asthma, allergies and bhr in urban black teenagers: the ... · dose ics plus leukotriene modifier...
TRANSCRIPT

Asthma training
Mike Levin
Division of Asthma and Allergy
Red Cross Hospital

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Asthma prevalence
• Asthma affects 20% of children
• Asthma is the commonest chronic disease in South African children.
• South Africa is ranked 25th worldwide in the prevalence of asthma
• South Africa is ranked fifth for asthma case fatality rates

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

What is asthma?
• Asthma is a disorder of the airways
• caused by reversible inflammation
• that leads to the air passages contracting
• in response to a wide range of stimuli
• with enhanced irritability of the airways
• and increased mucus secretion

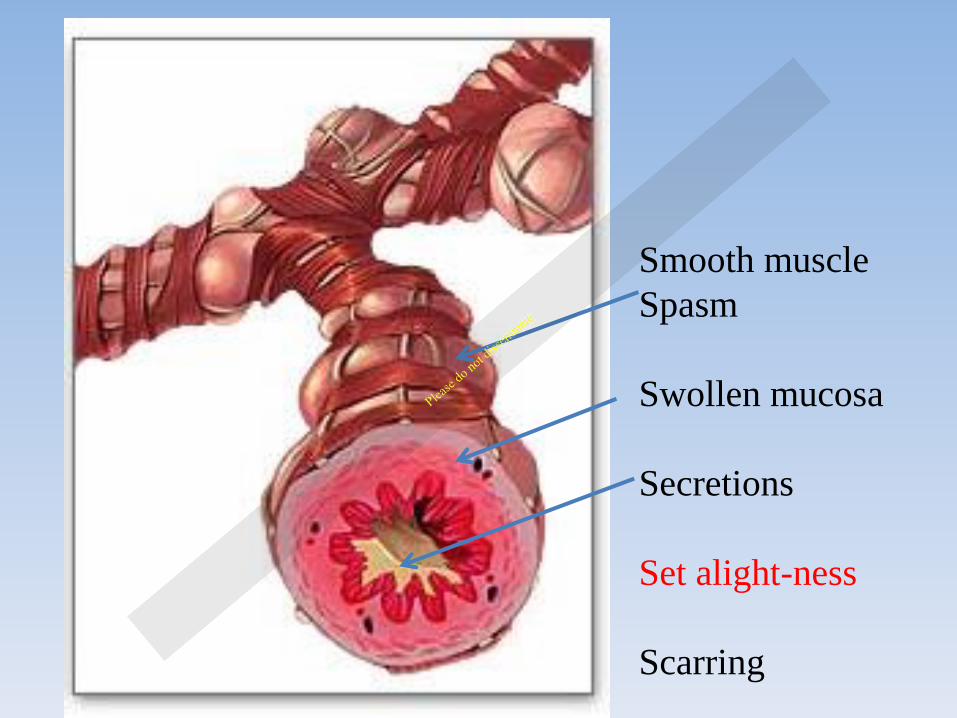
Smooth muscle
Spasm
Swollen mucosa
Secretions
Set alight-ness
Scarring

Allergic inflammation
• Inflammation is the most important aspect of asthma
• Inflammation causes the other features
• That’s why asthma needs treatment with regular controller therapy given every day whether the patient is symptomatic or not … to control the inflammation.

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

How do we diagnose it ??
recurrent wheeze and/or cough and/or dyspnoea
responsive to bronchodilators

How do we diagnose it ??
recurrent wheeze and/or cough and/or dyspnoea
responsive to bronchodilators

Has the patient had recurrent wheezing?
Does the patient have a cough at night?
Does the patient wheeze or cough after
exercise?
Does the patient experience symptoms
after exposure to allergens or pollutants?
Are symptoms seasonal?
Do the patient’s colds “go to the chest” or
take >10 days to clear up?

How do we diagnose it ??
recurrent wheeze and/or cough and/or dyspnoea
responsive to bronchodilators

Bedside test or < 5 Administer bronchodilator
Reassess after 10 minutes
Document respiratory rate
respiratory distress
auscultation
Bronchodilator and diary card over 2 weeks Trial of oral corticosteroids for 7 – 14 days
Bronchodilator response

Lung function tests 10 mins after bronchodilators
> 5 yrs FEV1 increase by > 12 % (15 %)
PEF increase by > 15 % (20%)
Diurnal variability > 20 %
Bronchodilator response

Respiratory
infections
worms
foreign body
lymph nodes
cystic fibrosis
Vocal cord
dysfunction
Exclude other conditions
Cardiac
pulmonary oedema
myocarditis
congenital abnormalities
GIT
G-O reflux disease
Mimics other diseases.
Asthma and atopy may coexist with other diseases.

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion
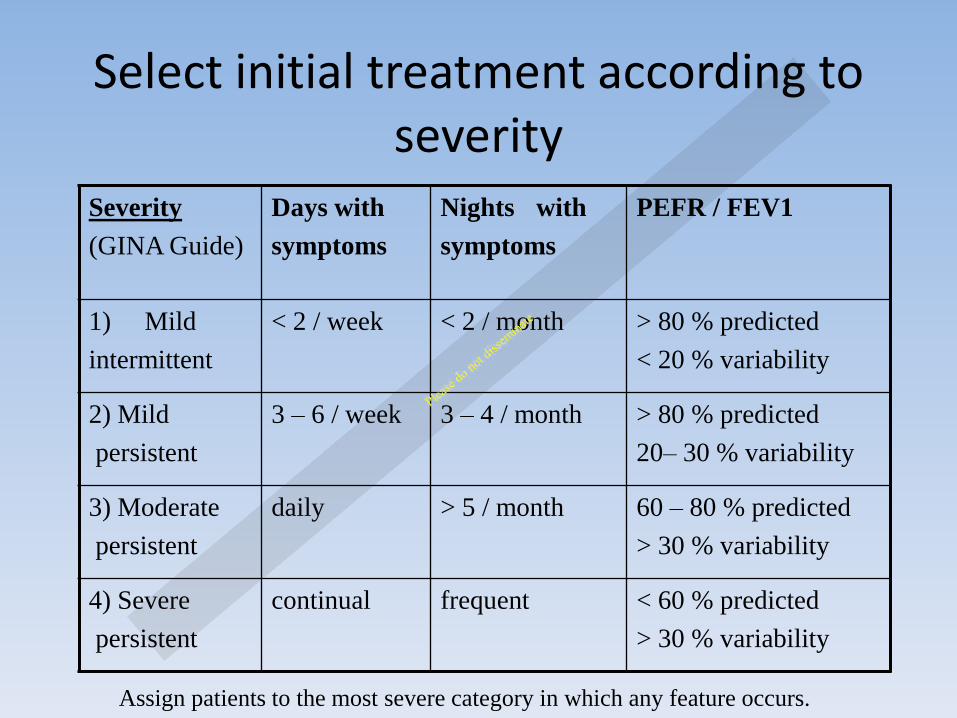
Select initial treatment according to severity
Severity
(GINA Guide)
Days with
symptoms
Nights with
symptoms
PEFR / FEV1
1) Mild
intermittent
< 2 / week < 2 / month > 80 % predicted
< 20 % variability
2) Mild
persistent
3 – 6 / week 3 – 4 / month > 80 % predicted
20– 30 % variability
3) Moderate
persistent
daily > 5 / month 60 – 80 % predicted
> 30 % variability
4) Severe
persistent
continual frequent < 60 % predicted
> 30 % variability
Assign patients to the most severe category in which any feature occurs.

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Step 1 Step 2 Step 3 Step 4 Step 5
Asthma education and environmental control
As needed reliever medication e.g. rapid-acting β2-agonist
No controller medication
required

Education
Goals of therapy
Minimal or no chronic symptoms day or night
Minimal or no exacerbations
No limitation on activity; school or parent’s work missed
Minimal use of inhaled B2 agonists
Minimal or no adverse effects from medication

Asthma medication
• Controllers (preventers) – Inhaled steroid pumps
– Long acting B2 agonists
– Leukotriene receptor antagonists
– Theophylline
• Relievers – SABA
– Ipratropium bromide

Step 1 Step 2 Step 3 Step 4 Step 5
Asthma education and environmental control
As needed reliever medication e.g. rapid-acting β2-agonist
No controller medication
required Select one
Low-dose inhaled steroid
(ICS)
Leukotriene modifier

Step 1 Step 2 Step 3 Step 4 Step 5
Asthma education and environmental control
As needed reliever medication e.g. rapid-acting β2-agonist
No controller medication
required Select one Select one
Low-dose inhaled steroid
(ICS)
Medium-dose ICS
Leukotriene modifier
Medium or Low-dose ICS plus
long-acting β2-
agonist
Low-dose ICS plus leukotriene
modifier

Step 1 Step 2 Step 3 Step 4 Step 5
Asthma education and environmental control
As needed reliever medication e.g. rapid-acting β2-agonist
No controller medication
required Select one Select one Select one
Low-dose inhaled steroid
(ICS)
Medium-dose ICS
Medium or high-dose ICS plus
long-acting β2-agonist
Leukotriene modifier
Medium or Low-dose ICS plus
long-acting β2-
agonist
Medium or high-dose ICS plus Leukotriene
modifier
Low-dose ICS plus leukotriene
modifier
Medium or high-dose ICS plus theophylline

Step 1 Step 2 Step 3 Step 4 Step 5
Asthma education and environmental control
As needed reliever medication e.g. rapid-acting β2-agonist
No controller medication
required Select one Select one Select one add either
Low-dose inhaled steroid
(ICS)
Medium-dose ICS
Medium or high-dose ICS plus
long-acting β2-agonist
Oral steroid (lowest dose)
Leukotriene modifier
Medium or Low-dose ICS plus
long-acting β2-
agonist
Medium or high-dose ICS plus Leukotriene
modifier
Anti-IgE treatment
Low-dose ICS plus leukotriene
modifier
Medium or high-dose ICS plus theophylline

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Asthma Control Characteristic
Follow up regularly.
Assess and move up and down treatment
algorithm according to control.
Daytime symptoms
Limitation of activities
Nocturnal symptoms/awakening
Need for reliever/rescue medication
Lung function (PEF or FEV1)
Assessing
Treating Monitoring

Asthma Control Characteristic Controlled
(all of the following) Partly controlled (any measure present)
Uncontrolled
Daytime symptoms None (twice or less/week)
More than twice/week Three or more characteristics of partly controlled asthma
Limitation of activities None Any
Nocturnal symptoms/awakening
None Any
Need for reliever/rescue medication
None (twice or less/week)
More than twice/week
Lung function (PEF or FEV1)
Normal <80% predicted or personal best (if known)

Reasons for poor asthma control
Incorrect diagnosis
Incorrect choice of inhaler and poor inhaler technique
Patient belief and adherence
Individual variation in response to
treatment
Smoking
Co-morbid rhinosinusitis

Before altering medication consider Is the diagnosis correct? Is there objective evidence of
asthma?
Are there any correctable trigger factors, e.g.
occupational sensitisers, does the patient smoke?
Other factors: Gastro-oesophageal reflux, ABPA
Does the patient have allergic rhinosinusitis? Treatment of
this may improve asthma control
Is the patient adherent to their existing therapy?
Is the patient able to use their inhaler properly?

Step 1 Step 2 Step 3 Step 4 Step 5
No controller medication
required Select one Select one Select one add either
Low-dose inhaled steroid
(ICS)
Medium-dose ICS
Medium or high-dose ICS plus
long-acting β2-agonist
Oral steroid (lowest dose)
Leukotriene modifier
Medium or Low-dose ICS plus
long-acting β2-
agonist
Medium or high-dose ICS plus Leukotriene
modifier
Anti-IgE treatment
Low-dose ICS plus leukotriene
modifier
Medium or high-dose ICS plus theophylline

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Controller medications
Inhaled glucocorticoids
(e.g. budesonide, fluticasone propionate)
Leukotriene modifiers
(e.g. montelukast, zileuton)
Long-acting inhaled
β2-agonists (LABA) (e.g. salmeterol,
formoterol)

Controller medications
• The most effective controller medication, delivering drugs directly to the airways
Inhaled glucocorticoids
(e.g. budesonide, fluticasone propionate)
Leukotriene modifiers
(e.g. montelukast, zileuton)
Long-acting inhaled
β2-agonists (LABA) (e.g. salmeterol,
formoterol)


Most asthmatics well controlled with low dose
inhaled steroids.
Side effects uncommon.
Inhaled corticosteroids

Low dose Medium High dose
Budesonide 100 – 200 200 - 400 400 – 800
(Budeflam, Pulmicort, Inflammide)
Beclomethasone 100 – 200 200 - 400 400 – 800
(Becotide, Beclate)
Fluticasone 50 – 125 125 – 250 250 – 500
(Flixotide)
Steroid doses
Document dose of MDIs accurately

Controller medications
• The most effective controller medication, delivering drugs directly to the airways
Inhaled glucocorticoids
(e.g. budesonide, fluticasone propionate)
• Used as add on particularly in children < 5
• Particularly appropriate for patients unwilling or unable to take ICS, or those that experience side effects with ICS
Leukotriene modifiers
(e.g. montelukast, zileuton)
Long-acting inhaled
β2-agonists (LABA) (e.g. salmeterol,
formoterol)


Uses for LTRA’s
• Monotherapy for mild asthma
• Monotherapy if patient noncompliant or steroid phobic
• Mild asthma with exercise induced component
• Aspirin sensitive asthma.
• Add on therapy for moderate persistent asthma
• Potential for steroid sparing effects
• Add on therapy for severe uncontrolled asthma.

Controller medications
• The most effective controller medication, delivering drugs directly to the airways
Inhaled glucocorticoids
(e.g. budesonide, fluticasone propionate)
• Used as add on particularly in children < 5
• Particularly appropriate for patients unwilling or unable to take ICS, or those that experience side effects with ICS
Leukotriene modifiers
(e.g. montelukast, zileuton)
• Synergistic effects
• Not monotherapy
• Not below 5
Long-acting inhaled
β2-agonists (LABA) (e.g. salmeterol,
formoterol)

Anti-inflammatory action is synergistic with steroids.
Reduce bronchial hyperresponsiveness and inhibit
release of inflammatory mediators and prevent plasma
exudation.
12 hour bronchodilation. Receptor desensitisation and
downregulation.
This effect prevented by concomitant steroid
administration.
Long acting B 2 agonists

Improves outcomes when added to medium or high
dose inhaled steroids.
Not first line agents
Use only as combination, never mono-therapy
Use as steroid sparing agents or as step up before
increasing steroids
Contraindicated below age of 5
Uses for LABAs

SMART therapy
• LABAs are formoterol and salmeterol
• Both have long duration of action
• Salmeterol has delayed onset of action
• Formoterol is rapid acting
• Symbicord maintenance and reliever therapy
• To “blunt” attacks



Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Drugs in acute asthma
Adrenaline B2 receptors relaxation
+ SABA’s relaxation
Acetylcholine Cholinergic receptors spasm
- Anticholinergics relaxation

Drugs in acute asthma
Adrenaline B2 receptors relaxation
+ SABA’s relaxation
Acetylcholine Cholinergic receptors spasm
- Anticholinergics relaxation

Oxygen therapy
• Monitor all patients
• Achieve O2 saturation of 95%, >93% in children
Inhaled rapid-acting β2-agonists
• MDI with spacer (unless hypoxic)
• Repeat (at least) 3 doses in first hour
Oral glucocorticoids
• Early administration
• Oral
Acute exacerbations

Acute asthma

Acute asthma


Administration of B2 agonists
• MDI/spacer 6-10 puffs – Each puff separately – Repeat every 20 minutes
• Drug (approved name) Salbutamol • Dose 6 or 10 puffs • Route INHAL via Spacer • Other directions 100 microgram MDI
• How frequently should I prescribe multidoses? • Multidose of bronchodilator gives an equivalent effect as a
nebuliser and therefore does not require to be given more frequently than you would give nebulised medication
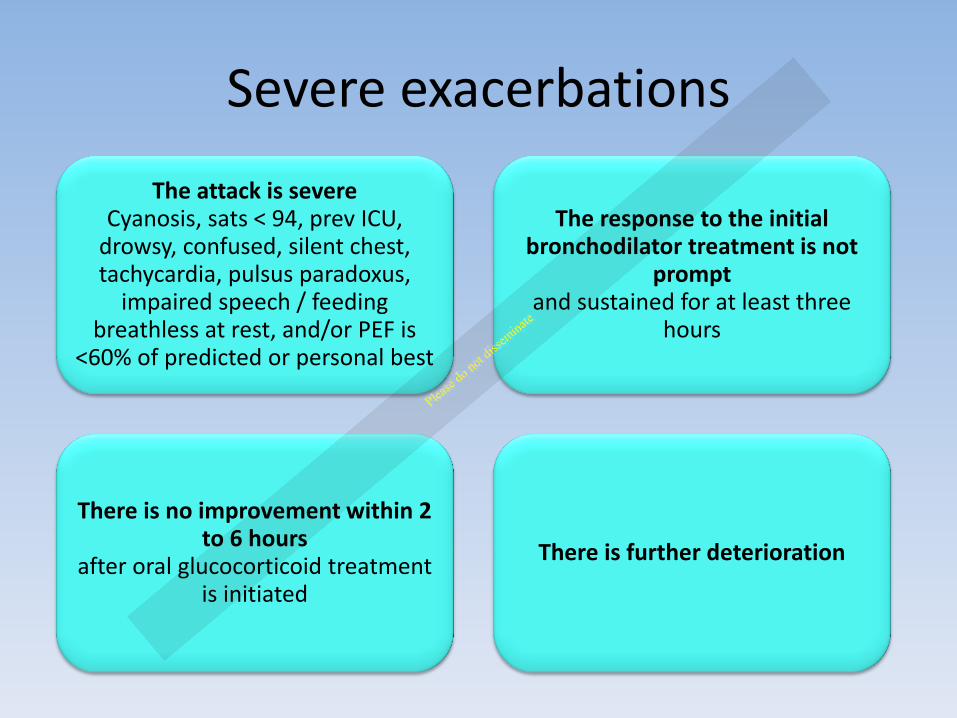
Severe exacerbations
The attack is severe Cyanosis, sats < 94, prev ICU,
drowsy, confused, silent chest, tachycardia, pulsus paradoxus,
impaired speech / feeding breathless at rest, and/or PEF is
<60% of predicted or personal best
The response to the initial bronchodilator treatment is not
prompt and sustained for at least three
hours
There is no improvement within 2 to 6 hours
after oral glucocorticoid treatment is initiated
There is further deterioration



Give adequate inhaled therapy before considering anything else


Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Using a MDI is not easy
Effective deposition of aerosols requires
– Slow inspiratory flow
– Deep inhalation and breath hold
– Quiet, non-distressed breathing

Timing is critical Actuation 1 second before inhalation
reduces inhaled mass by 90%
Late actuation results in the lung being filled with medication-free air and aerosol merely reaching the “dead space” and being exhaled
Delivery of medication via a MDI without a spacer is highly ineffective
Using a MDI is not easy

Spacers
Problems with spacers Spacer is less portable than MDI alone
Multiple actuations into spacer
Need comfortable but well sealed mask
Inspiratory flow to open holding valve with tidal breathing

Issues with nebulisers
• Flow rate of 6-8 l/min – Driven by O2 or air
• Dead volume of 0.5-1ml
• When a nebuliser starts “sputtering” delivery is minimal
• Filling volume of 4-5 ml

Overview • Introduction
• Physiology
• Diagnosis
• Severity
• Treatment
• Control
• Stage 3 of guidelines
• Acute asthma
• Drug delivery
• Conclusion

Inhaler technique
Prepare the device
• Check the orientation
• Actuate the device
• Shake the device if it is an MDI

Inhaler technique
Prepare the device
• Check the orientation
• Actuate the device
• Shake the device if it is an MDI
Prepare the body
• Breathe out fully away from the mouthpiece
• Consider differences between MDI and DPI devices

Inhaler technique
Prepare the device
• Check the orientation
• Actuate the device
• Shake the device if it is an MDI
Prepare the body
• Breathe out fully away from the mouthpiece
• Consider differences between MDI and DPI devices
mouthpiece in mouth
• Ensure a good seal and make sure the teeth are not in front of the device

Inhaler technique
Prepare the device
• Check the orientation
• Actuate the device
• Shake the device if it is an MDI
Prepare the body
• Breathe out fully away from the mouthpiece
• Consider differences between MDI and DPI devices
mouthpiece in mouth
• Ensure a good seal and make sure the teeth are not in front of the device
DPI
• Breathe as fast and as hard as possible from the beginning
MDI
• Start breathing slowly and actuate. Breathe in over 5 seconds and hold breath for 5 seconds
OR
