arthroscopic lat dorsi transfer
TRANSCRIPT
Lennard Funk Charlie Talbot Julia Walton
Indication for tendon transfer
• MRCT with Weakness
• Functional strength loss +/- pain
Clinically
• Pain
• Weakness
• Function loss
▫ Including ADLs
Pre-requisites of Transfer
• Intact deltoid
• Intact Subscapularis - maintain force-couple
• Good bone - fixation
• Compliant patient (young active)

Pre-Habilitation
• shoulder therapist
• Optimise Deltoid & function
• Activity modifications
• Re-assess before surgery

Biomechanics
▫ Gerber JSES 2008
▫ 3 different insertion sites
▫ Ant / post / inf GT
▫ Posterior most mechanically advantageous to ER

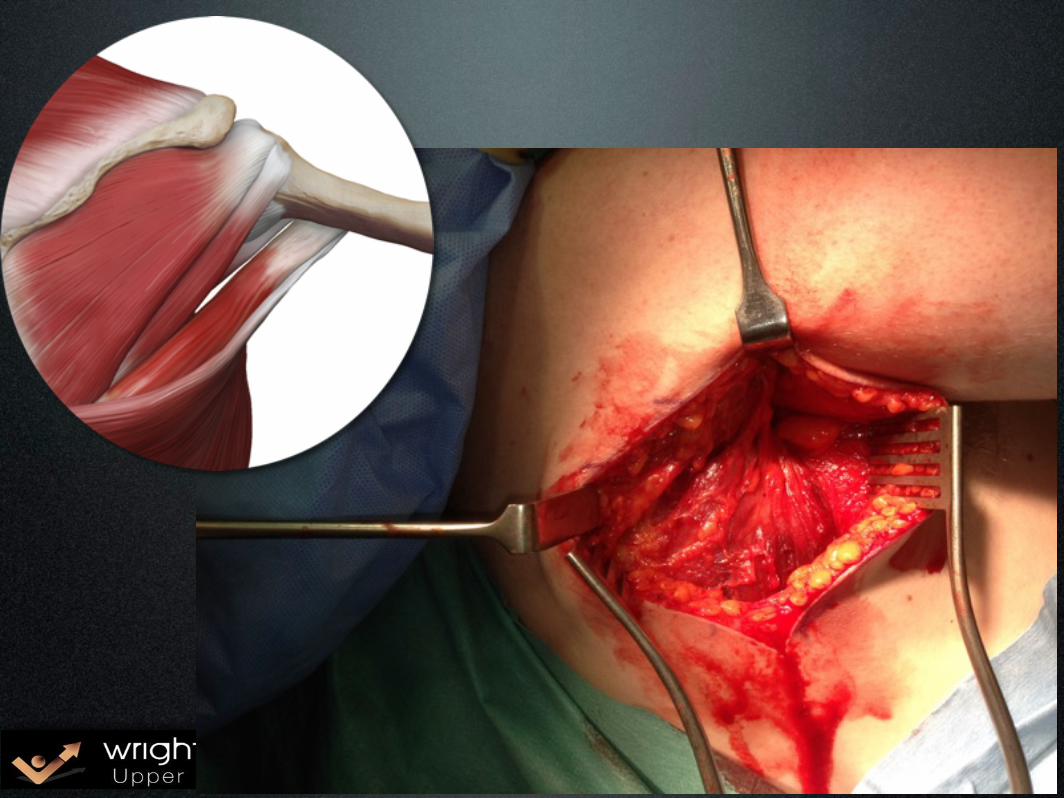
Principles of the technique
• Open: • Harvest Tendon • Mobilise tendon
• Arthroscopy: • Prepare surfaces • Develop track • Transfer tendon • Fixation

Position


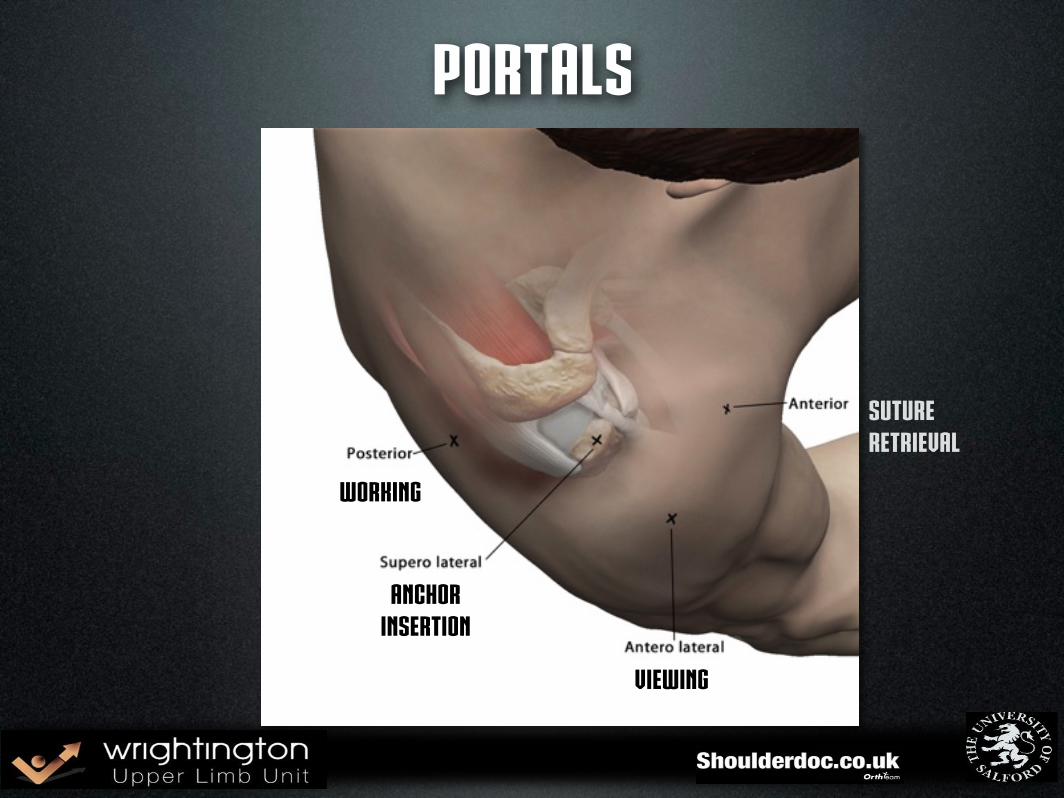
Portals
viewing
Anchorinsertion
Working
Suture Retrieval


Posterior Release

Humerus Prep

Suture retrieval

Tendon Retrieval
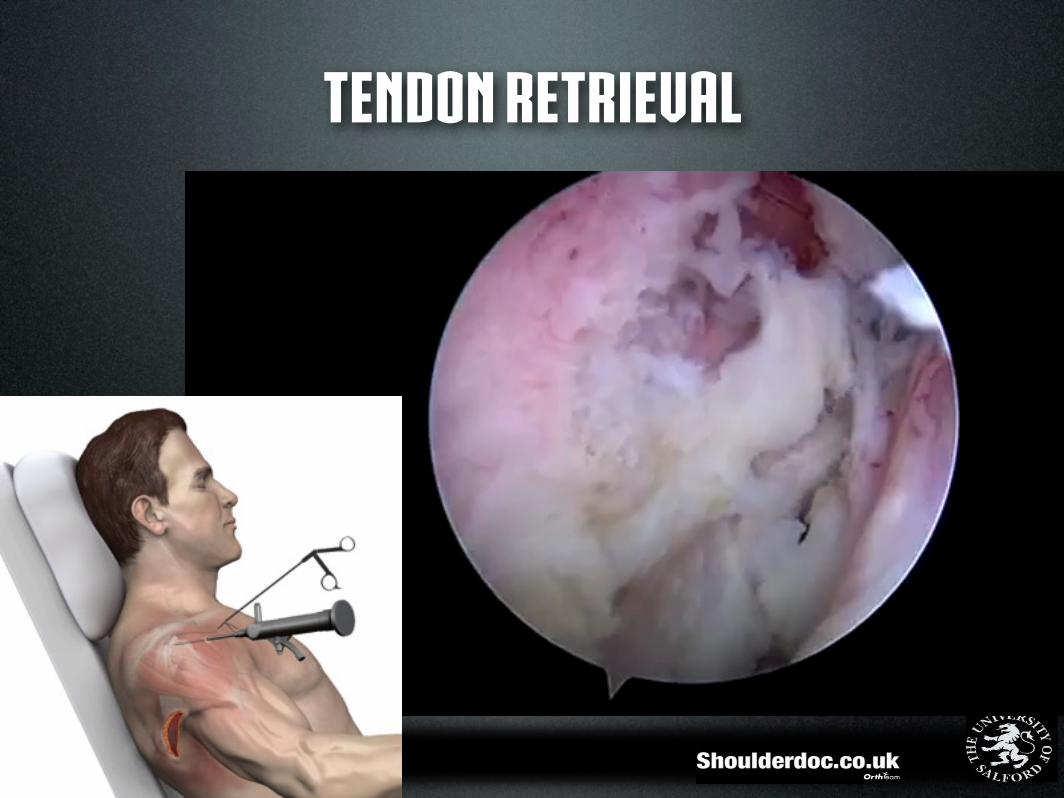
Tendon Retrieval
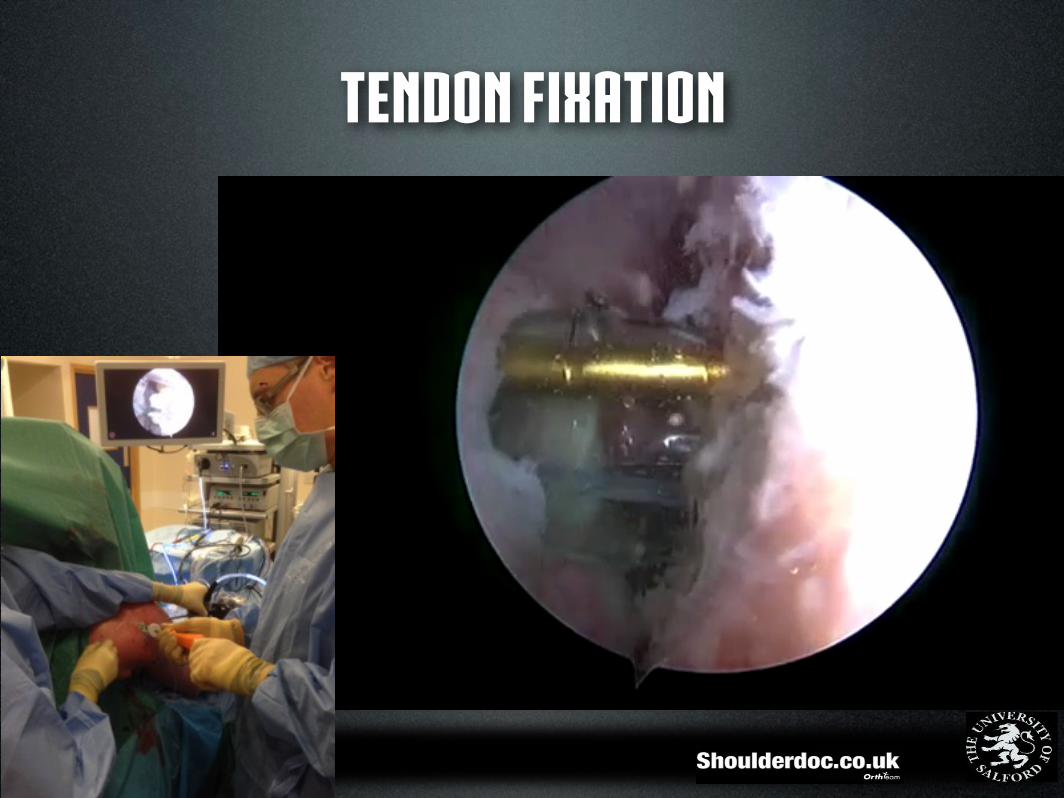
Tendon Fixation
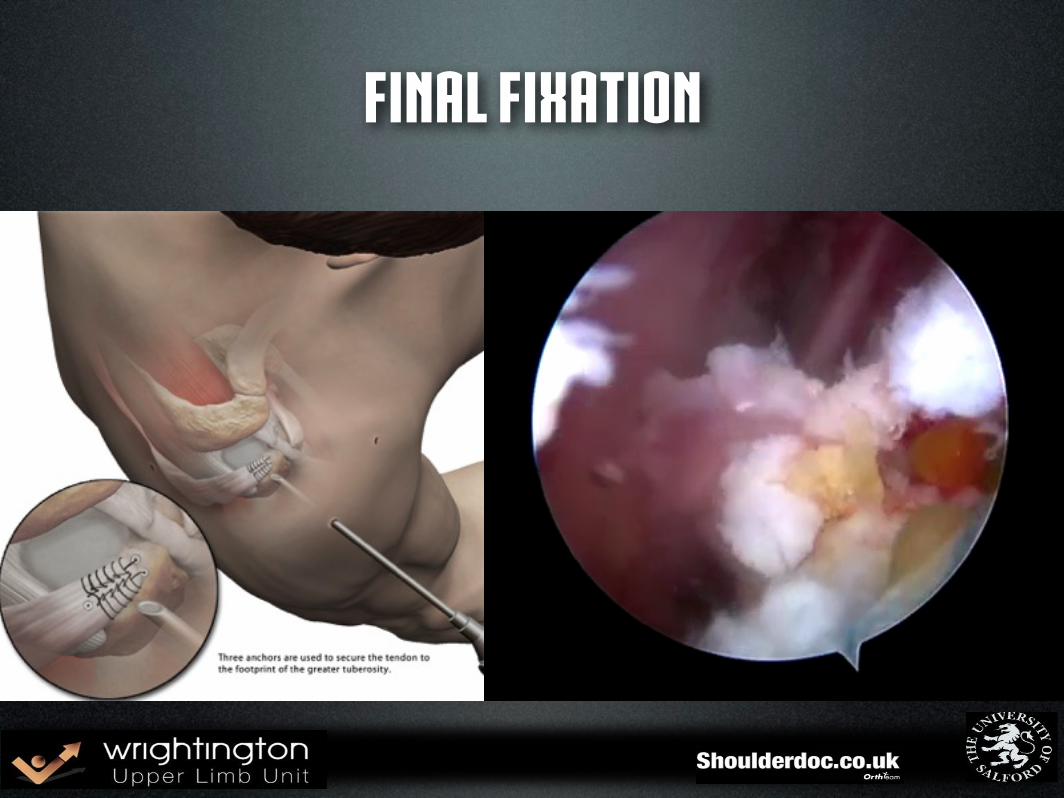
Final Fixation

Post Surgery ER brace - comfort only
pain management
limit NSAIDs
cold compression
Wound care
Early rehab.

Stage 1 Post Surgery (approx 0-3 weeks)
• Pain management
• Wound monitoring
• Closed active assisted ROM within safe zones
• Not forgetting the kinetic chain

Stage 1 Exercise ideas
Shoulderdoc

Stage 1 Exercise ideas - early kinetic chain
ShoulderdocShoulderdoc
Stage 1 Avoid…
• Horizontal adduction/internal rotation
• Early resisted external rotation
• Pain!
Stage 2 (approx 3-6 Weeks)
• Reduce sling support – wean from ER wedge
• Continue to increase active assisted ROM closed chain (Proprioceptive value) Quality of movement
• Facilitating hand over elbow
• Begin gentle isometric ER in neutral
The lat dorsi’s new roleShoulderdoc

Exercise ideas
•
Shoulderdoc
Stage 3 (approx 6-12 Weeks)
• Continue with active ROM reinforcing hand over elbow
• Tips…
• Break the movement down
• Start with eccentrically lowering arm to aid re-education
(Donaldson et al 2011)

Stage 3 (approx 6-12 Weeks)
• Commence open chain ROM leading to resistance work
• Continue to integrate kinetic chain and general conditioning as able
Goal specific rehab.

Stage 3 Exercise

Stage 3 Exercise Ideas

Stage 4 (3 Months +)
• Progress function - load/endurance
• unconstrained ROM
• Fitness & conditioning
• Return to work

Stage 4 (3 Months +)

Results
RCT not appropriate / feasible
Evidence cohorts / large case series

Results - Arthroscopic French MULTICENTER PROSPECTIVE STUDY
• J.Grimberg, J.Kany, Ph. Valenti, J. Garret, LD. Duranthon, VK Chang
• (Paris, Saint Jean, Lyon, Hawaï) • SECEC meeting, Lyon 2011

RESULTS
• 49 Patients (27 Dr JK, 11 Dr PhV, 11 Dr JG) • Mean age at surgery: 59,4 (31-73) • 23 primary surgeries, 26 secondary surgeries (1 to
6 previous surgical procedures) • Mean follow up : 21,2 months (12-42) • No lost to follow-up.

CLINICAL RESULTS
• CONSTANT SCORE
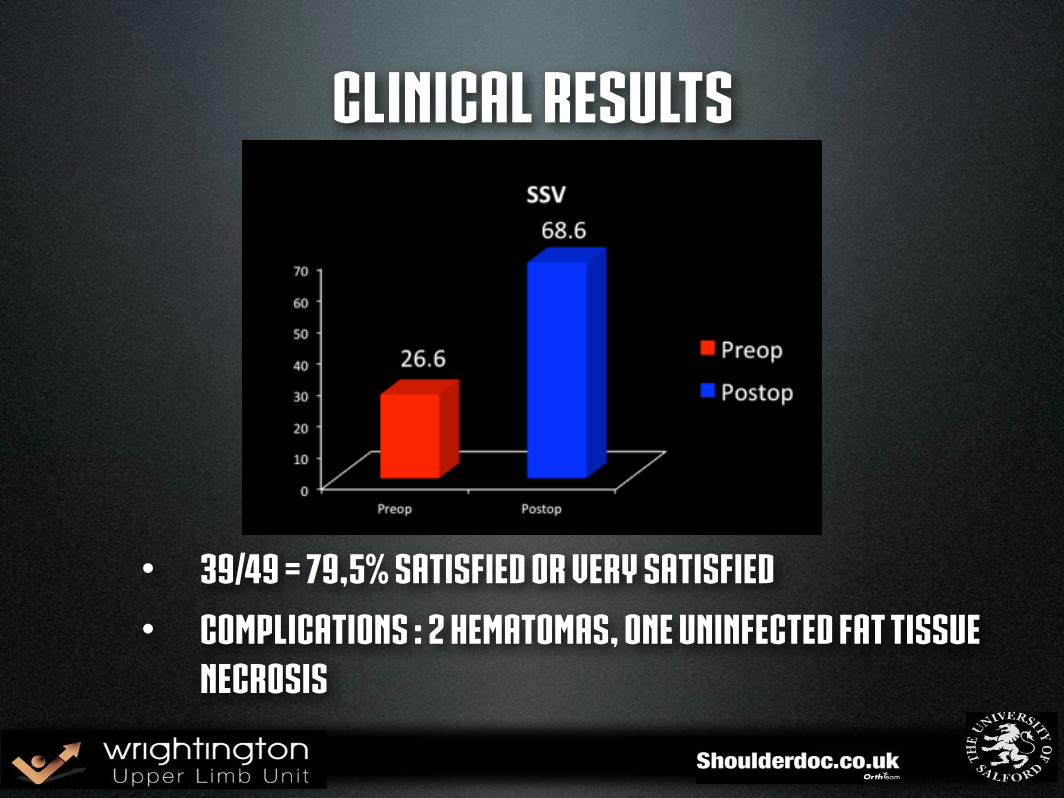
CLINICAL RESULTS
• 39/49 = 79,5% satisfied or very satisfied • Complications : 2 hematomas, one uninfected fat tissue
necrosis
MRI : one year postop
• 44 patients : 89,8% of patients controlled • 41 intact tendons : 93% of controlled patients • 3 tendon-bone secondary pull out probably linked to
bone weakness

MRI
LD muscle
LD tendon
Deltoid muscle

PREDICTING FACTORS• NO INFLUENCE ON CLINICAL RESULTS • Age > or < 65 • Sex • Manual/Light/Sedentary work • Preop active anteflexion > or < 90° • Zone of tendon fixation : superior or posterior
• PEJORATIVE FACTORS • Worker’s compensation • Preoperative surgery

Summary• Set REALISTIC Expectations
• pre-op specialist rehab.
• Patient MUST be committed
• Communication VITAL
• good graft fixation
• Open / arthroscopic (?)
