behavioral sleep medicine techniques for sleep apnea … · behavioral sleep medicine techniques...
TRANSCRIPT

© Associated Professional Sleep Societies, LLC 1
Behavioral sleep medicine techniques for sleep apnea patients
Jack D. Edinger, Ph.D., C.B.S.M.National Jewish Health, Denver, CO
Duke University Medical Center, Durham, NC
© Associated Professional Sleep Societies, LLC 2
Conflict of Interest Disclosures for Speakers1. I do not have any relationships with any entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients, OR
x 2. I have the following relationships with entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients.
Type of Potential Conflict Details of Potential Conflict
Grant/Research Support National Institutes of Health; Merck; Philips Respironics
Consultant
Speakers’ Bureaus
Financial support
Other Oxford University Press; Springer Press (Book Royalties)
3. The material presented in this lecture has no relationship with any of these potential conflicts, OR
x 4. This talk presents material that is related to one or more of these potential conflicts, and the following objective references are provided as support for this lecture:
1. Bjornsdottir E, Janson C, Sigurdsson JF, Gehrman P, Perlis M, Juliusson S, Arnardottir ES, Kuna ST, Pack AI, Gislason T, Benediktsdottir B. Symptoms of insomnia among patients with obstructive sleep apnea before and after two years of positive airway pressure treatment. Sleep. 2013;36(12):1901-9. doi: 10.5665/sleep.3226. PubMed PMID: 24293765; PubMed Central PMCID: PMC3825440.
2. Guilleminault C, Davis K, Huynh NT. Prospective Randomized Study of Patients with Insomnia and Mild Sleep Disordered Breathing. Sleep. 2008;31(11):1527-33. PubMed PMID: WOS:000260550100011.
© Associated Professional Sleep Societies, LLC 3
Presentation Objectives/OutlineWhat the BSM specialist has to offer OSA patients
Techniques for Promoting CPAP Adherence Graded Exposure Therapy for CPAP related claustrophobia Motivational Interviewing Risk Perception Enhancement through Personalized Videos
Interventions for Insomnia Disorder occurring comorbid to OSA
[Weight reduction interventions] – not discussed

© Associated Professional Sleep Societies, LLC 4
*Stepnowsky CJ, Jr., Moore, PJ. Nasal CPAP treatment for obstructive sleep apnea:
developing a new perspective on dosing strategies and compliance. J Psychosom Res. 2003
Jun;54(6):599-605.
• PAP is safe, effective non-invasive 1st line therapy• However PAP adherence remains a challenge
– Initial acceptance rate is 70-75%*– > 50% patients started on CPAP not using it after 1 year*– Most of those using PAP at 1 year, use it < prescribed*
• < entire night• < nightly use
PAP Adherence ‐ Background

© Associated Professional Sleep Societies, LLC 5
PAP Usage Across 12‐Month RCT
4.8
73.6
34.4
7
0
10
20
30
40
50
60
70
80
Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 Month 7 Month 8 Month 9 Month 10 Month 11 Month 12
Percen
t of sam
ple
Degrees of PAP Adherence Across 12 Months
0 hours per night > 0 & < 2 Hrs 2 to 4 Hrs 4 to 6 Hrs >= 6 hours
0
60
120
180
240
300
MONTH 1 MONTH 2 MONTH 3 MONTH 4 MONTH 5 MONTH 6 MONTH 7 MONTH 8 MONTH 9 MONTH 10 MONTH 11 MONTH 12
Minutes of U
se
PAP Mean Hrs Used/Night N = 273
© Associated Professional Sleep Societies, LLC 6
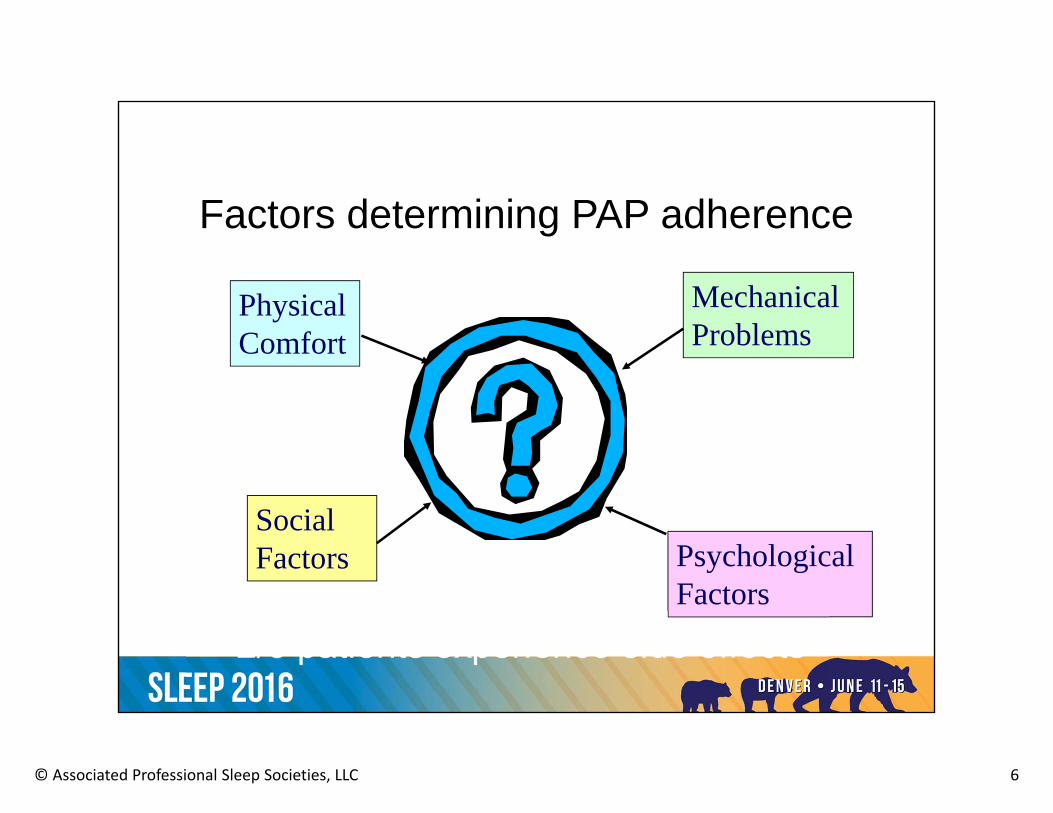
Factors determining PAP adherence
PhysicalComfort
Psychological Factors
Social Factors
Mechanical Problems

© Associated Professional Sleep Societies, LLC 7
Psychological factors affecting PAP use• Anxiety reactions
– Claustrophobia– fear of suffocation– sense of being trapped - panic
• Comorbid Psychiatric Conditions• Beliefs/Attitudes about OSA Risks and PAP
– “My OSA is not that serious”– “PAP does little to improve my symptoms”

© Associated Professional Sleep Societies, LLC 8
Conditioned Arousal
Panic/Anxiety
+ BellMeat powder
Drooling
UCSCS
UCR
Drooling
CR
ConfinementRestricted breathing
UCS
+ CS
UCR CR
Panic/Anxiety

© Associated Professional Sleep Societies, LLC 9
Mask Removal(PAP Avoidance)
= immediate anxiety
decrease
Reinforcement of Mask Removal
Anxiety
Anxiety

© Associated Professional Sleep Societies, LLC 10
Case Example

© Associated Professional Sleep Societies, LLC 11
Graded Exposure Treatment of PAP Anxiety ReactionsSample PAP Exposure Hierarchy
1. Connect the mask and hose to the PAP unit. Hold the mask over your face and turn on the PAP. Practice breathing with the machine on while you are awake.
2. Strap the mask on your head, and turn on the CPAP. Practice breathing with the mask on, starting with 5 to 10 min and gradually increasing time for longer periods up to 20 to 30 min.
3. Take a short daytime nap with PAP. Start with 5-10 minute nap and gradually increase up to 30 minutes +.
4. Reintroduce PAP into nighttime sleep. You can begin using it a portion of the night and gradually increase up to entire night.
*Proceed from one step to the next only when you are completely comfortable. If you feel any anxiety or discomfort, return to previous step, then proceed again when comfortable.
© Associated Professional Sleep Societies, LLC 12
Graded PAP Exposure: Tracking Progress

© Associated Professional Sleep Societies, LLC 13
Objective Measures of Practice Adherence
© Associated Professional Sleep Societies, LLC 14
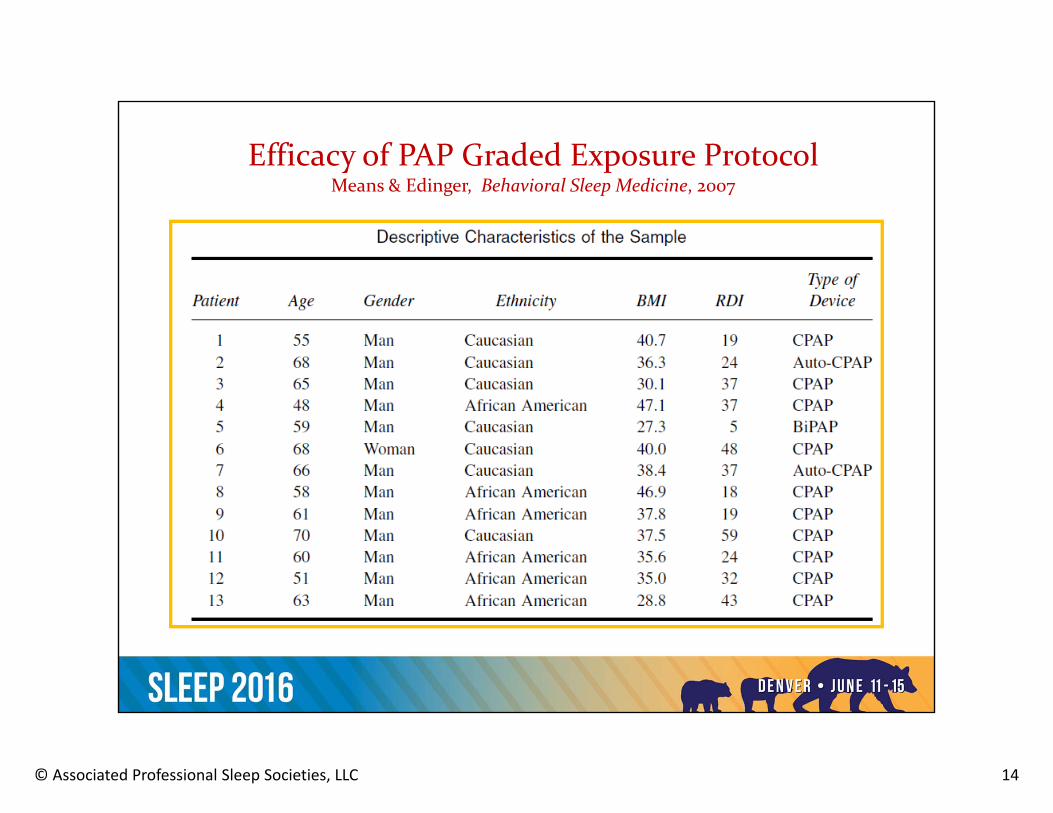
Efficacy of PAP Graded Exposure Protocol Means & Edinger, Behavioral Sleep Medicine, 2007
%

© Associated Professional Sleep Societies, LLC 15
Efficacy of PAP Graded Exposure Protocol Means & Edinger, Behavioral Sleep Medicine, 2007
© Associated Professional Sleep Societies, LLC 16
Case Example
• 60 year old African American Female• Marital status: Divorced• Hx of OSA since 2003 – AHI = 11• Hx of treatment with CPAP and BiPAP• Referred due to PAP intolerance
© Associated Professional Sleep Societies, LLC 17
Medical HistoryProblems Medication
List• Diabetes Ambien Albuterol• HTN Amlodipine• Obesity – BMI = 35.2 ASA• Osteoarthritis Wafarin• Renal Disease Cozaar• Asthma Allopurinol Zocar• GERD Insulin

© Associated Professional Sleep Societies, LLC 18
Psychiatric History
• PTSD related to hx of domestic violence• Engaged in active treatment (UCMC)
– Group and individual therapy– Sertraline for PTSD & Depression
• Benefiting from treatment but has recurrent memories of domestic abuse

© Associated Professional Sleep Societies, LLC 19
OSA Treatment History• Given Trials of CPAP & BiPAP• Most recent titration shows BiPAP @ 26/21
most effective• Patient intolerant to therapy
– Reminds her of ex-husband trying to suffocate her
– Gets palpitations when she hears PAP machine on
– Anxious when in same room as PAP• Longest usage per night = 3 hours• Not using PAP at all at time of referral
© Associated Professional Sleep Societies, LLC 20
Treatment Approach
• Graded Exposure • 6 visits between July 2013 and April 2014
– First visit (1 hr.) = assessment + treatment introduction
– Subsequent visits (30 min) = follow-up & support
© Associated Professional Sleep Societies, LLC 21
PAP Exposure Hierarchy
1. Get comfortable with CPAP in same room2. Connect the mask and hose to the PAP unit. Hold the mask over your face and
turn on the PAP. Practice breathing with the machine on while you are awake.
3. Strap the mask on your head, and turn on the CPAP. Practice breathing with the mask on, starting with 5 to 10 min and gradually increasing time for longer periods up to 20 to 30 min.
4. Take a short daytime nap with PAP. Start with 5‐10 minute nap and gradually increase up to 30 minutes +.
5. Reintroduce PAP into nighttime sleep. You can begin using it a portion of the night and gradually increase up to entire night.
*Proceed from one step to the next only when you are completely comfortable. If you feel any anxiety or discomfort, return to previous step, then proceed again when comfortable.

© Associated Professional Sleep Societies, LLC 22
Treatment Outcome
© Associated Professional Sleep Societies, LLC 23
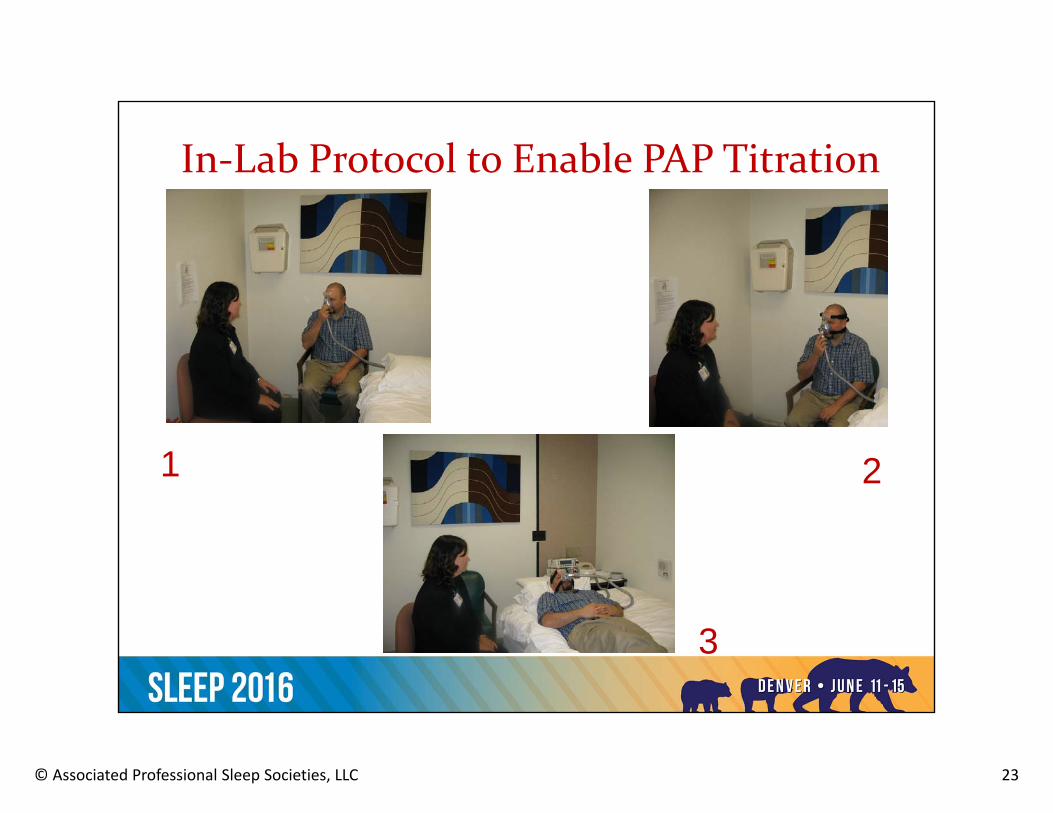
In‐Lab Protocol to Enable PAP Titration
1 2
3

© Associated Professional Sleep Societies, LLC 24
Motivational Interviewing Intervention for PAP Adherence
Aloia et al, Sleep, 2013

© Associated Professional Sleep Societies, LLC 25
Use of Personalized Videos to Enhance Risk Perception
Aloia et al., Sleep (suppl) 2013
Average CPAP Hourly Adherence By Group
2
4
6
8
week1
month1
month2
month3
allmon
ths
Date
Hour
s pe
r nig
ht
BPVNPV
6.2 hrs
4.2 hrs

© Associated Professional Sleep Societies, LLC 26
Management of the OSA Patient with Comorbid Insomnia Disorder

© Associated Professional Sleep Societies, LLC 27

© Associated Professional Sleep Societies, LLC 28
Relative Disease Risk: OSA+I vs. OSA‐IGupta & Knapp, PLoS ONE 9(3): e90021. doi:10.1371/
journal.pone.0090021

© Associated Professional Sleep Societies, LLC 29
Impact of comorbid apnea on insomnia patients’ medical and mental health
Data from Edinger et al. Archives of General Psychiatry, 2011
43.1
29.3
010
20304050607080
Insomnia +Apnea
Insomnia Only
%
DepressionNo Depression
N = 304 adults who met RDC for insomnia disorder

© Associated Professional Sleep Societies, LLC 30
ISI & Epworth Score RangesClinic Data – 65 OSA + Insomnia vs. 64 Insomnia only
0
25
50
75
100
Insomnia+OSA Insomnia Other
Daytime Sleepiness and Insomnia Diagnosis
ESS <= 10 ESS > 10
0
25
50
75
100
Insomnia+OSA Insomnia Other
ISI Score Ranges by Insomnia Grouping
ISI< 8 ISI 8-14 ISI 15-21 ISI >=22
P = .05P = .02
© Associated Professional Sleep Societies, LLC 31
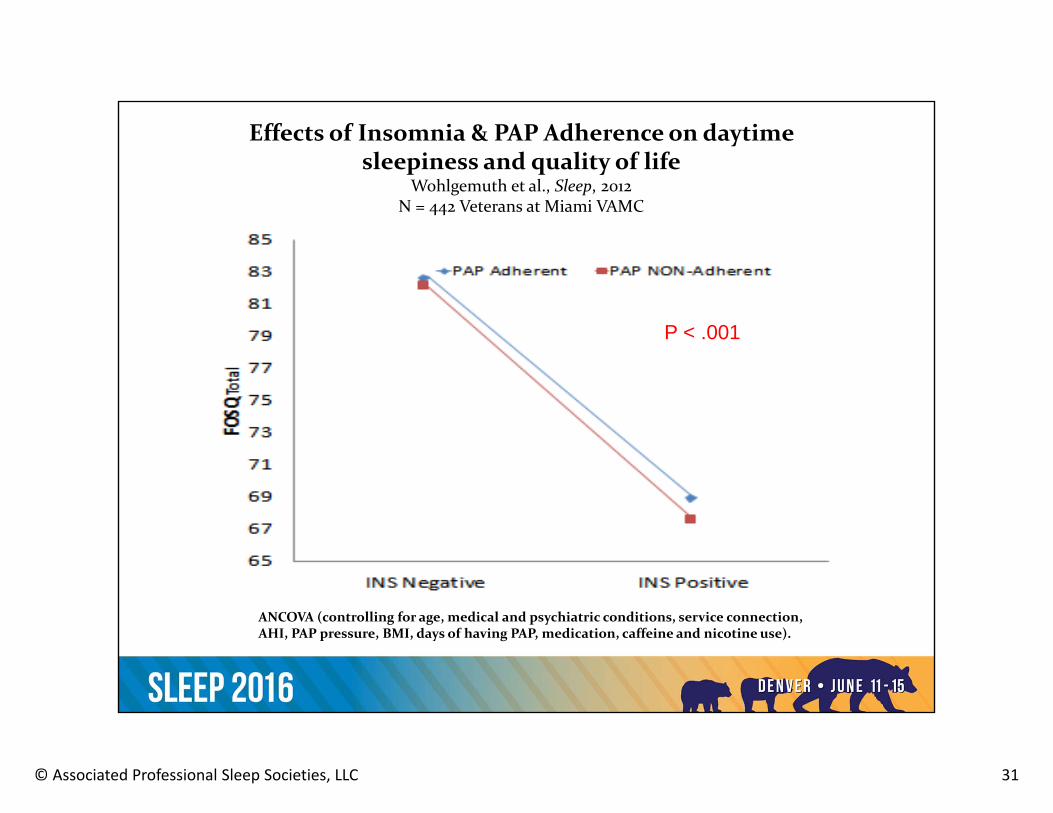
ANCOVA (controlling for age, medical and psychiatric conditions, service connection, AHI, PAP pressure, BMI, days of having PAP, medication, caffeine and nicotine use).
Effects of Insomnia & PAP Adherence on daytime sleepiness and quality of life
Wohlgemuth et al., Sleep, 2012N = 442 Veterans at Miami VAMC
P < .001
© Associated Professional Sleep Societies, LLC 32
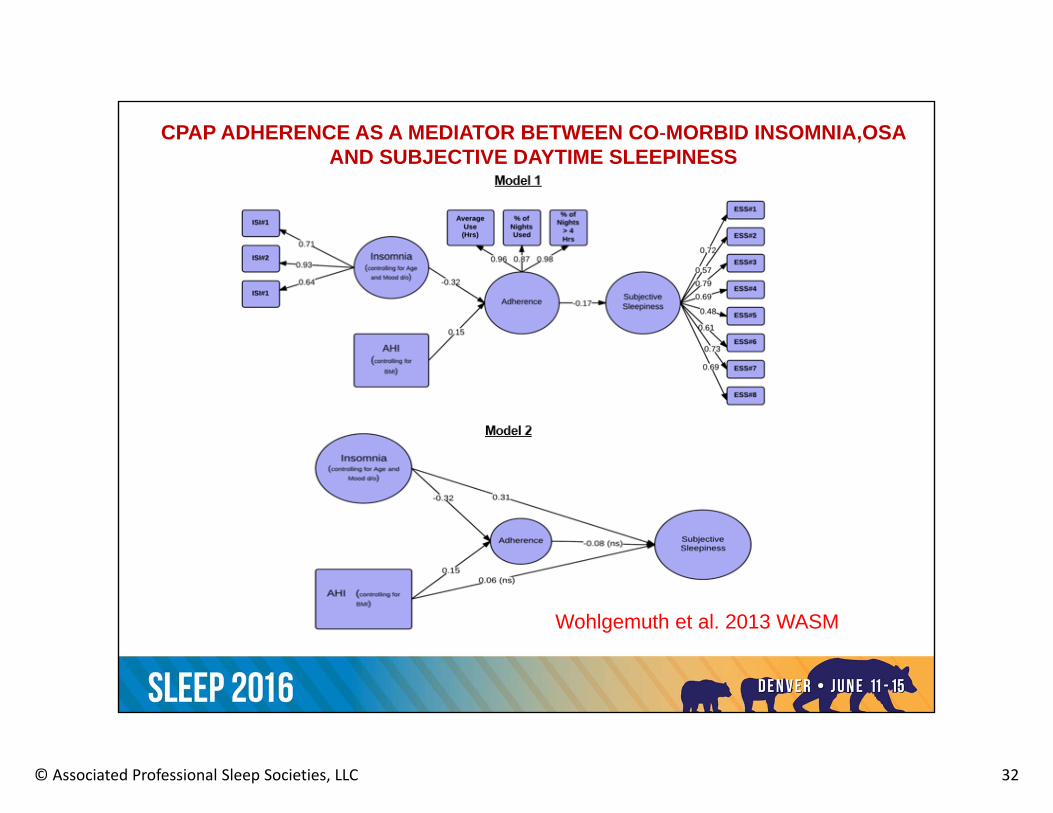
Wohlgemuth et al. 2013 WASM
CPAP ADHERENCE AS A MEDIATOR BETWEEN CO‐MORBID INSOMNIA,OSA AND SUBJECTIVE DAYTIME SLEEPINESS

© Associated Professional Sleep Societies, LLC 33
What is known about treating patients with comorbid insomnia & OSA?

© Associated Professional Sleep Societies, LLC 34
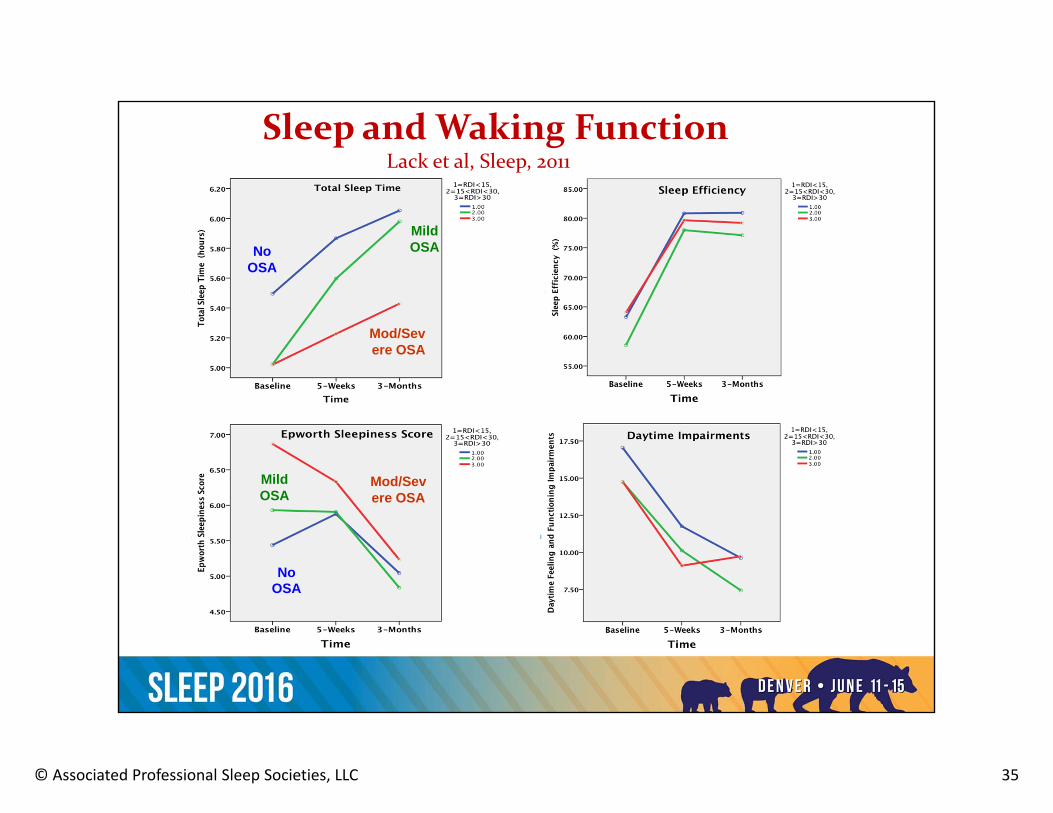
Efficacy of CBT with Comorbid insomnia &OSALack et al, Sleep, 2011
• N= 344 consecutive patients in an insomnia treatment program who met the criteria of chronic insomnia
• A full home diagnostic PSG was conducted pre-treatment. • Sample characteristics
• 219 with primary insomnia • 92 with co-morbid mild OSA (apnea/hypopnea index, 15<AHI<30) • 33 patients with moderate to severe OSA (AHI>30).
• Outpatient treatment program for insomnia • stimulus control therapy & bedtime restriction therapy • cognitive therapy (sleep education, sleep perception re-training, relaxation) • bright light therapies appropriate to needs of each patient.
• Measures = 7-day sleep diaries & daytime functioning questionnaires • Baseline, after 5 weeks and at 3 month follow-up.
© Associated Professional Sleep Societies, LLC 35
Sleep and Waking FunctionLack et al, Sleep, 2011
No OSA
Mod/Severe OSA
Mild OSA
No OSA
Mild OSA
Mod/Severe OSA

© Associated Professional Sleep Societies, LLC 36
Sequential Treatment CBT for Insomnia and OSA TherapyKrakow et al., Sleep and Breathing, 2004
ISI FOSQ
Results from 17 patients who received either PAP (n=14); Oral appliance (n=2); or surgical (n=1) OSA therapy after CBT

© Associated Professional Sleep Societies, LLC 37
CBT + Surgical Treatment of Comorbid OSA & InsomniaGuilleminault et al., Sleep, 2008

© Associated Professional Sleep Societies, LLC 38
Overall ConclusionsGuilleminault, et al., Sleep 2008
OSA treatment alone eliminated insomnia complaints in only 5 of 15 patients
CBT did not improve most sleep variables
Combined therapy needed to normalize sleep and associated complaints in the majority of subjects
© Associated Professional Sleep Societies, LLC 39
Clinical Considerations & Case Vignettes
© Associated Professional Sleep Societies, LLC 40
Sizing up the case
• What are presenting symptoms?– Are they specifically insomnia symptoms? Or….– Could they result from under-treated OSA?
• What is usage pattern and tolerance for OSA therapy?• What benefits does patient derive from OSA therapy?• Are there behavioral targets for CBT?• Does OSA therapy contribute to sleep disruption?• How should the treatment be sequenced?
– PAP then CBT– CBT then PAP– Simultaneous CBT + PAP

© Associated Professional Sleep Societies, LLC 41
Perpetuating Mechanisms + Treatment Approach
= Insomnia
and/or
and/or
Low sleep drive
Improper circadian timing
Excessive bedtime arousal
Napping
↑ TIB
Variable sleep schedules
Performance anxiety
Attentional bias
Active mind
Conditioned arousal
Unhelpful sleep beliefs
Cognitive therapies
Stimulus control
Sleep restriction
© Associated Professional Sleep Societies, LLC 42
The game of mix and match……..
CBT +

© Associated Professional Sleep Societies, LLC 43
Insomnia Symptom Improvements in PAP Users and Nonusers (N = 705 w OSA + Insomnia pre PAP)
Björnsdóttir et al. Sleep, 2013

© Associated Professional Sleep Societies, LLC 44
Insomnia Before and After PAP InitiationCaetano Mota et al. Rev Port Pneumol. 2012;18(1):15---21
24
56
80
13 12
25
0
30
60
90
Insomnia Pre‐PAP No Insomnia Pre‐PAP Total
# of Patients
Insomnia Before and After PAP
Group Pre‐ PAP # with Insomnia After PAP

© Associated Professional Sleep Societies, LLC 45
Special Consideration:OSA Patients who remain sleepy
• Modify SRT so that initial TIB = TST + 30 min.• Recommend short naps• Reassess OSA and treatment adequacy• Use counter-control instead of strict SC
– Less effective in beginning of night– Equally effective in middle of night

© Associated Professional Sleep Societies, LLC 46
Case 1:• 63-year-old single male BMI = 35 • Referred due to sleep onset/maintenance complaints• Medical Conditions:
– asthma, – hypertension, – aortic valve disease, – benign prostatic hypertrophy, – chronic migraine headaches, – gastroesophageal reflux disease, – chronic back pain.– Prior dx (10 yrs. ago) of OSA PAP trial but discontinued after 1
month• No Psychiatric history

© Associated Professional Sleep Societies, LLC 47
Case 1 continued:• Current findings
– His bedtime varied between 9:30 p.m. and 10:30 p.m.his rising time varied between 5:15 a.m. and 7:15 a.m.
– No pattern of napping– watches TV in bed 2 to 3 nights a week and reads in bed one
night per week– take Ambien CR, 12.5 m.g., and Melatonin, 10 m.g. to aid his
sleep and he reports that this medication is helpful.– Insomnia Severity Index = 11; Epworth = 2– Sleep study conducted the week before my consultation showed
a baseline AHI = 36; PAP @ 12 cm H2O reduced AHI to 1. • Assessment & Plan
– Mild insomnia but severe OSA– Allow patient to restart PAP therapy – Keep sleep diary for 2 weeks once using PAP on regular basis
and return to clinic to re-evaluate sleep symptoms

© Associated Professional Sleep Societies, LLC 48
Sleep Diary Post PAP Initiation

© Associated Professional Sleep Societies, LLC 49
Case 2• 37 yr. old married male• 2 year history of insomnia – mostly sleep onset difficulty• Insomnia began with suicide of co-worker/friend• Recently moved to Denver for work with charitable
organization – directs youth center • Work stressful – long hours & dysfunctional staff• Medical conditions = chronic bronchitis, GERD, and
cough all effectively treated. Patient does not view as contributory to sleep problems
• No history of mental/emotional problems• MSE – mildly anxious mood but otherwise normal• ISI = 20; Epworth Scale = 13• Diagnostic PSG showed AHI = 10 events/hour

© Associated Professional Sleep Societies, LLC 50
Case 2 ‐ continued• Reported sleep schedule: bedtime = 9:30 PM;
rise time = 5:00 AM• Works 10-12 hour days 6 days per week• Sundays works as pastor ½ of day• Usually watches TV in bed nightly• Has active mind in bed – thinks about work• Uses over the counter sleep aides intermittently
to manage sleep
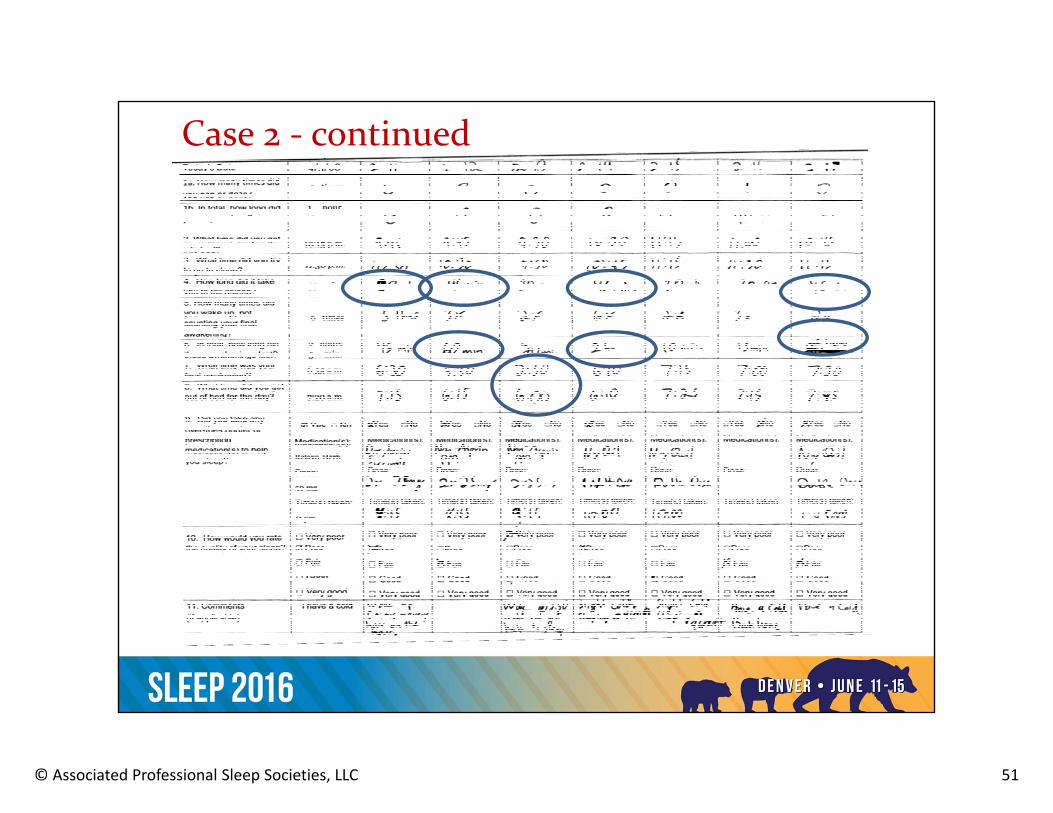
© Associated Professional Sleep Societies, LLC 51
Case 2 ‐ continued
© Associated Professional Sleep Societies, LLC 52
Treatment Plan:• Standard SC and SRT• Increase exercise for stress release• One hour buffer time prior to bed• Initiate CPAP concurrent to behavioral treatment
Case 2 ‐ continued

© Associated Professional Sleep Societies, LLC 53
Case 2 – after 6 weeks of CBT + PAP therapy
© Associated Professional Sleep Societies, LLC 54
Managing comorbid insomnia & OSA
• Emerging area of sleep medicine focus• CBT has proven effective alone and with OSA
therapies• Combined therapy presumed optimal but adherence to
therapies a challenge • Future studies should ascertain:
– Optimal therapies for sleep-wake and health outcomes– Strategies for making therapies acceptable/tolerable– Best treatment sequence
• Assure dissemination/translation of findings so patients have access to best treatment practices