bosniak classification & renal cystic disease
TRANSCRIPT

Bosniak Classification
& Renal Cystic Disease
By /
Shehab Emad
Resident Doctor at Urology Department
Qena University Hospital

Introduction
Renal cysts are a common finding on routine radiological studies. As such, patients are often referred to urologists for their opinion regarding potential intervention and follow-up.
Renal cysts, in general, may be classified as “simple” or “complex.” “Simple” cysts are best defined using sonographic criteria. These include :
1. Absence of internal echoes
2. Round / oval shape
3. Sharp , thin posterior walls
When all of the criteria met , the cyst is benign and no follow up is required .
The difficulty arises when cysts don’t meet the rigid criteria of “simple” definition .

Ultrasonographic picture of simple cyst

Historic points
In 1983, using early computed tomography (CT) scan technology, renal cysts were discovered in 33% of patients in the same age group.
The Bosniak renal cyst classification system was initially reported in 1986, using CT scan findings.
the Bosniak classification has been widely adopted and accepted because it addresses a difficult clinical problem and is easy to apply by both radiologists and Urologists.
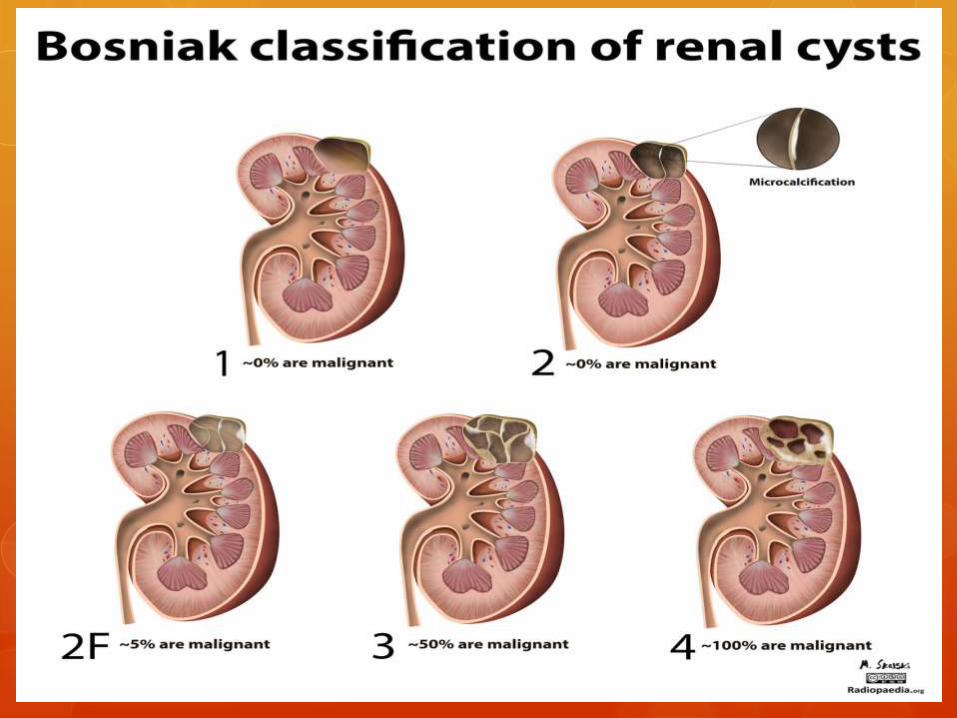
The original classification has divided renal cystic disease into IV categories .
However, It is usually easy to differentiate between lesions at the ends of the spectrum,i.e. the benign simple cysts (Bosniak I) and the clearly malignant Bosniak IV lesions as Simple cysts and solid tumours are usually straightforward to diagnose, but differentiating between complex renal cysts and cystic renal tumours can be difficult. There is a narrow margin between performing unnecessary surgery and missing a cancer.
BosniakIIF
After the original classification was described, it became obvious that some revision was in order because there were some category II cysts that were slightly more complicated than most category II lesions but not complicated enough to place in category III. For that reason, a category IIF (F for follow-up) was introduced in 1993

Bosniak Classification

Bosniak Classification Accuracy
Only a few studies have correlated cyst classification using the Bosniak system with histological findings after removal of kidneys at surgery. Thus there is a lack of evidence to support the classification’s ability to distinguish between benign and malignant masses.
One of these studies carried out on 82 cystic renal masses were resected from 77 patients (Five patients had two lesions evaluated.)
Those patients were evaluated prospectively according to Bosniak system , then underwent surgery and resected masses were sent for histopathology .

Bosniak Classification of Cystic Renal Masses
and Surgical Outcome of 82 lesions from 77
patients
MalignantBenignNO.category
044I
01111II
292049III
18018IV
473582Total

Interpretation of the study as regard proven
malignant risk in each category
TotalCategory IV
CategoryIII
CategoryII
Category I
study
8218/18 (100%)
29/49 (59%)
0/11(0 %)
0/4(0 %)
Proven malignant
risk

Management of renal cystic disease according to
Bosniak Classification
Management category
Ignore & No need for follow up I , II
Follow up II F
Surgical excision III , IV

Guidelines for follow up in Bosniak
Classification IIF
There are no national or international guidelines which stipulate for how long a patient with a Bosniak IIF lesion should undergo radiological surveillance
Literature has been provided to support the view that these patients should undergo surveillance for 5 years.
The suggested policy is “the minimum follow up policy”which is the policy to follow Bosniak IIF Renal cysts by CT scans at 6 months, and 1 year, and then annually until 5 years
This policy may be varied to take into account the age and comorbidity of the patient
Malignant risk in Bosniak IIF Lesions
There have been differing views on this in the literatures .
Some report that the malignancy risk is 12 % , others says that malignancy risk reach 20 % .
However , some authors believe that the malignancy risk of Bosniak IIF similar to Bosniak II !!!

Imaging modalities in following up Bosniak
IIF
According to Bosniak IIF cysts are potentially malignant and should be followed with CT examinations, performed to determine whether the cystic lesions change over time with regard to morphology and contrast enhancement pattern, subsequently resulting in an up- or downgrading.
Alternative imaging modalities includes a combination of ultra-sound and MRI in the follow-up for Bosniak IIF and reduces the lifetime radiation dose (once the lesion has been characterized by triphasic CT scan) especially, in patients younger than 50 years.


Prerequests for Bosniak Classification
1. Both unenhanced and contrast-enhanced thin-section CT scans should be obtained.
2. sections must be less than half the diameter of the lesion to allow adequate assessment (ideally < 5mm)
3. an adequate bolus of contrast material (at least 100 mL of a contrast agent) and at a rate of 2-3 ml/sec.
4. Timing of image acquisition is also critical. The contrast-enhanced images should be obtained in uniform nephrographic phases approximately 100 sec after the start of injection. Images obtained in the earlier corticomedullary differentiation phase may obscure the lesion or provide misleading information.
5. In the event of incidental discovery of a homogeneously high-attenuation renal mass in patients in whom no preliminary unenhanced scanning was performed, a delayed scan at 15 min may provide sufficient information to distinguish between a benign high-density cyst and a neoplasm. Deenhancement of the lesion suggests vascularity and the likelihood of neoplasm, whereas unchanging high attenuation is consistent with a high-density avascular cyst.

CT Vs MRI in Bosniak System
CT scan
The gold standard imaging modality used till now .
MRI Some studies carry out advantages
of MRI over CT in the form of :
1. MRI can be helpful with increasingly complex cyst identification. Recent developments with MRI scanning allow shorter breath holds and increased contrast resolution.
2. As such, the cysts may be characterized in greater detail, compared with CT scan.
3. The MRI may demonstrate poorly identified septa on CT scan and show enhancements that are not otherwise clearly perceived.
4. Also, MRI may differentiate between hemorrhagic cysts and solid enhancing masses.

CT Vs MRI Allogram compares between CT & MRI as regard specificity & sensitivity in differentiation between surgical and non-surgical Renal Cystic lesions using Bosniak System .
Solid line MSCT
Dotted line MRI

Who is he ??
Morton A Bosniak
Clinical Professor; Professor Emeritus of Radiology
Department of Radiology ,NYU Radiology Associates
