bridging the gap: palliative care and oncology in harmony
TRANSCRIPT

0

Bridging the Gap: Palliative Care and Oncology in Harmony
Grace Cullen Oligario, DNP, FNP-BC, ACHPN
Garrett Fontes, LMSW, OCW
October 10, 2014

VETERANS HEALTH ADMINISTRATION
Disclosure
• We are poor federal employees who have no financial or other conflict of interests related to this presentation to disclose.
• Any mention of off-label use of drugs will be clearly mentioned as such.
2

VETERANS HEALTH ADMINISTRATION
Objectives
• Discuss the evolution of palliative care and palliative care in oncology
• Discuss the benefits of palliative care in cancer care and the challenges in integrating palliative care in oncology
• Present a collaborative project between palliative care and oncology at the John D Dingell VA Medical Center
3

VETERANS HEALTH ADMINISTRATION
HISTORY OF PALLIATIVE CARE
• 1967, Dr. Dame Cicely Saunders creates the first modern hospice in London
• 1974, Florence Wald, Dean of the Yale School of Nursing founded the Connecticut Hospice
• Over the years, there was increasing recognition of the benefits of palliative care and hospice in the care of the terminally ill (Medicare Hospice Benefit, JCAHO hospice accreditation)
• 1991, the VA includes hospice care in the veterans’ benefits package; in 2002, they launched programs to increase access to hospice and palliative care, improve clinician education
National Hospice and Palliative Care Organization, 2014
4

VETERANS HEALTH ADMINISTRATION
HISTORY OF PALLIATIVE CARE
• 2006, The American Board of Medical Specialties recognized hospice and palliative medicine as a medical specialty
• Increasing published data on the benefits of palliative care
National Hospice and Palliative Care Organization, 2014
5

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology (ASCO)
• Founded in 1964 by a small group of physician members of the American Association of Cancer Research
• A separate society dedicated to issues on clinical oncology.
• Journal of Clinical Oncology, official journal.
American Society of Clinical Oncology, 2014
6

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
JOURNAL OF CLINICAL ONCOLOGY
1987-1997
• A search conducted on JCO using key word PC yielded 7 articles, 5 of which were on the palliative use of medications (3 on chemotherapy, 1 on hydromorphone and 1 on hematopoietic colony-stimulating factor)
• The 6th article was published in 1991; it was on a survey conducted among 598 randomly selected oncologists who subscribed to the JCO among 598 randomly selected physicians who subscribed to the JCO; found that coping with issues related to palliative or terminal care is the most important causative factor of burnout
Whippen and Canellos , 1991
7

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
JOURNAL OF CLINICAL ONCOLOGY
• The 7th article was on the challenges of performing an effectiveness research in PC
Rinck GC, Van den Bos AM, et al
8

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
• In 1998, ASCO surveyed its members and learned that 90% of the 3,227 medical, surgical, radiation, and pediatric oncologists who responded learned about palliative care through trial and error; 81% said they had inadequate coaching in discussing poor prognosis; 65% said they received inadequate education about controlling symptoms; 33% reported hearing lectures about palliative care issues during oncology fellowship training.
Ferris FD, Bruera E, et al, 2009
9

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
1998
• Published “Cancer Care During the Last Phase of Life” and the “Consensus Statement of Recommendations for High-Quality Cancer Care Developed by the American Federation of Clinical Oncologic Societies”; called for efforts to overcome the barriers to the integration of palliative care into cancer care, increase knowledge and skills pertaining to PC, and to improve the experience of patients and families receiving cancer care.
• Recognized that optimal EOL care involves access to state of the art PC rendered by PC clinicians and supported by PC experts when necessary.
ASCO, 1998
10

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
2008
• Published “Palliative Cancer Care a Decade Later: Accomplishments, the Need, Next Steps”; identified the current state of PC in cancer care and recommendations to facilitate integration of PC in comprehensive cancer care(4)
Accomplishments:
• Supported the launch of the Education in Palliative and End-of-life Care for Oncology (EPEC-Oncology) Curriculum in collaboration with the National Cancer Institute (NCI)
• Hospice use doubled from 540,000 in 1998 to 1,300,000 in 2006(5)
Ferris FD, Bruera E, et al, 2009
National Hospice & Palliative Care Organization, 2007
11

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
• More PC programs are integrated in cancer care programs
• Incorporation of PC in educational resources and activities
• Inclusion of PC in ASCO’s Annual Meeting and features in JCO
AREAS FOR IMPROVEMENT
• ASCO has not actively pursued steps to increase acceptance that can lead to earlier referral
• Model of care: When the complexity of a patient's suffering exceeds the experience of the primary cancer care team, consultation with palliative cancer care experts may be necessary
12

VETERANS HEALTH ADMINISTRATION
American Society of Clinical Oncology
VISION FOR 2020
• PC as a routine part of comprehensive cancer care, available in all cancer centers
13

VETERANS HEALTH ADMINISTRATION
Institute of Medicine
• Independent, nonprofit organization that provide unbiased and authoritative advice to decision makers and the public; many of their studies begin as specific mandates from Congress, others are requested by federal agencies and independent organizations
• 2001, “Improving Palliative Care for Cancer”; identified barriers of palliative care integration to cancer care: attitudinal, behavioral, economic, educational, legal, focus of research on cure and not palliative care
Institute of Medicine of the National Academies,2001
14

VETERANS HEALTH ADMINISTRATION
Institute of Medicine
Recommendations:
• The National Cancer Institute (NCI) should require research in palliative care and symptom control for recognition as a “Comprehensive Cancer Center”
• Private insurers should provide adequate compensation for end of life care
• Organizations that provide information about cancer treatment (NCI, American Cancer Society, etc.) should include information on palliative care throughout the course of disease on their patient materials
15

VETERANS HEALTH ADMINISTRATION
Institute of Medicine
• Published “Delivering High-Quality Cancer Care: Charting A New Course For A System in Crisis” in 2013
Findings:
• Many patients do not receive adequate information on goals of treatment, palliative care for symptom management and, side effect of treatments; due to lack of knowledge on how to provide the care or does not see PC as an important component of quality cancer care
16

VETERANS HEALTH ADMINISTRATION
Institute of Medicine
• Published “Dying in America” in 2014
• Pushed for advance care planning earlier and during multiple occasions in life based on a 2013 survey that showed 90% of Americans agreed to the benefit of end of life discussions with their families but only <30% have done it, and majority were >65 y/o with 1 or more chronic condition/s).
• American healthcare is poorly equipped to provide end of life care due to: shortage of palliative care experts, reluctance among providers to discuss end of life issues and, inadequate financial and organizational support for the needs of dying patients
• Calls for improved end of life training in medical schools
17

18

VETERANS HEALTH ADMINISTRATION
Barriers to PC Integration in Cancer Care
Views of Palliative Care
• Viewing of Palliative Care as alternative approach and philosophy to cancer care
• Association between palliative care and hospice care
Schenker, Crowley-Matoka, el al, 2014
19

VETERANS HEALTH ADMINISTRATION
Barriers to PC Integration in Cancer Care
Self-Defined Professional Roles
• Palliative Care as an integral role in the care they provide to the patients
• Referral to Palliative Care as neglecting responsibilities and patient abandonment
Schenker, Crowley-Matoka, el al, 2014
20

VETERANS HEALTH ADMINISTRATION
Barriers to PC Integration in Cancer Care
• Oncologists unaware of the availability of services and eligibility for referral to PC
• Limited outpatient PC clinics; 2010 study showed that only 59% of NCI cancer centers had PC outpatient clinics, and 22% for non-NCI centers
• Only 1/3 of PC program leaders identified their professional background as palliative care; board certification was not a requirement for physicians or nurses in a majority of programs
• While inpatient care services are more widely available for NCI cancer centers, only 56% of non-NCI centers reported having an inpatient consultation team.
Schenker, Crowley-Matoka, et al, 2014
Hui, Elsayem, Maxine et al, 2010
21

VETERANS HEALTH ADMINISTRATION
Barriers to PC Integration in Cancer Care
Limited effectiveness research in comprehensive palliative cancer care
• Course of disseminated cancer is diverse
• Physical and cognitive deterioration may hamper the completion of the study
• Quality of life and satisfaction scores are sometimes complicated and difficult to interpret
• Effective symptom management is typically subjective and ay be influenced by personal characteristics
Rinck GC, van den Bos, et al, 1997
22

VETERANS HEALTH ADMINISTRATION
Benefits to PC Integration in Cancer Care
• Patients with advanced cancer who receive palliative care consultations early in the course of their disease report better symptom control, quality of life, lower rates of depression and improved survival rates than those not receiving consultations
• Initiating palliative care upon diagnosis of advanced cancer also improves patients’ understanding of their prognosis
Temel JS, Greer JA, Muzikansky A, et al, 2010
Zimmermann C, Swami N, Rodin G, et al, 2012
Bakitas M, Lyons KD, Hegel MT, et al, 2009
23

VETERANS HEALTH ADMINISTRATION
Benefits to PC Integration in Cancer Care
• Early involvement of palliative care may also lead to lower total spending on inpatient health care by decreasing lengths of stay, admissions to the intensive care unit, and pharmacy and laboratory expenses
Meier DE., 2011
Gade G, Venohr I, et al, 2008
Ciemins EL, Blum L, et al, 2007
24

VETERANS HEALTH ADMINISTRATION
Benefits to PC Integration in Cancer Care
• Early outpatient palliative care decreases the need for acute care services, leading to fewer hospital admissions and emergency department visits.
• Patients receiving Palliative Care services are more likely to forgo costly inpatient care at the end of life than are other patients.
Temel JS, Greer JA, et al, 2010
Brumley R, Enguidanos S, et al, 2007
25

26

VETERANS HEALTH ADMINISTRATION
John D Dingell VA Medical Center
27

VETERANS HEALTH ADMINISTRATION
John D Dingell VA Medical Center
• 217 in-patient beds (acute, nursing home and psychiatry)
• Average age : 60
• Male, 91%, Female 9%
• 31 % of patients below the pension rate ($1054/month for single Veteran)
• 47% of Veterans receive compensation for service related injury/illness. 5% receive non-service related financial benefits.
• 15% of non-compensable Veterans are above the pension rate and have co-pays for medications and/or office visits.
28

VETERANS HEALTH ADMINISTRATION
John D Dingell VA Medical Center
• Service available to more than 330,000 veterans living in Wayne, Oakland, Macomb and St. Clair counties
US Department of Veterans Affairs, 2014
JDDVAMC, 2013
29
VETERANS HEALTH ADMINISTRATION
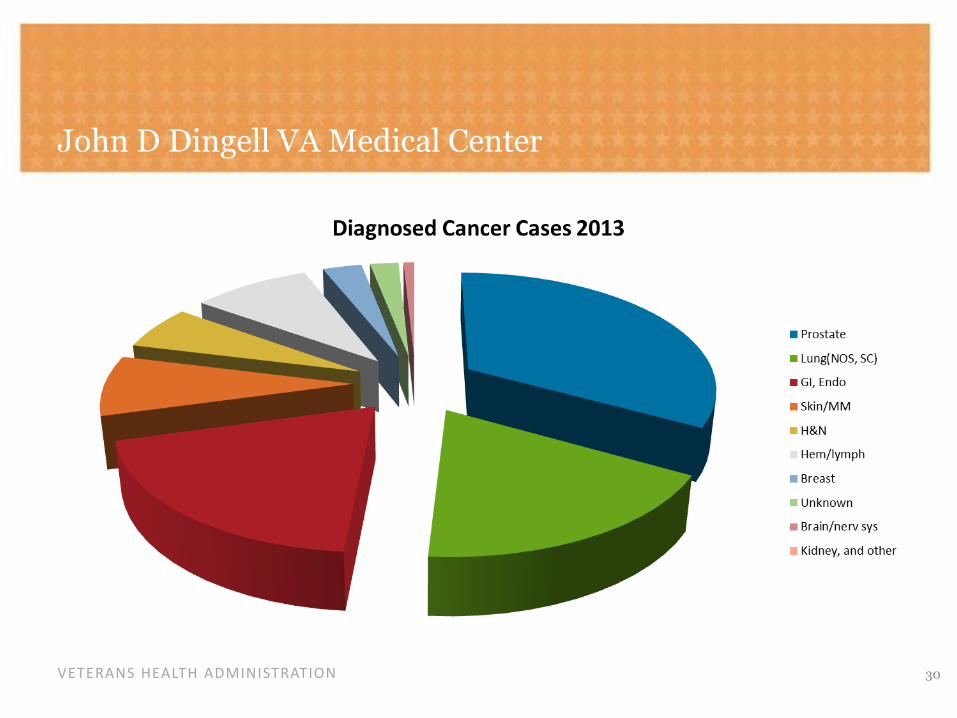
John D Dingell VA Medical Center
30

VETERANS HEALTH ADMINISTRATION
Challenges to Integration
• View of palliative care as a non-scientific discipline
• Belief that oncologists are skilled and knowledgeable in symptom management
• Equating PC with hospice care
31

VETERANS HEALTH ADMINISTRATION
Integrated Services
• Weekly Tumor Board
• Active palliative care representation in the Cancer Committee
• Regular “huddles” with chemotherapy nurses and other oncology staff
• Accessibility in the oncology and chemotherapy clinics
32

33
ABSTRACT
INTRODUCTIONDISCUSSION
METHODS
Authors: G. Oligario, DNP, FNP-BC, ACHPN; G. Fontes, LMSW, OSW-C
Overall Results In 2013, 29% of the referrals came from Acute Care and the rest came from oncology.
Shorter palliative care involvement and hospice length of stay in 2013 may have been
impacted by the advanced state of illness for a large number of the patients that year.
Many of these patients were not qualified for or did not pursued palliative
chemotherapy.
In 2007-09, 56% of the referrals came from acute care and 6% from oncology. This
indicates that oncology has been engaged in the collaborative and has taken ownership
of the referral process.
Average Urgent Care visits were impacted by PC involvement, decreasing from 1.8 days
to 1 day.
In 2013, there were about 3-4 patients who served as outliers wherein palliative care
involvement was not timely, taking over 100 to 200 days; possible causes identified:
New staff oncologist who was not familiar with the collaborative.
Increased work volume for palliative care prevented early capture of this delay as
evidenced by increasing total volume of consults.
Days
Urgent Care Visits
Medians
Median values for 2013 showed a slight increase in timeliness
but still fell within desired goals.
Continue to work with oncology and other services involved in sustaining
the success of this collaboration.
Expansion of efforts to improve the timeliness of PC involvement in other
Stage IV malignancies including esophageal, prostate, pancreatic, and colon cancers.
PALLIATIVE CARE AND ONCOLOGY ADVANCED LUNG CANCER COLLABORATIVE
Days
Days
PC Consults
Identified practice: Patients referred to PC if found not to be eligible for
palliative chemotherapy or they chose not to pursue disease modifying
therapies.
Proposed changes: PC consulted during initial Oncology visit. PC to see
the patient within 3 weeks and follows along with Oncology throughout
the disease trajectory.
Purpose: Improve QOL of patients with Stage IV lung cancer by
improving the timeliness of Palliative Care involvement and
minimizing Urgent Care/ED visits during the course of treatment.
PC involvement has been shown to improve QOL for both the patient
and family by focusing on symptom management, psychosocial
support and identifying goals of care.

VETERANS HEALTH ADMINISTRATION
Overall Results
34
Days

VETERANS HEALTH ADMINISTRATION
Overall Results
35
Median Days Median values for 2013 showed a slight increase in
timeliness but still fell within desired goals.

VETERANS HEALTH ADMINISTRATION 36
Palliative Care Consults

VETERANS HEALTH ADMINISTRATION 37

VETERANS HEALTH ADMINISTRATION
Outcomes/Conclusions
• In 2013, 29% of the referrals came from Acute Care and the rest came from oncology. In 2007-09, 56% of the referrals came from acute care and 6% from oncology. This indicates that oncology has been engaged in the collaborative and has taken ownership of the referral process.
• 93% of the patients referred to Palliative Care had Social Work involvement at time of diagnosis on baseline. Hiring of full time Oncology Social Worker likely impacted the number of referrals from Oncology service.
• Average Urgent Care visits were impacted by PC involvement, decreasing from 1.8 days to 1 day.
38

VETERANS HEALTH ADMINISTRATION
Outcomes/Conclusions
• Shorter palliative care involvement and hospice length of stay in 2013 may have been impacted by the advanced state of illness for a large number of the patients that year. Many of these patients were not qualified for or did not pursue palliative chemotherapy
• Increase in number of consults, nearly 100 more in 2013 as compared to the baseline, may have played a role in the timeliness of palliative care intervention as the size of the palliative care consult team did not change. It also to be noted that there were no palliative care fellows that year
39
VETERANS HEALTH ADMINISTRATION
Outcomes/Conclusions
• In 2013, there were about 3-4 patients who served as outliers wherein palliative care involvement was not timely, taking over 100 to 200 days; possible causes identified:
– New staff oncologist who was not familiar with the collaborative.
– Increased work volume for palliative care prevented early capture of this delay as evidenced by increasing total volume of consults.
40

VETERANS HEALTH ADMINISTRATION
Current Status of the Collaborative
• Continue to work with oncology and other services involved in sustaining the success of this collaboration.
• Expansion of efforts to improve the timeliness of PC involvement in other
Stage IV malignancies including esophageal, prostate, pancreatic, and colon
cancers.
41

VETERANS HEALTH ADMINISTRATION
Secrets to Success?
• Dedicated oncology/palliative care social worker and nurse practitioner, and the ability to be seen as part of the “team”, accessibility and visibility
• Supportive oncology as an initial approach
• Success in managing symptoms, psychosocial issues that reflects in improved patient and family satisfaction, as well as easing the load off of oncology
42

VETERANS HEALTH ADMINISTRATION
Areas for Improvement
Need for Continuing Education
• “Will re-assess PS in 2 weeks” (to see if qualified for chemotherapy)
• Reluctance in discussing poor prognosis
43

44

VETERANS HEALTH ADMINISTRATION
References
1. History of Hospice. National Hospice and Palliative Care Organization. http://www.nhpco.org. Accessed October 3, 2014.
2. Society History. American Society of Clinical Oncology. http://www.asco.org. Accessed October 3, 2014.
3. Whippen DA, Canellos GP. Burnout Syndrome in the Practice of Oncology: Results of a Random Survey of 1,000 Oncologists. J Clinical Oncol. 1991,9(10): 1916-1920.
4. Rinck, GC, van den Bos GAM, Kleijnen J, de Haes HJCJM, Schade E, Veenhof CHN. Methodologic Issues in Effectiveness Research on Palliative Cancer Care: A Systematic Review. J Clin Oncol, 1997. 15(4):1697-1707.
5. Ferris FD, Bruera E, Cherny N, Cummings C, Currow D, Dudgeon D, et al. Palliative Cancer Care a Decade Later: Accomplishments, the Need, Next Steps—From the American Society of Clinical Oncology. J Clin Oncol, published online before print May 18, 2009. doi: 10.1200/JCO.2008.20.1558
45

VETERANS HEALTH ADMINISTRATION
References
6. American Society of Clinical Oncology. Cancer care during the last phase of life. J Clin Oncol, 1998. 16:1986–1996.
7. Federation of Clinical Oncologic Societies. Access to quality cancer care: Consensus statement. J Clin Oncol , 1998.16:1628–1630.
8. National Hospice & Palliative Care Organization (2007) Facts and Figures: Hospice Care in America (National Hospice & Palliative Care Organization, Alexandria, VA) http://www.nhpco.org/i4a/pages/Index.cfm?pageid=3274
9. About the IOM. Institute of Medicine of the National Academies. http://iom.edu. Accessed October 3, 2014.
10. Palliative in Practice. Center to Advance Palliative Care. http://palliativeinpractice.org. Accessed September 23, 2014.
11. KaiserHealth News. www.kaiserhealthnews.org. Accessed September 23, 2014.
46

VETERANS HEALTH ADMINISTRATION
References
12. Schenker Y, Crowley-Matoka M, Dohan D, et al. Oncologist factors that influence referrals to subspecialty palliative care clinics. J Oncol Pract, December 3, 2013.
13. Hui D, Elsayem A, de La Cruz M, Berger A, Zhukovsky DS, Palla S, Evans A, Fadul N, Palmer JL, Bruera E. Availability and Integration of Palliative Care at US Cancer Centers. JAMA. 2010;303(11):1054-1061. doi:10.1001/jama.2010.258.
14. Temel JS, Greer JA, Muzikansky A, et al: Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 363:733-742, 2010.
15. Zimmermann C, Swami N, Rodin G, et al. Cluster-randomized trial of early palliative care for patients with metastatic cancer. Presented at the 2012 American Society for Clinical Oncology Annual Meeting, Chicago. 2012 Jun 1–5; abstract.
47

VETERANS HEALTH ADMINISTRATION
References
16. Bakitas M, Lyons KD, Hegel MT, et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: the Project ENABLE II randomized controlled trial. JAMA. 2009;302:741–749.
17. Meier DE. Increased access to palliative care and hospice services: opportunities to improve value in health care. Milbank Q. 2011;89:343–380.
18. Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11:180–190.
19. Ciemins EL, Blum L, Nunley M, Lasher A, Newman JM. The economic and clinical impact of an inpatient palliative care consultation service: a multifaceted approach. J Palliat Med. 2007;10:1347–1355.
20. Brumley R, Enguidanos S, Jamison P, et al. Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care. J Am Geriatr Soc. 2007;55:993–1000.
48

VETERANS HEALTH ADMINISTRATION
References
21. John D Dingell VA Medical Center, Detroit, Michigan. U.S. Department of Veterans Affairs. http://www.detroit.va.gov. Accessed October 6, 2014.
22. Detroit VA Medical Center Fiscal Year 2013 Organizational Data Profile. http://vaww.detroit.med.va.gov. Accessed October 6, 2014.
49