art science tissue viability supplement management of
TRANSCRIPT

art & science tissue viability supplement
Management of tissueexcoriation in older patients withurinary or faecal incontinenceCopson D (2006) Management of tissue excoriation in older patients with urinary or faecalincontinence. Nursing Standard. 21, 7, 57-66. Date of acceptance: August 21 2006.
SummaryThis article discusses good skin care in relation to the managementof incontinence. I t outlines the structure and functions of the skinand describes how the skin changes as we age. It examines howincontinence can damage the skin and provides an overview of thecurrent management methods that are used to prevent tissueexcoriation. It also suggests an effective alternative that could beused if previous strategies have failed and the skin beginsto breakdown, that is, the use of a silver regimen.
AuthorDale Copson is tissue viability nurse specialist, NottinghamUniversity Hospitals NHS Trust, Nottingham-Email: [email protected]
KeywordsOlder patients; Skin care; Tissue viability
These keywords are based on the subject headings from the BritishNursing Index. This article has been subject to double-blind review.For related articles and author guidelines visit our online archive atwww.nursmg-standard.co.uk and search using the keywords.
THE SKIN is the largest body organ and one ofthemost important (Torcora and Anagnostakos 1990,Gawkrodger 1997). It is an outer protectivecovering that is usually unbroken. It has a surfacearea of approximately l.Sin'nnd weighsapproximately 3kg. It hosts a variety of appendagessuch as blood vessels, nerves., swear glands,sebaceous (oil) glands and sensory receptors,makingir a complex and multifunctional organ.
The skin varies in its thickness depending onthe region of the body; it is thinner over theeyelids (0.6mm) and thicker (3mm or more) onthe back, palms and soles {Gawkrodger 1997,Stephen-Haynes and Gibson 2003). It consists ofthree separate layers, the epidermis, dermis andsubcutis (Figure I). These distinct layers areattached to each other, but arc segregated by anundulating or wavy borderline known as the Reteridge (Powell and Soon 2002).
NURSING STANDARD
The epidermal layer is the rough outer surfacethat consists of many layers of epithelial celis. Asnew epithelial cells are made the old ones die andslough (iff the skin, providing an impermeable yetrenewable barrier. The epidermis is maintainedby diffusion as nutrients contained in interstitialtissue fluid pass through the dermal blood vessels.This process supplies the epidermis with essentialvitamins, minerals and oxygen for regeneration.
The underlying dermal layer is vascularconnective tissue that receives one third ofthebody's circulating blood volume (Flanagan andCulieyl996).
The subcutis, often referred to as subcutaneoustissue, provides support for the dermis andconsists of adipose (fat) tissue, connective tissueand blood vessels (Gawkrodger 1997, Graham-Brown and Bourke 1998).
Healthy skin serves several purposes: itprotects the internal organs chemically, physicallyand biologically (Stepheii-Haynesand Gibson2005) (Box 1). Skin secretions and melaninprovide chemical protection. A plethora ofcommensal bacteria and yeasts cover the skin'ssurface; the acidity ofthe skin's secretions reducestbeir proliferation and controls possibleovergrowth. It has also been suggested thatsebum (an oily substance secreted by thesebaceous glands) contaitis chemicals that candestroy some bacteria. Melanin is a chemicalpigmentthat protects vulnerable tissue fromover-exposure tothe sun's harmful ultravioletrays (Graham-Brown and Bourke 1998). Theepidermis is hard, wbich means that the skin alsoprotects against physical and mechanical damagesuch as abrasions or accidental injury. It alsoprevents the diffusion of water and/or water-soluble compounds (electrolytes and proteins),thus safeguarding both their loss out of and entryinto the body (Mairis 1992).
The skin controls the body's temperaturethrough a process called thermoregulation(Tortora and Anagnostakos 1990). For example,
October 25 :: vol 21 no 7 :: 2006 57

art & science tissue viability supplement
when there is a decrease in the externaltemperature and the skin becomes cold, thedermal vessels constrict keeping; blood closer tothebody'score. We may Starr to shake togenerate heat energy and experience 'goosebumps'; these are caused by the erector pilimuscles contracting, forcing tbe bairsto stand onend to provide an insulatinglayerof air attbesurface of the skin. These responses are anattempt to conserve body beat and maintain asafe body temperature {Toole and Toole 1991).
Alternatively, when the external temperaturerises, tbe dermal blood vessels dilate and ourappearance may become flushed as blood passescloser to the surface ofthe skin. The swear glandsmay increase their secretory activity, resulting inincreased perspiration (sweating). The arrectorpili muscles relax, causing the hairs to lie fiat. Acooling effect is obtained when sweat evaporatesoff the surface of the skin, thus preventing usfrom overheating (Clark 1993).
Tortora and Anagnostakos (1990) note tbatremoval of waste products is made easier by tbeskin. Although the majority of nitrogen-containing waste Is expelled from tbe body asurine, small amounts of urea, uric acid andammonia are excreted from the body in sweat.
Tbe skin plays a pivotal role in tbe syntbesis ofvitamin D. Epidermal cells contain molecules ofcbolesterol, which can be irradiated byultraviolet ligbt and converted to vitamin D(Tortora and Anagnostakos 1990). Vitamin D iscarried in the derma! vessels to other parts of tbebody and plays a precursory role in calciummetabolism, since calcium cannot be absorbedwitbout tbis vitamin.
The skin allows us to detect external stimulithrough touch, prL'ssurc and pain. The skincontains numerous nerve endings and tactilereceptors. If activated, the receptors sendimpulses to the brain to evaluate whetber a tactileresponse is required (Clark 1993). Forexample,if we were to toucb an extremely bot object, tbetactile response from the brain would be toinstantaneously remove the part of tbe body incontact with tbe heat source to prevent skindamage.
In summary, the skin is a metabolically activeorgan. Unlike most other organs in tbe body, itscells are constantly dying and being replacedtbrougbout life, itconsists of tissues structurallyjoined together to perform specific tasks.
Maintaining skin integrity is a complexprocess and one tbat is often taken for granteduntil damage occurs. Skin damage can bappeneasily in many different ways, and whatever tbecause, the end result is often a wound. Whenwounds occur tbe protective function of tbe skin
FIGURE 1Structure of the
Sweat duct Hair shaft Arrector pili muscle
Stratum corneum
{horny layer)
Stratum granulosum
(granular cell layer)
Stratum spinosum
(prickle cell layer)
Stratum basale
{basal cell layer)
Cutaneous circulation
Nerve fibres
Sweat giand
Sebaceous gland
Hair follicle
58 October 25 :: vol 21 no 7:: 2006 NURSING STANDARD

art & science tissue viability supplement
is breached. It is therefore importanr to close thedefect as quickly as possible, thereby preventinginfection and iillowing normal skin function tooccur (Timmons 2006).Skin and ageing There are a number of factorsthat may aftect skin function (Holloway andJones 2005), all of which may be exacerbated byageing. As we get older the skin undergoes manystructural changes, which may make it susceptibleto disease and damage. Such changes include(Desai 1997):
• Thinning of the epidermis.
• Reduced vascularity.
y Reduced elasticity.
• Dehydration due to loss of water contetit.
• Decreased sensation.
• Reduced sebum production.
Alt of these changes have the potential to impedethe skin's primary function of protection.Furthermore, this protective function can berapidly weakened if the individual experiencesbouts of faecal and/or urinary incontinence.
Incontinence and its effect on skin
Involuntary loss of control ofthe bladder, bowelsor both, more often referred to as incontinence(Clooper and Gray 2001), is a condition thatmainly affects older patients (Department ofHealth (DH) 2000). It has been suggested thatfaecd! incontinence may affect 1 per cent ofadults in their own home and one in four innursingand residential accommodation (DH2000). Recent data .suggest chat .50 percent ofnursing home residents in Britain and NorthernIreland have urinary incontinence (Durrant andSnape 2003). Bale etal (2004), in a study of olderpatients cared for in a nursing home, found that
Main functions of the skin
• Protection
• Immunity
• Excretion
• Temperature regulation
• Reception of stimuli
• Synthesis of vitamin D
(Tortora and Anagnostakos 1990)
FIGURE 2
Severe excoriation as a result of urinary andfaecal incontinence
29 per cent of residents were incontuient of urine,65 per cent were doubly incontinent and 6 percetit were catheterised. Little evidence exists ofthe prevalence of incontinence in the acutesetting (Lyder 1997, Hughes2002). Skincareofincontinent patients is a significatit challenge forpractitioners (Cooper 2000).
Continuousorprotonged exposure of the skinto urine and/or faeces can result in loss of barrierfunction and epithelial breakdown. This is dueto rhe skin becoming too moist and fragile(macerated) and changes in its pH (Gray?/J/2002).ThepHof healthy skin is usually between4.0 and 5..5 (Cooperand Gray 2001), making itslightly acidic and inhibitingthe growth ofbacteria (Anthony 1993}.The mixture of urineand faeceson the skin alters the pH, making itmore alkaline and ideal for bacterialproliferation (Neander 1990). The prolongedeffects of this can result in local dermatitis, tissueexcoriation (Figure 2), irritation and/or pain, anincreased risk of pressure ulceration and possibleinfection (Rcrge/*?/1986, Barbenelefd/1997,Cooper 2000).
Management of compromised skin
The first and most common method of managingthe skin of incontinent patients is with soap,warm water, a flannel or soft wipe and towel todry. It is still not known what effect watertemperature has on the integrity of chc skin{Voegeli 2005). For the patient who hasoccasional incontinence this method may beacceptable. However, the frequency of washingwill be increased ifthe patient is continuouslywet and/or soiled. For this reason practitionersshould be aware of the potential detrimentaleffects that some soaps may have on the skin.
Most soaps are known to have a drying effectbecause they decrease the natural sebum contentof the epidermis (Cork 1997). They may alsoleaveresidueson the skin and if they are
60 October 25 :: vol 21 no 7 :: 2006 NURSING STANDARD

art & science tissue viability supplement
perfumed there is rhe possibility of chemicalirritarion, which may lead to skin breakdown{Wort/.man l99KKirsnerandFroelich 1998}.Friction damage from repeatedly drying the skinafter cleansing may also reduce the integrity ofthe epithelium, thus exacerbating the problem{Huh etallQQl). Therefore, if soap is to be usedto cleanse the skin of an incontinent patient, amild, pH-balanced and non-scented productshould be used, for example, baby soap orshampoo.
Foam cleansers are another popular productadvocated in healthcare settings (Cooper 2000),Cooper and Gray (2001) found these productswere far better at maintaining the skin ofincontinent patients than soap and water. Theyreduced the potential for friction damage, as wellas preventing the skin from drying out because oftheir emollient concent, which moisturised theskin thus maintaining its hydration aftercleansing. However, it is recommended that thepractitioner understands how these productsshould be used because a common error observedin clinical practice is the incorrect application ofthe foam. The simple mistake of applying thecleanser onto a soft wipe instead of directly ontotbe patient's skin is often made. By doing this thepractitioner will reduce tbe efficacy of theproduct because it must be in contact with theskin if it istoreducethepHandrehydrateandmoisturise it.
Barrier creams are often used in conj unctionwith a suitable cleansing regimen, for example,Sudocrcm®, Metanium® and Cavilon® DurableBarrier Cream. These are topical preparationsmanufactured to provide a protective harrierbetween the skin and the irritant effects of urineand/or faeces. This barrier is achieved byapplying a thin layer over compromised skin andintact skin that is at risk of tissue damage.However, over-application of these products mayreduce the effectiveness of continence pads ifworn by clogging or interfering with tbcirabsorbency (Williams 2001. Newton andCameron 2005), thus increasing the risk ofmaceration and possible excoriation.
Protection of broken skin may be achievedthrough the use of a film barrier, for example,Cavilon® No Sting Barrier Film, an alcohol-freeskin protector that, once applied, can last for upto 72 hours (Williams 1998). In many cases thisproduct is effective in managing damaged skin.However, if the patient has antibiotic orparenteral nutrition-induced faecal incontinenceor Closiridittm difficile., he or she can be washedseveral times an hour. The question to be asked in
these situations is 'bow often should Cavilon® beapplied?'
Faecal collectors are useful in tbese situations,however, not every patient is suitable for orwilling to bave these devices fitted. For this reasonNottingham University Hospitals NHS Trust basadopted an alternative approach to managingskin excoriation caused by incontinence.
An alternative approach to managingexcoriation
62 October 25 :: vol 21 no 7 :: 2006
When asked to describe the feeling of tissueexcoriation to tbe tissue viability nurse, manyolder patients describe it as 'an agonising burningsensation', 'dreading tbe thought of beingcleanedagain','Ican't bear to be touched'and '1just want the pain to go away'. As excoriation iscaused by a chemical reaction damaging thesurface of tbe skin (Cooper and Gray 200!), theeffect is, in essence, a chemical burn.
For many years burns patients have beentreated with a cream containing silver, which isrenowned for its broad-spectrum antimicrobialproperties (Russell and Hugo 1994, Lansdown2002a,Tboniasand McCubbin 2003).Flamazine® is a common example. It is a whitecreamcontainingsilversulfadiazine 1% w/vinasemi-solid oil in water emulsion. Its maintherapeutic indications are for the prophylaxisand treatment of infection in burns wounds (Holt1998,Howell 1998). it is also used in thetreatment and management of leg ulcers andpressure ulcers and abrasions (British NationalFormulary 2006).
Locally, this product has been successful inrapidly reducing tbe effects of tissue excoriationassociated with incontinence. However, there isno publisbed evidence to date tbat promotes theuse of silver sulfadiazine 1% cream for thiscondition.
After every episode of incontinence the skinshould be gcntlyclcanscdwith an appropriatecleansing agent and allowed to dry. A thin layerof Flamazine® cream should then be applied tothe affected atea(s); this should be carried outafterevery incontinent episode, or up to fourtimes a day until general cleansing or barriercreams or films c;ui be used to manage tbeproblem. If, after two weeks, the problem is notresolving tben an alternative method ofmanaging the incontinence should be sought, forexample, a faecal collection system orcatheterisation, if this has not previously beenconsidered. The benefits of using this product areusually observed in 24 to 48 hours, and mostpatients will state that they feel much morecomfortable and that the pain bas reduced.
Generally, silver sulfadiazine is well tolerated,but there have been occasional teports of
NURSING STANDARD
art & science tissue viability suppletnent
irritancy,argyria (staining, a dull blue or greycolouration of the skin) and associated stinging(Lansdown and Williams 2004). However, this ismore common when using silver nitratecompounds (Lansdown 2002b). To besystemically roxic. silver must be absorbed insufficient amounts to evoke irreversible changesin a target organ such as the kidney or liver.Coombes etal (1992) documented that therewere no measurable changes in serum silverlevels (normal level less than2.3mcg/l) in twovolunteers exposed to daily topical applications(3-5mm depth) of silver sulfadiazine for twoweeks. As only a thin layer (less than 1mm depth)of cream is applied to the incontinent patientusing the Flama/ine® regimen, it could be arguedthat the risk of high levels of silver beingabsorbed systemically is low.
Flamazine® is relatively thin in texture. Theadvantage of this is that it is almost painless onapplication and a small amount can be spreadover a large area. It also provides a soothingeffect (Kagan and Smith 2000). The risk ofinfection is also reduced because oftheantimicrobial propertiesof tbe silver in thecream. An example of the benefits oftheFlamazine® cream method is outlined in Box 2.Figure 3 shows the skin before the application of
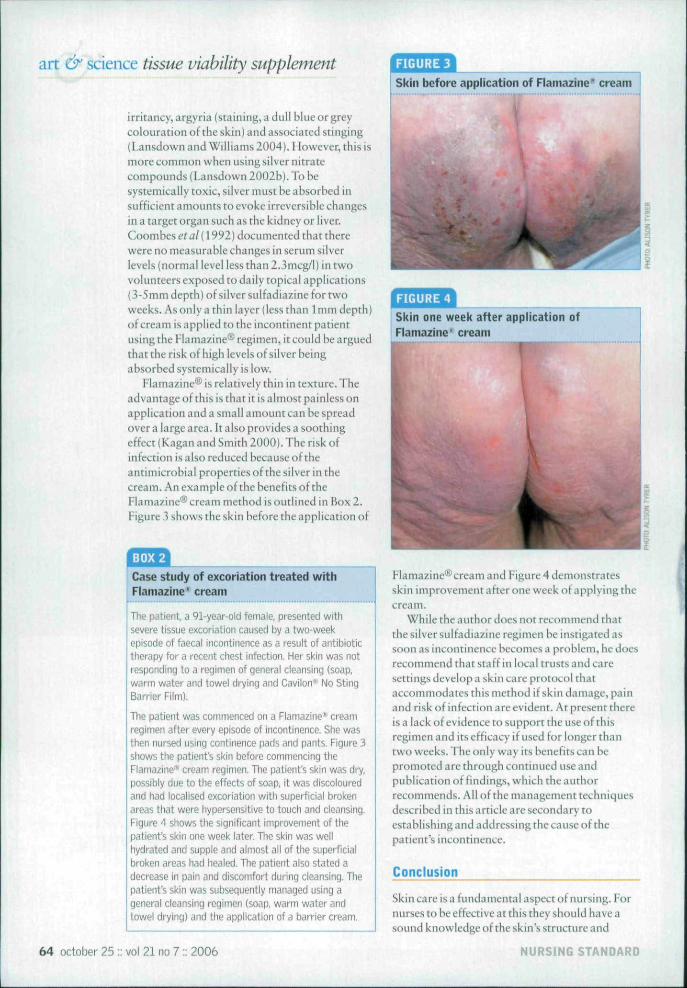
riGURE3Skin before application of Flama2ine^ cream
Skin one week after application ofFlamazine" cream
Case study of excoriation treated withFlamazine' cream
T i l . 1 1 91-year-old female, presented wil l isevere tissue excoriation caused by a two-weekepisode of faecal incontinence as a result of antibiotictherapy for a recent chest infection. Her skin was notresponding to a regimen of general cleansing (soap,warm water and towel drying and Caviion-- No StingBarrier Film).
The patient was commenced on a Flamazine''' creamregimen after every episode of incontinence. She wasthen nursed using continence pads and pants. Figure 3shows the patient's skin before commencing theFlamazine* cream regimen. The patient's skin was dry,possibly due to the effects of soap, it was discolouredand had localised excoriation with supei-ficial brokenareas that were hypersensitive to touch and cleansing.Figure 4 shows the significant improvement of thepatient's skin one week later. The skin was wellhydrated and supple and almost all ofthe superficialbroken areas had healed. The patient niso stated adecrease In pain and discomfort during cleansing. Thepatient's skin was subsequently managed using ageneral cleansing regimen (soap, warm water andtowei drying) and the application of a barrier cream.
FIama7-ine®cream and Figure4 demonstratesskin improvementafterone week of applying thecream.
While the author does not recommend thatthe silver sulfadiazine regimen be instigated assoon as incontinence becomes a problem, he doesrecommend that staff in local trusts and caresettings develop a skin care protocol thataccommodates this method if skin damage, painand riskof infection are evident. At present thereis a lack of evidence to support the use of thisregimenanditsefficacy if used for longer thantwo weeks. Tlie only way its benefits can bepromoted are through continued use andpublicationof findings, which the authorrecommends. All of the management techniquesdescribed in this article are secondary toestablishing and addressing the cause ofthepatient's incontinence.
Conclusion
Skin care is a fundamental aspect of nursing. Fornurses to be effective at this they should have asound knowledge of the skin's structure and
64 October 25 ;: vol 21 no 7:: 2006 NURSING STANDARD

art & science tissue viability supplement
function. They also need to be aware of skinchanges as a result ofthe ageing process, and thedamage that faecal and/or urinary incontinencemay cause to the protective function that tbe skinprovides. The mainstay of treatment formanagingcompromiscdskiniswitha mild
pH-balanced soap, warm water and a soft wipe.However, other methods are available if the skinbecomes further compromised, for example,barrier creams and films. Tbis article provides anoverview of the current management methodsthat could be used to prevent tissue excoriation. Italso suggests the use of silver sulfadiazine1 % cream as a simple yet effective alternative thatcould be used if previous strategies bave failedand the patient's skin begins to breakdown NS
References
Anthony D (1993) The assessment>.'[ \\v skill of the Hclerly patientwith ^iK'i.ifir reference to rteciibitusulcers and incontinence demitititis.Journal of Tissue Viability. 3, 3,85-93,
Bale S, Tebble N, Jones V, Price P(200'1) Tlie benefits ofiriipieinefitinc) a new skin eveprotocol in nursing homes. Journalof Ti5->i/c Vicibilily. 14, 2. 'I'l-SO
Barbenel JC, Jordan MM, NicolSM, Clark MO (1997) Incidence dpressure sores in thp GreaterGlasgow Health Board area. TheLancet 2, 8037, 548-550,
Berg RW, Biickingtiam KW,Stewart RL n')«6) Etiologicfarlf.ii'i in di,̂ |)l•|• dermatitis: the roleof urine, Paediatric Dermatology. 3.2,102-106,
British National Formulary(2006) Bnb'ih National FormularyNo 51 Si-itish Medical Associationand Royal Pharmaceutical Societyof Great Britain, London.
Clark RA (1993) Biology of dermalwoLind repair Dennatologic Clinics.11, 4, 647-666.
Coombes CJ, Wan AT,Masterton JP, Conyers RA,Pedersen J, Chia YT (1992) Doburn patients litwc a silver lining?Burn', 18. 3,179-184,
Cooper P (2000) The use ofClinisan in the skin care of theincorttiiienl patient. British Journalof Nursing. 9, 7. 445-448,
Cooper P, Cray D (2001)Comparison of two skin careregimes for incontinence, BritishJournal of Nursing. 10, 6 SuppI,S6-S20
Cork M (1997) The imporlarice ofskin barrier function. Journal of
Dermatotogical Treatment 8.S7-S13.
Department of Health (2000)Good Practice m ContinenceServices. The Stiitionery Office.London,
Desai H (1997) Ageing and wounds.Part 2: healing in old atje. Journal ofWound Care. b. 5.2i7-239.
Durrant J, Snape J (2003) Urinaryincontinence in imrsing homes forolder people. Age and Ageing. 32.1.12-18.
Flanagan M, Culley F (1996)Prvisure Area Management: TheFacts. Huntleigh Healthcare, Uiton.
Gawkrodger DJ (1997)Micioaiwtomy of Ihe skin. InGawtcrodger OJ (Ed) Dermatology:An lllustrotsd Colour Text. Secondedition. Churchill Livingstone,Edinburgh. 2-3.
Graham-Brown R, Bourke J(1998) Mosb/E Color Atlas and Textof Dermatology. Mosby, London.
Gray M, Ratliff C, Donovan A(2002) Perineai skin care for tlieincontinent patient. Advances inSkin and Wound Care. 15.4,170-178
Hoiloway S, Jones V (2005)The iinportiiMcp of skin care andassessment. British Journal ofNursing. \A. 22. \\72-mb.
Holt L (1998) Assessing andmanaging minor burns. EmergencyNurse. 6.2,14-16.
Howell F (1998) Management ofminor burn injuries, Pivdice Nurse.16, 4, 208-212.
Hughes S (2002) Do continenceaids lielp to maintain skin integrity?Journal of Wound Care. 11, 6.235-239,
Huh CH, Seo KI, Kim SD, Han JH,Eun HC (2002) Biopiiysical changesafter rrtechanical injuiy of thestratum roriieiini in normal skin,Confact Dermatitis. 46,1, 4-28.
Kagan RJ, Smith SC (2000)Evaluation and ti-eatnient ofthermal injuries. Dermatology
. 12,5, 334-350.
Kirsner RS. Froelich CW (1998)Soaps and detergents:understanding their composition andeffect. Ostomy/Wound Management44, 3A SutJpl. 62S-70S.
Unsdown AB (2002a) Silver, L itsantibactpfial properties andmechanism of action. Journal ofWound Care 11,4,125-130
Unsdown AB (2002b) Silver. 2:toisicity in mammals and litw itsproducts aid wound repair Journalof Wound Care. 11,5.173-177
Unsdown AB, WiOiams A (2004)How safi.' IS silver in wound care?Journal of Wound Core. D, 4.Dl-136,
Lyder CH (1997) Perinealtlennatitis in the elderly: a criticalreview of the literature. Journal ofGerontological Nursing- 23,12, 5-10.
Mairis E (1992) Four senses for afull skin assessment: observationand assessment of the skin.Professional Nurse. 7. 6, 376-380.
Neander KD (1990) Dermatologicalaspects of incontinence.Krankenpflege Journal. 28,10,509-513,
Newton H, Cameron J (2005) SkinCare in Wound ManagementMedical Communications UK,Holsworthy.
Powell J, Soon C (2002)Pliysiology of the skin. Surgery. 20.6, ii-'ri.
Russell AD, Hugo WB (1994)Antiinio-obial activity and action ofsilver Progress in MedicinalChemistry. 31, 3, 351-370-
Stephen-Haynes J, Gibson E(2003) Anatomy and Physiology:Wound Healing and WoundAssessment. Educational booklet.Wound Care Society, Huntingdon.
Thomas S, McCubbin P (2003)An in vitro analysis of theantimicrobial properties of 10silver-containing dressings.Journal of Wound Care. 12, 8,305-308.
Timmons J (2006) Skin function.!inl wound healing physiology.Wound Essentials. I 8-17.
Toole G, Toole S (1991)Homeostasis. In Toole G, Toole S(Eds) Understanding Biology forAdvanced Level. Second edition,Stanley Thornes, Cheltenham,534-550,
Tortora GJ, Anagnostakos NP(1990) Tilt? uiieyurnentary systemIn Tortora GJ. Anagnostakos NP(Eds) Principles of Anatomy andPhysiology. Sixth edition. HarperCollins, New York NY. 119-137
Voegeli D (2005) Skin hygienepractices, emollient therapy andskin vulnernbility. Nursing Times.101, 4, 57. 59
Williams C (1998) 3M Cavilon NoSting Barrier Film in the protectionof vulnerable skin. British Journal ofNursing. 7.10,613-615,
Wniiams C (2001) 3M CavilonDurable Barrier Cream in skinproblem management. BritishJournal of Nursing. 10.7, 469-472.
Wortzman MS (1991) Evaluationof mild skin cleansers. DermatologicClinics. 9,1.35-44,
66 October 25 :; vol 21 no 7 :: 2006 NURSING STANDARD
