beyond the basics: the art and science of tracing...
TRANSCRIPT
Session 2:
May 21, 2015
Beyond the Basics:
The Art and Science of
Tracing Interpretation
2015 Fetal Monitoring Lunch & Learn Series
Wisconsin Association for Perinatal Care (WAPC)
Faculty
Kathlyn Tambellini, BSN, RNC-OB, C-EFM
Clinical Development Coordinator, Perinatal Services
Wheaton Franciscan St. Joseph Wheaton Franciscan Healthcare - Elmbrook Memorial

Faculty
Melissa Gellings, MSN, RN-C-EFM, APNP
Women’s Outpatient Center Nurse Practitioner
Wheaton Franciscan St. Joseph
Notice of Disclosures • Notice of requirements for successful completion
– Registrants must attend full session and complete evaluation to receive contact hours
• Conflicts of Interest – None to report
• Financial Disclosures – None
• Sponsorship or commercial support – None
• Non-endorsement of products – The speaker does not endorse the use of any particular medications or
products as part of this educational session
Before we begin…
• Listen-only mode • Questions – please ask, please answer!
– Raise your hand – Type into the Question Pane – Out of time? Email [email protected]
• Technical problems: Email Barb Wienholtz at [email protected] or call at 608-285-5858, ext. 201

Before we begin… The content presented today is a case study. Components of this case were chosen based on their applicability to achieve learning objectives for this presentation. Do not assume the patient featured in the case was cared for by the instructor or at the facility at which the instructor is employed. The discussion will focus on interpretation of the electronic fetal monitoring (EFM) tracings for the purpose of education. At times, the discussion may lead to the care decisions made based on EFM interpretation. IF the instructor shares details regarding actual or potential care decisions, please note those decisions do not necessarily reflect the opinions of the instructor, a particular provider, the standard of care for any particular institution or facility, or of WAPC.

Objectives At the conclusion of the session, participants will be able to:
1. Systematically review the electronic fetal monitor strip 2. Identify and categorize the FHR pattern 3. Identify and discuss uterine activity patterns and their influence on the FHR baseline 4. Discuss the pathophysiology related to the tracing patterns identified 5. Discuss interventions for management and documentation of intrapartum fetal heart rate tracings

2008 NICHD Report The 2008 National Institute of Child Health
and Human Development (NICHD)
Report of Fetal Heart Rate Monitoring
• Defined standard fetal heart rate nomenclature
• Identified three categories for fetal heart rate interpretation
• Proposed future research
2008 NICHD Report
• Report endorsed by:
– ACOG (2009) Practice Bulletin #106 "Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation and General Management Principles”
– AWHONN-endorsed and incorporated in fetal monitoring
curriculum – American College of Nurse Midwives – American Academy of Family Practice
American College of Obstetricians and Gynecologists (2009, July). ACOG Practice Bulletin #106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Washington, D.C.: Author
ACOG Practice Bulletin #116 (2010)
"Management of Intrapartum Fetal Heart Rate Tracings"
• Reviewed: – Nomenclature – Fetal Heart Rate Interpretation (categories)
• Provided framework for evaluation and management of intrapartum patterns based on categories
• Assessment algorithm for fetal heart rate patterns
• Intrapartum resuscitative measures
• Management of uterine tachysystole American College of Obstetricians and Gynecologists (2009, July). ACOG Practice Bulletin #106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Washington, D.C.: Author
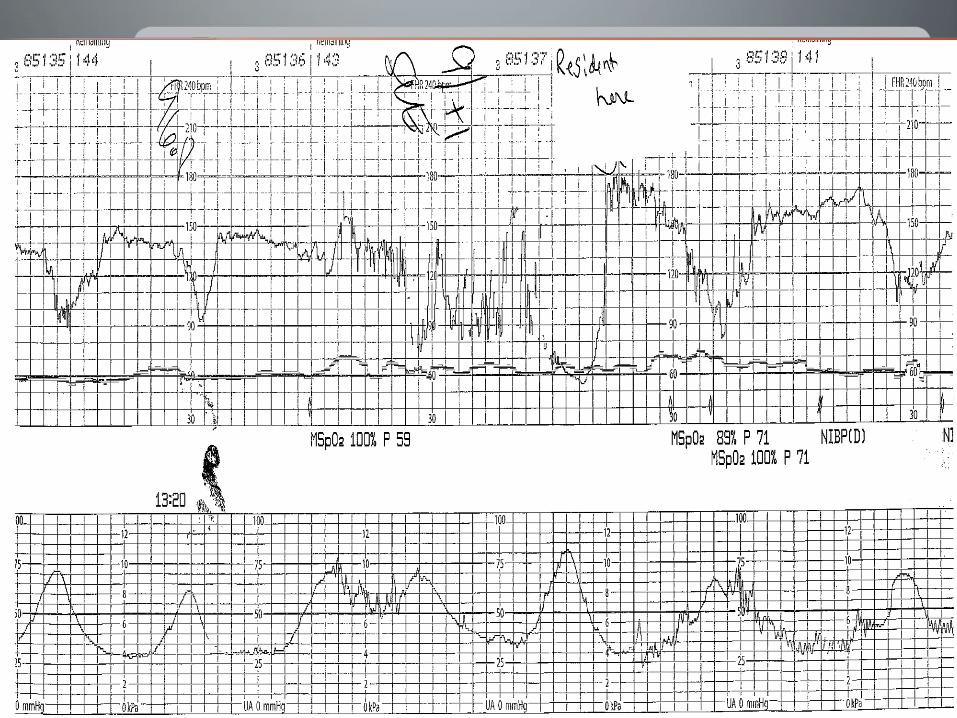
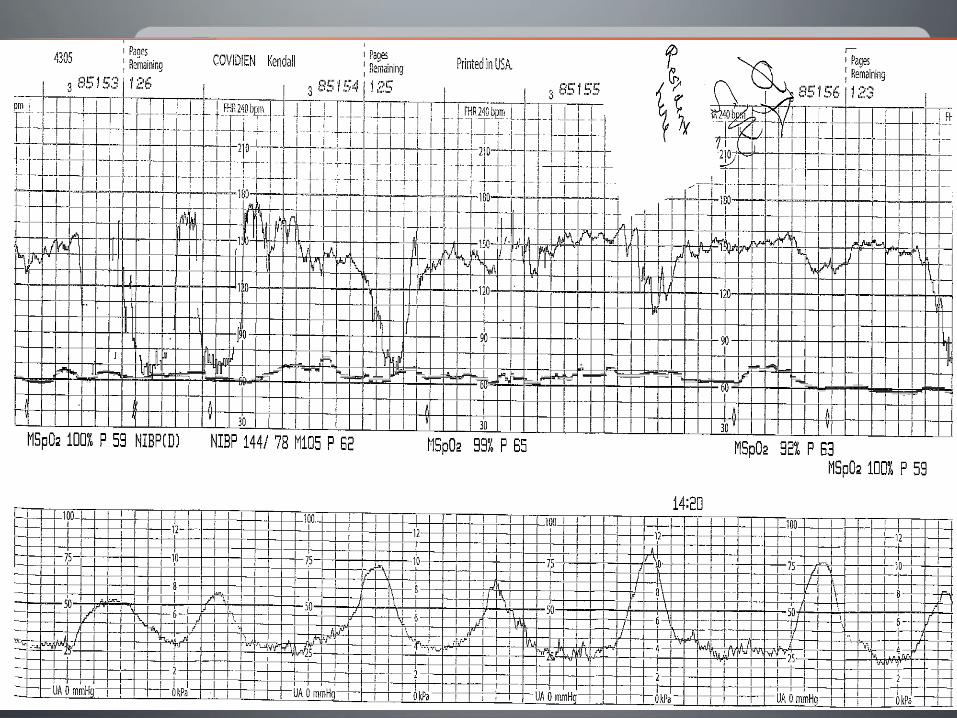
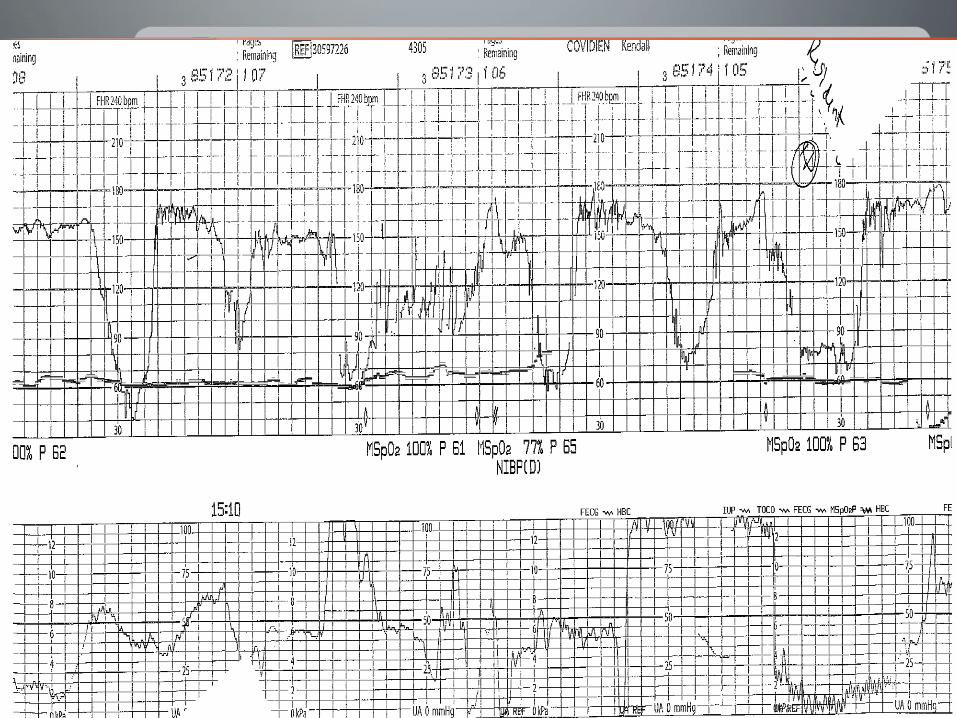
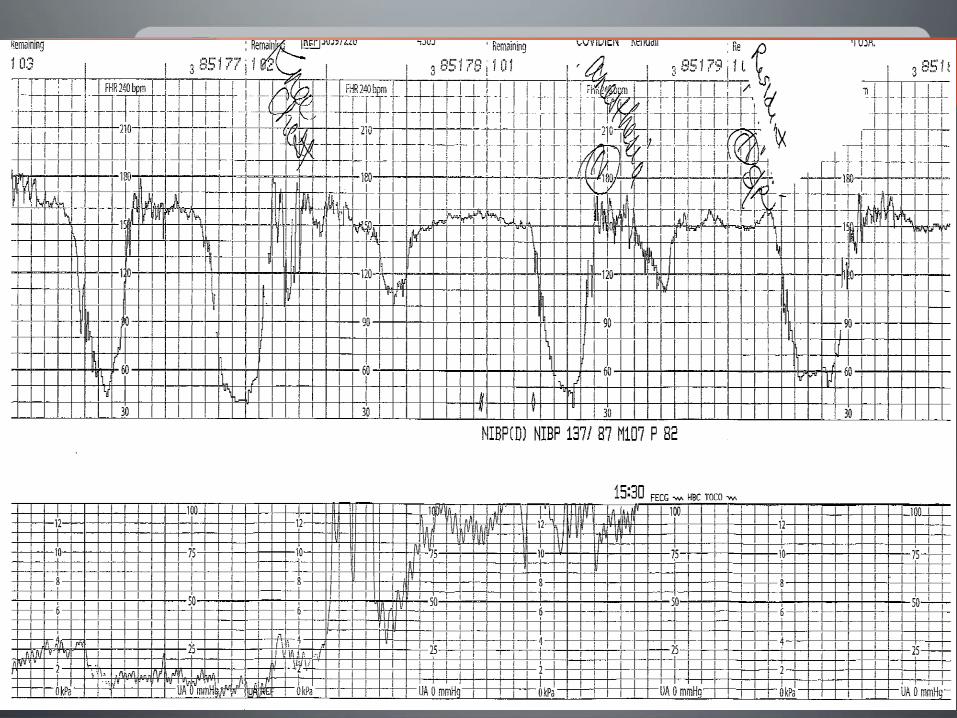
Systematic Review of Case Studies
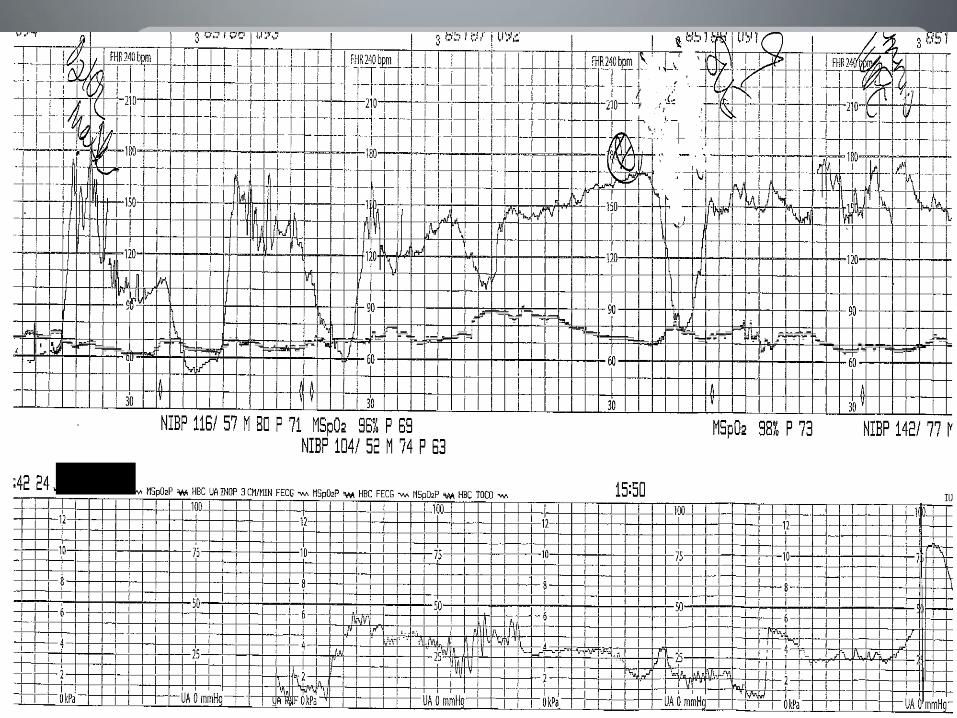
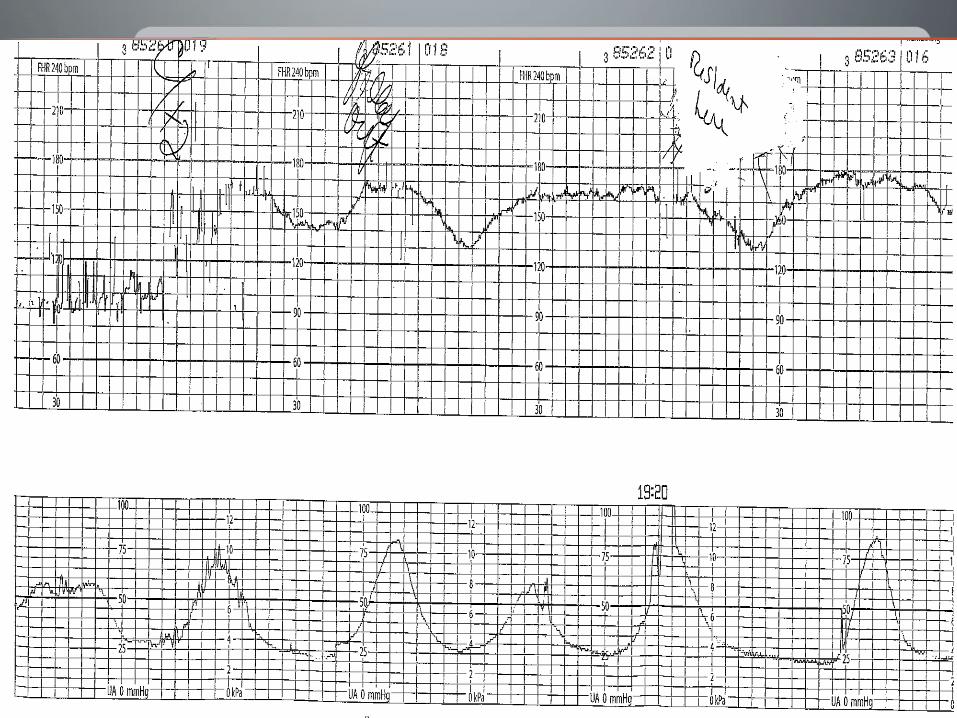
The following questions are used to evaluate every tracing, followed by specific questions:
1. What is the contraction pattern? (interval,
duration, resting tone if appropriate) 2. What is the baseline fetal heart rate? 3. What is the baseline variability? 4. Are there any periodic changes present? 5. Are there any episodic changes present? 6. What are the probable causes of the changes
present? 7. When was the last reassuring sign of fetal well-being?

Strip Review Discussion
• Interpretation
• Interventions/Communication
• Documentation in chart
Intervention/Communication
• SBAR
– Situation
– Background
– Assessment
– Recommendation
Definitions
• Baseline – The baseline Fetal Heart Rate is determined by approximating the
mean FHR rounded to increments of 5 beats per minute (bpm) during a 10-minute window, excluding accelerations and
decelerations and periods of marked variability (>25bpm) – Minimum of identifiable 2 minutes (not contiguous)
– Use prior 10 minute increment if no obvious baseline
– Normal: 110-160
– Bradycardia < 110
– Tachycardia > 160
Definitions
• Variability Fluctuations in the baseline FHR that are irregular in amplitude and
frequency
– Absent: 0
– Minimal <5
– Moderate 6-25
– Marked 25+
Definitions
• Decelerations – Early
• Fetal head compression • Mirrors contraction • Onset and nadir ≥ 30 seconds
– Late • Uteroplacental insufficiency • Onset and nadir ≥ 30 seconds after onset and peak of
contraction
– Variable • Umbilical cord compression • Onset to nadir is less than 30 seconds
– Prolonged • More than 2 minutes
Categories
• 1 – Normal baseline – Moderate variability – Can have accelerations and early decelerations
• 2 – Normal or abnormal baseline – Minimal, moderate, or marked variability – Can have accelerations or decelerations
• 3 – Absent variability or sinusoidal pattern
• 28 yo G2P0010 at 26.3wks, admitted after being seen in office for regular visit.
• In office dipped 3+ proteinuria and BPs 132/90, previous visits had elevated BP but protein dip negative.
• Denies HA/BV or RUQ pain • Sent to L&D for evaluation
– PIH labs done: WNL, EXCEPT URIC ACID of 7 – UA: 3+ protein, 24 hour protein started – BPs: 140-150/90-100
• MFM consult: – fetus with evidence of early growth restriction, 11%ile – Start Mag Sulfate, administer steroids, observe closely – Was stable on L&D after Mag Sulfate and steroids, to lying in
unit
Case 1 – Maternal History
• On day #4 pt was transferred back to L&D for elevated BPs 170s-180s/90s and persistent head ache.
• Plan for delivery:
–Vertex confirmed by US
–Epidural placed, cerclage removed, SVE: 1+/60/-3
–IOL: Pitocin, AROM
Background
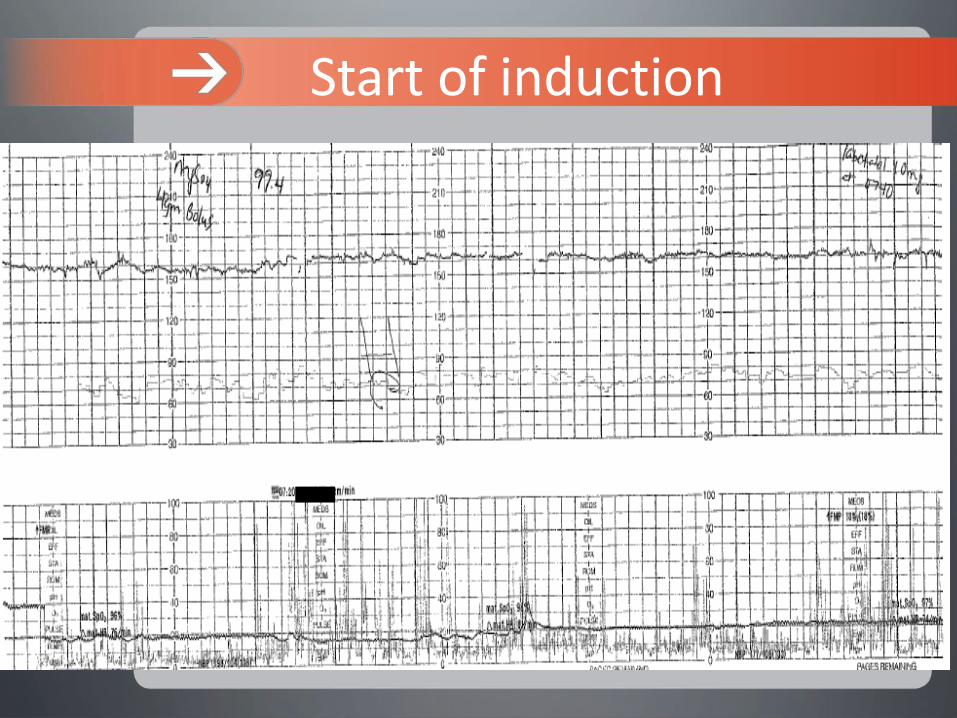
Start of induction
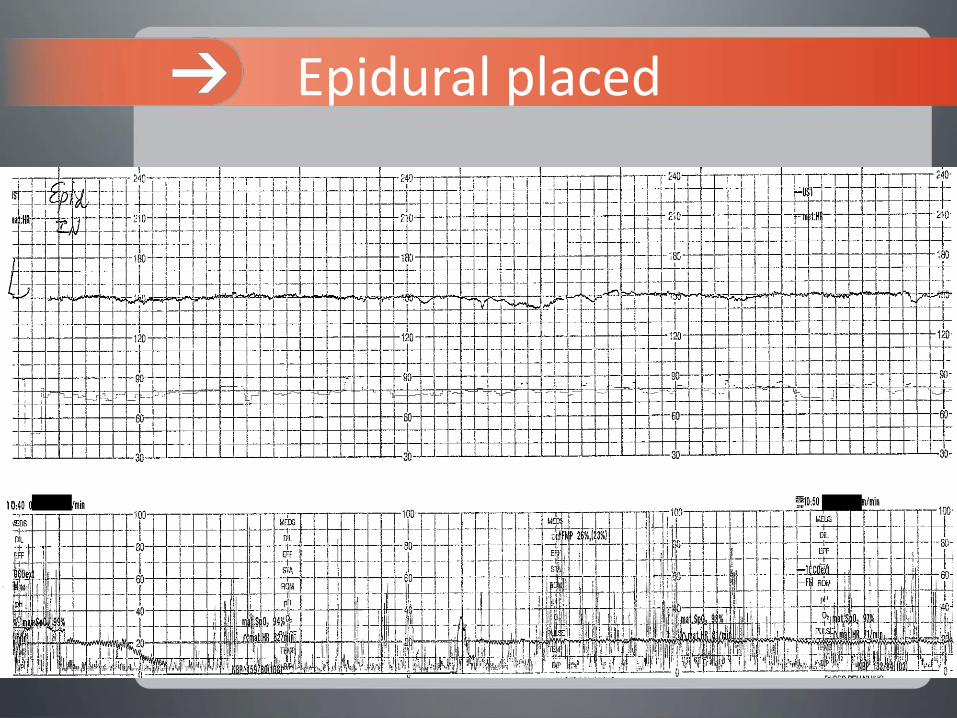
Epidural placed

Pitocin started
Provider here
AROM clear Int. monitor placed
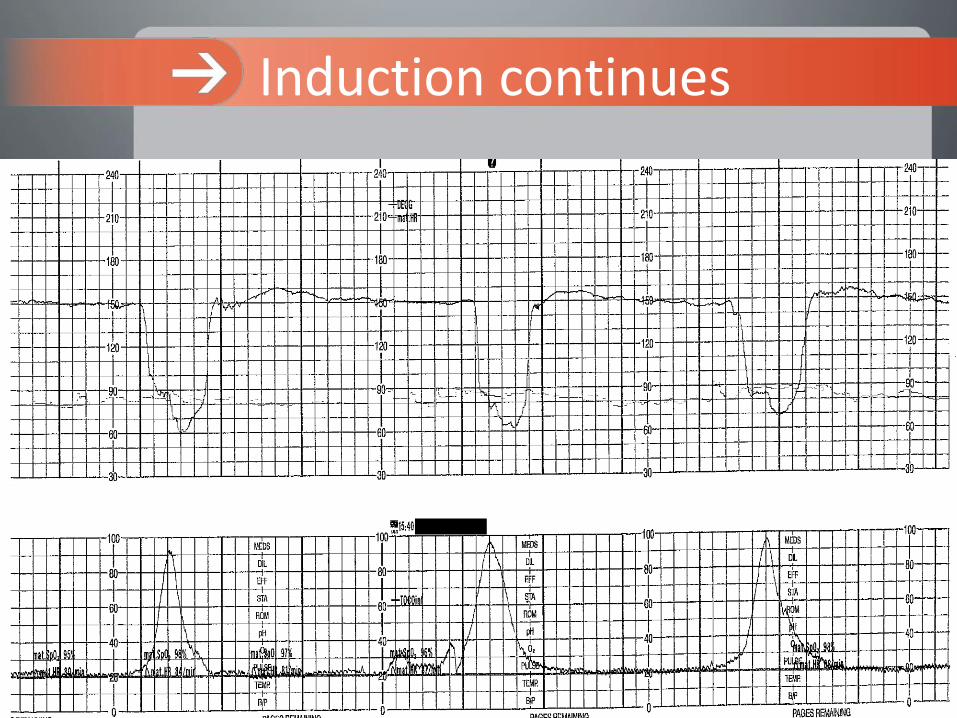
Induction continues
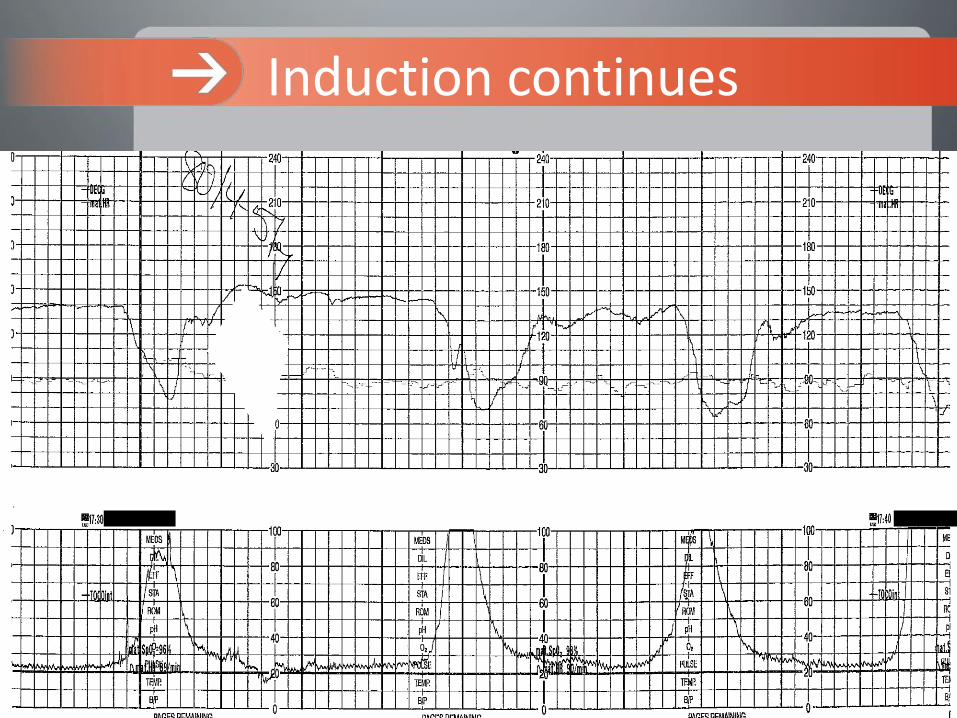
Induction continues

Induction continues

Induction continues

Delivery
Neonatal team present
WHAT WERE THE APGARS?

• Apgars:
–1 Min: 4
–5 Min: 6
• Intubated, given surfactant, and transferred to Neonatal unit
WHAT WAS THE CORD PH?

• Cord pH: 7.08
• PCO2: 84
• HCO3: 23.5
• Base Excess: -9.7
Cord gas
Case 2: Maternal History
• G1P0 at 37w4d
• Contractions and SROM
• Initial SVE @ 0920: 4-5cm
• BP 105/55, T 96.5, P 57
• GBS positive

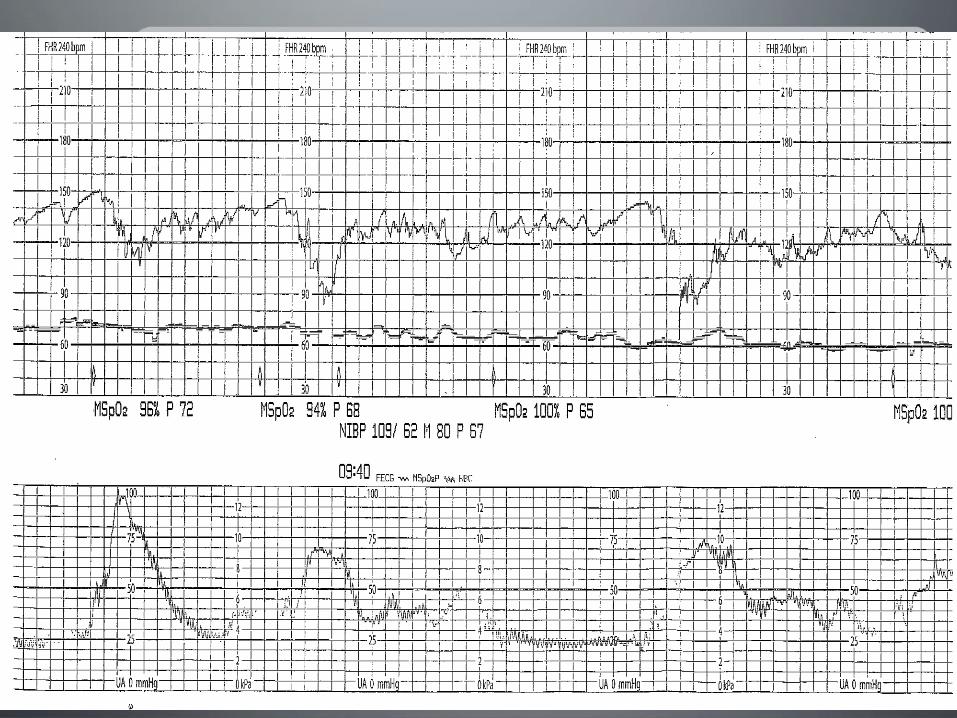
Admission


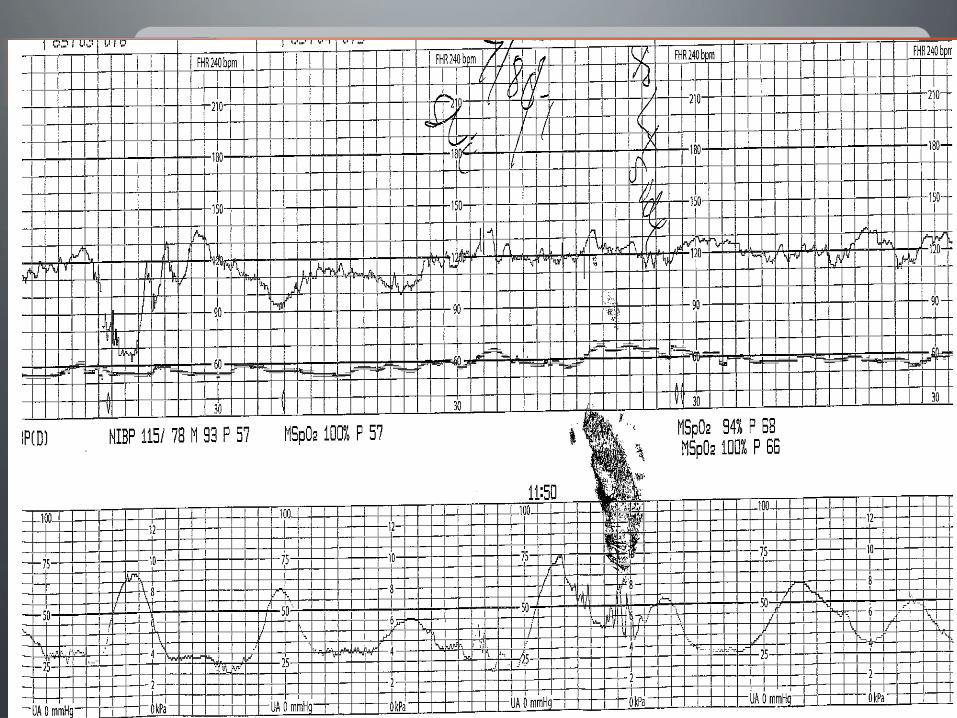
What can we do?!
•Amnioinfusion
Amnioinfusion
• Infusion of normal saline or lactated ringers via intrauterine pressure catheter
• Indications: Repetitive fetal heart rate decelerations
– Typically variable decelerations with oligohydramnios
Amnioinfusion
Adapted from North Market "Amnioinfusion Tipsheet"
• Follow your hospital’s protocol – Supplies
• IUPC • Infusion pump • 1 liter NS
– Technique • Connect NS to IUPC and attach pump • Administer bolus (300-500 cc) • Administer hourly rate as ordered
– Record • Amount/color of draining fluid • Uterine resting tone
Amnioinfusion
Hofmeyr GJ, Lawrie TA. Amnioinfusion for potential or suspected umbilical cord compression in labour. Cochrane Database of Systematic Reviews 2012, Issue 1. Art. No.: CD000013. DOI: 10.1002/14651858.CD000013.pub2.
• Outcomes – Reduced cesarean rate for fetal distress – No change in operative deliveries – Reduced repetitive variable decelerations – Higher mean umbilical artery pH – Reduced apgars of < 7 at 1 & 5 minutes – Less meconium below vocal cords (no change in
meconium aspiration) – No change to delivery time – No change to maternal infection


What were the Apgars?
Outcome
• NSVD at 1929
• Apgars 6 / 9
• Male infant
• 2580g/ 5lb 6oz
References
Hofmeyr GJ, Lawrie TA. Amnioinfusion for potential or suspected umbilical cord compression in labour. Cochrane Database of Systematic Reviews 2012, Issue 1. Art. No.: CD000013. DOI: 10.1002/14651858.CD000013.pub2.
American College of Obstetricians and Gynecologists. (2010). ACOG practice bulletin 116: Management of intrapartum fetal heart rate tracings. Obstetrics and Gynecology, 116(5), 1232-1240.
AWOHNN. (2003) Fetal heart monitoring principles and practices (3rd ed.). Washington, DC: Author.
Kennedy, B.B., Ruth, D.J, & Martin, E.J. (Eds.). (2009). Intrapartum management modules: A perinatal education program (4th ed.). Philadelphia: Lippincott, Williams & Wilkins.
Macones, G.A., Hankins, G.D., Spong, C.Y., Hauth, J., & Moore, T. (2008). The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: Update on definitions, interpretation, and research guidelines. JOGNN, 37(5), 510-515.
Discussion
Questions?
Comments?
Remember
• Fax or email attendance list to WAPC – fax: 608-285-5004
– email: [email protected]
• Evaluation will be sent via email from WAPC. Please complete to receive Continuing Education Credit.
• Continuing Education Certificate will be sent via email upon completion of evaluation.
• Archived version
• Become a member of WAPC! Join online: https://www.perinatalweb.org/n-pay/membership.asp
• Save the date for the 2016 WAPC Annual Perinatal Conference April 24-26, 2016, at the Osthoff Resort, Elkhart Lake.
Thank-you