assessment of lung as an oxygenator concept of ventilation – perfusion ratio, dead space, shunt...
TRANSCRIPT

ASSESSMENT OF LUNG AS AN OXYGENATORCONCEPT OF VENTILATION – PERFUSION RATIO, DEAD SPACE, SHUNT
Speaker : Dr. S Sai Janani
University College of Medical Sciences & GTB Hospital, Delhi

CONTENTS
• Ventilation – perfusion ratio Regional differences in ventilation Regional differences in perfusion Ventilation – perfusion ratio and
anesthetic implications• Dead space• Shunt• Anesthesia and dead space, shunt and V/Q mismatch• Assessment of lung as an oxygenator

VENTILATION- PERFUSION RATIO
• Defined as the ratio between ventilation and perfusion in a lung unit.
• Ventilation(V) = 4 L/ min• Perfusion(Q) = 5 L / min• V/Q = 0.8 (young adult)
• Differs in different lung regions due to regional differences in ventilation and perfusion.

Regional differences in ventilation: Compliance of the alveolus
PRESSURE SUPPORT NEEDED AT BASE > APEX
MORE LUNG VOLUME AT THE BASE

Regional differences in ventilation
• Lung is suspended from the hilum
The weight of the lung needs more pressure support from below than above
Pressure at the base > apex
Intra pleural pressure is less negative at the base and more negative at the apex

Regional differences in Ventilation
AT APEX:INTRAPLEURAL PRESSURE IS MORE NEGATIVE
ALVEOLI NEAR APEX MAXIMALLY INFLATED
DURING INSPIRATION, WHEN-VE THORACIC PRESSURE IS CREATED
∆PRESSURE BASE >∆PRESSURE APEX
VENTILATION BASE>APEX
IN AWAKE ERECT POSITION

Compliance…….
Regional differences in ventilation
• SUPINE POSITION:
• Dorsal region is dependent.
• Hence, ventilation is better dorsally than ventrally.
• Thus, the diaphragm is DESIGNED TO HAVE GREATER EXCURSIONS POSTERIORLY than anteriorly.

Ventilation in anesthetised pt.
1. FRC < CV. THE ALVEOLI IN THE DEPENDENT REGION COLLAPSE
2. THE PREFENTIAL DORSAL EXCURSION OF DIAPHRAGM IS LOST IN PARALYSIS

Atelectasis after anesthesia in the dependent parts
Augmented when higher FiO2 is used or during pre – oxygenationABSORPTION ATELECTASIS
Ventilation in anesthetised pt
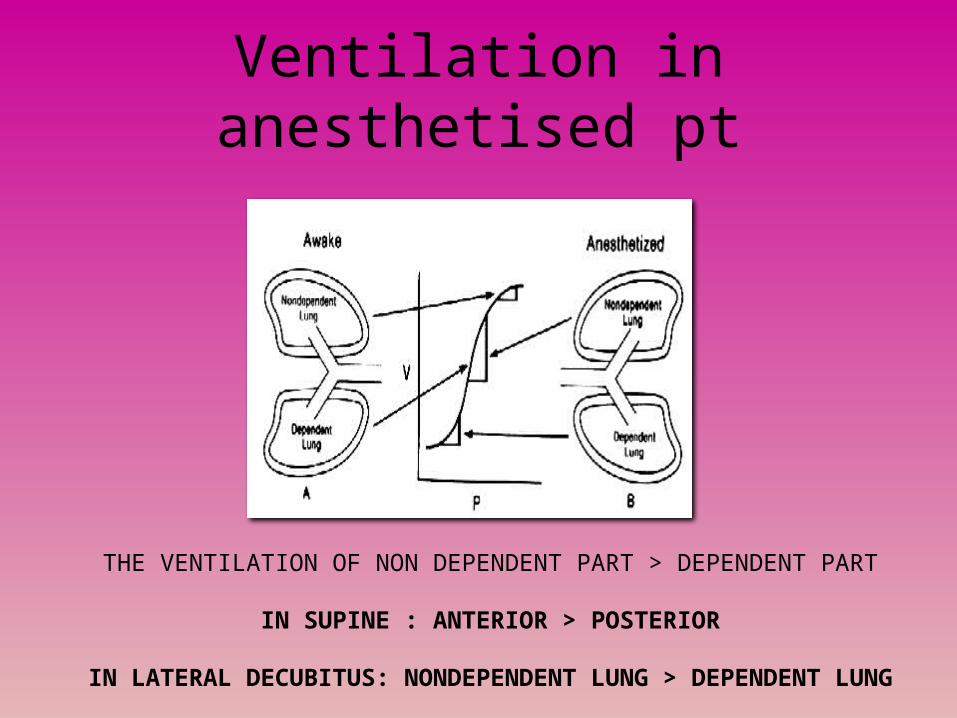
THE VENTILATION OF NON DEPENDENT PART > DEPENDENT PART
IN SUPINE : ANTERIOR > POSTERIOR
IN LATERAL DECUBITUS: NONDEPENDENT LUNG > DEPENDENT LUNG

REGIONAL DIFFERENCES IN PERFUSION
• Primary determinant – GRAVITY• Healthy adult – erect position:• Distance from apex to base = 30 cm• Assuming that pulm. Artery enters the lung
midway b/w apex and base- 15 cm H20 ( overcome)
+ 15 cm H20(gain)
PERFUSION AT BASE > APEX
PASCAL’S LAW
P = hῥg

Regional differences in perfusion

Regional differences in perfusion
Based on the differences in perfusion, the lung is divided onto West’s zones:
1. Alveolar pressure is constant from apex to base
2. If the pulm. Artery system is considered a continuous column of blood, the pressure exerted by the column above is greater at the base than at the apex (by 30cmH2O)

Regional differences in perfusion: The West’s Zones
ZONE I : MINIMAL BLOOD FLOWDEPENDS ON a-v DIFFERENCE

Regional differences in perfusion: The West’s Zones
ZONE I : MINIMAL BLOOD FLOWDEPENDS ON a-v DIFFERENCE
INDUCTION OF ANESTHESIA. ↓QT , “WASTED VENTILATION” ,ALVEOLAR DEAD SPACE

Regional differences in perfusion: The West’s Zones
ZONE II: WATERFALL EFFECT
DEPENDS ON a-A DIFFERENCE

Regional differences in perfusion: The West’s Zones
ZONE III: HIGH PERFUSIONDEPENDS ON a-v DIFFERENCE
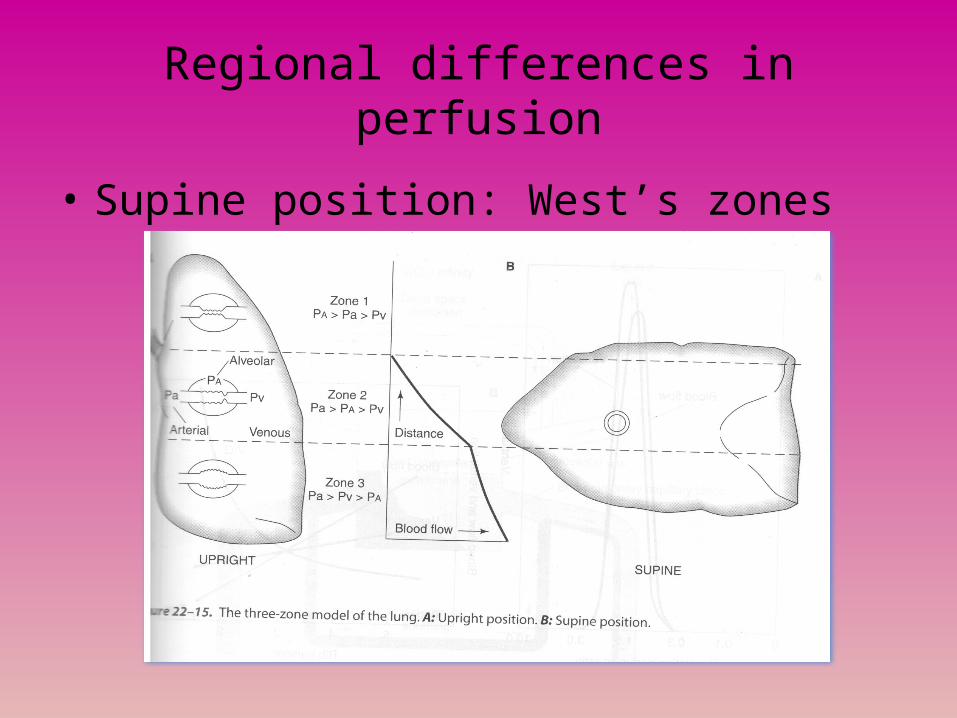
Regional differences in perfusion
• Supine position: West’s zones

VENTILATION – PERFUSION RATIO
↑ PERFUSION > ↑ VENTILATION FROM APEX TO BASEV/ Q AT APEX > V/Q AT BASE

Types of alveoli based on V/Q
SHUNT DEAD SPACE

Ventilation –Perfusion ratio
SHUNT DEAD SPACE
PHYSIOLOGICALLY THESE UNITS ARE NOT ABSOLUTE AND OCCUR AS A SPECTRUM

Arterial blood gases and V/Q
O2=40Co2 = 45 02 =100
Co2=40
02 = 103Co2 = 0
02 = 103Co2 = 0
SHUNT
DEAD SPACE
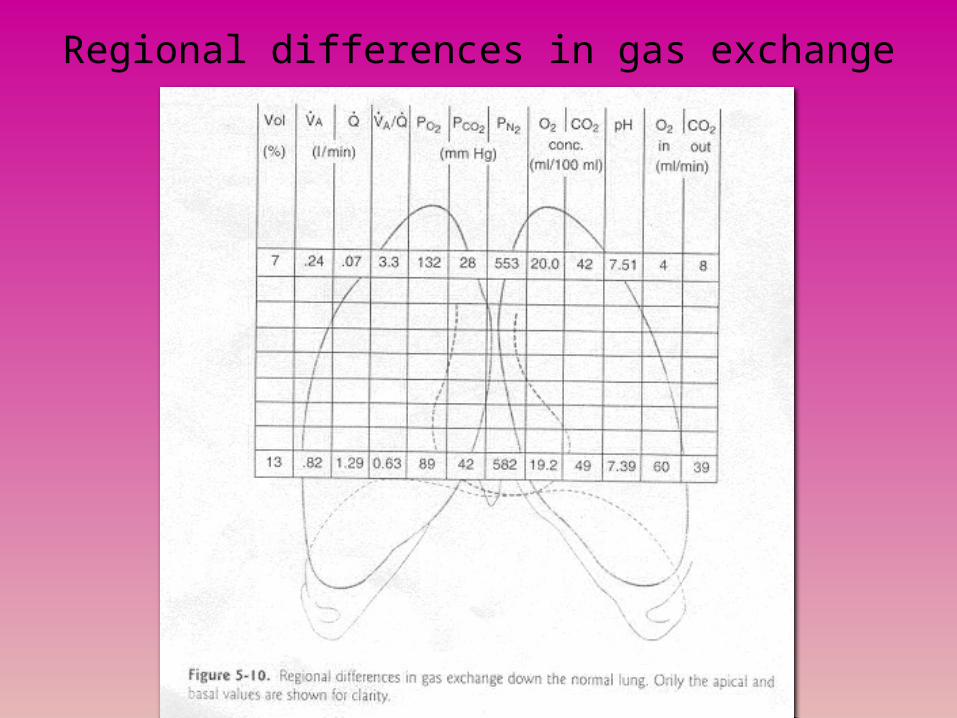
Regional differences in gas exchange

MEASUREMENT OF V/Q
• Regional differences- Measured by radioactive gases: Xe
• Single and multiple N2 breath tests
• By measuring (A-a)PO2
PAO2measured by alveolar gas equation
PAO2 = PIO2 – PACO2 + F
RPACO2 = PaCO2

MULTIPLE BREATH TEST

Hypoxic Pulmonary Vasoconstriction
• Adaptation of pulmonary blood flow to ventilation.
• Constriction of pulm. Blood vessels in areas Of reduced ventilation• GA attenuates HPV• > inhalational agents• Less attenuation when Thiopentone is used for induction

DEAD SPACE
• That portion of the respiratory tree in which no gas exchange takes place
• V / Q = ∞ • Volume occupied by the conducting system.• Represents “wasted ventilation”

DEAD SPACE
Types:• Anatomical dead space (Vd anat)• Physiological dead space (Vd phys)• Apparatus dead space

Dead spaceAnatomical dead space:The volume of the respiratory passages, extending
from nostrils and mouth down to (but not including) the respiratory bronchioles.
Varies with age and sexNormal = 150 mLYoung women = 100 mLOld men = 200 mLNormally = 1 mL / lb body weight or 2.2 mL / kg body
weight

Dead space…..
Anesthesia and Anatomical dead space:
Head tilt- chin lift (+40 mL)Depression of jaw with flexion of head (Airway obstruction) = - 30 mLTracheostomy / Pneumonectomy = ↓

Measurement of anatomical dead space
Modification of FOWLER’S Single breath N2 wash out method

Dead space
Physiological dead space (Vd phys):Fraction of tidal volume not available for gas
exchange.Anatomical + Alveolar dead spaceAlveolar dead space = ↑ V/Q regions = wasted ventilation


Physiological dead space
Normally, Anatomical dead space = Physiological dead
space = 1/3 tidal volume Expressed as that fraction of tidal volume
that contributes to “wasted ventilation” (Vd / Vt)
Vd / Vt = 0.25 – 0.4

Vd phys
Factors affecting Vd phys:
• Old age
• Upright position
• ↑ Tv
• ↑ RR
• Atropine
• T inspi < 0.5 secs during CMV
• ↑V/Q states
• Hypotension ( esp. with head up position)

Measurement of Physiological Dead space
PHYSIOLOGICAL DEAD SPACE AND ANESTHESIA:Roughly estimated by Cooper’s formula:
Measurement of Vd phys: (Vt – Vd)PACO2 = PeCO2 X Vt OR
(subtract apparatus dead space)
Vd phys = PaCO2 – PeCO2 PaCO2
Vd/ Vt = 33 + age /3 %
ENGHOFF’S MODIFICATION
OF BOHR EQUATION

Bohr Equation

Dead space…
Vd phys and the capnogram: (Non invasive measurement)
(PaCO2 – ETCO2) gradient increases when there is significant Vd alveolar thus increasing vd phys
Hence at that time, ETCO2 is an unreliable monitor for PaCO2

PaCO2
PeCO2
PaCO2
PeCO2
PeCO2
PaCO2


Dead space
APPARATUS DEAD SPACE:Volume of gas contained in any anesthetic
apparatus between the patient and that point in the system where rebreathing of exhaled
carbon dioxide ceases to occur

Dead spaceAnatomical face mask = ↑ Vd / Vt= 0.68COPA or LMA = Vd/Vt = 0.3 – 0.4ETT or Tracheostomy = ↓Vd/ VtBreathing circuits –
LengthDiameterCompressible volume ( 2 -3 mL gas for every 1 cmH2O
inspiratory pressure)

Dead space
• Pathologies producing dead space :
Anatomic:Rapid shallow breathing
Alveolar dead space:Acute pulmonary embolusRedistribution of pulmonary perfusion: ↓cardiac output Acute pulm. Hypertension
Ventilation > PerfusionPPVAlveolar septal destruction

SHUNT
Defined as blood that enters the arterial system without going through ventilated
areas of the lung.

Shunt…..Types:
1. Anatomical shunt: “True shunt” due to area in which there is absolutely no ventilation, but perfusion exists.
2. Physiological shunt: Normal degree of venous admixture due to true shunt + ↓V/Q ratio
3. Pathological shunt: Those forms of anatomical shunt which are not present in a normal subject.
4. Atelectatic shunt: Blood which has passed through collapsed regions of the lung.

Anatomical shunt
NORMAL ABNORMAL
Extra pulmonary Thebesian veins CnHD with R – L shunt
Pulmonary Bronchial veins AtelectasisPulm infectionPulm AV shuntsPulm neoplasmCircn in edematous lung

Physiological shuntPAO2 = 101
PaO2 = 97
(A- a) O2 = 5- 25 mmHg

SHUNT
(A – a) PO2 = 5 – 25 mmHg
PAO2 = 101
PaO2 = 97
AMOUNT OF MIXED VENOUS BLOOD
ADDED INORDER TO PRODUCED AN
OBSERVED (A-a) –
VENOUS ADMIXTURE

Shunt………..
Sources of venous admixture (5% CO)
↓V/Q ratio Shunt

Shunt……….
↓V/Q RATIO
SHUNT
OXYGENATION IN ↓V/Q AREAS – IMPROVES WITH ↑FiO2SHUNT IS REFRACTORY TO ↑FiO2

Calculating the shunt fraction…..
The shunt equation is derived as:Pulmonary capillary blood flow (Qc) + blood flow
through shunt(Qs) = cardiac output(Qt)
In terms of O2 content:( CcO2 X Qc)+(CvO2 X Qs) = (CaO2 XQt)
Qc + Qs = Qt

The shunt equation
Since, Qc = Qt – Qs,
(CcO2 X Qt) – (CcO2 X Qs)+ (CvO2 X Qs)
= (CaO2 X Qt)
Dividing both sides by Qt,
Qs = CcO2 – CaO2
Qt CcO2 - Cvo2

Shunt equation
• Inorder to remove CvO2 from the equation,We add and subtract CaO2 in the denominator.
Qs = (CcO2 – CaO2) Qt (CcO2 – CvO2 + CaO2 –Cao2)
• Since CaO2 – CvO2 = 5 in non critical patients,• And 3.5 in critical patients, we substitute in the
equation to get the Estimated shunt Equation

Estimated physiologic shunt equation……
• Does not need a pulm. Artery sample.• Non critical patients:• (Spontaneously breathing,mod. FiO2, mod.
CPAP)
Estimated Qs= (CcO2 – CaO2) Qt [5+(CcO2-CaO2)]

Estimated shunt equation…..
For critical patient:(Mechanical ventilation, High FiO2, high level of
positive end-expiratory pressure)
Estimated Qsp = (CcO2 –CaO2) Qt [3.5 + (CcO2 – caO2)]

Shunt Equation….
PHYSIOLOGIC SHUNT
INTERPRETATION
<10% NORMAL
10 -20% MILD
20 -30% MODERATE
>30% SEVERE

Shunt…..

Shunt producing pathology…
Anatomic:1.Congenital heart disease2.Pulmonary fistula3.Vascular lung tumors
Capillary shunting:1.Acute atelectasis2.Alveolar fluid3.Consolidation
Perfusion > Ventilation1.Hypoventilation2.Uneven distribution of ventilation3.Diffusion defect

Anesthesia and V/Q mismatch, shunt and dead space
BEFORE INDUCTION:AWAKE SUPINE SUBJECT
HPV
Dead space = Anatomical deadSpace
Minimal shunt
Ventilation perfusion relationships during anesthesia. Hedenstierna G, Thorax 1995; 50: 85 -91

After induction, with anatomical face mask and inhalational agent
ANESTHESIA INDUCEDANATOMICAL FACE MASK
INHALATIONAL AGENT:
HPV attenuatedAbsorption atelectasis- ↑ shuntHypotension by induction agent- ↑ alv Dead spaceFace mask – ↑ apparatus dead space↑ dead space, shunt and V/Q mismatch areasArterial oxygenation compromised
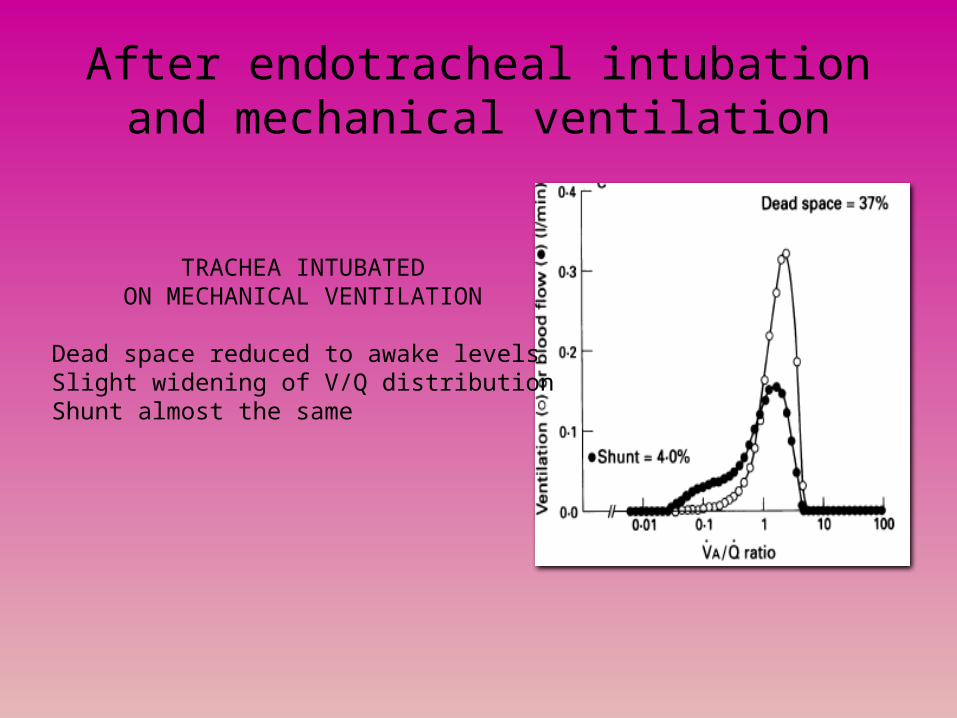
After endotracheal intubation and mechanical ventilation
TRACHEA INTUBATEDON MECHANICAL VENTILATION
Dead space reduced to awake levelsSlight widening of V/Q distributionShunt almost the same

Shunt and V/Q mismatch in anesthetised and awake individuals

ASSESSMENT OF LUNG AS AN OXYGENATOR
• Clinical assessment:• Level of consciousness ~ adequate cerebral oxygenation
• Vital signs: RR, HR, Blood pressure, temp.
• General physical examination:
• Head and neck:
• Inspection of face – any nasal flaring• cyanosis• pursed lip breathing• Neck: position of trachea• Shifted in upper lobe collapse• pneumothorax, • pleural effusion• lung tumor•

• Inspection:• Shape of the chest• Kyphosis• Scoliosis• Flattening• Over inflation
• Measurement of chest:• Rate of respiration• Rhythm• Chest expansion• Symmetry
• Percussion:• Resonance/ dullness
• Auscultation:• Breath sounds, adventitious sounds

Lung as an oxygenator……..ABG: • PaO2 = 80 – 100 mmHg• paCO2 = 35 -45 mmHg• P(A-a)O2 = 5- 25 mmHg (↑ V/Q mismatch, shunt)• PaO2/ FiO2 = 100 /0.2 = 500• O2 content = 19.8mL/dl blood• SpO2
ETCO2
V/Q mismatch
shunt
Lung as oxygenator:
Oxygenation indices:• PaO2• (A – a) PO2• PaO2 / FiO2 • PaO2 / FiO2 x Paw• Pao2 / PAO2• PaO2 / PvO2

Bibliography• 1.Respiratory Physiology- John.B.West 7th ed• 2.Egan’s Respiratory Care- 4 th ed• 3.Miller’s Anesthesia- 5th ed• 4. Textbook of Anesthesiology- Morgan 5 th ed• 5. Applied Respiratory Physiology- J.F.Nunn• 6. Textbook of Anesthesia- gray and Nunn• 7.Mechanical ventilation- Chang- 4th ed• 8.Clinical Application of Blood Gases- Shapiro- 5thed.• 9.understanding Anesthesia equipment- dorsch & dorsch- 7th ed.• 10.A practice of Anesthesia-Wiley 5 th ed.• 11.review of Medical Physiology – W.F. Ganong• 12.V/Q distribution and correlation of atelectasis in anesthetised paralysed humans-
JAP• 13. ventilation – perfusion ratio inAnesthesia –hedenstierna et al – Thorax- 1995 ;
50: 85- 91

THANK YOU