bone marrow failure and acute leukemia: more...
TRANSCRIPT
Bone Marrow Failure and Acute Leukemia: More mutations, more problems
6/18/13
Rebecca Olin, MD, MSCE BIOGRAPHY: Rebecca Olin MD MSCE is an Assistant Professor of Clinical Medicine at UCSF. After undergraduate work at Amherst College, she received her MD degree from University of Pennsylvania School of Medicine. She subsequently completed residency training in Internal Medicine and fellowship in Hematology/Oncology, both also at University of Pennsylvania. During fellowship she also received a Masters degree in Clinical Epidemiology, with a focus both on clinical trial development and outcomes research. She has been at UCSF as an Assistant Professor since 2009, and has a clinical practice which focuses on acute leukemia, myelodysplastic syndromes and other hematologic disorders, as well as stem cell transplantation. Her research area of interest is in evaluating quality of life and functional status in older stem cell transplant recipients, with a goal of learning more about how to make stem cell transplant safer. BIBLIOGRAPHY: 1. National Marrow Donor Program. Available from: BeTheMatch.org. 2. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington's disease chromosomes. The Huntington's Disease Collaborative Research Group. Cell. 1993 Mar 26;72(6):971‐83. 3. Byrd JC, Mrozek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC, et al. Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461). Blood. 2002 Dec 15;100(13):4325‐36. 4. Calado RT, Young NS. Telomere diseases. N Engl J Med. 2009 Dec 10;361(24):2353‐65. 5. Dohner H, Estey EH, Amadori S, Appelbaum FR, Buchner T, Burnett AK, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010 Jan 21;115(3):453‐74. 6. Sanz MA, Lo Coco F, Martin G, Avvisati G, Rayon C, Barbui T, et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups. Blood. 2000 Aug 15;96(4):1247‐53. 7. Shimamura A, Alter BP. Pathophysiology and management of inherited bone marrow failure syndromes. Blood Rev. 2010 May;24(3):101‐22.
6/14/2013
1
Bone Marrow Failure Syndromes and Acute Leukemia:
“More mutations, more problems”
Rebecca Olin MD MSCE
UCSF Mini Medical School
June 18 2013
A
Huntington Disease
Progressive neurological disorder
Typical onset in 30’s, progresses over 10-20 years until death
Genetically inherited – 50% chance
No treatment, no cure
MacDonald 1993
Overview
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
6/14/2013
2
Laboratory Values (Review)
We order a “CBC” = Complete Blood Count
RBC = red blood cells (erythrocytes)
Platelets
WBC = white blood cells Neutrophils
Lymphocytes
Monocytes
Basophils
Eosinophils
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview
Inherited BMFS
Acquired BMFS
Acquired Aplastic Anemia
“Aplastic” = failure to develop
“Aplastic anemia” is a misnomer because it is not just about anemia
Failure of the bone marrow to make enough cells of all three lineages Failure to make blood
Aka “The Empty Marrow”
Disorder of the bone marrow stem cell
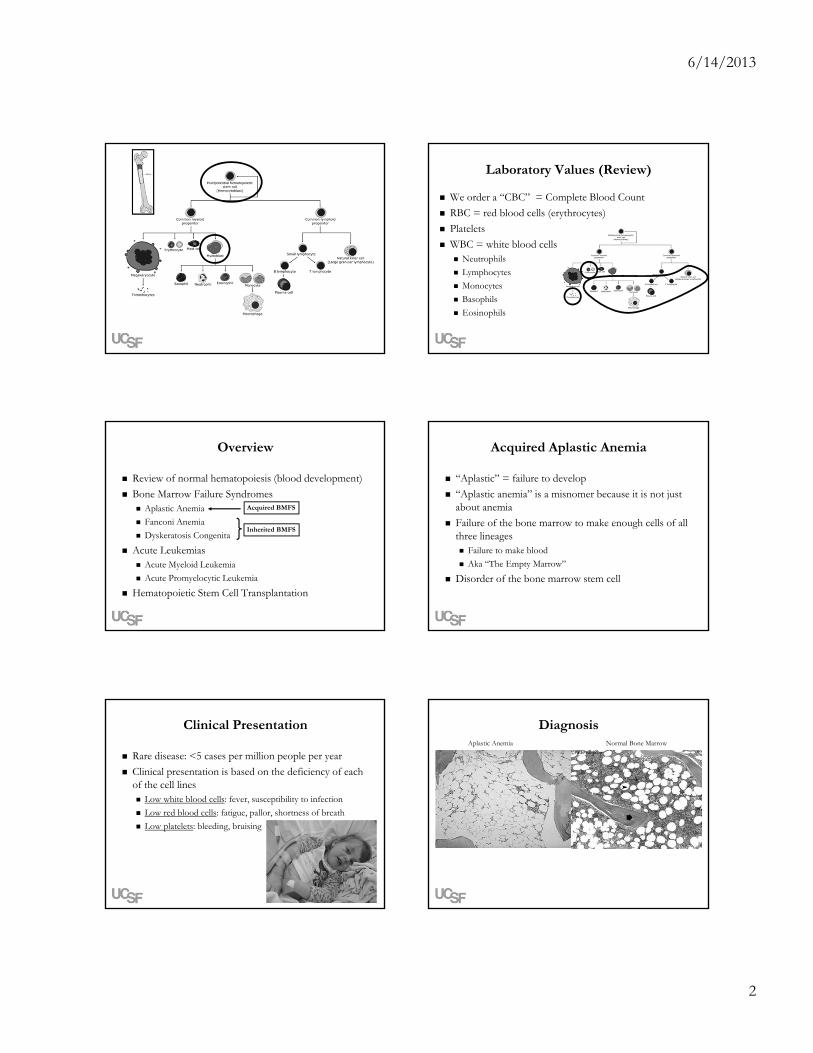
Clinical Presentation
Rare disease: <5 cases per million people per year
Clinical presentation is based on the deficiency of each of the cell lines Low white blood cells: fever, susceptibility to infection
Low red blood cells: fatigue, pallor, shortness of breath
Low platelets: bleeding, bruising
DiagnosisNormal Bone MarrowAplastic Anemia
6/14/2013
3
Causes of Aplastic Anemia
Chemicals – eg pesticides
Medications – wide variety
Viruses – hepatitis, HIV, parvovirus
Radiation
Inherited predisposition
MAJORITY ARE UNKNOWN “idiopathic”
Aplastic Anemia is an Autoimmune Disease
Patient’s own T-cells (T lymphocytes) are attacking the bone marrow stem cell
Treatment is based on suppressing the T-cells
Treatment of Aplastic Anemia
More later…
Anti-thymocyte Globulin (ATG)
TT
Cyclosporine
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview
Inherited BMFS
Acquired BMFS
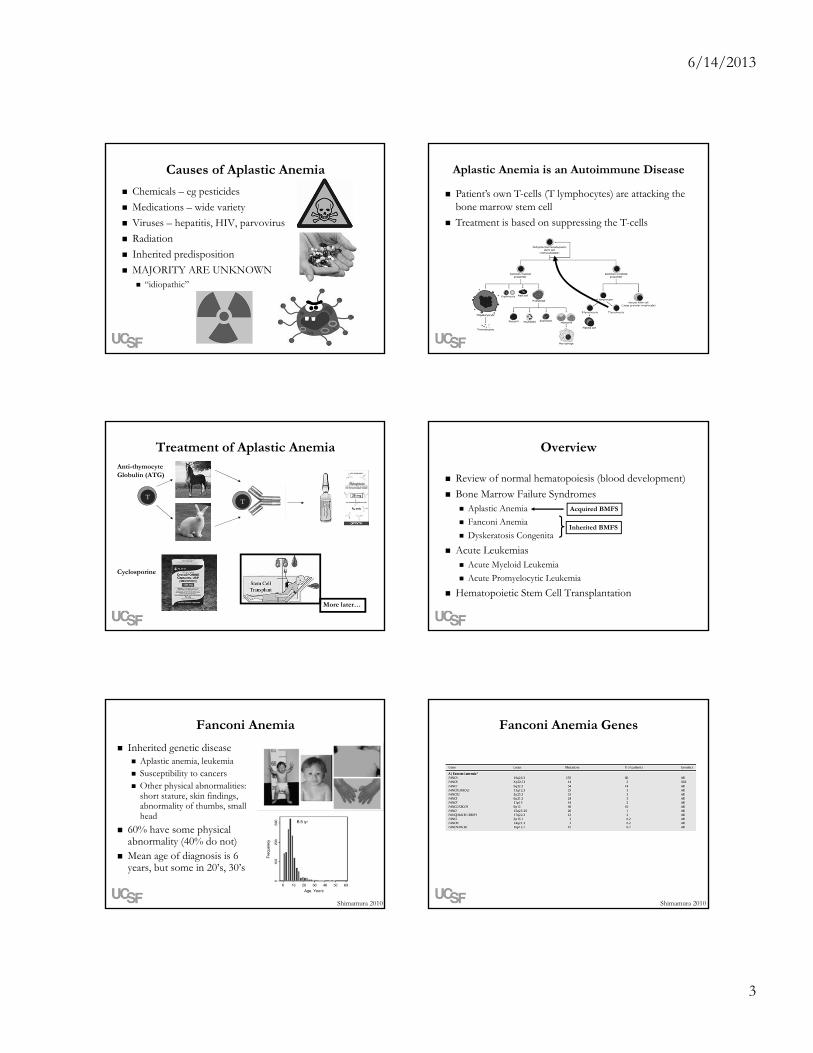
Fanconi Anemia
Inherited genetic disease Aplastic anemia, leukemia Susceptibility to cancers Other physical abnormalities:
short stature, skin findings, abnormality of thumbs, small head
60% have some physical abnormality (40% do not)
Mean age of diagnosis is 6 years, but some in 20’s, 30’s
Shimamura 2010
Fanconi Anemia Genes
Shimamura 2010
6/14/2013
4
DNA Damage
Up to one million events per cell per day!
DNA Repair
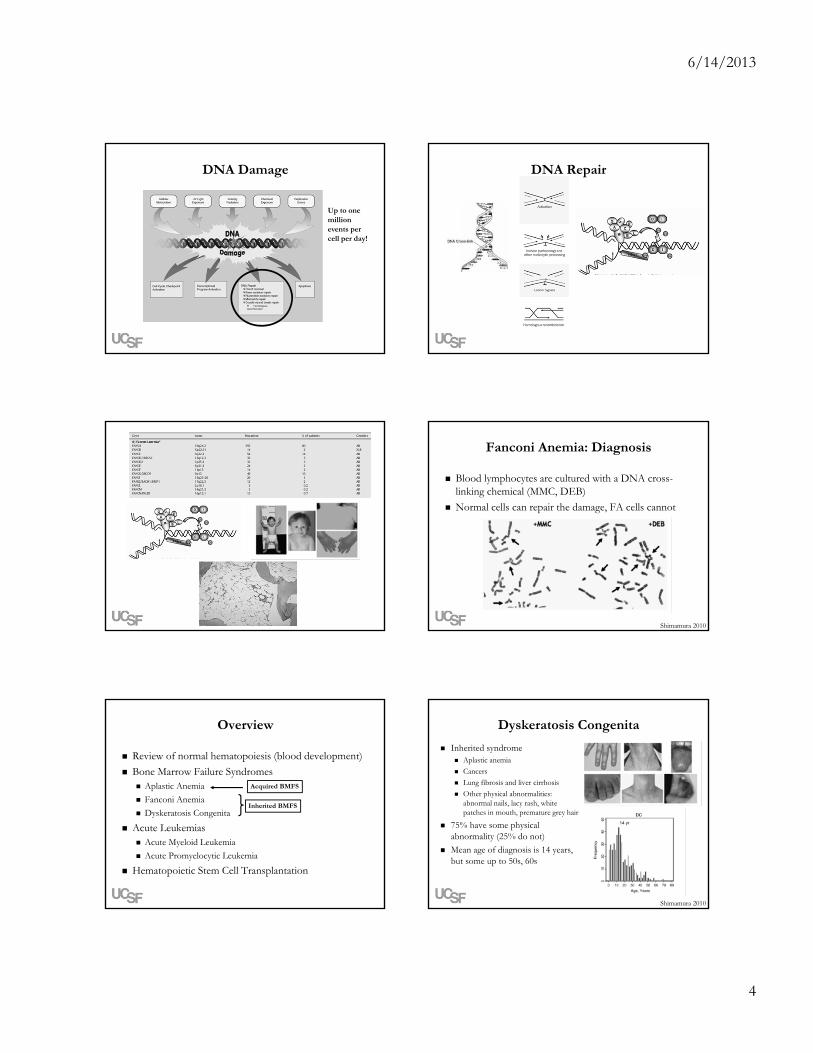
Fanconi Anemia: Diagnosis
Blood lymphocytes are cultured with a DNA cross-linking chemical (MMC, DEB)
Normal cells can repair the damage, FA cells cannot
Shimamura 2010
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview
Inherited BMFS
Acquired BMFS
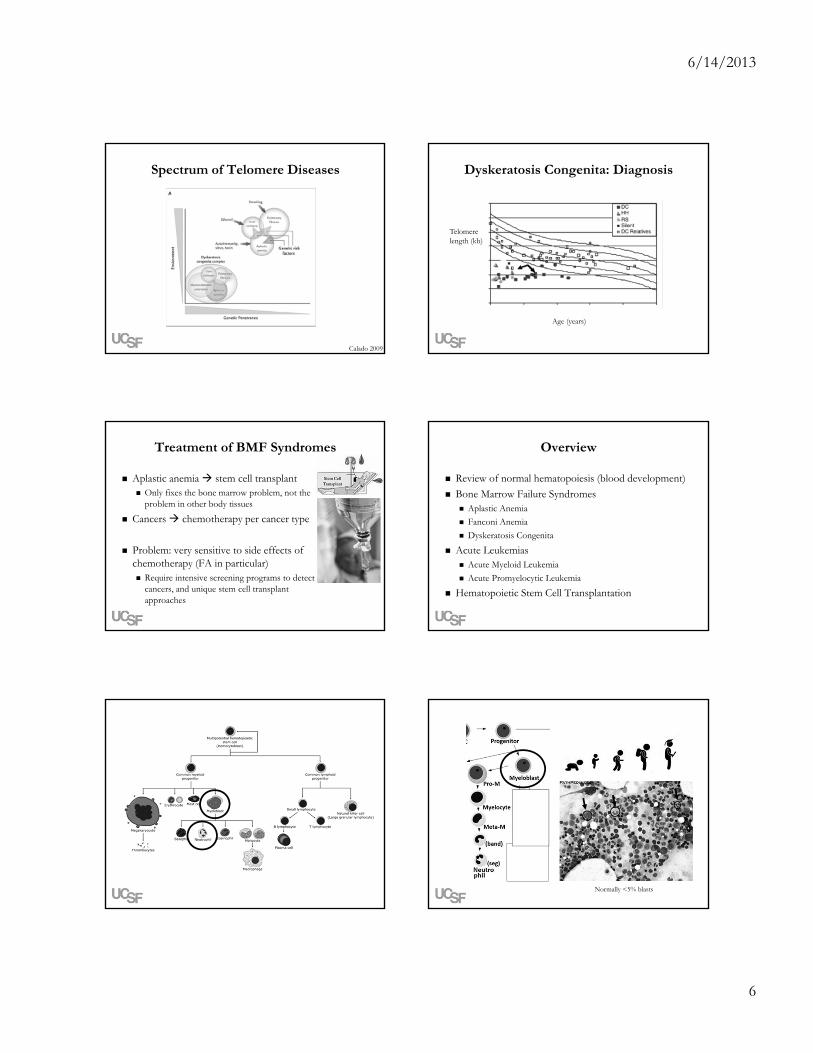
Dyskeratosis Congenita
Inherited syndrome Aplastic anemia
Cancers
Lung fibrosis and liver cirrhosis
Other physical abnormalities: abnormal nails, lacy rash, white patches in mouth, premature grey hair
75% have some physical abnormality (25% do not)
Mean age of diagnosis is 14 years, but some up to 50s, 60s
Shimamura 2010

6/14/2013
5
Dyskeratosis Congenita Genes Telomeres
Calado 2009
Telomere Function Every time a cell divides, a very small amount of DNA at the
ends of chromosomes is not replicated and therefore lost
Telomeres are “martyrs” to protect coding genetic material from being lost – telomeres get shorter instead
11 Kb – cord blood
6 Kb –age 90
Calado 2009
Telomere Maintenance
Enzyme complex called telomerase, containing both proteins and RNA
(Go UCSF!)Elizabeth Blackburn
Calado 2009
TERC
Cellular Consequences of Telomere Erosion
Calado 2009 Shimamura 2010
6/14/2013
6
Spectrum of Telomere Diseases
Calado 2009
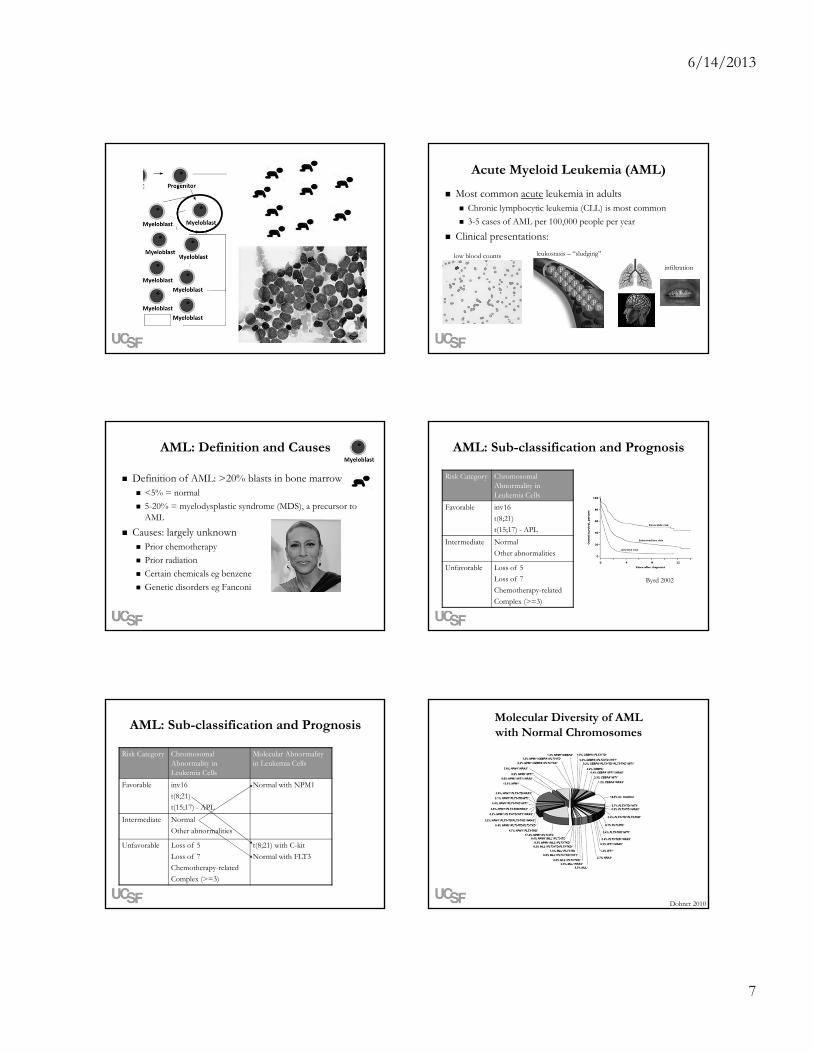
Dyskeratosis Congenita: Diagnosis
Telomere length (kb)
Age (years)
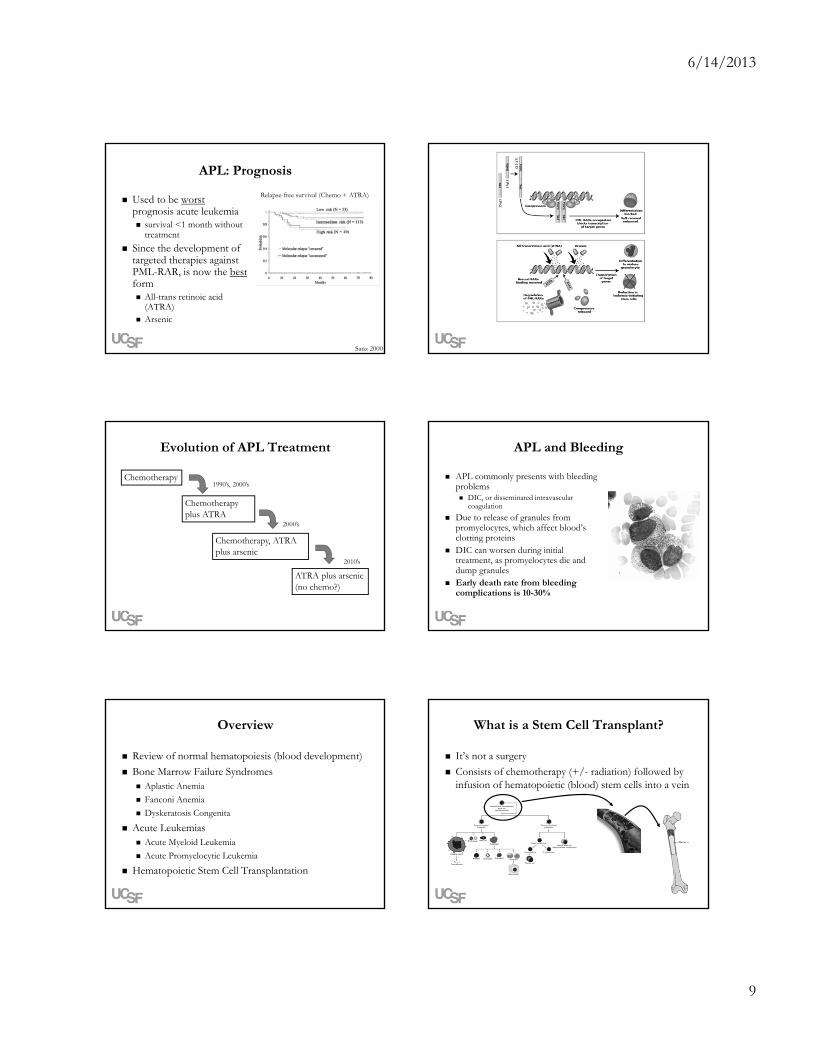
Treatment of BMF Syndromes
Aplastic anemia stem cell transplant Only fixes the bone marrow problem, not the
problem in other body tissues
Cancers chemotherapy per cancer type
Problem: very sensitive to side effects of chemotherapy (FA in particular) Require intensive screening programs to detect
cancers, and unique stem cell transplant approaches
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview
Normally <5% blasts
6/14/2013
7
Acute Myeloid Leukemia (AML)
Most common acute leukemia in adults Chronic lymphocytic leukemia (CLL) is most common
3-5 cases of AML per 100,000 people per year
Clinical presentations:
BB
BB
BB
BB
B
BB
BB
BB
BB
B
low blood counts leukostasis – “sludging”
infiltration
AML: Definition and Causes
Definition of AML: >20% blasts in bone marrow <5% = normal
5-20% = myelodysplastic syndrome (MDS), a precursor to AML
Causes: largely unknown Prior chemotherapy
Prior radiation
Certain chemicals eg benzene
Genetic disorders eg Fanconi
AML: Sub-classification and Prognosis
Risk Category Chromosomal Abnormality in Leukemia Cells
Favorable inv16
t(8;21)
t(15;17) - APL
Intermediate Normal
Other abnormalities
Unfavorable Loss of 5
Loss of 7
Chemotherapy-related
Complex (>=3)
Byrd 2002
AML: Sub-classification and Prognosis
Risk Category Chromosomal Abnormality in Leukemia Cells
Molecular Abnormality in Leukemia Cells
Favorable inv16
t(8;21)
t(15;17) - APL
Normal with NPM1
Intermediate Normal
Other abnormalities
Unfavorable Loss of 5
Loss of 7
Chemotherapy-related
Complex (>=3)
t(8;21) with C-kit
Normal with FLT3
Molecular Diversity of AML with Normal Chromosomes
Dohner 2010

6/14/2013
8
Process of Treating AML
Phase 1: Induction reduce the number of leukemia cells
in the body by orders of magnitude
goal: remission
= chemo
Phase 2: Consolidation get ride of every single last leukemia
cell in the body
goal: cure
= more chemo or stem cell transplant
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview
Normally <5% blasts
Acute Promyelocytic Leukemia (APL)
Defined by existence of t(15;17) translocation
Function of PML not well understood
Function of RAR proteins is to bind certain genes, promote normal differentiation of cells Abnormal RARα has abnormal function
15
17
PML
RARα
PML RARα
6/14/2013
9
APL: Prognosis
Used to be worstprognosis acute leukemia survival <1 month without
treatment
Since the development of targeted therapies against PML-RAR, is now the bestform All-trans retinoic acid
(ATRA) Arsenic
Relapse-free survival (Chemo + ATRA)
Sanz 2000
Evolution of APL Treatment
Chemotherapy
Chemotherapy plus ATRA
Chemotherapy, ATRA plus arsenic
ATRA plus arsenic(no chemo?)
1990’s, 2000’s
2000’s
2010’s
APL and Bleeding
APL commonly presents with bleeding problems DIC, or disseminated intravascular
coagulation
Due to release of granules from promyelocytes, which affect blood’s clotting proteins
DIC can worsen during initial treatment, as promyelocytes die and dump granules
Early death rate from bleeding complications is 10-30%
Review of normal hematopoiesis (blood development)
Bone Marrow Failure Syndromes Aplastic Anemia
Fanconi Anemia
Dyskeratosis Congenita
Acute Leukemias Acute Myeloid Leukemia
Acute Promyelocytic Leukemia
Hematopoietic Stem Cell Transplantation
Overview What is a Stem Cell Transplant?
It’s not a surgery
Consists of chemotherapy (+/- radiation) followed by infusion of hematopoietic (blood) stem cells into a vein
6/14/2013
10
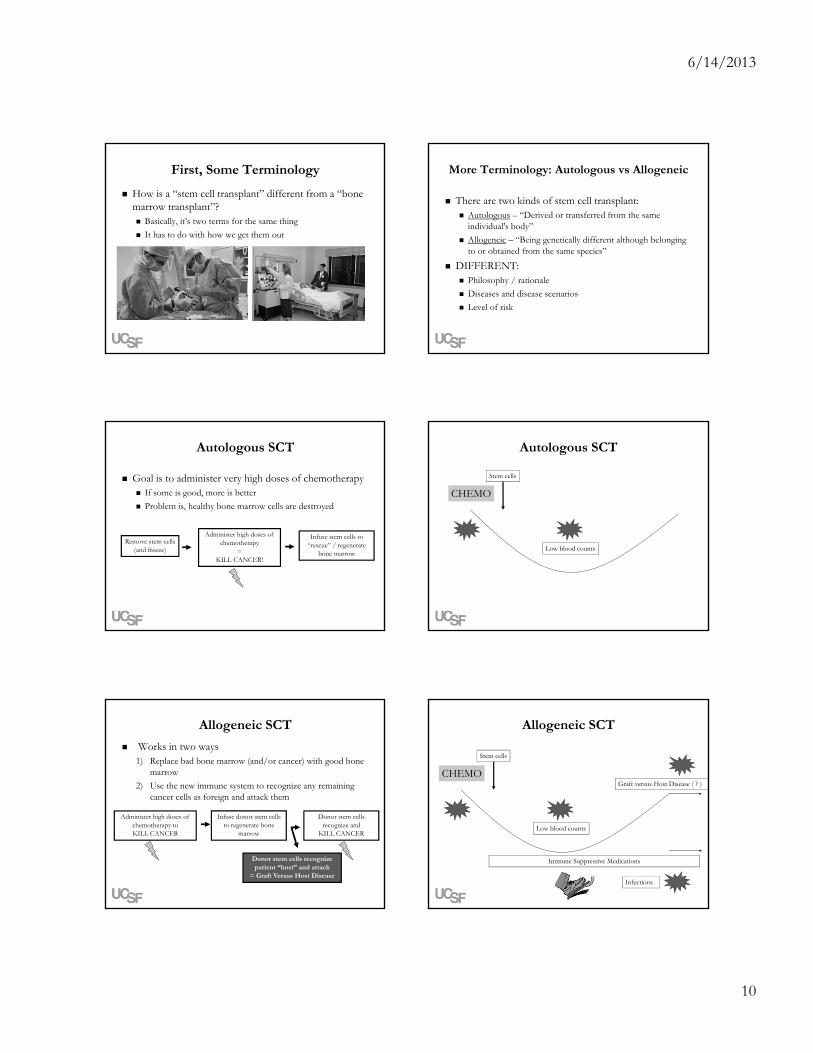
First, Some Terminology
How is a “stem cell transplant” different from a “bone marrow transplant”? Basically, it’s two terms for the same thing
It has to do with how we get them out
More Terminology: Autologous vs Allogeneic
There are two kinds of stem cell transplant: Autologous – “Derived or transferred from the same
individual's body”
Allogeneic – “Being genetically different although belonging to or obtained from the same species”
DIFFERENT: Philosophy / rationale
Diseases and disease scenarios
Level of risk
Autologous SCT
Goal is to administer very high doses of chemotherapy If some is good, more is better
Problem is, healthy bone marrow cells are destroyed
Remove stem cells(and freeze)
Administer high doses of chemotherapy
=KILL CANCER!
Infuse stem cells to “rescue” / regenerate
bone marrow
CHEMO
Stem cells
Low blood counts
Autologous SCT
Allogeneic SCT
Works in two ways1) Replace bad bone marrow (and/or cancer) with good bone
marrow
2) Use the new immune system to recognize any remaining cancer cells as foreign and attack them
Administer high doses of chemotherapy toKILL CANCER
Infuse donor stem cells to regenerate bone
marrow
Donor stem cells recognize and
KILL CANCER
Donor stem cells recognize patient “host” and attack
= Graft Versus Host Disease
CHEMO
Stem cells
Low blood counts
Graft versus Host Disease ( ? )
Infections
Allogeneic SCT
Immune Suppressive Medications

6/14/2013
11
Stem Cell SourceSibling donor – 25%
Half-matched donor: 50% if sibling 100% if parent or child
Matched unrelated donor
Umbilical cord blood
3
21
SCT Cures Disease and Saves Lives
http://BeTheMatch.org
Thank you for your attention!