board of directors - university college hospital meeting papers... · agenda meeting title: board...
TRANSCRIPT

BOARD OF DIRECTORS
14th SEPTEMBER 2016


Agenda
Meeting Title: Board of Directors
Date: Wednesday 14th September 2016 Time: 2.00pm
Venue: Education Centre, 1st Floor West Wing, 250 Euston Road Agenda item Attachment
1. Apologies for Absence and Declarations of Conflict of Interest
2. Minutes of the Meeting held on 13th July 2016
A
3. Matters Arising Report B
4.
Other urgent matters not appearing on the Matters Arising Report
5. Presentation: University College London Hospitals and UCL Biomedical Research Centre – Bid to NIHR Professor Bryan Williams, Director of Research & Development
6.
Chairman’s Report C
7. Chief Executive’s Report
D
8. Executive Board Report
E
9. Performance Report
F
10. Quality & Safety Committee Report G
11. Finance & Contracting Committee Report H
12. Report of the Audit Committee meeting held on 19th July • Annual Audit Report
I
13. Minutes of the Audit Committee meeting held on 24th May J
14. Any Other Urgent Business
15. Date of Next Meeting
Wednesday 9th November 2016.


A
Agenda Item 2
Minutes of the Meeting Held on 13th July 2016


Board of Directors Minutes of the Meeting held on 13th July 2016
Present Richard Murley, Chairman Harry Bush, Vice-Chairman Althea Efunshile, Non-Executive Director David Lomas, Non-Executive Director Rima Makarem, Non-Executive Director Kieran Murphy, Non-Executive Director Diana Walford, Non-Executive Director Caspar Woolley, Non-Executive Director
Geoff Bellingan, Medical Director, Surgery & Cancer Board Gill Gaskin, Medical Director, Specialist Hospitals Board Neil Griffiths, Deputy Chief Executive Charles House, Interim Medical Director, Medicine Board Tim Jaggard, Interim Finance Director Robert Naylor, Chief Executive Flo Panel-Coates, Chief Nurse
In attendance Laura Churchward, Interim Director of Strategic Development Simon Knight, Director of Planning & Performance Ben Morrin, Director of Workforce Tonia Ramsden, Director of Corporate Services (Board Secretary) Karin Roberts (Minutes)
Item Matters covered 7/1 Apologies for Absence
Apologies for absence were received from Tony Mundy. The Chairman drew the Board’s attention to the fact that this would be the last Board meeting attended by the Chief Executive.
7/2 7/3
Minutes of the Meeting held on 11th May 2016 The minutes were agreed subject to the date at the top of the minutes being changed to 11th May 2016. Proposal to Change the UCLH Constitution Richard Murley declared an interest in this item and Harry Bush, Vice Chairman took over as Chair.

7/4
The report set out an amendment to paragraph 9.10.3 of the Constitution; this had been proposed by the Council of Governors to enable it to reappoint the Chairman for a further six month period to 31 December 2017. His extension would provide stability and continuity in the senior leadership of the Trust following the departure of the Chief Executive in September 2016. The Board noted that a new Chief Executive would be unlikely to take up post before January 2017. Tonia Ramsden explained that any change to the Constitution required the approval of both the Council and the Board of Directors; the Council had discussed and approved the revision to the Constitution at a meeting on 5 July. Harry Bush said the revision to the Constitution, which would enable the Council to reappoint the Chairman, made it clear that any extension to a term of office would be made in exceptional circumstances and for a defined period. The Board unanimously approved the amendment to paragraph 9.10.3 of the Constitution and agreed that the revised Constitution would be effective from 13 July 2016. Matters Arising Report The report was noted. The Chief Executive advised that the Information Governance Strategy 2016-2018 had been approved by the Executive Board in June 2016; a copy had been circulated to Board members. Diana Walford asked about the blood tracking system and sought assurance that action was being taken to address the concerns that had been raised by the Quality and Safety Committee. Charles House reported that a business case was being developed. An option appraisal had been undertaken and the preferred option was being reviewed by the Finance Team. Diana Walford expressed her concern that the views of the Quality and Safety Committee might not be taken into account as part of the business case discussion. Gill Gaskin would ensure that the strong support of the Quality and Safety Committee for a blood tracking system was noted.
Action: Medical Directors, Medicine and Specialist Hospitals
7/5 7/6
Other Urgent Matters Geoff Bellingan advised that a Programme Lead for Theatres and the Elective Pathway (previously referred to as the Theatre Czar) had been appointed. The appointee was not a clinician but had significant experience of theatre redesign. Presentation: Social Media The Chairman welcomed Rachel Maybank, Associate Director of Communications. Rachel Maybank reported that 70% of adults used some form of social media. Although 97% of all UK adults had a Facebook profile, younger adults tended to use Twitter, WhatsApp, YouTube and Instagram. Social media was good for patients and staff as it cut across formal hierarchies. For UCLH it also provided
2

a platform to tell stories. All these forms of social media were promoted on the UCLH intranet and website. For staff there was also an opportunity to use internal forms of social media including the Good Deed Feed, where staff could give recognition to a colleague for something they had done, and the Staff Suggestion Scheme where others could comment and vote on ideas.
Rachel Maybank said there had been 1.7m unique visitors to the website last year. The current online strategy was to develop patient information for specialist areas, e.g. cancer services. We had also updated the website so it could be used on mobile devices. UCLH also had 11,000 followers on Twitter, 801 on Instagram, 5110 on LinkedIn and had published 243 films on YouTube. Twitter was mostly used for NHS staff to talk to other NHS staff although if an individual commented about UCLH services this was followed up. The development of films on YouTube had been very successful, e.g. a film on how to do an insulin injection which had more than 100,000 views. Increasingly, Instagram would be used for photographic archives and corporate information. There was also the possibility of developing LinkedIn for recruitment and Facebook to disseminate Trust information.
The Executive Board had agreed to review the online strategy. There would be a recruitment pilot for hard to recruit areas using films, and the social media guidelines and support available to staff would also be reviewed.
Caspar Woolley asked whether social media was currently managed corporately or was devolved. Rachel Maybank explained that the communications team managed all social media apart from Instagram which was managed by the Arts Curator and Freedom of Information Lead. She agreed that more could be done to encourage staff to open individual accounts which were seen as more authentic than team accounts.
The Chairman thanked Rachel Maybank for her presentation and suggested that this become an annual presentation. He also suggested that the Patient Experience Committee and the soon to be established People Committee may also want to get involved with this work.
Action: Chief Nurse & Director of Workforce
7/7
7/7.1
Chairman’s Report
The report was noted.
Appointment of a new Chief Executive
The Chairman announced the appointment of Professor Marcel Levi as the new Chief Executive. Professor Levi was currently Chairman of the Executive Board of the Academic Medical Centre in Amsterdam, a post he had held for the past seven years; he was a practising clinician with an active interest in research. He would take up his post as Chief Executive on 3 January 2017. Sir Robert Naylor would retire on 30 September 2016 and Neil Griffiths, Deputy Chief Executive would become Interim Chief Executive from 1 October 2016 to 2 January 2017.
The changes agreed to the UCLH Constitution would enable the Chairman and new Chief Executive to work together for the whole of 2017. The Board of Directors welcomed this news.
3

7/8 7/8.1 7/8.2 7/8.3 7/8.4 7/8.5
Chief Executive’s Report North Central London Sustainability and Transformation Plan (STP) The Chief Executive drew attention to the summary of progress on the North Central London Sustainability and Transformation Plan (STP) which was attached to the report. On 30 June, the draft case for change had been submitted by the NCL Transformation Board to NHS England. A more comprehensive case for change was planned to be submitted in September. NHS Improvement Q4 Monitoring Letter A letter from The NHS Improvement, attached to the report, confirmed the Trust’s Q4 risk ratings as 2 for financial sustainability and green for governance, as was anticipated. The letter referred to the Trust’s failure to achieve the A&E four-hour wait standard and multiple cancer wait standards. The Chief Executive advised that the Trust’s A&E performance was above the national average but we would need to identify areas where we could improve our performance, and this and Cancer were being discussed between the Trust and Camden CCG. He also reminded the Board that the failure of the 2-week breast cancer referral target was caused by key staff taking unplanned sick leave simultaneously. This has resulted in an agreement to work more collaboratively with other hospitals to ensure we could provide a robust and resilient service. EU Referendum The report on the EU referendum advised that UCLH employed more than the national average of EU staff. The Board noted that the Chief Executive had written to all staff to state how important EEA nationals were to the Trust and that we would do all we reasonably could to support their continuing employment at UCLH. National Institute for Health Research (NIHR) Biomedical Research Centre (BRC) Competition The Chief Executive drew attention to the impending international interview for renewal of the UCLH/UCL designation as an NIHR Biomedical Research Centre (BRC). He reminded the Board that the UCLH/UCL BRC had been designated ten years ago and renewed five years ago. It brought in £100 million in research income. The submission prepared for the NIHR showed that the BRC was ranked first in the UK for four of the five current research themes. Five new themes were being proposed. David Lomas said that the quality of the bid demonstrated the close working relationship between UCL and UCLH. Junior Doctors Industrial Action The report advised that the BMA had announced that their members had rejected the proposed new contract for junior doctors; the Secretary of State for Health had since confirmed that the new contract would be imposed later in the year. The Board noted that implementation plans were being drawn up.
4

7/9
7/9.1
Executive Board Report
Information Governance Issues
The Chief Executive drew the Board’s attention to the annual reports from the Senior Information Risk Officer (SIRO) and the Caldicott Guardian and to the Information Governance Strategy 2016-2018. The SIRO report advised that a digital maturity assessment had been carried out which identified areas of focus including cyber security and a scenario-based table top exercise was planned.
The Board noted that there had been five incidents involving disclosure of patient data, these had been reported to the Information Commissioner’s Office. The ICO had not taken any further action. A plan was in place to improve communications and update the IG mandatory training to ensure staff were fully aware of their responsibilities.
Rima Makarem asked about areas of weakness and that the Trust relied on CGI’s expertise in relation to cyber security. Neil Griffiths said he had been reassured of CGI’s expertise in this area.
Kieran Murphy asked about the digital maturity assessment and the Trust’s readiness and capability. Neil Griffiths said UCLH had made significant improvements in the past three months; the assessment had been done prior to e-case notes and pathology e-ordering.
The Chairman asked about risk appetite and it was agreed future reports would set this out more clearly.
The Board endorsed the Information Governance Strategy 2016-2018
7/9.2 Board Assurance Framework 2016/17 Opening Position
The Board Assurance Framework for 2016/17 Opening Position had been reviewed by the Audit Committee and the Board had given input at a Board Seminar on risk.
The Chief Executive updated the Board on the Specialist Tariff risk (set out on page 7). Although the Trust had received confirmation that HRG4+ would be implemented, Tim Jaggard advised that this would likely be transitional over a number of years.
It was proposed that the risk of insufficient trained nurses nationally and/or restrictions on agency/immigration controls leading to ongoing high nursing vacancy rates (set out on page 4) should be removed from the BAF. The Chairman felt that the removal of this risk should be reconsidered; the Board agreed the risk should be reviewed to take account of the current situation.
Action: Director of Workforce
The Chairman asked that the BAF focus more on risks rather than concerns identified and the Chief Executive confirmed that the BAF would be reviewed by the Executive Board a week before the Board meeting.
5

7/9.3 7/9.4
The Board endorsed the removal of only one risk highlighted on page 9 of the BAF which related to the alignment of Electronic Staff Record and Finance systems. Capital and Estates Issues The Board endorsed the granting of a three year lease to the British Medical Acupuncture Society for the occupation of space at the Royal London Hospital for Integrated Medicine and the extension of a lease to TDL relating to their use of space at 250 Euston Road, subject to the agreement of terms. Policies The Board noted that the Executive Board had approved the following new policies:
• Intellectual Property Rights (IPR) Policy • Chaperone Policy • Parking and Traffic Management Policy
7/9.5 7/9.6 7/9.7
There was discussion about the IPR Policy, and what expertise was available at UCLH to support IPR. The Chief Executive explained that arrangements were set out in the policy. UCLH had reached an agreement with UCL about how IPR would be managed between the two organisation. David Lomas confirmed the position of the BRC in relation to IPR and spin outs. UCL Business supported the process from licencing to spin outs and woul focus on supporting spin outs in the next five years. The Board also approved the revised Complaints Policy, subject to inclusion of the amendments requested by Harry Bush. Medical Devices Maintenance and User Training The report was noted. UCLH Nursing, Midwifery, Allied Health Professionals and Pharmacy Strategy 2016-2021 The report was noted. Communications and Marketing Update The report was noted.
7/10 Performance Report Simon Knight presented the report for May and said we had been below the STP trajectory of 90.9% in the Emergency Department due to high demand, bed pressures and specialty response time. Performance in the Urgent Treatment Centre (UTC) had been between 97% and 98%. Charles House advised that he chaired a weekly ED performance improvement meeting focussed on meeting the 4 hour target and improving patient flow. UCLH was working closely with Camden to improve access to step down beds and enhanced community support, e.g. for stroke patients. The early part of July had continued to be difficult with a high number of attendances and a high acuity of admissions.
6

The current focus was to maintain/improve performance in the UTC, reduce variation in practice and ensure that staffing levels remained resilient over the holiday period. Very few patients were admitted into the hospital from the UTC. Regarding diagnostic waits this continued to be challenging and the May STF trajectory of 97% had not been met. Positive progress had been made both in reducing the number of endoscopy breaches and the endoscopy backlog.
Work was also underway to balance Queen Square MRI demand and capacity and clear the backlog of patients waiting more than six weeks, using some outsourcing. However the backlog had been increased by the discovery of additional MRI patients, identified through a review of waiting lists. Gill Gaskin outlined the issues: requests for Queen Square imaging were made electronically via the CDR and these requests went through to the Radiology Information System (RIS) which then tracked patients through the process of request, triage, booking, scanning and reporting. An extract from the RIS was used to form a waiting list, which was used on a weekly basis to confirm that all requests had been actioned. A change had been made to the waiting list extraction algorithm in 2013 which led to some patients becoming ‘invisible’ and therefore omitted from the check that a booking had been made. The issue was identified when a consultant raised a concern about a patient wait and this had led to a review of the waiting lists. A review was underway of each patient apparently omitted from the waiting list. This had identified 827 who appeared not to have had the test requested and who might still need imaging; in approximately half, the requested test was an MR scan. Cases were being reviewed individually by experienced radiographers to establish if equivalent tests had already been provided (and some have been). If these were not identified, consultants would then review case records to see if imaging was still necessary. The review was at an early stage, but not all patients needed a test to be booked. To date, there was no evidence of patient harm. Gill Gaskin advised that there was a separate process for urgent requests which were dealt with on the day of receipt.
A second issue had impacted on the Queen Square Imaging backlog reporting which related to the system for separating requests on receipt into two categories – those to support treatment decisions which were subject to the 6 week wait target, and those for a surveillance scan on a specified future date which were not subject to the target. Some tests had been inappropriately labelled as surveillance scans and excluded from the 6 week target counting. This had now been corrected, adding to the number waiting. Together with the underlying capacity pressures, these two issues meant that additional MR capacity was needed at Queen Square, and this was being sourced via additional capacity on a mobile unit, and securing additional private provision. Gill Gaskin was asked to report back to the Board on when we would achieve compliance including these additional cases. Kieran Murphy suggested that we review the data to see whether the failure to undertake requested scans had made a difference to the patient outcomes.
Action: Medical Director, Specialist Hospitals
7

Concern was expressed about whether this could be happening elsewhere within the Trust. The Chief Executive could not reassure the Board that this situation could not happen again as there could always be operator errors. The Deputy Chief Executive advised that the Audit Committee would look at data quality and integrity as a matter of urgency.
Caspar Woolley said that we needed to develop a closed loop system so that requests which were not processed could be identified. The Chairman agreed to refer this to the QSC for discussion.
Action: Chairman With regard to cancer waits Simon Knight advised that the Trust was not meeting its STP trajectories. He confirmed that arrangements were in place with the Harley Street Clinic to outsource breast cancer appointments; this was helping us reduce our two week wait backlog. Geoff Bellingan advised that the 31 and 62 day targets were proving difficult to meet because of the overall number of cancer pathways which meant there could be no more than 6 breaches per month across 17 different pathways. The Chief Executive said that the target had been set at 85% to recognise complexity. Geoff Bellingan explained that every breach was examined to identify the reason for the failure to achieve the target. Caspar Woolley asked why these trajectories had been set three months earlier if they could be achieved. The Chief Executive said that STP funding would only be received if the trajectories were met. Geoff Bellingan was asked to circulate a note to the Board setting out a plan to meet the cancer targets.
Action: Medical Director, Surgery and Cancer Harry Bush raised theatre activity and said there appeared to be no trend of improvement in this area, despite previous discussions about improvements which could be made. Caspar Woolley also noted that although the position on elective activity was improving, the gap was widening on non-electives and the trend was downwards. He felt that the information could be presented differently to make it clearer. The nursing dashboard on recruitment was discussed. The Chairman thanked Ben Morrin and Flo Panel-Coates for their achievement over the past year in reducing vacancy levels. Ben Morrin confirmed that UCLH had the lowest nursing vacancy rates in London. The Chairman commented that, despite this work, the turnover of qualified nurses was 14% and the rate for nursing assistants was 25% to 28%.
7/11
Report of the Audit Committee meeting held on 24th May 2016 Rima Makarem presented the report which was noted. The Board agreed to extend the External Audit Policy for one year.
8

7/12 7/13
Minutes of the Audit Committee held on 19th April 2016 The minutes were noted. Entries in the Seal Register The report was noted.
7/14 Any Other Business Board members offered Sir Robert Naylor their appreciation and gratitude for his years of outstanding performance which had benefitted UCLH and its staff and patients. The Board wished him all the best for his retirement and new endeavours.
7/15
Date of Next Meeting The next meeting would be held on 14th September 2016.
9


B
Agenda Item 3
Matters Arising Report


UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
BOARD OF DIRECTORS
REPORT ON MATTERS ARISING FROM THE MEETING HELD ON 13th JULY 2016
Minute no.
Issue Action
7/4 Matters Arising report: business case for blood tracking system
This issue is referred to in the Executive Board report. Action completed
7/6 Presentation on Social Media –
• Annual presentation
• Involve Patient Experience Committee in the work
This has been added to the schedule of presentations for 2017.
The Board agreed that a small working group should meet to agree the Trust’s online development strategy. The group includes Lisa Anderton as the PEC representative. The first meeting will take place later this month.
7/9.2 Board Assurance Framework:
• Review risk associated with insufficient trained nurses
The Workforce Director and Chief Nurse are monitoring the impact of Brexit on retention, recruitment and the employment markets from which we recruit. At this stage, their assessment is that adding a new risk to the BAF is not justified.
7/10 Performance report: Plans to achieve compliance with targets: MRI at Queen Square and Cancer
A report is attached to the EB report which addresses these issues. Action completed
Items from previous meetings brought forward
Date of Meeting
Minute no.
Issue Outcome
March 2016
3/8.5 Executive Board report: Volunteers Service – further update
An update is included in the EB report. Action completed

Items from previous meetings carried forward to future meetings
Date of Meeting
Minute no.
Issue Outcome
March 2016
3/9 Performance Report: Longer term performance graphs
The graphs will be included in the September Performance report which will be presented to the Board in November, in order to capture a complete half-year’s data. Graphs showing trends for the second half of the year will be included in the Month 12 Performance Report that will be submitted to the Board next May.

C
Agenda Item 6
Chairman’s Report


UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
CHAIRMAN’S REPORT TO THE BOARD OF DIRECTORS
14 SEPTEMBER 2016
1. SIR ROBERT NAYLOR
Although Sir Robert Naylor is unable to attend this Board meeting, it is the last meeting of his term as Chief Executive. It is difficult to exaggerate what Sir Robert has done at UCLH in the 16 years as Chief Executive. He has been an immensely strong and clear sighted leader and should take great credit for the many excellent things that UCLH does today for its patients. He has overseen a significant rebuilding programme, notably the new University College Hospital which opened in 2005. He has been one of the foremost exponents of the benefits of Foundation Trust status and one of the leading strategic thinkers in the NHS. He has been a strong advocate of the model of clinical leadership which is now being more widely replicated around the NHS. For me, he has been an outstanding colleague and I very much appreciate the opportunity of working closely with him over the last 6 years. I know that he still has a great deal to contribute to healthcare, both in the UK and overseas, and I am sure that Board will join me in wishing him every success with his future plans.
2. PROFESSOR MARCEL LEVI Marcel Levi, as previously announced, joins UCLH as Chief Executive on 3 January 2017. He has a number of visits planned between now and then to get to know us better and will already have visited twice by the time of the Board meeting. I spent the day with him in Amsterdam on 1st August when we had quite detailed discussions about UCLH and I was able to visit his existing hospital and understand more about his role there. I know that Professor Levi intends to meet as many people as he can before starting formally in the New Year.
. 3. PROFESSOR SIR DAVID FISH
Professor Sir David Fish, Managing Director of UCLPartners and former Medical Director at UCLH, has announced his intention to retire on 27 September. Sir David had a distinguished career as a clinician and a senior manager at UCLH and, since 2009, has been an extraordinarily successful first Managing Director of UCLP. Through his tireless efforts and great qualities he has firmly established UCLP as the leading AHSC/AHSN in the country. He has overseen significant reconfiguration in the sector (notably cardiac/cancer) and more recently has played a key role in the reorganisation of healthcare in Essex. He has been a good friend to UCLH and to me personally during his time at UCLP and was particularly helpful during the Chief Executive recruitment process. Again, I am sure the Board will join me in thanking him for all he has done and wishing him a long and happy retirement. Arrangements are in hand to recruit a successor to Sir David for this critical role.
4. GOVERNOR ELECTIONS Voting for the Council of Governors closed in July. The results of the 2016 elections were as follows: Public: Maggie Gormley London Based Patient: Veronica Beechey – (re-elected)
Emma Dalton – (re-elected) Graham Cooper Jo Wagerman
Non-London based Patient: Gareth Long (elected unopposed)
1

Staff: Other Clinical Jessica Lipman (elected unopposed) Staff: Non-Clinical Janet Clarke Staff: Nurses & Midwives Josie Gladney (elected unopposed) I would like to congratulate everyone on their election and look forward very much to working with them.
5. BIOMEDICAL RESEARCH CENTRE BID
The Board is due to hear at the meeting from Professor Bryan Williams, Director of R&D, about the recent bid for renewal of our BRC status. I attended one of the rehearsal interviews on 8 July and was very impressed by the quality of the written and oral submissions and by the thoroughness of the preparation. At the time of writing, we still await the result of the bid.
6. LONDON CHAIRS MEETING On 11 July I hosted a meeting of a group of London Acute Trust Chairs to discuss matters of mutual interest. These sessions, which tend to happen about twice a year, are a useful forum for an informal exchange of views and sharing of experiences. A broader session, to which all London Chairs have been invited, is being separately organised for later in the autumn.
7. NHS IMPROVEMENT CHAIRS IMPROVEMENT PARTNERSHIP In a similar vein, NHS Improvement organised a group of some 25 Chairs from around the country and not just acute Trusts, to meet around three times a year and the latest meeting took place on 25 July. Inevitably there was a lot of discussion about financial pressures and everyone’s experience of Sustainability and Transformation Programmes.
8. VISIT BY THE DUCHESS OF CORNWALL On 8 September, HRH Duchess of Cornwall is due to visit the Podiatry Department at the RLHIM. The Duchess will be here in her role as Patron of the Royal College of Podiatrists and expressed an interest in having a site visit to one of the College’s faculties. Tariq Khan, Deputy Director for Podiatry and a member of the Royal College of Podiatrists, has helped to facilitate this visit.
9. WALKABOUTS I have started a new series of walkabouts approximately every 10/14 days with each of the Deputy Chief Nurses. My aim is to visit more regularly as many of the areas of the hospital as possible and we are trying to make sure that a non-executive colleague will join me as often as can be arranged. As ever, these sessions provide an opportunity to talk informally to staff and patients.
RICHARD MURLEY CHAIRMAN
2

D
Agenda Item 7
Chief Executive’s Report


1
UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
CHIEF EXECUTIVE’S REPORT TO THE BOARD OF DIRECTORS
14 SEPTEMBER 2016
PART ONE
1. SIR ROBERT NAYLOR
As referred to in the Chairman’s report, Sir Robert Naylor is unable to attend this Board meeting due to his annual leave commitments. This meeting is the last of his term as Chief Executive of UCLH. I have referred to the CEO transition arrangements in more detail further in this report but I would like to record my thanks to Robert for his strong leadership of UCLH over the last 16 years. His commitment and vision has shaped UCLH into what it is today and his legacy is the provision of top quality patient care, excellent education and world-class research. I am sure the Board will join me in wishing him well with his future plans.
2. NHS IMPROVEMENT – OPERATIONAL PLANS 2016/17
Attached as Appendix ‘A’, is a letter from NHS Improvement which confirms their acceptance of our 2016/17 operational plans. They have emphasised the importance of meeting our commitments to delivering safe care for patients within our resources. They have also emphasised the importance of our participation and supporting the Sustainability and Transformation Programme (STP) in the local healthcare system. They have no undue concerns about our plans but will be holding us to account for our delivery as we progress through the year. In line with their request we have published our plans on our website.
3. NHS IMPROVEMENT - Q1 2016/17 MONITORING
NHS Improvement has confirmed our finance risk rating of 2 and a governance rating of green. They have however raised concern about the failure to meet the 4-hour A&E standard and multiple cancer standards. They expect us to take prompt action to improve performance in these areas and have indicated that further intervention will be needed if performance does not improve. A copy of their letter is attached at Appendix ‘B’. We are working closely with Camden CCG to address a number of performance concerns, which include those raised by NHS Improvement.
4. CEO TRANSITION ARRANGEMENTS
While I am Interim Chief Executive, I have appointed Martin Wilson as interim Director of Improvement until 3 January 2017 to cover the key areas of my Deputy Chief Executive duties. He will lead on uclh future and Simon Knight, Director of Planning and Performance and his teams will report to Martin. He will also work closely with the Medical Directors and their teams. I will continue to lead on EHRS and digital services. Tonia Ramsden, Director of Corporate Services will chair the Risk Co-ordination Board and I plan to disband the Transformation Steering Group which focussed on uclh future. Issues from this monthly meeting will be considered by the Executive Board. Laura Churchward, who is covering as Interim Director of Strategic Development will begin her maternity leave from November. Catherine Pollard will join us from NHS Improvement to cover her role. As well as maintaining a focus on phase 4&5 she will also help develop UCLH’s role within the STP. Jonathan Gardiner will take on the role of Interim Deputy Director of Strategic Development moving from London Cancer to support Catherine. These arrangements remain in place for 12 months.

2
I am also pleased to announce that Dominic Firth has been appointed to the new post of Director of Commercial and Contract Management reporting to Tim Jaggard, Finance Director from 12 September. This post will focus on developing our commercial capability. Mike Foster, Director of Commissioning, will also be leaving us at the end of September. I am sure that the Board will wish to thank Mike for the excellent contribution he has made to the Trust in his time here. We wish him every success for the future.
5. CQC REPORT AND QUALITY SUMMIT
The Board will already be aware that the Care Quality Commission (CQC) rated UCLH as ‘Good’ in its inspection report published on 11th August 2016. We were very pleased with the rating which was a significant achievement and are grateful to our staff for the time spent preparing for the inspection and for their dedication to improving the care for our patients. Only a few London Teaching Hospitals have achieved this rating.
On 2 September 2016, we held a Quality Summit with the CQC and a range of stakeholders including representatives from the NHS England, NHS Improvement and our local Healthwatch. Professor Ted Baker, who led the CQC inspection said that the report was ‘very, very good’ and we should be proud that our DGH services are so highly rated as this can be a challenge for highly specialised trusts.
Robert Naylor presented our response to the report. All areas covered in the report would develop action plans, this included in the emergency department where action had already been taken to revise the model of care following a staff listening event. However, he also raised our disappointment about the timescale for the turnaround of the report which led to many factual inaccuracies remaining in the report despite being highlighted to the CQC.
Stakeholders agreed that it was a positive report but asked that the Trust also address some of the basic administrative issues and processes linked to IT. These are areas of work that form part of the uclh future programme.
We are developing a CQC action plan to deal with the key issues and have set up a CQC Executive Steering Group to oversee the delivery of that plan, the steering group will report to the Quality and Safety Committee.
6. JUNIOR DOCTORS INDUSTRIAL ACTION
The Board will be aware of the formal notice issued by the BMA on 31st August 2016 that its members intended to take industrial action for five consecutive days from 12th September between 8:00am and 5:00pm. The Trust’s business continuity planning process was immediately initiated to ensure we would be able to provide emergency services, urgent care provision and patient safety throughout the proposed period of action. This planning was led by the Medical Directors and Director of Workforce. This week the BMA suspended this proposed action in recognition of the lack of notice given for such action, but has announced its intention to take action as planned in October, November, and December between 8:00am and 5:00pm on the following dates:
5-11 October 2016 (break for weekend)
14- 18 November 2016
5- 9 December 2016 The action proposed in each instance is full action, with no emergency care provision. We are continuing our business continuity planning in preparation for the October.
Each division is developing a business continuity plan for its area, ensuring emergency services and urgent care provision can be maintained during the action;

3
The planning steering group for junior doctor action, chaired by the Director of Workforce,will review these plans and all arrangements to mitigate the impact of action on ourservices and patients;
We are working with UCL to ensure that our clinical academic staff prioritise clinical workwhen action is taken; and
We are looking at leave arrangements for the dates announced to minimise staffabsence.
I should also advise Board Members that new guidance has recently been issued from NHS England requiring the Board to sign off submissions to NHSE relating to the industrial action. This is to make sure that Boards are fully assured of the plans being taken to ensure patient safety during the action, and that trusts can recover from the impact of action.
7. NCL STP
A number of the Executive Directors attended the North Central London STP ‘lock-in’ which took place on 5th and 6th September at the King’s Fund. The intention of this exercise was to build on the work already completed through the STP and accelerate thinking to improve the overall plan. There is a new submission date for the STP which is now 21st October 2016.
The event was helpful and attended by around 70 senior leaders from North Central London. The lock-in itself did not produce any new ideas but focused on the existing workstreams as follows:
out of hospital care
productivity
consolidation
strategic narrative
developing new delivery and commissioning models
We continue to actively support the development of the STP.
NEIL GRIFFITHS DEPUTY CHIEF EXECUTIVE

NHS Improvement is the operational name for the organisation that brings together Monitor, NHS Trust Development Authority, Patient Safety, the National Reporting and Learning System, the Advancing Change team and the Intensive Support Teams.
Sir Robert Naylor Chief Executive Officer University College London Hospitals NHS Foundation Trust 2nd Floor Central 250 Euston Road London NW1 2PQ
2 August 2016
Dear Sir Robert,
Operational plans 2016/17
Thank you for submitting your final operational plan for 2016/17. I am writing to acknowledge receipt of your plan and to highlight the next steps.
‘Delivering the Forward View: NHS Planning Guidance 2016/17 – 2020/21’, set out our expectations for delivering high quality, sustainable services for the patients and communities that we serve. I would like to take this opportunity to recognise the significant work that has gone into delivering a clear plan for 2016/17 during a challenging period for the NHS.
It is critical that each trust meets the commitments in its annual plan to deliver safe, high quality services and the agreed access standards for patients within the resources available. This will mean maintaining an effective balance between demand and capacity and continuing to develop the workforce needed for local services.
The planning guidance also set out the steps to help local organisations deliver a sustainable, transformed health service and meet the three gaps identified in the Five Year Forward View: health and wellbeing; care and quality; funding and efficiency. This highlights the importance of your strategic work to help create a sustainable organisation as part of a strong local health care system with agreed Sustainability and Transformation Plans.
To this end, NHS Improvement will continue to work with trusts to review progress against your plans and to support you in the delivery of the required standards in line with our new oversight model.
Wellington House 135-155 Waterloo Road
London SE1 8UG
Email: [email protected] Tel: 020 3747 0000
www.improvement.nhs.uk
Chief Executive's ReportAppendix A

NHS Improvement is the operational name for the organisation that brings together Monitor, NHS Trust Development Authority, Patient Safety, the National Reporting and Learning System, the Advancing Change team and the Intensive Support Teams.
Next Steps Following our review of your plan, NHS Improvement has no undue concerns. However, we will be holding the trust to account for delivering 2016/17 CIP and financial trajectory through the year. NHS Improvement will undertake on-going monitoring, support and escalation as necessary against the specific areas identified in this letter and the key domains and indicators outlined in the NHS Improvement oversight model. In addition, we would request that Trusts publish their finalised plan summaries on their websites by 26 August 2016 and advise their NHS Improvement regional relationship manager when this has been completed. We will continue to work with you to ensure you are able to access the necessary development support to strengthen the Trust’s capability and capacity for delivery. Our central commitment to delivering a strong provider landscape can only be achieved through your success. We will ensure that wherever possible we support you to deliver your ambitions. In return, our expectation is a simple one - that the commitments you make through this planning round and through locally agreed contracts are delivered in full.
If you wish to discuss the above or any related issues further, please feel free to contact me or a member of the team. Yours sincerely
Victoria Woodhatch Portfolio Director NC&E London NHS Improvement

31 August 2016
Sir Robert Naylor Chief Executive University College London Hospitals NHS Foundation Trust 2nd Floor Central 250 Euston Road London NW1 2PQ
Dear Sir Robert,
Q1 2016/17 monitoring of NHS foundation trusts
Our analysis of your Q1 submissions is now complete. Based on this work, the trust’s current ratings are:
Financial sustainability risk rating: 2
Governance rating: Green
These ratings will be published on NHS Improvement’s website in September.
NHS Improvement is the operational name for the organisation which brings together Monitor and the NHS Trust Development Authority. In this letter, “NHS Improvement” means Monitor exercising functions under chapter 3 of Part 3 of the Health and Social Care Act 2012 (licensing), unless otherwise indicated.
The trust has been allocated a financial sustainability risk rating of 2 in line with the trust’s
plan, but has failed to meet the A&E four hour standard and multiple cancer standards.
NHS Improvement uses the above targets (amongst others) as indicators to assess the
quality of governance at foundation trusts. A failure by a foundation trust to achieve the
targets applicable to it could indicate that the trust is providing health care services in
breach of its licence, which could lead to consideration of enforcement action1.
We expect the trust to take prompt action to improve performance against these access
standards and achieve sustainable compliance with the targets in line with its submitted
improvement trajectories. NHS Improvement has decided not to open an investigation to
assess whether the trust could be in breach of its licence at this stage, but will consider
further action if performance does not improve. At this time the trust’s governance rating will
remain as ‘Green’. Should any other relevant circumstances arise, NHS Improvement will
1 Under the Health and Social Care Act 2012, taking into account, as appropriate, our published guidance on
the licence and enforcement action including our Enforcement Guidance (www.monitor-nhsft.gov.uk/node/2622) and the Risk Assessment Framework (www.monitor.gov.uk/raf).
Wellington House 133-155 Waterloo Road London SE1 8UG
T: 020 3747 0000 E: [email protected] W: improvement.nhs.uk
Chief Executive's ReportAppendix B
consider what, if any, further action may be appropriate. In the meantime we will work with
you to support and enable improvement in these areas; and the relationship team will be in
touch shortly to discuss next steps.
A report on the aggregate performance of all NHS providers (Foundation and NHS trusts) from Q1 2016/17 is available on our website (in the Resources section), which I hope you will find of interest. For your information, we have issued a press release setting out a summary of the report’s key findings. As discussed in our Q1 meeting, there will be a number of changes in roles within the relationship teams at NHS Improvement as we implement the new structure. If there are any changes to your relationship team we will ensure you are informed as soon as possible. If you have any queries relating to the above, please contact me by telephone on 020 3747 0619 or by email ([email protected]). Yours sincerely,
Victoria Jeffries Senior Regional Manager cc: Mr Richard Murley, Chairman,
Mr Tim Jaggard, Finance Director

E
Agenda Item 8
Executive Board Report


UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
Executive Board Report to the Board of Directors, September 2016
1. Electronic Patient Identification System for Blood Transfusion Services
Board members will recall that the Quality & Safety Committee had asked the EB toevaluate the benefits of introducing an electronic blood tracking system. At the lastBoard meeting it was reported that the EB had supported a proposal in principle,following which a business case was submitted to the Capital Investment Board (CIB)and agreed subject to review by ICT.
Subsequently, the CIB made a recommendation to the EB that the system should beimplemented. The Medical Directors were satisfied that this scheme will improvepatient safety and experience, as well as reducing costs over time by eliminating thecurrent requirement for two separate blood samples to be taken and processed. TheEB approved the scheme.
2. Performance Issues – Queen Square MRI, Diagnostics and Cancer Waits
The EB received an update which set out the current performance against trajectoriesfor key access targets and actions underway to achieve compliance with standards.The Board will recall the lengthy discussion on these issues at the last meeting. Thereport is attached at appendix A.
3. uclh future Programmes Update
The EB reviewed a progress report on uclh future which included RAG ratings for eachof the programmes based on actual year-to-date savings against forecast. While anumber of programmes are behind plan at Q1, many are forecast to make progressduring the year. Although there is a shortfall on savings from uclh future schemes thatshould contribute to the CIP built into the Trust’s financial plan, other areas of the CIPare over-performing.
The EB discussed whether there may be a need at a future time to consider investingmore in these schemes to ensure progress was made, or to change the focus of theprogrammes. However, EB members acknowledged that improvements to patient careand positive system changes are being achieved and, overall, the project is moving inthe right direction.
A progress report is attached at appendix B.
4. Volunteers’ Service
Earlier this year the Board received a report on the development of the volunteers’service, how they were recruited and trained, and priorities for the short to mediumterm. It was agreed that a further update would be presented after six months.
The EB received the Annual Voluntary Services report for 2015/16 which highlightedthe significant changes and investment made in new initiatives during the year. Theseinclude:

• A new centralised recruitment and induction process for all volunteers involvingadvertisements on the jobs section of the Trust website, an initial telephoneinterview followed by a group assessment session, before a full day groupinduction. This includes infection control and fire safety training and a tour ofhospital sites.
• An ongoing training programme designed to complement volunteering, includingsessions on learning disability, wheelchair training, being a dementia friend,mealtime assistance and anti-boredom training.
• Introduction of a system whereby volunteers give a regular commitment to onespecific ward or area, rather than visiting several wards during their shift. This hasenabled volunteers to become integrated members of the team and make more of adifference to patients.
• A new manager for Citybeat UCLH Hospital Radio has been appointed; a review ofthe service was undertaken and there are plans in place to make it more interactivewith patients.
• At the end of 2015/16 there were 233 active volunteers, with over 80 new volunteerroles in development across all sites.
Further progress has been achieved in Quarter 1 this year;
• There are now 247 active volunteers and an additional 80 recruits are about tocommence.
• Several volunteers visit UCH and the NHNN regularly with their Pets as Therapydogs.
• There are now volunteers at all our hospitals and the team are working on increasingnumbers specifically at the Queen Square site.
• In Q1 volunteers gave 3218 hours of their time and supported patients 39,083 times.• Additional support to the team has been provided by UCLH Charity who have
agreed to fund a new apprentice position (due to commence this month). This postwill help the voluntary service team to focus on increasing numbers to achieve theambition of having 500 active volunteers.
• Current work is aimed at encouraging non clinical staff to volunteer as diningcompanions/mealtime assistants during their lunchtimes or immediately after work.Initially focusing on one ward in the Tower, the project will be rolled out to otherwards if successful.
• During Volunteers Week a celebration was held to thank volunteers for their support. Itwas attended by over 40 people.
The Annual Voluntary Services Report will be published on the volunteering pages of the website.
5. Pathology e-Requesting
In October last year the EB approved the purchase of a new electronic requesting system for pathology tests as an interim solution ahead of the introduction of EHRS. The key objectives of the new system are to minimise request errors by supporting users to request the right tests at the right time, and provide the organisation with robust data.
Recently, the EB received a progress report on the implementation of e-requesting. There has been intensive work over the past three months to design, configure and test the system and it is now planned to pilot it on two UCH wards in October, following which will it will be evaluated and rolled out Trust- wide over a two month period. Training will be delivered via a short e-learning package and ‘how to’ guide that will be
2

disseminated to all users. However the system is considered to be fairly intuitive and many clinicians will have used a similar system elsewhere. One outstanding issue is the plan to include the prices of tests on the system to discourage unnecessary requests and thus lead to savings. The system also has demand management capability, such as flagging up when tests had been requested previously, which should also help to reduce pathology testing costs. 6. “Stronger Together”: The UCLH Nursing, Midwifery, AHP and Pharmacy Strategy
2016-2021 This document, which has been circulated separately to Board members, outlines the Trust’s five year strategy for Nursing, Midwifery, Allied Health Professions and Pharmacy. This is the first joint strategy the Trust has developed; it identifies high level strategic priorities for these professions and is closely aligned with UCLH’s strategic objectives and with the national nursing, midwifery and care staff strategy, ‘Leading Change, Adding Value’, launched in May. The strategy has been developed following a series of discussions and events over a number of months. It has been led by the Chief Nurse, with senior clinical leaders in nursing, midwifery, AHP and pharmacy and with engagement from a broad representation of nurses, midwives, AHPs and pharmacists, and from patient governors, medical and management colleagues. Annual objectives have been identified for 2016/17 and progress will be monitored quarterly by the Nursing & Midwifery Board which includes the AHP and Pharmacist lead for the Trust. 7. Influenza Vaccination Programme 2016/17 Each year all trusts are required by the Department of Health to provide assurance that
programmes are in place to immunise frontline health care workers against influenza. This year a CQUIN target for flu vaccination has been set which requires at least 75% of frontline staff to be vaccinated by the end of December 2016 if trusts are to receive 100% of funding. Achievement of between 65% and 74% will attract 50% of the payment, with no payment received for less than 65%.
Last year 57.8% of frontline clinical staff were vaccinated. The EB endorsed an
approach to ensuring that uptake is significantly increased this year, to further protect patients and staff. This will include a visible and sustained campaign with named ‘flu champions’ to promote uptake, greater availability of the vaccine in the workplace and a variety of approaches to delivery of vaccinations, such as peer vaccinators running clinics within their own departments and regular visits to all wards and departments to administer the vaccine to staff on duty. The communications team have been asked to develop a campaign plan focusing on posters, daily information on the intranet and a variety of other communication channels to raise awareness of the importance of immunisation.
Supplies of the vaccine have been ordered and will be available at the end of
September but the EB agreed that the publicity campaign should commence as soon as possible. The Board is requested to support the approach outlined above.
3

8. Infection Control Annual Report
The EB received the Infection Control Annual Report for 2015/16 which summarisesthe work undertaken in the Trust. The report had been reviewed by the Quality &Safety Committee. It is attached at appendix C.
9. Information Governance
Each year NHS Digital, previously the Health and Social Care Information Centre,reviews and refreshes the Information Governance Toolkit (IGTK) requirements onNHS trusts to ensure they represent industry-recognised best practice in informationgovernance, and to resolve any issues identified in the previous version. The toolkithas six standards covering issues such as IG Management Assurance, Confidentialityand Data Protection Assurance and Clinical, Corporate and Secondary UseInformation Assurance. The standards comprise a number of requirements, 45 ofwhich apply to acute trusts.
Each requirement has three levels; level three objectives consist of two parts; standardelements and those which must be re-evidenced on an annual basis to maintaincompliance. These requirements automatically lower a trust’s score when the baselineassessment is submitted. At the same time trusts make an assessment of the scoresthey think they will be able to achieve by final submission in March of the followingyear. Those levels are used to calculate a target score. Our baseline score in July2015 was 66%, with a final year end score of 77% in March 2016.
The latest version of the IG Toolkit has now been reviewed and a baseline complianceassessment has been completed. There are a number of changes to the requirementsof the toolkit this year, the majority of which sit within the secondary use assurancerequirements.
UCLH has submitted a baseline score of 66% based upon our current evidence andthe higher target levels expected for this version of the toolkit. Starting the year with alower opening score in comparison to the closing score from the previous toolkit isnormal and expected, given that a range of the current toolkit evidence requiresupdating during the 2016/17 reporting year.
Based on an assessment of the Trust’s ability to collate evidence and improve itsprocesses to meet the toolkit requirements a target score of 86% will be submitted. Aplan of overarching actions to ensure the target score is reached will be monitored bythe Records and Information Governance Group reporting to the Digital ServicesDelivery Board.
SIR ROBERT NAYLOR CHIEF EXECUTIVE
4

Executive Board Report Appendix A
A) Elective access update: Diagnostics and RTTSeptember 2016
1. Introduction and Executive Summary
This document provides an update to the trust board on diagnostic and elective waiting time performance. We continued to prioritise meeting these challenging patient access targets.
We are not achieving our STF trajectory for diagnostic waits. This is driven by non-compliance in neuro-MRI and ultra-sound. Positively, we achieved the standard for endoscopy in July.
We have completed the consultant level review of the cohort of additional neuro-MRI patients that were identified recently and are the subject of the current SI. To date we have identified no clinical harm. We have full visibility of the neuro-MRI demand and have secured considerable additional outsourced capacity to treat all patients and address the underlying capacity gap. We are projecting compliance against the standard for November in neuro-MRI, which will lead to overall trust compliance in the same month.
Although we have had strong performance against RTT standards we are closely tracking recent increases in our RTT backlog. We are still achieving the 92% standard, but have identified a series of actions we need to take that will maintain delivery of this standard in the short term, with issues such as additional data validation, confirmation that all patients are being booked in turn and the provision of additional capacity in high volume specialties to reduce the number of patients waiting more than 18 weeks for treatment.
2. Diagnostics six week wait performance
Performance against the STF trajectory for diagnostics is as follows (the standard is 99%):
April May June July Aug Sept Oct Nov Dec Jan Feb Mar
Diagnostics trajectory96.0% 97.0% 97.7% 98.3% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Diagnostics actual 94.4% 95.4% 93.7% 96.3%
Within the STF framework there are no monies attached to achievement of the diagnostics trajectory, so this does not represent a financial risk. However, we do have a contract performance notice in place from our local CCG and they may be able to levy contractual fines on that basis (although our overall assessment is that the terms of the STF trajectory protect us from contractual fines). We are now planning to deliver compliance in November.
July performance has improved. Endoscopy achieved compliance at modality level as planned and we now need to ensure ongoing compliance. Areas of non-compliance were:
• 59 breaches in non-obstetric ultrasound, which is a decrease from 68 in June. This is beingdriven by a lack of sonographer capacity. The division is recruiting for an additional post;undertaking in-house training funded by HEE and has increased its outsourcing in order toreduce the backlog.
• 249 breaches in MRI – 244 of which were in Queen Square. These did not include thepatients subject to the Serious Incident investigation (see section below). The division hasincreased its capacity through outsourcing and review of weekend working. Includingclearance of the SI backlog, we are projecting compliance for November.
1

2.1 Queen Square MRI Performance Recovery Queen Square declared a Serious Incident following the discovery of a cohort of patients who had not been visible on the QS imaging waiting list. The parameters for the report have now been updated to correct this. Detailed consultant review of the requests has been completed. 188 patients still require imaging, of which 136 require MRI. There are no capacity pressures in the other, non-MRI, diagnostic modalities. No evidence of harm has been found to date; however, some patients require imaging to be completed before this can be definitively ascertained. The full SI report for this incident is due for submission by 27th September, but full assessment of whether any harm has occurred may only be possible once outstanding imaging has been completed. In addition to the SI issues we have secured additional capacity to manage increases in demand for MR at QS. Additional capacity has been secured through three different outsourcing contracts totalling an additional 910 scans each month. On this basis we return to 6 week compliance is from November onwards for MRI. As part of uclh future we have completed a detailed trust wide audit on current CT and MR demand and capacity. This has reviewed utilisation for each scanner and has benchmarked performance to others in the NHS. We are very much in the “middle of the pack” overall. However, we have identified issues (late starts, DNAs, planning, scheduling) that we can improve to further increase utilisation. 2.2 Improved Diagnostic Reporting One action within our diagnostics remedial action plan was to confirm that all relevant diagnostic activity is being captured against the 15 modalities in the monthly return. As part of this work, we have identified that not all patient waiting times were being reported on the monthly diagnostic waiting time return. The additional procedures that may require inclusion in the monthly reporting are across the non-obstetric ultrasound, barium swallow, audiology, echocardiography, neurophysiology, sleep studies, urodynamics and cystoscopy modalities. The waiting times for these range between zero and 13 weeks. However, some of these tests will not be reportable on the monthly return because they may be therapeutic or have a zero week wait. While these tests should have been reported externally, no impact on care is anticipated as the requests for tests are known within departmental systems and in many cases these pathways have been being tracked within RTT and cancer pathways. Clinical leads are being asked to undertake clinical risk assessments for each of the modalities where new reportable activity has been identified. 3. RTT incomplete pathways performance We have been consistently maintaining compliance with the 92% incomplete RTT standard since November 2014. We have seen an increase in our backlog over the last three months due to increased referrals and some specific capacity issues. The backlog has increased by 594 patients since the start of May to 2,512 patients (based on latest weekly snapshot). The key areas of increase have been at RNTNE, Queen Square and EDH. Positively, the number of waiters over 40 weeks is not increasing and we still have not reported any 52 week waiters. We are taking further action to address the increased backlog and will track this very carefully.
2

B) Cancer Waiting Times PerformanceSeptember 2016
1. Introduction and Executive Summary
UCLH continues to see significant growth for cancer services. Demand for 2 week wait appointments has increased by 53% (1,066 referrals more) from Q4 2014-15 to Q1 2016-17. However, we have not achieved the 62 day standard since May 2013. Whilst most breaches are driven by late referrals, we are also failing to achieve compliance within those pathways that start at UCLH (known as internal performance). Breast, head and neck and urology have been the tumour sites with the most internal breaches in 2015/16 to date.
Key actions to address include shortening waits at the front end of the pathway, implementing new, innovative models of care and improving our capacity resilience through call off contracts with independent sector providers in certain areas.
We are also working with referring trusts to reduce late referrals. Despite this, the volume of late referrals is far higher than we had assumed in our sustainability and transformation fund (STF) trajectory which means that our current expectation of achievement in October will likely not be delivered.
2. UCLH Performance
UCLH has not achieved the 62 day cancer access standard pathway since May 2013. Comparison against a national peer group indicates significant challenges for specialist cancer centres, with none of the hospitals included achieving the overall 62 day standard since January 2014.
Figure 1: 62 day performance – UCLH & peer group
Source: NHS England performance data and UCLH performance data
3

UCLH has also failed to consistently achieve the 85% standard for internal performance. In quarter one of the current financial year, there have been 27 internal breaches compared to a target level of 18 over the period required to achieve the target. The provisional internal performance for July is 82.2%, which is improved on previous months but is still below standard.
Figure 2: UCLH Internal and Overall 62 day Performance
Source: UCLH Cancer Performance data
3. Performance against sustainability and transformation fund (STF) trajectory The following table shows performance year to date against the STF trajectory (July performance is still provisional).
April May June July Aug Sept Oct Nov Dec Jan Feb Mar
Cancer 62 day trajectory 66.7% 73.7% 76.7% 80.3% 82.0% 82.0% 85.5% 85.5% 85.5% 85.7% 85.0% 85.7%
Cancer 62 day actual 70.9% 64.8% 58.7% 67.7% Quarter one monies are paid on the basis of agreeing the trajectories, so these are secure. There are significant risks to achievement of the monies in quarter two to quarter four. NHS Improvement will reconsider release of monies where trajectories have failed if we can demonstrate that we are delivering internal compliance and that we are treating referrals that we receive within a reasonable time-frame. 3.1 Internal Performance
Breast (9), Urology (5) and Head & Neck (5) account for 70 percent of these internal breaches. There are a variety of factors which result in breached pathways:
- Breast breaches relate to a service resilience challenge at the front end of the pathway which has now been resolved with outsourcing to the private sector. There were no breast breaches recorded in July.
4

- Urology breaches are caused by a combination of patient choice in deferring diagnostics or choice of treatment type, alongside some recognised capacity challenges for patients receiving HIFU treatment.
- Head & Neck breaches are typically complex pathways and require significant pathway innovation to achieve the 62 day standard consistently.
An additional pressure on achieving the cancer access standards concerns the growth in demand for services at UCLH. Demand for 2 week wait appointments has increased by 53% (1,066 referrals more) from Q4 2014-15 to Q1 2016-17. Three tumour pathways (skin, head & neck and breast) account for almost two thirds of this growth in demand. Performance delivery against the 2 week wait standard has been driven primarily by breast cancer, which has accounted for 53 percent of all 2 week wait breaches from September 2015 to June 2016. 3.2 External Performance
There has been significant engagement with referring hospitals to improve late referrals. Despite this, we are still seeing large volumes of late referrals. There have been 116 late referrals to UCLH in the first six months of 2016; three hospitals account for 82 of these late referrals;
• The Royal Free • Barking Havering and Redbridge • Barts Health
We have requested trajectories from each referring hospital to project the date by which they will be able to refer patients on time (before day 38). Based on these, we could not achieve a compliant overall position until January 2017 at the earliest (pushed back from October 2016 which is the STF trajectory). This is also dependent on the submitted trajectories being delivered, which has not so far been the case for all referring hospital during the first quarter of 2016/17. We have raised this with NHSE.
4. Priorities for action
Actions to achieve compliance against the cancer access standards are set out in a comprehensive action plan. Key actions to deliver internal compliance are as follows: 4.1 Resilience
- All tumour pathways have developed business continuity plans. - Effective outsourcing contracts have been established in a number of pathways,
particularly breast, for 2 week waits, and urology, for robotic surgery. - In highly specialised services where outsourcing is not an option, additional resilience is
being developed in house. For example, there has been an expansion of the Head and Neck Clinical Oncology service to increase the number of specialists from 2wte to 3.5wte. However, some specialities are proving more difficult to recruit effectively to, for example, securing a permanent consultant specialising in HIFU.
- There have been issues concerning resilience of MDT Coordinator support in some tumour pathways. A float MDT Coordinator has been recruited to help increase resilience of support to MDTs. An additional MDT Co-ordinator has also been recruited into GI.
4.2 2 week waits
- All tumour pathways have submitted plans to achieve a median 7 day wait for first appointments.
- Additional capacity has been identified to support improved performance in urology and gynaecology pathways.
5

- Improvement in Upper GI pathways is dependent on recruitment and retention of nurse endoscopists, which has been challenging.
4.3 Capacity
- Additional capacity has been generated in Urology for robotic prostatectomy pathways through increasing the number of patients per list.
- Work is underway in Imaging to deliver the timed milestones for diagnostics and is expected to include a case for both outsourcing and in house investment.
4.4 Pathway innovation and improvement
- Some pathways are inherently complex, requiring multiple diagnostics and complicated treatments. Head and Neck pathways are proving to be the most consistently complex. Pathway improvements planned include:
o Streamlining dental extraction for patients on radiotherapy treatment pathways. o Collaborating with experts in industry to shorten the process for planning
radiotherapy treatments through application of artificial intelligence. o Agreeing improvements to referral pathways from partner hospitals for patients
on surgical pathways to improve matching of capacity and demand.
- Recognising the complexities of inter-trust patient pathways, a significant project has been undertaken to develop single ratified timed pathways for the region. This work has been led by the London Cancer Tumour Pathway Board Directors and is supported by the UCLH Cancer Vanguard.
4.5 Improved cancer reporting - We are working to develop a new suite of cancer reports which will support tracking
staff and operational managers to track patients, and will also provide improved monitoring reports to managers. This will include predictive reporting.
- As well as a new suite of reports we will improve accessibility to the data held in infoflex, our cancer system. This will enable more responsive ad-hoc analysis of cancer performance as required.
- This work has started and we will start to see outputs from it by end October. 5. Next Steps We will continue to progress the current action plan to deliver improved cancer waits.
6

uclh future programme update
Summary
There has been good progress with the development of the CoordinationCentre, Exemplar Ward roll-out, As-Is plus, and OD which are all on plan.
The Diagnostics programme has produced an excellent productivityanalysis and is now progressing with implementing the recommendations(including running Improvement Week at University College Hospital from5 to 11 September and redesigning Queen Square’s referral and bookingprocess). Good progress made on pathology e-requesting, but theimplementation delay presents some risk to the delivery of financialbenefits in-year leading to the amber rating (although the team areaiming to recover by year end through targeted work with divisions).
The Elective and Theatres programme has produced a first draft scopefor discussion – there will be a more detailed presentation of theproposed work in September with forecast financial costs and benefits.
The Access and Patient administration programme is progressing well.A review of patient admin services (covering 850 WTE) is underway andsuppliers have been shortlisted for a new digital dictation and voicerecognition system for outcome letters. The programme is rated amberreflecting the risks around full 2016/17 financial benefits delivery. Thisrelates to the DNA reduction initiative, which uses predictive analysis totarget reminders. We have demonstrated, through a pilot of 5000 calls,that it is cost effective. Scaling up has been slower than anticipated.Recovery is forecasted by the year end.
Programmes of Care revised its delivery plan to take into account the2016/17 contract. It was agreed via TSG that in the short term theprogramme should refocus on the delivery of two CQUINs in 2016/17.Although most of the financial benefits of CQUINs have already beenaccounted for in operating budgets, there are no other mechanisms fordelivering this benefit across UCLH. The programme will then refocus to drive transformation in otherspecialties. This will be essential if some of the proposed contract changes are agreed for 2017/18 and 2018/19,which would change the mechanisms to charge for follow-up outpatient services.
The urgent care programme and The uclh Institute have supported delivery of the revised model in ‘majors’.The programme is working with clinical teams across the divisions to complete the upcoming national 7 DayCare audit. The programme plan will be impacted by the recent CQC findings.
The original £2.7m savings forecast has been reduced to £2.3m. This is due to Elective and Theatres savingsof £387k being under review pending the presentation of the revised scope.
All other programmes are forecasting financial performance to be recovered.
Executive Board ReportAppendix B

Highlights
Admin and Patient Access Shortlisting is complete for the Clinical Outcomes letter procurement; affecting 150 admin staff and 2,500 clinicians. Demonstrations from the three bidders took place on 5 September. This procurement will reduce costs and address key quality risks by shortening letter turnaround times, which is a key priority for patients and commissioners. New appointment letters were rolled out earlier this year. The first full activity analysis of the admin workforce has been completed and compares resource usage across divisions. It shows 850 WTE staff in scope. The next step is to develop a new operating model for the admin service and discussions with staff side are taking place on a monthly basis. 100 ‘Admin change leaders’ have been enlisted to support a wide range of change. We have piloted telephone reminders using predictive analysis to focus on patients most likely to not attend appointments. After 5,000 calls at the end of June, it has shown to be cost effective and efforts are now focused on scaling up. This has been slower than anticipated resulting in a slower achievement of run rate benefits, but financial recovery is forecast for 16/17.
Diagnostics The pathology e-requesting (order comms) project is progressing well with significant work completed in designing and testing the system. The aim is to pilot the system on two wards in October ahead of rollout across UCLH. There is some risk to the delivery of financial benefits due to the delay in implementation but the team are aiming to mitigate this through targeted work with divisions on CIP plans ahead of rollout. The Imaging Productivity Study and report have been completed and the team are now progressing with implementing the recommendations to deliver an increase in MR and CT productivity. Key actions include: University College Hospital Improvement Week from 5 to 11 September to test a number of recommendations; DNA action through rolling out text messages to all patients and phone calls to high risk patients; redesign of QS referral and booking process to support MR recovery; a review of the booking schedules to minimise wasted slots; and development of regular metrics to track productivity. The Imaging Data Rationalisation project is progressing well and has agreed a clear plan with stakeholders to provide consistent operational and performance data and metrics across all sites and modalities, and reduce the number of different reports from around 40 down to approximately eight.

Exemplar ward
Our pre-12 discharge CQUIN target has been met for quarter one.
Rolling roster go-live for the first three wards is scheduled for 5 September.
Exemplar Ward Accreditation is on track to meet schedule for 2016/17.
Programmes of Care Programmes of Care is currently working on three core areas of delivery:
Delivering improvements within paediatric diabetes and maternity - these two large services already have year-of-care/pathway tariffs which mean financial benefits from programmes of care can be realised this year: these are not yet fully quantified, leading to the amber rating. Achievements include launch of Skype clinics, reduction in maternity scanning and streamlining of complex maternity pathways.
Re-designing the pathways for Epilepsy, Parkinson's disease and Headache in partnership with Camden, Islington, Barnet CCGs and Royal Free London NHS FT. Positive feedback received from Camden CCG.
Progressing work to enable the successful delivery of 2 CQUINs which are worth ~£750k in 2016/17: (a) Telemedicine and (b) Patient Activation Measurement (PAM) which is a measure of how involved patients are in managing their own condition. Deliverables for Q1 and Q2 payments are on track.
Coordination Centre
The team carried out site visits to New Cross hospital, Wolverhampton and Aarhus, Denmark from July-Aug to review bidder systems in situ.
The preferred bidder was identified at EBT on 31 Aug. Following the 10-day standstill period, the programme team will work with the preferred bidder to develop the full business case and contract from 14 September to 17 October.
Elective and Theatres The new Programme Lead started on 25 July and the programme is being re-scoped and agreed with key stakeholders. The new plan of work will be finalised by the end of September. The programme currently has just one workstream operational; the development of an e-form for pre-assessment and is on schedule. Due to the re-scoping taking place, the financial benefits have been reduced from £387k to £0 and a new work plan and analysis of financial benefits are being worked up for 2017/18 delivery.
Urgent Care
The revised ‘majors’ model is now in operation and initial analysis show promising signs of positive impact on patient flow. A significant amount of programme resource will focus on working with divisions to deliver the upcoming 7 Day Care audit in September. The Emergency Care Pathway Improvement Plan has also been reviewed. Initial meetings have been held to agree a way forward for scoping Transfers of Care and 48 Hour pathway streams. Programme scope will need to consider the recent CQC findings.

The uclh Institute Good progress made on improvement capability building and a range of educational programmes have been launched. A learning package has been created for Exemplar Ward. The uclh Institute continues to support urgent care with the change of the use of the acute floor, the Diagnostics programme with improvement week, and also started work to support the Elective Care programme. A series of three tailored learning events have been designed to support the 100 plus APA change leaders to deliver the programme; (1) Leadership, (2) Being a Catalyst for Change, and (3) Train the Trainer.
Demand and capacity
Has been reviewed on-the-day bed demand for the Tower and this is being compared with the level of cancelled operations and A&E performance.
Data is being collected on potential discharges, which will allow for an assessment of how reliable these figures are.
The re-modelling of Queen Square MRI and endoscopy has been completed for the Diagnostics programme. CT and Ultrasound for University College Hospital are on track to be completed by 2 September.
An accelerated 2-year planning timetable has been announced by NHSI and this will need to be accommodated.
The team are working with the Corporate PMO to define clear deliverables for uclh future programmes against realistic timelines.
Organisational Development The e-network portal that allows staff who have been trained to interact with each other has been launched. User feedback is currently being collected and analysed. Mapping of interdependencies is still taking place across the uclh future portfolio.
DTP / EHRS
iCare – improving care through technology We aim to achieve this by appointing the right digital transformation partner (DTP) and successfully implement the right EHRS. The re-procurement of the contract for UCLH outsourced ICT services (digital transformation partner) is on track:
Three bidders were selected into the final competitive dialogue stage
One bidder withdrew from the process
We expect to receive the final detailed responses from the remaining bidders by early September
View of identifying preferred bidder in October
We are engaging with clinicians and other staff across six focus areas at UCLH to clarify the potential benefits and savings of implementing an EHRS; Discharge process, Emergency Department, EPMA, Pharmacy, Theatres, Trust-wide scheduling. The intention is to formally identify and consider for approval the EHRS preferred bidder at the October Board.

As-Is plus
Single Sign On Technical design has been completed and the platform is being built. On track for delivery by end of November 16. There is a risk around scope creep with the additional costs for card readers. An exception report has been raised for review.
Pathology e-requesting Technical design and test strategy complete and the system configuration is under way. Delayed by approximately eight weeks. Go-live planned for late October 2016. There is a risk around resistance moving from paper request form to electronic version. Team will be using a communications plan, coupled with a trust-wide eLearning schedule.
eCasenotes
Procurement is under way (pursuing two procurement routes) Project plan has been re-baselined and approved to include the new procurement route. There is a risk around resistance moving from the paper casenotes to eCasenotes. Demonstrations will be set up for clinical engagement.
e-CareLogic enhancements (AMU/PDD) Release date scheduled for Sunday 4 September. Consistent Planned Discharge Date (PDD) across systems – updated in real-time between Carecast and eCareLogic. Ward handover feature for AMU – patient lists where data will be recorded in real-time, making it more accurate and up-to-date.

EPMA EPMA has rolled out to all wards in scope and a closure report will go to As-Is plus Board for review in September. BAU team hired and managing open risks

Infection Control Annual Report
2015 – 2016
Executive Board ReportAppendix C

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
2
1.0 Contents
2.0 Executive Summary
3
3.0 Summary of performance 2014-2015
4
3.1 3.2 3.3 3.4 3.5 3.6 3.7
MRSA bacteraemia Clostridium difficile Meticillin sensitive staphylococcus aureus (MSSA) bacteraemia Intravenous device related infections Hand hygiene compliance Surveillance and infection control audits Antibiotics sterwardship
4
4
5
5
6
6
7
3.8 Gram negative micro-organisms
7
3.9 Influenza
7
3.10 Norovirus 8 3.12
MRSA screening
8
4.0 Other significant issues
8
4.1 Estates and planning
8
4.2 Outbreaks and incidents 8
Appendix 1 Infection control provision and arrangements
10
Appendix 2 Summary of Trust Infection Control work plan 2016-17 Healthcare associated bacteraemia plan 2016-17
11 15
Appendix 3 Graphs and tables
16
Appendix 4 Definition of catheter associated and related blood stream infection
25

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
3
2 Executive Summary 2.1 This is the report of the Director of Infection Prevention and Control (DIPC) and summarises
the work undertaken in the organisation for the period 1 April 2015 to 31 March 2016. 2.2 There were 90 cases of Clostridium difficile in UCLH during this period against a trajectory of
97 reportable hospital-acquired; 65 cases were successfully appealed and 25 cases were classified using the Public Health England (PHE) criteria, as lapses in care which included delay in sampling and isolation. Root causes were primarily associated with appropriate antibiotic usage and recurrent C.difficile infection.
2.3 There were 2 cases of MRSA bacteraemia against a trajectory of 0.
2.4 There were 30 cases of MSSA bacteraemia during this period.
2.5 A strategy of C. difficile reduction, prevention and management was agreed and delivered by a task and finish group. This work reflected the findings from root cause analysis and learning from other organisations. This included optimising antibiotic stewardship, improving prompt isolation of cases of diarrhoea, environment cleaning, hand hygiene and rapid testing for C.difficile.
2.6 The mean hand hygiene compliance score was 94.3% and overall reporting compliance of
areas was 80.1%. By March 2016 the new Infection Control Continuous Quality Improvement (ICCQI) Reporting Tool was in use by 82.6% of reporting auditing sites
2.7 The surveillance of surgical site infection (SSI) continued. There were no significant changes
in infection rates between 2014 and 2015; caesarean sections consistently have had lower infection rates than observed nationally (1.26% vs. 3.58%). In Spinal and colorectal surgery the rates of SSI prompted investigation, visits to operating theatres, teaching and improvements where possible. In orthopaedic surgery the numbers of infections were low but minor changes had a disproportionate effect on the reported rates. Each infection is now checked with the consultant responsible.
2.8 Mitigation and enhanced monitoring continued to control pseudomonas in tap water in high risk areas.
2.9 A brief summary of the progress made on the 2015 -16 annual plan is included in this report.
The plan of work to be undertaken in 2016-17 is included in Appendix 2.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
4
3.0 Summary of Infection Prevention and Control performance 2015-16
3.1.0 MRSA bacteraemia
3.1.1 There was a further year on year reduction in the number of MRSA bacteraemia cases. (Graph 1 Appendix 3). There were 2 cases of MRSA bacteraemia against a national trajectory of 0.
3.1.2 In the first case the root cause was associated with care and documentation of a long term IV line and the prescribing of appropriate antimicrobials. In the second case it was not possible to identify a root cause.
3.1.3 Education, training and support was provided to improve practice in IV line insertion and management, obtaining blood cultures.
3.2.0 Clostridium difficile (C.difficile)
3.2.1 UCLH reported 90 hospital-attributed cases in this period (Graph 2a of Appendix 3). The ribotype strains identified were diverse reflecting the distribution and carriage in the community (Graph 2b, Appendix 3).
3.2.2 UCLH continues to test more cases than most other trusts for C.difficile infection. The rationale is that early detection and treatment improves patient outcomes. However this increases ascertainment. In addition cases are predominantly identified in patients with haematological or oncological conditions requiring chemotherapy where early treatment is particularly beneficial.
3.2.3 65 of the 90 hospital acquired C. difficile toxin positive cases were successfully appealed with the clinical commissioning group (CCG). The successful appeals were predominantly related to patients who required antibiotics which were prescribed and delivered in accordance with the UCLH policy which reflects best practice. 25 cases were classified as ‘lapses in care’. This included isolation in a single room delayed beyond two hours, poor completion of stool chart and stool sampling delay.
3.2.4 The root cause of most of the cases was associated with appropriate antibiotics in patients with infections which are not preventable and life threatening if not treated with antibiotics. As in previous years, many of these patients were immuno-suppressed. Reviews indicated that antibiotic prescribing was appropriate and in line with microbiological and clinical advice.
3.2.5 Laxative usage was appropriate in the cases reviewed and often related to constipation related to treatment such as pain control. A high percentage of cases had an underlying bowel disease such as Crohns disease or previous colectomy and it was sometimes difficult to determine when they had a change in bowel pattern. Steroid treatment has also been a contributory factor in many of the cases identified. Approximately 10% of the cases reported had recurrent C.difficile infections and 17% had had C. difficile antigen detected previously.
3.2.6 The main learning points from the review of these cases for 2015-6 were associated with recognizing diarrhea as soon as possible, obtaining specimens early and disseminating learning from the RCA process. A C. difficile task and finish group facilitated the C.difficile reduction plan based on the key learning from RCA results.
3.2.7 During this period UCLH undertook work to identify microorganisms in the environment
particularly associated with efficacy of cleaning. In addition an evaluation of UV environmental decontamination systems was undertaken by the Environmental Laboratory. Results from this work suggested that UV decontamination (following cleaning) could be utilised instead of HPV in some instances. This could lead to efficiencies in bed utilisation. UV environmental decontamination will be introduced in 2016-2017.
3.2.8 Deep cleaning of the patient environment across the Trust was undertaken.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
5
3.3.0 Meticillin sensitive staphylococcus aureus (MSSA) bacteraemia
3.3.1 Graph 3 (Appendix 3) illustrates the trend at UCLH from April 2006:
3.3.2 There were 30 cases of hospital acquired MSSA bacteraemia in 2015-16. There is no national target but an internal ambition of <27 cases was not achieved. The root cause of these cases are summarised in Table A below, some cases had more than one root cause.
Table A - RCA of MSSA cases
Inadequate on-going care of IV lines 6
IV line with no lapses in care identified 8
Contaminated blood sample 4
Surgical Wound Infection 3
Chronic wound Infection 3
Aspiration Pneumonia or chest infection 2
Unknown 1
Patient admitted with a bacteraemia 1
Other 6
3.3.3 The care of IV devices remains an important issue. However there has been an increase in
the number of cases with no lapse in care since the launch of the invasive device tool which aimed to standardise documentation and care.
3.3.4 Contaminated blood culture samples indicate incorrect technique in sampling and documentation of sampling still requires improvement. A blood culture pack has been introduced which prompts good practice in sampling and documentation.
3.4.0 Intravenous device related infections
3.4.1 Vascular access devices (VADs) are widely used across the Trust for the administration of medication, physiological monitoring and carrying out blood processing. VADs can be short term peripheral IV Cannulas which last a few days, to long term tunnelled devices that can last years. In recent years more medium term VADs (midlines) and long term VADs (PICCs and Hickman lines) have been inserted at UCLH. Most wards have direct contact with patients with medium and long term devices.
3.4.2 The VAD care of central venous and Midlines was audited to determine the rate of infection using international definitions and compliance with standards and an evidence based care bundle.
3.4.3 From 1st October 2015 to 31st March 2016, 289 VADs were audited over 4586 line days i.e. the number of days the line was in place.
3.4.4 Nationally very few organisations currently collect this data and therefore there is no UK comparator.
3.4.5 The definitions of catheter associated blood stream infection (CA-BSI) and catheter related blood stream infection rate (CR-BSI) are complicated and are included in Appendix 4. This will be a measurement which will take place in future.
3.4.6 The results of the audit are summarised in Table B below.
Table B - VADs audit October 2015 – March 2016
Line days CA-BSI CA-BSI Rate CR-BSI CR-BSI Rate
Central VADs
2739 7 2.56 Per 1000 line days 2 0.73 Per 1000 line days
Midlines 1847 2 1.08 Per 1000 line days 2 1.08 Per 1000 line days

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
6
No 3.5.0 Hand hygiene compliance
3.5.1 Education, training and promotion work continued to promote hand hygiene compliance. The Trust achieved 94.3% hand hygiene compliance during this period (Graph 4 Appendix 3).
3.5.2 Improvements to the hand hygiene compliance system to ensure continuous improvement continued and incorporated work to remove factors which are a barrier to compliance. By March 2016 the new ICCQI reporting tool was in use by 82.6% of reporting auditing sites.
3.5.3 Hand hygiene products (soap, alcohol hand gel and hand cream) were standardised across UCLH two years ago though ensuring product dispensers are refilled continues to be a challenge.
3.5.4 Training in hand hygiene continued throughout the year and e-learning is mandatory on induction.
3.6.0 Surveillance and infection control audits
3.6.1 Surveillance of infection information is available on the UCLH staff intranet at ward, division and board level. Data are validated regularly by the Trust epidemiologist and any trends are identified to clinical areas for discussion and possible action.
3.6.2 Surveillance of surgical site infection (SSI) is undertaken in all specialities for at least 3 months every year. Post- operative patients are followed up for 30 days following surgery (1 year where an implant is involved) and we report this data to PHE on a quarterly basis. This is summarised in Table 1 Appendix 3.
3.6.3 Infection rates did not change significantly relative to the previous year (2014-15) in all followed-up categories of surgery; infection rates for caesarean sections were consistently below national average (1.26 vs 3.58%); in contrast infection rates for Spinal, colorectal, and total hip replacement were above national average.
3.6.4 Colorectal surgery was an area of concern with rate of 18% against a national rate of 10%. High ascertainment and tertiary referral work may account for some of the differences, efforts continue to identify the causes and drive improvement. Maintenance of patient core temperature before and during surgery has been a particular focus of attention..
3.6.5 Intensive work with spinal surgeons resulted in the introduction of topical suppression for Staphylococcus aureus as well as comparison between surgical techniques and skin preparation compliance. Rates have shown temporary reductions but currently show 2.5% vs national average of 1.2%.
3.6.6 In total hip replacement the rate stands at 1.7% (i.e. 5 infections) vs. national rate 0.6%. Greater scrutiny of each infection with the surgeons is now being taken. A brief period of increased rates was carefully investigated and has terminated. Each individual infection is now checked with the consultant responsible for additional information to produce a more accurate picture.
3.6.7 Visits, audits, consultant discussions and presentations have been used to raise awareness of the rates of SSI. Continuous monitoring and support action is required to ensure improvement occurs. In some areas such as orthopaedic surgery the numbers of infections are low and minor changes in numbers have a disproportionate effect on the rates reported.
3.6.8 A number of additional Trust wide audits were undertaken during this period by the surveillance and infection control team including:
Cleanliness and integrity of commodes
Cleanliness and safe management of Trusts' sluices
Prevention of SSI Audit (NICE guidelines)
Compliance with correct completion of stool charts
Compliance with isolation signage and management
UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
7
Compliance with correct completion of wound charts
Taps, Sinks, Hand Hygiene Compliance products 3.6.9 Results of these audits were fed back to staff and education and support was provided. The
new IC QI tool allows staff to include areas of low compliance in a continuous improvement cycle and therefore Trust-wide re-auditing is now not required where local actions are in place for area specific issues.
3.7.0 Antibiotic stewardship
3.7.1 The Antibiotic usage committee (AUC) met monthly and reported to the Quality and Safety Committee. Compliance data and reports are available from the AUC.
3.7.2 Quarterly audits were conducted manually Trust-wide to measure compliance with the key indicators of antimicrobial prescribing.
3.7.3 The AUC has a rolling agenda to produce, review and ratify all trust antimicrobial guidelines.
3.7.4 The antibiotic App is established and has been updated to reflect current guidelines and recent changes.
3.7.5 An e-learning package is now included on the UCLH learning portal for all doctors and pharmacists as ‘essential for role’ training.
3.7.6 A generic presentation was developed to allow Committee members to promote stewardship messages at their respective governance / audit days.
3.7.7 The lead surgeon from each of the surgical specialties that have the highest rate of non-compliance to local guidelines were invited to the Committee to discuss current problems and formulate an action plan for improvement.
3.8.0 Gram negative micro-organisms
3.8.1 In 2015-16 24 patients with carbapenemase producing organisms (mostly Klebsiella pneumoniae and Pseudomonas aeruginosa, but also other gram negatives, such as Enterobacter) were detected: 17 in UCLH inpatients, six in private patients and two from St Pancras (Graph 7d in Appendix 3). The prevalence of carbapenem resistant organisms is likely to rise alongside neighbouring trusts. At present UCLH has been successful in limiting the incidence by good infection control procedures and spread is very limited. Hence screening has been limited to reactive screening of wards when cases have been identified. Reduction in the usage of meropenem is key to overall control.
3.8.2 This includes a large number of common micro-organisms which may be responsible for Health Care Acquired Infection (HCAI). During this period a number of highly resistant gram negative micro-organisms were identified in patient samples, many of which were imported from abroad or from other health care providers. This is becoming a significant issue for the Trust. Screening for some organisms will be mandatory in future.
3.8.3 Three graphs 5, 6, 7a in Appendix 3 illustrate the incidence of gram negative bacteraemia but not the resistance patterns in trust patients. We present recent trends of Carbapenem resistance in the two most common Gram-negative causes of bacteraemia: E coli (graph 7b) and Pseudomonas species (graph 7c) to illustrate the fact that the occurrence of multiply resistant cases depends on the organism detected in blood. Although these cases are rare among UCLH inpatients, their occurrence warrant close monitoring as most are potentially fatal. As antibiotic resistance increases it will be increasingly difficult to treat these patients in future. Overall the number of these cases is significantly higher than MRSA or MSSA.
3.9.0 Influenza
3.9.1 There was a peak in influenza in the first quarter of 2016. (Appendix 3 Graph 8).
3.9.2 Staff were offered the influenza vaccine during this period. 3582 vaccines were delivered by Occupational Health and peer vaccinators. There was a 57.8% uptake in clinical staff.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT 8
3.10.0 Norovirus
3.10.1 There was a late start to the peak norovirus season again this year with significantly fewer cases for 2 years running relative to previous years (Appendix 3 Graph 9).
3.10.0 MRSA screening
3.11.1 MRSA screening of selected groups of patients continued. (Table 2 Appendix 3). In 2015-6 a review of screening for MRSA will be undertaken in response to DH guidance https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/345144/Implementation_of_modified_admission_MRSA_screening_guidance_for_NHS.pdf
3.11.2 The use of molecular screening is not cost effective for all patients requiring screening and this will be reviewed in 2015-6.
4.0 Other significant issues
4.1 Estates and Planning
4.1.1 The ICT directorate continued to support and provide advice to numerous schemes to develop or create facilities and services.
4.1.2 Collaborative work with the Estates and Facilities Division continues to improve monitoring and reporting on cleaning standards and maintenance and monitoring of the estate.
4.1.3 The monitoring and eradication of Pseudomonas in taps and showers continues. A system of regular shower head changes in high risk areas has been established and water outlet testing is in place.
4.1.4 The operational Water Management group has led on mitigation and management of this issue with support from ICT.
4.1. 5 Enhanced water testing has been undertaken on the Neonatal unit (NNU), Haematology and
Oncology areas in compliance with DoH guidelines and advice.
4.2 Outbreaks and incidents
4.2.1. Last year there were a total of 158 bed days lost due to infection exposures and one confirmed outbreak. The outbreak occurred in January 2016 involving seven confirmed cases of Influenza A on UCH ward T13N. The ward was shut for 7 days and the outbreak was contained with 79 bed days lost. There were no serious outcomes to patients.
4.2.2 The remaining bed days were lost when bays/beds across the Trust were temporarily closed to admissions and transfers due to infection control concerns such as norovirus, influenza and para-influenza. Isolation in single rooms in the Trust continues to be of particular limitation and the infection control team and clinical site managers have been closely liaising daily in order to review and prioritise isolation needs and ensure timely isolation.
4.2.3 Contact tracing was undertaken in a number of instances including cases of shingles and chicken pox. There has been a marked increase in the prevalence of measles this year with 12 cases presenting to the Trust and most required contact tracing.
4.2.4 There were a cluster of 7 patients on UCLH ward T7 who tested positive for a Carbapenem Resistant Organism (CRO). However these were not all the same strain, two were confirmed transmission and the remainder were identified following active surveillance on a care of the elderly ward. Controls were applied and patient contacts were screened in compliance with national guidance. Implementation of the DH guidelines and Safety Alert relating to CRO screening is underway.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
9
4.2.5. There were three separate incidents of pulmonary TB cases admitted to an open ward. Contact tracing of staff and patients was completed and no transmission was identified.
4.2.6 There were 9 suspected cases of MERS admitted to the Emergency department of which 5 were admitted to hospital. All cases received negative results. The MERS decision algorithm was followed. There has been additional personal protective equipment (PPE) training.
Annette Jeanes Director of Infection Prevention and Control

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT 10
Appendix 1Infection Control Provision and Arrangements . 1.0 The Infection Control department provides an infection control service for the University
College London Hospitals NHS Foundation Trust (UCLH). A service is also provided for Harley Street @ UCH.
2.0 The Trust is required to meet the duties of the Hygiene Code, NHS Litigation Authority (NHSLA) and the Core standards of the Care Quality Commission. In addition there is a requirement to demonstrate compliance with NICE and best practice guidance.
3.0 The infection control service is delivered and facilitated by an infection control team which includes staff in different disciplines and boards. The team covers all sites of the Trust. The funded establishment1 is currently:
9.6 WTE infection control nurses (ICN)
1.0 WTE consultant nurse
1.0 WTE microbiologist
1.0 WTE epidemiologist
4.6 WTE surveillance staff
1.0 WTE antibiotic pharmacist
1.0 WTE Infection Control Co-ordinator
0.4 WTE decontamination advisor
4.0 Other members of the team include:
Microbiologists, virologists, Infectious diseases, environmental monitoring officers,matrons, infection control liaison practitioners, Occupational Health and sterileservices.
The neonatal and special care baby unit fund an embedded part-time infection controlnurse who is supported and supervised by the infection control team.
The UCH ITU and NHNN ITU’s fund part-time infection control link nurses who aresupported by the infection control team.
5.0 The Director of Infection Prevention and Control (DIPC) is the consultant nurse infection control. The job description of the DIPC contains both roles. In the last year this role now also includes management of the IC team and decontamination lead.
6.0 The core infection control service includes an infection control advisory service, proactive infection prevention work and education and training throughout the organisation. It also undertakes audit, policy formulation and advice, surveillance and epidemiology, outbreak and control management. A significant aspect of their work is advising on planning.
7.0 An advisory service is operated daily and out of hours. This is provided by the on-call microbiology and virology service. At week-ends there is an infection control nurse on-call from 09.00-17.00.
8.0 There is a daily meeting of microbiology, virology and infection control staff to review clinical information and service responses. The core infection control team meets weekly to formally review infection control issues and performance.
9.0 The Trust infection control committee (TICC) is chaired by the DIPC and meets bi-monthly with representatives from boards and key service areas. The minutes are available on the intranet. This committee reports to the QSC.
10.0 The ICT work closely with the CCG and PHE and other stakeholders. Examples include: C.difficile RCAs are reviewed regularly with the CCG. Post infection reviews are undertaken on all MRSA & MSSA bacteraemia and MRSA PIR are reported to PHE
1 This includes posts which are funded by other departments such as pharmacy

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
11
Appendix 2 Summary of Trust infection control work plan 2016-17
Issue / plan Key Actions and progress
1. Infection control advice is required to deliver safe patient care and to prevent transmission of infection or outbreaks
Delivery of infection control advisory service An infection control nurse delivers a reactive service
Monday to Friday 9-5 and an on-call service 9-5 on weekends and bank holidays.
Microbiologists and virologists provide 24 hour cover for infection control.
All significant incidents and outbreaks are reported at the weekly infection control team meeting, the Q&S meeting and TICC quarterly. In addition reports are sent to commissioners and Public Health England as required.
AAR and RCA are performed, reported and shared to identify and share lessons learnt
These are summarised in the monthly Q&S report.
2 Reduce C difficile HCAI infection in compliance with national targets and quality improvement
(See C.difficile reduction plan for full details )
Key areas of work:
Reduce delays in isolation
Reduce delays in rapid stool sampling and testing in the presence of diarrhoea
Improved documentation of stools using the Bristol stool chart
Maintain high standards of cleaning of the environment and equipment.
Achieve and maintain improvements in Antibiotic stewardship
Optimal use of personal protective equipment (PPE) and hand-washing.
Review and improve Root cause analysis (RCA) process and shared learning
Appropriate and timely treatment and support of patients with CDT and antigen positive CD.
Communication campaign
3 Improve antibiotic management and prescribing practice and achieve DH targets
The trust Antibiotic usage committee (AUC) leads this and produces an annual report
Compliance with the trust antibiotic prescribing and management guidelines is reported quarterly to TICC and Q&S and reported on score cards.
Areas for improvement include IV- oral switch, stop dates, surgical prophylaxis
See AUC annual report for plan
4 Optimal insertion and management of invasive devices
(See bacteraemia reduction plan)
5 Improve governance and accountability of infection prevention and control
1. The Trust board are responsible for minimising and controlling HCAI as part of the overall risk management strategy, reflecting the expectations of the Health and Social care Act (2008)
2. Significant HCAI including MRSA bacteraemia and C.difficile are investigated and reported. Learning is shared across the organisation.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
12
3. A Medical Director acts as the trust board lead for infection prevention and control. The DIPC is directly accountable to the CEO.
4. Evidence of changes made to practices are reported by boards and divisions including audits which will reported to area, Board Q&S and TICC
5. The Antibiotic usage committee act to improve prescribing compliance with the support of Boards and clinicians and audits will be reported to Q&S.
6. Estates, facilities and planning, work with the IC team and contribute to the IC strategy and this is reflected in structures and processes across the organisation
7. Trust Infection Control committee continues to meet bi-monthly
6 Provision of infection control policies and guidance
1. Infection prevention and control department review and update policies, guidelines and information in line with relevant current information.
2. Policies, guidelines and other relevant information are available on the UCLH intranet on the Infection control page.
3. Additional guidance is available by phone from the infection control department and via the on-call service.
4. Each clinical area has a nominated ICN and an IC link person to cascade information and provide guidance.
7 Information for patients and staff will be provided
The infection control team continue to design and produce the format for infection prevention and control information for patients with clinicians.
8 Audit of service delivered, practice, compliance with policies, guidance and outcomes of care
In addition to surgical site surveillance, audits are undertaken on key infection control issues and reported back to clinicians and managers.
This process will continue and reflect new guidance and risks. Area specific audits are included in the continuous quality improvement tool which is monitored monthly.
9 Improve efficiency and quality of the service provided by the IC team
Maintain and improve the established link nurse system and on-going education and training of all staff including cleaners, engineers, volunteers , IT and non-clinical staff.
10. Isolation improvements Limited capacity and a measure of ‘time to isolation’ based on the national target of within 2 hours of request continue as challenges.
Isolation practice and capacity will continue to be monitored, intermittently audited and reported.
The use of the isolation prioritisation tool will be reviewed and improved.
The trust is building and planning additional isolation facilities.
11. HCAI surveillance Surveillance and reporting of infections is established
Work will continue to automate collection and upload data; simplify data and make it more accessible and useful; provide timely reports to clinicians and other key stakeholders.
Work to improve intravenous invasive device surveillance will commence this year for central lines, mid and long lines
The Trust will participate in the national HCAI point

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
13
prevalence survey in October 2016.
Reports continue to be produced for Q&S and quarterly for the TICC. This is accompanied by relevant statistical and epidemiological information.
12 Reduction of surgical site and wound infection
Surgical wound infection surveillance is established. Work to improve surgical wound management continues to focus on areas with rates above national reported rates of SSI.
13 MRSA screening of selected high risk patients
Screening will continue to be delivered to reduce the risk of infection. In addition this year culture based screening in non-urgent cases will be introduced and the requirement for screening in low risk areas will be reviewed.
14 Identify, prevent and control CRO
National guidance will be reviewed and applied
This will include discussion with Commissioners and clinicians to identify key areas of work within UCLH and in conjunction with primary care.
A plan will be developed to identify, prevent and control CRO
14 Optimal Hand hygiene and Infection Control compliance
Auditing and reporting is already established and will continue.
The IC quality improvement tool has been developed and will be further established. In addition it will be updated in line with guidance, practice and evidence.
An e-learning module is mandatory for clinical new starters.
15 Compliance with national decontamination guidance across the Trust
Work continues to ensure compliance with recommended practice.
A program of review of local decontamination practice will continue.
The ICT will work with procurement to ensure any items purchased meet decontamination requirements
16 Prevention of sharps injuries. In compliance with national and EC guidance which increases the requirement to prevent needle stick and other sharps injuries.
The established system for reporting and managing NSI and splash injuries will continue.
The Trust has already introduced a range of safer devices and this will continue.
17 Provision of expert Infection control advice on planning, building, renovations and other developments
Infection control will continue to provide advice and support.
Standardisation of furniture, fittings and equipment will be supported.
18 Facilitate and support the optimal cleaning of the environment and equipment
HPV decontamination is established.
UV decontamination will be introduced
Work to improve education and support of cleaning and maintenance staff in infection control will be undertaken.
Monitoring of cleaning will include ATP and further work to improve standards achieved will be undertaken in conjunction with E&P and HMU.
Annual deep cleaning will continue

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
14
19. Facilitate and support the delivery of environmental controls including water and ventilation
Effective monitoring and controls will continue to be supported
The Water Hygiene group is established.
20. Provision of education and training in infection prevention and control
Continue to provide e-learning at induction and at updates.
The link person system will continue
Study days and ad hoc lectures will continue.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
15
Healthcare associated bacteraemia reduction plan 2016-17 Project Detailed
Actions Success measures Progress
1. Provision of optimal insertion and management of intravenous devices
IV line insertion training will be delivered
including all new medical recruits and other relevant staff IV nurse in post and
undertaking work as planned
IV training for FY1 and FY2 medical recruits delivered august 2015 and planned for August 2016.
Blood culture sampling training will be
delivered including all new medical recruits and other relevant staff
An IV study day for clinical staff will be provided in 2016.
Delivery and evaluation Study day for 2016 planned.
Evaluate the potential benefits of passive disinfection of needle free devices (name of product omitted intentionally)
Report and business case
Visit by a global subject matter expert has presented to UCLH key staff.
All IV related MRSA bacteraemia and where possible other significant bacteraemia will be followed up by the IV nurse and lessons learnt disseminated
Reduction in Trust wide bacteraemia
All MRSA and MSSA bacteraemia are currently followed up with a RCA/PIR. Report and learning routinely produced and shared Trust-wide.
Acutely ill patients requiring medium/long term IV lines to be considered for OPAT or UCLH at home
Increase in appropriate referrals to OPAT and UCLH at Home
Infection control IV team supporting the outpatient services. OPAT team inserting medium term lines.
Policies and guidelines revised and adapted
Updated policies based on current robust evidence
Policies updated and work now underway to standardise local policies to share best practice.
2. Auditing and monitoring of IV line insertion and subsequent care
IV team to undertake an on-going audit of long term IV devices on inpatients for medical, surgical and neuroscience areas.
Continue current audit and extend to Haematology, and oncology areas.
Audit in progress.
Participate in the PHE surveillance of blood stream infections in patients attending ICUs.
Report data to PHE on ICU bacteraemia cases and related CCA-BSI and CR-BSI
Pilot carried out on T3 and NNU.
3. Governance and accountability
Significant HCAI including MRSA bacteraemia will be reviewed via an RCA or PIR process and reported. Action plans reported and monitored at boards
Reports in minutes of divisional and board meetings
DH PIR and RCA reported to the divisions, boards and executive. Lessons learnt shared across the Trust.
Acton plans delivered and learning shared

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
16
4. Rationalisation and standardisation of products of IV related products and blood culture sets.
Review and standardisation of safety engineered peripheral cannula across the Trust
Standardised safe products in use
Introduction of (name of product omitted intentionally) cannula for the ward areas, (name of product omitted intentionally) for paediatrics and NNU, VPS in use in all other areas.
Standardisation of needle free devices Standardisation
In progress, trials currently underway and procurement are reviewing value for money.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT 17
Appendix 3
Graph 1 MRSA bacteraemia cases. HA = hospital-acquired (detected 2+ days after admission), CA = community-acquired (detected within 2 days of admission). T15 are private inpatients.
Graph 2a: Clostridium difficile cases; HA = hospital-acquired (detected 3+ days after admission, includes lapses in care, successful appeals and pending appeals), CA = community-acquired (detected within 3 days of admission), T15 as in Graph1; NREP = not reportable (because the illness was attributable to factors other than C difficile [HPA/PHE guidelines]). The HA incidence (black line with triangular markers) reflects the subset of HA cases relevant to the ambition – the increase at the end of the year is a reflection of the changes in appeal methodology enforced by the CCG in February 2015.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
18
Graph 2b: Distribution of C diff ribotypes, cases detected in 2015-16; HA = hospital-acquired (detected 3+ days after admission, includes lapses in care, successful appeals and pending appeals), CA = community-acquired (detected within 3 days of admission), COMM = detected in the community (GP, outpatients etc).

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
19
Graph 3: MSSA bacteraemia cases; HA = hospital-acquired (detected 2+ days after admission); CA = community-acquired (detected within 2 days of admission); T15 is a private patient’s ward.
Graph 4: Hand Hygiene compliance

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
20
Graph 5 Pseudomonas aeruginosa bacteraemias; HA = hospital-acquired (detected 2+ days after admission); CA = community-acquired (detected within 2 days of admission); T15 is a private patient’s ward.
Graph 6 E coli bacteraemia; HA = hospital-acquired (detected 2+ days after admission); CA = community-acquired (detected within 2 days of admission); T15 is a private patient’s ward.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
21
Graph 7a Other gram negative bacteraemia (hospital-acquired only, i.e. detected 2+ days after admission).
Graph 7b Percent Carbapenem resistance in E coli bacteraemias (all inpatients regardless of when detected, i.e. hospital- and community-acquired cases).

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
22
Graph 7c Percent Carbapenem resistance in Pseudomonas species bacteraemias (all inpatients regardless of when detected, i.e. hospital- and community-acquired cases).
Graph 7d Number of patients colonized/infected with carbapenemase-producing organisms

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
23
Graph 8 Influenza cases. HA = hospital-acquired (detected 2+ days after admission); CA = community-acquired (detected within 2 days of admission); T15 is a private patient’s ward.
Graph 9: Norovirus cases. HA = hospital-acquired (detected 5+ days after admission); CA = community-acquired (detected within 5 days of admission); T15 is a private patient’s ward.

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
24
Table 1 Surgical operations carried out at UCLH during 2015; N f-up = number followed up by the SSISS team; N Inf = number of infections detected in hospital among followed-up surgeries (HPA/PHE definitions);
Category of surgery
Number of operations
N f-up (%)
N Inf. (%)
National %‡
Caesarean section Cranial Knee replacement Large bowel Limb amputation Repair of neck of femur Small bowel Spinal Total hip replacement Thoracic surgery Urology
2063 1044 261 241 19 92
207 814 372 505 6372
872 (42) 613 (59) 74 (28) 224 (93) 9 (47) 27 (29) 186 (90) 612 (75) 154 (41) 157 (31) 294 (4.6)
11 (1.26) 9 (1.47) 0 (0.00) 41 (18.3) 1 (11.1) 1 (3.70) 17 (9.14) 18 (2.94) 3 (1.95) 5 (3.18) 8 (2.82)
3.58 (*) 1.36 0.29
7.08 (*) 3.19
- 4.21 (*) 1.14 (*) 0.59 (*)
- -
‡Comparisons with national rates use the subset of data collected nationally between April 2010 to October 2015 where that exclude patient-reported infections (PHE guideline); and there is no attempt to control for case-mix in this comparison. (*) = statistically significant difference (Chi-square test for proportions – highlighted only where the UCLH sample size is greater than 10 operations).
Table 2: MRSA screens at UCLH 2015-16.
Month Year N screenable N screened % screened MRSA positive (%)
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2015 2015 2015 2015 2015 2015 2015 2015 2015 2016 2016 2016
5507 5131 5577 5730 4992 6306 6299 6249 5778 4998 6567
Pending
3650 3501 3717 3696 3348 4006 3943 3889 3329 3077 3916
Pending
66.3 68.2 66.6 64.5 67.1 63.5 62.6 62.2 57.6 61.6 59.6
Pending
49 (1.3) 32 (0.9) 29 (0.8) 41 (1.1) 38 (1.1) 29 (0.7) 27 (0.7) 33 (0.8) 22 (0.7) 26 (0.8) 35 (0.9)
Pending (-)

UCLH NHS FOUNDATION TRUST INFECTION CONTROL ANNUAL REPORT
25
Appendix 4


F
Agenda Item 9
Performance Report


Report to Board of Directors
Current issues Action Month first raised
A&E (Page 8) Emergency department performance worsened from 91.8% in June to 89.7% in July. The department continues to be impacted by high demand with higher numbers of ambulance conveyance than expected. Higher acuity on wards is resulting in bed blockages and worsening specialty response times.
Changes to the acute assessment / acute care model have been implemented, following a series of rapid improvement events with staff. This change retains the acute assessment model whilst opening the floor to bring the care to the patient. It is expected to improve efficiency of patient flow though this area, including ambulance handover times, which we will be closely monitoring through a number of key matrices during this pilot period.
The implementation of a system for GP redirection has been delayed; delivery is now provisionally scheduled for September. Meetings are ongoing with CCG and local GPs the design a service model.
August 2015
Diagnostic waits
(Page 9)
Diagnostic waits continue to be challenged and we did not hit our July STF trajectory which was 98.3%. Endoscopy did achieve the standard, in line with their plan. This is the first time that the service have achieved in over three years.
In Queen Square MRI, we have an underlying demand and capacity gap which is driving the ongoing under-performance. We have now completed the consultant review of the additional cohort of patients that were not on the waiting list; this means that an additional 136 MRI long waiters will be added to the position for next month. The division have secured an additional 910 scans per month via three different outsourcing contracts. Some of this capacity is already in place now; all of it will be live in September. Based on this, we are forecasting compliance for November.
We have also reported non-compliance within non-obstetric ultrasound. This is due to two vacancies within the sonographer team. The division expect this to worsen for the August reported position. They are using increased outsourcing and internal ad-hoc lists to recover performance.Overall as a trust we are predicting compliance against the six week standard by November.
December 2014
Cancer waits
(Page 8)
The two week wait in breast continues to be worse than standard, although this is improving through use of the outsourcing contract. We are also progressing radiologist recruitment to provide additional resilience to the team. We should reach a sustainable, compliant position in September.
Currently we are not meeting our 62 Day STF trajectory for July for both internal and external pathways. Late referrals remain an issue. We have received trajectories from our main referring trusts showing the expected rate on late referrals. Unfortunately, based on these we cannot achieve the standard in October as planned. We are working with trusts to shorten pathways and have escalated this to the trusts' CCGs. We have improved our internal performance in July, although we are not yet compliant, despite planning to achieve this from June. We are still seeing breaches in head and neck (four) and urology (three). In all cases the breaches are predominately caused by pathway complexity or patient choice issues, review of the RCAs does show some capacity and administrative issues that we need to address.
31 Day performance has worsened in month. This is driven by urology, who are reported 15 breaches, and head and neck who are reporting six breaches.
July 2013

eVTE Risk Assessments completed (Page 10)
We were better than threshold for patients being risk assessed for VTE in July. Medicine board did not achieve target, emergency services were at 91.6%. Queen Square have agreed cohorting for regular day attenders on RBNQ which is now in place. They are compliant for the month of July. They are also compliant for April, May, and June after a refresh of their data with the new cohorting.
September 2014
Complaints responded to within target time (Page 13)
We were worse than threshold for complaints response times in July. Both medicine, and surgery and cancer boards responded to 100% of complaints within the target time. Queen Square had four complaints responded to after target time in neurosurgery due to delays in contacting the patient and waiting for medical records. Neurology had one complainant who they were unable to contact and specialist services had one complaint assigned to them at short notice. EDH had five complaints of which two were not compliant. One was due to a delay in the notes being available and the other due to the patient needing a consultation prior to responding to the complaint. Women’s health are reviewing all complaints weekly to ensure they are investigated within 25 days and established clear DM/DCD escalation routes. For July there was one very complex complaint in maternity.
February 2015

July 2016
Month 4 - July
Board of Directors Performance Report
Month 4 - July

1. Executive summaries
2. Finance 3. Delivery of CIP
4. Access
5. Patient Safety and Quality metrics
6. Workforce
7. Externally Reported Frameworks
Page Con
Board of Directors Performance ReportContents
Month 4 - July

Board of Directors Performance Report
LY to date LY to date
Tru
st
actu
al
Tru
st
thre
sh
old
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Tru
st
actu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
20
15
/16
Tru
st
actu
al
Tru
st
thre
sh
old
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Tru
st
actu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
20
15
/16
% Elective variance 0.2% 0.0% 50.5% 0.4% -8.2% -2.2% 64.4% 4.6% -11.5% Number of MRSA bacteraemias 0 0 0 0 0 0 0 0 0 2
% Daycase variance 2.7% 0.0% -7.5% 4.0% -9.5% -3.7% 2.5% -1.7% -8.0%
Number of clostridium difficile cases
reported (excluding successful
appeals)
7 8 0 6 1 21 6 10 5 29
% Non-elective variance 3.7% 0.0% 21.5% 2.5% 6.0% 6.9% 16.0% 0.2% 1.9%
Outpatient variance 2.4% -7.3% -2.6% -7.1% -0.7% 2.1% 1.8% -2.6%
All pressure ulcers acquired at UCLH 8 4 3 4 1 11 5 5 2 21
Inpatient falls with serious harm 1 0 0 1 0 2 1 1 0 1
Trust theatre utilisation 71.8% 85.0% 34.3% 74.3% 70.3% 72.1% 34.3% 73.1% 71.7% 71.6% % eVTE risk assessments completed 96.1% 95.0% 92.9% 97.1% 96.5% 96.2% 92.8% 97.3% 96.5% 96.0%
Tower Bed occupancyComplaints responded to within target
time79.7% 85.0% 100.0% 100.0% 60.0% 77.4% 81.0% 94.0% 66.7% 79.9%
Length of stay - elective 2.8 0.6 3.7 2.5 Friends & Family Test (IP survey) 94.3% 96.0% 93.7% 95.7% 93.1% 96.1% 96.5% 96.2% 95.5% 96.8%
Length of stay - non elective 4.8 5.3 7.7 3.4
% mandated training compliance 93.0% 95.0% 93.2% 93.6% 92.2%
% incomplete pathways < 18 weeks 93.2% 92.0% 98.1% 93.8% 92.1% 93.9% 98.3% 94.1% 93.0% 94.6% Appraisal rate 67.7% 95.0% 66.1% 66.3% 74.3%
% Diagnostic waiting list within 6 weeks 96.3% 99.0% 100.0% 98.5% 91.7% 95.0% 99.8% 94.4% 93.1% 97.6% Vacancy rate 8.8% 10.7% 3.7% 12.5% 8.3% 11.7%
Patients waiting longer than 52 weeks 0 0 0 0 0 0 0 0 0 1 Staff turnover rate 13.2% 13.9% 14.5% 10.7% 14.1%
A&E attendances within 4 hours 89.7% 95.0% 89.7% 89.4% 89.4% 97.7%% temporary staffing filled via
Bank90.4% 90.8% 87.4% 90.9% 92.5%
Cancer 62 day GP referral to treatment 67.7% 85.0% 100.0% 60.5% 75.0% 65.6% 88.9% 62.1% 69.0% 82.5%
Cancer 31 day subsequent surgery
treatment87.5% 94.0% 84.6% 90.9% 93.5% 100.0% 86.5% 98.6% 86.8%
Cancer 14 day referral to appointment 86.7% 93.0% 90.4% 89.6% 77.3% 86.0% 90.4% 90.2% 71.2% 92.4%April May June July Aug Sept Oct Nov Dec Jan Feb Mar
ED Trajectory 88.0% 90.9% 92.8% 95.0% 95.0% 95.0% 95.0% 92.9% 93.8% 95.0% 95.0% 95.0%
Tru
st
YT
D ED Actual87.8% 88.1% 91.8% 89.7%
Overall financial rating 2
Operational Performance (Debt Service
Cover) 1 Diagnostics trajectory96.0% 97.0% 97.7% 98.3% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0% 99.0%
Cash and Balance Sheet Performance
(Liquidity) 4Diagnostics actual
94.4% 95.4% 93.7% 96.3%Income and expenditure plan and CIP
delivery
Cancer 62 day trajectory 66.7% 73.7% 76.7% 80.3% 82.0% 82.0% 85.5% 85.5% 85.5% 85.7% 85.0% 85.7%
Cancer 62 day actual 70.9% 64.8% 58.7% 67.7%
RTT trajectory 93.3% 93.3% 93.3% 93.3% 93.3% 93.0% 92.8% 92.6% 92.4% 92.1% 92.1% 92.1%
RTT actual 94.5% 93.9% 93.8% 93.2%
Page 1
Month 4 - July
1.2 Executive summary: board performance
This month Year to date
Quality and
safety
Pages 12 - 15
Cancer waits
Page 10
Infection
Page 11Activity page
4
This month Year to date
Finance
Page 2Sustainability
and
transformation
fund
trajectories
Workforce
Pages 16 - 18
Efficiency
and
productivity
Page 7 - 8
ED, RTT, and
diagnostic
waits, access
page 8-9

Page 2
2. Financial Performance2.1 Financial Performance Summary
Month 4 - July
Area of review Key Highlights
NHS Improvement YTD
Financial Sustainability
Risk Rating (FSRR)
Month 4
actual
Month 4
plan
Month 3
actual
HEADLINE
FINANCIAL
PERFORMANCE
(Overall Rating)
The M4 I&E position before donation adjustments is £1.5m (rounded) ahead of plan (-£5.2m actual vs. -£6.8m plan) (YTD
overall rating = 2).
NHS clinical income is £4.3m ahead of the M4 YTD plan – (a) income from patient activity is £0.2m behind plan (+£0.2m in-
month) , (b) drugs, devices & pass-through income is £4.5m ahead of plan (+£1.5m in-month).
At M4 there has been no release from the Trust’s £10m Board contingency (YTD budget is £3.3m).
2 2 2
1a. Operational
Performance
(Capital Service
Cover)
The Trust’s YTD revenue available for capital service is £0.7m behind plan (+£17.0m actual vs. +£17.7m plan).
M4 clinical board positions are:
(a) Medicine is £1.8m ahead of plan (+£0.2m in-month),
(b) Specialist Hospitals is £0.6m behind plan (-£0.3m in-month),
(c) Surgery & Cancer is £0.8m ahead of plan (-£0.6m in-month).
(d) The Corporate budgets within EBITDA (including R&D and Education) are £3.1m behind plan, whilst finance income
(interest & JV profit share) is £0.3m ahead of plan.
Revenue of £17.0m is able to cover 1.09 times the Trust’s capital service (YTD rating = 1).
1 1 1
1b.Operational
Performance (I&E
Margin)
The M4 YTD bottom-line I&E position (i.e. after donation adjustments) is a normalised deficit of £5.8m, which produces an
I&E margin of -1.8% (YTD rating = 1).
There are no exceptional items reported in the M4 position.1 1 1
1c. Operational
Performance (I&E
Margin variance
from Plan)
The M4 YTD bottom-line I&E deficit is £1.4m ahead of plan (-£5.8m actual vs. -£7.2m plan).
Charitable donations to support capital projects are £0.1m behind plan at M4.
There is a variance of +0.5% between the actual I&E margin of -1.8% & planned I&E margin of -2.3% (YTD rating = 4).4 2 4
2. Cash & Balance
Sheet
Performance
(Liquidity)
The liquidity ratio shows that working capital (cash plus debtors less creditors) is able to cover 7 days of the Trust’s
operating expenses (YTD rating = 4).
At 31st July 2016 the Trust’s cash balance was £50.9m, £11.8m lower than the planned cash position of £62.7m.
The August month-end cash balance is £68m (£3m ahead of plan).
Of the current capital programme totalling £216m, 82% (£177m) is approved & in progress.
M4 YTD capital expenditure of £18.8m is £20.3m less than plan (of £39.1m).
4 4 4

Page 3
2. Financial Performance2.2 Service lines summary
Month 4 - July

Page 4
Month 4 - July
2. Financial Performance2.3 Clinical income summary

Page 5
Month 4 - July
3. Delivery of CIP3.1 CIP update

From October we will have a trend graph showing output per £ of pay and non pay
Page 6
3. Delivery of CIP3.2 Productivity and financial improvement
Month 4 - July

3. Delivery of CIP3.3 Efficiency and productivity
Tru
st
thre
sh
old
Tru
st
actu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Trust theatre utilisation 85% 71.8% 34.3% 74.3% 70.3%
Tower elective theatre utilisation 85% 73.0% 34.3% 75.2% 69.8%
Queen Square theatre utilisation 85% 71.3% 71.3%
Westmoreland St theatre utilisation 85% 74.2% 74.2%
Cancer Centre theatre utilisation 85% 65.6% 64.0% 67.5%
RNTNE theatre utilisation 85% 70.2% 70.2%
DNA rate 8% 12.7% 15.2% 12.6% 12.0%
Average length of stay for key
specialties - Elective admissions2.9 0.2 4.3 2.2
Average length of stay for key
specialties - Non-elective admissions5.0 5.3 9.1 3.3
Page 7
This month
Month 4 - July
30%
50%
70%
90%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Percentage trust theatre utilisation - All Services
Tower elective Queen Square theatre utilisation Cancer Centre theatre utilisation
RNTNE theatre utilisation Westmoreland St theatre utilisation Target
Theatre Utilisation - Tower theatre utilisation has worsened by 0.4% to 73.0%. GI division had low utilisation driven by the colorectal subspecialty where the anaesthetic length of time for daycase procedures was a significant factor and the division are exploring solutions with theatres. Surgical specialties maintained 76% utilisation for a third consecutive month. Senior management are working closely with teams to ensure that utilisation is maximised and increasing contact with patients to reduce DNA rates. Paediatrics have improved performance by 10% through interventions around list booking and using an Health Care Assistant to bring down patients to theatre; further improvements to be made with the anaesthetic team over the next two months. Women's health utilisation worsened with breast capacity being underutilised. They continue to improve patient throughput and ensure appropriate booking to reduce early finishes.
Queen Square are updating Opera with corrected theatre time-tables which will give an accurate view of utilisation. Westmoreland Street theatre utilisation remained static, senior management is continuing to work with teams to maximise utilisation and reduce DNA rates.
The cancer centre utilisation improved from 62.4% to 65.6% in July. Paediatrics are exploring whether the interquel (twice weekly) list can move from the theatre to the procedure room.
RNTNE's theatre utilisation has worsened from 71.1% in June to 70.2% in July. The main drivers were patient cancellation due to chillers not working, late start on Wednesday, and early finishes on some lists. Options to address these are being reviewed. While there is an overall improvement in EDH's theatre utilisation of 4% over the last four weeks, opportunity has been identified to increase the number of cases on two RNTNEH-based lists where daycare bed/recovery and equipment provision and currently limiting.

4. Access4.1 Emergency flow
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
All A&E attendances within 4 hours 95% 89.7% 89.7%
UTC attendances within 4 hours 95% 95.8% 95.8%
A&E to admission conversion rate
Tower bed occupancy
Hospital at home (bed days saved) 173
Delayed Transfers of care
% discharges by noon 15.9% 18.0% 18.5% 13.3%
Page 8
This month
Month 4 - July
9500
10000
10500
11000
11500
12000
12500
13000
80%
82%
84%
86%
88%
90%
92%
94%
96%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
A&
E a
ttendances w
ithin
4 h
ours
A&E attendances
A&E Attendances A&E attendances within 4 hours Target
To be developed by end of September 16
To be developed by end of September 16
0
100
200
300
400
500
600
700
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Bre
ach
es
Breach reasons
Beds Specialty delay Diagnostic ED Delay Other Transfer
This page has been developed to give a more granular and comprehensive suite of indicators on ED and emergency flow. Some indicators are still being developed but we aim to have these available by the end of September.
Emergency department performance worsened from 91.8% in June to 89.7% in July. The department continues to be impacted by high demand with higher numbers of ambulance conveyance than expected. Higher acuity on wards is resulting in bed blockages and worsening specialty response times.
The Urgent Treatment Centre maintained compliant performance throughout the month following improvements to the pathway made in May and June.
Changes to the acute assessment / acute care model have been implemented, following a series of rapid improvement events with staff. This change retains the acute assessment model whilst opening the floor to bring the care to the patient. It is expected to improve efficiency of patient flow though this area, including ambulance handover times, which we will be closely monitoring through a number of key matrices during this pilot period.
The implementation of a system for GP redirection has been delayed; delivery is now provisionally scheduled for September. Meetings are ongoing with CCG and local GPs the design a service model.

4. Access4.2 Access Targets - Referral to treatment
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
% incomplete pathways < 18 weeks 92% 93.2% 98.1% 93.8% 92.1%
Patients waiting > 52 weeks 0 0 0 0 0
Patients waiting 40-52 weeks 50 0 13 37
% data quality issues on waiting list 5% 11.1% 17.0% 14.7% 8.7%
% Diagnostic waiting list within 6 weeks 99% 96.3% 100.0% 98.5% 91.7%
% Last Minute Cancellations to Elective
Surgery0.6% 0.6% 0.0% 0.9% 0.2%
% Cancelled Operations Readmitted Within
28 Days95% 100.0% 100.0% 100.0%
Outpatient Cancellation Rate – Hospital
(adjusted to include only postponed
appointments)
5.4% 4.7% 7.5% 4.6%
Page 9
This month
Month 4 - July
0%
2%
4%
6%
8%
10%
12%
14%
90%
91%
92%
93%
94%
95%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
% d
ata
qualit
y is
sues
% I
ncom
ple
te p
ath
ways
< 1
8 w
eeks
Referral to treatment
% incomplete pathways < 18 weeks Target % data quality issues on waiting list
86%
88%
90%
92%
94%
96%
98%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
% Diagnostic waiting list within 6 weeks
% incomplete pathways < 18weeks
Target
The trust was compliant with the RTT open pathways target in July, achieving 93.2%. There were no 52 week waiters. Performance in some divisions deteriorated, Queen Square, EDH and RNTNEH were all non-compliant at divisional level. There has been a growth in the number of patients waiting more than 18 weeks. We are developing trajectories with divisions to bring waiting lists back down to our internal planned level. Diagnostic waits continue to be challenged and we did not hit our July STF trajectory which was 98.3%. Endoscopy did achieve the standard, in line with their plan. This is the first time that the service have achieved in over three years. In Queen Square MRI, we have an underlying demand and capacity gap which is driving the ongoing under-performance. We have now completed the consultant review of the additional cohort of patients that were not on the waiting list; this means that an additional 136 MRI long waiters will be added to the position for next month. The division have secured an additional 910 scans per month via three different outsourcing contracts. Some of this capacity is already in place now, all of it will be live in September. Based on this, we are forecasting compliance for November. We have also reported non-compliance within non-obstetric ultrasound. This is due to two vacancies within the sonographer team. The division expect this to worsen for the August reported position. They are using increased outsourcing and internal ad-hoc lists to recover performance. Overall as a trust we are predicting compliance against the six week standard by November.

4. Access4.3 Access Targets – Cancer
Thre
shold
Tru
st actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Last m
onth
valid
ate
d
perf
orm
ance
Two week wait from referral to date first seen93% 86.7% 90.4% 89.6% 77.3% 88.2%
Two week wait from referral to date first seen: breast symptoms 93% 74.9% 74.9% 79.5%
31-day wait from diagnosis to first treatment 96% 87.6% 85.7% 86.6% 93.1% 96.8%
31-day wait for second or subsequent treatment: surgery94% 87.5% 84.6% 90.9% 93.5%
31-day wait for second or subsequent treatment: drug treatments98% 99.1% 99.5% 96.8% 99.6%
31-day wait for second or subsequent treatment: Radiotherapy94% 94.3% 95.6% 87.5% 98.9%
31-day wait for second or subsequent treatment: other100.0% 100.0% 83.3%
62-day wait for first treatment from urgent GP referral to treatment85% 67.7% 100.0% 60.5% 75.0% 62.6%
62-day wait for first treatment from screening service referral90% 85.7% 85.7% 100.0%
62-day wait for first treatment from urgent GP referral to treatment
Internal only82.3% 100.0% 70.0% 100.0% 74.3%
Number of 104 day waits (from GP referral) Internal29 1 26 2
Number of 104 day waits (from GP referral) External16 0 16 0
% Inter trust referrals treated within 24 days of referral
* The trust threshold is an aggregate of individual clinical board thresholds
Page 10
Month 4 - July
This month
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Cancer 62 day referral targets
Target (GP referral to treatment) Cancer 62 day referral from screening to treatment
Target (screening to treatment) Cancer 62 Day GP referral to treatment
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Cancer 2 week referral targets
Cancer GP referral to appointment Cancer 14 day wait from referral (symptomatic breast) Target
Cancer performance for July is not yet fully validated; this page presents the current position which may change before the final submission date. This report also includes June's final submitted position for completeness. The two week wait in breast continues to be worse than standard, although this is improving through use of the outsourcing contract. We are also progressing radiologist recruitment to provide additional resilience to the team. We should reach a sustainable, compliant position in September. Currently we are not meeting our 62 Day STF trajectory for July for both internal and external pathways. Late referrals remain an issue. We have received trajectories from our main referring trusts showing the expected rate on late referrals. Unfortunately, based on these we cannot achieve the standard in October as planned. We are working with trusts to shorten pathways and have escalated this to the trusts' CCGs. We have improved our internal performance in July, although we are not yet compliant, despite planning to achieve this from June. We are still seeing breaches in head and neck (four) and urology (three). In all cases the breaches are predominately caused by pathway complexity or patient choice issues, review of the RCAs does show some capacity and administrative issues that we need to address. 31 Day performance has worsened in month. This is driven by urology, who are reported 15 breaches, and head and neck who are reporting six breaches.
To be developed by end of September 16

5. Quality5.1 Infection
Tru
st
thre
sh
old
Tru
st a
ctu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Number of MRSA Bacteraemias 0 0 0 0 0
Number of clostridium difficile cases
reported (excluding successful
appeals)
16 21 6 10 5
Number of clostridium difficile cases
due to lapses in care1
Number of MSSA Bacteraemias 9 10 3 4 3
% - Infection control improvement
compliance (this month)95.0% 94.2% 97.9% 93.1%
* The trust threshold is an aggregate of individual clinical board thresholds
Page 11
YEAR TO DATE
Month 4 - July
0
1
2
3
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
MRSA bacteraemia / infections - All Services
MRSA actuals monthly MRSA threshold monthly
MRSA actuals YTD MRSA threshold YTD
0
20
40
60
80
100
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Clostridium difficile infections post 48 hrs - All Services
CDiff Actuals Monthly excl. successful appeals CDiff Threshold Monthly
CDiff Actuals YTD excl. successful appeals CDiff Threshold YTD
We have reported 29 cases of C diff as at the end of July. Eight of these have been successfully appealed and 20 cases are still under review. Our worst case position currently is nine cases against the July year to date threshold of 16.
There were no MRSA cases in July.
There were two MSSA bacteraemias for July. There was one case in GI on T09 North for a colorectal patient with a probable contamination from their IV line. Documentation of the line care was inconsistent. The ward sister and matron are working closely with the infection control team to monitor documentation and infection control measures . Queen Square had one case on the Lady Anne Allerton ward . The finding from the post infection review is that the likely root cause is the cannula; there were signs of thrombophlebitis around the cannula insertion site. There was no documented daily review from the ward.

Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
% Harm free care (National Safety
Thermometer)95.0% 95.6% 88.8% 96.4% 98.5%
% Harm free care (Hospital acquired
only)95.0% 97.5% 94.1% 97.9% 99.1%
Patients with preventable dose
omissions8.0% 5.8% 7.9% 4.3% 6.0%
% eVTE Risk Assessments completed 95.0% 96.1% 92.9% 97.1% 96.5%
The trust threshold is an aggregate of individual clinical board thresholds
Page 12
5. Quality5.2 Safety
This month
Month 4 - July
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Patients with preventable dose omissions- All Services
Preventable dose omissions Target
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
VTE risk assessment - All Services
Percentage of Completed eVTE Risk Assessments Target
We were better than the threshold of 95% for the National Safety Thermometer harm free care indicator at 95.6%. However medicine board is not achieving compliance. This was driven by the infection division where a review of the audit indicates that this is being caused by potentially missed VTE prophylaxis being given to those identified at risk. Medical leads are to review and address this. We were better than threshold for patients being risk assessed for VTE in July. Medicine board did not achieve target, emergency services were at 91.6%. Queen Square have agreed cohorting for regular day attenders on RBNQ which is now in place. They are compliant for the month of July. They are also compliant for April, May, and June after a refresh of their data with the new cohorting.

5. Quality5.3 Safety
Tru
st
thre
shold
Tru
st
actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Inpatient falls with serious harm 0 1 0 1 0
Falls per 1000 beddays 1.5 3.4 6.5 2.7 2.8
Falls with harm per 1000 bed days 1.0 2.0 1.0 0.7
% of Serious Incidents
reports submitted within (60 working
days)
94.0%
Pressure ulcers acquired 4 8 3 4 1
Grade three pressure ulcers acquired 0 0 0 0 0
Grade four pressure ulcers acquired 0 0 0 0 0
The trust threshold is an aggregate of individual clinical board thresholds
Page 13
This month
Month 4 - July
* falls with serious harm include moderate, severe, and death categories in Datix
0
1
2
3
4
5
6
0
20
40
60
80
100
120
140
160
180
200
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Patient falls per 1,000 bed days and Overall - All Services
Inpatient falls with harm Patient falls Falls per 1000 beddays
0
2
4
6
8
10
12
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Pressure Ulcers acquired at UCLH split by Grade/Category - All Services
Grade 4 Grade 3 Grade 2
There were eight grade 2 HAPU reported this month, no grade 3 or medical device related incidents reported. There was one likely deep tissue injury (DTI). The eight Grade 2’s were located across a number of wards: T10S, AMU, T10N, EGA, T14N, A&E, T10M. Areas with more than one HAPU were: T10S Orthopaedics, AMU and Oncology. Three lessons shared this month are (1) improving intra-operative pressure relieving management (2) focusing on skin status on handover and transfer and (3) 100% compliance with SSKIN assessment on admission. Of note this month is the new appointment of a third tissue viability nurse (TVN). This post holder will significantly boost the capacity of the TVN team moving into winter.
There were 86 falls with no harm reported this month. There were 27 falls with low harm this month clusters include NHNN (9), heam/onc (3), AMU/ED (3), T08 (3). There was one moderate harm fall in Haematology, where a patient suffered a head injury following an unwitnessed fall. Three key learning points shared this month (1) re-assessment of falls risk following a change in NEWS (2) timely completion of falls risk assessment on admission (3) lying and standing BP in appropriate patients. This month the falls team successfully bid for funding from the UCLH charity to pilot an innovative falls bundle of interventions across our top ten high risk wards, the impact of this substantial £80K innovation grant will be reported to the Harm Free Care and QSC committees in Q4.

5. Quality5.4 Outcomes
Tru
st
thre
sh
old
Tru
st
actu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Emergency readmissions within 30
days3.1% 3.4% 7.5% 3.3% 1.3%
Cases of moderate harm in theatres
Cases of harm from sepsis
% Complete vital signs collected 96.0% 98.7% 90.0% 100.0% 98.8%
% deteriorating patients escalated
according to protocol90.0% 98.7% 100.0% 100.0% 97.5%
Local summary hospital-level mortality
indicator (1 yr rolling data)0.50 0.44 0.66 0.43
Page 14
This month
Month 4 - July
75%
80%
85%
90%
95%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
% Complete Vital Signs collected - All Services
Percentage of Complete Vital Signs New Target
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16
Emergency readmissions within 30 days (with PbR exclusions)
Emergency readmissions within 30 days (with PbR exclusions)
We were worse than target for emergency readmissions within 30 days. Medicine were worse than threshold at 7.5% for June. Divisions are pro-actively checking the readmissions report and correcting data quality issues but genuine readmissions are still making up a large proportion of the total. Emergency services has implemented a real-time process for identification and validation of readmissions for EDU and AMU We were compliant in achieving the threshold for vital signs observations in July. Medicine were worse than threshold, this was within the infection division which relates to one of the 16 patients audited who did not have an "alert, voice, pain, unresponsive "score recorded.
To be developed by end of September 16
To be developed by end of September 16

5. Quality5.5 Patient Experience
Tru
st th
resh
old
Tru
st a
ctu
al
Me
dic
ine
Su
rge
ry &
Ca
nce
r
Sp
ecia
list
Ho
sp
ita
ls
Complaints responded to within target
time85.0% 79.7% 100.0% 100.0% 60.0%
Inpatient friends and family test 96% 94.3% 93.7% 95.7% 93.1%
A and E friends and family test 94% 94.6% 94.6%
Outpatient friends and family test 92.0% 94.9% 86.7% 92.0%
% of hospital appointments postponed by
hospital5.4% 4.7% 7.5% 4.6%
Choose and book slot issues (two
months in arrears)26.1% 21.6% 48.2% 20.9%
Patient reported being seen within 15
minutes
Page 15
This month
Month 4 - July
0
20
40
60
80
100
0%10%20%30%40%50%60%70%80%90%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Patient experience - Complaints received
Number of Patient Complaints Complaints responded to within target time Target
0%
20%
40%
60%
80%
100%
Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16
Patient Experience - FFT scores and response rate (IP & AE)
Friends & Family Test (IP survey) New FFT AE score Friends and Family - IP Response Rate FFT AE response rate %
We were worse than threshold for complaints response times in July. Both medicine , and surgery and cancer boards responded to 100% of complaints within the target time. Queen Square had four complaints responded to after target time in neurosurgery due to delays in contacting the patient and waiting for medical records. Neurology had one complainant who they were unable to contact and specialist services had one complaint assigned to them at short notice . EDH had five complaints of which two were not compliant. One was due to a delay in the notes being available and the other due to the patient needing a consultation prior to responding to the complaint. Women’s health are reviewing all complaints weekly to ensure they are investigated within 25 days and established clear DM/DCD escalation routes. For July there was one very complex complaint in maternity. The inpatient FFT score has remained stable from last month below the threshold. The response rate for July is 18.5% which is improved from last month’s 14.2%. The A&E score remains above target, with a 15.6% response rate compared to 19.3% last month. The outpatient score of 92% is based on 1650 responses, after an unusually high score of 97% last month due to a very low response rate of 261.
To be developed by end of September 16

6. Workforce6.1 Performance indicators
Tru
st
Thre
shold
Tru
st A
ctu
al
Medic
ine
Board
Surg
ery
&
Cancer
Board
Specia
list
Hospitals
Board
Corp
ora
te
Board
Staff in Post (WTE)NA 7587.7 1513.5 2373.7 3036.7 663.9
% Temporary staffing filled via Bank90.8% 90.4% 87.4% 90.9% 92.5% 89.4%
Vacancy Rate (Trust Rate)10.7% 8.8% 3.7% 12.5% 8.3% 15.1%
Voluntary Turnover Rate (12 Month
Rolling)13.9% 13.2% 14.5% 10.7% 14.1% 18.6%
Page 16
Month 4 - July
This month Staff in Post: Staff-in-post has fallen slightly between month 3 and month 4.
Temporary staffing: Fill rates have improved slightly since month 3. We have worked with our bank staff to increase the number of hours they deliver for us. Locum doctors are included in the bank category.
Vacancies: The trust vacancy rate has fallen by 2% between month 3 and month 4. Medicine Board's vacancy rate has reduced by half since last month. The work that recruitment have undertaken with critical care and emergency department has begun to have an impact.
Turnover: The trust turnover rate has remained steady between month 3 and month 4, at 13.2%.
The Trust threshold target and Trust Actual for Vacancy & Turnover excludes Corporate

6. Workforce6.2 Performance indicators
Establishment FTE*
Tru
st
thre
shold
Tru
st actu
al
Medic
ine
Surg
ery
&
Cancer
Specia
list
Hospitals
Corp
ora
te
Functions
Sickness absence rate (%) 12m
RollingN/A 3.2% 3.3% 3.1% 3.4% 2.2%
Appraisal Tier 1 & 2 95% 67.7% 66.1% 66.3% 74.3% 57.1%
% Statutory and mandatory training
compliance95% 93.0% 93.2% 93.6% 92.2% 95.8%
Average time to recruit (request pack -
start date) (weeks)14.6 13.7 14.4 14.3 12.7 9.7
Average time to recruit (request pack
received - unconditional offer) (weeks)N/A 10 9.7 10.6 9.9 7.8
Page 17
Month 4 - July
This month Sickness absence: The sickness absence rate has remained steady between month 3 and month 4.
Appraisal: This year, we have brought our mid-year targets for appraisal forward. Yet, at the end of July, appraisal completion rates were below expectation. In part, this is explained by the final write-up stage, post appraisals, being delayed in view of holidays. In month 5, we know of significant progress which the Director for Education is monitoring closely. Devoted communications shall reach any responsible manager who remains behind target.
Mandated training: Mandatory training rates have fallen slightly between month 3 and month 4 and below the target of 95% at the trust level. The Director of Education is continuing to monitor the situation and working with responsible managers and trainers to improve the performance in areas that are currently falling below the target. No appraisal is signed off as satisfactory without the member of staff being 100% compliant.
Time to recruit: Average time to recruit has slightly reduced between month 3 and month 4

6. Workforce 6.3 Nursing and Midwifery Detailed Workforce Dashboard
Page 18
Month 4 - July

Estimated riskThresholds Weighting Jul 16 Q1 Comments
32 1.0 21 14
5 cases
successfully
reviewed
92% 1.0 93.2% 94.3%See page 8 for
detail.
85% 67.7% 66.2% See page 15 for
detail.
90% 85.7% 77.8%See page 9 for
detail
94% 87.5% 93.3%See page 9 for
detail
98% 99.1% 99.8%See page 9 for
detail
94% 94.3% 98.6%See page 9 for
detail
96% 0.5 87.6% 93.4%See page 9 for
detail
93% 86.7% 86.1%See page 9 for
detail
93% 74.9% 33.0%See page 9 for
detail
95% 1.0 89.7% 89.4% See page 8 for
detail
Green Green
Page 19
31-day wait from diagnosis to first treatment (all cancers)
Two week wait from referral to date first seen: all cancers
0.5
Two week wait from referral to date first seen: symptomatic breast patients
Maximum time of 18 weeks from point of referral to treatment - incomplete pathways
Overall governance rating / Monitor risk assessment framework
Month 4 - July
7. Externally Reported Frameworks7.1 NHS Improvement Indicators – Compliance Framework
Indicators
62 day wait for first treatment from urgent GP referral
1.0
62 day wait for first treatment from consultant screening service referral
31 day wait for second or subsequent treatment: Surgery
1.031 day wait for second or subsequent treatment: anti cancer drug treatments
31 day wait for second or subsequent treatment: Radiotherapy
Incidence of Clostridium difficile year to date
A&E: Maximum waiting time of four hours from arrival to admission/ transfer/ discharge

5.3 Performance against corporate objectives
Quarterly Review
Annual objectives Measurement / target Rationale for Q1 RAG rating
Strategic objective: Provide highest quality care within our resources
1. Deliver “Sign upto Safety”campaign so that we further reduceharm to patients
Tony Mundy Reduce number of incidents per month with harm caused by unrecognised or delayed treatment of sepsis from an average of 1.6 / month.
Monitoring being developed
To work towards 95% compliance with the sepsis bundle of care
Will be based on case note audits, these are being implemented
90% patients escalated to the Patient Emergency Responseand Resuscitation Team using agreed tool
We achieved 30% by the end of Q1
96% of vital signs taken Achieved 98.1%
Reduce the number of cases of harm in operating theatres by 50% on 2015/16 Monitoring being developed
2. Maintain upperdecile SHMI results
Tony Mundy Deliver upper decile national SHMI performance each quarter UCLH placed 4th in latest SHMI, with 0.53.
3. Maintain patientexperienceratings
Flo Panel-Coates
Maintain overall scores in inpatient, outpatient and cancersurveys
National cancer patient experience survey results overall poor compared to other trusts. However, of the 14 questions asked last time we have shown improvements in all bar 1
Maintain scores on Friends and Families test Inpatient FFT scores dipped slightly in June to 94.2%which is below threshold. ED was above threshold with95.6%
4. Achieve hospitalacquired infectiontargets
Charles House
No cases of MRSA
Clostrum difficile threshold to be set in line with national target We have reported 14 cases against a trust threshold of 16.
Reduction in the number of Clostridium difficile cases attributed to lapses in healthcare on 15/16
Only 1 case has been confirmed as a lapse in care, 8 cases have been successfully appealed. 7 cases are still under review.
5. Improve bookingandcorrespondencewith patients andGPs
Gill Gaskin Increase use of electronic communication with GPs andpatients on Quarter 1 baseline
Q1 is setting baseline
Improve % of discharge summaries sent within 24 hours on quarter 1 baseline
Q1 is setting baseline
Reduction in choose and book slot issues from 15/16 Data for Q1 is not yet published
Reduction in outpatient DNA rates from 15/16 The DNA rate reduced to 11.5% in Q1, from 12% in15/16
Reduction in inpatient and outpatient cancellation rates from 15/16
The outpatient cancellation rate remained steady at 4.9%,whilst the inpatient cancellation rate was 0.5%, which is under the 0.6% threshold.
Reduction in the number of patient complaints related to pooradministration on 15/16
Monitoring being developed
Deliver co-ordination centre to agreed time-scales Business case produced by September

5.3 Performance against corporate objectives
Quarterly Review
Strategic objective: Improve patient pathways through collaboration with partners
1. Meet A&E waiting time targets
Charles House
Performance against the 4 hour wait in line with our STP trajectory
We were behind trajectory each month in the year: April was 87.8% against 88%, May was 88.1% against 90.1%and June was 91.*% against 92.8%
Increase number of patients re-directed to primary care from ED, on quarter 1 baseline.
This is planned to start from September
2. Meet 18 weekand diagnosticwaiting timestargets
Neil Griffiths Achieve Trust compliance with the national RTT waiting times standard
Q1 performance was 93.8% against 92% standard.
100% of RTT patient booked within 18 weeks Deliver specialty level compliance with RTT each month Bring down average waiting times for elective treatment
Have achieved specialty level compliance in all areas except one.
Achieve trust compliance with the diagnostic waits standard from July
This will not be achieved in July. Revised trajectory being developed. We achieved 93.7% in June against a trajectory of 97.7%.
3. Meet cancerwaiting timestargets
Geoff Bellingan
Delivery of reduced 62 day breaches in line with the Trust’s trajectory, with eventual compliance by October 2016.
In April we achieved 70.9% against a trajectory of 66.7%.In May was achieved 64.8% against a trajectory of 73.7%and in June we achieved 58.4% against a trajectory of 76.7%
Deliver compliance against the 62 day standard for thosepatients referred to us from GPs in line with agreed trajectory.
In April we achieved 80.5% against a trajectory of 76.9%.In May was achieved 76.9% against a trajectory of 77.5%and in June we achieved 74.35% against a trajectory of 85%
4. Implement thecancer vanguardproject
Geoff Bellingan
Secure full vanguard funding Received 50%, £2.4m, this was only confirmed in June
Deliver vanguard in line with project plan Late confirmation of funds has put deliverables at risk
5. Deliver phase 4,phase 5, ED andqueen squaredevelopmentmilestones
LauraChurchward
Deliver phase 4 build milestones in line with plan Time-scales have slipped but should be recoverable
Deliver phase 5 build milestones in line with plan This is on track
Deliver the Queen Square development milestones in line withplan
Time-scales have slipped on this programme
6. Develop newpathways fordiabetes, MSK,COPD and frailelderly patients
Charles House
Agree clinical pathways for each condition jointly with CCGs Diabetes & COPD pathways agreed with Camden. UCLHresponding to procurement process for Camden MSK. Other pathways currently in development
Agree contracting/funding arrangements for each pathway Agreed contracting arrangements for diabetes in Camdenvia Integrated Practice Unit. UCLH responding to procurement process for CamdenMSK. Other arrangements currently being developed
Implement pathways in line with project plan Have achieved pathway developments in line with projectplan.

5.3 Performance against corporate objectives
Quarterly Review
Strategic objective: Support the development of our staff to deliver their full potential
1. Improve staffexperience
Ben Morrin Improved results for the annual staff survey for 2016 with a focus on bullying and harassment and discrimination. This will be reported when we receive the annual staff
survey results
2. Improvedevelopmentopportunities forstaff
Ben Morrin Increase the numbers from all staff groups participating in non-mandatory training opportunities including 80 newapprenticeship appointed by March 2017. This should be delivered in line with agreed quarterly trajectory.
On track to meet our target of 20 new apprenticeships by the end of September and a further 80 by the end of March.
3. Achieve targets forstaff retention,vacancies andtemporary staffingusage
Ben Morrin Vacancy rate below 5% by end of March 2017 (excluding corporate posts). This should be delivered in line with agreedquarterly trajectory
10.4% in June. This is in line with trajectory
Turnover below 13% by end March 2017 (excluding corporate posts). This should be delivered in line with agreed quarterly trajectory.
13.2% reported in June against the 14% standard for Q1
Over 95% of all temporary shifts filled by bank rather than agency by March 2017. This should be delivered in line with agreed quarterly trajectory.
89.5% achieved in June against 90% Q1 threshold
4. Support patientsafety by ensuringstaff completemandatory training
Ben Morrin More than 95% of our staff have completed mandated training 94.7% in June which is in line with trajectory
5. Improve the qualityof appraisals forour staff
Ben Morrin 95% staff are appraised, with objectives targeted at strategic priorities and their personal development [As pert tiers Exec by end April’ tier 2 by end July; all others by end September]
This will be reported when we receive the annual staff survey results
6. Improve the UCLHexperience formedical and dentaltrainees
Ben Morrin An improvement in satisfaction ratings as measured by feedback from UCL for undergraduates and the GMC survey forjunior doctors
For 2016 results: of the programmes for which we have a result, 22 have demonstrated an improved satisfactionscore of 22 and 25 have demonstrated a decreased satisfaction score. This is above the national average.

5.3 Performance against corporate objectives
Quarterly Review
Strategic objective: Achieve financial sustainability
1. Achieve financialtargets
Tim Jaggard Deliver against I&E budgets set for 2016/17 Q1 I&E performance & forecast ahead of plan
Deliver agreed CIP Forecast & YTD performance under plan
Deliver cash flow plan (exact measure to be confirmed by Director of Finance)
YTD balance and forecast above plan
2. Contribute to North CentralLondon’ssustainability andtransformationplan
Tim Jaggard Deliver contribution to development of STP Trust involved in financial modelling, clinical cabinet and specific work streams
Deliver service change in line with the STP
3. Deliver agreedcontracts withcommissioners
Tim Jaggard Deliver activity plan in line with contract Q1 activity above contracted level – risk relating tocommissioner affordability and payment of over-performance
Deliver QIPP in line with contract Developing plans to support commissioner QIPP initiatives, but not yet delivering
Deliver CQUIN Q1 delivery of CQUIN is expected to be 100% in all areas except for sepsis
4. Improve utilisationof beds, theatres,imaging andoutpatientservices
Medical Directors
Improve theatre utilisation to 85% by year end Q1 utilisation was 72.4%
Deliver consistent bed occupancy of 85% for acute medical beds and 90% for all other beds
Bed utilisation has been consistently higher than this (90-93% for medicine) which has impacted on emergency flow


G
Agenda Item 10
Quality & Safety Committee Report


Quality and Safety July 2016 summary report to Board of Directors September 2016 1. Quality Account 2016-17 QSC received the quarter one update on the quality account for 2016-17, for assurance. The quality priorities in the quality account (2015/16) which describe the priorities for 2016/17 will be monitored every quarter but as requested by the QSC the progress of the priorities will be reported via the relevant committee’s report or already established reporting. Priority 1: Patient Experience - to maintain our overall patient experience scores as measured by the Friends and Family Test (FFT) questions and to improve patient experience in priority areas as measured by local and national surveys – this will be covered in the patient experience report which will come to the September QSC. Priority 2 Safety to reduce surgery related harm, reduce the harm from unrecognised deterioration, reduce harm from sepsis and continue Trust wide learning from serious incidents was reported to July QSC as the Sign up to Safety report (see minute 3). Priority 3 Clinical Outcomes - to set up a mortality surveillance group and a mortality governance structure. This was reported to the July QSC (see minute 2). 2. Mortality Governance report In response to an initiative by NHS England which aims to take a common systematic approach to potentially avoidable deaths, the trust has agreed, as one of its quality objectives, to set up a mortality surveillance group (MSG) and mortality governance structure. Although the trust has a low Summary Hospital Level Mortality Indicator we want to ensure that we are learning as much as possible from deaths in order to improve safety and care. We plan to ensure that there is high quality systematic review of deaths in all specialties, including accurate coding. QSC received an update on progress with this objective. The date for the first MSG meeting has been agreed for early August 2016. The group will be chaired by the corporate medical director and will be made up of: the directors for Quality and Safety and Planning and Performance, the Deputy Chief Nurses for the Medicine Board and Surgery and Cancer Board, consultants in anaesthesia, ITU, care of the elderly, emergency services and surgery. The membership is based on the model included in the guidance from NHSE. There will also be junior doctor representation on the group. 3. Sign up to Safety QSC received the quarter one update on progress with this quality objective, for assurance. 3.1 Reducing Surgical Harm 3.1.1 Our aim is a 10% increase in reporting surgical incidents in theatres. The baseline figure for average monthly incidents for 2014/15 was 6.75 per month so this is an increase of 30% compared with the baseline. 3.1.2 Our aim is a 10% increase in near misses being reported (within the 10% increase) The baseline figure for average monthly near misses reported for 2014/15 was 0.83 per month. Taking into account the increase in reporting, the adjusted increase is 62%. 3.1.3 Our aim is a 50% reduction in incidents leading to harm The baseline figure for average monthly incidents of harm for 2014/15 was 0.92 per month. In Quarter 1 of 2016/17, no incidents with harm were reported, this is a 100% decrease compared with the baseline. 3.1.4 Observational audits of checklist use which over time identify improvement in the use of the checklist and associated behaviour in all our theatres continue in rotating locations trust-wide twice a month during Surgical Safety Walk rounds. Audits of 13 patients were
undertaken in May and June 2016. Learning is being fed back through multiple mechanisms e.g. At the Sharp End, local governance meetings, audit day presentations and via other Surgical Safety Walk rounds. The ‘lack of surgical engagement’ referenced in the report is to be discussed & taken forward. 3.2 Deteriorating patients 3.2.1 Our aim is a 96% vital signs completed per patient / per ward, based on a sample of 10 per ward per month The average percentage compliance with the completion of vital signs baseline for 2014/15 was 87.9%. The percentage of Vital Signs completed for 2016/17 Q1 until May 2016 is 99%. 3.2.2 Our aim is 90% patients escalated to the Patient Emergency Response and Resuscitation Team (PERRT) using an agreed communication tool (now agreed to be SBAR) This metric was only recorded in 38% of patients seen by the PERRT (compared to 31% in 2015/16). For those patients where the metric was recorded, 70% of patients were escalated using SBAR. Work has begun by the PERRT team to improve the documentation of this trust priority, but improvements are still required. The team are also leading on work to improve the use of SBAR in all communications regarding deteriorating patients across the trust. 3.2.3 Our aim is a 20% reduction in the mean number of incidents reported per month leading to harm. Quarter 1 2016/17 the average number of incidents with harm is 9.7 per month, this is an increase of 83% compared with the baseline of 5.3 per month. This is because we have seen a large increase in the category ‘unexpected outcome/ deterioration/ death’ which is largely a result of complications being increasingly reported since the introduction of Duty of Candour. This is a positive step towards increased openness and transparency, a core component of a good safety culture, however further work needs to be done to identify which of these incidents are relevant to failure to detect and manage deterioration. 3.3. Sepsis The following progress has been made in Quarter 1 of 2016/17:
• The sepsis project to improve timely and effective screening and treatment of patients with sepsis went live on 8th June in the Emergency department (ED).
• A trust-wide sepsis campaign ‘Sepsis: Spot it. Stop it’ has been rolled out to support the implementation of the new sepsis protocol in ED. An Insight story was released and the Insight pages updated to support the communication of best practice and availability of supporting materials as all key documents are now available on the intranet.
• UCLH is now signed up to the two Sepsis CQUINs for 2016-17. The data collection requirements for this CQUIN are great and the targets aspirational. Funding for a specialist Sepsis Nurse has been approved to support the collection of the required data and to undertake improvement activities and the recruitment process will begin imminently. Quarter 1 targets were partially met but work is underway to achieve our trajectory
• A new leadership structure has been established for the sepsis improvement work at UCLH. Cathy Mooney, Director for Quality and Safety is the executive lead for the work, supported by 4 Clinical leads responsible for implementation in their area. The team are being supported by the Sepsis Steering Group.
Baseline data for improvements in identification and treatment of sepsis has been collected for the period Sept 15 – March 16 using the UCLP sepsis collaborative agreed methodology. This data for confirmed adult sepsis patients arriving in ED shows that we need to improve

the timeliness of best practice care such as antibiotics within the hour, fluids within the hour and vital signs completed on arrival, as well as documentation of the care we provide 3.4 Call for Concern In 2015/16 16 calls were received. 3 were from one patient regarding discharge from ED; 3 were regarding medical care (lack of review, treatment plan and requesting removal of stent by a consultant); 4 were from one patient regarding nursing care; 2 were regarding nursing care; 1 was a discharge concern; 2 were regarding analgesia and 1 was a complaint regarding the Site Managers response. All these Calls for Concern were resolved. 3.5. Continually learn A new patient feedback system has been introduced to collate ‘friends and family’ data at UCLH. This system will also be providing localised surveys for inpatients, with additional surveys in other areas being phased in over the coming year. The new provider offers a more efficient and easy-to-use service, as well as saving valuable time for UCLH staff. 3.5.1 Monthly quality and safety bulletins to continue and to include a ‘good catch’ story every month to encourage learning from near misses. Quality & Safety bulletins continue to be distributed on a monthly basis. The next bulletin will be sent out week commencing 18th July. Content of these bulletins change depending on current safety priorities. 3.5.2 Publication of learning from serious incidents on our website. Summaries of Serious Incidents reported and closed have recently started to be sent to divisions. The decision about whether we publish these on our website will be made in due course. 3.5.3 At least two quality forums per year focusing on safety. At least two have been planned for this financial year and the first one will take place on 19th July. This will focus on learning from the experience of the CQC inspection. 3.5.4 Education services will support teams in sharing their learning from After Action Reviews (AARs) more widely. At least two stories based on one or more AARs to be published in the Quality and Safety Bulletin. AAR has now been incorporated into the Quality Improvement (QI) toolset used by the newly formed UCLH Institute Improvement Team. We plan to promote learning from AARs via the quality and safety bulletin starting next quarter 3.5.5 Achieve the national guidelines for investigation reports being completed following a serious incident (60 working days). Nine SIs were reported in Quarter 1. Of the 2 due for completion in this quarter both were completed within 60 working days. 3.5.6 Have no further ‘Never Events’ reported. There has been 1 Never Event reported in the last quarter. 3.5.7 Consider using rate of recurrence of similar serious incidents (or root causes and contributory factors) as an indication of learning Quarterly incident analysis reports are used to ensure that information is disseminated to the front line about trust level and divisional incident types and trends. In instances of reoccurrence of a similar incident, previous root causes/ contributory factors are cross referenced, and completion of previous actions checked prior to investigation. 3.5.8 Continue with improving care rounds and the focus on learning building on the experience of the CQC Inspection in March 2016 Improving Care Walk Rounds continue to take place twice a month. Additional leaders for these are being recruited and trained to improve sustainability. 3.6 Update: Honesty UCLH aims to be open and candid with our patients, their families and the public on issues of patient safety and in our management of incidents.

The Duty of Candour e-learning package is now in the final testing phase with clinical colleagues. More information on the Duty of Candour can be found in the Quarterly paper to the QSC on Duty of Candour compliance. 3.7. Collaborate UCLH are taking a leading role across UCLP in the work to improve rapid assessment and treatment of Sepsis and Acute Kidney Injury (AKI), sharing our approach and learning across the UCLP network. UCLH is a key member of the UCLP Patient Safety Collaborative and UCLH staff participate in all related shared learning activities. 3.8 Support Schwartz Centre Rounds have been running at UCLH since April 2014 and funding has been secured until 2017. Over 650 members of staff have attended the Rounds which have taken place on a number of sites and covered a range of topics. 80% of attendees would recommend Schwartz Centre Rounds to their colleagues. 4. Annual Patient Safety Report 2015/16 QSC received the trust Annual Safety Report designed to complement the trust Quality Account, providing information and learning relating to incidents, serious incidents, risks, Duty of Candour, Sign up to Safety, CQC preparation and contributions from the Patient Safety and Risk Steering Group committees. The Medication Safety Committee Annual Report is included. Examples of how the trust shares learning are included throughout the document, in addition to key performance information and progress with patient safety projects and programmes undertaken by the trust through the year. The report also addresses the commitments made in the report from last year. It was agreed that the trust needs to undertake more case note audits for monitoring the duty of candour. A review of annual reports to be undertaken to establish ongoing requirement and to establish whether annual reports have to be reviewed by the board of directors prior to external release or whether QSC approval is sufficient. 5. Patient Experience Report QSC received the summary report for quarter four. There were no issues to escalate this quarter from Patient Experience Committee (PEC) but the discussions included:
• The report from Integrated Experience Group • Draft patient and staff experience priorities • Disabled parking update
PEC welcomed the new non-executive director to her first meeting in June, and noted she will be taking over as the chair from August. 6. Duty of Candour QSC received the quarter one report 2016-17. Compliance continues to improve and now stands at 87% for the verbal section and 83% for the written notification as measured on Datix. Divisions continue to work to improve.
Performance timescales have been introduced in accordance with the trust duty of Candour policy and commissioner performance indicators. Trust case note audits do not show such good compliance and we plan to do these more regularly, resources permitting. Key findings from the internal audit are included within the report. It is expected that the full report will be considered following the Audit Committee review.

7. Clinical Audit QSC received the Annual Report for 2015-16. This will now be provided to the Clinical Quality Review group. 8. Adult Safeguarding QSC received the quarterly report from the Adult Safeguarding committee. It was noted that in line with other acute trusts the trust is challenged by the current requirements around Deprivation of Liberty, however it was noted that a consultation is underway to overhaul the regulations. The Safeguarding team were commended for the progress with training and compliance. 9. Infection Control and prevention QSC received the Infection Control and Prevention Annual report for 2015-16. QSC noted the increase in MSSA bacteraemia cases which is as good an indicator as MRSA of the quality of Infection control practices. However the trust appears to have turned the corner in relation to C.difficile which is felt to be the result of better reporting practices, and better access for staff to the dedicated infection control team. It was noted that the trust has not had any deaths or serious morbidity such as requirement for colectomy, since the hospital at 235 Euston Road was opened. 10. Trust Quality & Safety Performance QSC received the Performance Book for May 2016. QSC recommended that inappropriate measures (%) are to be removed from mandatory training tables and the usefulness of friends and family test to be considered by the PEC. 11. Care of surgical instrumentation QSC received feedback about the central sterile supply department (CSSD). It has been identified that the trust requires a rolling instrument replacement programme but this is in competition with other financial priorities. The theatres and anaesthesia division has undertaken to conduct audit of instrument repairs required and servicing across all sites. 12. National neurosurgical audit programme (NNAP) QSC received a briefing on the results of the national audit and UCLH’s performance. The audit shows that we do the most elective neurosurgery in the UK and have the best mortality rate. The audit also identified that our length of stay is longer than the national average and work will be done to reduce this. QSC asked for an update after next year’s audit. 13. Blood transfusion QSC received a summary of blood transfusion audits in 2015/16 and the 6 month audit plan from June 2016, for assurance. Work is ongoing to improve the transfusion Knowledge based assessment for Theatre staff. The trust is to introduce prompt sheets for staff lanyards. Audit is to be conducted into the timing of prescribing and administration of blood products to assess compliance.


H
Agenda Item 11
Finance & Contracting Committee Report


UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST FINANCE & CONTRACTING COMMITTEE REPORT TO THE BOARD OF DIRECTORS
1. Introduction 1.1 This report updates the Board of Directors on the issues considered at the meeting of
the Finance and Contracting Committee (FCC) on Wednesday 7th September 2016, relating to the financial performance and contracting position of the Trust as at 31st July 2016.
1.2 The Board of Directors is asked to: • Note the financial performance for the first four months of the 2016/17 financial
year, • Note the high level planning timetable in order to meet the NHS Improvement
annual planning & contracting deadlines, • Note the contracting update provided to the Committee, and • Note the other updates (Queen Square and Productivity) also presented to the
Committee.
2. Financial Performance 2.1 The Trust’s year-to-date income and expenditure performance at month 4, when
reported prior to donation-related adjustments, was a deficit of £5.2m. The Finance Director informed the Committee that, as set out table 1 below, this year-to-
date position was £1.5m better than plan and was achieved without any release from the Trust’s Board contingency, although there were significant future risks that may require use of the Board contingency.
Table 1 – 2016/17 month 4 financial position
2.2 The Finance Director drew the Committee’s attention to the most recent bottom-up forecast generated from clinical boards and corporate areas, which indicated that the Trust remained on track to deliver its plan at year-end. The Finance Director outlined some of the key assumptions contained within the forecast, including:
• The forecast assumed 100% receipt of sustainability and transformation (STF) funding. However, there was a risk of a proportion being withheld as a result of shortfall against agreed operational targets in line with the recent guidance issued from NHS Improvement, if trajectories are not restated in light of recent activity growth.
• The Trust’s £10m Board contingency was assumed to be required in full.
Page 1 of 4

2.3 The Committee agreed that the Trust’s year-end forecast to NHS Improvement should remain unchanged at a £11m deficit (i.e. delivery of plan).
2.4 The Finance Director mentioned that further progress had been made in identifying new CIP schemes and converting previously red RAG rated schemes to green/amber.
The month 4 CIP position showed that the Trust had delivered year-to-date savings of £11.7m, which was £2.6m (rounded) greater than the planned target of £9.2m. The full-year forecast showed that schemes totalling £38.4m had now been identified, which was £1.9m above the Trust target of £36.5m. The recurrent impact of the forecast, i.e. recognising the full year effect of mid-year schemes offset by non-recurrent savings, showed £38.8m of savings.
2.5 The Trust’s cash balance at 31st August 2016 (month 5) was £68m, which was £3m higher than plan, mainly due to a timing benefit in relation to loan draw-down and the earlier than planned receipt of Quarter 1 STF funding.
3. Financial Planning Update
3.1 The Finance Director advised the Committee that NHS Improvement had informed the Trust that both the contracting round and annual planning were to be concluded by 23rd December 2016, 4 months earlier than in 2016/17.
3.2 The Finance Director welcomed the stated aim of NHS Improvement, which was to provide certainty and stability for a two-year planning and contracting cycle, through early publication of a national tariff, CQUIN framework, NHS standard contract, provider sustainability and transformation fund, and NHS commissioner business rules covering both 2017/18 and 2018/19.
3.3 The Finance Director pointed out that a significantly condensed planning & contracting process would need to be run much earlier than usual to enable the Trust to meet NHS Improvement’s timescales, as follows:
• Approval of the draft 2017/18 and 2018/19 plan by the November Board, • Submission of commissioner activity plans, consistent with final plan by 21st
November 2016, • Approval of the final 2017/18 and 2018/19 plan by the Board in December.
3.4 The Finance Director informed the Committee that the Trust would need to radically simplify the planning round this year and also ensure that the underpinning activity plans, to inform both planning & contracting, were gathered promptly.
3.5 The Finance Director also provided an update on a recently released engagement document, which explained a number of policies that NHS Improvement and NHS England were proposing for the national tariff, the most significant of which were:
• The move to a two year tariff (covering 2017/18 and 2018/19), • Updates to national prices to reflect the HRG4+ phase 3 currency design and
updated cost data, • Changes to specialist top-ups, and • Adjustments to specific prices with the intention of mitigating specific impact.
3.6 The Committee discussed the intention of NHS Improvement and NHS England to put in place an outpatient follow-up block arrangement as part of the two-year tariff. The Committee noted that this was a significant risk for specialised and tertiary services, which were often chronic, and had no onward referral pathway. Additionally, there was a risk that due to the same issue existing in other NHS trusts, UCLH could see a big influx of referrals with other trusts looking to avoid follow-ups by referring onwards to UCLH’s tertiary services.
Page 2 of 4

4. Contracting Update 4.1 The Director of Planning and Performance provided the Committee with a brief update
on 2016/17 contract performance.
4.2 The Committee noted that Trust had now issued month 1 and 2 reconciliation statements, which provided a summary of adjusted monthly payments, reflecting actual activity volumes over contracted activity volumes, to all commissioners in line with the contract. The Committee also noted that this should facilitate much more timely payment of contractual over performance than in previous years.
4.3 The Director of Planning and Performance pointed out that there was a significant level of over performance across all contracts at month 3, which in part could be explained by commissioners contracting for lower levels of activity than the Trust had said was needed.
The Director Planning and Performance also mentioned, however, that the Trust continued to work with local commissioners in response to their queries concerning increased activity and cost in the Trust’s outpatient and maternity services, in order to understand the drivers and develop mitigating actions.
5. Queen Square Financial Update 5.1 The Medical Director for Specialist Hospitals provided the Committee with an update on
Queen Square’s financial performance, including delivery of CIP and year-end forecast. This followed on from a presentation given by the Divisional Manager for Queen Square to FCC in July.
The Medical Director also briefly highlighted the potential implications to the division of the national tariff proposals for 2017/18 and 2018/19 that were currently out to consultation.
5.2 The Medical Director pointed out that Queen Square remained in a challenged financial position in 2016/17 and informed the Committee that at month 4, the division’s financial position was an adverse variance to plan of £1.6m, which was driven by a combination of under delivery against NHS clinical income (an adverse variance of £0.8m) and other income (£0.8m).
5.3 The Medical Director informed the Committee that the division’s activity plan for the remainder of the year was particularly stretching and mentioned that plans had been put in place to minimise activity loss over the summer, with initial projections suggesting that there was likely to be good utilisation of capacity in August.
5.4 The Medical Director also informed the Committee that up to £1.6m of the division’s 2016/17 CIP target of £8.5m was at risk of not being delivered, although work was on-going to identify further CIP schemes.
5.5 The Finance Director informed the Committee that there remained a clear expectation for Queen Square to target, as a minimum, delivery of its planned position over the remaining months of the year; there remained significant risks to Queen Square’s position, particularly around the division’s redevelopment programme, as well as recruitment, contracting issues and workforce turnover, impacting upon activity.
The Committee also noted the importance of the right level of staff being in place at Queen Square to deliver patient services safely and effectively.
5.6 The Committee asked if the division could provide a further update to FCC in December, focusing on the underlying productivity assumptions, and plans to achieve the necessary efficiency gains, contained within its financial projections.
Page 3 of 4

6. Productivity Update 6.1 The Committee was provided with a report outlining the Trust’s proposed approach to
taking forward the Carter agenda to increase productivity by learning from best practice and national benchmarks.
6.2 The Committee noted that a Productivity Delivery Group (PDG), reporting to the Executive Board, had been established to oversee the delivery of Lord Carter’s recommendations at UCLH. The PDG was chaired by the Finance Director as Senior Responsible Owner (SRO) for the programme and involved senior representatives for each key workstream covered by Carter, including the Medical Director for Specialist Hospitals Board as Clinical SRO.
6.3 The Finance Director informed the Committee that the PDG was proposing to focus its efforts in two key areas:
a) Proactively providing simple metrics and analysis to support boards and divisions in understanding progress against Carter benchmarks and driving action,
b) Supporting workstream leads to develop robust workplans for delivering on the Carter agenda and provide light touch monitoring to support both external and Executive Board reporting.
6.4 The Finance Director pointed out that the Carter report proposed an ambitious agenda for all acute hospitals, and the Trust did not have the capacity or resources to tackle it all at once. The Finance Director advised the Committee that each of the Carter recommendations was being worked through in detail to understand the implications for UCLH and urgent work being undertaken to identify key areas of opportunities and how the Trust should prioritise the recommendations.
The Committee noted that the PDG was currently prioritising the following areas of work: • Provision of simple productivity data to all divisions • Provision of targeted information about high cost items (e.g. bed days, MRI
scans) to theatres, wards and clinics to encourage an increased focus on value for money
• Development of meaningful clinical productivity metrics for specialties, starting with trauma & orthopaedics and ENT as pilot areas
• Theatre, outpatient and diagnostic productivity programmes (building on uclh future)
• Taking forward nursing recommendations (particularly as part of the Exemplar Ward programme)
• Rolling out electronic job planning and e-rostering, and • Development of Hospital Pharmacy Transformation Plan.
6.5 The Finance Director informed the Committee that the PDG would be in a position shortly to report monthly productivity metrics, aligned to the national Carter adjusted treatment cost (ATC) index that would allow the Trust to be able to track delivery of improvements within the productivity programmes and more widely in each clinical division.
Harry Bush Tim Jaggard Chair of FCC Finance Director 8th September 2016
Page 4 of 4

I
Agenda Item 12
Audit Committee Report


UNIVERSITY COLLEGE LONDON HOSPITALS NHS FOUNDATION TRUST
Report to Board of Directors – 14 September 2016
MAIN POINTS FROM THE AUDIT COMMITTEE
The Audit Committee (AC) met on 19 July to consider the following important matters. 1. Internal Audit (IA)
1.1 IA Assurance Reports – 2015/16 The AC reviewed seven reports with varied findings. Four of the reports were in progress; the opinion will be carried forward to 2016/17. One of the reports (RTT) received an amber rating. The AC noted that management had accepted the recommendations in the reports and had action plans in place to deliver these. IA also advised that there were a number of outstanding actions from previous reports to be followed up; action was being taken jointly with the Trust to improve delivery of the recommendations.
The report and rating were:
Report Rating Assurance Referral to Treatment (RTT) amber limited CGI service provision – ICT Service provider yellow reasonable IT project delivery/management yellow reasonable Duty of Candour yellow reasonable Research yellow reasonable High cost drugs yellow reasonable Cost improvement programmes (CIP) yellow reasonable
Discussion focused on the research, Duty of Candour, and IT project delivery reports.
The AC had discussed RTT at its May meeting when it considered a report on the quality account. A follow up report on RTT and other data issues is at 5.2 below.
1.2 Research The AC had previously met with Nick McNally, Divisional Manager for R&D to discuss research administration following an incomplete audit. This second audit focused on the process to support financial reporting but also commented on the previous review. It advised that although the logging of all project documentation had improved there was still more work to be done on the general administration of projects, this included a recommendation to have a central repository for information. On financial reporting, IA commented that the budget cost centre for each study was not always captured; one of the recommendations included a revised standard operating procedure and budget sign off process. This would be in place by October. The AC noted that not all the recommendations had a clear action plan however; IA advised that all recommendations had been accepted and the majority implemented. The AC asked IA to refer the report to the Divisional Manager for R&D to seek assurance that there were no outstanding actions. 1.3 Duty of Candour (DoC) The Duty of Candour requires the Trust to be open with patients when mistakes made in their care had led to significant harm. The audit aimed to look at how well the DoC policy was working. IA advised that although they had identified some weaknesses in policy application the staff they met understood the DoC and took it seriously. The weaknesses were mostly recording errors related to follow up of incidents; the policy required a letter to be sent to the patient after incident review and if harm had been
1

caused. In some cases (26%) there was no record that a letter had been sent or a record of the reason why it had not been sent. Three clinical divisions had identified leads to support staff to understand the DoC responsibilities; in these areas the policy had been better implemented. The AC noted the recommendations which included a review of the policy; it also referred the report to the QSC for discussion. 1.4 IT Project Delivery/Management IA had reviewed three IT projects and advised that the management of projects overall was generally satisfactory. The recommendations were mostly about improving practice including strengthening project monitoring and financial governance. The AC noted that one of the projects (RIS/PACS) had a high number of actions relating to the lack of technical expertise being available to support the project. It was concerned that this might indicate a future project management risk. Tim Jaggard, Finance Director, advised that a corporate PMO was being established to support and record the flow of project documents, this would help mitigate the risk. The AC agreed to invite David Hill, Director of Digital Services, to its September meeting to discuss IT projects oversight. 1.5 Audit Plan 2016/17 The AC reviewed the final IA plan for 2016/17 prepared by TIAA; this had been presented in draft at the May meeting. The plan had been reviewed against the audit risk universe and would be grouped into nine domains to ensure the effective use of audit resources. It was agreed that cyber security should be added to the plan and that the AC would review the scope of the finance audits before they commenced. Flexibility had been built into the plan to allow for any emerging risks. The AC approved the IA plan.
2. Counter Fraud The AC reviewed the Local Counter Fraud Specialist’s (LCFS) progress report. The risk profile heat map was based on emerging cases and this indicated an increase in working during NHS time across the LCFS client base. The AC noted that as well as the regular counter fraud meetings, the head of workforce who leads on fraud issues holds monthly meetings with counter fraud; this has helped improve the management of casework. LCFS also advised that the annual self-review against the NHS Protect standards had been completed and the Trust had reported a green rating. This means UCLH is able to demonstrate that it is a low risk organisation.
3. Raising Concerns The AC received an annual update report on whistleblowing (raising concerns) from the Ben Morrin, Director of Workforce. Since the last update in July 2015 the Trust had implemented a new policy, which included the recommendations from the Freedom to Speak Up report1. One of these was the introduction of an independent guardian accessible 24 hours a day for individuals to raise their concerns with. This service had been introduced in June and would be evaluated after six months.
11 issues had been raised compared to 13 in the previous year; all were investigated. The AC also asked whether, from these issues, the Trust was gaining a better understanding of what bullying and harassment meant. The AC was advised that not all reported issues were about bullying and harassment but where this was the case the guardian service will help staff and managers to reflect on their different experiences of the same incident. The AC welcomed this approach.
1 Sir Robert Francis, Freedom to Speak Up Report, An independent review into creating an open and honest reporting culture in the NHS
- 2 –

4. Risk and Assurance 4.1 Finance Metrics Report The AC considered a quarterly report on financial control. It reported the June position or the most recent if June data was not available. The metrics included aged debts (see the bad debt report at 5.1 below), aged creditors, performance against the Better Payments Practice Code (BPP), agency and consultancy spend, and invoice and trading information. The AC discussed the metrics on BPP and agency staff. BPP had improved between April and June. This indicated an increased use of purchase orders, invoice approval and payment. The next report would propose a KPI for the next three quarters. On agency spend the AC was pleased to note that this had reduced significantly since June 2015. Agency staff were only being used in service areas where there was no other supply option. The trend on consultancy was noted. This area of spend appeared to be less under control however, the AC noted it included staff with specific expertise brought in to support projects such as the recent digital transformation work. The next report would provide more detail on this metric. 4.2 Board Assurance Framework The AC received the opening Board Assurance Framework for 2016/17 which had also been presented to the Board on 13 July. It set out 17 risks including two new risks. One related to the delivery of ‘Paper-free at the Point of Care’ – preparing and aligning local digital plans, the second highlighted the impact of unfilled junior doctor posts on training, workload and resources. The report also advised the removal of two risks. The AC was concerned about the removal of the risk relating to nurse staffing and supported the view of the Board that the removal of this risk be reconsidered by the Executive Board. The AC also discussed two Sustainability and Transformation Plan (STP) risks and suggested that the impact of the STP on the Trust’s service strategy should be taken into account when assessing the risk, this was agreed. It was also agreed that an update on the productivity metrics in place to deliver the ‘Carter’ Agenda, the risk relating to financial sustainability/efficiency, should be provided to the Finance and Contracting Committee (FCC).
5. Other assurance matters
5.1 Bad Debt Report The AC considered a report on bad debt from Paul Sutton, Accounting and Treasury Manager. It was advised that much of the debt was aged and that all avenues for chasing the debt had been exhausted. The reported debt was deemed uncollectable with no chance of recovery. In one case the individual concerned had died. The AC will hold a deep dive seminar on the overseas visitor’s process in the autumn which will cover the pathway from identification of a patient when they attend a UCLH hospital to payment management. 5.2 Data Quality Assurance The AC reviewed a quarterly report from Simon Knight, Director of Performance and Planning which summarised the key actions from the quality account audit of three indicators - RTT, the A&E four hour wait, and the six week wait from request to diagnostic procedure. The audit had identified a number of areas to be addressed including data collection in real time, ongoing data testing, and developing training to help staff understand the importance of data accuracy to patient care. On RTT and diagnostic waits, the AC noted that the Trust had revised its access policy to better describe the pathway rules and improve data collection. It had engaged the CCG and governors in this process. A modified training package will also be introduced
3

to support the policy. Individuals will need to pass their training, this will ensure that staff are appropriately trained to better manage patients through the pathways. On data accuracy, the performance team will undertake sample audits to test whether the rules are being applied correctly and run tests across all features of each pathway. The AC will return to this issue in September.
5.3 Quality Impact Assessment (QIA) Governance The AC reviewed a report from Guy Dentith, Deputy Director of Finance on QIA governance. The report set out the framework in place to assess the potential risks of a cost improvement plan (CIP) on patient care. The criteria advised a) what schemes had to undergo a risk assessment and b) what had to be considered. The latter included clinical safety and patient and staff experience. The AC noted the process was supported by a central PMO and suggested the FCC may wish to consider these assessments as part of its ongoing review of CIPs.
5.4 Waivers report The AC reviewed a six monthly report on waivers from Pia Larsen, Director of Procurement and Supply Chain. This showed that the number of waivers was broadly consistent with the previous year. It was agreed that the next report would also provide a more detailed analysis of the reason for the waiver. The AC also noted that the waiver process had been revised and the Trust’s Standing Financial Instructions were being updated to align these with the new process.
6. Annual Report of the Work of the Audit CommitteeAC Members reviewed the committee’s Annual Report for the year 2015/16 - attachedfor Board Members only.The report gives an overview of the Committee’s activities and demonstrates to theBoard and the Council of Governors how the AC discharged its responsibilities duringthe year. It confirms that the AC reviewed its terms of reference and completed areview of how it operates, no specific areas required development.The AC also considered the work of both auditors and the report advises that DeloitteLLP have been appointed as the Trust’s external auditors for three years commencingwith the 2016/17 accounts.
ACTION: The Board is asked to endorse the report and note the areas the AC will focus on in 2016/17. The report will be circulated to the Council of Governors and placed on the Trust’s website.
Rima Makarem Audit Committee Chair
- 4 –

Audit Committee Annual Report
Report of the work of the Audit Committee during 2015/16

Introduction by the Chair of the Audit Committee I am pleased to present this Annual Report to the Board of Directors and the Council of Governors. It provides an overview of the Audit Committee’s activities from April 2015 to March 2016 and sets out how the Committee has met its key priorities. In addition to the regular activities, we followed up work with the UCLH information team on data integrity and how good quality information can help staff and patients make informed decisions. We will focus more time on this important topic in 2016/17. We also spent time discussing the risk and assurance process and this year, management provided a more in-depth risk report which allowed us to better understand the overall picture of corporate and clinical risk at organisational and divisional level. We are satisfied with the approach management are taking. I am fortunate to be supported by excellent non-executive colleagues, who help discharge the committee’s responsibilities to provide independent assurance on the effectiveness of the Trust’s system of integrated governance. We are supported by management, as well as internal and external audit and the counter-fraud team. I am grateful to all for their contribution. I firmly believe that an effective Audit Committee can help UCLH deliver its vision to deliver top quality care, excellent education and world class research through improving processes to support better patient outcomes and enhance confidence in corporate, clinical and financial governance. This will be important in the coming years given the financial pressures facing the NHS.
Rima Makarem Non-Executive Director Chair, Audit Committee

3
Contents
Role of the Audit Committee Page 4
Membership and Meetings Page 4
Board Governance Arrangements Page 5
Business of the Committee Page 5
Risk Management Assurance and Governance Page 5
Raising Concerns (Whistleblowing) Processes Page 6
Internal Audit Page 6
Counter Fraud Page 7
External Audit, Review of Financial Statements and Annual Reports
Page 7
External Audit Tender Page 7
Non Audit Work Page 7
Evaluation and Assessment and Briefing Page 8
Looking forward to 2016/17 Page 8
Conclusion Page 8
Appendix A – UCLH Internal Audits 2015/16 Page 9

4
Report of the work of the Audit Committee during 2015/16
1. Role of the Audit Committee
1.1 The Audit Committee’s (Committee) main role is to provide independent assurance to the Board of Directors (Board) on the effectiveness of UCLH’s internal control and governance arrangements. It follows the best practice guidance set out in the current NHS Audit Committee Handbook1. Its responsibilities are described in terms of reference; these were reviewed in March 2016 and are available on the UCLH website www.uclh.nhs.uk
2. Membership and Meetings
2.1 Four independent non-executive directors are members of the Committee.
2.2. Brief CVs of all members including any declared interests are available on the UCLH website. Both Harry Bush and Kieran Murphy have recent and relevant financial experience.
2.3. The Committee met seven times during the year and attendance at the meetings is recorded below. Two further meeting (19 April and 24 May 2016) were also held to review the annual accounts and annual reports for the year.
Members
21 April 2015
21 May 2015
21 July 2015
15 Sept 2015
17 Nov 2015
19 Jan 2016
15 Mar 2016
Rima Makarem
Harry Bush
Kieran Murphy
x
Diana Walford
Table above – Member’s attendance at meetings in 2015/16
2.4. The internal and external auditors, the deputy chief executive, finance director and deputy finance director, and the director of corporate services regularly attend meetings to assist the Committee with its duties. Other directors and senior managers are invited to attend to provide assurance on specific items. The counter fraud service provider attends four times a year and the chief executive attends annually to discuss the annual accounts. The chief executive and the chairman attended the meetings held in May.
2.5. The Committee members also held private meetings with both the external audit partner and the head of internal audit during the year.
1 Health Financial Management Association (HFMA) Governance and Audit Committee
Dr. Rima Makarem Member from July 2013 and Chair from January 2014
Dr. Harry Bush Member from December 2011
Mr. Kieran Murphy Member from January 2014
Dr. Diana Walford Member from February 2012

5
3. Board Governance arrangements
3.1. There are three other Board committees: finance and contracting; investment; and quality and safety (QSC), all with a monitoring and oversight role. Audit Committee members are familiar with the work of these committees, attending all of them between them. This strengthens the Audit Committee’s effectiveness. This is particularly notable when it considers clinical risk issues. The QSC oversees all aspects of clinical governance including clinical audit and provides assurance on the annual quality account. The Audit Committee regularly cross-refers clinical matters to the QSC, who then report back on their discussions.
4. Business of the Committee
4.1. The Committee has an annual work plan, developed from its terms of reference, to which areas of risk for are added for review in the course of the year. In 2015/16, assurance on data quality and the review of financial metrics were added to the plan. The following provides an overview of the business conducted during the year demonstrating how an effective Committee can bring benefits.
5. Risk Management, Assurance and Governance
5.1. The Committee has continued to review the operation and management of the risk and assurance framework. The principal UCLH risks are set out in more detail in the UCLH annual report 2015/16.
5.2. During the year the Committee reviewed the Board Assurance Framework (BAF) and asked management to centre it on strategic rather than operational objectives. This enabled better monitoring of the strategic objectives and discussion focused on the key risks to their delivery as well as on the effectiveness of the BAF process. In year the Committee sought additional information on risk appetite and requested that external sources of assurance be included in the BAF. In 2016/17 the operational objectives will be monitored through the chief executive’s performance pack.
5.3. The Committee reviewed a quarterly risk report from the risk co-ordination board, the executive committee with oversight of risk. Last year members commented on a new risk matrix which would better describe the impact of a risk on UCLH, this now forms part of the report. As well as reviewing the Trust’s principal red risks, the Committee also focused on the high clinical and non-clinical amber risks. It also received an overview of the Trust’s risk profile. This additional information gave the Committee the opportunity to seek assurance on emerging risks and in year it asked for more information relating to cybersecurity, estate management, and data integrity.
5.4. Preparing the Annual Governance Statement (AGS) is an important part of the governance process. To ensure that the AGS can be recommended for inclusion in the annual accounts, the Committee received regular reports on the control framework and the internal assurance processes throughout the year. These included:
- A compliance statement on how the requirements of the AGS had been met.
- A report on the successful roll-out of the revised Standing Financial Instructions and Scheme of Delegation, in particular the changes to the procurement processes and how these had improved budget management.
- A report on finance metrics which included write-off of aged debts, losses and special payments. It also included new metrics such as agency and

6
consultancy spend. The Committee agreed this new comprehensive report will strengthen the assurance provided on financial control. It will be presented three times a year.
5.5. The Committee also requested and received separate reports from management on items including CQC preparedness, business continuity and working whilst sick. The latter has been included in the new anti-fraud and bribery policy as an example of fraud that could lead to dismissal.
5.6. The Committee also followed up progress against issues it had identified in 2014/15 including medical job appraisal. It noted that management had focused on improving compliance with mandatory training (to limit risk and maintain safe working practice). This year during their appraisal, clinicians were asked to declare if they had completed mandatory training. If it is not completed it will affect their opportunity to be considered for a clinical excellence award.
6. Raising Concerns (Whistleblowing) processes
6.1 The Raising Concerns (Whistleblowing) process was reviewed by the Committee who discussed how concerns were investigated. In 2014/15 it explored how a concern raised outside UCLH was dealt with. This year a review had been undertaken to identify what common themes emerged from the concerns raised and how the Trust was dealing with these. This will be followed up in 2016/17.
7. Internal Audit
7.1 TIAA Ltd was appointed as internal auditors from 2015/16 for three years and a draft risk-based work plan for the coming year was approved in May 2015. The outgoing auditors carried forward two reports into the 2015/16 year.
7.2 Each assurance report included an opinion and a management action plan to address any weaknesses. A senior member of the management team attended the Committee to present the plan for a report assigned an amber or red opinion; the Committee subsequently followed up the actions. The 2015/16 reports are listed in Appendix A. A summary with comparative figures from last year is shown in the table below. This year we were pleased to note that there were no red opinions.
Assurance
Reports 2014/15
Reports 2015/16
number percent number percent
Green: Substantial Assurance 4 15 2 9.5
Green / Amber or Yellow: Reasonable Assurance
16 59 17 81
Amber / Red or Amber: Some/Limited Assurance
7 26 2 9.5
Red: Cannot take Assurance/ No Assurance
- - - -
Total reports 27 100 21 100
Advisory 6 - 4 -
7.3 The Committee referred some reports to other committees for a more in-depth discussion. For example, the report on the process for completion of the WHO safe surgery checklist was sent to the QSC.

7
7.4 It also reviewed the internal audit annual report for the year including the Head of Internal Audit’s (HOIA) opinion. The opinion was one of reasonable assurance which was subsequently included in the AGS. Four reports will be carried forward into 2016/17.
8. Counter Fraud
8.1 RSM, formally Baker Tilly, the local counter fraud services (LCFS) provider, presented updates on fraud and a counter-fraud annual report to the Committee. These detailed the fraud policy work and gave an analysis of emerging fraud risks across the provider sector and the wider NHS. They showed that more pro-active anti-fraud work was being carried out and also included information about cases under investigation.
9. External Audit, Review of Financial Statements and Annual Reports
9.1 In April 2015, the Committee reviewed and agreed the external audit plan with Deloitte LLP and received quarterly progress reports and briefings throughout the year. The reports highlighted changes to accounting policy and recommendations for improvements in internal controls. The Committee discussed risks and weaknesses that required attention and the management response on how recommendations would be implemented. Further details about the plan and the audit fees can be found in the annual report and accounts.
9.2. The final audited accounts had an unqualified opinion, with no weaknesses identified.
9.3 The Committee reviewed both the annual report and quality report. Both provided a narrative on the achievements for 2015/16 and on the delivery of the Trust’s strategic objectives and quality indicators. The finding on the quality report included a modified opinion in respect of Referral to Treatment (RTT) and the A&E 4 hour waits indicators. Data integrity had already been added to the annual workplan; the Committee will track the improvements relating to RTT and A&E in the coming year.
9.4 The Committee recommended the 2015/16 annual report and accounts to the Board.
10. External Audit Tender
10.1 Deloitte LLP has been the external auditors for five years, appointed from 2011/12. Following an open tender process, the Council of Governors appointed Deloitte LLP in April 2016 to provide the external audit service on a three-year contract commencing with the 2016/17 Accounts. This may be extended for up to 2 years.
10.2 The Committee will assess the auditors’ work in June 2017 to ensure that the work is of a sufficiently high standard and fees are reasonable.
11. Non Audit Work
11.1 The Committee reviewed the engagement of the external auditors’ policy which governs the use of non-audit services. Deloitte had only carried out work required by a regulator in 2015/16 which is allowed under the policy.

8
12. Evaluation and Assessment and Briefings
12.1 The Committee’s performance was evaluated by an external advisory firm and self-assessed against the checklist in the audit handbook. No significant issues were identified and it was considered that it could provide assurance to the Board that it functioned well. The key issue to emerge related to the internal audit service and how support might be given to both the audit service and management to deliver the plan. Action was taken in year to facilitate this.
12.2 Committee members attended two workshops, cybersecurity and nursing recruitment, to assist them with their responsibilities. Also, an annual session on risk management and assurance was held jointly with the Board at which members discussed the strategic risks facing UCLH. The internal and external auditors also provided regular audit, governance and legal briefings for the Committee.
13. Looking forward to 2016/17
13.1 The Committee will give priority to the following areas:
review the effectiveness of information governance processes;
review processes that relate to the raising concerns policy;
review the proactive LCFS work in particular relating to cybersecurity;
review reports on data integrity and quality governance;
find out how the trust prepares its staff for a major incident;
consider how the BAF and risk report can be made more dynamic and delivered in a more timely way to the Committee and Board.
It will also keep under review the effectiveness of its own working arrangements.
14. Conclusion
14.1 The Committee feels that the information in this report and the reports provided to the Board throughout 2015/16 demonstrate how it adds value to the overall governance of UCLH. It has held management to account in particular for the implementation of improved internal control on financial policy. In completing its work it places considerable reliance on the work of both internal and external audit and is able to conclude that the UCLH’s systems are generally sound.
14.2 In making this statement, the Committee thanks Tim Jaggard, Finance Director, for his support. It also acknowledges the support given by external audit.
14.3 The Board is asked to endorse the Annual Report of the Audit Committee which will be presented to the Council of Governors in October.
Rima Makarem
Chair, Audit Committee
July 2016
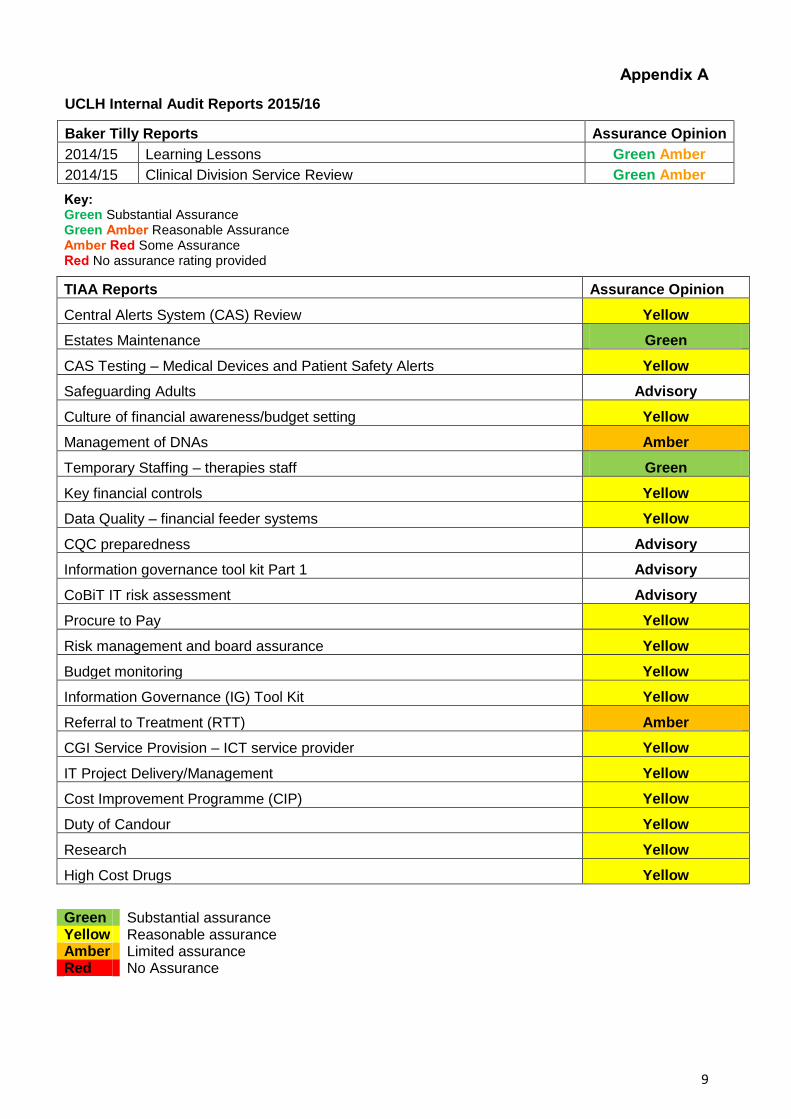
9
Appendix A
UCLH Internal Audit Reports 2015/16
Baker Tilly Reports Assurance Opinion
2014/15 Learning Lessons Green Amber
2014/15 Clinical Division Service Review Green Amber
Key: Green Substantial Assurance Green Amber Reasonable Assurance Amber Red Some Assurance Red No assurance rating provided
TIAA Reports Assurance Opinion
Central Alerts System (CAS) Review Yellow
Estates Maintenance Green
CAS Testing – Medical Devices and Patient Safety Alerts Yellow
Safeguarding Adults Advisory
Culture of financial awareness/budget setting Yellow
Management of DNAs Amber
Temporary Staffing – therapies staff Green
Key financial controls Yellow
Data Quality – financial feeder systems Yellow
CQC preparedness Advisory
Information governance tool kit Part 1 Advisory
CoBiT IT risk assessment Advisory
Procure to Pay Yellow
Risk management and board assurance Yellow
Budget monitoring Yellow
Information Governance (IG) Tool Kit Yellow
Referral to Treatment (RTT) Amber
CGI Service Provision – ICT service provider Yellow
IT Project Delivery/Management Yellow
Cost Improvement Programme (CIP) Yellow
Duty of Candour Yellow
Research Yellow
High Cost Drugs Yellow
Green Substantial assurance Yellow Reasonable assurance Amber Limited assurance Red No Assurance

University College London Hospitals NHS Foundation Trust Trust Headquarters 2nd Floor Central 250 Euston Road London NW1 2PG Tel No 020 344 79976 Email address: [email protected] Web address www.uclh.nhs.uk

J
Agenda Item 13
Audit Committee Minutes


1
AUDIT COMMITTEE (AC)
Minutes of the meeting held on Tuesday 24th May 2016
Present: Audit Committee Members Rima Makarem Non-Executive Director and Chair (RM) Harry Bush Non-Executive Director (HB) Kieran Murphy Non-Executive Director (KM) Non-Members Sir Robert Naylor Chief Executive (RN) Richard Murley Chairman (RMu) (From 10am) Tonia Ramsden Director of Corporate Services (TR) Tim Jaggard Director of Finance (TJ) Dominic Firth Deputy Director of Finance (Interim) DF Paul Grady Internal Audit, TIAA (PG) Phil Lazenby Internal Audit, TIAA (PL) Anthony Hargreaves Deloitte, External Audit (AH) Craig Wisdom Deloitte, External Audit (CW) Rachel Maybank Associate Director, Communications (RMy), For Item 5a Cathy Mooney Director of Quality & Safety, For Item (CM), For Items 4 and 5b Simon Knight Director of Planning & Performance, For Item (SK) For Item 4 Mairi Bell Chief Accountant; Minutes
Matters Covered
1. Apologies for Absence
Diana Walford (DW), Non-Executive Director
Neil Griffiths (NG), Deputy Chief Executive 2. Minutes of the Meeting held on 19th April
The minutes were agreed. 3. Matters Arising AC agreed to close the following MA items as completed: MA 338, MA 339, MA 340, MA 344, MA 335, MA 345, MA 328

2
Matters Covered
MA 347 – PG advised AC that more work was needed on the Internal Audit plan for 2016-17, and that useful feedback had been received from TJ. PG proposed circulating the plan by 31st May. RM agreed. MA 348 – Counter Fraud provided confirmation that the three LPEs’s selected for 2016-17 were Overseas Visitors, Pharmacy and Procurement. MA 350 - TR confirmed this had been completed. MA 305 – TJ updated on the BRC process, advising that implementation of the PQQ was done and feedback was positive. TJ added that there was a downward pressure on overhead % retained by Trusts with benchmarking being done to review this. TJ further added that the next deadline in the process would be the following week. TJ suggested that this was more appropriately an FCC issue and proposed redirecting to that committee. MA 324-326 – TJ confirmed these would be on the July agenda. MA 343 – AH confirmed this would come to the July meeting. MA 351 – DF updated AC on the review carried out by PwC on behalf of DH, noting that PwC had reviewed the 2014-15 year end and month 9 of 2015-16, focussing particularly on provisions, income and other areas identified by DH, including asset valuations. DF nothing substantive was found to suggest any change to UCLH’s accounting treatment, noting particularly that the year-end valuation process was underway at the time of the PwC review. DF advised that UCLH had seen output specific to UCLH and had made a factual accuracy review, but had no right to review the conclusions of the overall piece of work. RM asked if there were any recommendations for UCLH. DF replied that there were none. 4. External Audit CW presented two reports from Deloitte, covering the audit of Financial Statements, and the review of the Quality Account. 4a. Financial Statements Audit CW noted that the audit process had been very smooth this year, despite the additional complexity of some of the adjustments made. CW advised that the audit opinion on the accounts was expected to be clear and unmodified, with no exceptions raised. CW added that a modified opinion was expected on the Quality Accounts, but this would not impact the financial numbers. CW noted no significant adjustments were unprocessed. CW drew AC attention to the impact of exceptional items, on page 5 of the report. CW then highlighted significant risks addressed in the audit. CW noted that in addressing revenue recognition, the auditors had found the provision to be prudent, but

3
Matters Covered
within an acceptable range. CW noted that with regard to property valuation and the alternative site proposal, UCLH had demonstrated a high level of rigour and a well- documented approach. CW noted that the going concern work had focussed on cash flow and that auditors were in agreement with the Trust’s view of this. It was highlighted that AC had been robust in their challenge and consideration of these areas. CW noted that due to additional pressures, management override of key controls had been included as a significant risk item, but that no evidence of management bias had been found, and that changes made were appropriate. RM asked how Middlesex Annex had been treated. TJ replied that this was the same as the previous year with no impairment beyond the District Valuer’s view.TJ noted that discussions with the UCLH Charity were on-going in respect of the site. CW noted that Deloitte had considered the circumstances of the Middlesex Annex and remained content with the Contingent Liability note included. RM asked about the recommendation for Road Traffic Act (RTA) claims on page 37. TJ explained that this was a separate payment system for the Trust to recover additional funding for patients from road traffic accidents. TJ added that the accrued income had been based on a historical estimate and the Trust had not accessed specific information available online. TJ confirmed the process would be updated immediately. KM asked about the PFI lifecycle adjustment and noted it was unclear as to whether there was scope to exercise judgement. TJ replied that judgement would be based on evidence available; noting that while the PFI model was the best evidence available the Trust wouldn’t normally expect to have access to this. KM asked about Deloitte’s view. CW replied that Deloitte had considered the source of evidence and whether it was reliable. CW added that PFI experts at Deloitte had reviewed the model comparing the current one with the original proposed model on which lifecycle prepayments had originally been based. CW noted that a number of assumptions had changed in the 10 years since operation of the site commenced. CW concluded that Deloitte were in agreement with management’s view of the proposed change. KM asked what had substantively changed. DF replied that the original accounting was based on a pre-build model and early years spend had not been as originally expected, although this was now starting to increase as the building aged. HB asked about the mismatch of receivable balances, and what this meant. CW replied that this showed a net position between UCLH and NHS counterparties, net of provisions. CW added that this was one measure considered in assessing the receivable position. CW noted that agreement confirmed that an invoice had been swapped, not that it would necessarily be agreed or paid, noting for example that March flex data was not confirmed until after the Agreement of Balances exercise had been completed. CW highlighted that the figures had been adjusted to exclude provisions and provide a direct comparison to the previous year.

4
Matters Covered
4b. Quality Account Audit CW presented Deloitte’s report on the Quality Account, noting that data quality had been a challenge for many NHS Trusts and that UCLH was not an outlier. AC discussed some proposed amendments to some of the ratings indicated, giving agreement for updates to be made after the meeting subject to discussion with CW and agreement of SK and TJ. 5. Annual Report and Accounts, including Quality Account 5a Annual Report RMy attended to present the final version of the Annual Report. RM noted the page turning reviews which had taken place, and asked if there were any further comments. RMy advised that design work was on-going. HB asked about the wording on the lifecycle adjustment. TJ confirmed this had been updated. RM asked about the comparative comment on A&E performance on page 17. TR agreed to check and confirm this. AC agreed wording subject to TR’s confirmation. 5b Quality Report CM attended to present the Quality Account. CM highlighted two things from the consistency check – figures on page 5 to be changed to reflect a full year position, and a total to be corrected on page 41. RM asked about priorities on page 27 and whether these should state “this should be improving or maintaining patient experience”. CM replied that this would be maintaining standards if already high. RMu added that some explanation would be required to note why maintaining would be good. RM asked about the discussion of never events on page 35, and if aspiring to no more never events would be setting up to fail. CM replied that the aspiration needed to be to have none. RN added that the definition of never events can be challenging. CM added that never events were often put right at the time and often led to no patient harm. RMu suggested qualifying the statements. 5c Remuneration Report DF presented the final Remuneration Report, noting that the main change from the draft presentation in April was the inclusion of the Fair Pay Multiple. RMu asked about benchmarking of this figure. DF confirmed that benchmarking had been done with similar Trusts, and the UCLH figure had been consistent with the others reviewed.

5
Matters Covered
5d Annual Governance Statement DF presented the final Annual Governance Statement (AGS) noting that some redrafting had been attempted since the April AC, but that this had been challenging due to the prescribed format and wording. DF noted that some new wording had been added in respect of the Quality Account and a paragraph on how the Board seeks assurance had also been added. HB asked about the wording in the penultimate paragraph about ED and whether there would be similar wording for RTT. DF replied that the comment was specific to ED. HB commented that the AGS was not referencing the Deloitte opinion on RTT. AH replied that Deloitte were satisfied that data quality issues raised had been acknowledged in the report. RMu asked about pathway complexity and what this meant. RM suggested that maybe patient complexity would be a better description. TJ agreed to review this and omit it if the other reasons provided sufficient information. HB queried the wording on page 13 and DF agreed to change the order of the paragraphs. 5e Final Year End Accounts & Commentary DF presented the final year end accounts and commentary, highlighting changes made since the April AC in the 1st table and in Appendix 2. DF noted that movements related largely to reclassifications, also noting that the AOB item from the previous AC, PFI lifecycle, was now included in the figures. RMu asked whether the true bottom line was £56m or £31m. TJ replied that it was £31m. DF added that the structure of the SOCI was mandated down to the total surplus or deficit for the year. KM asked if there was freedom over the items disclosed in the box below the SOCI disclosure. DF noted this had been reviewed by Deloitte. KM asked what the purpose of the disclosure was. DF noted that this was to show the position reported to management. RMu asked if £31m was the position reported to management, TJ confirmed it was. RMu noted that the box reconciled the I&E outturn to the management accounts. TJ suggested moving the note describing this above the box. HB asked if a covering statement could be added. AH replied that it was difficult to move from the prescribed format of the SOCI. 6 Internal Audit 6a Internal Audit Progress Report PG presented the Internal Audit Progress Report, noting that the year had been finished some way short of the plan, but that all issues had been resolved for audits materially impacting on the end of year opinion. PG added that one audit, Duty of Candour, had moved back towards reasonable assurance from a previous concern that a limited

6
Matters Covered
assurance may be issued. PG added that the RTT 18 weeks audit had not been finalised in time for inclusion in the report, but noted that the opinion would be limited assurance, with similar issues identified to those noted by Deloitte in the Quality Account review. PL described the RTT audit in more detail, noting that a wide sample had been reviewed, covering four key areas, with one area being found to have a particularly high level of non-compliance. PL noted that no patient care implications had been identified from these instances of non-compliance. Overall, PL noted that as non-compliance was focussed in one area and that the impact on patient care was low, the opinion had been balanced between reasonable and limited assurance. PL added that as the review had been asked to focus on compliance with reporting requirements, the opinion overall had to be given as limited. RN commented that much of the action plan in response would be focussed on education and training. PL noted that there would have been an expectation that internal monitoring and validation would have picked up more of the problems. RM asked if any of the reports not yet seen would have limited assurance. PG replied that they would all be reasonable assurance, adding that for the two audits where draft reports were not yet available there was no expectation of any major issues from the fieldwork completed. PG added that these two audits were Clinical Pathways and Hospital at Home. PG noted that there would be nothing requiring additional disclosure in the AGS. PG noted that there were common themes emerging from the audit work of data quality and consistency, where in some areas processes were in place but were not being followed. PL added that some Trusts did more Quality Account specific review work earlier in the year to help with highlighting problems. RM noted that SK had requested the inclusion of RTT on the audit plan to assist with this. PG highlighted the four audits which had been finalised since the last report, two with reasonable assurance and two with limited assurance. KM asked about the Readmissions audit, noting that it appeared only one Clinical Board had been responsive to the recommendations. PL replied that the recommendations on this audit were the least developed of the four audits presented, and that more feedback on the recommendations was expected. KM asked if this was really a resource issue. PG replied that while impractical recommendations were undesirable, not enough resources was not always a sufficient response. PG added that the reporting was based on what was felt to be reasonable, and that testing and revisiting outcomes of recommendations would be required. RM asked who the overall lead for the audit was. PL replied that this was part of the problem, with an overall lead from Medicine Board who had been less involved than expected in the audit. TJ commented that a single lead was necessary at the planning stage. PL replied that this audit did have a single named contact but that issues had still been experienced. RM suggested that this should have been issued to EB for resolution. RN added that this should have been escalated through the appropriate line management channels. TR suggested that

7
Matters Covered
individual emails should be sent to audit owners when the plan is circulated, outlining the escalation process. TR agreed to do this. RM asked if there were any questions on the Discharge audit. PL noted that there was a good system available, ADDIT, which had not yet been fully rolled out with some areas keeping manual spreadsheets instead. PG added that this was leading to potential duplication of work. PL noted that there was a high level of confidence this issue would be resolved. RM asked about the workforce (sickness management) audit, and queried what the advantage of the Bradford score would be. PL replied that the current process was quite free form, with some people unaware of the return to work process, and some people not responding to the audit query. PL added that there was not a consistently applied framework, and that absence wasn’t managed as it would be in the private sector. PL further added that many organisations, including a number of Trusts, already used the Bradford factor to highlight patterns of repeated absence. HB expressed amazement that something similar was not in use by the Trust. PL noted that the recommendation had initially been resisted by HR, and that the results can sometimes be counter intuitive. HB commented that longer absences were often better understood and that patterns needed to be investigated. PG added that patterns in Departments could also be seen. PL noted that while the Trust was reasonable when benchmarked to other Trusts, it wouldn’t be if benchmarked more widely. PL commented that while recommendations had been made, these were unlikely to enough and that follow up audits would be required. HB suggested Ben Morrin should attend AC to discuss processes. TR asked which areas had been reviewed. PL replied that the audit had covered all areas, but that compliance on the medical side was much better than on the administrative side. RM asked about the Cancer audit, where the key findings appeared alarming, but reasonable assurance had been given. PL replied that data issues were a result of a timing mismatch between month end and week end reporting, with UCLH reporting being done over week ends, and this often being in conflict with month end dates. PL noted that most Trusts presented information as it was uploaded, but that audit responses had been with validated data a month in arrears. RM confirmed that the Board saw unvalidated data. PG added that in some organisations performance reporting was linked to a data quality rating to prevent Board misunderstanding. RM noted that page 25 suggested that data input was inaccurate, but the report said otherwise. PL responded that the testing was on revalidated data, not the data presented to the Board. PG acknowledged that the use of the word “markedly” in the Executive Summary overstated the level of concern. RN stated that the Board would continue to review unvalidated data to avoid delay in seeing the data. TJ added that Board reporting was in month, but performance reporting was on historical validated data.

8
Matters Covered
ACTION – BM to attend a future AC to discuss absence management audit and progress on implementing recommendations. ACTION – TR to co-ordinate sending emails to individual audit owners when audit plan is finalised. 6b Internal Audit Annual Report and Head of Internal Audit Opinion PG introduced the Internal Audit annual report and Head of Internal Audit Opinion (HIAO). HB noted that there was different wording on the HIAO on pages 1 and 6 and that the wording on page 6 was better. PG confirmed that the opinion was reasonable assurance, and that the correct wording had been used in the AGS. RM highlighted use of the word interim on pages 5 and 6. PG apologised and confirmed that the report was final, and agreed to immediately reissue a corrected version with the word removed. HB noted that only 4% of audits were completed in the time allocation. PL confirmed that there had been a lot of slippage against the plan which specified audit time. 7 Review of External Audit Engagement DF confirmed that no non-audit services had been procured from Deloitte in the financial year 2015-16. 8 Recommendation of Accounts to the Board RM asked if AC recommended the Accounts to the Board. AC members confirmed that they did and this was agreed.
Date of Next Meeting 9am, Tuesday 19th July 2016, Chairman/CEO Meeting Room , 2nd floor central, 250 Euston Road