autoinflammatory and periodic febrile...
TRANSCRIPT

Autoinflammatory
and Periodic
Febrile Syndromes
John J. Cush, MD
Baylor Research Institute
Baylor University Medical Center
Dallas, Texas
Dr John Cush
@RheumNow

Disclosure Information
• Investigator—Amgen, Celgene, Novartis, Pfizer,
UCB
• Consultant—Abbott, BMS, Celgene,
Genentech, Janssen, Pfizer, Savient, UCB

Febrile Syndromes Defined
• Autoinflammatory syndromes: characterized by
attacks of inflammation unrelated to infection,
autoantibodies or Ag-specific T cells.
– Defines the innate immune system
– Typically seen in infants and children
• Periodic Fevers: subset of autoinflammatory syndr.
– Hereditary/monogenic or acquired
– Recurrent fever, inflammatory Sxs, Disease-free intervals
• FUO: fever >101oF for more than 2-3 wks,
documented on several occasions after
extensive evaluation (hospital x 1 week?)

Patterns of Fever Fever Patterns
◄Continuous: above baseline thru-out the day
(infection, sepsis, Typhoid fever, etc)
◄Continuous Fever (resp to antipyretics)
◄Remittant: rises but falls to an elevated
baseline (infection, SBE, abscess)
◄Quotidian: rises but falls to baseline daily
(malaria, SoJIA, AOSD)
◄Undulant (Pel-Epstein):Hodgkins lymphoma
◄Relapsing fever: typical of Borreliosis
Mackowiak P. Frontiers in Bioscience 9: 2297-2301

Fever in Rheumatic Disease
• HIGH GRADE FEVER – Still’s disease
– Macrophage activation syndrome
– Septic arthritis, opportunistic infections
– Polymyalgia rheumatica, Giant Cell arteritis
– Kikuchi-Fujimoto syndome
• LOW GRADE FEVER – Lupus
– Early onset of Rheumatoid arthritis
– Gout: often mistaken for acute septic arthritis
– Small Vessel Vasculitis (HSP, Sweets syndrome)
Carsons SE. Infect Dis Clin North Am. 1996 Mar;10(1):67-84

Periodic Fevers
ADOLESCENTS/ADULTS
• Adult-onset Still’s disease
• FMF
• Muckle-Wells syndrome
• Cyclic neutropenia
• Schnitzler syndrome
• Polymyalgia Rheumatica
• Giant Cell Arteritis
• Kikuchis syndrome
NEONATES/CHILDREN
• Systemic onset JIA
• TRAPS
• Familial Mediterranean Fever
• Cryopyrinopathies (CAPS)
– Familial Cold Auto- inflammatory
syndrome
– Muckle-Wells syndrome
– NOMID/CINCA
• PFAPA syndrome
• Blau Syndrome

Spectrum of Autoinflammatory Syndromes
Autosomal recessive
• Familial Mediterranean fever
• HyperIgD (HIDS)
• Deficiency IL-1Ra (DIRA)
• Deficiency IL -36R (DITRA)
• Familial pustular psoriasis
Majeed syndrome
Autosomal-dominant
• TRAPS
• FCAS
• Muckle-Wells syndrome
• NOMID/CINCA
• PAPA syndrome
Adapted from Haskes P. Pediatr Clin North Am. 2012 Apr;59(2):447-70
Granulomatous
• Blau syndrome
• Early onset sarcoidosis
Other, nongenetic
• Marshall (PFAPA) syndrome
• Systemic JIA / Adult Still’s
• Behçet syndrome
• Recurrent pericarditis
• Chronic recurrent multifocal
osteomyelitis (CRMO)
• Schnitzler syndrome
• Gout

INFEVERS
http://fmf.igh.cnrs.fr/ISSAID/infevers/

Febrile Disorders in Adults
Autoinflammatory % adult
• Schnitzler >80%
• DITRA > 80%
• Cyclic
Neutropenia 50%
• AOSD ~33%
• TRAPS <30%
• FMF <20%
• Muckle-Wells <20%
Rheumatic FUO adults
• AOSD
• Gout
• PMR/GCA/Vasculitis
• Hemophagocytic syndr
• Crohns colitis
• Sweets syndrome
• Kikuchi-Fujimoto syndr
• Lymphoma/leukemia

Understanding Autoinflammatory Syndromes
• Age
• Fever
– duration, magnitude, periodicity
• Cutaneous features
• Organ specific
– CNS
– Serositis
• Complications
– Amyloid
– Waldenstroms

Organization of the Immune System

Immune Responses
Immunity Innate Adaptive
Role 1st line Defense
(prime adaptive)
Recognition of self
from non-self
Response Minutes/Hrs
nonspecific
Days/Weeks
Ag-specific, Memory
Cells Epithelial, PMNs,
macrophages T, B, dendritic cells
Cytokines IL-1, IL-6, TNF, IL-8 IFN, IFN, IL-2, IL10
Provoked? stress, immunization or trauma Non-self, drugs
Disorders
Autoinflammatory :
innate responses w/o
AutoAbs
Autoimmune :
w/ auto-reactive T&B
cells, Ab
Prototypic Dz CAPS Lupus

Innate Immune Response
Tissue Damage
Microbes
DAMPs PAMPs
Pattern Recognition Receptors
TLR NLR CLR
, MSU, crystals, silica,asbestos
, hyaluron, ATP, HMGB-1
NLRP3
Inflammasome
NLR NOD like receptors TLR: Toll-like receptors CLR: C-type lectin receptor
IL-1
, Bacterial LPS,
PGN, flagellin,
zymosan,toxin

Inflammasome
http://flipper.diff.org/app/items/info/4713

Joint Pain and Fever
• 36 yr old Moroccan male w/ 5 yrs of intermittent
swelling/pain/warmth wrist, dorsum hand, elbow
• Episodes last x 3 days, fever, pink eye, CP
• Meds: On hydroxychloroquine x 1 yr (+ benefit?)
• Prior negative evaluation: included labs,
serologies, CXR, EKG, SF crystal negative
• Denies abdominal pain, LBP, heel pain, rash, hives
• +PPD 16 mm and 13cm Spleen on abdominal US

What is the most likely diagnosis for this
patient w/ episodes of fever, arthritis,
conjunctivitis?
1. Tuberculosis
2. Reactive arthritis
3. TRAPS
4. Adult-onset Still’s disease
5. Familial Mediterranean Fever

Familial Mediterranean Fever • Linked to Mediterranean Ancestry
• Ancestry should not exclude consideration
Samuels Medicine 1998;77:268-97.
Sephardic Jews,
Armenians, Turks,
North Africans,
Arabs,
Moroccans,
Italians, Greeks,
Japanese
United States:
uncommon in
Ashkenazi Jews.

Familial Mediterranean Fever - I
• Triad: Fever>38oC, Painful Serositis or Erythema
• Sephardic Jews, Armenians, Turks, N.Africans,
Arabs, Italians, Morrocans
• Bouts/Fever: lasts 1-3 d remit; variable periodicity
• 120K worldwide
• Onset:
childhood or
adolescents
• < 20 yrs in 80%
• MEFV gene
mutations
Padeh S. Rheum Dis Clin N Am 33 (2007) 585–623

Familial Mediterranean Fever - II
• Arthritis: recurrent monarthritis (chronic in 5% hip/SI)
– Peritonitis > Pleuritis > Pericarditis
– Skin: BLE erysipelas-like rash (painful)
– Myalgias, orchitis, aseptic meningitis, HSP, PAN
• Labs: high WBC, ESR, CRP during attacks
• Amyloidosis: manifest as proteinuria/nephrotic syndr.
• Dx made by rectal or BM Bx
• >100 missense mutations of MEFV
– 5 most common genotypes~80% of cases – (M694V, M6941, M680I, V726A, E148Q).
• Rx: Colchicine, Anakinra
Padeh S. Rheum Dis Clin N Am 33 (2007) 585–623
Crocus (Colchicum autumnale)

• Autosomal recessive MEFV mutation on gene 16p13
• MEFV (stands for MEditerranean FeVer)
– Encodes 781 AA protein Pyrin (AKA marenostrin)
– Pyrin: binds & inhibits caspase-1 • negative regulator of inflammasome function
– Defective pyrin (in PMNs) leads to unregulated Caspase-1 ( IL-1, IFNγ, TNFα, IL-6, IL-8)
• Over 100, mostly missense, mutations of MEFV
– 5 most common genotypes ~80% of cases
– (M694V, M6941, M680I, V726A, E148Q).
• Zygosity and mutation type determines the severity of the disorder and age of onset
Familial Mediterranean Fever

Sporadic Fevers
• 19 yr old Belgian male onset of febrile episodes
lasting 5-15 days, occurring 2-3 x yearly
– Assoc. w/ abdominal pain, LBP, arthralgia, T 40-41C
– Reponds to steroids
• Dx w/ AOSD, given HCQ, MTX without benefit
• At age 31 he develops new features of diarrhea,
proteinuria and creatinine = 2.3 mg/dl
• A diagnostic test was done

What Diagnostic Test Was Done?
1. ANA, dsDNA serologies
2. Ferritin
3. cANCA (PR3 Ab)
4. Colonoscopy w/ biopsies
5. Renal biopsy
Jadoul Kidney International (2001) 59, 1677–1682

TRAPS (AKA Hibernian Fever)
• 1945: 1st described in Irish, Scottish, Austrian, N. European
• Autosomal dominant; Missense mutations in genes encod-
ing for type I p55 TNF receptor (TNF-RI) (TNFRSF1A).
• 75% onset by age 10 yrs (mean 3 yrs; adults described)
• Characterized by arthralgia, myalgia, painful migratory rash,
abdominal pain, conjunctivitis, oral ulcers, scrotal swelling
• Febrile attacks that last 1-3 weeks
• Effective Rx: NSAID, Steroid (not colchicine)
– Rx:etanercept (anakinra in some) – Reports of worsening with infliximab
Haskes P. Pediatr Clin North Am. 2012 Apr;59(2):447-70
Arthritis & Rheumatism 2012; 64:908 ETN in 14 TRAPS pts
[----ETN-----] [ none ]

CAPS
Cryopyrin Associated Periodic Syndromes (also known as the Cryopyrinopathies)
• Autosomal dominant disorders
• Gain of function mutations of NACHT domain
of NLRP3 (includes the cold-induced
autoinflammatory syndrome-1 [CIAS1] gene)
• Cryopyrin(pyrin) expressed PMNs monocytes.
• FCAS, Muckle-Wells syndrome & NOMID
• Features: fever, urticarial-like rash,
conjunctivitis, bone and joint symptoms, and
elevated inflammatory markers such as CRP.
• CAPS patients respond well to IL-1 inhibition
Haskes P. Pediatr Clin North Am. 2012 Apr;59(2):447-70
Muckle-Wells Syndrome (MWS)
• 1st reported 1962
• Autosomal dominant CIAS-1 defect (lifelong)
• ~90% before age 20yrs; ~60% before 10yrs.
• Triad: rash, nerve deafness, amyloid nephropathy
• Urticarial rash, arthralgia, fever/chills 1/3,
abdominal pains 20%, conjunctivitis 10%
• 50-60% sensorineural hearing loss
• 25% develop amyloidosis
• Labs: elevated WBC, ESR, CRP
• Rx: IL-1 inhibition
Haskes P. Pediatr Clin North Am. 2012 Apr;59(2):447-70

Schnitzler Syndrome
• Rare, acquired autoinflammatory Dz in Adults
• Chronic nonpruritic urticaria & IgM gammopathy.
PLUS:
– Periodic fever <104F, arthalgia/itis, bone pain,
hepatosplenomegaly, lymphadenopathy,
increased WBC, ESR or anemia
• Other Sxs:lymphadenopathy, wt. loss, pancreatitis
• Complications: Disabling skin rash, fever, bone
involvement. Anemia or lymphoplasmacytic
malignancy (Waldenstroms in ~15% of pts.)
• Treatment: anakinra
Besada E. Clin Rheumatol. 2010 May;29(5):567-71 Lipsker D Medicine 2001; 80(1): 37-44.

19 yr. old autistic Nigerian male w/
recurrent urticaria, fever, pericarditis
• History began 9 mos ago with recurrent Urticaria
on Trunk, back, arms. 3-7 days fever 101-102F
• C/O occasional arthralgias, limping
• CP, pericarditis pericardial window 4 mos ago
• No response to HCQ, great response to steroids
• Hx: Autism, tympanostomies, congenital Ptosis
• Currently afebrile, no synovitis, nl HEENT
• Labs W 14.6, Hct 40, CRP 21.4 mg/dl, ESR53,
ACE 81, Ferritin 463, borderline +PR3 Ab

19 yr. old autistic Nigerian male w/
recurrent urticaria, fever, pericarditis
• What diagnostic treatment or test should you
order?
1.Trial of colchicine 0.6 mg bid
2.Trial of anakinra 100 mg sc qhs
3.TNF-R1 gene test for TRAPs
4.MEVF gene test for FMF
5.CIAS-1 gene test for CAPS

< 1 day FCAS IL-1 inhibitor CIAS-1
NLRP3
1-3 days
FMF Colchicine
Anakinra MEFV
MWS IL-1 inhibitor CIAS-1
NLRP3
3-7 days
HIDS Anakinra MVK
PFAPA Tonsillectomy
Steroids
Anakinra
7-21 days TRAPS Etanercept TNF-R1
Daily Fevers >39oC
SoJIA AOSD
Schnitzler
Anakinra
Tocilizumab
<16yr
16-35y
Algorithm for Undiagnosed Periodic Fever > 38oC
Fever Duration Dx Consideration Diagnostic Test/Intervention
NA
NA
<1 yr

Distinguishing Features of Autoinflammatory Dz
Adapted from Haskes P. Pediatr Clin North Am. 2012 Apr;59(2):447-70
Aphthous ulcers: PFAPA, HIDS, TRAPS,
Cyclic neutropenia
Pustulosis: PAPA, DIRA, DITRA, PASH
Arthritis: NOMID, Still’s, MWS, PAPA, DIRA
Conjunctivitis: TRAPS, MWS, FMF, Schnitzler,
DITRA, Cyclic Neutropenia
Common: Fever, serositis, arthralgia, myalgia (low PPV)
Amyloidosis: FMF, TRAPS, MWS, NOMID
CNS: MWS,
NOMID
Urticaria: CAPS/MWS, AOSD, SoJIA, Schnitzler

Italian Gal w/ Fever, sore throat, rash,
arthritis, serositis, lymphadenopathy, HSM
• 23 yr. WF admitted to hospital with 6wk hx of
fevers of 104F, rash, and a sore throat.
• C/O myalgias, BL wrist pain, abdominal pain, and
rash over the trunk, neck & extremities.
• PMHx: rheumatic fever at 9 yrs, FUO, hepatitis.
• Review of systems was otherwise negative.
• Hospital course (20d) was notable for pleuritis,
pericarditis, lymphadenopathy, splenomegaly,
WBC= 40K, and increased hepatic enzymes

What is the most likely diagnosis for this patient w/
prolonged fevers, arthritis, rash, serositis and
organomegaly?
1. Rheumatic fever
2. TRAPS
3. Adult-onset Still’s disease
4. Familial Mediterranean Fever
5. Schnitzlers syndrome

Still’s Disease
Systemic inflammatory disorder
Young adults (up to age 35yrs)
Quotidian fevers, evanescent rashes, arthritis, sore throat, serositis, organomegaly, leukocytosis and a marked acute phase response
No diagnostic or serologic tests
Syndrome = diagnosis of exclusion.
Systemic exacerbations and/or chronic arthritis, and disease-free intervals.
Cush JJ. Adult onset Still’s disease. Bull Rheum Dis 2000; 49(6):1-4

JIA Variants
JIA Variant % Age Sex ANA RF Features
Pauciarticular
Type 1 50 1-8 F <60% 0
<4 Joints
Uveitis
Pauciarticular
Type 2 10 9-16 M 0 0
Knee, Hip, Ankle
Juvenile Spondylitis
Polyarticular
RF+ 5 10-16 F <70% 100
RA in children
Erosive Dz >50%
Polyarticular
RF(-) 15 3-9 F 0 0
Symmetric polyarthritis
Erosive <15%
Systemic 20 5-16 F=M 0 0
Fever, rash, serositis,
organomegaly, incr.
WBC, ESR, CRP
AOSD - 17-35 F=M 0 0
Fever, rash, serositis,
organomegaly, incr.
WBC, ESR, CRP

Sir George Frederick Still (1868–1941)
“On a form of chronic joint disease in children”
1897
Farrow SJ. Rheumatology 2006; 45:777

Quotidian (Spiking) Fever
Patterns in AOSD Quotidian

Author/Yr #AOSD(%) Time (yrs) Source
Bywaters ‘71 14 20 Rheum. Dept
Goldman ‘80 13 4 Rheum. Dept
Del Paine ‘83 7 9 Rheum. Dept
Cush ‘85 21 15 Rheum. Dept
Nkoghe ’02 17 13 Infect. Dz Dept
Mert ’03 20(15%) 17 Infect. Dz. Dept
Bujak ‘73 10 (5%) 11 200 FUO pts
Aduan ‘79 21 (6%) 15 347 FUO pts
Larson ‘82 5 (5%) 10 109 FUO pts
Kazanjian ‘92 5 (6%) 6 86 FUO pts
Knockaert ‘92 4 (9%) 9 45 FUO pts
Tabak ’03 13 (11%) 17 117 FUO pts
Frequency of AOSD and FUO
1-2 per year in most hospitals; AOSD #1 Rheumatic cause of FUO

Rheumatoid or “Still’s” Rash
• Characteristically evanescent (esp. with fever)
• Salmon-pink (faint erythema) maculopapular
• Trunk, neck, and extremities
• Dermatographism
• Koebner phenomenon
Uncommon in AOSD: pruritus, urticaria, dermal
plaques, facial rash, alopecia, erythema
nodosum, Raynaud’s phenomena



LK: Carpal Ankylosis
8/72 3/73

Intercarpal Ankylosis
Cush JJ, et al. Arthritis Rheum; 30:186-94, 1987

Common Features
Sore throat 70%
Weight loss 65%
Myalgias 75%
Hepatosplenomegaly 40%
Hepatic dysfunction 70%
Lymphadenopathy 65%
Pleuritis 40%
Pericarditis 30%
Abdominal Pain 30%
Pneumonitis 20%
Myocarditis rare
Cush JJ. Adult onset Still’s disease. Bull Rheum Dis 2000; 49(6):1-4
Myocarditis
19yoLM w/ T 104, WBC 64k, Pleuro-
pericarditis, Myocarditis, Splenomegaly

Lab Abnormalities in AOSD
• Negative ANA & RF 95%
• Neutrophilic leukocytosis 90%
• Anemia chronic disease 75%
• ↑↑ESR, ↑CRP, ↑Platelets 90%
• Hypoalbuminemia 75%
• Hyperferritinemia 50%
Cush JJ. Adult onset Still’s disease. Bull Rheum Dis 2000; 49(6):1-4
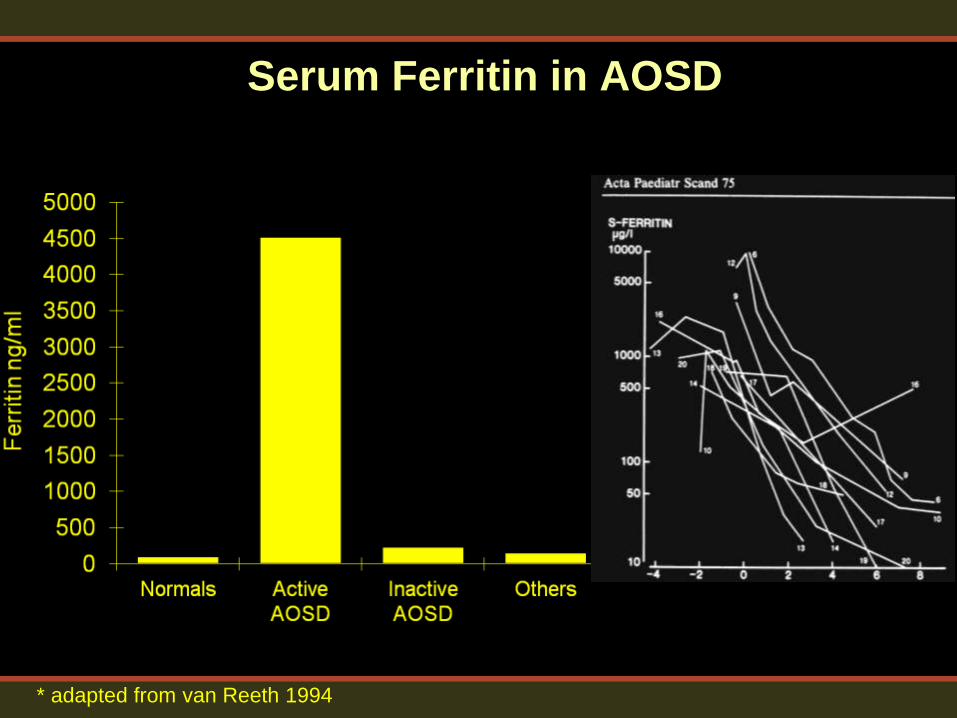
Serum Ferritin in AOSD
* adapted from van Reeth 1994

Hemophagocytic syndrome
(Macrophage Activation Syndrome - MAS)
• Dx: Histiocytic erythrophagocytosis on BM Bx
• Dz: SLE, RA, AOSD, SoJIA, PAN, MCTD, PSS, Sjogrens,
Sarcoid, Bacterial/Viral Infx, TBC, NHL, renal transplant
• Familial: rare, autosomal recessive, perforin gene mutation
• Fever, hepatosplenomegaly, LFTs, pancytopenia, DIC
• Labs: Very low > high WBC, CRP but ESR
– Hyperferritinemia
• High mortality rate: 8.2 - 38.5%
– Assoc w/ corticosteroid dose and thrombocytopenia
• Rx: Steroids, CyA, IL-1 Inhibitors, Abx (underlying dz)
Dhote R, etal. Arthritis Rheum 2003; 49:633
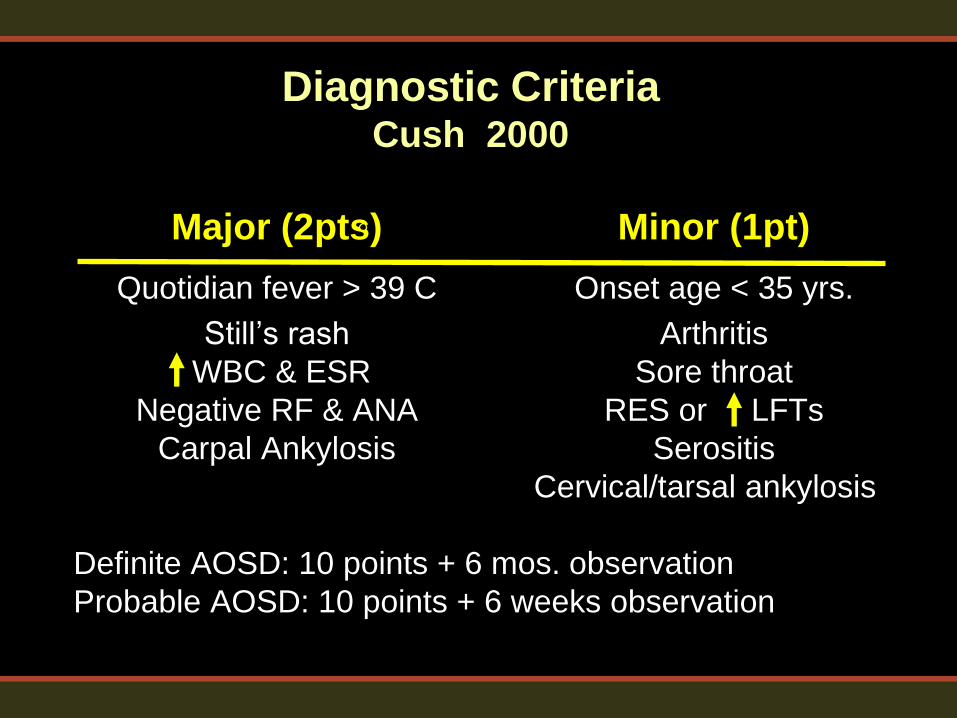
Diagnostic Criteria Cush 2000
Major (2pts) Minor (1pt)
Quotidian fever > 39 C Onset age < 35 yrs.
Still’s rash Arthritis
WBC & ESR Sore throat
Negative RF & ANA RES or LFTs
Carpal Ankylosis Serositis
Cervical/tarsal ankylosis
Definite AOSD: 10 points + 6 mos. observation
Probable AOSD: 10 points + 6 weeks observation

AOSD: Keys to Diagnosis
• Daily Fevers > 39oC
• Circadian illness: Temps same time EVERY
night or later afternoon (not 7AM!)
• “Still’s rash” - evanescent
• Confirm using Cush or Yamaguchi Criteria
• Diagnostic response to IL-1 inhibition?
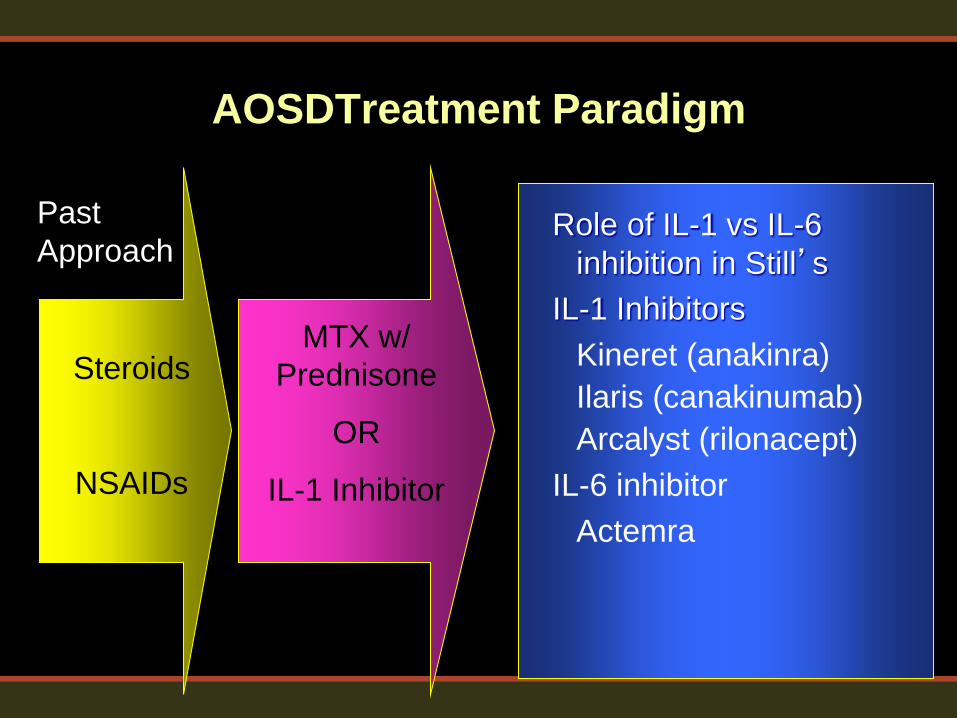
AOSDTreatment Paradigm
Steroids
NSAIDs
MTX w/
Prednisone
OR
IL-1 Inhibitor
Role of IL-1 vs IL-6
inhibition in Still’s
IL-1 Inhibitors
Kineret (anakinra)
Ilaris (canakinumab)
Arcalyst (rilonacept)
IL-6 inhibitor
Actemra
Past
Approach

Effects of IL1, IL6, and TNF
Clinical Feature IL-1 IL-6 TNF
Fever > 39C + + +
Exanthem + 0 +
Myalgias + +/- +
Arthralgias/itis + + +
Weight loss + + ++
Leukocytosis + ++ +
Acute Phase Rxn + ++ +


Biologic Therapies in AOSD
• TNF inhibitors
– Effective in polyarthritis
– Less so for systemic disease (Infliximab?)
• Anti-IL-6 Tocilizumab
– Studied in SoJIA and AOSD
• Anti-IL-1 Anakinra
– Systemic and articular disease
• IL-18 as a Target?

Tocilizumab in AOSD
• 36 pts w/ OL TCZ – 8mg q 2-4 weeks in
MTX/DMARD-IR pts (42% prev Rx anakinra)
• Joints more refractory than systemic Sxs Ortiz-Sanjuan etal. Arthritis Rheumatol. 2014 Feb
WBC CRP
Ferritin Pred

Anakinra: Time to Response in SoJIA/AOSD
Ann Rheum Dis. 2008 Mar;67(3):302-8

Anakinra: Time to Response in AOSD
Laskari et al. Arthritis Res Ther. 2011; 13(3): R91.
Overall 7/25 Nonresponders

BL/AOSD: 55 WM, w/ ST, pleuritic CP, fever
104F, 65# wt loss, WBC 50k, Ferritin 28,000
Anakinra 100mg/d
Prednisone 20 mg/d Methotrexate 12.5-20 mg/wk
Leflunomide 20 mg/d Infliximab Singulair, colchicine

Anakinra
Microarrays pattern of inflammation that improves w/ Anakinra Rx

Cost of Therapies
Generic Dose Given Annual
Cost
Methotrexate 15-20 mg po Weekly $600
Etanercept 50 mg sc Weekly $35000
Anakinra 100 mg sc Daily $47000
Canaknumab 180 mg sc Every 8
wks $114,000
Rilonacept 150 mg sc Every 2
weeks $288,000
Tocilizumab 4-8 mg/kg IV Every
month $22-44,000

Injection Site Reactions
• Anakinra ISR may occur in 1st 28 days
• Frequency of ISR
– Anakinra 71% (RA)
– Canakinumab 9% (CAPS)
– Rilonacept 48% (CAPS)
Data from Package inserts: anakinra, canakinumab, rilonacept Photos courtesy J. Cush, MD

Understanding Febrile Syndromes
• Adults: Stills, Schnitzler, TRAPs, FMF
• Fever: 1-3 FMF, 7-21 TRAPS, qd AOSD
• Cutaneous features
– Hives: MWS, Still’s
– Pustular: PAPA, DIRA, DITRA, PASH
• Organ specific
– CNS - MWS
– Serositis: AOSD, TRAPs, FMF
• Complications: MAS
– Amyloid: FMF, TRAPS, CAPS
– Waldenstroms, gammopathy; Schnitzlers

Questions?