biomarker-guided interventions of clinically relevant...
TRANSCRIPT

amr®
15 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
Biomarker-Guided Interventions of Clinically Relevant Conditions Associated with Autism Spectrum Disorders and Attention Deficit Hyperactivity Disorder James Jeffrey Bradstreet, MD, MD(H), FAAFP; Scott Smith, PA; Matthew Baral, ND; Daniel A. Rossignol, MD, FAAFP
AbstractAutism spectrum disorders (ASD) and attention-deficit hyperactivity disorder (ADHD) are common and complex neurodevelopmental conditions. Diagnostic criteria for these conditions have traditionally relied solely on behavioral criteria without consideration for potential biomedical underpinnings. Newer evidence, however, reveals that ASDs are associated with: oxidative stress; decreased methylation capacity; limited production of glutathione; mitochondrial dysfunction; intestinal dysbiosis; increased toxic metal burden; immune dysregulation, characterized by a unique inflamma-tory bowel disease and immune activation of neuroglial cells; and ongoing brain hypoperfusion. Many of these same problems are common features in children with ADHD. These medical conditions, whether co-morbidities or etiopathogenic, would be expected to have synergistically negative effects on the development, cognition, focus, and attention of affected children. It is likely these biological abnormalities contribute significantly to the behavioral symptoms intrinsic in these diagnoses. However, treatment for these underlying medical disorders is clinically justified, even if no clear immediate behavioral improvements are observed. This article reviews the medical literature and discusses the authors’ clinical experience using various biomarkers for measuring oxidative stress, methylation capacity and transsulfuration, immune function, gastrointestinal problems, and toxic metal burden. These biomarkers provide useful guides for selection, efficacy, and sufficiency of biomedical interventions. The use of these biomarkers is of great importance in young children with ADHD or individuals of any age with ASD, because typically they cannot adequately communicate regarding their symptoms. (Altern Med Rev 2010;15(1):15-32)
BackgroundAutism (autistic disorder), Asperger syndrome,
and pervasive developmental disorder (not otherwise specified) comprise a heterogeneous spectrum of neurodevelopmental disorders collectively termed autism spectrum disorders (ASD). They are behaviorally defined and character-ized by restrictive and repetitive behaviors along with impairments in communication and social interaction. The number of children diagnosed with ASD has substantially increased over the last decade1-3 and ASD currently affects an estimated one out of 91 individuals in the United States.4 However, since ASD occurs four times as frequently in males than females,5 reporting the prevalence of ASD in all children significantly underestimates the number of affected males. A reasonable extraction of the overall data when applied to the male population finds that one in 58 are likely affected with ASD,4 and the prevalence of affected males approaches two percent of the general population in additional studies.6,7 ASD is traditionally considered a “static” encephalopathic disorder8 without any known cure and few proven effective biomedical interventions. Furthermore, attention-deficit hyperactivity disorder (ADHD), which affects 4-12 percent of school age children,9 is behaviorally characterized by features of inatten-tion, hyperactivity, and impulsivity.10 While ADHD and ASD present complex medical problems for physicians, interventional strategies may be streamlined for many children as a result of advances in biomarker research. Given the large number of affected children and the continued increase in prevalence of both disorders, a simpli-fied treatment approach is needed for implementa-tion by primary care providers.
James Jeffrey Bradstreet, MD, MD(H), FAAFP Director, International Child Develop-ment Resource Center, Melbourne, FL; adjunct professor of pediatrics, South-west College of Naturopathic Medicine, Tempe, AZCorrespondence address: International Child Development Resource Center, 3800 West Eau Gallie Boulevard, Melbourne, FL 32934; phone: 321-259-7111Email: [email protected]
Daniel A. Rossignol, MD, FAAFP – Associate medical director, International Child Development Resource Center, Melbourne, FL
Scott Smith, PA – Staff physician assistant, International Child Development Resource Center, Melbourne, FL
Matthew Baral, ND – Chairman of the pediatric medicine program and associate professor of pediatrics, Southwest College of Naturopathic Medicine, Tempe, AZ

amr®
Volume 15, Number 1 Alternative Medicine Review 16Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
Recent evidence reveals that many children with ASD have multiple medical problems, including increased oxidative stress,11-13 decreased methyla-tion capacity with limited transsulfuration,12,14 mitochondrial dysfunction,15,16 increased toxic metal burden,17-21 intestinal dysbiosis skewed toward an overgrowth of Clostridia species,22-24 immune dysregulation with a unique inflammatory bowel disease and immune activation of glial cells in the brain,25-28 combined with central nervous system (CNS) hypoperfusion or abnormal regula-tion of blood supply to the brain.29,30 Furthermore, some of these medical problems, including oxida-tive stress,31-33 metal toxicity,34,35 decreased methylation,36 mitochondrial dysfunction,37 and cerebral hypoperfusion38 have also been described in children with ADHD (Table 1). A review of approximately 4,000 records of children evaluated at our centers with predominately ASD diagnoses affirms the frequent co-occurrence of these underlying biological problems. Certainly these factors adversely impact neurodevelopment, immune function, and gastrointestinal (GI) health. The difficulties of evaluating the synergistically negative effects of these abnormalities in the pediatric population will likely preclude controlled interventional studies. Given the broad array of pediatric sub-specialties typically involved in these disorders (e.g., neurology, psychiatry, gastroenter-ology, immunology, and toxicology), it is a daunt-ing task for a single medical provider to align the skills and expertise necessary to integrate appro-priate care. Importantly, the presence of behavioral symptoms consistent with autism or ADHD does not necessarily preclude the recovery from or diminishing of these symptoms through the treatment of underlying pathophysiologies. In fact, recovery from autism, although not widely published, is commonly observed. Consistent with the authors’ observations of recovery assisted by biomedical interventions, O’Hara and Szakacs recently published the recovery from autism in one child.39 Other investigators have also reported recovery of 38 children with autism primarily through Applied Behavioral Analysis (ABA) Therapy.40 In the ABA literature, normalization of IQ and behavior is consistently reported,41-43 which implies reversibility of the underlying condition in at least some children.
Despite numerous challenges, children with these medical disorders deserve the hope of a better quality of life and the possible recovery from the core features of their disorders. Fortunately,
the progress made in defining the underlying processes of these conditions has led to numerous published studies that define clinically useful and commercially available biomarkers for both ASD and ADHD. Based on this body of medical litera-ture, as well as the authors’ extensive clinical experience over the past 12 years, unless the underlying major biological disruptions are addressed, they will perpetuate autistic and ADHD symptoms, adversely impact the child’s develop-ment, and prevent potential improvements in symptoms and overall functioning.
Researchers have examined the use of biomark-ers in children with ASD for over 20 years.44 Chakravarty defines a biomarker as “a characteris-tic that is objectively measured and evaluated as an indicator of normal biological or pathogenic processes or pharmacological responses to a therapeutic intervention.”45 Biomarkers do not need to be exclusive to a particular disorder. For example, oxidative stress is reported as a common feature of vascular diseases46 as well as many CNS disorders, including ASD, schizophrenia,
Alzheimer’s disease, HIV-dementia, and parkinson-ism.47,48 Oxidative stress therefore represents a common etiopathological factor of diverse clinical conditions, but cannot be used as a specific diagnostic requirement of any exclusive disorder. It is medically reasonable to assume that the relief of oxidative stress would be associated with diminu-tion of some features of these disorders, or at least
Table 1. Biomedical Problems Described in ASD and ADHD
BIOMEDICAL PROBLEM
Oxidative stress
Decreased methylationand transsulfuration
Mitochondrial dysfunction
Metal toxicity
Intestinal dysbiosis
Immune dysregulation / in�ammation
Cerebral hypoperfusion
ASD
Yes
Yes
Yes
Yes
Yes
Yes
Yes
ADHD
Yes
Yes
Yes
Yes
No
No
Yes
Key words: autism, autistic, ADD, ADHD, ASD, attention deficit, biomarkers

amr®
17 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
prevent or slow their progression. The biomarkers described in this article are not exhaustive or all inclusive, but are intended to target the core biomedical issues frequently observed in children with ASD or ADHD. Utilizing biomarkers is of greater importance in individuals with ASD, because they typically cannot adequately communi-cate their symptoms. As with any medical diagnos-tic evaluation, a clinician must rely on the history, physical examination, and relevant biomarkers for proper diagnosis and treatment.
Basic BiomarkersSeveral abnormalities described in children with
ADHD and ASD that can be screened with simple laboratory tests are summarized in Table 2.
➧ CBC: A complete blood count (CBC) with differential can be performed. Abnormalities described in some children with ASD include a high blood monocyte count49 and abnormal lymphocyte function.50-53 The CBC can also provide insights into allergies, anemia, and platelet counts. Platelet elevation, a nonspecific marker of immune activation, were observed in
ASD and were responsive to biomedical intervention.162
➧ CMP: A comprehensive metabolic panel (CMP) that includes liver and kidney testing is helpful. High albumin has been described in some children with ASD.54 Elevations in transami-nases can be associated with mitochondrial disorders and, along with other markers, may support the need for skin or muscle biopsy for a more definitive diagnosis.55,56 Determining renal and hepatic function prior to intervention with medications represents a reasonable clinical protocol.
➧ Magnesium: Magnesium (Mg) deficiency, which can be measured by any standard laboratory, occurs in up to 95 percent of children with ADHD.57 In a six-month, controlled study of 75 children with ADHD and magnesium deficiency (documented by low serum and red blood cell [RBC] magnesium) who all received standard pharmacological treatments for ADHD, a significant decrease in hyperactivity was observed with the addition of oral magnesium (200 mg/day) in 50 children compared to the 25 children who did not receive magnesium (p<0.05).58 In a six-month, controlled study of 33 children with ASD, the use of vitamin B6 (0.6 mg/kg/day) and magnesium (6 mg/kg/day) led to a significant reduction of autistic symptoms in 70 percent of the children (p<0.0001), including improvements in social interaction, communication, and stereotypies; no adverse effects were observed. When the B6/Mg treat-ment was stopped the undesired behavior returned within several weeks.59
➧ Zinc: Zinc can be measured by any standard laboratory. In one study of 48 children with ADHD and 45 typically developing children, mean serum zinc levels were significantly lower in the ADHD group (p<0.001).60 Other investi-gators studied a group of 48 children with ADHD and observed that lower serum zinc levels correlated with parent and teacher rankings of inattention (p=0.004 for both).61 In a controlled study of 45 autistic children compared to 41 typically developing children, plasma and RBC zinc levels were significantly lower in the autism group (p<0.05).62
➧ Other minerals: One study reported that children with ASD and pica had lower hair chromium.63 Low hair iodine and lithium levels have also been described in some children with ASD.63 A study of 20 children with autism and 15
Table 2. Basic Biomarkers and Clinical Significance
Basic Biomarker
Complete blood count
Comprehensive metabolic
Magnesium
Zinc
Other minerals
Iron
Hypothyroidism
Cholesterol
Testosterone
Clinical Signi�cance
Anemia, abnormal white count, platelet count
Electrolyte, liver, or renal abnormalities
De�ciency associated with hyperactivity
De�ciency associated with inattention
Low chromium associated with pica; low lithium associated with irritability
De�ciency associated with insomnia, lower IQ, attention problems
De�ciency associated with developmental delay and inattention
De�ciency associated with irritability
Increase associated with aggression

amr®
Volume 15, Number 1 Alternative Medicine Review 18Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
typically developing children reported signifi-cantly lower RBC selenium (p<0.0006) in the autism group.64 A reasonable method to determine mineral content is to assess packed red blood cell (PRBC) element concentrations, a technique that has been evaluated in the pediatric population.65
➧ Iron: Iron deficiency appears to be relatively common in ADHD;66 serum ferritin is low in many children with ADHD compared to typi-cally developing children.67,68 Iron deficiency characterized by low serum ferritin is also observed in many children with ASD.69,70 In a randomized, double-blind, placebo-controlled study of 23 ADHD children with serum ferritin levels less than 30 ng/mL, supplementation with ferrous sulfate (80 mg/day) over a 12-week period was well-tolerated and significantly improved ADHD symptoms (p<0.008) com-pared to no improvements in the placebo group.71 In an eight-week, open-label study of 33 children with ASD, supplementation with iron (6 mg/kg/day) significantly improved sleep and increased mean serum ferritin levels. The investigators suggested that children with ASD should be routinely screened for iron deficiency and recommended obtaining serum ferritin and iron levels.72
➧ Hypothyroidism: Hypothyroidism has been described in some children with ASD73 and ADHD;74 therefore, screening for hypothyroid-ism with a blood test for thyroid-stimulating hormone is recommended. Normal ranges for children vary among laboratories. It is not unusual to see two standard deviations signify a 10-fold difference in TSH levels. TSH levels at the mean or lower are considered optimal by these authors. Elevated TSH may be a reflection of iodine deficiency, an easily corrected nutri-tional problem.
➧ Cholesterol: A subset of children with ASD have abnormally low cholesterol levels, with one study demonstrating that 19 percent of children had a cholesterol level below 100 mg/dL.75 Cholesterol levels below 145 mg/dL have been associated with a three-fold increased risk of aggression and suspension from school in typically developing children.76
➧ Testosterone: A small percentage of children with ASD may have elevated testosterone levels.77 Elevated fetal testosterone levels also appear to be associated with a higher likelihood of developing ASD.78 Thus, measuring levels of
serum testosterone and related androgens may be indicated. In the authors’ clinical experience, the typical features of precocious puberty may not be present in all hyperandrogenic states. If indicated by height percentiles, a wrist radio-graph for bone age may also be helpful. A child with a bone age that is advanced more than two standard deviations, when combined with elevated androgens, should be considered for a complete precocious puberty evaluation.
Oxidative Stress Biomarkers Oxidative stress is a common finding in many
children with ASD12,13,47 and ADHD.31-33 Glutathione is the primary intracellular antioxidant and has been shown to limit mercury-induced neurotoxic-ity.79 Impaired glutathione production contributes to oxidative stress, which may delay the clearance of heavy metals and certain xenobiotics.80 In two prospective studies, over 50 percent of children with ASD had significantly lower plasma levels of glutathione and cysteine (p<0.001 for both) compared to typically developing children.12,14 James et al hypothesized that because of these findings, “autistic children would be expected to have difficulty resisting infection, resolving inflammation, and detoxifying environmental contaminants.”12 The following biomarkers, summarized in Table 3, can be measured to assess the level of oxidative stress.
➧ Reduced glutathione (GSH) and oxidized glutathione (GSSG):12 An Internet search of laboratory providers for this special testing found several commercially available companies capable of measuring these valuable markers. Measuring total glutathione along with GSSG and/or GSH will help determine the patient’s oxidation status.
➧ Levels of major antioxidant proteins in the serum (standard blood tests): Transferrin (an iron-binding protein) and ceruloplasmin (a copper-binding protein) are antioxidant proteins significantly decreased in children with ASD compared to typically developing chil-dren.13,81 One study reported that lower levels of these proteins were associated with regression and loss of previously acquired language skills in children with ASD.81 Results of such testing should be viewed with caution, however, since a variety of conditions influence the levels of either protein, making interpretation challenging.

amr®
19 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
➧ Blood ammonia and lactate (lactic acid): Ammonia is derived from the deamination of the amine group of amino acids by gut bacteria or the liver. The process of detoxifying ammonia via the urea cycle is metabolically expensive and expends three valuable, high-energy ATP molecules for every ammonia molecule pro-cessed. Hyperammonemia is more toxic for children than adults and can lead to permanent CNS damage.82
➧ Lactate is a by-product of the anaerobic metabo-lism of glucose. Typically, clinicians look for serum lactate levels greater than 2.5 mM/L for support of mitochondrial disease,83 although lactate levels can be normal in some mitochon-drial diseases.84 Lactate can be elevated in a variety of disorders other than ASD, but levels above 2 mM/L support mitochondrial dysfunc-tion when proper sampling techniques are followed. When possible, lactate and ammonia levels should be drawn without a tourniquet after the venipuncture or IV is started. Ideally, the child should be calm or sedated during the
process and may require premedication to obtain accurate results. Increased lactate levels may require confirmation with a separate blood draw. Elevation in either ammonia or lactate likely reflects a state of mitochondrial hypofunc-tioning in ASD15,85,86 and are standard tests at all hospitals. The blood used for ammonia and lactate testing requires immediate icing once placed in the specimen tubes. As a precaution-ary note when interpreting the meaning of elevated serum lactate, the authors have observed elevations after high-dose probiotic supplementation with Lactobacillus species, secondary to the bacterial metabolic contribu-tion to blood lactate levels.
➧ Serum carnitine profile: Carnitine levels are often lower in children with ASD15 and may reflect mitochondrial dysfunction and nutri-tional deficiencies. This test should be routine for any child with hypotonia or other signs and symptoms of mitochondrial dysfunction.
➧ Urinary 8-hydroxyguanine (8-OHG): This is a marker of RNA oxidation in the mitochondria and cell cytoplasm and is an easily obtained urinary marker useful for evaluating intracel-lular oxidative stress.87 Although the DNA marker of oxidative stress (8-hydroxy-2-deoxy-guanosine, 8-OHdG) is not elevated in most cases of ASD,88 it is elevated in some children with ADHD.33 As far as the authors are aware, 8-OHG testing is currently commercially available only from Laboratoire Philippe Auguste (Paris, France), although several U.S. laboratories can measure DNA oxidation.
➧ Urinary isoprostane: This is a marker of fatty acid oxidation that reflects cell membrane (extracellular) oxidative stress and is elevated in many children with ASD when compared to controls.88 This test is available from Laboratoire Philippe Auguste (Paris, France).
➧ Vitamin D: Deficiency of vitamin D is an emerging concern among many practitioners. It is interesting to note that vitamin D deficiency and autism share the common qualities of enlarged brain size and ventricles.89,90 The authors have also observed increased rates of autism in some darker-skinned populations and insufficient vitamin D may be partly respon-sible.91 Vitamin D status is important to consider because of its role in reducing oxidative
Table 3. Oxidative Stress Biomarkers
Biomarker
Reduced and oxidized glutathione
Antioxidant proteins: transferrin and ceruloplasmin
Ammonia and lactic acid
Carnitine pro�le
Urinary 8-hydroxyguanine
Urinary isoprostane
Vitamin D
Clinical Signi�cance
Low levels associated with impaired detoxi�cation and increased oxidative stress
Low levels associated with regression in children with autism
High levels are nonspeci�c markers of mitochondrial dysfunction
Low levels associated with mitochondrial dysfunction
Increased levels associated with mitochondrial dysfunction and oxidative stress
Increased levels consistent with fatty acid oxidation
Low levels associated with lowered glutathione levels and increased oxidative stress

amr®
Volume 15, Number 1 Alternative Medicine Review 20Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
stress through both GSH production and as an antioxidant itself.92-94 Vitamin D panels are available from many commercial laboratories. When evaluating a potential deficiency state, a decrease of the 25-hydroxycholecalciferol form is diagnostic of inadequate dietary intake.
Methylation Capacity and Transsulfuration Biomarkers
Methylation and transsulfuration pathways represent core areas of metabolic activity. These connected and interdependent pathways generate required methyl-donors via the conversion of methionine to S-adenosylmethionine (SAMe), which in turn donates its methyl group to catechol-amine neurotransmitters, cell membranes, DNA, and other body chemicals or structures. The end product is homocysteine, which is merely demeth-ylated methionine. Excess homocysteine is required to generate cysteine, the rate-limiting step for the production of the vital and dominate intracellular antioxidant glutathione. An oxidized intracellular condition would inhibit the methio-nine cycle, making the reducing capacity of glutathione critical to its own production. It is well accepted that neurons are extremely sensitive to oxidation, making GSH essential for neuronal survival.95 James et al documented methylation and transsulfuration disruption in a majority of children with ASD.12,14,96 Deficiency, as measured by decreased levels of fasting plasma cysteine or its dimer (cystine), may predict improvement with methylcobalamin injections and/or folinic acid.14,96 The use of 5-methyltetrahydrofolate (5-MTHF) may also be useful. Logically, deficits in this pathway could be the result of nutritional deficien-cies of methionine (an essential amino acid), folate, and/or vitamin B12 along with other vitamin cofactors. As mentioned, deficient methylation-transsulfuration could also be the result of increased oxidative stress. The following biomark-ers, summarized in Table 4, can be checked to assess methylation and transsulfuration pathways.
➧ Fasting plasma cysteine or cystine: Cysteine is the sulfur-containing amino acid that acts as the rate-limiting step in the production of GSH, the key intracellular defense against oxidative stress. Cysteine and GSH are also involved in defending against heavy metal and xenobiotic toxicity.
➧ Fasting plasma methionine: Methionine, an essential amino acid, is the main methyl donor via the intermediary SAMe.
➧ Plasma sulfate: Sulfate is often low in children with ASD.97 Several studies report that the conjugation of sulfate to acetaminophen (an indicator of deficient phase 2 hepatic sulfation-detoxification) is impaired in children with ASD.98-100 Deficient sulfation in turn may impair the detoxification of many chemicals and metabolites, such as phenolic xenobiotics that could adversely impact brain function.101
Immune BiomarkersIt is difficult to obtain a direct measurement of
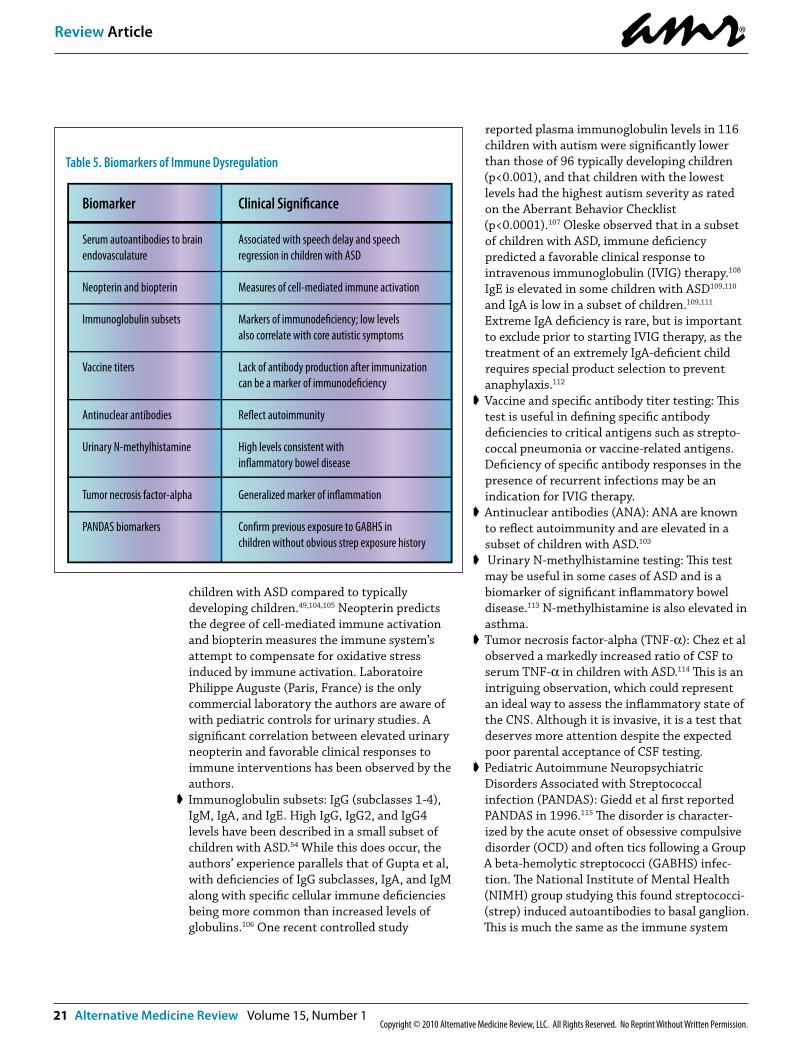
brain inflammation; even cerebral spinal fluid (CSF) studies offer inconsistent findings. Given the literature demonstrating the presence of both cerebral oxidation and inflammation in ASD, a pattern of up-regulation of cellular immunity combined with other features of immune dysregu-lation can help form a clinical picture. The follow-ing biomarkers, summarized in Table 5, may reflect this immune dysregulation.
➧ Serum autoantibodies to brain endovascula-ture:102,103 This test is performed exclusively at the Neuromuscular Laboratory at Washington University in St. Louis, MO. Details related to specimen handling and requirements are available at their website. In the authors’ practice, the presence of either IgG or IgM antibodies to brain endovasculature is common (exceeding 50% of ASD) and predicts speech delay or regression. It is consistent with and probably (although unconfirmed) a marker for autoimmune vasculitis of the brain, as depicted in the brain immune studies of Vargas et al.28
➧ Neopterin and biopterin: These biomarkers are often elevated in the urine and monocytes of
Table 4. Biomarkers of Methylation and Transsulfuration
Biomarker
Cysteine or cystine
Methionine
Sulfate
Clinical Signi�cance
Low levels associated with impaired glutathione production
Low levels associated with impaired glutathione production
Low levels associated with impaired detoxi�cation
amr®
21 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
children with ASD compared to typically developing children.49,104,105 Neopterin predicts the degree of cell-mediated immune activation and biopterin measures the immune system’s attempt to compensate for oxidative stress induced by immune activation. Laboratoire Philippe Auguste (Paris, France) is the only commercial laboratory the authors are aware of with pediatric controls for urinary studies. A significant correlation between elevated urinary neopterin and favorable clinical responses to immune interventions has been observed by the authors.
➧ Immunoglobulin subsets: IgG (subclasses 1-4), IgM, IgA, and IgE. High IgG, IgG2, and IgG4 levels have been described in a small subset of children with ASD.54 While this does occur, the authors’ experience parallels that of Gupta et al, with deficiencies of IgG subclasses, IgA, and IgM along with specific cellular immune deficiencies being more common than increased levels of globulins.106 One recent controlled study
reported plasma immunoglobulin levels in 116 children with autism were significantly lower than those of 96 typically developing children (p<0.001), and that children with the lowest levels had the highest autism severity as rated on the Aberrant Behavior Checklist (p<0.0001).107 Oleske observed that in a subset of children with ASD, immune deficiency predicted a favorable clinical response to intravenous immunoglobulin (IVIG) therapy.108 IgE is elevated in some children with ASD109,110 and IgA is low in a subset of children.109,111 Extreme IgA deficiency is rare, but is important to exclude prior to starting IVIG therapy, as the treatment of an extremely IgA-deficient child requires special product selection to prevent anaphylaxis.112
➧ Vaccine and specific antibody titer testing: This test is useful in defining specific antibody deficiencies to critical antigens such as strepto-coccal pneumonia or vaccine-related antigens. Deficiency of specific antibody responses in the presence of recurrent infections may be an indication for IVIG therapy.
➧ Antinuclear antibodies (ANA): ANA are known to reflect autoimmunity and are elevated in a subset of children with ASD.103
➧ Urinary N-methylhistamine testing: This test may be useful in some cases of ASD and is a biomarker of significant inflammatory bowel disease.113 N-methylhistamine is also elevated in asthma.
➧ Tumor necrosis factor-alpha (TNF-α): Chez et al observed a markedly increased ratio of CSF to serum TNF-α in children with ASD.114 This is an intriguing observation, which could represent an ideal way to assess the inflammatory state of the CNS. Although it is invasive, it is a test that deserves more attention despite the expected poor parental acceptance of CSF testing.
➧ Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infection (PANDAS): Giedd et al first reported PANDAS in 1996.115 The disorder is character-ized by the acute onset of obsessive compulsive disorder (OCD) and often tics following a Group A beta-hemolytic streptococci (GABHS) infec-tion. The National Institute of Mental Health (NIMH) group studying this found streptococci- (strep) induced autoantibodies to basal ganglion. This is much the same as the immune system
Table 5. Biomarkers of Immune Dysregulation
Biomarker
Serum autoantibodies to brain endovasculature
Neopterin and biopterin
Immunoglobulin subsets
Vaccine titers
Antinuclear antibodies
Urinary N-methylhistamine
Tumor necrosis factor-alpha
PANDAS biomarkers
Clinical Signi�cance
Associated with speech delay and speech regression in children with ASD
Measures of cell-mediated immune activation
Markers of immunode�ciency; low levels also correlate with core autistic symptoms
Lack of antibody production after immunization can be a marker of immunode�ciency
Re�ect autoimmunity
High levels consistent with in�ammatory bowel disease
Generalized marker of in�ammation
Con�rm previous exposure to GABHS in children without obvious strep exposure history

amr®
Volume 15, Number 1 Alternative Medicine Review 22Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
forming cross-reactive antibodies between GABHS and heart valves in rheumatic heart disease. Both OCD and tic exacerbations are often observed in the ASD population, but cultures are often negative or there is no clear antecedent strep infection. This makes the diagnosis of PANDAS challenging since, apart from the clinical picture of a positive throat culture preceding the onset of new OCD and tic behaviors, there is no clinically reliable diagnos-tic testing available. The basal ganglion autoanti-body tests are not commercially available and traditional antibody testing for strep (anti-streptolysin-O and anti-DNase B) can be deceptive since many healthy children carry high titers for a long time after infection or during strep outbreaks at school (personal communication from Sue Swedo, MD, NIMH). Although treatment for this condition is controversial, prolonged courses of antibiotics have been proposed116 and in the authors’ experience may be helpful in select ASD-PANDAS cases. The group at NIMH is also investigating novel treatments, including immunomodulatory therapies such as therapeu-tic plasma exchange (TPE) and IVIG, with some benefits noted.117 The authors, although not experienced with TPE, have found monthly infusions of IVIG are needed for extended periods of time in order to see improvements when ASD and PANDAS-like symptoms occur together.
Gastrointestinal BiomarkersGastrointestinal inflammation has been
described in many children with ASD.27,118,119 Other GI problems (reflux, constipation, food sensitivi-ties, and abnormal flora) are also common. For example, Horvath et al reported significant GI symptoms in a study of 36 autistic children referred to a gastroenterologist, including reflux esophagitis (69%), chronic gastritis (42%), chronic duodenitis (67%), and low intestinal carbohydrate digestive enzyme activity (58%).120 Another study of 50 children with ASD and 50 typically develop-ing children reported that 70 percent of the ASD group had a history of GI problems compared to 28 percent of the control group (p<0.001).121 Common GI problems found in one study of 112 autistic children included diarrhea (28%), gaseousness (60%), bloating (38%), abdominal pain (38%), and fecal impaction (19%). Importantly, 80 percent of the children with autism had at least one GI-related
problem and these problems were significantly more common compared to 44 typically developing siblings.122 Several studies also report dysbiosis in children with ASD, including significant over-growth of Clostridia species22-24 and yeast (Candida albicans)123 in the GI tract compared to typically developing children. The following biomarkers, summarized in Table 6, can be obtained to assess these problems.
➧ Fecal testing: Calprotectin,124,125 eosinophil X,126 and S100A12127 are markers of GI inflammation. While these tests are significant when elevated, a negative study may not necessarily exclude significant pathology, so several studies may be required to rule out inflammatory bowel issues. Calprotectin did not correlate well with ASD symptoms in one small study;128 however, in the authors’ ASD population, fecal calprotectin is frequently elevated above 50 mcg/g and is sometimes greater than 100 mcg/g.
➧ Intestinal permeability: Abnormal absorption of lactulose and mannitol, used to determine altered GI permeability, is a reported positive finding in over 40 percent of children with ASD.129 However, this is not a consistent finding in the authors’ practice population. Increased intestinal permeability could not be reproduced in another, albeit smaller, population studied.130
➧ Urinary organic acids: Thousands of these laboratory assessments have been performed on children with ASD at the authors’ centers over the past 12 years and most demonstrate abnormalities in the citric acid cycle, which may be markers of mitochondrial dysfunction. Abnormal levels of citric acid and succinate are observed in most children when screened for urinary organic acids. Abnormally high levels of formiminoglutamic acid, which would be consistent with a functional folate deficiency (despite normal blood levels), and 3-methylhisti-dine (a metabolite of muscle catabolism in the presence of negative nitrogen balance) are commonly observed in patients prior to the onset of biomedical interventions such as nutritional supplementation, dietary changes, and medications. It is also common to find increased levels of methylmalonic acid131 despite elevated serum B12, which would seem to indicate impaired utilization of this vitamin.

amr®
23 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
Several commercial laboratories offer organic acid testing with expanded evaluation beyond the typical testing. These expanded panels include investigation of bacterial and fungal metabolites that would reflect intestinal dysbiosis. In the authors’ clinical experience, elevated yeast and anaerobic bacteria biomark-ers in the urine appear to correlate with clinical responses to antifungal and/or antibacterial interventions. This is supported by the observa-tion that oral vancomycin has been demon-strated to create short-term behavioral improve-ment in 80 percent of ASD children studied.132 Currently, a study has been approved and funded to investigate the clinical response from fluconazole, a commonly prescribed antifungal observed to have clinical benefits in ASD. In addition, quantitative analysis of bacterial DNA in the gut has been used in children with ASD22 and will hopefully be routine in the future. The levels of beneficial bacteria compared to pathogenic bacteria in the GI tract are a major determinant of intestinal immune function.133
➧ Gluten intolerance: Individuals with celiac disease are more likely to develop neurological disorders such as ADHD and developmental delay, hypotonia, and learning disorders;134 thus, a celiac panel (available from major medical laboratories) can be evaluated. A 2008
retrospective study of 150 children with ASD found a three-fold higher prevalence of celiac disease than in the general pediatric population. The investigators suggested all children with ASD should be screened for celiac disease, regardless of the presence of GI problems.135
➧ Food allergy: In an eight-week study of 36 children with autism, the elimination of allergic foods (determined by a positive skin test) led to significant improvements in autistic behaviors (p<0.05), and worsening of these behaviors when the allergic foods were reintroduced.136 Serum IgE and IgG testing to specific food antigens may be helpful in some cases. Several commercial laboratories now offer large panels of IgG testing of various food antigens. Jenkins and Vickers studied this with a laboratory in the United Kingdom but found inconsistent and unreliable results.137 Oehling et al, however, found in vitro IgG4 and IgE food testing helpful in atopic children and called skin testing into question for its decreased specificity.138 This is an area that remains complex and controversial, while requiring the combined use of clinical skills, elimination and reintroduction food challenges, and appropriate laboratory interpre-tation to provide useful insights and interventions.
Table 6. Biomarkers of Gastrointestinal Dysfunction
Biomarker
Calprotectin, eosinophil-X, S100A12
Intestinal permeability
Organic acid testing
Gluten intolerance testing (Celiac panel)
Food allergy panel
Stool culture and microscopic evaluation
Clinical Signi�cance
Markers of in�ammatory bowel disease and food allergy related bowel in�ammation, as well as infection or parasitosis
Increased permeability consistent with bowel in�ammation
Can indicate functional vitamin B12 and folate de�ciency as well as intestinal dysbiosis
Could indicate a need for further formal testing for celiac disease
Removal of allergic foods associated with improved autistic symptoms in some children
Can identify intestinal dysbiosis, parasites, and pathogens

amr®
Volume 15, Number 1 Alternative Medicine Review 24Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
➧ Stool culture and microscopic investigation: Screens for parasites, yeast, and abnormal bacteria are particularly important in cases associated with unexplained diarrhea, bloating, anal itching or redness, reflux, or apparent abdominal pain. Treatment of abdominal pain in children with ASD has been shown to improve certain core autistic behaviors.139
Heavy Metal BiomarkersWhile lead surveillance is well accepted in cases
of mental retardation and certain at-risk popula-tions, the threat posed by mercury receives less attention from most practitioners. This occurs despite cord blood evidence that one of six children in the United States is born with exposure to levels of mercury high enough to cause impairments in IQ.140 Several studies report that lead exposure is associated with hyperactivity and ADHD21,34,141-143 as well as ASD.21,144 In a study of 277 children, hair lead levels significantly correlated with ADHD.34 In another study of 4,704 children, 4.2 percent of whom had ADHD, blood lead levels of 2-5 µg/dL increased the risk of ADHD four-fold (95% confidence interval (CI): 1.2-14.0).35 In a study of 150 children with blood lead levels under 3.5 µg/dL, lead levels were significantly higher in children with ADHD compared to controls (p<0.05) and were significantly associated with hyperactivity and impulsivity.143
In a study of 52 children with ADHD and 59 typically developing children, mean blood mercury levels were associated with ADHD; a blood mercury level above 29 nmol/L was associated with a 9.7-fold (95% CI: 2.6-36.5) increased risk of ADHD.145 With specimens collected in the late 1990s through 2001, Bradstreet et al demonstrated a six-fold increase in mercury after a three-day provocation with dimercaptosuccinic acid (DMSA, a chelator of lead and mercury) in 221 children with ASD compared to 18 age-matched typically developing children (p<0.005).19 In a later but smaller study of a three-dose DMSA provocation followed by 24 hours of collection, Soden et al claimed to find no difference between children with autism and controls in urinary output of heavy metals.146 However, given the small population in this study (15 children with ASD compared to 221 in the Bradstreet et al study) and concerns regard-ing the statistical methods, it is difficult to assess the significance of the Soden study. In a separate case report, exposure to mercury from a broken thermometer was associated with the development
of autistic features in one child.147 Furthermore, several epidemiological studies correlate environ-mental mercury exposure with the prevalence of ASD.148-151 More recently, Adams et al demonstrated a significant correlation between the relative level of urinary excretion of heavy metals, including mercury, after a DMSA provocation and the severity of autism.17
In situations where there is chronic, low level exposure to heavy metals, a history of exposure and clinical signs and symptoms are the key features of diagnosis. Past heavy metal intoxication is difficult to establish with present blood, hair, or urinary levels, since metals quickly move into preferred target organ sites like the brain, liver, heart, and kidneys, as is the case with organic mercury. Despite this diagnostic dilemma, the following biomarkers, summarized in Table 7, may be useful to assess heavy metal body burden.
➧ Lead: Blood lead levels should be tested in children with ASD who also have pica.152 Furthermore, given the association between lead and an increased risk of ADHD, children with ADHD should also be tested. Intellectual impairment in children with blood lead concen-trations below 10 mcg/dL has been docu-mented.153 This would seem to indicate any lead exposure is a potential threat to the IQ of developing children. Since it is well accepted that lead leaves the blood fairly rapidly to deposit into organs and the bone matrix, blood levels only indicate relatively recent
Table 7. Biomarkers of Heavy Metals
Biomarker
Blood lead
Packed RBC test
Urinary fractionatedporphyrins
Heavy metal challenge
Clinical Signi�cance
Increased levels associated with recent exposure
Can re�ect recent exposure to toxic metals such as mercury, arsenic, lead, and others
Increased levels associated with increased body burden of toxic metals and other xenobiotics
Increased urinary output of metals after chelator administration associated with increased body burden of toxic metals

amr®
25 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
environmental exposure154 and blood or urine porphyrin levels may be better indicators of past exposure.155
➧ Packed RBC levels of minerals and toxic metals (especially mercury, lead, and arsenic): RBC levels reflect ongoing exposure or rapid turnover from tissue reservoirs, as is the case when lead from prior exposure is liberated from bone during bone growth spurts. Rather than reflecting past exposures, these measurements tend to reflect the child’s current environmental exposures and relative efficiency of naturally eliminating these heavy metals. A full mineral and metal panel test of PRBCs is helpful since it measures nutritional minerals as well as toxic metals.
➧ Urinary fractionated porphyrins: These molecu-lar precursors of the heme structure have been found to be abnormally elevated in five studies of children with ASD18,20,156-158 and are suitable to assess the current body burden of metals.159 Most commercial laboratories are not set up to determine precoproporphyrin (pCP, also known as ketoisocoproporphyrin or KICP) levels.20,160 Increased pCP is the more sensitive indicator for mercury burden.159 If porphyrins are elevated compared to controls, then a post-chelation challenge with a six-hour urine toxic metal assay as described by Bradstreet et al19 should be considered. In the authors’ experience, oxidative stress is further capable of triggering an abnormal prophyrin response, apart from apparent heavy metal intoxication.
➧ Heavy metal challenge: This test is performed with a six-hour urine collection for the determi-nation of heavy metals following a dose of an appropriate metal chelator.19 Six hours is typically long enough since most studies
demonstrate that the majority of urinary metal excretion after chelation occurs during the first six hours. Given the difficulty of collecting urine specimens from many children, a first morning urine collection after a bedtime dose of a chelator may be an alternative way to test relative body metal burden.
Biomarker Directed TreatmentGeneral Concepts of Biomedical Interventions
The fundamental goal of any integrative medical intervention is to create an ideal physiological state for optimal functioning, healing, growth, and development. Defining and treating the medical conditions or co-morbidities of ASD or ADHD would be expected to lead clinicians to specific interventions. Equally, using these biomarkers would be expected to gauge the efficacy of selected therapies. This is the same logic that medicine applies to measuring serial blood glucose levels during insulin therapy for diabetes. It follows then (by example) that the detection of oxidative stress would lead to antioxidant therapy, and a finding of inflammation would lead to some form of anti-inflammatory therapy. The expectation would then be to monitor the abnormal biomarker(s) while adjusting therapy to normalize the abnormal physiology.
Five general areas should be considered for biomedical interventions (Table 8), for which there is a great deal of overlap and interaction: (1) detoxification, (2) restoration of healthy gut flora, (3) reduction of oxidative stress, (4) normalization of immune function throughout the body, and (5) supplementation with adequate nutrients and micronutrients as well as enzymes (when neces-sary) to ensure proper digestion.
Detoxification requires the elimination of environmental toxicants (e.g., heavy metals, petrochemicals, and other xenobiotics) from both the external and internal environment. This is a complex process beyond the scope of this article, involving elimination of dietary sources of mercury, lead surveillance and removal (within the home, school, or other frequented sites), and heavy metal chelation using one or more of the available substances known to bind metals in children with objective evidence of metal toxicity. The use of organic foods and the elimination of indoor pesticides are encouraged wherever possible as additional measures to reduce toxic exposure. As noted previously, Adams et al demonstrated a correlation between toxic metal burden and the
Table 8. General Areas of Biomedical Intervention
Biomedical Intervention
Detoxi�cationRestoration of healthy gut �oraReduction of oxidative stressNormalization of immune functionNutritional supplementation

amr®
Volume 15, Number 1 Alternative Medicine Review 26Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
severity of autism.17 In the later phases of that study, they also demonstrated significant reduc-tions in many of the core features of autism over a short course of DMSA treatment.161 The exact mechanism whereby a short course of DMSA treatment might improve autism symptomatology is uncertain, but it may involve changes in thiol metabolism or a reduction in oxidative stress.162
Biomedical interventions also focus on the creation of a healthy intestinal ecosystem. While this has not received much attention from main-stream medicine until recently, it has been a cornerstone of integrative medicine and naturopa-thy for decades. The internal ecosystem requires healthy flora and the elimination of pathogenic microbes. It also requires the ability to digest complex food molecules into simple mono-amino acid and monosaccharide forms so proper absorp-tion can take place. For example, some investiga-tors have noted improvements in children with ASD using probiotics163 and digestive enzymes.164
The process of supporting individual health also requires the elimination of excessive free radicals (which lead to oxidative stress) and the simultane-ous reduction of excessive immune activation, which is often the driving force for free radical production. Multiple studies have shown antioxi-dants such as vitamin C,165 carnosine,166 carni-tine,167 and methylcobalamin injections along with folinic acid96 improve certain behaviors in children with ASD. Likewise, some antioxidants, including pycnogenol,168 carnitine,169 and zinc170 improve behaviors in children with ADHD.
Since a variety of physiological systems may be malfunctioning at the same time, the utilization of nutrients is often impaired at multiple levels. For this reason, the initial use of nutrient doses higher than the Recommended Daily Allowance (RDA) may be required. Once biochemical systems begin to function normally and inflammation and oxidation are normalized, supplementation can usually be reduced to more traditional levels. For example, studies in children with ASD171 and ADHD172 report behavioral improvements with the use of a multivitamin/mineral complex.
Given the overwhelming significance of poten-tial CNS inflammation in many children with autism, developing an effective interventional strategy for this condition is a priority. Unfor-tunately, no therapeutic approach has been documented to reduce brain inflammation in ASD. However, Chez et al reported that children with
autism who received autoimmune treatments (such as steroids or IVIG) had much lower CSF TNF-α levels compared to children who did not receive such treatments.114 Despite the lack of rigorous scientific investigation, the need to treat CNS inflammation justifies reasonable efforts to abate the disease process. Families should be given appropriate informed consent for any potential innovative approaches. In the authors’ clinical experience and in the published literature, the use of anti-inflammatory medications173,174 and other novel immune-modifying agents (e.g., IVIG) appear beneficial for use in many cases of ASD.108,109,175,176 Furthermore, an integrative treatment plan may draw on numerous natural substances (e.g., curcumin – a well defined anti-inflammatory). The biomarkers discussed in this article can help establish and monitor the sufficiency of the treatment regimens selected by the practitioner.
An in-depth discussion of the biomedical treatments available for treating ASD is beyond the scope of this article, but a recent review outlines many of the potential biomedical treatment options in ASD including nutritional supplementa-tion, diet, medication, and non-biological treatments.175
ConclusionsBoth ASD and ADHD are currently diagnosed
using only behavioral criteria. This article reviews evidence that ASD is a multifaceted biomedical disorder characterized by oxidative stress, decreased methylation capacity, limited transsulfu-ration production of cysteine and GSH, mitochon-drial dysfunction, intestinal dysbiosis, increased toxic metal burden, cerebral hypoperfusion, and complex immune dysregulation characterized by both a unique inflammatory bowel disease and activation of neuroglial cells. Children with ADHD also share many of these same underlying features. It seems clear that successful treatment of ASD and ADHD requires clinicians to utilize a holistic approach that considers nutritional deficits, biochemical disruption, toxic exposures, and immunological abnormalities. The biomarkers discussed in this article are useful to guide the selection, efficacy, and sufficiency of biomedical interventions, which would likely include nutri-tional supplementation, dietary changes, and specific medications for treating GI pathogens and reducing inflammation.

amr®
27 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
Conflict of Interest DeclarationNone of the authors has a financial
relationship with the laboratories listed in this article. The authors treat indi-viduals with ASD and ADHD in clinical practice with many of the treatments reviewed in this article. Three authors are parents of children with ASD.
AcknowledgementThe authors express appreciation to
Bernie Rimland, PhD (posthumously), Jon Pangborn, PhD, and Sidney Baker, MD, for their longstanding efforts to raise awareness of the biomedical aspects of ASD and ADHD.
References1. Chakrabarti S, Fombonne E. Pervasive
developmental disorders in preschool children. JAMA 2001;285:3093-3099.
2. Bertrand J, Mars A, Boyle C, et al. Prevalence of autism in a United States population: the Brick Township, New Jersey, investigation. Pediatrics 2001;108:1155-1161.
3. Baird G, Charman T, Baron-Cohen S, et al. A screening instrument for autism at 18 months of age: a 6-year follow-up study. J Am Acad Child Adolesc Psychiatry 2000;39:694-702.
4. Kogan MD, Blumberg SJ, Schieve LA, et al. Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics 2009;124:1395-1403.
5. Fombonne E. Epidemiology of autistic disorder and other pervasive develop-mental disorders. J Clin Psychiatry 2005;66:3-8.
6. Baird G, Simonoff E, Pickles A, et al. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet 2006;368:210-215.
7. Centers for Disease Control and Prevention (CDC). Mental health in the United States: parental report of diagnosed autism in children aged 4-17 years – United States, 2003-2004. MMWR Morb Mortal Wkly Rep 2006;55:481-486.
8. Muhle R, Trentacoste SV, Rapin I. The genetics of autism. Pediatrics 2004;113:e472-e486.
9. Brown RT, Freeman WS, Perrin JM, et al. Prevalence and assessment of attention-deficit/hyperactivity disorder in primary care settings. Pediatrics 2001;107:E43.
10. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
11. Yao Y, Walsh WJ, McGinnis WR, Pratico D. Altered vascular phenotype in autism: correlation with oxidative stress. Arch Neurol 2006;63:1161-1164.
12. James SJ, Melnyk S, Jernigan S, et al. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am J Med Genet B Neuropsychiatr Genet 2006;141B:947-956.
13. Chauhan A, Chauhan V. Oxidat 0ive stress in autism. Pathophysiology 2006;13:171-181.
14. James SJ, Cutler P, Melnyk S, et al. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr 2004;80:1611-1617.
15. Filipek PA, Juranek J, Nguyen MT, et al. Relative carnitine deficiency in autism. J Autism Dev Disord 2004;34:615-623.
16. Rossignol DA, Bradstreet JJ. Evidence of mitochondrial dysfunction in autism and implications for treatment. Am J Biochem Biotech 2008;4:208-217.
17. Adams JB, Baral M, Geis E, et al. The severity of autism is associated with toxic metal body burden and red blood cell glutathione levels. J Toxicol 2009;2009:1-7.
18. Geier DA, Kern JK, Garver CR, et al. Biomarkers of environmental toxicity and susceptibility in autism. J Neurol Sci 2009;280:101-108.
19. Bradstreet JJ, Geier DA, Kartzinel JJ, et al. A case-control study of mercury burden in children with autistic spectrum disorders. J Am Physicians Surg 2003;8:76-79.
20. Nataf R, Skorupka C, Amet L, et al. Porphyrinuria in childhood autistic disorder: implications for environmental toxicity. Toxicol Appl Pharmacol 2006;214:99-108.
21. Eppright TD, Sanfacon JA, Horwitz EA. Attention deficit hyperactivity disorder, infantile autism, and elevated blood-lead: a possible relationship. Mo Med 1996;93:136-138.
22. Song Y, Liu C, Finegold SM. Real-time PCR quantitation of clostridia in feces of autistic children. Appl Environ Microbiol 2004;70:6459-6465.
23. Parracho HM, Bingham MO, Gibson GR, McCartney AL. Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children. J Med Microbiol 2005;54:987-991.
24. Finegold SM, Molitoris D, Song Y, et al. Gastrointestinal microflora studies in late-onset autism. Clin Infect Dis 2002;35:S6-S16.
25. Jyonouchi H, Geng L, Ruby A, Zimmerman-Bier B. Dysregulated innate immune responses in young children with autism spectrum disorders: their relationship to gastrointestinal symptoms and dietary intervention. Neuropsychobiology 2005;51:77-85.
26. Balzola F, Barbon V, Repici A, et al. Panenteric IBD-like disease in a patient with regressive autism shown for the first time by the wireless capsule enteroscopy: another piece in the jigsaw of this gut-brain syndrome? Am J Gastroenterol 2005;100:979-981.
27. Ashwood P, Anthony A, Torrente F, Wakefield AJ. Spontaneous mucosal lymphocyte cytokine profiles in children with autism and gastrointesti-nal symptoms: mucosal immune activation and reduced counter regulatory interleukin-10. J Clin Immunol 2004;24:664-673.
28. Vargas DL, Nascimbene C, Krishnan C, et al. Neuroglial activation and neuroinflammation in the brain of patients with autism. Ann Neurol 2005;57:67-81.
29. Ohnishi T, Matsuda H, Hashimoto T, et al. Abnormal regional cerebral blood flow in childhood autism. Brain 2000;123:1838-1844.

amr®
Volume 15, Number 1 Alternative Medicine Review 28Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
30. Ito H, Mori K, Hashimoto T, et al. Findings of brain 99mTc-ECD SPECT in high-functioning autism – 3-dimen-sional stereotactic ROI template analysis of brain SPECT. J Med Invest 2005;52:49-56.
31. Ross BM, McKenzie I, Glen I, Bennett CP. Increased levels of ethane, a non-invasive marker of n-3 fatty acid oxidation, in breath of children with attention deficit hyperactivity disorder. Nutr Neurosci 2003;6:277-281.
32. Ross MA. Could oxidative stress be a factor in neurodevelopmental disor-ders? Prostaglandins Leukot Essent Fatty Acids 2000;63:61-63.
33. Chovanova Z, Muchova J, Sivonova M, et al. Effect of polyphenolic extract, Pycnogenol, on the level of 8-oxogua-nine in children suffering from attention deficit/hyperactivity disorder. Free Radic Res 2006;40:1003-1010.
34. Tuthill RW. Hair lead levels related to children’s classroom attention-deficit behavior. Arch Environ Health 1996;51:214-220.
35. Braun JM, Kahn RS, Froehlich T, et al. Exposures to environmental toxicants and attention deficit hyperactivity disorder in U.S. children. Environ Health Perspect 2006;114:1904-1909.
36. Dvorakova M, Sivonova M, Trebaticka J, et al. The effect of polyphenolic extract from pine bark, Pycnogenol on the level of glutathione in children suffering from attention deficit hyperactivity disorder (ADHD). Redox Rep 2006;11:163-172.
37. Richardson AJ. Omega-3 fatty acids in ADHD and related neurodevelopmental disorders. Int Rev Psychiatry 2006;18:155-172.
38. Amen DG, Carmichael BD. High-resolution brain SPECT imaging in ADHD. Ann Clin Psychiatry 1997;9:81-86.
39. O’Hara NH, Szakacs GM. The recovery of a child with autism spectrum disorder through biomedical interven-tions. Altern Ther Health Med 2008;14:42-44.
40. Granpeesheh D, Tarbox J, Dixon DR, et al. Retrospective analysis of clinical records in 38 cases of recovery from autism. Ann Clin Psychiatry 2009;21:195-204.
41. Eikeseth S, Smith T, Jahr E, Eldevik S. Outcome for children with autism who began intensive behavioral treatment between ages 4 and 7: a comparison controlled study. Behav Modif 2007;31:264-278.
42. Cohen H, Amerine-Dickens M, Smith T. Early intensive behavioral treatment: replication of the UCLA model in a community setting. J Dev Behav Pediatr 2006;27:S145-S155.
43. McEachin JJ, Smith T, Lovaas OI. Long-term outcome for children with autism who received early intensive behavioral treatment. Am J Ment Retard 1993;97:359-372; discussion 373-391.
44. Israngkun PP, Newman HA, Patel ST, et al. Potential biochemical markers for infantile autism. Neurochem Pathol 1986;5:51-70.
45. Chakravarty A. Regulatory aspects in using surrogate markers in clinical trials. In: Burzykowski T, Molenberghs G, Buyse M, eds. Statistics for Biology and Health. The Evaluation of Surrogate Endpoints. New York, NY: Springer Science+Business Media, Inc.; 2005:13-51.
46. Bruchfeld A, Carrero JJ, Qureshi AR, et al. Elevated serum macrophage migration inhibitory factor (MIF) concentrations in chronic kidney disease (CKD) are associated with markers of oxidative stress and endothelial activation. Mol Med 2009;15:70-75.
47. Sajdel-Sulkowska EM, Lipinski B, Windom H, et al. Oxidative stress in autism: elevated cerebellar 3-nitrotyro-sine levels. Am J Biochem Biotech 2008;4:73-84.
48. Reynolds A, Laurie C, Mosley RL, Gendelman HE. Oxidative stress and the pathogenesis of neurodegenerative disorders. Int Rev Neurobiol 2007;82:297-325.
49. Sweeten TL, Posey DJ, McDougle CJ. High blood monocyte counts and neopterin levels in children with autistic disorder. Am J Psychiatry 2003;160:1691-1693.
50. Warren RP, Yonk LJ, Burger RA, et al. Deficiency of suppressor-inducer (CD4+CD45RA+) T cells in autism. Immunol Invest 1990;19:245-251.
51. Denney DR, Frei BW, Gaffney GR. Lymphocyte subsets and interleukin-2 receptors in autistic children. J Autism Dev Disord 1996;26:87-97.
52. Stubbs EG, Crawford ML. Depressed lymphocyte responsiveness in autistic children. J Autism Child Schizophr 1977;7:49-55.
53. Yonk LJ, Warren RP, Burger RA, et al. CD4+ helper T cell depression in autism. Immunol Lett 1990;25:341-345.
54. Croonenberghs J, Wauters A, Devreese K, et al. Increased serum albumin, gamma globulin, immunoglobulin IgG, and IgG2 and IgG4 in autism. Psychol Med 2002;32:1457-1463.
55. Weissman JR, Kelley RI, Bauman ML, et al. Mitochondrial disease in autism spectrum disorder patients: a cohort analysis. PLoS One 2008;3:e3815.
56. Poling JS, Frye RE, Shoffner J, Zimmerman AW. Developmental regression and mitochondrial dysfunction in a child with autism. J Child Neurol 2006;21:170-172.
57. Kozielec T, Starobrat-Hermelin B. Assessment of magnesium levels in children with attention deficit hyperactiv-ity disorder (ADHD). Magnes Res 1997;10:143-148.
58. Starobrat-Hermelin B, Kozielec T. The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactiv-ity disorder (ADHD). Positive response to magnesium oral loading test. Magnes Res 1997;10:149-156.
59. Mousain-Bosc M, Roche M, Polge A, et al. Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. II. Pervasive developmental disorder-autism. Magnes Res 2006;19:53-62.
amr®
29 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
60. Bekaroglu M, Aslan Y, Gedik Y, et al. Relationships between serum free fatty acids and zinc, and attention deficit hyperactivity disorder: a research note. J Child Psychol Psychiatry 1996;37:225-227.
61. Arnold LE, Bozzolo H, Hollway J, et al. Serum zinc correlates with parent- and teacher- rated inattention in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2005;15:628-636.
62. Yorbik O, Akay C, Sayal A, et al. Zinc status in autistic children. J Trace Elem Exp Med 2004;17:101-107.
63. Adams JB, Holloway CE, George F, Quig D. Analyses of toxic metals and essential minerals in the hair of Arizona children with autism and associated conditions, and their mothers. Biol Trace Elem Res 2006;110:193-209.
64. Jory J, McGinnis WR. Red-cell trace minerals in children with autism. Am J Biochem Biotech 2008;4:101-104.
65. Oshiro M, Mimura S, Hayakawa M, Watanabe K. Plasma and erythrocyte levels of trace elements and related antioxidant enzyme activities in low-birthweight infants during the early postnatal period. Acta Paediatr 2001;90:1283-1287.
66. Starobrat-Hermelin B. The effect of deficiency of selected bioelements on hyperactivity in children with certain specified mental disorders. Ann Acad Med Stetin 1998;44:297-314. [Article in Polish]
67. Konofal E, Lecendreux M, Arnulf I, Mouren MC. Iron deficiency in children with attention-deficit/hyperactivity disorder. Arch Pediatr Adolesc Med 2004;158:1113-1115.
68. Konofal E, Cortese S, Marchand M, et al. Impact of restless legs syndrome and iron deficiency on attention-deficit/hyperactivity disorder in children. Sleep Med 2007;8:711-715.
69. Latif A, Heinz P, Cook R. Iron defi-ciency in autism and Asperger syn-drome. Autism 2002;6:103-114.
70. Dosman CF, Drmic IE, Brian JA, et al. Ferritin as an indicator of suspected iron deficiency in children with autism spectrum disorder: prevalence of low serum ferritin concentration. Dev Med Child Neurol 2006;48:1008-1009.
71. Konofal E, Lecendreux M, Deron J, et al. Effects of iron supplementation on attention deficit hyperactivity disorder in children. Pediatr Neurol 2008;38:20-26.
72. Dosman CF, Brian JA, Drmic IE, et al. Children with autism: effect of iron supplementation on sleep and ferritin. Pediatr Neurol 2007;36:152-158.
73. Gillberg IC, Gillberg C, Kopp S. Hypothyroidism and autism spectrum disorders. J Child Psychol Psychiatry 1992;33:531-542.
74. Weiss RE, Stein MA, Trommer B, Refetoff S. Attention-deficit hyperactiv-ity disorder and thyroid function. J Pediatr 1993;123:539-545.
75. Tierney E, Bukelis I, Thompson RE, et al. Abnormalities of cholesterol metabolism in autism spectrum disorders. Am J Med Genet B Neuropsychiatr Genet 2006;141B:666-668.
76. Zhang J, Muldoon MF, McKeown RE, Cuffe SP. Association of serum choles-terol and history of school suspension among school-age children and adoles-cents in the United States. Am J Epidemiol 2005;161:691-699.
77. Geier DA, Geier MR. A clinical and laboratory evaluation of methionine cycle-transsulfuration and androgen pathway markers in children with autistic disorders. Horm Res 2006;66:182-188.
78. de Bruin EI, Verheij F, Wiegman T, Ferdinand RF. Differences in finger length ratio between males with autism, pervasive developmental disorder-not otherwise specified, ADHD, and anxiety disorders. Dev Med Child Neurol 2006;48:962-965.
79. Sanfeliu C, Sebastia J, Ki SU. Methylmercury neurotoxicity in cultures of human neurons, astrocytes, neuro-blastoma cells. Neurotoxicology 2001;22:317-327.
80. Deth R, Muratore C, Benzecry J, et al. How environmental and genetic factors combine to cause autism: a redox/methylation hypothesis. Neurotoxicology 2008;29:190-201.
81. Chauhan A, Chauhan V, Brown WT, Cohen I. Oxidative stress in autism: increased lipid peroxidation and reduced serum levels of ceruloplasmin and transferrin – the antioxidant proteins. Life Sci 2004;75:2539-2549.
82. Cagnon L, Braissant O. Hyperammonemia-induced toxicity for the developing central nervous system. Brain Res Rev 2007;56:183-197.
83. Chinnery PF. Mitochondrial disorders overview. http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=gene&part=mt-overview [Accessed January 19, 2010]
84. Chinnery PF, Turnbull DM. Mitochondrial medicine. QJM 1997;90:657-667.
85. Oliveira G, Diogo L, Grazina M, et al. Mitochondrial dysfunction in autism spectrum disorders: a population-based study. Dev Med Child Neurol 2005;47:185-189.
86. Correia C, Coutinho AM, Diogo L, et al. Brief report: High frequency of biochemical markers for mitochondrial dysfunction in autism: no association with the mitochondrial aspartate/glutamate carrier SLC25A12 gene. J Autism Dev Disord 2006;36:1137-1140.
87. Svoboda P, Maekawa M, Kawai K, et al. Urinary 8-hydroxyguanine may be a better marker of oxidative stress than 8-hydroxydeoxyguanosine in relation to the life spans of various species. Antioxid Redox Signal 2006;8:985-992.
88. Ming X, Stein TP, Brimacombe M, et al. Increased excretion of a lipid peroxida-tion biomarker in autism. Prostaglandins Leukot Essent Fatty Acids 2005;73:379-384.
89. Eyles D, Brown J, Mackay-Sim A, et al. Vitamin D3 and brain development. Neuroscience 2003;118:641-653.
90. Cannell JJ. Autism and vitamin D. Med Hypotheses 2008;70:750-759.

amr®
Volume 15, Number 1 Alternative Medicine Review 30Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
91. Bejerot S, Humble M. Increased occurrence of autism among Somali children – does vitamin D deficiency play a role? Tidsskr Nor Laegeforen 2008;128:1986-1987. [Article in Swedish]
92. Garcion E, Wion-Barbot N, Montero-Menei CN, et al. New clues about vitamin D functions in the nervous system. Trends Endocrinol Metab 2002;13:100-105.
93. Berk M, Ng F, Dean O, et al. Glutathione: a novel treatment target in psychiatry. Trends Pharmacol Sci 2008;29:346-351.
94. Lin AM, Chen KB, Chao PL. Antioxidative effect of vitamin D3 on zinc-induced oxidative stress in CNS. Ann N Y Acad Sci 2005;1053:319-329.
95. James SJ, Slikker W 3rd, Melnyk S, et al. Thimerosal neurotoxicity is associated with glutathione depletion: protection with glutathione precur-sors. Neurotoxicology 2005;26:1-8.
96. James SJ, Melnyk S, Fuchs G, et al. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr 2009;89:425-430.
97. Waring RH, Ngong JM, Klovrza L, et al. Biochemical parameters in autistic children. Dev Brain Dysfunct 1997;10:40-43.
98. O’Reilly BA, Waring RH. Enzyme and sulphur oxidation deficiencies in autistic children with known food/chemical intolerances. J Orthomolecular Med 1993;8:198-200.
99. Alberti A, Pirrone P, Elia M, et al. Sulphation deficit in “low-functioning” autistic children: a pilot study. Biol Psychiatry 1999;46:420-424.
100. Horvath K, Perman JA. Autistic disorder and gastrointestinal disease. Curr Opin Pediatr 2002;14:583-587.
101. McFadden SA. Phenotypic variation in xenobiotic metabolism and adverse environmental response: focus on sulfur-dependent detoxification pathways. Toxicology 1996;111:43-65.
102. Connolly AM, Chez M, Streif EM, et al. Brain-derived neurotrophic factor and autoantibodies to neural antigens in sera of children with autistic spectrum disorders, Landau-Kleffner syndrome, and epilepsy. Biol Psychiatry 2006;59:354-363.
103. Connolly AM, Chez MG, Pestronk A, et al. Serum autoantibodies to brain in Landau-Kleffner variant, autism, and other neurologic disorders. J Pediatr 1999;134:607-613.
104. Messahel S, Pheasant AE, Pall H, et al. Urinary levels of neopterin and biopterin in autism. Neurosci Lett 1998;241:17-20.
105. Messahel S, Pheasant AE, Pall H, Kerr AM. Abnormalities in urinary pterin levels in Rett syndrome. Eur J Paediatr Neurol 2000;4:211-217.
106. Gupta S. Immunological treatments for autism. J Autism Dev Disord 2000;30:475-479.
107. Heuer L, Ashwood P, Schauer J, et al. Reduced levels of immunoglobulin in children with autism correlates with behavioral symptoms. Autism Res 2008;1:275-283.
108. Oleske J. Another view of autism. The University of Medicine & Dentistry of New Jersey Research 2004;Winter:22-23.
109. Gupta S, Aggarwal S, Heads C. Dysregulated immune system in children with autism: beneficial effects of intravenous immune globulin on autistic characteristics. J Autism Dev Disord 1996;26:439-452.
110. Stern L, Francoeur MJ, Primeau MN, et al. Immune function in autistic children. Ann Allergy Asthma Immunol 2005;95:558-565.
111. Warren RP, Odell JD, Warren WL, et al. Brief report: immunoglobulin A deficiency in a subset of autistic subjects. J Autism Dev Disord 1997;27:187-192.
112. Plioplys AV. Intravenous immunoglobu-lin treatment in autism. J Autism Dev Disord 2000;30:73-74.
113. Winterkamp S, Weidenhiller M, Otte P, et al. Urinary excretion of N-methylhistamine as a marker of disease activity in inflammatory bowel disease. Am J Gastroenterol 2002;97:3071-3077.
114. Chez MG, Dowling T, Patel PB, et al. Elevation of tumor necrosis factor-alpha in cerebrospinal fluid of autistic children. Pediatr Neurol 2007;36:361-365.
115. Giedd JN, Rapoport JL, Leonard HL, et al. Case study: acute basal ganglia enlargement and obsessive-compulsive symptoms in an adolescent boy. J Am Acad Child Adolesc Psychiatry 1996;35:913-915.
116. Snider LA, Lougee L, Slattery M, et al. Antibiotic prophylaxis with azithromy-cin or penicillin for childhood-onset neuropsychiatric disorders. Biol Psychiatry 2005;57:788-792.
117. Swedo SE, Garvey M, Snider L, et al. The PANDAS subgroup: recognition and treatment. CNS Spectr 2001;6:419-422,425-426.
118. Balzola F, Daniela C, Repici A, et al. Autistic enterocolitis: confirmation of a new inflammatory bowel disease in an Italian cohort of patients. Gastroenterology 2005;128:A303.
119. Torrente F, Ashwood P, Day R, et al. Small intestinal enteropathy with epithelial IgG and complement deposition in children with regressive autism. Mol Psychiatry 2002;7:375-382,334.
120. Horvath K, Papadimitriou JC, Rabsztyn A, et al. Gastrointestinal abnormalities in children with autistic disorder. J Pediatr 1999;135:559-563.
121. Valicenti-McDermott M, McVicar K, Rapin I, et al. Frequency of gastrointes-tinal symptoms in children with autistic spectrum disorders and association with family history of autoimmune disease. J Dev Behav Pediatr 2006;27:S128-S136.
122. Horvath K, Perman JA. Autism and gastrointestinal symptoms. Curr Gastroenterol Rep 2002;4:251-258.

amr®
31 Alternative Medicine Review Volume 15, Number 1Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
123. Jyonouchi H, Geng L, Ruby A, et al. Evaluation of an association between gastrointestinal symptoms and cytokine production against common dietary proteins in children with autism spectrum disorders. J Pediatr 2005;146:605-610.
124. Canani RB, Terrin G, Rapacciuolo L, et al. Faecal calprotectin as reliable non-invasive marker to assess the severity of mucosal inflammation in children with inflammatory bowel disease. Dig Liver Dis 2008;40:547-553.
125. Diamanti A, Colistro F, Basso MS, et al. Clinical role of calprotectin assay in determining histological relapses in children affected by inflammatory bowel diseases. Inflamm Bowel Dis 2008;14:1229-1235.
126. Peterson CG, Hansson T, Skott A, et al. Detection of local mast-cell activity in patients with food hypersensitivity. J Investig Allergol Clin Immunol 2007;17:314-320.
127. Sidler MA, Leach ST, Day AS. Fecal S100A12 and fecal calprotectin as noninvasive markers for inflammatory bowel disease in children. Inflamm Bowel Dis 2008;14:359-366.
128. Fernell E, Fagerberg UL, Hellstrom PM. No evidence for a clear link between active intestinal inflammation and autism based on analyses of faecal calprotectin and rectal nitric oxide. Acta Paediatr 2007;96:1076-1079.
129. D’Eufemia P, Celli M, Finocchiaro R, et al. Abnormal intestinal permeability in children with autism. Acta Paediatr 1996;85:1076-1079.
130. Robertson MA, Sigalet DL, Holst JJ, et al. Intestinal permeability and glucagon-like peptide-2 in children with autism: a controlled pilot study. J Autism Dev Disord 2008;38:1066-1071.
131. Wakefield AJ, Murch SH, Anthony A, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Lancet 1998;351:637-641.
132. Sandler RH, Finegold SM, Bolte ER, et al. Short-term benefit from oral vancomy-cin treatment of regressive-onset autism. J Child Neurol 2000;15:429-435.
133. Sheil B, Shanahan F, O’Mahony L. Probiotic effects on inflammatory bowel disease. J Nutr 2007;137:819S-824S.
134. Zelnik N, Pacht A, Obeid R, Lerner A. Range of neurologic disorders in patients with celiac disease. Pediatrics 2004;113:1672-1676.
135. Barcia G, Posar A, Santucci M, Parmeggiani A. Autism and coeliac disease. J Autism Dev Disord 2008;38:407-408.
136. Lucarelli S, Frediani T, Zingoni AM, et al. Food allergy and infantile autism. Panminerva Med 1995;37:137-141.
137. Jenkins M, Vickers A. Unreliability of IgE/IgG4 antibody testing as a diagnostic tool in food intolerance. Clin Exp Allergy 1998;28:1526-1529.
138. Oehling A, Fernandez M, Cordoba H, Sanz ML. Skin manifestations and immunological parameters in childhood food allergy. J Investig Allergol Clin Immunol 1997;7:155-159.
139. Buie TM. Gastroesophageal reflux in children with autism: how do children present and can one test these children? J Pediatr Gastroenterol Nutr 2005;41:505.
140. Stern AH. A revised probabilistic estimate of the maternal methyl mercury intake dose corresponding to a measured cord blood mercury concen-tration. Environ Health Perspect 2005;113:155-163.
141. David OJ. Association between lower level lead concentrations and hyperac-tivity in children. Environ Health Perspect 1974;7:17-25.
142. David OJ, Hoffman SP, Clark J, et al. The relationship of hyperactivity to moderately elevated lead levels. Arch Environ Health 1983;38:341-346.
143. Nigg JT, Knottnerus GM, Martel MM, et al. Low blood lead levels associated with clinically diagnosed attention-deficit/hyperactivity disorder and mediated by weak cognitive control. Biol Psychiatry 2008;63:325-331.
144. Lidsky TI, Schneider JS. Autism and autistic symptoms associated with childhood lead poisoning. J Appl Res 2005;5:80-87.
145. Cheuk DK, Wong V. Attention-deficit hyperactivity disorder and blood mercury level: a case-control study in Chinese children. Neuropediatrics 2006;37:234-240.
146. Soden SE, Lowry JA, Garrison CB, Wasserman GS. 24-hour provoked urine excretion test for heavy metals in children with autism and typically developing controls, a pilot study. Clin Toxicol (Phila) 2007;45:476-481.
147. Chrysochoou C, Rutishauser C, Rauber-Luthy C, et al. An 11-month-old boy with psychomotor regression and auto-aggres-sive behaviour. Eur J Pediatr 2003;162:559-561.
148. Palmer RF, Blanchard S, Wood R. Proximity to point sources of environ-mental mercury release as a predictor of autism prevalence. Health Place 2009;15:18-24.
149. Palmer RF, Blanchard S, Stein Z, et al. Environmental mercury release, special education rates, and autism disorder: an ecological study of Texas. Health Place 2006;12:203-209.
150. Windham GC, Zhang L, Gunier R, et al. Autism spectrum disorders in relation to distribution of hazardous air pollutants in the San Francisco bay area. Environ Health Perspect 2006;114:1438-1444.
151. Rury J. Links between environmental mercury, special education, and autism in Louisiana. Masters Thesis. Louisiana State University, 2006.
152. Filipek PA, Accardo PJ, Baranek GT, et al. The screening and diagnosis of autistic spectrum disorders. J Autism Dev Disord 1999;29:439-484.
153. Canfield RL, Henderson CR Jr, Cory-Slechta DA, et al. Intellectual impair-ment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 2003;348:1517-1526.
154. Clarkson TW. The three modern faces of mercury. Environ Health Perspect 2002;110:11-23.
155. Bergdahl IA, Vahter M, Counter SA, et al. Lead in plasma and whole blood from lead-exposed children. Environ Res 1999;80:25-33.
amr®
Volume 15, Number 1 Alternative Medicine Review 32Copyright © 2010 Alternative Medicine Review, LLC. All Rights Reserved. No Reprint Without Written Permission.
Review Article
156. Geier DA, Geier MR. A prospective study of mercury toxicity biomarkers in autistic spectrum disorders. J Toxicol Environ Health A 2007;70:1723-1730.
157. Geier DA, Geier MR. A prospective assessment of porphyrins in autistic disorders: a potential marker for heavy metal exposure. Neurotox Res 2006;10:57-64.
158. Austin DW, Shandley K. An investiga-tion of porphyrinuria in Australian children with autism. J Toxicol Environ Health A 2008;71:1349-1351.
159. Heyer NJ, Bittner AC Jr, Echeverria D, Woods JS. A cascade analysis of the interaction of mercury and copropor-phyrinogen oxidase (CPOX) polymor-phism on the heme biosynthetic pathway and porphyrin production. Toxicol Lett 2006;161:159-166.
160. Woods JS, Echeverria D, Heyer NJ, et al. The association between genetic polymorphisms of coproporphyrinogen oxidase and an atypical porphyrino-genic response to mercury exposure in humans. Toxicol Appl Pharmacol 2005;206:113-120.
161. Adams JB, Baral M, Geis E, et al. Safety and efficacy of oral DMSA therapy for children with autism spectrum disorders: part B – behavioral results. BMC Clin Pharmacol 2009;9:17.
162. Adams JB, Baral M, Geis E, et al. Safety and efficacy of oral DMSA therapy for children with autism spectrum disor-ders: part A – medical results. BMC Clin Pharmacol 2009;9:16.
163. Blades M. Autism: an interesting dietary case history. Nutr Food Sci 2000;30:137-140.
164. Brudnak MA, Rimland B, Kerry RE, et al. Enzyme-based therapy for autism spectrum disorders – is it worth another look? Med Hypotheses 2002;58:422-428.
165. Dolske MC, Spollen J, McKay S, et al. A preliminary trial of ascorbic acid as supplemental therapy for autism. Prog Neuropsychopharmacol Biol Psychiatry 1993;17:765-774.
166. Chez MG, Buchanan CP, Aimonovitch MC, et al. Double-blind, placebo-con-trolled study of L-carnosine supplemen-tation in children with autistic spectrum disorders. J Child Neurol 2002;17:833-837.
167. Ellaway CJ, Peat J, Williams K, et al. Medium-term open label trial of L-carnitine in Rett syndrome. Brain Dev 2001;23:S85-S89.
168. Trebaticka J, Kopasova S, Hradecna Z, et al. Treatment of ADHD with French maritime pine bark extract, Pycnogenol. Eur Child Adolesc Psychiatry 2006;15:329-335.
169. Torrioli MG, Vernacotola S, Peruzzi L, et al. A double-blind, parallel, multi-center comparison of L-acetylcarnitine with placebo on the attention deficit hyperactivity disorder in fragile X syndrome boys. Am J Med Genet A 2008;146:803-812.
170. Bilici M, Yildirim F, Kandil S, et al. Double-blind, placebo-controlled study of zinc sulfate in the treatment of attention deficit hyperactivity disorder. Prog Neuropsychopharmacol Biol Psychiatry 2004;28:181-190.
171. Adams JB, Holloway C. Pilot study of a moderate dose multivitamin/mineral supplement for children with autistic spectrum disorder. J Altern Complement Med 2004;10:1033-1039.
172. Harding KL, Judah RD, Gant C. Outcome-based comparison of Ritalin versus food-supplement treated children with AD/HD. Altern Med Rev 2003;8:319-330.
173. Bradstreet JJ, Smith S, Granpeesheh D, et al. Spironolactone might be a desirable immunologic and hormonal intervention in autism spectrum disorders. Med Hypotheses 2007;68:979-987.
174. Boris M, Kaiser CC, Goldblatt A, et al. Effect of pioglitazone treatment on behavioral symptoms in autistic children. J Neuroinflammation 2007;4:3.
175. Rossignol DA. Novel and emerging treatments for autism spectrum disorders: a systematic review. Ann Clin Psychiatry 2009;21:213-236.
176. Boris M, Goldblatt A, Edelson SM. Improvement in children with autism treated with intravenous gamma globulin. J Nutr Environ Med 2005;15:169-176.