arthroscopic management of rotator cuff tears larissa 2016
TRANSCRIPT
ArthroscopicManagementofRotatorCuffTears
AaronVenouziouOrthopaedic SurgeonSt.Luke’sHospital
Thessaloniki

Anatomy
SupraspinatusAbduction
InfraspinatusExt.rotation
Teres minorExt.Rotation
SubscapularisInt.Rotationadduction
RotatorCuff
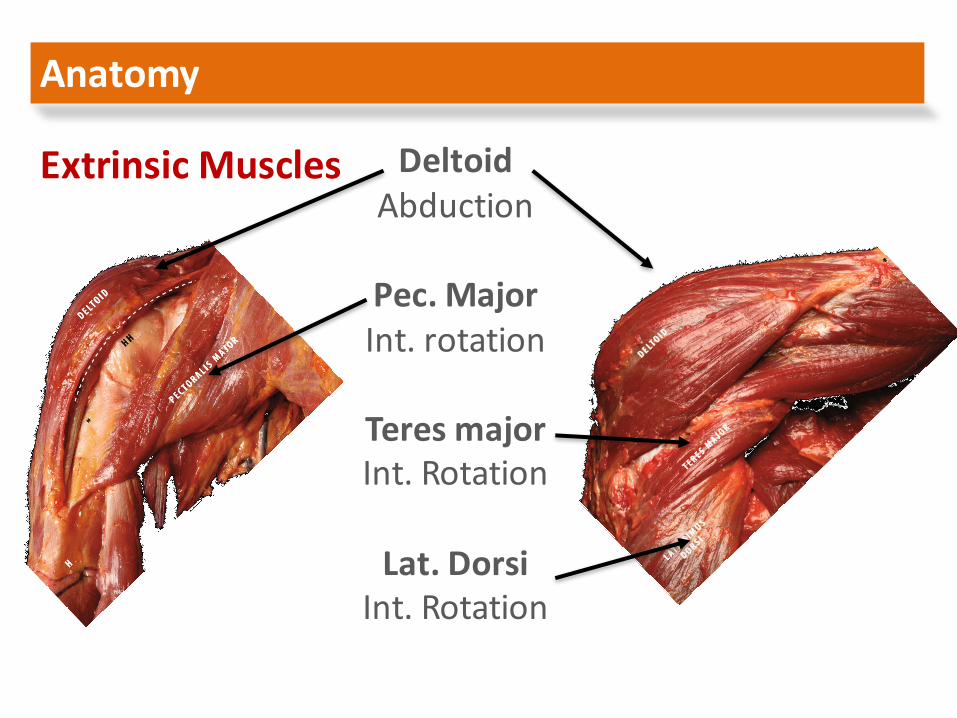
Anatomy
DeltoidAbduction
Pec.MajorInt.rotation
Teres majorInt.Rotation
Lat.DorsiInt.Rotation
ExtrinsicMuscles
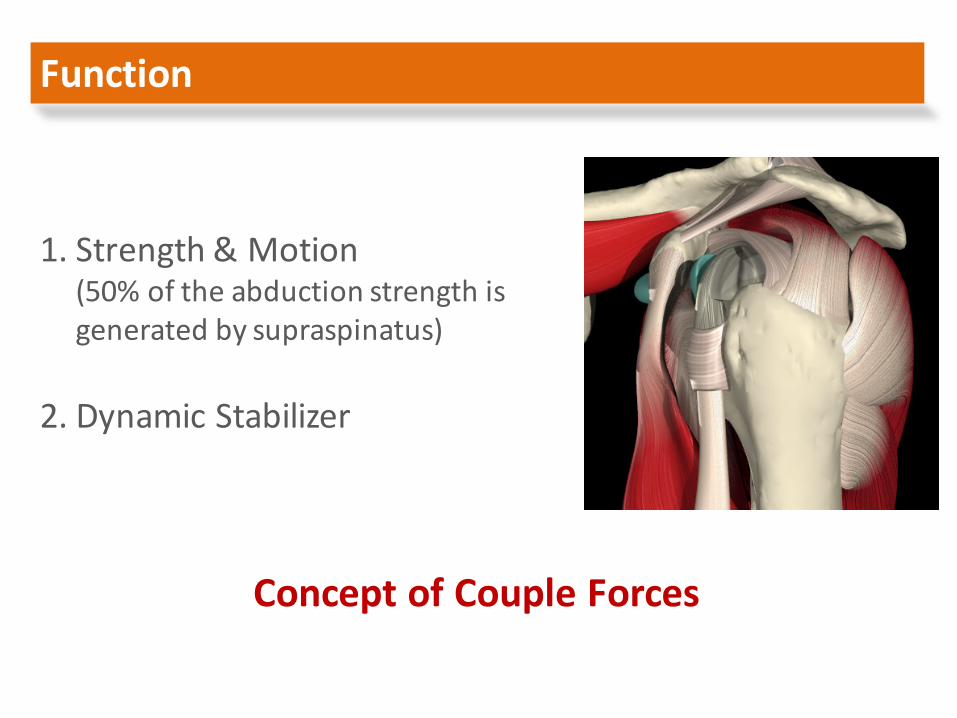
Function
1. Strength&Motion(50%oftheabductionstrengthisgeneratedbysupraspinatus)
2. DynamicStabilizer
ConceptofCoupleForces
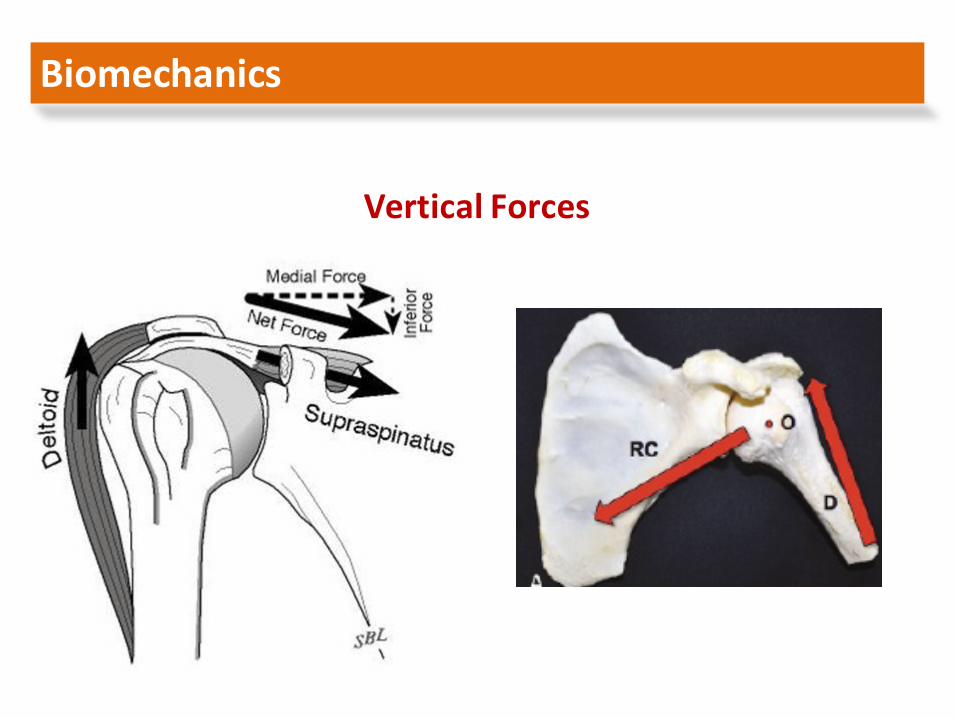
Biomechanics
VerticalForces
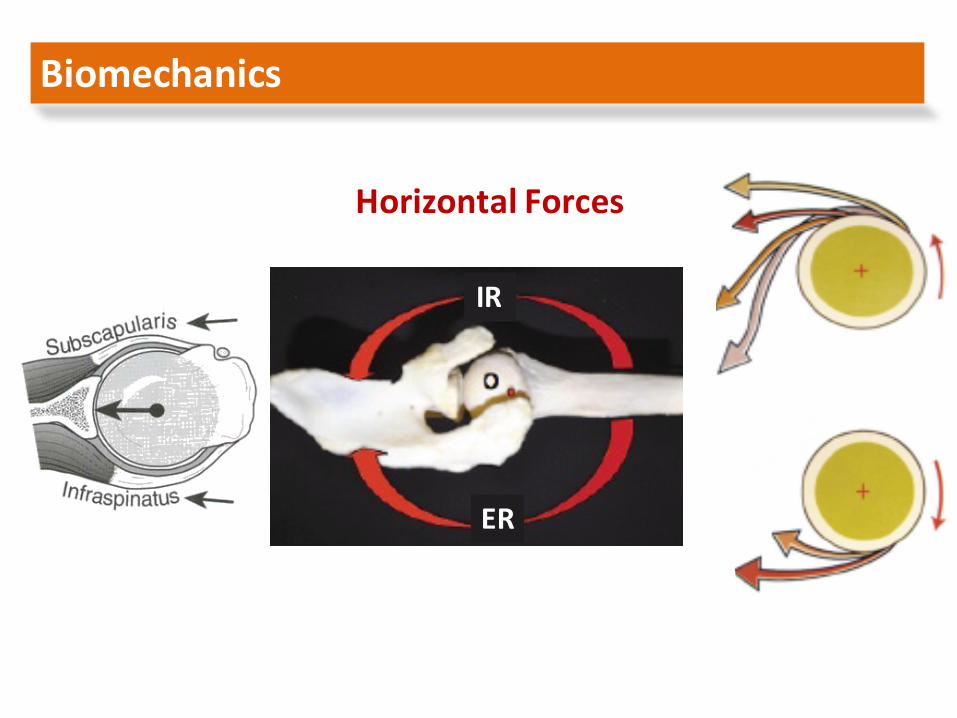
Biomechanics
HorizontalForces
IR
ER
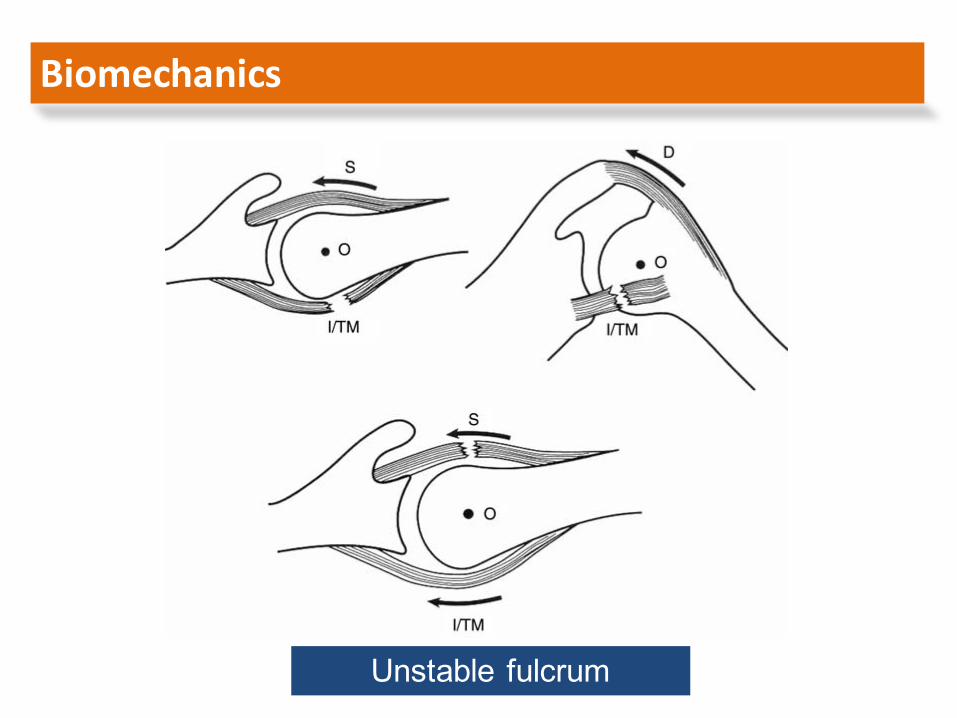
Biomechanics
HorizontalForces
Unstable fulcrum
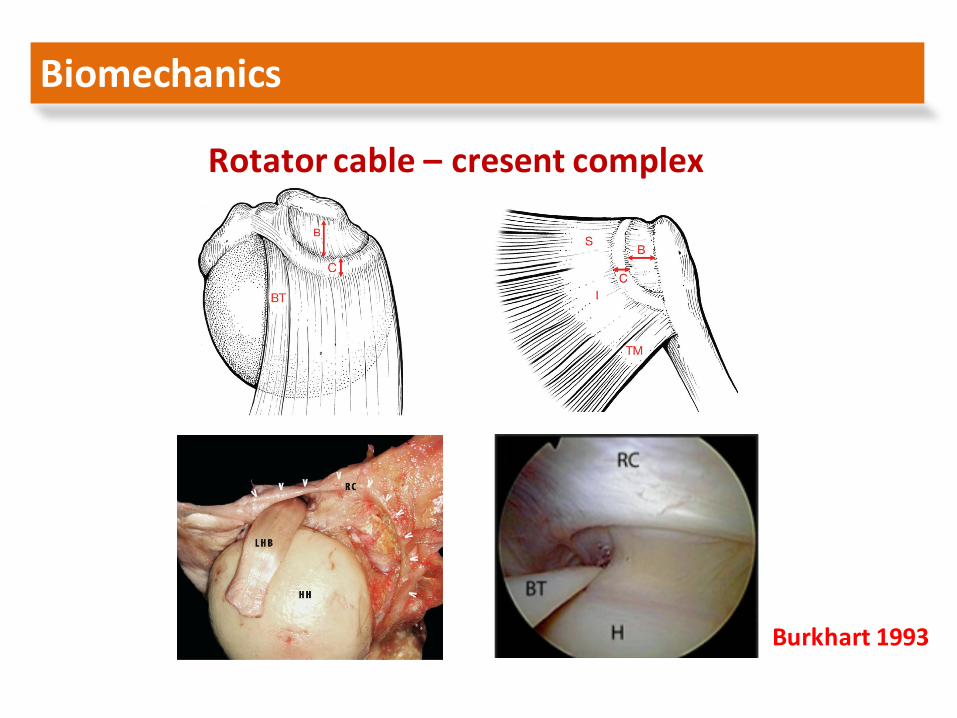
Biomechanics
Rotatorcable– cresent complex
Burkhart1993
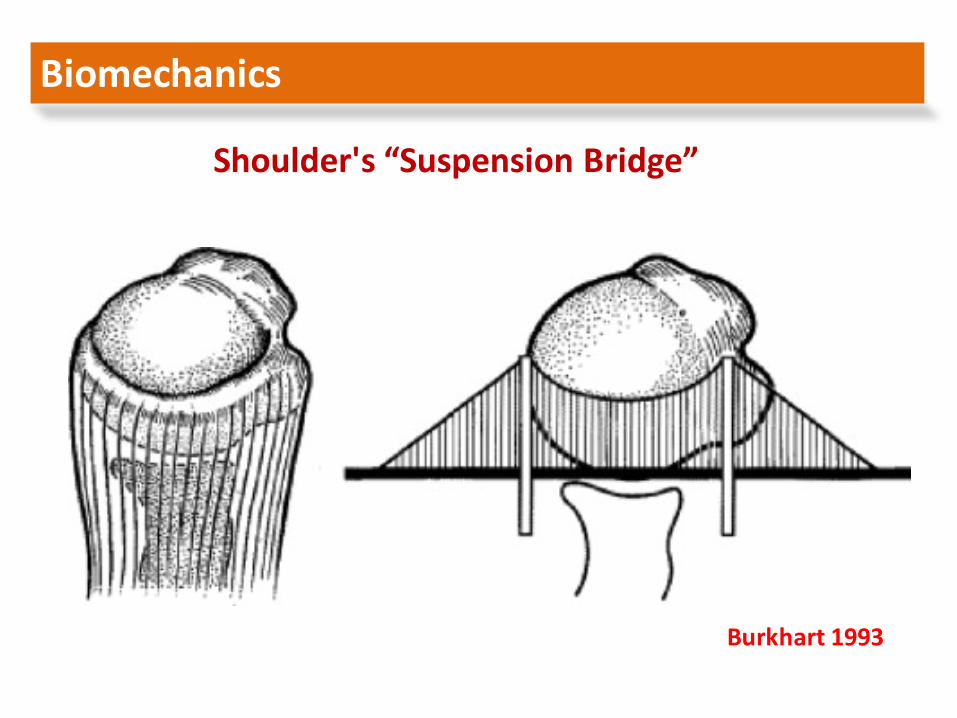
Biomechanics
Shoulder's“SuspensionBridge”
Burkhart1993
Rotator cuff disease is awidespectrum
ofclinical conditions,which range from
asymptomatic partial thickness tears to
symptomatic rotator cuff arthropathy
RotatorCuffDisease
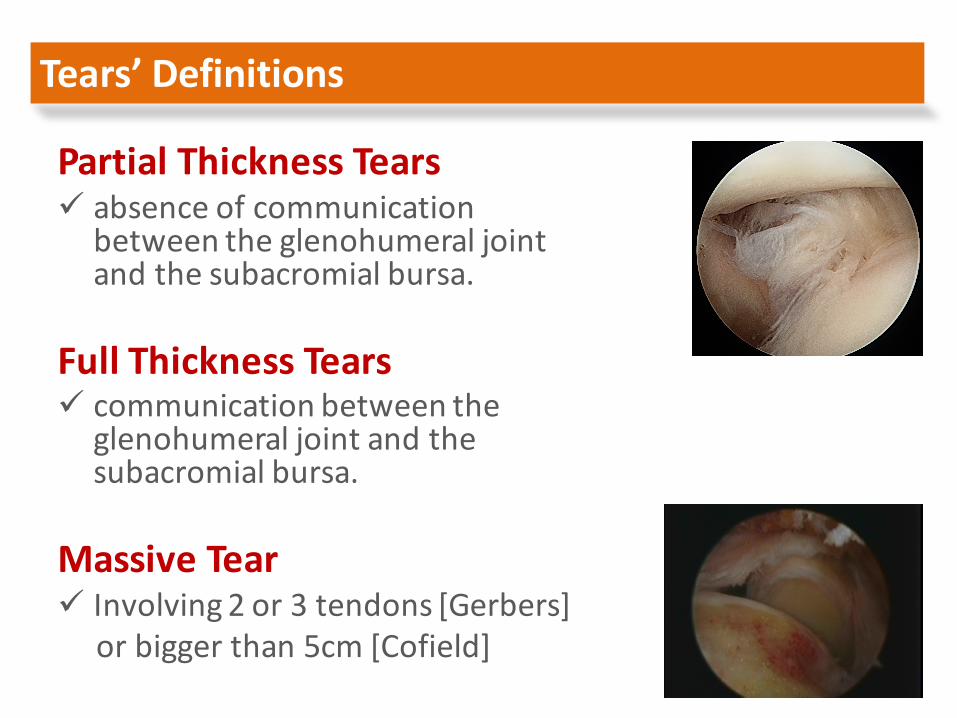
Tears’Definitions
PartialThicknessTearsü absenceofcommunication
betweentheglenohumeral jointandthesubacromial bursa.
FullThicknessTearsü communicationbetweenthe
glenohumeral jointandthesubacromial bursa.
MassiveTearü Involving2or3tendons[Gerbers]
orbiggerthan5cm[Cofield]
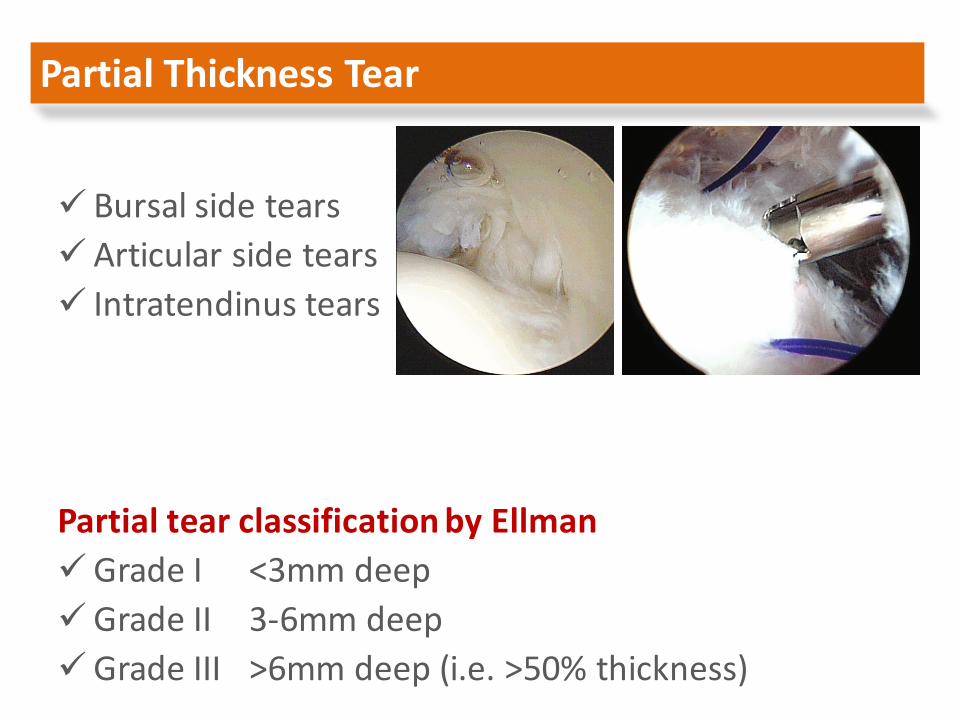
PartialThicknessTear
ü Bursalsidetearsü Articularsidetearsü Intratendinus tears
PartialtearclassificationbyEllmanüGradeI <3mmdeepüGradeII 3-6mmdeepüGradeIII >6mmdeep(i.e.>50%thickness)
Incidence
üRotatorCuffFrequency:30%ofpopulation
üSignificantcorrelationwithage
Sher JS,Arthroscopy1995
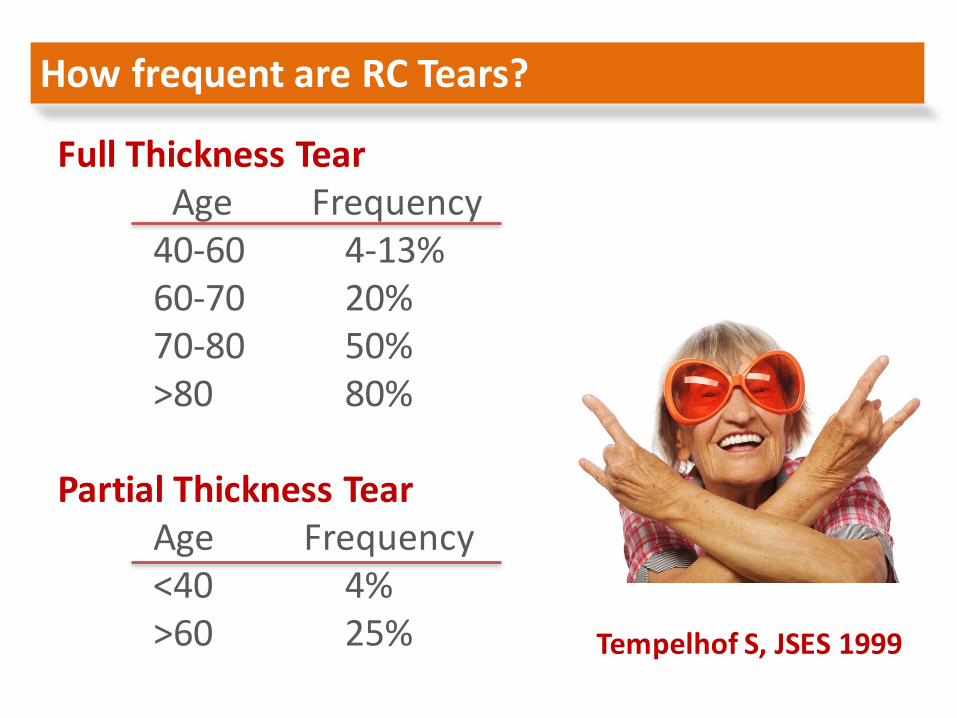
HowfrequentareRCTears?
FullThicknessTearAge Frequency40-60 4-13%60-70 20%70-80 50%>80 80%
PartialThicknessTearAge Frequency<40 4%>60 25% Tempelhof S,JSES1999
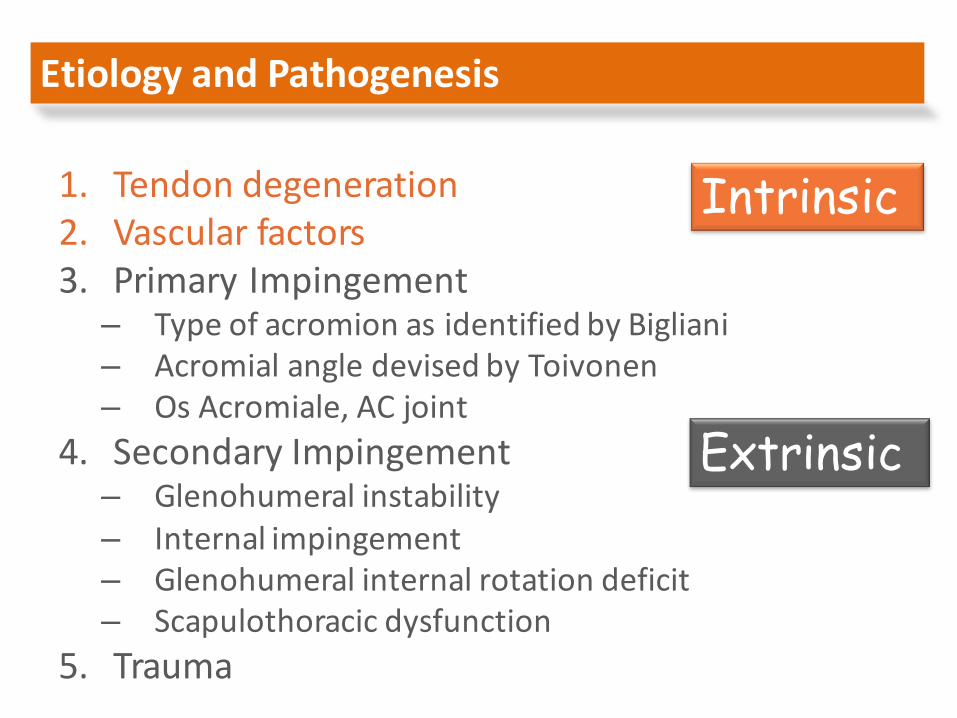
EtiologyandPathogenesis
1. Tendondegeneration2. Vascularfactors3. PrimaryImpingement
– TypeofacromionasidentifiedbyBigliani– AcromialangledevisedbyToivonen– Os Acromiale,ACjoint
4. SecondaryImpingement– Glenohumeral instability– Internalimpingement– Glenohumeral internalrotationdeficit– Scapulothoracic dysfunction
5. Trauma
Intrinsic
Extrinsic

– VascularSupply
TendonDegeneration
üagerelated
üchangeinproteoglycanandcollagencontent
“criticalzone”ofhypovasculararityatarticularsurface,anterioredge,ofsupraspinatus1cmproximaltoinsertion
Whichcamefirst?
Intrinsic Extrinsic or
ü type3acromionisacquired,notdevelopmentalasaresponsetotractionappliedviatheCAligament.
ü rotatorcuffabn occurwithoutchangesofacromion.
ü articular-sidedpathologyisdominant.
EvidenceAGAINSTsubacromial externalimpingement:
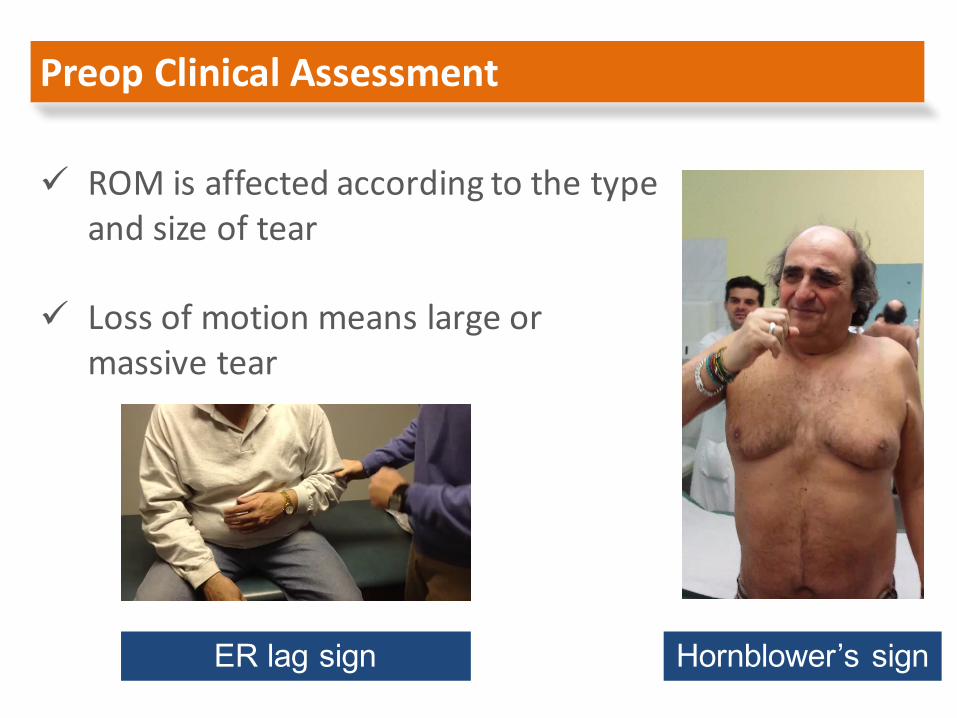
ü ROMisaffectedaccordingtothetypeandsizeoftear
ü Lossofmotionmeanslargeormassivetear
Preop ClinicalAssessment
ER lag sign Hornblower’s sign
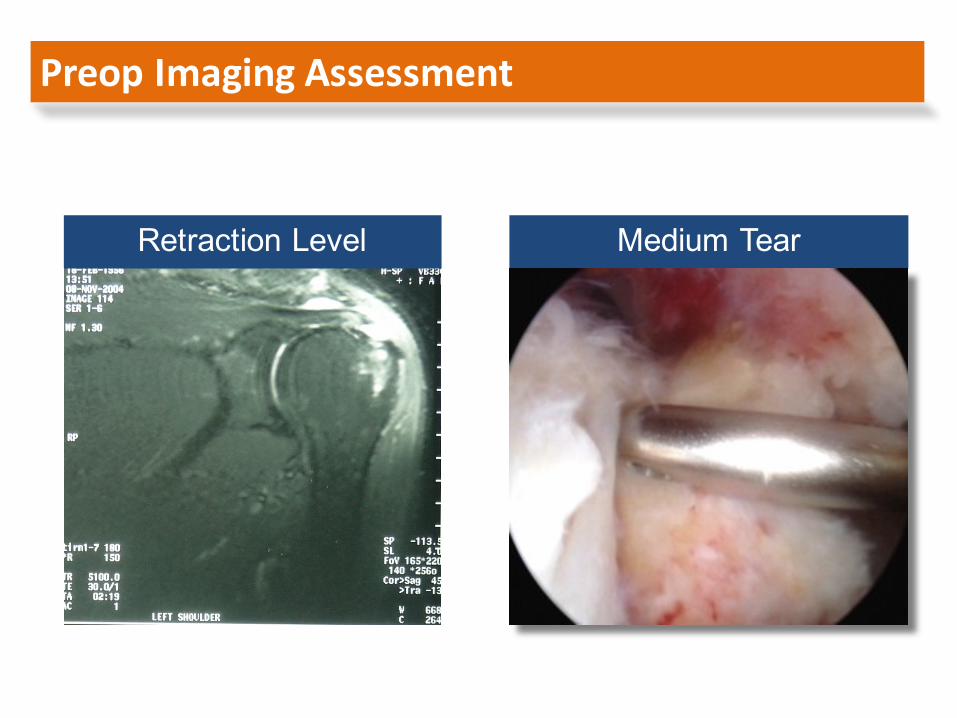
Preop ImagingAssessment
Retraction Level Medium Tear
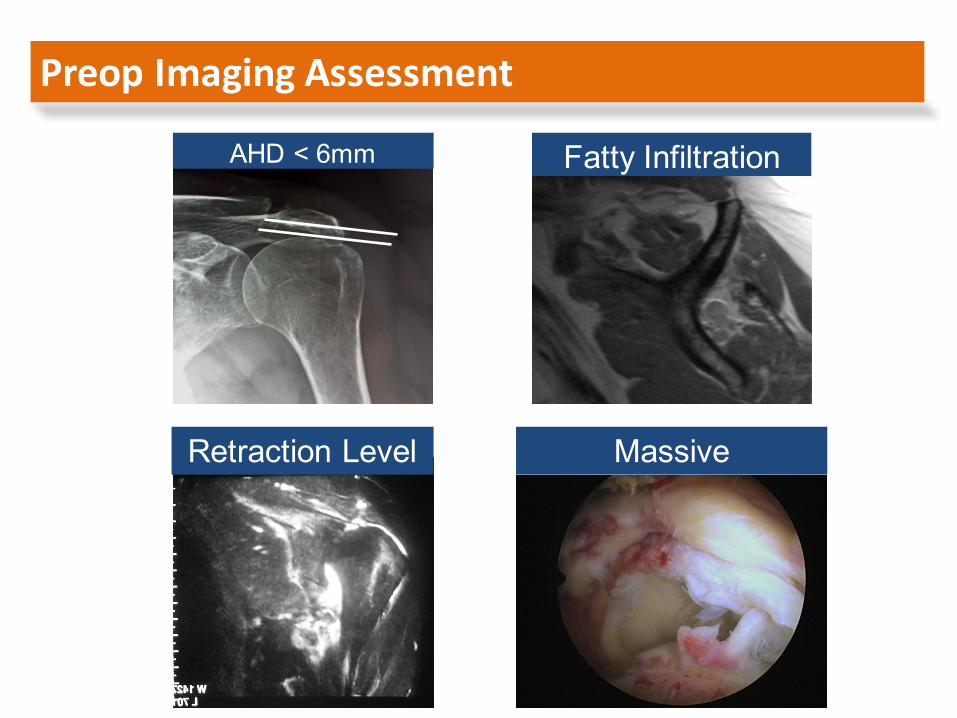
Preop ImagingAssessment
AHD < 6mm
Retraction Level
Fatty Infiltration
Massive
Non-Operative
ü 45-80%SatisfactoryResults
BUT
ü Symptomresolution???ü Tearprogression???ü Fattydegeneration???ü ProgressiontoRC
arthropathy ???
Operative
90% Good to Excellent Results at 10 years
[Iannotti Wolf]
Treatment

RisktoBenefitRatio
ü RotcufftearsDONOThealspontaneously
ü Tearrepairability
ü PatientProfile,Age,Symptoms
ü ThinkofSize,ElasticityandChronicity
ü Fattyinfiltrationisnotfullyreversible
Treatment
GroupingthePatients
GroupI: patientswithminimalriskofprogressiontoirreversiblechangestotherotatorcuff
GroupII: patientswithhighriskofprogression
GroupIII: patientswhohaveprogressedalready
[YamaguchiK.,2006,NiceShoulderCourse]
OperativeTreatment
GroupI
ü About50yearsoldwithtendinosis ordegenerative partialarticularsidetears
ü Theyrespondverywelltononoperativetreatment(about50-60%resolutionofthesymptoms)
ü Theriskofprogressionisverylowbuttheyneedobservation
OperativeTreatment
Non operative treatment - observation

GroupII
ü Youngerthan65yearswith– Smallormediumsizetears– Acutetearsofanysize– Tearswithrecentacutelossoffunction
ü Patientsnonresponsivetoconservativetx
ü Acutetearsoroverusetearsinathletes
OperativeTreatment
Early surgical repair to avoid irreversible changes
GroupIII
üOlderthan70years– withlargeormassivetearsand– irreversibledamagetotherotcuff
OperativeTreatment
They can benefit from rotator cuff repair, even a partial repair
Yamaguchi, JBJS 2006
Burkhart, Arthroscopy 2007
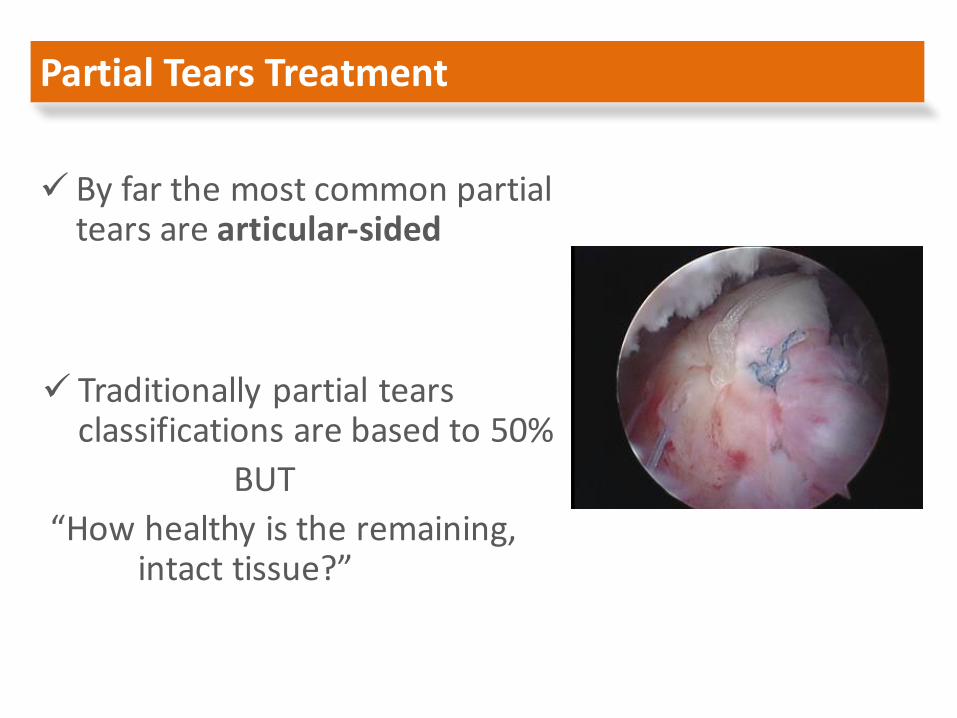
ü Byfarthemostcommonpartialtearsarearticular-sided
PartialTearsTreatment
ü Traditionallypartialtearsclassificationsarebasedto50%
BUT“Howhealthyistheremaining,
intacttissue?”
üDebridementü In-situRepairü Converttofullthickness,Debride,Repairü CONSERVATIVE
PartialTearsTreatment
ü Becausemosttearsaredegenerative,option3shouldbethebestformostcases
ü Traumaoryoungathletesarecandidatesforin-siturepair
Etiology makes the decision!!!
FullThicknessTears
ü Recognitionoftearpatternü Retractionandreleasesü RepairOptions:
Anchors: metallicorabsorbable
Typeofstitch: Mason-Allen,Mattresssutures,Horizontalmattress,Simplesutures
Restorationoffootprint: DoublerowSinglerow
ArthroscopicRepair
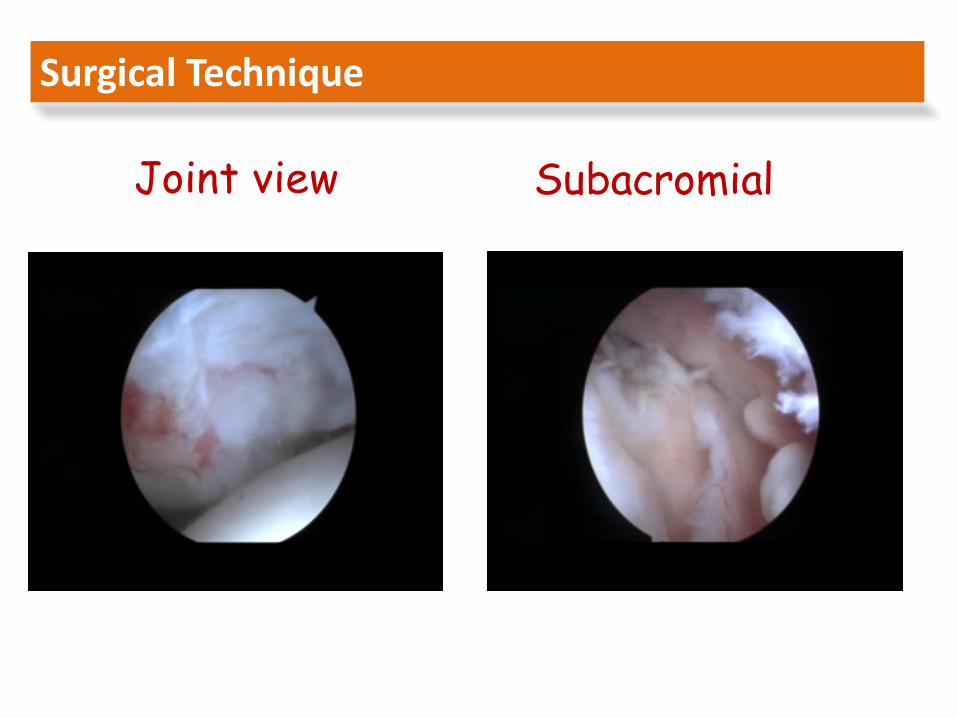
SurgicalTechnique
Joint view Subacromial view
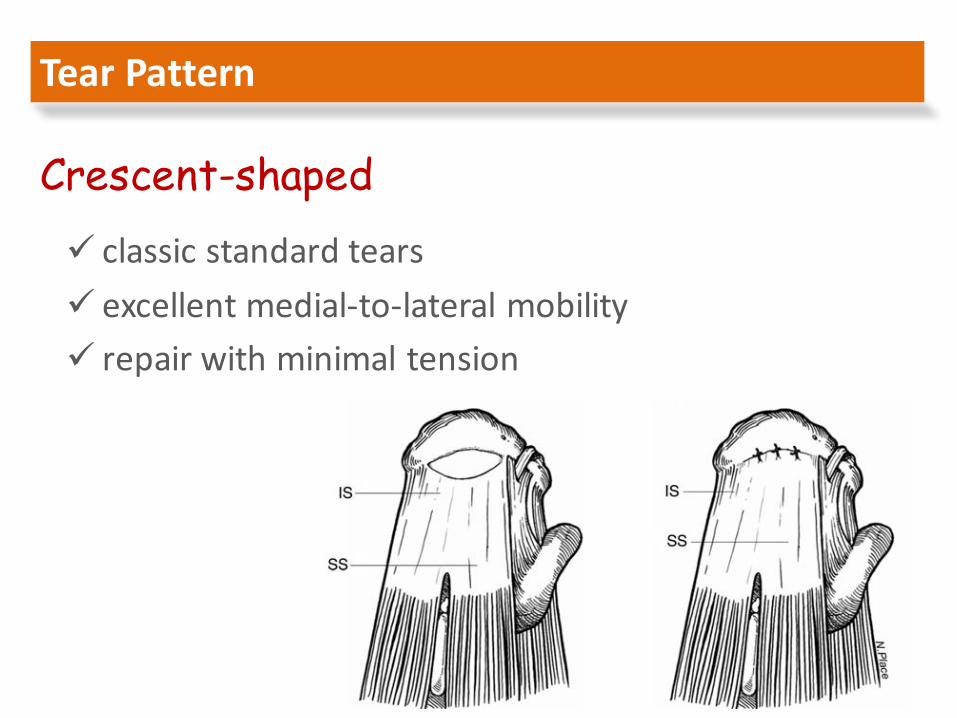
ü classicstandardtearsü excellentmedial-to-lateralmobilityü repairwithminimaltension
TearPattern
Crescent-shaped
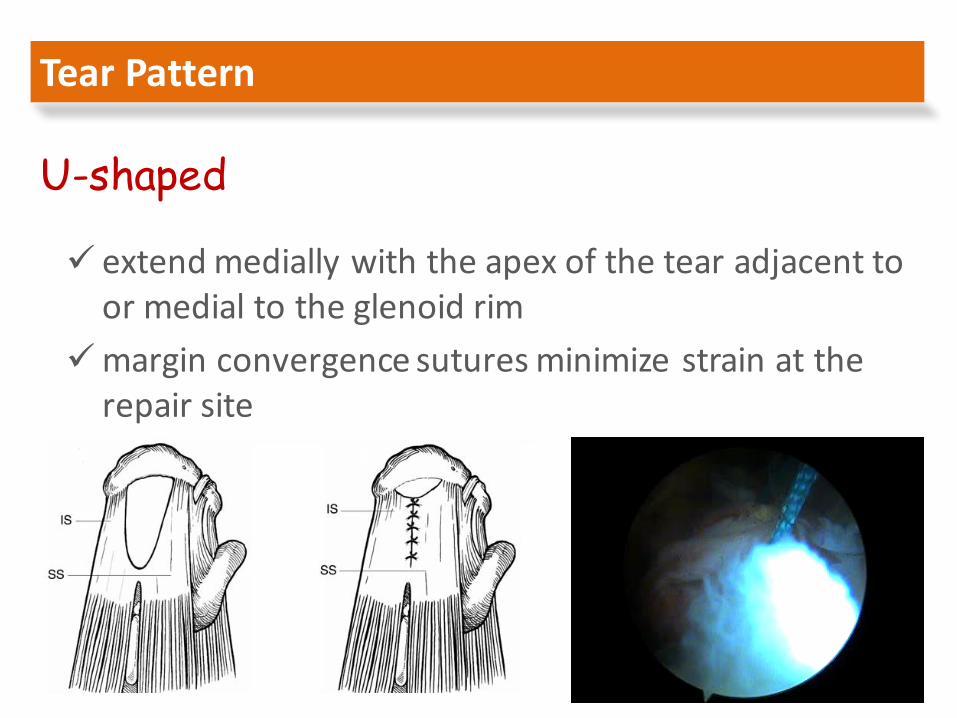
ü extendmedially withtheapexofthe tearadjacenttoormedialtotheglenoid rim
ümarginconvergence suturesminimizestrainattherepairsite
TearPattern
U-shaped
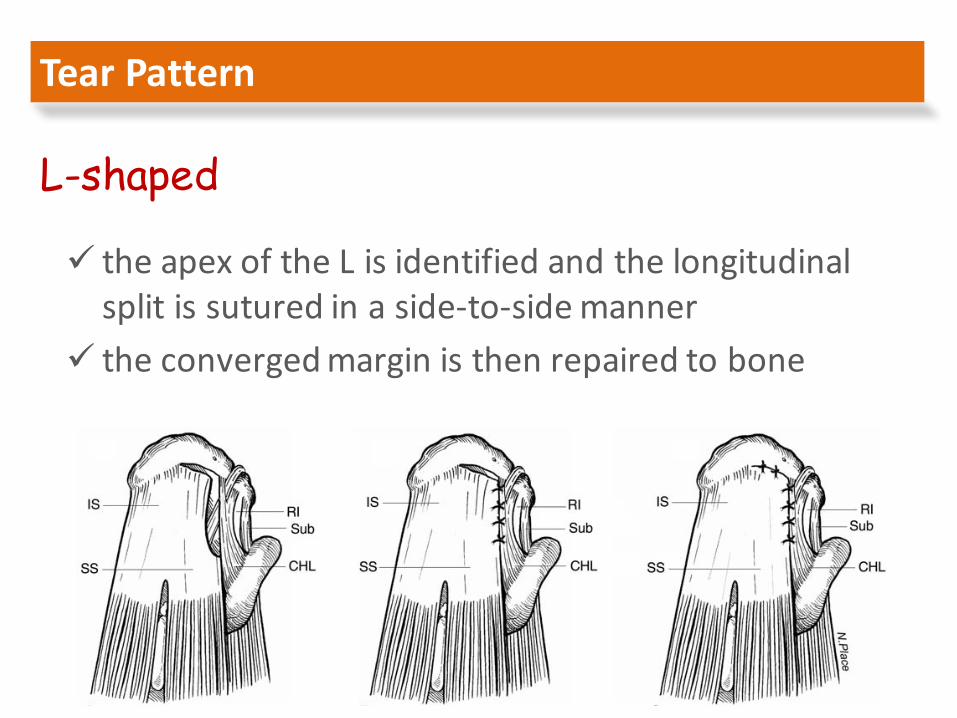
ü theapexoftheLisidentifiedandthelongitudinalsplitissuturedinaside-to-sidemanner
ü theconvergedmarginisthenrepairedtobone
TearPattern
L-shaped
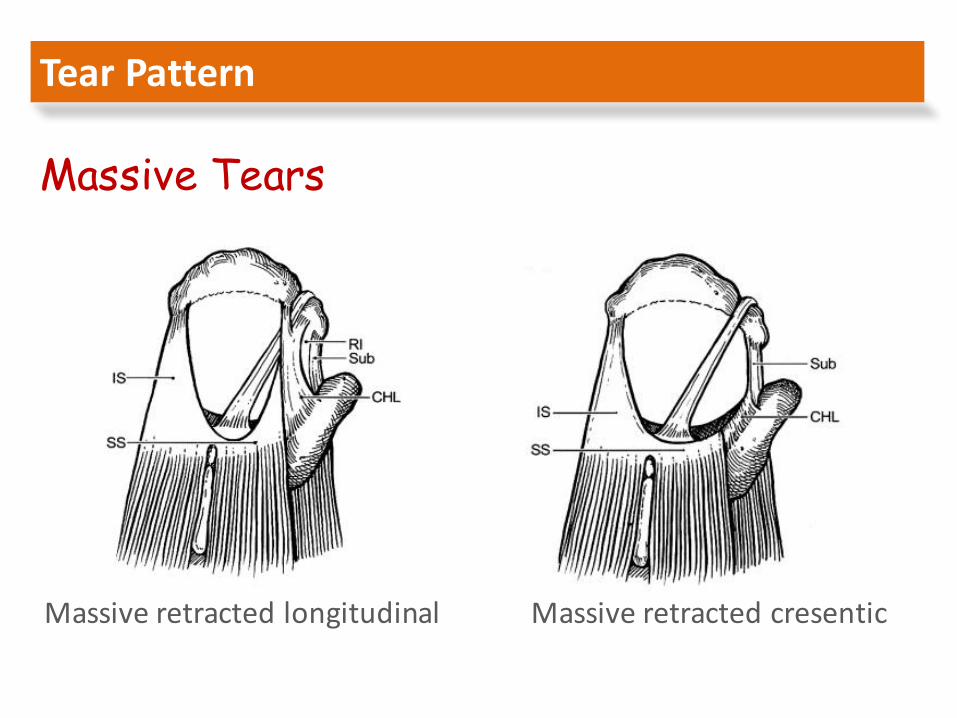
TearPattern
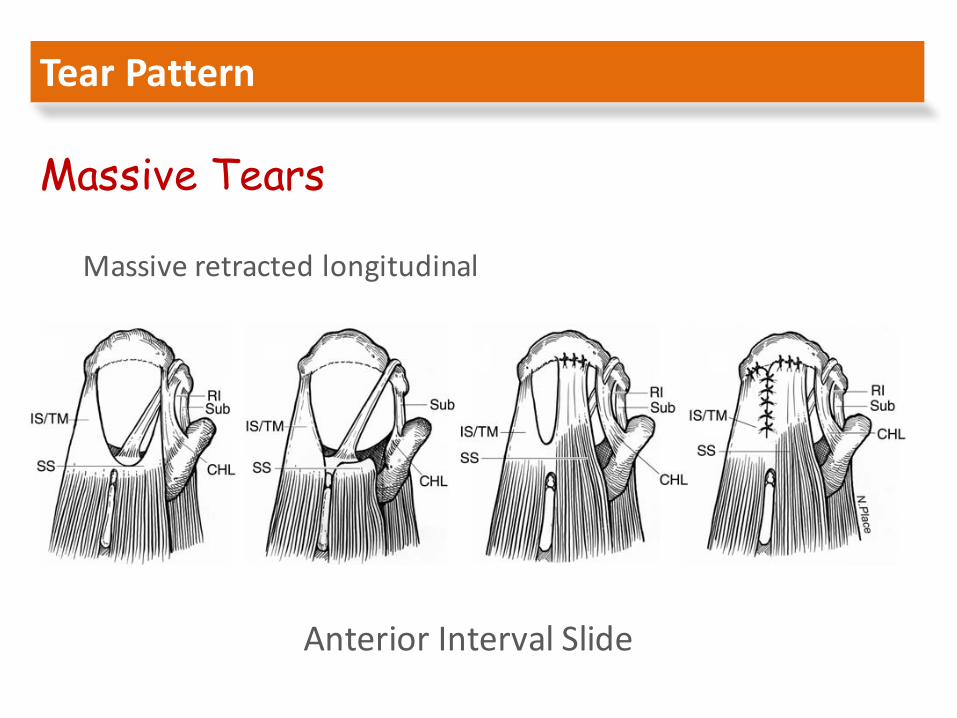
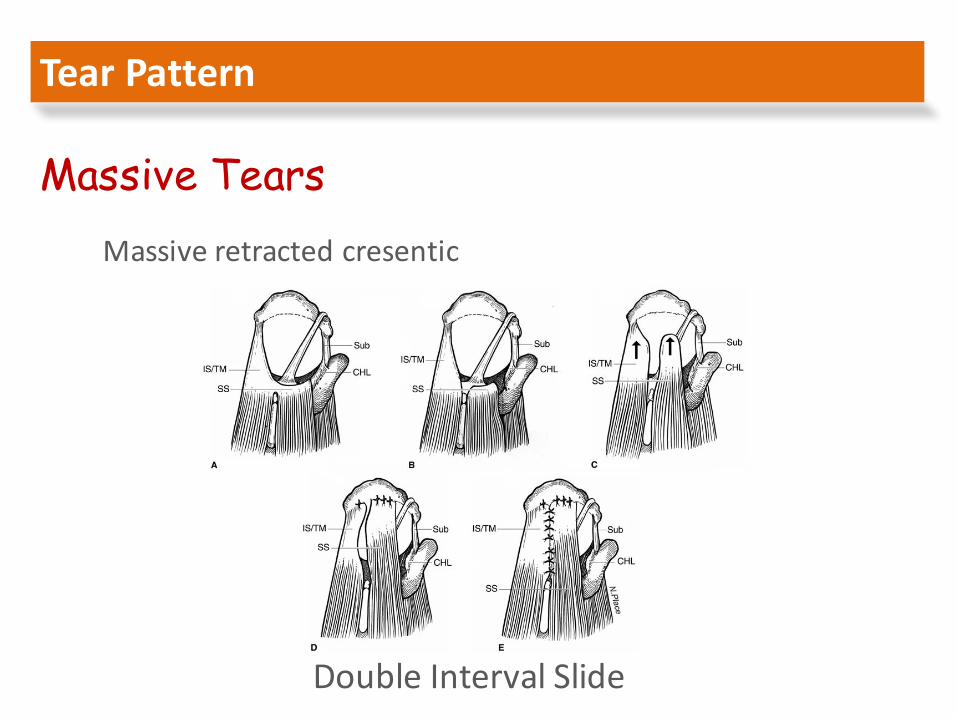
Massive Tears
Massiveretractedlongitudinal Massiveretractedcresentic
TearPattern
Massive Tears
Massiveretractedlongitudinal
AnteriorIntervalSlide
TearPattern
Massive TearsMassiveretractedcresentic
DoubleIntervalSlide
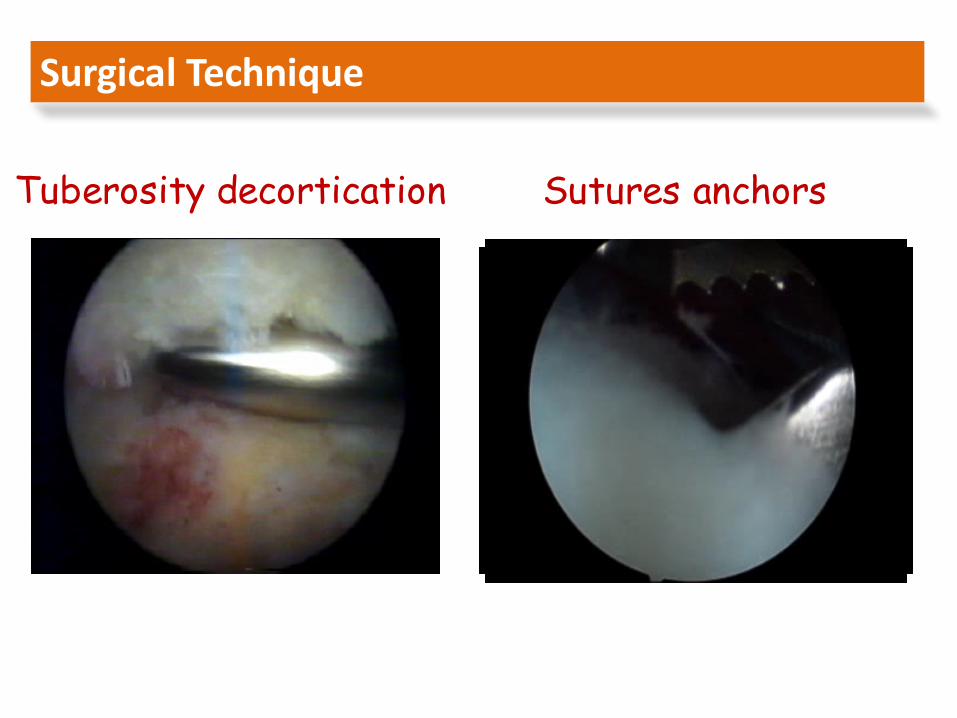
SurgicalTechnique
Tuberosity decortication Sutures anchors
ThequalityofFunctionalresultsdependson:
1. Thesizeofthepersistentdefect2. Associatedatrophyofthemuscles3. Integrityofthedeltoid4. Functionaldemandsofthepatient
FactorsaffectingRecurrenceoftear:
1. Advancedage2. Tearsize3. Fattydegeneration4. Chronicityandatrophy5. Poortendonquality6. Inappropriaterehabilitation7. Smoking8. Steroidinjections9. Diabetes
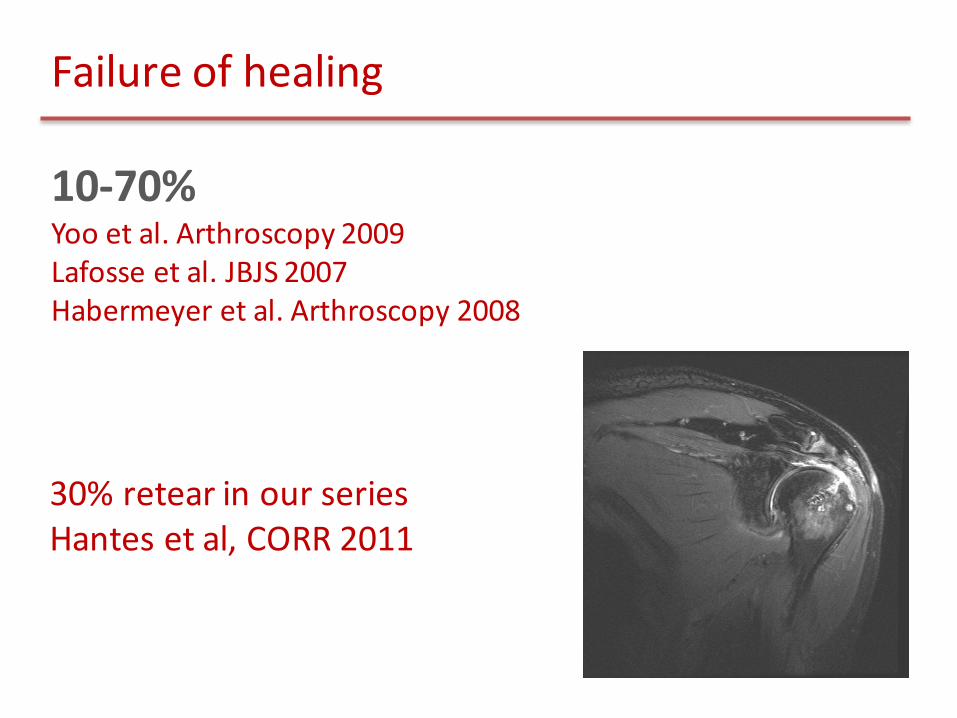
Failureofhealing
10-70%Yoo etal.Arthroscopy2009Lafosse etal.JBJS2007Habermeyer etal.Arthroscopy2008
30%retear inourseriesHantes etal,CORR2011
ResultsafterrepairofRCT
Goodexcellentresultsin85%to95%
PainreliefImprovementofmotionImprovementofstrength
Significantimprovementofshoulderfunction
ü RotCuffisextremelysignificantforthenormalfunctionoftheshoulder
ü RotCufftearscanbeasymptomatic
ü Symptomsproducedbyateardependon:– Size– Location– Functionaldemandsofthepatient
Conclusions
ü Ananatomicallydeficientbutbiomechanicalintactcuffispossible
ü Biomechanicalintactcuffisthecuffthatrestorestheequilibriumoftheforcecouples
ü Acuffteardoesnothealconservative
ü Acufftearafteroperativerepairmaynotheal
ü Partialhealingmayrestoresufficientpowertothecufftoequilibratetheforcecouples
Conclusions
