briefings on hospital safety - · infectious substances or diagnos-tic specimens by air? if so, do...
TRANSCRIPT

Here’s a pair of questions to throwout at your next safety-committeemeeting: Does your hospital shipinfectious substances or diagnos-tic specimens by air? If so, do theappropriate workers receive therequired training?
Those important questions drivethe Federal Aviation Administra-tion (FAA) when it visits hospitals.
What’s that, you ask—the FAA?Although this regulator probablyisn’t the first one you’d curse tothe sky about, medical sites some-times receive visits from its investi-gators. “Basically, the FAA enforcesregulations when it comes to thetransportation of hazardous
materials by air,” says RebeccaTrexler, an FAA spokesperson.
Training left wantingA big problem inspectors focus onstems from hospital workers notlearning how to properly ship air-bound packages that qualify ashazardous materials, says MarkCaputo. Caputo is the Northeast’sdistrict manager for Saf-T-Pak, acompany based in Edmonton, AB,Canada, that offers training onshipping infectious substances.
“It’s a lack of training due to igno-rance,” he says. “They simply don’tknow they’re supposed to be train-ed.” It is not unheard of for theFAA to conduct what it
—INSIDE—
Vol. 12 No. 6June 2004
Any employee could end up inthe crosshairs of the Joint Com-mission on Accreditation of Health-care Organizations (JCAHO) whenit comes to safety concerns dur-ing a survey.
“All of the [staff members] on theunits are walking targets for ques-tions about the hazards” in thoseareas, says Gary Tipton, safetyofficer at Redlands (CA) Commu-nity Hospital, which underwent aJCAHO visit in March.
Turn it on
Good lighting goes beyondjust seeing well—it canimprove worker performanceand rein in maintenanceactivities. See p. 4.
Hand-hygiene debate
A new amendment to the LifeSafety Code® allows hand-geldispensers in exit corridors,but regulators have yet to formally weigh in. See p. 6.
Survey monitor
Surveyors repeatedly pushedfor information about how ahospital identified its risksand what responses it took.See p. 8.
Tip of the month
Don’t forget simple steps tocombat tuberculosis, such as insisting that suspectedpatients wear surgical masksoutside isolation rooms. Seep. 12.
Enclosed
Find out the latest environmentof care trends during JointCommission surveys in yourfree special report.
> p. 2
Flying right, part 1
Learn when the FAA takes notice ofmedical centers shipping specimens
BRIEFINGS on HOSPITAL SAFETYBRIEFINGS on HOSPITAL SAFETYThe Newsletter for Hospital Safety Committees
How to teach workers about safetybefore the JCAHO comes a knockin’
But in Redlands’ case, employeeswelcomed such inquiries. “Staffwere lining up for questions be-cause they knew [the answers],”Tipton says.
Planning aheadThe roots of this enthusiasm goback to December 2002, whenTipton focused on increasingemployee safety education. Hecreated risk tables with variouspotential hazards, which he anddepartment directors scored
FOR PERMISSION TO REPRODUCE
PART OR ALL OF THIS NEWSLETTER FOR
EXTERNAL DISTRIBUTION OR USE IN
EDUCATIONAL PACKETS, PLEASE CONTACT
THE COPYRIGHT CLEARANCE CENTER
AT WWW.COPYRIGHT.COM OR
978/750-8400. > p. 7
Visit us online atwww.hcpro.com/safety.

calls “haz-strikes” on hospitals, Trexler says. If in-vestigators arrive, expect them to check on trainingrecords and how well you package air specimens(see the related story below for details about training).
Shipping samples by air is common at many medicalcenters, particularly large ones and teaching hospi-tals, Caputo says. For example, you might fly speci-mens to a reference laboratory for testing, or sendthem to a pharmaceutical company if your hospitalconducts clinical trials.
Shippers (i.e., the appropriate hospital workers)
FAA
Page 2 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
need to both classify items they offer for transportand package and label them properly. These itemsfall into two broad hazardous-materials categories:
1. Infectious substances—also known in FAAlingo as Division 6.2 materials—are packages thatcontain, or that you suspect contain, a pathogenthat causes disease in people or animals.
Hospitals must categorize infectious substancesunder one of four risk groups, with Risk Group 1presenting the lowest threat of disease and RiskGroup 4 offering the highest. For help with riskgroups, jot down this Web address from the
< p. 1
If you ship by air, here’s how to train for it
Under the Code of Federal Regulations, Title 49,section 172.704 lists the training requirementsthat hospitals must meet if they have employeeswho ship hazardous materials, including infec-tious substances and diagnostic specimens byair. The employer—in this case, the hospital—must provide each employee who ships haz-ardous materials with the following training:
✓ General awareness and familiarization trainingused to educate workers about the require-ments of the law and help them recognizehazardous materials on the job
✓ Job-specific training as it relates to work tasksand associated hazards
✓ Safety training, including emergency-responseinformation, how employees can protect them-selves from exposure to hazardous materials,and ways to avoid accidents
✓ Security training that highlights risks associatedwith hazardous-materials shipments and meth-ods that enhance this security
✓ Your site may also need to conduct in-depthsecurity training if it meets several high-riskcriteria, including shipping substances on afederal hit list of agents and toxins (go towww.cdc.gov/od/sap/ for the complete list)
Hospitals should conduct training within 90days for new employees who ship hazardousmaterials or for a current worker who changesjob functions, and also once every three yearsas part of ongoing education. You can use train-ing from a prior employer to satisfy these re-quirements, provided that you obtain a recordof this training.
Also, hospitals must maintain all records of cur-rent training for as long as each worker handleshazardous materials duty plus 90 days after thoseduties end. The records must include employeenames, most recent training dates, a descriptionor copy of the training materials, the name andaddress of the person who provided the train-ing, and certifications that the workers receivedtraining and related testing. Hospitals shouldsign off on these certifications.
Finally, any training that hospitals conduct tomeet the hazard-communications program ofthe Occupational Safety and Health Administra-tion or the Environmental Protection Agencymay replace the training specified earlier in thisarticle. The substitute training must parallel thecomponents noted above.

Page 3Briefings on Hospital Safety—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
National Institutes of Health: www4.od.nih.gov/oba/rac/guidelines_02/appendix_b.htm.
Determine the risk group using a variety of factors,including the medical history of the patient, symp-toms, and professional judgment. Substances thatfall under Risk Group 1 are exempt from FAA haz-ardous-materials regulations.
Ship infectious substances in triple packaging as fol-lows: a leak-proof primary container or envelope,leak-proof secondary packaging, an absorbent mate-rial between the primary and secondary layers, andan outer packaging. The packages are subject to a30-ft drop test and a puncture test, although mostsuppliers of these items have such certificationsavailable, Caputo says.
The primary or secondary packaging must also beable to withstand, without leaks, an internal pres-sure producing a pressure differential of at least 95kilopascals. A kilopascal is a unit of pressure—forcomparison, 10 kilopascals is the pressure you’d feelat a depth of about 3 ft underwater.
2. Diagnostic specimens come from humans andanimals and include substances such as blood andtissue. You transport them for diagnostic or investi-gational purposes. About 95% of samples shippedby air are diagnostic, which prompted a tighteningof the rules governing their transportation in 2003,Caputo says.
You need to pack diagnostic specimens in triplepackaging similar to that of infectious materials.However, the drop test for diagnostic specimens is3.9 ft. Note that if the diagnostic specimen possiblycontains a serious human disease from a Risk Group4 pathogen, you must classify and package it as aninfectious substance. Further, a diagnostic specimenis exempt from packaging rules if it
• contains a microorganism in Risk Group 1
• doesn’t contain a pathogen
• contains a pathogen that has been neutralized ordeactivated
These rules apply to hospitals and affected employ-ees if they will independently ship infectious sub-stances and diagnostic specimens by air. However, ifyou use an outside service to pick up your pack-ages, and that service then delivers those items toan airplane, the outside firm must comply with FAArules, not the hospital, Caputo says.
The roots of regulationThe FAA references laws from the U.S. Departmentof Transportation as published in the Code of Feder-al Regulations (CFR). CFR 49 is the place to look forvarious laws affecting air-bound specimens (see theresource box above for more help).
Under 49 CFR 171.11, you must ship hazardous mate-rials under the guidelines of the International CivilAviation Organization, which is a United Nations tech-nical agency. The International Air TransportationAssociation, a trade group, also has industry standardson shipping infectious materials.
For more information . . .Here are some resources to help you wadethrough the regulations for shipping infectioussubstances and diagnostic specimens:
• Code of Federal Regulations, Title 49—Thisvoluminous set of federal laws governs haz-ardous-materials transport. Go to www.gpoaccess.gov/ecfr/ and choose “Title 49” fromthe dropdown menu, and then click the linkfor “100–185.”
• Saf-T-Pak—This infectious-substances pack-aging company has a lot of useful informationon its Web site, particularly in the frequently-asked-questions section. Go to www.saftpak.com.
• Office of Hazardous Materials Safety—Thisfederal arm of the Department of Transporta-tion has various online resources about ship-ping specimens. Go to hazmat.dot.gov (notethat there is no “www” in the address). Youcan also call 800/467-4922 to learn more or to ask questions about hazardous-materials shipping.
Page 4 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
At its best, lighting in hospitals can help healthcareworkers perform their jobs better.
But safety officers and facility directors shouldn’ttake their building’s lights for granted, says HelenDiemer, vice president of The Lighting Practice,Inc., a design firm in Philadelphia. Lighting shapesthe environment of care and, thus, people’s per-ceptions of their surroundings, Diemer says.
The following four items discuss how light canimprove worker comfort and your building’simage:
Light as a guardianLighting is important in many different ways
beyond letting people see better. Good lighting inhospitals provides a sense of stability—a feelingthat the medical center has been in the communityfor a while and offers good care—while also offer-ing a warm welcome for anyone who enters it,Diemer says.
How do you accomplish that? To start, “there shouldn’tbe a lot of dark, murky shadows,” Diemer says.“People in hospitals tend to feel trapped and isolat-ed. We know proper design can help with this”problem, including the use of natural and electriclight.
For example, lighting the edges of a room makespeople feel more secure, and soft lighting makesfolks feel more comfortable, says Diemer.
There is no need to wash a room in light, either;most people don’t enjoy that experience. “Lightingisn’t peanut butter,” she says. “It does not have tobe spread evenly. It should be used in the placeswhere it’s needed.”
Strive for varying levels of light, which will drawpeople to a particular area.
A clear viewGlare can literally create big headaches for
nurses, physicians, and other clinicians. These em-ployees constantly read computer monitors, equip-ment screens, medication bottles, and patient charts,and glare can impair their ability to do so.
One way to reduce glare is to install low-watt bulbsand to balance brightness using natural daylight. Lightthat’s reflected off a fixture offers another good solu-tion to glare, as does using matte finishes for wallsand furniture. Matte finishes refer to those free ofshine or highlights.
Poor lighting can also affect a worker’s circadianrhythms—the body’s internal “clock” that regulatesdaily waking and sleeping cycles, Diemer says. Lightand darkness partially affect circadian rhythms to theextent that poorly lit areas may trigger your body tothink it needs sleep, according to the WebMD onlinesite (www.webmd.com).
Upkeep and laborLights can use as much as 30% of a hospital’s
energy, and light repairs and installations can takeup more time than expected, Diemer says.
On the other hand, good lighting promotes bettermaintenance, she adds. That benefit in turn makes iteasier for maintenance crews to work effectively, sotake the following actions in that regard:
• Minimize the number of lamp types you use in ahospital. Doing so “reduces the amount of stockyou have to keep for maintenance,” she says.
• Use fluorescent lamps, which offer the maximumbulb life. Fluorescent lights have improved inquality over the years and bring out good colorsin their surroundings, Diemer says. Be aware,though, that these lights also contain varyingamounts of mercury, which is a toxic metal highon environmental hit lists.
• Install lights where crews can reach them. Thefacilities department should involve itself in light-ing decisions by weighing in with concerns suchas whether there are ladders tall enough to reachhigh lamps.
Four reasons to see medical settings in better light
1
2
3
Page 5Briefings on Hospital Safety—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Look into these basic lighting concepts
In addition, promoting the frugal use of lights cansave money. “Even in hospitals, it’s unlikely youneed all the lighting on all the time,” Diemer says.
Control switches can help staff members better alter-nate light levels while avoiding energy waste. Also,look at automatic timers to shut off lights that em-ployees often forget about, such as in those storageand utility rooms.
The hospital’s imageFrom a building perspective, lights can cement
the first impressions of visitors as they approach thefront door, sit in the lobby, or wait for an elevator.
“I think the message here is it doesn’t have to looklike a hospital,” Diemer says. Two examples shepoints to include the lobby of the Connecticut
Children’s Medical Center (the fun lighting in thewaiting area adds to a science-museum theme) anda lighted exterior corner of a tower at Children’sMedical Center of Dallas that changes colors.
One approach is to think of how lighting plays arole in welcoming people to the best hotel lobbiesor your own living room. Those ideas can replicatethemselves in hospitals, she says.
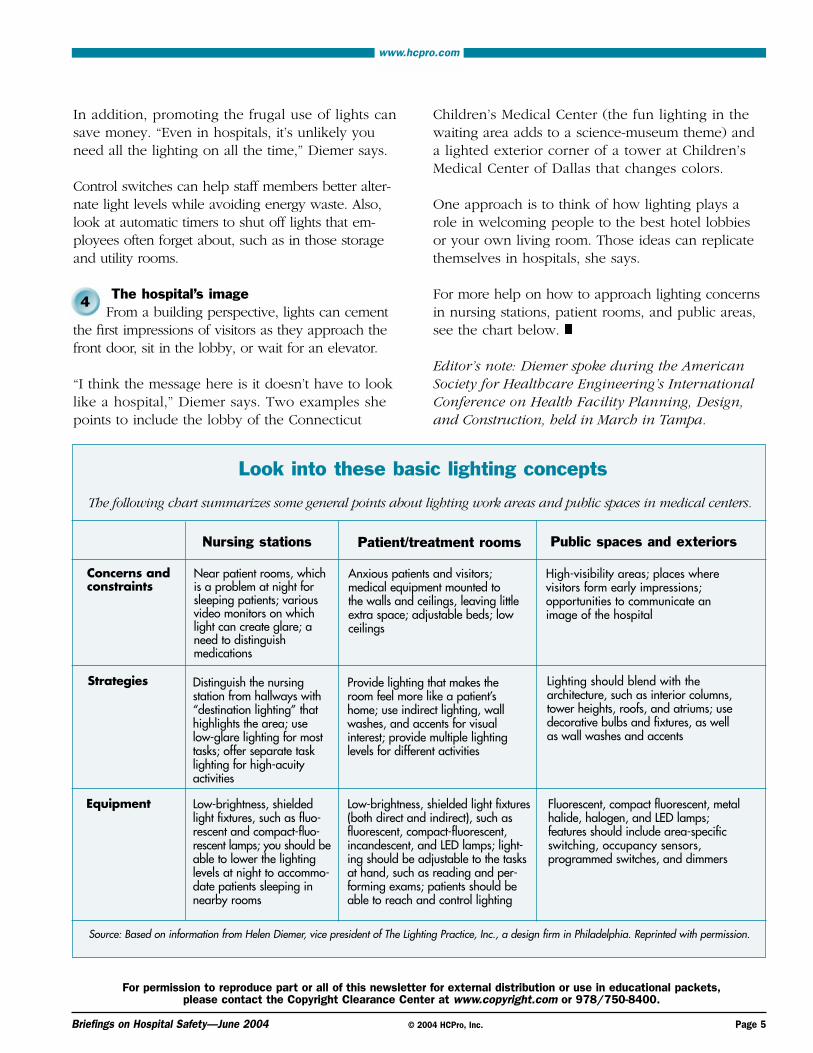
For more help on how to approach lighting concernsin nursing stations, patient rooms, and public areas,see the chart below.
Editor’s note: Diemer spoke during the AmericanSociety for Healthcare Engineering’s InternationalConference on Health Facility Planning, Design,and Construction, held in March in Tampa.
The following chart summarizes some general points about lighting work areas and public spaces in medical centers.
Nursing stations
Near patient rooms, whichis a problem at night forsleeping patients; variousvideo monitors on whichlight can create glare; aneed to distinguish medications
Anxious patients and visitors; medical equipment mounted to the walls and ceilings, leaving littleextra space; adjustable beds; lowceilings
High-visibility areas; places where visitors form early impressions; opportunities to communicate an image of the hospital
Lighting should blend with the architecture, such as interior columns,tower heights, roofs, and atriums; usedecorative bulbs and fixtures, as wellas wall washes and accents
Fluorescent, compact fluorescent, metalhalide, halogen, and LED lamps; features should include area-specificswitching, occupancy sensors, programmed switches, and dimmers
Provide lighting that makes theroom feel more like a patient’shome; use indirect lighting, wallwashes, and accents for visualinterest; provide multiple lightinglevels for different activities
Low-brightness, shielded light fixtures(both direct and indirect), such asfluorescent, compact-fluorescent,incandescent, and LED lamps; light-ing should be adjustable to the tasksat hand, such as reading and per-forming exams; patients should beable to reach and control lighting
Distinguish the nursing station from hallways with“destination lighting” thathighlights the area; use low-glare lighting for mosttasks; offer separate tasklighting for high-acuityactivities
Low-brightness, shieldedlight fixtures, such as fluo-rescent and compact-fluo-rescent lamps; you should beable to lower the lightinglevels at night to accommo-date patients sleeping innearby rooms
Concerns and constraints
Strategies
Equipment
Patient/treatment rooms Public spaces and exteriors
Source: Based on information from Helen Diemer, vice president of The Lighting Practice, Inc., a design firm in Philadelphia. Reprinted with permission.
4

Page 6 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Hand-gel dispensers in corridors
Code change awaits approval of CMS, JCAHO
An amendment to the 2000 and 2003 editions of the Life Safety Code says healthcare facilitiesmay install alcohol-based hand-gel dispensers inexit corridors, provided that the facilities meetthe following conditions:
➼ The corridors must be at least 6 ft wide➼ You must separate the dispensers by at least
4 ft➼ The maximum capacity for dispensers is 1.2 L
for those in rooms, corridors, and areas opento corridors; that amount increases to 2 L fordispensers in suites
➼ You can’t install dispensers over or directlyadjacent to electrical outlets and switches
➼ You can only install dispensers over carpetedfloors in smoke compartments protected bysprinklers
➼ Each smoke compartment may contain acumulative 10 gal of hand-gel solution in dis-pensers and a maximum of 5 gal in storage
Source: American Society for Healthcare Engineering.
The back-and-forth debates about allowing alcohol-based hand-gel dispensers in exit corridors seems tobe coming to a close.
On April 28, the National Fire Protection Associationannounced that its Standards Council approved a“technical interim amendment” to the 2000 and 2003editions of the Life Safety Code (LSC).
The amendment revises the healthcare chapters ofthe LSC to permit hand-gel dispensers in corridors(for more details, see the box on this page).
But if you don’t already have dispensers in your cor-ridors, it may be worth holding off on any installationuntil the Centers for Medicare & Medicaid Services(CMS) and the Joint Commission on Accreditation ofHealthcare Organizations (JCAHO) formally adoptthe amendment. As of May 3, neither group haddone so.
“I anticipate that CMS and JCAHO will issue state-ments regarding their reaction to the NFPA decisionand discuss their enforcement plans,” says DaleWoodin, executive director for advocacy at theAmerican Society for Healthcare Engineering (ASHE).ASHE lobbied heavily for the LSC amendments.
The installation of hand-gel dispensers straddled theline between hand-hygiene efforts promoted by theJCAHO and the Centers for Disease Control and Pre-vention, and the fire-safety risks of having flammableliquids along an exit route.
A study commissioned by ASHE last year suggestedthat there is a middle ground between these twoconcerns, which provided the foundation of therecent LSC amendment.
“By providing detailed criteria on the use and stor-age of alcohol-based hand rubs, the [amendment]provides guidance to minimize any potential fire riskwhile allowing hand-rub dispensers to be located inconvenient locations to maximize access and use by
healthcare workers,” ASHE wrote to its members.
Within the last few months, ASHE and other propo-nents of corridor dispensers ran into hiccups dealingwith technical LSC issues, such as the appropriatespot to place an amendment within the healthcarechapters and whether the change was of an emer-gency nature from a fire-protection standpoint.
Typically, LSC amendments must present a pressingneed for immediate action, and some NFPA mem-bers doubted that important infection-control con-cerns qualified as urgent fire-safety matters.
Check out the details of the hand-gel amendment

Page 7Briefings on Hospital Safety—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Enclosed with your issue of BHS is a free spe-cial report that details the latest informationabout the environment of care portion of sur-veys in 2004.
We’ve compiled the results from our online pollof surveyed hospitals to give you an up-to-datepicture of what the Joint Commission on Ac-creditation of Healthcare Organizations focuseson when it comes to safety.
We’ll continue to accumulate the results as themonths roll on. If your hospital recently under-went a survey—or if you’ll go through one inthe near future—please consider taking ourquestionnaire. E-mail Senior Managing EditorScott Wallask at [email protected] for a linkto the survey.
on a scale of 1–4, with 4 representing the highestrisks.
Then, Tipton sat down with department staffs—without the unit directors in the room—and askedfrontline workers about the scores. “The staff hadan opportunity to provide feedback about therisks,” he says.
The scores served the following two purposes:1. Broadly, they allowed the hospital to pick up on
high-risk areas and develop policies around them2. Tipton also used the information to craft a 25-
question quiz that looked at the seven environmentof care (EC) plans, with an emphasis on particu-larly risky areas, such as workplace violence
Tipton set a goal of quizzing 40 employees eachmonth and then using their results to map quarterlytrends and develop targeted education. As it turnsout, in 2003 he took in 1,278 quizzes, which provid-ed an excellent overview of where safety stood in
employees’ minds.
One wrong, you’re goneTipton was blunt when scoring the quizzes: If some-one answered one question wrong, he discountedthe entire quiz.
His thinking was that if one person answered some-thing incorrectly, it could indicate trouble with otheremployees, too, he says. “I didn’t want to give thesurveyors any room” to explore those results, headds.
Instead, he tightened up on educating employees.Tipton held training and inservices, using the follow-ing ideas:• As part of the hospital’s internal newsletter that
goes out with paychecks, he authored articles onhot safety topics
• He took digital photos of safety violations andsent them to the patient-care coordinators of the units in question to let them know whathappened
• He created a hazard room where he staged a“What’s wrong with this picture?” exercise, whereemployees tried to identify 25 hazards, such as anunsecured oxygen tank, a syringe left on a table,or confidential patient information in the trash can
The hazard room was a fun popular way to teststaff knowledge, Tipton says. About 800 employeeswalked through the room, and occasionally he drewparticipants’ names from a bowl to win a raffle fordonated gift certificates from local merchants.
These education efforts succeeded. In the secondquarter of 2003, 9% of those employees who tookthe safety quizzes failed. That number dropped tozero by the fourth quarter. “All that work paid individends,” Tipton says.
Editor’s note: To learn more from Tipton aboutwhat the JCAHO looked at during its visit to Red-lands Community Hospital, see “Survey Monitor”on the next page.
JCAHO < p. 1
Special report delves into2004 survey results
Page 8 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Survey monitor: The JCAHO wants you to detail your safety risks and how you offset these hazards
This survey occurred March 8–11 atRedlands (CA) Community Hospital, a182-bed acute-care facility.
During this visit from the Joint Commission on Ac-creditation of Healthcare Organizations (JCAHO), theconcept of knowing your site’s potential safety haz-ards took an overshadowing role. The two surveyorsrepeatedly wanted to know what risks the hospitalidentified within the seven environment of care (EC)plans and what it did in response to those findings.
“That’s a spin that a lot of people aren’t ready for,”says Gary Tipton, safety officer at the hospital. Fortunately, at Redlands, staff members armed themselves with knowledge about the seven plans, thanks to preparation that began in 2002.
See the related story on p. 1 for more about whatsteps the hospital took to ready staff members.Meanwhile, let’s continue with a look at how firesafety and security received the lion’s share of sur-veyor attention.
A backlog of washA broken linen-chute door latch landed the hospitala requirement for improvement (formerly known asa Type I recommendation). The surveyor checkedthe laundry-chute exit doors and found one that
didn’t close properly.
Expect this inspection during your survey, too, sinceit’s spelled out in the JCAHO’s presurvey packet thatit sends to hospitals.
At Redlands, the chute door’s latch bulged from thepressure of stacked linen bags, forcing the door slight-ly open, Tipton says. The door has a fusible link toclose it during a fire alarm, but that feature only workswhen the door remains fully open. In this case, it’sdoubtful that an alarm would have caused the doorto close any further than it already was, he says.
The hospital realized the latch needed repairs andlisted it on its plan for improvement in the Statementof Conditions. However, the surveyor still cited thehospital for the deficiency, which stung everyone.
“He wouldn’t give us any slack,” Tipton says. “But wefelt if this was the only thing he found [wrong], let’snot ruffle his feathers. We kept our mouths shut.”
Not what you want to hearLater, a surveyor and an accompanying entouragefrom the hospital were in a hallway when the facili-ty’s director of materials management walked by.The surveyor pulled her over and asked her wherea fire-alarm pull station was located.
BHS Subscriber Services Coupon Your source code: N0001
Name
Title
Organization
Address
City State ZIP
Phone Fax
E-mail address(Required for electronic subscriptions)
❑ Payment enclosed. ❑ Please bill me.❑ Please bill my organization using PO # ❑ Charge my: ❑ AmEx ❑ MasterCard ❑ VISA
Signature(Required for authorization)
Card # Expires(Your credit card bill will reflect a charge to HCPro, the publisher of BHS.)
❑ Start my subscription to BHS immediately.
Options: No. of issues Cost Shipping Total
❑ Print 12 issues $269 (BHSP) $18.00
❑ Electronic 12 issues $269 (BHSE) N/A
❑ Print & Electronic 12 issues of each $336 (BHSPE) $18.00
Sales tax(see tax information below)*
Grand total
Order online atwww.hcmarketplace.com and save 10%
Be sure to enter source code N0001 at checkout!
*Tax Information Please include applicable sales tax. Electronic subscriptions are exempt.States that tax products and shipping and handling: CA, IL, MA, MD, NJ,VA, VT, FL, CT, GA, IN, MI, NC, NY, OH, PA, SC, TX, WI. States that tax prod-ucts only: AZ, TN. Please include $21.95 for shipping to AK, HI, or PR.
Mail to: HCPro, P.O. Box 1168, Marblehead, MA 01945 Tel: 800/650-6787 Fax: 800/639-8511 E-mail: [email protected] Web: www.hcmarketplace.com

Hot spots: Life safety, security, and safety-riskidentification
EC requirements for improvement: Alinen-chute door didn’t latch properly
EC supplemental findings: NoneEC tracers: Several records-based reviews,
such as tracing how safety-committee deci-sions evolved
Quote of note: “We felt if this was the onlything he found [wrong], let’s not ruffle hisfeathers. We kept our mouths shut.”
Page 9Briefings on Hospital Safety—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
After looking around, the director answered that shedidn’t know, which prompted another staff member toshow the surveyor the nearest alarm box, Tipton says.“It was kind of spooky that she didn’t know,” espe-cially since she sits on the safety committee, he adds.
Sensing a potential problem, the surveyor askedsomeone to pull the alarm and had staff membersconduct a fire drill on the spot. Luckily, the exercisewent well, as 40 employees responded. As is normalduring drills at Redlands, Tipton handed out a seven-question fire-safety quiz to drill participants, whichhelped reassure the surveyor. He didn’t dwell on theslip-up with the pull station any further.
How do you stop abductions?During the building tour, surveyors often asked staffmembers security-related questions.
For example, security officers had to explain theirresponsibilities and qualifications, while clinicians onthe pediatrics unit discussed measures taken to avoidabductions of infants and children. Even a physicianconducting his rounds had to tell a surveyor how thehospital prevented abductions, Tipton says.
These interactions proved to Tipton that all workers,including volunteers and students, need to be awareof infant and child kidnapping policies in the hospital.
Giving a sense of order to the surveyors proved apowerful ally for the hospital. During a review of theemergency-management plan, Tipton presented theJCAHO with a binder that outlined the findings ofthe hazard vulnerability analysis, how the hospitalparticipates with city officials during disaster training,and various drill records.
Seeing the binder impressed the surveyor and so hedidn’t delve much further into emergency manage-ment, Tipton says.
Tracers are lightweightThe only safety tracers the surveyors conducted wererecords-based. For example, they reviewed the safe-ty-committee minutes, found various decisions, andwanted to see the paper trail of data that promptedthose votes. Tipton often found this information in
the annual safety-plan assessments.
Patient safety received a more thorough review. During the EC tour and interview, surveyors askedabout National Patient Safety Goals #5 (free-flowprotection of infusion pumps) and #6 (clinical alarms).All infusion pumps at Redlands feature free-flowprotection, so there wasn’t a lot to dwell on withGoal #5.
For clinical alarms, surveyors wanted to knowwhether• the hospital held inservices about this goal• various alarms actually worked• staff members could hear the alarms
To follow up on this review, the surveyors pulledbathroom emergency cords in two locations andwatched the staff respond to these alarms, Tiptonsays.
During the visit, the surveyors also• asked various people on each floor where the
nearest adjacent smoke compartment began• checked for barrier penetrations on each floor• looked at the conditions of hazardous-materials
storage areas• asked workers about medical-gas alarms• recommended that at least one physician partici-
pate on the safety committee
Currently, the safety committee doesn’t have a physician representative.
Survey at a glance

Page 10 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Bits & briefs
Eyewash standard gets a makeoverA eyewash standard commonly referenced by theOccupational Safety and Health Administration(OSHA) just received an update from its publisher,the American National Standards Institute (ANSI).
The 2004 version of Emergency Eyewash and Show-er Equipment, otherwise known as ANSI Z358.1,contains some revisions to note, says CristineFargo, technical projects coordinator for the Interna-tional Safety Equipment Association in Arlington, VA.Changes include the following:• An emphasis that the standard considers drench
hoses and personal wash units as supplementalequipment, meaning that they don’t necessarilyneed to provide 15-minute flushing capacities orhands-free operation
• An explanation for the required weekly operationof plumbed equipment; this test ensures that thewater or other fluid is available at the head of thedevice and also clears sediment out of the supplyline
Fargo’s association developed the revised edition of Z358.1. For more information or to purchase thestandard, go to www.safetyequipment.org/eyewash2.htm.
Venting against vendingBased on the following “attack,” we may need tochange BHS’ coverage to include the safety of inani-mate objects.
Police arrested a man on March 22 after he allegedlyshook and damaged a vending machine at NorthWoods Medical Center in Taunton, MA, according tothe Boston Herald. The incident—apparently precipi-tated when the machine ate the suspect’s dollar bill—also resulted in damage to a new tile floor.
Ironically, police also charged the man with drivingwhile not having a license. He lost that privilegefor allegedly not paying child support, the Heraldreported.
New goals could include surgical firesAlthough still unofficial, two proposed additions tothe National Patient Safety Goals could involve safe-ty issues. The Joint Commission on Accreditation ofHealthcare Organizations (JCAHO) released detailsabout the following possible goals:• Reduce the risk of surgical fires by teaching staff
members how to control heat, fuel, and oxygenconcentration in the operating room, drilling sur-gical team members, and reporting fires to groupssuch as the JCAHO and the Food and DrugAdministration
• Reduce patient falls by assessing each patient’srisk of falling, establishing a fall-reduction pro-gram, modifying the environment of care tominimize harm to patients if they fall, installingbed alarms for at-risk patients, using “low beds”for at-risk patients, and avoiding the use of full-length bed rails
The JCAHO will finalize decisions on any new Pa-tient Safety Goals later this year. To learn more on-line, go to www.jcaho.org/accredited+organizations/patient+safety/npsg.htm.
Minutia update, JCAHO styleSpeaking of the JCAHO, we saw some EC standardclarifications and corrections online recently. The listincludes errata about requirements for emergencymanagement, fire safety, medical equipment, andutilities.
To read the full list, go to www.jcrinc.com/subscribers/perspectives.asp?durki=2815, click on “hospitals,”and scroll down to the “EC” heading. We’ve foundit’s worth checking this site each month or so to seewhat’s new.
Federal electrical rules may evolveOSHA may overhaul various standards under itselectrical-installation regulations to bring them morein line with current fire codes.
The proposed changes will focus on safety in the

Page 11Briefings on Hospital Safety—June 2004 © 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
design and installation of electrical equipment inhospital and other businesses. The changes drawheavily from two publications from the NationalFire Protection Association (NFPA):
1. NFPA 70E, Electrical Safety Requirements forEmployee Workplaces (2000 edition)
2. NFPA 70, the National Electrical Code (2002 edition)
Existing electrical standards from OSHA rely on the1979 edition of NFPA 70E, which distances it fromcurrent practices and technology, according to theagency. You can find the full proposal by goingonline to www.osha.gov/wutsnew.html and scrollingto the April 13 entries.
Big lab controversy in BaltimoreWe don’t know all the details, but it sure seemslike the top dogs at Maryland General Hospital in Baltimore didn’t take claims of compromisedworker and equipment safety too seriously.
And the results haven’t been good: They’ve in-cluded more than 2,000 follow-up letters to labpatients, a worker who contracted HIV and hepati-tis, and series of hard-hitting newspaper articles.So far the resignations include of two lab direc-tors and the hospital’s president.
Various state and federal regulators concluded that
Maryland General issued hundreds of HIV andhepatitis test results even though lab equipmentreadings indicated that those results might be inac-curate, according to the Baltimore Sun. A formerlab worker sent the lab’s administrative director aletter months earlier outlining the problems. Theletter eventually made it to state officials, who sub-sequently investigated the claims.
The lab worker has sued the hospital, arguing thatshe became infected with HIV and hepatitis whenone of the lab machine’s in question malfunctionedand splattered her with infected blood, the Sunreports. She also sued the device’s manufacturer,Adaltis USA, Inc., of Allentown, PA.
A new weapon in hand hygiene?Who knows, someday you may start seeing signs inthe bathroom that say, “All employees must scantheir hands before returning to work.” If you do,remember to thank beef slaughterhouses.
A company in Florida called eMerge plans to mar-ket a scanner to healthcare facilities that detectsfecal traces and pinpoints where one’s hands needthe most scrubbing, according to the AssociatedPress.
The company already manufactures scanners thatexamine cow carcasses for fecal contamination. Itplans to tweak the devices and may start sellingthem to hospitals by the end of the year.
If you need formal statistics to help you back upthe well-known problem of occupational injury inthe nursing field, check out the following:
The U.S. Department of Labor reports that in2002, nursing aides and orderlies suffered 79,000injuries on the job—the second highest amountof occupational injuries in the country next totruck drivers. Of those injuries, all of whichrequired days away from work, 91% were towomen.
Nursing aides and orderlies usually suffered sprainsand strains to their shoulders and backs due tooverexertion related to lifting or moving patients.In a related ergonomics note, these people exhib-ited the highest number of musculoskeletal disor-ders (44,400) in 2002. The Labor Departmentdefines a musculoskeletal disorder as an injury tomuscles, nerves, tendons, joints, cartilage, andspinal discs. They don’t include injuries causedby slips, trips, falls, motor-vehicle accidents, orsimilar incidents.
Nursing jobs can hurt you
Page 12 Briefings on Hospital Safety—June 2004© 2004 HCPro, Inc.
www.hcpro.com
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
isolating patients.
The patient at the center of this case—a man withschizophrenia and HIV—came to a hospital in Wash-ington, DC, twice in March 2002 with a fever andcough. After learning that a test taken during the firststay showed evidence of tuberculosis, staff membersplaced the patient in an isolation room and tracedwhom he had contact with.
The patient met with several other patients and work-ers before the diagnosis, and surprisingly, “this con-tact continued even after the patient was placed inisolation,” according to the CDC.
The hospital later identified 1,045 people that theoriginal patient had some contact with, including784 staff members. Among those employees, 14%provided direct care to the original patient, 6% work-ed in the same ward but didn’t provide direct care,and 80% were other staff members who spent timein the ward.
In the March 19 issue of Morbidity and MortalityWeekly Report, health officials emphasized that hospi-tals must maintain basic infection-control practices fortuberculosis or risk needlessly exposing workers.
The information stems from an investigation con-ducted by the Centers for Disease Control and Pre-vention (CDC) in 2002. The CDC recommended thefollowing steps:• Place patients with suspected tuberculosis in
isolation rooms until you rule out infectioustuberculosis
• When transporting these patients for medical pro-cedures outside isolation rooms, require them towear surgical masks
• Develop infection-control policies for HIV-infectedpatients with lung symptoms that suggest tubercu-losis infections
HIV sometimes masks tuberculosis symptoms suchthat clinicians may not quickly recognize them, theCDC says. This confusion can lead to delays in
Tip of the month
Briefings on Hospital SafetyEditorial Advisory Board
Publisher/Vice President: Suzanne Perney Senior Managing Editor: Scott Wallask [email protected] Editor: Steven MacArthur, consultant, The Greeley Company, Marblehead, MA [email protected] Publisher: Bob Croce
Steven BryantPractice Director, Accreditation ServicesThe Greeley CompanyMarblehead, MA
Cherryl M. Crouch, CSPSafety Officer, Northwestern Memorial HospitalChicago, IL
Mark E. Furlane, JD, MBAPartner, Gardner, Carton & DouglasChicago, IL
Hugh P. GreeleyFounder, The Greeley CompanyMarblehead, MA
David N. Hill, RPA, CFM, BAEIM, MSHSADirector of Support ServicesHazelden Foundation, Center City, MN
Linda D. Lee, MS, REMDirector, EH&SUniversity of TexasMD Anderson Cancer CenterHouston, TX
Ray W. MoughalianPresidentRM Associates Inc.Haverhill, MA
John L. Murray Jr., CHMM, CSP, CIHSafety Director, Baystate Health SystemSpringfield, MA
Paul Penn, MS, CHEM, CHSPEnMagine/HAZMAT for HealthcareDiamond Springs, CA
Steve SchultzCorp. E&O Safety DirectorCape Fear Valley Health SystemFayetteville, NC
Kenneth S. Weinberg, PhDPresidentSafdoc Systems, LLCStoughton, MA
Steven Weinstein, MT(ASCP) MPH, CIC, HEMEnvironmental, Health & Safety SpecialistAbbott Laboratories, MediSense ProductsBedford, MA
Pier-George Zanoni, PE, CSP, CIHConsultantFacilities Management ConsultingSt. Johns, MI
Briefings on Hospital Safety (ISSN 1076-5972) is published monthly by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. Subscription rate: $269/year or $484/two years; back issues areavailable at $25 each. • Periodicals postage paid at Marblehead, MA 01945 and other mailing addresses. Postmaster: Send address changes to Briefings on Hospital Safety, P.O. Box 1168, Mar-blehead, MA 01945. • Copyright 2004 HCPro, Inc. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by anymeans, outside the subscriber’s facility, without prior written consent of HCPro, Inc., or the Copyright Clearance Center at 978/750-8400. Please notify us immediately if you have received an unau-thorized copy. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For renewal or subscription information, call customer service at 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to beincluded on this mailing list, please write to the Marketing Department at the address above. • Opinions expressed are not necessarily those of BHS. Mention of products and services does not con-stitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions.
Isolation and HIV savvy are two steps to rein in tuberculosis infections
A supplement to Briefings on Hospital Safety
How the JointCommission surveys
EC standardsin hospitals
Volume 1, January–April 2004
How the JointCommission surveys
EC standardsin hospitals
Volume 1, January–April 2004
How the JointCommission surveys
EC standardsin hospitals
Volume 1, January–April 2004
SAFETY
ALE
RT
SAFETY
ALE
RT
How the Joint Commission surveys EC standards in hospitals2
We rely on you for safety findings in surveysDear readers,
When the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) unveiled its revised sur-vey program in January, safety officers and facility directors wondered how it would affect their compliancewith the environment of care (EC) standards.
We decided to poll readers who took part in surveys this year to find out about their EC experiences. Onthe following pages, you’ll find an in-depth look at what standards received the most attention and whatproblems cropped up in safety.
This special report wouldn’t be possible without the help of those folks who responded to our online ques-tionnaire. Based on the poll’s early success, we anticipate running an update to this report later this year toprovide you with even more survey information.
We also want to note comments in our stories from the following two people who spoke during an April13 audioconference about recent JCAHO surveys, which HCPro, Inc., presented:• Karen Nelson, MPA, RN, executive director of clinical compliance and risk management at Brigham
and Women’s Hospital in Boston• Carol Butcher, RN, CPHQ, quality improvement/patient-safety manager at Harrison Hospital in
Bremerton, WA
If you have an upcoming survey, or recently completed one, and would like to participate in our poll,please e-mail me at the address below for the direct link to the Web site. I also welcome your thoughts onthis report or any other safety issue in healthcare.
Sincerely,
Scott WallaskSenior Managing [email protected]/639-1872, Ext. 3119
Facilities in the following states participated in our online questionnaire:
• California• Connecticut• Florida• Georgia• Illinois• Indiana• Iowa
• Louisiana• Maryland• Massachusetts• Missouri• North Carolina• North Dakota• Pennsylvania
• Texas• Virginia• Washington• West Virginia• Wisconsin

Volume 1, January–April 2004 3
An easier and better survey process, readers sayCheck out tips on what standards to pay special attention to
The revised survey approach seems to be a hit withsafety committees that have already dealt with a visitthis year from the Joint Commission on Accreditation ofHealthcare Organizations (JCAHO).
An online poll presented by Briefings on HospitalSafety received responses from 32 hospitals that under-went surveys from January to April—that’s roughly twosurveyed medical centers each week sending us infor-mation from the frontlines.
When asked about the JCAHO’s Shared Visions–NewPathways® program and how it related to safety toursduring a survey, about three-quarters of the respon-dents indicated it was better than the old approach. Onthe other hand, 16% said the program was about thesame as the earlier approach, and 6% said the JCAHO’schanges were for the worse.
Shared Visions puts a greater onus on hospitals to con-tinuously comply with JCAHO standards, includingthose covering the environment of care (EC). Newpieces of this process include surveyors armed withmore specific information about a hospital before theyvisit and the use of “tracer methodology,” in which sur-veyors track a patient or procedure through the facility.
Meanwhile, most folks (68%) said getting through theEC portion of the survey was easier under the SharedVisions program. See figures 1 and 2 for full details.
Point-by-point reviewWe asked safety officers and others who took ouronline questionnaire to rate how much each EC stan-dard figured into the survey. The chart on p. 4 detailstheir responses, but you should note the followinghighlights:
• The JCAHO universally discussed two particularstandards at all the hospitals who got in touch withus: EC.4.10 (emergency plan) and EC.9.10 (moni-toring the EC)
• Surveyors seem to ask the most detailed questionsabout EC.4.10 and EC.5.10 (fire-safety plan) accord-ing to safety folks, the majority of whom said theJCAHO heavily questioned them about these areas
• In more than half of the surveys, EC.1.30 (no-smoking policy) and EC. 7.50 (testing medical-gasand vacuum systems) received little or no discussion
The following are some ideas on embracing the abovebulleted points for future surveys. When it comes toemergency management under
Figure 1Overall, the JCAHO’s new survey process is:
0 10 20 30 40 50 60 70 80
Figure 2In your experience, getting through the
EC portion of this survey was:
Better than the oldapproach—74%
The sameas the oldapproach—16%
Worse than theold approach—6%
This was my first survey—3% Easier than past
surveys—68%
About the same aspast surveys—19%
More difficult thanpast surveys—10%
This was my firstsurvey—3%
continued on p. 5

How the Joint Commission surveys EC standards in hospitals4
Standards
EC.1.10 (safety plan)
EC.1.20 (testing safety elements)
EC.1.30 (nonsmoking policy)
EC.2.10 (security plan)
EC.3.10 (hazmat/waste plan)
EC.4.10 (emergency plan)
EC.4.20 (disaster drills)
EC.5.10 (fire-safety plan)
EC.5.20 (Life Safety Code® compliance)
EC.5.30 (fire drills)
EC.5.40 (testing fire equipment)
EC.5.50 (life-safety deficiencies/interim life-safety measures)
EC.6.10 (medical-equipment plan)
EC.6.20 (testing medical equipment)
EC.7.10 (utilities plan)
EC.7.20 (emergency power)
EC.7.30 (testing utilities)
EC.7.40 (testing emergency power)
EC.7.50 (testing medical gas/vacuum)
EC.8.10 (appropriate environment)
EC.8.20 (N/A—reserved for settings other than hospitals)
EC.8.30 (construction/renovation)
EC.9.10 (monitoring the EC)
EC.9.20 (identifying EC issues)
EC.9.30 (improving the EC)
Heavily discussed
45%
26%
13%
32%
19%
57%
42%
58%
48%
39%
10%
19%
27%
48%
19%
26%
23%
29%
10%
17%
N/A
13%
29%
26%
48%
Somewhat discussed
52%
71%
29%
65%
68%
43%
52%
35%
48%
48%
81%
71%
63%
39%
71%
68%
61%
68%
38%
57%
N/A
45%
71%
68%
45%
Not discussed
3%
3%
58%
3%
13%
0%
6%
6%
3%
13%
10%
10%
10%
13%
10%
6%
16%
3%
52%
27%
N/A
42%
0%
6%
6%
Look at what standards surveyors emphasized
Our online poll asked respondents the degree to which surveyors discussed or analyzed the environment of care (EC) standards. The highest percentages we received for any given standard may point to trends inupcoming surveys.
Volume 1, January–April 2004 5
EC.4.10, expect surveyors to review your hazard-vul-nerability analysis and how your facility would cooper-ate with community agencies during a disaster. At leastone surveyor recommended that a hospital review itshazard-vulnerability analysis annually. You may alsoneed to present your emergency-drill records.
Hospitals that are part of complex organizations—suchas ones that also include outpatient sites and homehealthcare—should make sure that those outer servicesare part of the overall hazard-vulnerability analysis orconduct separate hazard reviews for each entity.
Questions about EC.5.10 shouldn’t surprise anyone,because the JCAHO makes it clear that the majority of its building tours will focus on life-safety concerns.Typical activities include checking above ceilings forproper fire protection features, visiting linen/waste roomsand their chutes, following continuous exit paths, andreviewing fire-alarm and fire-pump operations.
EC.9.10 deals with monitoring conditions in the ECand the annual evaluations of the seven EC plans.Pay particular attention to the wording the JCAHOassigns to the annual evaluations—you must reviewthe objective, scope, performance, and effectivenessof each plan.
You may find it beneficial to prepare a matrix using the JCAHO’s six processes for managing risks in the EC:planning, teaching, implementing, responding, monitor-ing, and improving. The JCAHO notes this cycle in thesurvey package that it provides to hospitals.
Tracers take many formsAs mentioned earlier, the idea of patient tracers is atthe forefront of the Shared Visions program. Thesetracers offer plenty of opportunities to examine ECissues—for example, a surveyor reviewing a newborn’scase may ask staff members about infant-abductionpolicies.
The building tour and EC session also offer openingsfor “system tracers,” where surveyors review a proce-dure or decision, such as how you assess infectioncontrol during construction.
During the JCAHO’s survey in January, staff memberssaw utilities, bioterrorism, and emergency managementall come up during tracers, says Carol Butcher, RN,CPHQ, of Harrison Hospital in Bremerton, WA.
“Our safety director and environment of care managershad a little tougher time” than expected in handlingtracers because those folks traditionally are accustomedto being the only people surveyors ask about safetyissues, Butcher adds. Now, surveyors are likely toapproach anyone and test their EC knowledge.
That being said, it isn’t a definite that safety officerswill sweat through a tracer. In our online poll, 61% ofthe hospitals said the EC did not come up as its owntracer or as part of a patient tracer. However, theremaining 39% who did experience
Better survey continued from p. 3
What did surveyors trace?
During patient and system tracers, surveyorslooked at the following safety items:
• Processing ultrasound probes • Maintenance records of generators, fire/smoke
dampers, and waste chutes • Infection-control monitoring for airborne
substances• Personal-protective equipment for certain
clinical equipment• Investigation of an attempted patient suicide
(first discovered by the surveyor in the safety-committee minutes)
• Training of outside law enforcement and corrections officers
• End-user training on medical equipment• Patient safety on a geropsychiatric unit• Risk assessments stemming from evidence
of suicide hazards• Security-officer responsibilities in the
emergency department• Child-abduction prevention policies • Rental equipment
continued on p. 6
How the Joint Commission surveys EC standards in hospitals6
Other safety tidbits to watch forSecurity-sensitive areas, particularly infant and pediatricwards, came up during many surveys. Expect to fieldquestions about your infant-abduction policy.
The training of security officers and outside policeoften also surfaces during the tour of buildings ordepartments.
Although surveyors won’t automatically visit construc-tion areas, several hospitals in our poll indicated thatthey answered questions about ongoing projects. Onearea noted was whether the safety officer involvedother departments in preconstruction planning.
Hazardous-materials management is also a potentialtopic for discussion. Several hospitals mentioned sur-veyors prodding them about how they handle a haz-mat from when it enters the building to when itleaves, whether they correctly complete waste mani-fests, and what kind of decontamination proceduresthey have in place for hazmat incidents.
As with any roundup of survey results, a share of hos-pitals received requirements for improvement (formerlyType I recommendations) and supplemental findings.See the related story on p. 7 for details on these hotspots.
EC-related tracers shared some interesting observations(see the box on p. 5).
Hospitals must prepare staff members for tracer ses-sions, says Karen Nelson, MPA, RN, of Brigham andWomen’s Hospital in Boston. Tracers “can be a bitintimidating for a staff member, even a seasoned staffmember,” when a surveyor watches your every move,she says, based on her experiences from a JCAHO sur-vey in February.
An emphasis on hand hygieneOf the three National Patient Safety Goals that explicitlyinvolve EC matters, two out of the three came up duringmost surveys. The following is a quick rundown of howmany sites had to discuss compliance with these goals:
• Goal #5 (ensuring that infusion pumps have free-flow protection)—48% of respondents
• Goal #6 (ensuring that staff members can hear clin-ical alarms and test these levels)—70%
• Goal #7 (reducing hospital-acquired infectionsthrough greater hand hygiene and related sentinel-event reporting)—74%
During her JCAHO visit, a surveyor observed a surgeonclean his hands as he scrubbed for an operation, Butchersays.
continued from p. 5Better survey
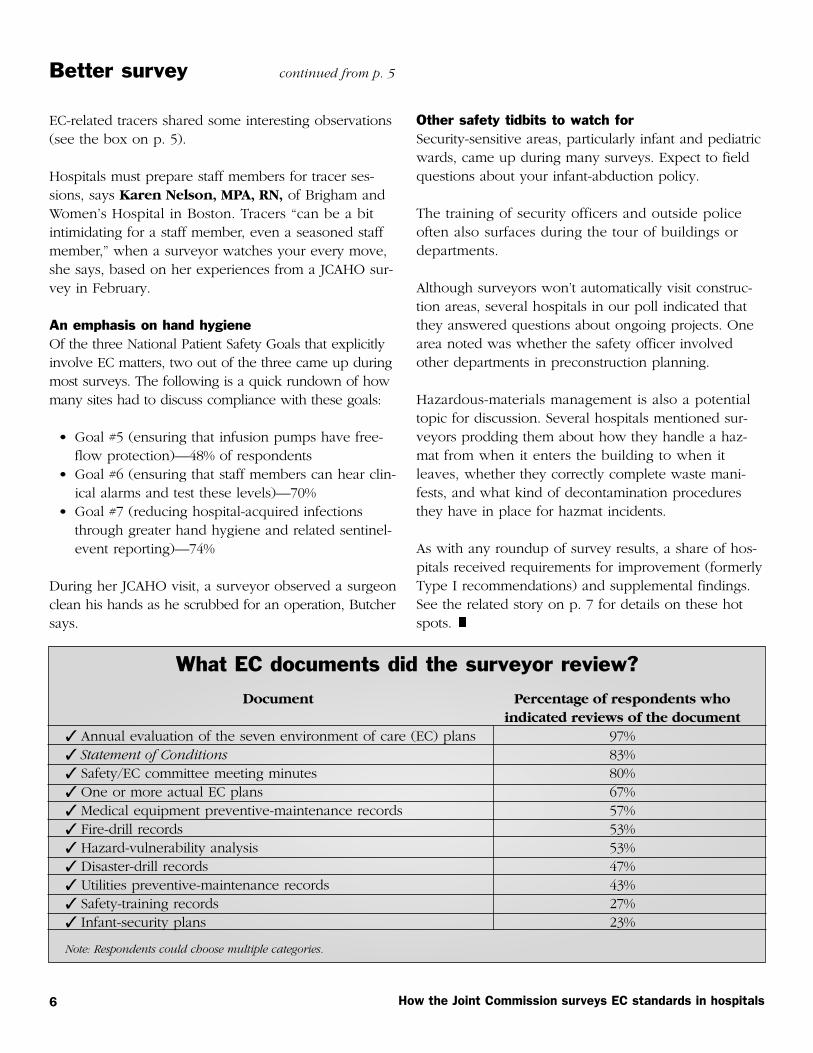
What EC documents did the surveyor review?
Document
✓ Annual evaluation of the seven environment of care (EC) plans✓ Statement of Conditions✓ Safety/EC committee meeting minutes✓ One or more actual EC plans✓ Medical equipment preventive-maintenance records✓ Fire-drill records✓ Hazard-vulnerability analysis✓ Disaster-drill records✓ Utilities preventive-maintenance records✓ Safety-training records✓ Infant-security plans
Percentage of respondents who indicated reviews of the document
97%83%80%67%57%53%53%47%43%27%23%
Note: Respondents could choose multiple categories.
Volume 1, January–April 2004 7
First, the good news: By far, most hospitals thatresponded to our online poll (84%) didn’t receiveany requirements for improvement in the environ-ment of care (EC).
The few noted citations—formerly known as TypeI recommendations—centered on fire safety.
For example, a surveyor from the JointCommission on Accreditation of HealthcareOrganizations (JCAHO) handed one hospital arequirement for improvement under EC.5.20. Thisstandard requires compliance with the Life SafetyCode (LSC ) and the Statement of Conditions.
In particular, the surveyor noted problems withbarrier penetrations, roller latches, linen chutes,and kitchen hoods.
Exits and doors grab attentionAt another site, a surveyor was displeased at notfinding an exit sign he felt should have been in a certain location. The hospital installed the signbefore the survey ended. Obstructed exit signs re-sulted in a requirement for improvement in a dif-ferent hospital.
Also, a surveyor issued a citation for door require-ments in the LSC, with door gaps wider than 1/8in and louvers in doors being prime concerns.
Fire drills required under EC.5.30 received atten-tion at one facility, which took home a citation forbeing unable to demonstrate consistent drills ina unit. Surveyors also found the fire-alarm-testingsystem faulty at that site.
Our respondents noted two other requirementsfor improvement that they received: improperlyconducting a hazard-vulnerability analysis(EC.4.10—emergency-management plans) and aneed to perform more environmental-risk assess-ments (seven EC plans).
Details on supplemental findingsA bit lower on the ladder, butimportant nonetheless, are supple-mental findings in the EC.
A little more than one-third of the respondents (37%)reported receiving these findings from the JCAHO.
Again, fire safety proved to be a sticky point for somehospitals, including findings for not properly markingexit stairs, a lack of battery-operated lights in anoperating room, improperly sealed fire-wall penetra-tions, and a recommendation to install sweeps undertwo doors to improve fire safety—all of which fallunder EC.5.20.
Further, one site received a supplemental findingbecause staff members missed two fire extinguishersduring an inspection (EC.5.40—maintaining fire-safetyequipment).
Respondents also received supplemental findings forproblems in the following areas:
• Annual testing of radiation protective equipment(EC.3.10—handling hazardous-materials risks)
• A locked trash compactor didn’t have a working kill switch (EC.1.10—handling safetyrisks)
• Reviewing the effectiveness of EC plans annually(EC.9.10—monitoring EC conditions)
• A 95% completion rate for preventive maintenanceof clinical devices (EC.6.20—maintaining andinspecting medical equipment)
• Conducting a hazard-vulnerability analysis(EC.4.10)
• Safe transport of sharps by contracted services(EC.3.10)
Fire-safety problems lead citations

How the Joint Commission surveys EC standards in hospitals8
Before your next survey, test corrective plans by using staged conflicts with staff members
Under the new survey approach from the JointCommission on Accreditation of Healthcare Or-ganizations (JCAHO), if a surveyor identifies problems, be ready to provide him or her with any corrective-action plans that you may have developed.
It is beneficial to prove to the JCAHO that you have already identified the issue in question and areworking to address it. The surveyor will review theplan to verify that you, in fact, carried out correctiveactions, and will evaluate how it affects patientsreviewed under tracer methodology.
The surveyor may also be able to provide you withadditional suggestions for achieving compliance, sotake advantage of any advice they provide.
Pretend there’s a confrontationOne way to test employees about corrective plans isto stage a conflict during a mock survey betweenthe person playing the surveyor and staff members.
For example, set up a situation with the surveyor aheadof time in which he or she reaches a conclusion that
employees don’t agree with. In terms of the environ-ment of care, one example could be a conflict overwheeled carts waiting in a corridor.
Observe your staff members’ reactions closely, espe-cially if they try to argue with the surveyor. Generally,you don’t want to see employees ever argue with asurveyor, even when if they think that he or she hasmisinterpreted a JCAHO standard.
A calmer way of actingInstead, train employees to take a more subduedapproach.
If they think the surveyor’s interpretation on carts inthe corridor is beyond what the JCAHO calls for, tellthem to discuss their concerns with the survey teamleader. If the conflict involves the leader, then con-tact the JCAHO’s home office for a discussion.
Editor’s note: We adapted this tip from our publica-tion, The Tracer Methodology Mock Survey TrainingHandbook, published by HCPro, Inc. These hand-books come in packets of 25. For more information,go to www.hcmarketplace.com/Prod.cfm?id=2289.
06/04 SR2604
This special report is published by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. • Copyright 2004 HCPro, Inc.All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro or the Copyright Clearance Center at978/750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments orquestions, call 781/639-1872 or fax 781/639-2982. If you have questions, contact customer service at 800/650-6787, fax800/639-8511, or e-mail customerservice@ hcpro.com • Opinions expressed are not necessarily those of the editors.Mention of products and services does not constitute endorsement. Advice given is general, and readers should consultprofessional counsel for specific legal, ethical, or clinical questions. HCPro, Inc. is not affiliated in any way with theJoint Commission on Accreditation of Healthcare Organizations.