baseline vital signs
DESCRIPTION
yyyTRANSCRIPT

Baseline Vital Signs
Baseline Vital Signs
• Key signs used to evaluate a patient’s condition
• First set is known as baseline vitals • Repeated vital signs compared to the baseline
• Need at least 2 sets of vitals to show trending
Baseline Vital Signs
• PRBELLS• Pulse• Respiration• Blood pressure• Eyes• Lung sounds• LOC - Level of Consciousness• Skins

Pulse• Rate– Number of beats in 30 seconds x 2
– Number of beats in 15 seconds x 4
• Rhythm– Regular or irregular
• Quality– Bounding, strong, or weak (thready)

Normal Pulse Rates
Adults 60 to 100 beats/min
Children 70 to 150 beats/min
Infants 100 to 160 beats/min
Fast = Tachycardia - over 100 in adults
Slow= Bradycardia - under 60 in adults
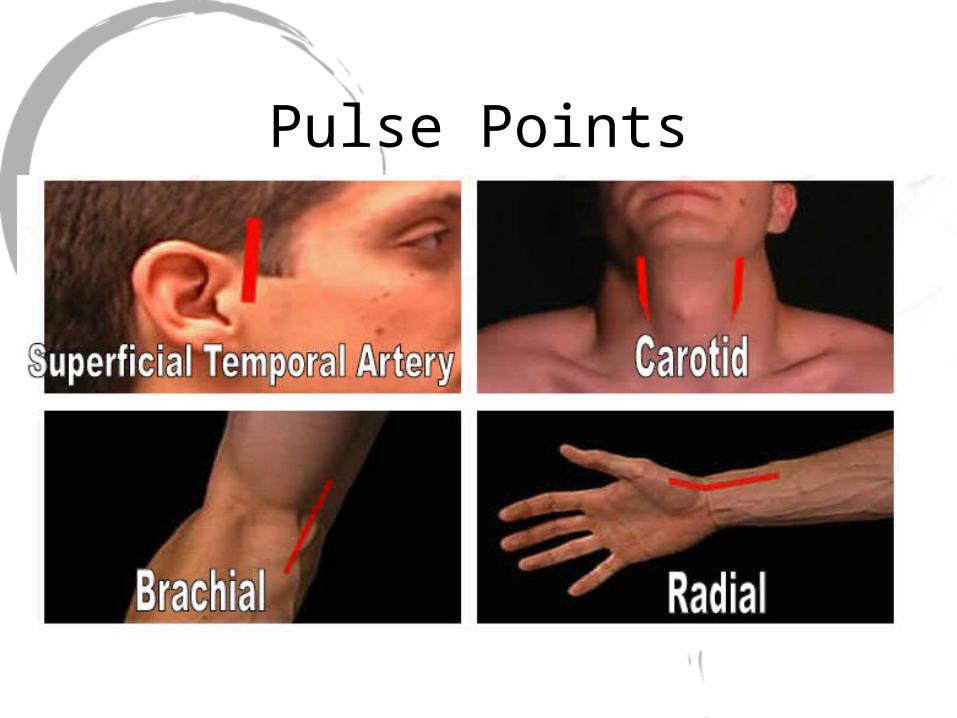
Pulse Points

Pulse Points

Pulse Points

Pulse Oximetry

Pulse Ox Enemies

Respirations
• Rate– Number of breathsin 30 seconds x 2
• Rhythm– Regular or irregular
• Quality– Character ofBreathing
• Effort– Normal orLabored
• Noisy respiration– Normal, stridor,wheezing,snoring, gurgling
• Depth– Shallow or deep

Respiratory Rates
Adults 12 to 20 breaths/min
Children 15 to 30 breaths/min
Infants 25 to 50 breaths/min

Common Terms
• Bradypnea= slow breathing
• Tachypnea= fast breathing
• Eupnea= normal breathing
• Apnea = no breathing

Blood Pressure
• A drop in blood pressure may indicate:– Loss of blood– Loss of vascular tone– Cardiac pumping problem

EquipmentSphymanometer & Stethescope

Measuring Blood Pressure
• Diastolic– Pressure during relaxing phase of the heart’s
cycle
• Systolic– Pressure during contraction
• Measured as millimeters of mercury (mm Hg)
• Recorded as systolic/diastolic

Blood Pressure

Auscultation of Blood Pressure1. Place cuff on patient’s arm.2. Palpate brachial artery and place stethoscope.3. Inflate cuff until you no longer hear pulse sounds.4. Continue pumping to increase pressure by an
additional 20 mm Hg.
5. Note the systolic and diastolic pressures as6. you let air escape slowly.7. Korotkoff Sounds8. 1st beat you hear is systolic9. Last beat you hear is diastolic10.As soon as pulse sounds stop, open the
valve and release the air quickly.

Palpation of Blood Pressure
1. Secure cuff.2. Locate radial pulse.3. Inflate to about 200 mm Hg.4. Release air until pulse is felt.5. Method only obtains systolic pressure.

Normal Ranges of Blood Pressure
Infants (newborn to 1 year) 50 to 95(systolic)
Children (1 to 8 years) 80 to 110 mm Hg(systolic)
Adults 90 to 140 mm Hg(systolic)

Pupil Assessment
• P - Pupils• E - Equal• A - And• R - Round• R - Regular in size• L - React to Light
Abnormal Pupil Reactions
• Fixed with no reaction to light• Dilate with light and constrict withoutlight…that’s a brain problem!• React sluggishly• Unequal in size• Unequal with light or when light isremoved

Pupil Reactions

Level of Consciousness
Name? Date? Place? Problem?
Lung SoundsTypes of Lung Sounds• Lung sounds are
typically broken down into three categories:• Normal (vesicular)• Decreased or
absent• Abnormal
(adventitious)

Lung Sounds• There are several types of abnormal lung sounds:
• Wheezes are caused by air flowing rapidly through narrowed airway passages
• Rhales are small bubbling or fine clicking sounds made when air is forced into collapsed alveoli and/or in the presence of fluid in the alveoli and/or bronchioles.
• Rhonchi are low-pitched, sonorous, rumbling, bubbling or gurgling sounds.
• Pleural rub, or friction rub, occurs when there is fluid in the pleural space between the lung tissue and the interior chest wall. There is commonly a grating, rubbing type of sound as the visceral (lung) and parietal (chest wall) pleura rub against each
other.

Lung Sounds

Skins


Reassessment of Vital Signs
• Reassess stable patients every 15 minutes.• Reassess unstable patients every 5 minutes

Patient HistorySAMPLE• S - Signs & symptoms
• OPQRST
• A - Allergies• M - Medications• P - Past medical history• L - Last oral intake• E - Events leading to incident

S - Signs & Symptoms
OPQRST
O - Onset
When & How did the symptom begin?
P - Provokes/Palliates
What makes the symptom worse?
What makes the symptom better?

S - Signs & Symptoms
OPQRSTQ - Quality
• How would describe the pain?/What does the pain feel like?
• DO NOT lead the patient
R - Region/Radiation• Where is the pain?• Does the pain travel anywhere else?

S - Signs & Symptoms
OPQRSTS - Severity
• How bad is the pain? Scale of 1-10
T - Time• How long have you had the symptom?

A - Allergies
• Medications
• Foods
• Environment

M - Medications
Are you taking any?
When did you last take your medication?
What are they?
What are they for?
May I see them?
May we take them with us?

P - Previous Medical History
• Pertinent• Related to this complaint• Complicating factor

L - Last Oral Intake
Food and/or Drink?
What?
When?

E - Events leading up to the incident
What happened?
When?