barriers to access: frustrations of people who use a wheelchair for full-time mobility
TRANSCRIPT

Barriers to Access: Frustrationsof People Who Use a Wheelchairfor Full-Time Mobility
Linda L. Pierce, MSN RNC CRRN
A phenomenological study wasconducted to answer the question,What is it likebeing an individual witha disability who uses a wheelchair forfull-time mobility and lives in societywith many potential barriers? A totalof9 people from Ohio and Pennsylvania composed the purposively selected sample. Colaizzi's method ofdata analysis was used to review transcriptions ofinterviews with those inthe sample. The analysis identified amajor theme: all participants hadfeelings offrustration concerning access. Four subtheme clusters relatedto this frustration emerged: issues ofindependence, attitudes ofothers toward people with disabilities, others'lack ofunderstanding ofthe situationsof individuals with disabilities, andlack ofinvolvement ofpeople with disabilities in decisions regardingthe development offacilitiesfor them. Thisstudy provides insights into the livedexperience ofaccessibility in today'senvironment for people with disabilities who use a wheelchair for fulltime mobility, offers direction forhealth professionals who work withthese individuals,and serves as an impetus for further research.
Address correspondence to LindaPierce, 413 Loyola Drive, Elyria,OH44035.
The passage of the Americans with Disabilities Act of 1990 (ADA) secured equalaccess to employment, recreation, transportation, and communication for 43 millionAmericans with disabilities. The purpose of the ADA is to provide a federal mandate toeliminate discrimination against people with disabilities, enforce the standards developed to protect them, and enforce the Fourteenth Amendment's aspects of integration,to ensure access for all within American society (see Figure 1).
Nonetheless, discrimination against individuals and their families can take manyforms. For example, architectural barriers are a form of discrimination that is not oftenunderstood by abled-bodied people, but they are especially distressing for people whouse a wheelchair for full-time mobility. It is important to remember that signs denotingthat buildings or public areas are accessible to people in wheelchairs do not guaranteethat these environments are, in fact, accessible.
According to Glass (1988), good communication is essential for promoting accessibility. Fain (1996) highlighted in a travel magazine article the fact that the American hotel industry is facing numerous lawsuits for failing to make accommodations accessibleto people with disabilities. In another article, Hahn (1993) reported that although Congress passed the ADA, access in the environment for people with disabilities has not become easy. Hahn found that assertive communication is the key to access.
Pertinent literatureStudies on accessibility are sparse in the research literature. Most published reports
primarily have addressed access to public buildings (Martin, 1987), shopping malls(Couch, 1992; Roberts, 1986), food stores (McClain & Todd, 1990), and restaurants(McClain et aI., 1993). Through a survey focused on 13 public buildings, Martin foundthat the median percentage of compliance to building codes governing accessibility was77%. Rest rooms, ramps, and parking were the major areas of noncompliance.
In Kansas City, Roberts (1986) noted consistent problems with narrow aisles, highshelves and racks, inaccessible dressing rooms, poorly adapted rest rooms, and heavydoors in shopping malls. In a more recent study (Couch, 1992) of shopping mall patronswho were observed entering and leaving a department store, a majority (65.5%) of the3,554 patrons chose ramps instead of steps to ascend or descend a height of approximately 5 feet that separated the mall level from a department store. Couch's data alsoindicated that 81 people would have had difficulty getting to the department store without a ramp. Of these, 51 were parents with babies in strollers or carriages. The secondlargest group needing ramps were those with disabilities. Five people used wheelchairsand another 19 had evident permanent or temporary physical disabilities. This study waslimited by the following factors: (a) observations that were limited to only one setting,(b) a step and ramp configuration that may have provided a convenience factor ratherthan demonstrated personal preferences, (c) uncontrolled demographic factors of theobserved individuals, and (d) the possibility of the use of steps by individuals as exerciseenhancers. Nevertheless, the results tentatively suggested that increased business and
120 Rehabilitation Nursing> Volume 23, Number 3· May/Jun 1998

greater customer satisfaction could be incentives that companies should consider when weighing the possibility of including ramps in their construction plans.
In a small survey of 20 grocery and convenience stores inthe urban and rural areas of one Midwestern state, McClain andTodd (1990) found that urban and rural convenience storesearned lower accessibility scores than grocery stores. These investigators hypothesized that grocery stores may have earnedhigher scores on the survey because of the architectural demands of the stores themselves. For instance, the use of grocery carts, which grocery stores provide but convenience storesdo not, necessitates ramps, accessible curbs, and doors that openeasily. These features, which are designed for carts, may alsoincrease accessibility for people in wheelchairs.
In another study designed to determine restaurants' compliance with the wheelchair accessibility standards found in Title III of the ADA, McClain et a1. (1993) compared 120 conventional and fast food restaurants in urban and rural settingsin three states. Although no notable differences emerged fromthese comparisons, these investigators found three problem areas for the restaurants. Parking the car was often an obstacle toeating out, as only 53% of the surveyed restaurants providedhandicapped parking spaces. Entering the buildings was also aproblem. Only 66% of the restaurants that needed a ramp provided one. Inside the facility, the major problems were accessible rest rooms and table height.
Figure 1. Overview of the Americans withDisabilities Act (ADA) of 1990
Title I. Access to EmploymentThere must be no discrimination in recruiting,hiring,promotion,job assignment, transfer,rate of pay, fringe benefits, or training.Facilitiesmust be readily accessibleto andusable by all.
Title II. Public ServicesPublic transit must be accessible to those in wheelchairs.
Title III. Public Accommodations and Related ServicesPrivate businesses(e.g., hotels, physicians' offices, shopping centers, restaurants) must provide accessibility.
Title IV. TelecommunicationsTelephoneservices offered to the public must includefulltelecommunication relay service for people who are hearing impaired.
Title V. Miscellaneous ProvisionsA local or state governmental law that providesgreaterprotectionfor the rights of persons with disabilitiesoverrides the terms of the ADA.
Note. From Public Law 101-336.
Recent follow-up projects related to the few available published studies are lacking. No definitive work has been reported in the literature to explore the lived experience of accessibility for people who use wheelchairs for full-time mobility;therefore, accessibility remains a relatively neglected issue.
Research questionThe research question that guided this study was, What is it
like being an individual with a disability who uses a wheelchairfor full-time mobility and lives in society with many potentialbarriers?
MethodDesign and conceptual approach: Phenomenology is the
study of essence (Ray, 1985) or "what makes something whatit is" (Ray, 1990, p. 173). The aim of phenomenology is to describe the human experience as it is lived (Oiler, 1982). In thisstudy, a phenomenological approach was used to examine thelived experience and achieve a fuller understanding through description, reflection, and direct awareness of accessibility issues for people with disabilities who use a wheelchair for fulltime mobility.
Sample: The sample consisted of 4 men and 5 women between 20 and 52 years of age. Some lived alone; others did not.All of the participants spoke English and were articulate. In addition, they all used a wheelchair for full-time mobility becauseof a physical disability and had lived in an urban communitysetting for at least the preceding 6 months.
Specificprocedures: Four nurse investigators collected datafor this study. Prior to beginning the data collection, one of thedoctorally prepared investigators, who was experienced withthe method, reviewed the interview procedures with the other investigators. The investigators obtained their institutional reviewboards' approval and the participants' informed consent. Theinvestigators then recruited a purposive sample of men andwomen from northern and central Ohio and western Pennsylvania. To select participants for the study, investigators usedpurposive sampling, which is based on personal judgments aboutpeople who would be most representative of the general population. An investigator contacted potential participants 1 weekprior to the data collection phase and offered them the opportunity to participate in the study. If participants agreed to takepart in the study, the investigator read the research question sothe participants could think about their responses. Each participant was assured that all data would be analyzed as groupresponses and that individual participants would not be identified. Finally, the investigator gave each participant an opportunity to contact her prior to the data collection date to ask anygeneral questions about the interview process.
Each one-on-one interview was held in a location chosen bythe participant, was audiotaped, and lasted approximately 1hour. On the day of the interview, the investigator once againread the participant the research question; the remainder of thetime was devoted to the participant's response. The investigator informed the participant that the audiotape could be stoppedat any time during the interview. At the end of each interview,
Rehabilitation Nursing s Volume 23, Number 3' May/Juri 1998 121
Barriers to Access
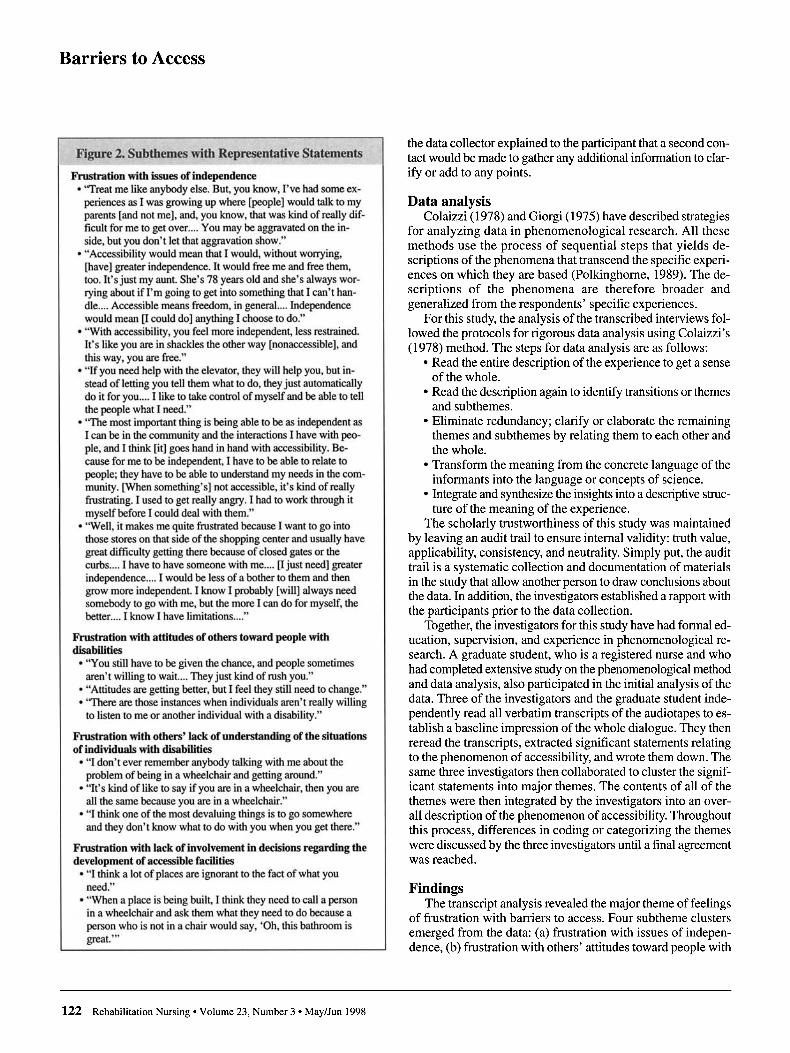
Figure 2. Subthemes with Representative Statements
Frustration with issues of independence• "Treat me like anybody else. But, you know, I've had some ex
periences as I was growing up where [people] would talk to myparents [and not me], and, you know, that was kind of really difficult for me to get over .... You may be aggravated on the inside, but you don't let that aggravation show."
• "Accessibility would mean that I would, without worrying,[have] greater independence. It would free me and free them,too. It's just my aunt. She's 78 years old and she's always worrying about if I'm going to get into something that I can't handle.... Accessible means freedom, in general .... Independencewould mean [I could do] anything I choose to do."
• "With accessibility, you feel more independent, less restrained.It's like you are in shackles the other way [nonaccessible], andthis way, you are free."
• "If you need help with the elevator, they will help you, but instead of letting you tell them what to do, they just automaticallydo it for you .... 1 like to take control of myself and be able to tellthe people what 1need."
• ''The most important thing is being able to be as independent as1can be in the community and the interactions 1have with people, and I think [it] goes hand in hand with accessibility. Because for me to be independent, 1have to be able to relate topeople; they have to be able to understand my needs in the community. [When something's] not accessible, it's kind of reallyfrustrating. 1 used to get really angry. I had to work through itmyself before 1could deal with them."
• "Well, it makes me quite frustrated because 1 want to go intothose stores on that side of the shopping center and usually havegreat difficulty getting there because of closed gates or thecurbs .... I have to have someone with me.... [I just need] greaterindependence.... 1 would be less of a bother to them and thengrow more independent. 1know 1probably [will] always needsomebody to go with me, but the more 1can do for myself, thebetter. ... 1 know 1have limitations...."
Frustration with attitudes of others toward people withdisabilities
• "You still have to be given the chance, and people sometimesaren't willing to wait.... They just kind of rush you."
• "Attitudes are getting better, but 1feel they still need to change."• ''There are those instances when individuals aren't really willing
to listen to me or another individual with a disability."
Frustration with others' lack of understanding ofthe situationsof individuals with disabilities
• "I don't ever remember anybody talking with me about theproblem of being in a wheelchair and getting around."
• "It's kind oflike to say if you are in a wheelchair, then you areall the same because you are in a wheelchair."
• "I think one of the most devaluing things is to go somewhereand they don't know what to do with you when you get there."
Frustration with lack of involvement in decisions regarding thedevelopment of accessible facilities
• "I think a lot of places are ignorant to the fact of what youneed."
• "When a place is being built, I think they need to call a personin a wheelchair and ask them what they need to do because aperson who is not in a chair would say, 'Oh, this bathroom isgreat.'"
122 Rehabilitation Nursing « Volume 23, Number 3' May/Jun 1998
the data collector explained to the participant that a second contact would be made to gather any additional information to clarify or add to any points.
Data analysisColaizzi (1978) and Giorgi (1975) have described strategies
for analyzing data in phenomenological research. All thesemethods use the process of sequential steps that yields descriptions of the phenomena that transcend the specific experiences on which they are based (Polkinghorne, 1989). The descriptions of the phenomena are therefore broader andgeneralized from the respondents' specific experiences.
For this study, the analysis of the transcribed interviews followed the protocols for rigorous data analysis using Colaizzi's(1978) method. The steps for data analysis are as follows:
• Read the entire description of the experience to get a senseof the whole.
• Read the description again to identify transitions or themesand subthemes.
• Eliminate redundancy; clarify or elaborate the remainingthemes and subthemes by relating them to each other andthe whole.
• Transform the meaning from the concrete language of theinformants into the language or concepts of science.
• Integrate and synthesize the insights into a descriptive structure of the meaning of the experience.
The scholarly trustworthiness of this study was maintainedby leaving an audit trail to ensure internal validity: truth value,applicability, consistency, and neutrality. Simply put, the audittrail is a systematic collection and documentation of materialsin the study that allow another person to draw conclusions aboutthe data. In addition, the investigators established a rapport withthe participants prior to the data collection.
Together, the investigators for this study have had formal education, supervision, and experience in phenomenological research. A graduate student, who is a registered nurse and whohad completed extensive study on the phenomenological methodand data analysis, also participated in the initial analysis of thedata. Three of the investigators and the graduate student independently read all verbatim transcripts of the audiotapes to establish a baseline impression of the whole dialogue. They thenreread the transcripts, extracted significant statements relatingto the phenomenon of accessibility, and wrote them down. Thesame three investigators then collaborated to cluster the significant statements into major themes. The contents of all of thethemes were then integrated by the investigators into an overall description of the phenomenon of accessibility. Throughoutthis process, differences in coding or categorizing the themeswere discussed by the three investigators until a final agreementwas reached.
FindingsThe transcript analysis revealed the major theme of feelings
of frustration with barriers to access. Four subtheme clustersemerged from the data: (a) frustration with issues of independence, (b) frustration with others' attitudes toward people with

disabilities, (c) frustration with other people's lack of understanding of the situations of individuals with disabilities, and(d) the desire of people with disabilities to become involved indecisions regarding the development of accessible facilities.Figure 2 lists subthemes and representative statements.
Frustration with issues of independence: All participantsdiscussed their feelings of frustration over being seen by others as dependent. Over and over again, they used words suchas "aggravation," "anger," and "worry." One young woman captured the essence of all the participants' frustration with tryingto be independent in her statement:
I get frustrated ...with sales clerks in stores where you arechecking out; for some reason ...people look at me whenI flick out my charge card.... They assume incorrectly thatpeople in wheelchairs don't have charge [cards]. Peopleask me where my mother lives and if she's at home. Shedoesn't have to be with me. I'm capable of taking care ofmyself and that kind of thing....Treat people like adults.We may be in wheelchairs and we may not handle thingslike you or your neighbors would, but treat us likeadults [I've had] to work through anger and frustra-tion When I was growing up, I was always the cute lit-tle handicapped child who was maybe never going togrow up to be a woman. And, suddenly, there I was, and,you know, people around me just didn't know how tocope with that. It's taken me years to kind of feel goodabout myself.
Issues of independence and access were clearly linked to frustrations with others' attitudes toward people with disabilities.
Frustration with the attitudes of others toward peoplewith disabilities: All of the participants expressed feelings offrustration with the attitudes of others. One woman expressedthis experience with remarkable candor in the following story:
I was at a fund-raiser...and had to use the bathroom. Well,this was the type of place that has weddings; it's supposedto be a hall. So I go into the bathroom, and I fit throughthe door, but none of the doors of the stalls were wideenough for me to get into. So I went out and went to thehat-check stand and said, "Excuse me, are there any bathrooms around here that are wheelchair accessible?" Thewoman there said, "Well, we thought those were." I said,"No. Can I talk to the manager?" The manager said thatthey were accessible, too, and says, "Everybody else canfit in there. Well, if I get a bucket and put it underneathyou, do you think you could use that?" I shook my headno and didn't say anything more. The two other peoplestanding there seemed stunned. Instead of losing my temper, I just walked away. It just made me mad.
The participant clarified her response this way: "I said, 'Whywasn't it changed? Why don't you move some of this stuff or puta little ramp down there so we can get in?'"
Not only were the participants frustrated with others' attitudes, but they were also frustrated that others did not truly understand the everyday situations that they experienced.
Frustration with others' lack of understanding of situations: All of the men and women talked of situations involving
accessibility issues related to shopping, restaurants, socialevents, schools, rest rooms, hotels, medical care, cars, andplanes. One older woman said this about hotels:
I have disabled friends that complained about the fact thatthey often travel with either an attendant or someone thatthey don't know very well but [who] has agreed totravel with them. They don't want to sleep in the samebed...[but] you can't often find [wheelchair-] accessiblerooms that have two beds in them. For some reason, [hotels] tend to think that disabled people need a king-sizebed. It's the strangest thing I have ever seen.
Participants' comments about situations such as this one indicated frustration with the lack of involvement of people withdisabilities in making decisions about the design of facilities.
Participants in our study shared a variety ofinsights on issues related to accessibility.
Frustration with the lack of involvement in decisions regarding the development of accessible facilities: Most of theparticipants said that they write letters to organizations andagencies to express their frustrations over their lack of accessand to suggest that, as one participant said, "They need to address them at this point." One man said this:
Doctors' offices are really bad and I was really surprised.Every physician's office I have been to-and I have beento many-does not have a treatment table that goes upand down. They either have to examine me in a chair orget two or three people to lift me and help. I think the government needs to set up some type of board with personswho are handicapped and have been in wheelchairs...sothe government knows what needs to be done in offices,hotels, motels, and restaurants to make them accessible.
Nonetheless, all of the participants were able to describe specificactivities that they engaged in to deal with their frustration withaccess. For instance, to decrease feelings of frustration overtheir lack of participation in decisions regarding the development of accessible facilities, one participant suggested this:"One thing I would like to make you aware of is to be sensitive." Another said, "I would say be really understanding."
DiscussionAlthough the women and men in this study identified their
very personal experiences related to frustration with barriers toaccess, the meanings associated with these experiences werebroader and yielded common subthemes. They were frustratednot only by issues related to independence but also by others'attitudes toward and lack of understanding of people with disabilities. In addition, they were frustrated by the insufficient involvement by people with disabilities in decisions regardingthe development of facilities to meet ADA requirements.
The findings of this study support and extend the work ofCouch (1992), McClain et al. (1993), McClain and Todd (1990),and Roberts (1986). However, the participants in this studyshared insights on issues of accessibility beyond those involv-
Rehabilitation Nursing> Volume 23, Number 3' May/Jun 1998 123

Barriers to Access
Assertive Communication Strategiesfor Dealing with Frustrations Relatedto Accessibility
Speaking up and listening• "Take control of self and be able to tell people what I need."• "Listen to what [people with disability] have to say."• "Whoever is building these places needs to talk to a person
in a wheelchair and get them to show what needs to bedone."
• '" used to demand things and say, 'Are you telling me thatyou can't do this?' I guess' tend to find that the nicer' am,the nicer people are back to me at this point, It makes a difference, and I think that if you are nice to people and pointthings out to them in a nice way, most people try to doeverything they can to try to make things accessible for meas well. That helps."
• '" choose services that are accessible. 'call and if they aren'tsure, then I ask them to check it out. Are there parkingspots? 'S there a cutdown curb? Will I be able to get to theelevator?"
• '" need to do for myself. I say, 'Excuse me, would you mindopening that door for me?' or 'Would you mind helping meup this curb?'"
• "Speak up in a polite way. 'find that people for the mostpart respect me for that communication."
• "[Some people might say] I'm no good for anything and I'min this wheelchair and I don't know why I'm on this earth.'guess what I'm saying to you is 'That's the wrong attitude.We have to speak for ourselves whether we are disabled orblack or whatever minority that you are.' I think you arenever going to go back to a time when these minorities willbe voiceless and not speak up for what they need and want....I think adjustment is ongoing and you have to continue toadjust. ... It's the part that we can control and change. So nomatter how accessible we make the world, physically andotherwise, it's really not going to make as much difference[unless we] help people be able to deal with whatever theyhave to deal with."
Teaching• '" think you have to teach people how to ask for help...in
terms of how people are taught to relate to people with special needs" .."
• "Certainly, the family support and friends ...teach people howto cope with loss.... You have to have somebody; that's whysupport groups are good."
• "The ones that are really cranky with you say, 'Weill don'thave to change my place.' Well, what you do is you givethem a wheelchair and say, 'Here, now you try to go useyour bathroom or try to get through this place.'''
Writing• "I will write a note about concerns that I have and tell them
that they need to address them at this point in time."• "I've become really good at writing letters. I find that it's a
nice way of just expressing my concerns.... A lot of times,with a letter you can state your case and then people cancome back to you."
124 Rehabilitation Nursing > Volume 23, Number 3· May!Jun 1998
ing shopping malls, stores, and restaurants. A recommendationfor further research is that studies be conducted to identify morespecific actions that people with disabilities can take along withan evaluation of their outcomes. Investigators should also consider replication of this study with people from a broader geographic area as well as with people living in rural settings.
This project is limited as to its transferability or the extentto which its findings can be used in other settings or with other groups. An important goal is to understand issues of accessibility not in just one isolated circumstance but in a broad, general sense. To this end, the investigators provided an in-depthdescription to enable the reader to reach a conclusion aboutwhether transfer of the findings to other settings is possible (seeFigure 2).
A strength of this study is that the participants who usedwheelchairs for full-time mobility recommended positive personal communication strategies they found valuable when dealing with their frustration related to access. Their assertive communication strategies (see the sidebar) suggest thoughtful,commonsense actions for promoting access. These personalcommunication strategies not only reflect the themes and reinforce the fundamental importance of being independent but alsosupport Glass' (1988) belief that expression of needs is criticalto obtaining access.
Implications for practiceRehabilitation nurses and other team members should as
sess people's readiness to participate and to evaluate outcomesthat result from incorporating communication strategies whenworking with people who have disabilities. Health professionals might be able to foster or strengthen feelings of independence and decrease feelings of frustration over accessibility issues for people who use a wheelchair for full-time mobility byusing the assertive communication strategies suggested by theparticipants in this study.
In general, rehabilitation professionals must be aware of theADA; educate clients, families, other healthcare providers, employers, and the public about the ADA provisions; and offer encouragement and counseling for these individuals. For instance,rehabilitation nurses in clinic settings can work with vocational counselors and people with disabilities to coordinate strategies for job accommodations. In addition, political activism byhealthcare professionals to effect change on behalf of theseclients is critical. This can be accomplished by identifying oneissue each year and acting on it, joining national groups to getaccess to information, developing relationships with elected officials, serving on local commissions, and acting as advocatesfor people with disabilities.
ConclusionThis study offers important insights into the lived experi
ence of people with disabilities who use a wheelchair for fulltime mobility. Healthcare professionals and policy makers mustbe cognizant of this information as they work with this segmentof the population and make plans to comply with the ADA nowand in the 21st century.

ReferencesAmericans with Disabilities Act of 1990, Pub. L. No. 101-336, §2, 104
Stat. 328 (1990).Colaizzi, P. (1978). Psychological research as the phenomenologist views
it. In R. Valle & M. King (Eds.), Existential phenomenological alternatives forpsychology (pp. 48-71). New York: Oxford University Press.
Couch, R. (1992). Ramps not steps: A study of accessibility preferences.Journal ofRehabilitation, 58(1), 65-69.
Fain, J. (1996, December). No ramp at the inn. Traveler, 31-32, 34.Giorgi, A. (1975). An application of the phenomenological method in psy
chology. In A. Giorgi, C. Fisher, & E. Murray (Eds.), Duquesne studies in phenomenological psychology (pp. 82-103). Pittsburgh: Duquesne University Press.
Glass, D. (1988). Accessibility and the American Congress of Rehabilitation Medicine. Archives ofPhysical Medicine and Rehabilitation, 69, 79-80.
Hahn, J. (1993, October 17). Mouth helps wheelchair traveler. The PlainDealer, p. 13.
Martin, L. (1987). Wheelchair accessibility of public buildings in Utica,New York. American Journal ofOccupational Therapy, 41,217-221.
McClain, L., Beringer, D., Kuhnert, H., Priest, 1., Wilkes, E., Wilkinson, S.,& Wyrick, L. (1993). Restaurant wheelchair accessibility. American JournalofOccupational Therapy, 47, 619-623.
McClain, L., & Todd, C. (1990). Food store accessibility. American Journal ofOccupational Therapy, 44, 487-491.
Oiler, C. (1982). The phenomenological approach in nursing research. Nursing Research, 31, 178-181.
Polkinghome, D. (1989). Phenomenological research methods. In R. Valle& S. Holling (Eds.), Existential-phenomenological perspectives in psychology(pp. 41-60). New York: Plenum Press.
Ray, M. (1985). A philosophical method to study nursing phenomena. InM. Leininger (Ed.), Qualitative research methods in nursing (pp. 81-92). NewYork: Grune & Stratton.
Ray, M. (1990). Phenomenological method for nursing research. In N.Chaska (Ed.), The nursing profession: Turning points (pp. 173-179). St. Louis:Mosby.
Roberts, K. (1986). Shopping for architectural barriers. Rehabilitation Nursing, 11(4),20-21.
Linda Pierce is an assistant professor at the Medical College ofOhio School ofNursing in Toledo and a doctoral candidate atWayne State University College ofNursing in Detroit.
AcknowledgmentsThe author acknowledges the contributions of co-investigators
Lorraine Rodriques-Fisher, EdD RN, Clare Hopkins, PhD RN,and Kathy Mitchell, MSN RN CRRN, in the conceptualizationof the original idea, data collection and analysis, and review ofthis paper. The author also thanks Sherri S. Winegardner, MSNRN, for her assistance in the initial data analysis and Judy Salter,MSN RN CRRN, for her thoughtful critique of this manuscript.
Partial funding for this project carne from a grant from theNorth Coast Chapter of the Association of Rehabilitation Nurses (ARN) and the Iota Psi Chapter of Sigma Theta Tau International.
This research was presented as a poster at the ARN 22nd Annual Educational Conference in Seattle.
This continuing education offering (codenumber RNC-129) will provide 1 contact hour to those who read this articleand complete the application form onpage 168.This independent study offering is ap
propriate for all rehabilitation nurses. By reading this article, the learner will achieve the following objectives:
1. Identify accessibility issues for people who use a wheelchairfor full-time mobility in today's society.
2. State implications for nursing practice related to personal communication strategies.
CLINICAL TOPICS
~ Rehabilitation nursing "basics"bowel and bladder protocolsskin integrityfall preventionsexualitybehaviorcoping and adjustmentpatient and family educationanatomy and physiology reviews
~ Orthopedic topics
~ Cardiopulmonary topics
~ Oncology
~ Pediatrics
~ Health promotion in chronic illnessand disability
Calling All Authors:Write for
Rehabilitation NursingToday!
Rehabilitation Nursing is seekingarticles on the clinical and practicemanagement topics listed here.
Articles should make strong nursingimplications and practice suggestions.Case studies are welcome.
For guidelines for authors,contact Rehabilitation Nursing,
800/229-7530, fax 847/375-4777,e-mail [email protected].,Web site www.rehabnurse.org.
PRACTICE MANAGEMENT TOPICS
~ Home healthcare issues
~ Subacute care issues
~ Case management issues
~ Outpatient care issues
~ Clinical pathways
~ Quality improvement
~ Delegation/unlicensed assistivepersonnel issues
~ Nurse entrepreneurship
~ Community-based care
~ Team management
~ Ethical issues
Rehabilitation Nursing- Volume 23, Number 3· May/Jun 1998 125