atésie de l’œsophage (ao)...–savoi la diffée si l’état de l’enfant est péoupant ou...
TRANSCRIPT

Atreacutesie de lrsquoœsophage (AO) Malformations associeacutees et eacuteleacutements du
pronostic
Pr Christian PIOLAT
Hocircpital Couple Enfant ndash CHU Grenoble
Universiteacute Joseph Fourier
Enseignement DESC Chirurgie Peacutediatrique mardi 1er octobre 2013
AO deacutefinition et classification
bull Interruption congeacutenitale de lrsquoœsophage dans sa portion thoracique avec ou sans fistule tracheacuteo-oesophagienne
bull 5 types anatomiques Classification de Ladd et Swenson
Epideacutemiologie
bull 14000
bull AO isoleacutee = 50 ndash sporadique ndash risque de reacutecurrence intra-familiale lt 1
bull AO associeacutee = 50
ndash Anomalies chromosomiques 8-27 (tri 13 18 21) ndash Del 22q112 (syndrome veacutelo-cardio-facial) ndash Associations VATER VACTERL VACTERL-H (hydroceacutephalie) ndash Syndromes CHARGE Feingold Opitz Pallister-Hall Potter
laquo schisis syndrome raquo Goldenhar G syndrome hellip
VATER - VACTERL
bull Vertebral
bull Anorectal
bull Tracheo
bull Esophageal
bull Radial limb renal anomalies
bull Limb anomalies
7-8 des AO
CHARGE
bull Coloboma
bull Heart defect
bull Choanal atresia
bull Growth and mental retardation
bull Genital hypoplasia
bull Ear anomalies
AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
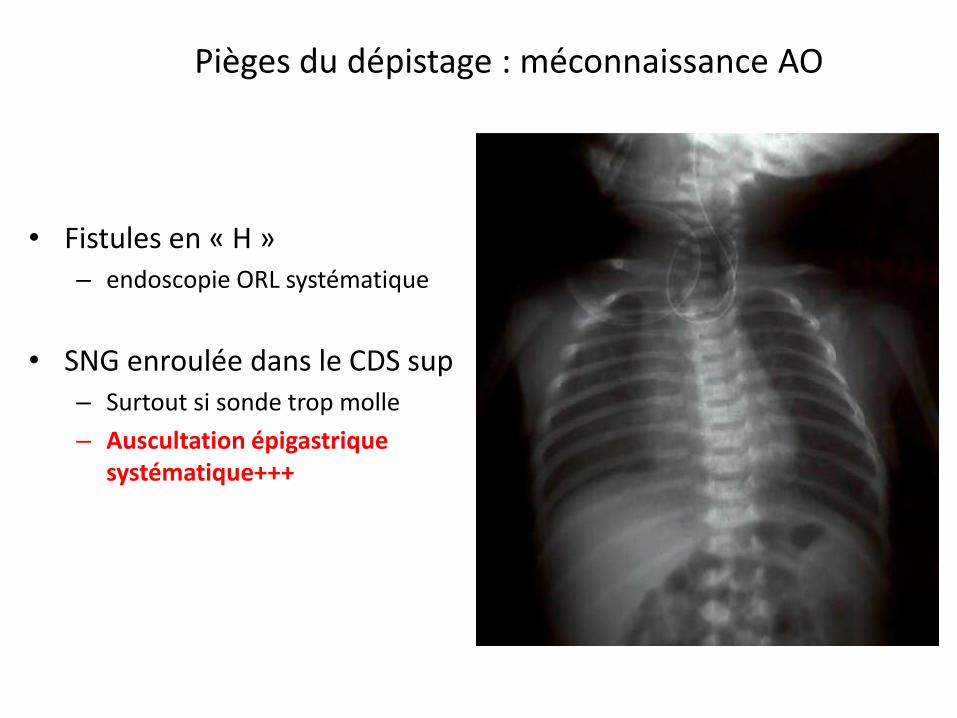
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

AO deacutefinition et classification
bull Interruption congeacutenitale de lrsquoœsophage dans sa portion thoracique avec ou sans fistule tracheacuteo-oesophagienne
bull 5 types anatomiques Classification de Ladd et Swenson
Epideacutemiologie
bull 14000
bull AO isoleacutee = 50 ndash sporadique ndash risque de reacutecurrence intra-familiale lt 1
bull AO associeacutee = 50
ndash Anomalies chromosomiques 8-27 (tri 13 18 21) ndash Del 22q112 (syndrome veacutelo-cardio-facial) ndash Associations VATER VACTERL VACTERL-H (hydroceacutephalie) ndash Syndromes CHARGE Feingold Opitz Pallister-Hall Potter
laquo schisis syndrome raquo Goldenhar G syndrome hellip
VATER - VACTERL
bull Vertebral
bull Anorectal
bull Tracheo
bull Esophageal
bull Radial limb renal anomalies
bull Limb anomalies
7-8 des AO
CHARGE
bull Coloboma
bull Heart defect
bull Choanal atresia
bull Growth and mental retardation
bull Genital hypoplasia
bull Ear anomalies
AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Epideacutemiologie
bull 14000
bull AO isoleacutee = 50 ndash sporadique ndash risque de reacutecurrence intra-familiale lt 1
bull AO associeacutee = 50
ndash Anomalies chromosomiques 8-27 (tri 13 18 21) ndash Del 22q112 (syndrome veacutelo-cardio-facial) ndash Associations VATER VACTERL VACTERL-H (hydroceacutephalie) ndash Syndromes CHARGE Feingold Opitz Pallister-Hall Potter
laquo schisis syndrome raquo Goldenhar G syndrome hellip
VATER - VACTERL
bull Vertebral
bull Anorectal
bull Tracheo
bull Esophageal
bull Radial limb renal anomalies
bull Limb anomalies
7-8 des AO
CHARGE
bull Coloboma
bull Heart defect
bull Choanal atresia
bull Growth and mental retardation
bull Genital hypoplasia
bull Ear anomalies
AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

VATER - VACTERL
bull Vertebral
bull Anorectal
bull Tracheo
bull Esophageal
bull Radial limb renal anomalies
bull Limb anomalies
7-8 des AO
CHARGE
bull Coloboma
bull Heart defect
bull Choanal atresia
bull Growth and mental retardation
bull Genital hypoplasia
bull Ear anomalies
AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

CHARGE
bull Coloboma
bull Heart defect
bull Choanal atresia
bull Growth and mental retardation
bull Genital hypoplasia
bull Ear anomalies
AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

AO Physiopathologie
Accumulation de salive CDSS Fausses-routes reacutegurgitations
Fistule oeso-tracheacuteale Inondation arbre respi par RGO distension gastrique
Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Diagnostic en salle de travail Deacutepistage systeacutematique
bull Eacutepreuve agrave la sonde et agrave la seringue permeacuteabiliteacute oesophagienne ndash Sonde 8 CH ndash 10 CH
ndash Distance tragus ndashombilic (20 cm)
ndash Auscultation eacutepigastre
bull Buteacutee vers 9-12 cm
bull Pas drsquoalimentation
bull Radio sonde en place
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
Piegraveges du deacutepistage meacuteconnaissance AO
bull Fistules en laquo H raquo ndash endoscopie ORL systeacutematique
bull SNG enrouleacutee dans le CDS sup ndash Surtout si sonde trop molle
ndash Auscultation eacutepigastrique systeacutematique+++
Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Risque deacutepistage perforation paroi post pharynx
bull Preacutematureacute++ difficulteacutes drsquointubation++
bull Fausse route (sonde trop rigide)
bull Radio profil
ndash SNG parallegravele au rachis trop rectiligne
Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Diagnostic neacuteonatal retardeacute (25)
bull Signes cliniques ndash Hypersialorrheacutee = hypersalivation laquo Nouveau-neacute
qui mousse raquo
ndash Reacutegurgitations fausses-routes salivaires
ndash Deacutetresse respiratoire cyanose encombrement broncho-pulmonaire
bull Inhalations lieacutees au reflux gastro-oesophago-tracheacuteal
bull Hypoventilation par distension gastrique
Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Conduite agrave tenir immeacutediate en cas drsquoAO suspecteacutee
bull Arrecirct immeacutediat de lrsquoalimentation orale bull Position proclive dorsal agrave 45deg bull Pose par la bouche drsquoune sonde oesophagienne
ndash en buteacutee (9-10 cm) ndash sonde drsquoaspiration pharyngeacutee ndash agrave double courant (Replogle Salem) ndash 10 CH ndash relieacutee agrave lrsquoaspiration murale (100 cm drsquoeau)
bull Laisser lrsquoenfant en ventilation spontaneacutee (fond drsquoO2) bull Radio sonde en place
Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Imagerie en urgence
bull Clicheacute thoraco-abdominal de face
bull Clicheacute centreacute de profil sonde en place
bull Clicheacute avec injection drsquoair ++
Confirmation du diagnostic Forme avec ou sans fistule inf Position CDS supeacuterieur Tracheacuteomalacie Malformations associeacutees
Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Radiographie thoracique de deacutepistage drsquoAO sonde en place
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
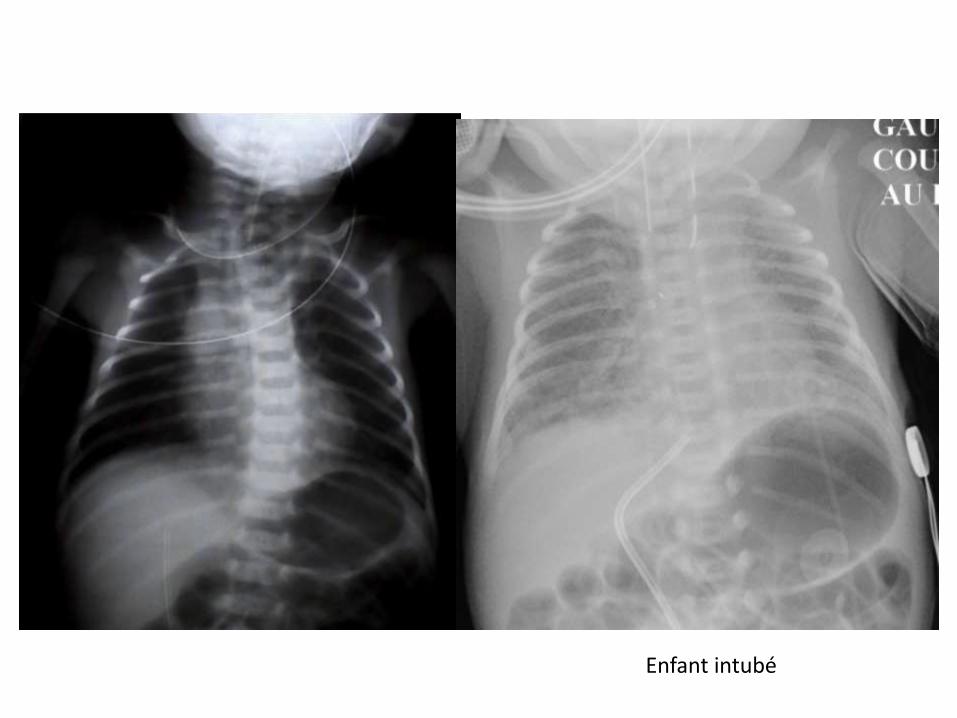
Julien type III 2003
Enfant intubeacute
Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Tiya 2009 Clicheacutes de profil avec injection drsquoair remarquez lrsquoaspect effileacute de la tracheacutee
Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Cardiopathie grave AO type I sans fistule inf
Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Mise en condition de lrsquoenfant transfert en milieu speacutecialiseacute (SAMU peacutediatrique)
bull A jeucircn strict
bull Position proclive dorsal agrave 45deg
bull Sonde oesophagienne en aspiration
bull Ventilation spontaneacutee (fond drsquoO2 eacuteventuellement)
bull Voie veineuse ndash perfusion
bull Protection contre hypothermie (couveuse)
bull Scope ndash SaO2
Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Recherche des malformations associeacutees
bull Initieacutee en preacutenatal en cas de diagnostic preacutenatal
bull Parfois initieacutee sur le lieu de naissance examen clinique RP + ASP
bull Toujours reacutealiseacutee dans le centre speacutecialiseacute recherche de principe des malformations associeacutees
Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Malformations associeacutees
Malformations Freacutequence approximative Diagnostic
Cardio-vasculaires (cardiopathies crosse
aortique droite)
15-16 Clinique RP Echo coeur
Oesophagiennes (steacutenoses) 04 Per-opeacuteratoire TOGD post-op
Gastro-intestinales (atreacutesies duodeacutenum grecircle)
24 ASP Echo abdo
ORL (atreacutesie choanes diasthegravemes)
Endoscopie ORL
Broncho-pulmonaires Clinique RP
Musculo-squelettiques (costo-verteacutebrales membres)
5 Clinique RP + ASP
Geacutenito-urinaires Clinique Echo abdo reacutenale et pelvienne
Ano-rectales 72 Clinique
Face SNC Clinique (dysmorphie) ETF
In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

In OrsquoNeill
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
Malformations associeacutees urgentes agrave deacutepister systeacutematiquement
bull Cardiopathies+++
bull Crosse aortique droite
bull Malformation anorectale
bull Atreacutesie duodeacutenale jeacutejuno-ileacuteale
bull Malrotation intestinale
Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Bilan preacute-opeacuteratoire obligatoire
bull Examen clinique complet
bull Biologie sanguine groupe Rh NFS iono calceacutemie CRP coag
bull Recherche colonisation bacteacuterienne
bull Clicheacute thoraco-abdominal de face
bull Echocardiographie
bull Echographie abdomino-reacutenale et pelvienne
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
Bilan drsquoopeacuterabiliteacute
bull Il tient compte de
ndash Type anatomique de lrsquoAO fistule eacutecart
ndash Age gestationnel et poids de naissance
ndash Etat pulmonaire et heacutemodynamique
ndash Associations malformatives
Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Critegraveres pronostiques preacute-opeacuteratoires
Article princeps Oesophageal atresia tracheo-oesophageal fistula A study of survival in 218 infants WATERSTON DJ CARTER RE ABERDEEN E Lancet 1962 Apr 211(7234)819-22
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
Chir Pediatr 198829(5)247-51 [Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports] [Article in French] Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Source Service de Chirurgie Peacutediatrique Hocircpital Saint-Vincent-de-Paul Paris Abstract In a consecutive series of 275 infants with esophageal atresia seen at Saint-Vincent-de-Pauls Hospital (Paris) between 1971 to 1987 the authors report the experience with 37 infants weighed under 2000 g (1345) 19 had severe additional malformations (5135) and 10 (27) had a respiratory distress syndrome As Abrahamson in 1972 (3) Cozzi an Wilkinson in 1975 (4) Rickham in 1981 (5) reported according to the criteria suggested in 1962 by Waterston (1) survival rate are related to additional congenital anomalies and initial respiratory distress (pulmonary dysmaturity or pneumonia) but seems more related to maturity (small-for-date babies) than to birth weight The authors recommend to perform a primary division of the tracheo-esophageal fistula and end-to-end esophageal anastomosis whenever possible
Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Am Surg 1999 Oct65(10)908-10 Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Dunn JC Fonkalsrud EW Atkinson JB Source Division of Pediatric Surgery University of California at Los Angeles School of Medicine 90095 USA Abstract The survival of infants with tracheoesophageal fistula was stratified by David J Waterston et al in 1962 This classification has been used as a guide to direct the timing of operative intervention in these infants This study examines the current applicability of this classification system The hospital records of 64 infants with esophageal atresia andor tracheoesophageal fistula were reviewed The survival rate was analyzed as a function of the infants risk stratification birth weight and additional anomalies Twenty-three infants were in Waterston Group A 20 infants in Group B and 21 infants in Group C The survival of all infants was 81 per cent Six infants died after recognition of severe anomalies and withdrawal of care four infants died of cardiopulmonary arrest and two infants died of sepsis The survival of infants in both Groups A and B was 100 per cent in contrast to 43 per cent survival in Group C Only infants who weighed lt1800 g or had severe additional anomalies were at risk of dying Therefore the classification of infants with esophageal atresia andor tracheoesophageal fistula may be simplified by combining Waterstons Groups A and B into a single risk stratum
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques
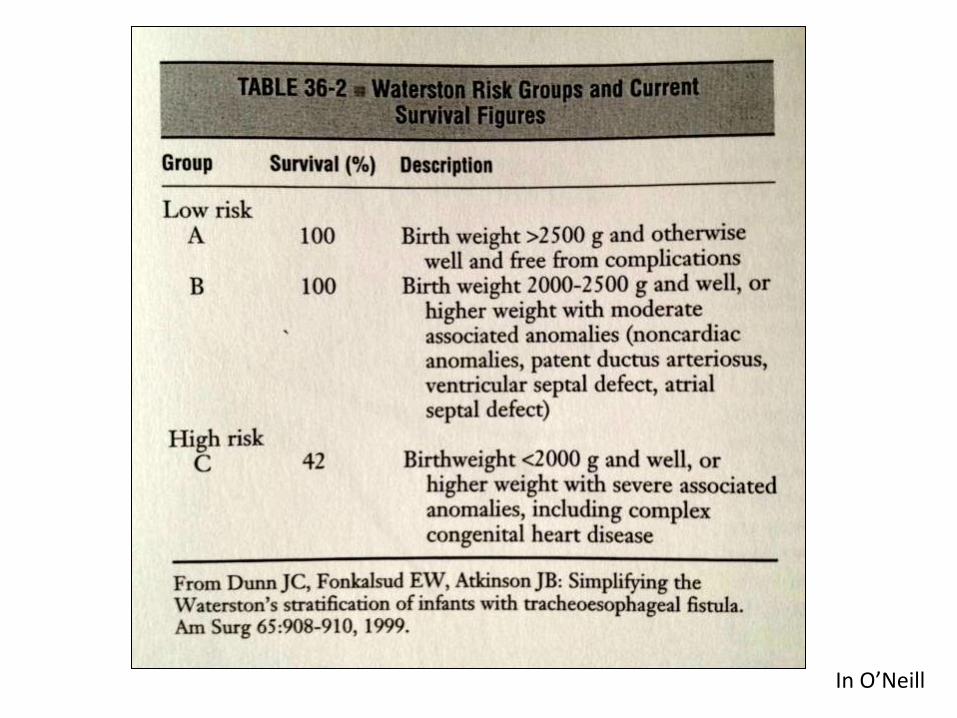
In OrsquoNeill
Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Classification de Waterston quelles conseacutequences
bull Cibler les enfants agrave risque chirurgical eacuteleveacute
bull Reacutealiser chez eux un traitement diffeacutereacute
ndash Ligature-section de la fistule oeso-tracheacuteale seule
ndash Gastrostomie drsquoalimentation + aspiration pharyngeacutee continue
ndash Anastomose oesophagienne diffeacutereacutee quand lrsquoeacutetat de lrsquoenfant le permet
Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Classification de Waterston qursquoen est-il aujourdrsquohui
bull Grands progregraves de la reacuteanimation neacuteonatale ndash Taux de survie excellents ndash Traitement chirurgical complet en 1 temps possible
mecircme pour les enfants lt 2000 gr
bull Principes de la classification restent valables
bull Actualisation
ndash Ne pas diffeacuterer lrsquoanastomose oesophagienne si elle est sans risque pour lrsquoenfant
ndash Savoir la diffeacuterer si lrsquoeacutetat de lrsquoenfant est preacuteoccupant ou lrsquoanastomose parait agrave haut risque de complication
Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

Reacutefeacuterences bibliographiques
bull Helardot P Bargy F Atreacutesie de lrsquoœsophage In laquo Pathologie congeacutenitale et acquise de lrsquoœsophage raquo VIegraveme Seacuteminaire drsquoEnseignement de Chirurgie Peacutediatrique Reims 1987
bull Levard G Mcheik JN Malformations congeacutenitales de lrsquoœsophage In laquo Pathologie congeacutenitale de lrsquoœsophage raquo Monographie du Collegravege National de Chirurgie Peacutediatrique Ed Sauramps F Becmeur 2006
bull Piolat C Robert Y Dyon JF Urgences en neacuteonatologie urgences thoraciques In Urgences Chirurgicales de lrsquoenfant JL Jouve PY Mure Doin 2012
bull OrsquoNeil etal Pediatric Surgery 5th Edition Mosby-Year Book Inc (1998)
bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques

bull Waterston DJ Bonham Carter RE Aberdeen E Oesophageal atresia tracheo-esophageal fistula Lancet 19621819ndash822
bull Sapin E Kurzenne JY Bargy F Wakim A Esteve C Egu JF Helardot PG Esophageal atresia in newborn infants weighing less than 2000 grams Apropos of 37 case reports Chir Pediatr 198829(5)247-51
bull Dunn JC Fonkalsrud EW Atkinson JB Simplifying the Waterstons stratification of infants with tracheoesophageal fistula Am Surg 1999 Oct65(10)908-10
Reacutefeacuterences bibliographiques