assessing the risk factors contributing … the risk factors contributing to occupational injuries...
TRANSCRIPT

ASSESSING THE RISK FACTORS CONTRIBUTING TO OCCUPATIONAL INJURIES
AMONG CEMENT WORKERS: A CASE OF EAST AFRICAN PORTLAND CEMENT
COMPANY
A RESEARCH PROJECT SUBMITTED IN PARTIAL FULFILMENT OF POST GRADUATE
DIPLOMA IN OCCUPATIONAL SAFETY AND HEALTH
2017
DECLARATION
This research project is my original work and has not been presented for award of a degree in any other
University for any other award.

ii
Signed: ……………………………… Date: ………………………
This research project has been submitted for examination with my approval as the University supervisor.
Signed: ……………………………… Date: ………………………
iii
DEDICATION
I would like to dedicate this work to my family and friends. Thank you so much for your continuous
encouragement to complete my studies.

iv
ACKNOWLEGEMENT
I would like to thank God for giving me strengthen, knowledge, skills and the opportunity to pursue this
noble course of ensuring that work environment are safe. To my family for financial, moral and spiritual
support be blessed in abundance.
Jomo Kenyatta University of Agriculture and Technology: Institute of Energy & Environmental
Technology, am very grateful for the opportunity granted to me to pursue the research.
To my supervisors, Mr Charles Mburu and Ms Purity Muthoni for encouraging me to do my research
on this specific topic, giving directions, valuable comments and constructive suggestions throughout
the research process. I have no words to express my heartfelt appreciation for your unreserved advice.
To East African Portland cement fraternity for allowing me to undertake the research in their
organization. The employees’ willingness and active participation in this research.
v
TABLE OF CONTENTS
DECLARATION ............................................................................................................................. i
DEDICATION ............................................................................................................................... iii
ACKNOWLEGEMENT ................................................................ Error! Bookmark not defined.
LIST OF TABLES ....................................................................................................................... viii
LIST OF FIGURES ....................................................................................................................... ix
OPERATIONAL DEFINITION OF TERMS ................................................................................ x
ACRONYMS AND ABBREVIATION ........................................................................................ xi
ABSTRACT ................................................................................... Error! Bookmark not defined.
CHAPTER ONE ............................................................................................................................. 1
INTRODUCTION ......................................................................... Error! Bookmark not defined.
1.0 Background Information ...................................................... Error! Bookmark not defined.
1.1 Statement of the Problem. ..................................................................................................... 2
1.2 Justification ........................................................................................................................... 3
1.3 General Objective .................................................................................................................. 4
1.3.1 Specific Objectives ......................................................................................................... 4
1.4 Research Questions ............................................................................................................... 4
1.5 Scope of the study ................................................................................................................. 4
CHAPTER TWO ............................................................................................................................ 5
LITERATURE REVIEW ............................................................................................................... 5
2.0 Introduction ........................................................................................................................... 5
2.1 Cement Manufacturing in Kenya .......................................................................................... 5
2.2 Cement Manufacturing Process ............................................................................................ 7
2.2.1 Mining and Quarrying .................................................................................................... 7
2.2.2 Raw Material Preparation ............................................................................................... 8

vi
2.2.3 Clinker Production (Pyro-Processing) ............................................................................ 9
2.2.4 Finish Grinding ............................................................................................................. 10
2.3 Theoretical Review ............................................................................................................. 10
2.3.1 Social Ecology Theory ................................................................................................. 10
2.4 Risk factors contributing to occupational injuries............................................................... 16
2.4.1 Exposure to dust ............................................................ Error! Bookmark not defined.
2.4.2 Contact with allergic substance ..................................... Error! Bookmark not defined.
2.4.3 Exposure to noise........................................................... Error! Bookmark not defined.
2.4.4 Physical Injuries ............................................................ Error! Bookmark not defined.
2.5 Conceptual Framework ....................................................................................................... 20
2.6 Critique of Literature ........................................................................................................... 21
2.7 Summary ............................................................................................................................. 23
2.8 Research Gap....................................................................................................................... 24
CHAPTER THREE ...................................................................................................................... 26
RESEARCH METHODOLOGY.................................................................................................. 26
3.1 Introduction ......................................................................................................................... 26
3.2 Research design ................................................................................................................... 26
3.3 Population............................................................................................................................ 26
3.4 Sample size and Sampling Procedure ................................................................................. 26
3.5 Data Collection Instruments ................................................................................................ 28
3.6 Data collection procedure.................................................................................................... 29
3.7 Testing of Instruments ......................................................................................................... 29
3.7.1 Reliability ..................................................................................................................... 29
3.7.2 Validity Tests ................................................................................................................ 29
3.8 Data analysis and Presentation ............................................................................................ 30

vii
3.9 Ethical Consideration .......................................................................................................... 30
CHAPTER FOUR ......................................................................................................................... 31
DATA ANALYSIS, INTERPRETATION AND DISCUSSION ................................................ 31
4.1 Introduction ......................................................................................................................... 31
4.2 Response Rate ..................................................................................................................... 31
4.3 Demographic Information ................................................................................................... 32
4.3.1 Gender .......................................................................................................................... 32
4.3.2 Age................................................................................................................................ 33
4.3.3 Respondents Work Experience ..................................................................................... 33
4.3.4 Education ...................................................................................................................... 34
4.4 The Causes of Accidents and Injuries among Workers ...................................................... 35
4.5 Risk Factors of Occupational Injuries among Workers ...................................................... 37
4.6 Challenges Facing Control of Accidents ................................................................................ 40
CHAPTER FIVE .......................................................................................................................... 41
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS................................................. 41
5.1 Introduction ......................................................................................................................... 41
5.2 Summary of Findings .......................................................................................................... 41
5.3 Conclusions ......................................................................................................................... 42
5.4 Recommendations ............................................................................................................... 43
5.5 Suggestions for Further Research ....................................................................................... 44
REFERENCES ............................................................................................................................. 45
APPENDIX 1: COVER LETTER ................................................................................................ 48
APPENDIX 3: STUDY WORK PLAN ........................................................................................ 52
APPENDIX 4: BUDGET ............................................................................................................. 53

viii
LIST OF TABLES
Table 4.1: Response Rate .............................................................................................................. 31
Table 4.2: Human factors .............................................................................................................. 36
Table 4.3: Environmental factors .................................................................................................. 37
Table 4.4: Mechanical factors ....................................................................................................... 37
Table 4.5: OHS risk factors and prevention measures .................................................................. 38

ix
LIST OF FIGURES
Figure 2.1: Simplified Process Schematic for Cement Making ...................................................... 8
Figure 2.2 Conceptual framework ................................................................................................ 20
Figure 4.1 Gender ......................................................................................................................... 32
Figure 4.2 Age .............................................................................................................................. 33
Figure 4.3 Work Experience ......................................................................................................... 34
Figure 4.4: Education .................................................................................................................... 34
Figure 4.4: Have you been involved in an accident? .................................................................... 35
x
OPERATIONAL DEFINITION OF TERMS
Hazard refers to the potential of any source that may cause harm to people (IAPA, 2007).
Injury is acute harm or damage to the body caused by exposure to physical energy (such as mechanical,
chemical, thermal etc.) in amounts or at rates that exceed the threshold of human tolerance (WHO,
2001).
Occupational accident- Accident occurring at the workplace which may cause damage to machinery,
tools or people
Occupational injury refers to any physical injury condition sustained on worker in connection with the
performance of his or her work in cement factories
Occupational safety - Risk identification at the workplace and preventive measures takes to reduce or
eliminate the hazard which may lead to accident.
Risk refers to the likelihood (probability) of injury or damage occurring to people as a result of exposure
to, or contact with, a hazard (Ridley & Channing, 1999).
Safety is a state in which hazards and conditions leading to physical or psychological harm are
controlled in order to preserve the health and well-being of individuals (WHO, 1998).

xi
ACRONYMS AND ABBREVIATION
ARM-Athi River Mining Limited
EAPCC-East Africa Portland Cement Company
FEV-Forced Expiratory Volume
ICD-International Classification of Diseases
ILO-International Labour Organization
OSH-Occupational Safety and Health
PEFR-Peak Expiratory Flow Rate
PPEs-Personal Protective Equipments
SPSS-Statistical Packages for Social scientists

xii
ABSTRACT
Since the ancient times, cement has been considered an essential component of infrastructure
development and most important input of construction industry. However, multiple of risks associated
with cement manufacturing processes often pose a danger to both the employer and the employees.
Statistics in the cement manufacturing shows increase in occupational injuries and diseases in the world
especially in developing countries. The aim of this study was to assess the risk factors contributing to
occupational injuries among cement workers; the study was guided by specific objectives; to find out
causes of accidents and injuries, to assess the distribution of occupational injuries and to determine
common risk factors of occupational injuries among workers in East African Portland Cement
Company. The study employed descriptive cross sectional study, stratified and simple random sampling
method. Data was collected through questionnaires, observational checklist and interviews. A total of
125 respondents duly filled and returned the questionnaires giving a respond rate of 65.25%.Majority of
the respondent were male (56%), mean age of between 36-46 years. The literacy level was high since
majority of the respondents had a minimum education level of o level (31%), college (40%) university
(29%).with work experience of (5-7 years 42%).Data analysis was done using SPSS and Microsoft
excel, presentation was done using bar graphs, pie charts and tables. (32%) of the respondents had
experienced injuries for the last one year. This is significant to the study since the respondents were able
to articulate the causes of the occupational injuries, which include use of heavy machinery, splintering
objects, falls, contact with hot surfaces, and falling objects. They also agreed that human, environmental
and machinery were the main risk factors causing occupational injuries. The research Findings
concurred with other study done among factory workers in Addis Ababa which demonstrated that the
most frequent causes of occupational injury were machinery 42 (29.4%), Human 29 (20.3%) and
environmental factors. The study showed distribution of the occupational injuries cut across all the
departments with process recording the highest (11), packing plant (10) Mechanical (9) Electrical (7)
mining (6) dispatch and logistic (5) administration (2).The study revealed that eyes, fractures, burns, cut
wounds and back injuries were the most common occupational injuries experienced. Therefore,
protecting the health and safety of people in the workplace is a community expectation that makes good
business sense. This empirical study set a base for further advanced studies on risk factors contributing
to occupational ill health as it will be beneficial to the scholars and researchers.

1
1.0 Background Information
Globally, majority of adults and children devote much of their working hours at work. Work
provides numeral economic and other benefits to the society. At the same time, people at work
face a variety of hazards owing to chemicals, biological agents, physical factors, adverse
ergonomic conditions, allergens, a complex network of safety risks, and many and varied
psychological factors. In addition to injuries, more than 100 occupational diseases have been
classified according to the tenth revision of the International Classification of Diseases and
Related Health Problems (ICD-10). Broadly, these include respiratory, musculoskeletal,
cardiovascular, reproductive, neurotoxin, skin and psychological disorders, hearing loss and
cancers (David, et al. 2005).
Factories represent one of the most important strategic manufactures and a basic element in the
economic development of any country. Workers in factories constitute an important productive
aggregate in the community (David, et al., 2005 & Baskett, 2007). Work is viewed as important
to one’s life experience; most adults spend about fulfilling one third of their time at work. About
45% of the world’s population and 58% of the population over 10 years of age constitute the
global workforce (Rodgers, 2010) and (Gupter, & Ghai, 2007).
Occupational accidents and diseases cause great economical loss and human suffering and loss
(Prashar, 2008). The economic cost is high and takes different dimensions yet public awareness
of occupational safety and health (OSH) impacts tends to be low (ILO-OHS, 2010).
Unfortunately, OHS awareness it does not get the priority it merits both at national and
organizational level. Many countries all over the world have domesticated international laws and
regulations on occupational health and safety to suit their requirements. For instance, in Kenya,
the Occupational Health and Safety Act 2007 was enacted in 2007 as a policy document in
controlling hazards. It spells out the responsibility of both the employer and the worker in
ensuring a healthy worker by ensuring safe working environment and safe working practices for
the welfare of all workers. Cement use has increased steadily in Kenya over the years due to
increase in construction activities and expansion of infrastructure for development with the aim
of achieving the vision 2030. The increased demand for construction materials has consequently
2
led to an increase in production of cement (“The Global Cement Report,” 2011). It is however
necessary for cement producing companies to increase the number of employees and to upgrade
their production technology to accommodate this increase in the demand for cement. Cement
factories are considered to be highly exposed to pollutants in terms of particulate emission and
exposure to such environments could have acute or chronic health implications. Cement workers
have been shown to be susceptible to a lot of life threatening debilities or health problems, which
can be attributed to their working environment as these factories are characterized by dusty
environment and the use of heavy machinery (Pournourmohammadi et al., 2008). Cement
manufacturing is associated with many risk factors and workers expose themselves to many
occupational hazards that cause diseases and injuries at work.
Many risk factors cause more than one type of outcome of interest. For example, exposure to
asbestos can result in malignant conditions of the lung and the pleura, malignant conditions of
the peritoneum, and nonmalignant conditions of the lung (asbestosis). Some exposures, such as
occupational noise, are well characterized. Others have not been well characterized or are multi-
faceted, but the condition they cause is clear (such as occupational injuries). It is against this
background that the study seeks to assess the risk factors contributing to occupational injuries in
East African Portland Cement Company.
1.1 Statement of the Problem.
The International Labor Organization (ILO, 2008) estimate that more than 2Million workers die
each year from work related accidents and diseases. It further estimates 270 million suffer
accidents and at least 335,000 fatal injuries occur annually. This accounts for 4% of the world’s
Gross domestic product (GDP) (USD 1.25 Trillion. In Africa according to Southern African
Development community (2013) report indicates 49.42 injuries per 1000 workers and a fatally of
2.6 per 1000 workers. In Kenya according to Directorate of Occupational Health and Safety
Services (2003) in 9 districts reported 11,540 occupational accidents of which 145 were fatal and
9 occupational illnesses. In EAPCC more than five employees go on sick leave monthly due to
occupational health and safety related issues. In the same year (2015) 29 occupational accidents
and illness were reported from different departments. Workers in the cement sector are exposed
to many occupational hazards which may contribute to diseases and work injuries. Work exposes
workers to different hazards, which may have tremendous harmful effect on their health. These

3
hazards may result from physical, chemical or mechanical agents. The chemical hazards arise
from excessive airborne concentrations, chemicals could occur through either inhalation, dermal
or ingestion and through contaminated hands. Occupational injuries such as trauma fracture and
wounds represent the leading cause of morbidity and mortality among workers. It is against this
background that the study seeks to assess the risk factors contributing to occupational injuries
among cement workers in East Africa Portland Cement.
1.2 Justification
In order to contain any anticipated adverse health outcomes associated with the increase in
construction activity, it is important to also ensure that these activities do not adversely affect the
health of cement workers and all those involved in these construction activities. It is therefore
imperative to investigate risk factors contributing to occupational injuries among cement
workers, build a baseline database on common health problems among cement workers in Kenya
and the analysis of which should guide occupational health policy reforms in cement production
industry in the country. Therefore, the rationale of the study will be to provide data on the
common health problems faced by cement workers in Kenya and to know whether the cement
workers are aware of the potential dangers they face during routine work. The research will
provide information for the effective planning and organization of safety measures and
implementation of policies that would improve the health status of workers by ensuring that
cement manufacturers maintain high safety records. This empirical study will set a base for
further advanced studies on risk factors contributing to injuries as it will be beneficial to the
scholars and researchers.

4
1.3 General Objective
The main objective of the study was to assess risk factors contributing to occupational injuries
among cement workers with specific reference to East African Portland Cement Company.
1.3.1 Specific Objectives
i. To find out causes of accidents and injuries among workers in East African Portland
Cement Company.
ii. To assess the distribution of occupational injuries among workers in East African
Portland Cement Company.
iii. To determine common risk factors of occupational injuries among workers in East
African Portland Cement Company.
1.4 Research Questions
i. What are the causes of accidents and injuries among workers in East African Portland
Cement Company?
ii. What is the distribution of occupational injuries among workers in East African Portland
Cement Company?
iii. Which are the common risk factors of occupational injuries among workers in East
African Portland Cement Company?
1.5 Scope of the study
The study sought to assess the risk factors contributing to occupational injuries among cement
workers with reference to East African Portland Cement Company. The respondents will be
drawn from East African Portland cement workers in the factory.

5
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This chapter provides a detail review of relevant literature on the tenets required to find answers,
connect to the research questions and justify the hypothesis. This chapter covers theoretical
review, conceptual framework, critique of literature, summary and research gap.
2.1 Cement Manufacturing in Kenya
Cement known as adhesive is a fine, gray powder which sets and then hardens into a solid,
strong material. It is mainly used to make concrete and mortar for construction. Cement is made
by heating limestone with other materials (such as clay) to get ‘clinker’ which is further
processed to make Cement. Cement is a vital product and the key constituent of concrete. In
Kenya, cement history started in the early 1930s when in 1933, East Africa Portland Cement
(EAPCC) began as a trading company importing cement. Blue Circle Industries of United
Kingdom formed the company. The plant’s initial capacity was 60,000 tonnes a year, but
presently it stands at 700,000 tonnes a year. EAPC targets 1.3 million tones towards end of year
2007 (www.eastafricanportland). EAPC has a market capitalization of 10 billion (NSE, 2014). In
1951, Bamburi Cement Ltd was founded and Lafarge a company from France is the principal
shareholder of Bamburi Cement Ltd. At inception the annual capacity was 140,000 tonnes of
cement but at present it stands at 2.1 million tonnes a year and a market capitalization of 70
billion shilling (www.bamburicement.com). ARM (Kenya) was established in 1974 and its
principle shareholder is the Paunrama family.
Initially it was a mineral extraction and processing company and later in 1996, the cement
division began operation. The company targets a capacity production of 200,000 tonnes a year by
end of 2007 and has a market capitalization is 8.7 billion (www.armkenya.com). The Kenyan
Cement industry has mainly been dominated by Bamburi Cement Company Limited a subsidiary
of Lafarge Company based in France. The indigenous cement companies in Kenya are Athi
River Mining and East African Portland Cement Company Limited. Bamburi Cement Company
derives tremendous advantages from being part of the Lafarge group, including access to cutting

6
edge technologies for cement manufacture, management and technical support. The second
largest player in the industry is Athi River Mining Limited (ARM) which is separated into two
distinct divisions; ARM Cement Ltd which concentrates on cement, lime and related products
and ARM Minerals and Chemicals for the manufacture and sale of minerals and specialty
building and related products. East African Portland Cement Company Ltd (EAPCC) is the third
largest cement manufacturer which concentrates on cement only. It is effectively government
controlled through a direct government stake and indirectly through National Social Security
Fund (Kenya Economic Survey, 2010).
Several challenges confront the cement industry which include high cost of electricity due to
high tariffs as well as inadequate power supply, costly imported coal, small capacities for clinker
and cement production, lobbying for the introduction of concrete roads in Kenya that will require
plenty of cement and inadequate support from the government on policy issues. The industry is
also confronted by poor quality of power due to interruptions/outages leading to inefficiencies in
production systems and breakdowns and high cost of transport caused by dilapidated roads. The
Kenyan cement industry has seen the entry of four new foreign investors who have established
cement plants in the country in the recent past. One of this is Mombasa Cement which is a
subsidiary of Tororo Cement Company in Uganda and is producing with the help of Taiheiyo
Cement Corporation, the largest cement producer in Japan. This foreign based company is
equipped with advanced technology which enables it to produce more efficiently hence offering
lower prices. The other companies are National Cement Company Limited (Devki Group) and
Savannah Cement Limited (Kenya Economic Survey, 2010).
The demand for cement in Kenya is estimated to be about 3 million tons per year. The seven
companies produce about 3.5 million tons, of which Bamburi Cement produces 2.3 million tons.
These companies also export their products to other neighboring countries including Somalia,
Democratic Republic of Congo, South Sudan, Mozambique, Rwanda and Burundi (Mumero,
2011). The increased purchase of cement is attributable to continued demand for housing and
accommodation due to increase in Kenya’s population. Increased private building projects and
also increased government expenditure on roads and building projects caused the increase in
cement consumption during the past 3 years (Kenya Economic Survey, 2010).

7
2.2 Cement Manufacturing Process
Since calcium silicates are the primary constituents of Portland cement, the raw material for the
production of cement must provide calcium and silica in suitable forms and proportions.
Naturally occurring calcium carbonate materials such as limestone, chalk, marl, and sea-shells
are the common industrial sources of calcium, but clay or dolomite (CaCO3.MgCO3) are usually
present as impurities. Clays and shales, rather than quartz, are the preferred sources of additional
silica in the raw-mix for making calcium silicates because quartizitic silica does not react easily
with lime.
2.2.1 Mining and Quarrying
The most common raw materials used for cement production are limestone, chalk and clay. The
major component of the raw materials, the limestone or chalk, is usually extracted from a quarry
adjacent to or very close to the plant. Limestone provides the required calcium oxide and some
of the other oxides, while clay, shale and other materials provide most of the silicon, aluminum
and iron oxides required for the manufacture of portland cement. The raw materials are selected,
crushed, ground, and proportioned so that the resulting mixture has the desired fineness and
chemical composition for delivery to the pyroprocessing systems (see Figure 2.1). It is often
necessary to raise the content of silicon oxides or iron oxides by adding quartz sand and iron ore,
respectively. The quarried material is reduced in size by processing through a series of crushers.
Normally primary size reduction is accomplished by a jaw or gyratory crusher, and followed by
secondary size reduction with a roller or hammer mill. The crushed material is screened and
stones are returned. More than 1.5 tons of raw materials are required to produce one ton of
portland cement (Greer et al., 1992; Alsop & Post, 1995).

8
Figure 2.1: Simplified Process Schematic for Cement Making
2.2.2 Raw Material Preparation
After primary and secondary size reduction, the raw materials are further reduced in size by
grinding. The grinding differs with the pyroprocessing process used. In dry processing, the
materials are ground into a flowable powder in horizontal ball mills or in vertical roller mills. In
a ball (or tube) mill, steel-alloy balls (or tubes) are responsible for decreasing the size of the raw
material pieces in a rotating cylinder, referred to as a rotary mill. Rollers on a round table fulfill
this task of comminution in a roller mill. Utilizing waste heat from the kiln exhaust, clinker
cooler hood, or auxiliary heat from a stand-alone air heater before pyroprocessing may further
dry the raw materials. The moisture content in the kiln feed of the dry kiln is typically around
0.5% (0 - 0.7%).
When raw materials are very humid, as found in some countries and regions, wet processing can
be preferable. In the wet process, raw materials are ground with the addition of water in a ball or
tube mill to produce slurry typically containing 36% water (range of 24-48%). Various degrees

9
of wet processing exist, e.g. semi-wet (moisture content of 17-22%) to reduce the fuels
consumption in the kiln.
2.2.3 Clinker Production (Pyro-Processing)
Clinker is produced by pyroprocessing in large kilns. These kiln systems evaporate the inherent
water in the raw meal, calcine the carbonate constituents (calcination), and form cement minerals
(clinkerization). The main pyroprocessing kiln type used is the rotary kiln. In these rotary kilns a
tube with a diameter up to 25 feet is installed at a 3-4 degree angle that rotates 1-3 times per
minute. The ground raw material, fed into the top of the kiln, moves down the tube
countercurrent to the flow of gases and toward the flame-end of the rotary kiln, where the raw
meal is dried, calcined, and enters into the sintering zone. In the sintering (or clinkering) zone,
the combustion gas reaches a temperature of 3300–3600 °F.
In a wet rotary kiln, the raw meal typically contains approximately 36% moisture. These kilns
were developed as an upgrade of the original long dry kiln to improve the chemical uniformity in
the raw meal. The water (due to the high moisture content of the raw meal) is first evaporated in
the kiln in the low temperature zone. The evaporation step makes a long kiln necessary. The
length to diameter ratio may be up to 38, with lengths up to 252 yards. The capacity of large
units may be up to 4000 short tons of clinker per day.
In a dry rotary kiln, feed material with much lower moisture content (0.5%) is used, thereby
reducing the need for evaporation and reducing kiln length. The first development of the dry
process took place in the U.S. and was a long dry kiln without preheating (Cembureau, 1997).
Later developments have added multi-stage suspension preheaters (i.e. a cyclone) or shaft
preheater. Pre-calciner technology was more recently developed in which a second combustion
chamber has been added between the kiln and a conventional pre-heater that allows for further
reduction of kiln fuel requirements. Once the clinker is formed in the rotary kiln, it is cooled
rapidly to minimize the formation of a glass phase and ensure the maximum yield of alite
(tricalcium silicate) formation, an important component for the hardening properties of cement.
The main cooling technologies are either the grate cooler or the tube or planetary cooler. In the
grate cooler, the clinker is transported over a reciprocating grate through which air flows

10
perpendicular to the flow of clinker. In the planetary cooler (a series of tubes surrounding the
discharge end of the rotary kiln), the clinker is cooled in a counter-current air stream. The
cooling air is used as secondary combustion air for the kiln.
2.2.4 Finish Grinding
After cooling, the clinker can be stored in the clinker dome, silos, bins, or outside. The material
handling equipment used to transport clinker from the clinker coolers to storage and then to the
finish mill is similar to that used to transport raw materials (e.g. belt conveyors, deep bucket
conveyors, and bucket elevators). To produce powdered cement, the nodules of cement clinker
are ground to the consistency of face powder. Grinding of cement clinker, together with
additions (3-5% gypsum to control the setting properties of the cement) can be done in ball mills,
ball mills in combination with roller presses, roller mills, or roller presses. While vertical roller
mills are feasible, they have not found wide acceptance. Coarse material is separated in a
classifier that is re-circulated and returned to the mill for additional grinding to ensure a uniform
surface area of the final product. Traditionally, ball mills are used in finish grinding, while many
plants use vertical roller mills. In ball or tube mills, the clinker and gypsum are fed into one end
of a horizontal cylinder and partially ground cement exits from the other end.
2.3 Theoretical Review
2.3.1 Social Ecology Theory
Social ecology theory considers the interrelationship between personal and environmental factors
in human health and illness (Stokols, 1996). Its roots derive from public health and epidemiology
but now also encompass other aspects such as health and safety (Green, Richard & Potvin,
1995). Its use in injury prevention stems from the recognition that large scale public health issues
such as occupational injury are too complex to be explained by a single orientation (Stokols,
1996). There is growing recognition that individual behavioral strategies to encourage safe
practice may be ineffective in a culture with an unsupportive environment or unfavorable social
norms (Schmid, Pratt & Howze, 1995). Therefore, interventions must be directed at multiple
levels and multiple sections (Green et al., 1995). These multiple levels range from immediate
peers and friends to cultural and organizational norms. Multiple sections include home, work,
community and national environments.

11
Stokols (1996) describes several core principles of social ecology. The first principle accepts that
environmental settings have multiple physical, social and cultural “dimensions” that influence
health outcomes. By this principle the environment may have a cumulative effect on health as
well as a specific influence. A second principle of social ecology holds that personal attributes
such as genetics, psychological dispositions (personality) and behavior, along with
environmental factors, influence health. Therefore, environmental conditions that adversely
affect one individual may hold little significance to another. Consequently, researchers in social
ecology have found that compatibility with one’s surroundings is an important predictor of well-
being (Stokols, 1996). Social ecology also considers the premise of passive interventions in
addition to more traditional active interventions (Stokols, 1996). Active interventions require that
an individual perform voluntary and sustained effort to enact behavioral change. That is, the
individual must actively work to change behavior. However, behavioral interventions requiring
active participation have been difficult to sustain over prolonged periods of time. Passive
interventions, by contrast, can be more effective in that they target larger numbers of individuals
simultaneously and may not require voluntary or sustained effort on the part of the individual
(Stokols, 1995). Public service announcements promoting injury prevention are examples of
passive intervention. Lastly, social ecology approach to health promotion and injury prevention
is highly integrated with other disciplines. No one perspective is considered singularly.
Ecological approaches consider a variety of preventive strategies including public health and
epidemiology, behavioral and social sciences, and cultural change models.

12
2.4 Literature Review
2.4.1 Causes of accidents and injuries among workers
Accidents are viewed as originating from a technical or human error. The multiple accidents
causation theory postulates that there are many contributory causes leading to an accident. The
causes are categorized into behavioral and environmental factors. Behavioral factors include
attitudes, skills and knowledge. Environmental factors include Worksite hazards and procedures
that contribute to injuries (Makhonge, 2005). Found that the causes of construction accidents in
Uganda include a lack of knowledge about safety rules, engaging an inexperienced workforce,
and lack of respect for safety. The main factors affecting safety in China were managers’ poor
safety awareness, lack of training, reluctance to commit resources to safety, and reckless
operations. The major reasons for serious and mortal accidents are inexperienced employees,
lack of qualifications and understanding risk on a construction site (Obure, 2002).
Smailyte, Kurtinaitis and Andersen (2004) carried out a survey in Malaysia to identify the causes
of accidents on construction sites; they found that unsafe methods, including incorrect
procedures, knowledge level, and disobeying procedures are the most frequent reasons for
accidents on construction sites. In addition to these causes, secondary causes of accidents
centered on management pressures, such as financial restrictions, lack of commitment,
inadequate policy and standards, deficient knowledge and information, restricted training and
task selection, and poor quality control systems. He further emphasized that incomplete
structural connections, temporary facilities, tight work areas, varying work surface conditions,
continuously changing work-sites, multiple operations and crews working in close proximity are
common causes of construction-related deaths and injuries.
The five main sources of accidents on construction sites include site conditions such as the
nature and physical layout of the work, location and weather, equipment and materials
specification such as paint and asbestos that have the potential to cause illhealth problems. The
human factors include human behavior, competence, attitude and management such as leadership
and safety culture of the organization. The job factors include the nature of the task, design,

13
detail, duration and the size of the structure itself. Also, the causes of accidents are due to
worker turnover and false acts; inadequate safety performance; improper cleaning and unusable
materials; destiny; low tool maintenance; supervisory fault; and misplacing objects (Ribeiro,
2002).
Zeleke (2011) conducted a more comprehensive study in the USA and classified the causes into
human and physical factors. Human factors were due failed to secure and warn; Failed to wear
personal protective equipment (PPE); horseplay; operating equipment without authority;
operating at unsafe speed; personal factor; remove safety device; serviced moving and energized
equipment; took unsafe position or posture; used defective tool or equipment; and other unsafe
action. While, physical factors were due to; unsafe act of another person(s); disregard known
prescribed procedures; defects of accident source; dress or apparel hazard; environmental hazard;
fire hazard; hazardous arrangement; hazardous method; housekeeping hazard; improper
assignment of personnel; inadequately guarded; public hazard; and other unsafe conditions.
Mathias (1990) in a study in Uganda and concluded the causes of accidents were mainly due to
lack of awareness of safety regulations; lack of enforcement of safety regulations; poor regard
for safety by people involved in construction projects; engaging incompetent personnel; non-
vibrant professionalism; mechanical failure of construction machinery/equipment; physical and
emotional stress; and chemical impairment. Hazards are classified into the most influential
factors i.e. unique nature of the industry; job site conditions; unsafe equipment; unsafe methods;
human elements; and management factors. They further concluded that major immediate causes
were due to failure to use personal protective equipment; improper loading or placement of
equipment or supplies; failure to warn co-workers or to secure equipment; and improper use of
equipment.
Makhonge (2005) in a study suggested that the causes of accidents were due to lack of proper
training; deficient enforcement of safety; safety equipment not provided; unsafe methods or
sequencing; unsafe site conditions; not using provided safety equipment; poor attitude toward
safety; and isolated and sudden deviation from prescribed behavior. The causes of accidents were
due poor safety awareness from top leaders; lack of training; poor safety awareness of project
managers; reluctance to input resources for safety; reckless operation; lack of certified skill

14
labor; poor equipment; lack of first aid measures; lack of rigorous enforcement of safety
regulation; lack of organizational commitment; low education level of workers; poor safety
conscientiousness of workers; lack of personal protective equipment (PPE); ineffective operation
of safety regulation; lack of technical guidance; lack of strict operational procedures; lack of
experienced project managers; shortfall of safety regulations; lack of protection in material
transportation; lack of protection in material storage; lack of teamwork spirits; excessive
overtime work for labor; shortage of safety management manual; lack of innovative technology;
and poor information flow.
2.4.2 Distribution of occupational injuries among workers
In a case study conducted in Bangladesh, it was found that arm, leg, hand finger, Eye and head
covered 82.81% of total injury frequency and 76.56% of total injuries were by welding, bucket
elevator, belt conveyor and weight lifting. The study reported that workers in the age group of
21-25 and 51-55 were more exposed to injuries and low experienced and high experienced
workers have 84.38% of total injury frequency. Most (78.13%) of injury occurred by highly
skilled and unskilled workers. Insufficient supply of Personal Protective Equipment, poorly
maintained Personal Protective Equipment, discomfort when using Personal Protective
Equipment and overconfidence were found to be the major causes of injury (Buckley, 2016).
In a study done in Cairo, Egypt 65.7 % of the studied sample were not wearing PPE, but only
34.3 % of workers used PPE.34.3 % of workers studied using aprons as one of PPE followed by
goggles (28.0%).Concerning availability of PPE (78.0%) reported that they are not enough in
their work area before health promotion program which they differed in post test program to be
enough as reported by the majority (85.8%). There were good ventilation, sufficient light and fire
extinguisher in the factory, ambulance car, and medical clinic inside the factories, pre
employment examination. There were also punishment for those workers not using PPE,
presence of leisure time for journeys, emergency plan in cases of emergency, application of
emergency plan on real ground and presence of specific employees to identify occupational risks.
In addition, there was presence of internal auditors to cFheck safety, presence of medical records
for each worker and part time during working day. However, there was no enough space between
machines, no periodic medical examination, no periodic checking of PPE, no periodic workers

15
training on occupational safety, no role of internal auditors is played and no computerizing of
medical records (Badri and Saeed, 2008).
In a cross sectional study done in Afar, Workers between 17 to 29 age, workers who used to
work more than 48 hours per week , workers without health and safety training, workers addicted
to alcohol and workers with sleeping disorders were associated significantly with occupational
injury. Sex, educational level, monthly salary, job category, work experience, job satisfaction
and use of personal protective devices did not show an association with occupational injury. In a
cross sectional study done in Kombolcha textile factory, educational status and marital status of
workers showed statistically significant association with occupational injury. Workers who had
only 1–8 years of education were more likely to report work-related injury than those with more
than nine years of education. Hours worked per week, manual handling of very heavy objects
(>20 kg), need for visual concentration for the task, maintenance of machine and sleep disorder
also showed significant association with work-related injury. Workers who were used to work
>48 hours per week were more likely to be injured than those spend 48 hours or less. Workers
who had sleep disorder in their workplace were almost 3-times more likely to report work-related
injuries than their counterparts. But, age, sex, employment pattern, monthly income, working
experience, safety supervision, health and safety training, drinking alcohol, chewing chat, job
satisfaction and using PPE did not show significant associations with occupational injuries
(Badri and Saeed, 2008).
Workers who were young, less experienced, daily laborer, mechanic and welder by job category,
sleep disorder, working 48 hours or below per week, job satisfaction and workplace supervision,
were significantly associated with occurrence of occupational injuries. Respondents who worked
48 hours and below per week and those who supervised regularly at the time of the survey were
less likely to experience work related injury than those who were worked more than 48 hours per
week and not supervised. Whereas sex, educational level, marital status, monthly salary, health
and safety training, alcohol consumption, chewing chat, use of PPE, were not associated with
occupational injury in a study done among small and medium scale industrial workers in North
Gondar (10). A Case Control Study among textile factory workers in Amhara regional state
revealed that sex, age, training on health and safety, sleeping disorder, job stress were associated

16
with occupational injury .Workers who complained problems of sleeping disturbance were more
likely to report two times excess occupational injury compared with workers who did not report
problem of sleeping disturbance. Workers who were stressed due to their job were about 2 times
more likely to report occupational injury compared with workers who were not stressed due to
their job. However religion, ethnicity, marital status, educational level, employment condition,
monthly salary, work experience, work place supervision, chat chewing, cigarette smoking,
alcoholic drink consumption, job dissatisfaction and use of PPE and did not show significant
association with occupational injury (Al-Neaimi, Gomes and Lloyd, 2001).
2.4.3 Risk factors contributing to occupational injuries
In the cement manufacturing industry there is the use of potentially hazardous materials and
processes, which occur on a large scale as well as being labour intensive. Some of the health
hazards that can be attributed to cement manufacturing industry include exposure to dust, high
temperatures and noise, contact with allergic substances and injuries relating to slips and falls
and machinery hazards (Marlowe & Mansfield, 2002).
Workers of cement factories are exposed to cement dust at various stages of the manufacturing
which include quarrying and handling of raw materials, during the manufacturing and grinding
of the raw materials into clinker, blending and addition of additives and finally packaging and
shipping of the finished products. Main entries of cement dust particles into the body are by
inhalation or swallowing as such its target of deposition is the respiratory tract and the
gastrointestinal tract respectively with skin and eye contact being minor. Their physical and
chemical property of importance includes particle size and density, shape and penetrability,
surface area and the respiratory response to its alkalinity making its pathogenesis probably due to
its irritating, sensitizing and pneumoconiotic properties (Meo, 2004).
According to Meo et al. (2008) occupational exposure to cement dust can cause various health
problems. General clinical manifestations of cement workers due to exposure to cement dust
includes chronic cough, phlegm production, impairment of lung function, chest tightness,
bronchial asthma, restrictive lung disease, skin irritation, conjunctivitis, stomach ache, watery
and itching eyes, headache, boils, fatigue as well as cancers of the lung, stomach and colon
(Oleru 1984). A study carried out by Maier et al. (1999) suggests that there is increased risk for
17
head and neck cancers among workers in the construction industry and can be attributed to
occupational carcinogenic agents such as cement dust, asbestos, tar products, paints, metal and
wood dust. This study also shows that among number of subject exposed to wood dust, organic
chemicals, and coal product or to cement showed an increases relative risk for head and neck
cancer after exposition to wood dust and cement with cancer risk due to cement exhibition
showing a positive correlation to the duration of exposition and remained 1999). Continuous
exposure of workers to cement dust have been shown to statistically significantly associated with
the development of pterigium and conjunctivitis. Mirzaee & Kebriaei showed that exposure to
cement dust is associated with acute respiratory symptoms and chronic ventilatory function
impairment such as wheezing, shortness of breath, cough, phlegm and dyspnae and was high
among the exposed workers than the unexposed workers (Mirzaee & Kebriaei, 2008).
Al-Neaimi, Gomes & Lloyd, (2001) demonstrated that inhalation of cement dust irritates the
respiratory epithelium leading to coughing, wheezing, dyspnoea, sinusitis, shortness of breath,
bronchitis and bronchial asthma being significantly greater among the exposed workers
compared to the unexposed workers. There was a high prevalence of respiratory symptoms
among workers of a cement factory in the United Arab Emirates and health problems such as
cough and phlegm were found to be related to exposure of dust, cumulative dust and smoking
habit with chronic bronchitis being related to smoking habit (Ahmed & Abdullah, 2012)
Merenu et al. (2007) and Smailyte, Kurtinaitis & Andersen (2004) suggests that chronic
exposure to cement dust impairs lung function with studies showing that lung function, vital
capacity and Forced Expiratory Volume (FEV) percentage were significantly lower in workers
exposed to cement dust compared to those unexposed and excess mortality risk from malignant
neoplasms and a borderline increased risk of death from lung cancer. Although occupational
exposure to cement dust leads to higher prevalence of respiratory symptoms, diseases and
impaired ventilatory functions smoking also increases the effect of these adverse effects (El-
Dine, Sadek, Zayet, & Mahfouz, 2004). The duration of exposure to cement dust shows that long
term exposure to the dust has significant impairment on lung functions (Meo, Al-Drees, Al
Masri, Al Rouq, & Azeem, 2013).

18
According to Badri & Saeed (2008) and Kakooei et al. (2011) reduction in Forced Vital
Capacity, Forced Expiratory Volume (FEV) and Peak Expiratory Flow Rate (PEFR) were
exposure to Portland cement dust may result in restrictive pulmonary diseases. Greater
prevalence of chronic respiratory symptoms and the reduction of ventilatory capacity among
cement workers has been reported to be due to chronic exposure to Portland cement dust (Yang
et al., 1996) and a study conducted by Al-Neaimi et al. (2001) has concluded that adverse
respiratory health effects that were observed among cement workers could not be explained by
age, BMI and smoking and therefore was probably caused by their exposure to cement dust. A
study to determine the effect of long term exposure to cement dust on lung function in non-
smoking cement mill workers shows significantly impaired lung functions in the mill workers
indicating that long term exposure to cement dust can affect lung functions (Meo et al., 2013).
A study conducted by Smailyte, Kurtinaitis & Andersen (2004) showed evidence of slightly
increased risk from rectal cancer and for colon cancer, members in the group with the highest
risk were those with the longest period of work since first exposure. Findings of a study
conducted among construction workers showed that male workers who regularly consume
alcohol and tobacco represent an extreme risk group for head and neck cancer as well as the need
for the concurrence of smoking and exposure to cement dust to produce severe respiratory
impairment (Maier et al. 1999).
Cohort studies carried out among workers of a cement plants for at least five years between the
years 1950 and 1980 concluded that there was no association between exposure to cement dust
and death from stomach cancer and this was attributed to the low statistical power given by the
cohort (Amandus, 1986) however findings from Koh et al. (2013) suggests a potential
association between exposure in the cement industry and an increased risk of stomach cancers
and rectal cancers.
“Contact of cement powder with moist skin or contact of skin with wet cement, can be very
irritating, however other ingredients, such as silica and other metal and alkali oxides will also
contribute to the cement” (Winder & Carmody, 2002). According to Winder & Carmody (2002),

19
cement dermatitis can be due to the high alkalinity nature of cement, which can damage the skin
directly and also the presence of chromates in cement produces sensitization. Studies conducted
among cement workers and construction workers in Taiwan showed that there were a high
percentage of the workers with occupational cement hand dermatitis with a greater portion of
them being sensitive to chromate and there was the advocacy for the regulation of the addition of
ferrous sulphate and the promotion of the use of personal protective equipments, improvement of
work practices and health education (Wang et al. 2011). Although dichromate is seen to be the
prominent allergen of construction workers, there is the need to address other important
occupational allergens such as thiurams, N Isopropyl-N’- phenyl-p-phenediamine (IPPD) and
cobalt and its prevention methods (Uter et al., 2004).
The main sources of noise pollution in a cement factory or plant are the grinding mills and the
exhaust fans and the control of noise pollution is by the use of silencers for the fans, room
enclosures for mill operators, noise barriers as well as the use of personal hearing protections if
the noise cannot be reduced (International Finance Coporation, 2007). A study conducted in a
cement factory in Tanga, Tanzania showed that noise pollution is a problem in cement factories,
and has adverse health effects on the workers, which in turn interferes with workers performance
(Mndeme & Mkoma, 2012). According to Hernández-Gaytán et al. (2000) and Soleo et al.
(1989), noise is a serious risk factor in certain areas such as the crude or baked mills department
of cement factories and increase number of hearing loss cases can be due to the occupational
noise exposure found in this industry.
Occupational injury is deemed to be a serious problem in any industry as injuries directly affect
the productivity of the industry through loss of productive hours as well as loss of money as
compensation. Studies conducted in selected cement industries in Bangladesh showed that
workers over 50 years of age were more prone to injuries, as well as most skilled and unskilled
personnel’s also being injured with most of these injuries were caused by welding, bucket
elevator and belt conveyor. Insufficient supply of personal protective equipments, poorly
maintained equipments, discomfort during the use of personal protective equipment and over
confidence also contributed to the causes of injuries (Iqbal et al., 2010). Unhealthy workplace
and work processes can put workers’ health at risk and this can be seen in a study conducted in
Brazil to evaluate work process and its effects on the health of workers in a cement factory
20
where levels of particulate matter and noise measured were of high values than maximum limits
set by the Brazilian legislation and opinions expressed by the workers (Ribeiro et al., 2002).
2.5 Conceptual Framework
A conceptual framework is a research tool intended to assist a researcher to develop awareness
and understanding of the situation under scrutiny and to communicate. According to Bogdan and
Mugenda and Mugenda (2003) a conceptual framework is a basic structure that consists of
certain abstract blocks which represent the observational, the experiential and the
analytical/synthetical aspects of a process or system being conceived. An independent variable is
that variable which is presumed to affect or determine a dependent variable. It can be changed as
required, and its values do not represent a problem requiring explanation in an analysis, but are
taken simply as given.
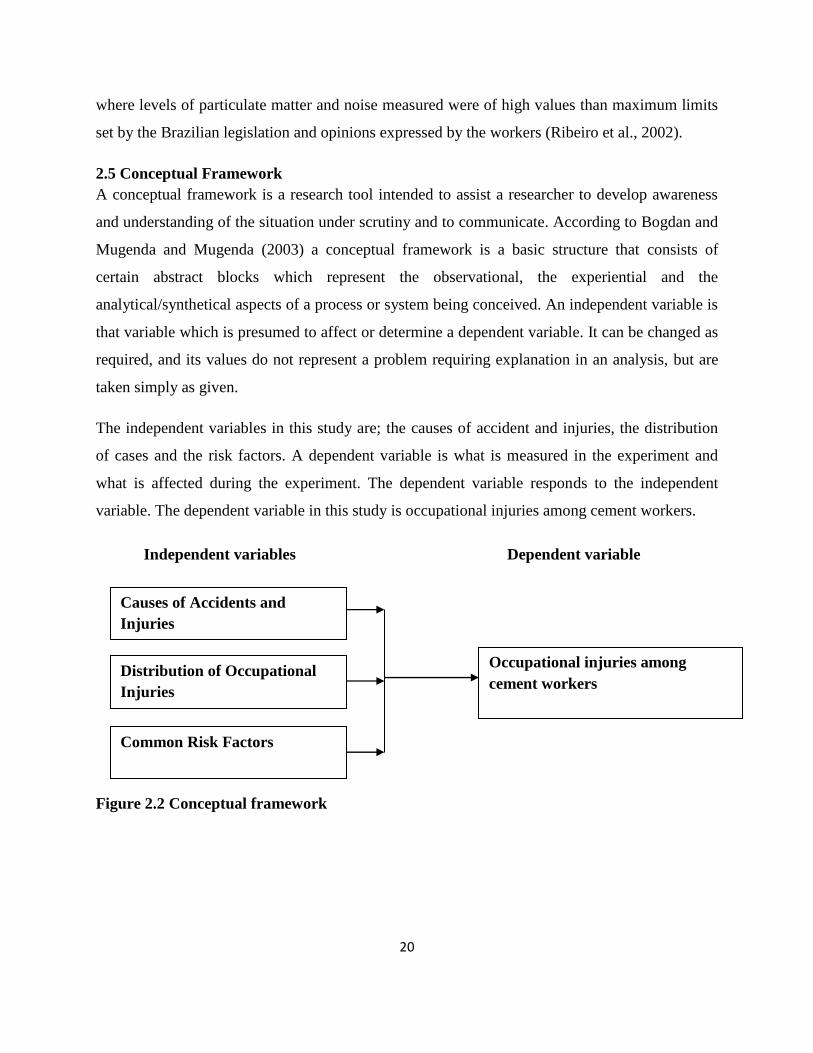
The independent variables in this study are; the causes of accident and injuries, the distribution
of cases and the risk factors. A dependent variable is what is measured in the experiment and
what is affected during the experiment. The dependent variable responds to the independent
variable. The dependent variable in this study is occupational injuries among cement workers.
Independent variables Dependent variable
Figure 2.2 Conceptual framework
Causes of Accidents and
Injuries
Distribution of Occupational
Injuries
Common Risk Factors
Occupational injuries among
cement workers

21
2.6 Critique of Literature
There are several potential and risk factors that leads to injuries. According to (Marlowe &
Manfield 2002) they state that '' in cement manufacturing industry there is use of potentially
hazardous materials and processes, which occur on a large scale as well as being labor
intensive". They further states that health hazards that can be attributed to cement manufacturing
industry include exposure to dust, high temperatures and noise, contact with allergic substances
and injuries relating to slips and falls and machinery hazards.
Meo (2014) articulates that cement factories workers are exposed to cement dust at various
stages. Main entries of cement dust particles into the body are by inhalation or swallowing as
such its target of deposition is the respiratory tract and the gastrointestinal tract while skin and
eye contact being minor. According to Meo et al. (2008) occupational exposure to cement dust
can cause various health problems. A study carried out by Maier et al. (1999) suggests that there
is increased risk for head and spinal injuries as a result of manual handling and fall from working
at height unsafely. According to Winder & Carmody (2002), cement dermatitis can be due to the
high alkalinity nature of cement, which can damage the skin directly. A study conducted in a
cement factory in Tanga, Tanzania showed that noise pollution is a problem in cement factories,
and has adverse health effects on the workers, which in turn interferes with workers performance
(Mndeme & Mkoma, 2012).
According to (Iqbal et.al.,2010) Physical Injuries Occupational injury is deemed to be a serious
problem in any industry as injuries directly affect the productivity of the industry through loss of
man hours as well as loss of money through compensation and direct medical bill. Other studies
conducted in selected cement industries in Bangladesh, showered that workers were more prone
to injuries, as well as most skilled and unskilled personnel’s also being injured with most of
these injuries were caused by welding, bucket elevator and belt conveyor. Insufficient supply of
personal protective equipments, poorly maintained equipments, discomfort during the use of
personal protective equipment and over confidence also contributed to the causes of injuries.

22
Dermal exposure to cement has been implicated in allergic dermatitis and inhalation of the dust
has been shown to play a part in some cases of laryngeal, stomach and lung cancer and
impairment of lung function (Smailyte, Kurtinaitis, & Andersen, 2004). Also epidemiological
studies have indicated that exposures to cement dust has health problems such as chest tightness,
phlegm production, skin irritations, conjunctivitis, catarrh, stomach ache, boils, chronic cough,
chronic bronchitis, burning, itching, runny eyes, headache, fatigue and biochemical alterations in
cement workers (Pournourmohammadi et al., 2008). Although several census-based studies have
shown an increased risk of cancer in cement factory workers, studies conducted by Pukkala,
(2011); Olsen & Sabroe (1984) concluded that this risk could also be attributed to other social
habits and life styles such as smoking.
The use of heavy machinery in such industries drives the need for skilled personnel but yearly
these experienced personnel are faced with various industrial accidents, which lead to different
types of occupational injuries. These occupational injuries have substantial effect on the
economy of the nation in that they cause major loss in productivity and productive hours, skilled
manpower, finances as well as a source of suffering to the victim and their families (Iqbal, Iqbal,
Taufiq, & Ahmed, 2010). Noise is a physical environmental factor that greatly affects human
health, the use of heavy machinery and equipments in the cement manufacturing process which
contribute large amount of noise to the industry is a cause for concern for safety and health of its
workers (Mndeme & Mkoma, 2012).
In Kenya, it is noted that cement workers have continued to suffer from injuries and illness due
to work related exposures (Makhonge, 2005). Accidents are financially, physically and
emotionally costly to individual workers, their families, their organizations and the nation as
whole. These risks can be minimized by use of personal protective equipments if properly
selected and worn by workers (Kirenga, 2004). Creating a safe and healthy workplace is
therefore crucial hence occupational health and safety is important to everyone at workplace
(Kirenga, 2004). Personal Protective Equipments (PPEs) plays a prominent role in ensuring
overall health and safety in cement factories. PPEs includes the clothes offering protection
against the weather which are intended to be worn or held against a person at work and which

23
provides protection against risks to his health or safety (OSHA, 2007). This study therefore seeks
to establish the risk factors contributing to occupational injuries among cement workers with
specific reference to East African Portland Cement Company.
2.7 Summary
From the literature review it is evident that health and safety measures are necessary in a work
place environment to ensure worker’s safety and well being so as: To maintain and improve
productivity and quality of work; To minimize absenteeism and labour turnover; To reduce
indiscipline and accidents; To improve employee motivation and morale; To reduce spoilage and
cost operations and; To reserve the physical and mental health of employees. But for this to be
realized a good health and safety management system and program should be put in place by
providing; a written statement of safety policy, organization and allocation of responsibilities for
health and safety matters, train employees in health and safety matters, establish safety
committee, ensure first aid facilities, provide appropriate procedures and documentations to
minimize accidents and to regularly consult with employee representatives.
Cement is produced through a series of processes including quarrying, crushing, milling,
blending, and kiln burning to form clinker, cement milling and packaging. Dust is emitted during
these processes. Exposure to dust produced during the cement manufacturing process is known
to cause chronic respiratory ailments in the form of cough, sputum, wheezing, dyspnea, chronic
bronchitis and adversely alter the pulmonary function indices.
The cement industry is one of the most vital industries for the Kenyan economy and a major
employer of labour from the production and consumption level (Ewuzie and Ibhafiden, 2010).
Occupational disease and injuries constitute a major health problem for cement workers in
Kenya. This is why several measures are established to protect workers health.
Control measures at source, path and persons exposed to the hazards, together with education in
occupational health and safety are the ideal means of preventing occupational diseases and
injuries from the manufacture of cement. Workers' knowledge about the hazards associated with

24
their jobs and workers education especially instructions on control and use of personal protective
measures will reduce and may even eliminate some occupational health risks.
2.8 Research Gap
According to Oxenburgh et al., (2004), the health and safety of all employees is closely linked to
the company’s productivity in all workplaces. In most cases, occupational safety and health
(OSH) is largely measured by negative outcomes such as workplace injury and illness but these
measures have a shortfall, for instance, a low incidence of injury does not necessarily mean that
adequate safety systems and controls are in place.
At some cement manufacturing factories, attention is mainly on negative outcomes. As long as
there are no serious accidents, occupational health and safety policies and practices are not
carried out fully. As a result, threats to employees’ safety are not eliminated in time because
accident-prone areas are not recognized and taken care of before accidents occur. It is therefore
important that the conditions that pose threat to the safety and health of the workers are identified
and addressed.
These studies done in Ethiopia by Senbeto (2011) indicated that there were different causes of
occupational injury. According to a study done in eleven urban industries in Addis Ababa, it was
indicated that being hit by or against objects and falling were the commonest causes of work-
related injuries. Findings of a study done among factory workers in Addis Ababa demonstrated
that the most frequent causes of occupational injury were machinery 42 (29.4%), and being hit
by or against objects 29 (20.3%). Department of Environmental Health in Ministry of Health in
Ethiopia reported that striking (25.5%), falling (12.8%), and flying objects from machines
(8.5%) were the major causes of occupational injury [17]. Similarly the Amahara regional
BOLSA reported that machinery (36.7%), mishandling (15.3%), falling (14.5%), and hand tools
(6.2%) were the commonly complained occupational injury types among manufacturing
industrial workers. The study focused on textile industry while the current study will be based on
cement industry.

25
All of the above studies except few were focused on the characterization of occupational injury
among industrial workers. However, to solve occupational health and safety problems of the
workforce, advanced epidemiological studies are essential for policy makers, public health
experts and program implementers Johansson, et al (2010). Therefore, this case study will be
designed to fill the gap by identifying the risk factors contributing to occupational injuries among
cement workers, which, is very important for the development and strengthening of legislations
and intervention priorities to safeguard the health and safety of the work force.
26
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Introduction
This chapter presents the research design, target population, sampling technique and sample size,
data sources and data collection instruments, data collection procedure and data analysis.
3.2 Research design
The study adopted and employed descriptive survey design which according to Mugenda and
Mugenda (2003) determines and reports the way things are. According to Kombo and Tromp
(2009) descriptive research design is suitable as it collects information about people’s attitudes,
opinions or habits.
3.3 Population
Polit and Hungler (1999) refer to the population as an aggregate or totality of all the objects,
subjects or members that conform to a set of specifications. In this study the population was all
employees in East Africa Portland Cement. The total population was 1687. All employees who
are directly engaged in the production process within the study period and who have been
working at least for one year in the selected factory irrespective of gender were included in the
study.
3.4 Sample size and Sampling Procedure
The role of sample size is crucial in all statistical analysis. According to Sivo et al.,
(2006), the more sophisticated the statistical analysis, the larger the sample size needed.
According to the sampling tables by Bartlett, et al (2001) calculated based on Krejcie and
Morgan’s 1970 table and Cochran’s 1977 sample size formula suggest at least 5
participants per construct and not less than 100 individuals per data analysis is suitable
sample size for a study. The total population was 1687. According to Mugenda
&Mugenda (2003). Cited that a sample representation of 10% to 30% is considered as
the true representation.

27
According to Neuman (2000), the size of a sample for a particular study will be calculated as
follows:
Where n = the required sample size, when the target population is more than 10,000
Z = is standard normal deviation at the required confidence level (1.96) at 0.05
p = is the proportion of the target population estimated to have the characteristics being
measured when one is not sure, so one takes middle ground (0.5)
q = 1-p
d = the level of statistical significance
Therefore n =
This gives a sample size of 384 which can be adjusted when population is less than 10,000 using
the following relationship (Neuman, 2000).
nf is the desired sample size when population is less than 10,000
n is the desired sample size when population is more than 10,000
N is the total population of the workforce =1687
nf= 384 = 192
1+384/1687
Therefore Sample size is 192.
The study thus applied simple random sampling. Using simple random sampling, the study
sampled 192 respondents as shown in the formula above.
28
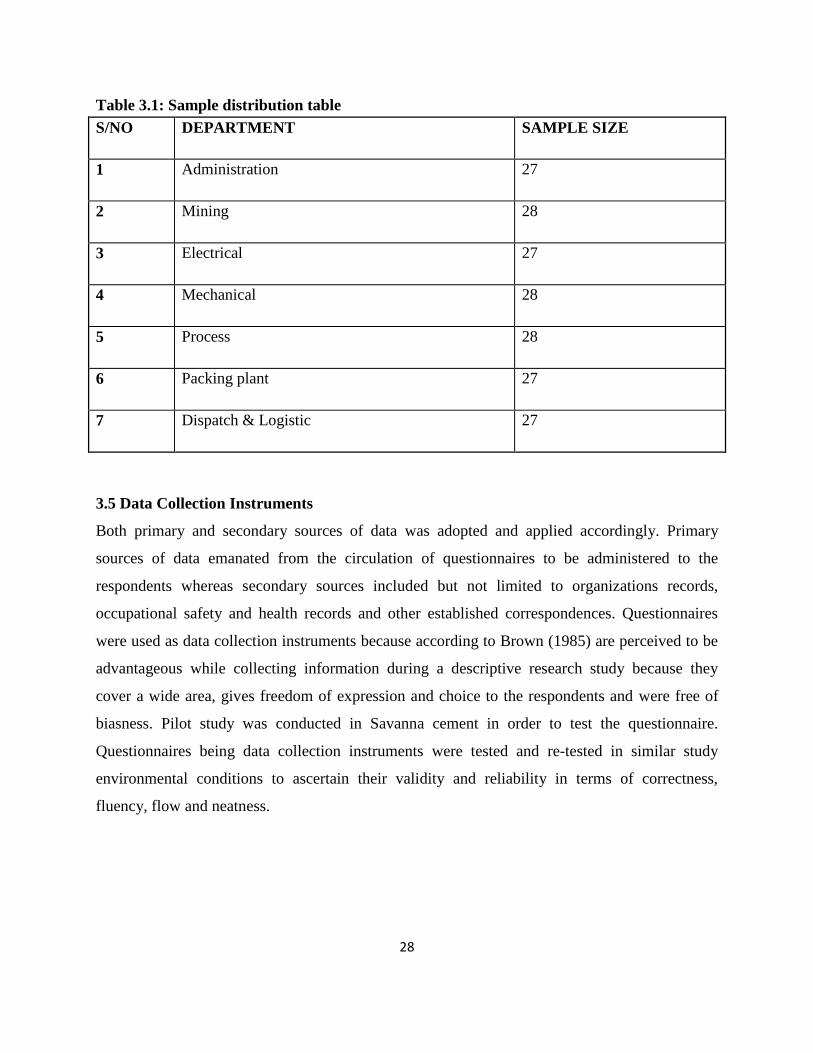
Table 3.1: Sample distribution table
S/NO DEPARTMENT SAMPLE SIZE
1 Administration 27
2 Mining 28
3 Electrical 27
4 Mechanical 28
5 Process 28
6 Packing plant 27
7 Dispatch & Logistic 27
3.5 Data Collection Instruments
Both primary and secondary sources of data was adopted and applied accordingly. Primary
sources of data emanated from the circulation of questionnaires to be administered to the
respondents whereas secondary sources included but not limited to organizations records,
occupational safety and health records and other established correspondences. Questionnaires
were used as data collection instruments because according to Brown (1985) are perceived to be
advantageous while collecting information during a descriptive research study because they
cover a wide area, gives freedom of expression and choice to the respondents and were free of
biasness. Pilot study was conducted in Savanna cement in order to test the questionnaire.
Questionnaires being data collection instruments were tested and re-tested in similar study
environmental conditions to ascertain their validity and reliability in terms of correctness,
fluency, flow and neatness.

29
3.6 Data collection procedure
Primary data was collected through administering a questionnaire. The researcher personally
administered the questionnaires. In distributing the questionnaire, the researcher applied drop
and pick later method where the respondents were given three days to complete the
questionnaires after which the filled-in questionnaires were collected. Every effort was used to
ensure that the quality of data collected is high and credible.
3.7 Testing of Instruments
3.7.1 Reliability
The internal consistency of the research instrument was assessed using Cronbach’s alpha
coefficient which is commonly used when there are multiple rating scale questions in a
survey/questionnaire that form a scale. The internal consistency Cronbach’s Alpha (α) ranges
from 0 to 1 and it is a reliability coefficient that reflects how well the measurements items
positively correlate to one another. In line with Nunnaly (1978) recommendation, only constructs
with cut off of 0.7 and greater was considered for further analysis in the study. To enhance the
reliability of the survey instrument for this study, a pilot study was conducted on one
organization that were not used in the final study then Cronbach’s Alpha coefficient was
calculated to establish internal consistency of the instrument.
3.7.2 Validity Tests
Validity was measured using the methodology proposed by Crocker et al (1986) which
calculates validity coefficients that identify what percentage of variance in the criterion variable
is accounted for by the testing measure, or predictor variable. The calculation of both reliability
and validity was done using the results of the pilot study. The aim is to get their feedback on the
clarity and adequacy of the questions in collecting the target information (Nunnaly, 1978). In the
current study pilot questionnaires were administered through drop and pick later method to one
cement manufacturing firm which were not included in the target sample. Their feedback was
used to improve the questionnaires and compute the reliability coefficient.

30
3.8 Data analysis and Presentation
The collected data was sorted out by removing raw data aiming at creating orderliness prior to
data analysis which forms the beginning of detecting, rectifying and sorting out any error which
may occur due to the mix ups of data collection (Obure, (2002). Data editing was done by
perusing completed data collection instruments (questionnaires). Collected data was coded and
edited as required and thereafter processed by the Statistical Packages for Social scientists
(SPSS). Data entry was done by keying of data as per the assigned codes and final checks made
for accuracy and completeness purposes. The SPSS (version 22) processor processed and
released a result which was expected to be qualitative in nature. According to Gray (2004)
qualitative data provides effective and rich descriptions of the study findings including
explanations demonstrating sequential flow of events. Collected and analyzed data was expected
to answer research study questions. The analysed data was presented in tables, figures and charts.
3.9 Ethical Consideration
Ethics are norms governing human conducts which have a significant impact on human welfare.
It involves making a judgment about right and wrong behavior. Bryman (2007) states that it is
the responsibility of the researcher to carefully assess the possibility of harm to research
participants, and the extent that it is possible; the possibility of harm should be minimized. The
researcher recognized that the issue under study is sensitive because it involved the core business
of the organization. Therefore, there was need to protect the identity of the respondents as much
as possible. This meant that the questionnaires never required the respondent’s names or details
that may reveal their identity. The researcher also adhered to strict confidentiality of the
information gathered and assured the respondents that the research was meant for academic
purposes only.

31
CHAPTER FOUR
DATA ANALYSIS, INTERPRETATION AND DISCUSSION
4.1 Introduction
The broad objective of the study was to assess risk factors contributing to occupational injuries
among cement workers with specific reference to East African Portland Cement Company. The
first section gives demographic information of the respondents which helps to depict the
characteristics of respondents in East African Portland Cement Company. The second section
deals with analysis of data on each of the three objectives based on descriptive statistics.
4.2 Response Rate
The study targeted respondents from East African Portland Cement Company. Questionnaires
were sent to 192 respondents drawn from various departments. Table 4.1 shows the response
rate.
Table 4.1: Response Rate
S/No Department Questionnaires
Administered
Questionnaires
Returned
Percentage
1 Administration 27 20 74.07
2 Mining 28 19 67.86
3 Electrical 27 17 62.96
4 Mechanical 28 19 67.86
5 Process 28 16 57.14
6 Packing plant 27 17 62.96
7 Dispatch & Logistic 27 17 62.96
Total 192 125 65.10
Source: Survey Data, (2017)

32
Out of 192 questionnaires administered, 125 were filled and returned representing a response rate
of 65.10%.This response rates was considered adequate for analysis. According to Mugenda and
Mugenda (2003), a sample representation of 10% to 30% is acceptable for such studies.
4.3 Demographic Information
In order to achieve the main purpose of this study, the researcher found it useful to find out the
demographic information of the respondents. The demographic information of the respondents
included: gender, age, work experience, level of education and specialty/line of duty.
4.3.1 Gender
The research sought to find out the gender of the respondents. In this study the respondents
sampled were expected to comprise both male and female employees in East African Portland
Cement Company. As such, the study required the respondents to indicate their gender by ticking
on the spaces provided in the questionnaire. Figure 4.2 shows the distribution of the respondents
by gender.
56.00%
44.00%
Male
Female
Figure 4.1 Gender
Source: Survey Data, (2017)
From the study, 56% of the employees involved in the study comprised of males while 44% of
them were females. The findings show that the firm studied had both male and female staff. The
findings imply that the views expressed in these findings are gender responsive and can be taken
as representative of the opinions of both genders as regards to the study.
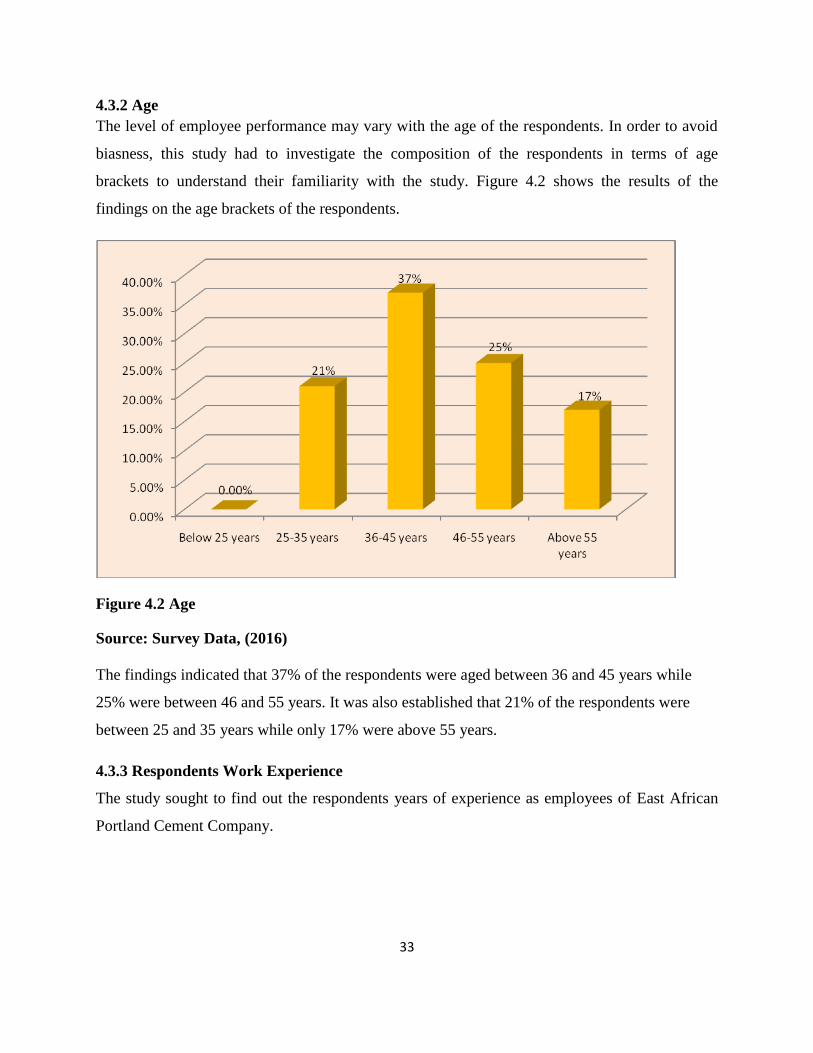
33
4.3.2 Age
The level of employee performance may vary with the age of the respondents. In order to avoid
biasness, this study had to investigate the composition of the respondents in terms of age
brackets to understand their familiarity with the study. Figure 4.2 shows the results of the
findings on the age brackets of the respondents.
Figure 4.2 Age
Source: Survey Data, (2016)
The findings indicated that 37% of the respondents were aged between 36 and 45 years while
25% were between 46 and 55 years. It was also established that 21% of the respondents were
between 25 and 35 years while only 17% were above 55 years.
4.3.3 Respondents Work Experience
The study sought to find out the respondents years of experience as employees of East African
Portland Cement Company.

34
0.00%10.00%20.00%30.00%40.00%50.00%
1 to 4 5 to 7 8 to 10 >10
17.78%
42.22%
22.22% 17.78%
Years
Figure 4.3 Work Experience
Source: Survey Data, (2017)
According to the analysis of findings, majority (42.22%) of the respondents had worked in the
company for 5 to 10 years followed by 22% who had worked for a period of 8 to 10 years. It was
also noted that 17.78% of the respondents had worked for Less than one year and a similar
percentage had worked for over 10 years. Figure 4.3 shows the summary of the findings.
4.3.4 Education
The study sought to find out the education level of the respondents findings are shown in figure
4.4.
0%
10%
20%
30%
40%
Secondary/primary College University first degree
31%40%
29%
Figure 4.4: Education
Source: Survey Data, (2017)

35
The findings indicate that 40% of the respondents had college level of education while 31% had
attained secondary level of education. Further analysis indicated that 29% of the respondents had
attained university education with at least undergraduate degree.
4.4 The Causes of Accidents and Injuries among Workers
The respondents were asked to indicate whether they have been involved in an accident in the
last one year. Figure 4.5 shows the summary of the findings.
Figure 4.4: Involved in an accident
Source: Survey Data, (2017)
It was established that only 32% of the respondents had been involved in accident while 68% had
not. This implies that occupational injuries are minimal in East Africa Portland Cement
Company.
In this study the respondent indicated that most common agent stated as cause was machinery,
splintering objects, falls, hot substances and being hit by falling objects. The respondents were
also presented with statements concerning the causes of accidents and injuries among cement
workers to rate on a five point likert scale. The risk factors were categorized into human,
environmental and mechanical factors. Findings are presented in table 4.2

36
Table 4.2: Human factors
Source: Survey Data, (2017)
According to the analysis of the findings, the respondents indicated that failure to follow safety
rules caused injuries as shown by a mean of 4.2 and a standard deviation of 0.8. Other humian
factors that caused occupational injuries as indicated by the respondents include; improper
posture (M=3.9, SD=0.8), lack of attention (M=3.7, SD=0.9) and improper lifting (M=3.6,
SD=0.6). Table 4.2 shows the findings of the study.
In seeking to find out the environmental factors causing occupational injuries, the respondents
indicated that broken floors was a common factor causing injuries as shown by a mean of 4.2 and
a standard deviation of 0.8. The other factors leading to injuries that was cited by the
respondents included misplaced objects (M=4.0,SD=0.8) and harzadous chemicals
(M=4.0,SD=0.9). The other factors shown in table 4.3 are; slippery floors, poor
illumination/lighting, source of electricity and fire.
Human factors Mean SD
Failure to follow safety rules 4.2 0.8
Lack of attention 3.7 0.9
Improper posture 3.9 0.8
Improper lifting 3.6 0.6
Environmental factors Mean SD
Broken floors 4.2 0.8
Misplaced objects 4.0 0.7
Slippery floors 3.9 0.6
Hazardous chemicals 4.0 0.9
Poor illumination/lighting 3.8 0.7
Source of electricity
3.8 0.8
Fire 3.6 0.6

37
Table 4.3: Environmental factors
Source: Survey Data, (2017)
The study also sought to find out the mechanical factors causing occupational injuries among
cement workers. According to the findings, rapidly moving parts caused occupational injuries as
supported by a mean of 4.5 and a standard deviation of 0.7. It was also established that heavy
tools caused occupation injuries as shown by a mean of 4.2 and a standard deviation of 0.9.
Further findings indicated that unsafe tools also caused occupational injuries as shown by a mean
of 4.0 and a standard deviation of 0.9. Table 4.4 shows the findings of the study.
Table 4.4: Mechanical factors
Source: Survey Data, (2017)
4.5 Risk Factors of Occupational Injuries among Workers
The respondents were asked to indicate whether they had been trained on OHS risk factors
within their working area where it was established that all the workers in East African Portland
Cement.
In all the cement production process, there are hazards in the cement production phases such as
quarrying, crushing, clinker production, milling processes at raw mill, cement milling and coal
milling, material transport and storage. The following table shows the risk factors and possible
prevention measures in the cement manufacturing process.
Mechanical factors
Mean SD
Unsafe tools 4.0 0.9
Rapidly moving parts 4.5 0.7
Heavy tools
4.2 0.9

38
Table 4.5: OHS risk factors and prevention measures
Area OHS risk factor Prevention measures
QUARRYING Drilling
• Fall from height
• Hurling of material
Movement of heavy goods
vehicles
• The collapse of a floor level
• Mechanical movement of the
drill
• Exposure to noise and dust
Charging and ignition
• Inappropriate use of
explosives
• Fall from height
• The collapse of a floor level
• Hurling of material
• Exposure to noise and dust
and vibration
• Movement of heavy goods
vehicles
• The moving parts of the bore
holing machinery
• Falls from height
• Material falling from height
• Crushing of quarry table
• Hurling of material
• Presence of dust and noise
• Movement of earth moving
equipment
• Job safety analysis and work
permit
• Isolation of the charging and
ignition area
• Use of minimum explosives
• Authorised person in charge
• Pre-approved explosion plan
• Safety signage
• Safety warnings
• No smoking
RAW MATERIAL
STORAGE
Airborne dust Use of the stacker and
reclaimer system to collect
dust
• Routine cleaning of the area
• Good housekeeping
RAW MATERIAL
MILLS,
HOMOGENISATIO
N AND RAW
MATERIAL
STORAGE
• Back firing of the furnace
• Noise
• Dust
• Absence of protective barrier
• Absence of guards
• Electrocution
• Hot material
• Use of fuel safety device
(fusible link)
• Use of a tag in / tag out
system during
maintenance
• Use of a closed circuit
surveillance system
• Use of a dust suction system
THE CLINKER
PRODUCTION
PROCESS
PREHEATING OF
MATERIAL
• High temperatures
•Superheated material
particles
• Use of a safe system of work
– no accidental operation (tag
in/ tag out procedures)

39
CEMENT AND
RAW MATERIAL
STORAGE SILO
CLEANING
• Noise during the cleaning
operation
• Falling material from the silo
walls
• Dusty environment
• Operator getting overcome
by material at the base of the
silo
• Use of dust suction system
• Floor preparation
• Use of safety signage
• Use of tag in/ tag out
procedures
• Use of blind flanges
• Continual supervision
• Provision of adequate
lighting
• Provision of sufficient
ventilation using bag
filters
PACKAGING • Dusty environment
• Falling material
• Moving parts of packaging
machinery
• Movement of heavy trucks
• Existence of third parties
(truck drivers) in the area
• Use of a dust suction system
• Use of appropriate PPEs
• Training of personnel
• Adequate machine guarding
• Use of safety signage
LOADING AND
UNLOADING
• Overhead loads
• Use of lifting equipment
• Falling of loads
• Dusty environment
• Use of authorised personnel
• Provision of appropriate
maintenance to the
lifting equipment
• Use of load limiting devices
• Routine cleaning of the area
FUEL STORAGE • Use of naked flames near
fuel
storage
• The creation of hot spots
during
maintenance activities
• The hurling of hot material
in the
fuel area
• Electrical discharges
(Thunderbolt,
electrostatic charges during
refuelling , short circuits)
• Existence of a work permit
system for working
near the fuel storage
• Maintenance and control of
the anti-discharge
system
LIFTING
EQUIPMENT
• Crush of the load or the
lifting
mechanism onto operatives
• Use of authorised and trained
personnel
• Existence and compliance

40
• Fall of the load to be lifted
due
to the failure of the lifting gear
• Insufficient or inappropriate
securing of the load
• Tilting of the load during its
transportation
• Crashing of the load on the
building
• Electrocution as a result of
lifting mechanism contacting
o/h
lines
with work
instructions
• Safe operation of the
stopping mechanism,
the breaks and the lifting lines
• Check on a routine basis the
hook
mechanism
• Always secure the load using
the approved
straps
• Always avoid the lifting of
loads overhead
from working operatives.
Source: Survey Data, (2017)
4.6 Challenges Facing Control of Accidents
The respondents indicate that there were challenges in the control of accidents in cement
manufacturing process. Some of the challenges include: poor supervision of the workers at
workplace; risky behavior of workers at the factory; inadequate safety education, illustration and
proper use of safety harnesses; inadequate provision of safety harnesses; employment of
incompetent safety officers by the sub-contractors; the attitude of the management towards
workers employed by subcontractors in respect of their health and safety at the factory premises;
improper use of PPE by the workers; provision of defective ppe by the sub-contractors to the
workers and improper use of workplace equipment (e.g., steel ladders) by the workers.
A sequence of events has to occur before a hazard will cause harm to a person. Understanding
the sequence of events provides valuable information about how to control the risk from the
hazard. If one or more of the events in the sequence can be stopped or changed, the overall risk
may be eliminated entirely or reduced. Duty-holders are required to ensure health and safety by
controlling risks. Risks must be controlled by eliminating them so far as reasonably practicable
or, if this is not possible, reducing the risks that remain so far as reasonably practicable.

41
CHAPTER FIVE
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
5.1 Introduction
This chapter summarizes the study and makes conclusion based on the findings. The
recommendations of the study and areas for further research are also presented.
5.2 Summary of Findings
The respondents were asked to indicate whether they have been involved in an accident in the
last one year. It was established that only a few respondents had been involved in accident while
majority had not. This implies that occupational injuries are minimal in East Africa Portland
Cement Company.
In this study the respondent indicated that most common agent stated as cause was machinery,
splintering objects, falls, hot substances and being hit by falling objects. The respondents were
also presented with statements concerning the causes of accidents and injuries among cement
workers to rate on a five point likert scale. The risk factors were categorized into human,
environmental and mechanical factors.
According to the analysis of the findings, the respondents indicated that failure to follow safety
rules caused injuries. Other human factors that caused occupational injuries as indicated by the
respondents include; improper posture, lack of attention and improper lifting. In seeking to find
out the environmental factors causing occupational injuries, the respondents indicated that
broken floors was a common factor causing injuries. The other factors leading to an injury that
was cited by the respondents included misplaced objects. The other factors were; slippery floors,
poor illumination/lighting, source of electricity and fire.
The study also sought to find out the mechanical factors causing occupational injuries among
cement workers. According to the findings, rapidly moving parts caused occupational injuries. It
was also established that heavy tools caused occupation. Further findings indicated that unsafe
tools also caused occupational injuries.

42
The respondents were asked to indicate whether they had been trained on OHS risk factors
within their working area where it was established that all the workers in East African Portland
Cement. In all the cement production process, there are hazards in the cement production phases
such as quarrying, crushing, clinker production, milling processes at raw mill, cement milling
and coal milling, material transport and storage.
The respondents indicate that there were challenges in the control of accidents in cement
manufacturing process. Some of the challenges include: poor supervision of the workers at
workplace; risky behavior of workers at the factory; inadequate safety education, illustration and
proper use of safety harnesses; inadequate provision of safety harnesses; employment of
incompetent safety officers by the sub-contractors; the attitude of the management towards
workers employed by subcontractors in respect of their H&S at the factory premises; improper
use of PPE by the workers; provision of defective PPE by the sub-contractors to the workers and
improper use of workplace equipment (e.g., steel ladders) by the workers.
5.3 Conclusions
Workplaces can be dangerous; there are many hazards that have the potential to kill, injure or
cause ill health or disease. Protecting the health and safety of people in the workplace is a
community expectation that makes good business sense. Workplace incidents can have a
dramatic impact on people’s lives (people in the workplace, families and friends), and they can
have significant financial impacts on organizations through loss of skilled staff and lost
production of goods or services.
A safe and healthy workplace and compliance with the law does not happen by chance or
guesswork. Good health and safety is all about eliminating and controlling hazards and risks.
This is best achieved by a proper consideration of the sources of harm and what can be done to
prevent the harm from occurring. The health and safety performance of the cement industry as a
whole is lagging behind that of other, more proactive, sectors of manufacturing industry. Within
the sector, there is a wide range of performances. There is a particular need for the industry to
encourage and help those companies and plants that are significantly under-achieving to raise
their safety standards to ensure a sustainable industry that meets social and employment
expectations.

43
5.4 Recommendations
Based on the findings, the followings are recommended:
Occupational health and safety should be included in any training course to newly-hired workers.
Workers should be adequately informed about the specific hazards associated with their jobs and
the safety measures that they should follow to protect themselves. The management should make
effort to encourage and supervise the use of personal protective equipment by the cement
workers.
Every level of employee, from the most senior executive to the newly hired worker, clearly
understands what is expected. There are specific, demanding standards for each person in all
major work activities. Without adequate standards, there can be no meaningful measurement,
evaluation, correction or commendation of performance.
The company should make safety a line management responsibility and accountability. Safety is
better served when it is so ingrained into every activity that it becomes impossible to ignore it.
There is little talk of doing things the safe way and more talk of doing things the right way.
Safety is equal to all considerations of production, costs, and quality. This is reflected in
performance appraisals, salary adjustments, and promotions.
There is need to incorporate safety into the business process as an operational strategy. Leaders
around the world increasingly recognize that a well-managed safety system provides an
operational strategy to improve overall management. But in recent years a significant number of
major organizationsF have discovered that applying the tools and techniques of good safety
management gives them not only reduced injuries and illnesses but also measurable
improvements in efficiency, quality and productivity.
The company should use proactive health and safety measurements. Leading management
consultants have emphasized: “If you can’t measure it, you can’t manage it; if you can’t manage
it, you can’t improve it”. The heart of safety management is measuring performance in
quantifiable, objective terms. Leading companies constantly assess their process to determine if
they are adequately controlling risk. Scaling the heights of health and safety excellence requires

44
the same leadership skills as attaining excellence in any other area. Health and safety
performance is a reflection of corporate culture and senior management influences that culture
more than any other group. As in other areas, executive leadership will dictate the kind of safety
performance it insists on.
5.5 Suggestions for Further Research
This study sought to assess the risk factors contributing to occupational injuries among cement
workers in an attempt to bridge the gap in knowledge that existed. Although the study attained
these objectives, it mainly focused on East African Portland Cement Company only. There is
need to replicate the study looking at the wider view to include other cement manufacturing
company in Kenya.

45
REFERENCES
Ahmed, Hafiz Omer, & Abdullah, A. a. (2012). Dust exposure and respiratory symptoms among
cement factory workers in the United Arab Emirates. Industrial health, 50(3), 214–
22. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22453209 (28/06/2016)
Al-Neaimi, Y. I., Gomes, J., & Lloyd, O. L. (2001). Respiratory illnesses and ventilator function
among workers at a cement factory in a rapidly developing country. Occupational
medicine (Oxford, England), 51(6), 367–73.
Amandus, H. E. (1986). Mortality from stomach cancer in United States cement plant and quarry
workers, 1950-80. British journal of industrial medicine, 43(8), 526–8.
Badri, O. A. El, & Saeed, A. M. (2008). Effect of exposure to cement dust on lung function of
workers at Atbara Cement Factory. Kharoum Medical Journal, 01(02), 81–84.
Buckley, J. (n.d.). A History of Cement. Retrieved May 26, 2013, from
http://www.rumford.com/articlemortar.html (28/06/2016)
Koh, S. B. (2012). Adverse health outcomes in residents exposed to cement dust. Toxicology and
Environmental Health Sciences, 3(4), 239–244. doi:10.1007/s13530-011-0101-6
Cowen, H. (1988). The manufacture of Portland cement., 1–8. Retrieved from
https://mospace.library.umsystem.edu/xmlui/handle/10355/17830 (21/05/2016)
El-Dine, H. M. G., Sadek, R. R., Zayet, H. H., & Mahfouz, E. M. (2004). Respiratory problems
among workers in El-Minia cement factory (p. 197).
Guo, Y. L., Wang, B. J., Yeh, K. C., Wang, J. C., Kao, H. H., Wang, M. T., … Chen, C. J.
(1999). Dermatoses in cement workers in southern Taiwan. Contact dermatitis,
40(1), 1–7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9928797
(28/06/2016)
Iqbal, S., Iqbal, M., Taufiq, Z. M., & Ahmed, S. M. (2010). Identification of Occupational Injury
among the Workers of Selected Cement Industries in Bangladesh-A Case Study.
Journal of Chemical …, C(1), 22–28.
Johansson, L., Albin, M., Jakobsson, K., & Mikoczy, Z. (2010). Histological type of lung
carcinoma in asbestos cement workers and matched controls. British journal of
industrial medicine, 49(9), 626–30.

46
Kakooei, H., Gholami, A., Ghasemkhani, M., & Hosseini, M. (2011). Dust Exposure and
Respiratory Health Effects in Cement Production. Acta Medica Iranica, 50(2), 0–4.
Kirenga, A.P. (2004). African Newsletter on Occupational health and Safety. Occupational
injuries and diseases. 20-30
Koh, D.-H., Kim, T.-W., Jang, S., & Ryu, H.-W. (2013). Dust exposure and the risk of cancer in
cement industry workers in Korea. American journal of industrial medicine, 56(3),
276–81.
Kombo and Tromp (2009) Proposal and Thesis Writing, published by Pauline publications,
printed by Don bosco Printing Press, Nairobi.
Makhonge, P.W. (2005). African Newsletter on Occupational health and Safety.Good practices
in occupational health and safety.18-24
Marlowe, I. and Mansfield, D. (2002). Environment, Health and Safety Performance
Improvement (p. 58).
Mathias, C. G. T. (1990). Prevention of occupational contact dermatitis. Journal of the American
Academy of Dermatology, 23(4), 742–748.
Meo, Sultan A. (2004). Health Hazards of Cement Dust. Saudi Medical Journal, 29(9), 1–20.
Merenu, I. A., Mojiminiyi, F. B. O., Njoku, C. H., & Ibrahim, M. T. O. (2007). The Effect of
Chronic Cement Dust Exposure on Lung Function of Cement Factory Workers in
Sokoto , Nigeria. African Journal of Biomedical Research, 10(May), 139–143.
Mndeme, F. G and Mkoma, S. L. (2012). ASSESSMENT OF WORK ZONE NOISE LEVELS
AT A CEMENT FACTORY IN TANGA, TANZANIA. Ethiopian Journal Of
Environmental Studies and Management, 5(3), 225–231.
Mugenda and Mugenda (2003) Research methods Qualitative and Quantitative approaches,
published by Acts press, printed by Laba Graphics Limited, Nairobi.
Neuman, W. L. (2000) Social Research Methods: Qualitative and Quantitative Approaches.
Fourth Edition. Boston.
Obure M.J (2002), Handbook on Data Analysis Using SPSS, Nairobi, M & O Data Experts
Training and Consultants, Nairobi.

47
Oleru, U. G. (1984). Pulmonary Function and symptoms of Nigerian workers exposed to cement
dust. Environmental Res.
OSHA, (2007). Occupational Safety and Health Act No 15 of 2007. An Act of parliament of the
government of Kenya.
Pournourmohammadi, S., Khazaeli, P., Eslamizad, S., Tajvar, a, Mohammadirad, a, &
Abdollahi, M. (2008). Study on the oxidative stress status among cement plant
workers. Human & experimental toxicology, 27(6), 463–9.
Smailyte, G., Kurtinaitis, J., & Andersen, A. (2004). Mortality and cancer incidence among
Lithuanian cement producing workers. Occupational and Environmental Medicine,
61(6), 529–534.
Ribeiro, F. (2002). [The work process and occupational health risks in a cement factory].
Cadernos de saúde pública, 18(5), 1243–50.
Smailyte, G., Kurtinaitis, J., & Andersen, A. (2004). Mortality and cancer incidence among
Lithuanian cement producing workers. Occupational and Environmental Medicine,
61(6), 529–534.
Uter, W., Ruhl, R., Pfahlberg, A., Geier, J., Aschnuch, A., & Gefeller, O. (2004). Contact
Allergy in Construction Workers: Results of a Multifactorial Analysis. Annals of
Occupational Hygiene, 48(1), 21–27.
Winder, C., & Carmody, M. (2002). The dermal toxicity of cement. Toxicology and Industrial
Health, 18(7), 321–331. doi:10.1191/0748233702th159oa
Zeleke, Z. (2011). Respiratory Health among Cement Workers in Ethiopia (p. 71).

48
APPENDIX 1: COVER LETTER
Caroline C. Boinet
Email: [email protected]
Mobile: 0722550725
28th June 2015
Dear Sir/Madam,
RE: DATA COLLECTION
Am post graduate student at the Jomo Kenyatta University of Agriculture and Technology
undertaking a post graduate diploma in Occupational Safety and Health. One of my academic
outputs before graduating is a research project and for this I have taken a topic on “Assessing the
risk factors contributing to occupational injuries among cement workers: A case of East
African Portland Cement Company”
You have been selected to form part of the study. This is to kindly request you to assist me in
collecting data by responding to the Questionnaire. The information you provide will be used
strictly for academic purpose and will be treated with utmost confidence. A copy of the final
report will be available to you upon request. Your assistance will be highly appreciated.
Yours sincerely
Caroline C. Boinet

49
APPENDIX 2: QUESTIONNAIRE
Jomo Kenyatta University of Agriculture and Technology
Department of Environmental and Energy Technology
ASSESSING THE RISK FACTORS CONTRIBUTING TO OCCUPATIONAL INJURIES
AMONG CEMENT WORKERS: A CASE STUDY OF EAST AFRICAN PORTLAND
CEMENT COMPANY
Please answer the questions by filling the space provided or ticking in the appropriate box.
A. Demographic Information
Date: _______________________
Questionnaire No.: ____________
Section: _____________________
a) Gender Male [ ] Female [ ]
b) Age
Below 25 yrs [ ] 26-30yrs [ ] 31-40 yrs [ ] Above 40 yrs [ ]
c) Working Experience In Cement Industry
3 – 5 years [ ] 6-10 years [ ] 11 – 15 years [ ] above 15 years [ ]
d) Highest level of Education
Primary [ ] Secondary [ ] College [ ] University [ ]
e) Specialty /line of duty
SECTION B:
1. THE CAUSES OF ACCIDENTS AND INJURIES AMONG WORKERS IN EAST
AFRICAN PORTLAND CEMENT COMPANY.
a) Have you been involved in an accident for the last one year? Yes [ ] No [ ],
b) If yes ,briefly describe what happened
_____________________________________________________________________

50
_____________________________________________________________________
_____________________________________________________________________
c) What was the root cause for the accident?
_____________________________________________________________________
_____________________________________________________________________
2. The statements below are concerned with the causes of accidents and injuries among
cement workers. Please tick the one that best describes your opinion. Use the following
Scale. 1- Strongly Disagree, 2- Disagree, 3- Neutral, 4- Agree 5- Strongly Agree.
Risk Factors Situation Scale
Human factors
Failure to follow safety rules
Lack of attention
Improper posture
Improper lifting
Environmental factors
Broken floors
Misplaced objects
Slippery floors
Hazardous chemicals
Poor illumination/lighting
Source of electricity
Fire
Other factors
Mechanical factors
Unsafe tools
Rapidly moving parts
Heavy tools
Others (please

51
3. RISK FACTORS OF OCCUPATIONAL INJURIES AMONG WORKERS IN
EAST AFRICAN PORTLAND CEMENT COMPANY.
a) Have you been trained on OHS risk factors within your work/working area?
Yes [ ] No [ ],
If yes briefly describe the training:
________________________________________________________________________
_______________________________________________________________________
b) Which are the OHS risks present in your area of work?
S/No OHS Risk Source Existing Mitigation Measures
1.
2.
3.
4.
5.
4. CHALLENGES FACING CONTROL OF ACCIDENTS
a) Do you face any challenges while addressing accident control programs / measures? Yes
[ ] No [ ], If yes state them briefly.
________________________________________________________________________
Suggest ways of improving the safety performance of the company through elimination
of OHS risks or accident prevention?
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Thank You for the Cooperation. Your inputs shall be treated with maximum
confidentiality and to be utilized for academic research purpose only
specify)……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………

52
APPENDIX 3: STUDY WORK PLAN
The study will be done during the day to for three weeks during which history taking, reviewing
of medical data and administering questionnaires, data analysis and interpretation will be done.
Activities Month 1 Month 2 Month 3 Month 4
Presentation of concept paper
Writing of proposal and
presentation.
Collection of data
Data Interpretation

53
APPENDIX 4: BUDGET
Below is the summary of the estimated budget required to successfully undertake the study.
ITEM ESTIMATES COST (KSHS)
Proposal development costs 9,000.00
Data collection costs 18,000.00
Data analysis costs 21,000.00
Production of the final document 22,000.00
TOTAL 70,000.00
The budget will cater for payment for data collection, travelling expenses, typing and printing
process, photocopies, questionnaires and letters to the respondents, final production and binding
of the project copies.