back to basics - hematology objectives lmcc objectives – anemia fatigue – jaundice –...
TRANSCRIPT

Back to Basics -Hematology

Objectives
• LMCC objectives– Anemia
• fatigue
– Jaundice– Lymphadenopathy– Elevated hemoglobin– Splenomegaly– Neck mass– Venous thrombosis

PRINCIPLES - Anemia
• Anemia is not a disease• Investigation should be logical
– Start with CBC and Blood film• Leads to other tests
– non specific– specific
• Guides therapy

Further Principles
• Symptoms are more related to rate of fall in hemoglobin not level.
• Non specific symptoms• More specific symptoms• Drug History – including EtOH• Physical examination

Anemia and Fatigue
What’s the link?Hemoglobin in RBCs
– Iron-containing oxygen transport protein– Function to transport oxygen to every tissue in
the body
Starts With CBC
• High yield parameters– Hgb– MCV: approach– Reticulocyte count
• Morphology– Blood film (smear)
• Confirmatory tests


Peripheral blood filmMorphology Lab tests DiagnosisHypochromic, microcytic Low Fe, high TIBC, low
ferritinIron deficiency
Hypochromic, microcytic High Hb A2 or high Hb F Beta-thalassemia
Macrocytic Low B12 or low folate B12 or folate deficiency
Macrocytic, other cell lines abnormal
Normal B12,folate, low WBC, low plt
Myelodysplasia(other possibilities)
Normocytic, normochromic
Low Fe, low TIBC, abnormal liver, abnormal kidney, high ESR, normal or high ferritin
Anemia of chronic inflammation

Peripheral blood film
Morphology Lab tests DiagnosisNucleated RBC, Teardrops
Other cell lines, marrow aspirate and biopsy
Myelofibrosis, Marrow infiltration
Schistocytes Coombs test, PTT, INR, fibrinogen
Microangiopathic hemolytic anemie, ie. DIC
Spherocytes Coombs test, Osmotic fragility
Immune hemolysis, Hereditary spherocytosis
Sickle cells Sickle prep. Sickle cell syndromes
Target cells Abnormal Hb electrophoresis
HbC, D, thalassemia

• Test results- Hgb 77 g/L- MCV 66f/L- RBC 3.2 x1012/L- WBC 5.6 x106/L- Plat 525 x109/L- Retic count
‘normal’
This is a 55 year old woman who has fatigue. Her only other symptom is a craving for chewing ice cubes. Apartfrom being pale her examination is normal.

Microcytic, hypochromic
STAGES OF IRON DEPLETION
Loss of body storesFall in serum ironAnemia develops MicrocytosisHypochromasia

ASSESSMENT OF IRON STATUS
• Identify high risk groups• Children• Menstruation• Pregnancy - Lactation• Frequent Blood Donors• Chronic GI loss• Malabsorption• Diet

IRON BALANCE
Ingest 10-20 mg. per day Absorb 1-3 mg per day Lose 1 + mg per day
– menstrual loss 30-50 ml Total iron content in body 3 – 4 grams
most in RBC (~2.5 g) Stores 1 gram – ferritin, hemosiderin Easy to achieve negative balance
INVESTIGATION OF CAUSE
Investigate when cause not Clear Symptoms of cause often unreliable Upper GI cause higher Yield If upper GI lesion found then a colonic
lesion unlikely TESTS - Radiologic, Endoscopic Biopsy,
Angiographic.

THERAPY
Replace ironTreat underlying cause if possible

Anemia of Chronic disease
• Usually mild to moderate anemia• normocytic normochromic• low retic count• Low serum Fe and low TIBC sat % 15-20• Ferritin normal or high• A responsible disease is present• Usually a systemic disorder

SIDE TRACK ….Very High Iron
• Mulitple regulators of iron metabolism
• Think of – reactive/inflammatory processes
• Infection, inflammation, malignancy, alcoholic liver disease, nonalcoholic steatohepatitis, metabolic syndrome
– hemochromatosis

Hemochromatosis• Fe overload• Genetic predisposition to increased Fe absorption
– hepcidin• Common• Screen with Fe saturation (ferritin)
– >=60% males– >=50 women
– >=45% - lower cutoff advocated by some guidelines
• Confirm with Genetic testing: HFE gene• 3 genes tested C282Y ( H63D , S65C)• Treatment - phlebotomy

BACK TO ANEMIA….

• Test results- Hgb 85 g/L- MCV 110 fL- RBC 3.9 x1012/L - WBC 2.4 x106/L- Plat 89 x109/L
- Retic count
A 65 year old woman is referred to you because of memoryloss. Her family physician had received tests which included bilirubin of 28 mol/L and an LDH of 1560 U/L. He waspuzzled by these results.
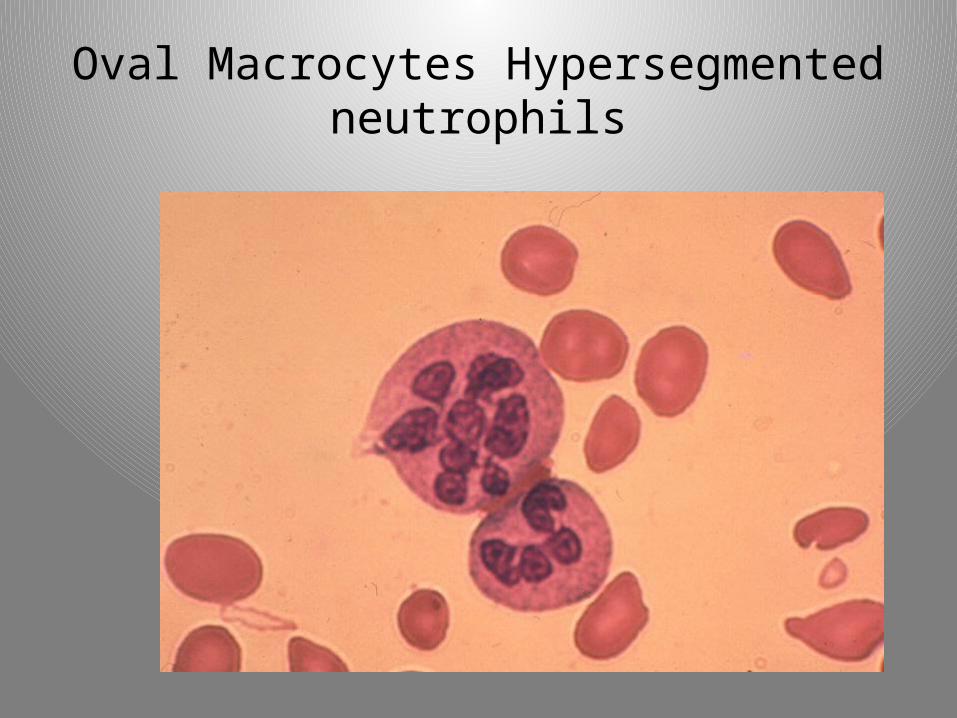
Oval Macrocytes Hypersegmented neutrophils

Megaloblastic Anemias
Vitamin B12Folic Acid

Reasons for measuring B12
• Investigation of macrocytic anemia• Investigation of any anemia• Investigation of fatigue• Routine Geriatric Screen• Investigation of neurologic symptoms

Symptom Complex
• Classic presentation uncommon• Often a screen in older patients• Memory loss prominent• Neuropathy• Non specific symptoms of anemia

Causes
Pernicious anemia• 10 % of all cobalamin deficiencies• Antibodies against intrinsic factor
– malabsorption

Causes of Low Serum B12
Malabsorption of free cobalamin• Pernicious anemia• Post gastrectomy state• Small bowel diseases

Causes of Low Serum B12
Malabsorption of food cobalamin• Atrophic gastritis• Postgastrectomy state• Chronic nonspecific gastritis • H2 receptor blocking agents, PPI

Tests
• CBC - RBC indices– Most are macrocytic
• Blood film– Macro-ovalocytes - hypersegmented polys
• Retic count
• Serum B12• Biochemical abnormalities
– LDH bilirubin elevated seconday to ineffective erythropoiesis an premature RBC destruction in the bone marrow

Folic acid deficieny
• Dietary source is vegetables• Absorption no specific carrier• Deficiency mainly dietary.• Alcoholism a risk• Anemia macrocytic• No neurologic symptoms• Measure Serum folate (food supplementation)

Therapy
Replace B12 - folic acid

Therapy
• Vitamin B12• IM• Oral• Folic acid
– pregnancy– treatment

Jaundice: Hemolytic anemias
• History of jaundice and anemia– Biochemical and clinical definition
• Elevated bilirubin: unconjugated hyperbilirubinemia in hemolysis (ddx: decreased hepatic uptake or conjugation CHF, Gilbert’s syndrome, neonatal jaundice)
• May have splenomegaly• May have a family history• anemia with reticulocytosis• specific morphologic changes• LDH : elevated• Specific tests follow morphology

What is the abnormality ?
Spherocytes

What is the abnormality ?
Bite cells
Oxidative hemolysis

What is the abnormality
fragment

Which anemia is this ?
Common anemias
• Iron deficiency• Megaloblastic anemias• Secondary anemias of chronic diseases • Hemolytic anemias: immune, non-immune Spherocytic
fragmentation

PRINCIPLES
• Anemia is not a disease• There is usually a cause• investigation should be logical • Start with CBC and Blood film• Leads to other tests
– non specific– specific
• Guides therapy