bleeding and transfusion in the operating room - sabm · bleeding and transfusion in the operating...
TRANSCRIPT

1
Bleeding and Transfusion in the Operating Room
Richard K. Spence MD, MHA, FACS

2
New Rationale: John Bell, Textbook of Surgery, 1812
“ Is not this fear of hemorrhage uppermost in the minds of young surgeons? Were this one danger removed, he would go forward in his profession, almost without fear.”

3
TOPICS
BLEEDING IN THE OR - HOW OFTEN, WHICH PATIENTS, WHY ?
TREATMENT IS TRANSFUSION THE ANSWER?
RISK/BENEFIT EQUATION OF TRANSFUSION
PREVENTION AND REDUCTION OF TRANSFUSION

4
INCIDENCE OF HEMORRHAGE IN THE OPERATING ROOM
Japanese Society of Anesthesiologists (JSA) annual survey (2003) - 1,367,790 pts from 782 hospitals Life-threatening hemorrhage (LTH) reported in
1,011 pts = 0.074% Irita K et al. Masui, 2005;54(1):77-86
Hemorrhagic complications in elective surgery - COMPARE™ data: N = 130,641
Incidence = 960/130,641 = 0.075% Data on file, COMPARE™, Haemonetics®

5
SOURCES OF LIFE-THREATENING HEMORRHAGE IN THE OPERATING ROOM
Main sources of bleeding were abdominal aorta (15.4%)
thoracic aorta (14%)
liver (12.6%)
intracranial (8.2%)
pelvic organs (8%)
coeliac/mesenteric artery (7.8%) and
lung (7.1%). Irita K et al. Masui, 2005;54(1):77-86

6
WHY DO PATIENTS BLEED IN THE OPERATING ROOM?
1. “IT’S A PART OF THE PROCEDURE.”
2. INADVERTENT INJURY: THE “OOPS” FACTOR?
3. MICROVASCULAR BLEEDING
7
HIGH-RISK PROCEDURES FOR TRANSFUSION FROM THE LITERATURE
Cardiac Surgery Shehata et al, Vox Sang,
2007
Head & Neck for Squamous Ca
Jecker et al, Hno, 2005
Liver transplantation Bertelli et al, Transplant
Proc, 2005
Joint replacement Nelson C et al, Clin Orthop,
1998
Spine Vitale et al, Spine J, 2002
Abdominal surgery in cirrhotic pt Garrison et al, Ann Surg,
1984
AAA repair Healy et al, Ir J Mede Sci,
2007
TAA repair Conrad et al, Ann Thorac
Surg, 2007
C-section for placental abnormalities Imberti et al, Acta Anaesthesiol
Belg, 1990

8
Hemorrhagic Complications: Incidence by Procedure Group
0
0.5
1
1.5
2
2.5
% PTS
% PTS 2.3 2.1 2 2 1.8 1.8 1.7 1.5 1.5 1.5 1.2 1.2 0.8
ENDO MALE GEN ENT NEURO GU HEMLYM\P MS RESP FEM GEN CVS GI SKIN BREAST
N = 130,641 pts. P 0.0001 across groups

9
Hemorrhagic Complications: Incidence by Specific Procedure - Top 15
0
2
4
6
8
10
12
14
16
18
% PTS
% PTS 16.7 12.5 11.1 11.1 9.1 6.4 5.3 4.7 4.6 4.5 4.1 3.7 3.6 2.8 2
ENDO
BILIARYVAD
PANC
CYSTCBDE
PULM
VALVE
LIVER
TXP
TOTAL
PANCTAH AAA
EXC LGE
INTTAA
DISTAL
PANC
ABD
VASCMVR AVR
N = 130,641 pts. P <.0001 across groups

10
THE “OOPS” FACTOR?
629 injuries trocar injuries from 1993 - 1996. 408 (65%) vascular, primarily aorta and vena cava.
Bhoyrul S et al. J Am Coll Surg.2001;192(6):677-83
FDA report of 1384 trocar injuries cited surgical technique, device problems and patient characteristics as contributing factors.
Fuller J et al. J Minim Invasive Gynecol, 2005;12(4):302-7
“Approximately 75% to 90% of intraoperative and early postoperative bleeding is due to technical factors.”
Marietta M et al.Transplant Proc.2006;38(3):812-4

11
THE “OOPS” FACTOR?
Up to 40% of all splenectomies are done for iatrogenic injury. Most common with left hemicolectomy, open anti-reflux procedures and left nephrectomy.
Cassart K & Munro A. J R Coll Surg Edinb,2002;47(6):731-41
7/404 (1.7%) vascular injuries during major renal and adrenal retroperitoneoscopic surgery
Meraney AM et al. J Urol. 2002;168(5):1941-4
54/480 (11% ) spine patients with intraoperative vascular injury. 45/54 (83%) minor. 83% involved exposure of L4-5.
Hamden AD et al. J Vasc Surg, 2008;48(3):650-4

12
LIFE-THREATENING HEMORRHAGE IN THE OPERATING ROOM: ASSOCIATED FACTORS
Factors associated with LTH Delayed decision making (15.6%)
Delayed admission to OR for surgery (16.3%)
Anesthesia management problem (28.1%)
Delayed arrival of blood products (25.5%)
Surgical management problem (16.3%). Irita K et al. Masui, 2005;54(1):77-86

13
High-Risk Surgery in the JW
Cardiovascular surgery in Jehovah's Witnesses. Report of 542 operations without blood transfusion
Ott DA & Cooley DA, JAMA,1977;238(17):1256-8
Major gynecologic and obstetric surgery in Jehovah's Witnesses (N = 165)
Bonakdar MI et al. Obstet Gynecol, 1982; 60(5):587-90
Total hip arthroplasty in Jehovah's Witnesses without blood transfusion (N = 89).
Nelson CL & Bowen WS. J Bone Joint Surg [Am], 1986;68(3):350-3
Preoperatively assessing and planning blood use for elective vascular surgery (N = 120)
Spence RK et al. Am J Surg, 1994;168(2):192-6
Transfusion free surgery: single institution experience of 27 consecutive liver transplants in Jehovah's Witnesses
Jabbour N et al. J Am Coll Surg, 2005;201(3):412-7

14
PROCEDURE AND ERROR-RELATED BLEEDING
1. Procedures that involve cutting into the cardiovascular system may involve more risk, and errors do occur in the best of circumstances, but REMEMBER
2. Shed blood can be recovered, processed and returned to the patient for ALL these procedures, and
3. ALL these procedures can and have been done with minimal blood loss by using careful technique and meticulous hemostasis.

15
MICROVASCULAR BLEEDING AND OOZING - WHAT’S GOING ON ?
Quantitative and/or Qualitative problems with Platelets and/or Coagulation Factors
Drug effects and Interactions
Massive transfusion - dilution
Transfusion reaction Melting Ice Cream Truck sculpture by "The
Glue Society”, Australia

16
Platelets and Coagulation Factors - Quantitative Disorders
Hereditary Fanconi, Alport, Bernard-Soulier syndromes
Factor deficiencies - Hemophilia, Von Willebrand’s disease
Decreased production Vitamin B12 deficiency
Leukemia, Myelodysplastic syndrome
Sepsis
Liver failure
Increased destruction ITP, TTP, DIC, SLE, HUS
Dilutional Massive transfusion

17
Platelets and Coagulation Factors - Qualitative Disorders
Medications Heparin/Warfarin - prophylaxis
COX inhibitors Aspirin/NSAIDs
Glycoprotein IIb/IIIa inhibitors Abciximab, Epifibitide, Tirofiban
ADP inhibitors Clopidogrel, Ticlopidine
Chemotherapeutic agents
Valproic acid
Herbals
Von Willebrand’s disease

18
Risk of Bleeding with Prophylactic Anticoagulation
Rivaroxaban v. enoxaparin in TKR % THR: Major bleeding TKR = 0.6%; 0.5%; THR = 0.3%; 0.1%
Lassen MR et al. N Engl J Med.2008;358(26):2776-86
Erikkson BI et al. N Engl J Med.2008;358(26):2765-75
Bleeding incidence = 6.7% with LMWH v. 2.7% with conventional heparin but all MINOR
Bergqvist D et al. Br J Surg. 1988;7599):888-91
High risk orthopedic surgery - no major bleeding in trial of LMWH v. UFH
Simmoneau G et al. Arch Intern Med.1993;153(13):1541-6
426 pts - all general anesthesia, all LMWH: 1/426 (0.2%) bleeding
Howard A et al. Br J Surg. 2004;91(7):842-7
Incidence of
MAJOR bleeding
less than 1%

19
Herbal Medicines with Coagulation Effects
Ginkgo biloba
Licorice root
Ginger
Garlic
Gingseng
Clove
Fenugreek
Feverfew

20
Preoperative Strategies
Identify and record patient’s medications
Stop meds before surgery if possible…and safe
Convert from long acting/irreversible drug to reversible drug Coumadin to Heparin
Use smaller dose Pre-operative aspirin increases post-operative bleeding, but
this may be avoided by the use of aspirin doses <325 mg/day.
Sun JC et al. Eur Heart J, 2008;29(8):1057-71
Correct nutritional deficiencies
Use specific factors for hereditary disorders
Desmopressin for von Willebrand’s

21
What About Patients on Dual Therapy after PCI and Stenting?
Dual therapy = Clopidogrel and ASA
Risk of stent thrombosis increased if therapy is discontinued early, especially if surgical pt,
Silber S et al. Herz, 2008; 33(4):244-53
Chassot PG et al. Br J Anaesth. 2007;99(3):316-28
Best evidence says MUST continue therapy until stents are endothelialized
3 mos for bare metal stents; up to 1 yr for drug-eluting stents
Rate of bleeding and transfusion for CABG similar with/without cessation of clopidogrel Song SW et al. Circ J. 2008;72(4):626-32
Consider converting from irreversible drug (Clopidogrel) to reversible drug (Eptifibitide)
Consult the cardiologist!!!

22
Trauma, Transfusions and Recombinant Factor VIIa
380 patients in Level I & II trauma centers at risk of death from hemorrhage
Mean time from admission to rFVIIa = 4.6 hrs.
Average 18 units RBCs before rFVIIa
Death from hemorrhage = 30%
Predictors of poor response pH <7.2
Platelet count <100,000
Blood pressure </= 90mm Hg
“Precise role of rFVIIa in traumatic hemorrhage is unclear.”
“First, correct shock, acidosis and thrombocytopenia.”
Knudson MM et al, 2011, J Amer Coll Surg, 22:1, 87-95
23
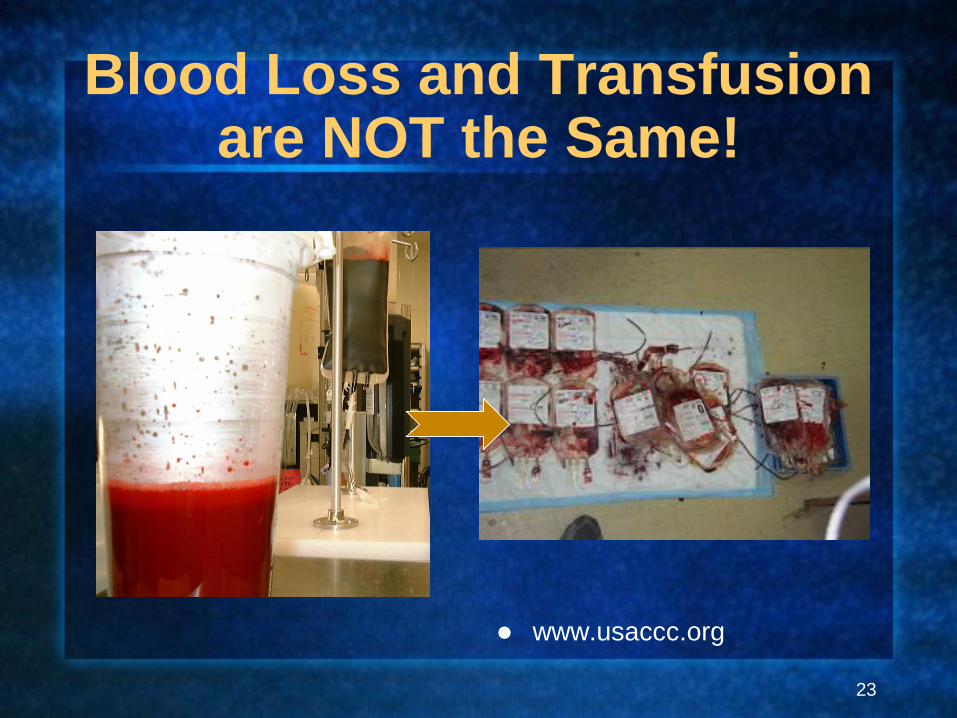
Blood Loss and Transfusion are NOT the Same!
www.usaccc.org
24
Why Do We Transfuse? Historical Transfusion Standards
James Blundell (1812): transfuse only following life-threatening hemorrhage
Multiple authors (19th century - 1940’s): transfuse only following life-threatening hemorrhage or to treat severe anemia
Adams and Lundy (1941): transfuse to an H/H of 10/30 before surgery
Received knowledge (1941-1988): transfuse as deemed needed
NIH Consensus Conference(1988): transfuse based on clinical evidence and Hgb < 8 gm/dL

25
Rationale for Transfusion Over Time
1667 - Correct mental disturbances
Jean Baptiste Denis and surgeon Paul Emmerez transfused lamb’s blood into a 16 yr old boy to correct his “dull and lumpish spirit.”
Antoine Mauroy had “escaped from his wife’s control.”
Deaths and lawsuits lead to ban for 150 years.

26
Rationale for Transfusion Over Time
1818 - Preventing death from active blood loss James Blundell
performs 1st allogeneic human blood transfusion on post-partum women - 50% successful
1818 and on - Uncertainty We are “all at sea” on
this subject

27
Rationale for Transfusion 1880 - 1900
Reports on 243 transfusions for “severe hemorrhage” -
Life-saving in 40.9%.
Experiments in transfusion for “severe hemorrhage”
Jennings - Transfusion: 1884 Geo Crile, Sr. - Hemorrhage and Transfusion: 1899

28
Bernheim, Blood Transfusion, Hemorrhage and the Anemias, 1917
Death from hemorrhage can be prevented by transfusion
Surgery made possible by transfusion
BUT, only anecdotal evidence

Rationale for Transfusion 1880 - 1900 - II
•Risk of reaction = 1:2 or 3
•Success = volume and use of fresh, whole blood
•Cult of itinerant “surgical” transfusionists develops

30
Military experience with
fresh, whole blood

31
Immediate Life-Threatening Condition…AND Hemoglobin!
BLEEDING CARDIOPULMONARY COMPROMISE
STILL POSSIBLE
IV ACCESS CONTROL PAIN
TREAT HYPOTHERMIA CORRECT PH TO > 7.20
1. BOLUS 20 ML/KG RL/NS, repeat X 2 2. TRANSFUSE TO HBG > 10 G/Dl 3. FIND AND CONTROL BLEEDING SITES
Scientific American Handbook of Trauma, 2000

32
Immediate Life-Threatening Condition…AND Hemoglobin!
http://www.trauma.org/archive/resus/massive.html
If Hb > 10g/dl transfusion is rarely indicated.
If Hb < 7g/dl transfusion is usually necessary.
If Hb between 7 and 10 g/dl, clinical status, PvO2 and ER are helpful in defining transfusion requirements

33
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”

34
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”

35
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”

36
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”

37
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”

38
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”
6. “THIS IS WHAT I WAS TAUGHT TO DO.”

39
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”
6. “THIS IS WHAT I WAS TAUGHT TO DO.”
7. “I ALWAYS TRANSFUSE THIS TYPE OF PATIENT.”

40
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”
6. “THIS IS WHAT I WAS TAUGHT TO DO.”
7. “I ALWAYS TRANSFUSE THIS TYPE OF PATIENT.”
8. “THE NURSE CALLED AND TOLD ME HE NEEDED BLOOD.”

41
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”
6. “THIS IS WHAT I WAS TAUGHT TO DO.”
7. “I ALWAYS TRANSFUSE THIS TYPE OF PATIENT.”
8. “THE NURSE CALLED AND TOLD ME HE NEEDED BLOOD.”
9. “THE ANESTHESIOLOGIST/HOSPITALIST/ PA/ NP/ RESIDENT/PRIMARY CARE DOC DID IT - NOT ME!”

42
WHY DO YOU TRANSFUSE?
1. THE PATIENT “NEEDS”, “REQUIRED” A TRANSFUSION BECAUSE
1. “THE HEMOGLOBIN WAS LOW.”
2. “HE WAS ANEMIC.”
3. “SHE NEEDED MORE OXYGEN.”
4. “WE’D LOST A LOT OF BLOOD.”
5. “SHE WAS DIZZY AND LIGHT-HEADED.”
6. “THIS IS WHAT I WAS TAUGHT TO DO.”
7. “I ALWAYS TRANSFUSE THIS TYPE OF PATIENT.”
8. “THE NURSE CALLED AND TOLD ME HE NEEDED BLOOD.”
9. “THE ANESTHESIOLOGIST/HOSPITALIST/ PA/ NP/ RESIDENT/PRIMARY CARE DOC DID IT - NOT ME!”
10. “I WAS ONLY FOLLOWING ORDERS.”

43
WHAT DETERMINES RBC TRANSFUSION? THE “USUAL SUSPECTS”?
Blood loss? Most literature discusses
TRANSFUSION not BLOOD LOSS - they are not the same!!
Patient status Co-morbidities
Urgency of operation
Surgeon - experience, training and choice
Hemoglobin/Anemia
Female gender
Advanced age
BSA
Captain Renault: “Major Strasser
has been shot. Round up the
usual suspects.” (Casablanca, 1942)

44
FACTORS ASSOCIATED WITH RBC TRANSFUSION
N = 130,171 elective surgical patients
FACTOR OR CI P
GENDER (F) 1.7 1.6 - 1.8 <.0001
ANEMIC ON ADM 0.6 0.56 - 0.65 <.0001
HX ANEMIA 1.75 1.6 - 1.9 <.0001
ANY HEART DISEASE
1.18 1.1 - 1.3 <.0001
CHARLSON 0.19 0.15 - 0.23 <.0001
NADIR HGB 13944 9198 - 21148 0.0000

45
ADMISSION HGB GROUP - NUMBER PATIENTS BY GROUP
0
1000
2000
3000
4000
5000
6000
7000
N PTS
N PTS 230 464 1446 2435 3701 5389 6569 6325 4805 2957 1564 1583
5 6 7 8 9 10 11 12 13 14 15 16
67%

46
RBC Transfusion by Admission and Nadir Hemoglobin
0
10
20
30
40
50
60
70
NADIR ADM
NADIR 50 66 58 52 34 17 12 10 9.6 10 9 9 9.2
ADM 48 66 57 50 38 27 23 17 14 14 15 14 17
4.1-5 5.1-6 6.1-7 7.1-8 8.1-9 9.1-1010.1-
11
11.1-
12
12.1-
13
13.1-
14
14.1-
15
15.1-
16
16.1-
17

47
RBC Transfusion in Patients with AHD
by Hemoglobin Group - % transfused
0
10
20
30
40
50
60
70
80
AHD YES AHD NO
AHD YES 33.3 58 53.3 50 42 31 27 20.3 16.8 16.8 14.6 15.1 20.8 19.1 14.4
AHD NO 60.3 71.4 60.2 49.5 35.6 25.1 20.2 15.3 12.1 12.1 16.1 13.1 13.7 15.8 14.4
<5 5.1-6 6.1-7 7.1-8 8.1-99.1-
10
10.1-
11
11.1-
12
12.1-
13
13.1-
14
14.1-
15
15.1-
16
16.1-
17
17.1-
18>18
P <.0006
P <.03

48
0
1
2
3
4
5
6
7
8
9
% RBCS YES % RBCS NO CHARLSON
% RBCS YES 0 0 2.5 4 3.7 1.3 2.8 3.3 4 3.4 4.15 4.4 4.3 2.1 2.2
% RBCS NO 5.9 8 2.4 2.6 4.5 1.6 0.84 0.88 0.78 0.84 0.84 0.79 1.2 1.2 0.34
CHARLSON 1.6 2 1.5 1.4 1.5 1.4 1.35 1.3 1.2 1.3 1.4 1.5 1.3 1.2 1
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
P <.0001
HGB RANGE
Impact of RBCs on mortality in elective, non-cardiac surgery patients with any heart disease -
Plenary Session presentation, AABB Annual Meeting, 2008, Montreal
RBC Transfusion and Mortality in
Elective, Non-Cardiac Surgery

49
RBC Transfusion Incidence by Procedure Group
0
5
10
15
20
25
% PTS RBCS
% PTS RBCS 20 18 22 20 21 18 22 19 20 21 20 20 17 20.5
CVS ENDO ENT EYEFEM
GENGI GU
HEML
YM\P
MALE
GENMS
NEUR
ORESP SKIN MISC
N = 130,641 pts. P <.0001 across groups

50
RBC TRANSFUSION VARIABILITY - THE AUSTRIAN STUDY
N = 1401 THR, 1296 TKR, 777 CABG Gombotz H et al, Transfusion, 2007;47(8):1468-80
0
50
100
% P
TS
T
RA
NS
FU
SE
D
PROCEDURE TYPE
HIGH LOW
HIGH 85 87 63
LOW 16 12 37
THR TKR CABG

51
RBC TRANSFUSION VARIABILITY BY HOSPITAL - JOINT REPLACEMENT
0
10
20
30
40
50
60
70
80
% PTS
% PTS 32 22 16.7 7.3 28 74 64.5 32 38.5 45 16.5 39 1.5
A B C D E F G H I J K XXX EBS

52
RBC TRANSFUSION VARIABILITY BY SURGEON - COLECTOMY
A B C D E F G H I J K L M N O P Q
% PTS RBCS
0
10
20
30
40
50
60
70
% PTS RBCS
% PTS RBCS 67 50 31 17 33 40 0 33 29 25 0 20 60 14 13 20 40
A B C D E F G H I J K L M N O P Q
N = 2,056 pts.

53
RBC TRANSFUSION VARIABILITY BY SURGEON - LYSIS OF ADHESIONS
A B C D E F G H I J K L M N O P Q
% PTS RBCS
0
10
20
30
40
50
60
70
80
90
% PTS RBCS
% PTS RBCS 25 0 0 25 0 60 60 20 20 0 40 33 17 86 14 25 78
A B C D E F G H I J K L M N O P Q
N = 2,136 pts.

54
RBC TRANSFUSION VARIABILITY BY SURGEON - BREAST
A B C D E F G H I J K L M N O P Q
% PTS RBCS
0
10
20
30
40
50
60
70
80
90
% PTS RBCS
% PTS RBCS 20 60 20 0 40 0 0 83 67 17 43 71 14 0 11 10 27
A B C D E F G H I J K L M N O P Q
N = 2,080 pts.

55
When Are RBCs Transfused? Transfusion by Perioperative Day
0
10
20
30
40
50
60
% P
TS
TR
AN
SF
US
ED
0
50
100
150
200
250
% PTS N UNITS
% PTS 9 50 26 14 11 5 1 2 2 9
N UNITS 48 199 94 51 40 19 4 9 12 32
PREOP OP POD 1 POD 2 POD 3 POD 4 POD 5 POD 6 POD 7POD
>1 WK

56
Risk versus Benefit in Blood Transfusion: Known Risks of Blood Transfusion
Reactions
TTD
Microchimerism
TRIM
TRALI
TACO
Cytokine infusion
Human error

57
Risk Vs. Benefit is in the Eyes
of the Beholder
BUT, known risks should outweigh
perceived benefits every time

58
Studies of RBC Transfusion Association with Infection
A. Taylor - Orthopedics: Y = 14.3%; N = 5.8%
A. Crit Care Med,2006;34(9):2302-8
B. Innerhofer - Orthopedics: Y = 12%; N = 6.9%
A. Transfusion, 2005;45(1):103-10
C. Dunne - Trauma/combat: Y = 69%; N = 18%
A. Am Surg, 2006;72(7):619-25
Hill - 23 peer-reviewed articles (1986 to 2000)- 13,152 pts. (5,215 transfused; 7,937 non-transfused
OR of postoperative bacterial infection with RBCS =as 3.45
(range, 1.43-15.15), p < or = 0.05
Hill, Gary E et al. J Trauma 2003 May;54(5):908-14.
0
10
20
30
40
50
60
70
% P
TS
WIT
H IN
FE
CT
ION
A B C
AUTHORS
WITH RBCS W/O RBCS
These results provide overwhelming
evidence that ABT is associated with a
significantly increased risk of
postoperative bacterial infection in the
surgical patient.

59
Allogeneic Blood Transfusion, Cancer Recurrence and Survival
Author Cancer N Pts Year Survival Recurrence
Drezner Esoph 235 2000 NA
Balachandran Ampullary 113 2007 NA
Dhar Gastric 640 2000 NA
Pysz Breast 863 77-95
Van de
Watering
Colorectal* 657 2001
Kaibori Hepatic 285 2007
Amato Colorectal 12,127 2006 NA
Jensen Colorectal** 740 2000

60
The RBC Storage Lesion
Decreased oxygen delivery Loss of 2,3, diphosphoglycerate (2,3 DPG) shifts O2 dissociation curve to left = hemoglobin
attracts oxygen and holds onto it but doesn’t release it well. Suttner, Anesth Analg, 2004
Deformed cells RBCs lose flexibility and cannot get into the capillaries, thereby decreasing delivery of
oxygen to cells in need. Chin-Yee I and Spence RK, Blood Storage in: Perioperative Transfusion Medicine, 2006, eds. Spiess, Shander, Spence. P.
199-210.
Accelerated RBC death Stored RBCs die more quickly than fresh cells. They release free hemoglobin, a potent
vasoconstrictor. Vasoconstriction of capillaries decreases oxygen delivery to tissues. Luten M., Cell Mol Biol, 2004
Affects both Allogeneic and Autologous RBCs Ghio M et al, Transfusion, May 6 2008

61
Koch C et al., Duration of Red-Cell Storage and
Complications after Cardiac Surgery.
N Engl J Med, 2008, 358(12):1229-1239
The Older the Blood, the Worse the Outcome
Multiple studies in a variety of patients have shown that the age of the transfused blood has a negative impact on patient outcomes.
Pneumonia Van de Watering, Transfusion,
2006
ICU patients Tinmouth, Transfusion, 2006
Cardiac surgery Vamvakas, Transfusion, 1999

62
Giving MORE Blood Does NOT Improve Outcomes
The TRICC Trial: 357 ICU pts. randomized to maintenance of either 8 gm/dL (restrictive group) vs. 10 gm/dL (liberal group)
• Hébert et al. N Engl J Med. 1999;340:409-417
The PINT Trial: ELBW infants randomly assigned within 48 hrs of birth to maintenance of low or high Hgb transfusion thresholds.
Kirpalani H, J Pediatr, 2006;149(3):301-307
RBC transfusion to 8 gm/dL vs. 10 gm/dL in severe brain injury patients
George et al, Neurocrit Care, 2008;Feb 14
For ALL THREE TRIALS: Transfusion rate lower in restrictive groups
No statistically significant differences between groups in primary outcomes.

63
Benefit of Blood Products - What Can We Conclude?
Evidence of benefit from RBC transfusion is hard to find
Most benefit is assumed and not scientifically proven
Some patients will benefit from blood transfusion but we need to do a better job of identifying who they are
No prospective, randomized trials have ever been done to establish the life-saving benefit of RBC transfusion
Giving MORE blood is NOT better
As a result, many RBC transfusion are probably unnecessary
Patients transfused without need get RISK, not BENEFIT

64
All Blood Products Carry Risk
FFP PLATELETS

65
FFP and CRYO GUIDELINES
DO USE FFP FOR Single or multiple specific, diagnosed coagulation
factors deficiencies
DIC with bleeding
DO NOT USE FFP FOR Warfarin reversal
Vitamin K deficiency
To correct INR/PT/PTT in the absence of bleeding
Hypovolemia
DIC without bleeding
DO USE CRYO FOR Documented fibrinogen deficiency
DIC with bleeding

66
How Do I Prevent and/or Reduce Blood Loss?
• Halstedian principles
• Temporary vascular occlusion
• Stop bleeding, don’t use it as a guide to transfusion!
• “I HAD TO DO THIS QUICKLY, SO I IGNORED THE BLEEDING”
• Anatomic dissection • “IF IT BLEEDS WHEN YOU CUT
IT, IT’S A VESSEL!’
• CLAMP, THEN CUT!
• Experienced hands • SLOW BAD, FAST BAD, FAST
GOOD
• Preop embolization
• Staging of procedures
• CUSA, cautery, LASER, etc.
• Fibrin glues, etc.
• Laparoscopic and lap-assisted surgery
• Image-guided surgery
• Robotics
• Minimally-invasive, endovascular, etc.

67
Halsted’s Surgical Principles
Handle tissue gently
Dissect along anatomic planes
Maintain hemostasis
Use fine sutures
Use sharp dissection

68
“Next, an example of the very same procedure when done correctly!”
Know
The
Procedure!!

The surgeon has many tools available to control bleeding.
Know them and use them wisely.

70
THE MAIN REASONS WE TRANSFUSE
TO TREAT ANEMIA AND RAISE H&H
PHYSICIAN CHOICE

71
Blood Loss in Surgery - Basic Concepts
Most general surgical procedures can be done with minimal blood loss
Reducing surgical blood loss improves outcomes by reducing RBC transfusion
Allogeneic blood carries risk that can be avoided
Preoperative planning is essential for blood avoidance

72
WHAT CAN WE CHANGE IN OUR TRANSFUSION PRACTICE?
1. PREVENTION - WORDS HAVE POWER, SO STOP SAYING THE PATIENT “NEEDS” OR “REQUIRED” A TRANSFUSION
1. WHERE’S THE PROOF? WHY DID THE PT “NEED” A TRANSFUSION?
2. IF YOU CHOSE TO TRANSFUSE USE CLINICAL CRITERIA AND DOCUMENT BOTH YOUR REASONS AND RESULTS
1. ADD TO SURGICAL TIME-OUT?
3. IF ARE YOU TREATING A NUMBER, NOT A PATIENT
1. WHO FEELS BETTER - YOU OR THE PATIENT?
73
TREAT ANEMIA PREOP
Treatable anemia
should be a CONTRAINDICATION
to elective surgery.

74
Perioperative Blood Management Policies
Tolerate asymptomatic anemia
Transfuse on a case-by-case basis Document both rationale and results
Transfuse one unit at a time
Right blood to the right patient at the right time
Prevent and control blood loss
Use fresh, not stored, autologous blood
Maximize oxygen delivery
Restore RBC preop
Involve the patient
Follow policies and procedures
Track, measure and monitor
Listen, learn and share Spence RK, Surgical Red Blood Cell Transfusion Policies. Am J
Surgery, 1995; 170, [6A] (Suppl)

75
Any Questions?