brain tumor headaches from bedside to bench
TRANSCRIPT

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 1/8
Philippe Goffaux, PhDDepartment of Neurosurgery and
Neuro-oncology,
Université de Sherbrooke,
Faculty of Medicine,
Sherbrooke, Québec, Canada
David Fortin, MD
Department of Neurosurgery and
Neuro-oncology,
Université de Sherbrooke,
Faculty of Medicine,
Sherbrooke, Québec, Canada
Reprint requests:
Philippe Goffaux, PhD,Department of Neurosurgery and
Neuro-oncology,
Faculty of Medicine,
Université de Sherbrooke,
3001 12th Avenue North,
Sherbrooke, Québec, Canada J1H 5N4.
E-mail: Philippe.Goffaux@
USherbrooke.ca
Received, May 24, 2009.
Accepted, January 11, 2010.
Copyright © 2010 by the
Congress of Neurological Surgeons
Prevalence estimates indicate that 35% to90% of us will experience headaches at leastonce in our lives.1 It is clear, therefore, that
headaches are extremely prevalent. The most com-mon type of headache is tension type headache(69%-88%) followed by migraine (6%-25%) andcluster headaches (0.006%-0.24%).1,2 In somecases, headaches do not readily fit into the classi-fication categories established by the InternationalHeadache Society. These headaches are often sim-ilar to primary headaches but have atypical fea-tures or an atypical course and are thus referred toas atypical headaches. Prevalence estimates for
atypical headaches are scarce; however, a relatively recent study conducted to test the utility of mag-netic resonance imaging (MRI) in the evaluationof chronic headache revealed that 15.9% of referredcases were atypical, whereas 40% of cases weremigraine-like and 17.6% were tension-typeheadaches.3 Although interesting, this estimatemust be considered cautiously because atypicalcases are more likely to be considered for neu-roimaging and are thus more likely to represent a
biased prevalence estimate. Nevertheless, it is impor-tant to properly investigate atypical headachesbecause major abnormalities were found after MRIin 14.1% of cases, as opposed to 0.6% for migraineand 1.4% for tension-type headaches.3
Although headaches are rarely the result of a brain tumor, brain tumors are frequently associ-ated with headaches. In fact, studies on this issueindicate that approximately 50% of patients reportheadache pain; estimates range between 33% and71%.4-10 Headaches, however, are rarely the solepresenting symptom of intracranial mass lesions,occurring as such in only 10% of cases.8,10,11
More frequently, brain tumor headaches are ac-companied by nausea, emesis, papilledema, blurredvision (in the context of intracranial hyperten-sion), personality changes, seizures, and/or otherfocal neurological signs.12,13 A change in preex-isting headache pain can also be indicative of a mass lesion.4,7 These comorbid symptoms areconsidered “red flags” and call for further diag-nostic efforts, lest the presence of a lesion bemissed (see Table 1 for a list of red flags).
REVIEW
NEUROSURGERY VOLUME 67 | NUMBER 2 | AUGUST 2010 | 459
Brain Tumor Headaches: From Bedside to Bench
ALTHOUGH MOST PEOPLE who have headache pain do not present with an underlyingmass lesion, a large number of patients with brain tumors do report headache (as many as60% in our institution). The problem for clinicians is that the tumor-headache associationis not universal, as evidenced by anecdotal reports of patients with large tumors and increasedintracranial pressure, but a complete absence of headache pain. In this review, we exam-ine more than 80 years of research on brain tumor headaches, delineating the link betweentumor location, laterality, growth rate, and pain. Most importantly, we position our reviewwithin the context of current etiological theories and propose new models involving theperipheral and central sensitization of nociresponsive neurons. This review will help clini-cians understand why debulking surgery sometimes fails to alleviate neoplastic headachepain in select patients. A brief examination of headaches as a result of surgery and adju-vant chemoradiation therapy is also provided. Headaches can be an early indicator of cen-
tral nervous system tumors. However, headaches are present in a wide variety of othercondition, and are sometimes (surprisingly) absent in patients with primary neoplasms ormetastatic tumors. This observation complicates the possibility of linking headaches tobrain tumors. Nevertheless, some generalizations concerning brain tumor headaches canbe drawn. The following sections review these generalizations, presenting caveats where appropriate. Lingering questions in the field are also addressed and presented togetherwith promising future research avenues.
KEY WORDS: Brain tumor headache, Diagnostic utility, Intracranial neoplasm, Pathogenesis, Traction hypothesis
Neurosurgery 67:459-466, 2010 DOI: 10.1227/01.NEU.0000372092.96124.E6 www.neurosurgery-online.com
7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 2/8
In addition to the utility of accompanying clinical red flags,headaches, in and of themselves, can be of some diagnostic value.For example, most brain tumor headaches are described as dull,aching pain. They are rarely described as throbbing or pulsat-ing 4,5,7-9 (but see Pfund et al6 for an exception). The general con-sensus seems to be that brain tumor headaches mimic tension-typeheadaches more so than any other.4,13 Sometimes, however, braintumor headaches are similar to migraine-like headaches (in approx-
imately 10% of cases4,6). Unfortunately, these observations indi-cate that the type of pain felt cannot definitively point to the cor-rect diagnosis. Nevertheless, drawing parallels between brain tumorheadaches and idiopathic or primary headaches (eg, tension typeor migraine; see description and comparison in Table 2) can beuseful, especially given the sometimes complex mechanisms under-
lying the development of brain tumor headaches.
LOCALIZATION OF HEADACHE PAIN:DOES IT ECHO TUMOR LOCATION?
Historically, it was thought that the topographic distributionof headaches could have some predictive value in determining thelocation of underlying mass lesions. The advent of structural imag-ing, however, has largely rendered this objective obsolete. All thesame, more than 80 years of research on this issue have providedvaluable data. For example, we now know that certain tumor loca-tions are more likely to be associated with specific headache loca-tions, especially when headaches are assessed early in the diseaseprocess, before their generalization. In this manner, infratentorialor posterior fossa lesions are more frequently associated with occip-ital than frontal or temporal headaches.8,14 Infratentorial tumorscan also be accompanied by nuchal pain and cervical musclespasms.6,14 Supratentorial tumors, on the other hand, are morefrequently associated with vertex and frontal pain.4,9,14 Unfortunately,frontal pain has poor localizing value because it can be producedby tumors that are far removed from frontal areas.5 In addition,
460 | VOLUME 67 | NUMBER 2 | AUGUST 2010 www.neurosurgery-online.com
GOFFAUX AND FORTIN
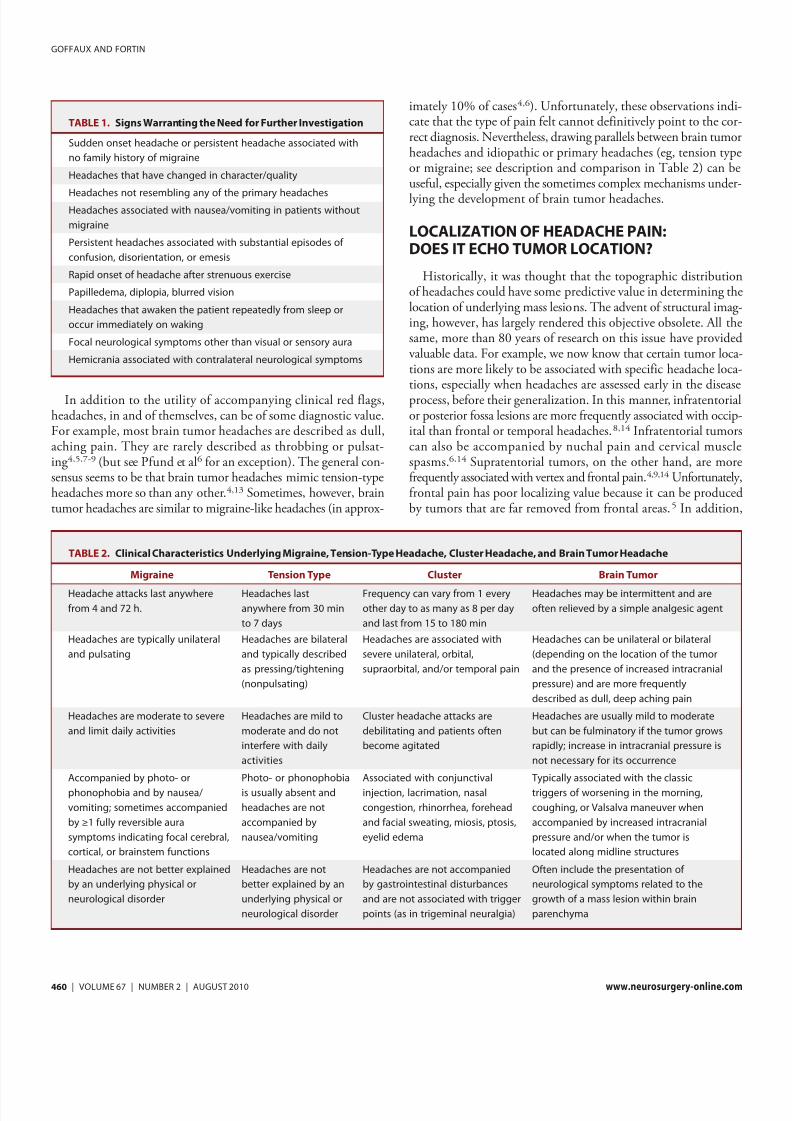
TABLE 1. Signs Warranting the Need for Further Investigation
Sudden onset headache or persistent headache associated with
no family history of migraine
Headaches that have changed in character/quality
Headaches not resembling any of the primary headachesHeadaches associated with nausea/vomiting in patients without
migraine
Persistent headaches associated with substantial episodes of
confusion, disorientation, or emesis
Rapid onset of headache after strenuous exercise
Papilledema, diplopia, blurred vision
Headaches that awaken the patient repeatedly from sleep or
occur immediately on waking
Focal neurological symptoms other than visual or sensory aura
Hemicrania associated with contralateral neurological symptoms
TABLE 2. Clinical Characteristics Underlying Migraine, Tension-Type Headache, Cluster Headache, and Brain Tumor Headache
Migraine Tension Type Cluster Brain Tumor
Headache attacks last anywhere
from 4 and 72 h.
Headaches last
anywhere from 30 min
to 7 days
Frequency can vary from 1 every
other day to as many as 8 per day
and last from 15 to 180 min
Headaches may be intermittent and are
often relieved by a simple analgesic agent
Headaches are typically unilateral
and pulsating
Headaches are bilateral
and typically described
as pressing/tightening
(nonpulsating)
Headaches are associated with
severe unilateral, orbital,
supraorbital, and/or temporal pain
Headaches can be unilateral or bilateral
(depending on the location of the tumor
and the presence of increased intracranial
pressure) and are more frequently
described as dull, deep aching pain
Headaches are moderate to severe
and limit daily activities
Headaches are mild to
moderate and do not
interfere with daily
activities
Cluster headache attacks are
debilitating and patients often
become agitated
Headaches are usually mild to moderate
but can be fulminatory if the tumor grows
rapidly; increase in intracranial pressure is
not necessary for its occurrence
Accompanied by photo- or
phonophobia and by nausea/
vomiting; sometimes accompanied
by ≥1 fully reversible aura
symptoms indicating focal cerebral,
cortical, or brainstem functions
Photo- or phonophobia
is usually absent and
headaches are not
accompanied by
nausea/vomiting
Associated with conjunctival
injection, lacrimation, nasal
congestion, rhinorrhea, forehead
and facial sweating, miosis, ptosis,
eyelid edema
Typically associated with the classic
triggers of worsening in the morning,
coughing, or Valsalva maneuver when
accompanied by increased intracranial
pressure and/or when the tumor is
located along midline structures
Headaches are not better explained
by an underlying physical or
neurological disorder
Headaches are not
better explained by an
underlying physical or
neurological disorder
Headaches are not accompanied
by gastrointestinal disturbances
and are not associated with trigger
points (as in trigeminal neuralgia)
Often include the presentation of
neurological symptoms related to the
growth of a mass lesion within brain
parenchyma

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 3/8
published prevalence estimates pairing supratentorial tumors withfrontal headaches indicate that this association happens in less than50% of cases,4,9 a statistic that is insufficiently convincing to beof diagnostic utility.
Despite the limited utility of localization attempts, correspon-dence between headache topography and tumor location is much
greater when the objective is merely to identify the laterality of lesions. Headaches, it seems, occur more frequently on the ipsi-lateral side of unilateral tumor(s), particularly in the absence of increased intracranial pressure. In the absence of high intracranialpressure, Suwanwela et al9 found that headaches correctly pre-dict the lateralization of supratentorial lesions in 100% of cases.This is probably attributable to the absence of extensive braindisplacement and ventricular obstruction,14 both of which tendto produce distal (far removed from the source responsible forcausing increased pressure) rather than proximal (close to thetumor) traction on pain-sensitive structures (eg, veins and meningealarteries). In the absence of distal traction, headaches occur region-ally and are thus more predictive of tumor location. For similarreasons, dural tumors produce headaches that develop in closeproximity to the tumor site.4 When intracranial pressure is high,however, headache pain has very limited localizing/lateralizing value, mostly because the distal traction produced by increasedpressure activates pain-sensitive structures in widespread areas.These findings point to the importance of paying attention tothe pathogenesis of brain tumor headaches. The next sectiondeals specifically with this issue.
PATHOGENESIS OF BRAIN TUMOR HEADACHES
Traction Hypothesis
The most frequently cited cause of brain tumor headache is thepresence of traction on intra- and extracranial pain-sensitive struc-tures. In brain cancer, traction results from the expansion of tumoraltissue, edema, and/or hemorrhage.5 Intra- and extracranial pain-sensitive structures potentially include venous sinuses, dural and cere-bral arteries, dura, skin, subcutaneous and muscle tissue, and theperiosteum of the cranium. Brain parenchyma, however, is insen-sitive to pain because it lacks the presence of pain receptors (ie,free nerve endings). A number of tumor-associated features tend tovalidate the traction hypothesis of brain tumor headaches. Forexample, tumor-associated peritumoral edema, papilledema, andsupratentorial midline shifts (eg, shifts of the pineal body, thirdventricle, or interpeduncular cistern) are all key markers of increased
intracranial pressure and can all be linked with the presence of dif-fuse, poorly localized headaches.4,6 Only pressure-induced trac-tion can explain these associated findings.
It is important to point out that increased intracranial pres-sure can lead to headaches that are often described by patientsas transitory but intense. One possible explanation for the devel-opment of such acute pain is a periodic obstruction of the ven-tricular system (eg, ball valving of a mass within the ventricularsystem or intermittent compression of a mass [often peduncu-lated] on the system). A change in posture, exertion, coughing,
or the Valsalva maneuver can all lead to such periodic obstruction. Acute-onset headaches can also occur as a result of abnormalpressure waves or “plateau” waves. These waves, originally describedby Lundberg,15 occur after the onset of a space-occupying eventand/or increase in intracranial pressure and are caused by a vasodila-tory cascade consisting of (1) an increase in blood volume as a
result of vasodilation, (2) a decrease in cerebral perfusion pressure,and (3) a sharp elevation in intracranial pressure.16 The normalautoregulatory response that would otherwise vasoconstrict islost (or at least delayed) during plateau waves.17 Pressure wavescan last anywhere from 5 to 30 minutes, which coincides withthe rapid-onset, short-duration headache described by patients who have documented plateau waves. Headaches associated witha mass lesion are often worse in the morning because brain edema increases overnight from the effects of gravity in the supine posi-tion (because of a lack of gravity-assisted drainage of the venoussystem) and because sleep normally increases arterial PCO2 (highPCO2 levels cause vasodilation, which, together with the effectsof disease, increases intracranial pressure). When associated withprojectile vomiting and an abrupt worsening of the mental state,such headaches are always a cause for concern. Although a masslesion is not necessary for the appearance of such symptoms, fur-ther investigation is a good idea because a number of other neu-rological conditions can also present evidence of intracranialhypertension (eg, brain injury, hydrocephalus, subarachnoidhemorrhage).
The growth rate of space-occupying lesions also plays an impor-tant role in predicting the occurrence of traction and headachepain.5,6,13 Tumors that increase rapidly in size can cause sharp,intense pain because the intracranial space does not have a chanceto adapt to the increased pressure. As described previously, this is
thought to result from the sudden irritation of pain-sensitive struc-tures. Slow-growing tumors, on the other hand, produce headachesthat are transitory and occur only later in the course of disease,principally because protracted mechanical adaptation to the expand-ing tumor is possible.
Despite the value of intracranial pressure in forecasting braintumor headaches, an important limitation must be addressed.Markers of intracranial pressure (eg, papilledema, ventricularshifts, compression) do not systematically predict headache painin patients with brain tumors. This may result from the lack of specificity provided by such markers. In other words, papilledema or ventricular shifts may be good markers of increased intracra-nial pressure, but they are not specifically tied to the appearance
of headaches. Obtaining more direct measures of brain, blood, orcerebrospinal fluid (CSF) parameters may help to establish a closer link between intracranial pressure and distal traction onpain-sensitive structures. Along these lines, Loghin and Levin13
recently argued that we should turn our attention to the measure-ment of CSF dynamics because changes here may be importantin helping to predict when increased intracranial pressure is asso-ciated with brain tumor headaches. Interestingly, neurosurgeonshave known for quite a while (since the 1940s) that a progres-sive distention of the lateral ventricle with a balloon during sur-
NEUROSURGERY VOLUME 67 | NUMBER 2 | AUGUST 2010 | 461
BRAIN TUMOR HEADACHES

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 4/8
gery provokes homolateral headache pain. This is thought to
occur because of an ensuing irritation of adjacent pain-sensitivestructures/vessels.18 In the same manner, saline solution injec-tions into the ventriculosubarachnoid system stretches arterio-vascular networks, activating nociceptive afferents, which canprovoke pain along venous and arterial branches19 (see Figurefor a depiction of tumor growth effects on trigeminovascular freenerve endings).
Unfortunately, researchers have not capitalized on these orig-inal findings, and so there is currently a remarkable lack of data describing the role played by CSF circulatory dynamics in braintumor headaches. To address this limitation, future studies shouldobtain explicit measures of CSF pressure and flow and avoidextrapolation based on the presence or absence of surrogate mark-
ers such as papilledema and ventricular compression/displacement.Measuring CSF pressure, however, is a complicated and invasiveendeavor, often involving lumbar punctures or the use of intra-ventricular catheters. Moreover, in the presence of mass effects,lumbar punctures are ill-advised, given the risk of tonsilar herni-ation. A much safer option is to use noninvasive techniques tomeasure CSF flow through the cerebral aqueduct, foramen of Monro, or the prepontine cistern. This can be achieved using MRI with phase contrast.20-22 Using this technology, McGirtet al20 found that occipital headaches were strongly associated
with hindbrain CSF flow abnormalities, even in the absence of visible compression on MRI. Measuring CSF flow, therefore,may help to detect subtle pathological changes (eg, arachnoidscarring and minor occlusions of the ventricular system) missedby conventional MRI. CSF obstruction may also explain why some patients continue to report headaches even after successful
surgical debulking (ie, approximately 15% of patients with pre-treatment headaches report persistent posttreatment headaches6).Despite the possibility that such patients present with idiopathicrather than symptomatic headaches, the prospect of continuedCSF flow obstruction remains. Future research in this field isneeded to illuminate this possibility.
A final clinical feature that tends to validate the traction hypoth-esis is tumor location. Although tumor location does not alwayspredict where headaches will occur, it adequately predicts whetherheadaches will occur. Tumors that typically provoke headachesinclude intraventricular, midline, and posterior fossa lesions.5,6,9
Here again, CSF flow obstruction, followed by internal hydro-cephalus and local or distal traction, is the most likely explanation.
Cranial or Cervical Nerve Compression
Although direct compression of cranial (eg, trigeminal) and cer-vical (C1 and C2) nerve roots is a possible cause of brain tumorheadaches, a large number of neuro-oncology patients present noevidence of nerve compression or entrapment despite reporting headache pain. Nerve compression, in fact, is very rarely cited as a cause of brain tumor headache.10 Even in patients with Chiari Imalformations, nerve compression resulting from the downwarddisplacement of posterior fossa structures into the foramen mag-num does not always cause headaches.20 Furthermore, the paindescribed by patients with brain tumor headaches is very different
from the intense, paroxystic pain felt when sensory afferents arestretched or compressed, as in the case of trigeminal neuralgia.5
When cervical nerve compression does occur, the associatedheadache may be accompanied by muscle tenderness and the pres-ence of myofascial trigger points. In this situation, headaches would probably be aggravated by neck movements and externalpressure over the upper cervical or occipital region on the symp-tomatic side.
In cases in which the tumor is located near the cervicomedullary junction, entrapment of the occipital nerve or extensive intra-medullary or C1 level hemorrhaging can cause symptoms thatmimic occipital neuralgia (a condition characterized by chronicpain in the upper neck, back of the head, and behind the eyes23).
Pain localized in the back of the head and up to or behind theeye, therefore, suggests a posterior fossa localization and indi-cates a possible, albeit rarely occurring, compression of the greateroccipital nerve.24 More frequently, infratentorial lesions pro-duce pain that can be referred to one or more regions of the heador face. Because this type of presentation is also true of cervico-genic headaches, it is important to consider the set of charac-teristics that generally indicate the presence of cervicogenic, asopposed to neoplastic, headaches. Symptoms more closely tiedto cervicogenic headaches include (1) pain that begins in the
462 | VOLUME 67 | NUMBER 2 | AUGUST 2010 www.neurosurgery-online.com
GOFFAUX AND FORTIN
FIGURE. Innervations of dura and blood vessels by branches of the trigeminal nerve terminate within the trigeminocervical complex extending from the brainstem to the dorsal horns of C1 and C2. According to the traction hypoth-esis, expanding tumor tissue and peritumoral edema produce a progressive irri-tation of intracranial pain-sensitive structures. Depending on the presence or absence of increased intracranial pressure, traction effects can be either far removed or located close to the presenting lesion, resulting in headaches that are, respectively, described as diffuse or well circumscribed in nature.

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 5/8
occipital region and then progressively spreads upward into thehead, (2) pain that can be made worse (or actually initiated) by head or neck movements, and (3) the presence of marked ten-derness in the suboccipital region.
Peripheral Sensitization
In cases in which intracranial pressure produces a prolongedirritation of pain-sensitive structures, afferent branches innervat-ing cerebral, venous, and pial vessels (afferent branches innervat-ing cerebral, venous, and pial vessels primarily appear from theplexus of unmyelinated fibers that arise from the ophthalmic divi-sion of the trigeminal nerve and from upper cervical dorsal roots)may eventually release proinflammatory neuropeptides at the siteof inflammation, further enhancing vascular edema and the con-sequent infiltration of immune cells. This focal antidromic reactionis known as neurogenic inflammation, a phenomenon that pre-dominantly involves the release of substance P and calcitonin gene-related peptide and is thought to underlie some forms of refractory
headache pain.25
Substance P and calcitonin gene-related peptidefacilitate plasma protein extravasation, vascular permeability, andmast cell degranulation, each of which contributes to the periph-eral sensitization of nociceptive fibers.26 If prolonged, neurogenicinflammation can lead to structural changes in the dura mater that will maintain headache pain well beyond the resorption of intracra-nial pressure.27 Although neurogenic inflammation plays a key role in the development of idiopathic headache,26,28 it is not yet clear what percentage of intractable headache pain in brain tumor patientsis attributable to this prolonged inflammatory response. Addressing this question is particularly relevant because brain tumors nor-mally release proinflammatory agents,29 adding to the chemicalsoup already present as a result of mechanical irritation.
Central Sensitization and Impaired Brainstem Inhibition
Over the past few decades, the basic neuroscience of brain tumorheadache has focused on the irritation of pain-sensitive pericranialstructures. More recently, however, the central sensitization of sec-ond-order trigeminovascular neurons and the impaired responseof mesencephalic modulatory neurons have been studied in greaterdetail and are now considered key players in the development andmaintenance of prolonged headache pain.25,30,31 Thus, in predis-posed individuals, prolonged irritation from pericranial structurescan lead to the sensitization of trigeminal convergent neurons. Thisinduces (1) a reduction in the activation threshold of nociceptors,
(2) an increased response to afferent stimulation, and (3) an enlarge-ment of peripheral receptive fields. These mechanisms are consis-tent with the development of prolonged, refractory headache painin patients presenting with primary supratentorial lesions and offeran explanation for why surgical debulking does not systematically abolish all pain in all patients.
Sensory afferents originating from the meninges and cranial ves-sels terminate within the medullary dorsal horn of the caudaltrigeminal nucleus, whereupon they synapse onto convergent neu-rons.32-34 Prolonged stimulation from primary afferents provokes
local hypersensitivity to painful drives. Local segmental hypersen-sitivity is considered a hallmark of central sensitization and has,historically, been very difficult to control. This underscores theimportance of quickly addressing initial symptoms of pain. It isimportant to point out, however, that increased excitability to con-verging synaptic inputs may additionally result from a decrease in
local segmental inhibition. It is now well established that nocicep-tive drives entering spinal and trigeminocervical neurons are sub- ject to modulation by descending inhibitory efferents arising frombrainstem nuclei, including the periaqueductal gray, the locuscoeruleus, and the nucleus raphe magnus.35,36 Under normal con-ditions, endogenous inhibitory responses produce profound anti-nociception even on trigeminovascular inputs.37 Interestingly,dysfunctional pain-modulating circuits in the brainstem haverecently been found in patients with migraine38 and tension-type39
headaches, suggesting a pathogenic contribution of inhibitory sys-tems in headache pain. The possibility of deficient brainstem inhi-bition and/or segmental hypersensitivity resulting from prolongedpericranial irritation as a cause of refractory headache pain in neuro-oncology patients remains to be tested. Doing so could explain why remission of neoplastic headache pain occurs in some patientsand not in others.
VEILING HEADACHE PAIN BECAUSE OFTUMOR-INDUCED SENSORIAL DEFECTS
Although the growth of a mass lesion can produce fulminatory headache pain, it can also lead to significant sensorial defects, thusinterfering with the proper processing of pain intensity and/orunpleasantness. This possibility was originally raised by Kunkleet al, 5 who noticed that some of their neuro-oncology patients
displayed apathy, especially when the tumor was located near thefrontocallosal region. This affliction can lead to gross deficits inthe proper processing and articulation of pain. Logically, whenpatients are apathetic, headache pain will be underreported, pos-sibly biasing overall prevalence estimates.
Despite the importance of paying attention to the possibility of tumor-induced sensorial deficits, very little research has been car-ried out on this issue. One exception is the work by Greenspanet al,40,41 who showed that neoplastic lesions involving the pari-etal operculum, either alone or with the adjacent posterior insula,lead to elevated heat and pinprick pain thresholds. Interestingly,the authors also found that cold-pain tolerance was greater on thehand contralateral to the lesion, especially when the tumor involved
a large part of the insula. Because cold-pain tolerance involves moreaffective/motivational aspects of pain than threshold tests, thisconfirms recent suggestions that propose that the insula is involvedin both affective and sensory/discriminative processes.42 Finally,it is important to point out that lesions that spared the parietaloperculum were associated with normal threshold values. Thesefindings suggest that the functional integrity of nociresponsiveneurons located within the parietal operculum are essential to theproper processing of painful signals and may alter the perceptionof headache pain when compromised by a nearby lesion.
NEUROSURGERY VOLUME 67 | NUMBER 2 | AUGUST 2010 | 463
BRAIN TUMOR HEADACHES

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 6/8
DISTINGUISHING SURGICAL FROM BRAINTUMOR HEADACHES
In most instances, patients with primary or metastatic braintumors will require some form of surgical intervention. Thismeans that surgery-induced pain (ie, cranial or headache pain)
is a likely prospect. Important to clinicians is the fact that neu-rosurgery-induced headaches display a different set of charac-teristics and a more predictable evolution than tumor-inducedheadaches. For example, surgical pain is somatic in nature andusually remains confined to the affected dermatome.43This is notthe case of brain tumor headaches. Furthermore, surgical headachesare defined as pulsating or pounding, much like migraineheadaches but unlike brain tumor headaches.44 Finally, post-craniotomy headaches appear within the first 48 hours of surgery and rapidly wane thereafter. Such fleeting pain is not a commonpresentation for brain tumor headaches.
Interestingly, patients who have neoplastic headaches com-monly report an alleviation of their symptoms after surgery. Thisimprovement strongly suggests that patients must have had a vari-ant of hypertension headache and indicates that debulking sur-gery must have decreased the ill effects of prolonged traction onpain-sensitive structures. It appears, therefore, that alleviating intracranial hypertension by any means, including surgery, willhelp to reduce the tension-type pain that develops concomitantly with increased pressure. Unfortunately, the clinical price to bepaid for neurosurgery is the possible appearance of temporary postcraniotomy pain. Despite this possibility, such pain-for-painsubstitutions are warranted because postoperative pain is muchless severe than hypertensive headache pain, not to mention clin-ically defensible.
Although postcraniotomy pain is common, it is not ubiquitousand appears to be closely tied to the surgical approach chosen andto the cranial region involved. For example, cranial base surgeriessuch as suboccipital or subtemporal craniotomies are particularly prone to the development of severe postoperative pain.45 Standardpterional craniotomies must also be included in the group of usualsuspects because they often provoke intense postsurgical pain. Inview of the fact that cranial base and pterional surgeries produce sig-nificant pain, one can presume that pain-sensitive structures arecompromised during these interventions. This is consistent withanatomic data and our own clinical experience showing that softtissue, dura mater, and pericranial muscles found near the cranialbase (all proven pain-sensitive structures) are massively violated
during suboccipital, subtemporal, and pterional craniotomies. Infurther support of this explanation, Rocha-Filho et al46 confirmedthat postcraniotomy patients with headache pain have greater mas-ticatory muscle tenderness and greater joint limitations than patients without headaches, thus highlighting the importance of preserving muscle integrity if postcraniotomy pain is to be avoided.
Finally, it is important to note that, compared with other typesof surgery, craniotomies are usually considered less painful. Thismay explain why postoperative pain is not regarded as a clinicalpriority in the neurosurgical context.47 We must also remember
that there is a constant need for the neurosurgery staff to pre-serve and assess the wakefulness of patients. Thus, aggressive anal-gesic treatments, along with their accompanying side effects, may be ill-advised. Nevertheless, it is estimated that at least 60% of patients report postcraniotomy pain.47 Furthermore, pain is ratedas an important quality of life concern for neuro-oncology patients,
as evidenced by recent studies on patient well-being.48-52Togetherthese findings advocate for expending greater efforts in the bat-tle against postcraniotomy pain. Interestingly, a study conductedby Stoneham and Walters53 revealed that opiophobia among neu-roanesthetists constitutes a continuing barrier to the ultimateresolution of postoperative pain. The authors found that even if 97% of consultant members of the Neuroanesthesia Society of Great Britain used intramuscular codeine for postoperative anal-gesia and even if most members thought it provided inadequateanalgesia, only 3% of those surveyed would ever consider using stronger opioids during the postoperative period. The remain-ing 97% would not consider stronger opioids because of prevail-ing fears regarding cardiorespiratory depression and alteredconsciousness (ie, traditional prejudices against the use of opi-oids). Clearly, more work is needed to address these (nevertheless)legitimate fears, while also encouraging the proper control of postoperative pain.
ADJUVANT THERAPIES AS AGENTS OF PAIN
After surgical resection of a mass lesion, adjuvant chemother-apy and/or ionizing radiotherapy are often necessary. These addi-tional treatments do not systematically cause pain in neuro-oncology patients, but have been known to do so in a small percentage of cases. For example, acute radiotherapy-induced encephalopathy
can occur within 2 weeks of radiation treatment onset and cancause headache pain because of white matter edema (secondary todiffuse myelin sheath damage) and an ensuing increase in intracra-nial pressure.54,55 Treatment with corticosteroid therapy is recom-mended to alleviate this type of headache pain. Clinicians, however,must be careful to properly wean patients off corticosteroid ther-apy because an abrupt cessation can cause corticosteroid with-drawal syndrome, making it difficult to differentiate disease effectsfrom the consequences of hormonal rebound.
Chemotherapeutic agents can also cause temporary headachesin neuro-oncology patients. For example, temozolomide, one of the most commonly used drugs to treat malignant gliomas, cancause headaches in as many as 25% of patients.56 Plotkin and
Wen57 report that thalidomide, methotrexate, cisplatin, etoposide,imatinib, and hydroxyurea may also cause headaches. Unfortunately,the underlying neurobiology of chemotherapy-induced headachepain is still poorly understood. One possible explanation is thatchemotherapeutic agents produce oxidative stress, alter cytokineregulation, and/or induce deficits in neuronal repair, all of whichcan lead to decreased central nervous system function, inflamma-tion, and increased pain.58This hypothesis is also consistent witha growing amount of research showing that the chemotherapy agents most closely associated with inflammatory cytokine release
464 | VOLUME 67 | NUMBER 2 | AUGUST 2010 www.neurosurgery-online.com
GOFFAUX AND FORTIN

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 7/8
11. Boiardi A, Salmaggi A, Eoli M, Lamperti E, Silvani A. Headache in brain tumours:
a symptom to reappraise critically. Neurol Sci . 2004;25(suppl 3):S143-S147.12. Christiaans MH, Kelder JC, Arnoldus EP, Tijssen CC. Prediction of intracranial
metastases in cancer patients with headache. Cancer . 2002;94(7):2063-2068.13. Loghin M, Levin VA. Headache related to brain tumors.Curr Treat Options Neurol .
2006;8(1):21-32.14. Dalessio DJ. Mechanisms of headache. Med Clin N Am. 1978;62(3):429-442.
15. Lundberg N. Continuous recording and control of ventricular fluid pressure in neu-rosurgical practice. Acta Psychiatr Scand Suppl . 1960;36(149):1-193.
16. Rosner MJ, Becker DP. Origin and evolution of plateau waves. Experimental obser-vations and a theoretical model. J Neurosurg . 1984;60(2):312-324.
17. Castellani G, Zweifel C, Kim DJ, et al. Plateau waves in head injured patients requir-ing neurocritical care. Neurocrit Care . 2009;11(2):143-150.
18. Ray BS, Wolff HG. Experimental studies on headache; pain-sensitive structures of the head and their significance in headache. Arch Surg . 1940;41:813-856.
19. Fay T. A new test for the diagnosis of certain headaches: the cephalalgiogram. Dis Nerv Syst . 1940;1:312-315.
20. McGirt MJ, Nimjee SM, Floyd J, Bulsara KR, George TM. Correlation of cere-brospinal fluid flow dynamics and headache in Chiari I malformation. Neurosurgery .2005;56(4):716-721.
21. McGirt MJ, Nimjee SM, Fuchs HE, George TM. Relationship of cine phase-con-
trast magnetic resonance imaging with outcome after decompression for Chiari Imalformations. Neurosurgery . 2006;59(1):140-146.
22. Stoquart-Elsankari S, Baledent O, Gondry-Jouet C, Makki M, Godefroy O, MeyerME. Aging effects on cerebral blood and cerebrospinal fluid flows. J Cereb Blood Flow Metab. 2007;27(9):1563-1572.
23. Hashiguchi A, Mimata C, Ichimura H, Kuratsu J. Occipital neuralgia as a present-ing symptom of cervicomedullary dural arteriovenous fistula. Headache . 2007;47(7):1095-1097.
24. Garza I. Craniocervical junction schwannoma mimicking occipital neuralgia.
Headache . 2007;47(8):1204-1205.25. Welch KM. Contemporary concepts of migraine pathogenesis.Neurology . 2003;61(8
suppl 4):S2-S8.26. Goadsby PJ. Migraine: a disorder involving trigeminal brainstem mechanisms. In:
Basbaum A, Bushnell MC, eds. Science of Pain. Oxford, UK: Elsevier; 2009:461-468.27. Bendtsen L. Central sensitization in tension-type headache-possible pathophysio-
logical mechanisms. Cephalalgia . 2000;20(5):486-508.28. Buzzi MG, Bonamini M, Moskowitz MA. Neurogenic model of migraine. Cephalalgia .
1995;15(4):277-280.
29. Nitta T, Ebato M, Sato K, Okumura K. Expression of tumour necrosis factor-alpha,-beta and interferon-gamma genes within human neuroglial tumour cells and brainspecimens. Cytokine . 1994;6(2):171-180.
30. Bartsch T, Goadsby PJ. Increased responses in trigeminocervical nociceptive neuronsto cervical input after stimulation of the dura mater. Brain. 2003;126(Pt 8):1801-1813.
31. Bartsch T, Goadsby PJ. The trigeminocervical complex and migraine: current con-
cepts and synthesis. Curr Pain Headache Rep. 2003;7(5):371-376.32. Dostrovsky JO, Davis KD, Kawakita K. Central mechanisms of vascular headaches.
Can J Physiol Pharmacol . 1991;69(5):652-658.33. Strassman AM, Raymond SA, Burstein R. Sensitization of meningeal sensory neu-
rons and the origin of headaches. Nature . 1996;384(6609):560-564.34. Burstein R, Yamamura H, Malick A, Strassman AM. Chemical stimulation of the
intracranial dura induces enhanced responses to facial stimulation in brain stemtrigeminal neurons. J Neurophysiol . 1998;79(2):964-982.
35. Behbehani MM. Functional characteristics of the midbrain periaqueductal gray.Prog Neurobiol . 1995;46(6):575-605.
36. Fields HL, Basbaum AI. Anatomy and physiology of a descending pain control sys-tem. In: Bonica BJ, ed. Advances in Pain and Research and Therapy . New York, NY:
Raven Press; 1979:427-440.37. Leonard G, Mathieu D, Kenny B, Blanchard J, Goffaux P, Marchand S. Evidence
of descending inhibition deficits in atypical trigeminal neuralgia. Pain Res Manag .2008;13:11
38. Sandrini G, Rossi P, Milanov I, Serrao M, Cecchini A, Nappi G. Abnormal mod-ulatory influence of diffuse noxious inhibitory controls in migraine and chronictension-type headache patients. Cephalalgia . 2006;26(7):782-789.
39. Pielsticker A, Haag G, Zaudig M, Lautenbacher S. Impairment of pain inhibition
in chronic tension-type headache. Pain. 2005;118(1-2):215-223.
NEUROSURGERY VOLUME 67 | NUMBER 2 | AUGUST 2010 | 465
BRAIN TUMOR HEADACHES
are also the most likely to cause neuropathic pain.59 Additionalresearch is necessary to identify patients most at risk of the devel-opment of neuropathic or vascular pain after the use of chemother-apeutic agents to treat their malignancy. Prospective studies thatevaluate interindividual differences in circulating and central nerv-ous system cytokine concentrations are also needed to clearly estab-lish the putative link between chemotherapy, inflammation, and pain.
CONCLUSION
Despite historical attempts to establish headache pain as a pathog-nomonic marker of brain tumor, the prevalence of headache painin neuro-oncology patients is insufficiently high and its presentationtoo diverse to justify using this symptom as a diagnostic index. A care-ful clinical workup and a thorough examination of the patientremain, to date, the most valuable way to establish the etiologicalsignificance of headache pain and the necessity for physicians toconduct additional tests. Among neuro-oncology patients, intracra-
nial pressure and traction on pain-sensitive structures remain themost likely cause of headache pain. However, it is clear that forsome patients, peripheral and central sensitization contributes tothe pain felt during and after removal of their mass lesion. Finally,it is important to point out that despite the absence of pain recep-tors in brain parenchyma, neurosurgery and adjuvant chemoradi-ation therapy can be a source of pain and discomfort for patients.This is often overlooked in our desire to treat the underlying malig-nancy, but deserves our full attention if we are to help patients main-tain a better quality of life for as long as possible.
Disclosure
The authors have no personal financial or institutional interest in any of the drugs, materials, or devices described in this article.
REFERENCES
1. Dousset V, Henry P, Michel P. [Epidemiology of headache]. Rev Neurol (Paris).2000;156(suppl 4):4S24-4S29.
2. Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a gen-
eral population-a prevalence study. J Clin Epidemiol . 1991;44(11):1147-1157.
3. Wang HZ, Simonson TM, Greco WR, Yuh WT. Brain MR imaging in the evalua-
tion of chronic headache in patients without other neurologic symptoms. Acad Radiol . 2001;8(5):405-408.
4. Forsyth PA, Posner JB. Headaches in patients with brain tumors: a study of 111
patients. Neurology . 1993;43(9):1678-1683.
5. Kunkle EC, Ray BS, Wolff HG. Studies on headache: the mechanisms and signif-
icance of the headache associated with brain tumor. Bull N Y Acad Med . 1942;
18(6):400-422.6. Pfund Z, Szapary L, Jaszberenyi O, Nagy F, Czopf J. Headache in intracranial
tumors. Cephalalgia . 1999;19(9):787-790.
7. Rushton JG, Rooke ED. Brain tumor headache. Headache . 1962;2:147-152.
8. Schankin CJ, Ferrari U, Reinisch VM, Birnbaum T, Goldbrunner R, Straube A.
Characteristics of brain tumour-associated headache. Cephalalgia . 2007;27(8):904-911.
9. Suwanwela N, Phanthumchinda K, Kaoropthum S. Headache in brain tumor: a
cross-sectional study. Headache . 1994;34(7):435-438.
10. Vazquez-Barquero A, Ibanez FJ, Herrera S, Izquierdo JM, Berciano J, Pascual J.
Isolated headache as the presenting clinical manifestation of intracranial tumors: a
prospective study. Cephalalgia . 1994;14(4):270-272.

7/23/2019 Brain Tumor Headaches From Bedside to Bench
http://slidepdf.com/reader/full/brain-tumor-headaches-from-bedside-to-bench 8/8
466 | VOLUME 67 | NUMBER 2 | AUGUST 2010 www.neurosurgery-online.com
GOFFAUX AND FORTIN
40. Greenspan JD, Winfield JA. Reversible pain and tactile deficits associated with a cerebral tumor compressing the posterior insula and parietal operculum. Pain.1992;50(1):29-39.
41. Greenspan JD, Lee RR, Lenz FA. Pain sensitivity alterations as a function of lesionlocation in the parasylvian cortex. Pain. 1999;81(3):273-282.
42. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain. 2005;9(4):463-484.
43. Gee JR, Ishaq Y, Vijayan N. Postcraniotomy headache. Headache . 2003;43(3):276-278.
44. de Gray LC, Matta BF. Acute and chronic pain following craniotomy: a review. Anaesthesia . 2005;60(7):693-704.
45. Vijayan N. Postoperative headache in acoustic neuroma. Headache. 1995;35(2):98-100.
46. Rocha-Filho PA, Fujarra FJ, Gherpelli JL, Rabello GD, de Siqueira JT. The long-termeffect of craniotomy on temporalis muscle function.Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2007;104(5):e17-e21.
47. De BG, Lorenzetti A, Migliore M, Spagnoli D, Tiberio F, Villani RM. Postoperativepain in neurosurgery: a pilot study in brain surgery. Neurosurgery . 1996;38(3):466-469.
48. Ortiz-Cardona J, Bendo AA. Perioperative pain management in the neurosurgicalpatient. Anesthesiol Clin. 2007;25(3):655-74, xi.
49. Whitton AC, Rhydderch H, Furlong W, Feeny D, Barr RD. Self-reported compre-hensive health status of adult brain tumor patients using the Health Utilities Index.
Cancer . 1997;80(2):258-265.50. Gustafsson M, Edvardsson T, Ahlstrom G. The relationship between function, qual-
ity of life and coping in patients with low-grade gliomas. Support Care Cancer .2006;14(12):1205-1212.
51. Goffaux P, Boudrias M, Mathieu D, Charpentier C, Veilleux N, Fortin D. Developmentof a concise QOL questionnaire for brain tumor patients. Can J Neurol Sci .2009;36(3):340-348.
52. Armstrong TS, Cohen MZ, Eriksen LR, Hickey JV. Symptom clusters in oncology patients and implications for symptom research in people with primary brain tumors. J Nurs Scholarsh. 2004;36(3):197-206.
53. Stoneham MD, Walters FJ. Post-operative analgesia for craniotomy patients: cur-rent attitudes among neuroanaesthetists. Eur J Anaesthesiol . 1995;12(6):571-575.
54. Cross NE, Glantz MJ. Neurologic complications of radiation therapy.Neurol Clin.2003;21(1):249-277.
55. Moretti R, Torre P, Antonello RM, et al. Neuropsychological evaluation of late-onset post-radiotherapy encephalopathy: a comparison with vascular dementia. J Neurol Sci . 2005;229-230:195-200.
56. Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temo-zolomide versus dacarbazine in the treatment of patients with advanced metastaticmalignant melanoma. J Clin Oncol . 2000;18(1):158-166.
57. Plotkin SR, Wen PY. Neurologic complications of cancer therapy. Neurol Clin.
2003;21(1):279-318, x.58. Kannarkat G, Lasher EE, Schiff D. Neurologic complications of chemotherapy agents. Curr Opin Neurol . 2007;20(6):719-725.
59. Myers JS, Pierce J, Pazdernik T. Neurotoxicology of chemotherapy in relation tocytokine release, the blood-brain barrier, and cognitive impairment. Oncol Nurs Forum. 2008;35(6):916-920.
COMMENTS
This review is quite interesting since in the literature the discussion onthe topic headache and brain tumors is seldom approached. All of us
neurosurgeons, in the everyday clinical experience we are aware of thissymptom in patients harboring a brain tumor. All the aspects of the patho-physiology and clinical presentation of the secondary headache are wellpresented and discussed, mainly the one post radiotherapy and that con-
comitant with chemotherapy. The different aspects of the headache,including the hypothesis of a peripheral origin, of central sensitization,and the ones due to inhibition from mesencephalic modulating struc-tures to the peripheral pain inputs are covered and discussed.
In conclusion, the authors should be complimented for giving us thisexhaustive review on a simple but important aspect of our relationship
with the patients affected by brain tumors, in which the failure of long term therapeutic success may be compensated with the interpersonalrelationship.
Giovanni Broggi Milan, Italy