basic ambulance assistants (baa) activity for...
TRANSCRIPT
Basic Ambulance Assistants (BAA) Activity for 2015
Activity: EE2 (15)
General Theme: Training
Topics:
Using Checklists to Minimize Mistakes in the Field
If you don’t have a checklist you probably should
Wake County EMS Clinical checklist
Prevent Medical Errors in the Field with Cognitive Strategies
Approved for (3) Clinical Continuing Educational Units
1
EE2 (15)
Use Checklists to Minimize Mistakes in the Field
Shaughn Maxwell, EMT-P | From the June 2014 Issue | Tuesday, June 3, 2014
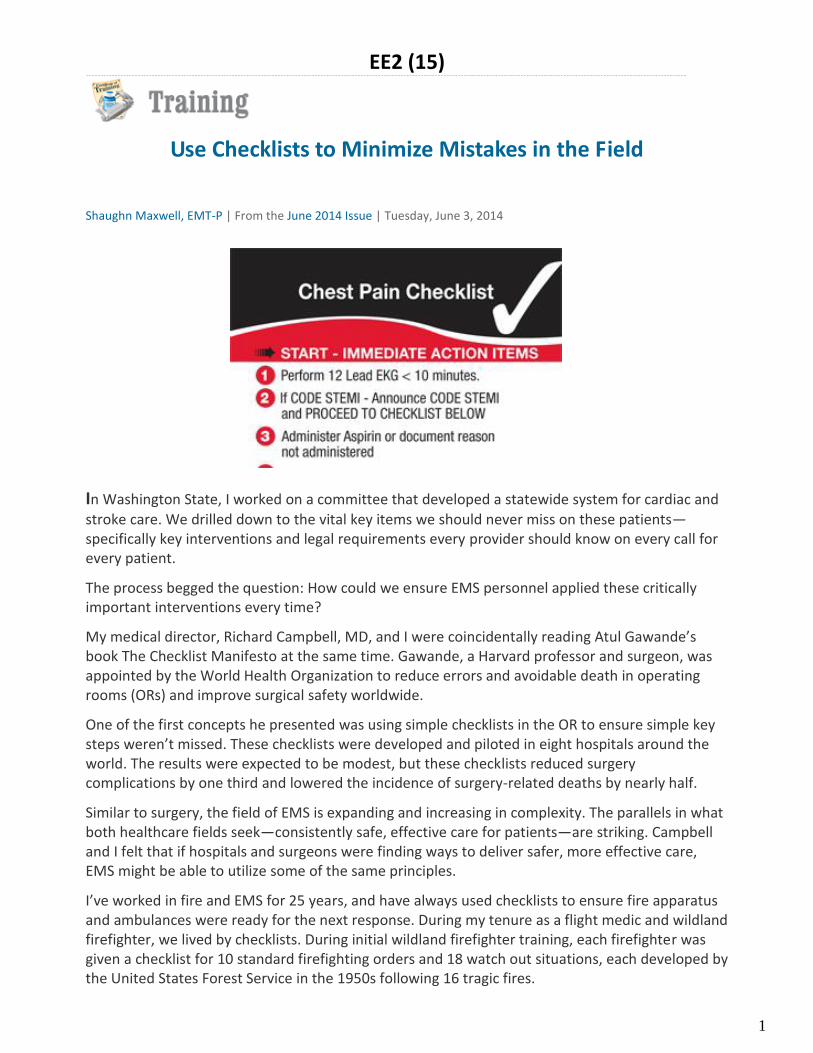
In Washington State, I worked on a committee that developed a statewide system for cardiac and
stroke care. We drilled down to the vital key items we should never miss on these patients—specifically key interventions and legal requirements every provider should know on every call for every patient.
The process begged the question: How could we ensure EMS personnel applied these critically important interventions every time?
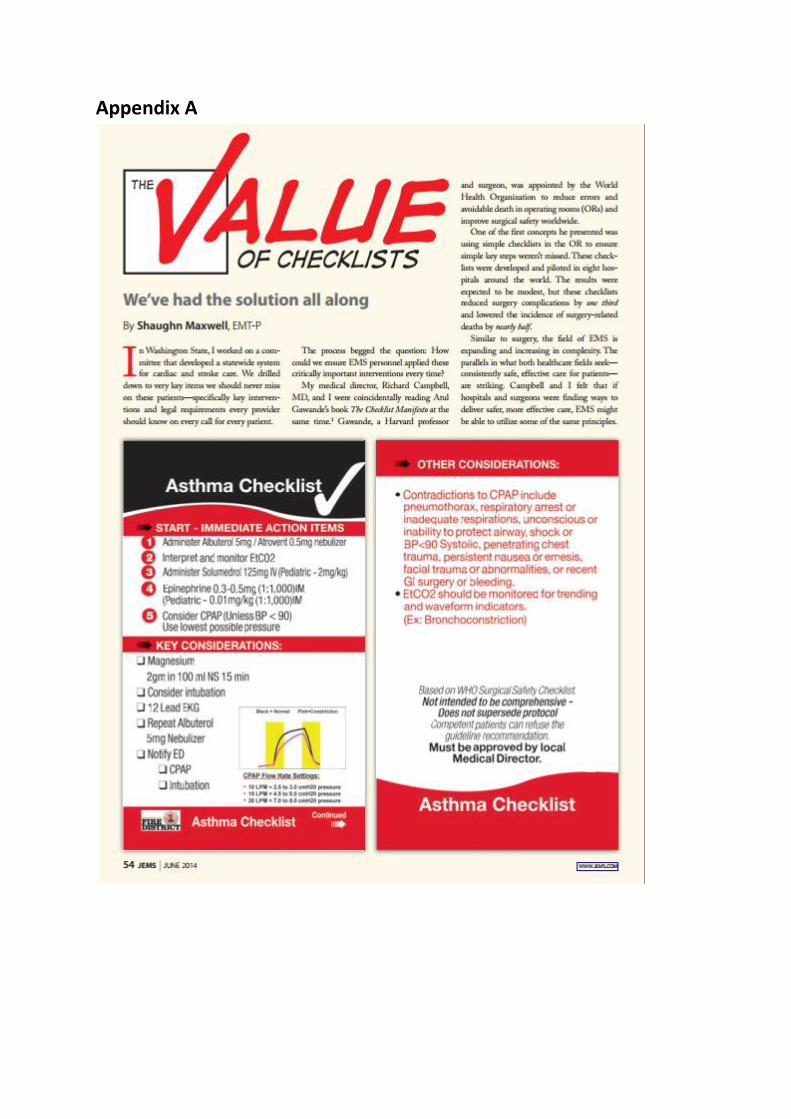
My medical director, Richard Campbell, MD, and I were coincidentally reading Atul Gawande’s book The Checklist Manifesto at the same time. Gawande, a Harvard professor and surgeon, was appointed by the World Health Organization to reduce errors and avoidable death in operating rooms (ORs) and improve surgical safety worldwide.
One of the first concepts he presented was using simple checklists in the OR to ensure simple key steps weren’t missed. These checklists were developed and piloted in eight hospitals around the world. The results were expected to be modest, but these checklists reduced surgery complications by one third and lowered the incidence of surgery-related deaths by nearly half.
Similar to surgery, the field of EMS is expanding and increasing in complexity. The parallels in what both healthcare fields seek—consistently safe, effective care for patients—are striking. Campbell and I felt that if hospitals and surgeons were finding ways to deliver safer, more effective care, EMS might be able to utilize some of the same principles.
I’ve worked in fire and EMS for 25 years, and have always used checklists to ensure fire apparatus and ambulances were ready for the next response. During my tenure as a flight medic and wildland firefighter, we lived by checklists. During initial wildland firefighter training, each firefighter was given a checklist for 10 standard firefighting orders and 18 watch out situations, each developed by the United States Forest Service in the 1950s following 16 tragic fires.

2
It would be unthinkable to arrive on scene and have a medication or piece of equipment missing. It would be equally catastrophic to run out of fuel on an emergency incident. When evaluation of vehicle checks uncovers problems, it’s often tracked back to someone not checking the equipment or supplies.
Gawande’s book inspired us. If checklists could leverage high-consequence industries like surgical medicine, air travel and nuclear power to a higher level of success, certainly we could take them beyond vehicle checks.
Checklist Development Even with thousands of hours of training and thousands of calls, EMTs and paramedics can still forget simple, key things. Who hasn’t arrived on the ramp at the hospital and realized they forgot to put oxygen on the patient or administer aspirin to a chest pain patient?
Campbell and I set out to develop checklists for our high acuity 9-1-1 calls. To start our list, we used a consensus paper published in Prehospital Emergency Care titled, “Evidence-based performance measures for emergency medical services systems: A model for expanded EMS benchmarking.”
The paper studied the best available evidence to determine which conditions are most influenced by EMS interventions. The review also evaluated which interventions had the highest potential to impact outcomes.
One specific way to measure the impact of a procedure that stood out to us was the NNT, or number needed to treat. According to its website, www.thennt.com, “The NNT offers a measurement of the impact of a medicine or therapy by estimating the number of patients that need to be treated in order to have an impact on one person. The concept is statistical, but intuitive, for we know that not everyone is helped by a medicine or intervention—some benefit, some are harmed, and some are unaffected. The NNT tells us how many of each.”
Our initial list of conditions that needed a checklist included trauma, congestive heart failure, chronic obstructive pulmonary disease, stroke, chest pain/ST-segment elevated myocardial infarction, seizures, asthma, anaphylaxis and cardiac arrest. Although these represent only 20% of our calls, they’re some of our most critical interventions.
We then determined other emerging conditions where studies or complexity indicated checklists could enhance EMS performance. Sepsis and post-resuscitation care are two examples. For example: ACLS has simplified the resuscitation process. However, post-resuscitation care has increased in complexity. So we developed a checklist for return of spontaneous circulation (ROSC).
We tested this checklist in our ACLS courses. Starting in the classroom setting, Campbell asked our paramedics to write down every action that should be performed after ROSC. Very few people could quickly list all 11 action items on our ROSC checklist.
“If this were my family member, I would expect the paramedics to remember 100% of the actions that would contribute to the best possible outcome, right?” Campbell asked the students. We then gave the class the ROSC checklist and found it created an effective, organized approach for the team and provided instant confidence for the team leader.
Checklists for high-acuity EMS situations were sent to our crews, and we later had the opportunity to share some of our success with Gawande. He was incredibly encouraging and connected me with other experts in his field to support our efforts. I felt like I was walking among giants.

3
We were also able to review Gawande’s checklists developed for use in OR crisis situations, and his results showed that checklists not only enhanced teamwork in medical crisis situations, but also reduced errors and/or missed steps by 75%. We were convinced that this must become an EMS best practice.
Confident that we were on the right path, Campbell and our team of medical services officers spent hours developing and publishing a checklist each month. This may not seem very fast, but with some checklists requiring up to 50 revisions, I realized the enormity of our mission. Good checklists require extensive knowledge, persistence and focus to develop.
(see Appendix A for a larger version of these checklists)
Conclusion Utilizing checklists is a huge paradigm shift; I describe it as giving someone the answers during the most important test: saving a life.
A few years ago, I and many colleagues were called to a once-in-a-career event. It involved an explosion, two structure fires, a wildland fire and a 50-person mass casualty incident (MCI). As

4
soon as I arrived, I was assigned to serve as the medical group supervisor and was handed the MCI board, called “the MCI checklist.” That day, everything went right and I’ll always be confident that I remembered everything—because I used a checklist.
Not every call is a once-in-career event. However, for the patient it’s potentially a once-in-a-lifetime event. The patient requires the very best care. Even if seems routine to us, checklists make sure we don’t miss anything.
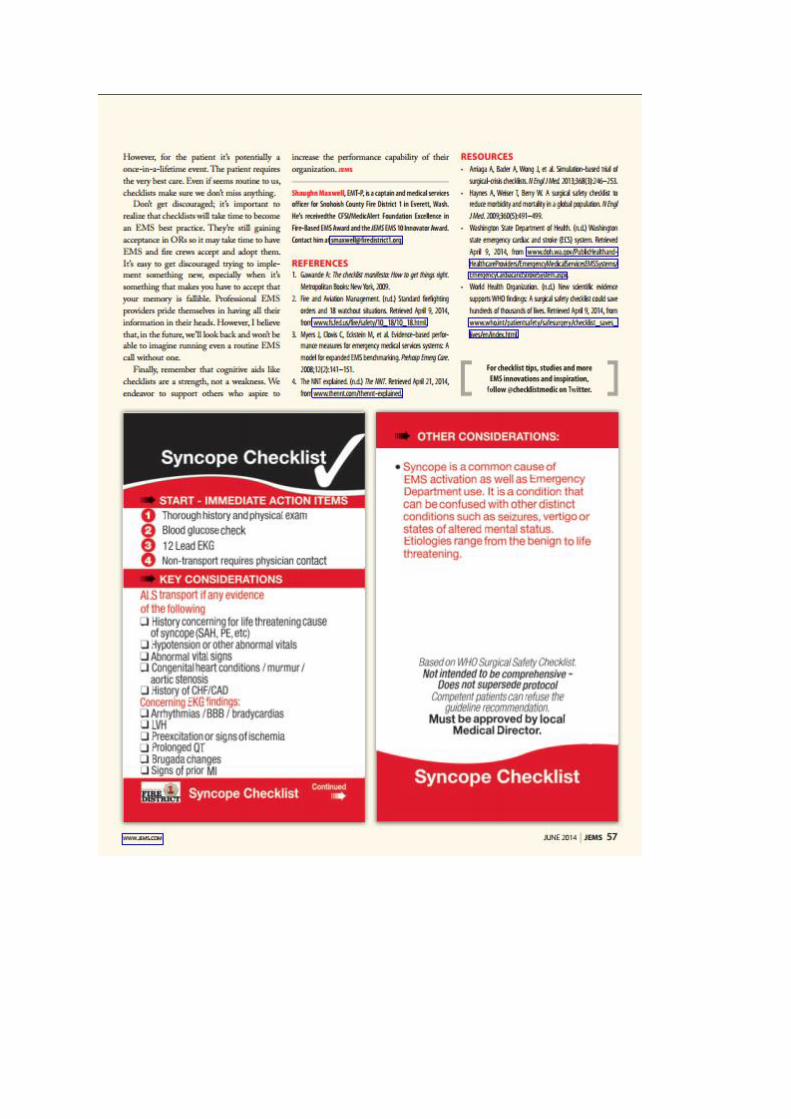
Don’t get discouraged; it’s important to realize that checklists will take time to become an EMS best practice. They’re still gaining acceptance in ORs so it may take time to have EMS and fire crews accept and adopt them. It’s easy to get discouraged trying to implement something new, especially when it’s something that makes you have to accept that your memory is fallible. Professional EMS providers pride themselves in having all their information in their heads. However, I believe that, in the future, we’ll look back and won’t be able to imagine running even a routine EMS call without one.
Finally, remember that cognitive aids like checklists are a strength, not a weakness. We endeavour to support others who aspire to increase the performance capability of their organization.
References (Available on request)
If You Don't Have a Checklist, You Probably Should BY BY RAPHAEL M. BARISHANSKY, MPH ON OCT 31, 2010
"If something so simple can transform intensive care, what else can it do?"--Atul Gawande, 2010
Checklists seem to be all the rage these days. There are checklists for managers, checklists that are
industry-specific, and even a book titled The Checklist Manifesto: How to Get Things Done Right by
Atul Gawande, MD, MPH, which states that every profession could be more effective if checklists
were used for various tasks.
As proof to Gawande's thesis, the book offers examples from several industries where safety is
paramount--specifically surgery and air travel--and there is heavy reliance on checklists to ensure
that everything is covered and covered correctly. So, do checklists have a place in EMS? Can our
operations, safety and perhaps even managerial processes benefit from this approach?
Overview
Checklists can be small or large, with varying degrees of complication depending on the specific
situation they are being developed to cover. According to Gawande, a comprehensive checklist
should be:
5
Precise
To the point
Easy to use
Only a reminder of critical steps
Practical
The essence of a checklist is taking all of the actions that go into a larger scheme-- actions that
have the potential to vary due to time, person performing the actions, day of the week, the
weather and a host of other variables--and putting them in written order so the same essential
actions happen in the same format independent of all of those aforementioned variables.
Sometimes a checklist may be essential for an event that is important but not frequently seen,
such as your EMS agency's response to a pandemic.
Examples
A good example of checklist utilization comes from Wake County (NC) EMS. Chief Skip Kirkwood
says that his EMS agency utilizes checklists to ensure that EMS providers "dot their I's and cross
their T's" in a number of clinical scenarios, including cardiac arrest management, CHF patients and
asthmatics, as well as for determining legal capacity, mental capacity and/or medical or situational
capacity. Another example of clinical checklists with a quality assurance bent comes from
the Eastern Pennsylvania EMS Council and covers a host of clinical interventions like airway
management, CHF patients, seizure management, OB/GYN emergencies, etc.
An extremely applicable checklist comes from the Monmouth-Ocean Hospital Service Corporation
(MONOC), a CAAS-accredited EMS agency in New Jersey that utilizes a comprehensive checklist to
assist supervisory personnel in investigating motor vehicle accidents in which departmental
vehicles are involved. Their checklist specifically prompts the supervisor to address various critical
points, such as seatbelt utilization, whether a traffic light was involved, whether the unit was en
route to a call or hospital at the time of the accident and weather conditions at the time, and also
reminds supervisors to take pictures of the scene.
Another checklist, developed and utilized by Lancaster County EMS providing EMS services in the
Charlotte, NC, area, specifically addresses myriad issues that field supervisors can and will face
over the course of a shift, where to funnel complaints and where in the agency personnel manual
to find information. This list is clearly specific to various supervisory responsibilities and includes
both day-to-day realities, such as location of spare equipment, checking the supervisor's unit and
overall system status, as well as more out-of-the-ordinary issues like communicating with the
media or contacting a PIO to handle media situations, coordinating mutual aid requests, and
6
knowing when to contact administration for major incidents (i.e. bomb threats, major employee
injury etc.).
Conclusion
One of the underlying elements that is recurrent throughout Gawande's book is that by looking for
the answers to simple, often overlooked questions, we can avoid potentially large mistakes.
Gawande counsels agencies to get employees to embrace checklists by assuring they are easy and
quick to use, adaptable to a variety of settings and of obvious benefit.
The use of applicable checklists in EMS agencies has the potential to take some of the risk out of
what we do. They worked for Sully Sullenberger, the pilot who landed his plane successfully on the
Hudson River. I think they can work for your EMS agency as well.
Raphael M. Barishansky, MPH, is program chief of public health preparedness for the Prince
George's County (MD) Health Department and a member of EMS World Magazine's editorial
advisory board. [email protected].

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 1
Cardiac Arrest Checklist: ____ Code Commander is identified ____ Monitor is visible and a dedicated provider is viewing the rhythm with all leads attached ____ Continuous compressions are on-going ____ O2 cylinder with oxygen in it is attached to BVM ____ Mask travels with bag, regardless of what airway is in place ____ EtCO2 waveform is present and value is being monitored ____ ITD is in place if appropriate ____ Access has been obtained (IV or IO) ____ Gastric distention is not a factor ____ Esophageal temperature probe is in place and temperature is visible ____ D50 and sodium bicarbonate have been considered and/or administered ____ Tension PTX has been considered ____ Family is receiving care and is at the patient’s side
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 2
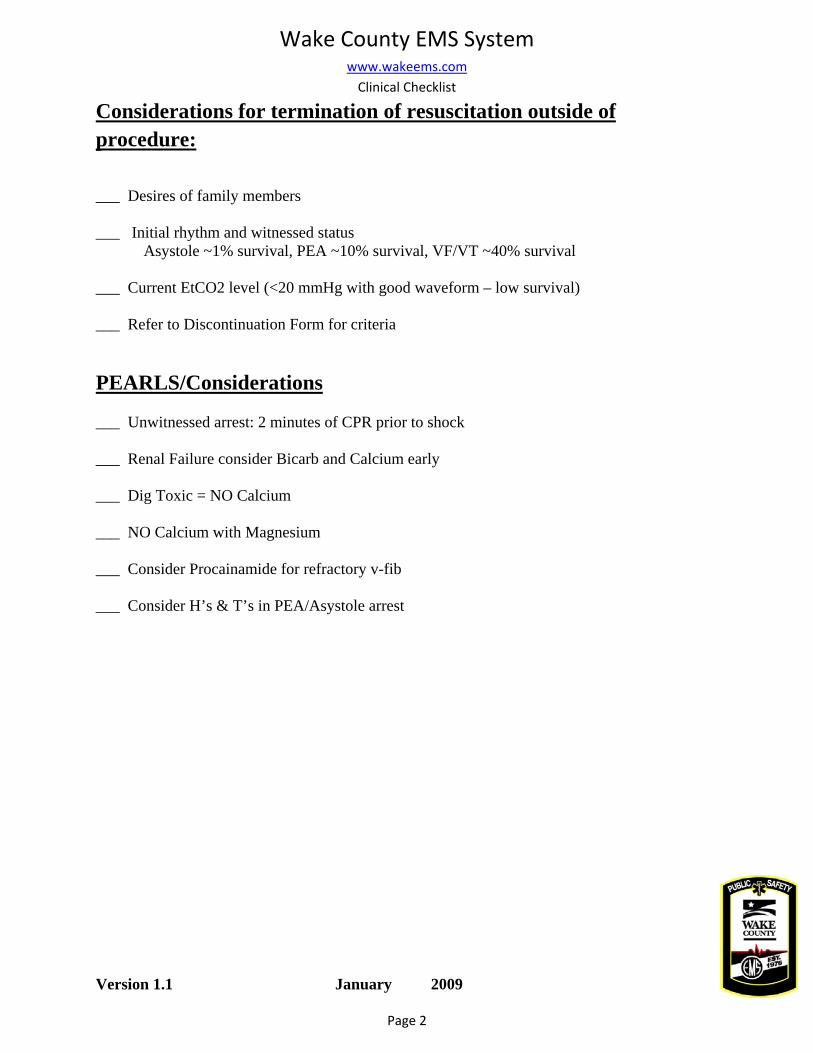
Considerations for termination of resuscitation outside of procedure:
___ Desires of family members ___ Initial rhythm and witnessed status Asystole ~1% survival, PEA ~10% survival, VF/VT ~40% survival ___ Current EtCO2 level (<20 mmHg with good waveform – low survival) ___ Refer to Discontinuation Form for criteria PEARLS/Considerations ___ Unwitnessed arrest: 2 minutes of CPR prior to shock ___ Renal Failure consider Bicarb and Calcium early ___ Dig Toxic = NO Calcium ___ NO Calcium with Magnesium ___ Consider Procainamide for refractory v-fib ___ Consider H’s & T’s in PEA/Asystole arrest
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 3
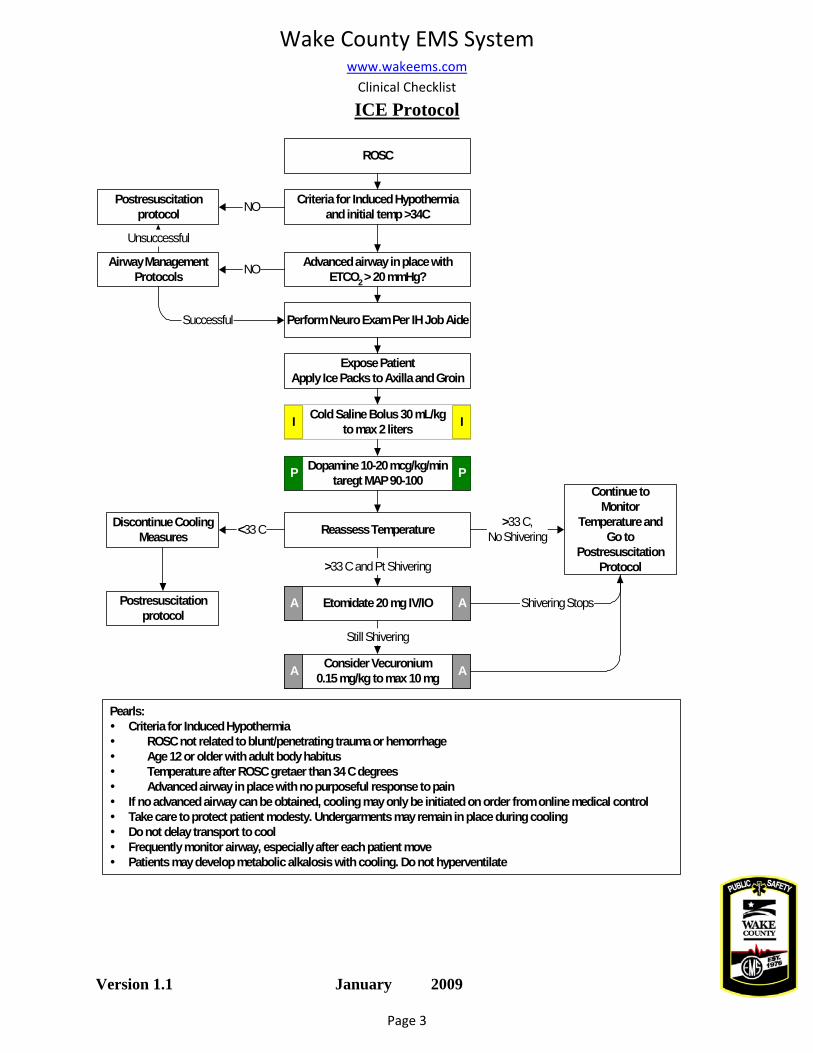
ICE Protocol
Pearls:Criteria for Induced Hypothermia
ROSC not related to blunt/penetrating trauma or hemorrhageAge 12 or older with adult body habitusTemperature after ROSC gretaer than 34 C degreesAdvanced airway in place with no purposeful response to pain
If no advanced airway can be obtained, cooling may only be initiated on order from online medical controlTake care to protect patient modesty. Undergarments may remain in place during coolingDo not delay transport to coolFrequently monitor airway, especially after each patient movePatients may develop metabolic alkalosis with cooling. Do not hyperventilate
ROSC
Consider Vecuronium0.15 mg/kg to max 10 mg
Etomidate 20 mg IV/IO
Still Shivering
Criteria for Induced Hypothermiaand initial temp >34C
Postresuscitationprotocol
Airway ManagementProtocols
Advanced airway in place withETCO2 > 20 mmHg?
NO
Perform Neuro Exam Per IH Job Aide
NO
Successful
Expose PatientApply Ice Packs to Axilla and Groin
A A
A A
Continue toMonitor
Temperature andGo to
PostresuscitationProtocol
Cold Saline Bolus 30 mL/kgto max 2 litersI I
Dopamine 10-20 mcg/kg/mintaregt MAP 90-100 PP
Reassess Temperature >33 C,No Shivering
Postresuscitationprotocol
Discontinue CoolingMeasures <33 C
>33 C and Pt Shivering
Shivering Stops
Unsuccessful

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 4
Induction of Hypothermia
Etomidate
For
Eto
mid
ate
2mg/
mL
onl
y All Patients Eligible for Induction Receive
20 mg = (10 cc)
Vecuronium
Weight Dose (mg) Volume (cc) 30 3 3 35 3.5 3.5 40 4 4 45 4.5 4.5 50 5 5 55 5.5 5.5 60 6 6 65 6.5 6.5 70 7 7 75 7.5 7.5 80 8 8 85 8.5 8.5 90 9 9 95 9.5 9.5
For
Vec
uron
ium
1m
g/m
l onl
y.
0.15
mg/
kg to
max
10m
g.
100 10 10

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 5
Trauma 1 & Alert Criteria
“Trauma 1 Due to _________________”
• BP < 90, RR < 8 • GCS < 8 • Penetrating injury to head, neck or torso • Paralysis • Airway Compromise • Respiratory Distress
OB Trauma 1 22 weeks or greater with potential for injury, or meeting alert criteria, or restrained on a long spine board Pediatric Trauma 1 Less than 12 years of age with potential for injury or meeting adult trauma 1 or trauma alert criteria Trauma Alert “Trauma Alert Due to ________________”
• Altered Mental Status (GCS 9-12) • Flail chest or multiple rib fractures • Blunt chest trauma • Abdominal pain after blunt trauma • Pelvic pain/pelvic fractures • 2 or more long bone fractures • Pulse > 120 after traumatic injury with BP > 90 • Extremity injury with potential for loss of limb • Significant vascular injuries • Burns with potential airway compromise • Age > 60 with significant mechanism of injury • Pedestrian struck by car • Ejection from vehicle • MVC with speed > 40 mph • Fall greater than 20 ft or more than 2x pt’s height
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 6
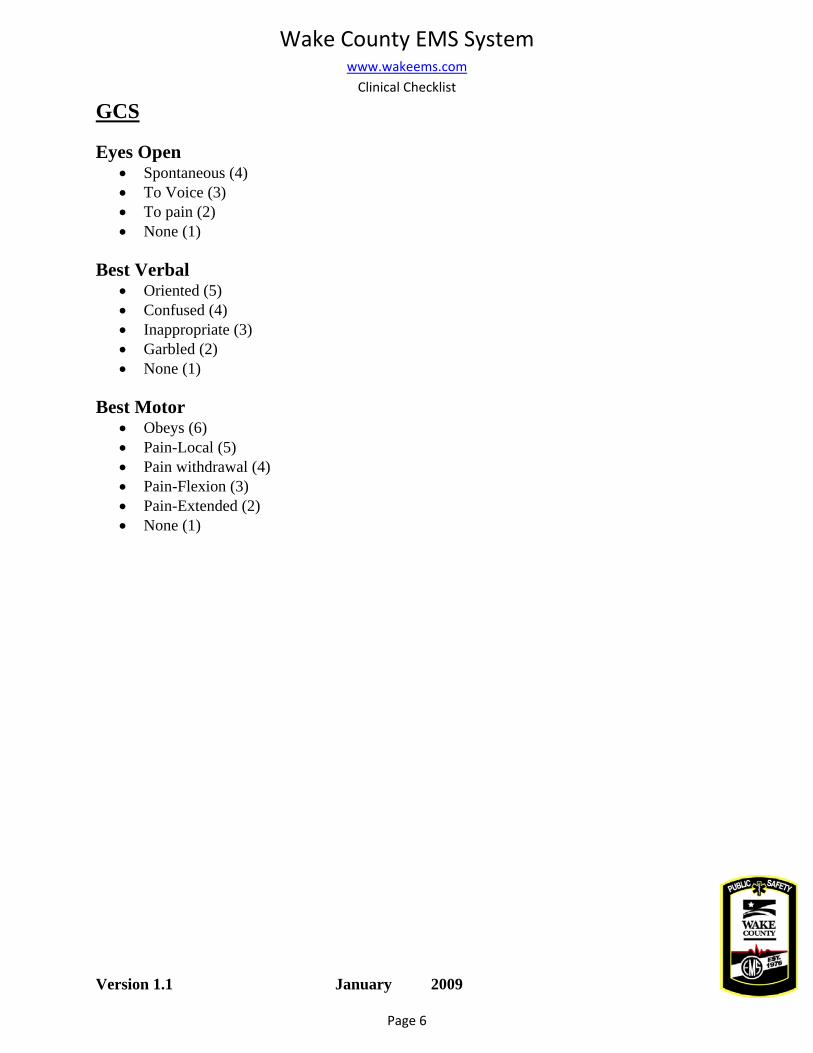
GCS
Eyes Open • Spontaneous (4) • To Voice (3) • To pain (2) • None (1)
Best Verbal
• Oriented (5) • Confused (4) • Inappropriate (3) • Garbled (2) • None (1)
Best Motor
• Obeys (6) • Pain-Local (5) • Pain withdrawal (4) • Pain-Flexion (3) • Pain-Extended (2) • None (1)

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 7
CHF Checklist
___ CPAP ___ NTG & Vasotec for HTN ___ Dopamine & Fluids for hypotension ___ 12-Lead for suspected AMI Asthma Checklist ___ CO2 & O2 readings ___ Consider Magnesium ___ Epi IV for severe cases ONLY ___ CPAP with Albuterol

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 8
Determining Capacity
___ Legal Capacity
• Ensure at least 18 years of age • If < 18 y.o. must be married or have a decree from courts • Pt’s with court decree of incapacity cannot refuse care
___ Mental Capacity
• Start with the presumption that all patients are mentally competent unless your assessment clearly indicates otherwise
• Ensure that patient is oriented to person, place, time and purpose • Establish that patient is not a danger to himself or others • Ensure that patient is capable of understanding the risks of refusing care or transportation
and any proposed alternatives • Check to be sure that patient is exhibiting no other signs or symptoms of potential mental
incapacity, including drug or alcohol intoxication, unsteady gait, slurred speech, etc. • Ask patient to echo back information you provide including:
o The lack of a complete evaluation o The risks of undiagnosed illness
___ Medical or Situational Capacity
• Ensure that patient is suffering from no acute medical conditions that might impair his or her ability to make an informed decision to refuse care or transportation
• If possible, rule out conditions such as hypovolemia, hypoxia, head trauma, unequal pupils, metabolic emergencies (e.g., diabetic issues); hypothermia, hyperthermia, etc.
• Attempt to determine if patient lost consciousness for any period of time • If any conditions above impair patient’s decision making ability, patient may not have the
capacity to refuse care and your documentation should clearly establish that the patient understood the risks, benefits and advice given to him

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 9
Cardizem (Diltiazem) Dosing
First Dose
Weight (kg) Dose (.25mg/kg) Volume (cc)
20 5 1 25 6.25 1.25 30 7.5 1.5 35 8.75 1.75 40 10 2 45 11.25 2.25 50 12.5 2.5 55 13.75 2.75 60 15 3 65 16.25 3.25 70 17.5 3.5 75 18.75 3.75
80+ 20 4
Car
dize
m (2
5mg/
5 m
l ON
LY
) Fi
rst D
ose:
0.2
5 m
g/kg
. G
ive
over
2 m
ins.
Max
20
mg
per
dose
MAX DOSE 20 mg

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 10
Cardizem (Diltiazem) Dosing cont.
Second Dose
Weight (kg) Dose (.35mg/kg) Volume (cc)
20 7 1.4 25 8.75 1.75 30 10.5 2.1 35 12.25 2.45 40 14 2.8 45 15.75 3.15 50 17.5 3.5 55 19.25 3.85
60+ 20 4
Car
dize
m (2
5mg/
5 m
l ON
LY
) Se
cond
Dos
e: 0
.35
mg/
kg.
Giv
e ov
er 2
min
s. M
ax 2
0 m
g pe
r do
se
Maximum Dose is 20 mg/dose, even at 0.35 mg/kg. For 60+ kg pt weight,
use 20 mg.
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 11
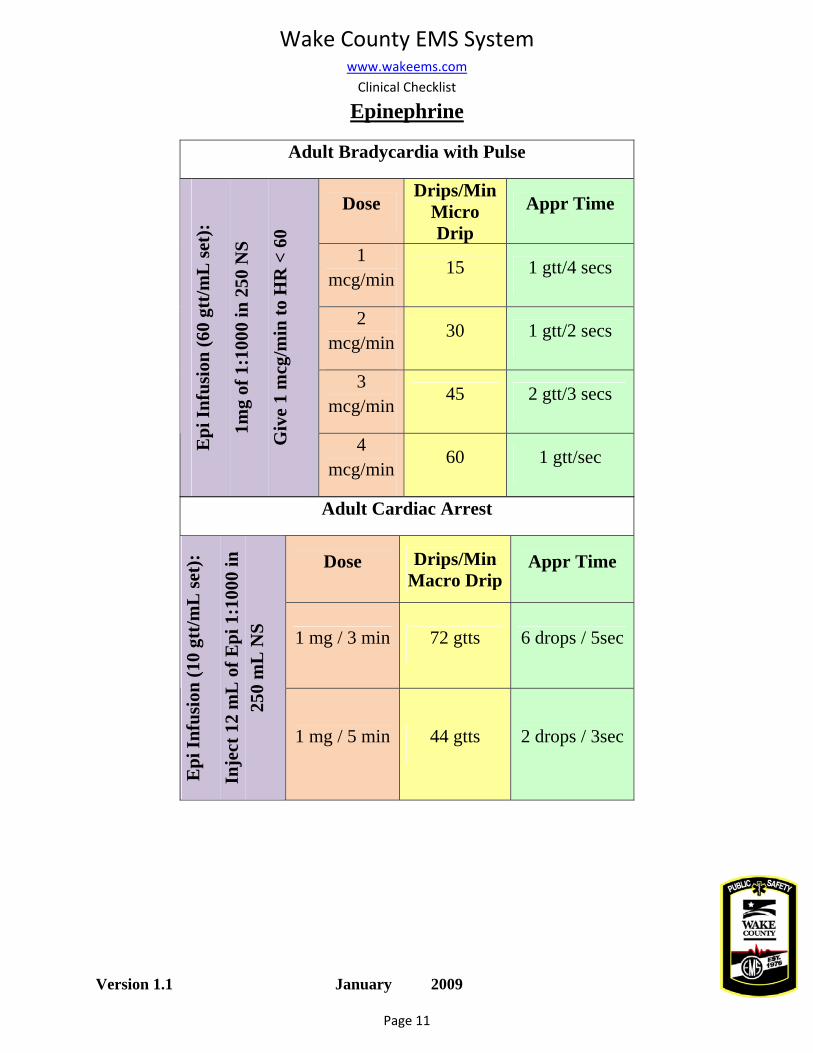
Epinephrine
Adult Bradycardia with Pulse
Dose Drips/Min
Micro Drip
Appr Time
1 mcg/min
15 1 gtt/4 secs
2 mcg/min
30 1 gtt/2 secs
3 mcg/min
45 2 gtt/3 secs
Epi
Infu
sion
(60
gtt/m
L se
t):
1mg
of 1
:100
0 in
250
NS
Giv
e 1
mcg
/min
to H
R <
60
4 mcg/min
60 1 gtt/sec
Adult Cardiac Arrest
Dose Drips/Min Macro Drip
Appr Time
1 mg / 3 min 72 gtts 6 drops / 5sec
Epi
Infu
sion
(10
gtt/m
L se
t):
Inje
ct 1
2 m
L o
f Epi
1:1
000
in
250
mL
NS
1 mg / 5 min 44 gtts 2 drops / 3sec
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 12
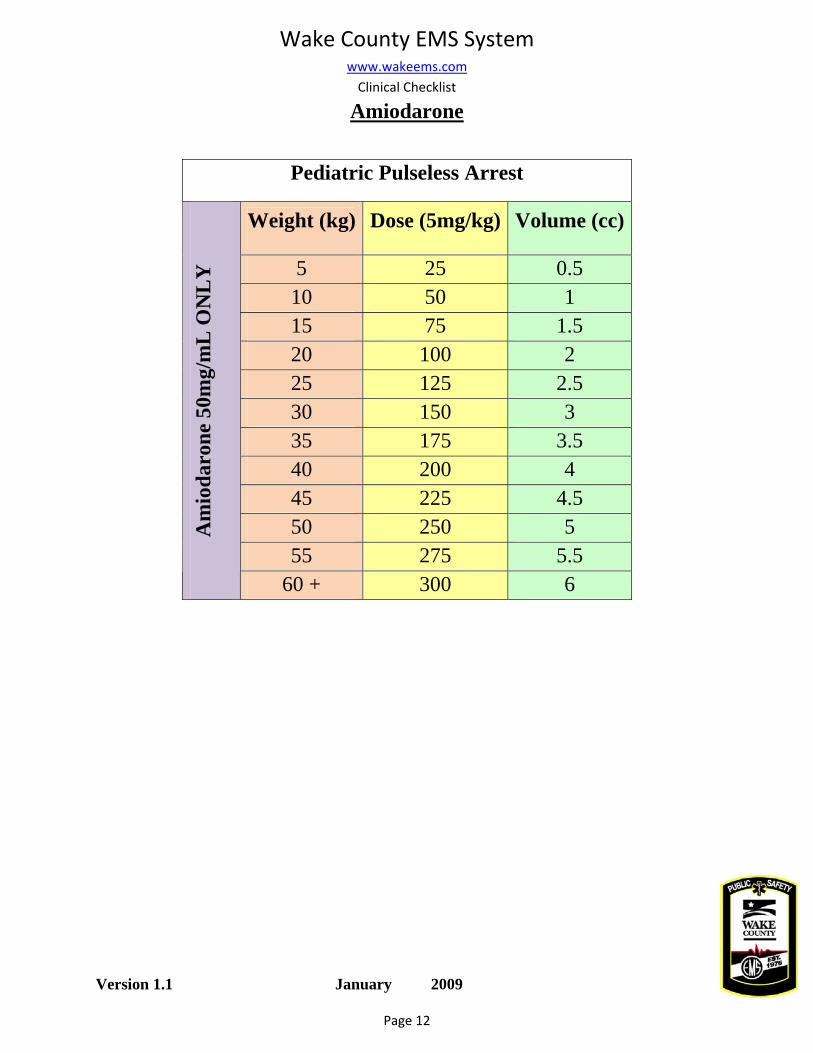
Amiodarone
Pediatric Pulseless Arrest
Weight (kg) Dose (5mg/kg) Volume (cc)
5 25 0.5 10 50 1 15 75 1.5 20 100 2 25 125 2.5 30 150 3 35 175 3.5 40 200 4 45 225 4.5 50 250 5 55 275 5.5
Am
ioda
rone
50m
g/m
L O
NL
Y
60 + 300 6
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 13
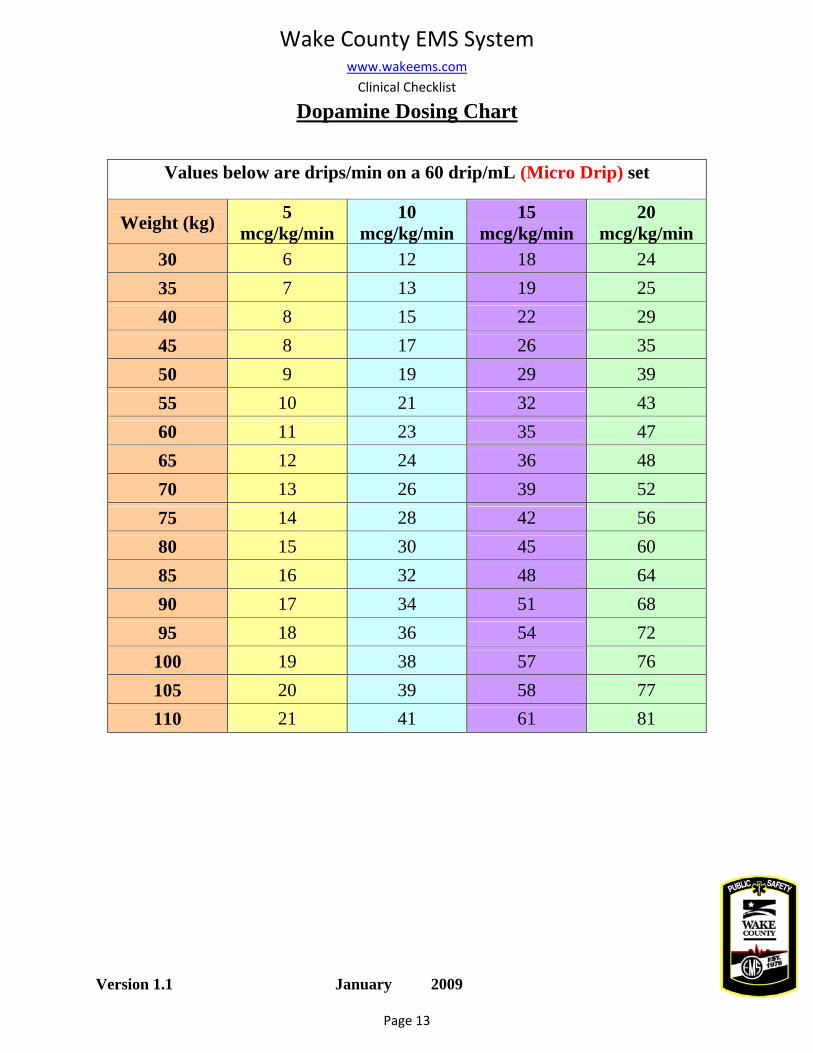
Dopamine Dosing Chart
Values below are drips/min on a 60 drip/mL (Micro Drip) set
Weight (kg) 5 mcg/kg/min
10 mcg/kg/min
15 mcg/kg/min
20 mcg/kg/min
30 6 12 18 24 35 7 13 19 25 40 8 15 22 29 45 8 17 26 35 50 9 19 29 39 55 10 21 32 43 60 11 23 35 47 65 12 24 36 48 70 13 26 39 52 75 14 28 42 56 80 15 30 45 60 85 16 32 48 64 90 17 34 51 68 95 18 36 54 72
100 19 38 57 76 105 20 39 58 77 110 21 41 61 81

Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 14
Dopamine Dosing Chart Cont.
Approx. Timing on a 60 drip/mL (Micro Drip) set from calculations above
Weight (kg) 5 mcg/kg/min
10 mcg/kg/min
15 mcg/kg/min
20 mcg/kg/min
30 1 drip/10 secs 1 drip/5 secs 1 drip/ 3 secs 2 drips/5 secs
35 1 drip/10 secs 1 drip/5 secs 1 drip/ 3 secs 2 drips/5 secs
40 1 drip/8 secs 1 drip/4 secs 2 drips/ 3 secs 1 drip/2 secs
45 1 drip/8 secs 1 drip/4 secs 2 drips/3 secs 1 drip/2 secs
50 1 drip/6 secs 1 drip/ 3 secs 1 drip/2 secs 2 drips/3 secs
55 1 drip/6 secs 1 drip/ 3 secs 1 drip/2 secs 2 drips/3 secs
60 1 drip/6 secs 1 drip/3 secs 1 drip/2 secs 4 drips/5 secs
65 1 drip/5 secs 2 drips/5 secs 3 drips/5 secs 4 drips/5 secs
70 1 drip/5 secs 2 drips/5 secs 2 drips/3 secs 4 drips/5 secs
75 1 drip/4 secs 1 drip/2 secs 2 drips/3 secs 1 drip/ sec
80 1 drip/4 secs 1 drip/2 secs 3 drips/4secs 1 drip/sec
85 1 drip/4 secs 1 drip/2 secs 4 drips/5secs 1 drip/sec
90 1 drip/4 secs 1 drip/2 secs 4 drips/5secs 1 drip/sec
95 3 drips/10 secs 3 drips/5 secs 1 drip/sec 6 drips/5 secs
100 1 drip/3 secs 2 drips/3 secs 1 drip/sec 6 drips/5 secs
105 1 drip/3 secs 2 drips/3 secs 1 drip/sec 4 drips/3 secs
110 1 drip/3 secs 2 drips/3 secs 1 drip/sec 4 drips/3 secs
Wake County EMS System
www.wakeems.com Clinical Checklist
Version 1.1 January 2009
Page 15
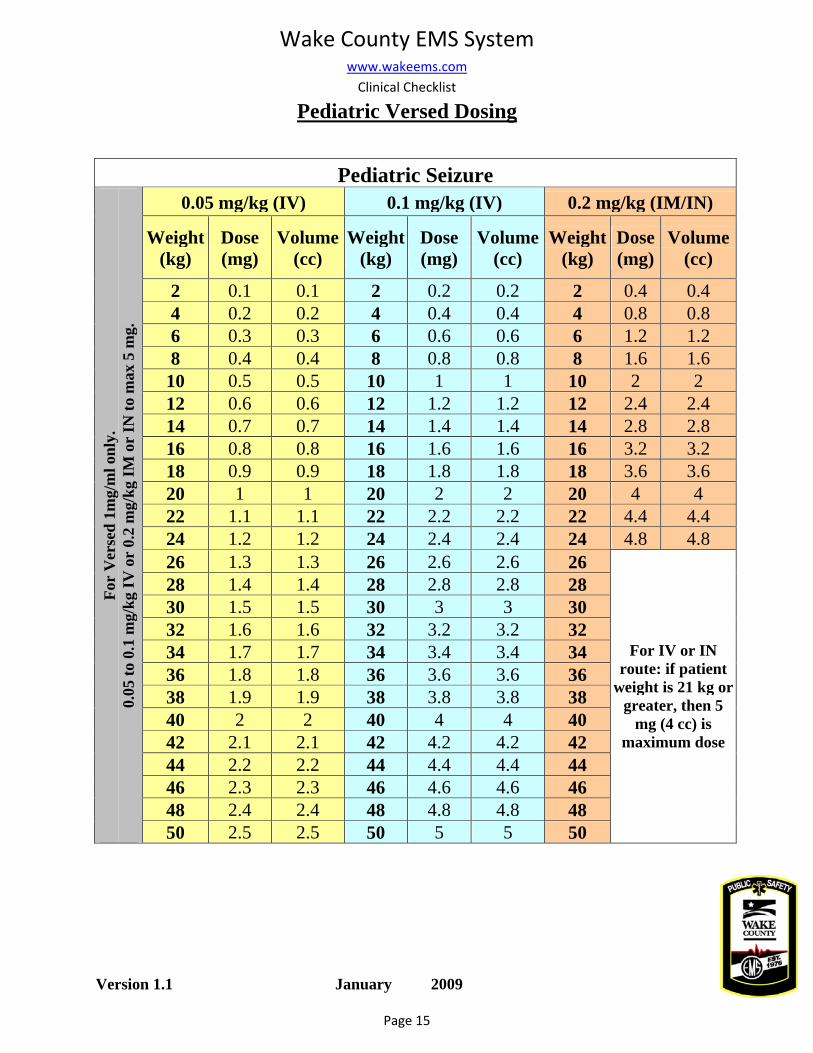
Pediatric Versed Dosing
Pediatric Seizure 0.05 mg/kg (IV) 0.1 mg/kg (IV) 0.2 mg/kg (IM/IN)
Weight (kg)
Dose (mg)
Volume (cc)
Weight (kg)
Dose (mg)
Volume (cc)
Weight (kg)
Dose(mg)
Volume (cc)
2 0.1 0.1 2 0.2 0.2 2 0.4 0.4 4 0.2 0.2 4 0.4 0.4 4 0.8 0.8 6 0.3 0.3 6 0.6 0.6 6 1.2 1.2 8 0.4 0.4 8 0.8 0.8 8 1.6 1.6
10 0.5 0.5 10 1 1 10 2 2 12 0.6 0.6 12 1.2 1.2 12 2.4 2.4 14 0.7 0.7 14 1.4 1.4 14 2.8 2.8 16 0.8 0.8 16 1.6 1.6 16 3.2 3.2 18 0.9 0.9 18 1.8 1.8 18 3.6 3.6 20 1 1 20 2 2 20 4 4 22 1.1 1.1 22 2.2 2.2 22 4.4 4.4 24 1.2 1.2 24 2.4 2.4 24 4.8 4.8 26 1.3 1.3 26 2.6 2.6 26 28 1.4 1.4 28 2.8 2.8 28 30 1.5 1.5 30 3 3 30 32 1.6 1.6 32 3.2 3.2 32 34 1.7 1.7 34 3.4 3.4 34 36 1.8 1.8 36 3.6 3.6 36 38 1.9 1.9 38 3.8 3.8 38 40 2 2 40 4 4 40 42 2.1 2.1 42 4.2 4.2 42 44 2.2 2.2 44 4.4 4.4 44 46 2.3 2.3 46 4.6 4.6 46 48 2.4 2.4 48 4.8 4.8 48
For
Ver
sed
1mg/
ml o
nly.
0.
05 to
0.1
mg/
kg IV
or
0.2
mg/
kg IM
or
IN to
max
5 m
g.
50 2.5 2.5 50 5 5 50
For IV or IN route: if patient
weight is 21 kg or greater, then 5
mg (4 cc) is maximum dose
7
Prevent Medical Errors in the Field with Cognitive Strategies
Aaron K. Sibley, MD, FRCPC | David Fu, MD | Rob Woods, MD, FRCPC | From the December 2014 Issue | Thursday,
December 4, 2014
Photo: Don’t force pieces of evidence to support your initial diagnosis. Take the time to take into account all vital
signs and aspects of the scene. Photo Kevin Link
EMS is dispatched to the home of an 82-year-old female with a chief complaint of shortness of
breath. On arrival, the crew learns she has had a dry cough for a week and is now complaining of significant malaise and shortness of breath when she lies flat, but denies any chest pain.
On examination, they find her respirations to be laboured, but she’s not in severe distress. Vital signs are: heart rate of 114 beats per minute (sinus rhythm), respiratory rate of 28 breaths per minute, blood pressure of 154/105 mmHg, oral temperature of 99.5 degrees F, and O2 saturation is 90% on room air.
On auscultation of the lungs, crackles are heard at both bases. Suspecting the patient of having heart failure, the paramedics examine her legs and find mild peripheral edema.
A large number of prescription medication bottles are found near the patient’s bedside, most of them cardiovascular medications: hydrochlorothiazide, ramipril and metoprolol.
Based on a presumptive diagnosis of heart failure, 40 mg of furosemide is administrated by IV. On ED arrival, the EMS crew mentions to the on-duty resident that the “fluid-loaded patient” is hypoxic, and may need more diuretic.
Shortly after, the patient develops a temperature of 103.3 degrees F and a chest X-ray shows left lower lobe pneumonia. Unfortunately, by this time, the patient’s kidneys have suffered some initial injury from the IV furosemide and she requires fluid resuscitation for the next week in hospital.
Introduction Prehospital healthcare providers face difficult circumstances every day in their role as emergency responders, dealing with people in their most vulnerable states and often at the pinnacle of emotional intensity. While EMTs and paramedics have been trained to operate in such high-stress environments, they’re ultimately human, and thus make mistakes.
This article discusses the types of medical errors that may occur in prehospital healthcare and suggests ways EMS providers may prevent them from occurring.

8
The Scope of Medical Errors in Healthcare Adverse events have been described as unintended complications caused by healthcare management that result in death, disability or prolonged hospital stay.1 The Canadian Adverse Events Study estimated that in 2000, 185,000 adverse events occurred in acute care patients admitted to Canadian hospitals.1 It’s estimated 70,000 of all adverse events in this population were preventable.
Although it may be comforting that the majority of these events didn’t result in long-term impairment or disability, it’s alarming that 15% of them resulted in death.1 The statistics are even more staggering in the United States. The landmark report “To Err is Human” stated that as many as 98,000 Americans die in hospitals each year as a result of medical error, exceeding deaths caused by car crashes, breast cancer and AIDS.2
Unfortunately, the problem isn’t getting better. Follow-up studies tracking American hospitals between 2001 and 2007 showed no improvement in medical error despite efforts in improving patient safety.3
Medical error has become so prevalent some researchers fear the predictable and widespread nature of adverse events has made itself commonplace. Such a perception could potentially result in inaction and the continued suffering of patients.
EMS Medical Errors Not surprisingly, the ED is often the apex of medical error occurrence. Recent multi-centre studies have determined that rates of medical error in EDs were higher than expected, even with efforts made in patient safety.
Experts argue conditions in the ED cause it to be error-prone. The concurrent management of high volumes of patients and significant diagnostic uncertainty, matched with frequent disturbances, a hectic work environment, staff fatigue and circadian dyschronicity, presents the perfect storm for medical errors to occur.
Prehospital care providers face similar challenges. One study determined the majority of errors committed and reported by prehospital care providers were related to clinical judgment (54%), rather than skill-based (21%) or medication errors (15%).
As with other healthcare workers, prehospital healthcare providers make errors in diagnosis, medication administration and procedures.9–14 Additionally, in a study of the prevalence of error in the prehospital setting, Hobgood determined that while prehospital health providers demonstrated the capacity to identify and disclose error, there was question as to whether error-identifying skills were applied in practice homogeneously.
From this, we may predict the volume and impact of prehospital error might be largely underrepresented.
Types of Medical Errors Typically encountered medical errors can be categorized into three types: procedural, affective and cognitive.
Procedural error: These occur during technical procedures such as IV cannula insertion or endotracheal (ET) intubation. Individuals who have limited experience with the procedure often make procedural errors. Once the individual is familiar with and repeats the procedure, the rate of error usually decreases. In this regard, procedural error might be mitigated by simulations, supervised practice and/or experience over time.

9
Affective error: These occur as a result of emotions, such as assuming a known alcoholic patient is unresponsive because they’re intoxicated, when in reality they may have a serious unrelated condition such as a subdural hematoma secondary to trauma.
Because the clinician’s judgment is clouded by emotion, the best and most logical course of action may be ignored for something more in line with the emotional response. The potential solution for affective errors is to recognize and be aware of the emotion and act accordingly.
Cognitive error: Cognition is the scientific word for “the process of thought.” Thus, cognitive errors are made during the thought process. Research into cognitive error has been quite extensive, likely due to its potential for prevention. However, there’s still limited insight into specific preventative strategies for cognitive error.
Cognitive errors are further subdivided into skill-based, rule-based and knowledge-based errors.
Skilled-based errors have the least to do with cognition because once the skill is learned and
practiced, the amount of thought required decreases and the skill is performed in “autopilot.”
Rule-based cognition requires thought, but only to the extent of memorization. An example of
rule-based activity is the ACLS algorithm. While difficult algorithms require more cognition, errors
can be mitigated by creating simpler algorithms or increasing the accessibility of references
through decisional aids.
Knowledge-based activities require integration of presented information (e.g., history and physical
exam) and the knowledge and experience of the healthcare provider in order to decide on a
diagnostic course.
Patient factors such as dementia, language barriers and comorbidities can increase the likelihood of error occurrence. However, an element of our own thought process, called heuristics, is the main cause of cognitive error in emergency care settings. Heuristics are strategies that simplify clinical decision-making.
In essence, heuristics are cognitive shortcuts. In situations where time, information and resources are limited, heuristics are valuable in achieving the results you want quickly. However, simplifying the thought process with heuristics, unavoidably leads to “misses” and, consequently, adverse events.
An example of a heuristic is automatically titrating oxygen to achieve oxygen saturations of 100% in all patients with a chief complaint of shortness of breath, regardless of underlying illness. Although this may be appropriate treatment for the majority of patients with shortness of breath, recent clinical evidence suggests it may be harmful for particular presentations including chronic obstructive pulmonary disease and acute coronary syndromes. A list of common cognitive errors is presented on p. 56.
How to Prevent Errors As the old dictum states, the first step is recognizing that a problem exists. The next step is achieved by actively using cognitive strategies to rectify those pitfalls in thinking.
The concept of metacognition, or “thinking about your thinking,” is the ideological basis behind creating strategies to intervene in your own thinking process and thus prevent cognitive error. The goal is to train your mind into recognizing when you’re taking inappropriate cognitive shortcuts and correct your approach accordingly.

10
One way to effectively apply metacognition to practice is by using cognitive forcing strategies. Croskerry defines cognitive forcing strategies as purposeful conscious tactics utilized in specific situations to avert error by specifically recognizing and counteracting cognitive errors themselves. They’re essentially mental checks that offset detrimental heuristics.
There are two types of cognitive forcing strategies: generic and specific. Generic strategies are used to counteract one class of cognitive error. For example, to prevent anchoring, which occurs when you form a diagnosis in your mind with the presented evidence, you force yourself to explain every other piece of evidence in order to consider all possibilities.
Specific cognitive forcing strategies arise after a unique experience that typically has an unexpected or poor outcome. For example, after a failed ET intubation last week, you now force yourself to change one aspect of laryngoscopy (e.g., blade change) following each unsuccessful attempt at intubation.
Other more familiar strategies are also useful in counteracting cognitive error. The use of simulation in prehospital education is an excellent method to observe cognitive errors being made without risk to patients. From these simulations, common points of error can be teased out and strategies to prevent them can be created.
Videos highlighting both correct and incorrect approaches to a clinical problem can also be reviewed to help learners. In addition, mentally rehearsing a patient encounter can be a useful strategy when time and resources are few.
Many clinicians have already started to use checklists and handheld computers to assist them in practice. (See “The Value of Checklists: We’ve had the solution all along,” by Shaughn Maxwell, EMT-P, in the June issue.) By decreasing reliance on memory through the use of checklists, devices or handbooks, providers may mitigate errors including drug dosing mistakes and deviations from protocol.
Finally, obtaining feedback about your care after transferring a patient can provide a starting point for finding errors. Ask your medical director to help you obtain information about a patient’s course in hospital to determine if your suspected diagnosis and treatment were correct.
The desired outcome of decreasing medical errors in the field stems from adequate surveillance, reporting and intervention. Leadership from local EMS as well as governing bodies are essential in providing patient-safety infrastructure. Suggestions of simple ways to prevent cognitive error in the field are presented below.
Case Review Continued If we look closely at this case, we can see a number of cognitive errors were made. The provider quickly jumped to the diagnosis of heart failure and strengthened it through confirmation bias—looking for information that supported the idea—such as finding mild leg edema and cardiac medications on the kitchen table.
Completing a thorough history and physical examination and looking for details that disprove your theory, for instance the low-grade elevation in temperature and cough, may help you consider other potential causes of your patient’s presentation. In this way we may prevent premature closure.
Despite some diagnostic uncertainty, this patient was treated with a diuretic. Giving diuretics to a patient with pneumonia or sepsis may be harmful. The feeling that we need to provide some treatment (as opposed to waiting for more evidence to support our treatment) is known as a commission bias.

11
Finally, passing on the information to hospital staff that the diagnosis is “X” may be harmful to a patient because diagnoses often stick to a patient as they pass from one healthcare provider to another. It makes it difficult to consider other possibilities and may cause a patient to receive an inappropriate treatment. This is known as diagnostic momentum.
What can be done the next time this type of patient is encountered?
1. Review your protocol for acute shortness of breath, and see if anything needs to be adjusted;
2. Have a metacognitive strategy to consider all pieces of information prior to categorizing the cause of shortness of breath; and
3. Contribute to forming a differential diagnosis but leave the final diagnosis to the caregivers who have access to old charts, laboratory and radiologic investigations.
Conclusion Medical error is a reality for those who practice medicine in a fast-paced and often high-stress acute care environment. It’s important for providers to recognize we’ll often make mistakes. However, as professionals, it’s our duty to attempt to limit medical error by recognizing potential areas where it may occur and preventing errors before they occur. Cognitive forcing strategies can be useful tools in helping prevent errors and provide better care to patients.
Acknowledgements: We thank Brian Rowe, MD, for his careful review and helpful editorial comments, as well as Sandy Campbell, BA, MLS, AFALIA(CP), for her assistance with a comprehensive literature search. Finally, we acknowledge the dedication and commitment of our prehospital healthcare providers to improving medical care in the field.
10 Cognitive Errors Every EMT & Paramedic Makes
1. Anchoring: The tendency to perceptually lock onto salient features in the patient’s initial presentation too early in the diagnostic process, and failing to adjust this initial impression in the light of later information. 2. Availability: The disposition to judge things as being more likely, or frequently occurring, if they readily come to mind. Thus, recent experience with a disease may inflate the likelihood of its being diagnosed. Conversely, if a disease hasn’t been seen for a long time (is less available), it may be under-diagnosed. 3. Commission bias: Results from the obligation toward beneficence, in that harm to the patient can only be prevented by active intervention. It’s the tendency toward action rather than inaction. It’s more likely in overconfident clinicians. 4. Confirmation bias: The tendency to look for confirming evidence to support a diagnosis rather than look for disconfirming evidence to refute it, despite the latter often being more persuasive and definitive. 5. Fundamental attribution error: The tendency to be judgmental and blame patients for their illnesses (dispositional causes) rather than examine the circumstances (situational factors) that might have been responsible. 6. Multiple alternatives bias: A multiplicity of options on a differential diagnosis may lead to significant conflict and uncertainty. The process may be simplified by reverting to a smaller subset with which the clinician is familiar but may result in inadequate consideration of other possibilities. 7. Omission bias: The tendency toward inaction and rooted in the principle of nonmaleficence. In hindsight, events that have occurred through the natural progression of a disease are more
12
acceptable than those that may be attributed directly to the action of the clinician. The bias may be sustained by the reinforcement often associated with not doing anything, but it may prove disastrous. 8. Diagnosis momentum: Once diagnostic labels are attached to patients they tend to become stickier and stickier. Through intermediaries (patients, paramedics, nurses, physicians), what might have started as a possibility gathers increasing momentum until it becomes definite, and all other possibilities are excluded. 9. Premature closure: A powerful cognitive error accounting for a high proportion of missed diagnoses. It’s the tendency to apply premature closure to the decision- making process, accepting a diagnosis before it has been fully verified. The consequences of the bias are reflected in the maxim: “When the diagnosis is made, the thinking stops.” 10. Search satisfying: Reflects the universal tendency to call off a search once something is found. Comorbidities, second foreign bodies, other fractures, and coingestants in poisoning may all be missed. Also, if the search yields nothing, diagnosticians should satisfy themselves that they have been looking in the right place.
Five Simple Strategies to Prevent Cognitive Errors
1. Incorporate simulation into your training plan. Search for places where errors may occur and develop ways to prevent them. Mentally running through a patient encounter can be a good use of brief periods of downtime.
2. Force yourself to consider additional diagnoses. Despite the patient having a classical presentation of diagnosis A, mentally consider possible diagnosis B and C.
3. Be wary of diagnostic labels, especially ones passed on from other healthcare professionals. Being labeled a “psych” patient can have serious consequences if incorrect.
4. Regularly ask for feedback and modify your care based upon it. Contact your medical director to obtain patient information. Find out what happened to patient “A” when you dropped him off in the ED.
5. Use checklists, a handbook or electronic handheld device to decrease reliance on memory. Double check drug doses in this manner whenever possible.
References (Available on request)
Appendix A


13
QUESTIONNAIRE EE2 (15)
INTRODUCTION
Question 1: With how much did the checklists, which were piloted in eight hospitals, reduce surgery complications?
A: 25%
B: 33% C: 50% D: 75%
Question 2: Is it TRUE that when evaluation of vehicle checks uncovers problems, it is often tracked back to someone not checking the equipment or supplies?
A: YES
B: NO
CHECKLIST DEVELOPMENT Question 3: Which of the following statements are TRUE with regard to the effect of administering medicine or an intervention?
A: It is always beneficial to the patient
B: A patient cannot be unaffected by medicine C: Medicine do not harm D: Some patients can benefit, but some are harmed
E: Some patients can be unaffected
Question 4: Which of the following effects did the handing out of the ROSC checklist have?
A: It created an effective and organized approach for the team
B: It provided instant confidence for the team leader C: Both of the above
TRAINING
INSTRUCTIONS Read through the article and answer the multiple choice questions provided here. Questions are based on the reading material only
and therefore no additional research needs to be done.
Please note that some questions may have more than one answer; in the case of the latter please “tick” every correct answer.
When done, fax through only your answer sheet to the fax number given on the answer sheet and wait for your 24 - hour receipt - of - confirmation SMS
USE CHECKLISTS TO MINIMIZE MISTAKES IN THE FIELD
Question 5: According to results, Gawande’s checklists that were developed to use in an OR crisis situations, reduced errors and/or missed steps by what percentage?
A: 90%
B: 75% C: 50% D: 25% E: 10%
APPENDIX A
Question 6: What is the first immediate action item when dealing with a seizure patient?
A: Obtain vital signs
B: Apply oxygenation C: Administer benzodiazepine D: Assess blood glucose level E: Obtain 12-lead EKG
Question 7: Syncope is a condition that can be confused for which of the following?
A: Vertigo
B: Asthma C: Seizures D: Stroke E: States of altered mental status
Question 8: Do the 11 steps of the ROSC checklist include administering albuterol?
A: YES
B: NO
14
CONCLUSION Question 9: Is it TRUE or FALSE that even if it seems routine to you, for the patient it could be an once-in-a-lifetime event and as such requires the very best care?
A: TRUE
B: FALSE
Question 10: Is the following statement TRUE or FALSE? “Cognitive aids like checklists are a weakness and not a strength.”
A: TRUE
B: FALSE
IF YOU DON’T HAVE A CHECKLIST, YOU PROBABLE SHOULD
OVERVIEW Question 11: According to Gawande which of the following should a comprehensive checklist be?
A: Practical
B: To the point C: Precise D: Easy to use E Only a reminder of critical steps
Question 12: Is it TRUE that as actions vary because of time, persons performing the actions, the weather as well as a host of other variables, it is important to write down the order of actions so that the same essential actions happen in the same way even if all the above changes?
A: YES
B: NO
EXAMPLES – Wake County EMS Checklist Question 13: In the Determining Capacity checklist which of the following are addressed?
A: Only legal and mental capacity
B: Only medical or situational capacity C: Legal, mental and medical or situational capacity D: Only mental capacity
Question 14: Which of the following form part of the Wake County EMS System Clinical Checklist?
A: CHF checklist B: Asthma checklist C: Cardiac arrest checklist D: Considerations for termination of resuscitation
outside of procedure E: Induction of hypothermia
15
Question 15: Was the diagnosis of heart failure and the administration of 40mg furosemide to the 82 year old female correct?
A: YES
B: NO
THE SCOPE OF MEDICAL ERRORS IN HEALTHCARE
Question 16: Which one of the following causes the most deaths in the USA?
A: Breast cancer
B: AIDS C: Car crashes
D: Medical error
Question 17: After efforts in improving patient safety, did follow-up studies show an improvement in medical error?
A: YES
B: NO
EMS MEDICAL ERRORS
Question 18: Which of the following are possible reasons why conditions in the ED cause it to be error-prone?
A: The work environment is hectic B: The pay is not good C: Staff fatigue and circadian dyschronicity (effect of
working late night/night shifts) D: The concurrent management of high volumes of
patients and significant diagnostic uncertainty E: No training
Question 19: What percentage of errors committed and reported by prehospital care providers were related to medical errors?
A: 21%
B: 15% C: 54% D: 68%
TYPES OF MEDICAL ERRORS
Question 20: Which of the following types of medical errors occur during technical procedures?
A: Cognitive errors B: Affective errors C: Procedural errors
Question 21: Which of the following are preventative strategies for cognitive errors?
A: Recognize and be aware of the emotion and act
accordingly B: It might be mitigated by simulations C: It might be mitigated with supervised practice
D: There is still limited insight into specific preventative strategies
Question 22: Which one of the following subdivisions of cognitive errors requires integration of present information?
A: Knowledge-based activities B: Skill-based errors C: Rule-based errors
Question 23: Which of the following patient factors can increase
the likelihood of error occurrence?
A: Dementia
B: Language barriers C: Comorbidities D: All of the above
HOW TO PREVENT ERRORS Question 24: Which one of the following cognitive forcing strategies arise after a unique experience that typically has an unexpected or poor outcome?
A: Generic B: Specific
PREVENT MEDICAL ERRORS IN THE FIELD WITH COGNITIVE STRATEGIES
16
Question 25: Which of the following can be useful strategies to counteract cognitive error?
A: The use of simulation in prehospital education
B: Videos highlighting both correct and incorrect approaches to a clinical problem
C: Mentally rehearsing a patient encounter D: Decrease reliance on memory through the use of
checklists, devices or handbooks E: All of the above
CASE REVIEW CONTINUED
Question 26: If you have a theory about what is wrong with the patient, which of the following should you do?
A: Complete a thorough history
B: Make a quick diagnosis and stick with it C: Look for details that disprove your theory that
may help you consider other potential causes D: Complete a thorough physical examination
Question 27: “Passing on the information to hospital staff that the diagnosis is ‘X’ may be harmful because the diagnosis sticks and it makes it difficult to consider other possibilities and may cause the patient to receive inappropriate treatment.” This is known as which of the following?
A: Commission bias
B: Diagnostic momentum C: Confirmation bias D: Omission bias
Question 28: Which of the following is described as “The tendency to be judgmental and blame patients for their illness”?
A: Omission bias B: Commission bias C: Confirmation bias D: Diagnostic momentum E: Fundamental attribution error
Question 29: Which one of the following reflects the universal tendency to call off a search once something is found?
A: Premature closure B: Confirmation bias C: Search satisfying D: Omission bias E: Anchoring
Question 30: Which of the following are simple strategies to prevent cognitive errors?
A: Use checklists, a handbook or electronic handheld device
B: Be wary of diagnosis labels C: Regularly ask for feedback and modify your care
based upon it D: Force yourself to consider additional diagnoses E: Incorporate simulation into your training program

17
This article is accredited for THREE Clinical (3 CEU’s)
ANSWER FORM (If your personal details have not changed, only complete the sections marked with an asterisk *)
EE2 (15) Activity 2 of 2015
TRAINING: Use Checklists to Minimize Mistakes in the Field
If You don’t have a Checklist you Probably Should Wake County EMS System Clinical Checklist
Prevent Medical Errors in the Field with Cognitive Strategies
I hereby declare that the completion of this document is my own effort without any assistance. Signed:_________________________________ Date:_____________________
Please rate the article:
FAX TO 0866144200 OR 012 653 2073 AFTER COMPLETION
*HPCSA No Postal address
*Initials and Surname
*Employer
ID Number
E-mail Address Fax Number
FOH Number Contact Number
*How would you like to receive your results for this activity (IAR? FAX EMAIL POST
*Time spent on activity _____Hour _____Min Is this for an audit? YES
NO When did you receive this activity?
A B C D E A B C D E A B C D E
1 11 21
2 12 22
3 13 23
4 14 24
5 15 25
6 16 26
7 17 27
8 18 28
9 19 29
10 20 30
POOR 1
FAIR 2
AVERAGE 3
GOOD 4
EXCELLENT 5
Mark /30 PERCENTAGE % (PASS RATE 70%)
PASSED FAILED
MODERATED BY: DATE:
PO Box 71
Wierda Park
0149
400 Theuns van
Niekerk Street,
Wierda Park, 0149
www.fohcpd.co.za
Cell: 074 230 3874
Tel: 012 653-0133/
2373/ 2873
Mon-Fri: 07:30-16:30