blood pressure goals for diabetic patients over 60...
TRANSCRIPT

Blood Pressure Goals for Diabetic Patients Over 60 Years of Age: Is It Time They Earned Some Slack?
Ashley Marshall, PharmD PGY-1 Pharmacy Resident
South Texas Veterans Health Care System, San Antonio, Texas Division of Pharmacotherapy, The University of Texas at Austin College of Pharmacy
Pharmacotherapy Education and Research Center The University of Texas Health Science Center at San Antonio
January 30, 2015
Objectives:
1. Describe the pathophysiology and risk factors associated with hypertension in diabeticpatients
2. Compare the benefits and precautions in treating elevated blood pressures in the elderly3. Review the evidence supporting current guideline blood pressure goal recommendations in
the elderly4. Formulate a recommendation regarding blood pressure goals in elderly diabetics based on
evaluation of published literature

A. Marshall 1
9.1
24.4
37.7
52
63.9
72.1
6.7
17.6
34
52
70.8
80.1
0
10
20
30
40
50
60
70
80
90
20-34 35-44 45-54 55-64 65-74 ≥75
Pe
rce
nta
ge
(%
)
Age (years)
Men
Women
BACKGROUND
I. Hypertension (HTN)1 A. Epidemiology
i. Affects approximately 77.9 million adults in the United Statesii. One in three adults will develop HTN in their lifetime
iii. Estimated health care cost in 2009 was $51.0 billioniv. Prevalence increases with age
a. 18-39 years: 6.8%b. 40-59 years: 30.4%c. 60 years: 66.7%
v. Differences in sexa. <45 years: men>womenb. 45 to 64 years: men=womenc. 65 years: women>men
Figure 1. Percentage of Patients with Hypertension1
B. What is HTN?2-3 i. Definition
a. Systolic blood pressure (SBP) ≥140 mmHgb. Diastolic blood pressure (DBP) ≥90 mmHg
ii. Blood Pressure (BP)=Cardiac Output (CO) x Total Peripheral Resistance (TPR)a. CO=Heart Rate x Stroke Volumeb. ↑CO↑SBPc. ↑TPR↑DBP
iii. Causesa. Primary Hypertensionb. Secondary Hypertension
1. Chronic kidney disease2. Cushing syndrome3. Parathyroid/thyroid disease4. Pheochromocytoma5. Primary aldosteronism6. Medications
A. Marshall 2
iv. Diagnosis a. Mean of two or more seated readings b. Consisting of two or more separate appointments
v. Isolated Systolic Hypertension a. Defined as SBP >140 mmHg and DBP <90 mmHg b. Present in >25% of those ≥80 years of age c. Caused by decrease in elasticity of arterial wall
Table 1. Classification4
Category SBP, mmHg DBP, mmHg
Normal < 120 < 80
Pre-hypertension 120-139 80-89
Stage I Hypertension 140-159 90-99
Stage II Hypertension 160 100
C. Pathophysiology2
i. Renin-angiotensin-aldosterone system (RAAS) a. Increase release of renin from juxtaglomerular cells in kidney b. Renin catalyzes angiotensinogen to angiotensin I c. Angiotensin-converting enzyme (ACE) converts angiotensin I to
angiotensin II (ATII) d. ATII is a potent vasoconstrictor ↑TPR
ii. Aldosterone a. ATII promotes aldosterone synthesis and release b. Increase sodium and water retention ↑blood volume c. Promotes tissue remodeling and vascular dysfunction
iii. Sympathetic Nervous System (SNS) activation a. ↑TPR b. ↑HR c. ↑Heart contractility ↑CO
D. Risk factors for developing HTN1
i. Age
ii. Ethnicity a. Highest prevalence in blacks, particularly black females b. Blacks develop higher blood pressures earlier in life
iii. Family history of hypertension and genetic factors iv. Lower education and socioeconomic status v. Overweight/obese
vi. Lower physical activity vii. Tobacco use
viii. Psychosocial stressors ix. Sleep apnea x. Dietary factors
a. Dietary fats

A. Marshall 3
b. Higher sodium intake c. Lower potassium intake d. Excessive alcohol intake
E. Complications from untreated HTN1 i. Myocardial infarction (MI)
ii. Stroke iii. Chronic kidney disease (CKD) iv. Heart failure (HF) v. Retinopathy
vi. Death a. Primary or contributing cause of death in over 348,000 patients b. On average, total life expectancy ↓ by 5 years
vii. Benefits seen with even small reduction of 5mmHg in SBP5 a. Reduction in total cardiovascular (CV) risk: 20% b. Reduction in stroke: 30% c. Reduction in MI: 25%
II. Diabetes Mellitus (DM)1,6
A. Definition i. Hemoglobin A1c 6.5%
ii. Fasting plasma glucose 126 mg/dL iii. 2-hour plasma glucose 200 mg/dL during an oral glucose tolerance test iv. A random plasma glucose 200 mg/dL with symptoms of hyperglycemia
a. Polyuria b. Polydipsia c. Polyphagia
v. If hyperglycemia not absolute, testing should be repeated to confirm results B. Epidemiology
i. Approximately 29 million with DM a. Nine percent of total population
b. Twenty-seven percent of adults 65 years of age c. Men 13.6% vs women 11.2%
ii. Over eight million with undiagnosed DM iii. Over 87 million with prediabetes
C. Pathophysiology i. Insulin resistance
a. Inability to metabolize glucose properly b. Potentiated by obesity
ii. Impaired insulin secretion a. Insufficient insulin production and release from beta-cells in pancreas b. Most patients with 50% loss of beta-cell function at diagnosis
D. Risk factors of DM i. On average, total life expectancy ↓ by six years
ii. Macrovascular a. Coronary heart disease (CHD)
1. Over 68% of deaths in diabetics >65 years of age 2. Two to four times higher than adults without diabetes
b. Cerebrovascular events c. Peripheral artery disease
A. Marshall 4
iii. Microvasculara. Nephropathyb. Retinopathyc. Neuropathy
BENEFIT OF BP TREATMENT
I. DM and HTN6-7 A. Prevalence
i. HTN present in 75-85% of patients with DMii. Higher risk due to overlapping complications
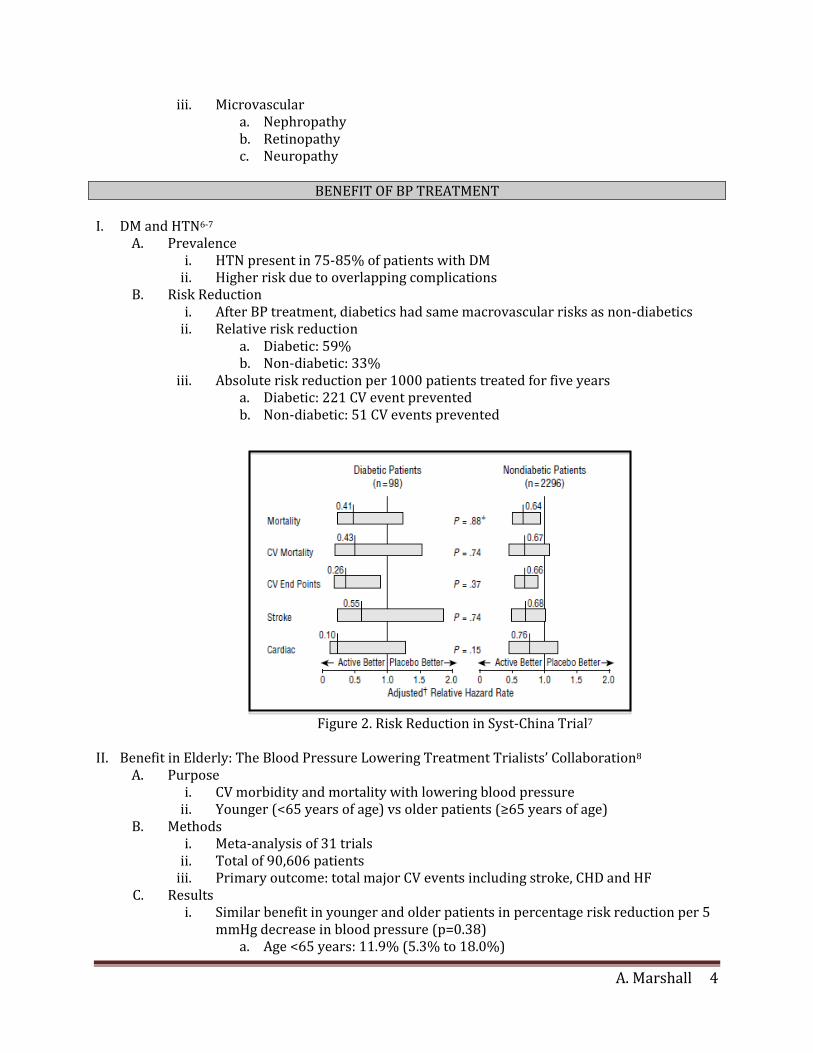
B. Risk Reduction i. After BP treatment, diabetics had same macrovascular risks as non-diabetics
ii. Relative risk reductiona. Diabetic: 59%b. Non-diabetic: 33%
iii. Absolute risk reduction per 1000 patients treated for five yearsa. Diabetic: 221 CV event preventedb. Non-diabetic: 51 CV events prevented
Figure 2. Risk Reduction in Syst-China Trial7
II. Benefit in Elderly: The Blood Pressure Lowering Treatment Trialists’ Collaboration8
A. Purpose i. CV morbidity and mortality with lowering blood pressure
ii. Younger (<65 years of age) vs older patients (≥65 years of age)B. Methods
i. Meta-analysis of 31 trialsii. Total of 90,606 patients
iii. Primary outcome: total major CV events including stroke, CHD and HFC. Results
i. Similar benefit in younger and older patients in percentage risk reduction per 5mmHg decrease in blood pressure (p=0.38)
a. Age <65 years: 11.9% (5.3% to 18.0%)
A. Marshall 5
b. Age ≥65 years: 9.1% (3.6% to 14.3%)ii. No difference in effect of different medication classes between age groups
D. Conclusion i. Benefit of treating hypertension is present regardless of age
ii. Similar percentage risk reduction but absolute risk reduction increases as ageincrease
III. Which is more important? SBP vs. DBP5
A. Increase in SBP correlated with increase in mortality i. For every 10 mmHg increase, ~10% increase in stroke, CV events and death, and
all-cause mortalityii. Coronary events not significant
B. Relationship between DBP and mortality not significant i. Inversely correlated
ii. Increase in DBP trended towards decrease in all-cause (p=0.05) and CV deaths(p=0.08)
C. Conclusion i. Lowering of SBP most associated with decreased mortality and stroke, but not
coronary eventsii. Greatest absolute benefit seen in males, age ≥70 years, and prior CV events
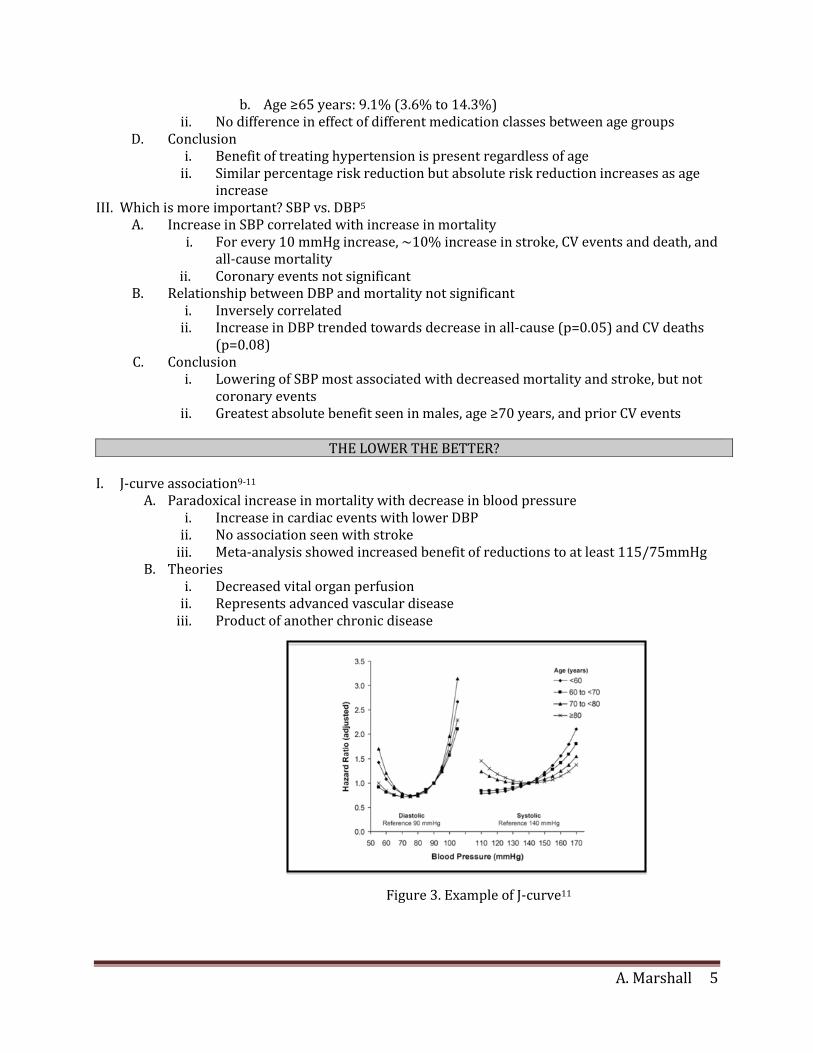
I. J-curve association9-11 A. Paradoxical increase in mortality with decrease in blood pressure
i. Increase in cardiac events with lower DBPii. No association seen with stroke
iii. Meta-analysis showed increased benefit of reductions to at least 115/75mmHgB. Theories
i. Decreased vital organ perfusionii. Represents advanced vascular disease
iii. Product of another chronic disease
Figure 3. Example of J-curve11
THE LOWER THE BETTER?

A. Marshall 6
II. Falls12 A. Pathophysiology
i. Age related inability to compensate to maintain adequate blood perfusion to brain with change of position
ii. Further impairment by prolonged CV disease B. Incidence
i. Approximately 33% of those ≥65 years ii. Rises to 50% at ≥85 years
C. Hip fractures i. Mortality
a. In first year from home: 33% b. In first three months from nursing home: 33% c. In first year from nursing home: 50%
ii. Survivors: 66% have decreased mobility and 50% have chronic pain iii. Emotional iv. Recent meta-analysis showed no increase in falls with anti-hypertensives13
a. Decreased risk with prolonged treatment b. Increased risk with initiation
III. Polypharmacy14-15 A. Definition
i. Any medication without a clinical indication ii. Estimated that 58.6% take at least one unnecessary medication
iii. Generally considered five or more medications a. Over 37% of men and 36% of women aged 75+ b. Almost 46% of those ≥65 years of age take more than six unique
medications yearly B. Consequences
i. Increase of 30% in healthcare cost ii. Increased adverse events
a. Over four million medical visits related to adverse event reported in 2005
b. Incidence in elderly: 35% in outpatient and 40% inpatient c. Increase of 88% in risk of adverse event with five or more medications
iii. Drug interactions iv. Medication non-adherence v. Diminished functional status/cognitive impairment
a. Five or more medications: 22% b. Ten or more medications: 54%
A. Marshall 7
WHAT IS THE CURRENT EVIDENCE?
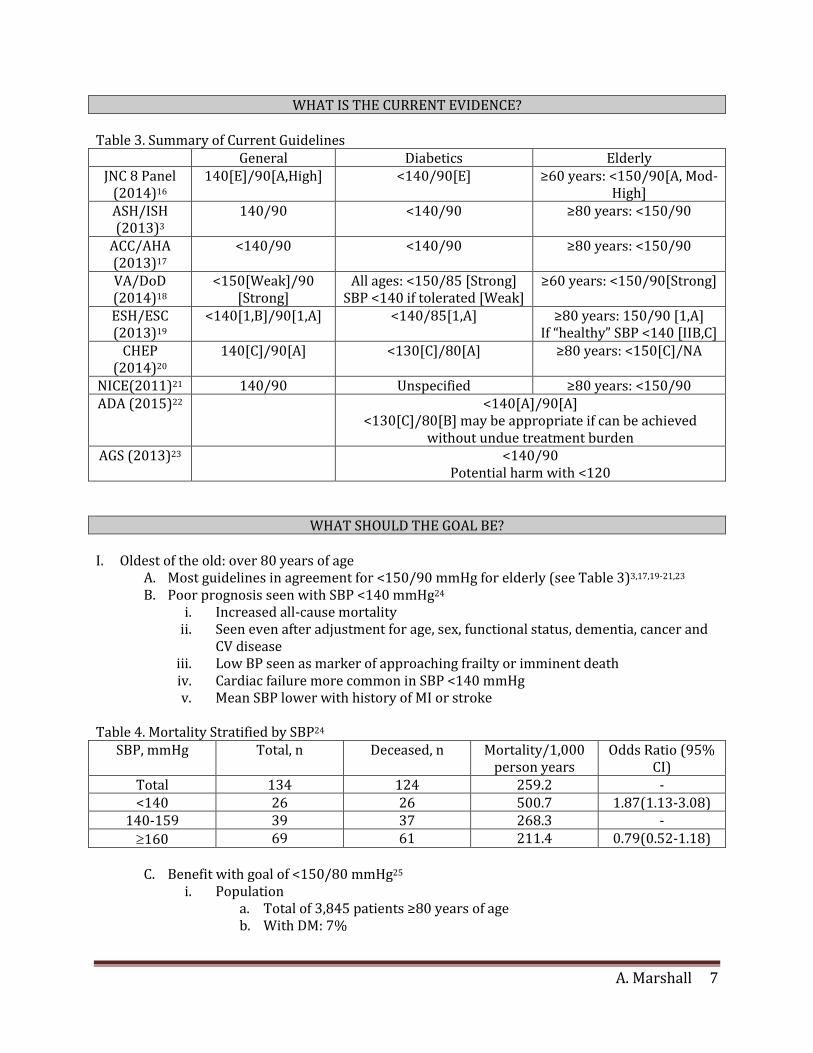
Table 3. Summary of Current Guidelines General Diabetics Elderly
JNC 8 Panel (2014)16
140[E]/90[A,High] <140/90[E] ≥60 years: <150/90[A, Mod-High]
ASH/ISH (2013)3
140/90 <140/90 ≥80 years: <150/90
ACC/AHA (2013)17
<140/90 <140/90 ≥80 years: <150/90
VA/DoD (2014)18
<150[Weak]/90 [Strong]
All ages: <150/85 [Strong] SBP <140 if tolerated [Weak]
≥60 years: <150/90[Strong]
ESH/ESC (2013)19
<140[1,B]/90[1,A] <140/85[1,A] ≥80 years: 150/90 [1,A] If “healthy” SBP <140 [IIB,C]
CHEP (2014)20
140[C]/90[A] <130[C]/80[A] ≥80 years: <150[C]/NA
NICE(2011)21 140/90 Unspecified ≥80 years: <150/90 ADA (2015)22 <140[A]/90[A]
<130[C]/80[B] may be appropriate if can be achieved without undue treatment burden
AGS (2013)23 <140/90 Potential harm with <120
WHAT SHOULD THE GOAL BE?
I. Oldest of the old: over 80 years of age A. Most guidelines in agreement for <150/90 mmHg for elderly (see Table 3)3,17,19-21,23 B. Poor prognosis seen with SBP <140 mmHg24
i. Increased all-cause mortalityii. Seen even after adjustment for age, sex, functional status, dementia, cancer and
CV diseaseiii. Low BP seen as marker of approaching frailty or imminent deathiv. Cardiac failure more common in SBP <140 mmHgv. Mean SBP lower with history of MI or stroke
Table 4. Mortality Stratified by SBP24 SBP, mmHg Total, n Deceased, n Mortality/1,000
person years Odds Ratio (95%
CI) Total 134 124 259.2 - <140 26 26 500.7 1.87(1.13-3.08)
140-159 39 37 268.3 -
160 69 61 211.4 0.79(0.52-1.18)
C. Benefit with goal of <150/80 mmHg25 i. Population
a. Total of 3,845 patients ≥80 years of ageb. With DM: 7%
A. Marshall 8
ii. Intervention a. Indapamide ± perindopril vs placebo b. Goal BP <150/80 mmHg achieved in 20% of placebo and 48% active
treatment iii. Results
a. Statistically significant decrease in overall mortality and HF b. Non-statistically significant decrease in stroke, death from CV cause and
death from stroke D. Changes as we age12,26
i. Change in CV hazard ratio a. For age >65 increases with SBP >140 b. For age >75 increases with SBP >150
ii. Stroke reduction decreases with age a. Aged 50-59: ↓62% b. Aged 80-89: ↓33%
E. Clinical Recommendations i. Goal SBP <150 mmHg
a. Due to frailty and limited lifespan, recommend regardless of presence of DM
b. Clear CV benefit seen in HYVET trial c. SBP <140 mmHg may be associated with increased mortality d. Desire to avoid initiation of medications due to risk of falls
ii. Goal DBP <90 mmHg a. Excluded from HOT trial b. No current evidence to support DBP <80 mmHg
iii. May consider SBP <140 mmHg a. Can be tolerated with no adverse events b. No fall risk c. High stroke risk
II. The middle men: 60-79 years A. Inconsistent
i. JNC 8 and VA/DoD raised goal to 150/90 mmHg for those 60 years ii. Remaining recommendations remain consistent with those <60 years
iii. Not all guidelines differentiate if age or DM take priority in BP goal B. JNC 8 dispute27
i. Consensus statement from an expert panel ii. Recommendation to raise goal to 150/90 mmHg not unanimous
iii. Minority view a. Strong support that SBP >150 mmHg has increased CV risk b. Insufficient evidence to raise BP goal from present 140 mmHg
C. Remaining thoughts/questions i. Not all answers may be found in randomized controlled trials
ii. Are we too strict with our blood pressure treatment in elderly diabetics? iii. Is age or presence of DM primary determinant of goal?

A. Marshall 9
LITERATURE REVIEW
Ogihara T, et al. Target blood pressure for treatment of isolated systolic hypertension in the elderly: valsartan in elderly isolated systolic hypertension study (VALISH). Hypertension. 2010;56:196-202.28
Purpose To determine if strict BP control (<140 mmHg) is superior to moderate BP control (140 mmHg to 149 mmHg) in reducing CV morbidity and mortality
Design Multicenter, parallel-group, prospective, randomized, open-label, blinded end point study conducted in Japan
Population Inclusion 70-84 years of age with primary
isolated systolic hypertension (SBP>160 mmHg and DBP <90 mmHg)
Exclusion SBP 200 mmHg or DBP 90 mmHg Stroke or MI in prior 6 months Severe HF (NYHA III and IV) Atrial fibrillation Renal dysfunction (SCr 2 mg/dl)
Outcomes Primary: composite of the following CV events: sudden death, fatal or nonfatalstroke, fatal or nonfatal MI, HF or other CV related death, hospitalization for CVdisease and renal dysfunction
Secondary: each component of primary end point, total mortality, new onset orexacerbation of angina, and adverse events
Methods Patients randomized to achieve SBP goal of either <140 or 140 mmHg to 149mmHg
Valsartan titrated to ≤160mg was initial therapy followed by any additionalanti-hypertensive therapy necessary to achieve BP target
Patients visited clinic every 3 months for minimum of 2 years Investigators asked to complete case report forms to document endpoints
Results Baseline characteristics not significantly different except for smoker ratio(strict: 21% vs moderate: 17.4%)
Median follow-up 3.07 years
Strict (N=1545) Moderate (N=1534) p-value (<0.05)
Mean BP, mmHg 136.6/74.8 142.0/76.5 Primary endpoint 47(3.04%) 52(3.39%) 0.383
All-cause mortality 24(1.55%) 30(1.96%) 0.78 CV death 11(0.71%) 11(0.72%) 0.97
Fatal and non-fatal stroke 16(1.04%) 23(1.50%) 0.68 Fatal and non-fatal MI 5(0.32%) 4(0.26%) 1.23
Renal insufficiency 5(0.32%) 2(0.13%) 2.45 Diabetes present Primary endpoint
211 8.06%
188 7.45% 0.737
Adverse Events* 18.2% 17.9% 0.851 *Most were gastrointestional or respiratory symptoms
Conclusion Strict BP control may not offer any additional CV event benefit over moderatecontrol
Blood pressure targets of <140 mmHg are safely achievable in relatively
healthy patients 70 years of age
A. Marshall 10
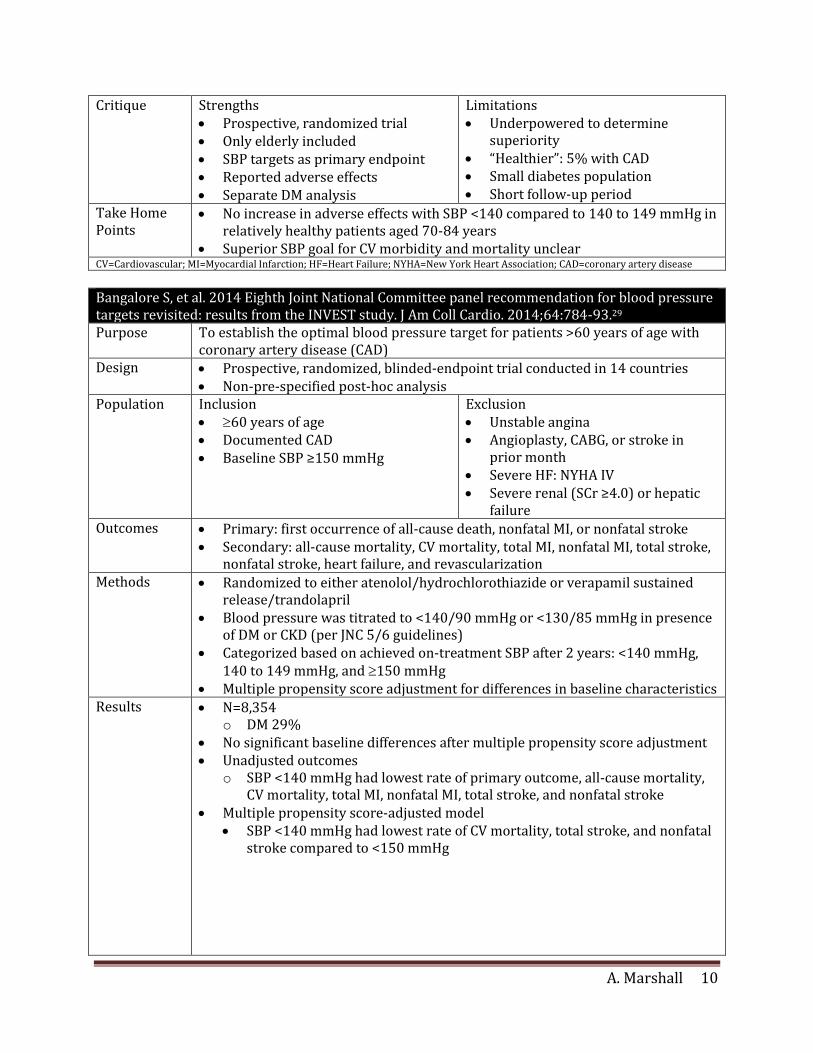
Critique Strengths Prospective, randomized trial Only elderly included SBP targets as primary endpoint Reported adverse effects Separate DM analysis
Limitations Underpowered to determine
superiority “Healthier”: 5% with CAD Small diabetes population Short follow-up period
Take Home Points
No increase in adverse effects with SBP <140 compared to 140 to 149 mmHg in relatively healthy patients aged 70-84 years
Superior SBP goal for CV morbidity and mortality unclear CV=Cardiovascular; MI=Myocardial Infarction; HF=Heart Failure; NYHA=New York Heart Association; CAD=coronary artery disease
Bangalore S, et al. 2014 Eighth Joint National Committee panel recommendation for blood pressure targets revisited: results from the INVEST study. J Am Coll Cardio. 2014;64:784-93.29
Purpose To establish the optimal blood pressure target for patients >60 years of age with coronary artery disease (CAD)
Design Prospective, randomized, blinded-endpoint trial conducted in 14 countries Non-pre-specified post-hoc analysis
Population Inclusion 60 years of age Documented CAD Baseline SBP ≥150 mmHg
Exclusion Unstable angina Angioplasty, CABG, or stroke in
prior month Severe HF: NYHA IV Severe renal (SCr ≥4.0) or hepatic
failure Outcomes Primary: first occurrence of all-cause death, nonfatal MI, or nonfatal stroke
Secondary: all-cause mortality, CV mortality, total MI, nonfatal MI, total stroke, nonfatal stroke, heart failure, and revascularization
Methods Randomized to either atenolol/hydrochlorothiazide or verapamil sustained release/trandolapril
Blood pressure was titrated to <140/90 mmHg or <130/85 mmHg in presence of DM or CKD (per JNC 5/6 guidelines)
Categorized based on achieved on-treatment SBP after 2 years: <140 mmHg, 140 to 149 mmHg, and 150 mmHg
Multiple propensity score adjustment for differences in baseline characteristics Results
N=8,354 o DM 29%
No significant baseline differences after multiple propensity score adjustment Unadjusted outcomes
o SBP <140 mmHg had lowest rate of primary outcome, all-cause mortality, CV mortality, total MI, nonfatal MI, total stroke, and nonfatal stroke
Multiple propensity score-adjusted model SBP <140 mmHg had lowest rate of CV mortality, total stroke, and nonfatal
stroke compared to <150 mmHg
A. Marshall 11
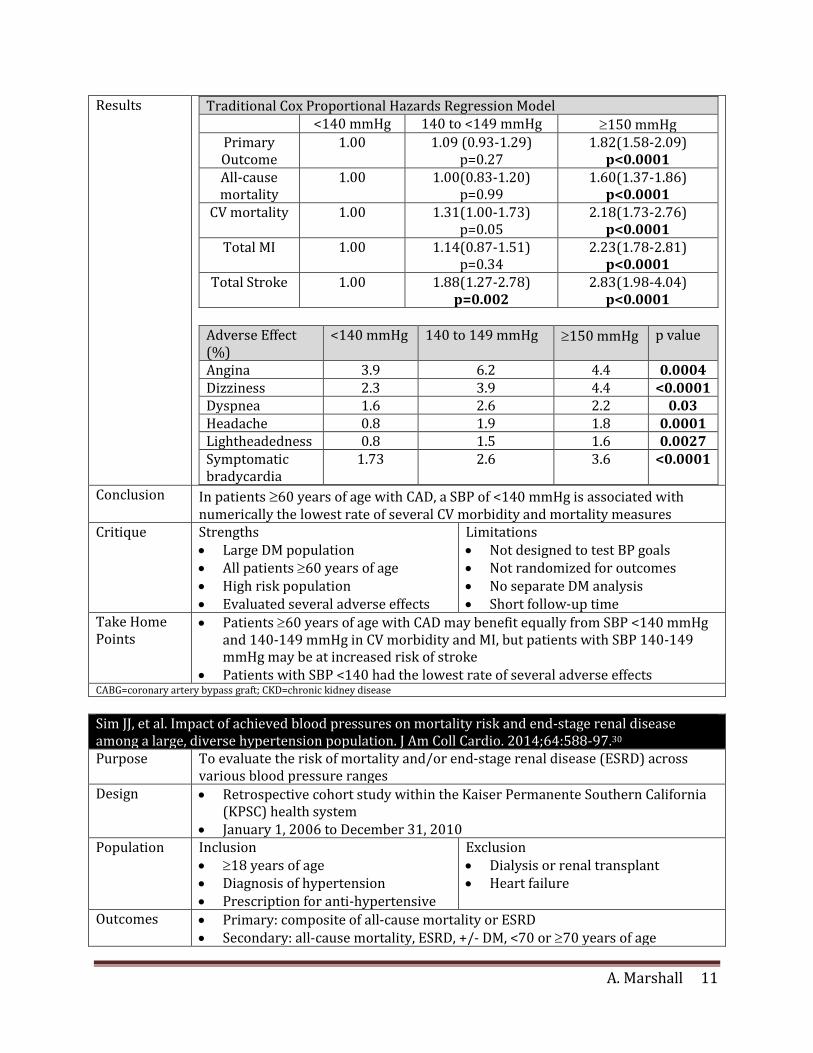
Results Traditional Cox Proportional Hazards Regression Model <140 mmHg 140 to <149 mmHg 150 mmHg
Primary Outcome
1.00 1.09 (0.93-1.29) p=0.27
1.82(1.58-2.09) p<0.0001
All-cause mortality
1.00 1.00(0.83-1.20) p=0.99
1.60(1.37-1.86) p<0.0001
CV mortality 1.00 1.31(1.00-1.73) p=0.05
2.18(1.73-2.76) p<0.0001
Total MI 1.00 1.14(0.87-1.51) p=0.34
2.23(1.78-2.81) p<0.0001
Total Stroke 1.00 1.88(1.27-2.78) p=0.002
2.83(1.98-4.04) p<0.0001
Adverse Effect (%)
<140 mmHg 140 to 149 mmHg 150 mmHg p value
Angina 3.9 6.2 4.4 0.0004 Dizziness 2.3 3.9 4.4 <0.0001 Dyspnea 1.6 2.6 2.2 0.03 Headache 0.8 1.9 1.8 0.0001 Lightheadedness 0.8 1.5 1.6 0.0027 Symptomatic bradycardia
1.73 2.6 3.6 <0.0001
Conclusion In patients 60 years of age with CAD, a SBP of <140 mmHg is associated with numerically the lowest rate of several CV morbidity and mortality measures
Critique Strengths Large DM population All patients 60 years of age High risk population Evaluated several adverse effects
Limitations Not designed to test BP goals Not randomized for outcomes No separate DM analysis Short follow-up time
Take Home Points
Patients 60 years of age with CAD may benefit equally from SBP <140 mmHg and 140-149 mmHg in CV morbidity and MI, but patients with SBP 140-149 mmHg may be at increased risk of stroke
Patients with SBP <140 had the lowest rate of several adverse effects CABG=coronary artery bypass graft; CKD=chronic kidney disease
Sim JJ, et al. Impact of achieved blood pressures on mortality risk and end-stage renal disease among a large, diverse hypertension population. J Am Coll Cardio. 2014;64:588-97.30
Purpose To evaluate the risk of mortality and/or end-stage renal disease (ESRD) across various blood pressure ranges
Design Retrospective cohort study within the Kaiser Permanente Southern California (KPSC) health system
January 1, 2006 to December 31, 2010 Population Inclusion
18 years of age Diagnosis of hypertension Prescription for anti-hypertensive
Exclusion Dialysis or renal transplant Heart failure
Outcomes Primary: composite of all-cause mortality or ESRD Secondary: all-cause mortality, ESRD, +/- DM, <70 or 70 years of age
A. Marshall 12
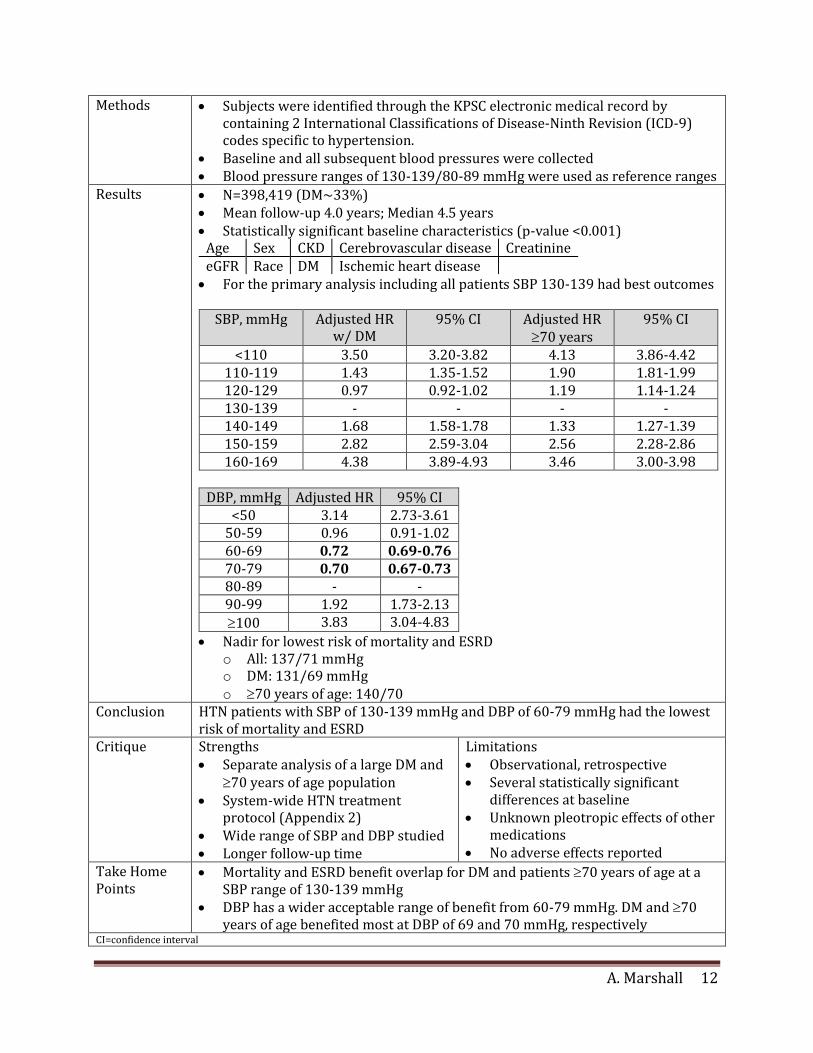
Methods Subjects were identified through the KPSC electronic medical record by containing 2 International Classifications of Disease-Ninth Revision (ICD-9) codes specific to hypertension.
Baseline and all subsequent blood pressures were collected Blood pressure ranges of 130-139/80-89 mmHg were used as reference ranges
Results N=398,419 (DM~33%) Mean follow-up 4.0 years; Median 4.5 years Statistically significant baseline characteristics (p-value <0.001)
Age Sex CKD Cerebrovascular disease Creatinine eGFR Race DM Ischemic heart disease For the primary analysis including all patients SBP 130-139 had best outcomes
SBP, mmHg Adjusted HR
w/ DM 95% CI Adjusted HR
70 years 95% CI
<110 3.50 3.20-3.82 4.13 3.86-4.42 110-119 1.43 1.35-1.52 1.90 1.81-1.99 120-129 0.97 0.92-1.02 1.19 1.14-1.24 130-139 - - - - 140-149 1.68 1.58-1.78 1.33 1.27-1.39 150-159 2.82 2.59-3.04 2.56 2.28-2.86 160-169 4.38 3.89-4.93 3.46 3.00-3.98
DBP, mmHg Adjusted HR 95% CI
<50 3.14 2.73-3.61 50-59 0.96 0.91-1.02 60-69 0.72 0.69-0.76 70-79 0.70 0.67-0.73 80-89 - - 90-99 1.92 1.73-2.13
100 3.83 3.04-4.83
Nadir for lowest risk of mortality and ESRD o All: 137/71 mmHg o DM: 131/69 mmHg o 70 years of age: 140/70
Conclusion HTN patients with SBP of 130-139 mmHg and DBP of 60-79 mmHg had the lowest risk of mortality and ESRD
Critique Strengths Separate analysis of a large DM and
70 years of age population System-wide HTN treatment
protocol (Appendix 2) Wide range of SBP and DBP studied Longer follow-up time
Limitations Observational, retrospective Several statistically significant
differences at baseline Unknown pleotropic effects of other
medications No adverse effects reported
Take Home Points
Mortality and ESRD benefit overlap for DM and patients 70 years of age at a SBP range of 130-139 mmHg
DBP has a wider acceptable range of benefit from 60-79 mmHg. DM and 70 years of age benefited most at DBP of 69 and 70 mmHg, respectively
CI=confidence interval

A. Marshall 13
Liu L, et al. The felodipine event reduction (FEVER) study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens. 2005;23:2157-72.31
Purpose To assess the incidence of cardiovascular events between the treatment blood pressures of a diuretic and calcium channel antagonist combination and diuretic monotherapy.
Design Multicenter, prospective, double-blind, randomized, placebo-controlled, parallel group trial conducted among 109 hospitals and clinics in China
Population Inclusion Aged 50-79 years SBP 210 mmHg and DBP
<115mmHg if treated SBP 160-210 mmHg or DBP 95-
115mmHg if untreated If 60 years of age, were required to
have clinical evidence or history of a CV event or presence of at least 2 CV risk factors*
If >60 years of age, required to have one event or one risk factor*
Exclusion Stroke or MI in previous 6 months Secondary HTN Unstable angina SCr >2.0 mg/dl Uncontrolled DM (fasting BG >180
mg/dl despite therapy)
Outcomes Primary: time to first fatal and nonfatal stroke Secondary: all CV events + composite of various CV outcomes, death from any
cause Methods Open label hydrochlorathiazide 12.5mg daily for 6 weeks
Randomized to: o Hydrochlorathiazide+ felodipine 5mg daily o Hydrochlorathiazide + placebo
If BP>160/95 mmHg on two consecutive visits, could receive additional HCTZ 12.5mg and any other non-calcium channel antagonist antihypertensive agent
Results Mean follow-up time: 40 months Felodipine (%)
N=4841 Placebo (%)
N=4870 HR (95% CI) p-value
BP, mmHg 137.3/82.5 142.5/84.0 Stroke 177(3.7) 251(5.2) 0.73(0.60-0.89) 0.0019
All CV events 241(5.0) 334(6.9) 0.73(0.61-0.86) 0.0002 All-cause death 112(2.3) 151(3.1) 0.69(0.54-0.89) 0.0053
CV death 73(1.5) 101(2.1) 0.67(0.48-0.91) 0.0112 Heart Failure 18(0.4) 27(0.6) 0.70(0.37-1.30) 0.2604 Renal failure 10(0.2) 8(0.16) 1.38(0.54-3.52) 0.4994
DM: ~13%(n=1241) Mean difference in BP: 4/2 mmHg Adverse events (AE)
o Felodipine group had more flushing and ankle edema o Similar incidences of dizziness, headache, fatigue and palpitations
Conclusion A decrease in BP as small as 4/2 mmHg can provide substantial decreases in risk of cardiovascular outcomes

A. Marshall 14
Critique Strengths Randomized, double-blinded Add-on therapy and other
pleotropic medications assessed Only elderly included Reported AE
Limitations Short follow up time No separate analysis of only DM
patients May not be applicable to US
population
Take Home Points
A SBP <140 mmHg was shown superior to <150 mmHg in decreasing risk of stroke,
CV events, and death in this population of patients 60 years of age that included DM patients.
*male sex, current smoking of more than one cigarette per day during at least 1 year, total serum cholesterol ≥220 mg/dl within the previous year or lipid-lowering treatment, diabetes mellitus, left ventricular hypertrophy, proteinuria, body mass index >27 kg/m2

A. Marshall 15
SUMMARY I. Limited support for SBP <140 mmHg
A. Most high level evidence trials only compared treatment <150 mmHg vs no treatment B. CV differences
i. Most studies show no difference in CV events or death ii. Majority show decrease risk of stroke
C. Adverse effects i. Little to no risk of increased adverse effects
ii. Some data to support decrease in adverse effects II. Wider acceptable DBP range
A. Limited trials with DBP goals as endpoints i. Most support for <80 mmHg is result of HOT trial
a. Mean DBP achieved 81 vs 85 mmHg b. Only significant in DM population of ~1,500 patients
ii. Analysis showed 60-79 mmHg had greatest benefit iii. Difficult to distinguish effect of SBP from DBP iv. DBP not as important for CV benefit
III. Relationship between BP and risk A. Linear for stroke risk B. U or J shaped for cardiovascular
CLINICAL RECOMMENDATIONS
I. Patients 80 years of age A. Goal <150/90 mmHg
i. Due to frailty and limited lifespan, recommend regardless of presence of DM ii. Excluded from VALISH and FEVER
iii. Increased mortality shown with >85 years iv. Less stroke benefit achieved with treatment v. Avoidance of drug initiation due to increased risk of falls
B. May consider <140/90 mmHg i. “Physically fit”
ii. High stroke risk II. Patients 60-79 years of age
A. Primary target of SBP <140 mmHg i. Most important in those at increased risk of stroke
ii. Though conflicting, may provide benefit over SBP <150 mmHg iii. Limited negative consequences seen in trials iv. If very frail, may use target of <150 mmHg
B. DBP goal uncertain i. Insufficient RCT to show <80 mmHg superior to <90 mmHg
ii. No current evidence shows one more harmful in CV events or adverse effects iii. Although not a primary endpoint, most studies achieved a DBP <80 mmHg iv. Recommend DBP goal <80 mmHg if can be reached without undue harm to
patient v. Recommend DBP goal <90 mmHg if very frail or AE present at <80 mmHg
III. Patient specific A. Patient’s preference for more or less aggressive treatment B. Values on falls vs CV benefit C. Treat based on “physiological” age instead of chronological
A. Marshall 16
REFERENCES 1. American Heart Association. Heart Disease and Stroke Statistics—2014 Update: A report from the
American Heart Association. Circulation. 2013;129:e28-e292. 2. Saseen JJ and Maclaughlin EJ. Chapter 19. Hypertension. In: DiPiro J, Talbert R, Yee G, et al. (eds):
Pharmacotherapy: A Pathophysiologic Approach. 8 e. New York, McGraw-Hill, 2011. 3. Weber MA, Schiffrin EL, White WB, et al. Clinical Practice Guidelines for the Management of
Hypertension in the Community: A Statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2013.
4. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-72.
5. Staessen JA, Gasowski, J, Wang JG, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000;355:865-72.
6. Triplitt CL and Reasner CA. Chapter 83. Diabetes Mellitus. In: DiPiro J, Talbert R, Yee G, et al. (eds): Pharmacotherapy: A Pathophysiologic Approach. 8 e. New York, McGraw-Hill, 2011.
7. Wang JG, Staeseen JA, Gong L, et al; the Systolic Hypertension in China (Syst-China) Collaborative Group. Chinese trial on isolated systolic hypertension in the elderly. Arch Intern Med. 2000;160:211-20.
8. Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomized trials. BMJ. 2008;336:1121-3.
9. Messerli FH, Mancia G, Conti R, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med. 2006;144:884-93.
10. Lewington S, Clarke R, Oizilbash N, et al. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903-13.
11. Denardo SJ, Gong Y, Nichols WW, et al. Blood pressure and outcomes in very old hypertensive coronary artery disease patients: an INVEST substudy. Am J Med. 2010;123(8):719-26.
12. Close JT. Prevention of falls in older people. Disabil Rehabil. 2005;27(18-19):1061-71. 13. Zang G. Antihypertensive drugs and the risk of fall injuries: a systematic review and meta-analysis.
Int J Med Sci.2013;41(5):1408-17. 14. Terrie YC. Understanding and managing polypharmacy in the elderly. Pharmacy Times. 2004.
Accessed at http://www.pharmacytimes.com/publications/issue/2004/2004-12/2004-12-9094 on 29 December 2014.
15. Maher RL Jr, Hanlon JT, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1): doi:10.1517/14740338.2013.827660.
16. James PA, Oparil S, Carter BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507-20.
17. Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA Guideline of the Assessment of Cardiovasclar Risk: A Report of the American college of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2013.
18. The Diagnosis and Management of Hypertension Working Group. VA/DoD Clinical Practice Guidelines for the Diagnosis and Management of Hypertension in the Primary Care Setting. 2014. Accessed at http://www.healthquality.va.gov/guidelines/CD/htn/VADoDCPGfortheManagementofHTN.pdf on 29 December 2014.
19. Mancia G, Fagard R, Narkiewicz K, et al; Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31:1281-357.
20. Canadian Hypertension Education Program. 2013 Canadian Hypertension Education Program (CHEP) Recommendations. Markham, Ontario, Canada: Hypertension Canada;2014. Accessed at http://www.hypertension.ca/en/chep on 15 December 2014.
A. Marshall 17
21. National Institute for Health and Care Excellence. Hypertension: clinical management of primary hypertension in adults. 2011. Accessed at http://www.nice.org.uk/guidance/cg127/resources/guidance-hypertension-pdf on 29 December 2014.
22. American Diabetes Association. Cardiovascular disease and risk management. Diabetes Care. 2015;38(Suppl. 1):S49-S57.
23. American Geriatric Society Expert Panel. Guidelines abstracted from the American Geriatrics Society Guidelines for improving the care of older adults with Diabetes Mellitus: 2013 Update. JAGS. 2013;61:2020-6.
24. Rastas S, Pirttila T, Viramo P, et al. Association between blood pressure and survival over 9 years in a general population aged 85 and older. J Am Geriatr Soc. 2006;54:912-8.
25. Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 ears of age or older. N Engl J Med. 2008;358:1887-98.
26. Ogihara T, Nakao K, Fukui T, et al. The optimal target blood pressure for antihypertensive treatment in Japanese elderly patients with high-risk hypertension: a subanalysis of the Candesartan Antihypertensive Survival Evaluation in Japan (CASE-J) trial. Hypertens Res. 2008;31:1595-601.
27. Wright JT Jr, Fine LJ, Lackland DT, et al. Evidence supporting a systolic blood pressure goal of less than 150 mmHg in patients aged 60 years or older: the minority view. Ann Intern Med. 2014;160:499-503.
28. Ogihara T, Saruta T, Rakugi H, et al; the Valsartan in Elderly Isolated Systolic Hypertension Study Group. Target blood pressure for treatment of isolated systolic hypertension in elderly: Valsartan in Elderly Isolated Systolic Hypertension (VALISH) study. Hypertension. 2010;56:196-202.
29. Bangalore S, Gong Y, Cooper-DeHoff RM, et al. 2014 Eighth Joint National Committee Panel recommendations for blood pressure targets revisited: results from the INVEST study. J Am Coll Cardiol. 2014;64(8):784-93.
30. Sim JJ, Shi J, Kovesdy CP, et al. Impact of achieved blood pressures on mortality risk and end-stage renal disease among a large, diverse hypertension population. J Am Coll Cardiol. 2014:64:588-97.
31. Liu L, Zhang Y, Liu G, et al; FEVER Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens. 2005;23:2157-72.
32. SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. JAMA. 1991;265:3255-64.
33. Staessen JA, Fagard R, Thijs L, et al, for the Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet 1997;350:757-64.
34. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 1998;317:703-13.
35. ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2000;283:1967-75.
36. ADVANCE Collaborative Group. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomized controlled trial. Lancet 2007;370:829-40.
37. The ACCORD Study Group. Effects of intensive blood-ressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-85.
38. Hansson L, Zanchetti A, Carruthers SG, et al; the HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomized trial. Lancet. 1998;351:1755-62.

A. Marshall 18
Appendix A. Summary of Trials with Elderly Diabetics Trial Participants Intervention Outcomes Take Away Supporting SBP <150 mmHg SHEP32 (1991) N=4736
(12.3% DM) Age ≥60 years
If SBP >180, goal: SBP <160; If SBP 160-179, goal SBP ↓20 mmHg vs placebo
Mean achieved BP: 143/68 vs 155/72 ↓36% stroke (p=0.0003)
BP <145/70 improved outcomes compared to <155/75
Syst-Eur33 (1997) N=4695 (10.5% DM) Age ≥60 years
SBP <150 mmHg vs placebo ↓42% stroke (p=0.0003) ↓26% all cardiac endpoints (p=0.03)
Treating to SBP <150 provides CV protection
Syst-China7 (2000) N=2394 (4.1% DM) Age ≥60 years
SBP <150 mmHg vs placebo ↓38% stroke
↓37% CV events
↓39% mortality
Treating to SBP <150 provides CV protection
UKPDS 3834 (1998) N=1148 (100% DM) Age: 25-65 years
<150/85 mmHg vs. <180/105 mmHg
Mean achieved BP: 144/82 vs 154/87 ↓32% mortality (p=0.019) ↓21% MI (NS) ↓44% stroke (p=0.013) ↓37% microvascular (p=0.0092)
Mean BP of <145/85 superior to <155/90
Supporting SBP <140 mmHg ALLHAT35 (2000) N=24316
(DM=43%) Age >55 years
Doxazosin vs chlorthalidone
Mean achieved BP: DM: 137/75 vs 136/75 nonDM: 137/77 vs 135/77
BP reduction to <140/80 had CV benefit
ADVANCE36 (2007)
N=11,140 DM=100% Age >55
Perindopril+indapamide vs placebo
Achieved BP: 139.4/78.8 ↓9% macrovascular+ microvascular (p=0.04) ↓18% CV mortality (p=0.03)
BP of <140/80 showed CV benefit compared to placebo
ACCORD37
(2010) N=4733 DM=100% Age >40 years
SBP <120 mmHg vs <140 mmHg
Mean SBP achieved: 119.3 vs 133. CV events: 1.87% vs 2.9% (NS) All-cause mortality: 1.28% vs 1.19% (NS) Stroke: 0.32% vs 0.53% (p=0.01) Adverse effects: 3.3% vs 1.3% (p<0.001)
No additional CV benefit, but decreased stroke in <120 vs <140 ↑AE with goal 120
Supporting DBP goals HOT38
(1998) N=18,790 DM=1,501 (8%) Age 50-80 years
DBP goals of <90 vs <85 vs <80 mmHg
Achieved DBP: 85.2 vs 83.2 vs 81.1 DM: ↓51% in CV events in <80 vs <90 (p=0.005)
Primary trial cited to support DBP <80 mmHg, but most patients did not reach goal.
DM=Diabetes Mellitus; NS=Nonsignificant ; BP=blood pressure, SBP=systolic blood pressure; DBP=diastolic blood pressure; AE=adverse events

A. Marshall 19
Appendix B. Kaiser Permanente Southern California Hypertension Algorthim29