bone biomarkers related to osteoarthritis · bone biomarkers related to osteoarthritis m. p....
TRANSCRIPT

Bone Biomarkers Related to Osteoarthritis
M. P. Engbersen, Z. Huang, and V. B. Kraus
ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Role of Bone in OA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Biomarkers of Collagen Type I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Markers of Synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Markers of Degradation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Other Collagenous Biomarkers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Collagen Type II . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Non-collagenous Biomarkers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Osteocalcin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Periostin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Cytokine-Related Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Bone Sialoprotein . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20DKK-1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20TRAP5b . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Bone Markers in Clinical Trials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Other Diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Potential Applications to Prognosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Summary Points . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Key Facts of Osteoarthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
M. P. Engbersen and Z. Huang have contributed equally.
M.P. Engbersen • Z. Huang • V.B. Kraus (*)Division of Rheumatology, Duke Molecular Physiology Institute, Duke University School ofMedicine, Durham, NC, USAe-mail: [email protected]; [email protected]; [email protected]
# Springer Science+Business Media Dordrecht 2016V.R. Preedy (ed.), Biomarkers in Bone Disease, Biomarkers in Disease: Methods,Discoveries and Applications, DOI 10.1007/978-94-007-7745-3_35-1
1

AbstractIt is evident that the bone plays a vital role in osteoarthritis (OA) diseasepathogenesis, progression, and symptomatology. The close interaction of thebone and cartilage in the pathogenesis of OA and the knowledge that OA is adisease of the whole joint provide a strong rationale for investigating bonebiomarker changes in OA. The evaluation of bone biomarkers is important forgaining a greater understanding of the role of bone pathology in OA and a meansfor developing new diagnostic and prognostic tools for therapeutic developmentsand early OA intervention. Although comparisons among studies are difficultbecause different assays and assay parameters are used and different assays reflectdifferent outcomes, many bone-related biomarkers have shown great promise asdiagnostic, prognostic, and efficacy of intervention biomarkers for OA. Theseinclude the traditional bone biomarkers, CTX-I and NTX-I and osteocalcin. Thestrong association of these traditional bone biomarkers with urinary C-terminaltelopeptide of type II collagen (CTX-II) from the articular cartilage confirms thestrong association of bone resorption with cartilage degradation. To date, resultsusing bone biomarkers in OA trials provide examples of the modifiability of thewhole joint organ by bone-acting agents. Based on recent data, tartrate-resistantacid phosphatase 5b (TRAP5b), periostin, and endothelin-1 (ET-1) show greatpromise and can be considered new OA-related bone biomarkers. More studiesare required in the context of treatment trials to determine which bone biomarkerswill be most relevant for drug development and use in the clinic.
KeywordsOsteoarthritis • Bone • Biomarkers • Resorption • Formation • Turnover • Colla-gen • Subchondral • Articular
List of AbbreviationsALP: Alkaline phosphataseBIPEDS: Burden of disease, Investigative, Prognostic, Efficacy of
intervention, Diagnostic or Safety biomarkersBMD: Bone mineral densityBML: Bone marrow lesionBSP: Bone sialoproteinCT: Computed tomographyCTX and CTX-I: C-terminal telopeptide of type I collagenCTX-II: C-telopeptide of type II collagenDKK-1: Dickkopf WNT signaling pathway inhibitor 1DMOADs: Disease-modifying OA drugsDpd: Deoxypyridinoline (also called lysyl-pyridinoline or LP)ECLIA: Electrochemiluminescence immunoassayELISA: Enzyme-linked immunosorbent assayET-1: Endothelin-1HYL-Pyr: Hydroxylysyl-pyridinoline (also called pyridinoline or HP)
2 M.P. Engbersen et al.

ICTP: Carboxy-terminal telopeptide of type I collagenIL-6: Interleukin-6JSN: Joint space narrowingKL-score: Kellgren and Lawrence grade (of radiographic severity of
OA)KOOS: Knee injury and osteoarthritis outcome scoreMMPs: Matrix metalloproteinasesMRI: Magnetic resonance imagingNTX and NTX-I: N-terminal telopeptide of type I collagenOA: OsteoarthritisOC: Osteocalcin (intact protein indicative of bone formation;
fragments of OA indicative of bone resorption)OFELY: “Os des Femmes de Lyon,” a longitudinal cohort study for
assessing osteoporosis and secondary OAPICP: Procollagen type I C-terminal propeptidePINP: Procollagen type I N-terminal propeptidePIIANP: N-propeptide of type IIA procollagenPOSTN: PeriostinS: SerumSF: Synovial fluidTRACP5b: Tartrate-resistant acid phosphatase 5bWNT: Wingless-related integration site
Introduction
Osteoarthritis (OA) is one of the most common medical conditions confronting thesociety today. It is estimated that 27 million people in the United States are currentlydiagnosed with this disease (Lawrence et al. 2008). Increased life expectancy andobesity are driving a marked increasing incidence of OA. It is, therefore, natural toexpect a concomitant rise in the direct and indirect costs of managing OA.
Currently, there are no disease-modifying OA drugs (DMOADs). There arehowever, palliative, illness-modifying treatments such as analgesics, physical ther-apy, and ultimately, joint replacement. One reason for this state of affairs is thatapplication of DMOADs requires the ability to detect early stages of OA and monitorits progression. Although an OA diagnosis typically relies on clinical and radio-graphic features, half of the patients with radiographic OA do not exhibit symptomsand vice versa (Bijlsma et al. 2011).
Identifying biomarkers that characterize OA at early stages, such as during theprolonged molecular, pre-radiographic, or asymptomatic phase, before the develop-ment of irreversible anatomic degradation (radiographic abnormality) or illness(pain, functional deformity, gait abnormality), has become an important goal foradvancing OA research and therapeutics (see Kraus et al. for summary of diseasestages (Kraus et al. 2015)). The development of clinical symptoms and/or radiolog-ical observable changes in arthritic joints is preceded by an extensive process ofbiochemical and mechanical disturbances of the whole joint organ. By the time that
Bone Biomarkers Related to Osteoarthritis 3

cartilage damage occurs, the joint pathology is generally considered irreversible.Early intervention requires early disease indicators. Because of the differentialadaptive capacity of the bone, bone changes in OA occur rapidly and are discerniblemore readily than cartilage abnormalities (Goldring and Goldring 2010), the “canaryin the mine” phenomenon. For this reason they present quite attractive potentialbiomarkers for detecting OA early. This chapter will focus on summarizing thecurrent and potential ability of bone biomarkers to fulfill roles as OA-related Burdenof disease, Investigative, Prognostic, Efficacy of intervention, Diagnostic, or Safety(BIPEDS) biomarkers.
Pathology
OA has long been characterized as an upregulation and imbalance of degradation(catabolism) and repair (anabolism) of cartilage components (Aigner et al. 2007).Cartilage-degrading proteinases and chondrocyte apoptosis lead to a net breakdownof the extracellular matrix. In an attempt to repair, clusters of chondrocytes form inand around damaged areas of the cartilage during early stage degeneration (Aurichet al. 2005). Both catabolic and anabolic cartilage biomarkers have been evaluated inOA, including the C-terminal telopeptide of type II collagen (CTX-II) (Valdeset al. 2014) and the N-propeptide of type IIA collagen (PIIANP) (Rousseauet al. 2004), respectively.
Role of Bone in OA
Although bone alterations on radiographs have been definitively associated with OAfor over 50 years (Kellgren and Lawrence 1957), it has only recently been widelyaccepted that OA is a disease of the whole joint organ involving, in addition toprogressive degradation of cartilage, alterations of the synovium, menisci, ligaments,and subchondral bone (Bijlsma et al. 2011) (see Fig. 1). Bony features reflecting OAinclude subchondral bone sclerosis, bone marrow lesions (BMLs), bone cysts,osteophytes (Sharma et al. 2013; Hunter et al. 2014; Hunter et al. 2011), and alteredbone trabecular integrity (Kraus et al. 2009; Kraus et al. 2013). Increasedsubchondral bone resorption occurs at an early stage in the development of OA(Funck-Brentano and Cohen-Solal 2015). A range of investigations has shownpositive effects on cartilage health when bone resorption is suppressed (Karsdalet al. 2014) confirming the role of bone factors in the cross talk between the cartilageand bone and the pathogenesis of OA (Table 1).
Subchondral bone marrow edema-like lesions (BMLs) and cyst-like lesions arecommon findings in OA. BMLs are associated with both clinical symptoms andsigns, including pain and OA progression (Xu et al. 2012; Zhang et al. 2011). BMLsevolve into subchondral cyst-like lesions suggesting that BMLs could be a precysticphase or that BMLs facilitate formation of cysts (Crema et al. 2010).
4 M.P. Engbersen et al.

Osteophyte formation is a clear indicator of radiographic OA and is a majordeterminant of the Kellgren and Lawrence (KL) grade, the most commonly usedsystem for grading radiographic OA severity (Hart and Spector 1995). Even thoughit is still often unclear whether the bone abnormalities develop independently orsecondary to articular cartilage degradation, and whether the abnormalities arecaused by an altered mechanical or biochemical environment, it is evident that thebone plays a vital role in OA disease pathogenesis, progression, andsymptomatology.
Fig. 1 Diagrammatic overview of osteoarthritis pathology. Sagittal view of the knee joint.(a) normal joint with joint structures labeled; (b) OA joint with osteoarthritis features indicateddemonstrating pathology of the whole joint organ (Courtesy Hiskia Pepijn Jansen)
Bone Biomarkers Related to Osteoarthritis 5

Biomarkers of Collagen Type I
Collagen type I is the most abundant organic component of the bone constituting95 % of the bone collagen. Therefore, various epitopes of collagen type I are anatural choice for following changes in bone metabolism in OA. However, colla-gen type I is also found, but to a lesser extent, in the extracellular matrix of othertissues like the skin, dentin, cornea, vessels, and tendons (Lombardi et al. 2012), soit is important to qualify these biomarkers in the context of OA to determine theirutility.
Table 1 Markers with a relationship to the bone and a putative role in osteoarthritis
Biomarker Protein of origin Relationship to the bone
Current BIPEDSa
biomarker category forosteoarthritis
PINP Collagen type I Bone formation B, P, D (" in OA)
PICP Collagen type I Bone formation I (?" in early OA)
CTX-I Collagen type I Cathepsin K and MMP releasedindicator of bone resorption
P, E (" in OA)
ICTP Collagen type I MMP released indicator of boneresorption
P (" in hip OA)
NTX-I Collagen type I Bone resorption P, E (" in OA)
Hyl-Pyr Collagen of thebone, cartilage, andother tissues
Bone resorption I (" in OA)
DPD Collagen type I ofthe bone
Bone resorption I (" in OA)
CTX-II Collagen type II Cartilage degradation D, P, E (" in OA)
OC Non-collagenous Bone formation# B, P, E (" in OA)
Periostin Non-collagenous Non-collagenous I (" in OA subchondralbone)
IL-6 Cytokine Bone resorption D, E (" in OA)
Leptin Adipokine Bone resorption (centrallymediated); bone formation(peripherally mediated)
D, E (" in OA)
ET-1 Vasoconstrictorinduced bycytokines
Bone formation I (" in OA)
BSP Bone formation andmineralization
I (" in OA)
Dkk-1 Non-collagenous Bone resorption by inhibitingosteoblast development
I (# in OA)
Trap5b Protease Bone-degrading enzyme I (" in OA)aBIPEDS = burden of disease, investigative, prognostic, efficacy of intervention, diagnostic, safetyas described in Bauer et al. (2006) and Kraus et al. (2011); for names of biomarkers, see list ofabbreviations
6 M.P. Engbersen et al.

Markers of Synthesis
When a triple helical form of the collagen precursor is secreted to the extracellularmatrix by osteoblasts, the procollagen protein is cleaved of its C- and N-terminalpropeptides whose concentrations in the circulation reflect synthesis of collagen typeI and, therefore, bone synthesis. The propeptides can be detected in serum usingsandwich enzyme-linked immunosorbent assays (ELISAs) or electrochemilumi-nescence immunoassays (ECLIAs) (Kumm et al. 2013; He et al. 2013). Althoughcollagen type I propeptides may also arise from other tissues (such as the skin,vessels, fibrocartilage, and tendons), most nonskeletal tissues exhibit a slowerturnover than the bone and contribute very little to the circulating pool ofprocollagen type I N-terminal propeptide (PINP) (Research 2015). In a 6-yearstudy of knee OA, PINP exhibited both prognostic and diagnostic potential, espe-cially for progressive osteophytosis; OA progression was preceded by enhancedbone formation, reflected in elevated PINP (Kumm et al. 2013). Interestingly, theassociations were strongest for the first 3 years of follow-up suggesting that thisbiomarker is most informative during the early radiographic stages of OA. Kummet al. chose not to use KL grades but rather a system described by Nagaosaet al. (Nagaosa et al. 2000) that scores joint space separately from osteophyte; theysuggest this scoring system has advantages for identifying early stages of OA. Twoprior studies utilizing KL grades identified positive trends but not significant asso-ciations of PINP with an OA diagnosis (Davis et al. 2007) and paradoxically,reduced OA progression (Berry et al. 2010). Although these results would appearcontradictory to Kumm et al., possibly different forms of PINP were detected in thedifferent studies. PINP can be detected in the circulation as two different forms, the“intact” or trimeric molecule and as a monomer. In osteoporosis subjects withnormal renal function, the predominant form of PINP detected in circulation is thetrimeric form. However, monomeric PINP fragments may accumulate in patientswith renal failure or metastatic bone disease (Research 2015; Koivula et al. 2012). Inaddition, the study by Berry et al. used non-fasting samples, and serum PINP levelshave been shown to vary modestly (4 %) but significantly depending on fed versusfasting status (Clowes et al. 2002).
Despite the fact that the procollagen type I C-terminal propeptide (PICP) is awidely used bone turnover biomarker, much like PINP, little research has been doneto evaluate PICP as an OA biomarker. A study in 2002 showed no association ofsynovial fluid PICP levels with grade of OA severity by the Outerbridge and Neyesclassification system; however samples were obtained after a 50 ml saline lavage ofthe joint (Schmidt-Rohlfing et al. 2002). As a result, neither of these procollagenpeptides have been researched extensively as bone synthesis biomarkers forOA. Nevertheless, PINP shows potential for use as a burden of disease and prog-nostic biomarker in OA. PICP and PINP behave as independent proteins withdifferent liver and lymph clearance (Koivula et al. 2012). PINP from soft as opposedto hard (bone) tissues generally reaches the circulation indirectly via the lymph,while changes in lymph flow do not detectably affect the circulating concentration ofPICP. This suggests that the contribution of soft tissues to the circulating
Bone Biomarkers Related to Osteoarthritis 7

concentration of PINP is normally quite small. Based on the fact that serum PINP hasbeen recommended as the preferred bone synthesis reference marker for osteoporo-sis, further research of its particular utility as an OA biomarker would appear to bewarranted.
Markers of Degradation
Collagen type I is degraded by various proteins, implying that various degradationproducts can be found in either serum or urine. Matrix metalloproteinases (MMPs),like MMP-8, can degrade collagen type I. Cathepsin K, involved in systemic boneresorption, can also degrade collagen type I (Fardellone et al. 2014).
The cross-linked C-telopeptide of collagen type I (CTX-I) is a preferred bio-marker for monitoring bone resorption of osteoporosis (Vasikaran et al. 2011).There are a number of carboxy-terminal telopeptide epitopes of collagen type I(CTX-I) in serum and urine as well as various assays specific to each of the fourpossible isomers of CTX: alpha-L, beta-L, alpha-D, and beta-D, whereby alphaand beta refer to the non-isomerized and isomerized forms of aspartate, respec-tively, and L and D refer to non-racemized and racemized forms of aspartate,respectively (Cloos and Fledelius 2000). Baseline serum concentrations of CTX(beta isomers) have been associated with an increase in BML scores over 2 years(Pelletier et al. 2010). A recent paper by Heubner et al. showed a strong correlationbetween joint space narrowing (JSN) and osteophyte progression with urinaryalpha CTX, the non-isomerized form of CTX indicative of turnover of new bone(Huebner et al. 2014). The same study showed a correlation between kneeperiarticular bone turnover, demonstrated by bone scintigraphy, and urinaryalpha CTX. In a study of 600 knee OA subjects from the osteoarthritis initiative,higher baseline urinary alpha CTX-I and higher 12- and 24-month time-integratedconcentrations of urinary alpha CTX-I and serum CTX-I predicted the risk of thecombination of pain and radiographic OA worsening over 4 years (Krauset al. 2016). These results underscore a strong association of bone remodelingand OA progression.
In a 16-week study on the effect of weight loss in obese OA patients, serum (betaisomeric) CTX-I increased significantly and in proportion to the amount of weightloss, but the change in CTX-I was not associated with the change in patient-reportedoutcomes (quantified by four items of the knee injury and osteoarthritis outcomescore (KOOS-4)) (Bartels et al. 2014).
Another carboxy-terminal cross-linked telopeptide of type I collagen includesICTP. The generation of ICTP and CTX depends on different collagenolytic path-ways; cathepsin K releases CTX but not ICTP, while matrix metalloproteinasesrelease both carboxy-terminal epitopes (Garnero et al. 2003). There are also assaysrecognizing ICTP. In 2005, Berger et al. found higher levels of ICTP in the bone butnot serum in association with rapidly destructive hip OA, compared to healthycontrols (Berger et al. 2005). Since then, not much research has been done evaluatingICTP as a biomarker for OA.
8 M.P. Engbersen et al.

Cross-linked N-telopeptide of collagen type I (NTX-I) is much like CTX-I and iscommonly used as a biomarker of bone resorption. Urinary NTX-I may be preferredto serum or plasma NTX-I in a clinical setting because it is not as sensitive tocircadian changes and is not affected by food intake (Baxter et al. 2013). Recently,urinary NTX-I concentrations did not show significant differences by differingseverities of radiological knee OA by KL grade in a large cohort of 1200 subjects(Tanishi et al. 2014). However, the higher quartiles of the uCTX-II and uNTX-Ilevels gradually included higher numbers of grade �2 OA subjects in women over60-year-old, suggesting a possible diagnostic value of NTX-I in women. Similarly,in another study of women, urinary NTX was not associated with any radiographicknee OA phenotypes (Blumenfeld et al. 2013).
In a UK study of 216 postmenopausal women not receiving any bone-modifyingmedication who had a baseline knee radiograph and a repeat radiograph 4 years later,higher baseline urinary NTX-I was associated with risk for radiographic progressionof knee OA (Bettica et al. 2002). The UK study results contradict the findings ofBerry et al. who reported a significant association between higher bone resorptionmarkers, CTX-I and NTX-I, and reduced cartilage loss in a subgroup of subjects withhigh bone formation (as demonstrated by PINP) (Berry et al. 2010). However, theUK findings agree with results of a study of 600 knee OA subjects from theosteoarthritis initiative, wherein higher 12- and 24-month time-integrated concen-trations of urinary and serum NTX-I predicted the risk of the combination of painand radiographic knee OA worsening over 4 years with a similar trend for baselineNTX-I concentrations (Kraus et al. 2016). Baseline serum NTX has also beenassociated with a modest risk of incident and progressive radiographic hip OA(Kelman et al. 2006). The same group found that change in NTX-I over 6 yearswas not significantly correlated with concurrent radiographic hip OA progression(Chaganti et al. 2008).
As collagen is degraded by osteoclast-derived proteases, non-reducible collagencross-links are released into the bloodstream and urine. These molecules, calledhydroxylysyl-pyridinoline (HYL-Pyr) or deoxypyridinoline (Dpd), are believed tooriginate from different tissues. Whereas HYL-Pyr is mainly derived from thecartilage (also bone, tendon, and vessel connective tissue), Dpd is derived almostexclusively from the bone and dentin (Lombardi et al. 2012). Overall, there havebeen few publications of these biochemical markers in human OA (van Spilet al. 2010). A study in the guinea pig model of knee OA, comparing a controlstrain (non-OA Strain 13) to an OA susceptible strain (Hartley), showed that theHartley strain had a higher rate of bone formation (based on sOC) and boneresorption (based on uHyl-Pyr and uDPD) at a young age with persistence of agreater rate of bone formation at 12 months of age (Huebner et al. 2002). Theresearch on the relationship between free urinary HYL-Pyr and Dpd and OA hasseemingly halted over the last decade. This may be the result of a paper written in2003 that found no significant correlations in a 3-year follow-up study of knee OAusing these biomarkers (Bruyere et al. 2003).
A study in the context of acute trauma to the anterior cruciate ligament showedincreased levels of collagen type I and II degradation markers (CTX, NTX, CTX-II)
Bone Biomarkers Related to Osteoarthritis 9
in synovial fluid. In turn, these levels correlated with serum levels (Catterallet al. 2010). Knee trauma in adolescence is a well-known risk factor for the laterdevelopment of OA (Lohmander et al. 2007) suggesting that these changes incollagen metabolism may be early triggers of OA. Connecting collagen typeI-derived biomarkers in serum or urine directly to clinical and/or radiological OAscores at the joint level however has been difficult. Thus, in general the bonecollagen-related biomarkers may be useful for predicting incident OA, particularlyincited by trauma, as well as progression of OA (Tables 2 and 3).
Other Collagenous Biomarkers
Collagen Type II
Collagen type II makes up 80–95 % of all protein in the articular cartilage. It istherefore a logical biomarker for following cartilage metabolism. Considering theobvious role of cartilage degradation in OA pathophysiology, degradation productsof collagen type II have shown great promise as OA biomarkers.
Although this might not seem directly relevant to a discussion of biomarkers ofthe bone, Eyre and Lohmander have suggested that uCTX-II probably originatesmostly from osteoclast-degraded mineralized collagen type II. Supporting a miner-alized tissue source for uCTX-II are data showing that levels are very low inindividuals with pycnodysostosis compared with age-matched controls (Lohmanderand Eyre 2008). Pycnodysostosis is a rare lysosomal storage disease of the bonecaused by mutation of the gene encoding the enzyme cathepsin K involved in boneresorption wherein osteoclasts function normally to demineralize the bone but do notadequately degrade the organic matrix.
Support for alterations of bone collagen type I metabolism involvement inincreased cartilage degradation was provided by a study of subjects with osteogen-esis imperfecta (a family of collagen type I mutations giving rise to fragile bones andfractures). In this study, patients with osteogenesis imperfecta had high uCTX-IIlevels similar to those of subjects with knee OA. In this same study, patients withknee OA had high ratios of alpha/beta uCTX-I (a marker indicating low collagentype I maturation) that were also associated with higher uCTX-II levels (Rousseauet al. 2010). A study by van Spil et al. has also made a strong argument regarding therelationship of uCTX-II and bone resorption (van Spil et al. 2013). In a study of theCHECK cohort (1002 knee and hip patients) with early OA, uCTX-II was morestrongly associated with the bone markers (uCTX-I, uNTX-I, sPINP, and sOC) thanwith other cartilage markers, and both uCTX-II and the bone markers showed anabrupt increase (“menopausal shift”) in women aged 48–53 years. This couldsuggest a cross talk between the cartilage and subchondral bone, or, as van Spilet al. suggest, this biomarker could represent osteoclastic resorption of the calcifiedcartilage. Further investigation is needed on the exact origin of this epitope to gain aclearer appreciation and understanding of the insights it provides in OA.
10 M.P. Engbersen et al.

Table
2Anov
erview
ofmentio
nedstud
iesregardingtype
1collagen-derivedbiom
arkers
Marker
Study
Assay
used
Mainou
tcom
eBIPEDS
catego
ryOA
site
Sou
rce
PIN
PBerry
etal.2
010
UniQ™
PIN
PRIA
;Orion
Diagn
ostica
Highlevelsof
PIN
Pareassociated
with
low
cartilage
loss
(P=
0.02
,n=
117)
Diagn
ostic
Knee
Serum
Davis
etal.2
007
Electrochem
iluminescence
immun
oassay,R
oche
Nosign
ificant
correlationwith
KL-score,
sclerosis,or
jointspacewidth
was
foun
d(n
=119)
–Knee
Serum
Kum
metal.2
013
Electrochem
iluminescence
immun
oassay,R
oche
Overthefirst3yearsof
follo
w-up,
sign
ificant
prog
nosticanddiagno
sticvaluewas
foun
d(n
=35
,P=
0.00
5andn=
33,P
=0.04
6);
only
aprog
nosticvalueforthelast3years
(n=
22,p
=0.02
2)
Progn
ostic/
diagno
stic
Knee
Serum
PIC
PSchmidt-
Roh
lfing
etal.2
002
ELISAkit;Metra
Biosystem
s,MB
004
PICPin
lavage
syno
vialfluidshow
edno
correlationwith
diseaseseverity
(n=
72)
–Knee
Syn
ovial
fluid
NTX
Bettica
etal.2
002
NTx,
Osteomark;
Ostex
Bon
eresorptio
nisincreasedin
prog
ressiveOA
andno
tinno
nprogressive
OAin
postmenop
ausal
wom
en(n
=21
6,P<
0.00
1)
Diagn
ostic
Knee
Urine
Kelman
etal.2
006
OsteomarkNTx
NTXassociated
with
anincreasedrisk
ofincident
radiog
raph
ichipOA(adjustedORof
1.38
perS
Dincrease
inNTX
(95%
CI1.07–1
.79),n
=39
7)
Progn
ostic
Hip
Serum
Chaganti
etal.2
008
ELISAkit,Osteomark
Nosign
ificant
concurrent
associationof
changes
inserum
NTX
over
6yearsandradiog
raph
ichip
OA
prog
ression(n
=67
7)
–Hip
Serum
Berry
etal.2
010
Serum
OsteomarkNTx,
Inverness
Medical
Highlevelsof
NTXareassociated
with
low
cartilage
loss
(P=
0.02
,n=
117)
Diagn
ostic
Knee
Urine
Blumenfeld
etal.2
013
OsteomarkNTxELISAkit,
InvernessMedicalInno
vatio
nsNTX
notsign
ificantly
associated
with
anyOA
phenotyp
esof
radiog
raph
ickn
eeOA
(n=
1007
wom
enon
ly)
–Knee
Urine
(con
tinued)
Bone Biomarkers Related to Osteoarthritis 11

Table
2(con
tinue
d)
Marker
Study
Assay
used
Mainou
tcom
eBIPEDS
catego
ryOA
site
Sou
rce
vanSpil
etal.2
013
OsteomarkNTxUrine,W
ampo
lelabo
ratories
NTX
was
strong
lyassociated
with
uCTX-II
(n=
1002
,p<
0.00
5)–
Hip&
knee
Urine
Tanishi
etal.2
014
OsteomarkNTxELISAkit,
InvernessMedicalInno
vatio
nsNosign
ificant
difference
betweenOA
grou
psby
KL-score
(n=
1200
)bu
thigh
estqu
artileof
subjectsbasedon
uNTXanduC
TXXIIwere
enriched
formoresevere
OA
(KL-score
�2)
Diagn
ostic
Knee
Urine
Kraus
etal.2
016
Com
petitiveinhibitio
nELISA,
ALERE-O
steomark(Inv
erness
Medical)
Tim
e-integrated
concentrationov
er12
and
24mon
thsof
both
serum
andurineNTX
predictedcombinedpain
andradiog
raph
icstructuralprog
ressionof
OA
over
4years
(n=
600)
Progn
ostic
Knee
Serum
andurine
CTX
Pelletier
etal.2
010
Serum
CrossLapsELISA,IDSLtd
Serum
values
ofCTXispredictiv
eof
ahigh
erBMLscore(n
=116,
P=
0.02
)Progn
ostic
Knee
Serum
Berry
etal.2
010
Serum
CrossLaps®
ELISA,IDS
Highlevelsof
CTXareassociated
with
low
cartilage
loss
(P=
0.01
,n=
117)
Progn
ostic
Knee
Serum
vanSpil
etal.2
013
Urine
CrossLapsEIA
,IDS
uCTX
was
strong
lyassociated
with
uCTX-II
(n=
1002
,p<
0.00
5)–
Hip
and
knee
Urine
Bartels
etal.2
014
Urine
CrossLaps®
EIA
,IDS
CTX-Iincreasedsign
ificantly
with
weigh
tloss
(P=
0.00
5,n=
192);CTX-Ichange
was
not
associated
with
thechangesin
KOOS-4
score
(n=
192)
–Knee
Urine
Huebn
eretal.2
014
Sandw
ichELISA,N
ordic
Bioscience
αCTXlevelswerecorrelated
with
theprog
ression
ofJSNandosteop
hytes,with
theintensity
ofbo
nescintig
raph
icup
take
(n=
117,
P=
0.04
1)
Progn
ostic
Knee
Urine
Kraus
etal.2
016
Serum
CrossLaps®
ELISA,IDS
Tim
e-integrated
concentrationov
er12
and
24mon
thspredictedcombinedpain
and
radiog
raph
icstructuralprog
ressionof
OAov
er4years(n
=60
0)
Progn
ostic
Knee
Serum
12 M.P. Engbersen et al.

Kraus
etal.2
016
Com
petitiveinhibitio
nELISA,alpha
andbetaCrossLaps(CTX-I),ID
SBaselineCTXIα
(resorptionof
thenewbo
ne)and
time-integrated
concentrationov
er12
and
24mon
thsCTXIα
andCTX-1β(resorptionof
the
olderbo
ne)predictedcombinedpain
and
radiog
raph
icstructuralprog
ressionof
OAov
er4years(n
=60
0)
Progn
ostic
Knee
Urine
ICTP
Berger
etal.2
005
Radioim
mun
oassay,O
rion
Diagn
ostica(FIN
-021
01Espoo
,Finland
)
IncreasedICTPin
OA
bone
butno
tserum
ofsubjectswith
rapidlydestructivehipOA
comparedwith
controls(n
=47
)
Diagn
ostic
Knee
Serum
HYL-
Pyr
Bruyere
etal.2
003
Pyrilink
s®competitiveenzyme
immun
oassays(EIA
),Metra
Biosystem
s
Nosign
ificant
correlations
foun
dbetweenthis
markerandjointspacewidth
orWOMACscore
atbaselin
eor
whencomparing
thechange
after
3years(n
=76
)
–Knee
Urine
Dpd
Bruyere
etal.2
003
Pyrilink
s-D™
competitiveenzyme
immun
oassays(EIA
),Metra
Biosystem
s
Nosign
ificant
correlations
foun
dbetweenthis
markerandjointspacewidth
orWOMACscore
atbaselin
eor
whencomparing
thechange
after
3years(n
=76
)
–Knee
Urine
Bone Biomarkers Related to Osteoarthritis 13
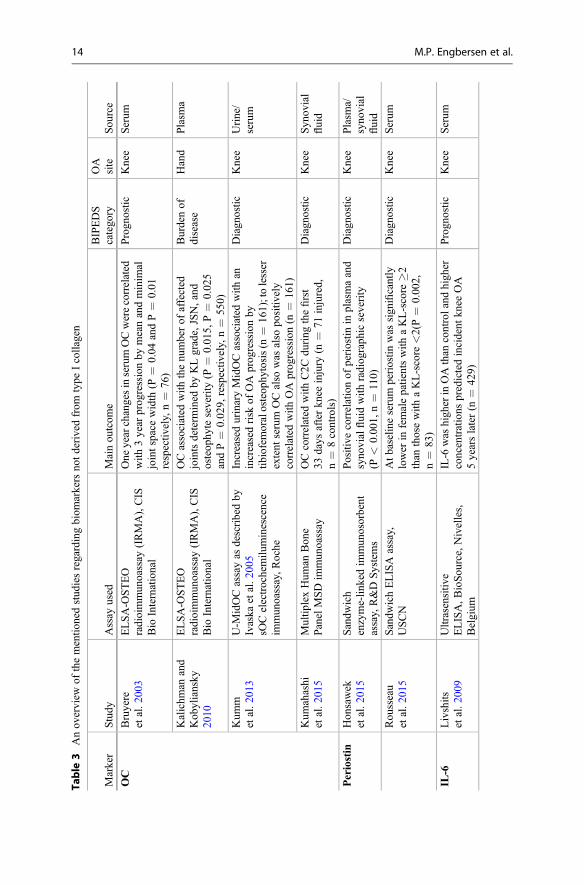
Table
3Anov
erview
ofthementio
nedstud
iesregardingbiom
arkersno
tderivedfrom
type
Icollagen
Marker
Study
Assay
used
Mainou
tcom
eBIPEDS
catego
ryOA
site
Sou
rce
OC
Bruyere
etal.2
003
ELSA-O
STEO
radioimmun
oassay
(IRMA),CIS
Bio
International
One
yearchangesinserumOCwerecorrelated
with
3year
prog
ressionby
meanandminim
aljointspacewidth
(P=
0.04
andP=
0.01
respectiv
ely,n=
76)
Progn
ostic
Knee
Serum
Kalichm
anand
Kob
yliansky
2010
ELSA-O
STEO
radioimmun
oassay
(IRMA),CIS
Bio
International
OCassociated
with
thenu
mberof
affected
jointsdeterm
ined
byKLgrade,JSN,and
osteop
hyteseverity
(P=
0.01
5,P=
0.02
5andP=
0.02
9,respectiv
ely,n=
550)
Burdenof
disease
Hand
Plasm
a
Kum
metal.2
013
U-M
idOCassayas
describedby
Ivaska
etal.2
005
sOCelectrochemilu
minescence
immun
oassay,R
oche
IncreasedurinaryMidOCassociated
with
anincreasedrisk
ofOA
prog
ressionby
tibiofemoralosteop
hytosis(n
=16
1);tolesser
extent
serum
OCalso
was
also
positiv
ely
correlated
with
OA
prog
ression(n
=16
1)
Diagn
ostic
Knee
Urine/
serum
Kum
ahashi
etal.2
015
Multip
lexHum
anBon
ePanelMSDim
mun
oassay
OCcorrelated
with
C2C
during
thefirst
33days
afterkn
eeinjury
(n=
71injured,
n=
8controls)
Diagn
ostic
Knee
Syn
ovial
fluid
Periostin
Hon
sawek
etal.2
015
Sandw
ich
enzyme-lin
kedim
mun
osorbent
assay,R&D
Systems
Positive
correlationof
periostin
inplasmaand
syno
vialfluidwith
radiog
raph
icseverity
(P<
0.00
1,n=
110)
Diagn
ostic
Knee
Plasm
a/syno
vial
fluid
Rou
sseau
etal.2
015
Sandw
ichELISA
assay,
USCN
Atbaselin
eserum
periostin
was
sign
ificantly
lower
infemalepatientswith
aKL-score
�2than
thosewith
aKL-score
<2(P=
0.00
2,n=
83)
Diagn
ostic
Knee
Serum
IL-6
Livshits
etal.2
009
Ultrasensitiv
eELISA,B
ioSou
rce,Nivelles,
Belgium
IL-6
was
high
erin
OAthan
controland
high
erconcentrations
predictedincident
knee
OA
5yearslater(n
=42
9)
Progn
ostic
Knee
Serum
14 M.P. Engbersen et al.
Stann
usetal.2
010a
Solid-phase,two-site
chem
iluminescent
enzymeim
mun
ometricassay,
Immulite
IL-6
(EURO/DPCLlanb
eris,
Gwyn
edd,
UK)
IL-6
was
associated
with
increasedmedial
tibiofemoraljointspacenarrow
ingand
predictedloss
ofbo
thmedialandlateraltib
ial
cartilage
volume,andchange
inIL-6
was
associated
with
increasedloss
ofmedialand
lateraltib
ialcartilage
volume
(n=
172)
Diagn
ostic,
prog
nostic
Knee
Serum
Stann
usetal.2
010b
Solid-phase,two-site
chem
iluminescent
enzymeim
mun
ometricassay,
Immulite
IL-6
(EURO/DPCLlanb
eris,
Gwyn
edd,
UK)
Serum
IL-6
associated
with
hipJSNinfemales
(N=
193)
Diagn
ostic
Hip
Serum
Oritaetal.2
011
IL-6
sand
wichELISA,R
&D
Systems
Syn
ovialfluidIL-6
negativ
elycorrelated
with
KLgradeandWOMACscore(n
=50
)Diagn
ostic
Knee
Syn
ovial
fluid
Rub
enhagen
etal.2
012
Multip
lexim
mun
oassay
8-plex,
R&D
Systems
Nocorrelationfoun
dwith
OA
byKL-score
(n=
82)
–Knee
Syn
ovial
fluid
Huebn
eretal.2
016
Sandw
ichELISA
assay,
MesoS
caleDiscovery
Weigh
tloss
was
respon
siblefor54
%of
the
redu
ctionin
IL-6
Efficacy
ofinterventio
nKnee
Serum
Leptin
Stann
usetal.2
010b
Radioim
mun
oassay
LIN
CO
Research;
now
partof
Millipore
Leptin
associated
with
JSNin
wom
en(P
=0.02
4andP=
0.00
2,respectiv
ely,
n=
193)
Diagn
ostic
Hip
Serum
DKK-1
Laneetal.2
007
Goatantih
uman
Dkk
-1capture
ELISA,R
&D
Systems
Higherlevelsof
Dkk
-1wereassociated
with
diminishedrisk
ofOA
prog
ressionin
elderly
wom
en(P
=0.00
7,n=
701)
Diagn
ostic,
prog
nostic
Hip
Serum
Hon
sawek
etal.2
010
Sandw
ichELISA,Q
uantikine,
R&D
Systems
Plasm
aandsyno
vialfluid(SF)Dkk
-1bo
thinverselycorrelated
with
radiog
raph
icseverity;bo
thcorrelated
(SF<
plasma);and
plasmaDKK-1
was
lower
than
control
(n=
35OA,1
5controls)
Diagn
ostic
Knee
Plasm
a,syno
vial
fluid
(con
tinued)
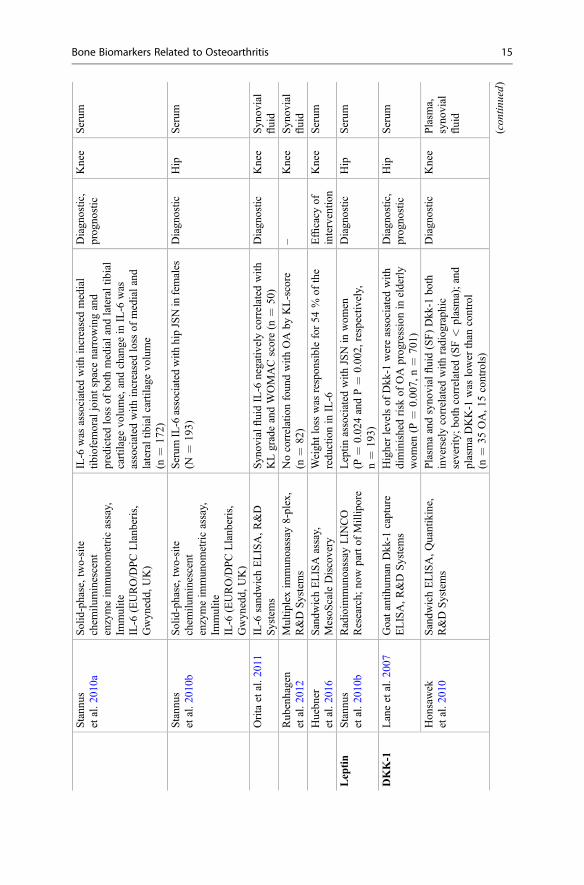
Bone Biomarkers Related to Osteoarthritis 15

Table
3(con
tinue
d)
Marker
Study
Assay
used
Mainou
tcom
eBIPEDS
catego
ryOA
site
Sou
rce
TRAP5b
Nwosu
etal.2
016
Immun
oenzym
aticassay
(Bon
eTRAP),ID
SSerum
TRAP5b
(detectstheactiv
eisoform
from
osteoclastsindicatin
gtheprocessof
bone
resorptio
n)associated
with
knee
pain,
subcho
ndralsclerosis,andpredictiv
eof
knee
pain
worsening
Diagn
ostic,
prog
nostic
Knee
Serum
ET-1
Nahiretal.1
991
Radioim
mun
oassay
Syn
ovialfluidET-1high
erin
OA
than
serum
ET-1in
controlsandsimilarto
syno
vialfluid
from
rheumatoidarthritis
(n=
7OA,n
=11
RA)
Diagn
ostic
Knee
Syn
ovial
fluid
BSP
Con
rozier
etal.1
998
Inhibitio
nELISA
(non
commercial)
Inversecorrelationof
BSPwith
severity
ofosteop
hyteandsclerosis(N
=48
)Diagn
ostic
Knee
Serum
Otterness
etal.2
000
ELISA
Nodifference
betweenOA
andcontrols
(n=
40)
–Knee
Serum
16 M.P. Engbersen et al.

Non-collagenous Biomarkers
Osteocalcin
Osteocalcin (OC), a non-collagenous and vitamin K-dependent protein, plays anactive role in the organization of the extracellular matrix. Osteocalcin is synthesizedby osteoblasts, odontoblasts, and hypertrophic chondrocytes (Hauschka et al. 1989).Its exact function remains unclear but it is widely regarded as a bone formationmarker. In vitro, subchondral OA osteoblasts have been shown to synthesize moreosteocalcin compared to normal osteoblasts (Couchourel et al. 2009).
Three-year radiological progression of knee OA could be predicted by a 1-yearincrease in serum OC (Bruyere et al. 2003). Plasma OC has been associated withseverity of hand OA based on KL grade and osteophyte grade (Kalichman andKobyliansky 2010). These two studies suggest that OC has prognostic and burden ofdisease value for knee and hand OA, respectively. One study reported no differencein serum OC comparing advanced hip OA patients sampled just prior to jointreplacement and labeled “controls” in contrast to patients with osteonecrosis of thefemoral head just prior to joint replacement (Floerkemeier et al. 2012). Interestingly,synovial fluid OC correlated with synovial fluid C2C, a type II collagen-specificbiomarker, during the first month after severe knee injury (Kumahashi et al. 2015).This observation is indicative of a simultaneous alteration in the bone and cartilageturnover in the earliest phases after joint injury suggesting that these biomarkers mayprovide means of monitoring possible development of posttraumatic OA.
The main route of circulating OC catabolism is renal filtration and degradation.Fragmented but not intact forms of OC have been found in urine (Ivaska et al. 2005).Ivaska et al. developed three OC immunoassays (urinary MidOC, LongOC, andTotalOC) to detect and quantify various molecular forms of urinary OC. In contrastto intact OC, which is a bone formation marker, fragments of OC are consideredbone resorption markers. High concentrations of all three analytes were negativelycorrelated with bone mass, and all three correlated with bone turnover rates assessedby conventional serum markers, CTX-I, bone alkaline phosphatase (ALP),TRACP5b, and total OC. No clear evidence for qualitative differences among theanalytes was observed in different clinical samples of elderly women distinguishedby different bone turnover rates. Higher urinary MidOC and serum OC were bothsubsequently associated with risk of knee osteophyte progression (Kummet al. 2013). Among the bone markers tested (serum PINP, CTX-I, and OC),MidOC was the strongest risk predictor of progressive osteophytosis. Takentogether, these results suggest that OC and urinary MidOC show the greatest promisefor use in OA.
Periostin
Periostin has only recently gained the attention of OA researchers. Like osteocalcin,periostin is also a vitamin K-dependent factor. Periostin, also called osteoblast-
Bone Biomarkers Related to Osteoarthritis 17

specific factor-2, is an integrin-binding protein, well known in the oncology fieldbecause of its involvement in cell adhesion and migration (Wong et al. 2013) andimplicated in bone healing. A transcriptomic study by Chou et al. showed that thePOSTN gene, which encodes periostin, was upregulated 15.65-fold in OAsubchondral bone as compared to non-OA bone (Chou et al. 2013b). Anotherstudy in humans and one in rats showed similar results (Chou et al. 2013a; Zhanget al. 2012). Increased synovial and plasma periostin levels were correlated withradiographic severity of knee OA (Honsawek et al. 2015). Oddly enough, serumlevels of periostin seemed to show an opposite effect. Periostin levels were lower inwomen with prevalent OA and in OA progressors compared to controls in theall-female, “Os des Femmes de Lyon” (OFELY) cohort (Rousseau et al. 2015).These two studies used a different sandwich ELISA and a different sample type tomeasure periostin levels. More research will be needed to clarify these seeminglycontradictory results.
Cytokine-Related Factors
An increasing evidence is emerging with regard to the role of inflammation in thepathogenesis of OA (Orlowsky and Kraus 2015). Dysregulation of the complementsystem is proven to play an important role (Wang et al. 2011). Obesity and diabetes,both risk factors of OA, are often associated with systemic inflammation, especiallywhen accompanied by metabolic syndrome. Subchondral plate bone loss is, in fact,associated with hypertension and type 2 diabetes mellitus (Wen et al. 2013). Below arole of certain cytokines that share a close relationship with the bone tissue in OA isdescribed.
Interleukin-6 (IL-6) plays a pro-inflammatory role in OA, and in the presence ofIL-1beta, TNF-alpha, and interferon gamma, expression is increased in chondrocytes(Bender et al. 1990; Guerne et al. 1990). Aside from its influence on chondrocytesand the cartilage, IL-6 induces bone resorption by acting as a stimulus to osteoclastdevelopment (Manolagas and Jilka 1995). In OA, IL-6 levels exhibit conflictingresults. In an animal (guinea pig) model of knee OA, serum IL-6 levels were higherin the OA group than controls (Huebner and Kraus 2006). In humans, synovial fluid(SF) IL-6 levels have been both negatively correlated (Orita et al. 2011) and notcorrelated (Rubenhagen et al. 2012) with knee OA severity based on KL grade. IL-6was associated with increased medial tibiofemoral joint space narrowing andpredicted loss of both medial and lateral tibial cartilage volume, and change inIL-6 was associated with increased loss of medial and lateral tibial cartilage volume(Stannus et al. 2010a). In women with hip OA, serum IL-6 correlated with jointspace narrowing but not with the presence of osteophytes (Stannus et al. 2010b). Inthe Chingford female cohort, serum IL-6 was higher in OA than control and higherconcentrations predicted incident knee OA 5 years later (Livshits et al. 2009). In theOA LIFE clinical trial in knee OA (n = 129 subjects with available longitudinalserum samples), the combination of pain coping skills training and lifestyle
18 M.P. Engbersen et al.

behavioral weight management for 6 months significantly reduced inflammatorymarkers including sIL-6, serum high sensitivity CRP, and leptin (Huebneret al. 2016). Reductions in leptin and IL-6 were significantly correlated withreductions in weight, BMI, and WOMAC pain; reductions in IL-6 were correlatedwith improvements in physical function. Weight loss was responsible for 54 % of thechange in IL-6. There are a number of possible explanations for mixed IL-6 results.For example, circadian rhythm could be influencing fluctuations in IL-6 levels.Modest sleep deprivation increases serum IL-6 (Mabey and Honsawek 2015). Theclinical trial results with serum IL-6 suggest that the inflammatory state in OA can bemonitored and successfully modified.
Leptin is an adipokine that influences bone metabolism by both a central pathway,via the hypothalamus, and a peripheral pathway, via osteoblast and bone marrowmesenchymal stem cells (Chen and Yang 2015). Leptin-deficient and leptin receptor-deficient mice have increased bone mass (Ducy et al. 2000). Central leptin seems topromote bone resorption, while peripheral leptin has a bone protective effect (Chenand Yang 2015). A role for leptin in OAwas first suggested in 2003 when increasedlevels of leptin were observed in OA synovial fluid and cartilage (Dumondet al. 2003). In the same study, the level of cartilage destruction was also correlatedwith increased leptin levels. Leptin expression was also found in various OA jointtissues such as synovial membranes, osteophytes, and infrapatellar fat tissues(Gegout et al. 2008). Interestingly, in osteophyte explants, the adiponectin/leptinratio was much higher compared to the other investigated tissues, suggesting a highlevel of leptin production in osteophytes. In subchondral osteoblasts of OA patients,leptin protein production was increased twofold and, gene expression, fivefoldcompared to non-OA osteoblasts (Mutabaruka et al. 2010). JSN grade correlatedpositively to serum concentration of leptin in a patient cohort of 193 individuals(Stannus et al. 2010b). In the aforementioned OA LIFE clinical trial, weight loss wasresponsible for all of the change in leptin (Huebner et al. 2016). These results showthe promise of leptin as a biomarker of not only cartilage damage but also ofsubchondral bone alterations. Even though leptin seems to be involved in thepathogenesis of OA, its systemic involvement in metabolic syndrome and obesitymay render it too nonspecific as a biomarker to be of clinical utility for OA.
Endothelin-1 (ET-1), a strong vasoconstrictor, induced by cytokines, has alsoproven to be an important factor in bone formation. Osteoblast-targeted endothelin Areceptor knockout mice typically exhibit decreased bone formation rate anddecreased osteoblast density (Clines et al. 2011). In RA, both synovial fluid andsET-1 are elevated compared with sET-1 of controls (Haq et al. 1999). In a small22 patient study, ET-1 was detectable and equivalent in SF of RA, OA, and acuteinflammatory arthritis; these values were twice that of plasma ET-1 from controls(Nahir et al. 1991). A recent review by Sin et al. suggests a central role of ET-1 in OApathogenesis owing to its role in osteoblast activation and elevation of sET-1 inobesity and diabetes that are known risk factors for OA (Sin et al. 2015). Because ofits involvement in bone formation, ET-1 may be a potential biomarker for early OAdevelopment and subchondral sclerosis.
Bone Biomarkers Related to Osteoarthritis 19

Bone Sialoprotein
Bone sialoprotein (BSP) is a highly conserved glycoprotein among mammals thatmakes up about 10 % of non-collagenous bone matrix protein. Expressed mainly bymature osteoblasts, it can activate osteoclasts, either directly or indirectly, via alpha(v) beta integrin (Nakamura et al. 2003). BSP plays a role in the nucleation ofhydroxyapatite (Yang et al. 2010), the major non-organic component of the bone,thus suggesting a role in bone mineralization (Lis 2008). In fact, BSP has beenidentified for a long time primarily as a bone and subchondral bone formationbiomarker (Wollheim 1999).
BSP has not been extensively researched as a biomarker. In a small study of39 subjects with large joint (hip or knee) OA, no significant difference in sBSP wasobserved comparing OA to control individuals (Otterness et al. 2000). Similarly, anolder study found that baseline levels of sBSP were unrelated to hip OA progression.However, an inverse correlation was found between sBSP level and osteophytegrade and sclerosis grade (Conrozier et al. 1998).
BSP was found to be associated with chondrocyte hypertrophy in OAchondrocytes and to promote cartilage angiogenesis. Hypertrophic differentiationof chondrocytes leads to secretion of proteases, chief among them MMP-13intimately associated with OA development and progression.BSP-immunoreactive chondrocytes in the cartilage were associated with the sever-ity of histological cartilage lesions, OA severity by Mankin grade and withvascular density at the osteochondral junction (Pesesse et al. 2014). These resultssuggest that this bone biomarker could also be a marker for cartilage alterations inthe context of OA, particularly as they relate to hypertrophic-like changes in OAchondrocytes.
DKK-1
Dickkopf WNT signaling pathway inhibitor 1 (Dkk-1) is a recently discoveredbiomarker that acts as a negative regulator of osteoblast development and activityby inhibiting the Wingless-related integration site (WNt) signaling pathway (Baronand Kneissel 2013). Serum Dkk-1 was measured in a cohort of 701 subjects dividedinto four groups: no radiographic hip OA, incident radiographic hip OA, stableradiographic OA, and progressive radiographic hip OA. Higher levels of Dkk-1 wereassociated with a diminished risk of OA progression (Lane et al. 2007). Honsaweket al. reported similar results in patients with knee OA. Dkk-1 levels were signifi-cantly lower in OA patients than in healthy controls, and both plasma and synovialDkk-1 were inversely correlated with radiographic severity (KL) (Honsaweket al. 2010). These results demonstrate both OA diagnostic and prognostic capabil-ities for Dkk-1.
20 M.P. Engbersen et al.

TRAP5b
Osteoclasts release the bone-degrading enzyme, tartrate-resistant acid phosphatase5b (TRAP5b), during bone resorption. In a cohort of 129 knee OA subjects, serumTRAP5b was significantly associated with knee pain and subchondral sclerosis andbaseline TRAP5b positively predicted knee pain worsening (Nwosu et al. 2016).These results suggest that TRAP5b may facilitate the selection of patients forinterventions targeting the bone component of the joint.
Bone Markers in Clinical Trials
ome of the bone marker candidates mentioned above have been evaluated in thecontext of OA clinical trials. Oral salmon calcitonin has consistently demonstratedsignificant reductions in the degradation markers, urinary and serum CTX-I andCTX-II, and modest but significant reductions in the bone formation marker, sOC(Karsdal et al. 2015; Karsdal et al. 2010b; Karsdal et al. 2010a; Bagger et al. 2005).Compared to placebo, vitamin D supplementation significantly increased serumalkaline phosphatase in patients with vitamin D insufficiency with knee OA (Sanghiet al. 2013). SheaFlex70, an extract of an African shea tree, reduced serumosteocalcin and uCTX-II in a 15-week OA trial; however mean concentrations ofeach of these biomarkers during the first week of treatment were higher in thetreatment group compared to placebo, so the subjects may not have been adequatelyrandomized; thus results must be interpreted with caution (Cheras et al. 2010).Another trial studying the relationship between biomarker changes and radiologicalOA progression in patients taking risedronate showed a dose-dependent reduction ofuNTX-I but no association of uNTX-I and radiological progression (Garneroet al. 2008).
Other Diseases
Although most of the abovementioned biomarkers are well known in other bone-related diseases, including osteoporosis, RA, osteosarcoma, and osteogenesisimperfecta (Lombardi et al. 2012), their use in OA appears promising for indicatingthe whole joint response during disease development and treatment. They candistinguish bone from cartilage metabolism and may have a particular role indifferentiating between OA patient phenotypes. They may also facilitate identifica-tion of drug targets and quantify target engagement in the case of bone-actingstructural modifying OA trials.
Bone Biomarkers Related to Osteoarthritis 21

Potential Applications to Prognosis
Up until now, none of the bone-derived biomarkers have been sufficient for thediagnosis and prognosis of OA, be it of the hand, knee, or hip. This reviewdemonstrates the difficulties and challenges in identifying reliable biomarkers ofOA (Wieland et al. 2005; Bijlsma et al. 2011; van Spil et al. 2010). There arechallenges in biomarker research in general that are not unique to the OA field.First, there is the issue of identifying the relationship between the systemic com-partment and the joint compartment. Many of the biomarkers are secreted in thesynovial fluid, blood, and even urine. Biomarker levels in the synovial fluid canreport on the local joint metabolism, while biomarkers in the blood may represent thetotal body burden of disease, which cannot be readily quantified by other modalities.Because whole body imaging to quantify OA burden is rarely feasible, it is partic-ularly challenging to qualify a biomarker against a gold standard representing thecontext of the total body burden of disease or disease progression.
Second, due to enzymatic and nonenzymatic modifications, most biomarkers inbody fluids exist in different forms. The biomarker assays used to detect a particularprotein often target different forms of the protein of interest. Thus, the results of themeasurements may only represent a portion of the total protein or protein fragmentconcentration.
Third, OA is now considered a disease with different phenotypes (pathogenicpathways). Each phenotype has its own characteristics with its own respectivebiomarkers or biomarker patterns. Therefore, it is ultimately important to be ableto qualify biomarkers in the context of specific and clear phenotypes. This is achicken and egg problem however, given the fact that the biomarkers themselvesmay be the best tools for differentiating specific phenotypes.
Fourth, the pathogenesis of OA has not been fully elucidated. Gaining moreknowledge in the field will greatly aid the understanding and interpretation of therole that specific biomarkers will have in a clinical setting. Future research shouldattempt to solve these issues to further advance the field and, eventually, find andfollow treatable targets and reduce patient burden of disease.
Although some bone-derived biomarkers have shown disappointing results forOA, others, like CTX-1, DKK-1, periostin, and osteocalcin, show great promise. Theability to overcome the challenges posed in biomarker research in general willdetermine the eventual role for bone-derived biomarkers in the clinic.
Summary Points
The recognition, summarized in this review, of the close interaction of the bone andcartilage in OA, provides a strong rationale for investigating bone changes in OAtrials. To date, osteocalcin and CTX-I have been the most widely studied biomarkersin OA studies and clinical trials. The results of these and other bone biomarkers inOA trials provide examples of the modifiability of the whole joint organ, demon-strating changes in bone metabolism and remodeling in the context of the evaluation
22 M.P. Engbersen et al.
of cartilage preservation. Future research is encouraged that continues and expandsthe use of biomarkers that holistically interrogate the whole joint organ, includingthe bone.
Key Facts of Osteoarthritis
– Osteoarthritis (OA) is the most common form of arthritis and a principal cause ofdisability.
– The prevalence of OA is increasing due to an aging world population (especiallyJapan, Europe, and North America).
– OA pathogenesis can be characterized as having disease (molecular,pre-radiographic, radiographic) and illness (symptomatic) phases.
– OA is a whole joint disease characterized by degeneration of the cartilage,menisci, and ligaments, subchondral bone changes, osteophyte formation, andsynovitis with significant cross talk between the cartilage and bone.
– A disease-modifying drug treatment for OA has yet to be approved.
References
Aigner T, Soder S, Gebhard PM, Mcalinden A, Haag J. Mechanisms of disease: role ofchondrocytes in the pathogenesis of osteoarthritis – structure, chaos and senescence. Nat ClinPract Rheumatol. 2007;3:391–9.
Aurich M, Squires GR, Reiner A, Mollenhauer JA, Kuettner KE, Poole AR, Cole AA. Differentialmatrix degradation and turnover in early cartilage lesions of human knee and ankle joints.Arthritis Rheum. 2005;52:112–9.
Bagger YZ, Tanko LB, Alexandersen P, Karsdal MA, Olson M, Mindeholm L, Azria M,Christiansen C. Oral salmon calcitonin induced suppression of urinary collagen type II degra-dation in postmenopausal women: a new potential treatment of osteoarthritis. Bone.2005;37:425–30.
Baron R, Kneissel M. Wnt signaling in bone homeostasis and disease: from human mutations totreatments. Nat Med. 2013;19:179–92.
Bartels EM, Christensen R, Christensen P, Henriksen M, Bennett A, Gudbergsen H, Boesen M,Bliddal H. Effect of a 16 weeks weight loss program on osteoarthritis biomarkers in obesepatients with knee osteoarthritis: a prospective cohort study. Osteoarthritis Cartilage.2014;22:1817–25.
Bauer DC, Hunter DJ, Abramson SB, Attur M, Corr M, Felson D, Heinegard D, Jordan JM, KeplerTB, Lane NE, Saxne T, Tyree B, Kraus VB. Classification of osteoarthritis biomarkers: aproposed approach. Osteoarthritis Cartilage. 2006;14:723–7.
Baxter I, Rogers A, Eastell R, Peel N. Evaluation of urinary N-telopeptide of type I collagenmeasurements in the management of osteoporosis in clinical practice. Osteoporos Int.2013;24:941–7.
Bender S, Haubeck HD, Van de Leur E, Dufhues G, Schiel X, Lauwerijns J, Greiling H, HeinrichPC. Interleukin-1 beta induces synthesis and secretion of interleukin-6 in human chondrocytes.FEBS Lett. 1990;263:321–4.
Berger CE, Kroner A, Stiegler H, Leitha T, Engel A. Elevated levels of serum type I collagenC-telopeptide in patients with rapidly destructive osteoarthritis of the hip. Int Orthop.2005;29:1–5.
Bone Biomarkers Related to Osteoarthritis 23

Berry PA, Maciewicz RA, Cicuttini FM, Jones MD, Hellawell CJ, Wluka AE. Markers of boneformation and resorption identify subgroups of patients with clinical knee osteoarthritis whohave reduced rates of cartilage loss. J Rheumatol. 2010;37:1252–9.
Bettica P, Cline G, Hart DJ, Meyer J, Spector TD. Evidence for increased bone resorption in patientswith progressive knee osteoarthritis: longitudinal results from the Chingford study. ArthritisRheum. 2002;46:3178–84.
Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice.Lancet. 2011;377:2115–26.
Blumenfeld O, Williams FM, Hart DJ, Spector TD, Arden N, Livshits G. Association betweencartilage and bone biomarkers and incidence of radiographic knee osteoarthritis (RKOA) in UKfemales: a prospective study. Osteoarthritis Cartilage. 2013;21:923–9.
Bruyere O, Collette JH, Ethgen O, Rovati LC, Giacovelli G, Henrotin YE, Seidel L, ReginsterJY. Biochemical markers of bone and cartilage remodeling in prediction of longterm progressionof knee osteoarthritis. J Rheumatol. 2003;30:1043–50.
Catterall JB, Stabler TV, Flannery CR, Kraus VB. Changes in serum and synovial fluid biomarkersafter acute injury (NCT00332254). Arthritis Res Ther. 2010;12:R229.
Chaganti RK, Kelman A, Lui L, Yao W, Javaid MK, Bauer D, Nevitt M, Lane NE, Study OFOsteoporotic Fractures Research Group, S. Change in serum measurements of cartilage oligo-meric matrix protein and association with the development and worsening of radiographic hiposteoarthritis. Osteoarthritis Cartilage. 2008;16:566–71.
Chen XX, Yang T. Roles of leptin in bone metabolism and bone diseases. J Bone Miner Metab.2015;33:474–485.
Cheras PA, Myers SP, Paul-Brent PA, Outerbridge KH, Nielsen GV. Randomized double-blindplacebo-controlled trial on the potential modes of action of SheaFlex70 in osteoarthritis.Phytother Res. 2010;24:1126–31.
Chou CH, Lee CH, Lu LS, Song IW, Chuang HP, Kuo SY, Wu JY, Chen YT, Kraus VB, Wu CC,Lee MT. Direct assessment of articular cartilage and underlying subchondral bone reveals aprogressive gene expression change in human osteoarthritic knees. Osteoarthritis Cartilage.2013a;21:450–61.
Chou CH, Wu CC, Song IW, Chuang HP, Lu LS, Chang JH, Kuo SY, Lee CH, Wu JY, Chen YT,Kraus VB, Lee MT. Genome-wide expression profiles of subchondral bone in osteoarthritis.Arthritis Res Ther. 2013b;15:R190.
Clines GA, Mohammad KS, Grunda JM, Clines KL, Niewolna M, Mckenna CR, MckibbinCR, Yanagisawa M, Suva LJ, Chirgwin JM, Guise TA. Regulation of postnatal trabecularbone formation by the osteoblast endothelin A receptor. J Bone Miner Res.2011;26:2523–36.
Cloos PA, Fledelius C. Collagen fragments in urine derived from bone resorption are highlyracemized and isomerized: a biological clock of protein aging with clinical potential. BiochemJ. 2000;345(Pt 3):473–80.
Clowes JA, Hannon RA, Yap TS, Hoyle NR, Blumsohn A, Eastell R. Effect of feeding on boneturnover markers and its impact on biological variability of measurements. Bone.2002;30:886–90.
Conrozier T, Saxne T, Fan CS, Mathieu P, Tron AM, Heinegard D, Vignon E. Serum concentrationsof cartilage oligomeric matrix protein and bone sialoprotein in hip osteoarthritis: a one yearprospective study. Ann Rheum Dis. 1998;57:527–32.
Couchourel D, Aubry I, Delalandre A, Lavigne M, Martel-Pelletier J, Pelletier JP, LajeunesseD. Altered mineralization of human osteoarthritic osteoblasts is attributable to abnormal type Icollagen production. Arthritis Rheum. 2009;60:1438–50.
Crema MD, Roemer FW, Zhu Y, Marra MD, Niu J, Zhang Y, Lynch JA, Javaid MK, Lewis CE,EL-Khoury GY, Felson DT, Guermazi A. Subchondral cystlike lesions develop longitu-dinally in areas of bone marrow edema-like lesions in patients with or at risk for kneeosteoarthritis: detection with MR imaging–the MOST study. Radiology.2010;256:855–62.
24 M.P. Engbersen et al.

Davis CR, Karl J, Granell R, Kirwan JR, Fasham J, Johansen J, Garnero P, Sharif M. Canbiochemical markers serve as surrogates for imaging in knee osteoarthritis? Arthritis Rheum.2007;56:4038–47.
Ducy P, Amling M, Takeda S, Priemel M, Schilling AF, Beil FT, Shen J, Vinson C, Rueger JM,Karsenty G. Leptin inhibits bone formation through a hypothalamic relay: a central control ofbone mass. Cell. 2000;100:197–207.
Dumond H, Presle N, Terlain B, Mainard D, Loeuille D, Netter P, Pottie P. Evidence for a key role ofleptin in osteoarthritis. Arthritis Rheum. 2003;48:3118–29.
Fardellone P, Sejourne A, Paccou J, Goeb V. Bone remodelling markers in rheumatoid arthritis.Mediators Inflamm. 2014;2014:484280.
Floerkemeier T, Hirsch S, Budde S, Radtke K, Thorey F, Windhagen H, Von Lewinski G. Boneturnover markers failed to predict the occurrence of osteonecrosis of the femoral head: apreliminary study. J Clin Lab Anal. 2012;26:55–60.
Funck-Brentano T, Cohen-Solal M. Subchondral bone and osteoarthritis. Curr Opin Rheumatol.2015;27:420–426.
Garnero P, Ferreras M, Karsdal MA, Nicamhlaoibh R, Risteli J, Borel O, Qvist P, Delmas PD,Foged NT, Delaisse JM. The type I collagen fragments ICTP and CTX reveal distinct enzymaticpathways of bone collagen degradation. J Bone Miner Res. 2003;18:859–67.
Garnero P, Aronstein WS, Cohen SB, Conaghan PG, Cline GA, Christiansen C, Beary JF, MeyerJM, Bingham CO, 3RD. Relationships between biochemical markers of bone and cartilagedegradation with radiological progression in patients with knee osteoarthritis receivingrisedronate: the Knee Osteoarthritis Structural Arthritis randomized clinical trial. OsteoarthritisCartilage. 2008;16:660–6.
Gegout PP, Francin PJ, Mainard D, Presle N. Adipokines in osteoarthritis: friends or foes ofcartilage homeostasis? Joint Bone Spine. 2008;75:669–71.
Goldring MB, Goldring SR. Articular cartilage and subchondral bone in the pathogenesis ofosteoarthritis. Ann N YAcad Sci. 2010;1192:230–7.
Guerne PA, Carson DA, Lotz M. IL-6 production by human articular chondrocytes. Modulation ofits synthesis by cytokines, growth factors, and hormones in vitro. J Immunol.1990;144:499–505.
Haq A, EL-Ramahi K, AL-Dalaan A, AL-Sedairy ST. Serum and synovial fluid concentrations ofendothelin-1 in patients with rheumatoid arthritis. J Med. 1999;30:51–60.
Hart DJ, Spector TD. Radiographic criteria for epidemiologic studies of osteoarthritis. J RheumatolSuppl. 1995;43:46–8.
Hauschka PV, Lian JB, Cole DE, Gundberg CM. Osteocalcin and matrix Gla protein: vitaminK-dependent proteins in bone. Physiol Rev. 1989;69:990–1047.
He T, Wu W, Huang Y, Zhang X, Tang T, Dai K. Multiple biomarkers analysis for the earlydetection of prosthetic aseptic loosening of hip arthroplasty. Int Orthop. 2013;37:1025–31.
Honsawek S, Tanavalee A, Yuktanandana P, Ngarmukos S, Saetan N, Tantavisut S. Dickkopf-1(Dkk-1) in plasma and synovial fluid is inversely correlated with radiographic severity of kneeosteoarthritis patients. BMC Musculoskelet Disord. 2010;11:257.
Honsawek S, Wilairatana V, Udomsinprasert W, Sinlapavilawan P, Jirathanathornnukul N. Associ-ation of plasma and synovial fluid periostin with radiographic knee osteoarthritis: cross-sectional study. Joint Bone Spine. 2015;82:352.
Huebner JL, Kraus VB. Assessment of the utility of biomarkers of osteoarthritis in the guinea pig.Osteoarthritis Cartilage. 2006;14:923–30.
Huebner JL, Hanes MA, Beekman B, Tekoppele JM, Kraus VB. A comparative analysis of boneand cartilage metabolism in two strains of guinea-pig with varying degrees of naturallyoccurring osteoarthritis. Osteoarthritis Cartilage. 2002;10:758–67.
Huebner JL, Bay-Jensen AC, Huffman KM, He Y, Leeming DJ, Mcdaniel GE, Karsdal MA, KrausVB. Alpha C-telopeptide of type I collagen is associated with subchondral bone turnover andpredicts progression of joint space narrowing and osteophytes in osteoarthritis. Arthritis Rheum.2014;66:2440–9.
Bone Biomarkers Related to Osteoarthritis 25

Huebner J, Landerman L, Somers T, Keefe F, Guilak F, Blumenthal J, Caldwell D, Kraus V.Exploratory secondary analyses of a cognitive-behavioral intervention for knee osteoarthritisdemonstrate reduction in biomarkers of adipocyte inflammation. Osteoarthr Cart. 2016;Apr 16.pii: S1063-4584(16)30015-2. doi: 10.1016/j.joca.2016.04.002.
Hunter DJ, Zhang W, Conaghan PG, Hirko K, Menashe L, Li L, Reichmann WM, Losina E.Systematic review of the concurrent and predictive validity of MRI biomarkers inOA. Osteoarthritis Cartilage. 2011;19:557–88.
Hunter DJ, Nevitt M, Losina E, Kraus V. Biomarkers for osteoarthritis: current position and stepstowards further validation. Best Pract Res Clin Rheumatol. 2014;28:61–71.
Ivaska KK, Käkönen S-M, Gerdhem P, Obrant KJ, Pettersson K, Väänänen HK. Urinaryosteocalcin as a marker of bone metabolism. Clin Chem. 2005;51:618–28.
Kalichman L, Kobyliansky E. Radiographic hand osteoarthritis and serum levels of osteocalcin:cross-sectional study. Rheumatol Int. 2010;30:1131–5.
Karsdal MA, Byrjalsen I, Henriksen K, Riis BJ, Christiansen C. Investigations of inter- andintraindividual relationships between exposure to oral salmon calcitonin and a surrogate markerof pharmacodynamic efficacy. Eur J Clin Pharmacol. 2010a;66:29–37.
Karsdal MA, Byrjalsen I, Henriksen K, Riis BJ, Lau EM, Arnold M, Christiansen C. The effectof oral salmon calcitonin delivered with 5-CNAC on bone and cartilage degradation inosteoarthritic patients: a 14-day randomized study. Osteoarthritis Cartilage.2010b;18:150–9.
Karsdal MA, Bay-Jensen AC, Lories RJ, Abramson S, Spector T, Pastoureau P, Christiansen C,Attur M, Henriksen K, Goldring SR, Kraus V. The coupling of bone and cartilage turnover inosteoarthritis: opportunities for bone antiresorptives and anabolics as potential treatments? AnnRheum Dis. 2014;73:336–48.
Karsdal MA, Byrjalsen I, Alexandersen P, Bihlet A, Andersen JR, Riis BJ, Bay-Jensen AC,Christiansen C. Treatment of symptomatic knee osteoarthritis with oral salmon calcitonin:results from two phase 3 trials. Osteoarthritis Cartilage. 2015;23:532–43.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis.1957;16:494–502.
Kelman A, Lui L, Yao W, Krumme A, Nevitt M, Lane NE. Association of higher levels of serumcartilage oligomeric matrix protein and N-telopeptide crosslinks with the development ofradiographic hip osteoarthritis in elderly women. Arthritis Rheum. 2006;54:236–43.
Koivula MK, Risteli L, Risteli J. Measurement of aminoterminal propeptide of type I procollagen(PINP) in serum. Clin Biochem. 2012;45:920–7.
Kraus VB, Feng S, Wang S, White S, Ainslie M, Brett A, Holmes A, Charles HC. Trabecularmorphometry by fractal signature analysis is a novel marker of osteoarthritis progression.Arthritis Rheum. 2009;60:3711–22.
Kraus VB, Burnett B, Coindreau J, Cottrell S, Eyre D, Gendreau M, Gardiner J, Garnero P,Hardin J, Henrotin Y, Heinegard D, Ko A, Lohmander LS, Matthews G, Menetski J,Moskowitz R, Persiani S, Poole AR, Rousseau JC, Todman M. Application of biomarkers inthe development of drugs intended for the treatment of osteoarthritis. Osteoarthritis Cartilage.2011;19:515–42.
Kraus VB, Feng S, Wang S, White S, Ainslie M, Graverand MP, Brett A, Eckstein F, Hunter DJ,Lane NE, Taljanovic MS, Schnitzer T, Charles HC. Subchondral bone trabecular integritypredicts and changes concurrently with radiographic and magnetic resonance imaging-determined knee osteoarthritis progression. Arthritis Rheum. 2013;65:1812–21.
Kraus VB, Blanco FJ, Englund M, Karsdal MA, Lohmander LS. Call for standardized definitions ofosteoarthritis and risk stratification for clinical trials and clinical use. Osteoarthritis Cartilage.2015;23:1233–41.
Kraus V, Collins J, Hargrove D, Losina E, Nevitt M, Katz J, Wang S, Sandell L, Hoffman S,Hunter D. Predictive validity of biochemical biomarkers in knee osteoarthritis – data from theFNIH OA biomarkers consortium. Ann Rheum Dis. 2016; Jun 13. pii: annrheumdis-2016-209252. doi: 10.1136/annrheumdis-2016-209252.
26 M.P. Engbersen et al.

Kumahashi N, Sward P, Larsson S, Lohmander LS, Frobell R, Struglics A. Type II collagen C2Cepitope in human synovial fluid and serum after knee injury – associations with molecular andstructural markers of injury. Osteoarthr Cart. 2015;Sep;23(9):1506–12.
Kumm J, Tamm A, Lintrop M, Tamm A. Diagnostic and prognostic value of bone biomarkers inprogressive knee osteoarthritis: a 6-year follow-up study in middle-aged subjects. OsteoarthritisCartilage. 2013;21:815–22.
Lane NE, Nevitt MC, Lui LY, de Leon P, Corr M. Wnt signaling antagonists are potential prognosticbiomarkers for the progression of radiographic hip osteoarthritis in elderly Caucasian women.Arthritis Rheum. 2007;56:3319–25.
Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, Gabriel S, Hirsch R,Hochberg MC, Hunder GG, Jordan JM, Katz JN, Kremers HM, Wolfe F, National Arthritis DataW. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States.Part II. Arthritis Rheum. 2008;58:26–35.
Lis K. Bone sialoprotein in laboratory diagnostic work-up of osteoarthritis. Ortop TraumatolRehabil. 2008;10:211–7.
Livshits G, Zhai G, Hart DJ, Kato BS, Wang H, Williams FM, Spector TD. Interleukin-6 is asignificant predictor of radiographic knee osteoarthritis: the chingford study. Arthritis Rheum.2009;60:2037–45.
Lohmander L, Eyre D. Biochemical markers as surrogate end points of joint disease. In: Reid D,Miller C, editors. Clinical trials in rheumatoid arthritis and osteoarthritis. New York: Springer;2008.
Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciateligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35:1756–69.
Lombardi G, Lanteri P, Colombini A, Banfi G. Blood biochemical markers of bone turnover:pre-analytical and technical aspects of sample collection and handling. Clin Chem Lab Med.2012;50:771–89.
Mabey T, Honsawek S. Cytokines as biochemical markers for knee osteoarthritis. World J Orthod.2015;6:95–105.
Manolagas SC, Jilka RL. Bone marrow, cytokines, and bone remodeling. Emerging insights into thepathophysiology of osteoporosis. N Engl J Med. 1995;332:305–11.
Mutabaruka MS, Aoulad Aissa M, Delalandre A, Lavigne M, Lajeunesse D. Local leptin produc-tion in osteoarthritis subchondral osteoblasts may be responsible for their abnormal phenotypicexpression. Arthritis Res Ther. 2010;12:R20.
Nagaosa Y, Mateus M, Hassan B, Lanyon P, Doherty M. Development of a logically devised linedrawing atlas for grading of knee osteoarthritis. Ann Rheum Dis. 2000;59:587–95.
Nahir AM, Hoffman A, Lorber M, Keiser HR. Presence of immunoreactive endothelin in synovialfluid: analysis of 22 cases. J Rheumatol. 1991;18:678–80.
Nakamura I, Rodan GA, Duong Le T. Regulatory mechanism of osteoclast activation. J ElectronMicrosc (Tokyo). 2003;52:527–33.
Nwosu L, Chapman V, Walsh D, Kraus V. Subchondral bone biomarkers as predictors of OA painprogression; linking structural pathology and pain. Osteoarthr Cart. 2016; 24(S51):73.
Orita S, Koshi T, Mitsuka T, Miyagi M, Inoue G, Arai G, Ishikawa T, Hanaoka E, Yamashita K,Yamashita M, Eguchi Y, Toyone T, Takahashi K, Ohtori S. Associations betweenproinflammatory cytokines in the synovial fluid and radiographic grading and pain-relatedscores in 47 consecutive patients with osteoarthritis of the knee. BMC Musculoskelet Disord.2011;12:144.
Orlowsky EW, Kraus VB. The role of innate immunity in osteoarthritis: when our first line ofdefense goes on the offensive. J Rheumatol. 2015;42:363–71.
Otterness IG, Swindell AC, Zimmerer RO, Poole AR, Ionescu M, Weiner E. An analysis of14 molecular markers for monitoring osteoarthritis: segregation of the markers into clustersand distinguishing osteoarthritis at baseline. Osteoarthritis Cartilage. 2000;8:180–5.
Pelletier JP, Raynauld JP, Caron J, Mineau F, Abram F, Dorais M, Haraoui B, Choquette D, Martel-Pelletier J. Decrease in serum level of matrix metalloproteinases is predictive of the disease-
Bone Biomarkers Related to Osteoarthritis 27

modifying effect of osteoarthritis drugs assessed by quantitative MRI in patients with kneeosteoarthritis. Ann Rheum Dis. 2010;69:2095–101.
Pesesse L, Sanchez C, Walsh DA, Delcour JP, Baudouin C, Msika P, Henrotin Y. Bone sialoproteinas a potential key factor implicated in the pathophysiology of osteoarthritis. OsteoarthritisCartilage. 2014;22:547–56.
Research MFFMEA. Test ID: PINP (Procollagen I Intact N-Terminal, Serum). 2015. Available:http://www.mayomedicallaboratories.com/test-catalog/Clinical+and+Interpretive/61695.Accessed 28 Dec 2015.
Rousseau JC, Sandell LJ, Delmas PD, Garnero P. Development and clinical application in arthritisof a new immunoassay for serum type IIA procollagen NH2 propeptide. Methods Mol Med.2004;101:25–37.
Rousseau JC, Chevrel G, Schott AM, Garnero P. Increased cartilage type II collagen degradation inpatients with osteogenesis imperfecta used as a human model of bone type I collagen alterations.Bone. 2010;46:897–900.
Rousseau JC, Sornay-Rendu E, Bertholon C, Garnero P, Chapurlat R. Serum periostin is associatedwith prevalent knee osteoarthritis and disease incidence/progression in women: the OFELYstudy. Osteoarthritis Cartilage. 2015;23:1736–1742.
Rubenhagen R, Schuttrumpf JP, Sturmer KM, Frosch KH. Interleukin-7 levels in synovial fluidincrease with age and MMP-1 levels decrease with progression of osteoarthritis. Acta Orthop.2012;83:59–64.
Sanghi D, Mishra A, Sharma AC, Singh A, Natu SM, Agarwal S, Srivastava RN. Does vitamin Dimprove osteoarthritis of the knee: a randomized controlled pilot trial. Clin Orthop Relat Res.2013;471:3556–62.
Schmidt-Rohlfing B, Thomsen M, Niedhart C, Wirtz D, Schneider U. Correlation of bone andcartilage markers in the synovial fluid with the degree of osteoarthritis. Rheumatol Int.2002;21:193–9.
Sharma AR, Jagga S, Lee SS, Nam JS. Interplay between cartilage and subchondral bone contrib-uting to pathogenesis of osteoarthritis. Int J Mol Sci. 2013;14:19805–30.
Sin A, Tang W, Wen CY, Chung SK, Chiu KY. The emerging role of endothelin-1 in thepathogenesis of subchondral bone disturbance and osteoarthritis. Osteoarthritis Cartilage.2015;23:516–24.
Stannus O, Jones G, Cicuttini F, Parameswaran V, Quinn S, Burgess J, Ding C. Circulating levels ofIL-6 and TNF-alpha are associated with knee radiographic osteoarthritis and knee cartilage lossin older adults. Osteoarthritis Cartilage. 2010a;18:1441–7.
Stannus OP, Jones G, Quinn SJ, Cicuttini FM, Dore D, Ding C. The association between leptin,interleukin-6, and hip radiographic osteoarthritis in older people: a cross-sectional study.Arthritis Res Ther. 2010b;12:R95.
Tanishi N, Yamagiwa H, Hayami T, Mera H, Koga Y, Omori G, Endo N. Usefulness of urinaryCTX-II and NTX-I in evaluating radiological knee osteoarthritis: the Matsudai knee osteoar-thritis survey. J Orthop Sci. 2014;19:429–36.
Valdes AM, Meulenbelt I, Chassaing E, Arden NK, Bierma-Zeinstra S, Hart D, Hofman A,Karsdal M, Kloppenburg M, Kroon HM, Slagboom EP, Spector TD, Uitterlinden AG, VanMeurs JB, Bay-Jensen AC. Large scale meta-analysis of urinary C-terminal telopeptide, serumcartilage oligomeric protein and matrix metalloprotease degraded type II collagen and their rolein prevalence, incidence and progression of osteoarthritis. Osteoarthritis Cartilage.2014;22:683–9.
Van Spil WE, Degroot J, Lems WF, Oostveen JC, Lafeber FP. Serum and urinary biochemicalmarkers for knee and hip-osteoarthritis: a systematic review applying the consensus BIPEDcriteria. Osteoarthritis Cartilage. 2010;18:605–12.
Van Spil WE, Drossaers-Bakker KW, Lafeber FP. Associations of CTX-II with biochemicalmarkers of bone turnover raise questions on its tissue origin: data from CHECK, a cohortstudy of early osteoarthritis. Ann Rheum Dis. 2013;72:29–36.
28 M.P. Engbersen et al.

Vasikaran S, Cooper C, Eastell R, Griesmacher A, Morris HA, Trenti T, Kanis JA. InternationalOsteoporosis Foundation and International Federation of Clinical Chemistry and LaboratoryMedicine position on bone marker standards in osteoporosis. Clin Chem Lab Med.2011;49:1271–4.
Wang Q, Rozelle AL, Lepus CM, Scanzello CR, Song JJ, Larsen DM, Crish JF, Bebek G, Ritter SY,Lindstrom TM, Hwang I, Wong HH, Punzi L, Encarnacion A, Shamloo M, Goodman SB, Wyss-Coray T, Goldring SR, Banda NK, Thurman JM, Gobezie R, Crow MK, Holers VM, Lee DM,Robinson WH. Identification of a central role for complement in osteoarthritis. Nat Med.2011;17:1674–9.
Wen CY, Chen Y, Tang HL, Yan CH, Lu WW, Chiu KY. Bone loss at subchondral plate in kneeosteoarthritis patients with hypertension and type 2 diabetes mellitus. Osteoarthritis Cartilage.2013;21:1716–23.
Wieland HA, Michaelis M, Kirschbaum BJ, Rudolphi KA. Osteoarthritis – an untreatable disease?Nat Rev Drug Discov. 2005;4:331–44.
Wollheim FA. Bone sialoprotein-a new marker for subchondral bone. Osteoarthritis Cartilage.1999;7:331–2.
Wong GS, Lee JS, Park YY, Klein-Szanto AJ, Waldron TJ, Cukierman E, Herlyn M, Gimotty P,Nakagawa H, Rustgi AK. Periostin cooperates with mutant p53 to mediate invasion through theinduction of STAT1 signaling in the esophageal tumor microenvironment. Oncogenesis. 2013;2:e59.
Xu L, Hayashi D, Roemer FW, Felson DT, Guermazi A. Magnetic resonance imaging ofsubchondral bone marrow lesions in association with osteoarthritis. Semin Arthritis Rheum.2012;42:105–18.
Yang Y, Cui Q, Sahai N. How does bone sialoprotein promote the nucleation of hydroxyapatite? Amolecular dynamics study using model peptides of different conformations. Langmuir.2010;26:9848–59.
Zhang Y, Nevitt M, Niu J, Lewis C, Torner J, Guermazi A, Roemer F, Mcculloch C, FelsonDT. Fluctuation of knee pain and changes in bone marrow lesions, effusions, and synovitis onmagnetic resonance imaging. Arthritis Rheum. 2011;63:691–9.
Zhang R, Fang H, Chen Y, Shen J, Lu H, Zeng C, Ren J, Zeng H, Li Z, Chen S, Cai D, Zhao Q. Geneexpression analyses of subchondral bone in early experimental osteoarthritis by microarray.PLoS One. 2012;7:e32356.
Bone Biomarkers Related to Osteoarthritis 29