be nefits guide - santa clara county, california...life and financial benefits retirement be nefits...
TRANSCRIPT

M A K I N G Y O U R D E C I S I O N S
H E A L T H
L I F E A N D F I N A N C I A L B E N E F I T S
R E T I R E M E N T
B E N E F I T S G U I D EC O U N T Y O F S A N T A C L A R A E M P L O Y E E S E R V I C E S A G E N C Y
B E G I N H E R E

The County of Santa Clara strives to provide you and your family with programs, tools, and resources to help you live a healthy life.
In this Benefits Guide, you’ll find the information you need to make your benefit elections either during annual enrollment periods or as a new hire. It’s easy to navigate the Benefits Guide if you’re viewing it online or on your mobile phone—use the icons along the top to jump to the section you want, and when you’re in a section, click or touch the subtopics. You can also click the arrows next to the page numbers to go back or forward.
We encourage you to carefully review this Benefits Guide to understand the options available to you and to enroll in the plans that best fit the needs of you and your family. Also, throughout the year, the guide can help you make informed health care decisions as you experience certain life events.
What’s New for 2017-2018 There are minimal changes to the County’s health plans for the 2017-2018 plan year:
• You’ll notice slight changes to the premium rates for medical coverage.
• We are also holding a special enrollment opportunity for theCounty’s supplemental life insurance and long-term disabilityinsurance plans. If you waived this coverage previously or would liketo increase the coverage you currently have, you may enroll now withno evidence of insurability requirement for most coverage options. Goto page 17 for details about supplemental life and page 22 for detailsabout long-term disability.
I T ' S O P E N E N R O L L M E N T — M AY 1 - 3 1 , 2 0 1 7
Instructions for enrolling are covered in the Making Your Decisions section. If you want to make benefit changes, be sure to submit the required paperwork by May 31, 2017 to your Employee Service Center. All election changes will go into effect on June 19, 2017. See page 34 for details.
< 2 >
A B O U T Y O U R C O U N T Y O F S A N T A C L A R A E M P L O Y E E B E N E F I T S
During the Open Enrollment period, we encourage you to review your benefit elections, your covered dependents, and make sure your decisions continue to meet your needs. Be sure to take a look at your current benefits available on your personalized Benefits Statement. To access your statement go to the County’s Connect website, click on the “Employment“ icon, and click on “My Benefits Statement.”
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
MEDICAL
The County of Santa Clara offers you three medical plan options. You can choose from two Health Maintenance Organization (HMO) plans and a Point of Service (POS) Plan. See the Plans at a Glance comparison chart on page 5 for highlights of key plan features and benefits.
About the HMO Plans With an HMO plan, you choose a Primary Care Physician (PCP) from a network of local healthcare professionals who will refer you to in-network specialists or hospitals when necessary. All of your healthcare is coordinated through that PCP.
You may choose the Kaiser Permanente Health Plan or Valley Health Plan. With Kaiser, you must live or work within a 30-mile radius of a Kaiser hospital. With Valley Health Plan, you must live or work in Santa Clara County.
Most services are covered at 100% with minimal or no office visit copayments. Out of network services are not covered except under life threatening emergency conditions.
About the Health Net POS Plan The Health Net Point of Service plan is a type of managed care health insurance plan that offers you a choice of different types of providers, separated into three “Tiers.” The benefits paid by the plan—and what you’ll pay out of your own pocket—will vary, based on your Tier choice when you receive your care. Here’s how it works:
Tier One: HMO Providers—You may pay the lowest share of the cost.
• Receive care from Health Net HMO providers located within a 30-mileradius of where you live or work.
• You select a Primary Care Physician (PCP) who coordinates your care andrefers you to specialists and hospitals if needed.
• You pay a $15 office visit copayment and the plan pays covered servicesat 100%.
K N O W B E F O R E Y O U G O …
The benefits provided under the POS Plan’s Tier One and Tier Two may be different than under Tier Three. For example, out of network well woman visits are not covered. Make sure you understand what’s covered—and what’s not—before you visit a provider. Contact Health Net at 800-522-0088 for details.
< 3 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
Don’t forget to take advantage of the free preventive care benefits that are offered through your County medical coverage.

H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
Tier Two: Preferred Provider Organization (PPO) Providers—You may pay more out-of-pocket.
• Receive care from a provider in a selected network of Health Netmedical doctors, hospitals, and other health care professionals (called a“PPO” network).
• Referrals for specialized care are not required.
• You pay a $20 office visit copay. Also, the plan pays 90% for manycovered services; you pay the remaining 10%.
Tier Three: Out of Network—You pay the most out-of-pocket.
• You may seek care out of network from any licensed provider.
• You need to meet a deductible for out of network care before the planbegins paying benefits.
• Then, the plan pays 70% of the charges it considers “usual, customary,and reasonable” for the services you receive. (This is also known asthe plan’s “maximum allowable amount.“ You are responsible for theremaining balance.
For more information, or to ask questions, contact your Department’s Employee Service Center or the plans directly:
Plan Customer Service Website
Kaiser Health Plan (Group 890) 800-464-4000 www.kaiserpermanente.org
Valley Health Plan (Group C, Policy A) 888-421-8444 www.valleyhealthplan.org
Health Net (Group 40785A) 800-522-0088 www.healthnet.com
< 4 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
Medical Plans at a Glance The chart below offers an overview of some of our medical plans’ features. The official plan documents offer a detailed explanation of covered services, limitations, and exclusions.
Kaiser HMO Valley Health Plan HMO Health Net POS
Type of Plan HMO—Services provided through Kaiser providers and facilities
HMO—Services provided through Valley Health Plan providers and contracted facilities
Members may use Health Net HMO or PPO network providers, or seek care out of network
Service Area Live/work with 30-mile radius of a Kaiser Hospital
Live/work in Santa Clara County To receive HMO-level benefits, live/work within a 30-mile radius of the doctor selected
Deductible None None HMO providers—NonePPO providers—None Out of Network—$200 per member/$600 per family per year
Annual Out-of-Pocket Maximum (Individual/Family)
$1,500/$3,000 $1,000/$2,000 Medical:HMO—$1,500/$4,500PPO—$2,000/$6,000Out-of-Network—$3,000/$9,000
Prescription Drug:In- and Out-of-Network— $2,000/$4,000
Medical and Prescription Drug Annual Out-of-Pocket Maximums are separate
Office Visits $10 copay No copay HMO—$15 copayPPO—$20 copayOut of Network—Plan pays 70% of the maximum allowable amount
Annual Routine Preventive Exam
No copay No copay HMO & PPO—No copayOut of Network—Covered only to age 18
Hospital Services $100 copay per admission No copay at Valley Health Plan hospitals
HMO—No copay if referred by PCPPPO—Plan pays 90% with prior authorizationOut of Network—Plan pays 70% of maximum allowable amount
Emergency Services
$35 copay at a Kaiser facility. Copay waived if admitted. Services at non-Kaiser facility are covered if deemed medically necessary. Must notify plan with 24-48 hours if you receive services from a non-Kaiser facility.
No copay in-network. Services at out of network hospitals are covered if deemed medically necessary. Must notify plan within 24-48 hours if you receives services out of network.
HMO—$50 copay at in-network hospital. PPO*—$75 copayOut of Network*—Plan pays 70% of maximum allowable amountCost sharing is waived if admitted
Urgent Care $10 copay at Kaiser facility No copay HMO—$35 copayPPO*—$50 copayOut of Network*—Plan pays 70% of maximum allowable amount
* PPO and Out of Network Services are charged at the HMO level if deemed emergent.
Continued on next page
< 5 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
Medical Plans at a Glance (Continued)
Kaiser HMO Valley Health Plan HMO Health Net POS
Prescriptions (Retail) Copay based on the type of drug and the supply you need: 30-day, 31- to 60-day, or 61- to 100-day supply
Generic—$5/$10/$15 copayBrand—$10/$20/$30 copay
No copay Generic—$5 copay for 30-day supplyBrand—$15 copay for 30-day supplyNon-Formulary—$30 copay for 30-day supply
Prescriptions(Mail order)
Generic—$5 copay for 30-day supply; $10 copay for 31- to 100-day supplyBrand—$10 copay for 30-day supply; $20 copay for 31- to 100-day supply
No copay Generic—$10 for 90-day supplyBrand—$30 for 90-day supplyNon-Formulary—$60 for 90-day supply(Maintenance medications can be obtained through mail order service or a contracted CVS pharmacy)
Chiropractic Care Not covered $10 copay, 20 visits per calendar year when referred by PCP
HMO—$5 copay, 20 visits per calendar year; plan providers contracted through American Specialty Health Plan (ASHP)PPO—Not coveredOut of Network—Not covered
Acupuncture Not covered $10 copay, 20 visits per calendar year when referred by PCP
Not covered
Covered Durable Medical Equipment
Plan pays 100% Plan pays 100% HMO—Plan pays 100%PPO—Plan pays 50%Out of Network—Not covered
Mental Health(Outpatient)
$10 copay No copay HMO—$ 15 copay PPO—$ 20 copay Out of Network—Plan pays 70% of maximum allowable amount
Mental Health (Inpatient)
$100 copay per admission No copay HMO—No copay PPO—Plan pays 90%, with prior authorization Out of Network—Plan pays 70% of maximum allowable amount
Well Woman Care No copay No copay HMO—No copay per annual visit PPO—No copay per annual visit Out of Network—Not covered
Well Baby Care No copay No copay HMO—No copay per office visit PPO—No copay per office visit Out of Network—Plan pays 70% of maximum allowable amount
< 6 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
2017-2018 HEALTH PLAN PREMIUM RATES
Medical Plan Premium Rates Your share of costs for medical coverage are based on the plan you choose and the family members you decide to cover, as follows:
• For the Kaiser and Valley Health HMO Plans, a four-tiered rate structure applies—you may choose to cover yourself only, yourself and your spouse/registered domestic partner, yourself and your child(ren), or yourself and your family.
• For the Point of Service Plan, a two-tiered rate structure applies—you may choose to cover yourself only or yourself and your family.
For most full-time coded employees, the County pays the cost of employee-only coverage for all health plans and the majority of the cost for covering your family members. Contribution structures are based on bargaining unit agreements, and your contributions are deducted from your paycheck on a pre-tax basis. Rates are subject to change each fiscal year.
If you are a full-time employee and your spouse or registered domestic partner also works for the County, all family members must enroll under one employee (subscriber), and the County will pay 100% of the family rate regardless of the health plan you choose.
Dental and Vision Plan Premium Rates The County pays the full cost of the dental and vision insurance for full-time coded employees and their eligible dependents.
Part-Time Employees Part-time employees share the cost of health, dental, vision, and basic life plans. These rates are prorated based on the number of regular hours an employee works each pay-period. Your contribution is deducted from your paycheck on a pre-tax basis. For more information on prorated costs, contact your Department’s Employee Service Center.
Payroll Deductions Employees are responsible for verifying that your payroll deductions are correct. If you experience a problem with your payroll deductions, contact your Department’s Employee Service Center immediately.
F I N D T H E 2 0 1 7 - 2 0 1 8 R AT E S
The medical plan rates, including the County’s contributions and your required bi-weekly payroll deductions, are available through the Employee Services Agency website, under “Employee Benefits.”
< 7 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

DENTAL
The County offers two dental plans to its employees:
Delta Dental With this plan you may choose a Delta Preferred Provider Organization (PPO) dentist, a Delta Premier dentist, or a non-network dentist that is a member of the California Dental Association. When you visit a Delta Dental dentist, you’ll pay a share of the contracted fee for most services. If you visit a non-network dentist, the plan pays its share of “allowable charges” for services provided and you are responsible for any balance.
Your costs are usually lower when you choose a Delta PPO dentist. Some providers may require you to complete a claim form, although most dentists will file the claim electronically for you.
Liberty Dental Liberty Dental is a Dental Health Maintenance Organization (DHMO). Similar to a medical HMO plan, you must live in the plan’s service area and receive care from participating dental providers. Copayments apply for specific services; however, there are usually no annual limits and no claim forms.
For more information, or to ask questions about dental coverage, contact your Department’s Employee Service Center or the plan directly:
Plan Customer Service Website
Delta Dental (Group 1766) 888-335-8227 www.deltadentalins.com
Liberty Dental Plan (Group 70001) 888-359-1088 https://client.libertydentalplan.com/scc
< 8 >
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

Dental Plans at a Glance The chart below provides a brief summary of each plan’s features. For additional information, covered services, limitations, and exclusions, you should consult each plan’s certificate of benefits.
Services Delta Dental Liberty Dental
Diagnostic/Preventive Plan pays 75%, you pay 25% and any balance due if you visit a non-network dentist
Plan pays 100%
Restorative Plan pays 75%, you pay 25% and any balance due if you visit a non-network dentist
Plan pays 100%
Crowns & Bridges Plan pays 75%, you pay 25% and any balance due if you visit a non-network dentist
Plan pays all but $75
Prosthodontics (dentures) Plan pays 75%, you pay 25% and any balance due if you visit a non-network dentist
Plan pays all but $100 each for upper and lower set
Annual Limits $2,000 per calendar year per member None
Orthodontic Plan pays 60% up to $2,000 lifetime per member, you pay 40% and any balance due
Plan pays all but $1,150
< 9 >
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

VISION
The County offers vision benefits from Vision Service Plan (VSP). You may select a provider from their list of optometrists or go out of network. When you make your appointment, mention to your selected provider’s office that you are a VSP member. The provider’s office will contact VSP for you and verify your eligibility.
Vision benefits cover an exam with a $20 copay and lenses every 12 months at no cost. The plan provides a $120 allowance for frames every 24 months. The plan does not cover scratch resistant coating, tinting, tinted contacts or designer frames. Some providers will offer you discounts on these items or discounts on a second pair glasses.
The plan also covers contact lenses up to $120 every 12 months in lieu of glasses, including the exam.
Contact VSP at 800-877-7195 or go to www.vsp.com to find a provider.
HEALTH CARE BONUS WAIVER
The Health Care Bonus Waiver program gives you the option to receive a taxable increase in gross wages by waiving the County’s medical coverage.
Full-time employees who elect to waive medical coverage receive $74 per pay period in taxable wages. Part-time employees who participate in this program receive a prorated amount for this benefit.
If you elect to participate in this program, you must complete the necessary paperwork and provide written documentation annually showing proof of medical coverage with an insurance program other than that provided by the County (e.g., your spouse’s employer’s plan).
< 10 >
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

Written documentation may include:
• A letter from the insurance company.
• A letter from your spouse’s or registered domestic partner’s employer.
• An annual benefits statement from another employer or insurance company.
All documentation must show current coverage for the plan year. Your health plan card is not sufficient proof of coverage.
Making Your Health Care Bonus Waiver Election • You have the opportunity elect the Health Care Bonus Waiver program
during each year’s Open Enrollment period. If you are currently participating and want to continue during the 2017-2018 plan year, you must re-elect the program; otherwise, the County will discontinue your Health Care Bonus Waiver and automatically waive your medical coverage.
• As a new hire, you’ll consider the waiver program when you make your medical plan election within 30 days of your hire date. You may elect a County-sponsored medical plan or to waive coverage. If you do not make an election, the County will automatically waive your medical coverage.
• You cannot change your Health Care Bonus Waiver election during the year unless you have a qualifying event, such as the birth of a child, death, marriage, or divorce. If you do have a qualifying event, you may change your election within 30 days of the event. Otherwise, you must wait until the program’s next Open Enrollment period to make a change.
< 11 >
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

HEALTH FLEXIBLE SPENDING ACCOUNT (HFSA)
This program allows you to set up a special account for paying out-of-pocket health expenses with tax-free dollars. You may contribute up to $2,500 per calendar year to this account.
Once established, here’s how your account works:
• You may use your funds to pay eligible expenses for you, your spouse,and your and qualified dependents, regardless of whether they areenrolled in the County’s medical, dental, and vision plans.
• The HFSA is a pre-funded benefit—this means you have access to yourfull annual election at any time during the year.
• The plan runs on a calendar year basis—so you may reimburse yourselffor expenses incurred between January 1 and December 31, 2017.
• The plan also includes a “grace period” following the end of thecalendar year. If you have funds left over, you can apply them forexpenses incurred from January 1 through March 15, 2018.
• The HFSA is administered by Navia Benefits Solutions, which chargesa $1.15 per pay period service fee for your account. (Note, you are not“double charged” this fee if you enroll in the Dependent Care AssistanceProgram as well.) The HFSA comes with a debit card; you can use it topay your providers directly for health care expenses. You can also setup an online account and submit claims online or through your mobilephone. Reimbursement payments are made via a check or direct depositto your bank account.
• Finally, with a flexible spending account, an IRS “use it or lose it” ruleapplies. Be sure to estimate the amount you want to contribute withcare. If you have money remaining in your account at the end of the planyear’s grace period, you forfeit those funds.
< 12 >
C O M M O N H F S A E L I G I B L E E X P E N S E S
The IRS determines which expenses are eligible for reimbursement. Some examples include:
• Prescription drugs
• Copays and coinsurance
• Deductibles
• Birth control
• Many over the countermedications, when prescribedby your doctor
• Dental work
• Orthodontia
• Glasses and contacts
• Chiropractic care
• Massage therapy
Refer to IRS Publication 502 for a complete list of eligible expenses.
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
Making Your HFSA Contribution Election • If you wish to participate in the HFSA, the IRS requires you to enroll and
elect your contribution amount each year.
• As noted previously, the program runs on a calendar year basis, fromJanuary 1 through December 31. Thus, during the fall of each year, you’llhave an opportunity to enroll during the annual enrollment period forFlexible Spending Accounts (typically in November). Your annual electionis deducted from your paycheck in equal increments.
• As a new hire, you may elect to participate in this program within 30 daysof your date of hire.
• You cannot change your annual election amount during the year unlessyou have a qualifying event, such as the birth of a child, death, marriage,or divorce. If you do have a qualifying event, you may change your HFSAelection within 30 days of the event. Otherwise, you must wait until theprogram’s next enrollment period to make a change.
Contact Navia Benefit Solutions at 800-669-3539 or go to www.naviabenefits.com/participants/benefits/health-care-fsa to learn more about this program.
< 13 >
H E A L T H
Medical Premium Rates Dental Vision Bonus Waiver Health FSA
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits
DEPENDENT CARE ASSISTANCE PROGRAM (DCAP)
The DCAP program allows you to set up a special account for paying dependent care services, which are necessary for you to work, with tax-free dollars. It’s a smart and convenient way to save on these expenses.
Through the program, you may reimburse yourself expenses related to:
• The care for your dependent children under age 13.
• The care for another dependent who is physically or mentally incapableof caring for him/herself; this includes elder day care.
You may contribute up to $5,000 per year to your account ($2,500 if you are married and filing separately). This limit is set by the IRS. Also note, if you participate in this program, you may not claim a Federal Income Tax Child Care Expense Credit on your tax return.
Your DCAP account works much like the Health Flexible Spending Account, as follows:
• The plan runs on a calendar year basis—so you may reimburse yourselffor expenses incurred between January 1 and December 31, 2017.
• The plan also includes a “grace period” following the end of thecalendar year. If you have funds left over, you can apply them forexpenses incurred between January 1 and March 15, 2018.
• The DCAP is administered by Navia Benefits Solutions, which chargesa $1.15 service charge per pay period fee for your account. (Note, youare not “double charged” this fee if you enroll in the HFSA as well.) Youcan set up an online account and submit claims online or through yourmobile phone. Reimbursement payments are made via a check or directdeposit to your bank account.
• Finally, with the DCAP, an IRS “use it or lose it” rule applies. Be sure toestimate the amount you want to contribute with care. If you havemoney remaining in your account at the end of the plan year’s graceperiod, you forfeit those funds.
< 14 >
C O M M O N D C A P E L I G I B L E E X P E N S E S
The IRS determines which expenses are eligible for reimbursement. Some examples include:
• Summer camp
• Day care
• After school programs
• Nanny care
• Work-related babysitting(your sitter cannot be a taxdependent)
• Elder care
Refer to IRS Publication 503 for more details regarding eligible expenses and providers.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

Making Your DCAP Contribution Election • If you wish to participate in the DCAP, the IRS requires you to enroll and
elect your contribution amount each year.
• As noted previously, the program runs on a calendar year basis, fromJanuary 1 through December 31. Thus, during the fall of each year, you’llhave an opportunity to enroll during the annual enrollment period forFlexible Spending Accounts (typically in November). Your annual electionis deducted from your paycheck in equal increments.
• As a new hire, you may elect to participate in this program within 30days of your date of hire.
• You cannot change your annual election amount during the year unlessyou have a qualifying event, such as:
› The birth of a child, death, marriage, or divorce.
› You have a change employment status.
› You move.
› There is a change in the cost of your provider’s services.
› When your child turns age 13.
› Your qualifying relative regains his/her ability for self-care.
If you have a qualifying event, you may change your DCAP election within 30 days of the event. Otherwise, you must wait until the program’s next enrollment period to make a change.
Contact Navia Benefit Solutions at 800-669-3539 or go to www.naviabenefits.com/participants/benefits/day-care-fsa to learn more about this program.
< 15 >
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

LIFE INSURANCE
Active hourly and salaried employees holding regular coded positions and working one-half time or more per week are eligible for County-sponsored life insurance.
Basic Life Insurance (Provided by the Standard Insurance Company) Employees in most bargaining units receive $25,000 of basic life insurance coverage. The County pays 100% of the cost for full-time coded employees. Part-time employees pay a prorated amount of the rate based on the number regular hours worked in each pay period.
You may designate any beneficiary for your County-provided life insurance benefits. However, it’s important to understand that California is a community property state. As such, you may want to consult with an attorney for legal advice regarding community property laws and how they apply to the distribution of your life insurance benefits.
< 16 >
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

Supplemental Life Insurance (Provided by the Standard Insurance Company) To add to your basic life insurance coverage, you may choose to purchase supplemental life insurance.
The amounts available for purchase are based on your bi-weekly salary, and you pay for the full premium cost for this coverage.
The chart below shows the different options and costs. For example:
• If your bi-weekly salary is $278.40 or less, you may elect Option I only, and your bi-weekly premium is $0.71 per pay period.
• If your bi-weekly salary falls between $576.81 and $773.60, you may elect Option 1, 2, 3, or 4, and you pay the applicable bi-weekly premium. Assuming you choose Option 3, you pay $2.02 per pay period.
• If your bi-weekly salary is above $3,855.94, you may elect Options 1 through 13, and you pay the applicable bi-weekly premium. Assuming you choose Option 10, you pay $14.31 per pay period.
Supplemental Life Insurance Premium Rates
Qualifying Bi-weekly Salary Option Coverage Amount Bi-Weekly Premium Rate
$278.40 or less 1 $31,000 $0.71
$278.41 to $382.40 2 $42,000 $1.13
$382.41 to $576.80 3 $63,000 $2.02
$576.81 to $773.60 4 $83,000 $2.66
$773.61 to $1,142.20 5 $125,000 $4.00
$1,142.21 to $1,538.45 6 $167,000 $6.01
$1,538.46 to $1,923 7 $209,000 $8.57
$1,923.01 to $2,307.69 8 $250,000 $10.25
$2,307.70 to $2,692.31 9 $299,000 $12.26
$2,692.32 to $3,076.92 10 $349,000 $14.31
$3,076.93 to $3,462.63 11 $399,000 $16.36
$3,462.64 to $3,855.93 12 $449,000 $20.65
$3,855.94 and above 13 $500,000 $29.50
< 17 >
S P E C I A L E N R O L L M E N T O P P O R T U N I T Y !
The County is offering a special enrollment opportunity for the supplemental life insurance plan during the Open Enrollment period (May 1 to 31, 2017).
If you are not currently participating, we encourage you to take a fresh look at this benefit and decide if it makes sense for you. Contact your Department’s Employee Service Center for an enrollment form.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

Making Your Supplemental Life Insurance Election—With a Special Enrollment Opportunity Between May 1-31, 2017• As noted above, your bi-weekly salary amount determines your eligibility
for the different coverage options (Options 1-13).
• You have the option to elect an “automatic increase formula” or a “fixed formula” when choosing your benefit. If you elect the “automatic increase formula,” your coverage will be updated automatically as your base salary changes as a result of a pay increase. If you choose the “fixed benefit“ option, your coverage option amount remains fixed and does not change when your salary changes.
• Your first opportunity to enroll occurs as a new hire—you may select any option you are eligible for and enroll within 30 days of your hire date. You are not required to provide “evidence of insurability” (defined in the plan's Summary Plan Description) if you enroll within your initial new hire window.
• As you continue employment with the County, you may enroll (or change your election) at any time. But if you missed your initial new hire window, you’ll be required to provide evidence of insurability.
• However, during this year’s Open Enrollment, the County is offering a special opportunity to purchase supplemental life insurance coverage or change your current coverage with limited restrictions—the evidence of insurability requirement is WAIVED for coverage Options 1 through 7 (up to $209,000). You may take advantage of this opportunity between May 1 to 31, 2017. If you are interested in enrolling in or changing your current supplemental life insurance election, contact your Department’s Employee Service Center.
< 18 >
W H AT I S E V I D E N C E O F I N S U R A B I L I T Y ?
When you sign up for certain benefits, such as life insurance and long-term disability insurance, the insurer may require you to provide information about your health status—also called “evidence of insurability.” This may include the release of your medical records and a getting a physical exam.
The Standard Insurance Company (our insurer) may ask you to complete the evidence of insurability process if:
• You do not enroll for supplemental life insurance or long-term disability insurance coverage within 30 days of your date of hire.
• If you request a change or increase to your coverage amount.
If required, the Standard Insurance Company will provide you with instructions and the form(s) needed for completing this process. It may take up to three months for an approval or denial of coverage from Standard.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

ACCIDENTAL DEATH AND DISMEMBERMENT INSURANCE
(AD&D)
(Provided by the Standard Insurance Company)To protect your family financially in the event of an accidental death or severe injury, you may choose to purchase accidental death and dismemberment insurance coverage for yourself and your spouse and children. You pay for the full premium cost for this coverage, and you may enroll or change your election at any time without restriction.
You may choose from the following coverage options:
AD&D Coverage Options
Employee Coverage Options… You select one
…PLUS decide whether you want to cover your spouse and/or children.
$10,000 The plan pays you a percentage of the value of your benefit in the event of your spouse’s and/or child’s death or covered loss (e.g., loss of sight, loss of a hand or foot) as follows:
• 60%foryourspouse—ifyouhaveaspouseonly.
• 20%perchild—ifyouhavechildrenonly.
• 50%foryourspouseand15%perchild—ifhave both a spouse and children.
A maximum benefit payout also applies:
• $250,000maxforthelossofyourspouse.
• $100,000maxforthelossofachild.
$20,000
$40,000
$60,000
$80,000
$100,000
$125,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
$450,000
$500,000
< 19 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

Your premium cost depends on the option(s) you choose. The costs are the same for full-time and part-time employees. The biweekly premium cost for coverage is:
AD&D Insurance Premium Rates
Benefit Amount Employee Only Coverage Coverage for Yourself and Your Spouse/Children
$10,000 $0.08 $0.12
$20,000 $0.16 $0.24
$40,000 $0.32 $0.48
$60,000 $0.48 $0.72
$80,000 $0.64 $0.96
$100,000 $0.80 $1.20
$125,000 $1.00 $1.50
$150,000 $1.20 $1.80
$200,000 $1.60 $2.40
$250,000 $2.00 $3.00
$300,000 $2.40 $3.60
$350,000 $2.80 $4.20
$400,000 $3.20 $4.80
$450,000 $3.60 $5.40
$500,000 $4.00 $6.00
The plan pays benefits under the following circumstances:
• In the event of death resulting from an accident, the plan pays 100% of the coverage amount.
• For of loss of a hand, foot, or eye, the plan pays 50% of the benefit amount.
• For the loss of more than one hand, foot, and/or eye, the plan pays 100% of the benefit amount.
Additional benefits and exclusions apply—refer to the plan’s certificate of benefits, available through the Employee Services Agency website, under “Accidental Death and Dismemberment Insurance.”
If you want to enroll or change your coverage, contact your Department’s Employee Service Center.
< 20 >
A D & D C O V E R A G E F O R D E P U T Y S H E R I F F S A N D C O R R E C T I O N A L O F F I C E R S
The County provides $20,000 of occupational AD&D coverage to all active to Sheriffs and Correctional Officers. Contact your Department’s Employee Service Center for more information. Also note, the plan’s certificate of benefits is available through the Employee Services Agency website, under “Accidental Death and Dismemberment Insurance.”
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits
TIME AWAY FROM WORK
Disability If you have a non-work-related illness or injury and become unable work for an extended period, the County offers disability benefits that partially replace your salary while you are away.
California State Disability Insurance (SDI)The State of California SDI program provides income replacement for eligible employees, due to their non-work-related illnesses or injuries, pregnancies, or childbirth.
The disability insurance program pays 55% of your weekly salary, up to $1,173. The benefit paid is based on the highest wages you earn during one quarter in a 12-month base period. Your claim may begin when your doctor certifies that your disability prevents you from doing your regular or customary job duties. Depending on the type of disability claim, the benefit may be paid for up to 52 weeks.
To learn more about eligibility and benefits covered through California SDI, go to www.edd.ca.gov/Disability/About_DI.htm.
There is a seven-day waiting period for disability benefits to commence. You may use sick leave and/or vacation time during this period. Then, you may integrate state disability insurance with your remaining sick leave and vacation time. One advantage of doing so is that you are paid as close to or equal to your regular pay while you are away from work. However, integration is not automatic. Within one week of your disability, you (or your designee) should notify your Department’s Employee Service Center to discuss your options. Otherwise, you may be placed on an unpaid leave of absence, which affects your pay and your medical, dental, vision, and life insurance benefits.
TA K E N O T E …
Pregnancy disability claims for most employees are covered under California’s SDI program. The typical disability period for a normal pregnancy is up to four weeks before your expected delivery date and up to six weeks (for normal delivery) or eight weeks (for Cesarean section) after the actual delivery. Following your pregnancy disability period, you may also be eligible to take an additional six weeks of leave through the California Paid Family Leave program as noted on the following page. < 21 >
Employees represented by certain bargaining units have an automatic deduction, of 1.00% of salary, up to a maximum of $100,880 taken from their bi-weekly pay for this coverage. This appears on your paycheck as CA DASDI/EE.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

Paid Family Leave (PFL) Paid Family Leave Plan is a part of California’s State Disability Insurance program (SDI). PFL provides up to six weeks of partial pay to employees who take time away from work to bond with a new child (including newly fostered and adopted children) or to care for a seriously ill family member.
The program pays 55% of an employee’s eligible salary; the minimum weekly benefit is $50; the maximum weekly benefit is $1,173.
To learn more about PFL, go to: www.edd.ca.gov/Disability/Paid_Family_Leave.htm.
Long-term Disability Insurance (Provided by the Standard Insurance Company)Most active hourly and salaried employees working one-half time or more per week are eligible for long-term disability coverage. This is a voluntary benefits plan—you pay the full premium cost for this coverage.
You may choose from two types of benefits:
1. Base Plan: This covers 66 ²/3% of your base salary. The maximum monthly salary amount considered for coverage is $22,500. The minimum monthly benefit is $216.67; the maximum monthly benefit is $15,000. Under the Base Plan, your benefit (and premium cost) automatically adjusts as your pay increases.
< 22 >
S P E C I A L E N R O L L M E N T O P P O R T U N I T Y !
The County is offering a special enrollment opportunity for the long-term disability insurance plan during the Open Enrollment period (May 1 to 31, 2017).
If you are not currently participating or would like to increase your coverage, we encourage you to take a fresh look at this benefit and decide if it makes sense for you. Contact your Department’s Employee Service Center for an enrollment form.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

2. Fixed Benefit Options: You select a benefit amount that is lower than what your monthly base salary provides. This is a fixed benefit amount and a fixed premium. If your salary increases, your benefit amount and premium will not change. You have several options to choose from, as follows:
Long-term Disability Plan—Fixed Benefit Options
Option Benefit Amount Minimum/Maximum Monthly Benefit
2 66 ²/3% of the first $2,275 of monthly base salary $216.67 minimum / $1,516.67 max
3 66 ²/3% of the first $2,600 of monthly base salary $216.67 minimum / $1,733.33 max
4 66 ²/3% of the first $2,925 of monthly base salary $216.67 minimum / $1,950 max
5 66 ²/3% of the first $3,250 of monthly base salary $216.67 minimum / $2,166.67 max
6 66 ²/3% of the first $3,574 of monthly base salary $216.67 minimum / $2,383.33 max
7 66 ²/3% of the first $3,900 of monthly base salary $216.67 minimum / $2,600 max
8 66 ²/3% of the first $4,225 of monthly base salary $216.67 minimum / $2,816.67 max
9 66 ²/3% of the first $4,875 of monthly base salary $216.67 minimum / $3,250 max
10 66 ²/3% of the first $5,850 of monthly base salary $216.67 minimum / $3,900 max
11 66 ²/3% of the first $6,500 of monthly base salary $216.67 minimum / $4,333.33 max
The bi-weekly premium cost for coverage is:
If deductions are being taken from your paycheck toward California SDI…
If deductions are NOT being taken from your paycheck toward California SDI…
The premium cost is $0.81 per $100 of your covered bi-weekly base salary.
The premium cost is $1.04 per $100 of your covered bi-weekly base salary.
Contact the Employee Benefits Department to learn more about the premium cost for the coverage level you are interested in purchasing.
Here is how the plan pays benefits:
• Benefits begin following 60 days of disability.
• The plan provides income replacement up to age 65, or Social Security Normal Retirement Age, whichever is longest.
• An age-graded benefit schedule applies for disabilities beginning at age 60 or later.
< 23 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
Your long-term disability insurance benefit payment may be reduced by other forms of income (e.g., workers compensation insurance and California State Disability Insurance payments).
The long-term disability insurance plan offered to County Executives, Physicians, and Dentists may vary from the benefits described in this guide For details, go to Employee Services Agency website, under “Long-term Disability Plan.”
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

Making Your Long-term Disability Insurance Election—With a Special Enrollment Opportunity Between May 1-31, 2017• As noted above, you may choose the base plan or one of the fixed
benefit options (Options 2-11).
• Your first opportunity to enroll occurs as you are a new hire—you may select any option and enroll within 30 days of your hire date. You are not required to provide “evidence of insurability” (defined in the plan’s Summary Plan Description) if you enroll within initial new hire window.
• As you continue employment with the County, you may enroll (or change your election) at any time. But if you missed your initial new hire window, you’ll be required to provide evidence of insurability to become insured.
• However, during this year’s Open Enrollment, the County is offering a special opportunity to purchase long-term disability insurance coverage or change your current coverage. You may enroll in the plan without evidence of insurability. However, a pre-existing condition limitation will apply during your first 12 months of coverage. Benefits will not be paid for a condition that occurred within 90 days before the coverage effective date (June 19, 2017).
You may take advantage of this special enrollment opportunity between May 1 to 31, 2017. If you are interested in enrolling in or changing your current long-term disability insurance election, contact your Department’s Employee Service Center.
< 24 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

Vacation/Scheduled Time Off (STO)Depending on your bargaining unit, employees earn Vacation or Scheduled Time Off (STO). Vacation/STO is accrued on an hourly basis, based on an eight-hour work day. Your accrued Vacation/STO is based on your years of employment with the County and the maximum allowable balance. Refer to the memorandum of agreement for your bargaining unit to see how your benefit is calculated.
When planning and taking Vacation/STO, you should talk with and secure approval from your manager.
Sick LeaveMost coded employees are eligible to accrue up to 96 hours of sick leave per year. Refer to the memorandum of agreement for your bargaining unit to see how your benefit is calculated.
Additional Types of LeavesSeveral other types of leave may be available to employees:
• Military leave—governed by the State California, for serving in the national or state military.
• Bereavement leave—in the event of the death of an immediate family member.
• Jury duty—to serve on a jury without a loss of pay.
• Leave Without Pay—may be granted to employees for up to one year.
Contact your Department’s Employee Service Center for more information.
< 25 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

HolidaysThe County observes the following holidays:
• New Year's Day
• Martin Luther King, Jr. Birthday (third Monday in January)
• Presidents’ Day (third Monday in February)
• Cesar E. Chavez’s Birthday (March 31)
• Memorial Day (last Monday in May)
• Fourth of July
• Labor Day (first Monday in September)
• Columbus Day (second Monday in October)
• Veterans’ Day (November 11)
• Thanksgiving Day and Friday after
• Christmas Day
Contact your Department’s Employee Service Center for more information.
< 26 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

ADDITIONAL BENEFITS
Gym DiscountsGym discounts for County employees are offered through the County’s Wellness Department. For the most current discounts available, visit the Wellness website on Connect.
Employee DiscountsThe County maintains a list of local businesses offering discounts to County employees. To view current offers, visit the Employee Discount Information page on Connect.
VTA Eco PassThe Eco Pass Clipper Card can be used for unlimited rides on the VTA bus or light rail systems. All eligible County employees are provided with a Clipper Card. For questions or replacement cards, please send an email to [email protected].
You will use the same Clipper card as long as you are part of the program. The County does not receive any information about how you use your card. When you retire or leave employment with the County, your card will be deactivated, but you can continue to use the card by loading personal funds to ride public transit. There is no need to return the card to the County.
The Eco Pass Clipper Card is not valid for free travel or discounts on any other transit system. However, additional fares from other agencies, including AC Transit, BART, CalTrain, Muni, and SamTrans, may be loaded on the same Clipper Card.
If you have questions about coordinating your Eco Pass Clipper Card with other transit services, you can contact Clipper customer service at [email protected] or 877-878-8883.
< 27 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
L I F E A N D F I N A N C I A L B E N E F I T S
Dependent Care Life Insurance AD&D Insurance Time Away From Work Additional Benefits

PUBLIC EMPLOYEES’ RETIREMENT SYSTEM (CalPERS)
Eligible County employees participate in the CalPERS defined benefit (DB) pension plan. The plan provides employees with a lifetime pension benefit based on a formula, rather than contributions made to a savings or 457 plan.
CalPERS pension benefits are funded through a combination of employer and employee contributions toward the plan.
• For “classic” employees in most bargaining units, the County pays the majority of the contributions required to fund plan benefits. The amount varies and is determined by bargaining unit agreement.
• “Non-classic” employees are required to pay at least half of the “normal cost” to fund their pension plan benefit.
To calculate your benefit at retirement CalPERS includes the following in its formula:
• For “classic” employees—your service credit, your “benefit factor,” and your final average compensation over a 12-month period.
• For “non-classic” employees—your service credit, your “benefit factor,” and your final average compensation over a 36-month period.
< 28 >
R E T I R E M E N T
CalPERS Deferred Compensation Plan Retiree Medical Coverage
TA K E N O T E …
As you read through this section of the Benefits Guide, note that there are two types of CalPERS members:
• Employees hired into the CalPERS system before January 1, 2013, who have not had a break in service of more than six months are considered CalPERS “classic” employees.
• Employees hired on or after January 1, 2013, are considered new or “non-classic” employees under the California Public Employees’ Pension Reform Act (PEPRA).
The plan rules vary based on your class of membership.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

The formula used to calculate your benefit is:
Service Credit—subject to applicable maximums
X Benefit Factor X
Final Average Compensation—
subject to applicable maximums
=CalPERS Retirement
Benefit
Note that your benefit factor is the percentage of pay to which you are entitled for each year of service. It is determined by your age at retirement and your membership type. Examples based on different employee types and ages are noted below.
Employee Type CalPERS Benefit Factors
Miscellaneous “Classic” Member 2.5% at age 55
Safety “Classic” Member 3% at age 50
Miscellaneous “Non-Classic” Member (hired into the CalPERS system on or after 1/1/2013)
2% at age 62, with a minimum age at retirement of 52 years
Safety CalPERS “Non-Classic” Member (hired into the CalPERS system on or after 1/1/2013)
2.7% at age 57
Here’s an example of a retirement calculation for a Miscellaneous “Non-Classic” Member, assuming retirement at age 62, with 20 years of CalPERS service and final average pay of $65,000.
Service Credit X Benefit Factor XFinal Average Compensation
=CalPERS Retirement
Benefit
20 Years X 2% X $65,000 =$26,000 per year
($2,167 per month)
This an example only— it is not a guarantee of a future benefit by CalPERS. Go to the CalPERS website at www.calpers.ca.gov to learn more about your specific retirement benefit. The site includes a benefit calculator, which you can use to estimate your benefit at different retirement ages. You can also request an official benefit estimate directly from CalPERS.
Contact your Department’s Employee Service Center if you have questions about your CalPERS contributions.
< 29 >
R E T I R E M E N T
CalPERS Deferred Compensation Plan Retiree Medical Coverage
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

DEFERRED COMPENSATION PLAN
The Deferred Compensation (DC) Plan is a defined contribution retirement savings plan that allows you to set aside compensation and defer payment of applicable federal and state taxes until you retire and take withdrawals from your account. Participating in this plan may lower your taxable income now; your tax obligation may also be lower in retirement.
You may make pre-tax contributions to this plan, up to an annual maximum limit determined each year by IRS regulations. You may change or stop your payroll contributions on a monthly basis.
The plan’s administrator is ICMA Retirement Corporation (ICMA-RC). You may invest your contributions in a variety of mutual funds and other types of investment vehicles. Making sound investment decisions is your responsibility and you can take advantage of the tools and resources offered by ICMA-RC. Go to www.icmarc.org/santa-clara.html to access forms, review plan investment options, and set up your personal account. To learn more about the investment options available to you, contact the County’s ICMA-RC representatives: Ray Ortiz, at 888-883-8571, or Rick Luerra at 866-837-9803.
If you have questions about the Deferred Compensation Plan, contact your Department’s Employee Service Center or call 408-299-5895.
< 30 >
TA K E N O T E …
Generally, you are not allowed to access your DC Plan funds while employed by the County. These funds are held in trust until you separate from service or retire. When you do, you will have various options for payout.
The DC Plan may allow you to take a loan from your account. Also, if you experience a catastrophic financial event, you may be allowed to take an emergency withdrawal from your account. However, this action is governed by very strict IRS regulations. You must pay applicable federal and state taxes on your withdrawal. If a loan is available to a participant, then an emergency withdrawal request will not be granted. For additional information on loans, contact ICMA-RC Investor Services directly at 800-669-7400.
R E T I R E M E N T
CalPERS Deferred Compensation Plan Retiree Medical Coverage
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

RETIREE MEDICAL COVERAGE
The County provides access to group health plan coverage to eligible retirees based on hire date, as follows:
• Tier 1: If you were hired on or after August 12, 1996, you are eligible for retiree medical coverage with a minimum of 2,088 days (8 years) of accrued County service.
• Tier 2: If you were hired on or after June 19, 2006, you are eligible for retiree medical coverage with a minimum of 2,610 days (10 years) of accrued County service.
• Tier 3: The hire date may vary by labor contract—in many cases, it’s on or after January 1, 2013. You are eligible for retiree medical coverage with a minimum of 3,915 days of County service (15 years).
Review your union memorandum of agreement for more details regarding eligibility.
After submitting your application to CalPERS and approximately 60 days prior to your planned retirement date, you should contact the Employee Benefits Department at 408-299-5880 or 800-541-7741 to set up an appointment to initiate enrollment in retiree medical coverage. Coverage is not automatic upon retirement; you must complete the necessary paperwork to maintain medical coverage after you retire.
For most retirees, the County pays for single coverage under the Kaiser retiree-only health plan. Retirees who elect a more expensive medical plan, or who elect to cover an eligible dependent, need to reimburse the County for the difference in the cost of the monthly premium.
< 31 >
R E T I R E M E N T
CalPERS Deferred Compensation Plan Retiree Medical Coverage
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

ELIGIBILITY
Medical If you are in a full-time or part-time coded position, you may enroll in one of the three health plans.
You may also enroll the following eligible members for coverage:
• Your current spouse.
• Your children, step children, or adopted children who are under age 26.
• Any other children under the age of 26 for whom you have legal guardianship (if legal guardianship was established prior to age 18).
• Your children, step children, adopted children, or any child you have legal guardianship for who is under the age of 26 and is incapable of self-support because of a physical or mental disability, which existed continuously prior to the age of 26 and continues to be certified as disabled on a semi-annual basis.
• Your registered domestic partner.
• Your registered domestic partner’s children if the children meet the same criteria of a child as described above.
< 32 >
K E E P Y O U R I N F O R M AT I O N U P T O D AT E
Be sure that your Department’s Employee Service Center has the most up to date information for you and your dependents. Make sure your home address is current, and that you have properly reported any additions or deletions of your eligible dependents as they occur.
M A K I N G Y O U R B E N E F I T S D E C I S I O N S
Eligibility Enrolling as a New Hire Open Enrollment Changes During the Year
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

Dental/Vision All regular hourly and salaried employees in coded positions, working one-half time or more in a week are eligible for these plans.
You may enroll the following eligible members on your dental and/or vision plan:
• Your spouse.
• Your unmarried children, step children, and adopted children who are under age 19.
• Any other unmarried children under the age of 19 entirely supported by you and for whom you have legal guardianship.
• Your unmarried children, step children, adopted children, or any child you have legal guardianship for who is over the age of 19 and is incapable of self-support because of a physical or mental disability, which existed continuously prior to the age of 19 and continues to be certified as disabled on a semi-annual basis.
• Your registered domestic partner.
• Your registered domestic partner’s children if the children meet the same criteria of a dependent child as described above.
The dental and vision plans require that dependents who reach age 19 must be full-time students in order to continue their coverage. You will need to provide proof of full-time student status to your Department’s Employee Service Center each year. If you fail to provide proof of eligibility, the County will remove the dependent from coverage.
Dependents who turn 23 and are enrolled in Delta Dental and vision coverage will be automatically removed from coverage at the end of their birth month. Dependents with Liberty Dental will be removed at age 24.
< 33 >
M A K I N G Y O U R B E N E F I T S D E C I S I O N S
Eligibility Enrolling as a New Hire Open Enrollment Changes During the Year
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

ENROLLING AS A NEW HIRE
Eligible employees have 30 days from your date of hire to enroll yourself and your eligible members in benefits. (Part-time employees may enroll in a health plan only, waive the dental and vision plan, or choose to enroll in the complete package.)
If you wait longer than 30 days from your date of hire to enroll or if you waive enrollment in your benefits, you must wait to enroll until the next annual Open Enrollment period.
The forms you need will be included with your new hire packet, or you can contact your Department’s Employee Service Center if you need copies.
ANNUAL OPEN ENROLLMENT
Open Enrollment is your once-a-year opportunity to review your health and financial benefit elections and make changes for the coming plan year. This year’s Open Enrollment period runs from May 1 to May 31, 2017.
During Open Enrollment you may choose to:
• Enroll in, waive, or change medical, dental or vision plans.
• Enroll or re-enroll in the Health Care Bonus Waiver Program—current participants must re-enroll!
• Enroll or remove eligible dependents for medical, dental, and/or vision plans. The following supporting documentation is required to enroll eligible dependents: birth certificate(s), marriage certificate, or certificate of domestic partner registry.
• Take advantage of the special enrollment opportunity for supplemental life insurance and long-term disability insurance coverage—enroll now with no evidence of insurability required!
< 34 >
Enrollment for the Health Care Flexible Spending Account and Dependent Care Assistance Program will occur during fall 2017. Elections are effective from January 1 through December 31, 2018.
M A K I N G Y O U R B E N E F I T S D E C I S I O N S
Eligibility Enrolling as a New Hire Open Enrollment Changes During the Year
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
D O N ' T M I S S T H E D E A D L I N E
If you wish to take action during Open Enrollment, contact your Department’s Employee Service Center to request the forms you need. The deadline is May 31, 2017. Your benefit elections are effective on June 19, 2017.

MAKING CHANGES DURING THE YEAR
You are not allowed to make changes to your benefits during the year unless you have a change in status such as marriage, birth, death, divorce, dissolution of domestic partnership, a dependent losing eligibility, or a change in your or your spouse’s job that affects benefits eligibility.
You must notify your Department’s Employee Service Center within 30 days of your status change. You may be allowed to change your benefits, consistent with the type of change. For example, if you have a baby, you may enroll her in your medical plan; however, you are not allowed to change from Kaiser to the POS medical plan.
Refer to the Annual Required Notices section of this guide for more information about changing your benefits mid-year.
< 35 >
M A K I N G Y O U R B E N E F I T S D E C I S I O N S
Eligibility Enrolling as a New Hire Open Enrollment Changes During the Year
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
Certain benefits allow you to make changes at any time during the year, including:
• The Deferred Compensation Plan.
• Accidental Death & Dismemberment Insurance.
• Supplemental Life and Long-term Disability Insurance.

C O N T A C T S
BENEFITS CONTACT INFORMATION
Need Help With… Contact… Phone or Website
Medical Plans Kaiser Permanente 800-464-4000 https://my.kp.org/santaclaracounty/
Valley Health Plan 888-421-8444 www.valleyhealthplan.org
Health Net 800-522-0088 www.healthnet.com/csc
Dental Plans Delta Dental 888-335-8227www.deltadentalins.com/index.html
Liberty Dental 888-359-1088 www.client.libertydentalplan/scc.com
Vision Service Plan VSP 800-877-7195www.vsp.com
Health Care Flexible Spending Account Navia Benefits Solutions 800-669-3539 www.naviabenefits.comDependent Care Assistance Program
State Disability Insurance Disability Insurance Program 800-480-3287www.edd.ca.gov
Supplemental Life Insurance The Standard Insurance Company 888-937-4783
Basic Life Insurance
AD&D Insurance
Long-term Disability Insurance
Deferred Compensation Plan ICMA— Retirement Corporation Rick Luerra—866-837-9803Ray Ortiz—888-883-8571www.icmarc.org/santa-clara.html
Public Employees Retirement System CalPERS 888-225-7377www.calpers.ca.gov
Eco Pass Commuter Program ESA—Employee Benefits [email protected]
< 36 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
C O N T A C T S
< 37 >
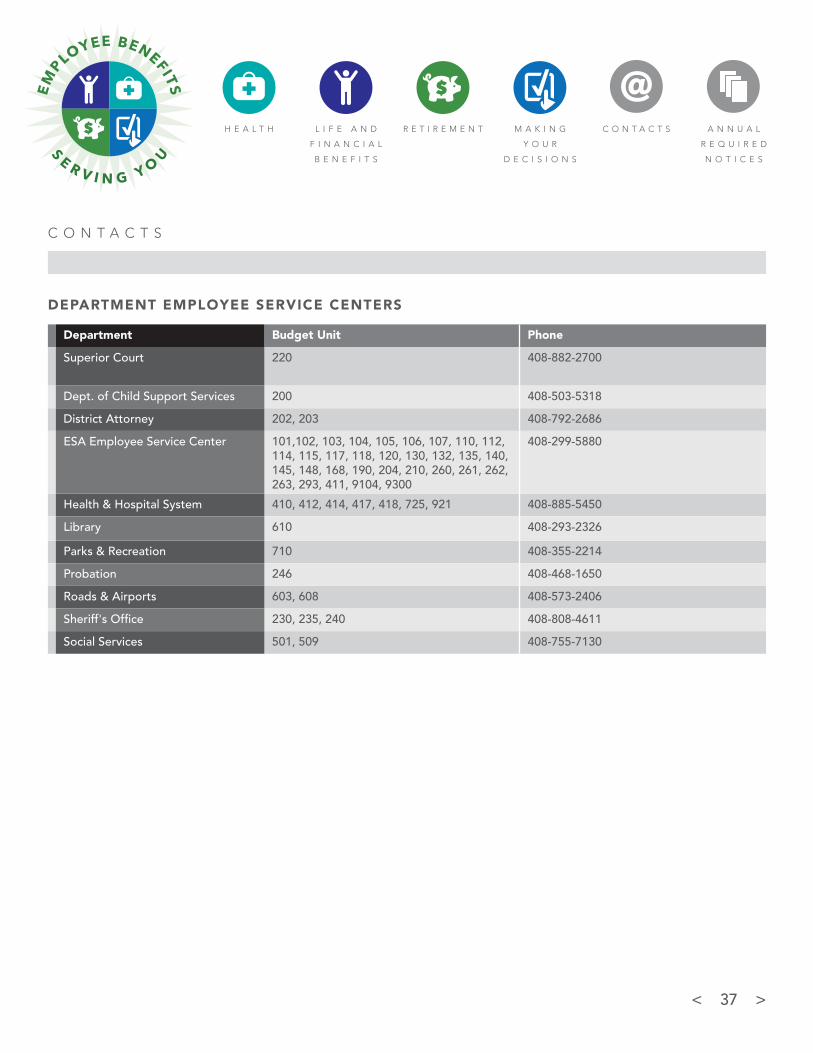
DEPARTMENT EMPLOYEE SERVICE CENTERS
Department Budget Unit Phone
Superior Court 220 408-882-2700
Dept. of Child Support Services 200 408-503-5318
District Attorney 202, 203 408-792-2686
ESA Employee Service Center 101,102, 103, 104, 105, 106, 107, 110, 112, 114, 115, 117, 118, 120, 130, 132, 135, 140, 145, 148, 168, 190, 204, 210, 260, 261, 262, 263, 293, 411, 9104, 9300
408-299-5880
Health & Hospital System 410, 412, 414, 417, 418, 725, 921 408-885-5450
Library 610 408-293-2326
Parks & Recreation 710 408-355-2214
Probation 246 408-468-1650
Roads & Airports 603, 608 408-573-2406
Sheriff's Office 230, 235, 240 408-808-4611
Social Services 501, 509 408-755-7130
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

A N N U A L R E Q U I R E D N O T I C E S
< 38 >
This document contains important employee benefit program notices of interest to you and your family. Please share this information with your family members. Some of the notices in this document are required by law and other notices contain helpful information. These notices are updated from time to time and some of the federal notices are updated each year.
This document includes the following:
• Mid-yearChangestoYourHealthCareBenefitElections
• IfYouDeclineMedicalCoverageOfferedthroughtheCounty
• IRSForm1095
• ImportantRemindertoprovidethePlanwiththeTaxpayerIdentificationNumber (TIN) or Social Security Number (SSN) of each enrollee in a health plan
• HealthInsurancePortabilityandAccountabilityAct(HIPAA)PrivacyReminder Notice
• Women’sHealthandCancerRightsActof1998(WHCRA)AnnualNoticeReminder
• AvailabilityofSummaryHealthInformation:TheSummaryofBenefitandCoverage (SBC) Document(s)
• Newborns’andMothers’HealthProtectionActNotice
• PatientProtectionRightsoftheAffordableCareAct
• FamilyandMedicalLeaveAct(FMLA)Reminder
• COBRACoverageReminder
• RemindertoKeepthePlanNotifiedofChangesinEligibilityforBenefits
• GeneralStatementofNondiscrimination:(DiscriminationisAgainsttheLaw)
• MedicareNoticeofCreditableCoverageReminder
• ImportantNoticefromtheCountyofSantaClaraaboutyourPrescriptionDrug Coverage and Medicare for 2017
• PremiumAssistanceunderMedicaidandtheChildren’sHealthInsuranceProgram (CHIP)
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
K E E P Y O U R I N F O R M AT I O N U P T O D AT E
If you have any questions regarding these notices and reminders, please contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].

A N N U A L R E Q U I R E D N O T I C E S
< 39 >
MID-YEAR CHANGES TO YOUR HEALTH CARE BENEFIT ELECTIONS
IMPORTANT: After this open enrollment period is completed, generally you will not be allowed to change your benefit elections or add/delete dependents until next years’ open enrollment, unless you have a Special Enrollment Event or a Mid-year Change in Status Event as outlined below:
Special Enrollment Event:
If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if your employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment within 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing towards the other coverage).
In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage, birth, adoption, or placement for adoption.
You and your eligible dependents may also enroll in this plan if you (or your dependents):
• havecoveragethroughMedicaidoraStateChildren’sHealthInsurance Program (CHIP) and you (or your dependents) lose eligibility for that coverage. However, you must request enrollment within 60 days after the Medicaid or CHIP coverage ends.
• becomeeligibleforapremiumassistanceprogramthroughMedicaid or CHIP. However, you must request enrollment within 60 days after you (or your dependents) are determined to be eligible for such assistance.
To request special enrollment or obtain more information, contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
Mid-Year Change in Status Event:
Because the County pre-taxes benefits we are required to follow Internal Revenue Service (IRS) regulations on if and when benefits can be changed in the middle of a plan year. The following events may allow certain changes in benefits mid-year, if permitted by the IRS:
• Changeinlegalmaritalstatus(e.g.marriage,divorce/legalseparation, death).
• Changeinnumberorstatusofdependents(e.g.birth,adoption, death).
• Changeinemployee/spouse/dependent’semploymentstatus, work schedule, or residence that affects their eligibility for benefits.
• CoverageofachildduetoaQualifiedMedicalChildSupportOrder(QMCSO).
• EntitlementorlossofentitlementtoMedicareorMedicaid.
• Certainchangesinthecostofcoverage,compositionofcoverage or curtailment of coverage of the employee or spouse’s plan.
• ChangesconsistentwithSpecialEnrollmentrightsandFMLAleaves.
• IfanemployeeiscoveredbyaCounty-sponsoredmedicalplan and the employee’s work hours are reduced so that the employee is expected to average less than 30 hours of service per month, the employee can request to be dropped from the medical plan to go enroll in the Health Insurance Marketplace or to enroll in their spouse’s group medical plan.
• IfanemployeeiscoveredbyaCounty-sponsoredmedicalplanand the employee is eligible to enroll in the Health Insurance Marketplace during its Open enrollment or Special enrollment period, the employee can request to be dropped from the medical plan to go enroll in the Health Insurance Marketplace.
You must notify the plan in writing within 30 days of the mid-year change in status event by contacting the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected]. The Plan will determine if your change request is permitted and if so, changes become effective prospectively, on the first day of the pay period, following the approved change in status event and your first premium payment (except for newborn and adopted children, who are covered back to the date of birth, adoption, or placement for adoption).

A N N U A L R E Q U I R E D N O T I C E S
< 40 >
Failure to give this Plan a timely notice (as noted above) may:
a. cause you, your Spouse and/or Dependent Child(ren) to lose the right to obtain COBRA Continuation Coverage,
b. cause the coverage of a Dependent Child to end when it otherwise might continue because of a disability,
c. cause claims to not be able to be considered for payment until eligibility issues have been resolved,
d. result in your liability to repay the Plan if any benefits are paid to an ineligible person.
IF YOU DECLINE MEDICAL PLAN COVERAGE OFFERED THROUGH THE COUNTY
The medical plan options offered by the County are considered to be minimum essential coverage (MEC) and meets the government’s minimum value standard. Additionally, the cost of medical plan coverage is intended to be affordable to employees, based on employee wages.
If you are in a benefits-eligible position and choose not to be covered by one of your employer’s medical plan options, you must maintain medical plan coverage elsewhere or you can purchase health insurance through a Marketplace (www.healthcare.gov), typically at the Marketplace annual enrollment in the fall each year.
Individuals without medical plan coverage could have to pay a penalty when they file their personal income taxes. Visit the Health Insurance Marketplace for detailed information on the individual shared responsibility payment penalty at https://www.healthcare.gov/fees-exemptions/fee-for-not-being-covered/.
If you choose to not be covered by a medical plan sponsored by the County at this enrollment time, your next opportunity to enroll for your employer’s medical plan coverage is at the next annual open enrollment time, unless you have a mid-year change event that allows you to add coverage in the middle of the County’s plan year.
IRS FORM 1095
Under the Affordable Care Act, employers (and in some cases insurance companies) are required to provide full-time employees, as well as other employees enrolled in a medical plan, with IRS Form 1095. The 1095 form should be provided to you annually.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
For each month of the calendar year that you were enrolled in a medical plan, this 1095 form documents that you (and any enrolled family members) met the federal requirement to have “minimum essential coverage or MEC,” meaning group medical plan coverage. Having minimum essential coverage means you and your family members may not have to pay a penalty when you file your personal income taxes. Visit the Health Insurance Marketplace at https://www.healthcare.gov/fees-exemptions/fee-for-not-being-covered/ for detailed information on the individual shared responsibility payment penalty.
If you receive a 1095 form, you do not need to attach the form to your personal income tax return or wait to receive the form before filling your tax return. If you receive a form this year, you should keep it in a safe place with your other tax records because you may need to produce it if requested by the IRS. (For large employers, a copy of the form 1095 will also be provided to the IRS.)
Reminder: if you have not been covered by a medical plan during the calendar year you will not receive a Form 1095. If you have been covered by various medical plans during the calendar year, you may receive more than one IRS form.
IMPORTANT REMINDER TO PROVIDE THE PLAN WITH THE TAXPAYER IDENTIFICATION NUMBER (TIN) OR SOCIAL SECURITY NUMBER (SSN) OF EACH ENROLLEE IN A HEALTH PLAN
Employers are required by law to collect the taxpayer identification number (TIN) or social security number (SSN) of each medical plan participant and provide that number on reports that will be provided to the IRS each year. Employers are required to make at least two consecutive attempts to gather missing TINs/SSNs.
If a dependent does not yet have a social security number, you can go to this website to complete a form to request a SSN: http://www.socialsecurity.gov/online/ss-5.pdf. Applying for a social security number is FREE.
If you have not yet provided the social security number (or other TIN) for each of your dependents that you have enrolled in the health plan, please contact your Department's Employee Service Center to provide this information.

A N N U A L R E Q U I R E D N O T I C E S
< 41 >
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA) PRIVACY NOTICE REMINDER
The Health Insurance Portability and Accountability Act (HIPAA) of 1996 requires health plans to comply with privacy rules. These rules are intended to protect your personal health information from being inappropriately used and disclosed. The rules also give you additional rights concerning control of your own healthcare information.
This Plan’s HIPAA Privacy Notice explains how the group health plan uses and discloses your personal health information. You can request a copy of this Notice from the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
WOMEN’S HEALTH AND CANCER RIGHTS ACT OF 1998 (WHCRA) ANNUAL NOTICE REMINDER
You or your dependents may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending physician and the patient for:
• Allstagesofreconstructionofthebreastonwhichthemastectomy was performed;
• Surgeryandreconstructionoftheotherbreasttoproduceasymmetrical appearance;
• Prostheses;and
• Treatmentofphysicalcomplicationsofthemastectomy,including lymphedema.
These benefits will be provided subject to the same deductibles, copayment and coinsurance applicable to other medical and surgical benefits provided under the various medical plans offered by the County. For more information on WHCRA benefits, contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
AVAILABILITY OF SUMMARY HEALTH INFORMATION: THE SUMMARY OF BENEFIT AND COVERAGE (SBC) DOCUMENT(S)
The health benefits available to you represent a significant component of your compensation package. They also provide important protection for you and your family in the case of illness or injury.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
As required by law, across the US, insurance companies and group health plans like ours are providing plan participants with a consumer-friendly Summary of Benefits and Coverage (SBC) as a way to help understand and compare medical plan benefits. Choosing a health coverage option is an important decision. To help you make an informed choice, the SBC, summarizes and compares important information in a standard format.
Each SBC contains concise medical plan information, in plain language, about benefits and coverage, including, what is covered, what you need to pay for various benefits, what is not covered and where to go for more information or to get answers to questions. SBC documents are updated when there is a change to the benefits information displayed on an SBC.
Government regulations are very specific about the information that can and cannot be included in each SBC. Plans are not allowed to customize very much of the SBC documents. There are detailed instructions the Plan has to follow about how the SBCs looks, how many pages long the SBC should be, the font size, the colors used when printing the SBC and even which words are to be bold and underlined.
To get a free copy of the most current Summary of Benefits and Coverage (SBC) documents for our medical plan options, contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
NEWBORNS' AND MOTHERS' HEALTH PROTECTION ACT NOTICE
Hospital Length of Stay for Childbirth: Under federal law, group health plans generally may not restrict benefits for any hospital length of stay in connection with childbirth for the mother or the newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, the Plan may pay for a shorter stay if the attending Physician (e.g., Physician, or Health Care Practitioner), after consultation with the mother, discharges the mother or newborn earlier.
Also, under federal law, plans may not set the level of benefits or out-of-pocket costs so that any later portion of the 48-hour (or 96-hour) stay is treated in a manner less favorable to the mother or newborn than any earlier portion of the stay.

A N N U A L R E Q U I R E D N O T I C E S
< 42 >
In addition, the Plan may not, under federal law, require that a Physician or other Health Care Practitioner obtain authorization for prescribing a length of stay of up to 48 hours (or 96 hours). However, to use certain providers or facilities, or to reduce your out-of-pocket costs, you may be required to obtain precertification. For information on precertification for a length of stay longer than 48 hours for vaginal birth or 96 hours for C-section, contact Health Net at 800-522-0088 or Kaiser at 800-464-4000 or Valley Health at 888-421-8444 to precertify the extended stay. If you have questions about this Notice, contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
PATIENT PROTECTION RIGHTS OF THE AFFORDABLE CARE ACT
Designation of a Primary Care Provider (PCP) and Direct Access to OB/GYN Providers:
The County-sponsored medical plans do not require the selection or designation of a primary care provider (PCP). You have the ability to visit any in-network (or non-network) health care provider; however, payment by the Plan may be less for the use of a non-network provider. To locate an in-network provider, visit www.healthnet.com/portal/home.do or www.valleyhealthplan.org or www.kaiserpermanente.org.
You also do not need prior authorization from the Plan or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology (OB/GYN), contact Health Net at 800-522-0088 or Kaiser at 800-464-4000 or Valley Health at 888-421-8444.
FAMILY AND MEDICAL LEAVE ACT (FMLA) REMINDER
The FMLA entitles eligible employees of covered employers to take unpaid, job-protected leave for specified family and medical reasons with continuation of group health insurance coverage under the same terms and conditions as if the employee had not taken leave. Employees are eligible if they
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
have worked for a covered employer for at least 12 months, have 1,250 hours of service in the previous 12 months, and if at least 50 employees are employed by the employer within 75 miles. Eligible employees are entitled to twelve (12) workweeks of leave in a 12-month period for:
• thebirthofachildandtocareforthenewbornchildwithinone year of birth;
• theplacementwiththeemployeeofachildforadoptionorfoster care and to care for the newly placed child within one year of placement;
• tocarefortheemployee’sspouse,child,orparentwhohasaserious health condition;
• aserioushealthconditionthatmakestheemployeeunableto perform the essential functions of his or her job;
• anyqualifyingexigencyarisingoutofthefactthattheemployee’s spouse, son, daughter, or parent is a covered military member on “covered active duty;” or
Twenty-six (26) workweeks of leave during a single 12-month period to care for a covered servicemember with a serious injury or illness if the eligible employee is the servicemember’s spouse, son, daughter, parent, or next of kin (military caregiver leave).
All covered employers are required to display and keep displayed a poster prepared by the Department of Labor summarizing the major provisions of The Family and Medical Leave Act (FMLA) and telling employees about their rights and responsibilities and how to file a complaint. We display the FMLA poster at our worksite. More information on FMLA is available at: http://www.dol.gov/whd/fmla/ or contact the Labor Relations Department by phone at 408-299-5880.
Certain Employee Responsibilities Related to FMLA: Employees must provide 30 days advance notice of the need to take FMLA leave when the need is foreseeable. When a 30-day notice is not possible, the employee must provide notice as soon as practicable and generally must comply with an employer’s normal call-in procedures.

A N N U A L R E Q U I R E D N O T I C E S
< 43 >
Employees must provide sufficient information for the employer to determine if the leave may qualify for FMLA protection and the anticipated timing and duration of the leave. Sufficient information may include that the employee is unable to perform job functions, the family member is unable to perform daily activities, the need for hospitalization or continuing treatment by a health care provider, or circumstances supporting the need for military family leave.
Employees also must inform the employer if the requested leave is for a reason for which FMLA leave was previously taken or certified. Employees also may be required to provide a certification and periodic recertification supporting the need for leave.
COBRA COVERAGE REMINDER
In compliance with a federal law referred to as COBRA Continuation Coverage, this plan offers its eligible employees and their covered dependents (known as qualified beneficiaries) the opportunity to elect temporary continuation of their group health coverage when that coverage would otherwise end because of certain events (called qualifying events).
QualifiedbeneficiariesareentitledtoelectCOBRAwhencertainevents occur, and, as a result of the event, coverage of that qualified beneficiary ends (together, the event and the loss of coverage are calledaqualifyingevent).QualifiedbeneficiarieswhoelectCOBRAContinuation Coverage must pay for it at their own expense.
Qualifyingeventsmayincludeterminationofemployment,reduction in hours of work making the employee ineligible for coverage, death of the employee, divorce/legal separation, or a child ceasing to be an eligible dependent child under the terms of the plan, if a loss of coverage results.
In addition to considering COBRA as a way to continue coverage, there may be other coverage options for you and your family. You may want to look for coverage through the Health Care Marketplace. See https://www.healthcare.gov/. In the Marketplace, you could be eligible for a tax credit that lowers your monthly premiums for Marketplace coverage, and you can see what your premium, deductibles, and out-of-pocket costs will be before you make a decision to enroll. Being eligible for COBRA does not limit your eligibility for Marketplace coverage or for the tax credit. Additionally, you may qualify for a special enrollment opportunity for another group health plan for which you are eligible (such as a spouse’s plan) if you request enrollment within 30 days, even if the plan generally does not accept late enrollees.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
The maximum period of COBRA coverage is generally either 18 months or 36 months, depending on which qualifying event occurred.
In order to have the chance to elect COBRA coverage after a divorce/legal separation or a child ceasing to be a dependent child under the plan, you and/or a family member must inform the plan in writing of that event no later than 60 days after that event occurs. That notice must be sent to the County’s Human Resources department via first class mail and is to include the employee's name, the qualifying event, the date of the event, and the appropriate documentation in support of the qualifying event (such as divorce documents).
If you have questions about COBRA contact the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].
REMINDER TO KEEP THE PLAN NOTIFIED OF CHANGES IN ELIGIBILITY FOR BENEFITS
You or your Dependents must promptly furnish to the County’s Employee Benefits Department by phone at 408-299-5880 or by email at [email protected] information regarding change of name, address, marriage, divorce or legal separation, death of any covered family member, birth or change in status of a Dependent Child, Medicare enrollment or disenrollment, an individual meets the termination provisions of the Plan, or the existence of other coverage. Proof of legal documentation will be required for certain changes.
Notify the Plan preferably within 31 days, but no later than 60 days, after any of the above noted events.

A N N U A L R E Q U I R E D N O T I C E S
< 44 >
Failure to give your Department's Employee Service Center timely notice of the above noted events may:
a. cause you, your Spouse and/or Dependent Child(ren) to lose the right to obtain COBRA Continuation Coverage,
b. cause the coverage of a Dependent Child to end when it otherwise might continue because of a disability,
c. cause claims to not be able to be considered for payment until eligibility issues have been resolved,
d. result in your liability to repay the Plan if any benefits are paid to an ineligible person. The Plan has the right to offset the amounts paid against the participant’s future medical, dental, and/or vision benefits.
In accordance with the requirements in the Affordable Care Act, your employer will not retroactively cancel coverage (a rescission) except when premiums are not timely paid, or in cases when an individual performs an act, practice or omission that constitutes fraud, or makes an intentional misrepresentation of material fact that is prohibited by the terms of the Plan. Keeping an ineligible dependent enrolled (for example, an ex-spouse, overage dependent child, etc.) is considered fraud. If you have questions about eligibility contact your Department's Employee Service Center.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
GENERAL STATEMENT OF NONDISCRIMINATION: (DISCRIMINATION IS AGAINST THE LAW)
The County of Santa Clara complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. The County does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex. The County:
a. Provides free aids and services to people with disabilities to communicate effectively with us, such as:
› Qualifiedsignlanguageinterpreters
› Written information in other formats (large print, audio, accessible electronic formats, other formats)
b. Provides free language services to people whose primary language is not English, such as:
› Qualifiedinterpreters
› Information written in other languages
If you need these services, contact the Labor Relations Department.
If you believe that The County has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with: Labor Relations, County Government Center, East Wing, 70 West Hedding Street, 8th Floor, San Jose, California 95110-1705. You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, the Labor Relations Department is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services, 200 Independence Avenue SW., Room 509F, HHH Building, Washington, DC 20201, 1-800-868-1019, 800-537-7697 (TDD). Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.

A N N U A L R E Q U I R E D N O T I C E S
< 45 >
Free Language Assistance: The following chart displays the top 15 languages spoken by individuals with limited English proficiency in the state of California.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S

A N N U A L R E Q U I R E D N O T I C E S
< 46 >
IMPORTANT NOTICE FROM THE COUNTY OF SANTA CLARA ABOUT YOUR PRESCRIPTION DRUG COVERAGE AND MEDICARE FOR 2017
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with the County of Santa Clara and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. All employers are required to send this notice on an annual basis. If you wish to continue with your County sponsored medical plan, no action is required.
There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare prescription drug plans provide at least a standard level of coverage set by Medicare. Some plans
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
may also offer more coverage for a higher monthly premium.
2. The County of Santa Clara has determined that the prescription drug coverage offered by Health Net, Kaiser Permanente and Valley Health Plan are, on average for all plan participants, expected to pay out as much as the standard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to December 7th.
However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
MEDICARE NOTICE OF CREDITABLE COVERAGE REMINDER
If you or your eligible dependents are currently Medicare eligible, or will become Medicare eligible during the next 12 months, you need to be sure that you understand whether the prescription drug coverage that you elect under the Medical Plan options available to you are or are not creditable with (as valuable as) Medicare’s prescription drug coverage.
To find out whether the prescription drug coverage under the County-sponsored medical plan options is or is not creditable, you should review the Plan’s Medicare Part D Notice of Creditable Coverage starting below.
It is also available from the Employee Benefits Department by phone at 408-299-5880 or by email at [email protected].

A N N U A L R E Q U I R E D N O T I C E S
< 47 >
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you and/or your dependent decide to enroll in a Medicare drug plan, you and/or your dependent will be required to drop your existing County of Santa Clara medical plan coverage. If you disenroll from a Medicare prescription drug plan anytime in the future, you will be eligible to re-enroll in a County sponsored plan within 30 days of disenrollment from the Medicare prescription drug plan or during the annual Open Enrollment period each May.
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your coverage with the County of Santa Clara and don’t enroll in a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay more (a penalty) to join a Medicare drug plan later.
If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
For More Information About This Notice Or Your Current Prescription Drug CoverageContact the County of Santa Clara Employee Benefits Office at 408-299-5880 or toll-free at 800-541-7749. Note: You will receive this notice annually and at other times in the future if the coverage through the County of Santa Clara changes. You also may request a copy of this notice at any time.
For more information about your options under Medicare prescription drug coverage…More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
• Visitwww.medicare.gov
• CallyourStateHealthInsuranceAssistanceProgramforpersonalized help (see the inside back cover of your copy of the Medicare & You handbook for their telephone number),
• Call1-800-MEDICARE(1-800-633-4227).TTYusersshouldcall1-877-486-2048.
For people with limited income and resources, extra help paying for Medicare prescription drug coverage is available. Information about this extra help is available from the Social Security Administration (SSA) online at www.socialsecurity.gov, or you can call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show that you are not required to pay a higher premium amount.

A N N U A L R E Q U I R E D N O T I C E S
< 48 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
PREMIUM ASSISTANCE UNDER MEDICAID AND THE CHILDREN’S HEALTH INSURANCE PROGRAM (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of January 31, 2017. Contact your State for more information on eligibility.
State Website Phone/Email
ALABAMA – Medicaid http://myalhipp.com/ 1-855-692-5447
ALASKA – Medicaid The AK Health Insurance Premium Payment Program:http://myakhipp.com/ Medicaid Eligibility: http://dhss.alaska.gov/dpa/Pages/medicaid/default.aspx
ARKANSAS – Medicaid Website: http://myarhipp.com/ 1-855-MyARHIPP (855-692-7447)
COLORADO – Health First Colorado (Colorado’s Medicaid Program) & Child Health Plan Plus (CHP+)
Health First Colorado: https://www.healthfirstcolorado.com/
Health First Colorado: 1-800-221-3943/ State Relay 711
CHP+: https://www.colorado.gov/HCPF/Child-Health-Plan-Plus
CHP+ Customer Service: 1-800-359-1991/ State Relay 711
FLORIDA – Medicaid http://flmedicaidtplrecovery.com/hipp/ 1-877-357-3268
GEORGIA – Medicaid http://dch.georgia.gov/medicaid Click on Health Insurance Premium Payment (HIPP)
404-656-4507
INDIANA – Medicaid Healthy Indiana Plan for low-income adults 19-64:http://www.in.gov/fssa/hip/
1-877-438-4479
All other Medicaid: http://www.indianamedicaid.com
1-800-403-0864
IOWA – Medicaid http://dhs.iowa.gov/ime/members/medicaid-a-to-z/hipp 1-888-346-9562
KANSAS – Medicaid http://www.kdheks.gov/hcf/ 1-785-296-3512
Continued on next page
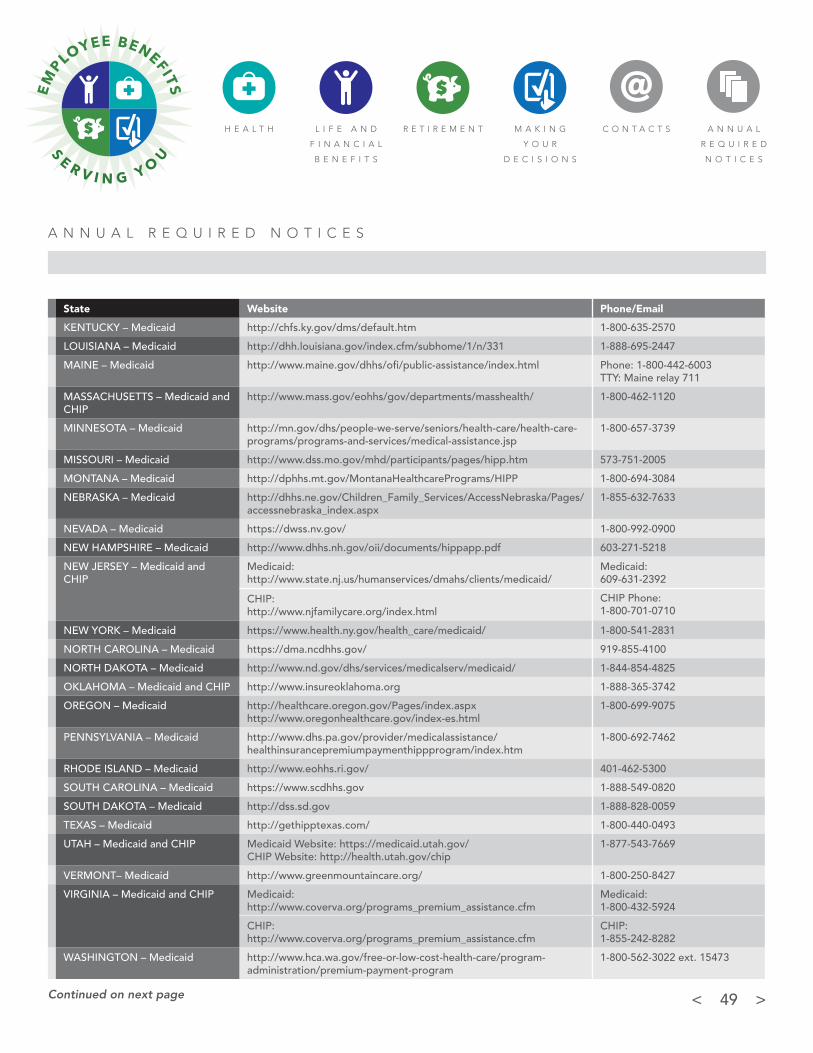
A N N U A L R E Q U I R E D N O T I C E S
< 49 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
KENTUCKY – Medicaid http://chfs.ky.gov/dms/default.htm 1-800-635-2570
LOUISIANA – Medicaid http://dhh.louisiana.gov/index.cfm/subhome/1/n/331 1-888-695-2447
MAINE – Medicaid http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-442-6003TTY: Maine relay 711
MASSACHUSETTS – Medicaid and CHIP
http://www.mass.gov/eohhs/gov/departments/masshealth/ 1-800-462-1120
MINNESOTA – Medicaid http://mn.gov/dhs/people-we-serve/seniors/health-care/health-care-programs/programs-and-services/medical-assistance.jsp
1-800-657-3739
MISSOURI – Medicaid http://www.dss.mo.gov/mhd/participants/pages/hipp.htm 573-751-2005
MONTANA – Medicaid http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP 1-800-694-3084
NEBRASKA – Medicaid http://dhhs.ne.gov/Children_Family_Services/AccessNebraska/Pages/accessnebraska_index.aspx
1-855-632-7633
NEVADA – Medicaid https://dwss.nv.gov/ 1-800-992-0900
NEW HAMPSHIRE – Medicaid http://www.dhhs.nh.gov/oii/documents/hippapp.pdf 603-271-5218
NEW JERSEY – Medicaid and CHIP
Medicaid: http://www.state.nj.us/humanservices/dmahs/clients/medicaid/
Medicaid: 609-631-2392
CHIP Phone: 1-800-701-0710
CHIP:http://www.njfamilycare.org/index.html
NEW YORK – Medicaid https://www.health.ny.gov/health_care/medicaid/ 1-800-541-2831
NORTH CAROLINA – Medicaid https://dma.ncdhhs.gov/ 919-855-4100
NORTH DAKOTA – Medicaid http://www.nd.gov/dhs/services/medicalserv/medicaid/ 1-844-854-4825
OKLAHOMA – Medicaid and CHIP http://www.insureoklahoma.org 1-888-365-3742
OREGON – Medicaid http://healthcare.oregon.gov/Pages/index.aspxhttp://www.oregonhealthcare.gov/index-es.html
1-800-699-9075
PENNSYLVANIA – Medicaid http://www.dhs.pa.gov/provider/medicalassistance/healthinsurancepremiumpaymenthippprogram/index.htm
1-800-692-7462
RHODE ISLAND – Medicaid http://www.eohhs.ri.gov/ 401-462-5300
SOUTH CAROLINA – Medicaid https://www.scdhhs.gov 1-888-549-0820
SOUTH DAKOTA – Medicaid http://dss.sd.gov 1-888-828-0059
TEXAS – Medicaid http://gethipptexas.com/ 1-800-440-0493
UTAH – Medicaid and CHIP Medicaid Website: https://medicaid.utah.gov/CHIP Website: http://health.utah.gov/chip
1-877-543-7669
VERMONT– Medicaid http://www.greenmountaincare.org/ 1-800-250-8427
VIRGINIA – Medicaid and CHIP Medicaid: http://www.coverva.org/programs_premium_assistance.cfm
Medicaid: 1-800-432-5924
CHIP: http://www.coverva.org/programs_premium_assistance.cfm
CHIP: 1-855-242-8282
WASHINGTON – Medicaid http://www.hca.wa.gov/free-or-low-cost-health-care/program-administration/premium-payment-program
1-800-562-3022 ext. 15473
State Website Phone/Email
Continued on next page

A N N U A L R E Q U I R E D N O T I C E S
< 50 >
H E A L T H L I F E A N D
F I N A N C I A L
B E N E F I T S
R E T I R E M E N T M A K I N G
Y O U R
D E C I S I O N S
C O N T A C T S A N N U A L
R E Q U I R E D
N O T I C E S
WEST VIRGINIA – Medicaid http://www.dhhr.wv.gov/bms/Medicaid%20Expansion/Pages/default.aspx
1-877-598-5820, HMS Third Party Liability
WISCONSIN – Medicaid and CHIP https://www.dhs.wisconsin.gov/publications/p1/p10095.pdf 1-800-362-3002
WYOMING – Medicaid https://wyequalitycare.acs-inc.com/ 307-777-7531
To see if any other states have added a premium assistance program since January 31, 2017, or for more information on special enrollment rights, contact either:
U.S. Department of Labor U.S. Department of Health and Human ServicesEmployee Benefits Security Administration Centers for Medicare & Medicaid Serviceswww.dol.gov/agencies/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565
Paperwork Reduction Act StatementAccording to the Paperwork Reduction Act of 1995 (Pub. L. 104-13) (PRA), no persons are required to respond to a collection of information unless such collection displays a valid Office of Management and Budget (OMB) control number. The Department notes that a Federal agency cannot conduct or sponsor a collection of information unless it is approved by OMB under the PRA, and displays a currently valid OMB control number, and the public is not required to respond to a collection of information unless it displays a currently valid OMB control number. See 44 U.S.C. 3507. Also, notwithstanding any other provisions of law, no person shall be subject to penalty for failing to comply with a collection of information if the collection of information does not display a currently valid OMB control number. See 44 U.S.C. 3512. The public reporting burden for this collection of information is estimated to average approximately seven minutes per respondent. Interested parties are encouraged to send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, Employee Benefits Security Administration, Office of Policy and Research, Attention: PRA Clearance Officer, 200 Constitution Avenue, N.W., Room N-5718, Washington, DC 20210 or email [email protected] and reference the OMB Control Number 1210-0137.
OMB Control Number 1210-0137 (expires 12/31/2019)
State Website Phone/Email

County of Santa Clara, Employee Services Agency
70 W. Hedding Street, East Wing, 8th Floor, San Jose, CA 95110
Phone 408-299-5880
Email [email protected]
https://www.sccgov.org/benefits