderations.
Those who will be using the system must beinvolved in its design from the beginning. Onceimplemented, onsite technical assistance is neces-sary to ensure that any technological problems canbe immediately addressed and rectified. It is im-portant that the system be conveniently located soproviders can access it easily. Adequate trainingmust be provided, and the presence of a facilitatorwill ensure that consultations run smoothly. Asdesktop multimedia telemedicine platforms be-come available to place in the health care provid-er’s office, issues of cost, location, convenience,and the operational and maintenance difficultiesof telemedicine will diminish significantly.
One of the barriers to telemedicine is the lackof technical standards. To achieve an integratednetwork of providers, the ability to interconnectusing uniform standards will be essential. (Tech-nical standards are discussed in detail in chapter2.)
Earlier telemedicine demonstration projectsoften did not survive when funding ended. Somealso ceased to function when individuals who hadspearheaded the projects left. Some recent federalgrants made for telemedicine demonstration proj-ects are building in safeguards to ensure that proj-ects have the ability to continue beyond the pilotstage. Some researchers suggest that relying onany government funding can be a potential imped-iment to implementation. Administrators willneed to be convinced that telemedicine consulta-tions will provide the possibility of generating
97 J.H. Sanders, “Telemedicine: Challenges to Implementation,” paper presented at the Rural Telemedicine Workshop sponsored by theOffice of Rural Health Policy, Nov. 3-5, 1993, p. 9.
98 D.S. Puskin, “Telecommunications in Rural America: Opportunities and Challenges for the Health Care System,” Annals of the New YorkAcademy of Sciences, vol. 670, Dec. 17, 1992, pp. 71-72.

186 | Bringing Health Care Online: The Role of Information Technologies
revenue to cover their costs. Assuming reimburse-ment is available for services delivered using tele-medicine, a telemedicine system should only beinitiated if the economics can support its opera-tion.99
❚ Human InfrastructureWhile issues related to technology are importantand often get most of the attention, it is also appar-ent that organizational, management, and humanfactors also play a critical role in implementing atelemedicine system. As one telemedicine userpoints out:
In the final analysis, it will be the humancomponent at each end of the system—not thetechnology—that will determine whether it issuccessful or not.100
A family physician who worked in a hospitalthat had installed a little-used teleradiology sys-tem commented that “the personnel part of theequation is far more complex and difficult than thetechnology part of the equation.”101 For example,the nature of the relationship between the referringand consulting physicians may be a key factor inwhether or not a system is fully used. Existing re-ferral relationships between providers may needto be altered when telemedicine is introduced,which could cause some dislocations and affect itsuse.102
How well the system is organized, managed,and maintained, as well as whether or not it is con-veniently located, will help to determine its rate of
use. Several telemedicine programs have reportedthat scheduling can be a major problem. Becausetime is an important factor to busy professionals,they are likely to be more responsive to using tele-medicine if scheduling is efficient and convenient.This problem may be resolved when the telemedi-cine technology eventually reaches the physi-cian’s desktop.
Resistance to change is often a problem whennew technologies are introduced. Health care pro-fessionals are no exception, and many will not beinterested in or willing to participate in telemedi-cine. Some will feel threatened by the introduc-tion of technology into their practice. However, asone telemedicine pioneer put it:
Telemedicine does not replace the physicianor relegate him to a less important role. Teleme-dicine depends upon him and his special abili-ties, and it offers him a new way to practicemedicine. Through an interactive telemedicinesystem, the fundamental doctor-patient rela-tionship not only can be preserved, but poten-tially augmented, enhanced and more criticallyfocused.103
Nevertheless, telemedicine will change theway providers practice. Some practitioners willmiss the hands-on aspects of examining a patientthat has been such an integral part of their medicaltraining and experience.104 Some may also haveconcerns about the quality of the image or the abil-ity to make an accurate diagnosis based on theavailable equipment.105
99 J.H. Sanders, Professor of Medicine, Medical College of Georgia, personal communication, May 1995.
100 Office of Rural Health Policy, op. cit., footnote 14, p. 13.101 Tom Dean, quoted in “Is Telemedicine the Answer to Rural Health’s Problems?” Rural Health News, vol. 1, No. 2, spring 1994, p. 9.102 P. Whitten and T. Franken, “A Survey of Rural Primary Care Practitioners’ Attitudes and Perceptions of Telemedicine,” abstract book,
Second International Conference on the Medical Aspects of Telemedicine and Second Annual Mayo Telemedicine Symposium, April 1995,p. 6.
103 K.T. Bird, “Telemedicine: Concept and Practice,” in R.L. Bashshur, P.A. Armstrong, and Z.I. Youssef (eds.), Telemedicine: Explorationsin the Use of Telecommunications in Health Care (Springfield, IL: Charles C. Thomas, 1975), p. 90.
104 Researchers at the Georgia Institute of Technology are working on a project to design a glove that could be worn by the consultant thatwould mimic the hands-on experience.
105 Grigsby et al., Report 4, op. cit., footnote 8, p. 7.2.

Chapter 5 Telemedicine: Remote Access to Health Services and Information 1187
The American Telemedicine Association (ATA) was incorporated in 1993 to promote professional,
ethical, and equitable Improvement in health care delivery through telecommunications technology and
to enhance broad-based community telecommunications applications. The Association will: 1) promote
telemedical research and education; 2) assist in the development of telemedical policy and standards,
3) provide education to public and professional organizations; 4) interact with worldwide communica-
tion systems, 5) serve as a clearinghouse for telemedical information and services; and 6) support local
health care system initiatives in telemedicine, especially in medically underserved areas, In November
1994, the Board of Directors adopted a set of telemedicine policy priorities focused on practice guide-
Iines, privacy, Iiability, reimbursement, medical Iicensure, national disasters, technology development,
the national telecommunications Infrastructure, research and demonstrations, and interactive distance
Iearning.
ATA affords a structured forum for clinicians, technologists, research bodies, and public policy insti-
tutions. It has provided leadership in consumer advocacy for reimbursement, provided an emergency
response structure that Incorporated guidance from those at the site in a recent national disaster, stimu-
lated educational and political action with organized medicine, Initiated research and teaching recom-
mendations for medical schools by national medical leaders, and provided testimony before Congress,
SOURCES: American Telemedicine Association information sheet, n d , American Telemedicine Association Policy Priorties, Novem-ber 1994 and Jane Preston President, American Telemedicine Association, personal communication, May 14, 1995
TELEMEDICINE POLICY OPTIONSThere is ongoing activity and interest in telemedi-cine at the federal level in both the executiveand legislative branches. A community of peopleinterested in telemedicine—including representa-tives from federal agencies, Congress, telemedi-cine users, researchers, and vendors—meet in avariety of forums. Hearings have been held, semi-nars have been conducted, and demonstrations oftelemedicine have been provided. At the sametime, the number of organizations, conferences,newsletters, and journals related to telemedicineis rapidly proliferating, and online informationand discussion groups have helped to informpeople about its potential (see appendix E).
Responsibility for telemedicine policy isshared among federal, state, and local lawmakers,and many of the decisions affecting the diffusionof telemedicine are influenced largely by the pri-vate sector. Groups such as the American Teleme-
dicine Association have provided leadership inconsumer advocacy for reimbursement, sti-mulated educational and political action with or-ganized medicine, initiated research and teachingrecommendations for medical schools, and testi-fied before Congress (see box 5-3). Federal effortsto reform both health care and telecommunica-tions, each traveling its separate path, will have animpact on telemedicine’s progress. As noted byone telecommunications expert:
. . . Telemedicine barely rated a blip on the radarscreen when Congress debated new telecommu-nications legislation last year. This omission isall the more remarkable in [that] . . . the othermajor legislative initiative in the 103d Congresswas improving Americans’ access to health carewhile simultaneously controlling health carecosts . . . Congress dealt with communicationsin one hearing room and health care in another[and] failed to connect the two together. 106
106 Newton W. Minow, Director, The Annenberg Washington Program, “Telecommunications, Medicine and the Public Interest,” speech
given at the Second International Conference on the Medical Aspects of Telemedicine and Second Annual Mayo Telemedicine Symposium,Rochester, MN, Apr. 8, 1995.

188 | Bringing Health Care Online: The Role of Information Technologies
Aspects of telecommunications reform relatedto universal service, health care, and tariffs arerelevant to telemedicine. Health care reform ini-tiatives center on reducing costs and improvingaccess and quality. These goals reflect the trendstoward managed care, new competitive strategieson the part of health care providers, and the movetoward outpatient care and away from large inpa-tient facilities.
Federal telecommunications policymakers in-volved in reform initiatives have an important roleto play in ensuring that proposed legislation sup-ports the delivery of health care using telecommu-nications. The Snowe-Rockefeller amendment tothe Telecommunications Competition and Dereg-ulation Act of 1995, S. 652, supports access to theNII for schools, libraries, and rural health careproviders. Section 253 of the Act on UniversalService calls for actions that will benefit consum-ers in rural and high-cost telecommunicationareas. In Congress, both the House/Senate Ad HocCommittee on Telemedicine and Health Care In-formatics and the Congressional Rural Caucuscontinue to explore the potential of telemedicineto meet the needs of their constituents. A teleme-dicine conference held at Airlie House in Virginia,in August 1994, was requested by the Ad HocCommittee, and a report was recently released thatsets out a policy agenda for telemedicine over thenext several years.107
Telemedicine is considered an integral part ofthe Administration’s NII planning efforts. A keyplayer is the Information Infrastructure TaskForce, a forum where both telecommunicationsand health care needs converge. Telemedicine isbeing addressed by a task force subgroup, andconsiderable progress has already been madetoward formulating telemedicine strategies. TheNational Telecommunications and InformationAdministration is helping to fund telemedicinedemonstration projects through its Telecommu-
nications and Information Infrastructure Assist-ance Program. The National Information Infra-structure Testbed, a nonprofit consortium, hasprovided telemedicine demonstrations as part ofits goal of advancing the NII (see box 5-4). Alongwith NII activities, federal agencies such as theOffice of Rural Health Policy, the Rural UtilitiesService, the National Library of Medicine, the De-partment of Defense, the Department of VeteransAffairs, the Agency for Health Care Policy andResearch, and the Health Care Financing Admin-istration support telemedicine in various ways(see appendix D).
Telemedicine is likely to proceed with or with-out federal support. However, federal governmentsupport will be required to guarantee that teleme-dicine benefits those who need it most—peopleliving in rural locations, inner city areas, and Na-tive American communities that the private sectoris likely to bypass for more lucrative areas. In atime of fiscal constraints, any federal funding pro-vided will need to be carefully monitored to en-sure it is being used wisely. If Congress wishes toencourage the diffusion of telemedicine, it canhave the most impact in the areas of research fund-ing and reimbursement for telemedicine services.The two are closely connected, in that formulatinga reimbursement policy is dependent on obtainingsatisfactory answers to many of the questionsraised about telemedicine.
❚ Federal Funding for TelemedicineResearch
One option for Congress is to continue to providefunding for telemedicine demonstration and eval-uation projects. Telemedicine research currentlyunder way is critical to answering many of thequestions about its efficacy and effectiveness.Proposed funding cutbacks could adversely affectthese efforts, many of which are just gettingstarted. Requiring matching funds or other con-
107 Bashshur et al. (eds.), Working Conference on Telemedicine Policy for the NII, sponsored by the Health Information and ApplicationWorking Group of the IITF Committee on Applications and Technology and the Senate/House Ad Hoc Steering Committee on Telemedicineand Health Care Informatics, coordinated by the Center for Public Service Communications (Washington, DC: May 1995).

Chapter 5 Telemedicine: Remote Access to Health Services and Information 1189
The National Information Infrastructure Testbed (NIIT) is a nonprofit consortium of over 50 members
formed by industry with participation by academic institutions and government agencies to accelerate
the development of a National Information Infrastructure (Nil) Members participate in a series of ap-
plication-focused demonstration projects designed to assess the technological, operational, and policy
issues associated with creating an NII. NIIT’s Healthcare Working Group consists of organizations such
as AT&T, Hewlett-Packard, Hughes Aircraft Co , Jet Propulsion Laboratory, Lawrence Livermore Nation-
al Laboratory, Network Systems Corp., Pacific Bell, Polaroid Corp., Sandia National Laboratories,
SunOptics Communications, University of Southern California (USC) Medical Center, the USC-Ad-
vanced Biotechnical Consortium, and WilTel. In September 1994, the NIIT presented a nationwide dem-
onstration via satellite to congressional and Administration staff in Washington, DC The demonstration
was based on a simulated medical emergency using teleconsultation, 3-D Imaging, and real-time col-
laboration in the diagnosis and treatment of a patient.1
SOURCE: Background materials provided by the National Information Infrastructure Testbed, Sept. 20, 1994
1 Background materials provided by the National Information Infrastructure Testbed, Sept. 20, 1994
tributions from those applying for federal grants a fertile area for federal support, perhaps in coop-is one way of leveraging investments in telemedi-cine projects. This mechanism necessitates a ma-jor investment and commitment on the part of thegrantees, which helps ensure that projects willcontinue after federal funding ceases. Innovativeapproaches to funding should be considered wher-ever possible to get the most out of scarce finan-cial resources.
Until recently, there was little or no coordina-tion of telemedicine activities among federalagencies. Mechanisms are now in place throughthe telemedicine working group of the Adminis-tration’s Information Infrastructure Task Force tomonitor and coordinate federal support of teleme-dicine, which is essential in the current climate ofbudget cutbacks and fiscal constraint. Representa-tives of federal agencies have been meeting regu-larly for over a year in an effort to shareinformation and begin to coordinate telemedicinefunding activities.
Current federal funding for telemedicine isheavily weighted toward rural communities. Be-cause telemedicine could provide a partial solu-tion to the severe problems faced by someinner-c it y health care providers, this also would be
eration with private sector organizations. Fundingfor telemedicine demonstrations in other areas,such as public health or geriatrics, could also pro-vide valuable information to Congress and theAdministration about its potential value in im-proving health care delivery.
❚ Fostering Cooperative StrategiesTo reduce the cost barriers of implementing tele-medicine, Congress could provide incentives toencourage cooperative efforts and consortia. Inmany small communities, it makes economicsense for groups to share the costs of implement-ing, operating, and maintaining a telecommunica-tions network. For example, schools, medicalclinics, libraries, social service agencies, and oth-ers who would benefit from improved informationservices may need to join forces to share the costsof a system. Federal funding could be designed toencourage and reward such cooperative efforts.
The U.S. military and NASA have been leadersin research related to telemedicine applications.The military has devised ways to use telecommu-nications to deliver health care to remote areas,whether for battlefield or peacekeeping opera-

190 I Bringing Health Care Online: The Role of Information Technologies
The Telemedine Information Exchange (TIE) was launched in February 1995 by the TelemedicineResearch Center (TRC) at the Oregon Health Sciences University in Portland, Oregon Begun with dem-onstration funding from the Health Care Financing Administration and several private corporations, TIEprovides a comprehensive telemedicine clearinghouse that is easy to use, easily accessible, compre-hensive, and continuously maintained TIE uses available health care Information resources, and cur-rently benefits those directly or indirectly affected by telemedicine, including health care providers, indi-viduals, community and economic development leaders, and rural-based corporations The databasesinclude complete bibliographic Information, listing of active telemedicine programs, Iegislative andfunding information, upcoming meetings, and relevant product and services. Updated weekly, TIE isavailable to users online, 24 hours-per-day, through use of computer modems, toll-free 800 number ser-vices in the continental United States (1 -800 -555 -5 TIE), and the Internet System via World Wide WebClient Access <URL http//tie.telemed.org/ >
SOURCE: D. A. Perednia, Oregon Health Sciences University, personal communication, May 9, 1995
(ions. In some cases, the military is cooperatingwith civilian health care personnel to deliver tele-medicine services. For example, EisenhowerMedical Center is working with the Medical Col-lege of Georgia to develop the “electronic house-call.” In addition, the Army’s health care systemin Georgia will utilize the civilian telemedicine in-frastructure. Walter Reed Army Medical Centerworks with North and South Carolina in collabo-rative telemedicine projects. In a pilot project, theNaval Hospital at Camp Lejeune will link EastCarolina University using asynchronous transfermode technology, focusing on emergency careand teleradiology.108 The military and the Depart-ment of Veterans Affairs have health facilitiesthroughout the country, and could be encouragedto cooperate with local civilian groups in settingup a telemedicine system. Wherever possible,cooperative efforts could be fostered to spread thefederal expertise as broadly as possible and takeadvantage of economies of scale and scope.
■ Disseminating Research ResultsIn many cases, the people who might benefit mostfrom telemedicine applications know very little
about them. The recent increase in seminars andmeetings on the subject, especialy those that offercontinuing medical education credits and researchpresentations, is beginning to fill some of theknowledge gap. Online databases are also helpfulin spreading information about telemedicine.However, as government-supported research re-sults become available, it is important that agen-cies disseminate these as widely as possible toproviders in rural and other underserved areas.The electronic clearinghouse concept would be auseful vehicle to educate potential users, althoughin many cases those with the greatest need to knowmay not have the means to access electronic data-bases.
Congress might wish to ensure that mecha-nisms exist to widely disseminate research resultsand other information about telemedicine. Thiscould be done by a federal agency within DHHS,such as the National Library of Medicine or theOffice of Rural Health Policy.
One of the original goals of the IITF’s telemedi-cine working group was to prepare an online data-base of federal telemedicine projects. When this iscomplete, and if it is kept current, it should pro-
108 From East Carolina University School of Medicine World Wide Web home page <URL:http://www.telemed.med.EDU/>.

Chapter 5 Telemedicine: Remote Access to Health Services and Information | 191
vide information that will track federal spendingon telemedicine. An electronic clearinghouse ofinformation concerning telemedicine would great-ly facilitate the sharing of all types of informationrelated to telemedicine. A viable alternative to afederal clearinghouse would provide support for aprivate-sector group, such as the Telemedicine In-formation Exchange (TIE) network operated bythe Telemedicine Research Center at the OregonHealth Sciences University (see box 5-5). This op-tion would avoid duplication of effort, although adatabase of federal activities might still be desir-able. The major problem with any online databaseis keeping it up to date. Sufficient staff and finan-cial support would be required to do this, whetherin the public or private sectors.
❚ Reimbursing for Telemedicine ServicesBecause the data that would support a uniform re-imbursement policy for telemedicine consulta-tions are not yet available, HCFA is movingslowly and deliberately in accumulating the nec-essary information on which to base a sound deci-sion. This seems a prudent strategy. Experi-menting with reimbursement in certain demon-stration sites will provide valuable insights thatwill eventually enable the agency to craft a carefulpolicy based on actual results. Congress may wishto ensure that adequate funding is provided tosupport those experiments. As the results of theseexperiments become available, Congress maywish to provide oversight and conduct hearings todetermine if further action is required.

Appendix A:Workshop
Participants
Federal Activities Workshop – May 17, 1994
Linda BrinkWalter Reed Army Medical
Center
Max BuffingtonHealth Care Financing
Administration
Robert EsterhayInternational Cancer
Information Center
J. Michael FitzmauriceAgency for Health Care Policy
and Research
James GarvieIndian Health Service
Susan KatzNational Institute of Standards
& Technology
Robert KolodnerDepartment of Veterans
Affairs
Thomas LewisNational Institutes of Health
Daniel MasysNational Library of Medicine
Carole MintzerOffice of Rural Health Policy
John SilvaAdvanced Research Projects
Agency
Paul TibbitsOffice of the Assistant
Secretary of Defense
Joan Turek–BrezinaOffice of the Assistant
Secretary for Planning andEvaluation
Norman WeissmanAgency for Health Care Policy
and Research
Anne Francoeur WilsonHealth Care Financing
Administration
| 193

194 | Bringing Health Care Online: The Role of Information Technologies
Consumer Workshop – July 26, 1994
Fred Wood (Chair)Office of Technology
Assessment
Farrokh AlemiCleveland State University
Gail CasperCase Western Reserve
University
Lowell F. ChristyEast Carolina University
School of Medicine
Tom FergusonSelf–Care Productions
Linda GolodnerNational Consumers League
David H. GustafsonUniversity of Wisconsin,
Madison
James C. HuntUniversity of Tennessee
Karen Storek LangeNew Parents Network
Edward J. MadaraAmerican Self-Help
Clearinghouse
Michael D. McDonaldThe C. Everett Koop Institute
Robert OlsonInstitute for Alternative
Futures
Warner V. SlackHarvard Medical School
Cost and Cost-Effectiveness Workshop – March 9, 1995
Mark GordonThomas Edison State College
Ruby GrewalColumbia University
Shyam HedaINOVA Health System
Tim HillThe Office of Management
and Budget
Harold LehmannJohn Hopkins University
Peter NewmannProject Hope Center for
Health Affairs
Clark ParamoreProject Hope Center for
Health Affairs
Stephen ParenteProject Hope Center for
Health Affairs

Appendix BReviewers
andContributors
Diane AdamsAgency for Health Care Policy
and Research
Laura AdamsMedical College of Georgia
Ace AllenKansas University Medical
Center
G. Octo BarnettMassachusetts General
Hospital
Rashid L. BashshurUniversity of Michigan
Joseph R. BinderRural Utilities Service
Catherine BritainRODEO NET
Naomi BroeringGeorgetown University
Alfred S. BuckJoint Commission on
Accreditation of HealthcareOrganizations
Eric ChristensonCAIRN Healthcare, Inc.
Robert B. CohenEconomic Consultant
Richard CorrellCenter for Health Care
Information Management
Stephen E. CrossCarnegie Mellon University
D. Sophocles DadakisConsultant
Deborah DeatrickHealth Commons Institute
Don DeMoroService Employees Union
International
Steve DownsNational Telecommunications
and InformationAdministration
Elizabeth A. DraperAPACHE Medical Systems,
Inc.
Joseph P. EaglinMacro International Inc.
Thomas D. EastLDS Hospital
Daniel EssinUniversity of Southern
California Medical Center
Lawrence FaganStanford University
Lawrence FrischHumboldt State University
Mark E. FrisseWashington University
Gary J. GagnonAPACHE Medical Systems,
Inc.
Francis GanongKurzweil Applied Intelligence
Reed M. GardnerLDS Hospital
| 195
196 | Bringing Health Care Online: The Role of Information Technologies
Rob GeenMACRO International, Inc.
John GlaserBrigham & Women’s Hospital
Jim GrigsbyUniversity of Colorado
W. Ed HammondDuke University
Linda M. HarrisThe George Washington
University
Debby HindusInterval Research Corp.
Debra HopkinsonAetna Life & Casualty
Max HouseMemorial University of
Newfoundland
Ron HuberCrawford County Hospital
Betsy L. HumphreysNational Library of Medicine
Lisa I. IezzoniBeth–Israel Hospital
Mary G. JonesAlliance for Public
Technology
Michael G. KienzleUniversity of Iowa
William A. KnausAPACHE Medical Systems,
Inc.
Andrew B. LeftonNational Health Information
Center
Gerald C. MacksNational Institutes of Health
William S. MahlerKansas University Medical
Center
Kathleen MathaiQuantitative Medicine
Kathleen McCormickAgency for Health Care Policy
and Research
Kathy MilhollandAmerican Nurses Association
Christopher P. MobergGeorgetown University
Hospital
Alan H. MorrisLDS Hospital
John NorrisConsultant
Keven PatrickU.S. Public Health Service
Douglas PeredniaOregon Health Sciences
University
Dena PuskinOffice of Rural Health Policy
Ron RibitzkyUniversity of Massachusetts
Medical Center
Richard RockefellerHealth Commons Institute
Dan RodeHealthcare Financial
Management Association
Jay H. SandersMedical College of Georgia
Chris SchmandtMIT Media Lab
Ben SchneidermanUniversity of Maryland
Harvey SchwartzAgency for Health Care Policy
and Research
Cary SennettNational Committee for
Quality Assurance
Kim SilvaSystems Plus
Thomas StairGeorgetown University
Hospital
Eric G. TangalosMayo Clinic
Michael TibbottApple Computer
Robbi WatnikHealthcare Financial
Management Association
OTA REVIEWERS
Elaine Power
David Jensen
Judy Wagner
David Wye

Appendix CApplications of
Clinical DecisionSupportSystems1
linical Decision Support Systems (CDSSs)—at leastthose whose effectiveness has been evaluated—performone or more of the following functions: diagnosis, drugdose determination, preventive care reminders, and active
(diagnostic or therapeutic) care advice.1 These applications andsome recent examples —including ones whose effectiveness hasnot been evaluated—are discussed in the following sections.With most of these systems, clinicians do not interact directlywith the computer; rather, staff personnel input the needed data onthe patient and provide the clinician with computer-printed re-ports.2
COMPUTER-AIDED DIAGNOSISThese systems are designed to assist the clinician in determiningthe patient’s exact diagnosis or the condition underlying his/herpresenting health problem. The systems take as input the patient’ssigns and symptoms, physical findings, test results, and back-ground information, and then report one or more possible diag-noses that match that combination of characteristics. The patientdata must ordinarily be manually key-entered in a particular for-mat required by the system. Rather than attempting to cover alldiagnoses, most systems focus on specific health problems.
1 Johnston et al., op. cit., footnote 1. Connelly and Bennett propose a similar schemefor classifying the functions of knowledge-based systems that have clinical laboratory ap-plications: classify (e.g., diagnosis), predict (e.g., adverse events), plan (i.e., recommendspecific actions), monitor (including alerts, reminders, and process control/scheduling),facilitate (make a human task easier), and convey (present data, conclusions, etc.). D.P.Connelly and S.T. Bennett, “Expert Systems and the Clinical Laboratory Information Sys-tem,” Clinics in Laboratory Medicine, vol. 11, No. 1, March 1991, pp. 136-138.
2 Johnston et al., op. cit., footnote 1, p. 137.| 197

198 | Bringing Health Care Online: The Role of Information Technologies
However, several systems, including Dxplain,3
Iliad,4 Meditel,5 and QMR,6 are designed to ad-dress the entire field of internal medicine. Theyemploy either deterministic or probabilistic/adaptive algorithms to produce a list of possiblediagnoses, ranked in order of likelihood.7
DRUG DOSE DETERMINATIONThese systems are designed to assist the clinicianin determining the proper dosage of a specificdrug for a particular kind of patient.8 Some evi-dence suggests that clinicians have a particularlydifficult time calculating drug dosages.9 Again,data on the patient is usually entered manually ina format required by the system. (The patient’sdiagnosis is usually assumed by the system, basedon the drug being used.) The algorithms in theknowledge base then ascertain the proper dosageof the drug in question, either as an exact quantityor as a permissible range. One example of such asystem generates estimates for dosing of amino-phylline for acute asthma cases presenting in theemergency room.10 Commercial programs havealso been developed for dosing of selected drugsbased on patient-specific characteristics and mea-sured drug concentrations.11
PREVENTIVE CARE REMINDERSThese systems are designed to remind the clini-cian to administer a particular preventive servicewhen the patient reaches a certain stage in theprocess of care for a given health problem (e.g.,retinal examination for diabetics), or simply a cer-tain stage of life (e.g., immunization). Unlikecomputer-aided diagnosis and drug-dose deter-mination, which are usually designed to providea single report in response to a specific set of dataon a given patient, a preventive care reminder sys-tem requires repeated input of data on the patientover time. This includes not only the patient’sdiagnoses and other clinical characteristics, butalso the treatments and tests administered andwhen they were administered. To the extent thatthe set of rules for generating reminders representsa model of the disease process for which a preven-tive service is to be administered, they constitutea type of formal clinical protocol.
The protocol specifies exactly what preventivetreatments should be performed at each stage inthe process of care for the health problem at hand,based either on the amount of time that has elapsedsince the previous stage (e.g., a previous treatmentor test) or on data values measuring the patient’s
3 Massachusetts General Hospital, Boston, MA.4 Applied Informatics, Salt Lake City, UT.5 Meditel, Devon, PA.6 CAMDAT, Pittsburgh, PA.7 E.S. Berner et al., “Performance of Four Computer-Based Diagnostic Systems,” New England Journal of Medicine, vol. 330, No. 25, June
23, 1994, pp. 1792-1796; R.A. Miller, “Medical Diagnostic Decision Support Systems—Past, Present, and Future,” Journal of the AmericanMedical Informatics Association, vol. 1, No. 1, January/February 1994, pp. 8-27.
8 R.W. Jelliffe et al., “Adaptive Control of Drug Dosage Regimens: Basic Foundations, Relevant Issues, and Clinical Examples,” Interna-tional Journal of Biomedical Computing, vol. 36, No. 1-2, June 1994, pp. 1-23.
9 S. Rolfe and N.J.N. Harper, “Ability of Hospital Doctors To Calculate Drug Doses,” British Medical Journal, vol. 310, No. 6988, May 6,1995, pp. 1173-1174.
10 E.R. Gonzales et al., “Computer-Assisted Optimization of Aminophylline Therapy in the Emergency Department,” American Journal ofEmergency Medicine, vol. 7, No. 4, July 1989, pp. 395-401.
11 Dasta et al., op. cit., footnote 1.

Appendix C Applications of Clinical Decision Support Systems | 199
condition at that point in time. The RegenstriefMedical Record System at Indiana University12
was apparently the first CDSS to develop a com-prehensive set of preventive care reminders, forexample, to administer influenza vaccinations.13
More specialized examples include two systemsthat provide reminders to perform blood pressuremeasurement and cervical cancer screening, re-spectively.14 The HealthQuiz program elicitsbackground information and risk factors from pa-tients, then compares their answers to detailedpreventive care guidelines, flags problems, andrecommends appropriate interventions.15
ACTIVE-CARE ADVICEThese systems are designed to assist the clinicianin performing diagnostic or therapeutic proce-dures (including pharmaceutical treatments)when the patient reaches certain stages in the proc-ess of care for a given health problem, again oftenmodeled in a formal clinical protocol. An active-care advisory system requires repeated input ofdata on the patient’s health problems, tests, andtreatments over time. The protocol specifies ex-actly what diagnostic and therapeutic proceduresshould be performed at each stage in the processof care for the health problem at hand. This type
of computer-based clinical advice can take six ba-sic forms:
1. Treatment recommendations (including phar-maceuticals) appropriate for the health problemat hand, for example, the MYCIN program thatprovides diagnostic and treatment advice forpatients with meningitis,16 and the antibioticconsultant component of the Health Evaluationthrough Logical Processing (HELP) system atLDS Hospital in Salt Lake City, Utah, that rec-ommends appropriate antibiotics in light of thepatient’s characteristics and specific infection,drawn from an electronic medical record.17
2. Reminders to the clinician to perform specificdiagnostic or therapeutic procedures at certainstages in the process of caring for the healthproblem at hand, such as adult respiratory dis-tress syndrome in the HELP system.18
3. Alerts to the clinician regarding potential ad-verse events, for example, worsening of the pa-tient’s condition, based on feedback ofabnormal test results.19
4. Feedback (including alerts) regarding ordersthat the clinician entered for the patient, includ-ing:
� possibly inappropriate treatments, given thepatient’s complicating health problems and/or
12 C.J. McDonald et al., “The Regenstrief Medical Record System: 20 Years of Experience in Hospitals, Clinics, and Neighborhood HealthCenters,” M.D. Computing, vol. 9, No. 4, July/August 1992, pp. 206-217.
13 C.J. McDonald, S.L. Hui, and W.M. Tierney, “Effects of Computer Reminders for Influenza Vaccinations on Morbidity During InfluenzaEpidemics.” MD Computing, vol. 9, No. 5, September-October 1992, pp. 304-312.
14 I. McDowell, C. Newell, and W. Rosser, “A Randomized Trial of Computerized Reminders for Blood Pressure Screening in PrimaryCare,” Medical Care, vol. 27, No. 3, March 1989, pp. 297-305; I. McDowell, C. Newell, and W. Rosser, “Computerized Reminders To Encour-age Cervical Screening in Family Practice,” Journal of Family Practice, vol. 28, No. 4, April 1989, pp. 420-424.
15 “’HealthQuiz’ Makes Preventive Care Guidelines Easy To Apply,” Report on Medical Guidelines & Outcomes Research, Jan. 26, 1995,pp. 5-6.
16 E.H. Shortliffe, “Computer Programs To Support Clinical Decision Making,” Journal of the American Medical Association, vol. 258, No.1, July 3, 1987, pp. 61-66.
17 R.S. Evans, D.C. Classen, and S.L. Pestotnik, “Improving Empiric Antibiotic Selection Using Computer Decision Support,” Archives ofInternal Medicine, vol. 154, No. 8, Apr. 25, 1994, pp. 878-884.
18 A.H. Morris, “Protocol Management of Adult Respiratory Distress Syndrome,” New Horizons, vol. 1, No. 4, November 1993, pp.593-602.
19 K.E. Tate, R.M. Gardner, and L.K. Weaver, “A Computerized Laboratory Alerting System,” M.D. Computing, vol. 7, No. 5, September-October 1990, pp. 296-301; D.M. Rind et al., “Effect of Computer-Based Alerts on the Treatment and Outcomes of Hospitalized Patients,”Archives of Internal Medicine, vol. 154, No. 13, July 11, 1994, pp. 1511-1517.

200 | Bringing Health Care Online: The Role of Information Technologies
background characteristics (even if the treat-ment would otherwise be appropriate for thehealth problem at hand), for example, alerts re-garding drug allergies in the order-entry systemat Brigham and Women’s Hospital in Boston;20
� possibly inappropriate treatments regardless ofthe patient’s health problems or characteristics,for example, commercial programs to detectdrug-drug and drug-nutrient interactions;21
� likely conflict or redundancy between a chosentest and others already ordered for the patient;22
� likely results of a test ordered for the patient; ifthe probability of an abnormal result is low, theclinician can reconsider whether the test is real-ly worth performing;23
� results of previous tests on the patient that arelike the one being ordered, so the clinician mayreconsider whether the test really needs to berepeated;24
� the cost of a test or treatment ordered for the pa-tient, so the clinician can reconsider whether itis really worth performing;25 and
� tests or treatments that would be less costlythan the one ordered, but equally effective intreating the health problem at hand.26
5. Prompts to the clinician for decisions regardingtesting or treatment options, or for entry of in-formation on the patient’s health problems orbackground, as in the drug order-entry systemat Brigham and Women’s Hospital.27
6. Prognoses of intensive care unit patients basedon such predictors as severity of illness (usingvital signs and other physical measures) andphysiological reserve (age and complicatinghealth problems) in the Acute Physiology andComprehensive Health Evaluation (APACHE)system.28 APACHE is also used as a method ofmeasuring severity of illness and risk-adjustingoutcome measures.29 An expanded prognosticmodel known as SUPPORT (Study to Under-stand Prognoses and Preferences for Outcomesand Risks of Treatments) is designed to predictsurvival to 180 days (rather than to discharge)and includes patients who are not severely ill.30
20 R. F. Gibson and B. Middleton, “Health Care Information Management Systems To Support CQI,” Clinical Practice Improvement: A NewTechnology for Developing Cost-Effective Quality Health Care, S.D. Horn and D.S.P. Hopkins (eds.) (New York, NY: Faulkner & Gray, 1994),pp. 116-117.
21 T.I. Poirer and R. Giudici, “Evaluation of Drug Interaction Microcomputer Software: Comparative Study,” Hospital Pharmacy, vol. 26,No. 1, January 1991, pp. 30-37; T.I. Poirer and R. Giudici, “Evaluation of Drug-Food/Nutrient Interactions Microcomputer Software Pro-grams,” Hospital Pharmacy, vol. 26, No. 6, June 1991, pp. 533-540.
22 Connelly and Bennett, op. cit., footnote 2.23 W.M. Tierney et al., “Computer Predictions of Abnormal Test Results: Effects on Outpatient Testing,” Journal of the American Medical
Association, vol. 259, No. 8, Feb. 26, 1988, pp. 1194-1198.24 W.M. Tierney et al., “Computerized Display of Past Test Results: Effect on Outpatient Testing,” Annals of Internal Medicine, vol. 107, No.
4, October 1987, pp. 569-574.
25 W.M. Tierney, M.E. Miller, and C.J. McDonald, “The Effect on Test Ordering of Informing Physicians of the Charges for Outpatient Diag-nostic Tests,” New England Journal of Medicine, vol. 322, No. 21, May 24, 1990, pp. 1499-1504.
26 W.M. Tierney et al., “Physician Inpatient Order Writing on Microcomputer Workstations: Effects on Resource Utilization,” Journal of theAmerican Medical Association, vol. 269, No. 3, Jan. 20, 1993, pp. 379-383.
27 Gibson and Middleton, op. cit., footnote 21.28 W.A. Knaus, D.P. Wagner, and J. Lynn, “Short-Term Mortality Predictions for Critically Ill Adults: Science and Ethics, Science, vol. 254,
No. 5030, Oct. 18, 1991, pp. 389-394; J.E. Zimmerman, W.A. Knaus, and M. Seneff, “Outcome Prediction in Intensive Care,” Intensive CareRounds, No. 10125 (Abingdon, England: The Medicine Group (Education), Ltd., January 1993).
29 L.I. Iezzoni, “Risk Adjustment for Medical Outcome Studies,” Medical Effectiveness Research Data Methods, M.L. Grady and H.A.Schwartz (eds.), Agency for Health Care Policy and Research, AHCPR Pub. No. 92-0056 (Rockville, MD: July 1992), pp. 83-97.
30 W.A. Knaus et al., “The SUPPORT Prognostic Model: Objective Estimates of Survival for Seriously Ill Hospitalized Adults,” Annals ofInternal Medicine, vol. 122, No. 3, Feb. 1, 1995, pp. 191-203.

Appendix DExecutive
BranchTelemedicine
Activities
n September 1993, the Clinton Administration published itsAgenda for Action report, outlining its vision of the Nation-al Information Infrastructure (NII) and specific actions thegovernment would take.1 By Executive Order 12864, the
President appointed the Information Infrastructure Task Force(IITF), under the direction of the Secretary of Commerce. TheIITF is comprised of high-level representatives of the federalagencies that play a role in developing and applying informationand telecommunications technologies, including independentagencies and commissions such as the Federal CommunicationsCommission. The President also appointed the Advisory Councilon the NII, which broadly represents the key constituencies af-fected by the NII (business, labor, academia, public interestgroups, and state and local governments).2
The IITF’s Committee on Applications and Technology coor-dinates efforts to develop, demonstrate, and promote applicationsof the NII and develops and recommends technology strategy andpolicy to accelerate its implementation. One of the subgroups ofthe Health Information and Applications Working Group is re-sponsible for telemedicine. The purpose of the telemedicine sub-group is to promote the efficient, effective use of telemedicine inthe delivery of health care services through the coordination offederal resources and policies. In August 1994, the IITF Health In-
1Information Infrastructure Task Force, “The National Information Infrastructure:Agenda for Action,” National Telecommunications and Information Administration,Washington, DC, Sept. 15, 1993.
2NII Principles and Actions: A Checklist of the Clinton Administration’s Progress,September 1993-94, September 1994, p. 3.
| 201

202 | Bringing Health Care Online: The Role of Information Technologies
formation and Applications Working Group con-vened a meeting of experts to devise a policy strat-egy for telemedicine. In April 1995, a report of theconference’s conclusions and recommendationswas released.3
In March 1995, Vice President Al Gore re-quested the Department of Health and Human Ser-vices (DHHS) to lead an interagency effort toaddress and resolve major policy issues involvedin the NII and the health sector.4 This effort is tobe coordinated with the ongoing work of the In-formation Infrastructure Task Force. With respectto telemedicine, DHHS was asked to prepare a re-port on current telemedicine projects, the range ofpotential telemedicine applications, and publicand private actions to promote telemedicine and toremove existing barriers to its use.
The federal government has funded a numberof pilot projects in telemedicine over the past 30years. There is currently a good deal of interest inand funding for both demonstration projects andevaluation projects, although proposed budgetcutbacks could have a significant negative effecton funding for telemedicine projects . A sample ofexecutive branch telemedicine activities is pro-vided below.
DEPARTMENT OF HEALTH AND HUMANSERVICESThe Office of Rural Health Policy (ORHP), in theHealth Resources and Services Administration,has been involved in telemedicine for more than5 years, mainly providing grant funding for dem-onstration projects. These have included TexasTech University (in cooperation with the HealthCare Financing Administration and the Assistant
Secretary for Planning and Evaluation), West Vir-ginia University’s Robert C. Byrd HealthSciences Center in Morgantown, and RODEONET in Oregon (described in chapter 5). ORHPsponsored a workshop in November 1993 to ex-plore major telemedicine policy issues and therole of telemedicine systems in rural health carenetwork development. Conference deliberationsresulted in the publication of the report, ReachingRural.5
In November 1994, ORHP awarded three-yeargrants totaling $4.5 million to support 11 teleme-dicine projects in 10 states. These were awardedunder the Rural Telemedicine Grant Program, andwill demonstrate the use of telemedicine as part ofrural health network development and provide abaseline of information for conducting a system-atic evaluation of telemedicine systems servingrural areas. Cost participation was required on thepart of grantees. In addition, continuation fundingof $800,000 was granted to the Robert C. ByrdHealth Sciences Center telemedicine pilot projectin West Virginia. In the fall of 1994, ORHP alsoawarded a grant for an 18-month evaluation oftelemedicine projects.
The Health Care Financing Administration(HCFA) is a key player in telemedicine in terms ofdeveloping policies for Medicare and Medicaidreimbursement of telemedicine services. Theagency has supported several research projects intelemedicine, most notably at Texas Tech Univer-sity (with the Assistant Secretary for Planning andEvaluation and ORHP) and Iowa Methodist Hos-pital in Des Moines. HCFA also supported theUniversity of Colorado’s Center for Health PolicyResearch in a study to develop a framework for
3Report of the Working Conference on Telemedicine Policy for the NII, sponsored by the Health Information and Application WorkingGroup of the IITF Committee on Applications and Technology and the Senate/House Ad Hoc Steering Committee on Telemedicine andHealth Care Informatics, April 1995.
4Vice President Al Gore, memorandum to Donna Shalala, Secretary of Health and Human Services, Washington, DC, Mar. 8, 1995.5Reaching Rural, Office of Rural Health Policy, Health Resources and Services Administration, Public Health Service, Department of
Health and Human Services, 1994.

Appendix D Executive Branch Telemedicine Activities | 203
evaluating various types of telemedicine.6 In thesummer of 1994, new grants were awarded as partof a congressionally supported research and dem-onstration program. HCFA provided startup fund-ing for the Clinical Telemedicine CooperativeGroup, an ad hoc alliance to share common tele-medicine research protocols and testing method-ologies; it also provided some startup funding forthe Telemedicine Information Exchange(TIE), adatabase established at the Telemedicine Re-search Center, Oregon Health Sciences Universi-ty. HCFA is also providing some of the support forthe Institute of Medicine’s study of evaluation cri-teria for telemedicine.
The National Library of Medicine (NLM),through the High Performance Computing andCommunications Program (HPCC), funds ap-plications research in a number of areas, includingtelemedicine. For example, the National Labora-tory for the Study of Rural Telemedicine at theUniversity of Iowa has recently received a three-year grant of $7.3 million to test the use of Iowa’sfiberoptic network to link medical facilities and li-braries at the University to hospitals, clinics, andperhaps doctors’ offices, throughout the state.Oregon Health Sciences University, University ofPittsburgh, and West Virginia University also re-ceived funding for telemedicine projects from theHPCC Health Care Awards. NLM is the principalfunder of an Institute of Medicine study under wayon criteria for evaluation of telemedicine projects.NLM has also compiled a telemedicine bibliogra-phy containing more than 1,600 citations that isalso available on the Internet.7
The Agency for Health Care Policy and Re-search (AHCPR) helped to support the develop-
ment of telemetry (transmitting electrocardiogramsand vital signs), and telemedicine (including theearly NASA STARPAHC project on the PapagoIndian Reservation in Arizona). It has also pro-vided support for meetings on telemedicine.
DEPARTMENT OF AGRICULTUREThe Rural Utilities Service (RUS) (formerly theRural Electrification Administration) sponsorsthe Distance Learning and Medical Link GrantProgram, which demonstrates the ability of ruralcommunities to utilize existing or proposed tele-communications systems to achieve sustainable,cost-effective distance learning or medical-linknetworks. Implemented in fiscal year 1993, a totalof $20 million in funding has been committed toa total of 61 projects. Approximately 20 of theseare primarily medical links and a majority havesome health-related aspects. For fiscal year 1995,a total of $7.5 million is available to fund $75 mil-lion in applications from about 250 applicants.8
For Medical Link Projects, RUS funds equipmentused in physician consultation, teleradiology, andeducating rural health care providers. Some of theequipment includes teleradiology workstations,x-ray scanners, and digital microscopes, as well asdistance-learning equipment such as encodingand decoding devices, specialized cameras andvideo monitors, video switchers, microphonemixers, computers, and local area networkingequipment.
DEPARTMENT OF COMMERCEIn October 1994, the National Telecommunica-tions and Information Administration (NTIA),through its Telecommunications and Information
6The Center for Health Policy Research, Denver, CO, produced four reports for HCFA. Jim Grigsby et al., Analysis of Expansion ofAccess to Care Through Use of Telemedicine and Mobile Health Services: 1) Literature Review and Analytic Framework, December 1993;2) Telemedicine Policy: Quality Assurance, Utilization Review, and Coverage, August 1994; 3) Study Summary and Recommendations forFurther Research, December 1994; and 4) Telemedicine Policy: Coverage and Payment, February 1995.
7”Telemedicine: Past, Present, and Future, January 1966 through March 1995,” Current Bibliographies in Medicine, CBM No. 95-4,National Library of Medicine, U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, Be-thesda, MD. Internet access through FTP to nlmpubs.nlm.nih.gov and login as anonymous.
8J.R. Binder, Director, Rural Development Assistance Staff, Rural Utilities Service, personal communication, May 10, 1995.

204 | Bringing Health Care Online: The Role of Information Technologies
Infrastructure Assistance Program (TIIAP),awarded more than $24 million for fiscal year1994 to support the development of the NII. A to-tal of 14 of 92 grants were for planning and dem-onstration projects that are designed to develop,demonstrate, and promote applications of in-formation technology that will educate, restrainhealth care costs, improve quality, and increaseaccess to health care with the potential for wide-scale deployment and interconnection over NIInetworks. Grantees were required to providematching funds.
DEPARTMENT OF DEFENSE (DOD)The Medical Research and Materiel Command,Fort Detrick, is conducting several telemedicineand teleradiology projects in cooperation withother branches of the military and various univer-sities. The Walter Reed Army Medical Center(WRAMC) has successfully employed telemedi-cine in Somalia, Croatia, Macedonia, and Haiti.WRAMC is also working with several southernstates to develop peacetime clinic and hospitalconsultation procedures. The Center has also tak-en the lead with the Uniformed Services Universi-ty of the Health Sciences in establishing a militarytelemedicine initiative to provide retrospectiveand prospective evaluations of the various proj-ects.
The Medical Diagnostic Imaging Support(MDIS) system, developed by DOD based on thecommercial Picture Archiving and Communica-tion System (PACs), is employed in several telera-diology networks that use satellites as well as landlines to connect military treatment facilities witheach other and with ambulatory clinics and uni-versity medical centers throughout the world.These projects include the Hilltop Plan (based onfour central sites in the United States and Korea),the AKAMAI project (linking Tripler Army Med-ical Center in Hawaii with several sites around thePacific Rim), and Project Daybreak (linking sev-
eral remote sites in Korea with Tripler as well asthe central site in Seoul). Future plans envision in-tegration of MDIS with other health care informa-tion systems, including computer-assisteddiagnosis programs, multimedia devices, and ref-erence databases.
Other branches of the military are also using avariety of telemedicine systems to better meettheir needs to deliver health care to their membersin a variety of settings. The Tri-Service Telemedi-cine Testbed Project, established in September1994, provides a plan for guiding the TestbedProject and integrating telemedicine technologiesinto the Military Health Services System. This ac-tion also implemented the National Digital Tele-medicine Testbed initiative of the DOD NationalPerformance Review. In July 1995, the ArmyMedical and Materiel Development Commandand the ISIS Center, Georgetown University Med-ical Center, co-sponsored a meeting to develop ap-proaches for DOD technology assessment andevaluation of telemedicine.9
NATIONAL AERONAUTICS AND SPACEADMINISTRATION (NASA)NASA has had a long-term involvement in tele-medicine activities. The agency is interested intelemedicine for medical care in space for futurelong-duration space platforms and to minimizerisk to astronauts. NASA was involved in the ear-ly STARPAHC Program, as well as the Space-bridge to Armenia, which provided consultationsvia satellite to a disaster area in 1988. NASA wasrecently involved in a joint effort with Russia, theSpacebridge to Moscow, to link several U.S. med-ical centers with a hospital in Moscow. Theagency also participated with the Mayo Clinic ina telemedicine feasibility study with the PineRidge Indian Reservation in 1994. In September1994, NASA joined with the Uniformed ServicesUniversity of the Health Sciences in sponsoringthe Second International Conference on Teleme-
9The Chestertown Roundtable, “Developing Approaches for DOD Technology Assessment and Evaluation of Telemedicine,” Chester-town, MD, July 30-August 1, 1995.

Appendix D Executive Branch Telemedicine Activities | 205
dicine: Remote Health Care and Disaster Re-sponse.10
DEPARTMENT OF VETERANS AFFAIRS(VA)The VA is testing the use of its electronic mail sys-tems for teleconsultation. This system handlestext, images, voice, scanned documents, electro-cardiogram signals, and patients’ reports. Usingthe VA’s wide area network, this capability will al-low consultations between physicians at differentVA locations. The Birmingham (AL) VAMCplans to purchase videoconferencing equipmentfor all VA medical centers in Alabama. Thisequipment will be placed in the treatment areas of
the hospitals. Physicians will be able to consultwith specialists prior to transporting patients forspecialty care, including discussing x-rays andother pertinent medical data. The patient will alsobe able to participate in these discussions, if feasi-ble and medically advisable. It is believed that thiswill greatly reduce the number of patients needingto be transported for care, and will also serve as aneducation tool for physicians. Also, the Tusca-loosa VAMC has transmitted radiology images tothe Birmingham VAMC for reading by the radiol-ogist in residence. The VA is also a supporter ofthe Institute of Medicine study of evaluation crite-ria for telemedicine.
10The conference proceedings are published in three special issues of the Journal of Medical Systems, vol. 19, No. 1, February 1995;vol. 19, No. 2, April 1995; and vol. 19, No. 3, June 1995.

Appendix EElectronic
HealthInformation
Sources
n enormous amount of health information is now avail-able in electronic form. Until recently, most of these re-sources were accessible through dial-up bulletin boardsystems or, if the files resided on a computer connected to
the Internet, through a number of different means of transferringcopies of the files from the source computer to a remote user’scomputer. Recently, however, a new graphical interface to the In-ternet, known as the World Wide Web (WWW), has made it pos-sible to rapidly retrieve, arrange, and display on web pages thecontents of files—rather than just their names—and for users totransfer from resource to resource along a virtually endless web ofhyperlinks with the click of a mouse button.
This appendix briefly surveys some of the audio, visual, textu-al, and hypertextual health information available on the WWW.The Uniform Resource Locator (URL) that accompanies eachelectronic resource identifies its location and filename and the ap-propriate method for accessing the files. The URLs are used byweb browser software, such as Netscape Navigator,1 Mosaic,2 orLynx,3 to locate and retrieve the files. This list of web sites repre-sents only a sample of the wide variety of free health informationthat is available on the WWW.
1 Netscape Communications Corp., <URL: http://home.netscape.com/ >. URLslisted in this appendix are accurate as of the date of publication but will change over time.The indices mentioned in the last section of the appendix should be consulted for updatedaccess information.
2 National Center for Supercomputer Applications, <URL: http://www.ncsa.uiuc.e-du >.
3 W3 Consortium, <URL: http://www.w3.org/hypertext/WWW/Lynx/Status.html >.| 207

208 | Bringing Health Care Online: The Role of Information Technologies
CONSUMER AND PATIENT INFORMATIONUniversity health clinics are a rich source of in-formation for consumers and patients. Sites suchas Healthwise4 at Columbia University, theHEALTHLINE Server5 at the University of Mon-tana, and the HealthInfo Gopher6 at Rice Univer-sity offer multimedia educational materials,advice columns, mailing lists, and other resourcesaddressing preventive medicine, nutrition, AIDS,sports medicine, drug and alcohol abuse, women’shealth, sexuality, and other general health in-formation topics. Abstracts and summaries of ar-ticles about health issues from newspapers and thepopular press are collected at sites such as Bio-medicine and Health in the News7 and Health andMedicine in the News.8 The Iowa Health Book atThe Virtual Hospital9 has patient information,such as a guide for helping a child cope with visit-ing a family member hospitalized in an intensivecare unit. The TALARIA Hypermedia ClinicalPractice Guidelines for Cancer Pain10 and thePharmInfoNet DrugDB11 (a descriptive databaseof pharmaceuticals and their effects, organized ac-cording to generic and trade names) are two otherexamples of resources available throughout theweb that may help consumers understand com-
plex medical care. In addition, the web indicessummarized at the end of this appendix containsubscription information for a huge variety of e-mail mailing lists and Usenet discussion groupsconcerning specific diseases and health condi-tions.
RESOURCES FOR HEALTHPROFESSIONALSNumerous web pages contain information and hy-perlinks designed for specific health profession-als. Nightingale,12 NP Web,13 Physician’s Guideto the Internet,14 and the Interactive Medical Stu-dent Lounge15 are sites designed respectively fornurses, nurse practitioners, physicians, and medi-cal students. Sites such as the Emergency Medi-cine and Primary Care Home Page16 provideresources and discussion forums for specializedhealth disciplines, and reference sites such as theCHORUS Collaborative Hypertext of Radiolo-gy17 contain quick reference materials. Cumula-tive indices of research literature from over 20different subject areas in biomedicine are main-tained at Current Bibliographies in Medicine.18 Avariety of sites are devoted to medical education.Some, such as the University of California at San
4 Columbia University Health Service, Health Education and Wellness Program, <URL: http://www.cc.columbia.edu/cu/healthwise/ >.5 University of Montana Student Health Services, <URL: http://healthline.umt.edu:700/ >.6 Rice University Student Health Service, <URL: gopher://riceinfo.rice.edu/11/Safety/HealthInfo >.7 University of Connecticut Health Center, Lyman Maynard Stowe Library, <URL: gopher://inform.uchc.edu/11go-
pher_root%3a%5b_data04._data0401%5d >.
8 University of Minnesota, <URL: gopher://lenti.med.umn.edu:71/11/news/citations >.9 University of Iowa College of Medicine, Department of Radiology, Electric Differential Multimedia Laboratory, <URL: http://indy.ra-
diology.uiowa.edu/VirtualHospital.html >
10 University of Washington, Department of Statistics, <URL: http://www.stat.washington.edu/TALARIA/TALARIA.html >.11 Pharmaceutical Information Associates, Ltd., <URL: http://pharminfo.com/drugdb/db_mnu.html >.12 University of Tennessee at Knoxville, College of Nursing, <URL: http://nightingale.con.utk.edu:70/0/homepage.html >.13 University of New Hampshire, Department of Nursing, <URL: http://unhinfo.unh.edu/unh/acad/health/nursing/index.html >.14 NetRep Explorist, <URL: http://www.netrep.com/global/biz/pgi/pgi.html >.
15 University of Kansas, <URL: http://falcon.cc.ukans.edu:80/~nsween/ >.16 Emergency Medicine Bulletin Board System, <URL: http://www.njnet.com/~embbs/ >.17 Medical College of Wisconsin, <URL: http://chorus.rad.mcw.edu/chorus.html >.18 National Library of Medicine, <URL: ftp://nlmpubs.nlm.nih.gov/bibs/cbm/ >.

Appendix E Electronic Health Information Sources | 209
Francisco Primary Care Teaching Module19 andThe Interactive Patient,20 are designed for medi-cal students and residents, and others—includingthe University of Washington Radiology Webserv-er,21 the Interesting Case Conference,22 and Med-Ed23—offer practice in diagnosis or continuingmedical education courses. MedSearch America24
is an electronic bank of job listings for health pro-fessionals.
MEDICAL IMAGESAs web browsers capable of displaying photo-graphic images and video clips have been devel-oped, the World Wide Web has become an idealmedium for distributing medical images forinstructional and historical purposes. The VisibleHuman Project25 documents human anatomy in aseries of magnetic resonance, photographic, andcomputerized tomography images of cross-sec-tions of a human body at one millimeter intervals;the Visible Embryo Project26 is a related compila-tion of images illustrating human developmentalembryology. The GE Three Dimensional Medical
Reconstruction27 page includes animated “fly-throughs” of heart arteries, the lungs, and thebrain, and a simulation of a baby delivery. A com-pendium of brain images is found at the WholeBrain Atlas.28 The Medical Illustrator’s HomePage29 serves as a contact point for medical illus-trators, publishers, authors, and medical schools.Nearly 60,000 historical images from the archivesof the National Library of Medicine are found inOnLine Images from the History of Medicine.30
An index of other medical imaging resources isfound at Medical Imaging on the Web.31
TELEMEDICINE AND RURAL MEDICINEInformation about distance medicine, telemedi-cine, and rural medicine can be found at the Tele-medicine Information Exchange,32 TelemedicineResources,33 REACH-TV,34 and RuralNet.35
HEALTH POLICY AND GOVERNMENTMany government agencies maintain WWW siteswith information for both health care profession-als and health care consumers. The web site at the
19 Stanford University and the University of California at San Francisco, Divisions of General Internal Medicine, <URL: http://www-med.Stanford.EDU/MedCenter/MedSchool/DGIM/Teaching/Modules-index.html >.
20 Marshall University School of Medicine, <URL: http://medicus.marshall.edu/medicus.htm >.
21 University of Washington, Department of Radiology, <URL: http://www.rad.washington.edu/ >.22 Massachusetts General Hospital, Department of Emergency Medicine, <URL: http://emergency.mgh.harvard.edu/wicc.htm >.23 Loyola University (Chicago) Medical Education Network, <URL: http://www.meddean.luc.edu/lumen/MedEd/Medpage.html >.24 MedSearch America, <URL: gopher://gopher.medsearch.com:9001/1 >.25 National Library of Medicine, <URL: http://www.nlm.nih.gov/extramural_research.dir/visible_human.html >.
26 National Museum of Health and Medicine, Human Developmental Anatomy Center <URL: http://bubba.afip.mil/ >.27 General Electric Corporate Research and Development, <URL: http://www.ge.com/crd/ivl/three_dim_medical.html >.28 Harvard Medical School, <URL: http://www.med.harvard.edu/AANLIB/home.html >.29 Mednexus, <URL: http://www.mednexus.com/med_illustrator/index.html >.30 National Library of Medicine, <URL: http://www.nlm.nih.gov/hmd.dir/oli.dir/ >.
31 Center for Advanced Studies, Research, and Development in Sardinia, <URL: http://www.crs4.it/~france/MEDICAL/institu-tions.html >.
32 Telemedicine Research Center, <URL: http://tie.telemed.org/ >.33 University of Washington, Image Computing Systems Laboratory, <URL: http://icsl.ee.washington.edu/~cabralje/tmresources.html >.
34 East Carolina University School of Medicine, Center for Health Sciences Communication, <URL: http://www.telemed.med.ecu.edu/telemenu.htm >.
35 Marshall University School of Medicine, <URL: http://ruralnet.mu.wvnet.edu/ >.

210 | Bringing Health Care Online: The Role of Information Technologies
Health Care Financing Administration36 containsinformation about Medicare and Medicaid, andthe web site at the Department of Health and Hu-man Services37 guides consumers to a wide vari-ety of health information available throughagencies such as the Food and Drug Administra-tion38 and the National Institute on Aging.39 TheHealth Services/Technology Assessment Text40
includes the full text of clinical practice guide-lines, quick-reference guides for clinicians, andconsumer brochures developed with the supportof the Agency for Health Care Policy and Re-search. The Centers for Disease Control and Pre-vention41 and the Public Health Service42
maintain WWW sites with information aboutcommunicable diseases, epidemics, and popula-tion-based health care. Many institutions, such asthe World Health Organization,43 maintain websites with information on international health is-sues. A useful index to governmental health in-formation resources is found at the NationalHealth Information Center.44
STANDARDSTwo useful web resources dedicated to the varioustechnical standards discussed throughout this re-port are the MSDS Healthcare Standards HomePage45 and the Gateway to Standards Organiza-tions.46
PROFESSIONAL ORGANIZATIONS ANDJOURNALSMany professional societies including the Ameri-can Medical Informatics Association,47 theAmerican Psychological Society,48 and the In-ternational Society of Nephrology49 maintainweb pages with membership information andnews about society activities and publications.Peer-reviewed academic journals are beginning toappear online, including The Digital Journal ofOphthalmology50 and The Journal of MedicalImaging,51 as well as government publicationssuch as the Morbidity and Mortality Weekly Re-port.52
36 Health Care Financing Administration, <URL: http://www.ssa.gov/hcfa/hcfahp2.html >.37 Department of Health and Human Services, <URL: http://www.os.dhhs.gov/ >.38 U.S. Food and Drug Administration, <URL: http://www.fda.gov/fdahomepage.html >.39 National Institute on Aging, <URL: gopher://gopher.os.dhhs.gov/1/dhhs/aoa/aoa/agepages >.40 National Library of Medicine, <URL: http://text.nlm.nih.gov/ >.
41 Centers for Disease Control and Prevention, <URL: http://www.cdc.gov/ >.42 Public Health Service, <URL: http://phs.os.dhhs.gov/phs/phs.html >.43 World Health Organization, <URL: http://www.who.ch/programmes/WHOProgrammes.html >.44 National Health Information Center, <URL: http://nhic-nt.health.org/ >.45 Duke University Medical Center Information Systems, <URL: http://www.mcis.duke.edu:80/standards/ >.
46 United Technologies National Standards System Network, <URL: http://hsdwww.res.utc.com/std/gateway/orgindex.html >.47 American Medical Informatics Association, <URL: http://amia2.amia.org/ >.48 American Psychological Society, <URL: http://psych.hanover.edu/APS/ >49 International Society of Nephrology—Renal Pathology Society, <URL: http://synapse.uah.ualberta.ca/synapse/000p0035.htm >.50 Massachusetts Eye and Ear Infirmary, Department of Ophthalmology, <URL: http://www.meei.harvard.edu/meei/DJOhome.html >.
51 Johns Hopkins University, School of Medicine, Department of Radiology and the William H. Welch Medical Library,<URL: http://jmi.gdb.org/JMI/ejourn.html >.
52 Centers for Disease Control and Prevention, <URL: http://www.crawford.com/cdc/mmwr/mmwr.html >.

Appendix E Electronic Health Information Sources | 211
INDICESThe World Wide Web resources listed above areonly a small fraction of the existing sites, and newsites are being developed at a very rapid pace. Sev-eral sites maintain current catalogs of health in-
formation resources on the Internet. The indexsites include Medical Matrix,53 IHPNet,54 Hospi-tal Web,55 The Whole Internet Catalog: Healthand Medicine,56 MedWeb,57 and the Yahoo! Medi-cine List.58
53 Internet Working Group of the American Medical Informatics Association, <URL: http://kuhttp.cc.ukans.edu/cwis/units/medcntr/Lee/HOMEPAGE.HTML >.
54 International Network for Interfaith Health Practices, <URL: http://www.interaccess.com/ihpnet/health.html >.
55 Massachusetts General Hospital, Department of Neurology, <URL: http://dem0nmac.mgh.harvard.edu/hospitalweb.html >.56 Global Network Navigator, <URL: http://nearnet.gnn.com/gnn/wic/med.toc.html >.57 Emory University Health Sciences Center Library, <URL: http://www.cc.emory.edu/WHSCL/medweb.html#toc2 >.58 Yahoo! Corp., <URL: http://www.yahoo.com/Health/ >.

Appendix FBoxes,
Figures, andTables
Boxes
Chapter 11-1: Effects on the Health Care Workforce1-2: Managed Care1-3: Grassroots Computer Networking: Lessons Learned
Chapter 22-1: The Content of Patient Records2-2: Speech and Handwriting Recognition2-3: Automated Data Collection and the Medical Information Bus2-4: The HELP System2-5: Digital Image Compression2-6: Security Technologies2-7: A Voice and Data Communications Primer2-8: HL7 and ICD-9-CM
Chapter 33-1: EDI and Electronic Commerce3-2: What is a Value-Added Network?3-3: EDI Standards3-4: Card Technology and Health Records
Chapter 44-1: Health Plan Performance Measures Used in the Health Plan and Employer Data and Informa-
tion Set (HEDIS)4-2: Provider Performance Measures Used in the Indicator Measurement System (IMSystem)
| 213

214 | Bringing Health Care Online: The Role of Information Technologies
Chapter 55-1: National Consortium for Telemedicine Evaluation5-2: Clinical Telemedicine Cooperative Group Organized by the Telemedicine Research Center,
Oregon Health Sciences University5-3: American Telemedicine Association5-4: National Information Infrastructure Testbed5-5: Telemedicine Information Exchange
Figures
Chapter 11-1: Information Technology Applications Currently Being Adopted
Chapter 22-1: Health Information Pathways to Hospital Information Systems2-2: Health Information on the Internet2-3: Messaging Standards for Clinical Institutions
Chapter 33-1: Health Care Industry Trading Relationships3-2: Payment-Related Transactions3-3: High-Level Architecture of a Community Health Information Network3-4: Common User Interface3-5: Federated Database Approach for a Community Health Information Network
Chapter 44-1: Algorithm Depicting a Clinical Practice Guideline for Evaluation and Care of Patients with
Heart Failure
Chapter 55-1: A Telemedicine Health Care Network5-2: East Carolina University Telemedicine Network5-3: Rural Area Networks
Tables
Chapter 22-1: Key Information Technologies for Health Care2-2: Storage Requirements for Imaging Techniques
Chapter 33.1: Estimates of Cost Savings for Payers, Providers, and Employers Through the Use of Informa-
tion Technology
Chapter 55-1: Summary of Telemedicine Application Categories

Appendix GAbbreviations
andGlossary
ACTSAdvanced Communications and Technology Sat-ellite
Administrative dataData used in the administration of public pro-grams or agencies or private businesses. In health,examples of administrative data are hospital dis-charge abstracts and health insurance claims andenrollment records.
Administrative simplificationEfforts to reduce the cost and complexity of healthcare through increased standardization and au-tomation of health care providers’ and insurers’administrative activities.
Admission/discharge record (or dischargeabstract)A synopsis of a patient record containing basicidentifying and financial information about a pa-tient, along with clinical information, includingthe admitting and final diagnosis and a summaryof procedures performed.
AffordancesBehaviors and actions that are allowed or enabledby a specific technology.
AHCPRAgency for Health Care Policy and Research
AITNArizona-International Telemedicine Network
AMAAmerican Medical Association
AMIAcute myocardial infarction
ANSIAmerican National Standards Institute
Arden SyntaxA computer language for encoding and sharingmedical knowledge in discrete modules.
ARPAAdvanced Research Projects Agency, DOD
Artificial neural networkA linked network of simple software-based pro-cessors, analogous to a biological neural network,that can be trained as an ensemble to respond con-sistently to a set of numerical input stimuli.
| 215

216 | Bringing Health Care Online: The Role of Information Technologies
ASC (Accredited Standards Committee)A committee chartered by ANSI to work on stan-dards in a particular area of commerce. For exam-ple, ASC X12 is the committee working on stan-dards for the insurance industry, including health.
ASTMAmerican Society for Testing and Materials
Asymmetric encryptionAn encryption scheme in which information in-tended for an individual is encoded with his/herwell-known, public encryption key, but may onlybe decoded with his/her private key (generatedfrom a guarded password).
ATM (asynchronous transfer mode)A fast networking protocol based on small, uni-form packets. ATM communications are suitablefor continuous transfer of large amounts of data,including video streams.
ATP (Advanced Technology Program)A Commerce Department program that fundscooperative development and validation of enab-ling technologies, including computer and in-formation technologies.
AuthenticatorA device that provides an internally stored or cal-culated response to verify a user’s identity whenlogging onto a computer. Only authorized usersare likely to both know a unique piece of informa-tion (the password) and be in possession of aunique piece of equipment (the authenticator).
Automated data collectionDirect transfer of physiological data from moni-toring instruments to a bedside display system or acomputer-based patient record.
BackboneA high-capacity communications channel thatcarries data accumulated from smaller branches ofa computer or telecommunications network.
BandwidthThe amount of information an electronic connec-tion can carry per unit of time, usually expressedin bits per second.
Biometric identifierA retinal pattern, fingerprint, or other anatomicalfeature that can be used by a computer program(along with appropriate interface equipment) topositively identify a user.
C-sectionCaesarean section
CABGCoronary artery bypass graft
CapitationA method of paying for health care based on a setfee per member (of the health care plan) per unit oftime.
CAT scanComputerized axial tomography scan
CBA (cost-benefit analysis)A comparison of the net costs of an interventionwith the net savings.
CD-ROMCompact disk, read-only memory
CDSSClinical decision support system
CEA (cost-effectiveness analysis)A structured, comparative evaluation of two ormore health care interventions.
CHESS (Comprehensive Health EnhancementSupport System)An interactive computer system developed at theUniversity of Wisconsin that provides informa-tion, social support, and problem-solving tools forpeople living with AIDS and HIV infection.

Appendix G Abbreviations and Glossary | 217
CHFCongestive heart failure
CHI (consumer health informatics)The study, development, and implementation ofcomputer and telecommunications applicationsand interfaces designed to be used by health con-sumers.
CHIN (community health information network)Electronic systems that facilitate community-wide exchange of clinical and administrative in-formation among providers, payers, banks, phar-macies, public health agencies, employers, andother participants in the health care system.
CHMIS (community health managementinformation system)An electronic system similar to a CHIN that has anexplicit emphasis on building a data repository foruse in assessing the performance of health careproviders and insurance plans.
Clinical decision supportThe use of information to help a clinician diag-nose and/or treat a patient’s health problem, in-cluding information about the patient and in-formation about the kind of health problemafflicting the patient and alternative tests andtreatments for it.
Clinical information systemHospital-based information system designed tocollect and organize data related to the care givento a patient, rather than administrative data.
Clinical practice guidelineAn outline of broad parameters for the diagnosis,treatment, prevention, or rehabilitation of a partic-ular health problem.
Clinical protocolA rigorous, detailed model of the process of carefor a particular health problem.
CMEContinuing medical education
Cochrane CollaborationAn international network of researchers that dis-tributes results of systematic reviews of random-ized controlled trials—or the most reliable evi-dence form other sources—on selected healthproblems.
Codec1) In telemedicine, an abbreviation for coder/de-coder, an electronic device that converts an analogelectrical signal into a digital form for transmis-sion purposes and decodes it the receiving end. 2)In computer-based video technology, an abbrevi-ation for compressor/decompressor, the softwarethat reduces the size of digitized video frames.
Coding standardA system for assigning alphanumeric codes tospecific words, concepts, or actions for the pur-pose of standardizing messages between comput-ers or organizations.
COMPASSA local dial-up computer data network in Oregonthat provides a variety of information services.
Computer-based patient recordA compilation in digital form of all the clinicaland administrative information related to the careof a single individual.
Confounding variableA factor other than the health service in questionthat may influence the outcome of that service.
Consensus standardA non-proprietary technological standard devel-oped through an open, participative process underthe aegis of a standards development organization.
Coordination of benefitsThe determination of primary payer, that is, thepayer whose coverage is applied first. A second-ary payer reimburses, subject to the terms of itscontract, that portion of a claim unpaid by the pri-mary payer.
218 | Bringing Health Care Online: The Role of Information Technologies
CPRComputer-based patient record
CPT-4 (Current Procedural Terminology, FourthEdition)A classification and coding system for health ser-vices maintained by the AMA that is used in bill-ing by clinicians and other noninstitutional pro-viders.
CQI (Continuous Quality Improvement)A method of analyzing and improving processesfor manufacturing products or delivering servicesto meet customer needs and expectations.
CSN (Community Services Network)A project in Washington, DC, that uses commu-nication and computer technologies to supportand coordinate health and human services at thecommunity level.
Data distillationAn informal label for the process of derivingmeaning from raw data.
Data repositoryThe component of an information system that ac-cepts, files, and stores data from a variety ofsources.
DDEDirect data entry
Decision supportSee Clinical decision support.
Demand managementA method of controlling health care costs by con-trolling access to health care services.
DEMPAQ (Developing and Evaluating Methodsto Promote Ambulatory Care Quality)A set of performance indicators for ambulatorycare providers that is being developed by HCFAfor its Medicare program.
DHHSDepartment of Health and Human Services
DICOM (Digital Imaging and Communications inMedicine)A standard for communications among medicalimaging devices.
Discharge abstractSee Admission/discharge record.
Disease managementA method of managing the care of a specific healthproblem (usually a chronic and costly disease)that employs the principles of continuous qualityimprovement, including the use of clinical prac-tice guidelines, outcomes measurement, and feed-back to providers and insurance plans.
DODDepartment of Defense
DRG (Diagnosis Related Group)A class of health problems derived from sets ofdiagnosis and procedure codes and used by HCFAto determine reimbursement for treatments.
DS-0, DS-1, DS-3Digital telecommunications channels capable oftransmitting 64 kilobits, 1.544 megabits, and 45megabits per second, respectively. The higher ca-pacity connections are suitable for high-volumevoice, data, or compressed video traffic.
DSP (digital signal processor)A special-purpose computer processor custom-ized to make rapid calculations associated withaudio or video data streams.
ECUEast Carolina University
ED-NETA statewide network created by the State of Ore-gon in 1989 that offers a full range of services forthose who have a need to communicate.
EDI (electronic data interchange)The application-to-application interchange ofbusiness data between organizations using a stan-dard data format.

Appendix G Abbreviations and Glossary | 219
Electronic mailing listsFree, subscription-based, electronic mail commu-nications on the Internet or commercial online ser-vices focused on defined topics.
EncoderDecision support systems used to facilitate accu-rate assignment of codes for clinical procedures.
Fault-tolerant computer systemsReliable computer systems incorporating redun-dant processors, disk drives, and power suppliesto ensure almost full-time operation of a criticalinformation network.
FDAFood and Drug Administration
FirewallComputer hardware and software that block unau-thorized communications between an institution’scomputer network and external networks.
Firms trialA form of randomized controlled trial in which pa-tients are randomly assigned to similar (“paral-lel”) providers who use different health services,rather than to different groups that receive differ-ent services from the same provider.
Frame relayA fast networking protocol in which data are pack-aged in variable-length frames for shuttling be-tween computer networks.
Functional imagingMedical imaging modalities that portray the func-tion (such as oxygen uptake) as well as themorphology of anatomical features.
GrouperSoftware used to deduce DRGs from sets of diag-nosis and procedure codes, or to analyze thegrouping decisions of medical coders for consis-tency and thoroughness.
Handwriting recognitionConversion of script or block lettering to comput-er-based text.
HCFAHealth Care Financing Administration
HEDIS (Health Plan and Employer Data Set)A set of performance indicators for managed careplans, developed by NCQA.
HELP (Health Evaluation through LogicalProcessing)A clinical information system at LDS Hospital inSalt Lake City, Utah.
HISPP (Healthcare Informatics StandardsPlanning Panel)A body created by ANSI to coordinate standardsdevelopment efforts among the various standardsbodies in health care.
HL7 (Health Level 7)An application-level interface specification fortransmitting health-related data transactions, gen-erally used within a single institution.
HMOHealth maintenance organization
HOSTHealthcare Open Systems and Trials consortium
HPCC (High Performance Computing andCommunications)An advanced technology program involving sev-eral agencies of the federal government, includingNLM and NIST.
Human capital approachA valuation technique used in cost-benefit analy-sis that assigns a monetary value to a human lifebased on an estimate of the individual’s projectedfuture earnings.
ICD-9-CM (International Classification ofDiseases, Ninth Revision, Clinical Modification)A classification and coding system for healthproblems and services, maintained by NCHS andHCFA, and used for billing by inpatient hospitalsand other institutional providers.

220 | Bringing Health Care Online: The Role of Information Technologies
IDS (integrated delivery system)An organized system of health care providersspanning a range of health care services.
IEEEInstitute of Electrical and Electronics Engineers
IHC (Intermountain Health Care)A provider organization based in Utah.
IITFInformation Infrastructure Task Force
IMSystem (Indicator Measurement System)A set of performance indicators for inpatient hos-pitals and other institutional providers maintainedby JCAHO.
Inference engineA computer routine that coordinates the activitiesof a knowledge- or rule-based decision supportsystem.
IPA (independent practice association)An organization that contracts with a managedcare plan to deliver health services at a single ca-pitation rate.
ISDN (integrated services digital network)A digital telephony protocol.
JCAHOJoint Commission on Accreditation of HealthcareOrganizations
JPEG (Joint Photographic Experts Group)A standard for compression of static images.
Knowledge-based systemA decision support system based on automated,systematized application of sets of rules or heuris-tics for analysis of raw data.
KUMCKansas University Medical Center
LAN (local area network)Communications lines linking a localized groupof computers, printers, and servers.
Laser optical cardA plastic device the size of a credit card that canhold large amounts of digital data. Typically, thedata cannot be altered once they are written to thecard.
LATA (Local Access Transport Area)A geographic region used to define telephoneareas.
LOINC (Laboratory Observation IdentifierNames and Codes)A set of universal names and codes for identifyinglaboratory test results in order to facilitate the ex-change and pooling of clinical laboratory results.
Magnetic stripe cardA plastic card with a magnetic strip on the backthat can store about 250 characters, mainly foridentification and verification of eligibility for in-surance benefits.
Managed care (or managed health care)A vaguely defined term referring to various sys-tems of health care delivery that attempt to man-age the cost, quality, and accessibility of healthcare.
Managed care organizationAn organization, such as an HMO or PPO, thatuses one or more techniques of managed care.
MCGMedical College of Georgia
Messaging standardA standard governing the structure of electronicmessages between computers.
Meta-analysisQuantitative synthesis of the statistical results ofnumerous studies on a given topic.
MIB (Medical Information Bus)A hardware and software standard (IEEE P1073)that enables standardized connections betweenmedical monitoring devices and clinical informa-tion systems.

Appendix G Abbreviations and Glossary | 221
MLM (Medical Logic Module)A component of the Arden Syntax.
MPEG (Motion Picture Experts Group)A video compression standard.
MRIMagnetic resonance imaging
MultiplexingCombination of many low-capacity communica-tions channels into one high-capacity commu-nications channel by interleaving the variouschannels in discrete time or frequency slices.
NASANational Aeronautics and Space Administration
NCHSNational Center for Health Statistics
NCHSRNational Center for Health Services Research
NCINational Cancer Institute
NCQANational Committee for Quality Assurance
NCVHSNational Committee on Vital and Health Statistics
NIINational Information Infrastructure
NISTNational Institute for Standards and Technology
NLMNational Library of Medicine
NTIANational Telecommunications and InformationAdministration
NUBCNational Uniform Billing Committee
OCR (optical character recognition)Automated scanning and conversion of printedcharacters to computer-based text.
OLAP (on-line analytical processing)A database architecture that supports querying ofcomplex, multidimensional databases.
ORHPOffice of Rural Health Policy
PACS (Picture Archiving and CommunicationsSystem)A computer-based system of storing and retriev-ing radiographic and other images in digital form.
Patient recordThe repository of information about an individualpatient, usually stored on paper, but more recentlyin electronic form in a computer system.
PayerInsurance company, self-insured employer, ad-ministrator, or other entity responsible for payingfor an individual’s health care.
PBM (pharmacy benefit management)A method of managing pharmaceutical benefitsfor insurers and employers that uses disease man-agement, pharmacy networks, negotiated dis-counts and rebates, lists of preferred drugs, andonline utilization review. Also, an organization(pharmacy benefit manager) that performs PBMservices.
PBX (private branch exchange)A institution’s internal phone system, which mayinclude voice messaging capabilities.
PCPersonal computer
PC card or PCMCIA cardA credit card-sized computer peripheral or periph-eral interface used with portable and desktop com-puters.
PDA (personal digital assistant)A handheld computer, usually with no keyboard,that is used for communications or data collectionand analysis.

222 | Bringing Health Care Online: The Role of Information Technologies
PDQ (Physician Data Query)A system of online (Internet) information regard-ing various cancers, ongoing clinical trials, and in-dividuals and organizations involved in cancercare, maintained by NCI.
PixelThe smallest displayable area on a computerscreen.
PPOPreferred provider organization
Primary dataData collected directly from individuals (e.g., sur-vey, observation) or documents (e.g., medical re-cord review).
Privacy ActThe Federal Privacy Act of 1974 (5 U.S.C. Sec-tion 552a, 1988), which protects individuals fromnonconsensual disclosure of confidential in-formation by government agencies.
Proprietary standardA technological standard developed by a singlevendor or vendor group. The standard’s specifica-tions may be publicized or held confidential.
Prospective researchResearch in which patients are observed as theyreceive health services.
Provider (or health care provider)Any person (physician, nurse, etc.) or institution(hospital, nursing home, etc.) that provides healthservices to patients.
PTCAPercutaneous transluminal coronary angioplasty
PurchaserAn organization (usually a large employer) thatpurchases health insurance (usually for its ownemployees).
Quality assessmentMeasurement and evaluation of the quality ofhealth services delivered to patients, usually fo-
cusing on the processes and outcomes of those ser-vices.
RAID (redundant array of independent disks)Multiple computer disks configured as a singledisk to provide either data redundancy or en-hanced access speed.
Randomized controlled trialA form of prospective research in which patientsare randomly assigned to groups that receive dif-ferent health services and are then observed fordifferences in outcome.
RBOC (Regional Bell Operating Company)A regional telephone company resulting from thedivestiture of the Bell System in the 1980s.
Relational databaseA collection of computer-based information thatis organized or accessed according to relation-ships between data items.
ReliabilityThe reproducibility of a measure, or the extent towhich the measure yields similar results each timeit is used on similar samples, or the extent to whichits components yield similar results for the sameor similar samples.
Report cardA summary set of indicators of the performance ofhealth care providers or insurance plans in deliver-ing health services to patients.
Retrospective researchResearch in which patients are observed after theyhave received health services
Risk adjustmentStatistical control of patient risk factors in theanalysis of the utilization and outcomes of healthservices; also, control of financial risk factorsfaced by insurance companies.
Risk factorsKey health problems and background characteris-tics that can affect the patient’s outcome, indepen-dent of the specific kinds of services received.

Appendix G Abbreviations and Glossary | 223
RMRS (Regenstrief Medical Record System)A clinical information system at the RegenstriefInstitute, Indiana University, Indianapolis, Indi-ana.
RODEO NETRural Options for Development and EducationalOpportunities Network
Rule-based expert systemA decision support system based on large num-bers of heuristics, or rules of thumb, derived fromanalysis of action patterns of experts or from pub-lished literature.
Run-length encodingA data compression scheme in which extended se-ries of repetitive data are replaced by the first itemin the series and a token indicating the length ofthe data run.
RUSRural Utilities Service (formerly the Rural Elec-trification Administration)
Secondary dataData originally collected for one purpose (e.g.,program administration) and then analyzed for adifferent purpose (usually research or evaluation).
Shared decision support systemsDesigned to inform patient/provider decisions re-garding prevention, diagnosis, management, andtreatment.
Smart cardA plastic device the size of a credit card with anembedded computer processor and memory.
SMS (Shared Medical Systems)A vendor of hospital information services andproducts.
SNOMED (Systematized Nomenclature ofMedicine)A system for classifying and coding health prob-lems, symptoms, and services.
Social interfaceA human-computer interface design approach inwhich users interact with representations of physi-cal objects or, in some cases, anthropomorphicagents displayed by their computer.
Speech recognitionAutomated conversion of spoken words into com-puter-based text. Some speech recognition sys-tems recognize only one person’s voice; others arespeaker-independent but recognize a more limitedvocabulary. They may recognize continuousspeech or, more commonly, require that slightpauses be inserted between words.
SSNSocial Security number
STARPAHCSpace Technology Applied to Rural Papago Ad-vanced Health Care, a 1970s cooperative teleme-dicine project supported by NASA, the IndianHealth Service, and the Papago people.
Statistical controlControl of confounding variables in retrospectiveresearch, either by classifying patients into groupsthat are homogeneous with respect to those vari-ables, or by adjusting for the variation in the out-come variable that is accounted for by those con-founding variables.
Structured data entryA data collection technique that constrains thelanguage and format of clinical descriptions forthe purpose of ensuring uniform, unambiguous,interchangeable messages.
Symmetric encryptionEncryption of a message with a key derived from apassword that must be known by both the sendingand receiving parties.
Systematic reviewExtraction of specific items of information fromnumerous research works on a given topic andcomparison of those items across those works us-ing structured methods.

224 I Bringing Health Care Online: The Role of Information Technologies
Tl, T3See DS-1, DS-3.
Tablet computerA computer with an integrated display and digitiz-er, rather than a keyboard. Also known as a clip-board or pentop computer.
TCP/lP (Transmission Control Protocol/InternetProtocol)A communications protocol governing data ex-changed on the Internet.
TelemedicineThe use of information technology to deliver med-ical services and information from one location toanother.
UMLS (Unified Medical Language System)A computer-based system for translating amongdisparate clinical nomenclatures, maintained bythe National Library of Medicine (NLM).
UNLS (Unified Nursing Language System)A system similar to the Unified Medical Lan-guage System (UMLS) that focuses on nursingservices.
ValidityThe extent to which an observed situation reflectsthe true situation. Internal validity is the extent to
which the results of a study reflect the true rela-tionship between an intervention and an outcome.External validity is the extent to which the resultsof a study may be generalized to other settings,etc.
VAN (value added network)A data communication network that provides ser-vices beyond normal transmission, such as errorcorrection or message storage and forwarding.
WEDIWorkgroup for Electronic Data Interchange
WHINWisconsin Health Information Network
WHOWorld Health Organization
WIC (Women, Infants and Children)A special supplemental food program adminis-tered by the U.S. Department of Agriculture.
Willingness-to-pay approachA valuation approach used in cost-benefit anal-
ysis that assigns monetary value to human life byconsidering how much individuals are willing topay for a reduction in the risk of death or illness.
SOURCES Some definitions adapted from P.R. Kongstvedt, Essentials of Managed Care (Gaithersburg, MD Aspen Publishers, 1995) Health Careand the Electron/c Superhighway A Provider Perspective on Electronic Data Interchange and Automated Medical Payment, Research Report No.
92-3 (Faulkner and Gray Washington, DC, 1992)
| 225
ndex
AAccess to care, 76, 163-164Access to information, 125-127, 130-132, 207-211Access to records, 115Administrative activities, 83
providers, 83-84providers and payers, 84-87
Administrative simplification, 31-32, 80-83Advanced Research Projects Agency, 170Agency for Health Care Policy and Research, 72,
73, 127, 129, 131, 154, 157, 188, 203AHCPR. See Agency for Health Care Policy and
ResearchAHSC. See American Hospital Supply Corp.AITN. See Arizona-International Telemedicine
NetworkAMA. See American Medical AssociationAmerican Hospital Supply Corp., 93American Medical Association, 155, 156, 157American Self-Help Clearinghouse, 25American Society for Testing and Materials, 68, 138American Telemedicine Association, 179, 187Analytic Systems Automated Purchasing, 93ANSI, 68ANSI X12, 69Arizona-International Telemedicine Network, 173ARPA. See Advanced Research Projects AgencyArtificial neural networks, 51-52ASAP. See Analytic Systems Automated PurchasingASTM. See American Society for Testing and
MaterialsAustralia, telemedicine, 176-177Authentication, 116Automated data collection, 46, 50-51
BBrigham and Women’s Hospital, 46
CCanada, telemedicine, 176CancerNet, 131Cards, 55, 99-100CBA. See cost-benefit analysisCDC. See Centers for Disease Control and
PreventionCD-ROMs, 131CEA. See cost-effectiveness analysisCenters for Disease Control and Prevention, 73, 103CHESS. See Comprehensive Health Enhancement
Support SystemCHI. See Consumer health informaticsCHIN. See Community Health Information NetworkCHMIS. See Community Health Management
Information SystemClaims inquiry, 87Claims services, 91Claims submission, 86Client-server architecture, 66-67Clinical decision support, 52-54, 124-142, 197-200
applications of, 197-200effectiveness and safety, 138-140, 153-155evaluation, 140-142information content, 136-138standards, 136-138, 155-158technology development, 135-136
Clinical information systems, 35-38Clinical literature, 126Clinical practice guidelines, 127-129Clinical practice improvement, 134Clinical protocols, 127-129, 133-134Clinical research, 126Clinical Telemedicine Cooperative Group, 179, 181,
203Cochrane Collaboration, 131Communications primer, 63-65Community Health Information Network, 16, 63,
95-96, 108-109

226 | Bringing Health Care Online: The Role of Information Technologies
Community Health Management InformationSystem, 16, 95-96
Community networking, 26, 95-103Community Services Network, 26COMPASS, 172Comprehensive Health Enhancement Support
System, 25, 174ComputerLink, 25Computer software, 67-68Confidentiality, 114-118, 183Congressional interest, 9Connect System, 25, 175Consumer health informatics, 24-26Consumer information sources, 208Continuous quality improvement, 134, 144Coordination, 78Cost containment, 11-13Cost-benefit analysis, 12-13Cost-effectiveness analysis, 12-13Cost management, 5-6Cost reduction, 16, 75CPT-4, 155, 156, 157CQI. See Continuous quality improvement
DDatabases, 42Data distillation, 49-54Data security, 115-118, 183Data sets, maximum, 120Decision support system. See Clinical decision
supportDemand management system, 24, 65DEMPAQ. See Developing and Evaluating Methods
to Promote Ambulatory Care QualityDepartment of Commerce, 203-204Department of Defense, 188, 189, 204Department of Health and Human Services, 9, 121,
159, 183, 202-203Department of Veterans Affairs, 179, 188, 190, 205Developing and Evaluating Methods to Promote
Ambulatory Care Quality, 145, 154DHHS. See Department of Health and Human
ServicesDICOM, 58Direct data entry, 87Dxplain, 139
EEast Carolina University School of Medicine,
170-171, 174EDI. See Electronic data interchangeEDI standards. See StandardsEFT. See Electronic funds transferElectronic commerce, 79, 82
Electronic data interchange, 81-83, 87-95, 103-122cost savings, 104-109system costs, 103
Electronic funds transfer, 92Electronic health information sources, 207-211Electronic house call, 168, 173-175Electronic order entry, 93Electronic publishing, 132Electronic signatures, 114Eligibility, 87Encounter reports, 87Encryption, 116Enrollment, 87Enterprise information systems, 35Enterprise networks, 102-103EOE. See electronic order entryEvidence-based medicine, 131Expert systems, 52-54, 132-133
FFDA. See Food and Drug AdministrationFee-for-service plan, 81, 143Financial institutions, 92-93Food and Drug Administration, 67-68, 76, 141, 154Forms, standardized, 93
GGeneral Accounting Office (GAO), 108Grassroots computer networking, 26-27
HHandwriting recognition, 46-47Harvard Community Health Plan, 174HCFA. See Health Care Financing AdministrationHealth care expenditures, 5-6Health Care Financing Administration, 13, 17, 19,
36, 87, 90, 104, 110, 112, 119, 121, 145, 154,155, 157, 171, 177, 178, 188, 191, 202-203
Health care reform, 6Healthcare Open Systems and Trials consortium, 72Health Evaluation through Logical Processing
System, 52-54, 133, 137Health Informatics Standards Planning Panel, 72Health information, life cycle, 34-42Health information, regulatory environment for,
112-115, 121Health information sources, electronic, 207-211Health maintenance organization, 8, 81Health Plan Employer Data and Information Set,
145-147, 154HEDIS. See Health Plan Employer Data and
Information SetHELP system. See Health Evaluation through
Logical Processing system

Index | 227
High-Performance Computing and CommunicationsProgram, 73, 179, 203
HISPP. See Health Informatics Standards PlanningPanel
HL7 standard, 70, 84HMO. See Health Maintenance OrganizationHospital information systems, 37HOST. See Healthcare Open Systems and Trials
consortiumHPCC. See High-Performance Computing and
Communications Program
IICD-9-CM standard, 70, 107, 156, 157Identifiers, 111-112, 120-121IITF. See Information Infrastructure Task ForceIliad, 139Imaging systems, 41
compression, 56-58techniques, 55
IMSystem, 146-149Indian Health Service, 159Industry fragmentation, 109-110Information Infrastructure Task Force, 8, 25, 62,
160, 181, 188, 189, 201Information needs, complexity of, 110Information Network for Public Health Officials,
103Information sources, electronic, 207-211Information technologies, 29-78
adoption levels, 2, 3challenges and opportunities, 2compression, 54-58data distillation, 49-54data security, 60-62display and retrieval, 58-60distributed computing, 66-68high-bandwidth communications, 62-66object-oriented software, 67-68storage, 54-58
INPHO. See Information Network for Public HealthOfficials
Integrated delivery system, 84Integration of health services, 6, 8Internet, 63, 207-211Islands of automation, 1, 30-34
JJob roles. See Workforce effectsJoint Commission on Accreditation of Healthcare
Organizations (JCAHO), 38, 146, 184
KKansas University Medical Center, 168-170Knowledge-based systems, 52-54, 132-133
LLDS Hospital, 129, 133Legacy systems, 35Legislative activities, 9-10, 122, 160, 187, 188Lewin-VHI, 104Liability, physician, 184Licensing, physician, 183-184Little, Arthur D., Inc., 104
MManaged care, 6, 7, 81, 143Mayo Clinic, 170MDIS. See Medical Diagnostic Imaging SupportMedicaid, 8, 87, 154, 155, 177Medical College of Georgia, 166-168Medical Diagnostic Imaging Support, 204Medical informatics, 30Medical Information Bus, 50-51Medical logic modules, 137Medicare, 8, 87, 112, 114, 121, 154, 155, 177Medicare Transaction System, 110, 112Meditel, 139MEDLINE, 130MIB. See Medical Information BusMTS. See Medicare Transaction System
NNACHA. See National Automated Clearing House
AssociationNASA. See National Aeronautics and Space
AdministrationNational Aeronautics and Space Administration, 73,
159, 170, 189, 204-205National Automated Clearing House Association, 92National Center for Health Services Research, 153,
154National Committee for Quality Assurance, 145National Committee on Vital and Health Statistics,
156, 157, 158National Consortium for Telemedicine Evaluation,
179-180National Council for Prescription Drug Programs,
69, 76, 95National Information Infrastructure, 8, 103, 160,
181, 188, 201National Information Infrastructure Testbed, 188,
189National Institutes of Health, 73
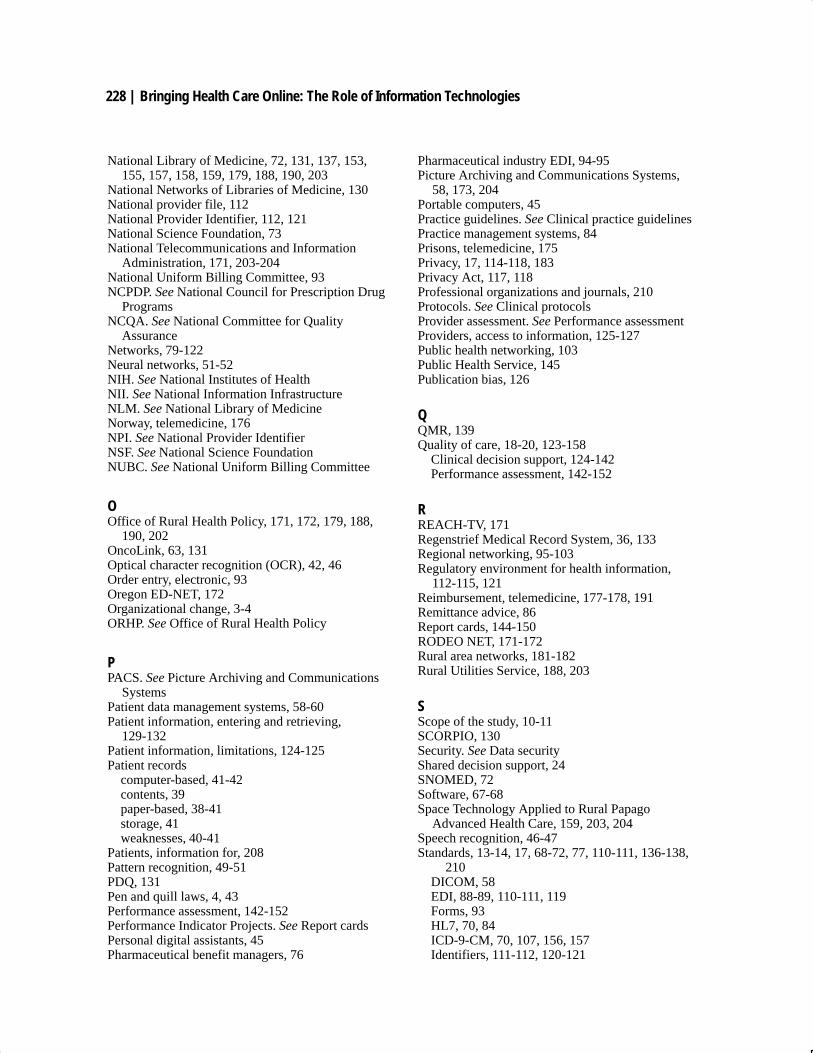
228 | Bringing Health Care Online: The Role of Information Technologies
National Library of Medicine, 72, 131, 137, 153,155, 157, 158, 159, 179, 188, 190, 203
National Networks of Libraries of Medicine, 130National provider file, 112National Provider Identifier, 112, 121National Science Foundation, 73National Telecommunications and Information
Administration, 171, 203-204National Uniform Billing Committee, 93NCPDP. See National Council for Prescription Drug
ProgramsNCQA. See National Committee for Quality
AssuranceNetworks, 79-122Neural networks, 51-52NIH. See National Institutes of HealthNII. See National Information InfrastructureNLM. See National Library of MedicineNorway, telemedicine, 176NPI. See National Provider IdentifierNSF. See National Science FoundationNUBC. See National Uniform Billing Committee
OOffice of Rural Health Policy, 171, 172, 179, 188,
190, 202OncoLink, 63, 131Optical character recognition (OCR), 42, 46Order entry, electronic, 93Oregon ED-NET, 172Organizational change, 3-4ORHP. See Office of Rural Health Policy
PPACS. See Picture Archiving and Communications
SystemsPatient data management systems, 58-60Patient information, entering and retrieving,
129-132Patient information, limitations, 124-125Patient records
computer-based, 41-42contents, 39paper-based, 38-41storage, 41weaknesses, 40-41
Patients, information for, 208Pattern recognition, 49-51PDQ, 131Pen and quill laws, 4, 43Performance assessment, 142-152Performance Indicator Projects. See Report cardsPersonal digital assistants, 45Pharmaceutical benefit managers, 76
Pharmaceutical industry EDI, 94-95Picture Archiving and Communications Systems,
58, 173, 204Portable computers, 45Practice guidelines. See Clinical practice guidelinesPractice management systems, 84Prisons, telemedicine, 175Privacy, 17, 114-118, 183Privacy Act, 117, 118Professional organizations and journals, 210Protocols. See Clinical protocolsProvider assessment. See Performance assessmentProviders, access to information, 125-127Public health networking, 103Public Health Service, 145Publication bias, 126
QQMR, 139Quality of care, 18-20, 123-158
Clinical decision support, 124-142Performance assessment, 142-152
RREACH-TV, 171Regenstrief Medical Record System, 36, 133Regional networking, 95-103Regulatory environment for health information,
112-115, 121Reimbursement, telemedicine, 177-178, 191Remittance advice, 86Report cards, 144-150RODEO NET, 171-172Rural area networks, 181-182Rural Utilities Service, 188, 203
SScope of the study, 10-11SCORPIO, 130Security. See Data securityShared decision support, 24SNOMED, 72Software, 67-68Space Technology Applied to Rural Papago
Advanced Health Care, 159, 203, 204Speech recognition, 46-47Standards, 13-14, 17, 68-72, 77, 110-111, 136-138,
210DICOM, 58EDI, 88-89, 110-111, 119Forms, 93HL7, 70, 84ICD-9-CM, 70, 107, 156, 157Identifiers, 111-112, 120-121

Index | 229
Messaging, 42, 68-69, 70, 72, 136of care, 126
STARPAHC. See Space Technology Applied toRural Papago Advanced Health Care
Structured data entry, 42SUPPORT model, 139
TTablet computers, 45Telecommunications and Information Infrastructure
Assistance Program, 203-204Telemedicine, 20-23, 159-191, 209
Access, 163-164Applications, 165-177Costs, 161-163, 180Development costs/financing, 185Evaluation, 178, 179Executive branch activities, 201-207Government role, 188-191Home-based, 173-175Human infrastructure, 186IITF subgroup on, 160, 189, 190-191, 201Legal/regulatory, 181, 183-184Other countries, 176-177Other sites, 175-176Potential effects, 160-165Quality of care, 164-165Research, 178-179, 190Technology and implementation, 185-186
Telecommunications infrastructure, 179-180Teleconsultations, 166-172Teleradiology and telepathology, 172-173
Telemedicine Information Exchange, 190, 203Texas Telemedicine Project, 168Tiber Group, 104TIE. See Telemedicine Information ExchangeTIIAP. See Telecommunications and Information
Infrastructure Assistance ProgramTri-Service Telemedicine Testbed Project, 204
UUnified Medical Language System (UMLS), 72,
137, 155, 157Urban telemedicine, 176User interfaces, 99, 101
VValue-added network (VAN), 83, 92
WWisconsin Health Information Network (WHIN), 63Workforce effects, 4, 5Workgroup for Electronic Data Interchange
(WEDI), 93, 104, 116, 117World Health Organization (WHO), 157World Wide Web (WWW), 63, 207