arterial air embolism in the cat brain - homepage |...
TRANSCRIPT

pH AND BBB LACTATE, NICOTINE UPTAKE/Oldendorf et al. 581
metabolism. In Hanson RW, Mehlman MA (eds) 23.Gluconeogenesis: Its Regulation in Mammalian Species. NewYork, Wiley, 1976, pp 165-220
21. Voorheis HP: Changes in the kinetic behaviour of threonine 24.transport into Trypanosoma brucei elicited by variation inhydrogen ion concentration. Biochem J 164: 15-25, 1977
22. Marks MJ, Medzihradsky F: Characterization of the transport 25.system for benzomorphans in leukocytes. Mol Pharmacol 10:837-848, 1974
Kaufman JJ, Koski WS, Benson DW: Temperature and pHsensitivity of the partition coefficient as related to the bloodbrain barrier to drugs. Exp Eye Res 25 (suppl) 201-203, 1977Ljunggren B, Norberg K, Siesjo BK: Influence of tissue acidosison restitution of brain energy metabolism following totalischemia. Brain Res 77: 173-186, 1974MacMillan V, Siesjo BK: Cerebral energy metabolism, InCritchley M, O'Leary JL, Jennett B: Scientific Foundations ofNeurology. Phil, FA Davis Co, 1972, pp 21-32
Arterial Air Embolism in the Cat Brain
H. FRITZ, M.D. AND K.-A. HOSSMANN, M.D.
SUMMARY In cats air embolism of the brain was produced by injecting 0.6 ml blood foam into the in-nominate artery proximal to the origin of both common carotid arteries. Air embolism caused transientischemia of the brain, reaching a maximum within 1 min after injection. Resolution of the air embolism begana few minutes later and was completed within 15 min in the center and within 30 min in the border zone of themain supplying arteries. During this phase tissue perfusion was inhomogenous with reduced flow rates in someareas and reactive hyperemia up to 300% in others. This resulted in venous hyperoxia and a decrease ofarteriovenous oxygen difference to as low as 2 ml/100 ml blood. Reactive hyperemia was accompanied bybrain swelling and an increase in intracranial pressure from 3.6 ± 1.2 to 12.3 ± 2.0 mm Hg. The reason forhyperemia was a decrease of cortical pH which fell from 7.33 ± 0.03 to 7.03 ± 0.05, and which caused a dila-tion of pial arteries up to 260%.
Immediately after embolism, the EEG flattened and oxygen consumption decreased. After normalization offlow, oxygen consumption returned to normal, but EEG only partially recovered. Air embolism had little effecton the water and electrolyte content of the brain, and produced very little damage to the blood-brain barrier.
Stroke Vol 10, No 5, 1979
THE EFFECT of ischemia on cerebral function,metabolism and structure is a highly controversialissue which, despite extensive research during the pastyears, has not been satisfactorily solved. Many in-vestigators feel that duration and intensity of ischemiaare the main denominators of tissue damage, whereasothers, including ourselves, are of the opinion thatpost-ischemic events are of equal if not greater impor-tance. Unexpected findings, such as the observationthat severe incomplete ischemia is more harmful thantotal cerebrovascular arrest, have added to the con-fusion.1' 2
It is of little help when the different results are ex-plained by differences in the experimental models aslong as the pathophysiology of these models is notprecisely known. We have, therefore, studied inprevious investigations different forms of ischemia,and we found that, in fact, the pathomechanism ofischemia varies considerably. Besides the duration andcompleteness of ischemia, the site of occlusion seemsto be of particular importance. For instance, followingembolism of the capillary bed with microspheres, thenet flow rate of the brain may remain constantbecause there is a redistribution of flow with
From the Max-Planck-Institut fur Hirnforschung, For-schungsstelle fur Himkreislaufforschung, Ostmerheimer Strasse200, D 5000, Koln 91, West Germany.
Supported by the Deutsche Forschungsgemeinschaft.
hyperemia in the non-occluded vessels. The main in-jurious factor is the breakdown of the blood-brainbarrier (BBB), leading within a few minutes to severevasogenic brain edema and intracranial hyperten-sion.3' * On the other hand, ischemia produced by ex-tracerebral interruption of blood supply (inflowocclusion), causes primarily a breakdown of theenergy producing metabolism, and an inhibition of allendergetic processes. But there is no change in thepermeability of the blood-brain barrier to serumproteins.6 Edema, if present, is of the cytotoxic type,and it is rapidly reversible upon restoration of bloodflow.8 Finally, occlusion of the middle cerebral arterycauses initially metabolic disturbances and a cytotoxictype of brain edema, but after a few hours vasogenicedema supervenes.7-8
In the present series of experiments we have studiedthe pathophysiology of air embolism, which is a modelof intracerebral small vessel occlusion. Air bubbles aretrapped in small intracerebral arteries, leading toacute interruption of blood flow in the supplyingterritories of the affected vessels.914 The site of occlu-sion, consequently, is proximal to the capillary bed butdistal from the large supplying arteries. We were,therefore, interested to know whether the path-ophysiology of air embolism resembles the inflowocclusion or the microembolism type of ischemia. Ourresults indicate that it combines elements of bothtypes, and that, for this reason, it is a useful model for
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

582 STROKE VOL 10, No 5, SEPTEMBER-OCTOBER 1979
studying the response of the brain to ischemia in amore general way.
Material and Methods
Twenty-eight cats weighing 1.9 to 3.5 kg wereanesthetized with intraperitoneal injection of pen-tobarbital (Nembutal®, 30 mg/kg), paralyzed withgallamine triethiodide (Flaxedil®, 10-20 mg/kg) andartificially ventilated with room air.
Blood pressure, body temperature and carbon diox-ide were monitored continuously, blood gases andarterial pH monitored intermittently. All measure-ments were maintained in the normal range through-out the experiments.
Reversible air embolism of the brain was producedby injecting 0.6 ml blood foam into the innominateartery proximal to the origin of both common carotidarteries. Foam was used to obtain small air bubbles byshaking 1 ml of heparinized blood in a 2 ml syringefilled with room air. The catheter used for injection ofblood foam was placed into the innominate artery viathe right subclavian artery. The tip of the catheter wasbrought into its correct position as follows: first, thecatheter was advanced into the aorta; this could bemonitored by injecting a bolus of 133Xenon through thecatheter and recording the radioactivity with a scin-tillation detector placed over the abdominal aorta. Asecond detector was then placed over the carotidartery, and the catheter was withdrawn stepwise untilinjection of Xenon resulted in an increased radioac-tivity only over the carotid artery, but not over the ab-dominal aorta. This occurred as soon as the tip wasdistal from the origin of the innominate artery at theaorta and proximal to the origin of the commoncarotid arteries. The correct placement was also con-trolled visually at the end of the experiment.
Blood foam was injected into the innominate arteryover a period of 10-15 sec.14 The catheter subse-quently was rinsed with blood and saline to remove therest of the air. Since the catheter was distal from theorigin of both carotid arteries, air embolism affectedboth hemispheres.
Extent and duration of embolism was followed byvital microscopy of the cortical surface.13 Acraniotomy was made over the gyrus lateralis andgyrus suprasylvius, and microphotographs were takenbefore and at different times after injection of bloodfoam. Changes in the diameter of pial vessels wereassessed on the same photographs and expressed aspercent of control (14 animals). The distribution of airin the brain was also studied by injecting carbon blackinto the innominate artery at 30 sec, 3 min and 50 minafter embolism, respectively (4 animals).
Cerebral Blood Flow
Cerebral blood flow was measured using the follow-ing 3 techniques: 1) A heated thermo-couple16 wasplaced on the frontal cortex, and qualitative changesof cortical blood flow were measured continuously bycalculating the heat conductance (5 animals). 2) Quan-titative determination of cerebral blood flow was per-
formed using the 133Xenon clearance technique.133Xenon was injected as a bolus into the innominateartery, and clearance was recorded using a modifica-tion of the venous sampling technique described byMeyer et al.16 For this purpose sagittal sinus bloodwas shunted into the femoral vein, and radioactivitywas monitored by passing the blood through a glasscoil near a scintillation detector (6 animals). 3) Xenonclearance following intra-arterial bolus injection wasalso monitored by an extracranial detector placed overthe skull after removal of the soft tissues. Theclearance curves were evaluated by biexponentialcurve fitting technique.
Cerebral Metabolic Rate
The cerebral metabolic rate of oxygen, glucose andlactate was calculated at the time of 133Xenonclearance measurements. Arterial-venous differenceswere determined by taking blood samples from thefemoral arteries and from the sagittal sinus. Theoxygen content of the blood was determined using adirect reading oxymeter (Lex-02-Con, LexingtonInstruments Corp., MA), and glucose and lactate bystandard enzymatic analysis. Blood flow was deter-mined by method (2), i.e. the sagittal sinus samplingtechnique, which has the advantage that blood flowwas measured in exactly the same tissue compartmentfrom which the venous samples were drawn (5animals).
ECoG
The electrocorticogram (ECoG) was recordedbilaterally from the frontal regions with bipolar silver-ball electrodes. The ECoG was written on a polygraph(Dynograph RM, Beckman Instruments, Fullerton,CA), and stored on a multichannel analogue taperecorder (Ampex Corporation, Redwood City, CA).Frequency analysis of the ECoG was performed byfast Fourier transform using a laboratory computer(PDP 12, Digital Equipment, Maynard, MA). Thesquare roots of the Fourier coefficients were calculatedto obtain linearity with ECoG amplitude," and the in-tensity of the ECoG was then expressed as the sum ofthese values. An ECoG frequency index was alsocalculated by dividing the ECoG intensity of the beta-and alpha-bands by that of the theta- and delta-bands(5 animals).
PH
Subarachnoid pH was monitored in 5 animals byplacing a flat surface pH combination electrode on thesurface of the parietal cortex (5 animals).
Brain Volume
Brain volume changes were monitored using adevice which has been described by Betz et al.16 Thisconsisted of an induction coil implanted in the skull,and a piston placed on the cortex. The movement ofthe piston was recorded using the induction coil. In-tracranial pressure was recorded with a transducer
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

ARTERIAL AIR EMBOLISM IN CAT BRAIN/Fr/fz and Hossmann 583
connected to the induction coil housing (5 animals).The BBB permeability was studied at different
times after embolism using 4 ml 2% Evans blue inbuffer as the intravascular tracer. The dye circulatedfor 15 min before the animal was killed (11 animals).
At the end of the experiment, the brain was re-moved, one hemisphere was used for the macro-scopical and fluorescence microscopical localizationof extravasated Evans blue, and the other hemispherefor determination of water and electrolytes. For thispurpose the brain was dissected in a moist chamber,and samples were taken from grey and white matter,dried to constant weight and subsequently digested inconcentrated HNO3 (11 animals). Statistical differ-ences were assessed using Student's /-test.
Results
Air Distribution and Recirculation
The time course of air embolism was studied byvital microscopy of the pial vasculature. Air bubblesappeared 35 ± 4 sec (n = 14) after the beginning ofinjecting blood foam into the innominate artery. Themaximum of embolism was reached first in the gyrussuprasylvius which is supplied by the middle cerebralartery and slightly later in the gyrus lateralis which is
80 i
60-o
1 40-uo
^ 20-
0-
Vascular
o
lo
P1 '°
—o o-
embol ism
o-.8 8 " - - - i5 g
340-
280-
g 220-Uo
o
160-
100-
the border zone between the anterior and middlecerebral arteries. There was also a difference betweenthe two gyri during recirculation: air bubbles dis-appeared from the gyrus suprasylvius within 15 min,whereas in the border zone some air was visible up to30 min after embolism (fig. 1).
The distribution of air in the brain was further in-vestigated by intra-arterial injection of carbon black.One minute after embolism, air was distributed allover the brain. After 3 min the the pial vasculature ofthe middle part of the lateral gyrus was still com-pletely embolized, the middle part of the pyriformlobe partly embolized. Both regions are border zonesbetween the arterial territories in which the perfusionpressure is lowest. The rest of the hemispheres showedno filling with air. Fifteen min after embolism thewhole brain was reperfused with the exception of a fewvessels in the lateral gyrus.
Changes in the Diameter of Pial Arteries
Pronounced vascular dilation occurred 3-4 minafter the beginning of embolism. Dilation reached amaximum of 150-260% of control after 10-15 min.Subsequently, the pial arteries gradually constricted;in a few vessels normal vascular tone returned within
Diameter of pial arteries
30 60 90 120min 30 60 90 120min
en
180-1
160-
140 -
120-
100-
Mean arterial blood pressure
I I
t 30 60 90 120min
7.4 -i
73-
7.2 -
7.1 -
7.0-
Cortical pH
t 30 60 90
FIGURE 1. Embolism of the cat brain by injection of 0.6 ml air into the innominate artery(arrow). Above left: Time course of embolism. Values represent the percentage of air-filledvessels in a representative experiment (solid line: gyrus suprasylvius; broken line: gyruslateralis). Right: Changes in the diameter of pial arteries after embolism (values of 2 repre-sentative animals). Triangles: control: circles: embolism. Below left: Changes of mean arterialblood pressure after embolism. Right: Changes of cortical pH after embolism. Means ±SE.Closed symbols: statistically different from control, p < 0.01.
120min
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

584 STROKE VOL 10, No 5, SEPTEMBER-OCTOBER 1979
60 min, but mostly vasodilation of about 40% was stillpresent after 2 hours (fig. 1).
Cerebral Blood Flow
Measurement of cerebral blood flow revealed quitedifferent results depending on the technique used (fig.2). Heat conductance fell by 2.05 ± 0.6 X 10"4
cal X cm1 X sec'1 X "C"1 (n = 5) immediately afterembolism. Subsequently, it improved with a slightovershoot of 1.24 ± 1.03 X 104 cal X cnr1 Xsec"1 X "C"1 (n = 5) at 12 min. Normalization or adecrease below control value came after 1-2 h (fig. 2).
This time course differed from the measurementsmade by sampling venous blood from the sagittalsinus following intraarterial 133Xenon injection. Therewas considerable hyperemia with peak flow rates of200-300% of control 5 min after embolism. Subse-quently, flow gradually decreased and returned to nor-mal after 1-2 h (fig. 2). The flow values obtained byextracranial monitoring of 133Xenon clearance, were inbetween. There was an average increase of 154% after5 min, and normal flow rates during the rest of the ex-periment.
The reason for the differences between the 3methods could be clarified by injecting 133Xenon im-mediately before embolism (fig. 3). Using the external
CBF (thermocouple)
Control Air embolism
o -2 -(J
I 30
CBF (133xenon)
60 90 120 min
£
oo
240 i
180
120 H
30 60 90 120 min
FIGURE 2. Changes of cerebral blood flow after embolismof the cat brain. Above: local heat conductance of the cor-tex. Below: clearance of intra-arterially injected 133Xenon.Solid line: sinus probe; broken line: external probe.Means ±SE Closed symbols: statistically different fromcontrols, p < 0.05. Note the different flow values obtainedby the various techniques (for explanation see text).
'* external probe
sinus probe
external probe
*>' sinus probe
3 min 3 min
FIGURE 3. Comparison of133Xenon clearance before andduring air embolism using the external and the sinus probe.Note transient flattening of the clearance curve recorded bythe external probe after embolism (arrow).
detector, Xenon clearance slowed down in parallelwith the decrease in heat conductance, but there wasan acceleration of clearance when Xenon activity wasmeasured simultaneously in blood withdrawn from thesagittal sinus. This is explained by the fact that boththe external probe and the thermocouple recordedblood flow from the whole tissue whereas the sinusprobe received blood only from those areas whichwere still perfused after embolism. Air embolism con-sequently leads to grossly inhomogenous perfusionwith reduced blood flow in some and increased flow inother regions.
Cerebral Metabolic Rate of Oxygen, Glucose, Lactate
During the initial 30 min after embolism, theabsence of steady state conditions resulted in con-siderable scatter of values. The tendency was a rapidincrease in glucose uptake and lactate clearance and adecrease in the metabolic rate of oxygen during the in-itial 15 to 30 min (fig. 4). Since the metabolic rate ofoxygen immediately after embolization was relativelylow and blood flow increased (see above), venoushyperoxia developed, and the arteriovenous oxygendifference fell to as low as 2 ml/100 ml (fig. 4).
Cortical pH
Cortical pH following embolism decreasedsignificantly from 7.33 ± 0.03 to 7.03 ± 0.05 (n = 5)within 4-5 min, followed by gradual normalizationwithin one hour (fig. 1). Subsequently, it slightlydecreased which, however, was a methodological errorbecause the same shift was observed in controlanimals.
Electrocorticogram
Air embolism led to a flattening of the electrocor-ticogram (ECoG) within 15 sec (fig. 5). Frequencyanalysis revealed that ECoG intensity in the alpha,beta and theta bands decreased to about 20-30% ofcontrol, followed by a gradual recovery to 50-70%after 30-60 min. Intensity of the delta band returnedto 80% within 5 min, but then gradually decreased to60% after 60 min (fig. 6). The relatively higher inten-
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

ARTERIAL AIR EMBOLISM IN CAT BRAIN/Fn7z and Hossmann 585
A-VDO-,
12
8Eo°
60 90 120 min
t 30 60 90 120 min
FIGURE 4. Changes of arterio-venous difference of oxygen(A-VDO2) and cerebral metabolic rate of oxygen (CMR03)after air embolism. Means ± SE. Closed symbols:statistically different from controls, p < 0.005.
sity in the faster frequency bands resulted in an in-crease of the frequency index indicating that at longerrecirculation times the ECoG became faster.
In one animal the ECoG was recorded si-multaneously in the gyrus suprasylvius and the gyruslateralis, and compared with the time course ofvascular embolism in both gyri (fig. 7). The gyrussuprasylvius is in the center of the supplying territoryof the middle cerebral artery whereas the gyruslateralis is the border zone between the middle andanterior cerebral arteries. Wash-out of air bubblesfrom the gyrus suprasylvius began 5 min after em-bolism and was reflected by the fast recovery of theECoG in this area. This was in contrast to the border
zone in which both air embolism and suppression ofECoG lasted considerably longer (fig. 7).
Brain Volume and Intracranial Pressure
Within 45-60 sec the brain began to swell; after 2min a peak displacement of the cortex of 160-260 nwas reached. Brain volume then gradually decreasedbut was still above normal after 15-20 min. Controlsdid not change more than ±39 n. Intracranial pressurerose from 3.6 ± 1.2 to 12.3 ± 2.0 mm Hg (n = 3) at45 sec, and decreased to 6.5 ± 0.75 mm Hg after15-20 min (fig. 8).
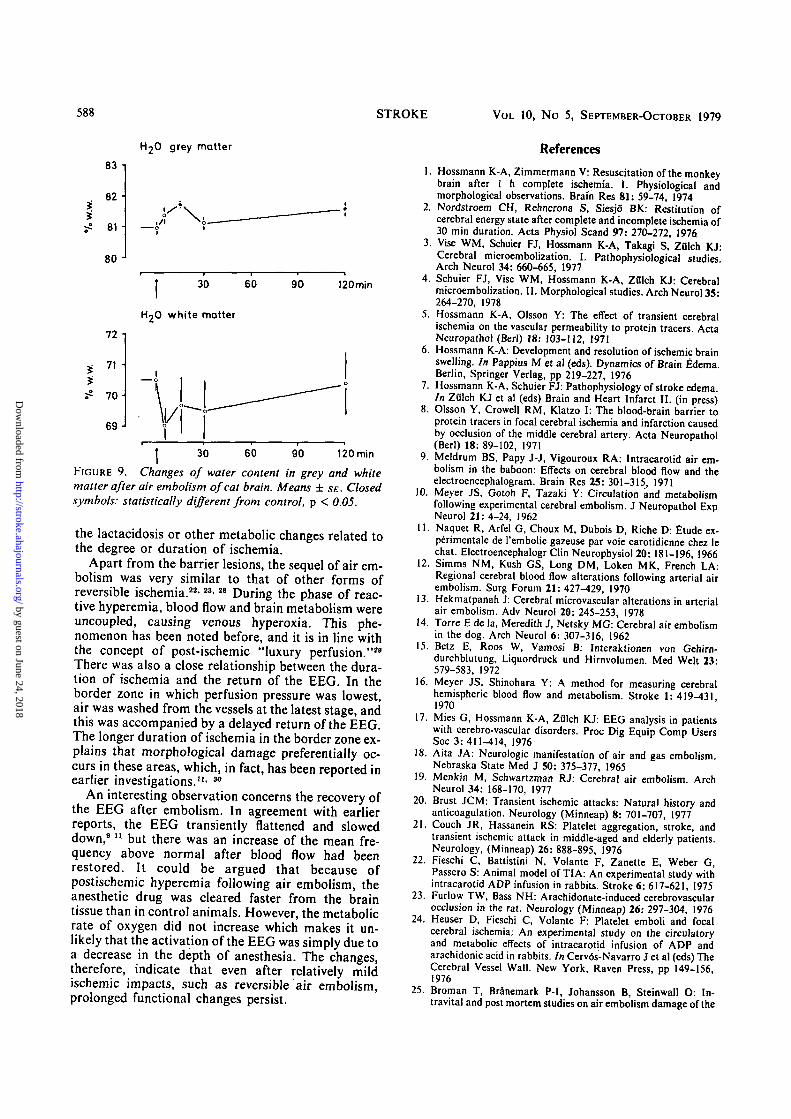
Brain Water and Electrolytes
Water content of the grey matter increased from81.0 ± 0.1 to 81.7 ± 0.1 (n = 3) 15 min after em-bolism, followed by a normalization after 30 min andsecondary increase after 2 h (81.6 ±0.2; n = 8).Water content of the white matter changed in the op-posite direction, but this decrease was not statisticallysignificant (fig. 9). Sodium and potassium increased inboth grey and white matter, reaching a maximumafter 5 min. These changes were not statisticallysignificant and presumably were due to an increase inblood volume during the phase of reactive hyperemia.
Blood-Brain Barrier
The permeability of the blood-brain barrier toEvans blue was not severely disturbed. Macroscopicalexamination revealed not more than a few very smallfaint blue spots in brain recirculated for 30 or 60 min.These spots were due to slight extravasation of thetracer around a few vessels, as detected byfluorescence microscopy (n = 4). At 15 min, or 2 hfollowing embolism, neither macroscopic nor micro-scopic damage was present (n = 7).
Discussion
The most important clinical counterparts to thepresent experimental situation are decompressionsickness and accidental air embolism in vessel
EEG
thermocouple
SAP
]300pV
o
u13 '
1211 -
10300
200100
' U0)in«_lll
uK
•S'o"
enXEE
FIGURE 5. Relationship between blood flowand electrocortical activity after air embolism.Assessment of blood flow by heat conductance(thermocouple). EEG: electrocorticogram,SAP: systemic arterial blood pressure.
1 min
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

586 STROKE VOL. 10, No 5, SEPTEMBER-OCTOBER 1979
10080 •
60 •40-20-
0-
100 n806040-20-0
10080-60-40-20-0-
Total power
30 60 90
Delta band
30
Alpha band
60 90
t 30 60 90
120 min
120 min
140-120100-8060-40-
10080 -I604020-0-
10080-604020
0 J
120 min
Frequency index
30
Theta band
30
Beta band
t 30
60
60
60
90
90
90
120min
120min
120 min
FIGURE 6. Fourier analysis of the electrocorticogram at different times after embolism(arrow). Values are expressed as percent changes of pre-embolic recordings. Triangle: controls;circles: embolism. Means ± SE. Closed symbols: statistically different from controls, p < 0.05.
catheterization.18' 19 During the early development ofextracorporeal circulation, several such accidentsstimulated experimental investigation of air em-bolism, and most of the knowledge about thepathological sequel has been accumulated since then.
Another clinical counterpart is transient ischemicattack (TIA).20-21 There is good evidence that mostTIAs are due to microembolism of the cere-brovascular bed with blood constituents which, after ashort period, are dissolved and washed out from thecerebral vasculature. This situation has beenmimicked by producing intravascular plateletaggregates with adenosine diphosphate or arachidonicacid which, however, also cause peripheral effectsresulting in severe hypotension.22"24 As demonstratedin the present series of experiments, air embolism doesnot have this side effect, and therefore may be a betterexperimental model for such attacks.
Besides its clinical aspects, air embolism is of in-terest for the understanding of the pathophysiology ofischemic brain damage. There is a strange relationshipbetween ischemia and BBB lesions which seems to de-pend on the site of the vascular occlusion. When totalblood flow to the brain is completely interrupted,barrier damage is absent even when other barrierbreakers, such as hypertension, supervene.5 On theother hand, embolism in a relatively small number ofcapillaries with 15 micron microspheres is im-
mediately followed by severe BBB damage, even whenthe total flow through the brain is not compromised.4
Air embolism apparently is between these 2 extremesituations: in some earlier experiments barrier lesionshave been observed11' 25~27 but in the present investiga-tion they were almost absent.
All 3 ischemic models — complete ischemia,microembolism, air embolism — have in commonsevere cerebral blood acidosis causing vasoparalysis ofthe vascular bed. When the brain is recirculated aftercomplete ischemia, the vascular bed is patent, andsince the vessels are dilated, considerable hyperemiaensues.28-29 As long as a no-reflow phenomenon can beavoided, this type of hyperemia is homogenous. Inmicroembolism, part of the capillary bed is per-manently occluded but there is increased flow throughthe non-occluded capillaries causing inhomogenousperfusion at the microcirculatory level.3 In air em-bolism, relatively large branches of the cerebralarteries are interrupted leading to transient completeischemia of the peripheral capillary bed. Asdemonstrated in this investigation, there is also con-siderable inhomogeneity of blood flow and hyperemiain the non-occluded vessels, but, in contrast tomicroembolism, redistribution of flow is at the macro-and not at the microcirculatory level. It is thereforesuggested that the barrier lesion depends on themicrocirculatory redistribution of flow rather than on
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from

ARTERIAL AIR EMBOLISM IN CAT BRAIN/Fr;7z and Hossmann 587
12010080604020
160140
12010080
6040
ion
i/i
o
occ
7060
504030
20
100
Gyrus suprasylvius
Total power
t 30 60min
Frequency index
t 30 60min
Vascular embolism
o
120
100
80-
60-
40-
20-
160 •]
140-
120-
100-
8 0 -
60 -
40 -
70-i
60-° 50-| 40-
8 30-!* 20-
10-0-
Gyrus lateralis
Total power
t 30 60min
Frequency index
o o
t 30 60min
Vascular embolism
FIGURE 7. Relationship between duration ofembolism and EEG changes in the gyrussuprasylvius (left) and thegyrus lateralis (right)of a representative animal. Values represent thepercentage of air-occluded vessels, the percentchanges of EEG-intensity (power) and the EEGfrequency index.
30 60min 30 60min
EEG
Brain volume
ICP
[200pV
FIGURE 8. Effect of embolism on the elec-troencephalogram (EEG), brain volume, in-tracranial pressure (ICP) and systemic arterialpressure (SAP). Note the rapid increase inbrain volume.
SAP
Imin
3002 0 0 mm100 Hg
0
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from
588 STROKE VOL 10, No 5, SEPTEMBER-OCTOBER 1979
H2O grey matter
83 -
82 -
81
80
r'
I 30 60
7O white matter
90 120min
72
71 -
70-
69-
I 30 60 90 120 min
FIGURE 9. Changes of water content in grey and white
matter after air embolism of cat brain. Means ± SE. Closedsymbols: statistically different from control, p < 0.05.
the lactacidosis or other metabolic changes related tothe degree or duration of ischemia.
Apart from the barrier lesions, the sequel of air em-bolism was very similar to that of other forms ofreversible ischemia.22'23-28 During the phase of reac-tive hyperemia, blood flow and brain metabolism wereuncoupled, causing venous hyperoxia. This phe-nomenon has been noted before, and it is in line withthe concept of post-ischemic "luxury perfusion."29
There was also a close relationship between the dura-tion of ischemia and the return of the EEC In theborder zone in which perfusion pressure was lowest,air was washed from the vessels at the latest stage, andthis was accompanied by a delayed return of the EECThe longer duration of ischemia in the border zone ex-plains that morphological damage preferentially oc-curs in these areas, which, in fact, has been reported inearlier investigations.11' 30
An interesting observation concerns the recovery ofthe EEG after embolism. In agreement with earlierreports, the EEG transiently flattened and sloweddown,911 but there was an increase of the mean fre-quency above normal after blood flow had beenrestored. It could be argued that because ofpostischemic hyperemia following air embolism, theanesthetic drug was cleared faster from the braintissue than in control animals. However, the metabolicrate of oxygen did not increase which makes it un-likely that the activation of the EEG was simply due toa decrease in the depth of anesthesia. The changes,therefore, indicate that even after relatively mildischemic impacts, such as reversible air embolism,prolonged functional changes persist.
10.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
References
. Hossmann K-A, Zimmermann V: Resuscitation of the monkeybrain after 1 h complete ischemia. I. Physiological andmorphological observations. Brain Res 81: 59-74, 1974
. Nordstroem CH, Rehncrona S, Siesjo BK: Restitution ofcerebral energy state after complete and incomplete ischemia of30 min duration. Acta Physiol Scand 97: 270-272, 1976
. Vise WM, Schuier FJ, Hossmann K-A, Takagi S, ZOlch KJ:Cerebral microembolization. I. Pathophysioloeical studiesArch Neurol 34: 660-665, 1977
. Schuier FJ, Vise WM, Hossmann K-A, ZOlch KJ: Cerebralmicroembolization. II. Morphological studies. Arch Neurol 35-264-270, 1978
. Hossmann K-A, Olsson Y: The effect of transient cerebralischemia on the vascular permeability to protein tracers. ActaNeuropathol (Berl) 18: 103-112, 1971Hossmann K-A: Development and resolution of ischemic brainswelling. In Pappius M et al (eds). Dynamics of Brain Edema.Berlin, Springer Verlag, pp 219-227, 1976Hossmann K-A, Schuier FJ: Pathophysiology of stroke edema.In Zulch KJ et al (eds) Brain and Heart Infarct II. (in press)Olsson Y, Crowell RM, Klatzo I: The blood-brain barrier toprotein tracers in focal cerebral ischemia and infarction causedby occlusion of the middle cerebral artery. Acta Neuropathol(Berl) 18: 89-102, 1971
Meldrum BS, Papy J-J, Vigouroux RA: Intracarotid air em-bolism in the baboon: Effects on cerebral blood flow and theelectroencephalogram. Brain Res 25: 301-315, 1971Meyer JS, Gotoh F, Tazaki Y: Circulation and metabolismfollowing experimental cerebral embolism. J Neuropathol ExpNeurol 21: 4-24, 1962Naquet R, Arfel G, Choux M, Dubois D, Riche D: Etude ex-perimentale de l'embolie gazeuse par voie carotidienne chez lechat. Electroencephalogr Clin Neurophysiol 20: 181-196, 1966Simms NM, Kush GS, Long DM, Loken MK, French LA:Regional cerebral blood flow alterations following arterial airembolism. Surg Forum 21: 427-429, 1970Hekmatpanah J: Cerebral microvascular alterations in arterialair embolism. Adv Neurol 20: 245-253, 1978Torre E de la, Meredith J, Netsky MG: Cerebral air embolismin the dog. Arch Neurol 6: 307-316, 1962Betz E, Roos W, Vamosi B: Interaktionen von Gehirn-durchblutung, Liquordruck und Hirnvolumen. Med Welt 23:579-583, 1972
Meyer JS, Shinohara Y: A method for measuring cerebralhemispheric blood flow and metabolism. Stroke 1: 419-4311970Mies G, Hossmann K-A, Ziilch KJ: EEG analysis in patientswith cerebro-vascular disorders. Proc Dig Equip Comp UsersSoc 3: 411-414, 1976Aita JA: Neurologic manifestation of air and gas embolism.Nebraska State Med J SO: 375-377, 1965Menkin M, Schwartzman RJ: Cerebral air embolism. ArchNeurol 34: 168-170, 1977Brust JCM: Transient ischemic attacks: Natural history andanticoagulation. Neurology (Minneap) 8: 701-707, 1977Couch JR, Hassanein RS: Platelet aggregation, stroke, andtransient ischemic attack in middle-aged and elderly patients.Neurology, (Minneap) 26: 888-895, 1976Fieschi C, Battistini N, Volante F, Zanette E, Weber G,Passero S: Animal model of TIA: An experimental study withintracarotid ADP infusion in rabbits. Stroke 6: 617-621, 1975Furlow TW, Bass NH: Arachidonate-induced cerebrovascularocclusion in the rat. Neurology (Minneap) 26: 297-304, 1976Heuser D, Fieschi C, Volante F: Platelet emboli and focalcerebral ischemia: An experimental study on the circulatoryand metabolic effects of intracarotid infusion of ADP andarachidonic acid in rabbits. In Cerv6s-Navarro J et al (eds) TheCerebral Vessel Wall. New York, Raven Press, pp 149-156,1976
Broman T, Branemark P-I, Johansson B, Steinwall O: In-travital and post mortem studies on air embolism damage of the
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from
ARTERIAL AIR EMBOLISM IN CAT BRAW/Fritz and Hossmann 589
blood-brain barrier tested with trypan blue. Acta Neurol Scand42: 146-152, 1966
26. Lee JC, Olszewski J: Effect of air embolism on permeability ofcerebral blood vessels. Neurology (Minneap) 9: 619-625, 1959
27. Nishimoto K, Wolman M, Spatz M, Klatzo I: Path-ophysiologic correlations in the blood-brain barrier damage dueto air embolism. Adv Neurol 20: 237-244, 1978
28. Hossmann K-A, Lechtape-Gruter H, Hossmann V: The role of
cerebral blood flow in the recovery of the brain after prolongedischemia. Z Neurol 204: 281-299, 1973
29. Lassen NA: The luxury-perfusion syndrome and its possiblerelation to acute metabolic acidosis localized within the brain.Lancet 2: 1113-1115, 1966
30. Brierley JB, Meldrum BS: The nature and distribution of braindamage due to air embolism. In Doin, (ed) L'embolie gazeusedu systeme carotidien. Laboratoires Sandoz, pp 180-183, 1974
Platelet Coagulant Activities in ArterialOcclusive Disease of the Eye
PETER N. WALSH, M.D. , D. PHIL (Oxon.), TULAY KANSU, M.D.,
PETER J. SAVINO, M.D., NORMAN J. SCHATZ, M.D., LARRY E. MAGARGAL, M.D.,
RICHARD E. GOLDBERG, M.D. , AND JAMES J. CORBETT, M.D.
SUMMARY Ischemic optic neuropathy and retinal arterial occlusion are 2 forms of arterial occlusive dis-ease affecting the eye. Reports in the literature suggest platelet hyperactivity in acute arterial occlusive dis-eases affecting other organ systems. Therefore, 14 patients with ischemic optic neuropathy and 17 patientswith central or branch retinal artery occlusion were studied to determine whether platelets have a role in thepathogenesis of these vascular occlusive disorders. The results of the following investigations were no differentin these patients compared with those in 18 control patients with non-vascular eye diseases: prothrombin times,partial thromboplastin times, plasma fibrinogen, factor V, factor VIII, platelet counts and threshold concen-trations of ADP, epinephrine and collagen resulting in secondary platelet aggregation and serotonin release. Incontrast, platelet coagulant activities concerned with the early stages of intrinsic coagulation were significantlyincreased in patients with retinal artery occlusion without hypertension or type IV hyperlipoproteinemia, butgenerally normal in patients with ischemic optic neuropathy and in patients with retinal artery occlusionassociated with hypertension, type IV hyperlipoproteinemia, diabetes mellitus and generalized atherosclerosis.These results are consistent with a platelet contribution to retinal arterial occlusive disease in patients withoutother known contributing factors such as hypertension, serum lipid abnormalities, diabetes mellitus andgeneralized atherosclerosis and may have implications regarding prophylaxis.
Stroke Vol 10, No 5, 1979
ARTERIAL occlusive disease affecting the eye maypresent either as ischemic optic neuropathy or retinalartery occlusion. Ischemic optic neuropathy resultsfrom acute infarction of the optic nerve which receivesits blood supply from the posterior ciliary artery.1 Theetiology of idiopathic ischemic optic neuropathy is un-known.2 In contrast, retinal ischemia due to retinalartery occlusion has been attributed to the occurrenceof platelet-fibrin emboli,8"6 to emboli of atheromatousmaterial,6"10 to hemodynamic factors or to circulatoryobstruction proximal to the eye.8 In addition, currentevidence suggests that platelets play an important partin the pathogenesis of both atherosclerosis and arterialthrombosis.11
From the Specialized Center on Thrombosis Research and Dept.of Medicine, Temple University School of Medicine (Dr. Walsh),and the Neuro-Ophthalmology Unit (Drs. Kansu, Savino, Schatz,Corbett) and Retina-Vascular Unit (Drs. Magargal, Goldberg),Wills Eye Hospital, Philadelphia, PA.
Reprints: Dr. Walsh, Room 421-OMS, Specialized Center forThrombosis Research, Temple University Health Sciences Center,3400 North Broad St., Philadelphia, PA 19140.
It has been shown that platelets participate in theinitiation of intrinsic coagulation and promote subse-quent intrinsic coagulation reactions that result inthrombin generation.12 Platelet coagulant activitiesconcerned with the initiation and early stages of in-trinsic coagulation were previously found to be in-creased 2-4-fold in patients with transient cerebralischemic attacks and normal serum lipids but not inpatients with transient ischemic attacks associatedwith type IV hyperlipoproteinemia.18 Similar abnor-malities of platelet coagulant activities were alsofound in patients with acute primary retinal veinthrombosis, and normal results were found in patientswith retinal vein occlusion secondary to other dis-eases.14 These observations suggest that platelets con-tribute to the development of acute arterial andvenous occlusive disease in certain patients, but otherfactors such as hypertension, atherosclerosis, serumlipid abnormalities and diabetes mellitus may be moreimportant pathogenetic factors in other patients. Toexamine the possible role of platelets in thepathogenesis of arterial occlusive diseases of the eye,we have studied platelet coagulant activities, platelet
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from
H Fritz and K A HossmannArterial air embolism in the cat brain.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.10.5.581
1979;10:581-589Stroke.
http://stroke.ahajournals.org/content/10/5/581World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 24, 2018http://stroke.ahajournals.org/
Dow
nloaded from