best practices to achieve quality pressure-volume loop data in large animal models
TRANSCRIPT

Best-Practices to Achieve Quality Pressure-Volume Loop Data in Large Animal Models
Filip Konecny, DVM PhDTransonic
Tim Hacker, PhDUniversity of Wisconsin
Andy HentonInsideScientific
Sponsored by:

InsideScientific is an online educational environment designed for life science researchers. Our goal is to aid in
the sharing and distribution of scientific information regarding innovative technologies, protocols, research
tools and laboratory services.

Thank you to our event sponsor
Best-Practices for Successful PV Loop Data Collection in Large Animals
Filip Konecny, DVM PhD
Applications Scientist & Surgical Trainer
Transonic
Copyright 2015 Transonic & InsideScientific . All Rights Reserved.

THIS WEBINAR IS TO PRESENT A SERIES OF
“LARGE ANIMAL BEST PRACTICES” THAT WILL
EVOKE CONFIDENCE IN YOUR PV LOOP DATA
WHILE YOU ARE COLLECTING IT.
WHEN FOLLOWED, THE SANITY CHECKS PRESENTED WILL
PREVENT THE MULTIDISCIPLINARY TEAM FROM COLLECTING
INNACURATE DATA
Webinar Objectives…
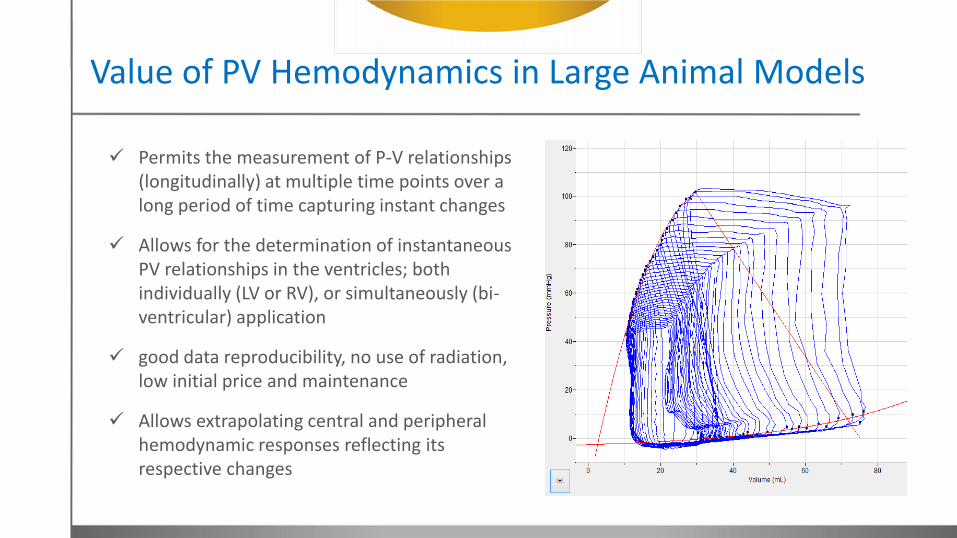
Permits the measurement of P-V relationships (longitudinally) at multiple time points over a long period of time capturing instant changes
Allows for the determination of instantaneous PV relationships in the ventricles; both individually (LV or RV), or simultaneously (bi-ventricular) application
good data reproducibility, no use of radiation, low initial price and maintenance
Allows extrapolating central and peripheral hemodynamic responses reflecting its respective changes
Value of PV Hemodynamics in Large Animal Models

Value of PV Hemodynamics in Large Animal Models
For more info please see our PV Workbook, pages 2-4
Echocardio (TTE) Cardiac CT Cardiac MRI PV (admittance)
Volumetry relies on geometric assumptions
Volumetry relies on geometric assumptions
Volumetry relies on geometric assumptions
PV corrects geometric assumption live
LOAD DEPENDENT LOAD DEPENDENT LOAD DEPENDENT LOAD DEPENDENT LOAD INDEPENDENT
Ventricle Pressure not measured
Ventricle Pressure not measured
Ventricle Pressure not measured
Ventricle Pressure measured/correlated with volume-live
Value of PV Hemodynamics in Large Animal Models
Click to Download the workbook

Control unit of PV system with “Large Animal” license, connects to data acquisition system (DAQ) using supplied analog cable.
Supplied HDMI cable connects the PV catheter to the control unit.
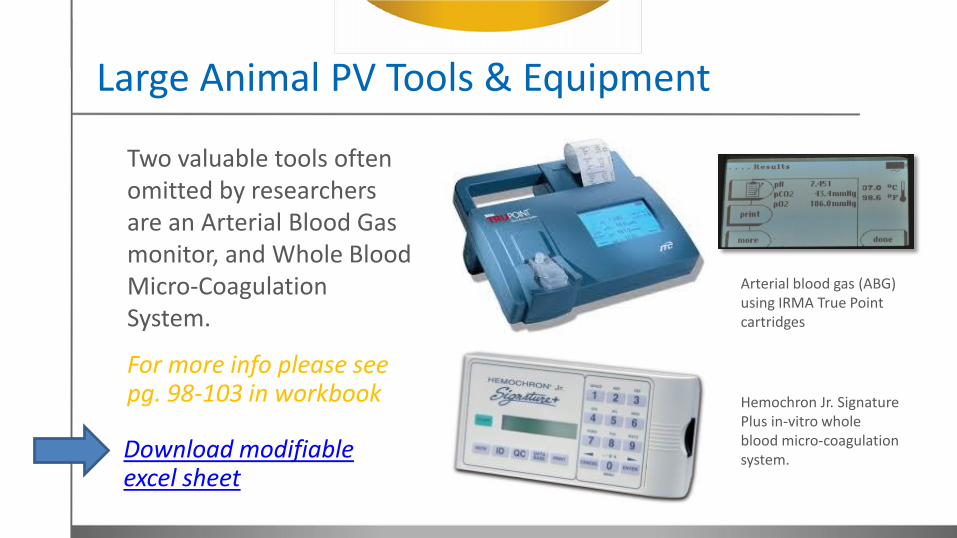
Large Animal PV Tools & Equipment
Large Animal PV Tools & Equipment
Hemochron Jr. Signature Plus in-vitro whole blood micro-coagulation system.
Two valuable tools often omitted by researchers are an Arterial Blood Gas monitor, and Whole Blood Micro-Coagulation System.
Arterial blood gas (ABG) using IRMA True Point cartridges
For more info please see pg. 98-103 in workbook
Download modifiable excel sheet

Variable Segment Length (VSL) Catheters
Excitation rings (1 and 4)
(1 and 5)
(1 and 6)
(1 and 7)
VSL Segm. 4
VSL Segm. 3
VSL Segm. 2
VSL Segm. 1

VSL Recording Rings to Ventricle Size
Size(OD)
Shaft Length
5F
45 inches(114.3cm)
Ventricle size
45-75mm
55-90 mm
5F -Pigtail (20, 30, 40, 50 mm) ring spacing
5F-Straight (50, 60, 70, 80 mm) ring spacing
Example of two 5F PV cathetersPigtail-AortaStraight-Apex
Numbers correspond to recording rings
VSL ring spacing is customizable
Data Accuracy Comes From Calibration
• PV systems track SV, EF and Contractility.
• Absolute Volume is mathematically calculated value.
• The calculation is based on three calibration values that the researcher needs to be aware of:
1. Stroke Volume Calibration Factor
2. Blood Resistivity (Rho)
3. Heart Type (Muscle Electrical Property)
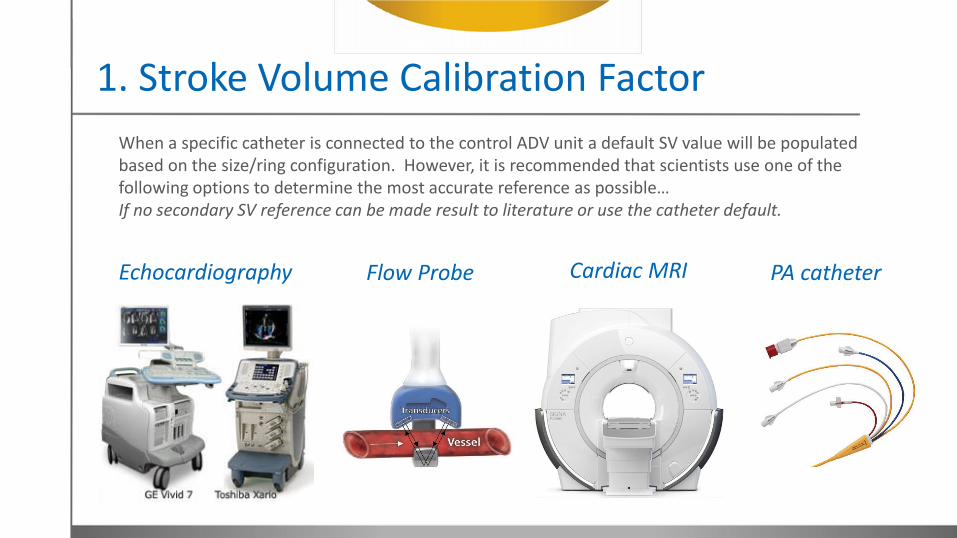
1. Stroke Volume Calibration Factor
When a specific catheter is connected to the control ADV unit a default SV value will be populated based on the size/ring configuration. However, it is recommended that scientists use one of the following options to determine the most accurate reference as possible… If no secondary SV reference can be made result to literature or use the catheter default.
Flow Probe PA catheterEchocardiography Cardiac MRI
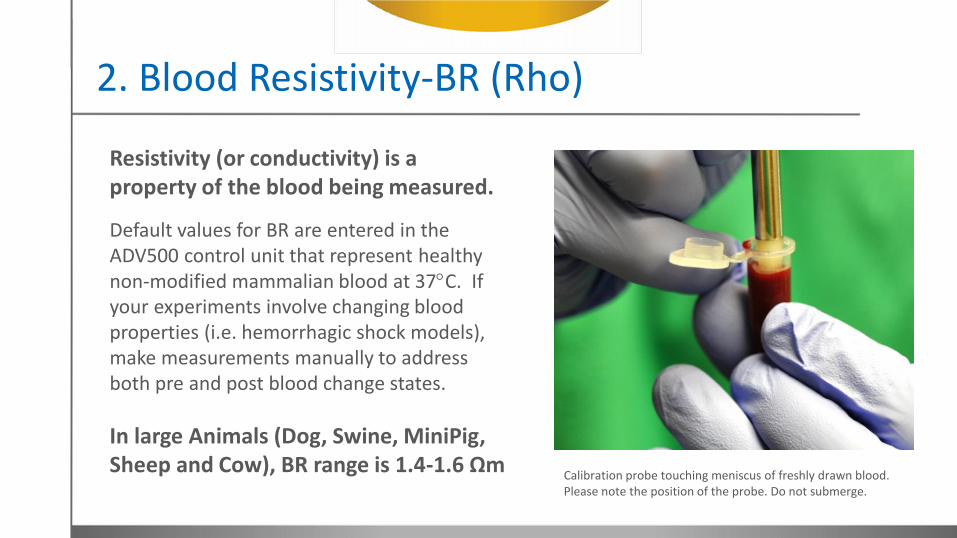
2. Blood Resistivity-BR (Rho)
Resistivity (or conductivity) is a property of the blood being measured.
Default values for BR are entered in the ADV500 control unit that represent healthy non-modified mammalian blood at 37C. If your experiments involve changing blood properties (i.e. hemorrhagic shock models), make measurements manually to address both pre and post blood change states.
In large Animals (Dog, Swine, MiniPig, Sheep and Cow), BR range is 1.4-1.6 Ωm
Calibration probe touching meniscus of freshly drawn blood. Please note the position of the probe. Do not submerge.
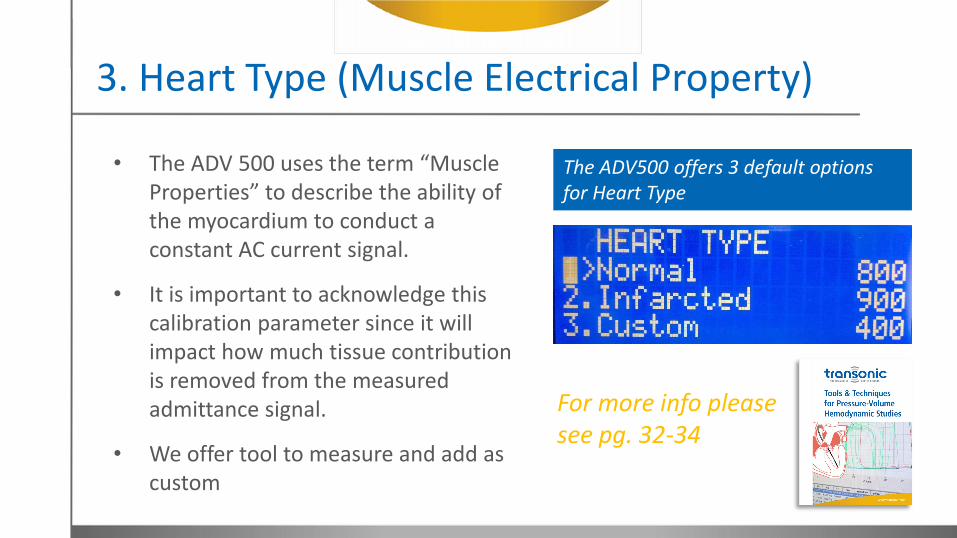
3. Heart Type (Muscle Electrical Property)
• The ADV 500 uses the term “Muscle Properties” to describe the ability of the myocardium to conduct a constant AC current signal.
• It is important to acknowledge this calibration parameter since it will impact how much tissue contribution is removed from the measured admittance signal.
• We offer tool to measure and add as custom
For more info please see pg. 32-34
The ADV500 offers 3 default options for Heart Type

Example: 72kg Swine
Animal Phase Range Phase Amplitude Magnitude Range Magnitude Amplitude
Swine large (>65kg) 1-3 degrees 1.5 degree 15-30 mS 4-6 mS
Example of left ventricle PV data using 7F PV catheter with pigtail; electrode ring spacing: 50,60,70,80mm
Insertion: RCA/Aorta
Active Segment: VSL 3
Note: Channel 1 and 2 (ECG)

Suggested Reading…
Large animal models of heart failure: a critical link in the translation of basic science to clinical practice.
Admittance-based pressure-volume loops versus gold standard cardiac magnetic resonance imaging in a porcine model of myocardial infarction.
Right Ventricular Energetics and Power in Pulmonary Regurgitation vs. Stenosis Using Four-Dimensional Phase-Contrast Magnetic Resonance
Invasive surgery reduces infarct size and preserves cardiac function in a porcine model of myocardial infarction.
Admittance-based pressure-volume loop measurements in a porcine model of chronic myocardial infarction.

Large Animal Left and Right Ventricular PV Loops
Tim Hacker, PhD
Director, Cardiovascular Physiology Core
University of Wisconsin-Madison
Copyright 2015 T. Hacker, Transonic & InsideScientific. All Rights Reserved.
A bit of background…
• Developed 22 different cardiovascular animal models in animals from mice to primates
• Measurement & imaging of structural and physiologic parameters in all models
• Currently using PV loops:– to measure LV function in stem cell treated infarcted swine hearts – to measure RV function a dog model of pulmonary hypertension
• Using the ADV500 system in large animals for 3 years and small animals for over 5
Our Tools & Equipment List
1. 0.035 J guide wires (several)
2. Guide catheters or long sheaths (9Fr)
3. 7 Fr VSL straight tip and pig tail catheters, 9 and 11 Fr sheaths
4. Swan-Ganz Catheter (thermodilution) to measure SV
5. Infusion pump for dobutamine
6. Patient monitor
7. Ventilator (intubate)
8. Percutaneous access kit (ultrasound)
Tip: Get the largest balloon you can find for occlusions (24 mm)

How we choose the right catheter
Approach: carotid, jugular, femoral, apical stab
Ventricle: right or Left
Heart Size: overall length and internal space
Operator Preference: over the wire vs. pig tail
What works for us:
• LV carotid = 7Fr pig tail VSL (terminal)
• LV femoral = 7Fr straight over the wire (survival)
• RV jugular = 7Fr straight over the wire (survival or terminal) with long curved sheath.
Anesthesia
Pre-anesthesia:
Pigs: Xylazine 2mg/kg and Telazol 4 mg/kg IM
Dogs: Morphine Sulfate 0.5 mg/kg and Acepromazine 0.5 mg/kg SQ
Extra anesthesia: Propofol 2-40 mg/kg IV
Procedure anesthesia: Isoflurane (2%)
Tip: learn about use of anesthetics and their reported hemodynamic effects before PV experimentation
Catheter Insertion
If Terminal -- Cut down of carotid or jugular
If Survival -- Percutaneous femoral or jugular (ultrasound guidance)
• 9-11 Fr sheaths (dilate up as needed to get the large sheaths in)
• Right Ventricle, we use a 60cm long sheath with an ‘L’ shaped tip to deliver the catheter to junction of the SVC and the RA
• We cover the catheter with a sleeve during insertion through the sheath’s diaphragm.
• Percutanous access of femoral vein for Swan Ganz and balloon
Tip: An experienced cardiologist is valuable to show you the ropes, but ultimately once in the vessels it is not overly difficult to place the catheters.
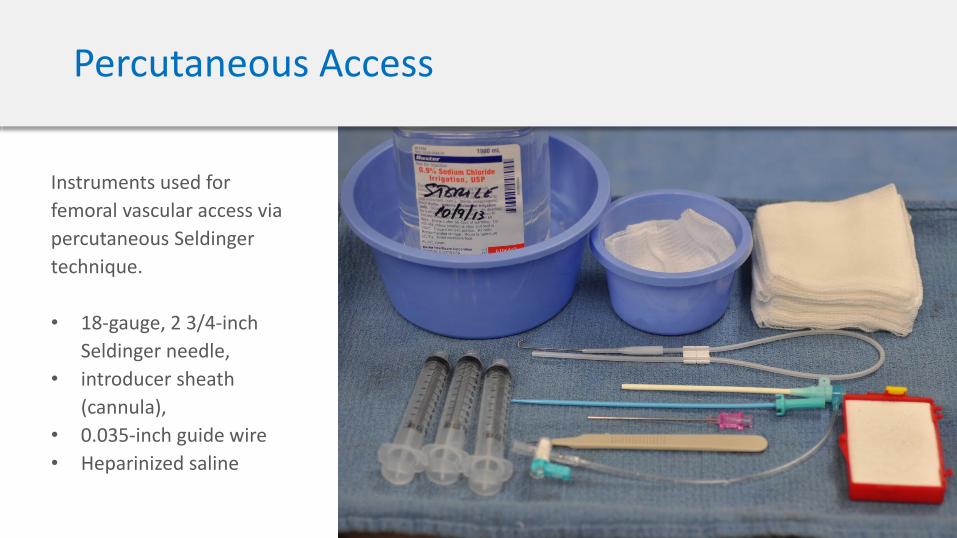
Percutaneous Access
Instruments used for
femoral vascular access via
percutaneous Seldinger
technique.
• 18-gauge, 2 3/4-inch
Seldinger needle,
• introducer sheath
(cannula),
• 0.035-inch guide wire
• Heparinized saline

Femoral vasculature
access via percutaneous
Seldinger technique.
Needle is inserted into the
arterial lumen to advance
an 0.035-inch guide wire
before the introduction of
a 7F sheath (cannula).
Percutaneous Access
Tip: Color code your lines (Artery = Red)
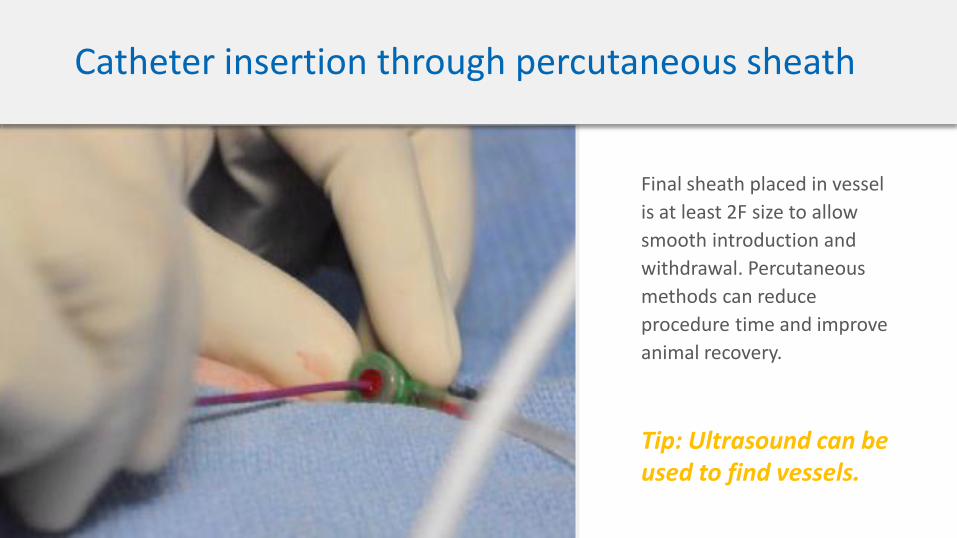
Catheter insertion through percutaneous sheath
Final sheath placed in vessel
is at least 2F size to allow
smooth introduction and
withdrawal. Percutaneous
methods can reduce
procedure time and improve
animal recovery.
Tip: Ultrasound can be used to find vessels.

Catheter Placement
1. Swan Ganz, use pressures and fluoroscopy to guide
2. PV catheter use contrast to get road map
3. Fluoro to guide into heart -- run wire or sheath to desired location
4. Note number of segments in ventricle
5. Check PV loops and phase/pressure to refine location
6. Run occlusion balloon to above diaphragm but below heart apex
Tip: Patience and a light touch are a key to proper placement.
Tip: Rotate catheter to get pressure window away from cords/papillary
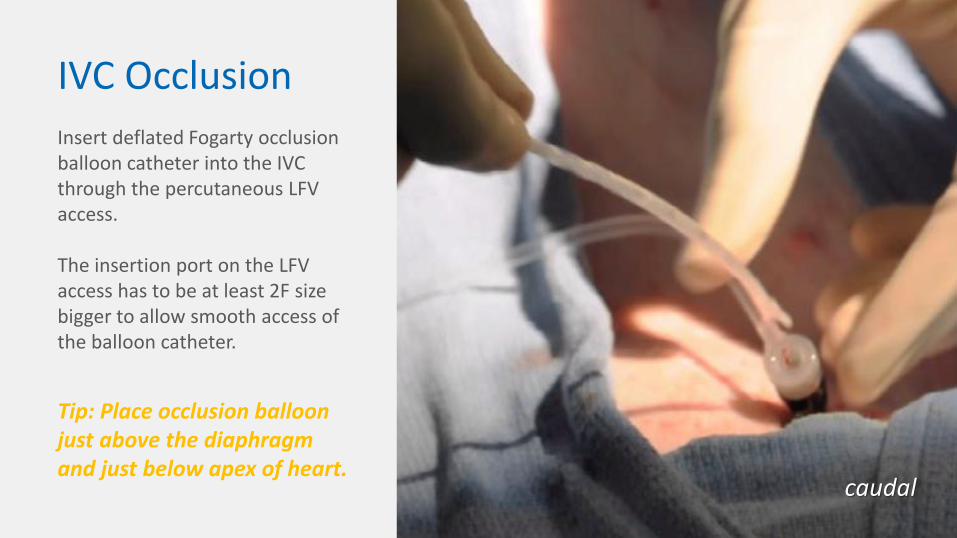
IVC Occlusion
caudal
Insert deflated Fogarty occlusion balloon catheter into the IVC through the percutaneous LFV access.
The insertion port on the LFV access has to be at least 2F size bigger to allow smooth access of the balloon catheter.
Tip: Place occlusion balloon just above the diaphragm and just below apex of heart.

Monitoring Physiology
Measurement Dog (10-20 kg) Swine (25-50 kg)
Temperature 99.5 - 102 F / 37.5 - 39.0 °C 100 - 102.5 F / 37.5 - 39.5 °C
Respiration Rate 12 - 18 breaths/min 12 - 20 breaths/min
Heart Rate 75 - 105 beats/min 85 - 115 beats/min
EtCO2 35 - 45 mmHg 35 - 45 mmHg
SpO2 93 - 100 % 93 - 100 %

Tip: vital signs monitoring is crucial for PV repeatability
Tip: Body temp and hydration changes will affect heart rate and SV
Tip: Check pressure & HR trends during long procedures to confirm stability
Monitoring Physiology
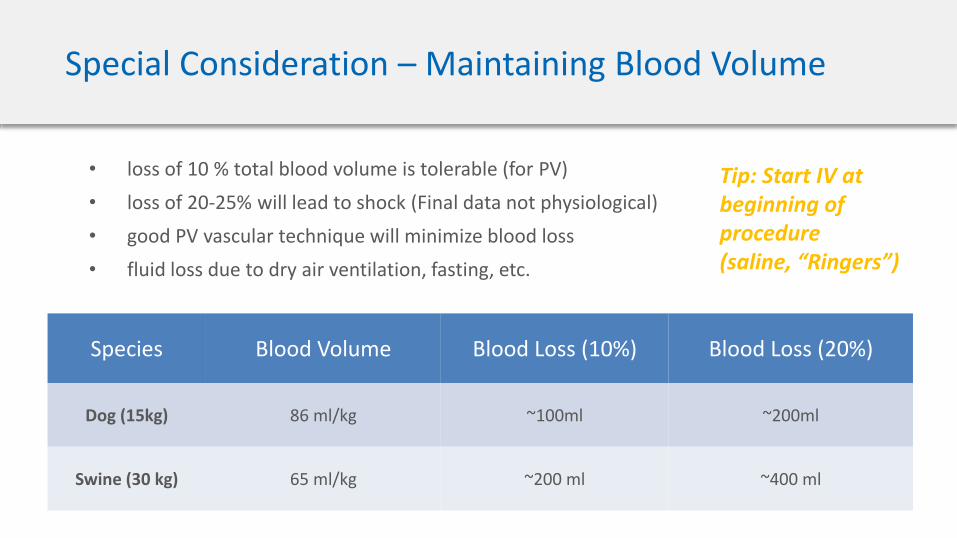
Special Consideration – Maintaining Blood Volume
• loss of 10 % total blood volume is tolerable (for PV)
• loss of 20-25% will lead to shock (Final data not physiological)
• good PV vascular technique will minimize blood loss
• fluid loss due to dry air ventilation, fasting, etc.
Species Blood Volume Blood Loss (10%) Blood Loss (20%)
Dog (15kg) 86 ml/kg ~100ml ~200ml
Swine (30 kg) 65 ml/kg ~200 ml ~400 ml
Tip: Start IV at beginning of procedure (saline, “Ringers”)
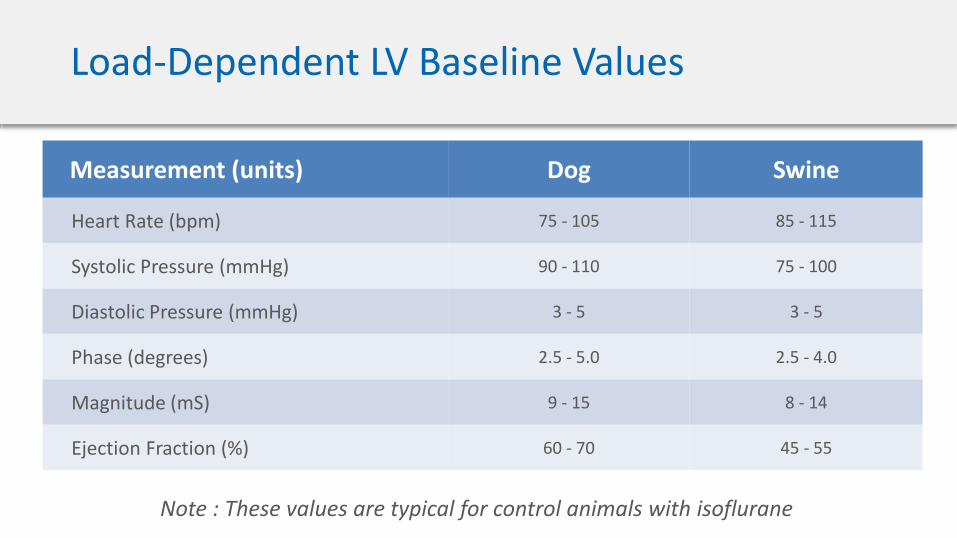
Load-Dependent LV Baseline Values
Measurement (units) Dog Swine
Heart Rate (bpm) 75 - 105 85 - 115
Systolic Pressure (mmHg) 90 - 110 75 - 100
Diastolic Pressure (mmHg) 3 - 5 3 - 5
Phase (degrees) 2.5 - 5.0 2.5 - 4.0
Magnitude (mS) 9 - 15 8 - 14
Ejection Fraction (%) 60 - 70 45 - 55
Note : These values are typical for control animals with isoflurane
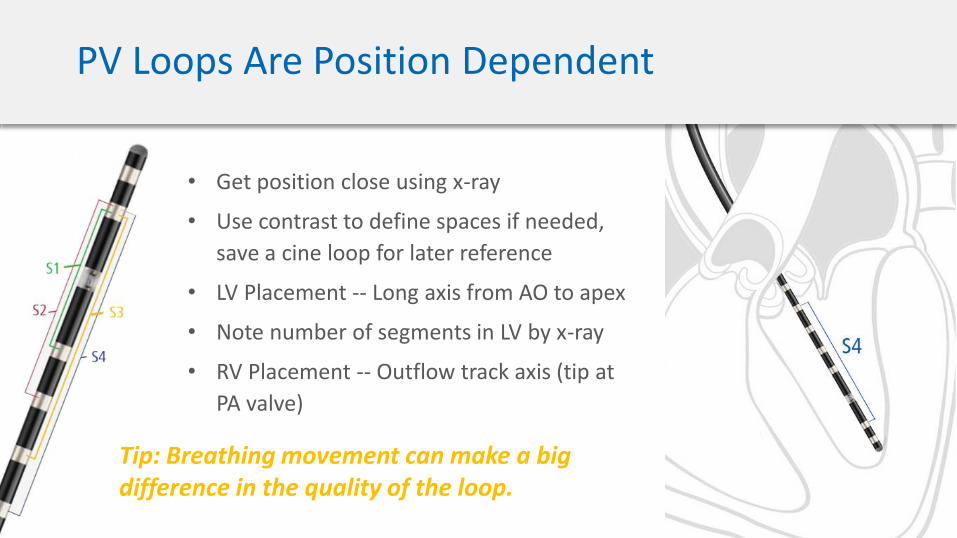
PV Loops Are Position Dependent
• Get position close using x-ray
• Use contrast to define spaces if needed,
save a cine loop for later reference
• LV Placement -- Long axis from AO to apex
• Note number of segments in LV by x-ray
• RV Placement -- Outflow track axis (tip at
PA valve)
Tip: Breathing movement can make a big difference in the quality of the loop.
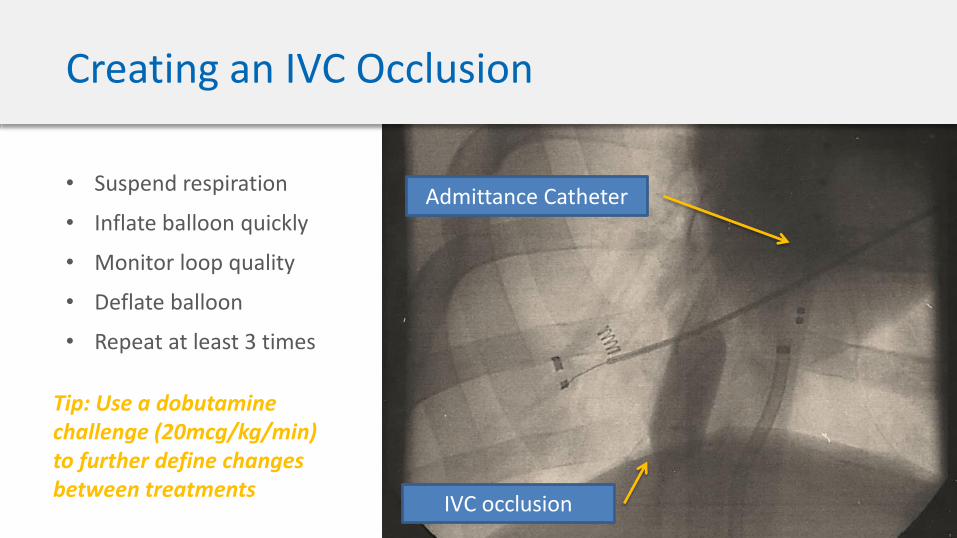
Creating an IVC Occlusion
IVC occlusion
Admittance Catheter
Tip: Use a dobutaminechallenge (20mcg/kg/min) to further define changes between treatments
• Suspend respiration
• Inflate balloon quickly
• Monitor loop quality
• Deflate balloon
• Repeat at least 3 times
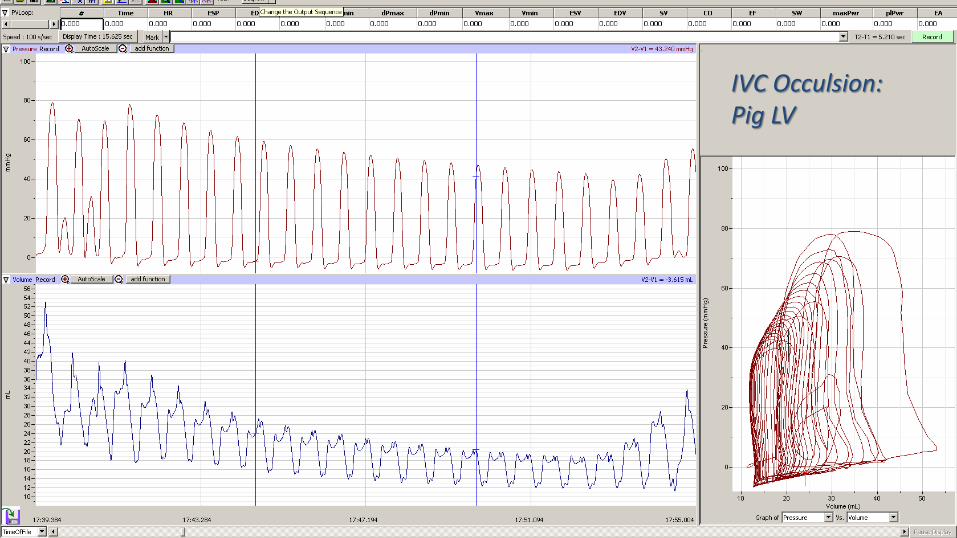
IVC Occulsion:Pig LV

IVC Occulsion: Dog LV
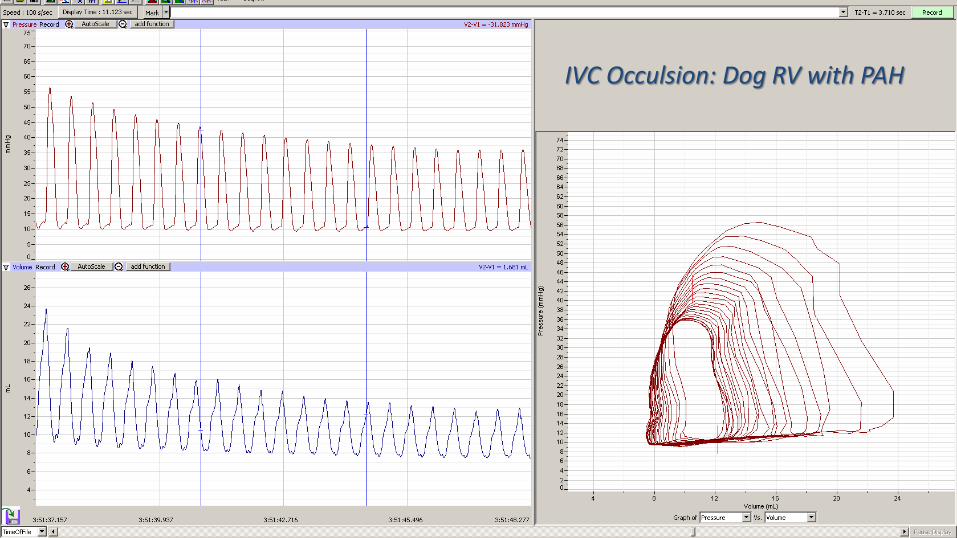
IVC Occulsion: Dog RV with PAH
Suggested Reading…
Intravenous Followed by X-ray Fused with MRI-Guided Transendocardial Mesenchymal Stem Cell Injection Improves Contractility Reserve in a Swine Model of Myocardial Infarction.
View additional publications from Dr. Tim Hacker
Thank You!For additional information on solutions for large animal PV loops and hemodynamic monitoring equipment please visit:
http://transonic.com/