arterial blood gases2
TRANSCRIPT
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 1/46
Z C HA R MA I NE L . Y UM A NGS E P T E M B E R 2 0 1 0
ARTERIAL BLOOD GAS

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 2/46
ABG???
y Arterial blood gas analysis
is an essential part of diagnosing andmanaging a patient¶s oxygenation status and
acid-base balancemeasures the acidity (pH) and the levels of
oxygen and carbon dioxide in the blood froman artery
This test is used to check how well your lungsare able to move oxygen into the blood andremove carbon dioxide from the blood.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 3/46
Acid Base Balance
The pH is a measurement of the acidity oralkalinity of the blood.It is inversely proportional to the number of
hydrogen ions (H+) in the blood.The more H+ present, the lower the pH will be.The fewer H+ present, the higher the pH will be.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 4/46
Acid Base Balance
y Normal blood pH range is 7.35 to 7.45
In order for normal metabolism to take place, the body must maintain thisnarrow range at all times.
y pH <7.35 decrease in the force of cardiac contractions
decrease in the vascular response to catecholamines
diminished response to the effects and actions of certain medications
y
pH > 7.45 int erferes with ti ssue oxygenati on and normal neurological and muscular functioning.
y Extreme acid-base derangements will interfere with cellular functioning, and if uncorrected, will lead to death.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 5/46
Maintenance of Acid Base Balance
y So how is the body able to self-regulate acid-base balance in order to maintain pH within the
normal range?
BUFFER SYSTEMS

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 6/46
Respiratory Buffer System
y A normal by-product of cellular metabolism is carbondioxide (CO2). CO2
y CO2 is carried in the blood to the lungs, where excessCO2 combines with water (H2O) to form carbonic acid
(H2CO3). CO2 + H2O = H2CO3y T he blood pH wi ll change accord ing t o the l evel o f
carboni c aci d present .
y This triggers the lungs to either increase or decrease the
rate and depth of ventilation until the appropriateamount of CO2 has been re-established.
y Activation of the lungs to compensate for an imbalancestarts to occur within 1 to 3 minutes.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 7/46
Renal Buffer System
y In an effort to maintain the pH of the blood withinits normal range, the kidneys excrete or retain
bicarbonate HCO3
y blood pH decreases (acidic) - the kidneys willcompensate by retaining HCO3
y blood pH rises (alkalotic) - the kidneys excreteHCO3 through the urine

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 8/46
COMPONENTS
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 9/46
y pH
Measurement of acidity or alkalinity, based on the hydrogen(H+) ions present.
The normal range is 7.35 to 7.45
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 10/46
y PaO2
The partial pressure of oxygen that is dissolved in arterial blood.
It measures how well oxygen is able to move from the airspaceof the lungs into the blood.
The normal range is 80 to 100 mm Hg
Desired PaO2
Ù 80 ± YEARS ABOVE 60
Example 75 y/o Female
PaO2 = 80 ± (75-60) = 65
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 11/46
y SaO2
The arterial oxygen saturation.
Oxygen saturation measures how much of the hemoglobin in
the red blood cells is carrying oxygen (O2 The normal range is 95% to 100%.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 12/46
y PaCO2
The amount of carbon dioxide dissolved in arterial blood.
how well carbon dioxide is able to move out of the body
The normal range is 35 to 45 mm Hg

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 13/46
y HCO3
The calculated value of the amount of bicarbonate in the bloodstream.
The normal range is 22 to 26 mEq/liter

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 14/46
ACID BASE DISORDERS

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 15/46
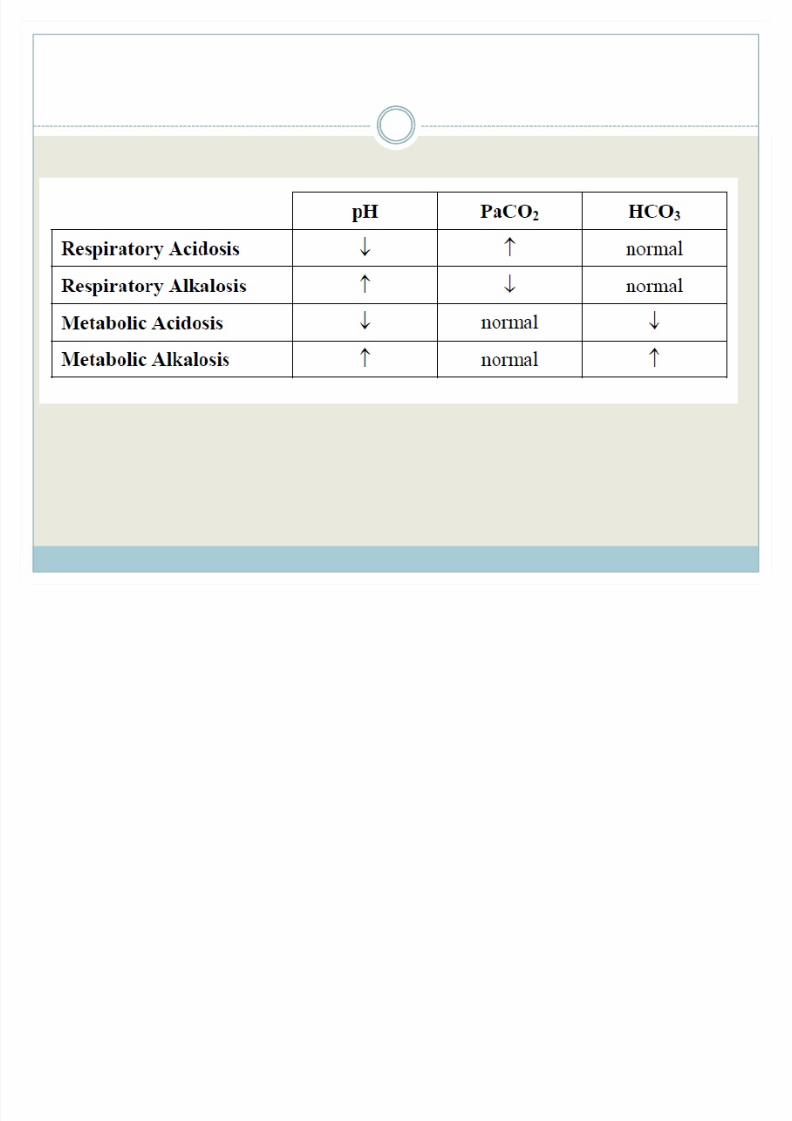
Respiratory Acidosis
y Low pH
y High PaCO2
y Primary increase in pCO2 resulting from alveolar
hypoventilation

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 16/46
Respiratory Acidosis
y Respiratory center depression Brainstem lesions narcotics, sedatives, or anesthesia
y Neuromuscular failure Impaired respiratory muscle function related to spinal cord injury,
neuromuscular diseases, or neuromuscular blocking drugsy Decreased compliance
Parenchymal (e.g pulmonary fibrosis, ARDS) Extraparenchymal (e.g. Abdominal distention, severe kyphoscoliosis)
y Increased airway resistance
COPD OSA
y Increased dead space Large pulmonary embolus

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 17/46
Respiratory Alkalosis
y High pH
y Low pCO2
y Primary decreased in pCO2 resulting from alveolar
hyperventilation

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 18/46
Respiratory Alkalosis
y Central nervous system stimulation Pain
Meningoencephalitis
SAH
Hepatic encephalopathy
y Hypoxemia Moderate asthma exacerbation
Acute pulmonary edema
Pulmonary embolus High altitude
pneumonia

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 19/46
Respiratory Alkalosis
y Drugs
Progesteroneµ
Salicylate poisoning
Xanthinesy Miscellaneous
Sepsis
Mechanical hyperventilation
pregnancy
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 20/46
Metabolic Acidosis
y Low pH
y low HCO3
y Primary decreased in plasma HCO3 due to either
HCO3 loss or accumulation of acid
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 21/46
Metabolic Acidosis
y High anion gap K etoacidosis ± diabetic, alcoholic, starvation
Lactic Acidosis
Intoxications ± e.g. Ethylene glycol, methanol, salicylate
Advanced Renal Failure Severe rhabdomyolysis
y Normal anion gap GI HCO3 loses (lower GI fistulas, diarrhea, ureterosigmoidostomy)
Renal tubular acidosis
Moderate renal insufficiency Acetazolamide use
Large volume saline resuscitation

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 22/46
Metabolic Alkalosis
y High pH
y High HCO3
y Primary increase in the plasma HCO3 due to either
H+ loss or HCO3 gain
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 23/46
Metabolic Alkalosis
y Chloride Responsive
Upper GI losses
Previous diuretic use
Recovery from chronic hypercapniay Chloride unresponsive
Effective mineralocorticoid excess
Current diuretic use
Bartter¶s or Gitelman¶s syndrome Severe hypokalemia
Excessive alkali administration

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 24/46
Steps on Dissecting Acid ± Base Disorder
y Step 1 : Predict what underlying mechanisms might be present based on the clinical scenario.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 25/46
Steps on Dissecting Acid ± Base Disorder
y Step 2: Verify that the ABG values are internally accurate
Simplified form of the Henderson-Hasselbach Equation:
[H+] (nmol/L) = 24 x pCO2 (mmHg) / [HCO3-] (meq/L)

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 26/46

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 27/46
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 28/46
Steps on Dissecting Acid ± Base Disorder
y Step 3:
If the blood is alkalotic or acidotic, we now need todetermine if it is caused primarily by a respiratory or metabolicproblem.
A. Assess the PaCO2 level.
Remember that with a respiratory problem, as the pHdecreases below 7.35, the PaCO2 should rise. If the pH risesabove 7.45, the PaCO2 should fall.
Compare the pH and the PaCO2 values. If pH and PaCO2are indeed moving in opposit e d i recti ons, then the probl em i s
pri mari ly res pi rat ory in nat ure.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 29/46
Steps on Dissecting Acid ± Base Disorder
y Step 3:
B. Assess the HCO3 value. Recall that with a
metabolic problem, normally as the pH increases,the HCO3 should also increase. Likewise, as the pHdecreases, so should the HCO3.
Compare the two values. If they are moving in the same d i recti on, then the probl em i s primarily metabolic in nature.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 30/46

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 31/46
CASE 1
y Jane Doe is a 45-year-old female admitted to thenursing unit with a severe asthma attack. She has
been experiencing increasing shortness of breath
since admission three hours ago.y Her arterial blood gas result is as follows:
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 32/46
y Follow the steps:
1. Clinical Prediction
2. Assess the pH.
3. Assess the PaCO2.
4. Assess the HCO3.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 33/46
Aci d osi s i s present ( decreased pH) with the P aCO2 being increased, reflecting a primary res pi rat ory probl em.
For thi s pati ent , we need t o i m prove the venti l ati on status by providing oxygen therapy, mechanical ventilation, pulmonary toilet or by administering bronchodilators.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 34/46
CASE 2
y John Doe is a 55-year-old male admitted to yournursing unit with a recurring bowel obstruction. Hehas been experiencing intractable vomiting for the
last several hours despite the use of antiemetics.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 35/46
y Follow the steps:
1. Clinical Prediction
2. Assess the pH.
3. Assess the PaCO2.
4. Assess the HCO3.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 36/46
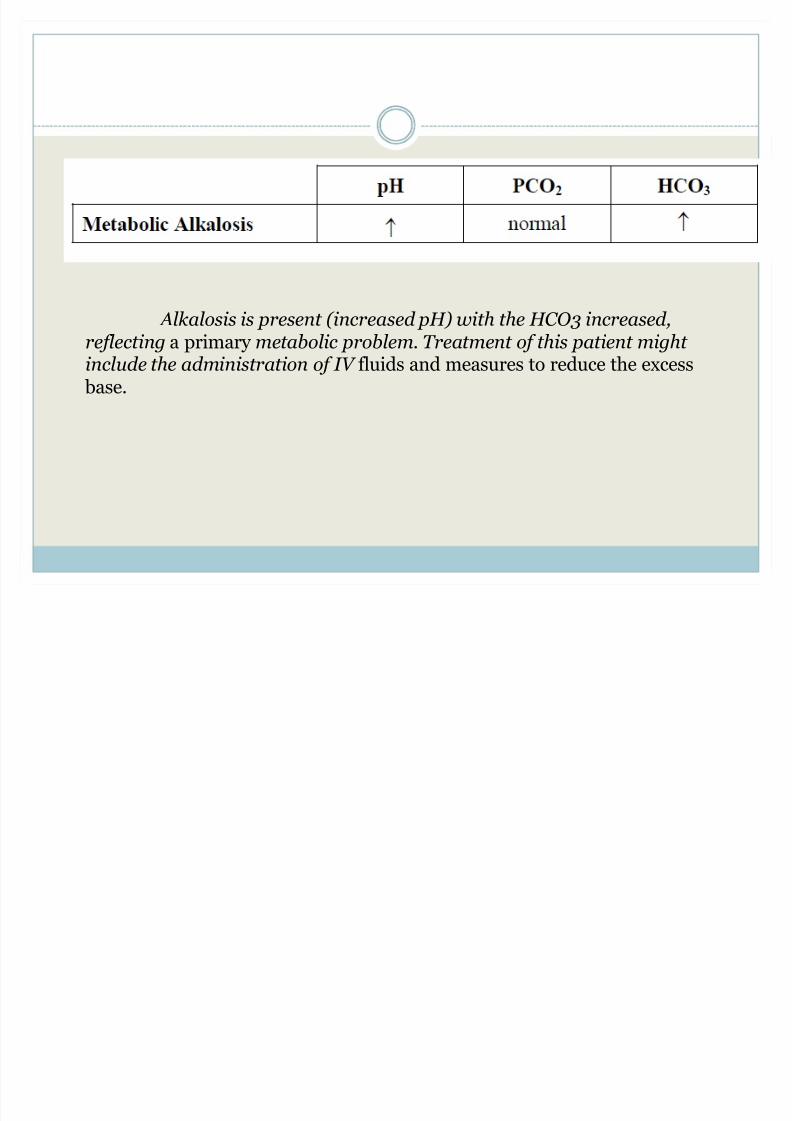
Alkalosi s i s present ( increased pH) with the H CO 3 increased, ref l ecting a primary met abol i c probl em. T reat ment o f thi s pati ent mi ght incl ude the admini st rati on o f IV fluids and measures to reduce the excess base.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 37/46
Compensation

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 38/46
Compensation
y body attempts to restore the normal blood pH duringan acid-base disorder
y compensation can be metabolic or respiratory in
origin

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 39/46
Respiratory Compensation
y Respiratory compensation
rapid process in which ventilation is adjusted to alter the pCO2
in response to a primary alteration in the [HCO3-].
Increased HCO3- levels will stimulate hypoventilation and a
subsequent rise in pCO2.
Decreased HCO3- levels will produce the opposite effect.
begins within seconds and can reach maximum effectiveness within 12-24 hours
Res pi rat ory com pensati on can never com pl et ely regain a normal blood pH. Other fact ors invol ved in venti l ati on cont rol , es peci ally the need f or oxygen, wi ll not allow f or full com pensati on.

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 40/46
Compensation
y Metabolic compensation is a slower process Occurs in two phases
Ù First phase involves intracellular non-bicarbonate buffers responsible for the first phase, which occurs immediately
Ù Second phase kidneys are responsible begins within hours, but takes 2 to 5 days to reach maximal
effectiveness kidneys achieve compensation by altering net bicarbonate
reabsoprtion and net acid excretion into the urine. Given enough time (up to 4 weeks) metabolic compensation may
be able to return the blood pH to normal in chronic respiratory disorders.2
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 41/46
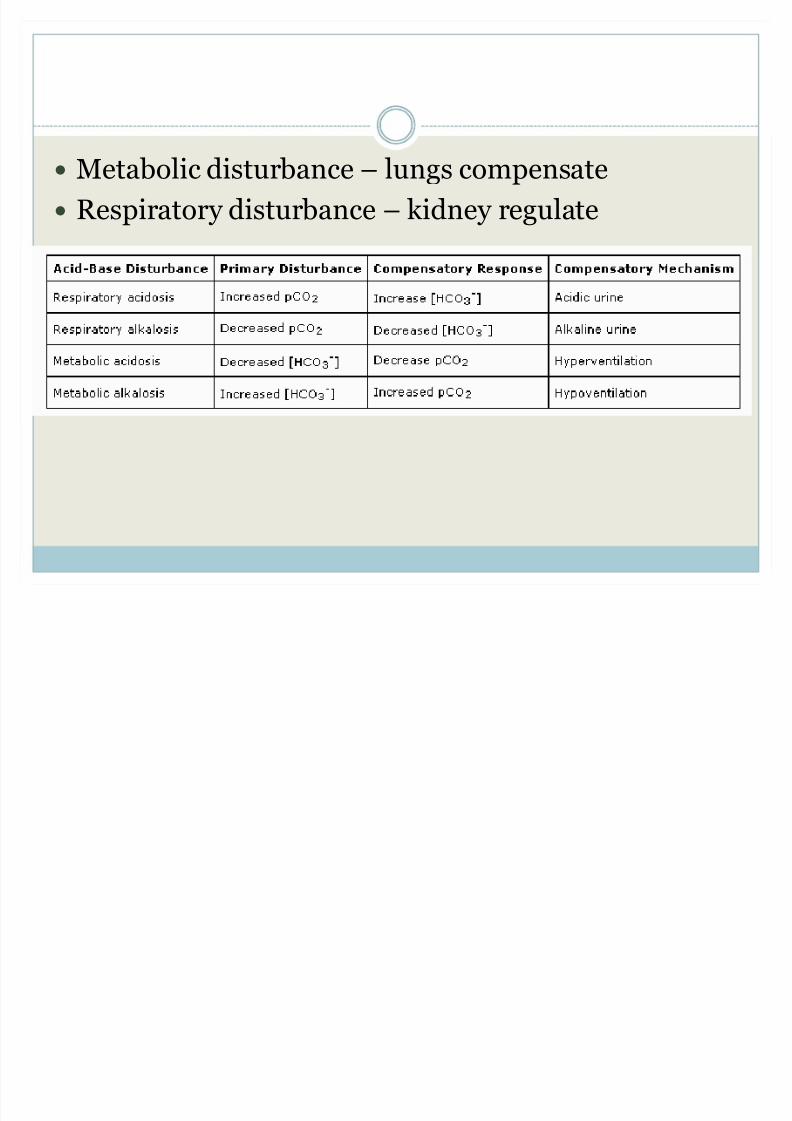
y Metabolic disturbance ± lungs compensate
y Respiratory disturbance ± kidney regulate

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 42/46
CASE 3
y Mrs. L is a thin, elderly-looking 61 year old COPDpatient. She has an ABG done as part of her routinecare in pulmonary clinic.
y Her ABG shows the following results
pH : 7.37
CO2: 63
pO2 : 58 HCO3: 35
SaO2: 89%

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 43/46
y Follow the steps:
1. Clinical Prediction
2. Assess the pH.
3. Assess the PaCO2.
4. Assess the HCO3.
8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 44/46
Clinical Prediction
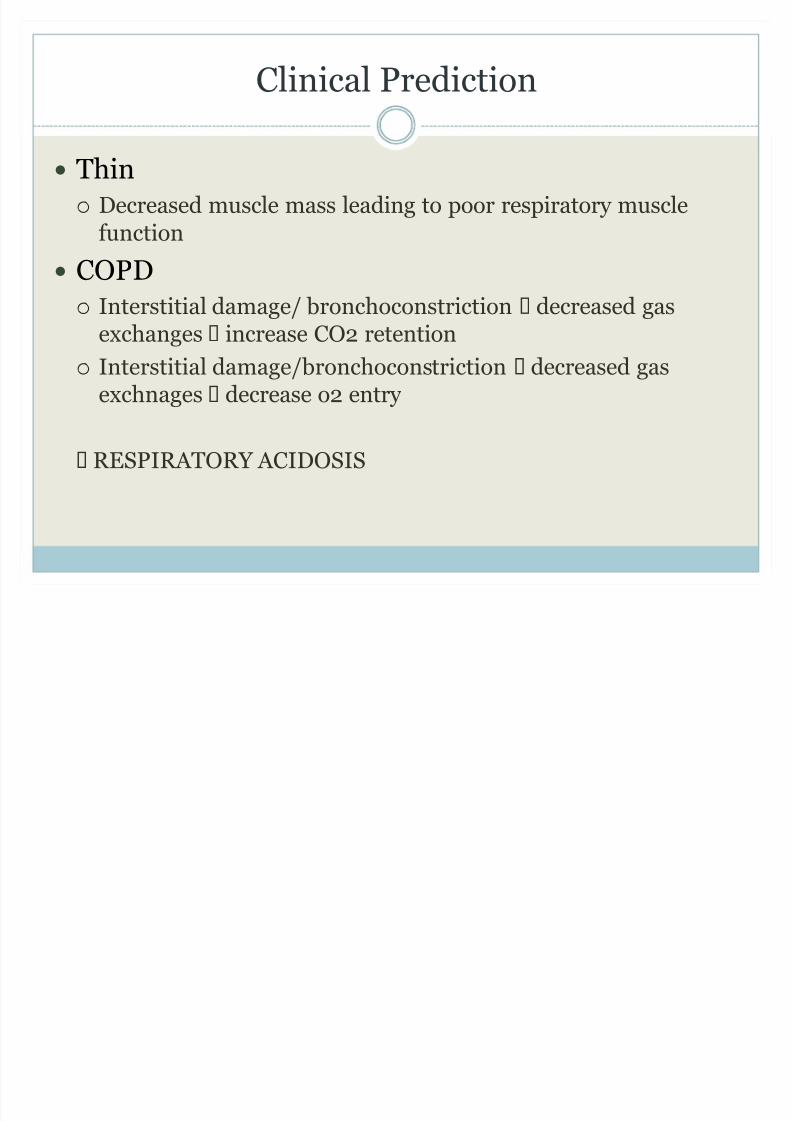
y Thin
Decreased muscle mass leading to poor respiratory musclefunction
y
COP
D Interstitial damage/ bronchoconstriction decreased gas
exchanges increase CO2 retention
Interstitial damage/bronchoconstriction decreased gasexchnages decrease o2 entry
RESPIRATORY ACIDOSIS

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 45/46
1. pH - acidic
2. Assess the PaCO2 - increased
3. Assess the HCO3 - increased
y pH : 7.37
y CO2: 63
y HCO3: 35 Simple compensated respiratory acidosis
Full compensation is evidenced by the normal pH in spte of heracid/base disorder
This is her baseline and doesn¶t require treatment

8/8/2019 ARTERIAL BLOOD GASES2
http://slidepdf.com/reader/full/arterial-blood-gases2 46/46
Actual Patient
y JL 35y/o female came in to the ER due to shortness of breathy Desired Fio2
A= pCO2/ 0.8 B = (713 x del FiO2/100) ± A C = p02/B Des FiO2 = (des PO2/C) + A/ 713 x 100
Del FiO2Ù NC = (# LPM x 4) + 20Ù FM = (# LPM ± 1) x 10
y Mechanical ventilator with the following settings: TV: 450, FiO2:60, PF:60and BUR:20. Dormicum was discontinued.
y Arterial blood gas pH 7.64
pCO2 29.8 pO2 109.1 HCO3 21.6mechanical ventilation settings were adjusted to FiO2:40%, Peak flow 45 and BUR:14.