autoimmune bullous lesions of skin
TRANSCRIPT

IMMUNE MEDIATED BULLOUS LESIONS
OF SKIN
BY EKTA JAJODIA

Blister – fluid filled cavity within or beneath the epidermis
VESICLES( <0.5cm in diam)
BULLAE(>0.5cm in diam)
PATHOLOGICAL EVELUATIONApproach to diagnosis-
1. Anatomical level of split/blister separation plane2. Mech. of blister formation3. In case of subepidermal blisters – presence/absence of
inflammation, pattern and specific cell types involved

ANATOMICAL LEVEL OF SPLIT Blister may form at any one of four diff levels-
1. Subcorneal/intracorneal2. Within spinous or malphigian layers3. Suprabasilar4. Subepidermal

MECHANISM OF BLISTER FORMATION
1. SPONGIOSIS – Accumulation of ECF within epidermis with resultant separation of keratinocytes
Stellate appearance of keratinocytes
2. ACANTHOLYSIS – Loss of keratinocyte cell-cell contact
Keratinocytes are rounded with condensed cytoplasm, large nuclei,peripheral condensation of chromatin and prominent nucleoli
Acantholytic cells are viable

3. RETICULAR DEGENERATION (Ballooning degeneration) – intracellular edema with secondary rupture of keratinocytes and its death
Desmosomal attachments connects strands of ruptured keratinocytic membrane to intact keratinocyte – gives irregular meshwork appearance to epidermis
4. CYTOLYSIS – disruption of keratinocytes- occurs when high levels of friction/heat damages structural matrix(keartin) and desmosomes
5. BASEMENT MEMBRANE ZONE DISRUPTION

AUTOIMMUNE BULLOUS DISEASES -TARGET ANTIGENS
DISEASE TARGET ANTIGENS
Pemphigus foliaceus Desmoglein 1
Herpetiform pemphigus Desmoglein 1
IgA pemphigus(SPD type) desmocollin 1
IgA pemphigus(IEN type) Desmoglein 1 or 3
Pemphigus vulgaris Desmoglein 3
Epidermolysis bullosa acquisita Type VII collagen

DISEASES TARGET ANTIGENS
Paraneoplastic pemphigus Desmoglein1,3Desmoplakin 1,2
Bullous pemphigoid BPAg1(230kDa)BPAg2(180kDa)
Pemphigoid gestationis BPAg2(180kDa)
Dermatitis herpetiformis Tissue transglutaminase
Linear IgA bullous dermatosis LABD97
Ocular cicatricial pemphigoid plectin
Cicatricial pemphigoid BPAg2, epiligrin
Deep lamina lucida pemphigoid 105kDa
Anti-p200 pemphigoid 200kDa

PEMPHIGOUS GROUP
Acantholysis – mech. of bulla formation here
Divided into 5 types-1. P. vulgaris – reactive form is P. vegetans2. P. foliaceus – lupus like variant- P. erythematosus Endemic variant – folo selvagem3. IgA pemphigus4. Drug induced pemphigus5. Paraneoplastic pemphigus

PATHOPHYSIOLOGY
Target Ags of P. are located in desmosomes which are prominent adhesion molecules Desmosome complex contains- a. Transmembrane constituents – desmoglein(DSG) and
desmocollins (DSC)b. Cytoplasmic constituents – plakoglobin(PG), plakophilin(PP)
and desmoplakin(DP) ECD of transmembrane constituent form dimers with adjacent
cell
Cytoplasmic domain of transmemb. constituent bind to PG

This PG links intermediate filaments (keratins) to desmosome via DP
DESMOSOME COMPLEX

ECD of DSG and DSC are targets for Abs
DSG1 – expressed in upper layers of epidermisIf Abs form- skin lesions occurNo mucous membrane lesions
DSG3 – expressed in deep layers of epidermis and mucous membraneIf Abs form- oral lesions with or without skin lesions occur
DISEASES TARGET ANTIGENS
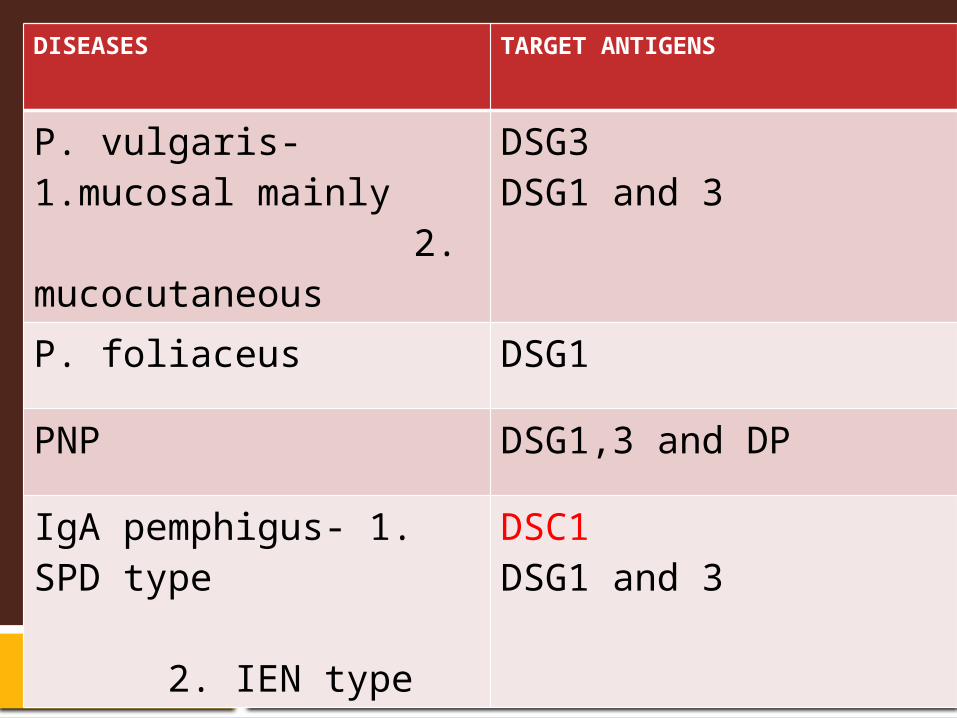
P. vulgaris- 1.mucosal mainly 2. mucocutaneous
DSG3DSG1 and 3
P. foliaceus DSG1
PNP DSG1,3 and DP
IgA pemphigus- 1. SPD type 2. IEN type
DSC1DSG1 and 3

PEMPHIGUS FOLIACEUS Recurrent crops of flaccid bullae that easily rupture – so shallow erosions and erythematous plaques Initially in face and trunk – then spreads to involve large areas of body Mucous membrane involvement is rare Target Ag – DSG1Ab – IgG4 subclass 2 types- a. lupus like – P. erythematosus b. endemic variant - fogo selvagem(wild fire) Develops in those who lives near rivers- its said that a black fly(simulium) may be a cause

Pemphigus : foliaceus erythematous : vulgaris : vegetans
SUPERFICIAL
DEEP

HISTOPATHOLOGY Earliest change – formation of vacuoles in intercellular spaces in upper layers of epidermis – these expand leading to cleft formation
Late lesions – epidermis- hyperplastic with parakeratosis and orthokeratosis
Superficial bulla with split high in granular layer or just beneath stratum corneum
Dyskeratotic cells with hyperchromatic nuclei – distinctive feature of granular layer
Bulla contains fibrin, neutrophils and scattered acantholytic keratinocytes (no bacteria present)

Superficial dermis is edematous with mixed inflammation with both eosinophils and neutrophils
Direct immunofluorescence – intercellular staining for IgG and C3 in both affected and normal skin
Indirect immunofluorescence – demonstrates circulating antibodies in nearly 90% of non endemic cases

2. Subcorneal blister c/o neutrophils and acantholytic cells3.Dyskeratotic hyperchromatic granular cells are diagnostic4. IgG deposited in upper layers of epidermis

PEMPHIGUS VULGARIS Target antigen DSG3 in only mucous lesion In case of mucocutaneous DSG3 and 1 both Abs are predominantly IgG4 subclass Initial lesion is oral blister with ulcers and erosions – weeks to months later cutaneous lesions In addition to oral lesions , other mucosal lesions may develop - conjunctiva, larynx and rarely esophagus, urethra, vulva, vagina
HISTOPATHOLOGY - earliest changes- edema and disappearance of intercellular bridges of keratinocytes in lower epidermis

Established lesions – suprabasal bullae with acantholysis Basal cells lose their intercellular bridges but remain attached to dermis giving a tombstone appearance Blister cavity contains acantholytic cells with some eosinophils and neutrophils Dermal changes are usually mild, superficial mixed inflammatory cell infiltrate No histological difference between drug induced P. vulgaris from idiopathic cases Immunostaining with monoclonal Ab 32-2B – detects DSG 1 and 3 – patchy pattern of staining seen in idiopathic cases and not in drug induced type DIF – demonstrates IgG in intercellular regions of epidermis

The earliest changes consist of intercellular edema with eosinophilic spongiosis leading to loss of intercellular bridges in the lower epidermis
SUPRABASAL BLISTER
The suprabasal blister contains few acantholytic cells, neutrophils and eosinophils. Note the dermal papillae lined by a single layer of basal keratinocytes, so-called villi

Lace like intercellular space deposition of IgG
PV – suprabasilarPF – subcorneal/within granular layer
IgA PEMPHIGUS
Intraepidermal vesicobullous eruption
Most common sites are axilla and groin. Can involve trunk and proximal extremities Mucous membranes are usually spared
2 types-1. Subcorneal pustular dermatosis (SPD) type2. Intraepidermal neutrophilic(IEN) type – lesions with central
crusts and peripheral vesiculation- so called sunflower lesions target Ags – in SPD type – DSC 1 in IEN type – DSG 1and 3

HISTOPATHOLOGY
In SPD type – sub corneal pustules with mild acantholysis In IEN type – intraepidermal pustules Underlying dermis shows mild inflammatory cell infiltrate
DIF – Intercellular deposition of IgA in epidermis In SPD type – increased intensity of staining in upper epidermis In IEN type – IgA staining is throughout the entire epidermis
IgG is present in small number of cases – known as IgA/IgG pemphigus

SPD – subcorneal pustule
Neutrophils and fibrin in blister cavity

PARANEOPLASTIC PEMPHIGUS Characterized by polymorphous skin lesions with features of both
erythema multiforme and pemphigus vulgaris in association with internal neoplasms, esp. NHL Other ass. are Hodgkin's disease, thymoma, hepatocellular carcinoma, MFH, castleman’s disease, etc PNP can precede diagnosis of malignancy, particularly in patients who develop castleman’s disease, or it may develop many years after development of tumor
7 clinical variants are recognized -1. Erythema multiforme-like (vacuolar interface dermatitis)2. pemphigoid-like (subepidermal blister)3. Pemphigus-like (suprabasilar blister)

4. GVHD-like5. Lichen planus pemphigoid/ lichen planus like (lichenoid inflammation)6. Cicatricial pemphigoid-like7. Linear IgA dermatosis-like
Poor prognosis
3 or more Abs are present in same patient-1. DP 1 ,22. Envoplakin3. DSC 2 ,34. DSG 1 , 35. Periplakin6. Plectin

Abs against DSG 3 are IgG 1 or 2 ( in P.vulgaris against DSG3 is IgG4) Autoantibodies may get deposited in skin, lungs, and other organs and may produce damage to these organs. Known as “paraneoplastic autoimmune multiorgan syndrome”(PAMS) Treatment is aimed at underlying malignancy to control the autoantibody production
HISTOPATHOLOGY - Lichenoid tissue reaction/ interface dermatitis with extension of infiltrate into reticular dermis Mostly lymphocytes but occasional eosinophils and neutrophils Suprabasal acantholysis and clefting may be seen
DIF – Intercellular and BM staining with C3 and IgG

Lichen planus like (lichenoid tissue reaction) and P. vulgaris like (suprabasal blister)
Both intercellular and BM staining with IgG

SUBEPIDERMAL BLISTERS To understand this , it is essential to have some knowledge of epidermal basement membrane zone(BMZ) From epidermis to dermis – 4 distinct components of BM1. Basal keratinocyte plasma membrane2. Lamina lucida3. Lamina densa4. Sublamina densa zone – including anchoring fibrils
BASAL KERATINOCYTE PLASMA MEMBRANE Plasma membrane incorporates hemidesmosomes Components of hemidesmosomes- 1. Intracellular component – Major bullous pemphigoid
antigen(BPAg1) / 230 kDa and plectin

2. Transmembrane component – Minor bullous pemphigoid antigen (BPAg2)/180kDa and α6β4 integrin
Abs to BPAg1 – in bullous pemphigoid
Abs to BPAg2 – in bullous pemphigoid pemphigoid gestationis cicatricial pemphigoid linear IgA bullous dermatoses
Abs to β4 of α6β4 - ocular cicatricial pemphigoid
Mutation of β4 - junctional epidermolysis bullosa

LAMINA LUCIDA
Weakest link in dermal-epidermal junction (DEJ) – so easily severed
M/L Ags ass with lamina lucida – laminin 5, 6, 1 uncein nidogen
defect in this Ags are common in Epidermolysis bullosa

LAMINA DENSA
main component is type IV collagen
Consist of 6 different chains alpha 1-6
Other components are- laminin1, nidogen, precelan

SUBLAMINA DENSA ZONE
Main component is anchoring fibrils(AF) which tether epidermis to papillary dermis
AF are composed of type VII collagen and laminin 332
Abs to type VII collagen seen in – EBA Bullous SLE

SALT-SPLIT SKIN IMMUNOFLUORESCENCE
Variant of indirect immunofluorescence Normal skin from a normal person is taken and soaked in 5ml NaCl
After 24hrs , the salt solution induces a subepidermal blister in the normal skin at the level of lamina lucida
Indirect immunofluorescence done- patient’s serum directed against the salt-split skin

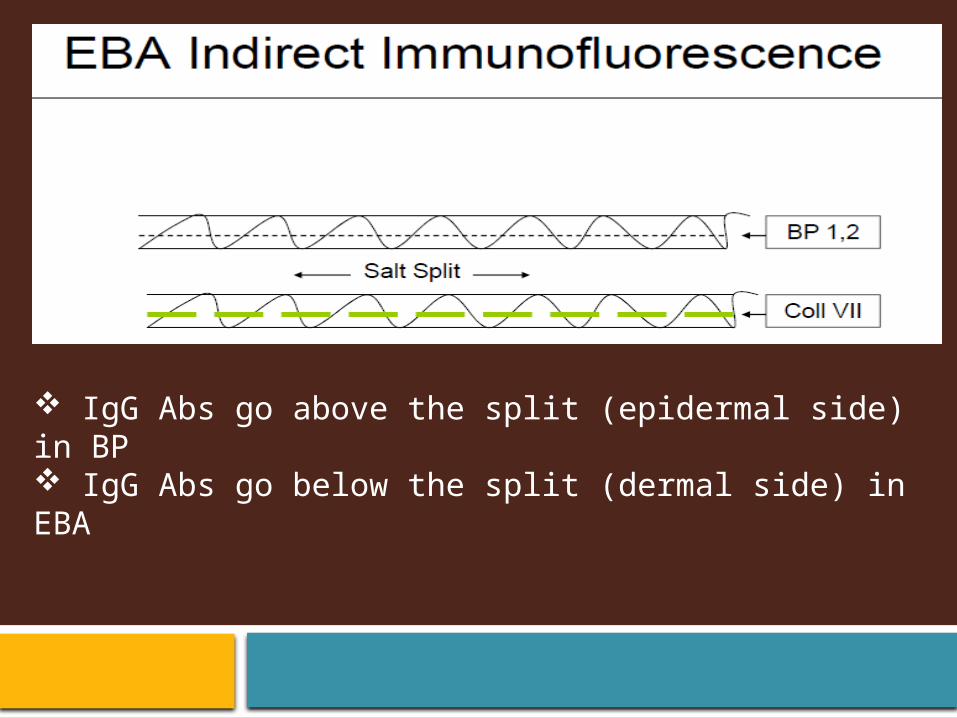
IgG Abs go above the split (epidermal side) in BP IgG Abs go below the split (dermal side) in EBA

B- Bullous pemphigoid; C - EBA

SUBEPIDERMAL BLISTERS
INFLAMMATORY CELLS DISEASES
With litle inflammation EB
With lymphocytes PNP
With eosinophils BPPemphigoid gestationis
With neutrophils DHLinear IgA bullous dermatosis

EPIDERMOLYSIS BULLOSA ACQUISITA Non inflammatory subepidermal bullae develop in areas subjected to minor trauma such as extensor surface of limbs Target antigen – EBA antigen which is a 290 kDa type VII collagen – a major component of anchoring fibrils
HISTOPATHOLOGY- classic form – non inflammatory subepidermal blisters bullous pemphigoid like – inflammatory blisters – mostly lymphocytes and neutrophils PAS stain- BM is split and most of the PAS positive material are in blister roof
DIF – linear deposition of IgG / C3/ C5 along BM zone
A useful clue to the presence of Abs targeting type VII collagen is presence of u-serrated pattern of linear IgG deposition Routine DIF cannot distinguish between EBA and bullous pemphigoid
SALT-SPLIT SKIN TECHNIQUE – Abs bind to dermal floor, deposited below lamina densa
Fluorescence overlay antigen mapping (FOAM) technique – can be used to determine site of deposits

Non inflammatory subepidermal bulla
Serrated deposition of IgG in blister base

BULLOUS PEMPHIGOID
Most common subepidermal blister Occurs primarily in elderly M/L tense bullae develop on normal or erythematous skin Oral lesions seen in 10-40% , but involvement of other mucosal areas is rare May occur in childhood – two types1. Infantile BP – in 1st yr of life – in acral areas2. Localised vulval BP- confined to vulva only Many clinical variants – 1. vesicular pemphigoid2. Pemphigoid vegetans3. Polymorphic pemphigoid 4. Pemphigoid excoriee

5. Drug induced pemphigoid6. Pemphigoid nodularis
Target antigens – BPAg1/230 kDa and BPAg2/180kDa Abs are – IgG4 and IgG1 Abs to BPAg2 is more associated with oral lesions, less responsive to steroids and poor prognosis
HISTOPATHOLOGY- Unilocular subepidermal blisters cell rich type – blister develop on erythematous skin - eosinophils predominant cell in blister cavity and in dermis – more than in arthropod bite reaction cell poor type – blister develop on normal skin – scant perivascular lymphocytic infiltrate with few eosinophils

In lesions of several days duration - blister may appear intraepidermal at its periphery as a result of regeneration
‘Caterpillar bodies’ – segmented , eosinophilic, PAS positive globules arranged in linear array in roof of blisters – feature of porphyria cutanea tarda – sometimes seem in BP
DIF – linear , homogenous deposition of IgG/C3 along BM
Salt-split skin technique- deposition found on the epidermal side of the blister

FIGURE 9-16. Bullous pemphigoid. (A) Prebullous phase, eosinophils are present at the dermoepidermal junction and in the dermis. (B) Cell-rich variant, subepidermal blister formation and an inflammatory infiltrate composed predominantly of eosinophils and a few neutrophils in the dermis and bullous cavity. (C) Cell-poor variant, subepidermal blister with few inflammatory cells.

Vesicular pemphigoid. There is a small subepidermal blister
subepidermal blister, the lumenof which contains eosinophils

Bullous pemphigoid. The basement membrane zone shows a linearpattern of staining for C3.
Salt-split skin IF – deposits on the blister roof (epidermal side)

PEMPHIGOID GESTATIONIS aka herpes gestationis rare, pruritic, vesicobullous dermatosis of pregnancy and puerperium occasionally seen in association with hyadatidiform mole or choriocarcinoma onset is in 2nd or 3rd trimester Subside within several weeks of delivery diagnosis can be made by commercially available BP180 ELISA Rarely neonate develops vesicular lesions due to transfer of maternal BP180 autoantibodies IgG1 class Ab (pemphigoid gestationis factor) is formed against a placental antigen – this cross reacts with BP180 antigen of BM

HISTOPATHOLOGY Early lesion – marked edema of papillary dermis Superficial and mid dermal infiltrate by lymphocytes, eosinophils and histiocytes Infiltrate is predominantly perivascular in location Established blister – is subepidermal , contains similar inflammatory infiltrate within the cavity Eosinophilic microabscesses may be formed in dermal papillae
DIF – Linear pattern of IgG or C3 in BM zoneSalt split skin – deposits in epidermal side
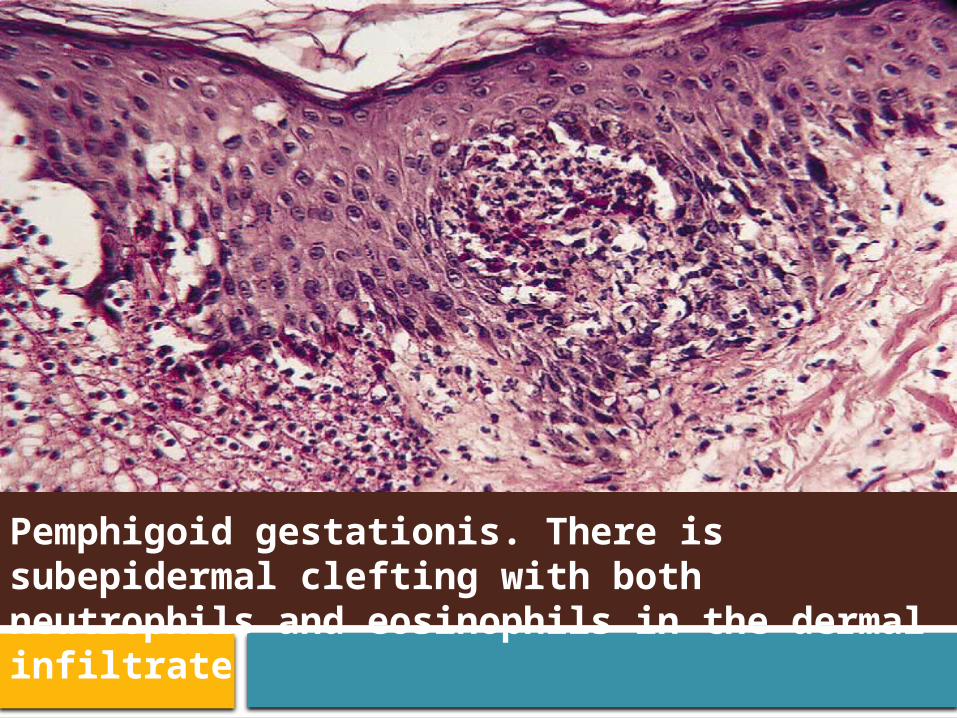
Pemphigoid gestationis. There is subepidermal clefting with both neutrophils and eosinophils in the dermal infiltrate
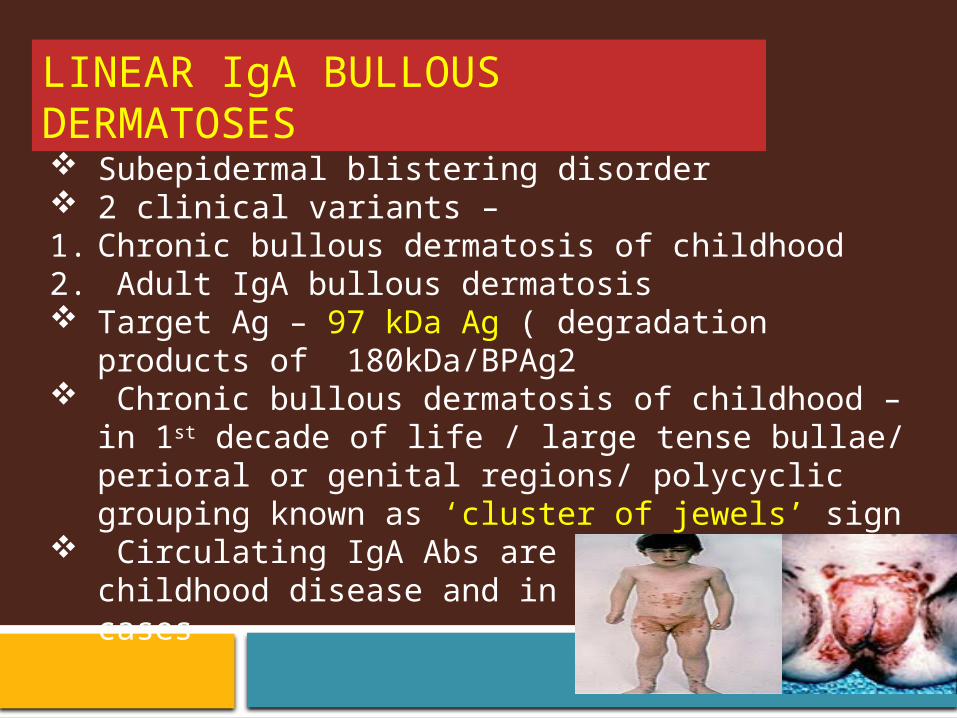
LINEAR IgA BULLOUS DERMATOSES Subepidermal blistering disorder 2 clinical variants – 1. Chronic bullous dermatosis of childhood2. Adult IgA bullous dermatosis Target Ag – 97 kDa Ag ( degradation products of
180kDa/BPAg2 Chronic bullous dermatosis of childhood – in 1st decade of life
/ large tense bullae/ perioral or genital regions/ polycyclic grouping known as ‘cluster of jewels’ sign
Circulating IgA Abs are present in 70% of childhood disease and in 20% of adult cases
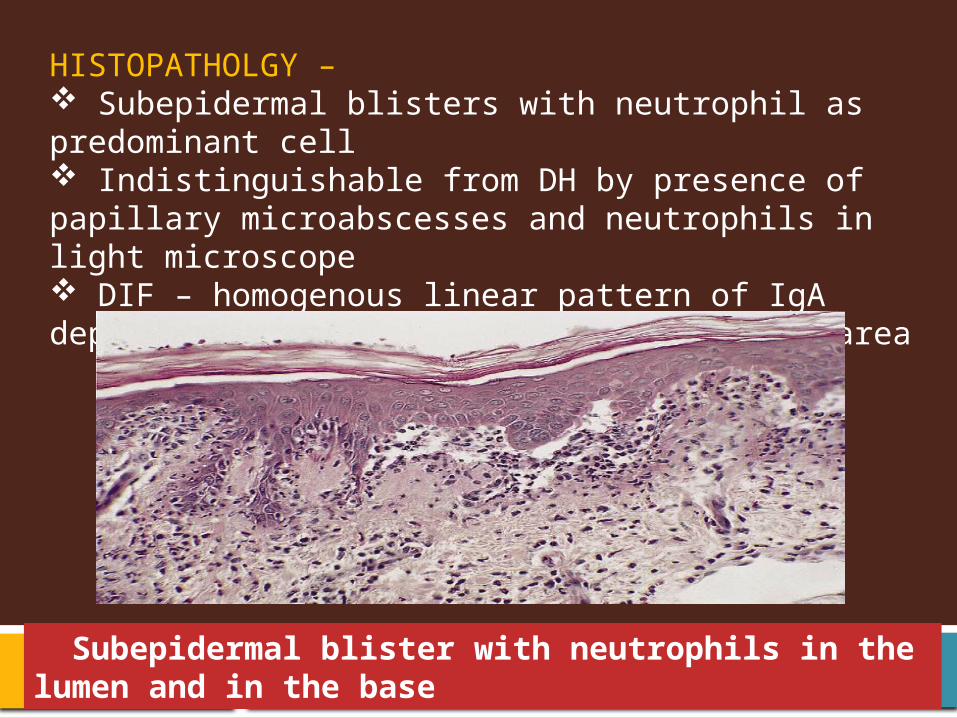
HISTOPATHOLGY – Subepidermal blisters with neutrophil as predominant cell Indistinguishable from DH by presence of papillary microabscesses and neutrophils in light microscope DIF – homogenous linear pattern of IgA deposition along BM zone of non-lesional area
Subepidermal blister with neutrophils in the lumen and in the base

DERMATITIS HERPETIFORMIS Subepidermal blistering disorder – intensely pruritic papules and vesicles – bullae are uncommon Ass. with high incidence of gluten sensitive enteropathy – in 90% cases and also with internal cancers, esp intestinal lymphoma Target Ag – tissue transglutaminase (tTG) sites- elbows, knees, shoulders, nape of neck onset – early adult life Gluten free diet – reversal of villous atrophy and skin lesions / also protective effect against development of lymphoma IgA Abs formed in gut binds with skin transglutaminase(TG) In skin 6 TG isoenzymes are present

Deposits mainly seen are IgA/TG3 aggregates in small blood vessels in papillary dermis This complex activates complement – chemotaxis of neutrophils in papillary dermis Also serum levels of IL-8 increases - increases the expression of CD11b on neutrophil cell surface – increase neutrophil function – enzymes released by these neutrophils destroy two BM components (laminin and type IV collagen) – formation of blisters
HISTOPATHOLOGY – Early lesions – collection of neutrophils and occasional eosinophils at tips of dermal papillae – papillary microabscesses Fibrin is also present at the tips of dermal papillae – imparting a necrotic appearance

In lesions of 36-48 hrs – neutrophil fragmentation occurs Very rarely intraepidermal neutrophils occur – confusion with IgA pemphigus
In older lesions – subepidermal vesiculation occurs Initially multilocular blisters due to interpapillary ridges – but after few days these attachments break down – formation of unilocular blister
Distinction between DH and linear IgA bullous dermatosis is impossible histologically Older lesions may resemble BP – eosinophils more predominant in the latter condition

DIF – Granular / fibrillary/ thready deposits of IgA in dermal papillae of perilesional and uninvolved skin
Deposition is greatest in normal skin adjacent to an active lesion
If DIF testing is negative – repeat test – negative results of DIF testing of 2 appropriately selected biopsy sites are strong indication that patient does not have DH

A- linear deposition of IgA along BM in linear IgA dermatosisB- granular deposits of IgA in the dermal papillae in DH
Dermatitis herpetiformis. A- There is a subepidermal blister , B/C- A microabscess is present in a dermal papilla


DERMATITIS HERPETIFORMIS


PEMPHIGUS FOLIACEUS

THANK
YOU