birt-hogg-dube syndrome. state-of-the-art review with ... · review with emphasis on pulmonary...
TRANSCRIPT
+ MODEL
Respiratory Medicine (2014) xx, 1e8
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/rmed
REVIEW
Birt-Hogg-Dube syndrome. State-of-the-artreview with emphasis on pulmonaryinvolvement
Aline Amaral Dal Sasso a,1, Luciana Camara Belem a,2,Glaucia Zanetti a,3, Carolina Althoff Souza b,4,Dante Luiz Escuissato c,5, Klaus Loureiro Irion d,6,Marcos Duarte Guimaraes e,7, Edson Marchiori a,*
a Federal University of Rio de Janeiro, Rio de Janeiro, Brazilb The Ottawa Hospital, University of Ottawa, Ottawa, Ontario, Canadac Federal University of Parana, Curitiba, Brazild Liverpool Heart and Chest Hospital and the Royal Liverpool University Hospital NHS Trusts, Liverpool,United Kingdome A.C. Camargo Cancer Center, Sao Paulo, Brazil
Received 22 August 2014; accepted 20 November 2014
KEYWORDSBirt-Hogg-Dube;Imaging;Lung diseases;Computed
Abberivations: BHDS, Birt-Hogg-DubeLAM, lymphangioleiomyomatosis; LCHcomplex.* Corresponding author. Rua Thomaz
fax: þ55(21)26299017.E-mail addresses: aline_sasso@hot
[email protected] ([email protected] (M.D. G1 Rua Figueiredo de Magalhaes, 9502 Avenida Ayrton Senna, 111/405, B3 Rua Coronel Veiga, 733/504. Cent4 Department of Diagnostic Imaging5 R. General Carneiro, 181, CEP 8006 Thomas Drive, Liverpool, United K7 Rua Paulo Orozimbo, 726, Aclimac
Please cite this article in press as: Dinvolvement, Respiratory Medicine (2
http://dx.doi.org/10.1016/j.rmed.2010954-6111/ª 2014 Elsevier Ltd. All rig
Summary
Background: Birt-Hogg-Dube syndrome (BHDS) is a rare, inherited autosomal-dominant disor-der characterized by the development of cutaneous lesions, renal tumors, pulmonary cysts,and spontaneous pneumothorax. The gene responsible for BHDS is located on the short armof chromosome 17 (17p11.2) and codes for the protein folliculin, which is believed to be an
syndrome; CT, computed tomography; FLCN, folliculin; HIF-1a, hypoxia-inducible factor 1-alpha;, Langerhans cell histiocytosis; mTOR, mammalian target of rapamycin; TSC, tuberous sclerosis
Cameron, 438, Valparaiso, CEP 25685.120. Petropolis, Rio de Janeiro, Brazil. Tel.:þ55 (24) 22492777;
mail.com (A.A. Dal Sasso), [email protected] (L.C. Belem), [email protected] (G. Zanetti),Souza), [email protected] (D.L. Escuissato), [email protected] (K.L. Irion),uimaraes), [email protected] (E. Marchiori)./506, Copacabana, CEP: 22031-012, Rio de Janeiro e Brazil. Tel.: þ55(32)91217945.arra da Tijuca, CEP 22793-000, Rio de Janeiro, Brazil. Tel.: þ55(21) 2433 3399.ro, CEP 25655-504, Petropolis, Rio de Janeiro, Brazil. Tel.: þ55(24)22429156., The Ottawa Hospital, 501 Smyth Road, Ottawa, K1H8L6, Canada. Tel.: þ1 613 737 8212.60-900, Curitiba, Parana, Brazil. Tel.: þ55(41)33435514.ingdom, L14 3 PE. Tel.: þ441617679073.ao, CEP 01535-001, Sao Paulo/SP, Brazil. Tel.: þ55(11) 32085327.
al Sasso AA, et al., Birt-Hogg-Dube syndrome. State-of-the-art review with emphasis on pulmonary014), http://dx.doi.org/10.1016/j.rmed.2014.11.008
4.11.008hts reserved.

2 A.A. Dal Sasso et al.
+ MODEL
tomography
Please cite this article in press as: Dinvolvement, Respiratory Medicine (2
oncogene suppressor protein.Methods: We reviewed currently published literature on the main characteristics of BHDS.Results: Pulmonary cysts and spontaneous pneumothorax are often the presenting manifesta-tions that lead to a final diagnosis in family members affected by the syndrome.Conclusions: Certain imaging characteristics of pulmonary cysts, including size and location,can suggest the diagnosis of BHDS based on chest computed tomography alone. The mainconcern in patients with BHDS is the increased risk of renal carcinoma. The aim of this reviewis to describe the main pathological, clinical, and imaging aspects of BHDS, ranging from itsgenetic basis to treatment, with emphasis on pulmonary involvement.ª 2014 Elsevier Ltd. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Epidemiology and genetic aspects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Pulmonary manifestations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Cutaneous manifestations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Renal manifestations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Other clinical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Pulmonary imaging findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Pulmonary function tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Imaging criteria for differential diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
Introduction
Birt-Hogg-Dube syndrome (BHDS) is a rare autosomal-dominant disorder characterized by the development ofcutaneous lesions, renal tumors, pulmonary cysts, causingspontaneous pneumothorax. In 1977, Birt, Hogg, and Dubeinvestigated members of the same family who presentedwith thyroid cancers. They found that some of them hadfibrofollicular skin tumors that occurred in an inheritedautosomal dominant pattern [1e3]. Although the familialdisorder was later named BHDS, the German dermatologistsHornstein and Knickenberg had reported similar inheritedskin tumors 2 years previously [4]. The genetic defectresponsible for BHDS has been mapped to a gene on chro-mosome 17p11.2, which encodes the tumor suppressorprotein folliculin (FLCN) [5e7].
Lung cysts have been described in most (77e89%) pa-tients with BHDS, and the estimated incidence of pneu-mothorax in these patients is 33e38% [2,5e8]. No evidenceof neoplasia, inflammation, or fibrosis has been found inassociation with these lung cysts [9]. Classically describedskin findings consist of the triad of hamartomas of the hairfollicles (fibrofolliculomas), tumors of the hair disk (tri-chodiscomas), and skin tags (acrochordons). Renal tumorswhen present are often multiple and bilateral [1,7,10,11].
al Sasso AA, et al., Birt-Hogg-Dub014), http://dx.doi.org/10.1016/
BHDS is probably underdiagnosed because of the widevariability of its clinical presentation [12]. This review de-scribes the main clinical, pathological, and imaging aspectsof BHDS.
Epidemiology and genetic aspects
BHDS is a rare entity, although its precise prevalence isunknown [8,13,14]. Approximately 200 families with path-ogenic FLCN mutations have been described in the litera-ture [13]. Mutation-prone regions tend to differ betweenaffected Japanese and Western families, which maypartially explain geographic differences in phenotypicpresentation [2,15].
The gene responsible for BHDS, located on the short armof chromosome 17 (17p12q11.2), was first identified in 2001based on a mapping analysis conducted in large familiesaffected by BHDS. The FLCN gene sequence was identifiedand named in 2002. It contains 14 exons, 11 of which codify,transcript mRNA and encodes a 579 aminoacid protein(FLCN) [2,7,13,16,17]. FLCN is expressed in a wide varietyof tissues, including skin, type-1 pneumocytes in the lungs,and distal nephron in the kidneys. The FLCN protein wasfound to be over expressed in proliferating epithelialfibrofolliculomas, but its expression was significantly
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008

Birt-Hogg-Dube syndrome 3
+ MODEL
reduced in renal tumor tissues from patients with BHDS,regardless of histological subtype [5,13,16].
Numerous mutations in the FLCN gene have beendescribed. The most frequent is a hot spot mutation thatoccurs within a polycytosine C8 tract of exon 11 and resultsin FLCN truncation [15,16,18e20]. To date, 142 unique DNAmutations of the FLCN gene have been implicated in thepathogenesis of BHDS [2].
BHD mutations in exon 9 have been associated with morelung cysts than those in other exons [6]. In addition, thesize and volume of the largest lung cyst have been found tobe significantly greater in individuals with BHD mutations inexons 9 and 12 than in those with mutations in other exons[6]. The potential relevance of exon 9 mutations for pre-disposition to cancer in BHDS has also been proposed [7,16].
Pathogenesis
The energy-sensing mammalian target of rapamycin(mTOR) pathway has been implicated in the pathogenesis ofseveral hereditary hamartoma syndromes, including BHDS[18]. FLCN is known to interact with the protein FINP1 andits homolog, FINP2, which in turn interact with 50 adenosinemonophosphateeactivated protein kinase, a key moleculethat negatively regulates mTOR activity. Inactivating mu-tations in this pathway result in dysregulated cell growthand protein synthesis, providing potential insight into themolecular mechanisms involved in BHDS [6,7,15,16,21,22].
Although unclear whether insufficient FLCN stimulatesor suppresses the mTOR pathway, some studies havedemonstrated increases in downstream molecules, such asS6 kinase and hypoxia-inducible factor 1-alpha (HIF-1a), inhuman BHDS renal tumors. In the lung, cyst-lining cells haveshown immunostaining positivity for phospho-mTOR andphospho-S6 ribosomal protein, suggesting that they areunder activated conditions [2,13,15,23]. As neoplasticproliferation is absent in cyst-lining cells, the mTORpathway may be less distinctively deviated in pulmonarycysts than in renal cell cancers [15].
The mechanisms of cyst development under the condi-tion of FLCN haploinsufficiency remain poorly understood.If accelerated mTOR signaling directly induces cysticremodeling, downstream molecules such as S6 ribosomalprotein may play a key role in pathogenesis. HIF-1a is a keymolecule contributing to aberrant angiogenesis in manytypes of cancer. Proliferation of blood vessels was noted inthe vicinity of pulmonary cysts [15]. Accelerated angiogenicsignaling is due in part to increases in HIF-1a and vascularendothelial growth factor associated with FLCN hap-loinsufficiency. These histopathologic findings support thenotion that the activation of angiogenic signaling contrib-utes to the development of BHDS-associated pulmonarycysts [15].
The involvement of mTOR pathway in the pathogenesis ofBHDS is also suggested by the phenotypic similarities of thissyndrome to tuberous sclerosis complex (TSC), which isknown to be caused by mTOR pathway dysregulation. How-ever, this is not the only signaling pathway implicated in thetumor suppressing action of the FLCN gene [2,15,18,24].
In the past several years, lung cyst pathogenesis hasbeen widely studied in pulmonary cystic diseases, such as
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
lymphangioleiomyomatosis (LAM), Langerhans cell histio-cytosis (LCH), and cystic lung light chain deposition disease[25]. Metalloproteinases appear to have an important rolein cyst formation [9,25]. These proteins belong to a familyof proteolytic enzymes mostly responsible for maintainingextracellular matrix remodeling, but they also affect cellmigration, angiogenesis, and pulmonary immunity. FLCNmutations may alter cytokines and proteases, which areimportant for extracellular matrix integrity. The pulmonaryarchitecture depends on interactions between collagen andelastin fibers in the extracellular matrix, which maintainalveolar wall integrity. The overexpression of metal-loproteinases leads to matrix breakdown, tissue destruc-tion, and cystic lesions [9,25].
Pathology
Although the pathology of renal and cutaneous manifesta-tions of BHDS has been well described, few reports havedescribed the histological characteristics of associatedpulmonary cysts [2]. In contrast to the neoplastic process inthe skin and kidney, no neoplastic changes have been re-ported in association with lung involvement [21,26].
By definition, cysts are well-circumscribed usually roundspaces with epithelial or fibrous walls of variable thickness.Macroscopically, cysts in BHDS are often elongated andsubpleural in distribution, with the total extent of lunginvolvement being less than 30% [27,28].
Microscopically, they are lined with pneumocytes andpartially enveloped by septal and/or pleural interstitialtissue. Alveolar cells lining the inner surface of the cystshow positive immune-staining for epithelial markers andsurfactant proteins. They may be attenuated or not easilyvisible; however, cuboidal cells resembling type II pneu-mocytes are often observed in the innermost layer [9,17].No reactive stromal proliferation or inflammation are pre-sent, except in case of rupture. The cyst wall extends to-ward the visceral pleura and is partially incorporated intothe parenchyma, interlobular septum, and/or bronchovas-cular bundle. In some cases, the walls are partially envel-oped by other alveolar walls, demonstrating an uniquearrangement of an alveolus or a few alveoli within the cyst.Occasionally, small veins protrude into the cystic space.These characteristic findings are important microscopicclues for the pathological diagnosis of BHDS [21,23].
Pulmonary cysts in BHDS are distinct from bullae,defined as cystic air spaces generated by destruction ofalveolar walls, and blebs, defined as intrapleural localizedair-containing lesions. However, examination of rupturedcysts can be misleading [2]. The histopathology of rupturedcysts causing pneumothorax is complicated due to me-chanical stress and tissue remodeling with associatedinflammation. Pleural thickening, interstitial bleeding, andhyalinization alter the original cyst architecture. Afterrupture, mesothelial invagination and bleb formation arefrequently observed. Cystic alveoli and fusion of the cystepithelium to the mesenchyme are diagnostic clues toBHDS-associated lung lesions, even at advanced stages withinflammatory changes [2,17,21,29]. The interlobular septain contact with a cyst may be edematous, possibly theresult of localized disturbance of circulation and venous
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008
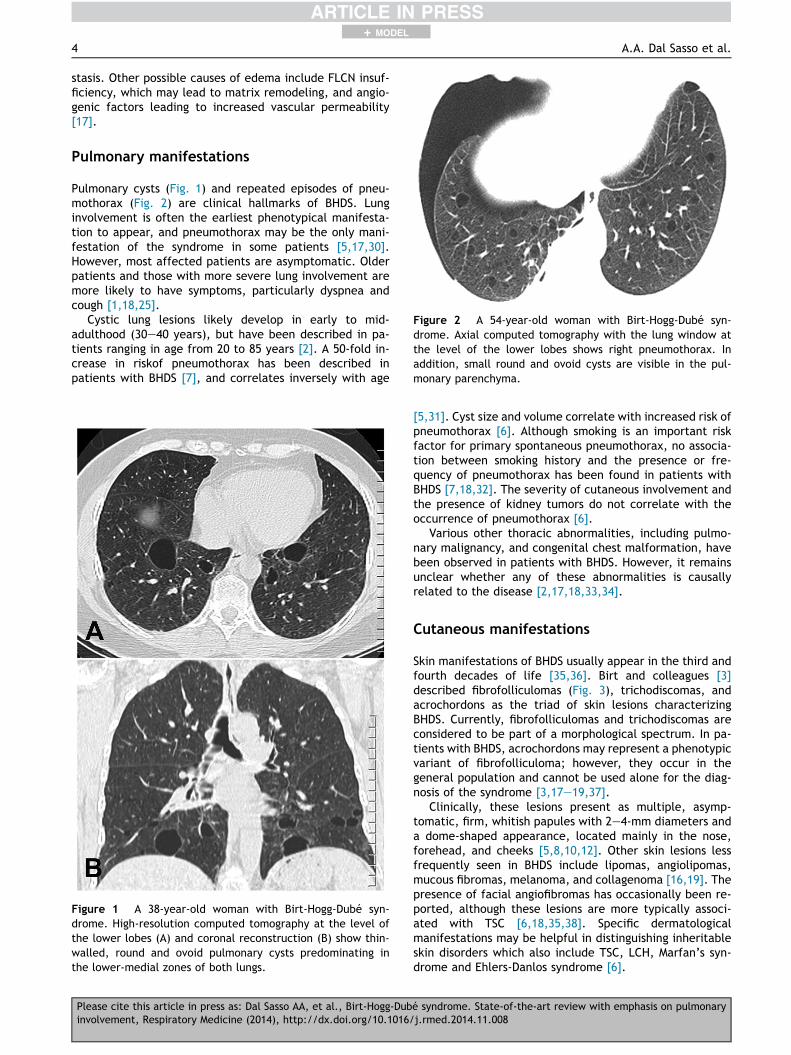
Figure 2 A 54-year-old woman with Birt-Hogg-Dube syn-drome. Axial computed tomography with the lung window atthe level of the lower lobes shows right pneumothorax. Inaddition, small round and ovoid cysts are visible in the pul-monary parenchyma.
4 A.A. Dal Sasso et al.
+ MODEL
stasis. Other possible causes of edema include FLCN insuf-ficiency, which may lead to matrix remodeling, and angio-genic factors leading to increased vascular permeability[17].
Pulmonary manifestations
Pulmonary cysts (Fig. 1) and repeated episodes of pneu-mothorax (Fig. 2) are clinical hallmarks of BHDS. Lunginvolvement is often the earliest phenotypical manifesta-tion to appear, and pneumothorax may be the only mani-festation of the syndrome in some patients [5,17,30].However, most affected patients are asymptomatic. Olderpatients and those with more severe lung involvement aremore likely to have symptoms, particularly dyspnea andcough [1,18,25].
Cystic lung lesions likely develop in early to mid-adulthood (30e40 years), but have been described in pa-tients ranging in age from 20 to 85 years [2]. A 50-fold in-crease in riskof pneumothorax has been described inpatients with BHDS [7], and correlates inversely with age
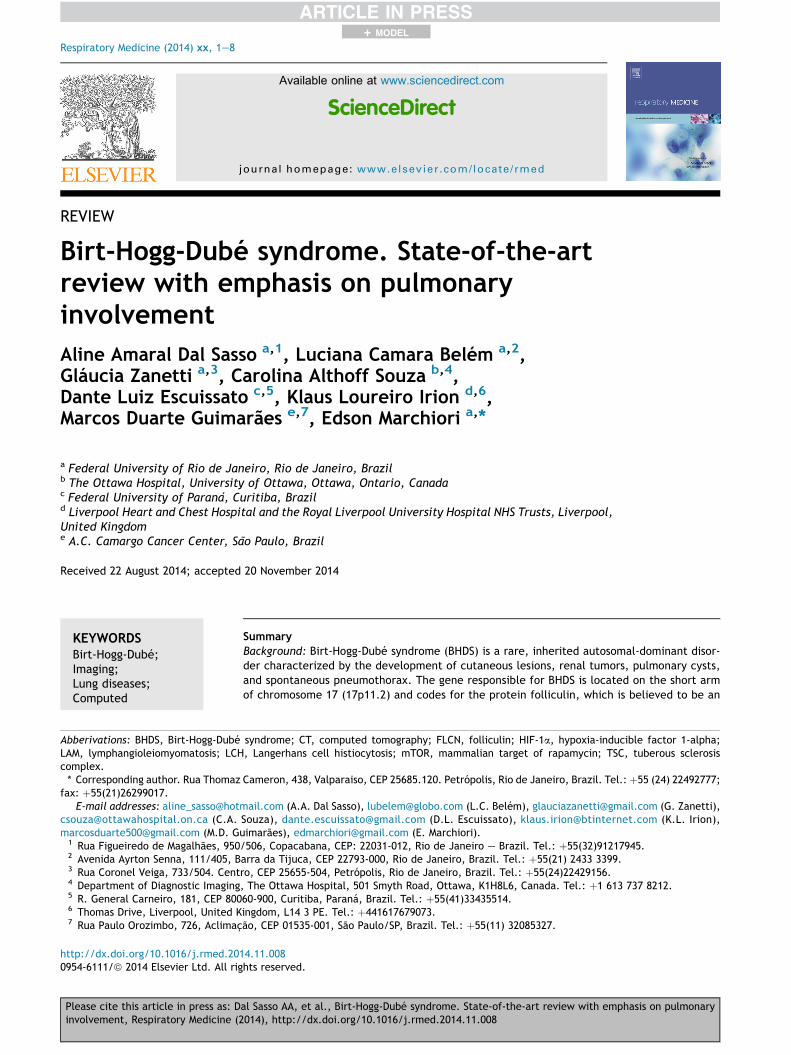
Figure 1 A 38-year-old woman with Birt-Hogg-Dube syn-drome. High-resolution computed tomography at the level ofthe lower lobes (A) and coronal reconstruction (B) show thin-walled, round and ovoid pulmonary cysts predominating inthe lower-medial zones of both lungs.
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
[5,31]. Cyst size and volume correlate with increased risk ofpneumothorax [6]. Although smoking is an important riskfactor for primary spontaneous pneumothorax, no associa-tion between smoking history and the presence or fre-quency of pneumothorax has been found in patients withBHDS [7,18,32]. The severity of cutaneous involvement andthe presence of kidney tumors do not correlate with theoccurrence of pneumothorax [6].
Various other thoracic abnormalities, including pulmo-nary malignancy, and congenital chest malformation, havebeen observed in patients with BHDS. However, it remainsunclear whether any of these abnormalities is causallyrelated to the disease [2,17,18,33,34].
Cutaneous manifestations
Skin manifestations of BHDS usually appear in the third andfourth decades of life [35,36]. Birt and colleagues [3]described fibrofolliculomas (Fig. 3), trichodiscomas, andacrochordons as the triad of skin lesions characterizingBHDS. Currently, fibrofolliculomas and trichodiscomas areconsidered to be part of a morphological spectrum. In pa-tients with BHDS, acrochordons may represent a phenotypicvariant of fibrofolliculoma; however, they occur in thegeneral population and cannot be used alone for the diag-nosis of the syndrome [3,17e19,37].
Clinically, these lesions present as multiple, asymp-tomatic, firm, whitish papules with 2e4-mm diameters anda dome-shaped appearance, located mainly in the nose,forehead, and cheeks [5,8,10,12]. Other skin lesions lessfrequently seen in BHDS include lipomas, angiolipomas,mucous fibromas, melanoma, and collagenoma [16,19]. Thepresence of facial angiofibromas has occasionally been re-ported, although these lesions are more typically associ-ated with TSC [6,18,35,38]. Specific dermatologicalmanifestations may be helpful in distinguishing inheritableskin disorders which also include TSC, LCH, Marfan’s syn-drome and Ehlers-Danlos syndrome [6].
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008

Figure 3 A 66-year-old man with Birt-Hogg-Dube syndrome.Multiple firm, white to skin-colored papules are visible on thenose and in the paranasal area. Biopsy demonstrated thatthese were fibrofolliculomas.
Figure 4 66-year-old man with Birt-Hogg-Dube syndrome.Axial in-phase T1-weighted magnetic resonance image (A)shows that the mass (arrows) has high signal intensity on T1,consistent with hemorrhagic or high proteinaceous content.Coronal HASTE T2-weighted magnetic resonance image (B)shows a large heterogeneous exophytic mass in the upper halfof the left kidney (arrows). There are central areas of necroticdegeneration with high T2 signal intensity. Cysts are seen onthe liver and on right kidney (arrowheads). Note also thehypointense rim on T1 and T2-weighted images around thetumor.
Birt-Hogg-Dube syndrome 5
+ MODEL
Renal manifestations
The most serious complication of BHDS is renal cancer(Fig. 4). The prevalence of renal tumors in these patients is23e34%, with a sevenfold increased risk of malignancywhen compared to the general population. Histologicalsubtypes include chromophobe oncocytomas (50%), chro-mophobe carcinomas (34%), clear cell carcinomas (9%),oncocytomas (5%), and papillary renal cell cancers (2%)[1,5,7,8,14,26]. Most renal tumors are bilateral, multifocal,and slow growing [11,13,19,24]. Benign renal cysts havealso been documented in patients with BHDS, but the exactprevalence in comparison to the general population iscurrently unknown [18,19,24]. Renal angiomyolipoma oc-casionally occurs in association with BHDS, but it is morefrequent in patients with TSC [1,5,15,24].
Other clinical findings
Several other lesions have been reported in BHDS includingbenign entities such as multinodular goiter, parathyroidadenoma, parotid-gland adenoma and oncocytoma, colo-rectal polyp and adenoma, neural tissue tumor, tricho-blastoma, connective tissue nevus, focal cutaneousmucinosis and cutaneous leiomyoma [5,10,11,18]. Malig-nant tumors include breast cancer, colorectal cancer, sar-coma of the leg, tonsillar cancer, basal and squamous-cellskin cancer, dermatofibrosarcoma protuberans, and cuta-neous leiomyosarcoma [5,7,10,11,18]. Other abnormalitiesobserved in patients with BHDS include flecked chorior-etinopathy, bullous emphysema, and internal carotid arteryaplasia [11,18]. However, their causal association withBHDS has not been clinically validated [16,18].
Pulmonary imaging findings
On computed tomography (CT), pulmonary cysts generallymanifest as a rounded lesion with well-defined interface
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
with normal lung parenchyma, usually containing air, or lesscommonly fluid. Cysts have variable wall thickness, usually<2 mm [28,39].
Certain CT imaging characteristics may suggest thediagnosis of BHDS-related cystic lung disease. In these pa-tients, cyst location differs from the typical apical locationof smoking-related emphysema and bullae/blebs seen inprimary spontaneous pneumothorax [2]. In BHDS, cysts aretypically located in the lower lung regions, distributedbilaterally, and intimately related to interlobular septaand/or visceral pleura, pulmonary arteries, and veins[8,18,29]. The number of cysts is quite variable [2,6,40] andtheir size range from a few millimeters to >2 cm althoughsmall (<1 cm) cysts are most commonly seen. The
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008

Table 1 Proposed diagnostic criteria for BHD [2].
Definite pulmonary BHD
1. Characteristica or compatibleb lung HRCT and skin biopsypositive for fibrofolliculoma or trichodiscoma
2. Characteristic or compatible lung HRCT and confirmedfamily history of BHD in first or second degree familymember
3. Characteristic or compatible HRCT and tissueconfirmation of renal chromophobe adenoma oroncocytoma
4. Characteristic or compatible HRCT and tissueconfirmation of genetic testing positive for BHD
Probable pulmonary BHD
1. Characteristic HRCT, exclusion of TSC and LAM, andpersonal or family history of pneumothorax
2. Compatible HRCT, exclusion of TSC and LAM, and any ofthe following:a. Family or personal history of renal tumorsb. Skin angiofibromac. Renal angiomyolipoma
Possible pulmonary BHD
Compatible or characteristic HRCT.a Characteristic lung HRCT findings: Multiple thin-walled
round, elliptical or lentiform well-defined air-filled cysts,without internal structure, in a basilar, medial and subpleuralpredominant distribution, with preserved or increased lungvolume, and no other significant pulmonary involvement (spe-cifically no interstitial lung disease).b Compatible HRCT findings: Thin walled cysts without the
more typical elliptical shape or subpleural distribution.
6 A.A. Dal Sasso et al.
+ MODEL
morphology of lung cysts varies within and amongst pa-tients, ranging from round to oval, lentiform, and lobu-lated/multiseptated. Cyst walls tend to be perceptible,thin, and uniform [8]. Tobino et al. [40] reported that mostpulmonary cysts in patients with BHDS were irregularlyshaped and that their extent did not change over time. Cystsize, morphology, and distribution patterns seem to beinherited within affected families and differ amongdifferent family groups [41,42].
Pulmonary function tests
Despite the presence of multiple lung cysts, pulmonaryfunction tests are usually normal or only mildly abnormal inpatients with BHDS [5,6,18]. Nevertheless, diffusion ca-pacity for carbon monoxide (adjusted for alveolar volume)was found to be mildly decreased, and absolute forcedexpiratory volume in 1 s was inversely correlated with cystarea measured by CT [2].
Diagnosis
The diagnosis of BHDS should be suspected in young patientspresenting with spontaneous pneumothorax, especiallythose with personal or family history of pneumothorax, skinlesions, or renal tumors [2,5,20]. In the system proposed byMenko et al. [18], the diagnosis of BHDS should be based onfulfillment of one major criterion (at least five adult-onsetfibrofolliculomas with histological confirmation of at leastone; pathogenic FLCN germline mutation) or two minorcriteria[multiple bilateral, basally located lung cysts with noother apparent cause, with or without spontaneous primarypneumothorax; early-onset (<50 years of age), multifocal,or bilateral renal cancer, or renal cancer of mixed chro-mophobe and oncocytic histology; first-degree relative withBHDS]. However, BHDS should be considered even in pa-tients who do not fulfill the diagnostic criteria but have anunderlying FLCN mutation [2,17,18,28].
New diagnostic criteria based mainly on chest CT char-acteristics of pulmonary cysts have been recently proposed[2] (Table 1).
Imaging criteria for differential diagnosis
The main differential diagnosis of BHDS include cystic lungdiseases, particularly LAM, lymphocytic interstitial pneu-monia (LIP), LCH and Pneumocystis jiroveci pneumonia[1,2,8]. The distribution of cysts along with ancillary find-ings on imaging studies may be helpful in distinguishingthese entities [6,27]. Diseases such as Marfan syndrome,homocystinuria, Ehler-Danlos syndrome, and alpha-oneantitrypsin deficiency can present with familial historiesof spontaneous pneumothorax and should also be consid-ered in the differential diagnosis of BHDS [2,6,8,21].
The presence of cysts in the setting of an autoimmunedisease, particularly Sjogren syndrome, is very suggestiveof LIP, which presents on CT as ground-glass opacities,poorly defined centrilobular nodules, and thin-walled cystswith a basal predominance. Although cysts may vary in size,they are often <30 mm in diameter and sparse. Additional
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
CT findings reported in LIP include peribronchovascularthickening, interlobular septal thickening, subpleural nod-ules, lymphadenopathy, and areas of consolidation [27,43].Pulmonary LCH is a smoking-related lung disease that in-cludes bronchiolocentric stellate interstitial nodules. Thenodules may subsequently cavitate and form thick- andthin-walled cysts. Frequently, nodules and cysts are seensimultaneously. The cysts are often irregular, bilobed orbizarrely shaped. P. jiroveci pneumonia is seen in patientswith immunosupression with acute or subacute respiratorysymptoms and typically presents on imaging studies withbilateral ground-glass opacities, occasionally with consoli-dation and nodules. Cystic lesions, or pneumatoceles, occurin approximately 30% of the cases, are typically transientand have upper zone predominance. Spontaneous pneu-mothorax can also occur [8,27].
Amongst the cystic lung diseases, LAM is the most difficultto differentiate from BHDS, especially when associated withTSC with renal and cutaneous involvement [1,2]. Similar toBHDS, TSC has a wide clinical spectrum. Patients with TSCusually show angiomyolipomas (70e90%), angiofibromas,hypopigmented macules, shagreen patch, and/or periungualfibromas [6]. Pulmonary LAM is a rare progressive diseasethat predominantly affects women of childbearing age. Menmay be affected in the setting of underlying TSC. Globally,LAM associated with TSC is 5- to 10-fold more common thansporadic LAM. Clinical manifestations include shortness ofbreath, cough, chest pain, chylous pleural effusions, he-moptysis, and occasionally respiratory failure although
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008

Birt-Hogg-Dube syndrome 7
+ MODEL
asymptomatic cases may occur. Spontaneous or recurrentpneumothorax may be the presenting finding in up to 50% ofpatients with LAM [44]. It has been suggested that LAMassociated with TSC most closely mimics BHDS on radiolog-ical exams. Cysts in BHDS and LAM are thin walled, but thoseassociated with LAM are smaller and more circular, homo-geneous, and equally distributed. The intervening lung pa-renchyma is typically normal in LAM although smallcentrilobular nodules, septal thickening, and focal ground-glass opacities have been reported [2,8,24,27].
Treatment
Patients with BHDS require evaluation by a multidisciplinaryteam and through investigation for multisystem complica-tions. From a pulmonary perspective, treatment is largelyfocused on treatment and prevention of pneumothorax.The management of pneumothorax in patients with BHDSdiffers from that recommended for patients with primaryspontaneous pneumothorax and is similar to that proposedfor patients with LAM. Given the high recurrence rate,surgical intervention with resection and pleurodesis is anacceptable option, even in patients with a first episode ofpneumothorax [2,5,41]. The prognosis of BHDS and LAM isquite different. LAM usually progresses to respiratoryinsufficiency, and BHDS does not [42]. LAM is extremelydifficult to treat, and the long-term prognosis is poor [44].On the other hand, BHDS lung cysts or pneumothoraceswere not associated with fatalities or chronic debilitation[6]. Patients should be informed that BHD cystic lung dis-ease typically does not result in respiratory failure. How-ever, patients with lung function impairment should beregularly followed by pulmonologists and periodic mea-surement of pulmonary function should be performed [2].
Patients should be cautioned about the increased risk ofpneumothorax in association with scuba diving and airtravel. Although no specific recommendations are availablefor BHDS, the British Thoracic Society guidelines [45]consider the presence of lung cysts and bullae a contrain-dication to diving due to increased risk of barotrauma andpneumothorax. In general, air travel is considered safe formost patients with BHDS [5,45]. Regular immunization andperiodic measurement of pulmonary function should beperformed in patients with BHDS. In addition, pneumo-coccal and annual influenza vaccination should be stronglyencouraged [2].
The main concern in BHDS is the development of renalcarcinoma [11,12]. Annual physical examination, magneticresonance imaging, and/or ultrasonography have been re-ported to be the best surveillance tools [30]. Due to theirbenign nature, no specific medical treatment is warrantedfor the cutaneous lesions of BHDS [11]. If required, surgicalremoval is the treatment of choice for solitary perifollicularfibromas whereas electrodessication may be helpful inremoving multiple lesions [13].
Conclusion
BHDS is a rare yet important genetic condition that remainsunderdiagnosed partly due to variable clinical presenta-tion. The presence of multiple papular skin lesions, renal
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
lesions, and/or a family history of pneumothorax or renalmalignancy are important diagnostic clues. Pulmonary cystson imaging studies may be the initial manifestation and areoften the finding to first suggest the diagnosis, highlightingthe role of CT in early diagnosis.
Awareness of the clinical manifestation of BHDS by pul-monologists and radiologists is pivotal in patients care as itallows early detection and management of complications,particularly renal malignancy.
Conflict of interest statement
The authors have no conflict of interest.
References
[1] Tomassetti S, Carloni A, Chilosi M, Maffe A, Ungari S,Sverzellati N, et al. Pulmonary features of Birt-Hogg-Dubesyndrome: cystic lesions and pulmonary histiocytoma. RespirMed 2011;105(5):768e74.
[2] Gupta N, Seyama K, McCormack FX. Pulmonary manifestationsof Birt-Hogg-Dube syndrome. Fam Cancer 2013;12(3):387e96.
[3] Birt AR, Hogg GR, Dube WJ. Hereditary multiple fibrofollicu-lomas with trichodiscomas and acrochordons. Arch Dermatol1977;113(12):1674e7.
[4] Hornstein OP, Knickenberg M. Perifollicular fibromatosis cutiswith polyps of the colonea cutaneo-intestinal syndrome suigeneris. Arch Dermatol Res 1975;253(2):161e75.
[5] Rehman HU. Birt-Hogg-Dube syndrome: report of a new mu-tation. Can Respir J 2012;19(3):193e5.
[6] Toro JR, Pautler SE, Stewart L, Glenn GM, Weinreich M,Toure O, et al. Lung cysts, spontaneous pneumothorax, andgenetic associations in 89 families with Birt-Hogg-Dube syn-drome. Am J Respir Crit Care Med 2007;175(10):1044e53.
[7] Toro JR, Wei MH, Glenn GM, Weinreich M, Toure O, Vocke C,et al. BHD mutations, clinical and molecular genetic in-vestigations of Birt-Hogg-Dube syndrome: a new series of 50families and a review of published reports. J Med Genet 2008Jun;45(6):321e31.
[8] Agarwal PP, Gross BH, Holloway BJ, Seely J, Stark P,Kazerooni EA. Thoracic CT findings in Birt-Hogg-Dube syn-drome. AJR Am J Roentgenol 2011;196(2):349e52.
[9] Goncharova EA, Goncharov DA, James ML, Atochina-Vasserman EN, Stepanova V, Hong SB, et al. Folliculin controlslung alveolar enlargement and epithelial cell survival throughE-cadherin, LKB1, and AMPK. Cell Rep 2014;7(2):412e23.
[10] Toro JR, Glenn G, Duray P, Darling T, Weirich G, Zbar B, et al.Birt-Hogg-Dube syndrome: a novel marker of kidneyneoplasia. Arch Dermatol 1999;135(10):1195e202.
[11] Pittet O, Christodoulou M, Staneczek O, Ris HB. Diagnosis ofBirt-Hogg-Dube syndrome in a patient with spontaneouspneumothorax. Ann Thorac Surg 2006;82(3):1123e5.
[12] Escuissato DL, de Almeida Teixeira BC, Warszwiak D,Zanetti G, Marchiori E. Renal tumor associated with pulmo-nary cysts: Birt-Hogg-Dube syndrome. Q J Med 2014;107(10):851e2.
[13] Ponti G, Pellacani G, Seidenari S, Pollio A, Muscatello U,Tomasi A. Cancer-associated genodermatoses: skin neoplasmsas clues to hereditary tumor syndromes. Crit Rev OncolHematol 2013;85(3):239e56.
[14] Klomp JA, Petillo D, Niemi NM, Dykema KJ, Chen J, Yang XJ,et al. Birt-Hogg-Dube renal tumors are genetically distinctfrom other renal neoplasias and are associated with up-regulation of mitochondrial gene expression. BMC Med Geno-mics 2010 Dec 16;3:59.
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008

8 A.A. Dal Sasso et al.
+ MODEL
[15] Nishii T, Tanabe M, Tanaka R, Matsuzawa T, Okudela K,Nozawa A, et al. Unique mutation, accelerated mTORsignaling and angiogenesis in the pulmonary cysts of Birt-Hogg-Dube syndrome. Pathol Int 2013;63(1):45e55.
[16] Palmirotta R, Savonarola A, Ludovici G, Donati P, Cavaliere F,DE Marchis ML, et al. Association between Birt Hogg Dubesyndrome and cancer predisposition. Anticancer Res 2010;30(3):751e7.
[17] Furuya M, Nakatani Y. Birt-Hogg-Dube syndrome: clinico-pathological features of the lung. J Clin Pathol 2013;66(3):178e86.
[18] Menko FH, van Steensel MA, Giraud S, Friis-Hansen L,Richard S, Ungari S, et al. Birt-Hogg-Dube syndrome: diagnosisand management. Lancet Oncol 2009;10(12):1199e206.
[19] Mota-Burgos A, Acosta EH, Marquez FV, Mendiola M, Herrera-Ceballos E. Birt-Hogg-Dube syndrome in a patient with mela-noma and a novel mutation in the FCLN gene. Int J Dermatol2013;52(3):323e6.
[20] Kunogi M, Kurihara M, Ikegami TS, Kobayashi T, Shindo N,Kumasaka T, et al. Clinical and genetic spectrum of Birt-Hogg-Dube syndrome patients in whom pneumothorax and/or mul-tiple lung cysts are the presenting feature. J Med Genet 2010;47(4):281e7.
[21] Koga S, Furuya M, Takahashi Y, Tanaka R, Yamaguchi A,Yasufuku K, et al. Lung cysts in Birt-Hogg-Dube syndrome:histopathological characteristics and aberrant sequence re-peats. Pathol Int 2009;59(10):720e8.
[22] Baba M, Hong SB, Sharma N, Warren MB, Nickerson ML,Iwamatsu A, et al. Folliculin encoded by the BHD gene in-teracts with a binding protein, FNIP1, and AMPK, and isinvolved in AMPK and mTOR signaling. Proc Natl Acad Sci U S A2006;103(42):15552e7.
[23] Furuya M, Tanaka R, Koga S, Yatabe Y, Gotoda H, Takagi S,et al. Pulmonary cysts of Birt-Hogg-Dube syndrome: a clini-copathologic and immunohistochemical study of 9 families.Am J Surg Pathol 2012;36(4):589e600.
[24] Byrne M, Mallipeddi R, Pichert G, Whittaker S. Birt-Hogg-Dubesyndrome with a renal angiomyolipoma: further evidence of arelationship between Birt-Hogg-Dube syndrome and tuberoussclerosis complex. Australas J Dermatol 2012;53(2):151e4.
[25] Pimenta SP, Baldi BG, Nascimento EC, Mauad T, Kairalla RA,Carvalho CR. Birt-Hogg-Dube syndrome: metalloproteinaseactivity and response to doxycycline. Clin (Sao Paulo) 2012;67(12):1501e4.
[26] Adley BP, Smith ND, Nayar R, Yang XJ. Birt-Hogg-Dube syn-drome: clinicopathologic findings and genetic alterations.Arch Pathol Lab Med 2006;130(12):1865e70.
[27] Seaman DM, Meyer CA, Gilman MD, McCormack FX. Diffusecystic lung disease at high-resolution CT. AJR Am J Roentgenol2011;196(6):1305e11.
[28] Silva CI, Marchiori E, Souza Jr AS, Muller NL, Comissao deImagem da Sociedade Brasileira de Pneumologia e Tisiologia.Illustrated Brazilian consensus of terms and fundamentalpatterns in chest CT scans. J Bras Pneumol 2010;36(1):99e123.
[29] Johannesma PC, Thunnissen E, Postmus PE. Lung cysts as in-dicator for Birt-Hogg-Dube syndrome. Lung 2014;192(1):215e6.
[30] Kunogi Okura M, Yae T, Nagashima O, Hirai S, Kumasaka T,et al. Pneumothorax developing for the first time in a 73-year-
Please cite this article in press as: Dal Sasso AA, et al., Birt-Hogg-Dubinvolvement, Respiratory Medicine (2014), http://dx.doi.org/10.1016/
old woman diagnosed with Birt-Hogg-Dube syndrome. InternMed 2013;52(21):2453e5.
[31] Zbar B, Alvord WG, Glenn G, Turner M, Pavlovich CP,Schmidt L, et al. Risk of renal and colonic neoplasms andspontaneous pneumothorax in the Birt-Hogg-Dube syndrome.Cancer Epidemiol Biomarkers Prev 2002;11(4):393e400.
[32] Kim EH, Jeong SY, Kim HJ, Kim YC. A case of Birt-Hogg-Dubesyndrome. J Korean Med Sci 2008;23(2):332e5.
[33] Hartman TR, Nicolas E, Klein-Szanto A, Al-Saleem T, Cash TP,Simon MC, et al. The role of the Birt-Hogg-Dube protein inmTOR activation and renal tumorigenesis. Oncogene 2009;28(13):1594e604.
[34] Ayo DS, Aughenbaugh GL, Yi ES, Hand JL, Ryu JH. Cystic lungdisease in Birt-Hogg-Dube syndrome. Chest 2007;132(2):679e84.
[35] Lopez V, Jorda E, Monteagudo C. Birt-Hogg-Dube syndrome:an update. Actas Dermosifiliogr 2012;103(3):198e206.
[36] Pavlovich CP, Walther MM, Eyler RA, Hewitt SM, Zbar B,Linehan WM, et al. Renal tumors in the Birt-Hogg-Dube syn-drome. Am J Surg Pathol 2002;26(12):1542e52.
[37] Przybycin CG, Magi-Galluzzi C, McKenney JK. Hereditary syn-dromes with associated renal neoplasia: a practical guide tohistologic recognition in renal tumor resection specimens. AdvAnat Pathol 2013;20(4):245e63.
[38] Schaffer JV, Gohara MA, McNiff JM, Aasi SZ, Dvoretzky I.Multiple facial angiofibromas: a cutaneous manifestation ofBirt-Hogg-Dube syndrome. J Am Acad Dermatol 2005;53(2Suppl. 1):S108e11.
[39] Hansell DM, Bankier AA, MacMahon H, McLoud TC, Muller NL,Remy J. Fleischner society: glossary of terms for thoracicimaging. Radiology 2008;246(3):697e722.
[40] Tobino K, Gunji Y, Kurihara M, Kunogi M, Koike K, Tomiyama N,et al. Characteristics of pulmonary cysts in Birt-Hogg-Dubesyndrome: thin-section CT findings of the chest in 12 patients.Eur J Radiol 2011;77(3):403e9.
[41] Onuki T, Goto Y, Kuramochi M, Inagaki M, Bhunchet E,Suzuki K, et al. Radiologically indeterminate pulmonary cystsin Birt-Hogg-Dube syndrome. Ann Thorac Surg 2014;97(2):682e5.
[42] Tobino K, Hirai T, Johkoh T, Kurihara M, Fujimoto K,Tomiyama N, et al. Differentiation between Birt-Hogg-Dubesyndrome and lymphangioleiomyomatosis: quantitative anal-ysis of pulmonary cysts on computed tomography of the chestin 66 females. Eur J Radiol 2012;81(6):1340e6.
[43] Marchiori E, Damato S, Rodrigues R, Valiante PM,Mendonca RG, Miyagui T, et al. Lymphocytic interstitialpneumonia: correlation of high-resolution computed tomog-raphy findings with anatomopathology. Radiol Bras 2002;35(4):199e203.
[44] Vianna FG, Marchiori E, Zanetti G, Mano CM, Sarcinelli-Luz B,Carvalho JF, et al. Tuberous sclerosis with pulmonary lym-phangioleiomyomatosis and renal angiomyolipomas.Computed tomographic findings: a case report. Cases J 2009Sep 11;2:9238.
[45] British Thoracic Society Fitness to Dive Group, Subgroup of theBritish Thoracic Society Standards of Care Committee. Britishthoracic society guidelines on respiratory aspects of fitness fordiving. Thorax 2003;58(1):3e13.
e syndrome. State-of-the-art review with emphasis on pulmonaryj.rmed.2014.11.008