are current time delays in endovascular treatment of
TRANSCRIPT
Central Journal of Neurological Disorders & Stroke
Cite this article: Mørkenborg ML, Steglich-Arnholm H, Holtmannspötter M, Krieger DW (2015) Are Current Time Delays in Endovascular Treatment of Stroke Acceptable? J Neurol Disord Stroke 3(2): 1099.
*Corresponding authorDerk W. Krieger, Department of Neurology, Copenhagen University hospital, Blegdamsvej 9, 2100 Copenhagen East, Denmark, Tel: 45 28117047, Fax: 45 3545 2626, Email:
Submitted: 28 January 2015
Accepted: 17 March 2015
Published: 18 March 2015
Copyright© 2015 Krieger et al.
OPEN ACCESS
Keywords•Endovascular treatment•Acute ischemic stroke•Time•Outcome•DIDO
Research Article
Are Current Time Delays in Endovascular Treatment of Stroke Acceptable?Marie-Louise Mørkenborg1, Henrik Steglich-Arnholm2, Markus Holtmannspötter3, Derk W. Krieger4*1Department of Neurology, Copenhagen University hospital, Denmark2Department of Neurology, Copenhagen University hospital, Denmark3Department of Radiology, Copenhagen University hospital, Denmark4Department of Neurology Copenhagen University hospital, Denmark
Abstract
Background: Endovascular treatment (EVT) is an attractive treatment modality in acute ischemic stroke (AIS) caused by large artery occlusions. The extreme time-sensitivity of revascularization procedures renders referral logistics critical for therapeutic success. EVT is currently considered in patients with contraindications for or failing to improve with IV-thrombolysis. Door-in-door-out (DIDO) and door-to-recanalization (DTR) intervals are useful to benchmark delays in corresponding coronary interventions with improved outcomes associated with DIDO ≤ 30 minutes and DTR ≤ 120 min according to current guidelines. This study aims to assess DIDO and DTR in patients undergoing EVT and to assess the impact on outcome.
Methods: Retrospective analysis of data and time delays on all consecutive patients transferred from a primary to a comprehensive stroke centre for EVT after failed IV-thrombolysis from June 2011- June 2013
Results: 62 consecutive patients were identified. Stroke severity was NIHSS 16, 2 (+/-5,5). DIDO was 101 min (+/- 36, 9), DTR was 242 min. (+/- 61, 5) and onset to recanalization time (OTR) was 331 min (+/-94). DIDO and DTR improved significantly (p<0,001) over the 2-year period. 3-months outcome correlated only with stroke severity and age.
Conclusion: In this cohort representing current clinical practice no patient was treated within recommended time interval for acute coronary interventions, although significant improvement was demonstrated over the 2-year period. Treatment delays exposed in this study mimic those reported in recent trials failing to show benefit of EVT. A paradigm shift in patient logistics is necessary for EVT to advance clinical outcomes in patients with AIS.
ABBREVIATIONSAIS: Acute Ischemic Stroke; EVT: Endovascular Treatment;
IV-tPA: Intravenous Tissue-Plasminogen-Activator; LAOs: Large Artery Occlusions; RCTs: Recent Randomized Controlled Trials; DTN: Door-to-Needle time; PCI: Percutaneous Coronary Intervention; DIDO: Door-In-Door-Out-time; DTB: Door-To-Balloon-Recanalization; DTR: Door-To-Recanalization; NIHSS: National Institute of Health Stroke Scale; OTR: Onset-To-Recanalization-time; TICI: Thrombolysis In Cerebral Infarction; SD: Standard Deviation.
INTRODUCTIONAcute ischemic stroke (AIS) is one of the leading causes
of death, and more importantly the primary cause of serious disabilities [1]. With the aging population, the number of patients affected and the impact for society at large is expected to increase. Time is of vital importance in maximizing the recovery of salvageable brain tissue in AIS. The particular time-sensitivity of reperfusion makes stratification and transport logistics critical in the treatment chain.
Currently, patients diagnosed with AIS within 4.5 hours of symptom onset are considered for thrombolysis with intravenous tissue-plasminogen-activator (IV-tPA) at non-endovascular treatment (EVT)-capable primary stroke centres (spokes). Patients with intracranial large artery occlusions (LAOs) and no clinical response to IV-tPA are considered for

Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 2/5
secondary EVT (‘IV-IA-bridging’) in compassionate use. In most current settings, if EVT is contemplated the patient is transferred to a comprehensive stroke centre (the hub). This inter-hospital patient transfer in this “hub-and-spoke” organization is very time-consuming, wasting valuable time in the extremely time-sensitive treatment chain.
IV-tPA has shown only limited effect in reperfusion large thrombus load in both anterior and posterior circulation [2], and it is generally assumed that EVT improves clinical recovery in such patients. Unfortunately recent randomized controlled trials (RCTs) [3-5] have failed to prove this. However these trials have been criticized for methodological flaws, such as selection bias, technical limitations, leading to incomplete reperfusion and most and foremost inexcusable time delays prior to initiation of EVT [6].
Secondary analyses of the recent trials have also helped to refine the target population for EVT in terms of advanced CT or MR imaging techniques [7] and clinical and vascular selection criteria [8]. For instance, in patients with confirmed LAOs the combined approach using IV-tPA as bridging therapy during transferral for EVT suggests higher rates of recanalization when compared with IV-therapy alone [9]. The final infarct volume tends to be smaller with EVT compared to either IV-tPA or no-reperfusion therapy and patients with more severe stroke seem to fare better with EVT than IV-tPA [10].
Compared to the first generation devices used in recent RCTs, progress has been made as novel devices are much more effective in achieving rapid and sufficient revascularization [11-13].
Favourable 3-months outcome following technically successful angiographic reperfusion has been shown to be time-dependent [14]. Current accepted benchmarks for in-hospital time delays in the management of acute stroke are only focusing on door-to-needle time (DTN) in IV-tPA but currently no corresponding benchmarks involve primary and secondary EVT.
In order to address the time delays, clinical precedence in interventional cardiology can be reviewed. The corresponding treatment to EVT in cardiology is percutaneous coronary intervention (PCI). Aware that most patients initially present at non-PCI-capable hospitals, Door-In-Door-Out-time (DIDO), defined as the time from admission to discharge at the referring hospital [15] and Door-To-Balloon-recanalization (DTB)-time, defined as time from admission to treatment, were introduced as performance measures in capturing time delays in PCI. DIDO < 30 minutes and DTB ≤120 minutes was significantly associated with improved outcomes [16].The increased awareness and national initiatives by the American Heart Association [17] led to a remarkable reduction of DIDO- and DTB-time in few years [18].
In this study we sought to assess DIDO and Door-To-Recanalization (DTR)-time to capture time delays in patients referred to EVT for AIS, and explores the impact of these delays on patient outcome.
METHODSThis is a retrospective, single-centre study.
Approval from the Danish Data Protection Agency was
granted (j.no. 2013-41-2365).
Approval from the Danish National Committee of Health Research Ethics was not required.
Data collection
All consecutive patients assessed at a primary stroke centre with severe stroke (National Institute of Health Stroke Scale (NIHSS)>=10) and contraindications or no immediate response to IV-tPA referred for EVT (bridging IV-IA-treatment) and transfer red via ambulance to the comprehensive stroke centre from June 2011 to June 2013 were identified.
Patient case histories were reviewed and clinical and radiological data were abstracted from patient charts and electronic databases. Door-In-time at the primary stroke centre was defined as the time of admission. Door-out-time was defined as the time of arrival in the transferring ambulance.
Recanalization-time was defined as time of last angiographic frame after recanalization or procedure failure.
Onset-To-Recanalization-time (OTR) was defined as time from symptom onset to time of recanalization.
Successful recanalization was defined according to the Thrombolysis in Cerebral Infarction (TICI) [19] score as a score of 2b-3.
Favourable outcome was defined as a modified Ranking Scale (mRS) of 0-2 at 3 months.
Statistical analysis
Data is presented as mean +/- standard deviation (SD). Univariate analyses were performed to identify predictors of favourable outcome. Posterior circulation AIS were omitted from this analysis.
P< 0, 05 was considered significant. All statistical analyses were performed using SPSS version 20 (SPSS Inc.).
RESULTSIn the two year period 65 consecutive patients were
identified, of which 3 patients (4,6%) were excluded. 1 patient was unidentifiable, 2 patients with unobtainable data (Figure 1).
Baseline characteristics for the remaining 62 patients are summarized in (Table 1).
The mean age was 65, 5 (+/-13, 1) years, 27 (44 %) were males, mean NIHSS was 16 (+/-6).
6patients (9,7%) were not treated with IV-tPA, 3 patients because of concurrent anticoagulant treatment, one patient because of recent head trauma, one patient outside IV-tPA time window and one patient because of a suspected intracranial haemorrhage.
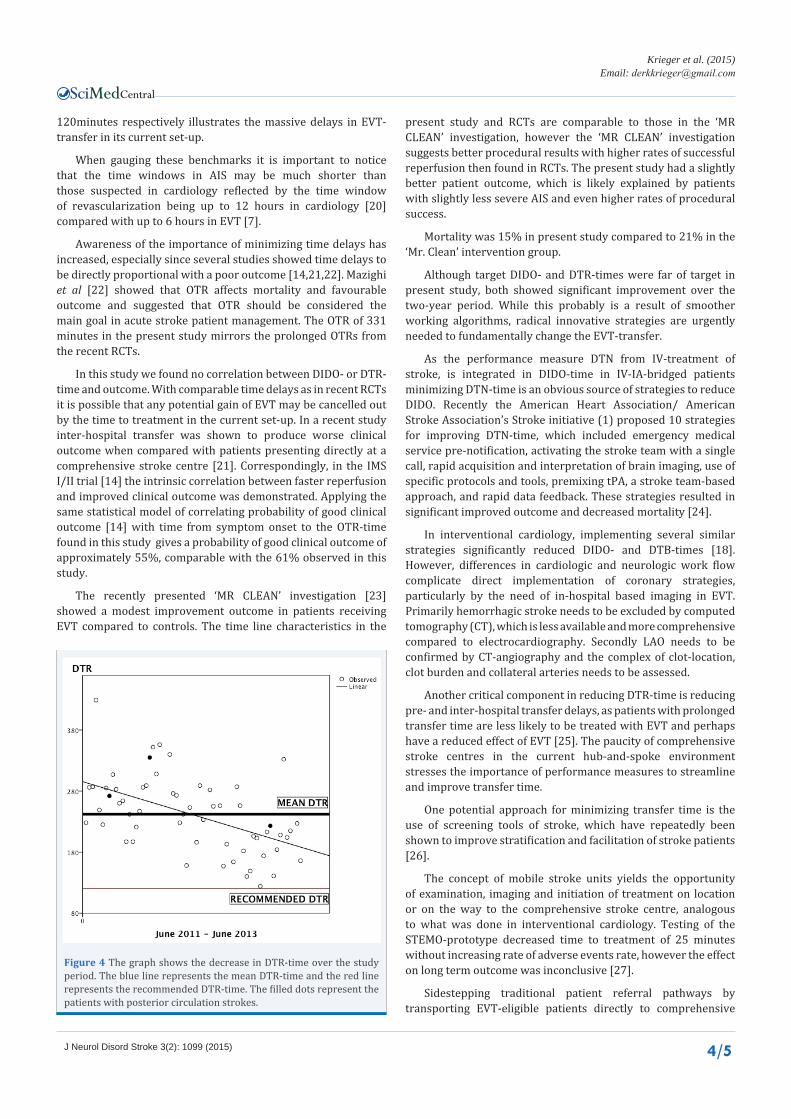
Mean DIDO was 101 min (+/-36, 9), mean DTR was 242 minutes (+/- 61, 5), mean OTR was 331 min (+/-94) We found no difference in DIDO and DTR between anterior and posterior circulation AIS (Figure 2, 3), why no benchmark differentiation seems necessary.

Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 3/5
Over the 2-year period a significant reduction in both DIDO (p<0,001) and DTR (p<0,001) could be shown (Figure 2, 3)
Successful recanalization (TICI 2b-3) was achieved in 40 patients (66%).
Favourable 3-months outcome (mRS 0-2) was seen in 37 patients (61%).
The overall mortality was 14, 8% (n=9).
In univariate analysis only age and stroke severity correlated with 3 months outcome.
DISCUSSIONThis study is the first to assess the recognized, efficacy-
proven performance measures from interventional cardiology in the AIS-setting.
Presently, none of the patients met the recommended DIDO or DTR-time windows from coronary interventions. Measuring delays to treatment in EVT is vital for comparison and monitoring of quality, but performance benchmarks have yet to be established.
The mean DIDO-time of 101 minutes and DTR-time of 242 minutes compared to the goals from PCI of 30 minutes and
Mean DIDO:101 min Transfer to CSC* Endovasculartherapy
Mean DTR 242 min
Figure 1 Treatment chain and times.*CSC: Somprehensive stroke center
Figure 2 Flow chart depicting selection of patients.
Figure 3 The graph shows the decrease in DIDO-time over the study period. The blue line represents the mean DIDO-time and the red line represents the recommended DIDO-time. The filled dots represent the patients with posterior circulation strokes.
Table 1: Baseline patient characteristics.
Age, years (SD) 65,5 (+/-13,1)
Male (%) 27 (44)
Non-bridged (%) 8 (13)
NIHSS on arrival PSC (SD) 16,2 (+/-5,5)
NIHSS on arrival CSC (SD) 12 (+/- 7,6)
NIHSS 24h (SD) 9,1 (+/- 7,9)
Delta NIHSS (SD) 6,9 (+/- 7,3)
DTN (n=48) (SD) 55 min (+/- 36)
TICI grade 2B-3 (%) 41 (67)
DIDO, min, (SD) 101 (+/-36,9)
DTR, min (SD) 242 (+/-61,5)
ORT, min, (SD) 331 (+/-94)
mRS 0-2 at 3months (%) * 36 (62)
mRS 3-6 at 3months (%) * 23 (38)PSC = Primary Stroke centreCSC = Comprehensive Stroke CentreDTN= Door-To-NeedleORT = Onset-to-Recanalization-Time*Only anterior circulation stroke
Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 4/5
120minutes respectively illustrates the massive delays in EVT-transfer in its current set-up.
When gauging these benchmarks it is important to notice that the time windows in AIS may be much shorter than those suspected in cardiology reflected by the time window of revascularization being up to 12 hours in cardiology [20] compared with up to 6 hours in EVT [7].
Awareness of the importance of minimizing time delays has increased, especially since several studies showed time delays to be directly proportional with a poor outcome [14,21,22]. Mazighi et al [22] showed that OTR affects mortality and favourable outcome and suggested that OTR should be considered the main goal in acute stroke patient management. The OTR of 331 minutes in the present study mirrors the prolonged OTRs from the recent RCTs.
In this study we found no correlation between DIDO- or DTR-time and outcome. With comparable time delays as in recent RCTs it is possible that any potential gain of EVT may be cancelled out by the time to treatment in the current set-up. In a recent study inter-hospital transfer was shown to produce worse clinical outcome when compared with patients presenting directly at a comprehensive stroke centre [21]. Correspondingly, in the IMS I/II trial [14] the intrinsic correlation between faster reperfusion and improved clinical outcome was demonstrated. Applying the same statistical model of correlating probability of good clinical outcome [14] with time from symptom onset to the OTR-time found in this study gives a probability of good clinical outcome of approximately 55%, comparable with the 61% observed in this study.
The recently presented ‘MR CLEAN’ investigation [23] showed a modest improvement outcome in patients receiving EVT compared to controls. The time line characteristics in the
present study and RCTs are comparable to those in the ‘MR CLEAN’ investigation, however the ‘MR CLEAN’ investigation suggests better procedural results with higher rates of successful reperfusion then found in RCTs. The present study had a slightly better patient outcome, which is likely explained by patients with slightly less severe AIS and even higher rates of procedural success.
Mortality was 15% in present study compared to 21% in the ‘Mr. Clean’ intervention group.
Although target DIDO- and DTR-times were far of target in present study, both showed significant improvement over the two-year period. While this probably is a result of smoother working algorithms, radical innovative strategies are urgently needed to fundamentally change the EVT-transfer.
As the performance measure DTN from IV-treatment of stroke, is integrated in DIDO-time in IV-IA-bridged patients minimizing DTN-time is an obvious source of strategies to reduce DIDO. Recently the American Heart Association/ American Stroke Association’s Stroke initiative (1) proposed 10 strategies for improving DTN-time, which included emergency medical service pre-notification, activating the stroke team with a single call, rapid acquisition and interpretation of brain imaging, use of specific protocols and tools, premixing tPA, a stroke team-based approach, and rapid data feedback. These strategies resulted in significant improved outcome and decreased mortality [24].
In interventional cardiology, implementing several similar strategies significantly reduced DIDO- and DTB-times [18]. However, differences in cardiologic and neurologic work flow complicate direct implementation of coronary strategies, particularly by the need of in-hospital based imaging in EVT. Primarily hemorrhagic stroke needs to be excluded by computed tomography (CT), which is less available and more comprehensive compared to electrocardiography. Secondly LAO needs to be confirmed by CT-angiography and the complex of clot-location, clot burden and collateral arteries needs to be assessed.
Another critical component in reducing DTR-time is reducing pre- and inter-hospital transfer delays, as patients with prolonged transfer time are less likely to be treated with EVT and perhaps have a reduced effect of EVT [25]. The paucity of comprehensive stroke centres in the current hub-and-spoke environment stresses the importance of performance measures to streamline and improve transfer time.
One potential approach for minimizing transfer time is the use of screening tools of stroke, which have repeatedly been shown to improve stratification and facilitation of stroke patients [26].
The concept of mobile stroke units yields the opportunity of examination, imaging and initiation of treatment on location or on the way to the comprehensive stroke centre, analogous to what was done in interventional cardiology. Testing of the STEMO-prototype decreased time to treatment of 25 minutes without increasing rate of adverse events rate, however the effect on long term outcome was inconclusive [27].
Sidestepping traditional patient referral pathways by transporting EVT-eligible patients directly to comprehensive
Figure 4 The graph shows the decrease in DTR-time over the study period. The blue line represents the mean DTR-time and the red line represents the recommended DTR-time. The filled dots represent the patients with posterior circulation strokes.

Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 5/5
stroke centres could potentially eliminate of the entire DIDO-time from the DTR-time. In the current study that would mean a decrease in time delay to recanalization of 101 minutes, which if applied to the statistical modelling mentioned above (14) would improve good outcome rate to about 75%.
These new perspectives are still in their infancy, but have great potential and may be an essential part of future stroke management.
LIMITATIONSThis study presents a single centre experience with limited
sample size and the results may not be generally applicable, as treatment protocols and transfer times differ between centres. However, patients were consecutive and from a high-volume centre, and therefore thought to be generally representable of normal AIS-population.
The retrospective design made it impossible to obtain all relevant data on all patients.
The exact time of recanalization was not evident in all patient cases why the end of the procedure-time was used, possibly overestimating the DTR and underestimating the effect of time.
As an inherent problem in uncontrolled studies outcomes are self-reported and unblinded, although mRS-certified colleagues obtained data.
Larger controlled multicentre investigations are needed.
CONCLUSION The present study assesses the recognized benchmarks DIDO-
and DTR-time, which was proven effective in PCI. The results are sobering and mirror the results from recent RCTs, suggesting that implementing strategies to reduce time delays to treatment in EVT may be critical in proving the efficacy of EVT.
New strategies are needed and learning from the experience in interventional cardiology provides a unique possibility for reducing these time delays and there by levelling the playing field between IV-tPA and EVT.
ACKNOWLEDGEMENT A special thanks to the participating patients and doctors.
Disclosure of Conflicts of interest
Dr. Holtmannspötter reports personal fees from Covidien, MicroVention and Sequent Medical, outside the submittet work.
None of the other authors have any conflicts of interest.
Authors’ contributions
MM participated in the design, carried out the analysis and interpretation of data, drafted, coordinated and revised the manuscript.
HSA helped in drafting the manuscript, analysis and in critical revision.
MH critically revised the manuscript.
DK planned the data collection and goals, critical revised and coordinated the manuscript.
All authors read and approved the final manuscript.
REFERENCES1. Fonarow GC, Smith EE, Saver JL, Reeves MJ, Hernandez AF, Peterson
ED, et al. Improving door-to-needle times in acute ischemic stroke: the design and rationale for the American Heart Association/American Stroke Association’s Target: Stroke initiative. Stroke. 2011; 42: 2983-2989.
2. Bhatia R, Hill MD, Shobha N, Menon B, Bal S, Kochar P, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action. Stroke. 2010; 4: 2254–2258.
3. Broderick JP, Palesch YY, Demchuk AM, Yeatts SD, Khatri P, Hill MD, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013; 368: 893-903.
4. Ciccone A, Valvassori L, Nichelatti M, Sgoifo A, Ponzio M, Sterzi R, Boccardi E. SYNTHESIS Expansion Investigators. Endovascular treatment for acute ischemic stroke. N Engl J Med. 2013; 368: 904-913.
5. Kidwell CS, Jahan R, Gornbein J, Alger JR, Nenov V, Ajani Z, et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med. 2013; 368: 914-923.
6. Nogueira RG, Gupta R, Dávalos A. IMS-III and SYNTHESIS Expansion trials of endovascular therapy in acute ischemic stroke: how can we improve? Stroke. 2013; 44: 3272-3274.
7. Gory B, Riva R, Turjman F. Endovascular treatment in patients with acute ischemic stroke: technical aspects and results. Diagn Interv Imaging. 2014; 95: 561-568.
8. Saver JL, Jovin TG, Smith WS, Albers GW, Baron JC, Boltze J, et al. Stroke treatment academic industry roundtable: research priorities in the assessment of neurothrombectomy devices. Stroke. 2013; 44: 3596-3601.
9. Mazighi M, Serfaty J-M, Labreuche J, Laissy J-P, Meseguer E, Lavallée PC, et al. Comparison of intravenous alteplase with a combined intravenous-endovascular approach in patients with stroke and confirmed arterial occlusion (RECANALISE study): a prospective cohort study. Lancet Neurol. Elsevier Ltd. 2009; 8: 802–809.
10. Rangaraju S, Owada K, Noorian AR, Nogueira RG, Nahab F, Glenn BA, et al. Comparison of final infarct volumes in patients who received endovascular therapy or intravenous thrombolysis for acute intracranial large-vessel occlusions. JAMA Neurol. 2013; 70: 831-836.
11. Nogueira RG, Lutsep HL, Gupta R, Jovin TG, Albers GW, Walker GA, et al. Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): a randomised trial. Lancet. 2012; 380:1231–1240.
12. Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al. Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. 2012; 380: 1241-1249.
13. Turk AS, Frei D, Fiorella D, Mocco J, Baxter B, Siddiqui A, et al. ADAPT FAST study: a direct aspiration first pass technique for acute stroke thrombectomy. J Neurointerv Surg. 2014; 6: 260-264.
14. Khatri P, Abruzzo T, Yeatts SD, Nichols C, Broderick JP, Tomsick TA; IMS I and II Investigators, . Good clinical outcome after ischemic stroke with successful revascularization is time-dependent. Neurology. 2009; 73: 1066-1072.
15. Wang TY, Nallamothu BK, Krumholz HM, Li S, Roe MT, Jollis JG, et al. Association of door-in to door-out time with reperfusion delays and outcomes among patients transferred for primary percutaneous coronary intervention. JAMA. 2011; 305: 2540-2547.
Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 6/5
16. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green L a, Hand M, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction--executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1999. J Am Coll Cardiol. 2004; 44: 671–719.
17. Bradley EH, Nallamothu BK, Herrin J, Ting HH, Stern AF, Nembhard IM, et al. National efforts to improve door-to-balloon time results from the Door-to-Balloon Alliance. J Am Coll Cardiol. 2009; 54: 2423-2429.
18. Krumholz HM, Herrin J, Miller LE, Drye EE, Ling SM, Han LF, et al. Improvements in door-to-balloon time in the United States, 2005 to 2010. Circulation. 2011; 124: 1038-1045.
19. Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, Dillon W. Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke. 2003; 34: 109-137.
20. Giugliano RP, Braunwald E; TIMI Study Group. Selecting the best reperfusion strategy in ST-elevation myocardial infarction: it’s all a matter of time. Circulation. 2003; 108: 2828-2830.
21. Sun CH, Nogueira RG, Glenn BA, Connelly K, Zimmermann S, Anda K, Camp D. “Picture to puncture”: a novel time metric to enhance outcomes in patients transferred for endovascular reperfusion in acute ischemic stroke. Circulation. 2013; 127: 1139-1148.
22. Mazighi M, Chaudhry SA, Ribo M, Khatri P, Skoloudik D, Mokin M,
et al. Impact of onset-to-reperfusion time on stroke mortality: a collaborative pooled analysis. Circulation. 2013; 127: 1980-1985.
23. Fransen PSS, Beumer D, Berkhemer OA, Berg LA Van Den, Lingsma H. et al. a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands?: study protocol for a randomized controlled trial MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands?: study protocol for a randomized controlled trial. 2014; 15: 343.
24. Fonarow GC, Zhao X, Smith EE, Saver JL, Reeves MJ, Bhatt DL, et al. Door-to-needle times for tissue plasminogen activatcor administration and clinical outcomes in acute ischemic stroke before and after a quality improvement initiative. JAMA. 2014; 311:1632–1640.
25. Prabhakaran S, Ward E, John S, Lopes DK, Chen M, Temes RE, et al. Transfer delay is a major factor limiting the use of intra-arterial treatment in acute ischemic stroke. Stroke. 2011; 42: 1626-1630.
26. Fassbender K, Balucani C, Walter S, Levine SR, Haass A, Grotta J. Streamlining of prehospital stroke management: the golden hour. Lancet Neurol. 2013; 12: 585-596.
27. Ebinger M, Winter B, Wendt M, Weber JE, Waldschmidt C, Rozanski M, Kunz A. Effect of the use of ambulance-based thrombolysis on time to thrombolysis in acute ischemic stroke: a randomized clinical trial. JAMA. 2014; 311: 1622-1631.

Central
Krieger et al. (2015)Email:
J Neurol Disord Stroke 3(2): 1099 (2015) 7/5
Mørkenborg ML, Steglich-Arnholm H, Holtmannspötter M, Krieger DW (2015) Are Current Time Delays in Endovascular Treatment of Stroke Acceptable? J Neurol Disord Stroke 3(2): 1099.
Cite this article