“because that is the ultimate goal here: how does this ... _lara... · dr. linda verhoef ....
TRANSCRIPT

Supervisors:
Dr. Elena Syurina VU University Amsterdam, De Boelelaan 1105, 1081
HV Amsterdam
Dr. Linda Verhoef National Institute for Public Health and the
Environment, Antonie van Leeuwenhoeklaan 9, 3721 MA, Bilthoven
Anja Haenen
National Institute for Public Health and the Environment, Antonie van Leeuwenhoeklaan 9, 3721
MA, Bilthoven
Dr. Renske Eilers National Institute for Public Health and the
Environment, Antonie van Leeuwenhoeklaan 9, 3721 MA, Bilthoven
“Because that is the ultimate goal here: How does
this help the client?”
Evaluation of elderly care physicians’ acceptability of the Dutch surveillance network for infectious diseases in nursing homes: a transdisciplinary approach
Global health Research Master thesis- April 2018
Written by:
Lara Hartog 2525056 [email protected] VU University Amsterdam, De Boelelaan 1105, 1081 HV Amsterdam

1
Contents List of tables and figures ............................................................................................................................... 4
Figures ........................................................................................................................................................... 4
Tables ............................................................................................................................................................ 4
List of abbreviations ...................................................................................................................................... 5
Part I The article………………………………………………………………………………………………………………………………………6
1. Abstract ................................................................................................................................................... 6
2. Introduction ............................................................................................................................................ 7
3. Conceptual framework ............................................................................................................................ 8 4. Research questions………………………………………………………………………………………………………………………….11
5. Methods ................................................................................................................................................ 10
5.1 Setting ............................................................................................................................................... 10
5.2 Sample ............................................................................................................................................... 11
5.3 Interviews .......................................................................................................................................... 11
5.4 Focus group discussion ..................................................................................................................... 12
5.5 Ethical considerations ....................................................................................................................... 13
5.6 Data analysis ..................................................................................................................................... 13
5.7 Rigor .................................................................................................................................................. 14
6. Results ................................................................................................................................................... 14
6.1 Acceptability...................................................................................................................................... 14
6.1.1 External factors .......................................................................................................................... 14
6.1.2 NH factors .................................................................................................................................. 14
6.1.3 ECP factors ................................................................................................................................. 15
6.1.4 Organization of SNIV .................................................................................................................. 16
6.1.5 Participation benefits ................................................................................................................. 22
6.1.6 Data collection ........................................................................................................................... 22
6.1.7 Acceptability of participation and each key activity .................................................................. 23
6.2 Suggestion for improvements ........................................................................................................... 24
6.3 Most suitable candidate ................................................................................................................... 27

2
7. Discussion ……………………………………………………………………………………………………………………………………….27 7.1 Summary key findings ...................................................................................................................... 27
7.2 Discussion key findings ..................................................................................................................... 27
7.3 Discussion applicability Auer et al. (26)’s template .......................................................................... 29
7.4 Strengths and limitations .................................................................................................................. 29
8. Conclusion ............................................................................................................................................. 30
Part II Updated extended research proposal .............................................................................................. 31
1. Introduction .......................................................................................................................................... 31
2. Conceptual framework .......................................................................................................................... 33
3. Research questions ............................................................................................................................... 36
4. Methods ................................................................................................................................................ 37
4.1 Overall design.................................................................................................................................... 37
4.2 SNIV ................................................................................................................................................... 37
4.3 Setting ............................................................................................................................................... 39
4.4 Sample ............................................................................................................................................... 39
4.5 Interviews .......................................................................................................................................... 40
4.6 Focus group discussion ..................................................................................................................... 41
4.7 Ethical considerations ....................................................................................................................... 42
4.8 Data analysis ..................................................................................................................................... 42
4.9 Trustworthiness ................................................................................................................................ 43
5. Time table .............................................................................................................................................. 43
References .................................................................................................................................................. 45
Appendix 1 - Annual questionnaire (in Dutch) ........................................................................................... 49
Appendix 2 - SNIV registration form (in Dutch) .......................................................................................... 53
Appendix 3 - Definitions SNIV (in Dutch) .................................................................................................... 54
Appendix 4 – Interface OSIRIS (in Dutch) .................................................................................................... 56
Appendix 5 – Anonymized feedback report (in Dutch) .............................................................................. 57
Appendix 6 - Example invitation mail (in Dutch) ........................................................................................ 69
Appendix 7- Information leaflet (in Dutch) ................................................................................................. 70
Appendix 8 - Interview guide (in Dutch) ..................................................................................................... 72
Appendix 9 - Consent form (in Dutch) ........................................................................................................ 77
Appendix 10 – Focus group discussion guide (in Dutch) ............................................................................ 78

3
Appendix 11 - Codebook interviews ( in Dutch) ......................................................................................... 85
Appendix 12 - Codebook Focus group discussion (in Dutch) ...................................................................... 97

4
List of tables and figures
Figures Figure 1. Auer et al. (26)’s Framework for the application and adaptation of the World Health
Organization’s injury surveillance guidelines…………………………………………………………………………………………9
Figure 1. Auer et al. (26)’s Framework for the application and adaptation of the World Health
Organization’s injury surveillance guidelines…………………………………………………………………………………………35
Tables Table 1. Overview of the accepted invitations and send invitations………………………………………….………….11
Table 2. Overview of participants’ profiles…………………………………………………………………………………………...12
Table 3. Overview of the initial structure of the focus group discussion……………………………………………….13
Table 4. Description of the major categories, sub categories, barriers and facilitators affecting ECPs’
acceptability and the related key activity and attribute…………………………………………………………………………17
Table 5. Overview and description of the suggestions for improvements provided by participants….….25
Table 6. Overview of the accepted invitations and send invitations………………………………………………………39
Table 7. Overview of participants’ profiles…………………………………………………………………………………………….40
Table 8. Overview of the initial structure of the focus group discussion………………………………………………..42

5
List of abbreviations AB= Antibiotics ECP= Elderly care physician EPF= Electronic patient file FGD= Focus group discussion Former-SNIV= NH that used to participate FR= Feedback report HAI= Healthcare-associated infections I= Interview ICT= Information and communications technology NH= Nursing home Non-SNIV= NHs that never participated in SNIV OSIRIS= Online System for infectious diseases registration within ISIS RIVM= Dutch National Institute for Public Health and the Environment SNIV= Surveillance network infectious diseases nursing homes SS= Surveillance system TD= Transdisciplinary UTI= Urine tract infections

6
Part I. The Article
1. Abstract Introduction: Successful infection prevention strategies are reliant on adequate surveillance systems (SSs). The Dutch surveillance network for infectious diseases in nursing homes (NHs) (SNIV) is a national SS that aims to provide insight in infection incidence rates to inform prevention policies on a national and local level. To ensure optimal SS functioning, regular evaluation of its acceptability among end-users is required. Research objectives: To identify facilitators and barriers for elderly care physicians’ (ECPs) acceptability of SNIV and to examine suggestions to improve them. Finally, to identify the most suitable candidate for the execution of SNIV according to ECPs. Methods: A transdisciplinary design, including ten semi-structured interviews and one focus group discussion, with three ECPs was employed. Transcripts were analyzed using open coding. Results: Six categories of facilitators and barriers for acceptability emerged: external factors, NH factors, ECPs factors, organization of SNIV, participation benefits, and data collection. Important factors within these categories were: perceiving SNIV as beneficial and relevant, simplicity and reliability of data collection. Suggestions for improvements included improving communication about SNIV, simplifying data collection and adapting the feedback reports to ECPs’ needs. The most suitable candidate for the overall execution was NH dependent, for infection diagnosis it was the ECP. Discussion and conclusion: Future improvements of SNIV should focus on enhancing communication about its utility and purpose, simplifying data collection with information computer technology adaptations and improving the feedback reports. Other national SSs may prosper with considering these aspects and applying the evaluation methods employed in this study.

7
2. Introduction Globally, healthcare-associated infections (HAI) represent the number one adverse outcome in healthcare settings, constituting a fundamental public health problem (1). Elderly people residing in nursing homes (NHs) are particularly vulnerable to contracting (healthcare-associated) infections, due their shared living environment, age-related changes in immune system functioning, comorbidities and cognitive impairment, which hampers the maintenance of proper hygiene standards (2-5). Additionally, infections among the elderly lead to more functional decline and higher morbidity and mortality rates compared to infections among the younger population (2, 3). The world’s aging population and recent changes in NH demographics towards an older population with more comorbidities and increased susceptibility to contracting infections, have significantly raised concerns with regards to the number of infections in NHs (6-8). One concern is the projected growth of the number of infection outbreaks in NHs and thereby the risk of spread to the general population (9, 10). This is particularly alarming when outbreaks of antibiotic (AB) resistant microorganisms, such as methicillin resistant staphylococcus aureus occur (11). Effective infection control strategies in NHs are therefore crucial (11). Successful infection prevention strategies are reliant on reliable surveillance data (12). Several studies have shown that infection surveillance is crucial for early identification and prevention of infection outbreaks in NHs (13). Infection incidence rates have also been shown to reduce after the implementation of adequate surveillance systems (SSs) (12, 14, 15). Moreover, surveillance data provides information about NH performance, specific risk factors and high-risk populations (12). This information is used for the development, implementation and evaluation of infection prevention strategies on a local level in NHs (16, 17). On a national level, SSs allow for benchmarking against comparable NHs and the national average, which is helpful for evaluating the current state of the art (12, 15). National SSs also facilitate comparisons across countries and provide information to national policy makers for the development of infection control guidelines (18). In the Netherlands, the Ministry of Health, Welfare and Sport already recognized the importance of a national SS in 2009 and commissioned the development of the surveillance network for infectious diseases in nursing homes (SNIV) (19). SNIV was developed by the Infectious Disease Control Center of the Dutch National Institute for Public Health and the Environment (RIVM). SNIV’s two aims are to provide insight in the number of infections in NHs and to inform infection prevention strategies, both on a local and national level. SNIV’s incidence module consists of a weekly registration of cases of gastroenteritis, influenza-like illness, probable pneumonia, urine tract infection (UTI) and deaths. The number of infections is registered at participating NHs by elderly care physicians (ECPs), who represent SNIV’s end-users. NHs are recruited through academic networks, national congresses, symposia and emails, only NHs with more than fifty residents are eligible for participation (19). Currently, 32 NHs participate in the incidence module. However, participant numbers have been slightly decreasing over the years (20). In order to apply SNIV’s data for infection prevention purposes, optimal functioning of SNIV is required. Successful operation of SSs is ensured by regular evaluations (21). Evaluation of data quality for example, is important to assure reliable data and have been examined for SNIV before (22). Evaluation of end-users’ willingness to work with the SS is important to ensure optimal utilization.

8
Hitherto, no studies have assessed end-users’ perspectives on SNIV, despite the importance of this insight for optimal operation of SNIV. Therefore, this study aimed to evaluate SNIV from the end-users’ perspective and inform future development and improvement of SNIV.
3. Conceptual framework SS evaluation guidelines and frameworks have been described extensively in literature (21, 23-25). However, most frameworks overemphasizes data quality and discard the influence of human interactions with the SS. Auer et al.(26)’s injury SS evaluation framework, on the other hand, provides a holistic view on (injury) SS evaluation and balances the emphasis on end-user’s evaluations and data quality measurements. Therefore, this framework was particularly useful for the purpose of this study, despite the fact that it was originally developed for the field of injury surveillance. The framework was used to guide this study’s research questions, interview guide and interpretation of the results. First, a brief explanation of the framework is provided, after which its applicability in public health disciplines, other than injuries, is argued. The framework was developed in 2011 to facilitate the application and adaptation of the World Health Organization injury surveillance guidelines (25, 26). It describes SSs in four key activities: data collection, analysis, interpretation and dissemination (Figure 1). Data collection implies the gathering and entering of data (25). Data analysis, refers to checking, transforming and modeling data. Data interpretation is the course of assessing, highlighting and explaining information. The final key activity, data dissemination includes active and passive dissemination. The latter implies defusing and sharing the results after data analysis and interpretation (25). Active dissemination involves an interactive exchange of information and stimulation of applying that information to current practices (26). For SNIV, data collection is organized by one designated person from participating NHs, who coordinates implementation of SNIV’s six steps of data collection. First, NH characteristics, such as size, resident demographics and infection prevention policies are gathered in an annual questionnaire (Appendix 1). Second, ECPs diagnose infections among their clients. Third, ECPs have to remember to register the infection, which is organized differently in each NH. For example, some register by emailing the infection to their secretary assistant, who collect all infections in one overview and others use a registration form (Appendix 2). Fourth, the ECPs check whether the diagnoses are in line with SNIV’s definition of the infection. SNIV’s definitions were selected by an expert team and are in accordance with Dutch clinical case definitions of the medical practice in NH settings (Appendix 3). Fifth, the total sum of infections per age group is collected from all registered infections of that week. The manner in which this is done is also NH dependent. Finally, the total number of infections is entered into an online system for infectious diseases within ISIS (OSIRIS). Screenshots of the interfaces are provided in Appendix 4. All NHs have a personalized login code and have the possibility of retrieving their registered data from OSIRIS at any time (19). The second key activity data analysis is performed by the SNIV project team at the RIVM, who also assume responsibility for overall data management and monitoring. Data is processed in an annual feedback report (FR), which is send to the designated person in the NHs (Appendix 5). Third, data interpretation is the responsibility of the NHs (25). For the final key activity, passive dissemination is done by the SNIV project team by sharing the FRs with the NHs (25). Active dissemination in SNIV is the

9
responsibility of NHs. Auer et al. (26) juxtaposed the four key activities against the SSs attributes, which are inherent qualities or characteristics of SSs that are required to be adequate (Figure 1). The nine attributes are: simplicity, flexibility, reliability, security and confidentiality, utility, timeliness, sustainability and acceptability (25). Each attribute is considered in relation to each of the four key activities. For example, simplicity refers to the ease of data collection methods as well as to simple data interpretation (26). Flexibility is the ability to adapt the system to meet stakeholders’ needs (26). Reliability concerns the accuracy and quality of the SS and the data it produces, which should be complete, reliable and replicable (26). Security and confidentiality refer to safeguarding the records (26). Utility concerns the value placed on a SS by its stakeholders in relation to its practicality and affordability (26). Timeliness is defined as the systems’ ability to generate up-to-date information (26). Sustainability involves the system’s long-term maintenance to pertain serving is goal (26). Lastly, acceptability is the willingness of stakeholders to work with the system and the extent to which results are achieved (26).
Figure 1. Auer et al. (26)’s Framework for the application and adaptation of the World Health Organization’s injury surveillance guidelines.

10
Auer et al.(26)’s framework conceptualized acceptability as the underlying factor, interlinked to all other attributes. For example, if ECPs perceive SNIV as simple, they are more likely to be willing to work with the system. Therefore, Auer et al. (BRON) suggests a system environment evaluation, which involves assessing stakeholders’ acceptability of the overall system. Lastly, the framework was built on the underlying notion that the intrinsic aim of any SS, in any health related field, is to produce knowledge and to disseminate that knowledge into action (26). For each SS this aim can be achieved by successful synergy between data collection, analysis, interpretation and dissemination. Auer et al.’s (26) framework provides a conceptualization for the evaluation of these four activities, regardless of the discipline in which they are used. Thus, under the condition that the SS under evaluation aims to produce knowledge and disseminate that knowledge into action, the framework can be applied in any discipline. Therefore the framework can be applied for the evaluation of SNIV, as SNIV aims to provide insight in the number of infections in NHs and to inform infection prevention strategies.
4. Research questions On Auer et al.(26)’s notion that acceptability is the underpinning attribute of all attributes, this study examined what the barriers and facilitators were regarding end-users’ acceptability of participation in the SNIV network and its data collection, interpretation and dissemination methods. Initially end-users’ opinions regarding data analysis was included. However, for SNIV data analysis is performed by the RIVM. Thus, end-users’ experiences with data analysis is limited. This study also identified what end-user’s suggestions for improvements of SNIV were and who they believed to be the most suitable candidate for the execution of SNIV.
5. Methods This explorative study was conducted in collaboration with the SNIV project team from the RIVM. A transdisciplinary (TD) design was applied, as this aligned with the system environment evaluation of Auer et al.(26). Additionally, TD studies have been shown to be valuable for evaluation research (23, 27-29). First, semi-structured interviews were conducted to identify barriers and facilitators. Then, this information was used to identify suggestions for improvements during a focus group discussion (FGD). In line with TD designs, the research questions, study design and interview guides were developed combining SNIV’s end-users’ and research team’s knowledge (28-30).
5.1 Setting The study took place in nine NHs, spread throughout the Netherlands from November 2017 until February 2018.

11
5.2 Sample A divers sample with a wide range of perspective was included by applying a maximum variation strategy (31). Participants were selected purposively based on their presumed attitudes towards SNIV (e.g. NHs that had decided to not participate after they attended presentations about SNIV). Three groups representing all SNIV’s (potential) end-users were selected: NHs that currently participate (SNIV NHs), that used to participate (former-SNIV) and that never participated in SNIV (non-SNIV). ECPs were chosen, because they are the most common designated person for SNIV and assume responsibility for diagnosing infections. However, in two cases the designated person for SNIV was not the ECP, therefore these persons were also invited. All participants were invited by email (Appendix 6) and received a reminder after two weeks. An information leaflet about the FGD attached to the FGD invitations (Appendix 7). ECPs from SNIV and former-SNIV NHs were selected from the SNIV database available at the RIVM. Non-SNIV NHs were selected from a list comprising all NHs in the Netherlands. In total, 56 invitations were send, three SNIV, one former-SNIV and six non-SNIV NHs agreed to participate in the interviews and three SNIV NHs in the FGD. The most common reasons for not participating were lack of time or interest. Table 1 shows the distribution of the invited NHs and Table 2 shows participants’ profiles.
5.3 Interviews Semi-structured interviews were chosen as this allows researchers to study specific topics in-depth and allows participants to discuss important topics for them (32). All interviews were conducted by yhe same female master student (LH), who received training in interviewing techniques and who was not acquainted to any of the participants. Most interviews were held in-person, one telephonic interview was conducted. The interviews were conducted in Dutch, lasted between 25-50 minutes and took place at a time, location and date at participants’ convenience. Participation was on a voluntary basis and no valuable incentives for participation were provided. An interview guide was developed based on the conceptual framework and in accordance with Castillo-Montoya’s guidelines (33) (Appendix 8). First, the research procedure and participants’ rights were explained. Then, the consent form was signed (Appendix 9) and the following topics were discussed: reasons for and against participation in SNIV, SNIV registration, FRs, interpretation and sharing of the FRs, person executing the registration and suggestions for improvement. Interview guides were slightly adapted for SNIV, former-SNIV and non-SNIV participants, but the outline remained similar. Some minor modifications were made to the guide after the first interviews.
Table 1. Overview of the accepted invitations and send invitations. Invited (n) Participated (n) Interviews (total) Former-SNIV NHs SNIV NHs Non-SNIV NHs
46 14 14 18
10 1 3 6
Focus group discussion (total) SNIV NHs
10 10
3 3
NH= Nursing home, SNIV= Surveillance network infectious diseases nursing homes (former= NH that used to participate in SNIV; non= NHs that never participated in SNIV)
12
For example, question number 10 (how did you hear about SNIV and what did you think this manner) was added after this topic came up during the first interview (Appendix 8). Additionally after the first five interviews the registration form, infection definitions and anonymized FRs (Appendix 2, 3 and 5, respectively) were brought to the interviews to facilitate the discussion.
5.4 Focus group discussion FGDs generate rich data, which is particularly useful for creating ideas for improvement (32). The FGD was homogeneous and was also facilitated by LH. Initially, the presence of an observer was planned. However, due to transportation constraints the observer could not be present. The FGD was held in Dutch and lasted two hours. An external location in Utrecht was chosen for its central location and accessibility. A FGD guide was developed in accordance with the TD principle of engaging multiple stakeholders. The guide was based on the findings from the interviews and a discussion of these findings with the SNIV project team. Two topics: the FRs and data collection methods of SNIV (Appendix 10), were selected based on their relevance to both the end-users’ and the SNIV project team. Additionally, improvements for these two topics seemed most achievable. The aim of the FGD was two-folded. First, to assess the extent of data saturation regarding the facilitators and barriers for the FRs and data collection methods. Second, to identify strategies and solutions for these barriers and facilitators. An overview the FGD structure is provided in Table 3.
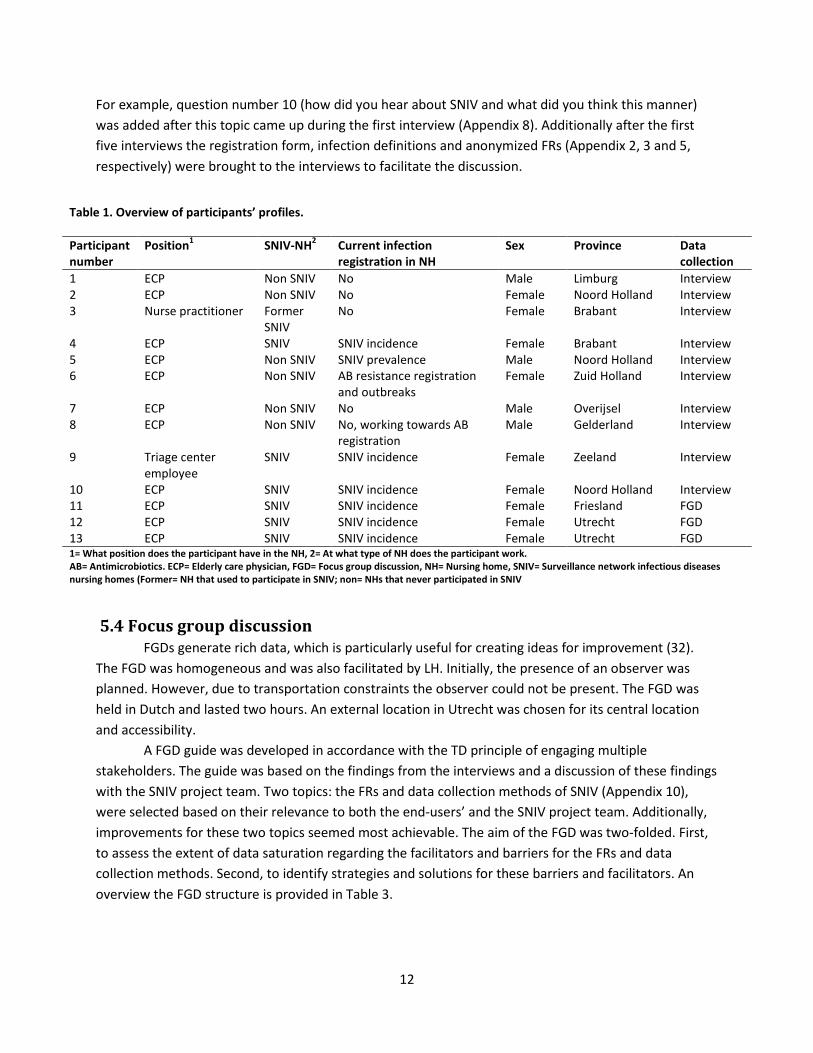
Table 1. Overview of participants’ profiles.
Participant number
Position1 SNIV-NH2 Current infection registration in NH
Sex Province Data collection
1 ECP Non SNIV No Male Limburg Interview 2 ECP Non SNIV No Female Noord Holland Interview 3 Nurse practitioner Former
SNIV No Female Brabant Interview
4 ECP SNIV SNIV incidence Female Brabant Interview 5 ECP Non SNIV SNIV prevalence Male Noord Holland Interview 6 ECP Non SNIV AB resistance registration
and outbreaks Female Zuid Holland Interview
7 ECP Non SNIV No Male Overijsel Interview 8 ECP Non SNIV No, working towards AB
registration Male Gelderland Interview
9 Triage center employee
SNIV SNIV incidence Female Zeeland Interview
10 ECP SNIV SNIV incidence Female Noord Holland Interview 11 ECP SNIV SNIV incidence Female Friesland FGD 12 ECP SNIV SNIV incidence Female Utrecht FGD 13 ECP SNIV SNIV incidence Female Utrecht FGD 1= What position does the participant have in the NH, 2= At what type of NH does the participant work. AB= Antimicrobiotics. ECP= Elderly care physician, FGD= Focus group discussion, NH= Nursing home, SNIV= Surveillance network infectious diseases nursing homes (Former= NH that used to participate in SNIV; non= NHs that never participated in SNIV

13
5.5 Ethical considerations Approval from an ethics committee was not required as the study did not fall under Dutch medical research involving human subjects act (34). Nonetheless, the principles of responsible research were applied (35). Written informed consent was obtained from all participants after a thorough explanation of the research and participants’ rights (Appendix 9). To guarantee participants’ right to privacy, only researchers of the SNIV incidence module had access to the documents. The recordings and transcripts were kept confidential and will be destroyed after five years. To ensure anonymity, no unique identifiers were linked to data and participants were registered using codes. Depending on participants’ preferences, a copy or a summary of the transcripts and the findings of the study were sent for validation.
5.6 Data analysis The interviews and FGD were recorded with a mobile phone and were transcribed verbatim. Transcripts were analyzed by qualitative content analysis in Atlas.ti (35). First, all transcripts were read repeatedly to obtain a clear understanding of the data. Then, open coding was applied to analyze data without imposing preconceived categories (36). The first two interviews were coded by two researchers separately, who then discussed the codes and developed a codebook. Two researchers independently applied the codebook to analyze the first six interviews to assess inter-rater reliability. Discrepancy in codes were discussed until consensus was reached and only minor changes were necessary. The final codebook (Appendix 11) was used to analyze the remaining transcripts. For the FGD, a new codebook was developed in a comparable manner (Appendix 12). For both codebooks, no consult with a third researcher was required. Emerging categories, sub categories and corresponding barriers and
Table 2. Overview of the initial structure of the focus group discussion. Description Introduction Short introduction of the research, the FGD, confidentially matters and signing the consent forms Introduction round: Each participant introduces themselves and their NH
Topic 1 Feedback reports Identify facilitators and barriers
Participants write down three positive and three negative aspects on post-its, which are then discussed with the whole group
Identify solutions Participants write down solutions for each positive and negative aspect, which are then discussed with the whole group and additional solutions may be identified
Select top solutions A top five is selected to discuss in more detail In-depth discussion The top five is discussed in more detail. Break
Theme 2 Data collection methods of SNIV Identify facilitators and barriers
Participants write down three positive and three negative aspects on post-its, which are then discussed with the whole group
Identify solutions Participants write down solutions for each positive and negative aspect, which are then discussed with the whole group and additional solutions may be identified
Select top solutions A top five is selected to discuss in more detail In-depth discussion The top five is discussed in more detail. Closure Summarize and conclude the FGD FGD= Focus group discussion, NH= Nursing home, SNIV= Surveillance network for infectious diseases in nursing homes

14
facilitators were identified by both researchers independently, and then discussed and described in the results.
5.7 Rigor O’brien et al. (37)’s and Tong et al. (38)’s recommendations for enhancing trustworthiness of qualitative research were applied. Potential sources of bias are addressed in the discussion section. Dependability was established by cross-checking codes during data analysis and by applying triangulation of qualitative data sources, enhancing the quality and credibility of data analysis (35). Confirmability was ensured by reflexive data collection and analysis processes (35).
6. Results Data analysis delineated the results into three parts. The factors influencing end-users’ acceptability are described first, followed by the suggestions for improvements and the most suitable candidate for the execution of SNIV.
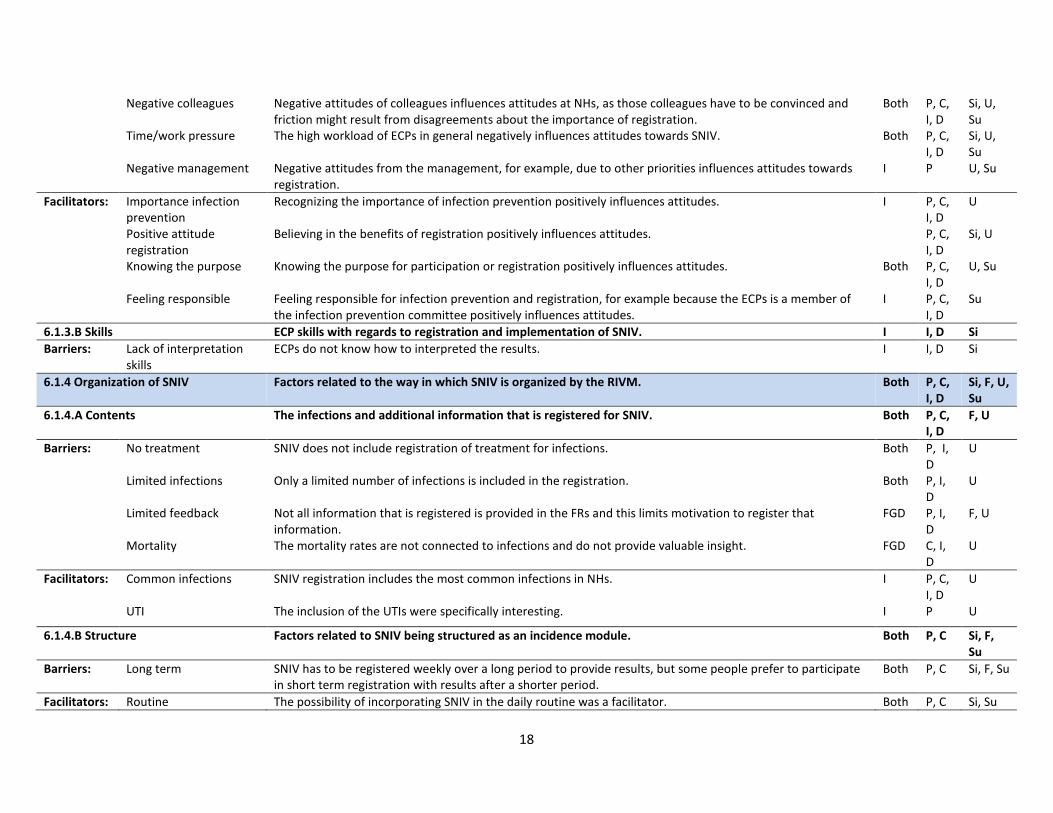
6.1 Acceptability The barriers and facilitators influencing ECPs’ acceptability of participation, data collection, interpretation and dissemination were interlinked and often overlapped. Therefore, data is first described according to six categories of factors that influence acceptability of all aspects. Then, acceptability of each aspect is considered separately. The six major categories were: external factors, NH factors, ECP factors, organization of SNIV, participation benefits and data collection. Within these six major categories, several sub categories with barriers and facilitators emerged, an overview of this and the SNIV activity that was influenced by the factors is provided in Table 4. To facilitate interpretation of the barriers and facilitators, Table 4 also provides an overview of the attribute from Auer et al. (26)‘s framework, to which the factors applied.
6.1.1 External factors The government and one profession related organization were mentioned as external bodies which influenced acceptability of participation and data collection (Table 4). Participants held varying views with regards to the influence of the government. Some indicated that prioritization of infection prevention by the government stimulated participation, whereas others said that it did not make a difference. In accordance with this, some participants advocated a more prominent role for the government with regards to infection registration legislation. However, others indicated that participation should be driven by intrinsic motivation and that mandated registrations demotivate ECPs and hamper data collection and quality. One non-SNIV participant suggested that the decision to not participate in SNIV, might have been influenced by the lack of advice from a profession related organization, though this participant also indicated that the influence was only minor.
6.1.2 NH factors NH factors influenced ECPs’ acceptability of participation and all three activities. Two facilitators related to NHs were identified. First, having prior experience in research aided the implementation and organization of SNIV and lowered the bar for participation in SNIV (Table 4). Second, determining a clear

15
purpose for the registration facilitated participation and all activities. However, the lack of a predetermined goal for participation or the FRs was also considered as demotivating and hindered data collection and quality of the data collected. For example, during the interviews one participant stated: “ You need to start with determining why you need data, what you want to do with it and what conclusions you want to draw from it, before you start with collecting data, and not the other way around.” Other barriers are described in Table 4, some examples are: high staff turn-over, having a self-designed registration system and only participating in SNIV with a few NHs of the entire institution. The latter complicated data collection, because registration was more often forgotten if it was not implemented throughout the institution. The interpretation and discussion of the FRs at institutional wide meetings was also hindered, as SNIV results were not relevant for the entire institution. For non-SNIV participants, this was sometimes provided as a reason for not participating. Finally, NH structure was also mentioned as a barrier. One participant indicated that due to the home-like setting of the institution, routine registrations were complicated.
6.1.3 ECP factors 6.1.3.A Attitudes ECPs’ attitudes both facilitated and challenged acceptability of participation and all activities. A relatively equal balance of positive and negative attitudes towards SNIV was found amongst participants. The importance of infection registration, specifically in light of AB resistance, local infection prevention or national infection data was acknowledged by all participants, including those with more negative attitudes. Differences in attitudes were related to differences in the perceived usefulness of registration or the FRs. This related to a previously described NH barrier, the lack of a predetermined goal. ECPs who were a member of the NH infection prevention committee also indicated that they felt responsible for infection prevention, which positively influenced their attitudes. Negative attitudes were influenced by negative attitudes of co-workers or management. Participants often complained about having to convince co-workers to participate in SNIV or register for SNIV. After weighing the costs and benefits of participation, some respondents concluded that the workload and time investment of participation were too high in comparison to the profits. Interestingly, non-SNIV participants often based their conclusions on assumptions, rather than facts. This is illustrated by the following quote of participant 4: “But I think it is an investment and I just, yeah the effort, I still don’t see the return of it.”. “Of course, I do not have any experience with the registration. I simply have a suspicion that it is a time investment, that will be hanging over our heads every week like a dark cloud.”. This demonstrates the central role of attitudes in the decision-making process for participation in SNIV. In addition to that, attitudes also played a significant role for acceptability of data collection, interpretation and dissemination. SNIV participants for example, explained how the quality of data collection was impeded by the lack of motivation from colleagues and how this influenced the interpretation and dissemination of the results. 6.1.3.B Skills One participant indicated that not knowing what the results meant or how they could be interpreted, restrained her from using and sharing the FRs.

16
6.1.4 Organization of SNIV The way in which SNIV is organized both facilitated and hindered ECPs’ acceptability of participation and the other three activities. There were four sub categories: the contents, the structure, the project team and the resources. 6.1.4.A Contents The types of infections included in SNIV were a topic for debate (Table 4). Some participants were positive about the included infections and one specifically considered participation due to the inclusion of UTIs. However, all respondents criticized the lack of registration of treatment, especially with regards to ABs and described how this restrained them from participating or from using the results. Another point raised during the FG was the absence of a link between mortality and infections in the registration and the FRs. This hampered their willingness to register mortality, as data would not be used in the FRs. 6.1.4.B. Structure The weekly registration for SNIV was both facilitator and barrier for participation and data collection. Some participants favored the possibility of integrating SNIV in the NH routine, whereas others preferred to participate in short term registrations, such as a prevalence study. 6.1.4.C SNIV project team The SNIV project team was related to facilitators and barriers for the participation and all other activities. One major barrier was the lack of clarity about SNIV. Participants indicated that they did not have a clear understanding of what SNIV was, how it worked, what its goals and purposes were and why they should participate. For example, one FGD participant said: “Because we then received a very nice flyer of SNIV or the RIVM to participate, but it did not clarify what we would get out of it. Or how it would help us, therefore we decided not to participate. Despite our believe that infection prevention was important.” Additionally, one respondent mentioned that the presentations provided by SNIV were a major reason for not participating, due to the lack of quality and professionality. Whereas others decided to participate after the presentation or indicated that the support of the RIVM with FR interpretation was helpful. 6.1.4.D Resources Participants often suggested that assistance from the RIVM would be helpful for convincing colleagues to participate, data entry, and interpretation and dissemination of the FRs. Views with regards to financial compensation were discordant. Participants in favor of financial support indicated that it could convince colleagues and management to participate. However, they also agreed with participants that were against financial incentives, that participation should be due to intrinsic motivation rather financial incentives.

17
Table 3. Description of the major categories, sub categories, barriers and facilitators affecting ECPs’ acceptability and the related key activity and attribute.
Category and sub Category
Factors Description Method1
Activity2
Attribute3
6.1.1 External Factors Factors external to SNIV, ECPs and the NHs. I P, C U, Su Barriers No advice from
profession related organizations
Lack of advice to participate in SNIV from profession related organizations. I P U, Su
Not compulsory by government
Lack of legislation for infection registration by the government. I P Su
Facilitators: Government awareness Attention to infection prevention by the government stimulates participation. I P, C U, Su 6.1.2 NH factors Factors related to the NHs. P, C,
I, D Si, F, R, U, Su
Barriers: Size SNIV requires a minimum of 30 clients, NHs with less clients are excluded from participation. I P, C Su NH structure The way the NH is organized limits participation. For example, no strict administration guidelines, no
administrative assistance, home-like settings, small scale, new NHs and organizations. Both P, C,
I, D Si, F, R, Su
Lack of capacity The organization lacks capacity for participation. For example, not enough staff. Both P, C Su Staff turn-over The high turn-over rate in staff limits participation and data collection, because new ECPs are not used to
registration of do not see the purpose for registration. I P, C,
D Su
Primary care The NH needs to focus on providing high standard care to their residents, before extra activities like SNIV can take place.
I P, C, I, D
U, Su
Own registration The institution has their own infection registration. I P U Complete institution Only a part of the institution participates, this limits the relevance of the FRs for the entire institution and
limits data collection because ECPs from other NHs are not used to register for SNIV. I P, C,
I, D U, Su
No purpose The NH does not have a goal or purpose for participation. Both P, C, I, D
U
Facilitators: Other research The institution has participated in earlier research and this facilitates participation and implementation. I P, C Si, U Determine purpose The institution has determined a purpose for participation. Both P, C,
I, D U
6.1.3 ECP factors Factors related to or caused by the ECPs. P, C, I, D
Si, U, Su
6.1.3.A Attitude
Held attitudes or beliefs towards registration or SNIV.
Both P, C, I, D
Si, U, Su
Barriers: Negative attitudes registration
Not believing in the benefits of registration negatively influences attitudes. Both P, C, I, D
Si, U, Su
Not knowing the purpose
Not knowing the purpose for participation or registration negatively influences attitudes. Both P, C, I, D
U, Su
18
Negative colleagues Negative attitudes of colleagues influences attitudes at NHs, as those colleagues have to be convinced and friction might result from disagreements about the importance of registration.
Both P, C, I, D
Si, U, Su
Time/work pressure The high workload of ECPs in general negatively influences attitudes towards SNIV. Both P, C, I, D
Si, U, Su
Negative management Negative attitudes from the management, for example, due to other priorities influences attitudes towards registration.
I P U, Su
Facilitators: Importance infection prevention
Recognizing the importance of infection prevention positively influences attitudes. I P, C, I, D
U
Positive attitude registration
Believing in the benefits of registration positively influences attitudes. P, C, I, D
Si, U
Knowing the purpose Knowing the purpose for participation or registration positively influences attitudes. Both P, C, I, D
U, Su
Feeling responsible Feeling responsible for infection prevention and registration, for example because the ECPs is a member of the infection prevention committee positively influences attitudes.
I P, C, I, D
Su
6.1.3.B Skills ECP skills with regards to registration and implementation of SNIV. I I, D Si Barriers: Lack of interpretation
skills ECPs do not know how to interpreted the results. I I, D Si
6.1.4 Organization of SNIV Factors related to the way in which SNIV is organized by the RIVM. Both P, C, I, D
Si, F, U, Su
6.1.4.A Contents The infections and additional information that is registered for SNIV. Both P, C, I, D
F, U
Barriers: No treatment SNIV does not include registration of treatment for infections. Both P, I, D
U
Limited infections Only a limited number of infections is included in the registration. Both P, I, D
U
Limited feedback Not all information that is registered is provided in the FRs and this limits motivation to register that information.
FGD P, I, D
F, U
Mortality The mortality rates are not connected to infections and do not provide valuable insight. FGD C, I, D
U
Facilitators: Common infections SNIV registration includes the most common infections in NHs. I P, C, I, D
U
UTI The inclusion of the UTIs were specifically interesting. I P U
6.1.4.B Structure Factors related to SNIV being structured as an incidence module. Both P, C Si, F, Su
Barriers: Long term SNIV has to be registered weekly over a long period to provide results, but some people prefer to participate in short term registration with results after a shorter period.
Both P, C Si, F, Su
Facilitators: Routine The possibility of incorporating SNIV in the daily routine was a facilitator. Both P, C Si, Su

19
6.1.4.C Project team The way in which the RIVM or the SNIV project team regulates and organizes SNIV. Both P, C, I, D
Ut
Barriers: Poor communication Communication or communication methods from the RIVM to the NHs are not sufficient. For example the presentations and emails do not provide clear instructions and the aim and benefits of SNIV are unclear. NHs are not involved in the network.
Both P, C, I, D
U, Su
Unclarity about purpose It is not clear what the purpose and goals of SNIV are. Both P, C, I, D
U, Su
Facilitators: Support Receiving support from the RIVM, for example with the interpretation or other questions is a facilitator. I P, C, I, D
U, Su
Clear presentation The presentation provided by the RIVM was clear and convinced the staff at the NH to participate in SNIV. I P U, Su 6.1.4.D Resources The resources that are available at the RIVM for SNIV participants. Both P, C Si, U,
Su Barriers: Lack of administrative
support There is no administrative assistant at the RIVM who enters the data into OSIRIS. I P, C Si, U,
Su Lack of financial
compensation Not receiving any financial compensation for participation is perceived as a barrier. Both P, C U, Su
6.1.5 Participation benefits Factors related to the potential benefit of participation or outcomes of SNIV. Both P, C, I, D
Si, F, R, U, T
6.1.5.A Feedback reports The feedback of NH results in the annual FR. Both P,I,D Si, F, U, T
Barriers: Unreliable The FRs or data in the reports are perceived as unreliable, because of the questionable reliability of data collection methods.
I P, I, D
R, U
Unclarity about usefulness
It is unclear where the reports could be used for. Both P, I, D
U
Old data The FRs include data of the previous year. Both P, I, D
U, T
Interpretation is Difficult
It is difficult to interpreted what the data means. Both P, I, D
Si, R, U
Not adaptable The FR are not adapted to NHs’ individual needs and requirements, for example because they are only provided once a year.
Both P, I, D
F, U, T
Does not include treatments
The reports do not include information about the treatment of infections. Both P, I, D
U
No advice The reports do not include an advice about what to do with the data. Both P, I, D
U
Facilitators: Insightful The reports provide insightful information about the current state of the art. Both P, I, D
U
Systematic and The information in the reports is systematic and generalizable. FGD P, I, U

20
generalizable D Visual The reports are visual (e.g. with graphs) which helps interpretation. FGD I, D Si, U Useful The reports can be used for a range of things: case examples, trends, benchmarking (with wards, national
average, comparable NHs, regional NHs), monitoring policies and interventions, daily practice, outbreak identification, documents for inspection, infection prevention.
Both P, I, D
U
6.1.5.B Other benefits Other benefits related to participation in SNIV. I P, C F, U Facilitator: Publication The possibility of contributing to scientific publications by participation in SNIV is seen as a facilitator. I P U Data access The ability to review one’s registered data in OSIRIS afterwards is seen as a facilitator. I P, C F, U Increasing awareness Participation in SNIV increases infection prevention awareness and this facilitates participation. I P U 6.1.6 Data collection Factors related to the way in which the number of infections and additional information is collected for
SNIV. Both P, C,
I, D Si, R, U, T, Su
6.1.6. Step 1. Annual questionnaire The questionnaire about the NH that is filled out annually is perceived as a barrier. I C Si Barriers: Lot of work and time Filling out the questionnaire takes a lot of time and requires a lot of work, because different information has
to be looked up and different people to be contacted. I C Si
Dependent on others You are dependent on multiple different people to provide information and fill out the questions. I C Si 6.1.6. Step 2. Diagnoses Diagnosing the infections is considered a barrier for SNIV. Both P, C,
I, D Si, R
Barriers: Challenging context It is difficult to diagnose an infection in a NH, for example because of the lack of qualified staff and residents who suffer from dementia who cannot communicate about their symptoms.
I P, C, I, D
Si, R
Based on prescription of AB
Infections are sometimes diagnosed by the administration of AB or not. Both P, C, I, D
Si, R
Comorbidities Elderly people often have multiple diseases which may also explain complaints, this complicates infections diagnosis.
I P, C, I, D
Si, R
Lack of golden standard There is no golden standard for diagnosing the infections included in SNIV. I P, C, I, D
Si, R
Varies per ECP Diagnosing an infection is subjective and varies across ECPs. I P, C, I D
R
6.1.6.Step 3. Remembering register for SNIV
After diagnosing you have to remember to register for SNIV and remember your colleagues to do so. Both P, C, D
Si, R, U, Su
Barriers: Dependent on others You are dependent on you colleagues to register and some do not register even after receiving reminders. Both P, C, Si, R, Su
Forget Forgetting to register. For example, because ECPs did not have access to a computer or a registration form at the time of diagnosis.
Both P, C Si, R, Su
No routine NHs that do not have a routine, or at which multiple ECPs work, forget to register more easily. Both P, C Si, Su Demotivating It is demotivating to keep reminding colleagues to register. Both P, C Si, Su Lot of time and work It is an investment to have to keep asking everyone to register. Both P, C Si, U,
Su

21
1= Through which data collection method was the factor identified: I= Semi-structured interview, FGD= Focus group discussion, Both= In both the semi-structured interviews and focus group discussion. 2= On which activity of the surveillance system does it have an impact. P= Participation in the network, C= Data collection, I= Data interpretation, D= Data dissemination. 3= To which attribute does it connect. Si= Simplicity, F= Flexibility, R= Reliability, U=Utility, T= Timeliness, Su= Sustainability. AB= Antibiotics, ECP= Elderly care physician, EPF= Electronic patient file, FGD= Focus group discussion, FR= Feedback report, I= Interview, NH= Nursing home, OSIRIS= Online System for infectious diseases registration within ISIS, RIVM= Dutch National Institute for Public Health and the Environment, SNIV= Surveillance network infectious diseases nursing homes, SS= Surveillance system, UTI= Urine tract infections
Facilitators: Routine Remembering to register is easier once a routine has been build. Both P, C Si, Su Reminders Receiving a reminder for the registration (e.g. by email, in the EPF, in the agenda or by the designated person
for SNIV). Both P, C Si, Su
Checking systems Checking EPF systems or the pharmacy for additional clients with infections. Both P, C Si, Su Designated person There is one person responsible for collecting all data and that person guarantees that everyone registers. Both P, C Si, Su 6.1.6.step 4. Checking definitions If you remembered to register, you have to check whether the diagnosis is according to SNIV’s definition. Both P, C,
I, D SI, R, Su
Barriers: Quality The definitions are not the right definitions for the infection. Both P, C, I, D
Si, R, Su
Not practical The definitions are not based on the practical use of it. For example, because some infections are diagnosed by the administration of AB.
Both P, C, I, D
Si, Su
Look up definition You have to remember the definition and otherwise look it up. I P, C Si, Su ECPs dependent Interpretation of the definition is ECP dependent. Both P, C,
I, D R
6.1.6.step 5. Collect all registrations All infections for SNIV need to be collected somewhere and summed to the total number of infections per age category for that NH.
Both P, C Si, R, T, Su
Barriers: Afterwards You have to look up the number of infections in the system afterwards and this is a barrier. Both P, C Si, T Double registration You have register in the EPF as well as for SNIV. I P, C Si Lot of time and work It is a lot of time and work to match all infections and calculate the ages. Both P, C Si No control There is no one who checks if all infections have been registered and if all registered infections are correct. FGD P, C R Facilitators: Simplicity The forms are easy to work with. Both C Si Little time It does not take a lot of time to fill out the forms and combine them. I P, C Si Routine Having a routine for the data collection facilitates the process. Both P, C Si, Su 6.1.6.step 6. Data entry OSIRIS Once you have the total number of infections it has to be registered in OSIRIS. Both P, C Si Barriers: Lot of time Registering and logging in a different systems is an extra time investment. Both P, C Si Lack of assistance Not having an administrative assistant is perceived as a barrier. Both P, C Si Complexity Working in a new system, having to log in and share codes with others is a challenge. I P, C Si Facilitators: Little time The registration in OSIRIS takes a little time Both P, C Si Assistance Having an administrative assistant facilitates participation in SNIV. Both P, C Si Simplicity OSIRIS is simple to work with. Both P, C Si

22
6.1.5 Participation benefits The potential benefits of participation were a controversial topic, specifically with regards to the FRs. This influenced acceptability of participation, data collection, interpretation and dissemination. 6.1.5.A Feedback reports Positive aspects of the FRs were the fact they were insightful, generalizable, systematic and visual. Additionally, participants mentioned a range of practices for which they could be used, such as benchmarking and improving and evaluating policies and interventions (more examples provided in Table 4). These factors facilitated participation and the interpretation and dissemination of the FRs. Other participants indicated that the FRs were not useful or that they did not know to use them. For example, because the FRs were not adaptable to NH needs or because their reliability was questionable (Table 4). Some participants also mentioned that the reports concerned data of the previous year and that it lacked explanations and advices, restricting the interpretation and usefulness of the FRs and their willingness to participate in SNIV. 6.1.5.B Other benefits Apart from the FRs, three other facilitators for participation and data collection were mentioned (Table 4): the possibility of contributing to a scientific publication, the ability to access one’s data in OSRIS and the fact that participation in SNIV increased infection prevention awareness at NHs. However, non-SNIV participants indicated that the potential benefits did not weigh up to the costs of participation.
6.1.6 Data collection The barriers and facilitators related to data collection influenced acceptability of participation in SNIV and all activities. The factors are described according to SNIV’s six data collection steps that were explained previously in the conceptual framework section. 6.1.6. Step 1. Annual questionnaire One participant considered the annual questionnaire as a major hurdle. Gathering the required information from different parties, such as management, clients and external parties, was considered a timely and daunting job and limited acceptability of this aspect of SNIV’s data collection. 6.1.6. Step 2. Diagnosis Only barriers with regards to diagnosing infections were identified. The trustworthiness of the diagnoses was often questioned by participants. This was caused by: the difficulties with determining an infection among the elderly, the challenging context of a NH, the lack of a golden standard and ECPs’ variations in diagnoses. All these factors distorted the reliability of the data collected, which hindered the interpretation and dissemination of the results and was a reason for non-SNIV ECPs to decline participation. This is summed up by the following quote of participant 5: “It is indeed a hindering factor [referring to diagnosis] for registration. First of all, you do not know what to register. Second of all, it is a problem for the interpretation of the statements, if not everyone registers correctly. Because what is it, that you receive back” 6.1.6.Step 3. Remember registration Remembering to register for SNIV was facilitated by integrating SNIV’s registration in the NH routine and getting used to registering. Further, having one designated person for SNIV also advanced data collection, as this person motivated and remembered colleagues to register and coordinated the data collection process (Table 4). However, remembering registration was also perceived as a major

23
barrier. One reason was that the current structure of SNIV does not allow ECPs to register infections simultaneously with the diagnosis (Table 4). Participants also described how their motivation was affected by colleagues who did not register, even after receiving multiple reminders. For example one participant said: “But it also makes you a little, well what I described earlier, like beating a dead horse, that I constantly have to ask others if they have something for SNIV.” Participants were mostly concerned with the impact of forgetting to register on data quality, as it lead to incomplete data, limiting the interpretation and dissemination of the results. The former-SNIV respondent also indicated that this was a major reason for their withdrawal from SNIV. 6.1.6.Step 4. Check definition Participants only described barriers with regards to SNIV’s infection definitions (Table 4). UTIs were most commonly used as an example, but the other definitions also encompassed shortcomings. Comparable to the diagnosis barrier, ECP’s interpretation of the definition was mentioned as a barrier. One participant indicated that the definitions were not practical and not in consonance with the NH practice. The definition barriers were problematic for accurate registration and affected data interpretation and dissemination and contributed to non-SNIV participants’ decisions to not participate. Finally, to check whether diagnoses where in line with SNIV’s definitions required extra work and time. More barriers are described in Table 4. 6.1.6.Step 5 Collect registration The weekly assembling of the total number of registrations was evaluated differently with regards to acceptability of SNIV’s data collection. Some respondents indicated that the registration form (Appendix 2) were clear and easy to fill out, especially once the NH had built a routine and structured registration. However, others felt it was time consuming and a lot of work, especially tracking down the past infections at the end of the week and gathering all forms. They indicated that it played a role in their decision to not participate. Table 4 describes other barriers. 6.1.6.Step 6. Entry in OSIRIS There was no uniform opinion among respondents about OSIRIS and most factors were identified as both facilitators and barriers for acceptability of participation and data collection. SNIV participants pointed out that OSIRIS was easy to use, and that the interface was clear. Whereas, non-SNIV participants declared that having to log in and work in a new system, with a new login code, was a tedious job and an important barrier for participation. A similar pattern was observed for the time investment of data entry. Additionally, the lack of administrative assistance at the NH or at the RIVM was brought up as barrier. Reversely, the presence of an assistant facilitated data entry and participation in SNIV.
6.1.7 Acceptability of participation and each key activity Acceptability of participation in SNIV was influenced by all six major categories. Some factors only applied to participation, with regards to the barriers these were: the lack of advice from profession related organizations, no legislation by the government, NHs having their own registration, negative attitudes of management and not meeting SNIV’s requirements with regards to size. Facilitators that only applied to acceptability of participation were: the registration of UTIs, the presentation provided by the SNIV project team, possibility of contributing to a scientific publication and increasing infection prevention awareness. All other factors also applied to at least one other activity.

24
ECPs’ acceptability of SNIV’s data collection was influenced by all major categories, except participation benefits. Most factors affecting data collection also affected participation. Only the annual questionnaire and the simplicity of the registration form were considered for data collection specifically. All facilitators and barriers affecting data interpretation also influenced data dissemination. Additionally, most factors also influenced data collection or participation. The lack of ECPs’ interpretation skills was the only barrier mentioned solely for interpretation and dissemination.
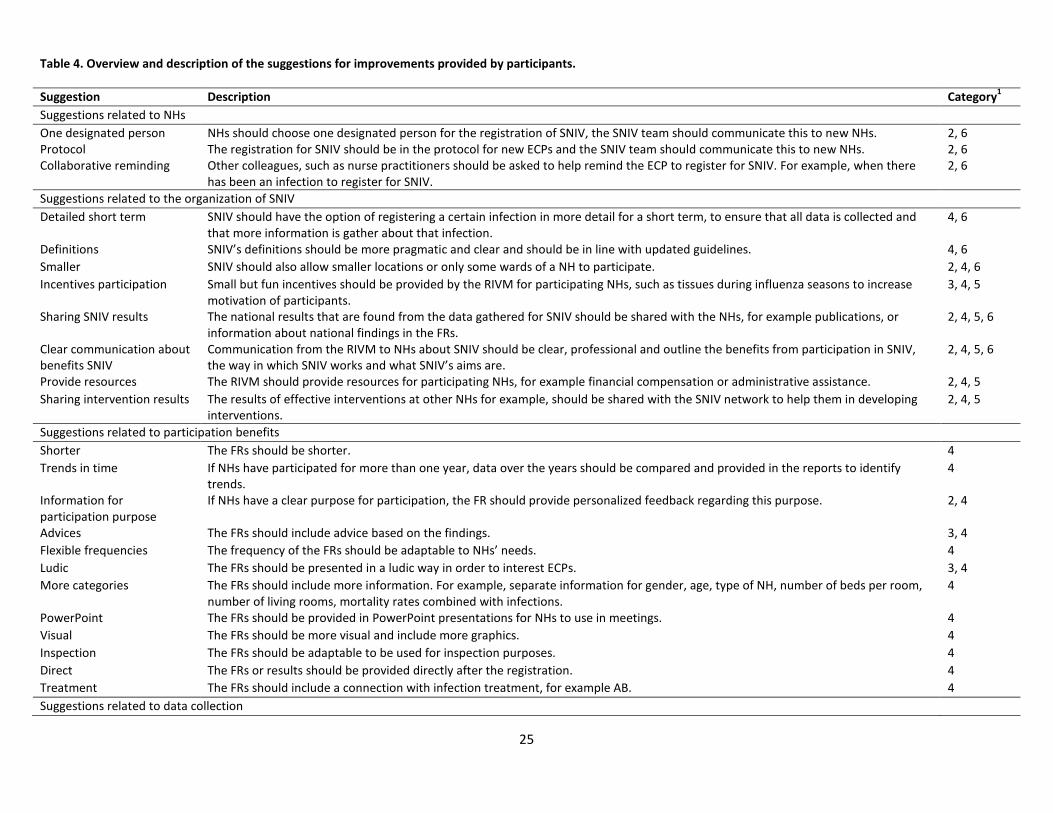
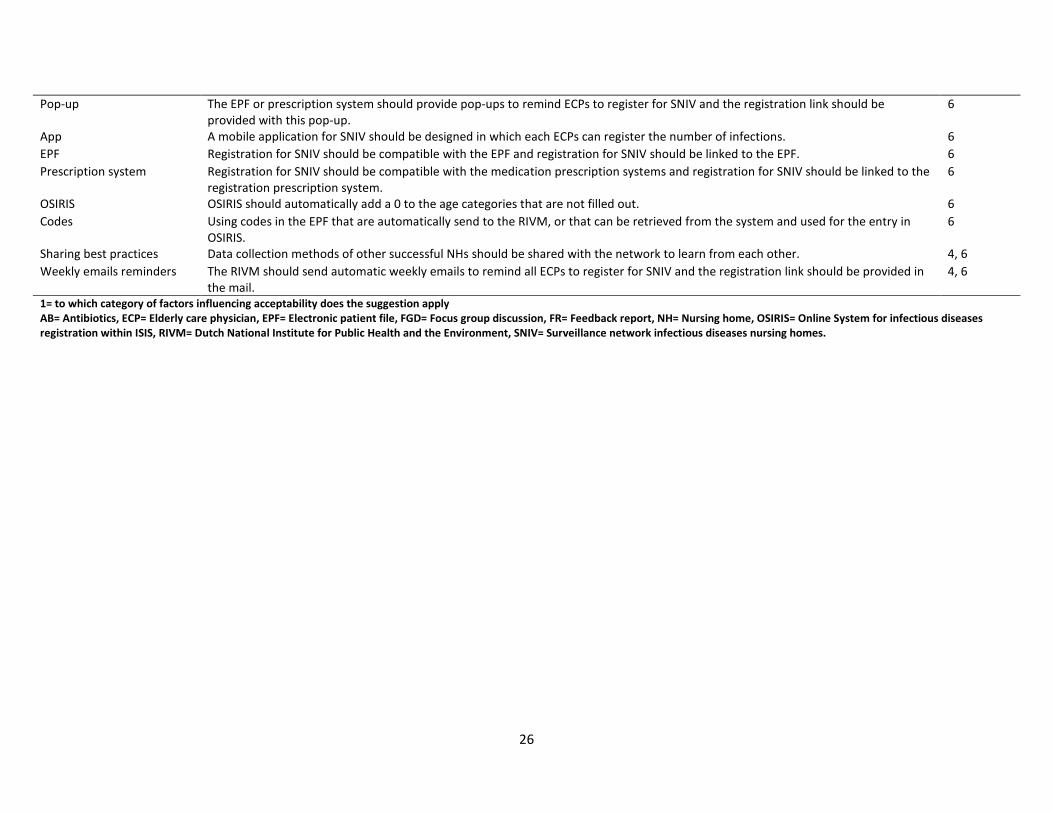
6.2 Suggestion for improvements Suggestions were provided for all major categories of factors influencing acceptability, except for external factors. The suggestions ae therefore categorized according to the same structure. Due to the interrelations between the categories, suggestions that applied to ECP factors also applied to the organization of SNIV and participation benefits. Therefore, only suggestions related to NHs, organization of SNIV, participation benefits and data collection were described. An overview is provided in Table 5. 6.2.1 NH suggestions Three suggestions for NHs were identified: describing the responsibility of SNIV in the protocol for new ECPs; assigning one designated person for SNIV; and inviting lower qualified co-workers to help remembering registration for SNIV. Table 5 provides an explanation for each suggestion. 6.2.2 Organization of SNIV suggestions Most improvements for the organization of SNIV related to improved communication and involvement of NHs. Specifically, more information was required about SNIV’s goals, purposes, data collection methods, outcomes, decisions and potential benefits for participants. Suggested manners for achieving this was by regular emails or presentations from the SNIV team or incorporate more information about SNIV in the FRs. These ideas were also suggested for improving ECPs’ attitudes and knowledge about participation benefits. Other suggestions are described in Table 5. 6.2.3 Participation benefits suggestions Improving participation benefits mostly related to improving the FRs and the communication about FRs’ utility. Suggestions included making the FRs shorter, more visual and graphical and providing results in a PowerPoint Presentation. Additionally, including advices, offer support with the interpretation of the FRs and provide personalized feedback for the NHs in the FRs, were commonly suggested by participants. A more detailed explanation can be found in Table 5. 6.2.4 Data collection suggestions Most suggestions for data collection were information and communications technology (ICT) related (Table 5). Adapting SNIV to be compatible with the electronic patient file (EPF) or treatment prescription systems were often suggested. This saves time and energy and addresses the issue of double registration, forgetting to register and having to log in to a different system. Other suggestions were to use codes for registering SNIV in the EPF. These codes could also be used to provide pop-ups if words such as infection are used in the EPF, to remind ECPs to register. In line with the pop-up, a weekly registration reminder mail from the RIVM was also proposed. Another software suggestion was to create a mobile application in which physicians can register directly after diagnoses. Additionally, participants suggested to share best practices of registration methods from different NHs, in order to learn from other NHs.
25
Table 4. Overview and description of the suggestions for improvements provided by participants. Suggestion Description Category1
Suggestions related to NHs One designated person NHs should choose one designated person for the registration of SNIV, the SNIV team should communicate this to new NHs. 2, 6 Protocol The registration for SNIV should be in the protocol for new ECPs and the SNIV team should communicate this to new NHs. 2, 6 Collaborative reminding Other colleagues, such as nurse practitioners should be asked to help remind the ECP to register for SNIV. For example, when there
has been an infection to register for SNIV. 2, 6
Suggestions related to the organization of SNIV Detailed short term SNIV should have the option of registering a certain infection in more detail for a short term, to ensure that all data is collected and
that more information is gather about that infection. 4, 6
Definitions SNIV’s definitions should be more pragmatic and clear and should be in line with updated guidelines. 4, 6 Smaller SNIV should also allow smaller locations or only some wards of a NH to participate. 2, 4, 6 Incentives participation Small but fun incentives should be provided by the RIVM for participating NHs, such as tissues during influenza seasons to increase
motivation of participants. 3, 4, 5
Sharing SNIV results The national results that are found from the data gathered for SNIV should be shared with the NHs, for example publications, or information about national findings in the FRs.
2, 4, 5, 6
Clear communication about benefits SNIV
Communication from the RIVM to NHs about SNIV should be clear, professional and outline the benefits from participation in SNIV, the way in which SNIV works and what SNIV’s aims are.
2, 4, 5, 6
Provide resources The RIVM should provide resources for participating NHs, for example financial compensation or administrative assistance. 2, 4, 5 Sharing intervention results The results of effective interventions at other NHs for example, should be shared with the SNIV network to help them in developing
interventions. 2, 4, 5
Suggestions related to participation benefits Shorter The FRs should be shorter. 4 Trends in time If NHs have participated for more than one year, data over the years should be compared and provided in the reports to identify
trends. 4
Information for participation purpose
If NHs have a clear purpose for participation, the FR should provide personalized feedback regarding this purpose. 2, 4
Advices The FRs should include advice based on the findings. 3, 4 Flexible frequencies The frequency of the FRs should be adaptable to NHs’ needs. 4 Ludic The FRs should be presented in a ludic way in order to interest ECPs. 3, 4 More categories The FRs should include more information. For example, separate information for gender, age, type of NH, number of beds per room,
number of living rooms, mortality rates combined with infections. 4
PowerPoint The FRs should be provided in PowerPoint presentations for NHs to use in meetings. 4 Visual The FRs should be more visual and include more graphics. 4 Inspection The FRs should be adaptable to be used for inspection purposes. 4 Direct The FRs or results should be provided directly after the registration. 4 Treatment The FRs should include a connection with infection treatment, for example AB. 4 Suggestions related to data collection
26
Pop-up The EPF or prescription system should provide pop-ups to remind ECPs to register for SNIV and the registration link should be provided with this pop-up.
6
App A mobile application for SNIV should be designed in which each ECPs can register the number of infections. 6 EPF Registration for SNIV should be compatible with the EPF and registration for SNIV should be linked to the EPF. 6 Prescription system Registration for SNIV should be compatible with the medication prescription systems and registration for SNIV should be linked to the
registration prescription system. 6
OSIRIS OSIRIS should automatically add a 0 to the age categories that are not filled out. 6 Codes Using codes in the EPF that are automatically send to the RIVM, or that can be retrieved from the system and used for the entry in
OSIRIS. 6
Sharing best practices Data collection methods of other successful NHs should be shared with the network to learn from each other. 4, 6 Weekly emails reminders The RIVM should send automatic weekly emails to remind all ECPs to register for SNIV and the registration link should be provided in
the mail. 4, 6
1= to which category of factors influencing acceptability does the suggestion apply AB= Antibiotics, ECP= Elderly care physician, EPF= Electronic patient file, FGD= Focus group discussion, FR= Feedback report, NH= Nursing home, OSIRIS= Online System for infectious diseases registration within ISIS, RIVM= Dutch National Institute for Public Health and the Environment, SNIV= Surveillance network infectious diseases nursing homes.

27
6.3 Most suitable candidate Participants gave varying answers with regards to the most suitable candidate for the execution of SNIV and indicated that this depended on the type of institution and its structure. For diagnosing the infections, all participants indicated that the ECP should assume responsibility. However, other data collection steps could also be executed by lower-qualified functions. For example, the medical secretaries or nurse practitioners could execute data entry in OSIRIS.
7. Discussion 7.1 Summary key findings Based on Auer et al. (26)’s injury SS evaluation template ECPs’ acceptability of participation in SNIV and its data collection, interpretation and dissemination was assessed. Six categories of facilitators and barriers influencing acceptability were identified: external factors, NH factors, ECP factors, organization of SNIV, participation benefits and data collection methods. Important factors within these categories were: perceiving SNIV as beneficial and relevant, simplicity of data collection and reliability of SNIV. The three main suggestions for improvements were related to enhancing communication about SNIV’s purpose and benefits, adapting the FRs and incorporate ICT adaptations in the data collection methods.
7.2 Discussion key findings The majority of facilitators and barriers applied to acceptability of participation and at least one of the key activities, highlighting the interrelatedness of these aspects and suggesting the need of a holistic approach to evaluate SNIV. Auer et al.(26)’s framework provides a clear template for such an approach. Applying this template to the six major categories identified in this study, showed that utility, simplicity, sustainability, reliability, flexibility and timeliness were relevant to SNIV’s end-users. Security and confidentiality were not relevant for SNIV. To provide insight in the extent to which SNIV achieves its aims and to provide starting points for improvements, the relation of each attribute to SNIV is discussed. Utility concerns the value placed on a SS and was a controversial topic for SNIV. Contradicting ECPs’ attitudes and knowledge about the benefits, resulted in different opinions regarding SNIV’s utility. Studies have demonstrated the importance of knowing a SS’ purpose and benefits in order for the SS to be perceived as valuable (23, 39-41). The differences in end-users’ utility perceptions may have several explanations. First, participants were selected based on presumed varying views and due to differences in institutional or personal priorities and experiences, different opinion were distinguished (42, 43). Second, communication about SNIV’s purpose, methods and benefits may have been hampered, resulting in differences in end-users’ knowledge (40). This is also supported by the finding that non-SNIV participants based their opinions about SNIV on assumptions and that improved communication was often suggested. More clarity about SNIV and its purpose and benefits is therefore recommended. For example by regular emails, more information in FRs or improved presentations. These communication strategies have been effective in improving involvement of participants in earlier studies and are relatively easy to implement (44, 45). Next, SNIV’s simplicity or lack thereof, mostly related to data collection. Reasons for the lack of

28
simplicity, such as registration time, dependency on others and lack clarity about the definitions, have also been identified in other SS evaluations (46-48). SNIV’s (perceived) simplicity is important for maintaining NHs in the network, recruiting new NHs, ensuring reliable data, and translating the findings from that that data into action and infection prevention strategies (23, 44, 49). Therefore, improvements of SNIV’s data collection methods are recommended. Various ICT adaptations were suggested, for example a mobile application, pop-ups or codes in the current EPF. Multiple studies have identified potential benefits of ICT improvements such as: simplified data collection processes, decreased registration burden and time investment and improved data quality (50-53). However, implementing ICT adaptations also holds potential challenges, such as high costs, lack of acceptability of ICT advancements and different EPF systems (50-52). Therefore, in order to overcome these barriers, such interventions require a careful development and implementation process, preferable with a TD component involving multiple stakeholders (54, 55). Additionally, non-SNIV ECPs more often perceived SNIV as complicated than SNIV participants, which may be the result of communication barriers that were explained before. Thus, improving communication might also address SNIV’s perceived simplicity. SNIV’s simplicity is also related to its sustainability, as complex systems are difficult to pertain (44). This is supported by the finding that SNIV’s data collection was facilitated by taking up SNIV in the daily routine. Besides simplicity, SNIV’s sustainability is also influenced by its perceived utility and NH structure. The influence of simplicity, utility and organizational factors (such as NH structure) on SSs’ sustainability has been identified before (41, 44, 49) and can be explained using Rogers diffusion model (56). This model conceptualizes how complex innovations negatively influence its long-term maintenance (56). Sustainability is important for accomplishing SNIV’s two aims by ensuring systematic and continuous data to inform national policies on infection prevention and minimize public health threats. SNIV’s sustainability may be improved by paying attention to simplifying its data collection process and optimizing communication. Reliability often concerned the reliability of SNIV’s data collection, the effect this had on the interpretation and dissemination of the FRs, and how this restrained ECPs from participating. The current data collection methods for SNIV are susceptible to mistakes and the lack of simplicity and utility for SNIV influence accuracy of data collection (40, 44). The importance of reliable data for effective SSs have often been described and have led to its prominent role in any SS evaluation framework (23, 25, 57). Besides the relevance of reliability to SNIV’s end-users’, reliability is also an important factor for the RIVM, as this influences the comparability of nationally acquired data (39). SNIV’s reliability has been evaluated before, but due to the low incidence rates, no conclusions could be drawn from this study (22). To cater to respondents concerns, future studies should focus on SNIV’s data quality, for example by assessing its sensitivity or positive predictive value and share these findings with end-users (25, 26). The next two attributes, flexibility and timeliness, were mostly negatively perceived with regards to the interpretation and dissemination of the FRs and hindered participation in SNIV. Studies have shown the importance of reviewing real-time data for evaluating interventions, policies and current practices and early identification of outbreaks (58, 59). Currently, the FRs comprise of data of the previous year and are only developed once a year. This limits their utility for prevention purposes. Additionally, the current FRs do not include advice or feedback customized to NHs’ needs, despite the known benefits of personalized feedback (46, 57). Assessing NHs’ needs may be helpful for developing more effective FRs in order to improve its utility for infection prevention purposes (57). Additionally, the
29
finding that the most suitable candidate for the execution of SNIV is institutional dependent, relates to the attribute of flexibility. Demonstrating the need for SNIV to be adaptable to NH structures and provide NHs with the possibility of arranging SNIV in a manner that is effective for them. This should therefore be clearly communicated to the NHs. No factors related to data security and confidentiality were identified in this study. This might be explained by the type of data that is collected for SNIV; only the sum of infections per age category is registered and the possibility of tracing this information back to patient level is limited (19). The general high trust among Dutch residents in their government may also explain why security and confidentiality were not mentioned as a barrier by the participants (60, 61). Another explanation could be the reputation of the RIVM as high quality research institute with close consideration of privacy issues (62).
7.3 Discussion applicability Auer et al. (26)’s template This was the first study to implement the injury SS evaluation template in a field other than injuries. Therefore, the applicability in the current context is also discussed. Using the template to guide the interviews provided insight on all activities of SNIV and proved valuable for understanding the overall acceptability of SNIV. All categories and factors that were identified during open coding fitted in the template, suggesting the relevance of the template’s attributes in the current context. The framework was helpful for interpreting, structuring and discussing the interrelations of the broad range of factors that were identified. Overall, the template proved to be useful in the context of infection surveillance and supports the assumption that it can be applied to any SS that aims to produce knowledge and disseminate that knowledge into action.
7.4 Strengths and limitations 7.4.1 Strengths Although the findings are specifically for SNIV, other national SSs may also prosper with considering these aspects and applying Auer et al. (26)’s framework. Further, several issues with regards to scientific rigor were addressed in the methods section. Starting data analysis with open coding instead of directed coding using the conceptual framework guaranteed that no preconceived assumptions stirred the analysis. Additionally, triangulation of data collection methods revealed that data saturation was reached for some factors. However, for the influence of external factors, NH factors and to some extent the ECP factors and participation benefits, more research is needed to assess whether there are more factors influencing acceptability. 7.4.2 Limitations The lack of data saturation for some factors was also a limitation of the study, as the number of participants included was restricted by the limited time available for the study. The extent to which these findings are recognized by other end-users needs to be assessed, specifically for former-SNIV and SNIV NHs. Next, ECPs with negative attitudes may have declined invitations, leading to a response bias. However, due to the purposive sampling, ECPs with known negative attitudes were also invited. Therefore, this effect seems negligible. Due to time limitations, only a system evaluation with end-users was conducted, limiting the generalizability of the findings to other stakeholders, such as the Ministry. Finally, this study only assessed Auer et al.(26)’s applicability for interpretation of results and guiding the study. Comparing

30
open coding with direct coding, based on the framework may provide valuable insight about the applicability of the template for analysis, yet this was beyond the scope of the current study.
8. Conclusion This study provides unique insight in end-users’ views with regards to their willingness to participate in SNIV and work with its data collection, interpretation and dissemination methods. The lack of a simple registration system and lack of clarity about SNIV’s purpose and participation benefits were identified as barriers. Future improvements of SNIV need to focus on these three areas, in order to retain end-users’ in SNIV and ensure reliable national infection data. Applying Auer et al.(26)’s injury SS’ template for the evaluation, revealed that SNIV’s acceptability was mostly influenced by the attributes of utility, simplicity, sustainability, reliability, flexibility and timeliness. Although the findings revealed facilitators, barriers and suggestions for improvements, specifically for SNIV, other national SSs may also prosper with considering these aspects and applying the evaluation methods of Auer et al. (26)’s framework.
31
Part II Updated extended research proposal
1. Introduction Globally, healthcare-associated infections (HAI) represent the number one adverse outcome in healthcare settings, constituting a fundamental public health problem (1). This is specifically problematic for the elderly population residing in nursing homes (NHs), as infections among this population cause more adverse outcomes compared to the younger population(2, 3). For example, mortality rates of infections are higher among the elderly than among the younger population (3). Additionally, elderly people in NHs are more vulnerable to contracting infections , due their dependence on care, shared living environment, age-related changes in immune system functioning, comorbidity of chronic illnesses and cognitive impairment which hampers the maintenance of proper hygiene standards (2-5). Furthermore, infections in NHs are a particular global health concern because of the expected rise in numbers and the potential threat to the public health (8). This expected increase can be explained by two main reasons. First, the world’s population is ageing at a rapid rate, consequently the number of elderly people residing in NHs is also predicted to grow significantly (6, 7). Second, the demographics of NH residents is shifting towards a more susceptible population with regards to contracting infections (8). Currently, NH residents are older, have more comorbidities and severer functional disabilities than one or two decades ago (8). The expanding number of infections in NHs poses serious threats to public health. More infections in NHs raises the risk of infection outbreaks and thereby the spread to the general population (9, 10). This is particularly alarming when outbreaks of antibiotic (AB) resistant microorganisms, such as methicillin resistant staphylococcus aureus occur (11). Effective strategies to prevent infections and infection outbreaks in NHs are therefore crucial (11). Successful infection control strategies are reliant on reliable surveillance data, making infection monitoring an essential part of infection prevention (12). The monitoring of infections is crucial for early identification and prevention of infection outbreaks in NHs (13). Additionally, studies have shown that infection surveillance significantly reduces infection incidence and by that decreases the risk of spreading to the general population (12, 14, 15). Moreover, surveillance data provides information about the current state of the art, specific risk factors and high-risk populations (12). This information provides guidance for the development, implementation and evaluation of future prevention strategies (16, 17). Besides the importance of surveillance data for infection control on the NH level, infection monitoring also serves a national purpose. National surveillance data allows for benchmarking against comparable NHs and the national average (12, 15). The process of benchmarking requires comparable and reliable data across all NHs. Implementation of a standardized surveillance system (SS), such as a national SS, has been shown to increase data quality and establish a comparable and reliable database (15, 18). A national SS also ensures representative and routinely collected data (15, 18). Finally, national surveillance data provides information to policy makers for the development of infection control guidelines and allows for comparisons across countries (15, 18). In the Netherlands, such a national SS has already been in place since 2009; the surveillance network infectious disease nursing homes (SNIV) (19). SNIV is a national SS of Dutch NHs in which

32
infection incidence and prevalence data is systematically registered. The aim of SNIV is two-folded; on the one hand, SNIV aims to gain insight in the prevalence and incidence of infections in NHs to provide national data and inform policy makers on a national level(19). On the other hand, SNIV aims to provide insight in the current state of the art for NHs in order to improve infection prevention on a local level (63). Nevertheless, optimal functioning of SNIV is essential for its utility for infection prevention purposes (21). The optimal operation, utility and use of resources for SSs is ensured by regular evaluations (21). Evaluations of data quality for example, are important to ensure reliable data and have been the focus of earlier studies on SNIV (21, 22). Hitherto, no studies have evaluated SNIV’s utility, appropriateness or acceptability from the end-users’ perspectives, despite its importance for successful implementation and performance of SSs (21). For SNIV the end-users are elderly care physicians (ECPs) in NHs. Insight in their views may be helpful in evaluating and improving SNIV. Therefore, the purpose of this study was to evaluate SNIV from the end- users’ perspective and inform future development and improvement of SNIV. For the purpose of this study, infection surveillance, was defined based on de Center for Disease Control and prevention definition of public health surveillance as: “the ongoing, systematic collection, analysis, interpretation, and dissemination of data regarding infections for use in public health action to reduce morbidity and mortality and to improve health”(21) .

33
2. Conceptual framework The injury surveillance evaluation template by Auer et al.(26) was used to guide the design of this study and to structure the report. Specifically, it was used for the development of the research questions and the interview guide and the interpretation of the results. This framework was chosen as it provides a holistic view on (injury) SS evaluation and includes multiple levels and stakeholders in its evaluation. It provides a clear overview for the evaluation of (injury) SSs and informing future improvements. Therefore, Auer et al.(26)‘s framework was particularly useful for the purpose of this study, despite the fact it was originally developed for the field of injury surveillance. First, a brief explanation of the framework is provided, after which its applicability in other fields of public health is argued. The framework was developed in 2011 to serve as a template for the application and adaptation of the World Health Organization (WHO) injury surveillance guidelines (26). The WHO guidelines serve as a manual for the evaluation of SSs and include a description of nine attributes that contribute to SSs’ functioning (25). An attribute is defined as a quality or a characteristic that is inherent of a SS (25). A successful SS requires all attributes to be adequate. The nine SS’ attributes defined by the WHO are: simplicity, flexibility, reliability, security, confidentiality, utility, timeliness, sustainability and acceptability (25). These attributes are highly interrelated, yet distinct. Simplicity refers to the ease of producing data and working with the SS (25). It should be straightforward and not wasting stakeholders’ time. Flexibility is the ability to adapt the system or aspects of the system to meet stakeholders needs (25). Reliability refers to the accuracy of the SS and the quality of the data produced, it should be complete, accurate and replicable (25). Security and confidentiality concern safeguarding the records and information that is entered, as well as the person or institutional that is entering the record (25). Utility concerns the value of a SS to its stakeholders in relation to the SS’ practicality and affordability (26). Timeliness is defined as the system’s ability to generate information that is up-to-date and whenever it is needed (25). Sustainability involves the system’s long-term maintenance and whether it is regularly updated to pertain serving is goal (25). Lastly, acceptability is the willingness of stakeholders to use the system and the extent to which results are achieved (26). Acceptability is interlinked to all other attributes. For example, the affordability of a SS in relation the value it has, highly influences stakeholders’ willingness to work with the system(26). Auer et al. (26) juxtaposed these attributes with SSs’ four key activities, to facilitate a holistic evaluation of the SS (Figure 2).The four key activities of SSs comprise of: data collection, analysis, interpretation and dissemination (25). Collection is the process of gathering and entering data (26). Data analysis refers to checking, transforming, running and modeling of data (26). Data interpretation is the course of assessing, highlighting and explaining information (26). Finally, data dissemination involves sharing and distributing the information with others. Dissemination can be divided into active and passive dissemination. The latter implies defusing and sharing the findings and knowledge after data analysis and interpretation (26). Whereas active dissemination involves an interactive exchange of information and stimulation of applying the knowledge into current practices (26). In the framework, each attribute is considered in relation to each of the four key activities. For example, simplicity refers to the ease of data collection methods, as well as the interpretation of that data (26). The framework differs from other SS evaluation frameworks in that it conceptualizes the

34
attribute of acceptability as the underlying factor of all attributes (26). This implies that the level of acceptability among stakeholders is dependent on the evaluation of the other attributes. For example, a SS’ reliability or utility influences stakeholders’ acceptability. Besides the link between acceptability and the other attributes, acceptability is also dependent on a range of other factors, such as the SS’ goals and objectives, focus, cultural factors, involvement and policies and practices, as demonstrated in Figure 2. This illustrates the importance of aligning SS’ goals with stakeholders objectives in order to achieve acceptability. Finally, acceptability is conceptualized as underpinning the evaluation at all levels of the system’s stakeholders (e.g. management, staff, data-entry staff and national policy makers). Three types of methods for SS evaluation were described by the WHO and Auer et al. (26): retrospective, process and system environment. The first two rely on review of records and data collection processes, and mainly evaluate the attributes of reliability and simplicity. The latter, on the other hand, involves interviews with stakeholders and assesses how they experience the system overall. Due to the limited amount of time and resources available for this study, only a system environment evaluation was conducted with the end-users’ as the only stakeholder group. This method was chosen as it provides most insight in ECPs’ views, which was the purpose of the study. Lastly, the applicability of the template in other fields of public health is argued. The framework was built on the underlying notion that the intrinsic aim of any SSs, independent of its field, is to produce knowledge and to disseminate that knowledge into action. For each SS this aim can be achieved by effective synergy between the four key activities of data collection, analysis, interpretation and dissemination. Auer et al. (26)’s framework provides a conceptualization for the evaluation of these four activities, regardless of the discipline of the generated data. Thus, under the condition that the SS under evaluation aims to produce knowledge and disseminate that knowledge into action, Auer et al. (26)’s framework can be applied in any discipline.

35
Figure 2. Auer et al. (26)’s framework for the application and adaptation of the World Health Organization (WHO) injury surveillance guidelines.

36
3. Research questions Following Auer et al. (26)’s notion that acceptability is the underlying factor of each of the other eight attributes, the research questions addressed the acceptability of a SS key functions. Specifically, the research questions were:
1. Which factors facilitate or hinder participation in the SNIV network? 2. Which factors facilitate or hinder the acceptability of data collection for SNIV? 3. Which factors facilitate or hinder the acceptability of data analysis for SNIV? 4. Which factors facilitate or hinder the acceptability of data interpretation for SNIV? 5. Which factors facilitate or hinder the acceptability of data dissemination for SNIV? 6. Who is the most suitable candidate for the execution of SNIV? 7. How can the facilitating factors be magnified and the hindering factors be addressed?
All research questions were addressed from the end-users’ perspective. The first research question regarding participation in SNIV was added, as examining why NHs do or do not join a national network may be helpful in improving SNIV. Finally, the sixth and seventh research questions were added as the SNIV team was particularly interested in these two aspects.

37
4. Methods
4.1 Overall design The study was conducted in collaboration with the SNIV project team of the Centre for Infectious Disease Control (Cib) of the Dutch National Institute for Public Health and the Environment (RIVM). A transdisciplinary (TD), design was applied for this qualitative explorative study, as this aligned with the system environment evaluation of Auer et al.(26). The iterative process of collecting, sharing and reassessing data, while engaging multiple stakeholders from different disciplines that is typical for TD research, lends itself perfect to evaluation and improvement research (23, 27-29). It provides opportunities to integrate stakeholders’ knowledge, which would otherwise remain unnoticed (23, 27-29). Additionally the emergent design and the capacity building nature of TD research increases the acceptability of the SS under evaluation (27). The study was conducted with NHs’ ECPs. First, ten semi-structured interviews were conducted in which the factors facilitating or hindering the end-users’ acceptability of SNIV were identified. Then, these findings were discussed in one focus group discussion (FGD) and potential solutions were sought.
4.2 SNIV The SS that was evaluated in this study is SNIV. SNIV was developed by the CIb of the RIVM in 2009 and includes various modules for infection registration in NHs (19). The development was commissioned by the Dutch Ministry of Health, Welfare and Sport to gain insight in the prevalence and incidence of infections in NHs on a national level in order to inform national infection control guidelines (19). On a local level, SNIV aims to provide insight in the current state of the art for NHs in order to improve infection prevention in NHs (19). SNIV includes a prevalence, incidence and in-depth AB resistant module. Participation in all modules is on a voluntary basis and data is entered anonymously (20). For the prevalence module, NHs enter a broad spectrum of data from all residents once or twice a year. This provides insight in various risk factors and risk groups within each NHs (19). The incidence module includes weekly registration of cases of gastroenteritis, influenza-like illness, probable pneumonia, urine tract infection(UTI) and deaths and is used to provide insight in trends and outbreaks to inform infection prevention strategies on both the local and national level (19). Additionally, on the local level the incidence module is used to monitor NHs policies and help prioritizing areas for improvement (19). The in-depth AB resistant module examines patterns of AB susceptibility of micro-organisms carried by residents. This is used to provide information for the development of AB policies on a national level (19). On the local level, NHs receive information about their current AB practices. Due to the limited amount of time and resources available for the study, only the incidence module was evaluated. The incidence module was chosen as this module is most often used for providing insights for prevention strategies. Moreover, the SNIV project team was most interested in NHs’ views on the incidence module as this module requires a minimum of thirty NHs to provide representative and comparable national data. However, participants numbers have been slightly decreasing over the years , despite the fact that there are over 450 NHs in The Netherlands, of which SNIV only recruited about 7%(64).
38
NH recruitment takes place through academic networks, national congresses and symposia and an annual recruitment mail to all NHs. Interested NHs can invite the SNIV project team to provide more information and presentations. NHs with more than fifty residents are eligible for participation (19). As of January 2018, 32 NHs of 19 institutions participated in the incidence module, as some institutions participate with multiple NHs. The infections included in the incidence module were chosen by an expert team during the development stage (19). The used definitions are in accordance with clinical case definitions of the medical practice in NH settings in the Netherlands and are supplemented in Appendix 3. In addition to the infection registration, several supplementary questions are required if a case is registered (19). For example, the age group in which the case took place or whether there was an outbreak, an example of a registration form (in Dutch) is provided in Appendix 2. For the incidence module, Auers et al. (26)’s first SS key function, data collection, involves the following six steps. First, NH characteristics, such as size, NH’s capacity, the clients, infection prevention and AB policies and collaborations with external parties are gathered in an annual questionnaire, which can be found in Appendix 1 (in Dutch). Step two implies diagnosing that the client has an infection. This involves visiting the client, assessing the client’s symptoms and sometimes performing a diagnostics test. After diagnosis, the ECP has to remember to register the infection. The registration is structured differently in each NH, some send an email to their secretary assistant, others register in their electronic patient file (EPF) and others mark the registration form of Appendix 2. Step four goes along with remembering to register and involves checking whether the diagnosed infection is in line with the SNIV definition of the infection (Appendix 3). Next, one person has to collect all registered infections, calculate the number of infections per age range and the total sum of infections from all wards of the NH. The manner in which this is done, is dependent on the structure of the NHs, some retrieve this information from the EPF, others from all emails, and others collect all registration forms from all wards. Finally, the sum of the infections is entered into in a web based-application, called OSIRIS (Online system for infectious diseases within ISIS). A screenshot of the OSIRIS interface is provided in Appendix 4. All NHs have a personalized login code. Data from other NHs is only visible to the researchers at the RIVM (19). The second key function, data analysis is performed by the researchers at the RIVM, who also manage the data. The results are processed in feedback reports (FRs) once a year. These FRs include the incidence rate over the past year in comparison to the national average and in comparison to other NHs of comparable size and organization, for each infection separately (19). To ensure anonymity, data from other NHs is provided as an average. The FRs are send to the person responsible for data entry, who are expected to share report with other NH staff. An example of a FR is provided in Appendix 5, to ensure anonymity the names and numbers of the report have been adapted. NHs have the possibility of retrieving their registered data from OSIRIS at any time in various output formats, such as Excel sheets. However, this output does not involve analysis. Data interpretation, the third function, concerns the understanding and usability of the FRs. Passive dissemination is done by the RIVM by sharing the FRs with the NHs. Actively using the FRs for improving policies and practices in the NHs is expected to be conducted by the NHs themselves.

39
4.3 Setting The study took place in various NHs in the Netherlands from November 2017 until February 2018. NHs from seven of the eight regional antibiotics resistance (ABR) care networks in the Netherlands were included, only the Gelders Antiobioticaresistentie & Infectiepreventie Network was not included. Regional AB resistance networks were created in 2016 by the Dutch government in response to the growing awareness to the importance of ABR. The networks play an important and active role with regards to AB resistance prevention on a regional level.
4.4 Sample For the interviews and FGD a purposive sampling strategy was applied, specifically a maximum variation sampling strategy. This type of sampling allows for a divers sample to be selected and a wide range of perspectives to be included (31). Therefore, participants were selected purposively based on their presumed attitudes towards SNIV (e.g. NHs that had decided to not participate after receiving presentations). For the interviews, ECPs from NHs that currently participate (SNIV NH), that used to participate (former-SNIV NH) and that never participated in the SNIV (non-SNIV NH) project, were invited. Henceforth, the SNIV project, refers to the incidence module of SNIV, NHs that participated in other SNIV modules are considered as non-SNIV. These three groups were chosen as they provide a divers sample of potential SNIV end-users. ECPs were selected as they are usually the designated person for SNIV and diagnose the infections. However, in cases where the designated person for SNIV was someone other than the ECP, that designated person was invited. All participants were invited by email and a sample email is added in Appendix 6. SNIV and former-SNIV NHs were selected from the SNIV database available at the RIVM. Non-SNIV NHs were selected from a list of all NHs in the Netherlands and known NHs that turned down participation in SNIV. For the FGD, only ECPs of SNIV NHs were invited. Only participants who did not participate in the interviews were invited for the FGD. A comparable invitation mail as Appendix 6 was used for the FGD invitations. In addition to the mail, an information leaflet about the FGD and the research was provided, the leaflet can be found in Appendix 7. FGD participants were also invited by mail and received a reminder after two weeks.
In total, 46 NHs were invited for the interviews and ten for the FGD. Data saturation was aimed for. However, due to time constraints only ten interviews and one FGD with three participants were
Table 6. Overview of the accepted invitations and send invitations. Invited (n) Participated (n) Interviews (total) Former-SNIV NHs SNIV NHs Non-SNIV NHs
46 14 14 18
10 1 3 6
Focus group discussion (total) SNIV NHs
10 10
3 3
NH= Nursing home, SNIV= Surveillance network infectious diseases nursing homes (former= NH that used to participate in SNIV; non= NHs that never participated in SNIV)
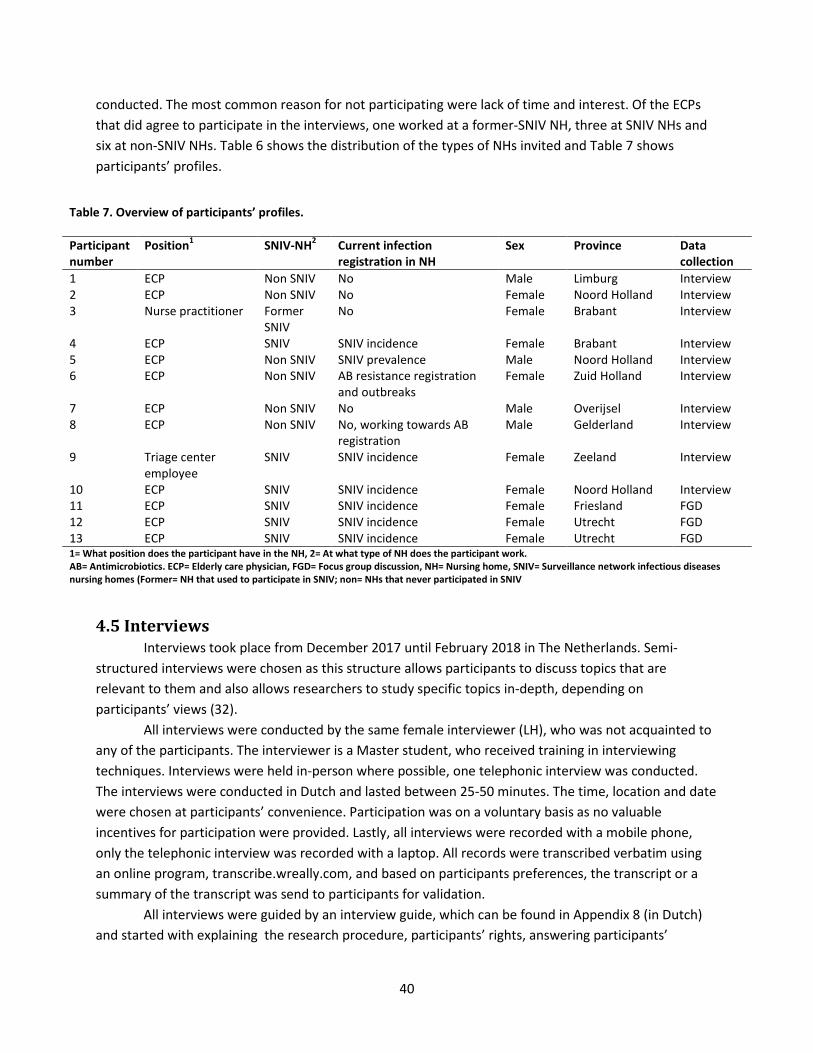
40
conducted. The most common reason for not participating were lack of time and interest. Of the ECPs that did agree to participate in the interviews, one worked at a former-SNIV NH, three at SNIV NHs and six at non-SNIV NHs. Table 6 shows the distribution of the types of NHs invited and Table 7 shows participants’ profiles.
4.5 Interviews Interviews took place from December 2017 until February 2018 in The Netherlands. Semi-structured interviews were chosen as this structure allows participants to discuss topics that are relevant to them and also allows researchers to study specific topics in-depth, depending on participants’ views (32). All interviews were conducted by the same female interviewer (LH), who was not acquainted to any of the participants. The interviewer is a Master student, who received training in interviewing techniques. Interviews were held in-person where possible, one telephonic interview was conducted. The interviews were conducted in Dutch and lasted between 25-50 minutes. The time, location and date were chosen at participants’ convenience. Participation was on a voluntary basis as no valuable incentives for participation were provided. Lastly, all interviews were recorded with a mobile phone, only the telephonic interview was recorded with a laptop. All records were transcribed verbatim using an online program, transcribe.wreally.com, and based on participants preferences, the transcript or a summary of the transcript was send to participants for validation. All interviews were guided by an interview guide, which can be found in Appendix 8 (in Dutch) and started with explaining the research procedure, participants’ rights, answering participants’
Table 7. Overview of participants’ profiles.
Participant number
Position1 SNIV-NH2 Current infection registration in NH
Sex Province Data collection
1 ECP Non SNIV No Male Limburg Interview 2 ECP Non SNIV No Female Noord Holland Interview 3 Nurse practitioner Former
SNIV No Female Brabant Interview
4 ECP SNIV SNIV incidence Female Brabant Interview 5 ECP Non SNIV SNIV prevalence Male Noord Holland Interview 6 ECP Non SNIV AB resistance registration
and outbreaks Female Zuid Holland Interview
7 ECP Non SNIV No Male Overijsel Interview 8 ECP Non SNIV No, working towards AB
registration Male Gelderland Interview
9 Triage center employee
SNIV SNIV incidence Female Zeeland Interview
10 ECP SNIV SNIV incidence Female Noord Holland Interview 11 ECP SNIV SNIV incidence Female Friesland FGD 12 ECP SNIV SNIV incidence Female Utrecht FGD 13 ECP SNIV SNIV incidence Female Utrecht FGD 1= What position does the participant have in the NH, 2= At what type of NH does the participant work. AB= Antimicrobiotics. ECP= Elderly care physician, FGD= Focus group discussion, NH= Nursing home, SNIV= Surveillance network infectious diseases nursing homes (Former= NH that used to participate in SNIV; non= NHs that never participated in SNIV

41
questions and signing the consent form (Appendix 9). Development of the guide was in accordance with Castillo-Montoya (33)’s four-phase process to interview protocol refinement, and was based on Auer et al. (26)’s framework and Flottorp et al.(65)’s checklist for identifying determinants of healthcare professional practice. The following topics were discussed: SNIV, reasons for infection registration, SNIV registration, SNIV FRs or results of infection registration systems, interpretation and sharing of the FRs, person executing the registration and suggestions for improvement. Interview guides were slightly adapted for SNIV, former-SNIV and non-SNIV participants, but the outline remained similar. Since the interviews were semi-structured, not all questions were addressed in each interview and topics that emerged during the interview were also discussed. During the process, some minor modifications were made to the guide in response to evaluations of the previous interviews. For example, question number 10 about the presentation provided by the SNIV team were added after this topic come up in the first interview and after the first five interviews the registration forms, infection definitions and FRs (Appendix 2, 3 and 5, respectively), were taken to the interviews, as participants indicated that this would facilitate the discussion of these topics.
4.6 Focus group discussion A FGD was chosen to identify solutions and areas for solutions as FGDs generate richer and fuller data than interviews and allow for discussions among participants (32). This has been proven particularly useful for evaluating fields for improvement (32). The FGD was homogeneous and was facilitated by one female researcher (LH). Initially, the presence of an observer was planned. However, due to transportation constraints the observer could not be present, the FGD was not rescheduled as the time and date was chosen at participants’ convenience. The FGD was held in Dutch and lasted two hours. An external location in Utrecht was chosen for the FGD, as Utrecht is a easily accessible and a central location in the Netherlands. A FGD guide was developed and is provided in Appendix 10. Based on the findings of the interviews and a discussion of these findings with the SNIV project team, two topics were chosen for the FGD; the FRs and data collection methods of SNIV. These were chosen as they showed to be relevant for both the interview participants and the SNIV project team. Additionally, improvements for these two topics seemed most achievable. The aim of the FGD was two-folded. On the one hand, it was to assess whether the barriers and facilitators found in the interviews regarding the FRs and data collection methods, were also recognized by the FG participants. On the other hand, the aim was to identify strategies and solutions to addressing these barriers and enhancing these facilitators. The FGD also provided an opportunity to assess the extent of data saturation for the two topics that were discussed. Participants were asked to write down their thought on post-it notes, in order to enhance understanding and engagement and involvement in the discussion . For both topics the structure was the same. First, participants wrote down three positive and three negative aspects on post-its, which were then discussed with the whole group. Next, participants wrote down solutions for each positive and negative aspect, which were then discussed with the whole group. After each round of discussion participants had the opportunity to add more post-its. At the end of the FGD, additional topics and solutions that came up were discussed and other solutions that were mentioned during the interviews were discussed to assess FGD participants’ opinions. Initially, selecting a top five of the solutions to be discussed in further detail was planned. However, as the FGD emerged most solutions were already

42
discussed in detail and the limited time available did not allow for a selection to be made. An overview of the initial
structure of the FGD is provided in Table 8. The FGD was recorded and transcribed verbatim and based
on participants preferences, the transcript or a summary of the transcript was send to participants for validation.
4.7 Ethical considerations Ethical approval from an ethics committee was not required for the current study, as it did not fall under Dutch medical research involving human subjects act (34). Nonetheless, the principles of responsible research were applied (35). First, informed consent was obtained from all participants after a thorough explanation of the research and their rights. All participants signed the consent form provided in Appendix 9. To guarantee participants right to privacy, only researchers of the SNIV incidence module at the RIVM had access to the audio recordings, transcripts and consent forms (35). The recordings and transcripts are kept confidential, and will be destroyed after 5 years. To ensure anonymity, no unique identifiers were linked to data and all participants were registered using codes, which were also used for reporting responses (35). Depending on participants’ preferences, they received a copy of the transcript or a summary of the transcript and the findings of the study.
4.8 Data analysis Data from both the interviews and the FGDs were analyzed in Atlas.ti using qualitative content analysis. First, all data were read repeatedly to obtain a clear understanding of the data. Then, open coding was applied. This type of analysis is useful to create a clear understanding of the issues without imposing preconceived categories (36). Open coding was done for the first two interviews by two
Table 8. Overview of the initial structure of the focus group discussion. Description Introduction Short introduction of the research, the FGD, confidentially matters and signing the consent forms Introduction round: Each participant introduces themselves and their NH
Topic 1 Feedback reports Identify facilitators and barriers
Participants write down three positive and three negative aspects on post-its, which are then discussed with the whole group
Identify solutions Participants write down solutions for each positive and negative aspect, which are then discussed with the whole group and additional solutions may be identified
Select top solutions A top five is selected to discuss in more detail In-depth discussion The top five is discussed in more detail. Break
Theme 2 Data collection methods of SNIV Identify facilitators and barriers
Participants write down three positive and three negative aspects on post-its, which are then discussed with the whole group
Identify solutions Participants write down solutions for each positive and negative aspect, which are then discussed with the whole group and additional solutions may be identified
Select top solutions A top five is selected to discuss in more detail In-depth discussion The top five is discussed in more detail. Closure Summarize and conclude the FGD FGD= Focus group discussion, NH= Nursing home, SNIV= Surveillance network for infectious diseases in nursing homes

43
researchers separately, from which codes and categories emerged. Then, the categories and codes were discussed and a codebook was developed. Then, the first six interviews were coded by the same two researchers independently, using the same codebook to assess the inter-rater reliability(36). Discrepancy in codes were discussed until consensus was reached, only minor changes were made and the final codebook is provided in Appendix 11. The FGD was also coded by two researchers independently, following the principles of open coding. The codes and categories were then discussed and a new codebook was developed, after which the FGD was coded again according to the final codebook, provided in Appendix 12. For both the interviews and FDG analysis, no consult with a third researcher was required. Emerging categories, sub categories and corresponding factors from the interviews and FGD were identified by both researchers independently, and then discussed and described in the results.
4.9 Trustworthiness In order to ensure trustworthiness of data, several issues were considered. First, the overall reporting of the study was done according to O’brien et al. (37)’s recommendations for the standards of reporting qualitative research. Additionally, the consolidated criteria for reporting qualitative research by Tong et al. (38) was used for the reporting of the methods and results section. Close attention was paid to the concept of transparency to provide a clear context for the interpretation of the findings. The methodology of the research is provided in detail, including details about the conducting researcher and additional documents were provided in Appendices. As part of this transparency, potential sources of bias and the concept of transferability are discussed in the discussion section. Additionally, cross-checking codes during data analysis is also a means of enhancing data quality. Finally, quality and credibility of data analysis were enhanced by applying triangulation of qualitative data sources . First, different point of views (e.g. SNIV, former- SNIV and non-SNIV NHs) were taken into account. Second, the findings from the individual interviews were assessed in a more public setting of the FGDs.
5. Time table Internship week Date What
1-5 13/11/2017-15/12/2017 Work on extended research proposal 3-6 27/11/2017-22/12/2017 Send out invitations for interview and
prepare interview guide 6 22/12/2017 Go/no-go evaluation Christmas break 7-12 08/01/2018-16/02/2018 Data collection 7 10/01/2018 Pick a date for the FGD 8 16/01/2018 Coding first two interviews 9 23/01/2018
25/01/2018 Finished coding all interviews Discuss preliminary findings of interviews and structure of FG with the supervisor

44
10 29/01/2018-02/02/2018 30/01/2018
Send reminded of the FGD to all participants Discuss preliminary findings of interviews and structure of FG with the SNIV project team
11 09/02/2018 FGD 12 12/02/2018-16/02/2018 Transcribing and analysis of FGD
13-17 19/02/2018-25/03/2018 Finishing analysis and report writing
17 25/03/2018 Hand-in draft version 20 13/04/2018 Deadline final version

45
References 1. WHO. Report on the Burden of Endemic Health Care-Associated Infection Worldwide- Clean Care is Safer Care. Geneva: World Health Organisation; 2011. 2. Koch AM, Eriksen HM, Elstrom P, Aavitsland P, Harthug S. Severe consequences of healthcare-associated infections among residents of nursing homes: a cohort study. J Hosp Infect. 2009;71(3):269-74. 3. Strausbaugh LJ, Sukumar SR, Joseph CL. Infectious Disease Outbreaks in Nursing Homes: An Unappreciated Hazard for Frail Elderly Persons. Clinical Infectious Diseases. Clinical Infectious Diseases. 2002;36:870-6. 4. Glezen WP, Greenberg SB, Atmar RL, Piedra PA, Couch RB. Impact of respiratory virus infections on persons with chronic underlying conditions. Jama. 2000;283(4):499-505. 5. Enserink R, Meijer A, Dijkstra F, van Benthem B, van der Steen JT, Haenen A, et al. Absence of Influenza A(H1N1) During Seasonal and Pandemic Seasons in a Sentinel Nursing Home Surveillance Network in the Netherlands. Journal of the American Geriatrics Society. 2011;59(12):2301-5. 6. World Population Ageing Report. United Nations; 2015. Contract No.: ST/ESA/SER.A/390. 7. commision E. Eurostat yearbook 2010 2010 [Available from: http://epp.eurostat.ec.europa.eu/cache/ITY_OFFPUB/KS-CD-10-220/EN/KS-CD-10-220-EN.PDF. 8. Juthani-Mehta M, Quagliarello VJ. Infectious Diseases in the Nursing Home Setting: Challenges and Opportunities for Clinical Investigation. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2010;51(8):931-6. 9. Van Esch G, Van Broeck J, Delmee M, Catry B. Surveillance of Clostridium difficile infections in a long-term care psychogeriatric facility: outbreak analysis and policy improvement. Archives of public health = Archives belges de sante publique. 2015;73(1):18. 10. Iijima Y, Iwamoto T, Nukuzuma S, Ohishi H, Hayashi K, Kobayashi N. An outbreak of rotavirus infection among adults in an institution for rehabilitation: long-term residence in a closed community as a risk factor for rotavirus illness. Scandinavian journal of infectious diseases. 2006;38(6-7):490-6. 11. Verkade E, Bosch T, Hendriks Y, Kluytmans J. Outbreak of methicillin-resistant Staphylococcus aureus ST398 in a Dutch nursing home. Infection control and hospital epidemiology. 2012;33(6):624-6. 12. Bond KC, Macfarlane SB, Burke C, Ungchusak K, Wibulpolprasert S. The evolution and expansion of regional disease surveillance networks and their role in mitigating the threat of infectious disease outbreaks. Emerging health threats journal. 2013;6. 13. Palumbo AJ, Loveless PA, Moll ME, Ostroff S. Evaluation of healthcare-associated infection surveillance in Pennsylvania hospitals. Infection control and hospital epidemiology. 2012;33(2):105-11. 14. Choi HJ, Adiyani L, Sung J, Choi JY, Kim HB, Kim YK, et al. Five-year decreased incidence of surgical site infections following gastrectomy and prosthetic joint replacement surgery through active surveillance by the Korean Nosocomial Infection Surveillance System. J Hosp Infect. 2016;93(4):339-46. 15. Schroder C, Schwab F, Behnke M, Breier AC, Maechler F, Piening B, et al. Epidemiology of healthcare associated infections in Germany: Nearly 20 years of surveillance. International journal of medical microbiology : IJMM. 2015;305(7):799-806. 16. Marchi M, Grilli E, Mongardi M, Bedosti C, Nobilio L, Moro ML. Prevalence of infections in long-term care facilities: how to read it? Infection. 2012;40(5):493-500. 17. Freeman R, Moore LS, Garcia Alvarez L, Charlett A, Holmes A. Advances in electronic surveillance for healthcare-associated infections in the 21st Century: a systematic review. J Hosp Infect. 2013;84(2):106-19. 18. Hajdu A, Eriksen HM, Sorknes NK, Hauge SH, Loewer HL, Iversen BG, et al. Evaluation of the national surveillance system for point-prevalence of healthcare-associated infections in hospitals and in long-term care facilities for elderly in Norway, 2002-2008. BMC Public Health. 2011;11:923-.

46
19. RIVM. Surveillance Netwerk Infectieziekten in Verpleeghuizen. Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu (RIVM); 2016. 20. Haenen A, Alblas J, De Greeff S, Veldman M-J. Surveillance of infections in nursing homes in the Netherlands, how to come from information to action. International Journal of Infection Control. 2014;10(4). 21. CDC. Frameworks for Evaluating Public Health Surveillance Systems for Early Detection of Outbreaks. Atlanta: Centers for Disease Control and Prevention:, Services UDoHaH; 2004. 22. Van den Brand M. Validation of infectious diseases surveillance in nursing homes in the Netherlands [Master thesis]. Bilthoven: VU UniversityAmsterdam; 2010. 23. Calba C, Goutard FL, Hoinville L, Hendrikx P, Lindberg A, Saegerman C, et al. Surveillance systems evaluation: a systematic review of the existing approaches. BMC Public Health. 2015;15(1):448. 24. Meynard JB, Chaudet H, Green AD, Jefferson HL, Texier G, Webber D, et al. Proposal of a framework for evaluating military surveillance systems for early detection of outbreaks on duty areas. BMC Public Health. 2008;8:146. 25. Holder Y, Peden M, Krug E, Lund J, Gururaj G, Kobusingye O. Injury surveillance guidelines. Geneva: World Health Organization; 2001 2001. 26. Auer AM, Dobmeler TM, Haglund BJA, Tilgren P. The relevance of WHO injury surveillance guidelines for evaluation: learning from the Aboboriginal Community-Centered Injury Surveillance System (ACCISS) and two institution-based systems. BMC Public Health. 2011;11. 27. Mariner JC, Hendrickx S, Pfeiffer DU, Costard S, Knopf L, Okuthe S, et al. Integration of participatory approaches into surveillance systems. Rev Sci Tech. 2011;30(3):653-9. 28. Calba C, Antoine-Moussiaux N, Charrier F, Hendrikx P, Saegerman C, Peyre M, et al. Applying participatory approaches in the evaluation of surveillance systems: A pilot study on African swine fever surveillance in Corsica. Prev Vet Med. 2015;122(4):389-98. 29. Calba C, Goutard FL, Vanholme L, Antoine-Moussiaux N, Hendrikx P, Saegerman C. The Added-Value of Using Participatory Approaches to Assess the Acceptability of Surveillance Systems: The Case of Bovine Tuberculosis in Belgium. PLoS One. 2016;11(7):e0159041. 30. Schulz K, Calba C, Peyre M, Staubach C, Conraths FJ. Hunters' acceptability of the surveillance system and alternative surveillance strategies for classical swine fever in wild boar - a participatory approach. BMC Vet Res. 2016;12(1):187. 31. Purposive sampling: Lund Research Ltd; 2012 [updated 2012. Available from: http://dissertation.laerd.com/purposive-sampling.php#types. 32. Then KL, Rankin J, ALi E. Focus group research: what is it and how can it be used? Canadian jornal of cardiovascular nursing. 2014;24(1):16-22. 33. Castillo-Montoya M. Preparing for Interview Research: The Interview Protocol Refinement Framework. The Qualitative Report. 2016;21(5):811-31. 34. CCMO. Your research: does it fall under the WMO The Hague: Central Committee on Research Involving Human Subjects; [Available from: http://www.ccmo.nl/en/your-research-does-it-fall-under-the-wmo. 35. Boeije H. Analysis in qualitative research. First ed. London: SAGE publications; 2010. 36. Hsieh HF, Shannon SE. Three Approaches to Qualitative Content Analysis. Qualitative health research. 2005;15(9):1277-88. 37. O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245-51. 38. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International journal for quality in health care : journal of the International Society for Quality in Health Care. 2007;19(6):349-57.

47
39. Mitchell RJ, Williamson AM, O'Connor R. The development of an evaluation framework for injury surveillance systems. BMC Public Health. 2009;9:260. 40. Russo PL, Havers SM, Cheng AC, Richards M, Graves N, Hall L. Characteristics of national and statewide health care-associated infection surveillance programs: A qualitative study. Am J Infect Control. 2016;44(12):1505-10. 41. Ekegren CL, Donaldson A, Gabbe BJ, Finch CF. Implementing injury surveillance systems alongside injury prevention programs: evaluation of an online surveillance system in a community setting. Injury Epidemiology. 2014;4(1):19-34. 42. Whittaker AA, Aufdenkamp M, Tinley S. Barriers and facilitators to electronic documentation in a rural hospital. J Nurs Scholarsh. 2009;41(3):293-300. 43. Kaasalainen S, Agarwal G, Dolovich L, Papaioannou A, Brazil K, Akhtar-Danesh N. Nurses’ Perceptions of and Satisfaction With the Medication Administration System in Long-Term-Care Homes. Canadian Journal of Nursing Research. 2010;42(4):59-79. 44. McKinnon AD, Ozanne-Smith J, Pope R. Optimizing the Utility of Military Injury Surveillance Systems: A Qualitative Study Within the Australian Defence Force. Military Medicine. 2009;174(5):470-9. 45. Cantrell J, Ganz O, Ilakkuvan V, Tacelosky M, Kreslake J, Moon-Howard J, et al. Implementation of a Multimodal Mobile System for Point-of-Sale Surveillance: Lessons Learned From Case Studies in Washington, DC, and New York City. JMIR Public Health and Surveillance. 2015;1(2):e20. 46. Paterson BJ, Kool JL, Durrheim DN, Pavlin B. Sustaining surveillance: Evaluating syndromic surveillance in the Pacific. Global Public Health. 2012;7(7):682-94. 47. Fossum M, Ehnfors M, Fruhling A, Ehrenberg A. An evaluation of the usability of a computerized decision support system for nursing homes. Appl Clin Inform. 2011;2(4):420-36. 48. Eley R, Fallon T, Soar J, Buikstra E, Hegney D. Barriers to use of information and computer technology by Australia's nurses: a national survey. J clin Nurs. 2009;18(8):1151-8. 49. Zargaran E, Schuurman N, Nicol AJ, Matzopoulos R, Cinnamon J, Taulu T, et al. The Electronic Trauma Health Record: Design and Usability of a Novel Tablet-Based Tool for Trauma Care and Injury Surveillance in Low Resource Settings. Journal of the American College of Surgeons. 2014;218(1):41-50. 50. Dubberke ER, Nyazee HA, Yokoe DS, Mayer J, Stevenson KB, Mangino JE, et al. Implementing Automated Surveillance for Tracking Clostridium difficile Infection at Multiple Healthcare Facilities. Infection control and hospital epidemiology : the official journal of the Society of Hospital Epidemiologists of America. 2012;33(3):305-8. 51. Chalfine A, Cauet D, Lin WC, Gonot J, Calvo-Verjat N, Dazza FE, et al. Highly sensitive and efficient computer-assisted system for routine surveillance for surgical site infection. Infection Control Hospital Epidemiology. 2006;27(8):794-801. 52. Woeltje KF, Lautenbach E. Informatics and epidemiology in infection control. Infectious diseases clinical north america. 2011;25(1):261-70. 53. Dixon BE, Siegel JA, Oemig TV, Grannis SJ. Electronic Health Information Quality Challenges and Interventions to Improve Public Health Surveillance Data and Practice. Public Health Reports. 2013;128(6):546-53. 54. Starren J, Tsau C, Bakken S, al. e. The role of nurses in installing telehealth technology in the home. Comput Inform Nurs. 2005;23:181-9. 55. Pahl-Wostl C. Participative and Stakeholder-Based Policy Design, Evaluation and Modeling Processes. Integrated Assessment. 2002;3(1). 56. Rogers EM. Diffusion of innovations: Simon and Schuster.; 1983. 57. Reeder B, Revere D, Olson DR, Lober WB. Perceived usefulness of a distributed community-based syndromic surveillance system: a pilot qualitative evaluation study. BMC Res Notes. 2011;4:187. 58. Kool JL, Paterson B, Pavlin BI, Durrheim D, Musto J, Kolbe A. Pacific-wide simplified syndromic surveillance for early warning of outbreaks. Global Public Health. 2012;7(7):670-81.

48
59. Birkhead GS, Klompas M, Shah NR. Uses of Electronic Health Records for Public Health Surveillance to Advance Public Health. Annual Review of Public Health. 2015;36(1):345-59. 60. van der Weerd W, Timmermans DRM, Beaujean DJMA, Oudhoff J, van Steenbergen JE. Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health. 2011;11:575-. 61. Arend J, Schmeets H. Social en institutioneel vertrouwen in Nederland. Den Haag: Centraal bureau voor de statistiek; 2015 January 2015. 62. van Wijk E, Meijer I. Research performance analysis for the SOR programme of the Rijksinstituut voor Volksgezondheid en Milieu (RIVM) 2011-2014/15. Leiden: CWTS 2017. 63. Bekendheid en imago RIVM 2015. TNS Nipo; 2015 November 2015. 64. Planbureau SeC. Zorg in de laatste jaren – Gezondheid en hulpgebruik in verzorgings en verpleeghuizen 2000-2008. SCP; 2011. Contract No.: 01-12. 65. Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: A systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8(35):1-11.

49
Appendix 1 - Annual questionnaire (in Dutch) U kunt het formulier ook invullen in OSIRIS datum:……………………………………………………………………………………………. Algemene gegevens Naam zorggroep:………………………………………………………………………………………… Naam locatie deelnemend verpleeghuis: …………………………………………………... (n.b. per deelnemende locatie apart een formulier invullen) Post adres verpleeghuis:…………………………………………………………………………. Postcode:………………………………………………………………………… ……………………… Plaatsnaam:……………………………………………………………………… ………………………. Contactpersoon SNIV (inhoudelijk verantwoordelijke) naam:………………………………………………… e-mail………………………………………........ Telefoonnummer:………………………………………………………………………………………… Contactpersoon OSIRIS (verantwoordelijke registratie in OSIRIS) naam:…………………………………………………. e-mail………………………………………........ Telefoonnummer:………………………………………………………………………………………… De vragenlijst bevat items over de volgende zes hoofdcategorieën: (1) Capaciteitsgegevens (2) Informatie over cliëntenpopulatie (3) Infectiepreventiebeleid (4) Antibioticabeleid (5) Mondzorg (6) Samenwerkingsverbanden (7) Automatisering Bedankt voor het invullen! U kunt het formulier invullen in OSIRIS of met de bijgevoegde antwoordenvelop (kosteloos) terugsturen. Secretariaat SNIV , RIVM - Centrum Infectieziektebestrijding Epidemiologie en Surveillance (interne postbak 75) Postbus 1, 3720 BA Bilthoven. (1) Capaciteitsgegevens 1. Totaal aantal bedden (volgens productieafspraken) in het verpleeghuis: ______ 2. Totaal aantal dagen met zorg en verblijf in 2013: ______ 3. Totaal aantal gemeenschappelijke ruimten (kantine, restaurant, recreatieruimte, enz) in het verpleeghuis die door alle zorgeenheden gebruikt (kunnen) worden: _____ ruimten 4. Aantal zorgeenheden: _____ (gedefinieerd als functionele eenheid met een vaste groep personeelsleden die gezamenlijk 24-uurs verzorging regelen voor een vaste groep patiënten, fysiek gescheiden van andere eenheden; ook vaak aangeduid als afdeling, unit, etage, locatie, leefgroep, en dergelijke) Indien bij U een zorgeenheid anders gedefinieerd is, gaarne toelichting: __________________________________________________________

50
5. Hoeveel bewoners zijn er per zorgzwaarte pakket: Pakket 4:. __________ Pakket 5:. ___________ Pakket 6:. _______________ Pakket 7:. ____________ Pakket 8:. ____________ Pakket 9:. _______________ Pakket 10:. ___________ 6. Werkt het verzorgend/verplegend personeel op één zorgeenheid? Ja Ja, maar er vindt incidenteel uitwisseling van verzorgend/verplegend personeel plaats Ja, maar er vindt regelmatig uitwisseling van verzorgend/verplegend personeel plaats Nee 7. Wordt er door het verzorgend/verplegend personeel dienstkleding gedragen? ja nee
(2) Informatie over cliëntenpopulatie 8. Welk deel van de cliënten is gevaccineerd tegen influenza in najaar 2013? ______% 9. Welk deel van het personeel is gevaccineerd tegen influenza in najaar 2013?? ______% 10. Heeft u campagne gevoerd om de influenza-vaccinatiegraad onder het personeel het afgelopen seizoen te verhogen? Ja Nee 11. Uit welke gemeenten (max. 3) komen het grootste deel van de cliënten? ……………………………….…………………………………………………………………………………... 12. In hoeverre hebben de bewoners van het verpleeghuis beschikking over: <25% 25-50% 50-75% >75% eigen kamer eigen toilet eigen badkamer 13. Kunt u per zorgeenheid (ZE) aangeven welk type zorgeenheid dit is (somatisch, psychogeriatrisch, revalidatie, palliatief, anders), hoeveel bewoners, verzorgende/verplegende personeelsleden en gemeenschappelijk ruimten (eetzalen, gezamenlijke woonkamers, recreatieruimten, enz) er zijn: Naam zorgeenheid Type zorgeenheid/Aantal bewoners/Aantal verzorgenden/Aantal gemeenschappelijke ruimten/*Frequentie bezoek van buiten(zelden/regelmatig/vaak) *mochten gemeenschappelijke ruimten (deels) gedeeld worden door meerdere zorgeenheden, wilt u dit dan duidelijk vermelden. 14. Globale leeftijdsrange van de bewoners in het verpleeghuis: Aantal bewoners <60 jaar :……………………………………………………………………….. Aantal bewoners 60-64 jaar:………………………………………………………………………. Aantal bewoners 65-74 jaar:………………………………………………………………………. Aantal bewoners 75-84 jaar:………………………………………………………………………. Aantal bewoners ≥ 85 jaar:…………………………………………….………………………..

51
(3) Infectiepreventiebeleid
15. Heeft uw verpleeghuis een infectiepreventiecommissie? Ja Nee Zo ja, wat is de samenstelling van de commissie? Medisch manager Ja Nee Verpleegkundig manager Ja Nee Microbioloog ziekenhuis Ja Nee Infectiepreventie adviseur Ja Nee Specialist ouderenzorg Ja Nee Anderen: _______________ 16. Heeft het verpleeghuis een eigen infectiepreventieadviseur in dienst? Ja Nee Indien ja, voor hoeveel uur per week? _______ Indien nee, met wie wordt overlegd in geval van vragen op het gebied van infectiepreventie Specialist ouderenzorg Ja Nee Infectiepreventie adviseur ziekenhuis Ja Nee Microbioloog ziekenhuis Ja Nee GGD Ja Nee RIVM-CIB Ja Nee Anderen _______________ 17. Welke testen gebruikt u bij bewoners met klachten of verschijnselen, die door een UWI veroorzaakt kunnen zijn*: Leukotest Nitriettest Dipslide Kweek anders, nl ........................................ ..................................................................................................................................................................... *meerdere antwoorden mogelijk (4) Antibioticabeleid 18. Heeft het verpleeghuis een antibiotica- of geneesmiddelencommissie? Ja Nee Zo ja, wat is de samenstelling van de commissie? Apotheker ziekenhuis Ja Nee Specialist(en) ouderenzorg Ja Nee Microbioloog ziekenhuis Ja Nee Anderen _______________ 19. Heeft het verpleeghuis een antibioticaformularium? Ja Nee Zo ja, is dit formularium gebaseerd op de richtlijnen van: SWAB Ja Nee NHG Ja Nee Ziekenhuis Ja Nee Anders, t.w. _______________ (5) Mondzorg 20. Wordt er in het verpleeghuis professionele mondzorg verleend door een mondhygiënist of tandarts? Ja, door een tandarts voor ……. uur per week Ja, door een mondhygiënist voor ……. uur per week Nee 21. Is in het verpleeghuis de Verenso richtlijn: 'Mondzorg voor zorgafhankelijke cliënten in verpleeghuizen' vertaald naar een protocol en wordt deze toegepast in de dagelijkse praktijk? Ja Nee

52
(6) Samenwerkingsverbanden 22. Medisch Microbiologisch Laboratorium (MML) voor diagnostiek: ............................................................. Contactpersoon:…………………………………………. e-mail………………………………………........ Telefoonnummer:…………………………………………………………………………………………. 23. Medisch Microbiologisch Laboratorium (MML) voor influenza diagnostiek: ……………………………. Contactpersoon:…………………………………………. e-mail………………………………………........ Telefoonnummer:………………………………………………………………………………………… 24. GGD ….…………………………………………………te …………………………………………….. Contactpersoon:…………………………………………. e-mail………………………………………........ Telefoonnummer:…………………………………………………………………………………………. *SNIV maakt afspraken met uw MML over het insturen van monsters bij uitbraken en informeert uw GGD over deelname aan SNIV. 25. Deelname in academisch netwerk? Ja / Nee Zo ja, welk academisch netwerk? ………………………………………………………………………….. (7) Automatisering 26. Gebruikt u een elektronisch systeem voor de registratie van patiëntgegevens? Ja / Nee Zo ja, wie is de leverancier van dit systeem? Tenslotte 27. Opmerkingen die voor deze surveillance van belang kunnen zijn: ……………………………………………………………………………………………………………… ……………………………………………………………………………………………………………… Bedankt voor het invullen!

53
Appendix 2 - SNIV registration form (in Dutch)

54
Appendix 3 - Definitions SNIV (in Dutch) Gastro-enteritis¹ - OF 3 of meer malen per dag dunne ontlasting, afwijkend van normaal voor deze persoon - OF dunne ontlasting en 2 van de volgende symptomen: Koorts, Braken, misselijkheid, buikpijn, buikkrampen, bloed of slijm bij de ontlasting - OF braken en 2 van de volgende symptomen: Koorts, misselijkheid, buikpijn, buikkrampen, bloed of slijm bij de ontlasting - OF 3 maal braken binnen 24 uur (zonder verder bijkomende klachten EN indien braken niet samenhangt met medicijngebruik) ¹ non-infectieuze oorzaak uitgesloten Influenza-achtig ziektebeeld - Acuut¹ begin van de symptomen² - EN tenminste één van de volgende systemische symptomen: koorts of koortsachtig gevoel, malaise, hoofdpijn, myalgie - EN tenminste één van de volgende drie respiratoire symptomen: Hoest, zere keel, benauwdheid/kortademigheid ¹ Snel opkomend ² Andere waarschijnlijkheidsdiagnoses uitgesloten Vermoedelijk pneumonie - Cliënten met minimaal één van de onderstaande symptomen worden verdacht van een lage luchtweginfectie, vermoedelijk pneumonie, als deze optreden als verandering ten opzichte van de daarvoor bestaande situatie en andere waarschijnlijkheidsdiagnoses uitgesloten: • tachypnoe • malaise • verwardheid • kortademigheid • hoesten (productief of niet productief) • koorts > 38°C of koorts in de afgelopen 48 uur • pijn in de borst (bij ademhaling) - EN met nieuwe focale (eenzijdige) afwijkingen bij auscultatie van de longen
Urineweginfectie (gebaseerd op de Verenso-richtlijn) - Er is sprake van een urineweginfectie wanneer er: • algemene dan wel mictie-gerelateerde klachten en/of verschijnselen bestaan EN • er bovendien tekenen van ontsteking zijn EN • er tevens een bacteriurie is. Ad 1: Pijnlijke, frequente mictie, onderbuiksklachten, anorexie, toegenomen verwardheid, sufheid,vermoeidheid, toegenomen incontinentie van urine en verminderde mobiliteit. Bij afwezigheid van een infectiebron elders. Ad 2: Ontsteking wordt vastgesteld met een leukocytenesterasetest of door microscopisch onderzoek van urinesediment. Ad 3: Bacteriurie wordt vastgesteld met nitriettest of urinekweek (niet van toepassing bij kathetergebruik).

55
Aanvullende gegevens, te registreren bij stellen diagnose Gastro-enteritis Is er vermoedelijk sprake van een outbreak: ja/nee Zijn er monsters opgestuurd naar MML: ja/nee Influenza-achtig ziektebeeld Hoeveel cliënten zijn er behandeld met Tamiflu/antivirale middelen? Is er vermoedelijk sprake van een outbreak: ja/nee Zijn er monsters opgestuurd naar MML: ja/nee Zijn er monsters opgestuurd naar RIVM: ja/nee Vermoedelijk Pneumonie Hoeveel monsters zijn er opgestuurd naar MML? Hoeveel cliënten zijn er doorverwezen naar het ziekenhuis? Urineweginfectie Urethrakatheter gerelateerd ja / nee (ja, als er in de laatste 7 dagen voorafgaand aan de registratiedag een urethrakatheter is gebruikt)

56
Appendix 4 – Interface OSIRIS (in Dutch)

57
Appendix 5 – Anonymized feedback report (in Dutch) Beste Lezer,
Voor u ligt de terugrapportage 2016 van SNIV. In deze terugrapportage vindt u de volgende informatie: het absolute aantal infecties per type infectie wat in uw instelling is geregistreerd in 2016, de leeftijd verdeling van bewoners met deze infecties, en de incidenties per infectie in uw instelling. Al deze getallen worden vergelijken met wat landelijk geregistreerd is.
Pagina 3 Karakteristieken verpleeghuis
Op pagina 3 vindt u de karakteristieken van uw instelling. In de referentiecijfers van SNIV vindt u ook de karakteristeken van instellingen en de incidentie die daar gemeten is. Zo kunt u in de referentiecijfers instellingen zoeken die dezelfde karakteristieken hebben als uw eigen instelling en daarmee uw incidentiecijfer vergelijken en beoordelen of u een hogere of lagere incidentie heeft dan vergelijkbare instellingen. Mogelijk liggen daar waar u een hogere incidentie heeft aanknopingspunten voor verbeteringen.
Pagina 4 Gastro-enteritis
Op pagina 4 ziet u in tabel 2 het aantal nieuwe episodes van gastro-enteritis in uw huis ten opzichte van de andere deelnemers aan SNIV. Absolute aantallen kunt u echter niet goed met elkaar vergelijken, daarvoor kunt u beter de incidentiecijfers in figuur 1 en in tabel 3 en 4 gebruiken.
Pagina 6 Influenza achtig ziektebeeld
Op pagina 6 ziet u in tabel 5 het aantal nieuwe episodes van influenza-achtig ziektebeeld in uw huis ten opzichte van de andere deelnemers aan SNIV. Absolute aantallen kunt u echter niet goed met elkaar vergelijken, daarvoor kunt u beter de incidentiecijfers in figuur 2 en in tabel 6 en 7 gebruiken.
Pagina 8 Vermoedelijke pneumonie
Op pagina 8 ziet u in tabel 8 het aantal nieuwe episodes van vermoedelijk pneumonie in uw huis ten opzichte van de andere deelnemers aan SNIV. Absolute aantallen kunt u echter niet goed met elkaar vergelijken, daarvoor kunt u beter de incidentiecijfers in figuur 3 en in tabel 9 en 10 gebruiken.
Pagina 10 Urineweginfecties
Op pagina 10 ziet u in tabel 11 het aantal nieuwe episodes van urineweginfecties in uw huis ten opzichte van de andere deelnemers aan SNIV. Absolute aantallen kunt u echter niet goed met elkaar vergelijken, daarvoor kunt u beter de incidentiecijfers in figuur 4 en in tabel 12 en 13 gebruiken.
Pagina 12 Mortaliteit
Op pagina 12 ziet u in tabel 14 het aantal sterftegevallen in uw huis ten opzichte van de andere deelnemers aan SNIV. Absolute aantallen kunt u echter niet goed met elkaar vergelijken, daarvoor kunt u beter de incidentiecijfers in figuur 5 en in tabel 15 en 16 gebruiken.

58
Samenvatting terugrapportage
In de vergelijking met de landelijke cijfers valt op UW VERPLEEGHUIS op alle onderdelen onder/boven het landelijk gemiddelde scoort in de incidenties.
Mocht u bij het vergelijken van de cijfers of voor het zoeken naar aanknopingspunten ondersteuning vanuit het SNIV team willen, neemt u dan contact met ons op.
Karakteristieken verpleeghuis
Tabel 1. Karakteristieken van UW verpleeghuis
Karakteristieken Beschrijving
Groot vs. klein verpleeghuis Verpleeghuis met minder dan 130 bedden (namelijk 120)
Gemeenschappelijke ruimten Verpleeghuis met 5 of meer gemeenschappelijke ruimten (namelijk 5)
Uitwisseling personeel tussen zorgeenheden Geen, of incidenteel uitwisseling van verzorgend/verplegend personeel
Eigen kamer >= 50
Eigen badkamer < 50%
Bovenstaande tabel geeft de karakteristieken van het verpleeghuis weer, zoals deze bij SNIV bekend zijn. De landelijke referentiecijfers zijn op een zelfde manier ingedeeld. Zo kunt u de gegevens voor uw verpleeghuis vergelijken met de referentiecijfers.
Gastro-enteritis
Tabel 2. Het absolute aantal gerapporteerde nieuwe episodes van gastro-entiritis per leeftijdscategorie, landelijk versus verpleeghuis
UW HUIS Landelijk
Aantal Percentage Aantal Percentage
<60 jaar 0 0,0 4 0,9
60-64 jaar 0 0,0 3 0,7
65-74 jaar 0 0,0 48 11,1
75-84 jaar 1 33,3 162 37,5
>=85 jaar 2 66,7 215 49,8
Totaal 3 100,0 432 100,0
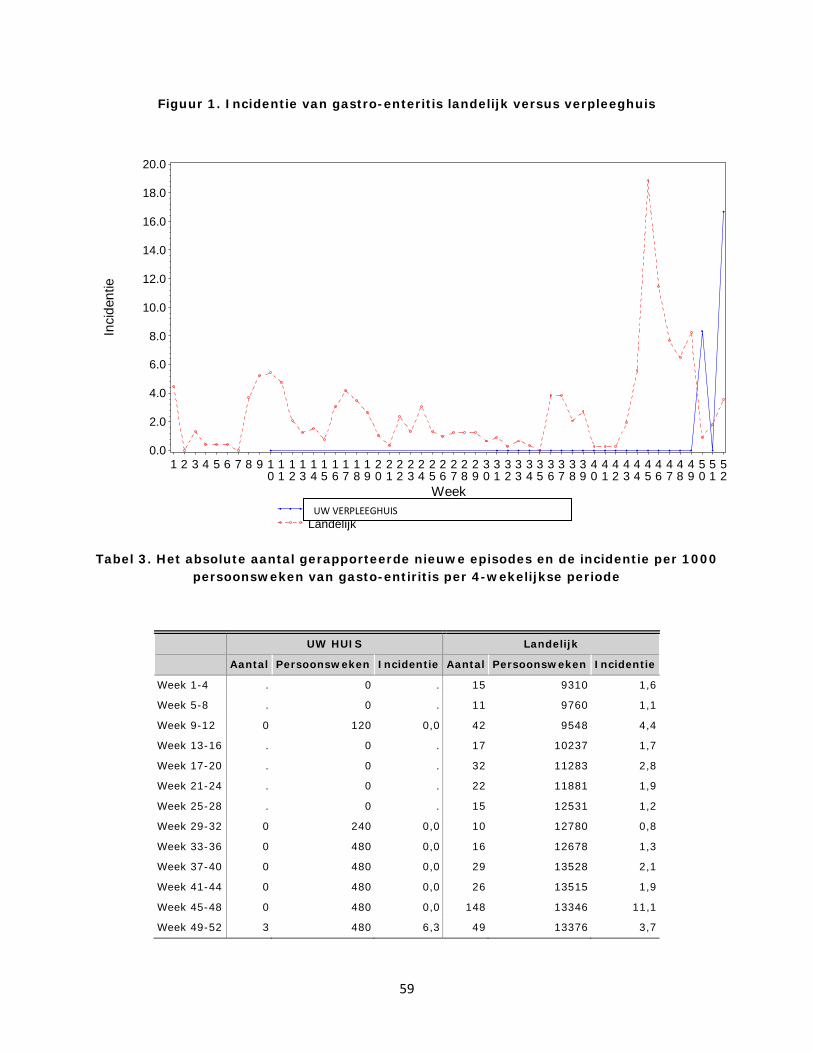
59
Figuur 1. Incidentie van gastro-enteritis landelijk versus verpleeghuis
Tabel 3. Het absolute aantal gerapporteerde nieuwe episodes en de incidentie per 1000 persoonsweken van gasto-entiritis per 4-wekelijkse periode
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Week 1-4 . 0 . 15 9310 1,6
Week 5-8 . 0 . 11 9760 1,1
Week 9-12 0 120 0,0 42 9548 4,4
Week 13-16 . 0 . 17 10237 1,7
Week 17-20 . 0 . 32 11283 2,8
Week 21-24 . 0 . 22 11881 1,9
Week 25-28 . 0 . 15 12531 1,2
Week 29-32 0 240 0,0 10 12780 0,8
Week 33-36 0 480 0,0 16 12678 1,3
Week 37-40 0 480 0,0 29 13528 2,1
Week 41-44 0 480 0,0 26 13515 1,9
Week 45-48 0 480 0,0 148 13346 11,1
Week 49-52 3 480 6,3 49 13376 3,7
Inci
dent
ie
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
Week
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
AMERSFOORT - de Lichtenberg, afd. VerplegingLandelijk
UW VERPLEEGHUIS
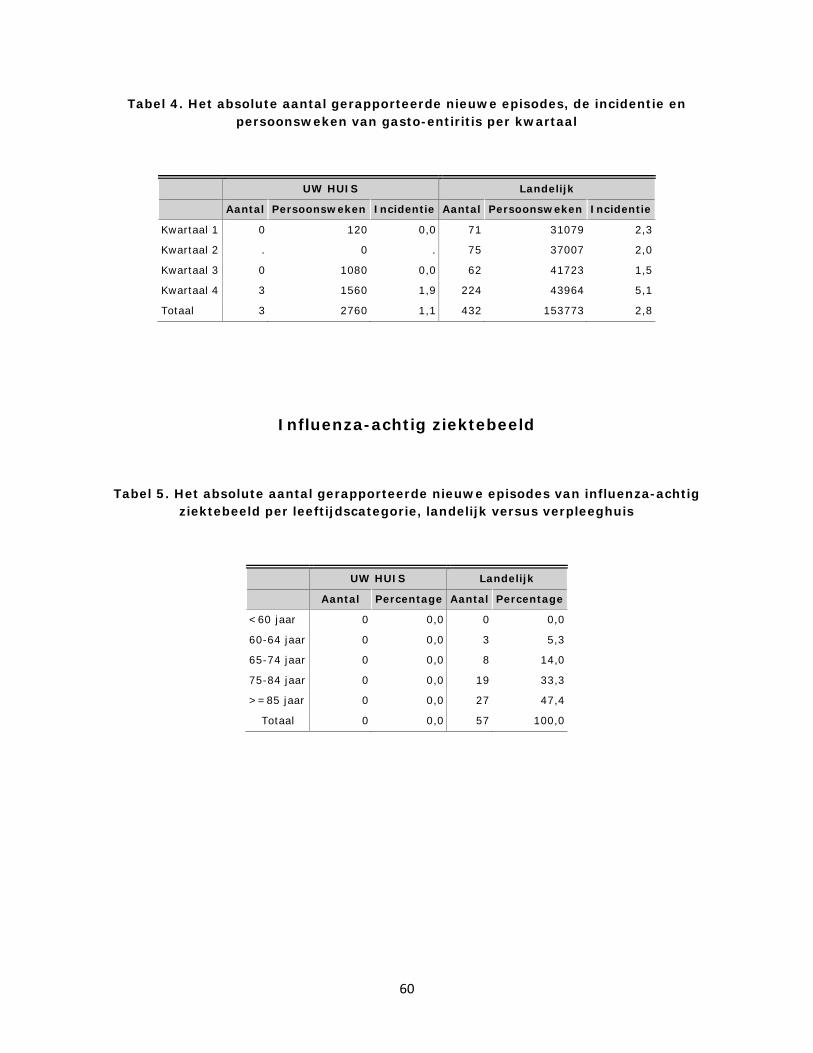
60
Tabel 4. Het absolute aantal gerapporteerde nieuwe episodes, de incidentie en persoonsweken van gasto-entiritis per kwartaal
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Kwartaal 1 0 120 0,0 71 31079 2,3
Kwartaal 2 . 0 . 75 37007 2,0
Kwartaal 3 0 1080 0,0 62 41723 1,5
Kwartaal 4 3 1560 1,9 224 43964 5,1
Totaal 3 2760 1,1 432 153773 2,8
Influenza-achtig ziektebeeld
Tabel 5. Het absolute aantal gerapporteerde nieuwe episodes van influenza-achtig ziektebeeld per leeftijdscategorie, landelijk versus verpleeghuis
UW HUIS Landelijk
Aantal Percentage Aantal Percentage
<60 jaar 0 0,0 0 0,0
60-64 jaar 0 0,0 3 5,3
65-74 jaar 0 0,0 8 14,0
75-84 jaar 0 0,0 19 33,3
>=85 jaar 0 0,0 27 47,4
Totaal 0 0,0 57 100,0

61
Figuur 2. Incidentie van influenza-achtig ziektebeeld landelijk versus verpleeghuis
Tabel 6. Het absolute aantal gerapporteerde nieuwe episodes en de incidentie per 1000 persoonsweken van influenza-achtig ziektebeeld per 4-wekelijkse periode
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Week 1-4 . 0 . 6 9310 0,6
Week 5-8 . 0 . 8 9760 0,8
Week 9-12 0 120 0,0 7 9548 0,7
Week 13-16 . 0 . 1 10237 0,1
Week 17-20 . 0 . 2 11283 0,2
Week 21-24 . 0 . 1 11881 0,1
Week 25-28 . 0 . 1 12531 0,1
Week 29-32 0 240 0,0 1 12780 0,1
Week 33-36 0 480 0,0 2 12678 0,2
Week 37-40 0 480 0,0 1 13528 0,1
Week 41-44 0 480 0,0 1 13515 0,1
Week 45-48 0 480 0,0 9 13346 0,7
Week 49-52 0 480 0,0 17 13376 1,3
Inci
dent
ie
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6
Week
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
AMERSFOORT - de Lichtenberg, afd. VerplegingLandelijk
UW VERPLEEGHUIS

62
Tabel 7. Het absolute aantal gerapporteerde nieuwe episodes, de incidentie en persoonsweken van influenza-achtig ziektebeeld per kwartaal
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Kwartaal 1 0 120 0,0 21 31079 0,7
Kwartaal 2 . 0 . 4 37007 0,1
Kwartaal 3 0 1080 0,0 5 41723 0,1
Kwartaal 4 0 1560 0,0 27 43964 0,6
Totaal 0 2760 0,0 57 153773 0,4
Vermoedelijk pneumonie
Tabel 8. Het absolute aantal gerapporteerde nieuwe episodes van vermoedelijk pneumonie per leeftijdscategorie, landelijk versus verpleeghuis
UW HUIS Landelijk
Aantal Percentage Aantal Percentage
<60 jaar 0 0,0 17 2,9
60-64 jaar 0 0,0 10 1,7
65-74 jaar 1 12,5 69 11,6
75-84 jaar 2 25,0 210 35,4
>=85 jaar 5 62,5 288 48,5
Totaal 8 100,0 594 100,0
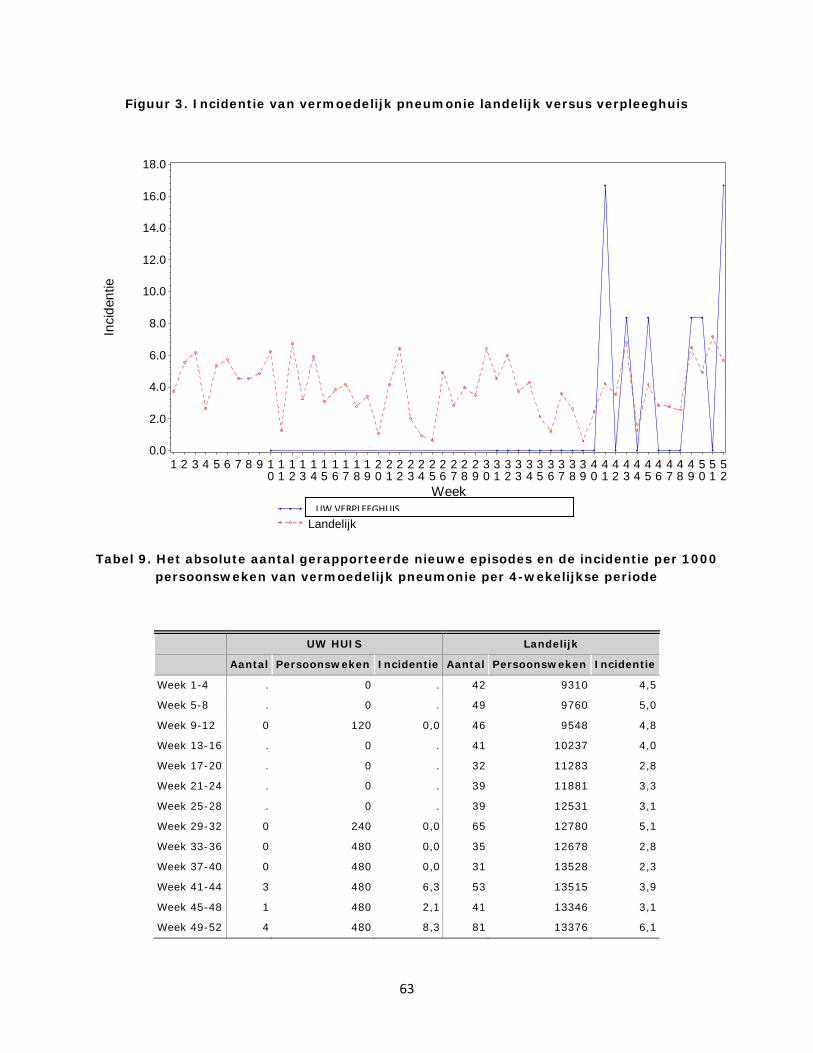
63
Figuur 3. Incidentie van vermoedelijk pneumonie landelijk versus verpleeghuis
Tabel 9. Het absolute aantal gerapporteerde nieuwe episodes en de incidentie per 1000 persoonsweken van vermoedelijk pneumonie per 4-wekelijkse periode
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Week 1-4 . 0 . 42 9310 4,5
Week 5-8 . 0 . 49 9760 5,0
Week 9-12 0 120 0,0 46 9548 4,8
Week 13-16 . 0 . 41 10237 4,0
Week 17-20 . 0 . 32 11283 2,8
Week 21-24 . 0 . 39 11881 3,3
Week 25-28 . 0 . 39 12531 3,1
Week 29-32 0 240 0,0 65 12780 5,1
Week 33-36 0 480 0,0 35 12678 2,8
Week 37-40 0 480 0,0 31 13528 2,3
Week 41-44 3 480 6,3 53 13515 3,9
Week 45-48 1 480 2,1 41 13346 3,1
Week 49-52 4 480 8,3 81 13376 6,1
Inci
dent
ie
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
Week
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
AMERSFOORT - de Lichtenberg, afd. VerplegingLandelijk
UW VERPLEEGHUIS

64
Tabel 10. Het absolute aantal gerapporteerde nieuwe episodes, de incidentie en persoonsweken van vermoedelijk pneumonie per kwartaal
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Kwartaal 1 0 120 0,0 145 31079 4,7
Kwartaal 2 . 0 . 121 37007 3,3
Kwartaal 3 0 1080 0,0 144 41723 3,5
Kwartaal 4 8 1560 5,1 184 43964 4,2
Totaal 8 2760 2,9 594 153773 3,9
Urineweginfectie
Tabel 11. Het absolute aantal gerapporteerde nieuwe episodes van urineweginfectie per leeftijdscategorie, landelijk versus verpleeghuis
UW HUIS Landelijk
Aantal Percentage Aantal Percentage
<60 jaar 0 0,0 48 3,0
60-64 jaar 1 5,6 26 1,6
65-74 jaar 0 0,0 160 10,0
75-84 jaar 5 27,8 569 35,6
>=85 jaar 12 66,7 794 49,7
Totaal 18 100,0 1597 100,0

65
Figuur 4. Incidentie van urineweginfectie landelijk versus verpleeghuis
Tabel 12. Het absolute aantal gerapporteerde nieuwe episodes en de incidentie per 1000 persoonsweken van urineweginfectie per 4-wekelijkse periode
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Week 1-4 . 0 . 88 9310 9,5
Week 5-8 . 0 . 117 9760 12,0
Week 9-12 0 120 0,0 121 9548 12,7
Week 13-16 . 0 . 100 10237 9,8
Week 17-20 . 0 . 99 11283 8,8
Week 21-24 . 0 . 117 11881 9,8
Week 25-28 . 0 . 142 12531 11,3
Week 29-32 0 240 0,0 110 12780 8,6
Week 33-36 4 480 8,3 126 12678 9,9
Week 37-40 4 480 8,3 141 13528 10,4
Week 41-44 5 480 10,4 139 13515 10,3
Week 45-48 1 480 2,1 161 13346 12,1
Week 49-52 4 480 8,3 136 13376 10,2
Inci
dent
ie
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
22.0
24.0
26.0
Week
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
AMERSFOORT - de Lichtenberg, afd. VerplegingLandelijk
UW VERPLEEGHUIS

66
Tabel 13. Het absolute aantal gerapporteerde nieuwe episodes, de incidentie en persoonsweken van urineweginfectie per kwartaal
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Kwartaal 1 0 120 0,0 358 31079 11,5
Kwartaal 2 - 0 - 354 37007 9,6
Kwartaal 3 6 1080 5,6 403 41723 9,7
Kwartaal 4 12 1560 7,7 482 43964 11,0
Totaal 18 2760 6,5 1597 153773 10,4
Mortaliteit
Tabel 14. Het absolute aantal gerapporteerde sterfgevallen per leeftijdscategorie, landelijk versus verpleeghuis
UW HUIS Landelijk
Aantal Percentage Aantal Percentage
<60 jaar 0 0,0 14 1,6
60-64 jaar 0 0,0 17 1,9
65-74 jaar 0 0,0 84 9,5
75-84 jaar 3 33,3 247 28,1
>=85 jaar 6 66,7 518 58,9
Totaal 9 100,0 880 100,0

67
Figuur 5. Incidentie van mortaliteit landelijk versus verpleeghuis
Tabel 15. Het absolute aantal gerapporteerde nieuwe episodes en de incidentie per 1000 persoonsweken van mortaliteit per 4-wekelijkse periode
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Week 1-4 . 0 . 68 9310 7,3
Week 5-8 . 0 . 74 9760 7,6
Week 9-12 0 120 0,0 56 9548 5,9
Week 13-16 . 0 . 56 10237 5,5
Week 17-20 . 0 . 64 11283 5,7
Week 21-24 . 0 . 64 11881 5,4
Week 25-28 . 0 . 59 12531 4,7
Week 29-32 2 240 8,3 65 12780 5,1
Week 33-36 3 480 6,3 71 12678 5,6
Week 37-40 1 480 2,1 75 13528 5,5
Week 41-44 1 480 2,1 69 13515 5,1
Week 45-48 2 480 4,2 76 13346 5,7
Week 49-52 0 480 0,0 83 13376 6,2
Inci
dent
ie
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
Week
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
AMERSFOORT - de Lichtenberg, afd. VerplegingLandelijk
UW VERPLEEGHUIS

68
Tabel 16. Het absolute aantal gerapporteerde sterfgevallen, persoonsweken en de incidentie van mortaliteit per kwartaal
UW HUIS Landelijk
Aantal Persoonsweken Incidentie Aantal Persoonsweken Incidentie
Kwartaal 1 0 120 0,0 207 31079 6,7
Kwartaal 2 . 0 . 200 37007 5,4
Kwartaal 3 6 1080 5,6 221 41723 5,3
Kwartaal 4 3 1560 1,9 252 43964 5,7
Totaal 9 2760 3,3 880 153773 5,7

69
Appendix 6 - Example invitation mail (in Dutch) Geachte mevrouw (name),
Naar aanleiding van uw functie als specialist ouderengeneeskunde bij (organisation) benader ik u. Via deze mail wil ik u graag uitnodigen voor een interview over uw ervaring en mening over het registreren van infectieziekten in verpleeghuizen.
Het RIVM-Centrum Infectieziektebestrijding heeft een Surveillance Netwerk voor Infectieziekten in Verpleeghuizen (SNIV) opgezet waarin verpleeghuizen wekelijks het aantal Gastro-enteritis, lage luchtweginfectie, influenza-achtig ziektebeeld en urineweginfecties op de afdeling registeren. Om het netwerk beter aan te laten sluiten op de praktijk zijn wij erg benieuwd naar uw ervaring en mening omtrent infectie registratie.
Het interview zal tussen 25-40 minuten duren en zal plaatsvinden op een voor u geschikte locatie, tijd en datum (in december of januari). De informatie uit het interview zal strikt vertrouwelijk worden behandeld en zal niet aan derden worden verstrekt of openbaar gemaakt.
Gaarne zie ik uw reactie per mail of telefonisch tegemoet. En mocht u nog verdere vragen hebben over SNIV, het interview of andere zaken dan kunt mij altijd via de mail of telefonisch bereiken. In de bijlage vindt u de brochure met meer informatie over SNIV.
Met vriendelijke groet,
Lara Hartog
Stagiaire RIVM- Centrum Infectieziektebestrijding 030-2743050 / 06-48451176 [email protected]
70
Appendix 7- Information leaflet (in Dutch)
Betreft: Uitnodiging focusgroep ‘Ervaringen SNIV’
Deel uw mening over en ervaringen met SNIV, met andere deelnemers en kom gezamenlijk tot ideeën voor verbetering.
16 januari 2018, Bilthoven
Beste SNIV deelnemer,
Sinds 2009 heeft het RIVM- Centrum voor infectiebestrijding het SNIV netwerk opgezet, met als doel beter inzicht krijgen in het voorkomen van infecties en antibioticumgebruik in verpleeghuizen en handvatten bieden voor specifieke infectiepreventie verbetermaatregelen. Om SNIV beter aan te laten sluiten bij de praktijk, is door het SNIV team een onderzoek in de vorm van focusgroepen opgezet.
De focusgroep Tijdens de focusgroep gaan ongeveer 6 deelnemers van SNIV met elkaar in gesprek over de positieve punten en knelpunten van de huidige SNIV surveillance en proberen we tot mogelijke oplossingen te komen. De focusgroep zal maximaal 2 uur duren. De informatie uit de focusgroep zal strikt vertrouwelijk worden behandeld en zal niet aan derden worden verstrekt of openbaar gemaakt. De focusgroep zal van 14.00-16.00 op vrijdag 9 februari plaatsvinden in het Business Centre Nederland (BCN), locatie Utrecht Centraal, gevestigd op de Catharijnesingel 48. Uw reiskosten zullen worden vergoed en na afloop van de bijeenkomst ontvangt u een kleine attentie in de vorm van een VVV bon.
Deelnemen Mocht u geïnteresseerd zijn in deelname, dan nodigen wij u graag uit om u uiterlijk woensdag 31 januari op te geven via de mail. Mocht u niet op vrijdag 9 februari beschikbaar zijn, maar wel geïnteresseerd zijn in deelname, dan horen wij dat ook graag. Wij kunnen dan samen kijken naar mogelijke andere oplossingen.
Praktische informatie Locatie: Business Centre Nederland (BCN), locatie Utrecht Centraal, Catharijnesingel 48. Datum: Vrijdag 9 februari
71
Tijd: 14.00-16.00 Reiskosten: Vergoed door het RIVM (parkeerkosten worden niet vergoed) Deelnemen: Mailen naar [email protected] uiterlijk woensdag 31 januari
Mocht u nadere toelichting wensen, dan zijn wij uiteraard daarvoor beschikbaar via Lara Hartog: 030-2743050 / 06-48451176 of mailen naar [email protected]
Wij hopen u te mogen verwelkomen op vrijdag 9 februari danken u alvast hartelijk voor uw moeite!
Met vriendelijke groet,
Lara Hartog

72
Appendix 8 - Interview guide (in Dutch) Introductie
• Voorstellen o Naam, studie, werk,
• Onderzoek en doel van het interview o Evalueren en verbeteren SNIV/ infectie registratie systeem o [Eventueel SNIV toelichten] o Incidentie meting o Doel interview is ervaringen en meningen in kaart brengen o Daarna focus groepen o Definitie infectie registratie
Bijhouden kan op allerlei manieren; papier, Excel, online, nationaal. • Werkwijze/aanpak interview
o 30-40 minuten o Anonimiteit o Vragen stellen, maar andere gerelateerde onderwerpen kunnen ook besproken worden o Eerlijkheid, geen goed of fout antwoord, verduidelijking vragen als dat nodig is o Opnemen, uit typen, o Stopzetten opname bij telefoontje o Wilt een transcript of samenvatting ontvangen? o Wilt u de resultaten ontvangen?
• Heeft u tot nu toe vragen? • Toestemmingsformulier tekenen
Interview [Opname aanzetten]
Introductievragen
1. Kunt u mij iets over uw functie als specialist ouderengeneeskunde vertellen/ Hoe zit een gemiddelde dag/week eruit
2. Waar bent u werkzaam? 3. Hoelang bent u al op deze locatie werkzaam?
Infectieregistratie
Dank u wel dit helpt mij om alles een beetje in context te plaatsen.
4. Kunt u mij in het kort vertellen wat er op deze locaties aan infectie preventie wordt gedaan? 5. En aan infectie registratie?

73
ALS ER WEL AAN REGISTRATIE WORDT GEDAAN Collectie Dank u wel. Ik zou u nu graag iets meer willen vragen over de manier waarop de informatie verzameld wordt.
6. Kunt u mij kort vertellen hoe de infectie registratie er op uw locatie aan toe gaat? Denk aan • wie verzamelen, • hoe verzamelen • wie en hoe registreren • wie en hoe controleren
7. Wat vindt u van deze manier (is het handig)?
Denk aan: • de duur van registratie, • begrijpbaarheid van richtlijnen, • haalbaarheid ( definities, tijd in praktijk), • betrouwbaarheid (kloppen de gegevens, zijn ze anoniem, zijn ze veilig/kan niemand anders
erbij), • nut ( heeft u iets aan deze manier van registreren)
8. Wat waren de redenen om te beginnen met infectie registratie/ SNIV?
a. Zijn er nog andere redenen behalve…. 9. Bent u bekend met SNIV? 10. Hoe is het toen gelopen? Wat vond u van de presentatie? 11. Als niet-deelnemers een eigen registratie hebben: Wat was de reden om het op deze wijze te
doen en niet met SNIV? a. Zijn er nog andere redenen behalve…. b. Wat is de reden dat niemand anders het heeft opgepakt?
12. Wanneer zou u overwegen om deel te nemen aan SNIV? 13. Wie is volgens u de meest geschikte persoon voor het uitvoeren? 14. Wat zou u helpen om het handiger/sneller/betrouwbaarder te doen? 15. Als u iets kon veranderen aan de manier waarop infecties worden geregistreerd, wat zou dat
zijn? 16. Hoe zou u dit haalbaar maken voor uzelf? 17. Als dit bij SNIV zou zijn, zou u dan overstappen op SNIV?

74
Analyse/interpretatie
U gaf net aan dat u [korte samenvatting van hoe registratie ging] doet u daarna nog iets met de gegevens? Bij ja:
18. Wat deed u daar mee? 19. Waarom deed u dat ermee? 20. Wat zou u er nog meer mee willen doen? 21. Wat vindt u hiervan?
Denk aan: • begrijpbaarheid gegevens en systeem, • haalbaarheid, • betrouwbaarheid (kloppen de gegevens, zijn ze anoniem, zijn ze veilig/kan niemand
anders erbij), • nut
Bij nee:
22. Waarom gebruikte u de gegeven nergens voor? 23. Wanneer zou u dit wel doen?
Spelen factoren als een rol: • begrijpbaarheid gegevens en systeem, • haalbaarheid, • betrouwbaarheid (kloppen de gegevens, zijn ze anoniem, zijn ze veilig/kan niemand
anders erbij), • nut
Disseminatie Dank u wel, ik zou het nu graag willen hebben over de disseminatie van die gegevens en over het delen ervan.
24. Deelt u de resultaten/gegevens wel eens met iemand? 25. Met wie en wat vinden zij daarvan? 26. Waarom wel/ niet? 27. Wanneer zou u de resultaten wel willen delen? 28. Wat is er nodig om daar voor te zorgen?
U gaf net aan dat u ….. nodig heeft om de resultaten met anderen te delen, als u nu helemaal vrij was om het ideale infectie registratie systeem zou mogen ontwikkelen hoe zou die eruit zien?
Dank u wel, dan wil ik als laatste onderwerp SNIV aankaarten.

75
29. Bij SNIV ontvangt u jaarlijks een terugrapportage, zou dit een overweging zijn om deel te nemen?
30. Hoe zou die terugrapportage er uit moeten zien?
Dank u wel voor uw inzichten over SNIV, Zijn er wat u betreft nog belangrijke dingen die meespelen als het gaat om infectie registratie?
31. Zijn er nog dingen/onderwerpen/aspecten waar u iets over kwijt wil, wilt toevoegen?
Oke, dan kort samen gevat, klopt het dat (samenvatting geven)? En (samenvatting) ziet u de infectie registratie het liefst? Dan wil ik u graag bedanken voor deelname
ALS ER NIET AAN REGISTRATIE WORDT GEDAAN
Infectie registratie
1. Zijn er specifieke redenen waarom dit niet wordt gedaan? 2. Welke?
a. Zijn er nog andere redenen behalve…. b. Wat is de reden dat niemand anders het heeft opgepakt?
3. Bent u bekend met SNIV? 4. Wat waren de redenen om niet deel te nemen?
a. Zijn er nog andere redenen behalve…. b. Wat is de reden dat niemand anders het heeft opgepakt? c. Wat vond u van de presentatie van het RIVM?
5. Hoe zou SNIV aangepast kunnen worden om deze redenen aan te pakken? 6. Wat zou een reden zijn om aan SNIV deel te nemen? 7. Wie zou volgens u het initiatief hierin moeten nemen?
Denk aan factoren als:
• Sturing vanuit het bestuur, • vanuit de landelijke of Europese overheid, • houdingen, • kennis, • bewustzijn van het belang van infectie registratie henzelf en bij collega’s, • verwachtingen van de uitkomst, • nut voor bewoners/verbetering van kwaliteit. • Financiële of niet financiële middelen voor deelnemen.
Als de houding van collega’s (zowel SOs als verpleegkundige) niet aan bod is gekomen:
8. Wat is over het algemeen mening op de locaties over infectie registratie? 9. Deelt u deze mening?

76
Collectie
Dank u wel. U gaf net aan dat u niet aan infectie registratie deed om [geef redenen]. Ik zou het nu graag over mogelijke manier van registreren willen hebben.
10. Hoe zou je in een ideale situatie aan de informatie willen komen? 11. Hoe registreren? 12. Als dit bij SNIV zo zou gebeuren zou u dan deelnemen? 13. Hoe zou je dit kunnen bereiken/haalbaarheid? 14. Wie is volgens u de meest geschikte persoon om de registratie te doen?
Analyse/interpretatie
Dank u wel, ik zou het nu graag willen hebben over het gebruik van registratie gegevens.
15. Wat voor informatie zou u willen? 16. Wat zou u hiermee willen doen? 17. Hoe zou u dit kunnen bereiken? 18. Als dit bij SNIV zo zou gebeuren zou u dan deelnemen? 19. Wie zou dit moeten doen? 20. Wanneer of wat voor gegevens zouden nuttig zijn?
Disseminatie
21. Zou de gegevens met iemand willen delen? 22. Waarom? 23. Hoe zou u in een ideale situatie data willen ontvangen en verspreiden?
Dank u wel, dan wil ik als laatste onderwerp SNIV aankaarten.
24. Bij SNIV ontvangt u jaarlijks een terugrapportage, zou dit een overweging zijn om deel te nemen?
25. Hoe zou die terugrapportage er uit moeten zien?
Dank u wel voor uw inzichten over SNIV, Zijn er wat u betreft nog belangrijke dingen die meespelen als het gaat om infectie registratie?
26. Zijn er nog dingen/onderwerpen/aspecten waar u iets over kwijt wil, wilt toevoegen?
Oke, dan even kort samen gevat, klopt het dat (samenvatting geven)? En (samenvatting) ziet u de infectie registratie het liefst? Dan wil ik u graag bedanken voor deelname
77
Appendix 9 - Consent form (in Dutch)
Toestemmingsverklaring
Deelname interview over ervaringen met en meningen over infectie registratie en SNIV
In te vullen door de deelnemer
Ik verklaar op een voor mij duidelijke wijze te zijn ingelicht over de aard, methode en doel van het onderzoek. Ik weet dat de resultaten uitsluitend voor analyse, wetenschappelijke publicaties en presentaties zullen worden gebruikt. Ik heb genoeg tijd gehad om te beslissen of ik mee zou doen en mijn vragen zijn naar tevredenheid beantwoord.
Ik weet dat deelname vrijwillig is. Ik weet dat ik op ieder moment kan beslissen om toch niet mee te doen. Daarvoor hoef ik geen reden te geven.
Ik geef toestemming voor geluidsopname tijdens het interview. Ik weet dat de geluidsopname wordt uitgewerkt en gecodeerd om de ervaringen en meningen rondom infectie registratie geheel anoniem en vertrouwelijk in kaart te brengen.
Naam deelnemer: ………………………………………………………………………….. Plaats en datum: …………………………………………………….. Handtekening deelnemer: ………...……..................
In te vullen door de uitvoerende onderzoeker
Ik heb een mondelinge en schriftelijke toelichting gegeven op het onderzoek. Ik zal resterende vragen over het onderzoek naar vermogen beantwoorden. De deelnemer zal van een eventuele voortijdige beëindiging van deelname aan dit onderzoek geen nadelige gevolgen ondervinden.
Naam onderzoeker: ………………………………………………………………………….. Plaats en datum: …………………………………………………….. Handtekening onderzoeker: ………...……...............

78
Appendix 10 – Focus group discussion guide (in Dutch) 1. Introductie (10 min) Doel: Uitleg geven over de focusgroep, de gang van zaken, afspraken, eventuele vragen beantwoorden en de toestemmingsformulieren ondertekenen.
• Voorstellen o Lara
Moderator Vragen stellen, niet actief deelnemen aan de discussie
o Anja Observant
• Opbouw onderzoek en doel focusgroep o SNIV en mogelijke verbeteringen inventariseren en evalueren o Interviews gehouden
Verschillende onderwerpen o Doel focus groep:
Positieve en negatieve aspecten SNIV tav 2/3 thema’s • De terugrapportages • Manier van registreren bij SNIV
Mogelijke oplossingen tov de negatieve aspecten Mogelijke manieren om positieve aspecten beter te benutten Uitlichten aantal oplossingen -> afhankelijk van de tijd Mening is waardevol voor SNIV en zal als input voor vervolg stap gebruikt, geen
garantie voor uiteindelijk wijzigingen • Werkwijze
o Agenda bespreken (2 uur met pauze) o Hapjes en drankjes pakken o Anonimiteit en privacy. o Eerlijkheid, geen goed of fout antwoord, verduidelijking vragen als dat nodig is o Het eens zijn of worden met elkaar is niet het doel, voornamelijk om jullie meningen en
ideeën in kaart te brengen, uitwisselen van elkaars werkwijze is voor na de FG. o Telefoon op stil-> ruimte verlaten bij telefoontjes o Opnemen, uit typen
• Zijn er tot nu toe vragen? • Toestemmingsformulier tekenen

79
2. Voorstel rondje (5 min) Doel: elkaar leren kennen en een vetrouwende omgeving creëren waarin iedereen zich vrij voelt om zijn mening te delen.
• Vertel allemaal kort: o Wie je bent, waar je werkt, hoelang je daar werkt en hoelang jullie al meedoen aan SNIV
• Naam op naambordjes schrijven
3. Thema 1: De terugrapportages (45 min) 3. a. Positieve en negatieve aspecten identificeren (15 min)
Doel: de belangrijkste positieve en negatieve aspecten van de terugrapportages identificeren. Evalueren of de gevonden aspecten van de interviews hier ook als belangrijk worden ervaren.
Vraag: Als deelnemer van SNIV ontvang je 1 keer per jaar een terugrapportage, met de cijfers van het afgelopen jaar ten opzichte van het jaarlijkse gemiddelde. Mijn vraag is: wat vinden jullie van de terugrapportages? Zouden jullie 3 positieve punten op kunnen schrijven en 3 negatieve.
o Op groene post-it’s de positieve, op roze de negatieve en schrijf elk punt op een aparte post-it
o Houd de post-it’s nog even voor jezelf, we zullen ze hierna bespreken o Kan nog meer of minder worden als het moeizaam gaat o Hier hebben jullie 3 minuten voor
• Met zn alle bespreken, vergelijken, erachter komen waarom dit de belangrijkste punten zijn. De post-it’s op een grote flipover plakken.
o Voorbeeldvragen: Zou ik u mogen uitnodigen om 1 van de positieve aspecten te delen en toe te
lichten? Had iemand anders ook zo iets opgeschreven? Wat bedoelde u daarmee? Kunt u mij uitleggen in welke situatie dat geldt? Wat vindt de rest van dit punt? Wat is de reden dat u dit punt zelf niet had opgeschreven? Met welke reden had u dat opgeschreven? Heeft iemand een punt wat hieraan gerelateerd is? Heeft iemand een nieuw positief punt? Zou u één van de negatieve punten kunnen toelichten?
• Alle post-it’s op geplakt en besproken? • Zijn er nog punten die hier niet bij staan?-> Ja want je vroeg alleen om de belangrijkste
o Waarom golden die punten niet als belangrijkste? o Als je nu nog de memo’s zou mogen wisselen, zou je dat willen?
• Kijken welke punten wij zelf nog hadden en testen wat zij ervan vinden en evt erbij plakken, als ze het niet relevant vinden niet erbij plakken.
80
o Uit de interviews kwam punt X ook naar voren, wat vinden jullie daarvan? • Bedanken voor de input, we zullen nu verder gaan met het bedenken van mogelijke oplossingen
voor elk van deze aspecten
3.b. Mogelijke oplossingen identificeren (15 min) Doel: zo veel mogelijk oplossingen identificeren en kort toelichten. Evalueren of de genoemde oplossingen in interviews en tijdens symposia aansluiten
• Bedenk voor elk aspect minimaal 1 oplossing -> dit op een andere kleur memo schrijven dat mag zo gek zijn als je wilt. Mag ook meerdere oplossingen per aspect
a. geef een out of the box voorbeeld om te helpen b. Jullie hebben hier 3 minuten voor
• Mogelijke manieren om te helpen met brainstormen als het niet lukt: a. Bekijk het vanaf de andere kant: Vraag je af wat het probleem veroorzaakt, waar komt
het door? Hoe maak je het probleem groter? b. Bekijk het probleem door de lens van het SNIV team, een huis dat nog niet deelneemt,
iemand die fel tegen registratie is, het medisch secretariaat. c. Hoe zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/1 van de genoemde
aspecten kunnen vervangen? d. Met wat zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/ 1 van de
genoemde aspecten kunnen combineren? e. Hoe zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/ 1 van de genoemde
aspecten kunnen aanpassen om aan een ander doel te helpen? f. Lijkt het op iets anders waar je van kunt leren? Bv val incidenten meten, BRMO’s etc g. Zou je het in een andere context kunnen gebruiken? h. Zou je iets kunnen toevoegen/weghalen? i. Zou je de nadruk ergens anders op kunnen leggen? j. Wat zou je geholpen hebben om aspect x wel te doen/minder negatief te ervaren/te
voorkomen? k. Hoe kan je aspect x vaker benutten/ duidelijker maken?
• Dan deze oplossingen met zn alle bespreken en toelichten 10 minuten • Voorbeeld vragen zijn:
a. Kunt u uitleggen wat u hiermee bedoelt b. Hoe zou dit er in de dagelijkse praktijk uitzien c. Wie zou dit uit voeren? d. Hoe draagt deze oplossing bij aan aspect x e. Hoe bedoelt u ….
• Tijdens de interviews werden de volgende oplossingen ook genoemd: lijst gebruiken, wat is jullie mening daarover?
• Nu we zo alle oplossingen aan het bespreken zijn, komen er dan nieuwe ideeën op die je nog zou willen opschrijven?

81
3.c. Selecteren (5 min) Doel: de meeste interessante oplossingen kiezen om vervolgens in meer detail te bespreken. Erachter komen hoe ze die oplossingen voor zich zien.
• Ik zou nu graag een aantal oplossingen in iets meer detail bespreken, daarom wil ik jullie vragen om voor je zelf een top 5 te maken van oplossingen die je voor jou het meest effectief zullen zijn, of waarvan jij het liefst hebt dat het SNIV team hier mee aan de slag ging.
• Geef 5 punten aan welke je het belangrijkst vindt, 4 aan die erna, 3 daarna, enzovoorts. • Tel de punten op en begin met bespreken van de hoogst scorende • Afhankelijk van het aantal bedachte oplossingen, als het er maar weinig zijn, kan je ook laten
kiezen welke ze willen bespreken en alles bespreken.
3.d. In meer detail bespreken (10 min) Doel: een duidelijkere uitleg van de hoogst scorende oplossingen, hoeft niet helemaal concreet of een ondervraging over of het haalbaar is of niet, vooral het in kaart brengen van hun mening en voorkeur van hoe ze de oplossing het liefst zouden zien.
• Ik zou graag met oplossing x willen beginnen, wat maakt deze oplossing belangrijk? • Overige probe vragen:
o Hoe zou dit er idealiter uit zien? o Wie zou het moeten uitvoeren, waar, waarom, wanneer, hoe vaak? o Hoe is dat anders dan bijvoorbeeld oplossing x o Wat is de reden dat deze zo hoog/laag scoort? o Als het SNIV team oplossing x wil toepassen, welke stap zouden ze dan als eerste
moeten zetten? En daarna? Waar moeten ze aan denken? • Aantal te bespreken oplossingen is afhankelijk van de tijd
4. Pauze (10 min)
5. Thema 2 Manier van registreren (40) 5. a. Positieve en negatieve aspecten identificeren (10 min) Doel: de belangrijkste positieve en negatieve aspecten van de manier van registreren bij SNIV identificeren. Evalueren of de gevonden aspecten van de interviews hier ook als belangrijk worden ervaren.
• Ik wil het nu graag hebben over een ander thema van SNIV en dat is het registreren van de infecties zelf. Ieder verpleeghuis heeft dat natuurlijk op zijn eigen wijze georganiseerd, maar als we het straks over de registratie gaan hebben, dan wil ik even uitleggen wat wij daaronder verstaan:
o Herkennen als infectie voor SNIV (niet de diagnose zelf) o Bijhouden/doorgeven van de infectie o Alle infecties van de afgelopen week van alle afdelingen combineren tot 1 geheel

82
o Invoeren in OSIRIS • Vraag: Ik zou jullie willen vragen om terug te denken aan een week waarin het registreren voor
SNIV heel soepel verliep. En ik zou jullie willen vragen om 3 redenen op te schrijven waarom dit soepel verliep.
o Op groene post-it’s de positieve en schrijf elk punt op een aparte post-it o Houd de post-it’s nog even voor jezelf, we zullen ze hierna bespreken
• Nu zou ik jullie willen vragen om terug te denken aan week waarin het redelijk moeizaam verliep, en drie redenen waarom dit moeizaam verliep.
o op oranje de negatieve o Kan nog meer of minder worden als het moeizaam gaat o Hier hebben jullie 3 minuten voor
• Met zn alle bespreken, vergelijken, erachter komen waarom dit de belangrijkste punten zijn. De post-it’s op een grote flipover plakken.
o Voorbeeldvragen: Zou ik u mogen uitnodigen om 1 van de positieve aspecten te delen en toe te
lichten? Had iemand anders ook zo iets opgeschreven? Wat bedoelde u daarmee? Kunt u mij uitleggen in welke situatie dat geldt? Wat vindt de rest van dit punt? Wat is de reden dat u dit punt zelf niet had opgeschreven? Met welke reden had u dat opgeschreven? Heeft iemand een punt wat hieraan gerelateerd is? Heeft iemand een nieuw positief punt? Zou u één van de negatieve punten kunnen toelichten?
• Alle post-it’s op geplakt en besproken? • Zijn er nog punten die hier niet bij staan?-> Ja want je vroeg alleen om de belangrijkste
o Waarom golden die punten niet als belangrijkste? o Als je nu nog de memo’s zou mogen wisselen, zou je dat willen?
• Kijken welke punten wij zelf nog hadden en testen wat zij ervan vinden en evt erbij plakken, als ze het niet relevant vinden niet erbij plakken.
o Uit de interviews kwam punt X ook naar voren, wat vinden jullie daarvan? • Bedanken voor de input, we zullen nu verder gaan met het bedenken van mogelijke oplossingen
voor elk van deze aspecten
5.b. Mogelijke oplossingen identificeren (15 min) Doel: zo veel mogelijk oplossingen identificeren en kort toelichten. Evalueren of de genoemde oplossingen in interviews en tijdens symposia aansluiten
• Bedenk voor elk aspect minimaal 1 oplossing -> dit op een andere kleur memo schrijven dat mag zo gek zijn als je wilt. Mag ook meerdere oplossingen per aspect
a. geef een out of the box voorbeeld om te helpen
83
b. Jullie hebben hier 3 minuten voor • Mogelijke manieren om te helpen met brainstormen als het niet lukt:
a. Bekijk het vanaf de andere kant: Vraag je af wat het probleem veroorzaakt, waar komt het door? Hoe maak je het probleem groter?
b. Bekijk het probleem door de lens van het SNIV team, een huis dat nog niet deelneemt, iemand die fel tegen registratie is, het medisch secretariaat.
c. Hoe zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/1 van de genoemde aspecten kunnen vervangen?
d. Met wat zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/ 1 van de genoemde aspecten kunnen combineren?
e. Hoe zou je SNIV/turven/OSIRIS/diagnose stellen/terugrapportages/ 1 van de genoemde aspecten kunnen aanpassen om aan een ander doel te helpen?
f. Lijkt het op iets anders waar je van kunt leren? Bv val incidenten meten, BRMO’s etc g. Zou je het in een andere context kunnen gebruiken? h. Zou je iets kunnen toevoegen/weghalen? i. Zou je de nadruk ergens anders op kunnen leggen? j. Wat zou je geholpen hebben om aspect x wel te doen/minder negatief te ervaren/te
voorkomen? k. Hoe kan je aspect x vaker benutten/ duidelijker maken?
• Dan deze oplossingen met zn alle bespreken en toelichten 10 minuten • Voorbeeld vragen zijn:
a. Kunt u uitleggen wat u hiermee bedoelt b. Hoe zou dit er in de dagelijkse praktijk uitzien c. Wie zou dit uit voeren? d. Hoe draagt deze oplossing bij aan aspect x e. Hoe bedoelt u ….
• Tijdens de interviews werden de volgende oplossingen ook genoemd: lijst gebruiken, wat is jullie mening daarover?
• Nu we zo alle oplossingen aan het bespreken zijn, komen er dan nieuwe ideeën op die je nog zou willen opschrijven?
5.c. Selecteren (5 min) Doel: de meeste interessante oplossingen kiezen om vervolgens in meer detail te bespreken. Erachter komen hoe ze die oplossingen voor zich zien.
• Ik zou nu graag een aantal oplossingen in iets meer detail bespreken, daarom wil ik jullie vragen om voor je zelf een top 5 te maken van oplossingen die je voor jou het meest effectief zullen zijn, of waarvan jij het liefst hebt dat het SNIV team hier mee aan de slag ging.
• Geef 5 punten aan welke je het belangrijkst vindt, 4 aan die erna, 3 daarna, enzovoorts. • Tel de punten op en begin met bespreken van de hoogst scorende • Afhankelijk van het aantal bedachte oplossingen, als het er maar weinig zijn, kan je ook laten
kiezen welke ze willen bespreken en alles bespreken.

84
5.d. In meer detail bespreken (10 min) Doel: een duidelijkere uitleg van de hoogst scorende oplossingen, hoeft niet helemaal concreet of een ondervraging over of het haalbaar is of niet, vooral het in kaart brengen van hun mening en voorkeur van hoe ze de oplossing het liefst zouden zien.
• Ik zou graag met oplossing x willen beginnen, wat maakt deze oplossing belangrijk? • Overige probe vragen:
o Hoe zou dit er idealiter uit zien? o Wie zou het moeten uitvoeren, waar, waarom, wanneer, hoe vaak? o Hoe is dat anders dan bijvoorbeeld oplossing x o Wat is de reden dat deze zo hoog/laag scoort? o Als het SNIV team oplossing x wil toepassen, welke stap zouden ze dan als eerste
moeten zetten? En daarna? Waar moeten ze aan denken? • Aantal te bespreken oplossingen is afhankelijk van de tijd
6. Extra vragen/oplossingen (5 min) Doel: mogelijke aspecten of oplossingen bespreken die door de door ons gekozen thema’s of opzet niet aan bod zijn gekomen, maar die de deelnemers wel graag willen bespreken.
• Hebben jullie nog mogelijke ideeën voor SNIV, die nog niet aan bod zijn geweest, of die niet per see bij 1 van deze punten aansluit, maar wel interessant is? Meer memo’s geven
• Dan overige oplossing uit de interviews aankaarten en vragen wat hun mening daarover is, als ze niet positief worden ontvangen, niet opplakken, anders wel.
7. Afsluiten (5 min) Doel: de focus groep met een tevreden gevoel afsluiten, en eventuele vragen toelichten
• Korte samenvatting geven • Zijn er nog vragen of aanvullingen? • Bedanken voor deelname, vervolg proces uitleggen • Bedankjes geven en reiskosten formulieren etc regelen

85
Appendix 11 - Codebook interviews ( in Dutch) Belemmerende factoren deelname Sub categorieën Betekenis Voorbeeld
1. Werving RIVM A. Presentatie B. Mail
De vorm en/of inhoud van de weving vanuit het RIVM zorgde ervoor dat mensen niet deelnamen of was niet overtuigend
• presentatie verzorgd door het RIVM droeg bij aan het niet deelnemen
• De wervingsmail was niet goed
• die een presentatie verzorgt. Ja, dat was bedroevend, dat vond ik echt heel bedroevend.
• Maar daar staat dan niet in wat dat dan precies in wat dat dan inhoudt. Dan moet je weer naar de website. Zo een mailtje,
2. Houding Gebrek aan motivatie en/of een negatieve houding tegenover infectieregistratie
maar ja we waren al niet enthousiast Ik denk dat mensen het niet belangrijk vinden
3. Collega’s Gebrek aan steun van collega’s om infecties te registreren/ deel te nemen/collega’s hebben een negatieve houding t.o.v. registratie.
maar ik heb natuurlijk wel support nodig van mijn collega's
4. Tijd Gebrek tijd en/of registreren kost (te) veel tijd het kost gewoon tijd extra. 5. Geen advies van organen Het gebrek aan advies vanuit externe organen (bv Verenso)
is een reden om niet deel te nemen Maar, heb ik niet via Verenso of anderszins gelezen, dat de SNIV ons eh, ons voorthelpt.
6. Administratie
A. OSIRIS
B. Extra werk C. Ondersteuning
De administratie die bij SNIV komt kijken wordt als een belemmerende factor gezien (algemene opmerkingen)
• Specifiek het registreren in OSIRIS is de belemmerende factor
• SNIV wordt gezien als extra werk bovenop alle registratie taken
• Specifiek het gebrek aan administratieve ondersteuning is de belemmerende factor
Weet je de intentie was er wel, maar van goh wie gaat dat nou bijhouden dan.
• nee maar dat was ook het grootste punt, dat je je data moet wegschrijven naar de website van het RIVM,
• Dan blijft het bij je eigen administratie, dus dat eh was • ja als het bij wijze van spreken iemand die je
administratief ondersteund, maar die hadden we niet,
7. Meerwaarde
A. SO’s
B. Dagelijkse praktijk
C. Organisatie
Deelnemer benoemt dat het registreren van infecties geen meerwaarde heeft (ten opzichte van de tijd dat het kost) of er is twijfel over de meerwaarde (niet gespecificeerd voor wie of wat de meerwaarde is).
• Het heeft voor de SO’s geen meerwaarde
• Het heeft voor de dagelijkse praktijk of bewoners geen meerwaarde
De vraag van levert het ons dan ook wat op, kregen we geen bevredigende antwoorden op. En dat was ook uiteindelijk waarom iedereen dacht ja hier gaan we dus niet mee verder.
• Zeker artsen moet je daarin overtuigen dat het een meerwaarde is voor hen.
• Betekent het ook daadwerkelijk iets voor de dagelijkse praktijk, het is natuurlijk ja?

86
D. Resultaten
• Het heeft voor het bestuur/ de organisatie geen
meerwaarde • De resultaten van SNIV geven niet de doorslag om
deel te nemen/ niet voldoende meerwaarde (bv Vergelijking met andere huizen)
• Maar als het gewoon is voor het grote goed, landelijk of voor het belang van een RIVM om data te vergaren, is dat ook belangrijk, maar voor de organisatie an sich minder.
• en levert het ons dan voldoende op aan het eind van het jaar om daar terugkoppeling over te krijgen?
8. Herinneren Het herinneren aan de registratie of aan het turven van infecties wordt als belemmerende factor genoemd
maar dan denk ik dat het meer bepalend is van he, denken we er inderdaad aan
9. Financieel Financiële bijdrage zorgt niet voor deelname Dit zullen wij nooit merken, dat stroomt altijd terug naar een de grote hoop
10. Management A. Steunen B. Prioriteit
Het management steunt deelname niet of belemmert deelname
• Ze steunen deelname niet • Infectie preventie/registratie heeft geen prioritiet
• Dan zegt mijn management op een gegeven moment ook van ja die tijdsinvestering gaan we niet doen.
• als het iets is wat onder hun (het management) zou gaan vallen, als het iets waar zij zich mee bezig zou moeten gaan houden, dat ze dan misschien andere prioritering zou gaan doen.
11. Sturing overheid Sturing vanuit de overheid om infecties te registreren wordt als probleem ervaren/of is geen doorslaggevende reden om deel te nemen
Het heeft wel invloed maar het werkt soms ook een beetje de andere kant van de goh net alsof we niks te doen hebben en dan moeten we weer lijstjes bijhouden.
12. Uitvoering
A. Achteraf
B. Aanleveren
C. Diagnose
D. Definitie
De uitvoering van de manier van registreren wordt als belemmerende factor voor deelname gezien = dus echt de reden voor geen deelname, anders bij data verzameling zetten. (algemene opmerkingen)
• Achteraf registreren of na zoeken van infecties wordt als lastig/probleem ervaren
• Het aanleveren van het aantal infecties is de reden
• Het stellen van de diagnose is moeilijk (bv door betrouwbaarheid) en is een belemmerende factor
• De opgestelde definities zorgen voor problemen of zijn niet betrouwbaar.
Ja en weet je het is eigenlijk nooit helemaal goed gegaan.
• dat je aan het einde van de week, want dat was een beetje de vrees ….. dat je het zelf bijgehouden moet hebben hoeveel infecties je hebt gezien.
• dat je hoe heet het, allerlei materialen moet verzamelen en dat je op het moment dat er zich iets voordoet, dat vraagt een bepaalde belasting van het personeel
• het si wel degelijk een belemmerende factor om aan registratie te doen. in de eerste plaats weet je dan niet goed wat je registreren moet,
• Eigenlijk weten we helemaal niet zo goed wat het is een urineweginfectie en een luchtweg infectie. En dat maakt het registreren redelijk lastig.
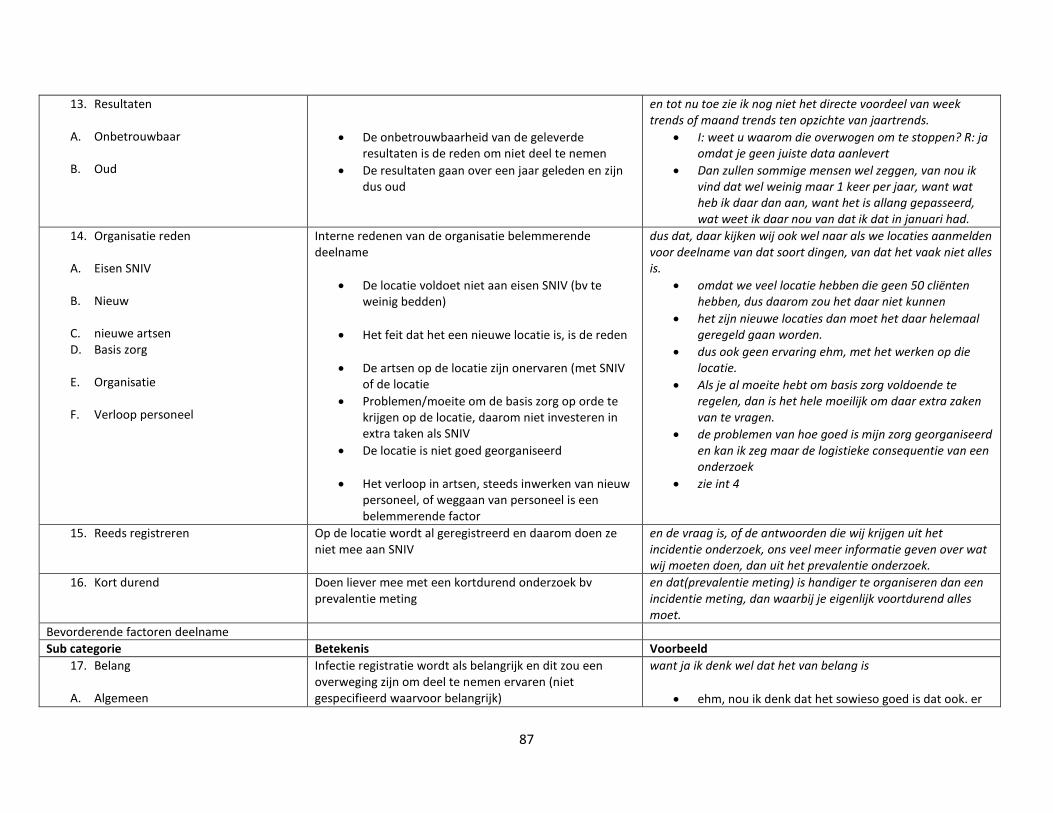
87
13. Resultaten
A. Onbetrouwbaar
B. Oud
• De onbetrouwbaarheid van de geleverde resultaten is de reden om niet deel te nemen
• De resultaten gaan over een jaar geleden en zijn dus oud
en tot nu toe zie ik nog niet het directe voordeel van week trends of maand trends ten opzichte van jaartrends.
• I: weet u waarom die overwogen om te stoppen? R: ja omdat je geen juiste data aanlevert
• Dan zullen sommige mensen wel zeggen, van nou ik vind dat wel weinig maar 1 keer per jaar, want wat heb ik daar dan aan, want het is allang gepasseerd, wat weet ik daar nou van dat ik dat in januari had.
14. Organisatie reden
A. Eisen SNIV
B. Nieuw
C. nieuwe artsen D. Basis zorg
E. Organisatie
F. Verloop personeel
Interne redenen van de organisatie belemmerende deelname
• De locatie voldoet niet aan eisen SNIV (bv te weinig bedden)
• Het feit dat het een nieuwe locatie is, is de reden
• De artsen op de locatie zijn onervaren (met SNIV of de locatie
• Problemen/moeite om de basis zorg op orde te krijgen op de locatie, daarom niet investeren in extra taken als SNIV
• De locatie is niet goed georganiseerd
• Het verloop in artsen, steeds inwerken van nieuw personeel, of weggaan van personeel is een belemmerende factor
dus dat, daar kijken wij ook wel naar als we locaties aanmelden voor deelname van dat soort dingen, van dat het vaak niet alles is.
• omdat we veel locatie hebben die geen 50 cliënten hebben, dus daarom zou het daar niet kunnen
• het zijn nieuwe locaties dan moet het daar helemaal geregeld gaan worden.
• dus ook geen ervaring ehm, met het werken op die locatie.
• Als je al moeite hebt om basis zorg voldoende te regelen, dan is het hele moeilijk om daar extra zaken van te vragen.
• de problemen van hoe goed is mijn zorg georganiseerd en kan ik zeg maar de logistieke consequentie van een onderzoek
• zie int 4
15. Reeds registreren Op de locatie wordt al geregistreerd en daarom doen ze niet mee aan SNIV
en de vraag is, of de antwoorden die wij krijgen uit het incidentie onderzoek, ons veel meer informatie geven over wat wij moeten doen, dan uit het prevalentie onderzoek.
16. Kort durend Doen liever mee met een kortdurend onderzoek bv prevalentie meting
en dat(prevalentie meting) is handiger te organiseren dan een incidentie meting, dan waarbij je eigenlijk voortdurend alles moet.
Bevorderende factoren deelname Sub categorie Betekenis Voorbeeld
17. Belang
A. Algemeen
Infectie registratie wordt als belangrijk en dit zou een overweging zijn om deel te nemen ervaren (niet gespecifieerd waarvoor belangrijk)
want ja ik denk wel dat het van belang is
• ehm, nou ik denk dat het sowieso goed is dat ook. er

88
B. Antibiotica C.
D. infecties
• Registreren van infecties is belangrijk voor het algemeen goed-> bv landelijke data
• Registreren is belangrijk in verband met antibiotica gebruik/resistentie
• Doordat infectie ziekten als belangrijk worden ervaren
data bekend worden over, he landelijk over het voorkomen van infecties.
• Zeker in de situatie waarin we landelijk ook steeds meer verzuild raken rondom alle multiresistente van BRMOs allerlei problemen die we tegen komen
• En dat is dan wel van belang denk ik, ook voor een hygiënist, want die linkt weer aan de GGD en de GGD heeft uiteindelijk ook weer een belang bij incidentie en prevalentie van infectie ziekte. Ja.
18. Verantwoordelijkheid
A. Voelen
B. Taken
Verantwoordelijkheid wordt als bevorderende factor voor deelname genoemd
• De SO uit de infectie commissie voelt zich verantwoordelijk over infectie registratie
• Het staat in de taakomschrijving van de SO
• Ja, ik ben toch vanuit het hygiëne werkgroep van onze verpleeghuizen….. dus wat dat betreft voelde ik me wel verantwoordelijk.
• ook in de taakomschrijving van de specialist ouderengeneeskunde staat dat je daar een belangrijke rol in hebt.
19. Houding Het hebben van een positieve houding ten opzichte van infectie preventie en registratie bevordert deelname
dus dan ja weet je het is heel leuk om en ik zie dan als ik dan die nieuwsbrieven lees, moet je kijken wat goed.
20. Voortrekker Één of enkele personen zijn de voortrekker wat betreft infectie registratie en bevorderen deelname
nou één van de artsen die is ook een, nou ja of ze nou wel of niet microbioloog is, dat weet ik niet. Maar die kwam daarmee
21. Eerdere deelname Deelname aan eerder infectie registratie onderzoek bevordert deelname aan SNIV/infectie registratie
… daar hebben we aan deelgenomen, aan de hand van dat was de volgende stap deelnemen aan de prevalentie studie van SNIV eigenlijk ook een vanzelfsprekende stap
22. Voordeel
A. Organisatie
B. Patiënten
C. Praktijk
D. SO’s
E. Vooraf
Het hebben van voordelen door deelname aan SNIV is een bevorderende factor of voordelen van deelname aan SNIV worden genoemd.
• Het moet specifieke voordelen voor de organisatie/ huis zelf (management niveau) hebben
• Voordelen voor de patiënten
• Voordelen voor de dagelijkse praktijk (verpleegkundige niveau)
• Voordelen voor de SO’s
ja juist. Het moet wat opleveren.
• wij nemen daar aan deel als het voor onze organisatie ook een winst betekent.
• en dan hebben mensen misschien minder antibiotica. En nou ja dat soort dingen en dat komt mensen dan ook wel weer tegoeden.
• Ja dat je jezelf kwaliteit gaat verbeteren, op alle diagnostische en behandel methode bij elkaar gewoon.
• niet alleen kijken kijken kijken naar de cijfers, maar wat betekent het voor mij.
• je moet eerst bepalen waarom je gegevens nodig hebt

89
• Je moet vooraf bepalen waarom je mee zou doen aan SNIV, wat je er voor voordeel uit haalt
ne wat je ermee wilt, en welke conclusies je eruit wilt trekken en dan de gegevens verzamelen. niet andersom.
23. Resultaten:
A. Vergelijken i. Landelijk
ii. Huizen
iii. Afdelingen
B. Trends
C. Huidige stand van zaken D.
E. Beleid
F. Dagelijkse praktijk
G. UWI
Het ontvangen van de resultaten van registratie wordt als reden gegeven om deel te nemen
• Wil resultaten gebruiken om te vergelijken o Met het landelijke gemiddelde o Met andere verpleeghuizen
o Met eigen afdelingen/ op afdelingsniveau
kijken
• Wil resultaten gebruiken om trends in de tijd te zien
• Wil resultaten gebruiken om de huidige stand van zaken te bepalen en/of problemen in het eigen huis te identificeren en verbeteren
• Wil resultaten gebruiken om (antibiotica) beleid op te maken
• Wil resultaten gebruiken om de praktijk op verzorgende niveau te verbeteren
• Wil specifiek naar de urineweginfecties kijken
Ehm incidentie studie bewust ook gekozen want als we dan willen deelnemen en we willen resultaten zien, dan moet het een incidentie studie zijn en niet een prevalentie studie
• Dat we die resultaten dan ook toe gespitst krijgen o op onze organisatie in verhouding met de
regio, met landelijk o Weet je als je ook verpleeghuizen kan
vergelijken met hoe jouw organisatie dat dan doet
o En dat rondom influenza en UWI he hangt dat samen in de tijd, met bepaalde afdelingen
• omdat je dan ook veel duidelijker in de tijd kunt zien waar de problemen zaten.
• Ook om vanuit de organisatie zelf, hoeveel problemen hebben we nu in het verpleeghuis, hoeveel.
• misschien ons beleid of eh nou ja dingen verbeteren en dat nou ja denk ik voor dit dan ook geld.
• dan zou het aanleveren van data ook om bij wijze van spreken op de werkvloer inzichtelijk te maken waar de problemen zitten,
• Die urineweginfectie heb ik niet gemeten, ehm, dus is natuurlijk op zich heel erg interessant, want er zijn, er is natuurlijk overbehandeling van urineweginfecties.
24. Alertheid Registreren van infecties helpt om alert te blijven op infectie preventie maatregelen en dit wordt als reden voor deelname/bevorderende factor/positief punt genoemd
Dat (infectie registratie) ja iets is waarbij je zeker in verpleeghuizen, als je niet alert blijft dan gaat de handhygiëne, überhaupt de hygiëne dan wordt ondergeschoven kindje,
25. Sturing overheid Beslissingen op overheid/inspectie niveau dragen bij aan deelname/infectie registratie/ nadenken over deelname
volgend jaar dan zal een overheid misschien anders beslissen of een inspectie bepaald eisen te stellen aan bepaalde data vergaring en dan moet, wordt je geacht hieraan deel te nemen, dan heb je geen keus meer.
26. Financieel
A. Formatie
Financiële bijdrage/vergoeding bevordert deelname aan SNIV (algemeen)
dat je bij wijze van spreken een x aantal uren een arts of een onderzoeker of een verpleegkundige die de data vergaard erbij krijt, dan heb je wat je wilt.

90
• als het in de vorm van formatie is • als financieel betekent dat het formatie erbij komt om dingen te doen
27. Tijd Deelname wordt als een kleine/geen tijdsinvestering gezien of een kleine/geen tijdsinvestering wordt als bevorderende factor genoemd voor deelname
Nee, ik niet want ik vind het helemaal niet tijdrovend
28. Opbouw registratie Deelnemer benoemt dat een goede opbouw/uitvoering van infectie registratie deelname bevordert/belangrijk is voor deelname
Dat het dan anders en beter georganiseerd is dan het aanvankelijk aandiende.
29. Presentatie De presentatie verzorgd door het RIVM zorgde voor deelname
Dus toen is [NAAM] hier geweest, en uitleg gegeven en toen waren de dokters hiervan ja goed dat moeten wij doen.
30. Management Het management steunt de keuze van de SO’s om deel te nemen.
31. Goede band Een goede band tussen de betrokkenen voor registratie bevordert deelname
Nou dan zit ik daar bovenop en een andere collega zat daar bovenop op haar woonerf, en nou dan is het overzichtelijk.
32. Publicatie De mogelijkheid tot een publicatie voor als een bevorderende factor genoemd voor deelname
Dat was dan leuk. En dan denk ik van, heb ik toch meegewerkt aan het wetenschappelijk artikel, staat leuk op je cv.
Ideaal beeld en suggesties Sub categorie betekenis Voorbeeld
33. Tijd Deelname moet een niet te grote tijdsinvestering zijn de tijdsinvestering moet niet te groot zijn, 34. Administratie
A. Ondersteuning
B. OSIRIS
Suggesties voor nieuwe of betere manieren van het administreren van het aantal infecties:
• Iemand die de administratie doet
• Veranderingen in OSIRIS
• als het bij wijze van spreken iemand die je administratief ondersteun
• het lijk me ook het handigst dat je 1 inlog hebt, 35. Software
A. landelijk
B. Huidige dossier
i. Codes
Een beschrijving van hoe de software idealiter zou werken (algemene opmerkingen)
• Een landelijk isis systeem
• De mogelijkheid tot registreren in het huidige systeem van het huis, en dat dit bij het RIVM aankomt
o Gebruik van codes
en je bent dat aan het beschrijven bij wijze van met 1 druk op de knop kan weer geven, dit is uiteindelijk voor de data van het RIVM. Dan ben je uiteindelijk heel makkelijk klaar.
• Het mooiste is natuurlijk, als je met een soort ISIS systeem werkt en dat gewoon uit landelijke data base, getallen worden getrokken.
• nou ja dan denk ik dat die aan het ECD gekoppeld moet zijn, wat ik ook zei.
o en dat dan, dat je de data gewoon genereerd vanuit de codes die je daar invult. Of dat die de codes misschien wel standaard ingevuld worden door het systeem.
36. Aanleveren Suggesties voor nieuwe of betere manieren over het A

91
A. Registreren tijdens diagnose
B. Formulier
C. Herinneren
i. Pop up
D. Protocol
aanleveren van de aantal infecties • Registreren/turven terwijl de diagnose wordt
gesteld of terwijl de SO met de patiënt/registratie bezig is
• Door een formulier te ontwikkelen waarop het bijgehouden kan worden
• Herinneren voor het aanleveren
o Door een pop-up systeem in het huidige dossier
• Opnemen in een protocol
• En het zou natuurlijk veel makkelijker zijn als je op het
moment dat je er mee bezig bent het kan wegschrijft. • ja oké maar dat is een kwestie van ehm van mijn part
een formulier ontwikkelen die we hier in ons verpleegdossier zouden kunnen maken
• nou ja daarvoor denk ik gewoon, moet je het iedere drie weken herhalen, want anders dan vergeten ze het.
o En als ik ene pop-up van hé je hebt hier geschreven gastro-enteritis, kan ik deze registreren, ja zo iets.
• En dat is overigens voor de artsen zo, in het inwerkprotocol staat dat er uitleg gegeven wordt over SNIV.
37. Resultaten: A. Flexibel
B. Inspectie
C. Advies
D. Vorm
E. Frequentie
i. Jaar ii. Kwartaal
F. Direct
G. Antibiotica
Suggesties voor de resultaten in het algemeen • Terugrapportages moeten aan de wensen van het
huis op dat moment aangepast kunnen worden.
• Terugrapportages moeten gebruikt kunnen worden om bepaalde dingen aan de inspectie te kunnen aantonen.
• Terugrapportages moeten ook advies voor het huis bevatten (bv suggesties welke preventie maatregelen ze nog kunnen nalopen)
• Over de vorm/format van terugrapportages of presentatie van de terugrapportages
• Over het aantal keer dat de rapportages gegeven zouden moeten worden
o Jaar o Kwartaal
• Terugkoppeling moet direct plaatsvinden
• Resultaten zijn gekoppeld aan antibiotica gebruik
• ja dat is denk ik ook wel voldoende, maar misschien dat een organisatie die heel druk bezig is met hygiëne kwaliteit op te krikken behoefte heeft aan vaker, dat weet ik niet, maar dat zou best kunnen
• die daar bij wijze van spreken onder de loep zitten van de inspectie dat die zo iets hebben, wij willen graag aantonen dat we het beter doen,
• dus al je dan iets terug zou krijgen dan ja, hoop je dat je ook een advies van iets erbij krijgt waar je wat mee kan
• Ja, toch wel over de mail met wat informatie, een overzicht van voor infecties.
• I: terug rapportage is één keer per jaar, wat vindt u daarvan? R: heb ik geen mening over dat weet ik niet.
o ja dat (1 keer per jaar) is denk ik ook wel voldoende
o het zou helpen als je het 4 keer per jaar kunt doen, maar dan is wel goed dat je ook een terugrapportage hebt.
• dan heeft het nut, want dan weet je direct oh ik registreer iets en omdat ik het nu registreer, krijg ik het ook weer
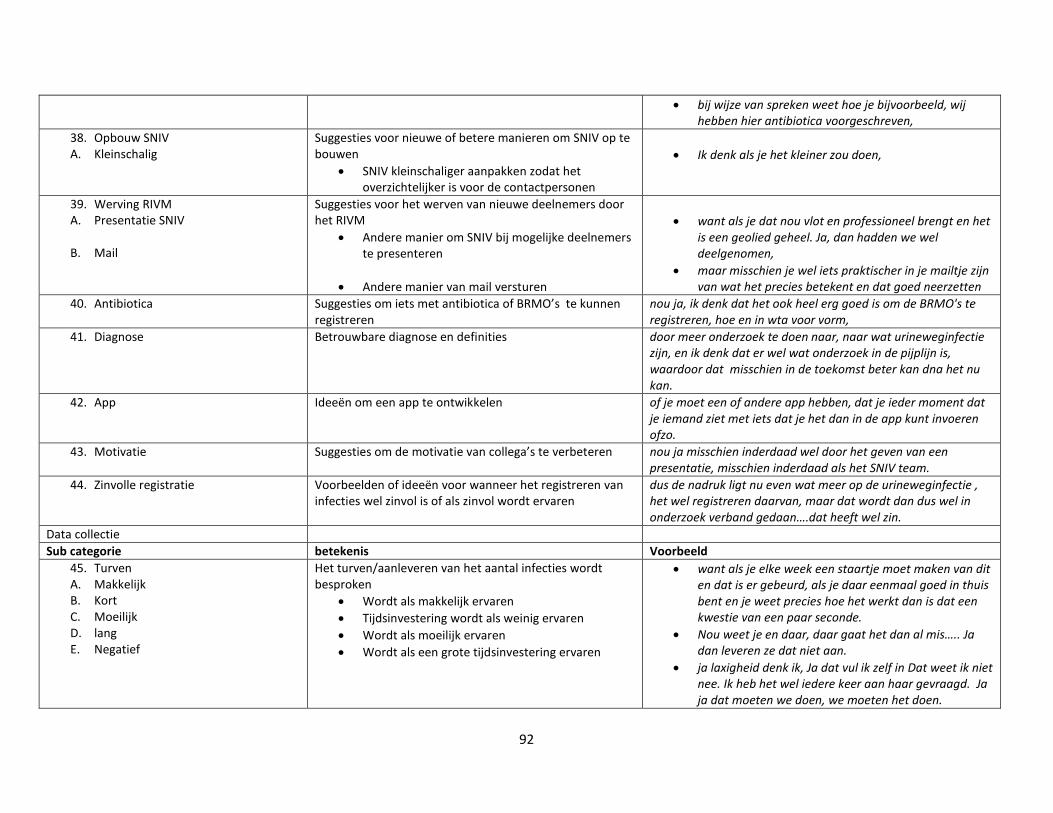
92
• bij wijze van spreken weet hoe je bijvoorbeeld, wij hebben hier antibiotica voorgeschreven,
38. Opbouw SNIV A. Kleinschalig
Suggesties voor nieuwe of betere manieren om SNIV op te bouwen
• SNIV kleinschaliger aanpakken zodat het overzichtelijker is voor de contactpersonen
• Ik denk als je het kleiner zou doen,
39. Werving RIVM A. Presentatie SNIV
B. Mail
Suggesties voor het werven van nieuwe deelnemers door het RIVM
• Andere manier om SNIV bij mogelijke deelnemers te presenteren
• Andere manier van mail versturen
• want als je dat nou vlot en professioneel brengt en het
is een geolied geheel. Ja, dan hadden we wel deelgenomen,
• maar misschien je wel iets praktischer in je mailtje zijn van wat het precies betekent en dat goed neerzetten
40. Antibiotica Suggesties om iets met antibiotica of BRMO’s te kunnen registreren
nou ja, ik denk dat het ook heel erg goed is om de BRMO's te registreren, hoe en in wta voor vorm,
41. Diagnose Betrouwbare diagnose en definities door meer onderzoek te doen naar, naar wat urineweginfectie zijn, en ik denk dat er wel wat onderzoek in de pijplijn is, waardoor dat misschien in de toekomst beter kan dna het nu kan.
42. App Ideeën om een app te ontwikkelen of je moet een of andere app hebben, dat je ieder moment dat je iemand ziet met iets dat je het dan in de app kunt invoeren ofzo.
43. Motivatie Suggesties om de motivatie van collega’s te verbeteren nou ja misschien inderdaad wel door het geven van een presentatie, misschien inderdaad als het SNIV team.
44. Zinvolle registratie Voorbeelden of ideeën voor wanneer het registreren van infecties wel zinvol is of als zinvol wordt ervaren
dus de nadruk ligt nu even wat meer op de urineweginfectie , het wel registreren daarvan, maar dat wordt dan dus wel in onderzoek verband gedaan….dat heeft wel zin.
Data collectie Sub categorie betekenis Voorbeeld
45. Turven A. Makkelijk B. Kort C. Moeilijk D. lang E. Negatief
Het turven/aanleveren van het aantal infecties wordt besproken
• Wordt als makkelijk ervaren • Tijdsinvestering wordt als weinig ervaren • Wordt als moeilijk ervaren • Wordt als een grote tijdsinvestering ervaren
• want als je elke week een staartje moet maken van dit en dat is er gebeurd, als je daar eenmaal goed in thuis bent en je weet precies hoe het werkt dan is dat een kwestie van een paar seconde.
• Nou weet je en daar, daar gaat het dan al mis….. Ja dan leveren ze dat niet aan.
• ja laxigheid denk ik, Ja dat vul ik zelf in Dat weet ik niet nee. Ik heb het wel iedere keer aan haar gevraagd. Ja ja dat moeten we doen, we moeten het doen.

93
46. Gewenning Het wennen aan registratie en doorgeven van infecties is belangrijk en het moet in het dagelijkse systeem komen
als je daar eenmaal goed in thuis bent en je weet precies hoe het werkt dan is dat een kwestie van een paar seconde.
47. Online registreren A. Makkelijk B. Kort C. Moeilijk D. lang E. Negatief
Opmerking over het invoeren van de infecties (in OSIRIS) • Wordt als makkelijk ervaren • Tijdsinvestering wordt als weinig ervaren • Wordt als moeilijk ervaren • Wordt als een grote tijdsinvestering ervaren
Maar je moet uiteindelijk wel ehm ja, je de software eigen maken, je moest inloggen in het RIVM, dus uiteindelijk het was niet zo vanzelf sprekend en nog die situatie
48. Betrouwbaarheid A. Diagnose B. definitie
Opmerkingen over de betrouwbaarheid van • De diagnose • De definitie
• Nou ene pneumonie, nou die kunnen ze in het ziekenhuis al niet diagnosticeren, laat staan in het verpleeghuis hè.
• nou ja het is soms wel lastig inderdaad want wanneer noem je iets nou een pneumonie
49. Definitie checken Opmerkingen over het herinneren van de definities/criteria
want dat is dan nog wel een dingetje waarvan ik denk oh ja dan moet je dus nog wel altijd even nadenken, voldoe ik dan wel aan de criteria dat iedereen ook al die criteria goed in zijn hoofd heeft voordat hij zegt van dit is een gastro enteritis en moet geregistreerd worden.
50. Bovenop De verantwoordelijke van de registratie zit bovenop dat het goed aangeleverd wordt en/of heeft goede contacten met de SO en/of dit wordt als belangrijk punt genoemd
En eh nu is die band tussen mij en de specialist ouderengeneeskunde, dus wij hebben hele nauwe banden. En nu zitten wij daar bovenop, als je het nu zou doen dat dat wel makkelijker zou gaan, omdat die lijntjes nu wel heel kort en heel direct zijn.
51. Herinneren Opmerkingen over het herinneren van de artsen om het aantal infecties door te sturen, als het niet als bezwaar of reden om niet deel te nemen wordt genoemd
ehm, ja weet je, ik denk dat het is, dat je het moet onthouden en daarna nog moet gaan registreren,
52. Huidige situatie
A. Positief B. Negatief
Deelnemer beschrijft de huidige manier van registreren (benoemd niet specifiek of dit positief of negatief is)
• Geeft aan dat dit een fijne manier is • Geeft aan dat is onhandige manier is
Uitvoerder 53. Aanleveren A. SO B. PV C. VS D. Afdelingsteam E. dip
Het aanleveren/diagnosticeren van de infecties en de aantallen moet worden gedaan door:
• De SO • Praktijkverpleegkundige • Verpleegkundig specialist • Afdelingsteam

94
• dipper 54. Invoeren A. SO B. MS C. Praktijkvk
Het invoeren van de infecties en de aantallen in OSIRIS moet worden gedaan door:
• SO • Iemand van het (medisch) secretariaat • Praktijkverpleegkundige
55. Ontvangen resultaten A. SO B. MS C. Manager
De resultaten/terugrapportage moeten door het RIVM worden gestuurd naar:
• SO • Iemand van het medisch secretariaat • (afdelings)manager
56. Actie nav resultaten A. SO
De persoon die iets moet ondernemer naar aanleiding van de resultaten:
• De SO moet de resultaten verwerken of gebruiken voor verbeteringen, veranderingen of beleidmaken
57. Deelname A. Management B. SO C. Management op advies van SO
De beslissing om deel te nemen moet worden genomen door:
• Management • SO’s • Management neemt de beslissing op advies van
SO
58. Stoppen deelname A. SO
De beslissing om te stoppen met deelname wordt gemaakt doror:
• De SO
Disseminatie 59. Overleggen A. SO’s B. Hygiëne C. Afdeling D. Organisatie E. FTO
De resultaten(zullen/moeten) worden besproken op overleggen
• Met SO’s van het desbetreffende huis • Van de hygiëne commissie/ infectie preventie
commissie etc • Met de afdelingen • Op overleggen van de gehele organisatie • Op het farmaco therapeutisch overleg
60. Delen A. SO’s B. Management
De resultaten/ terugrapportage (zullen/moeten)worden gedeeld met:
• Andere SO’s

95
C. afdelingen • Het management • Afdelingen (verpleegsters en verzorgers)
Overage 61. Voor hele organisatie doen: Deelnemers geven aan dat als ze deelnemen dat ze het
dan voor de hele organisatie moeten doen, Maar ik denk dat we dan, wel omdat we ook zo'n Cordaan overleg hebben we dan wel moeten ja voor heel Cordaan moeten doen.
62. jaarlijkse vragenlijst: het invullen van de jaarlijkse vragenlijst wordt als veel werk ervaren
I: en als er tgevraagd zou worden van nou, wat vindt u minder fijn aan deelname? R: het jaarlijks invullen van de formuliere, de vragenlijsten.
63. Verwachting RIVM deelnemers noemen iets over de verwachtingen van het RIVM
maar weet je, ik denk dat bij het RIVM wel heel veel gegeven bekend zijn en mogelijk ook als we de uitleg over de gegevens krijgen, dat degene die komt dan misschien ook wel literatuurstudies of weet ik het wat over.
Resulatten Sub categorie Betekenis Voorbeelden
64. Gebruik resultaten
A. Huidige evaluatie
B. Veranderingen meten C. Verbeteren/Beleid
D. Preventie
E. Praktijk
F. Patiënten
G. Trend
H. Antibiotica I. Uitbraak
J. Casus
De resultaten/terugrapportages zullen(ZULLEN, WORDEN HIER DUS NOG NIET VOOR GEBRUIKT ) worden gebruikt om:
• Naar het eigen functioneren van het huis op dat moment te kijken en/of te kijken waar aanpassingen nodig zijn
• Om te kijken of er verandering heeft plaats gevonden
• Om het huidige beleid aan te passen of situatie te verberteren
• Als input voor infectie preventie
• Om de dagelijkse praktijk te verbeteren
• Om de gezondheid van patiënten te verbeteren
• Om te vergelijken
• Voor antibiotica • Voor het identificeren/voorkomen van uitbraken
Toch kijken of we daar meer mee kunnen doen, dat we tot nu toe hebben gedaan.
• bekijken zijn we goed bezig met onze hygiëne maatregelen hier in huis. Of moet dat aangescherpt
• wij willen graag aantonen dat we het beter doen • Dus dat je dan die trends dan wel kan ontdekken zal ik
maar zeggen en misschien beleid op kan maken. • Of wel kan aangeven waar, nou ja belangrijke
speerpunten kunnen liggen, in het kader van infectie preventie
• om te spiegelen, naar de artsen naar de verpleegkundig specialisten, zitten wij goed op het gebied van de instructies aan de verpleging, zitten we goed op het gebied van het gebruik van de eerste diagnostische methoden, gebruiken we de kweek goed
• Ja minder ongemak. Kijk als je gastro-enteritis hebt en mensen, nou ja dat is niet echt leuk zou ik maar zeggen.
• dat je een trend kan zien van waar zijn die infecties, nemen ze toe.
• Wat heeft het, wat is de impact op ons antibiotica beleid.`

96
• Als casus op overleggen
• Van hé, kunnen wij zien dat er ergens bijvoorbeeld een resistente bacterie, een haard geeft, een lokale kleine uitbraak veroorzaakt, waar we dan op tijd bij kunnen zijn.
• en dat als casustiek gebruiken bij de vakgroep overleggen.
65. Interpretatie A. Betrouwbaarheid
B. Onervaren
C. ondersteuning
De interpretatie van de resultaten is moeilijk of beperkt • Door de betrouwbaarheid van de resultaten
• Door de onwetendheid van de SO
• Ondersteuning vanuit RIVM voor resultaten is
gewenst, is gedaan
• Dus en dat is denk ik wel het lastige dat het, de manier
waarop je registreer, bepaald voor een groot deel je getallen.
• wat kunnen wij hieruit concluderen, want dat vinden we moeilijk,
• of iemand van het SNIV team ons daarbij kan ondersteunen, van wat kunnen wij hieruit concluderen,
66. Terugzien Het kunnen terug kijken van de eigen aangeleverde data wordt als positief ervaren.
nou ja dat is als je het wel eens terug wil kijken Dat is handig.
67. Terugrapportage
A. Vergelijken i. Huizen
B. Niet
De terugrapportages of resultaten uit eigen registratie) worden gebruikt voor:
• Vergelijken • Andere huizen
• niks
• ik denk dat er misschien even naar gekeken wordt, maar er vind geen terugkoppeling plaats naar het artsen team.
68. Geen gebruik redenen
a. Onbetrouwbaar
b. Geen advies c. Prioriteit
d. Deel organisatie
e. Tijd
Redenen waarom de resultaten/terugrapportages niet gebruikt worden
• De terugrapportages zijn niet betrouwbaar voor het huis
• Omdat er verder geen advies in staat • SNIV resultaten/infectie preventie/registratie
heeft geen prioriteit
• Resultaten zijn niet beschikbaar voor hele organisatie
• Er is niet genoeg tijd om de resultaten te bespreken
• Ja ik denk dus omdat je geen juiste, ja jullie geven mooie rapportages, maar het klopt niet voor dit huis.
• er staan ook verder geen aanbevelingen bij. • Want nu met de fusie zullen er, best wel belangrijke te
agenderen onderwerpen komen, over de afstemming tussen de beide artsen team
• 1 van de redenen is ook wel, dat we het niet voor de hele organisatie doen, dus het is maar voor een deel van de artsen
• misschien ook wel de werkdruk.
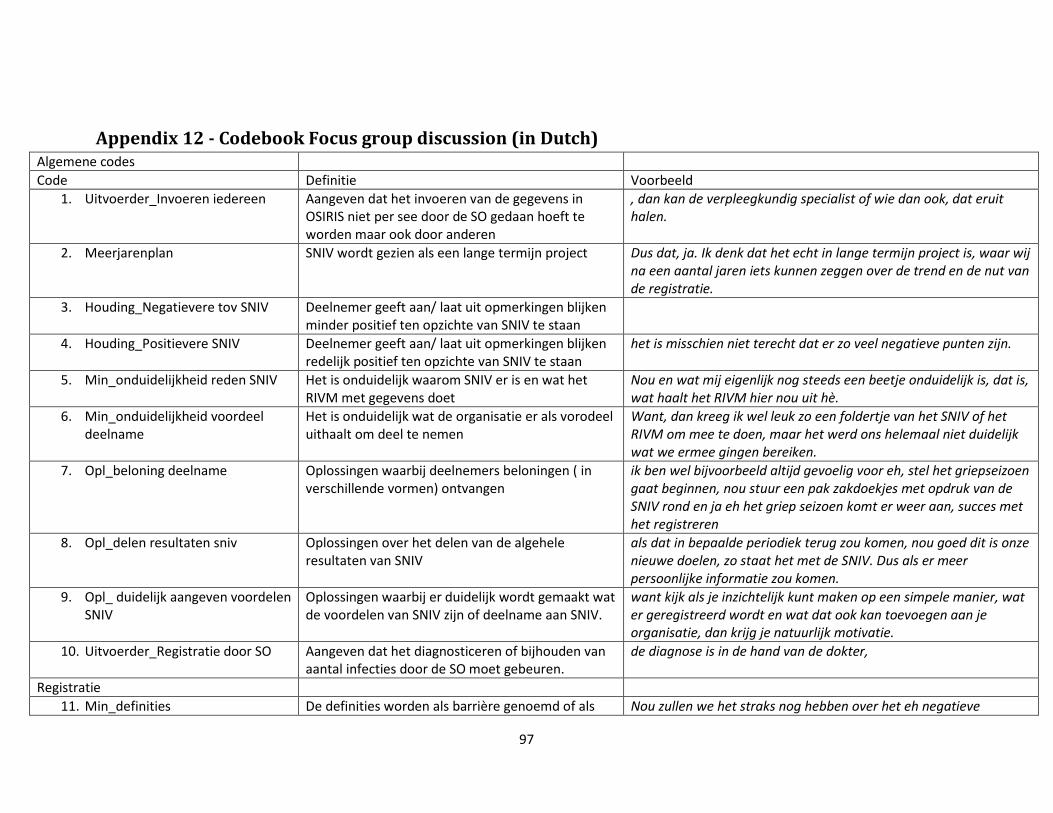
97
Appendix 12 - Codebook Focus group discussion (in Dutch) Algemene codes Code Definitie Voorbeeld
1. Uitvoerder_Invoeren iedereen Aangeven dat het invoeren van de gegevens in OSIRIS niet per see door de SO gedaan hoeft te worden maar ook door anderen
, dan kan de verpleegkundig specialist of wie dan ook, dat eruit halen.
2. Meerjarenplan SNIV wordt gezien als een lange termijn project Dus dat, ja. Ik denk dat het echt in lange termijn project is, waar wij na een aantal jaren iets kunnen zeggen over de trend en de nut van de registratie.
3. Houding_Negatievere tov SNIV Deelnemer geeft aan/ laat uit opmerkingen blijken minder positief ten opzichte van SNIV te staan
4. Houding_Positievere SNIV Deelnemer geeft aan/ laat uit opmerkingen blijken redelijk positief ten opzichte van SNIV te staan
het is misschien niet terecht dat er zo veel negatieve punten zijn.
5. Min_onduidelijkheid reden SNIV Het is onduidelijk waarom SNIV er is en wat het RIVM met gegevens doet
Nou en wat mij eigenlijk nog steeds een beetje onduidelijk is, dat is, wat haalt het RIVM hier nou uit hè.
6. Min_onduidelijkheid voordeel deelname
Het is onduidelijk wat de organisatie er als vorodeel uithaalt om deel te nemen
Want, dan kreeg ik wel leuk zo een foldertje van het SNIV of het RIVM om mee te doen, maar het werd ons helemaal niet duidelijk wat we ermee gingen bereiken.
7. Opl_beloning deelname Oplossingen waarbij deelnemers beloningen ( in verschillende vormen) ontvangen
ik ben wel bijvoorbeeld altijd gevoelig voor eh, stel het griepseizoen gaat beginnen, nou stuur een pak zakdoekjes met opdruk van de SNIV rond en ja eh het griep seizoen komt er weer aan, succes met het registreren
8. Opl_delen resultaten sniv Oplossingen over het delen van de algehele resultaten van SNIV
als dat in bepaalde periodiek terug zou komen, nou goed dit is onze nieuwe doelen, zo staat het met de SNIV. Dus als er meer persoonlijke informatie zou komen.
9. Opl_ duidelijk aangeven voordelen SNIV
Oplossingen waarbij er duidelijk wordt gemaakt wat de voordelen van SNIV zijn of deelname aan SNIV.
want kijk als je inzichtelijk kunt maken op een simpele manier, wat er geregistreerd wordt en wat dat ook kan toevoegen aan je organisatie, dan krijg je natuurlijk motivatie.
10. Uitvoerder_Registratie door SO Aangeven dat het diagnosticeren of bijhouden van aantal infecties door de SO moet gebeuren.
de diagnose is in de hand van de dokter,
Registratie 11. Min_definities De definities worden als barrière genoemd of als Nou zullen we het straks nog hebben over het eh negatieve

98
slecht ervaren aspecten. Want mij collega's vinden de definities soms vaag. 12. Min_gebrek
entousiasme/negatieve houding SNIV
Op de locatie (kan bij SO zelf of door collega’s) is een gebrek aan enthousiasme of een negatieve houding tov SNIV. Motivatie om te registreren is belangrijk
Nou als ik het woord SNIV noemt, dan begint iedereen al van oeeeh, nee, nee niet nog een keer. Nou dus dat geeft al aan hoe, enthousiast men is over het registreren. eh, je moet, het staat en valt met eraan denken en de wil om te registreren.
13. Min_doel registratie onbekend Het doel en nut van het registreren wordt niet erkend of is onduidelijk
alleen is de vraag of er uit komt, wat het RIVM er eigenlijk mee wil, beoogt, wat we er eigenlijk mee willen. Wat is het nut ervan.
14. Min_geen controle De registratie worden niet door RIVM of henzelf gecontroleerd ( dit kan als probleem worden ervaren hoeft niet) LET OP BIJ SCHRIJVEN ONDERSCHEID ZELF=CONTROLE EN RIVM=VALIDATIE
het wordt ook niet gecontroleerd he. Dat kun je nog bij de negatieve punten van de registratie kopje vertellen.
15. Min_ meer locaties, meer vergeten
Als je aan SNIV meedoet met meerdere locaties zorgt dat voor nadelen ( bv omdat je dan meer kans heb om te vergeten)
ga je meer locaties meedoen, gaat alles over meer personen. Meer schrijven, makkelijker vergeten.
16. Min_administratie invoeren Het invoeren van de infecties in OSIRIS wordt als negatief punt van registratie genoemd
Maar zij moet ook even eerst overzicht hebben, welke knopjes zij moet drukken, dus ergens, ergens als je de tijd optelt, dan kom je ook snel op die tijdsinvestering.
17. Min_afhnakelijk input anderen Bij registratie ben je afhankelijk van de input van anderen ( en dit kan als negatief punt worden ervaren)
Nou ja alles staat en valt met de input van ehm van collega's he.
18. Min_gebrek capaciteit Er is te weinig capaciteit om SNIV te doen Nou die routine hebben wij nu wel, alleen de capaciteit niet, dus wij blijven toch maar bij de 2 afdelingen
19. Min_ herinneren Het (zelf of je collega’s) eraan herinneren om te registreren wordt als belemmerende factor genoemd)
Ten eerste, en dat heb ik al eerder gezegd, vind ik het een dingetje dat ik mijn collega’s steeds weer moet herinneren aan het feit, denken jullie aan de SNIV
20. Min_terugzoeken Het moeten terugzoeken van d infecties en leeftijden van de afgelopen week wordt als probleem ervaren
maar ja als wij de lijstjes niet op dat moment invullen, dan is dat heel moeilijk om dat terug te zoeken
21. Min_tijd Registreren kost (redelijk veel)tijd Dus dat is, dus het is de voorbereiding wat de tijd kost. 22. Min_extra informatie Het opzoeken van de specifieke informatie die
nodig is (leeftijd etc) en het optellen ervan wordt als barrière/extra werk/overbodig ervaren
ja en dat is wel een heel gedoe, want bij elke geboortedatum moet je weer uitrekenen hoe oud is iemand. En dat is echt wel een frustratie
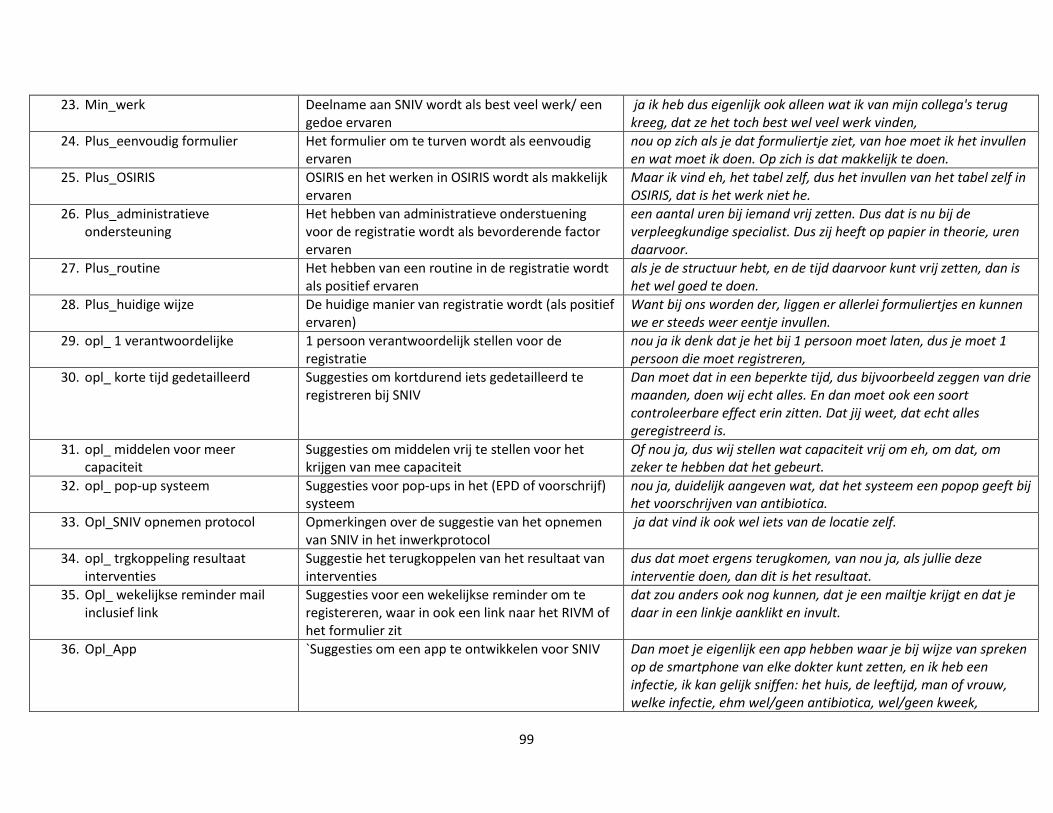
99
23. Min_werk Deelname aan SNIV wordt als best veel werk/ een gedoe ervaren
ja ik heb dus eigenlijk ook alleen wat ik van mijn collega's terug kreeg, dat ze het toch best wel veel werk vinden,
24. Plus_eenvoudig formulier Het formulier om te turven wordt als eenvoudig ervaren
nou op zich als je dat formuliertje ziet, van hoe moet ik het invullen en wat moet ik doen. Op zich is dat makkelijk te doen.
25. Plus_OSIRIS OSIRIS en het werken in OSIRIS wordt als makkelijk ervaren
Maar ik vind eh, het tabel zelf, dus het invullen van het tabel zelf in OSIRIS, dat is het werk niet he.
26. Plus_administratieve ondersteuning
Het hebben van administratieve onderstuening voor de registratie wordt als bevorderende factor ervaren
een aantal uren bij iemand vrij zetten. Dus dat is nu bij de verpleegkundige specialist. Dus zij heeft op papier in theorie, uren daarvoor.
27. Plus_routine Het hebben van een routine in de registratie wordt als positief ervaren
als je de structuur hebt, en de tijd daarvoor kunt vrij zetten, dan is het wel goed te doen.
28. Plus_huidige wijze De huidige manier van registratie wordt (als positief ervaren)
Want bij ons worden der, liggen er allerlei formuliertjes en kunnen we er steeds weer eentje invullen.
29. opl_ 1 verantwoordelijke 1 persoon verantwoordelijk stellen voor de registratie
nou ja ik denk dat je het bij 1 persoon moet laten, dus je moet 1 persoon die moet registreren,
30. opl_ korte tijd gedetailleerd Suggesties om kortdurend iets gedetailleerd te registreren bij SNIV
Dan moet dat in een beperkte tijd, dus bijvoorbeeld zeggen van drie maanden, doen wij echt alles. En dan moet ook een soort controleerbare effect erin zitten. Dat jij weet, dat echt alles geregistreerd is.
31. opl_ middelen voor meer capaciteit
Suggesties om middelen vrij te stellen voor het krijgen van mee capaciteit
Of nou ja, dus wij stellen wat capaciteit vrij om eh, om dat, om zeker te hebben dat het gebeurt.
32. opl_ pop-up systeem Suggesties voor pop-ups in het (EPD of voorschrijf) systeem
nou ja, duidelijk aangeven wat, dat het systeem een popop geeft bij het voorschrijven van antibiotica.
33. Opl_SNIV opnemen protocol Opmerkingen over de suggestie van het opnemen van SNIV in het inwerkprotocol
ja dat vind ik ook wel iets van de locatie zelf.
34. opl_ trgkoppeling resultaat interventies
Suggestie het terugkoppelen van het resultaat van interventies
dus dat moet ergens terugkomen, van nou ja, als jullie deze interventie doen, dan dit is het resultaat.
35. Opl_ wekelijkse reminder mail inclusief link
Suggesties voor een wekelijkse reminder om te registereren, waar in ook een link naar het RIVM of het formulier zit
dat zou anders ook nog kunnen, dat je een mailtje krijgt en dat je daar in een linkje aanklikt en invult.
36. Opl_App `Suggesties om een app te ontwikkelen voor SNIV Dan moet je eigenlijk een app hebben waar je bij wijze van spreken op de smartphone van elke dokter kunt zetten, en ik heb een infectie, ik kan gelijk sniffen: het huis, de leeftijd, man of vrouw, welke infectie, ehm wel/geen antibiotica, wel/geen kweek,

100
wel/geen katheter, 37. opl_best practices Suggesties om goed lopende registraties en
interventies van huizen als voorbeeld te stellen aan anderen
tips van een organisatie waar de registratie goed loopt zou je kunnen opgeven. Dus voorbeelden geven, van hoe het een en ander goed is georganiseerd.
38. Opl_compatibel met EPD Suggesties om de registratie te koppelen aan het EPD
het registratie systeem, is het compatibel met het EPD. het zou natuurlijk heel leuk zijn als je iets kan maken, waarbij het aan het EPD kan. Want dan kan je zelf ook uit EPD andere vragen halen.
39. opl_duidelijkere/pragmatische definities
Suggesties om de definities aan te passen duidelijkere definities met betrekking tot registreren van infectieziektes.
40. Opl_ formulier bij herinnering Suggestie om het formulier toe te voegen als je een vorm van herinnering stuurt naar SO’s
als de SNIV als de tijdens het elektronisch voorschrijfsysteem wel een SNIV opmerking komt, dan zou je wel verwachten dan moet er ook meteen een SNIV formulier geopend worden.
41. Opl_formulier op handige locatie Opmerkingen over het plaatsen van het formulier op een handige locatie
hebben wij niet. Of het hangt bij ons overigens bijna op alle artsen kamers.
42. Opl_hulp herinneren andere functies
Suggesties om andere functies ook mee te laten helpen met herinneren om te registreren
zorgcoördinatoren, en dan hoeven zij geen diagnose te stellen alleen maar oh, deze patiënt heeft wel een infectie, moet die niet bij de SNIV
43. Opl_koppelen voorschrijfsysteem Suggesties om SNIV aan het voorschrijfsysteem te koppelen en opmerkingen hierover
als je antibiotica voorschrijft komt de vraag, ja is dit een SNIV patiënt en als je dat met ja beantwoord, dat dat ergens gelijk centraal verzameld wordt, waar jij dat kunt uithalen, uitdraaien wekelijks
Terugrapportages 44. Min_ontbreken geregistreerde
info Niet alles wat je registreert komt terug in de rapportages en dat wordt als negatief ervaren
Bij het registreren moet je ook nog leeftijdscategorieën meenemen, maar die zie je nergens terug in mijn beleving.
45. min_Geen behandeling/antibiotica
Het behandelen/geven van antibiotica wordt niet meegenomen en dit wordt als negatief ervaren
ja, je kan wel heel leuk registreren, maar als je het effect niet kunt meten, dan eh ja. En je moet het koppelen eigenlijk he, ergens aan.
46. Min_onduidelijkheid over de bruikbaarheid
Geven aan dat ze niet precies weten wat ze met de terugrapportage kunnen doen
en dat ze nou niet precies wist wat ze der nou mee kon.
47. Min_Beperkte infecties Het meenemen van alleen de huidige infecties wordt als negatief ervaren
neemt niet alle infecties mee. Hé, dus dat, er zijn 4 groepen, dat is ook een beetje globaal.
48. min_Voordelen/trend kan pas na een aantal jaar
Voordelen en informatie uit de terugrapportages kan je pas na een aantal jaar zien
Dus ik denk dat wij wat meer tijd nodig hebben om het in perspectief te zien.
49. Plus_ Inzichtelijk De terugrapportages geven een goed overzicht van de infecties en trends en maken dit inzichtelijk.
toen heeft de apotheker ook bepaalde grafieken laten zien, op basis van antibiotica gebruik en dat kwam heel mooi samen met

101
die grafiek vanuit de SNIV rapportage, dus toen dacht ik ondanks dat het wel een globaal beeld is binnen de organisatie, en de SNIV geeft eigenlijk alleen een beeld over 2 afdelingen bij ons, de trend was vergelijkbaar.
50. Plus_trends in de tijd zien De mogelijkheid om na aantal jaar de trends in het eigen huis te zien wordt als positief ervaren
maar ik denk dat als wij dat over een paar jaar naast elkaar zetten, dat we het dan kunnen zien.
51. Plus_generaliserende data De generaliseerbaarheid van de resultaten wordt als positief ervaren
Op zich levert dat wel data op die gegeneraliseerd kan worden
52. Plus_ systematisch De systematische data wordt als positief ervaren Op zich levert dat wel data op die gegeneraliseerd kan worden en daarvoor is het ook systematisch.
53. Plus_visuele trg De visuele aspecte in de rapportage wordt als positief ervaren
Kijk als je alleen maar getallen hebt dan zie je dat niet, grafieken maken dingen duidelijk, dus dat vind ik wel leuk om te zien.
54. Opl_inleiding belang RIVM Sugegstied om in de terugrapportages in de inleiding iets over het belang van het RIVM en de trends die zij zien te zetten.
Welk belang heeft het RIVM bij al deze registraties en schrijf daar dan ook een leuk inleidend stukje over, in de jaarlijkse terugrapportages.
55. Opl_korter Suggesties om de rapportage korter te maken nou ja ik had opgeschreven, rapportages korter maken en meer visueel, daardoor wordt het overzichtelijk.
56. Opl_ trends naast elkaar leggen Suggesties om de trends van huizen die meerdere jaren mee doen naast elkaar te leggen
dan de trends over de jaren heen, naast elkaar zetten, dat wij de veranderingen zien.
57. Opl_inzoomen op reden voor deelname in trg
Suggesties om in het verslag in te gaan op de specifieke redenen van een organisatie om deel te nemen
wat is nou voor je organisatie de doorslaggevende reden om mee te doen? Ehm en, wellicht kan daar ook op worden ingezoomd in het verslag.
58. Opl_adviezen Suggesties om adviezen in de rapportages op te nemen
Bijvoorbeeld preventie maatregelen verhogen, dus ehm adviezen geven waardoor wij zien, van nou ja dat heeft effect. En als wij dan weer registreren, dat het dan iets verandert.
59. Opl_flexibele frequentie Suggesties om de frequentie van de terugrapportages flexibel te hebben voor de huizen
nou dat, maar dat moet je dan dus wel per huis aangeven, maar dat lijkt me voor jullie een hels karwij om elke keer per huis 2 keer per jaar te moeten doen.
60. Opl_ludiek Suggesties om de terugrapportages op ludieke wijze te rbengen
en dan is het natuurlijk wel heel erg leuk als je, zeg maar als, het RIVM, als je iets signaleert, dat ze daar een leuk plaatje of iets grappigs als laatste anekdote der bij doen.
61. Opl_meer categoriën Suggesties om mee categorieën te specificeren in de terugrapportages
als je gewoon naar de grafieken kijkt dan zie je wel dat er leeftijdscategorieën zijn, maar je ziet dat hier in de grafieken bijvoorbeeld niet thuis

102
62. Opl_overledenen koppelen aan infectie
Suggesties om de sterfgevallen ook de koppelen aan reden van overlijden
nu als je dat wel koppelt met de infecties, dus als je de vraag beantwoord, is de patiënt door infectie overleden, ja of nee.
63. Opl_ppt Suggesties om een ppt te leveren bij de terugrapportages
maar ik zou PowerPoint toch ook wel heel erg fijn vinden.
64. Opl_prgamatische oplossingen Suggesties om de terugrapportages pragmatisch te maken
denk ik dat bij de rapportage ook, dat de pragmatische oplossing heel voordelig is.
65. Opl_visueler Suggesties om te terugraportages visueler te maken rapportages korter maken en meer visueel, daardoor wordt het overzichtelijk.