bhs guidelines for the management of hypertension
DESCRIPTION
BHS Guidelines for the management of hypertension. BHS IV, 2004 and Update of the NICE Hypertension Guideline, 2006 Guidelines for management of hypertension: report of the fourth Working Party of the British Hypertension Society, 2004 BHS IV B Williams et al: J Hum Hyp (2004); 18: 139-185. - PowerPoint PPT PresentationTRANSCRIPT
BHS Guidelines for the management of hypertension
BHS IV, 2004 and Update of the NICE Hypertension Guideline, 2006
Guidelines for management of hypertension: report of the fourth Working Party of the British Hypertension Society, 2004 BHS IVB Williams et al: J Hum Hyp (2004); 18: 139-185.
www.nice.org.uk/CG034NICEguideline
www.bhsoc.org

•Measurement
Hypertension management issues
•Investigation
•Non-pharmacological treatment
•Thresholds for drug treatment
•Targets for drug treatment
•Drug choices – trial update
•Other treatments
•Follow-up
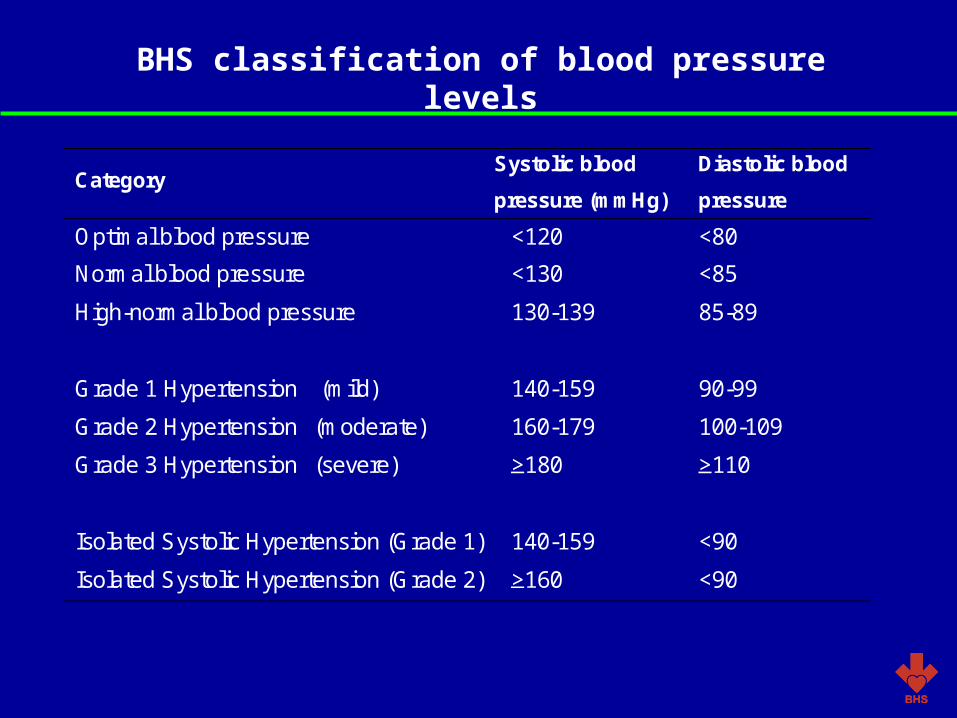
BHS classification of blood pressure levels
Category Systolic blood
pressure (mmHg)
Diastolic blood
pressure
(mmHg) Optimal blood pressure <120 <80
Normal blood pressure <130 <85
High-normal blood pressure 130-139 85-89
Grade 1 Hypertension (mild) 140-159 90-99
Grade 2 Hypertension (moderate) 160-179 100-109
Grade 3 Hypertension (severe) >180 >110
Isolated Systolic Hypertension (Grade 1) 140-159 <90
Isolated Systolic Hypertension (Grade 2) >160 <90
Potential indications for the use of ambulatory blood pressure monitoring
•Unusual variability
•Possible white coat hypertension
•Informing equivocal treatment decisions
•Evaluation of nocturnal hypertension
•Evaluation of drug-resistant hypertension
•Determining the efficacy of drug treatment over 24 hours
•Diagnoses and treatment of hypertension in pregnancy
•Evaluation of symptomatic hypotension
Routine investigations
• Urine strip test for protein and blood
• Serum creatinine and electrolytes
• Blood glucose - ideally fasted
• Blood lipid profile (at least total and high density lipoprotein (HDL) cholesterol) – ideally fasted for consideration of triglycerides
• Electrocardiogram

Lifestyle measures
•Maintain normal weight for adults (body mass index 20-25 kg/m2)
•Reduce salt intake to <100 mmol/day (<6g NaCl or <2.4 g Na+/day)
•Limit alcohol consumption to 3 units/day for men and 2 units/day for women
•Engage in regular aerobic physical exercise (brisk walking rather than weight lifting) for 30 minutes per day, ideally on most of days of the week but at least on three days of the week
•Consume at least five portions/day of fresh fruit and vegetables
•Reduce the intake of total and saturated fat

Target organ damageor
cardiovascular complicationsor
diabetesor
10 year CVD risk† 20%
>180/110 160 179100 109
140 15990 99
130 13985 89
<130/85
160/100 140 15990 99
<140/90
No target organ damageand
no cardiovascular complicationsand
no diabetesand
10 year CVD risk† <20%
* ** ***
Treat Treat Treat Observe, reassessCVD risk yearly
Reassessyearly
Reassessin 5 years
* Unless malignant phase of hypertensive emergency confirm over 1 2 weeks then treat** If cardiovascular complications, target organ damage or diabetes is present, confirm over 3 4 weeks then treat; if absent re-measure
weekly and treat if blood pressure persists at these levels over 4 12*** If cardiovascular complications, target organ damage, or diabetes is present, confirm over 12 weeks then treat: if absent re-measure
monthly and treat if these levels are maintained and if estimated 10 year CVD risk is 20%† Assessed with CVD risk chart
THRESHOLDS FOR INTERVENTIONInitial blood pressure (mmHg)


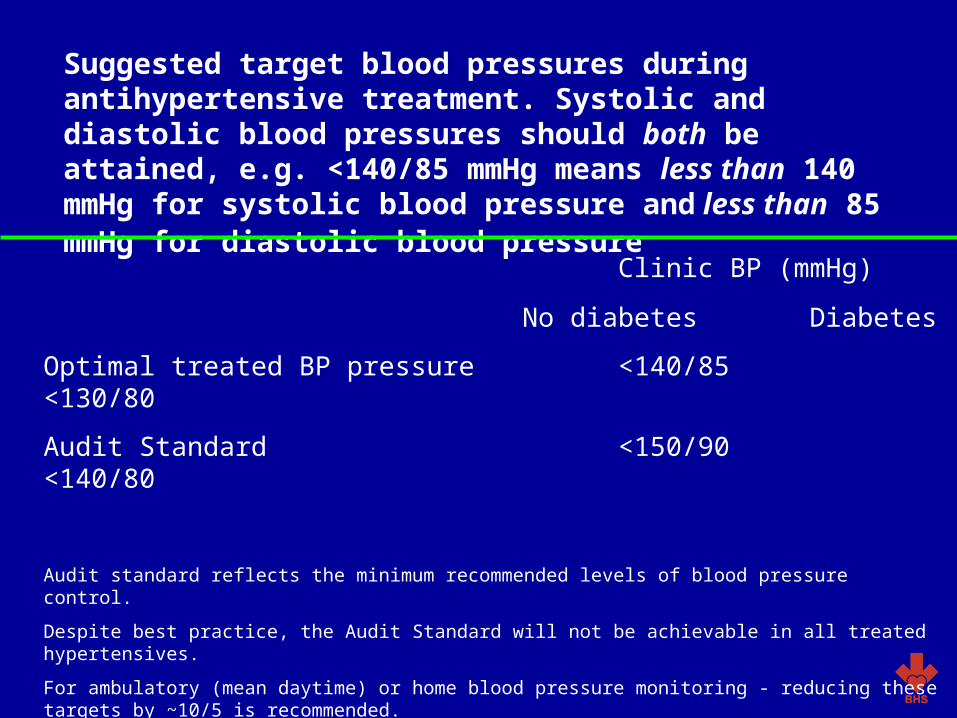
Suggested target blood pressures during antihypertensive treatment. Systolic and diastolic blood pressures should both be attained, e.g. <140/85 mmHg means less than 140 mmHg for systolic blood pressure and less than 85 mmHg for diastolic blood pressure
Clinic BP (mmHg)
No diabetes Diabetes
Optimal treated BP pressure <140/85 <130/80
Audit Standard <150/90 <140/80
Audit standard reflects the minimum recommended levels of blood pressure control.
Despite best practice, the Audit Standard will not be achievable in all treated hypertensives.
For ambulatory (mean daytime) or home blood pressure monitoring - reducing these targets by ~10/5 is recommended.


Compelling and possible indications, contraindications, and cautions for the major classes of antihypertensive drugs Class of drug
Compelling indications
Possible indications
Caution
Compelling contra-indications
Alpha-blockers
Benign prostatic hypertrophy
Postural hypotension, heart failure
Urinary incontinence
ACE-inhibitors
Heart failure, LV dysfunction, post MI or established CVD, Type I diabetic nephropathy, 2o stroke prevention
Chronic renal disease, Type II diabetic nephropathy, proteinuric renal disease
Renal impairment
PVD Pregnancy, renovascular disease
ARBs ACE inhibitor-intolerance, Type II diabetic nephropathy, hypertension with LVH, heart failure in ACE-intolerant patients, post MI
LV dysfunction post MI, intol-erance of other antihypertensive drugs, proteinuric renal disease, chronic renal disease,
heart failure
Renal impairment PVD
Pregnancy, renovascular disease

Compelling and possible indications, contraindications, and cautions for the major classes of antihypertensive drugs Class of drug
Compelling indications
Possible indications
Caution
Compelling contraindications
Beta-blockers MI, Angina
Heart failure Heart failure, PVD,
Diabetes (except with CHD)
Asthma/COPD, Heart block
CCBs (dihydropyridine)
Elderly, ISH Angina - -
CCBs (rate limiting)
Angina Elderly Combination with beta-blockade
Heart block Heart failure
Thiazide/thiazide-like diuretics
Elderly ISH Heart failure 2 o stroke prevention
Gout

Other medications for hypertensive patients
Primary prevention
(1) Aspirin: use 75mg daily if patient is aged 50 years with blood pressure controlled to <150/90 mm Hg and either; target organ damage, diabetes mellitus, or 10 year risk of cardiovascular disease of 20% (measured by using the new Joint British Societies’ cardiovascular disease risk chart)
(2) Statin: use sufficient doses to reach targets if patient is aged up to at least 80 years, with a 10 year risk of cardiovascular disease of 20% (measured by using the new Joint British Societies’ cardiovascular disease risk chart) and with total cholesterol concentration 3.5mmol/l
(3) Vitamins—no benefit shown, do not prescribe

Secondary prevention (including patients with type 2 diabetes)
(1) Aspirin: use for all patients unless contraindicated
(2) Statin: use sufficient doses to reach targets if patient is aged up to at least 80 years with a total cholesterol concentration 3.5 mmol/l
(3) Vitamins— no benefit shown, do not prescribe
Other medications for hypertensive patients

Targets for lipid lowering
Ideal - TC<4.0mmol/lor LDL <2.0mmol/lor 25% in TCor 30% in LDL-Cwhichever is the greater
‘Audit’ - TC <5.0mmol/lor LDL <3.0mmol/lor 25% in TCor 30% in LDL-Cwhichever is the greater
Lipid targets