body compositional and cardiometabolic effects of testosterone
TRANSCRIPT
1
Body compositional and cardiometabolic effects of testosterone therapy in obese men
with severe obstructive sleep apnea: a randomised placebo-controlled trial
Camilla M Hoyos1 BAppSc (Hons), MPH (Hons), PhD, Brendon J Yee1,2,3 MBChB,
FRACP, PhD, Craig L Phillips1,4 PhD, Elizabeth A Machan1 BAppSc (Hons), Ronald R
Grunstein2,3, MB BS, FRACP, MD, PhD, Peter Y Liu1,5 MB BS (Hons), FRACP, PhD*.
Endocrine and Cardiometabolic Research Group1 and Sleep and Circadian Research Group2, NHMRC Centre for Integrated Research and Understanding of Sleep (CIRUS) Woolcock Institute of Medical Research, University of Sydney and Royal Prince Alfred Hospital3 and Royal North Shore Hospital4 and Division of Endocrinology, Department of Medicine, David Geffen School of Medicine at UCLA, Harbor-UCLA Medical Center and Los Angeles Biomedical Research Institute
5
Word Count=3847
Running Title: Testosterone on Cardiometabolic Health
Keywords: Androgen Deficiency; Testosterone supplementation; Obstructive Sleep Apnea; Body
Composition; Cardiometabolic Health
*To whom correspondence should be addressed
Peter Y. Liu, Division of Endocrinology, Department of Medicine, David Geffen School of Medicine
at UCLA, Harbor-UCLA Medical Center and Los Angeles Biomedical Research Institute, 1000 W
Carson Street Torrance CA 90502
Tel: +1-310-222-1867
Fax: +1-310-533-0627
Page 1 of 31 Accepted Preprint first posted on 30 July 2012 as Manuscript EJE-12-0525
Copyright © 2012 European Society of Endocrinology.

2
Abstract
Background: The combination of male gender, obstructive sleep apnea (OSA) and obesity
magnifies cardiometabolic risk. There has been no systematic study evaluating whether
testosterone therapy can improve cardiometabolic health in obese men with OSA by
improving body composition, visceral abdominal fat and insulin sensitivity.
Objective: To assess body compositional and cardiometabolic effects of testosterone
treatment in obese men with severe OSA.
Design: An 18-week randomized, double blind, placebo-controlled, parallel group trial in 67
men.
Methods: Participants (age=49 ± 12years, apnea hypopnea index (AHI) =39.9 ± 17.7
events/hour, body mass index=31.3 ± 5.2 kg/m2) were placed on a hypocaloric diet and
received intramuscular injections of either 1000mg testosterone undecanoate (n=33) or
placebo (n=34) for 18 weeks. Outcomes were the changes in body composition (total muscle
mass; total and abdominal fat (total body dual-energy X-ray absorptiometry and
computerised tomography), weight, insulin sensitivity (homeostasis model assessment),
abdominal liver fat (computerised tomography), arterial stiffness (pulse wave analysis),
resting metabolic rate and respiratory quotient (indirect calorimetry), blood lipids and
metabolic syndrome from baseline to week 18.
Results: After 18 weeks, testosterone treatment increased insulin sensitivity (-1.14 units, -
2.27 to -0.01 95%CI, p<0.05), reduced liver fat (0.09 Hounsfield attenuation ratio, 0.009 to
0.17 95%CI, p=0.03) and increased muscle mass (1.6kg, 0.69 to 2.5 95%CI, p=0.0009) to a
greater extent than placebo. Other measures of body composition and regional adiposity as
well as the number of participants with metabolic syndrome did not change. Testosterone also
decreased arterial stiffness (augmentation index) by 3.2% (-6.01% to -0.46% 95%CI, p=0.02)
Page 2 of 31

3
and decreased the respiratory quotient (-0.04, -0.08 to -0.001 95%CI, p=0.04) after 18 weeks
compared to placebo.
Conclusion: Eighteen weeks of testosterone therapy in obese men with OSA improved
several important cardiometabolic parameters but did not differentially reduce overall weight
or the metabolic syndrome. Longer term studies are required.
Page 3 of 31

4
Introduction
Obesity occurs in 32% of all men in the USA 1 and many of these men develop obstructive
sleep apnea (OSA) 2, 3. The resulting intermittent hypoxia amplifies the cardiometabolic risk
of obesity by promoting atherogenesis through mechanisms that include inhibition of
triglyceride clearance, inactivation of lipoprotein lipase and induction of insulin resistance 4, 5
6. Indeed, all cause 7, 8 and cardiovascular 8, 9 mortality is amplified when untreated OSA is
combined with coexisting obesity and male gender . Understanding the mechanisms and
methods by which cardiometabolic risk may be reduced in this specific obese population is
therefore important.
Testosterone treatment increases muscle and decreases fat in hypogonadal and eugonadal
males 10, as well as in men with relative androgen deficiency related to age 11 or HIV 12. In
addition, testosterone therapy decreases visceral abdominal fat (VAF) 13-15
and improves
insulin sensitivity 16-20 in some, but not all 21-26 studies. Specific characteristics of the
populations studied may contribute to these discrepancies. Improved body composition
would be expected to improve cardiometabolic health including insulin sensitivity, VAF,
non-alcoholic fatty liver disease (NAFLD) and metabolic syndrome. No single study has
assessed the effect of testosterone on both radiographically measured VAF and liver fat 16
.
Few studies have assessed the impact of testosterone therapy on the metabolic syndrome 16.
Conversely, biochemical androgen deficiency is associated with increased cardiovascular
events 26 and testosterone therapy has been shown to improve arterial stiffness, an early
marker of atherosclerosis, in men with coronary artery disease or advanced age 27, 28.
Biochemical androgen deficiency is common in men with OSA 29, 30
, is more severe with
increasing hypoxemia and can be partly reversed by continuous positive airway pressure
therapy 31. Biochemical androgen deficiency is also common in obese men 29, especially with
Page 4 of 31

5
increasing adiposity 32
and can be partly reversed with weight loss 33, 34
. These data suggest
that men who are obese or who have OSA have some degree of relative androgen deficiency
29. Whether testosterone therapy is beneficial in these men requires direct evaluation by
randomised placebo controlled trials in this population.
Prior research has suggested that testosterone therapy may improve cardiometabolic risk in
older men with chronic heart failure 18
, abdominally obese men 14, 15
, and men with the
metabolic syndrome and/or diabetes 16, 17, 20, 35, 36, but may increase cardiovascular risk in frail
older men with limited mobility 37. Since the effect of testosterone therapy on
cardiometabolic risk has not been systematically studied in obese men with OSA who are at
magnified cardiometabolic risk and who have some degree of relative androgen deficiency,
we undertook a randomised placebo-controlled trial to directly determine this. We measured
change in anthropometry, abdominal visceral fat, total body fat and lean muscle, basal
metabolic rate, insulin sensitivity, blood lipids, and metabolic syndrome status. These
assessments included more precise measures of cardiometabolic risk including
radiographically determined liver fat and tonometry determined arterial stiffness. The effects
of testosterone therapy on sleep and breathing in this study have recently been published 38
.
Page 5 of 31

6
Subjects and Methods
Participants and Study Design
The entry criteria has been previously described in our report of respiratory effects 38. In
brief eligible participants were adult obese men with OSA, defined as aged 18 years or over,
body mass index >30kg/m2 and apnea hypopnea index (AHI) >10 events/hr by in-laboratory
polysomnography.
This was a randomised double-blind, placebo controlled, parallel group study. Eligible
participants were randomly assigned to receive intramuscular injections of either Reandron™
(Testosterone undecanoate 1000mg in 4ml castor oil vehicle, Bayer Schering) or 4ml oil
vehicle placebo at 0, 6 and 12 weeks. All participants were concurrently enrolled in a
lifestyle modification program in which a dietitian prescribed a 2500kJ (600kcal) daily deficit
diet based on a macronutrient content of <30% fat (with emphasis on reducing saturated fat in
the diet), 15% protein, and at least 55% carbohydrate. Advice on behavioural modification
and physical activity was also provided 38. At randomisation, subjects received a number in
ascending order that corresponded with a pre-numbered and pre-packaged treatment kit. A
computer-generated randomisation list was created using a block size of four. Subjects were
assigned to active medication or placebo in a 1:1 ratio. All researchers involved in the
conduct of the study were blinded to the treatment allocation for the duration of the study.
All subjects provided written informed consent and both the patient information sheet and
study protocol were approved by the Sydney South West Area Health Service Human
Research and Ethics Committee (Royal Prince Alfred Hospital Zone). The study is registered
with the Australia New Zealand Clinical Trials Network, number ACTRN12606000404527.
Page 6 of 31

7
Measurements
Anthropometry
Height and weight as well as waist, hip, neck, mid-arm and mid-thigh circumferences were
measured according to anthropometric recommendations 39 at each visit by a single observer.
Imaging
Body composition included measures of abdominal, liver and total fat and total lean muscle
mass by computerised tomography (CT) and dual-energy X-ray absorptiometry (DXA)
scanning which were performed at 0 and 18 weeks. Two 10mm contiguous images of both
the upper (T12) and lower (L4) abdomen were obtained by CT (16 slice light speed extra, GE
healthcare, Madison, Wisconsin, USA). The volumes of subcutaneous and visceral abdominal
fat (SCAF and VAF, respectively) in the abdomen were quantified using a validated software
tool (Hippofat™; CNR Institute of Clinical Physiology, Pisa, Italy) 40. Total fat and lean mass
were measured by total body DXA (Lunar Prodigy GE healthcare, Madison, Wisconsin,
USA).
Liver fat was estimated by liver and spleen Hounsfield unit attenuations (E-FILM™, Merge
Healthcare Milwaukee, Wisconsin, USA) from unenhanced CT slices in several homogenous
areas (≥ 10 cm2) that were adjacent to the T12/ L1 intervertebral space and free of
vasculature. The liver to spleen attenuation ratio (L/S ratio) was used to estimate liver fat 41.
A higher ratio indicates a lower liver fat content. Arterial stiffness and central blood pressure
were measured at 0, 6 and 18 weeks in the supine position by pulse wave analysis (PWA,
Sphymo-Cor; AtCor Medical; Sydney, NSW, Australia), a method that our group has
previously implemented in another study 41. A validated transfer algorithm was used to
calculate the aortic augmentation index (AIx), which is the ratio of the augmentation pressure
Page 7 of 31
8
(due to the reflected component of the pulse pressure wave) to pulse pressure, expressed as a
percentage. Resting metabolic rate and the respiratory quotient were determined by indirect
calorimetry (Delta Trak II Metabolic Monitor, Datex-Ohmeda Inc., Madison, Wisconsin,
USA).
Blood
Fasting venous blood was collected in the early morning at each visit. Standard biochemistry
and hematology panels, insulin, leptin, sex hormone-binding globulin and prostate-specific
antigen were all analysed by platform assays while low-density lipoprotein (LDL)-cholesterol
was calculated by the Friedewald equation 42. Blood glucose was determined by the
hexokinase method (Modular P®, Roche Diagnostics, Castle Hill, Australia) from blood
collected in sodium fluoride (Vacutainer; Becton Dickinson, Rutherford, NJ). Insulin
sensitivity was calculated by the homeostasis model assessment (HOMA-IR) method 43.
Luteinizing hormone and follicle-stimulating hormone concentrations were measured by
commercially available Delfia assays (Perkin-Elmer Life Sciences, Rowville, Australia) and
total testosterone by mass spectrometry (API-5000 triple-quadruple; Applied
Biosystems/MDS SCIEX, Ontario, Canada). Free testosterone was calculated using a mass
equation 44. Within assay coefficients of variation were less than 10% for all assays.
Determination of Metabolic Syndrome and Other Measurements
The metabolic syndrome was defined according to international consensus guidelines 45 and
the National Cholesterol Education Program’s Adult Treatment Program Panel Criteria III
using the previously described anthropometric, blood pressure and blood parameters 46
. A
score was given to each individual criterion and then summed together. Metabolic syndrome
was defined by a total score ≥3. At all visits physical activity was assessed by the physical
Page 8 of 31

9
activity scale for the elderly questionnaire and handgrip strength by dynamometer (Jamar, JA
Preston Co. Jackson, MI) as previously described 47. Lower urinary tract symptoms were
assessed at the same time by International Prostate Symptom Score 48. At each visit subjects
were asked to report adverse events, including injection-related adverse events such as
bruising, stinging or pain. Adverse events were categorized according to the Medical
Dictionary for Regulatory Activities (MedDRA) System Organ Class classification.
Statistical Analysis
The randomisation code was not broken until all data were collected and the database cleaned
and locked. The outcome variables for continuous variables were the calculated differences
from baseline at 6, 12 and 18 weeks. The between-group differences of all changes were
assessed by linear regression. Outcomes with repeated measures were assessed by mixed
model analyses and tested treatment, time and the interaction of treatment and time. Analyses
were adjusted by factors that, despite randomisation, significantly differed between groups at
baseline and were also a priori confounders of the outcome of interest. Normality of residuals
was confirmed.
The presence (or absence) of metabolic syndrome was assessed at every visit. The change in
the proportion of participants with or without the metabolic syndrome from baseline was
analysed separately at each subsequent visit by examining the treatment by syndrome
interaction. Repeated measurements were modelled in these analyses which utilised
generalised estimating equations which were then confirmed by Bayesian methods.
Additional analysis explored the influence of baseline testosterone on treatment effects in
order to assess potential thresholds of relative androgen deficiency which may identify
subgroups in whom testosterone may have enhanced effects. Baseline total and free
testosterone were included in separate regression models as a dichotomised factor using
Page 9 of 31

10
predefined cut points for total testosterone (8, 11 and 13nmol/L) and free testosterone (160,
220 and 280pmol/L) recently shown to be useful in the definition of late-onset hypogonadism
32, which included the definition stated in the current guidelines (total testosterone, 8nmol/L)
49. The statistical significance of the interaction terms of treatment and each dichotomised
variable were examined.
Analyses were performed using SAS version 9.2 (SAS Institute, Cary, North Carolina). Data
were considered significantly different at p<0.05 (two sided) and are presented as mean
differences ± standard errors, mean ± standard deviation or mean (95% CI), as indicated.
Page 10 of 31
11
Results
Eighty-one men were screened of whom 67 were randomised to receive either testosterone
(n=33) or matching placebo (n=34). Thirteen participants discontinued leaving 26 men in the
testosterone group and 28 men in the placebo group who completed the entire 18-week
treatment period. The flow of participants through the study has been previously published 38.
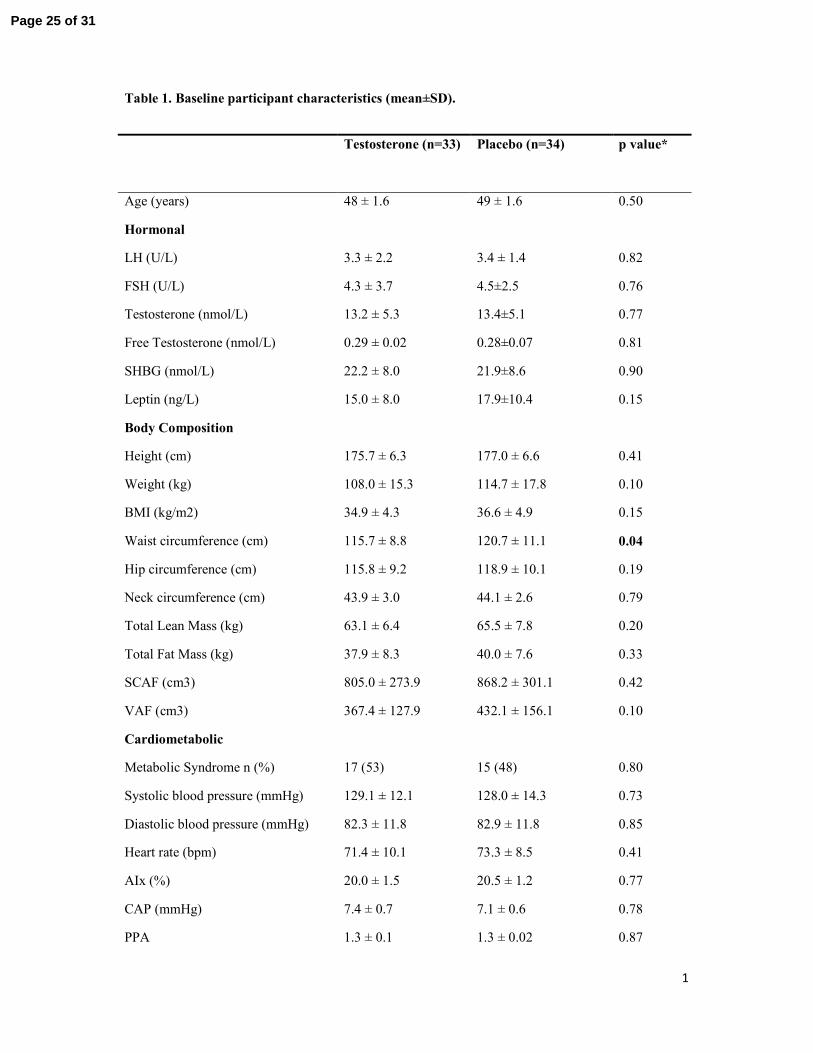
Baseline characteristics were comparable except testosterone-treated men had lower waist
circumference (table 1). Pre-existing cardiovascular disease was reported in 3 participants:
acute myocardial infarction (n=1, placebo), rheumatic valvular disease (n=1, placebo) and
transient ischemic attack (n=1, testosterone). There were no differences in the use of lipid-
lowering medications between the groups at baseline (table 1). All participants remained on
these medications for the duration of the study and no other participants started lipid-
lowering treatment during the course of the study. Medical Dictionary for Regulatory
Activities (MedDRA) defined adverse events were similar between the two groups (table 2).
Hormones and cardiometabolic effects
Testosterone therapy increased blood testosterone concentrations and suppressed
gonadotropins, often to the detection limit of the assay (table 3). Arterial stiffness (i.e.
augmentation index) was significantly less in the testosterone treated group compared with
the placebo group overall (table 3) and at 18 weeks (figure 1A). Central augmentation
pressure was also improved after testosterone compared to placebo (table 3). There were no
changes in heart rate, systolic or diastolic blood pressure in either group after 18 weeks of
treatment (table 3).
Testosterone treatment decreased insulin resistance (HOMA-IR) (figure 1B) and liver fat
(figure 1C) compared to placebo (table 3). Testosterone significantly increased LDL-
cholesterol compared to placebo (table 3). There were no changes in any other blood lipids,
Page 11 of 31

12
the total to high-density lipoprotein (HDL) cholesterol ratio or liver transaminases (table 3).
The respiratory quotient significantly decreased with testosterone compared to placebo
treatment indicating a shift to fat, rather than carbohydrate, utilisation (table 3). However
resting energy expenditure did not significantly improve more with testosterone than with
placebo (table 3). Testosterone therapy did not significantly alter the net development of
metabolic syndrome at week 6 (p=0.93), week 12 (p=0.33) nor week 18 (p=0.96) using a
consensus definition of metabolic syndrome 45. Analogous findings were obtained using an
alternate definition of metabolic syndrome 46.
Body Composition
Weight, body mass index and waist circumference as well as total fat, SCAF and VAF
significantly decreased over time due to the weight-loss program (p<0.0001), but there were
no significant differences between groups at any single timepoint or overall (table 3). In
contrast, testosterone therapy significantly increased lean muscle mass, compared with
placebo (figure 1D and table 3). There were no significant between-group differences in any
other anthropometric measurement ( table 3).
Prostate and hematological outcomes
Testosterone increased serum prostate-specific antigen and hematocrit compared to placebo,
but no participant met predefined withdrawal criteria and there was no change in self-
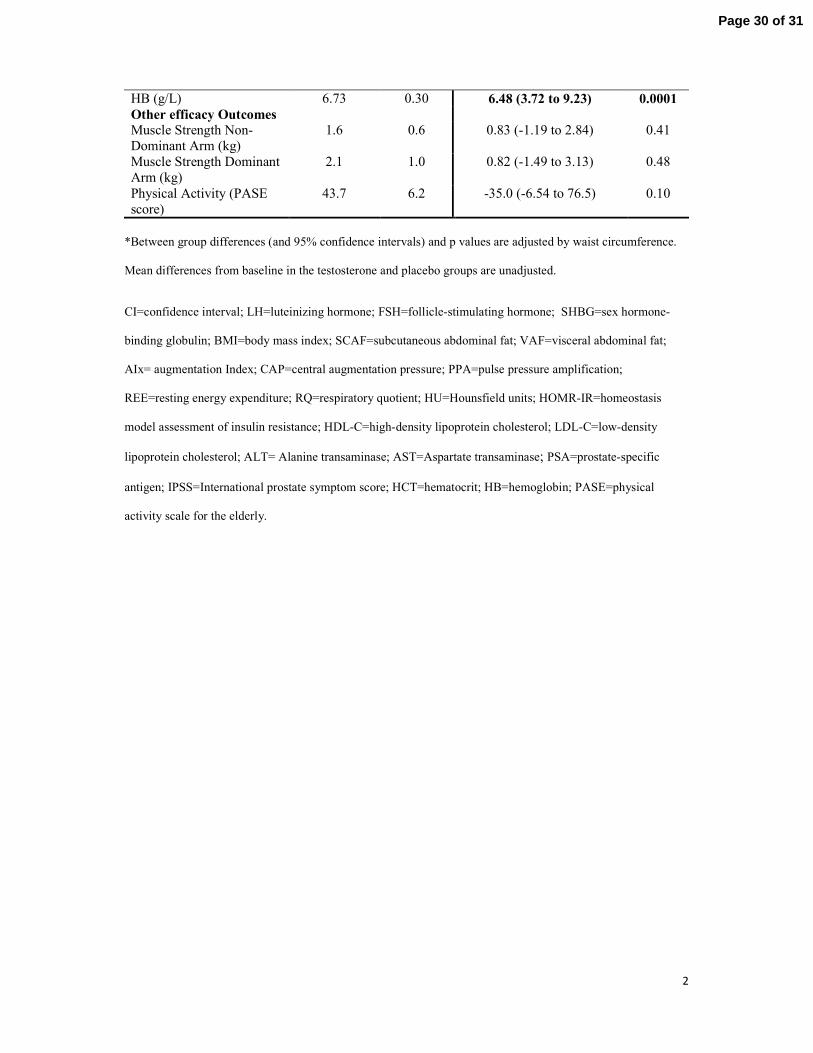
reported prostate symptoms in either group (table 3). Hemoglobin also increased with
testosterone compared to placebo (table 3). There were no other significant between-group
differences in blood hematology or other routine tests of renal and liver function (data not
shown).
Other efficacy outcomes and exploratory analysis
Page 12 of 31

13
Dominant and non-dominant hand strength increased with time (both p<0.05) but there were
no differences between groups (table 3). Physical activity was significantly increased
compared with placebo at week 6 (p=0.03); however there was no overall between-group
difference (table 3).
Exploratory analyses using total testosterone dichotomised by cutpoints of 8, 11 and 13 nM
and free testosterone dichotomised by thresholds of 160, 220 and 280pmol/L were performed
and the interaction between treatment and the dichotomised variable examined. The
interaction term of treatment and any dichotomised factor for testosterone were not
statistically significant for any measures of body composition. This indicates that the
testosterone treatment effects on body composition were not influenced by baseline
testosterone concentrations.
Page 13 of 31

14
Discussion
This is the first randomised placebo controlled study to examine the body compositional and
cardiometabolic effects of testosterone treatment in obese men with OSA. Indeed only two
previous studies, one of which we conducted, have examined pharmacological methods to
alter body composition in men with OSA 50, 51 and neither study was randomised nor
contained a no-treatment control. This study therefore adds to the very limited literature
examining mechanisms and methods by which cardiometabolic health and body composition
can be altered in men with OSA. We demonstrate that 18 weeks of testosterone therapy does
not further reduce weight, BMI or metabolic syndrome but does improve several important
cardiometabolic risk factors as well as lean muscle mass and respiratory quotient, in obese
men with OSA. This is a specific population in whom both relative androgen deficiency and
increased cardiometabolic risk have been documented. Recently published data from this
study has shown that testosterone mildly worsens sleep-disordered breathing in a time-limited
manner, irrespective of initial testosterone concentrations 38.
We demonstrate that testosterone therapy reduces liver fat and increases insulin sensitivity in
obese men with OSA. These changes in liver fat or insulin sensitivity should independently
decrease cardiovascular risk 52
. To our knowledge this is the first study of testosterone
therapy to accurately measure liver fat by CT imaging although there are now ongoing
studies examining the effect of transdermal testosterone treatment on liver fat in
hypogonadal men with (clinicaltrials.gov number: NCT01560546) and without diabetes
(NCT00700024). Transaminases did not change after testosterone treatment which is in
agreement with a previous 6 month randomised controlled trial in older men 53
although a
non-controlled study did find significant reduction in transaminases after 1 year 54. Imaging
techniques for the quantification of liver fat are sensitive and validated methods whereas
Page 14 of 31
15
transaminases may not detect changes in liver fat and can be influenced by a variety of
biological circumstances 55. Previous randomised placebo-controlled studies show that
testosterone increases insulin sensitivity in 3 populations of men: eugonadal abdominally
obese men, by euglycemic hyperinsulinemic clamp 13-15; biochemically androgen deficient
men with type II diabetes and/or the metabolic syndrome, by HOMA-IR 17, 35, 56-58 including a
meta-analysis of men with the metabolic syndrome 20
, and; elderly patients with chronic heart
failure, by HOMA-IR 18, 59. Another meta-analysis of diabetic men reported significant
reductions in HbA1c, fasting glucose and triglycerides, which may have resulted in an
improvement in insulin resistance although this was not directly assessed 36. Over the longer
term, these changes would be expected to reverse metabolic syndrome and NAFLD, although
we did not show a reduction in metabolic syndrome after 18 weeks. Only two other
randomised placebo controlled trials of testosterone therapy have examined effects on
metabolic syndrome, albeit in non-OSA populations 57, 58. Both reported reductions in
metabolic syndrome but were of longer-duration (1-2 years) and both specifically recruited
men with metabolic syndrome. However no studies thus far have targeted reversal of NAFLD
despite an independent association between low testosterone levels and hepatic steatosis, a
marker for NAFLD 60, 61. The prevalence of NAFLD is increasing particularity in patients
with cardio-metabolic risk factors and is associated with increased risk of liver damage and
possibly future CVD 52, 62 . Therefore a reduction in NAFLD by lowering liver fat could have
an important impact on disease burden. Our findings in conjunction with analogous data in
other populations suggest the utility of performing a longer term study.
Other cardiovascular risk factors were also generally improved after testosterone
supplementation. Arterial stiffness as measured by the augmentation index was significantly
reduced in the testosterone group compared with the placebo group. Similar findings have
been reported in men with chronic heart failure and low testosterone levels 27
and in men with
Page 15 of 31

16
acquired hypogonadism 28
. Augmentation pressure, an additional marker of arterial stiffness,
was also significantly improved at 18 weeks in the testosterone group compared to placebo.
These measures are validated predictors of cardiovascular risk 63. Testosterone therapy also
significantly altered substrate utilisation to favour oxidation of fat, rather than carbohydrate,
as shown by a significant reduction in the respiratory quotient. Such changes should promote
fat loss if persistent over the longer term, although this was not observed within the 18 week
treatment period. There was no change in the total to HDL cholesterol ratio, a standard
measure of coronary heart disease risk 64, although a small increase of uncertain clinical
relevance in LDL cholesterol was observed. In other studies, testosterone therapy has been
reported to either decrease 65, 66 or not change LDL cholesterol 53, 56, 67-69. There were no
changes to lipid-lowering therapy during the course of the study suggesting that the changes
in LDL cholesterol were not as a result of alterations in concomitant medications.
On balance, the improvements in insulin sensitivity, liver fat and arterial stiffness would
seem to outweigh the possible changes in LDL cholesterol, suggesting that testosterone
therapy generally improves cardiometabolic risk in obese men with OSA. Whether this
improvement persists beyond 18 weeks would need to be verified with longer-term studies.
Furthermore, the factors which ultimately prove to be decisive in modulating whether or not
cardiovascular events occur in response to testosterone therapy have not yet been determined,
but advanced age and immobility are two possibilities 37. However, baseline testosterone
concentrations do not appear to be relevant in this population. Such an analysis was possible
because participants were specifically selected to have both obesity and OSA, and therefore
to have relative androgen deficiency 29, rather than recruited on the basis of baseline
testosterone concentrations.
Testosterone increased lean muscle mass in this population which is consistent with previous
studies in both eugonadal and hypogonadal men 10, 11
. We did not observe a further reduction
Page 16 of 31

17
in total fat mass in contrast with previous randomised controlled studies, but many of these
were not performed in obese populations and therefore did not include lifestyle modification
10, 11. Indeed, the differential effect on muscle and fat we observed could also be explained by
the lifestyle modification program administered which was focussed on diet rather than
exercise. Furthermore, since chronic intermittent hypoxia directly influences the uptake of
triglycerides in animal models 5, testosterone effects on fat mass may differ between those
with and without OSA.
Unsurprisingly we did not detect a significant reduction in total weight compared with
placebo since testosterone would increase muscle and reduce fat resulting in attenuated net
changes. This finding is consistent with most 14, 15, 23, 70
but not all 35
previous randomised
controlled studies. We did not observe a reduction in VAF with testosterone compared to
placebo which may also be explained by the lifestyle modification program administered to
all participants and/or the influence of chronic intermittent hypoxia. Furthermore, this finding
is consistent with the hypothesis that changes in insulin sensitivity occur before changes in
VAF 15
. Nevertheless, previous randomised placebo-controlled studies using computer
imaging to estimate VAF have generally shown no change in VAF after 6-24 months of
testosterone treatment 21-24. One notable exception is a study of non-obese older men with age
related hypogonadism which reported a between-group reduction in VAF that was driven by
an increase in the placebo group 70. Testosterone has also been shown to reduce VAF in
abdominally obese men with low to normal testosterone levels after 8 and 9 months
treatment, despite no changes in any other body composition measurement including total
lean mass 13-15. It could be that abdominally obese men may be more susceptible to changes
in VAF compared to our population who were selected for generalised obesity as defined by
a BMI≥30kg/m2.
Page 17 of 31

18
It is currently unclear whether or not low testosterone levels are causally related to CVD or
whether it is simply a marker of illness 71, 72. In this study of obese men with OSA, a
population who may be at a greater risk of CVD, testosterone therapy improved some
markers of cardiometabolic health despite no reduction in weight, fat mass or OSA
parameters. However longer-term studies of the effect of testosterone therapy of hard
cardiometabolic endpoints in this particular population are required for confirmation.
There are some possible limitations that should be acknowledged. The duration of
testosterone treatment may have been too short to result in changes in some of the outcomes
measures 73. As all the participants received a weight loss program, we cannot extrapolate
these findings to men not receiving a weight loss program. However, all obese men with
OSA (such as ours) or without OSA ought to be placed on a weight loss program, so our
scientific study design appeared to be the most appropriate to answer a pragmatic clinical
question. Our findings also pertain to the use of intramuscular testosterone undecanoate.
Different modes of administration may have different results 74. Finally the cut points used to
examine the influence of baseline testosterone levels on the effects treatment on body
composition were developed for late-onset hypogonadism, not necessarily for obese middle-
aged men with OSA, nevertheless these cut points seemed to be a reasonable starting point.
The role of testosterone replacement in obese men with OSA in clinical practice needs to
consider all potential risks and benefits, including prostate, hematological and respiratory
effects 38, 75. Nevertheless, this mechanistic report of solely cardiometabolic effects show that
18 weeks of testosterone therapy may potentially improve certain important parameters of
cardiometabolic health and provides a basis on which future larger and longer term studies
can be implemented.
Page 18 of 31

19
Acknowledgements
We thank Roo Killick, Kerri Melehan, Farid Saad and the Data and Safety Monitoring
Committee which consisted of Professor Michael Hensley (chair), Associate Professor Val
Gebski and Professor Stephen Twigg. We also thank the men who participated in the study,
the sleep physicians and the study co-ordinators.
Conflicts of Interest
There is no conflict of interest to disclose.
Role of the funding source
Supported by the National Health and Medical Research Council of Australia (NHMRC)
through a project grant (512499), a Centre for Clinical Research Excellence in
Interdisciplinary Sleep Health (571421) and fellowships to CH, CP, RRG and PYL (512057,
571179, 202916 and 1025248, respectively). Bayer Schering supplied study drug, matching
placebo and $20,000 to date.
Page 19 of 31

20
References
1. Flegal KM, Carroll MD, Ogden CL & Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010 303 235-241.
2. Grunstein RR, Stenlof K, Hedner J & Sjostrom L. Impact of obstructive sleep apnea and sleepiness on metabolic and cardiovascular risk factors in the Swedish Obese Subjects (SOS) Study. Int J Obes Relat Metab Disord 1995 19 410-418.
3. Young T, Peppard PE & Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol 2005 99 1592-1599.
4. Ye J. Emerging role of adipose tissue hypoxia in obesity and insulin resistance. Int J Obes (Lond) 2009
33 54-66. 5. Drager LF, Li J, Shin MK, Reinke C, Aggarwal NR, Jun JC, Bevans-Fonti S, Sztalryd C, O'Byrne SM,
Kroupa O, Olivecrona G, Blaner WS & Polotsky VY. Intermittent hypoxia inhibits clearance of triglyceride-rich lipoproteins and inactivates adipose lipoprotein lipase in a mouse model of sleep apnoea. Eur Heart J 2012 33 783-790.
6. Iiyori N, Alonso LC, Li J, Sanders MH, Garcia-Ocana A, O'Doherty RM, Polotsky VY & O'Donnell CP. Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am J Respir Crit Care Med 2007 175 851-857.
7. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW & Grunstein RR. Sleep apnea as an
independent risk factor for all-cause mortality: the Busselton Health Study. Sleep 2008 31 1079-1085. 8. Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, Stubbs R & Hla KM. Sleep
disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008
31 1071-1078. 9. Marin JM, Carrizo SJ, Vicente E & Agusti AG. Long-term cardiovascular outcomes in men with
obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005 365 1046-1053.
10. Isidori AM, Giannetta E, Greco EA, Gianfrilli D, Bonifacio V, Isidori A, Lenzi A & Fabbri A. Effects of testosterone on body composition, bone metabolism and serum lipid profile in middle-aged men: a meta-analysis. Clin Endocrinol (Oxf) 2005 63 280-293.
11. Allan CA, Strauss BJ & McLachlan RI. Body composition, metabolic syndrome and testosterone in ageing men. Int J Impot Res 2007 19 448-457.
12. Bhasin S, Storer TW, Javanbakht M, Berman N, Yarasheski KE, Phillips J, Dike M, Sinha-Hikim I, Shen R, Hays RD & Beall G. Testosterone replacement and resistance exercise in HIV-infected men with weight loss and low testosterone levels. Journal of the American Medical Association 2000 283
763-770. 13. Marin P. Testosterone and regional fat distribution. Obes Res 1995 3 Suppl 4 609S-612S. 14. Marin P, Holmang S, Jonsson L, Sjostrom L, Kvist H, Holm G, Lindstedt G & Bjorntorp P. The effects
of testosterone treatment on body composition and metabolism in middle-aged obese men. Int J Obes Relat Metab Disord 1992 16 991-997.
15. Marin P, Holmang S, Gustafsson C, Jonsson L, Kvist H, Elander A, Eldh J, Sjostrom L, Holm G & Bjorntorp P. Androgen treatment of abdominally obese men. Obes Res 1993 1 245-251.
16. Jones TH. Effects of testosterone on Type 2 diabetes and components of the metabolic syndrome. J Diabetes 2010 2 146-156.
17. Jones TH, Arver S, Behre HM, Buvat J, Meuleman E, Moncada I, Morales AM, Volterrani M, Yellowlees A, Howell JD & Channer KS. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study). Diabetes Care 2011 34 828-837.
18. Caminiti G, Volterrani M, Iellamo F, Marazzi G, Massaro R, Miceli M, Mammi C, Piepoli M, Fini M & Rosano GM. Effect of long-acting testosterone treatment on functional exercise capacity, skeletal muscle performance, insulin resistance, and baroreflex sensitivity in elderly patients with chronic heart failure a double-blind, placebo-controlled, randomized study. J Am Coll Cardiol 2009 54 919-927.
19. Bhasin S. Effects of testosterone administration on fat distribution, insulin sensitivity, and atherosclerosis progression. Clin Infect Dis 2003 37 Suppl 2 S142-149.
20. Corona G, Monami M, Rastrelli G, Aversa A, Tishova Y, Saad F, Lenzi A, Forti G, Mannucci E & Maggi M. Testosterone and metabolic syndrome: a meta-analysis study. J Sex Med 2011 8 272-283.
21. Lovejoy JC, Bray GA, Greeson CS, Klemperer M, Morris J, Partington C & Tulley R. Oral anabolic steroid treatment, but not parenteral androgen treatment, decreases abdominal fat in obese, older men. Int J Obes Relat Metab Disord 1995 19 614-624.
Page 20 of 31

21
22. Frederiksen L, Hojlund K, Hougaard DM, Mosbech TH, Larsen R, Flyvbjerg A, Frystyk J, Brixen K & Andersen M. Testosterone therapy decreases subcutaneous fat and adiponectin in aging men. Eur J Endocrinol 2012 166 469-476.
23. Svartberg J, Agledahl I, Figenschau Y, Sildnes T, Waterloo K & Jorde R. Testosterone treatment in
elderly men with subnormal testosterone levels improves body composition and BMD in the hip. Int J Impot Res 2008 20 378-387.
24. Munzer T, Harman SM, Hees P, Shapiro E, Christmas C, Bellantoni MF, Stevens TE, O'Connor KG, Pabst KM, St Clair C, Sorkin JD & Blackman MR. Effects of GH and/or sex steroid administration on
abdominal subcutaneous and visceral fat in healthy aged women and men. J Clin Endocrinol Metab
2001 86 3604-3610. 25. Nair KS, Rizza RA, O'Brien P, Dhatariya K, Short KR, Nehra A, Vittone JL, Klee GG, Basu A, Basu
R, Cobelli C, Toffolo G, Dalla Man C, Tindall DJ, Melton LJ, 3rd, Smith GE, Khosla S & Jensen MD.
DHEA in elderly women and DHEA or testosterone in elderly men. N Engl J Med 2006 355 1647-1659.
26. Liu PY, Death AK & Handelsman DJ. Androgens and cardiovascular disease. Endocr Rev 2003 24 313-340.
27. Webb CM, Elkington AG, Kraidly MM, Keenan N, Pennell DJ & Collins P. Effects of oral testosterone treatment on myocardial perfusion and vascular function in men with low plasma testosterone and coronary heart disease. Am J Cardiol 2008 101 618-624.
28. Yaron M, Greenman Y, Rosenfeld JB, Izkhakov E, Limor R, Osher E, Shenkerman G, Tordjman K &
Stern N. Effect of testosterone replacement therapy on arterial stiffness in older hypogonadal men. Eur J Endocrinol 2009 160 839-846.
29. Liu PY, Caterson ID, Grunstein RR & Handelsman DJ. Androgens, obesity, and sleep-disordered breathing in men. Endocrinol Metab Clin North Am 2007 36 349-363.
30. Barrett-Connor E, Dam TT, Stone K, Harrison SL, Redline S & Orwoll E. The association of testosterone levels with overall sleep quality, sleep architecture, and sleep-disordered breathing. J Clin Endocrinol Metab 2008 93 2602-2609.
31. Grunstein RR, Handelsman DJ, Lawrence SJ, Blackwell C, Caterson ID & Sullivan CE.
Neuroendocrine dysfunction in sleep apnea: reversal by continuous positive airways pressure therapy. Journal of Clinical Endocrinology & Metabolism 1989 68 352-358.
32. Wu FC, Tajar A, Beynon JM, Pye SR, Silman AJ, Finn JD, O'Neill TW, Bartfai G, Casanueva FF, Forti G, Giwercman A, Han TS, Kula K, Lean ME, Pendleton N, Punab M, Boonen S, Vanderschueren D, Labrie F & Huhtaniemi IT. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med 2010 363 123-135.
33. Strain GW, Zumoff B, Miller LK, Rosner W, Levit C, Kalin M, Hershcopf RJ & Rosenfeld RS. Effect of massive weight loss on hypothalamic-pituitary-gonadal function in obese men. Journal of Clinical
Endocrinology & Metabolism 1988 66 1019-1023. 34. Hammoud A, Gibson M, Hunt SC, Adams TD, Carrell DT, Kolotkin RL & Meikle AW. Effect of
Roux-en-Y gastric bypass surgery on the sex steroids and quality of life in obese men. J Clin Endocrinol Metab 2009 94 1329-1332.
35. Kalinchenko SY, Tishova YA, Mskhalaya GJ, Gooren LJ, Giltay EJ & Saad F. Effects of testosterone supplementation on markers of the metabolic syndrome and inflammation in hypogonadal men with the metabolic syndrome: the double-blinded placebo-controlled Moscow study. Clin Endocrinol (Oxf) 2010 73 602-612.
36. Corona G, Monami M, Rastrelli G, Aversa A, Sforza A, Lenzi A, Forti G, Mannucci E & Maggi M. Type 2 diabetes mellitus and testosterone: a meta-analysis study. Int J Androl 2011 34 528-540.
37. Basaria S, Coviello AD, Travison TG, Storer TW, Farwell WR, Jette AM, Eder R, Tennstedt S, Ulloor J, Zhang A, Choong K, Lakshman KM, Mazer NA, Miciek R, Krasnoff J, Elmi A, Knapp PE, Brooks
B, Appleman E, Aggarwal S, Bhasin G, Hede-Brierley L, Bhatia A, Collins L, LeBrasseur N, Fiore LD & Bhasin S. Adverse events associated with testosterone administration. N Engl J Med 2010 363 109-122.
38. Hoyos CM, Killick R, Yee BJ, Grunstein RR & Liu PY. Effects of testosterone therapy on sleep and
breathing in obese men with severe obstructive sleep apnea: a randomised placebo-controlled trial. Clin Endocrinol (Oxf) 2012.
39. Lohmann TG, Roche AF & Martorell R. Anthropometric standardization referance maunal. Champaign, IL: Hunam Kinetic Books, 1988.
40. Demerath EW, Ritter KJ, Couch WA, Rogers NL, Moreno GM, Choh A, Lee M, Remsberg K, Czerwinski SA, Chumlea WC, Siervogel RM & Towne B. Validity of a new automated software program for visceral adipose tissue estimation. Int J Obes (Lond) 2007 31 285-291.
Page 21 of 31
22
41. Phillips CL, Yee BJ, Trenell MI, Magnussen JS, Wang D, Banerjee D, Berend N & Grunstein RR. Changes in regional adiposity and cardio-metabolic function following a weight loss program with sibutramine in obese men with obstructive sleep apnea. J Clin Sleep Med 2009 5 416-421.
42. Friedewald WT, Levy RI & Fredrickson DS. Estimation of the concentration of low-density lipoprotein
cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972 18 499-502. 43. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF & Turner RC. Homeostasis model
assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985 28 412-419.
44. Vermeulen A, Verdonck L & Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. Journal of Clinical Endocrinology & Metabolism 1999 84 3666-3672.
45. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM & Smith SC, Jr. Harmonizing the metabolic syndrome: a joint interim statement of the
International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009 120 1640-1645.
46. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002 106 3143-3421.
47. Liu PY, Wishart SM & Handelsman DJ. A double-blind, placebo-controlled, randomized clinical trial
of recombinant human chorionic gonadotropin on muscle strength and physical function and activity in older men with partial age-related androgen deficiency. Journal of Clinical Endocrinology & Metabolism 2002 87 3125-3135.
48. Barry MJ, Fowler FJ, Jr., O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK & Cockett AT.
The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol 1992 148 1549-1557; discussion 1564.
49. Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ,
Lunenfeld B, Morales A, Morley JE, Schulman C, Thompson IM, Weidner W & Wu FC. Investigation, treatment, and monitoring of late-onset hypogonadism in males: ISA, ISSAM, EAU, EAA, and ASA recommendations. J Androl 2009 30 1-9.
50. Yee BJ, Phillips CL, Banerjee D, Caterson I, Hedner JA & Grunstein RR. The effect of sibutramine-assisted weight loss in men with obstructive sleep apnoea. Int J Obes (Lond) 2007 31 161-168.
51. Ferland A, Poirier P & Series F. Sibutramine versus continuous positive airway pressure in obese obstructive sleep apnoea patients. Eur Respir J 2009 34 694-701.
52. Kotronen A & Yki-Jarvinen H. Fatty liver: a novel component of the metabolic syndrome. Arterioscler
Thromb Vasc Biol 2008 28 27-38. 53. Emmelot-Vonk MH, Verhaar HJ, Nakhai Pour HR, Aleman A, Lock TM, Bosch JL, Grobbee DE &
van der Schouw YT. Effect of testosterone supplementation on functional mobility, cognition, and other parameters in older men: a randomized controlled trial. Journal of the American Medical
Association 2008 299 39-52. 54. Haider A, Gooren LJ, Padungtod P & Saad F. Improvement of the metabolic syndrome and of non-
alcoholic liver steatosis upon treatment of hypogonadal elderly men with parenteral testosterone undecanoate. Exp Clin Endocrinol Diabetes 2010 118 167-171.
55. Ali R & Cusi K. New diagnostic and treatment approaches in non-alcoholic fatty liver disease (NAFLD). Ann Med 2009 41 265-278.
56. Kapoor D, Goodwin E, Channer KS & Jones TH. Testosterone replacement therapy improves insulin resistance, glycaemic control, visceral adiposity and hypercholesterolaemia in hypogonadal men with
type 2 diabetes. Eur J Endocrinol 2006 154 899-906. 57. Heufelder AE, Saad F, Bunck MC & Gooren L. Fifty-two-week treatment with diet and exercise plus
transdermal testosterone reverses the metabolic syndrome and improves glycemic control in men with newly diagnosed type 2 diabetes and subnormal plasma testosterone. J Androl 2009 30 726-733.
58. Aversa A, Bruzziches R, Francomano D, Rosano G, Isidori AM, Lenzi A & Spera G. Effects of testosterone undecanoate on cardiovascular risk factors and atherosclerosis in middle-aged men with late-onset hypogonadism and metabolic syndrome: results from a 24-month, randomized, double-blind, placebo-controlled study. J Sex Med 2010 7 3495-3503.
59. Malkin CJ, Jones TH & Channer KS. The effect of testosterone on insulin sensitivity in men with heart failure. Eur J Heart Fail 2007 9 44-50.
Page 22 of 31

23
60. Volzke H, Aumann N, Krebs A, Nauck M, Steveling A, Lerch MM, Rosskopf D & Wallaschofski H. Hepatic steatosis is associated with low serum testosterone and high serum DHEAS levels in men. Int J Androl 2010 33 45-53.
61. Kim S, Kwon H, Park JH, Cho B, Kim D, Oh SW, Lee CM & Choi HC. A low level of serum total
testosterone is independently associated with nonalcoholic fatty liver disease. BMC Gastroenterol 2012 12 69.
62. Targher G & Arcaro G. Non-alcoholic fatty liver disease and increased risk of cardiovascular disease. Atherosclerosis 2007 191 235-240.
63. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I & Struijker-Boudier H. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006 27 2588-2605.
64. Kinosian B, Glick H & Garland G. Cholesterol and coronary heart disease: predicting risks by levels
and ratios. Ann Intern Med 1994 121 641-647. 65. Tenover JS. Effects of testosterone supplementation in the aging male. Journal of Clinical
Endocrinology & Metabolism 1992 75 1092-1098. 66. Steidle C, Schwartz S, Jacoby K, Sebree T, Smith T & Bachand R. AA2500 testosterone gel
normalizes androgen levels in aging males with improvements in body composition and sexual function. J Clin Endocrinol Metab 2003 88 2673-2681.
67. Kenny AM, Prestwood KM, Gruman CA, Fabregas G, Biskup B & Mansoor G. Effects of transdermal testosterone on lipids and vascular reactivity in older men with low bioavailable testosterone levels. J
Gerontol A Biol Sci Med Sci 2002 57 M460-465. 68. Wang C, Swerdloff RS, Iranmanesh A, Dobs A, Snyder PJ, Cunningham G, Matsumoto AM, Weber T
& Berman N. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. Journal of Clinical Endocrinology & Metabolism 2000
85 2839-2853. 69. Wu FC & von Eckardstein A. Androgens and coronary artery disease. Endocr Rev 2003 24 183-217. 70. Allan CA, Strauss BJ, Burger HG, Forbes EA & McLachlan RI. Testosterone therapy prevents gain in
visceral adipose tissue and loss of skeletal muscle in nonobese aging men. J Clin Endocrinol Metab
2008 93 139-146. 71. Araujo AB, Dixon JM, Suarez EA, Murad MH, Guey LT & Wittert GA. Clinical review: Endogenous
testosterone and mortality in men: a systematic review and meta-analysis. J Clin Endocrinol Metab
2011 96 3007-3019. 72. Corona G, Rastrelli G, Monami M, Guay A, Buvat J, Sforza A, Forti G, Mannucci E & Maggi M.
Hypogonadism as a risk factor for cardiovascular mortality in men: a meta-analytic study. Eur J Endocrinol 2011 165 687-701.
73. Saad F, Aversa A, Isidori AM, Zafalon L, Zitzmann M & Gooren L. Onset of effects of testosterone
treatment and time span until maximum effects are achieved. Eur J Endocrinol 2011 165 675-685. 74. Jockenhovel F, Vogel E, Reinhardt W & Reinwein D. Effects of various modes of androgen
substitution therapy on erythropoiesis. Eur J Med Res 1997 2 293-298. 75. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS & Montori VM.
Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical
practice guideline. J Clin Endocrinol Metab 2010 95 2536-2559.
Page 23 of 31

Figure Legend
Figure 1. Changes from baseline in efficacy outcomes. Data are mean and SEM of the change from baseline.
Overall between group differences are indicated by the p value, determined by linear regression and adjusted
for baseline waist circumference.
Page 24 of 31
1
Table 1. Baseline participant characteristics (mean±SD).
Testosterone (n=33)
Placebo (n=34)
p value*
Age (years) 48 ± 1.6 49 ± 1.6 0.50
Hormonal
LH (U/L) 3.3 ± 2.2 3.4 ± 1.4 0.82
FSH (U/L) 4.3 ± 3.7 4.5±2.5 0.76
Testosterone (nmol/L) 13.2 ± 5.3 13.4±5.1 0.77
Free Testosterone (nmol/L) 0.29 ± 0.02 0.28±0.07 0.81
SHBG (nmol/L) 22.2 ± 8.0 21.9±8.6 0.90
Leptin (ng/L) 15.0 ± 8.0 17.9±10.4 0.15
Body Composition
Height (cm) 175.7 ± 6.3 177.0 ± 6.6 0.41
Weight (kg) 108.0 ± 15.3 114.7 ± 17.8 0.10
BMI (kg/m2) 34.9 ± 4.3 36.6 ± 4.9 0.15
Waist circumference (cm) 115.7 ± 8.8 120.7 ± 11.1 0.04
Hip circumference (cm) 115.8 ± 9.2 118.9 ± 10.1 0.19
Neck circumference (cm) 43.9 ± 3.0 44.1 ± 2.6 0.79
Total Lean Mass (kg) 63.1 ± 6.4 65.5 ± 7.8 0.20
Total Fat Mass (kg) 37.9 ± 8.3 40.0 ± 7.6 0.33
SCAF (cm3) 805.0 ± 273.9 868.2 ± 301.1 0.42
VAF (cm3) 367.4 ± 127.9 432.1 ± 156.1 0.10
Cardiometabolic
Metabolic Syndrome n (%) 17 (53) 15 (48) 0.80
Systolic blood pressure (mmHg) 129.1 ± 12.1 128.0 ± 14.3 0.73
Diastolic blood pressure (mmHg) 82.3 ± 11.8 82.9 ± 11.8 0.85
Heart rate (bpm) 71.4 ± 10.1 73.3 ± 8.5 0.41
AIx (%) 20.0 ± 1.5 20.5 ± 1.2 0.77
CAP (mmHg) 7.4 ± 0.7 7.1 ± 0.6 0.78
PPA 1.3 ± 0.1 1.3 ± 0.02 0.87
Page 25 of 31

2
Testosterone (n=33)
Placebo (n=34)
p value*
REE (kcal) 0.85 ± 0.05 0.83 ± 0.06 0.17
RQ 2006.7 ± 316.7 2033.0 ± 287.2 0.73
Liver Fat (HU) 0.9 ± 0.06 0.7 ± 0.3 0.12
Insulin (µIU/mL) 105.0 ± 83.2 109.4 ± 99.4 0.84
Glucose (mmol/L) 5.5 ± 0.9 5.6 ± 1.7 0.76
HOMA-IR (unit) 3.84 ± 0.57 4.47 ± 1.01 0.59
Hyperlipidemia-no. (%) 6 (18) 4 (12) 0.51
Statin Therapy- no. (%) 5 (15) 4 (12) 0.73
Total Cholesterol (mmol/L) 5.3 ± 1.0 5.2 ± 0.9 0.71
Total Cholesterol/HDL-C ratio 4.8 ± 0.3 4.6 ± 0.2 0.68
HDL-C (mmol/L) 1.2 ± 0.3 1.2 ± 0.3 0.97
LDL-C (mmol/L) 3.2 ± 0.9 3.2 ± 0.9 0.96
Triglycerides (mmol/L) 2.0 ± 0.2 2.1 ± 0.2 0.79
AST (U/L) 26.3 ± 8.7 26.2 ± 8.6 0.55
ALT (U/L) 42.9 ± 21.2 39.9 ± 20.0 0.99
Prostate and Haematology
PSA (ng/ml) 1.0 ± 0.7 1.0 ± 0.6 0.99
IPSS (score between 1-7) 5.0 ± 0.68 4.5 ± 0.85 0.63
HCT (L/L) 0.45 ± 0.03 0.46 ± 0.03 1.0
HB (g/L) 154.7 ± 9.7 153.0 ± 8.0 0.46
Values are mean ± SD or number (percent) as specified. *The p values were calculated by Student’s t-test or
Fisher’s Exact Test as appropriate
LH=luteinizing hormone; FSH=follicle-stimulating hormone; SHBG= sex hormone-binding globulin;
BMI=body mass index; SCAF=subcutaneous abdominal fat; VAF=visceral abdominal fat; AIx=augmentation
index; CAP=central augmentation pressure; PPA=peripheral pulse amplification; REE= Resiting Energy
Expenditure; RQ=Respiratory Quotient; HU=Hounsfield units; HOMR-IR=homeostasis model assessment of
insulin resistance; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol;
Page 26 of 31

3
ALT=Alanine transaminase; AST=Aspartate transaminase; PSA=prostate-specific antigen; IPSS=International
prostate symptom score; HCT=hematocrit; HB=hemoglobin
Page 27 of 31

Table 2. Adverse events
†p values from Fisher’s exact test
Adverse Event Category Number of events p value†
Testosterone
(n=33)
Placebo
(n=34)
All- n (%) 24 (73) 24 (71) 1.0
Administration site- n (%) 7 (21) 4 (12) 0.34
Cardiac- n (%) 1 (3) 0 (0) 0.49
Respiratory- n (%) 12 (36) 11 (32) 0.80
Musculoskeletal- n (%) 7 (21) 7 (21) 1.0
Renal and Urinary- n (%) 1 (3) 0 0.61
Page 28 of 31

1
Table 3. Changes from baseline in testosterone and placebo treated groups.
Unadjusted mean change
from baseline
Adjusted between-group
mean differences (95% CI)
Testosterone
(n=33)
Placebo
(n=34)
p
value*
Hormones and SHBG
LH (U/L) -2.90 0.52 -2.98 (-3.84 to -2.11) <0.0001
FSH (U/L) -3.53 0.23 -3.37 (-4.43 to -2.30) <0.0001
Testosterone (nmol/L) 3.83 0.69 5.73 (3.63 to 7.84) <0.0001
Free Testosterone
(nmol/L)
0.11 0.004 0.11 (0.06 to 0.16) <0.001
SHBG (nmol/L) 0.37 1.85 -1.35 (-3.29 to 0.59) 0.17 Leptin (ng/mL) -5.66 -4.45 -1.27 (-4.74 to 2.19) 0.47
Body Composition
Weight (kg) -1.54 -2.15 0.85 (-0.33 to 2.03) 0.16
BMI (kg/m2) -0.50 -0.71 0.30 (-0.10 to 0.69) 0.14
Waist Circumference (cm) -3.26 -3.51 0.25 (-1.27 to 1.76) 0.75
Hip Circumference (cm) -0.82 -1.42 0.61 (-1.28 to 2.49) 0.52
Waist-Hip Ratio -0.02 -0.019 -0.002 (-0.02 to 0.02) 0.81
Total Lean Mass (kg) 1.2 -0.4 1.6 (0.69 to 2.5) 0.0009
Total Fat Mass(kg) -3.1 -2.9 -0.02 (-1.4 to 1.4) 0.98 SCAF (cm3) -70.1 -48.3 -21.8 (-67.1 to 23.5) 0.34
VAF (cm3) -29.6 -44.4 23.1 (-23.4 to 70.0) 0.32
Cardiometabolic Systolic blood pressure
(mmHg)
1.7 0.5 2.3 (-3.0 to 7.6) 0.39
Diastolic blood pressure
(mmHg)
0.64 0.69 0.32 (-4.4 to 5.1) 0.89
Heart rate (bpm) -2.0 -2.6 1.3 (-3.3 to 5.8) 0.58
AIx (%) -0.79 2.20 -3.24 ( -6.01 to -0.46) 0.02
CAP (mmHg) -0.27 0.94 -1.28 (-2.56 to -0.004) <0.05
PPA 0.03 -0.02 0.04 (-0.0002 to 0.09) 0.06
REE (kcal) 81.6 24.1 42.6 (-69.3 to 154.5) 0.45 RQ -0.04 0.01 -0.04 (-0.08 to -0.001) 0.04
Liver Fat (HU) 0.11 0.05 0.09 (0.009 to 0.17) 0.03
HOMA-IR (units) -1.30 -0.37 -1.14 (-2.27 to -0.01) <0.05 Insulin (µIU/mL) -29.1 -9.33 -23.6 (-51.8 to 4.57) 0.10
Glucose (mmol/L) -0.36 -0.05 -0.22 (-0.71 to 0.26) 0.36
Total Cholesterol (mmol/L)
0.01 -0.10 0.12 (-0.14 to 0.38) 0.35
Total Cholesterol/HDL-C
ratio
0.13 0.001 0.18 (-0.14 to 0.50) 0.26
HDL-C (mmol/L) -0.06 -0.04 -0.02 (-0.09 to 0.05) 0.57
LDL-C (mmol/L) 0.21 -0.06 0.27 (0.03 to 0.54) 0.03
Triglycerides (mmol/L) -0.29 -0.16 -0.01 (-0.45 to 0.42) 0.95
ALT (U/L) -2.79 -1.14 -1.65 (-4.87 to 1.57) 0.31
AST (U/L) 1.68 1.63 0.04 (-4.20 to 4.28) 0.98
Prostate and Haematology
PSA (ng/mL) 0.21 -0.03 0.24 (0.10 to 0.38) 0.001
IPSS (score 1-7) 0.20 -0.06 0.01 (-1.63 to 1.65) 0.99
HCT (L/L) 0.03 -0.0004 0.03 (0.02 to 0.04) <0.0001
Page 29 of 31
2
*Between group differences (and 95% confidence intervals) and p values are adjusted by waist circumference.
Mean differences from baseline in the testosterone and placebo groups are unadjusted.
CI=confidence interval; LH=luteinizing hormone; FSH=follicle-stimulating hormone; SHBG=sex hormone-
binding globulin; BMI=body mass index; SCAF=subcutaneous abdominal fat; VAF=visceral abdominal fat;
AIx= augmentation Index; CAP=central augmentation pressure; PPA=pulse pressure amplification;
REE=resting energy expenditure; RQ=respiratory quotient; HU=Hounsfield units; HOMR-IR=homeostasis
model assessment of insulin resistance; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density
lipoprotein cholesterol; ALT= Alanine transaminase; AST=Aspartate transaminase; PSA=prostate-specific
antigen; IPSS=International prostate symptom score; HCT=hematocrit; HB=hemoglobin; PASE=physical
activity scale for the elderly.
HB (g/L) 6.73 0.30 6.48 (3.72 to 9.23) 0.0001
Other efficacy Outcomes
Muscle Strength Non-
Dominant Arm (kg)
1.6 0.6 0.83 (-1.19 to 2.84) 0.41
Muscle Strength Dominant
Arm (kg)
2.1 1.0 0.82 (-1.49 to 3.13) 0.48
Physical Activity (PASE
score)
43.7 6.2 -35.0 (-6.54 to 76.5) 0.10
Page 30 of 31

1
Weeks
0 18
Lean
Mass (
kg
)
-0.5
0.0
0.5
1.0
1.5D
p=0.0009
C
p=0.03
0 6 12 18
HO
MA
-IR
(u
nit
s)
-2
-1
0B
p<0.05
0 6 12 18
Au
gm
en
tati
on
In
dex
(%
)
-4
-2
0
2
4A
p=0.02
Weeks
0 18
Liv
er
Fat
(HU
)
0.00
0.05
0.10
0.15
Figure 1.
Page 31 of 31