approach to a patient with active urinary sediments
TRANSCRIPT

APPROACH TO A PATIENT
WITH ACTIVE URINARY
SEDIMENTS
Dr. Sayan Chakraborty
First Year PGT-MD Tropical Medicine
School of Tropical Medicine, Kolkata

Urine Microscopy
The ‘Liquid Renal Biopsy’!
INDICATIONS:
• Suspected urinary tract infection
• Suspected acute glomerulonephritis.
• Suspected acute interstitial nephritis
(requires staining for eosinophils).
• Unexplained acute or chronic renal failure.
• Haematuria (with or without proteinuria) on
urine dipstick test.
• Suspected urinary tract malignancy.

Classification of Urinary
Sediments
• Cells
• Renal casts
• Crystals
• Microorganisms
• Mucus
• Miscellaneous

Cells- Erythrocytes
Description
• Size: 7-8 µm in diameter
• Pale or yellowish, smooth
biconcave disk
• No nucleus or cytoplasmic
granules
• Normal: Less than 2
RBC/HPF
• Can originate from any part
of the urinary tract
Associated Conditions
Glomerulonephritis
Calculi
BHP/ Prostatitis
Carcinoma of
bladder/kidney
Trauma
IgA nephropathy
Urinary Schistosomiasis
etc.

Hematuria

Leucocytes
Description
• Typically neutrophils
(PMN)
• Larger than RBC, 10-12 µm
in diameter
• Contain nucleus and
cytoplasmic granules
• Brownian
movement (“glitter cells”)
• Normal: no more than 2
WBC/HPF
Associated Conditions
Can originate from any part
of the urinary tract
(glomerulus to urethra)
Increased In inflammatory
processes of the urinary
tract (pyuria)

PYURIA BACTERIURIA

EPITHELIA
• Squamous epithelia
• Large flat cell with central oval nucleus
• Transitional (bladder) epithelia
• Spindle shaped with large oval nucleus
• Maybe in sheet
• Renal tubular epithelia
• Small cell with large oval nucleus
• Most clinically significant

Squamous
Epithelial Cells
Large, flat,
irregular-shaped
cells
Principally from
the urethra and
vagina

Transistional
Epithelial Cells
2-4 times larger
than leukocytes
Round, pear-
shaped, tail-like
projections
Large round
nucleus

Renal Tubular Epithelial Cells
Description
• Slightly larger than WBC
• Flat, cuboidal or columnar
• One large round nucleus
Associated conditions
Tubular damage
Pyelonephritis
ATN
Salicylate intoxication
Transplant rejection

Renal Tubular Cells

Urinary Casts
• First described by Henry Bence
Jones (1813-1873)
• Cylindrical structures
• Formed in the distal convoluted
tubule and collecting ducts of nephrons
• Form via precipitation of Tamm-
Horsfall mucoprotein which is secreted
by renal tubule cells, and sometimes also
by albumin in conditions of proteinuria


Classification of Casts
Acellular casts
• Hyaline casts
• Granular casts
• Waxy casts
• Fatty casts
• Pigment casts
• Crystal casts
Cellular casts
• Red blood cell casts
• White blood cell casts
• Bacterial casts
• Epithelial cell casts

Hyaline Cast
Most common type of cast
Solidified Tamm-Horsfall
mucoprotein secreted from the tubular
epithelial cells.
CAUSES: Low urine flow, concentrated
urine, acidic environment, dehydration or
vigorous exercise.
Phase contrast microscopy leads to easier
identification.

HYALINE CASTS

Granular Casts
Second-most common type of cast
Result from the breakdown of cellular casts
or the inclusion of aggregates of plasma
proteins (e.g. albumin) or Ig light chains
Classified as fine or coarse depending on
the size of inclusions
Most often indicative of chronic renal
disease
The "muddy brown cast" seen in acute
tubular necrosis is a type of granular cast.

Fine Granular Cast Coarse Granular Cast

Waxy Casts
• End product of cast evolution
• Waxy casts fall under the umbrella of
“broad” casts
• Suggest very low urine flow associated with
severe, longstanding kidney disease such as
chronic renal failure.
• Formed in diseased, dilated ducts

Broad Cast
Waxy Cast

Fatty Cast • Hyaline casts with fat
globule inclusions
• Formed by the breakdown
of lipid-rich epithelial cells
• If cholesterol or cholesterol
esters are present -
“Maltese cross” sign under
polarized light
• Pathognomonic for high
urinary protein nephrotic
syndrome

Pigment Cast
• So named due to discolouration
• Formed by the adhesion of metabolic
breakdown products or drug pigments
• Caused by:
Hemoglobin in hemolytic anemia
Myoglobin in rhabdomyolysis
Bilirubin in liver disease.
Drug pigments, such as phenazopyridine

RBC Cast
• Always pathological, and is strongly
indicative of glomerular damage
• Causes:
Glomerulonephritis from various causes
Wegener's granulomatosus
Systemic lupus erythematosus
Goodpasture’s syndrome
Renal infarction
Subacute bacterial endocarditis

RBC Cast

WBC Cast
• Indicative of inflammation or infection
• Causes:
Pyelonephritis (strong suggestion)
Acute allergic interstitial nephritis
Nephrotic syndrome
Post-streptococcal acute
glomerulonephritis

WBC Cast

Bacterial Cast
• Found in pyelonephritis
• Seen in association with loose bacteria,
white blood cells, and white blood cell casts
• Discovery is rare, due to the infection-
fighting efficiency of neutrophils, and the
possibility of misidentification as a fine
granular cast.

Epithelial
Cell Cast
Stasis and
desquamation of
renal tubular
epithelial cells
following
tubular damage
and necrosis.

Crystals
In Acidic Urine
• Uric Acid
• Calcium Oxalate
• Cystine
• Leucine
• Cholesterol
• Tyrosine
• Sulfonamide
In Alkaline Urine
• Triple phosphate
• Ammonium biurate
• Calcium phosphate

CRYSTALS IN ACIDIC URINE

Uric Acid Crystal
Description
• Many different
shapes, diamond,
rhombic prism or
rosette
• Yellow or brown in
colour
Associated conditions
• Very common
• Can be normal
occurence
• Associated with
increased purine
metabolism

Uric Acid Crystals

Calcium oxalate crystal
Description
• Colorless, octahedral or
envelope
Associated Conditions
• Ingestion of oxalate-rich
foods: spinach, rhubarb,
tomatoes, garlic,
oranges, asparagus
• High intake of ascorbic
acid
• Ethylene glycol
poisoning

Calcium Oxalate
Crystal

Cystine Crystal
• Colorless, refractile, hexagonal plates
• Found in Congenital cystinosis or cystinuria

Leucine Crystal
Description
• Oily, highly
refractile, yellow or
brown spheroids and
concentric striations
Associated Conditions
• Clinically significant
• Maple syrup urine
disease, Oasthouse
urine disease, severe
liver disease
• Seen with tyrosine in
liver disease

Cholesterol Crystal
Description
• Large, flat,
transparent
• Notched corners
Associated Conditions
• Excessive tissue
breakdown
• Obstructed lymphatic
flow
• Nephritis and
nephrotic conditions

Tyrosine Crystal
Description
• Very fine, highly
refractile needles
• Black, yellow
• In sheaves or clusters
Associated Conditions
• Severe liver disease
• Tyrosinosis

CRYSTALS IN ALKALINE
URINE
Triple Phosphate Crystal
Description
• Colorless prisms
• 3-6 sides, oblique
ends
• Coffin lids
Associated Condition
• Can be found in
normal urines
• Chronic urinary
inflammation

Triple Phosphate Crystals
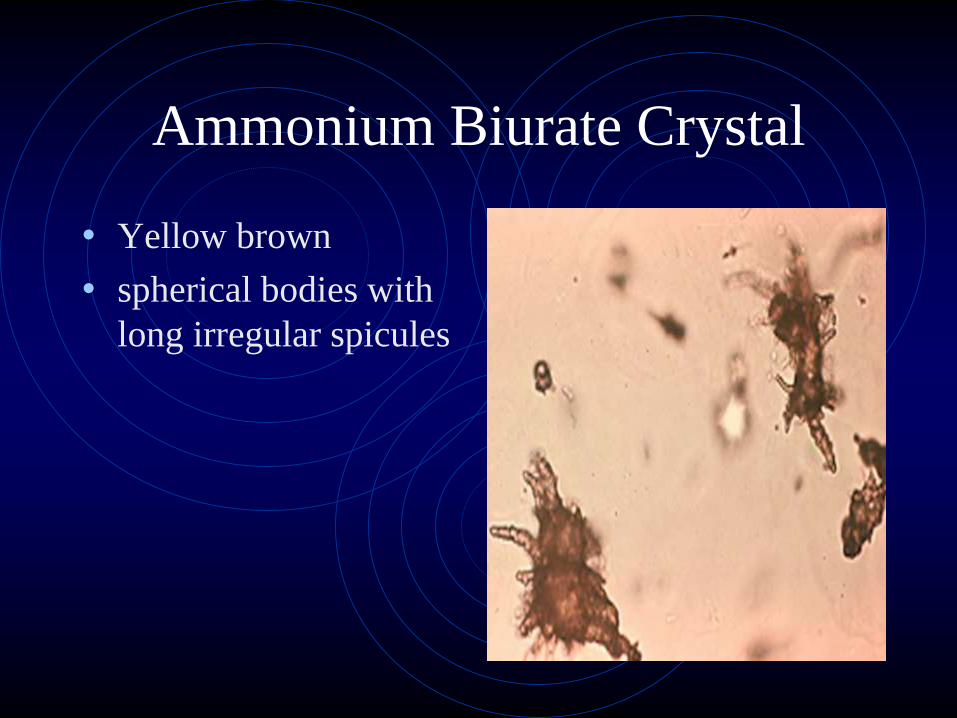
Ammonium Biurate Crystal
• Yellow brown
• spherical bodies with
long irregular spicules

Calcium Phosphate Crystal
• Long thin, colorless
needles
• One pointed end
• Arranged as
rosettes or star
• Can be found
normally

Active Urinary Sediments
• Indicates inflammation
in the glomerular
capillary wall
• The sediments are:
• Red blood cells/casts
• White cells/casts

Approach to a patient with RBCs
or RBC casts in urineHEMATURIA

Microscopic hematuria D/D
Glomerular
• Primary nephritis (post streptococcal glomerulonephritis, Ig A nephropathy, Anti-GBM disease)
• 2nd nephritis (SLE, Goodpasture’s syndrome, ANCA related vasculitis)
• Alport’s syndrome (hereditary nephritis)
• Thin basement membrane nephropathy (benign familial hematuria)

Microscopic hematuria D/D
contd..Extra-glomerular:
Renal
• Malignancy
• Vascular disease (malignant hypertension, AVM, nutcracker syndrome, renal vein thrombosis, sickle cell trait/disease, papillary necrosis)
• Infection (pyelonephritis, TB, CMV, EBV)
• Hypercalciuria
• Hereditary disease (polycystic kidney disease, medullary sponge kidney)

Microscopic hematuria D/D
contd..
Extra-renal
• malignancy (prostate, ureter, bladder)
• BPH
• Nephrolithiasis
• Coagulopathy
• Trauma

Extraglomerular vs Glomerular Hematuria in Urine Analysis
Extraglomerular Glomerular
Color (if
macroscopic)Red or pink
Red, smoky brown,
or "Coca-Cola"
Clots May be present Absent
Proteinuria <500 mg/dayMay be >500
mg/day
RBC morphology Normal Dysmorphic
RBC casts Absent May be present

Major causes of hematuria by age
and duration



Glomerular Hematuria with
active sedimentsHISTORY:
• Early morning periorbital puffiness,
oliguria, dark colored urine, edema or
hypertension
• Recent throat or skin infection may suggest
postinfectious glomerulonephritis
• Joint pains, skin rashes, and prolonged fever
in adolescents suggest a collagen vascular
disorder

• Skin rashes and arthritis can occur in
Henoch-Schönlein purpura and systemic
lupus erythematosus
• A family history that is suggestive of Alport
syndrome, collagen vascular diseases,
urolithiasis, or polycystic kidney disease is
important
• Passage of clots in urine suggests an extra-
glomerular cause

Physical Examination
• Measurement of the blood pressure (with an
appropriately sized cuff)
• Evaluation for the presence of periorbital
puffiness or peripheral edema
• Detailed skin examination to look for
purpura.
• Abdominal examination to look for palpable
kidneys

Initial Work up
• CBC, PT, INR, electrolytes, kidney function
• UA and microscopy to determine the number and morphology of RBC, crystal and casts
• Consider urine C/S
• Repeat UA in a few days

Further Work up
• Throat swab C/S, ASO titre, complement
levels for PSGN
• ANA, dsDNA for SLE
• Skin biopsy showing IgA deposition s/o
HSP
• ANCA for systemic vasculitis
• Imaging: USG, CT, Radionuclide studies

Renal Biopsy
Indications:
• Significant proteinuria
• Abnormal renal function
• Recurrent persistent hematuria
• Serologic abnormalities (abnormal complement,
ANA, or dsDNA levels)
• Recurrent gross hematuria
• A family history of end stage renal disease

Approach to a patient with pyuria
or WBC cast
Differential Diagnosis:
Asymptomatic Bacteriuria
Cystitis
Pyelonephritis
Prostatitis
Complicated UTI

CASE 1
A 40 year old female patient presented with
Dysuria
Frequency
Urgency
What is the approach for management?

Diagnostic ApproachPatient profile Management
1. Otherwise healthy woman, not
pregnant, clear history
Uncomplicated cystitis:
• No Urine c/s needed
• OPD management
2. Woman with unclear history or risk
factors for STD
Uncomplicated cystitis or STD:
• Dipstick, Urinalysis
• STD evaluation, pelvic examination
3. Male with pelvic, perineal or
prostatic pain
Acute prostatitis:
• Urinalysis and C/S
• Urologic evaluation
4. Indwelling urinary catheter CAUTI:
• Change or remove catheter
• Urinalysis, C/S
• Blood C/S if fever
5. All other patients Complicated UTI;
• Urinalysis, C/S
• Modify functional or anatomic
abnormality

Case 2
A patient presented with acute onset of:
Back pain
Nausea/vomiting
Fever
Possible cystitis symptoms
Approach?

Diagnostic Approach
Patient profile Management
Otherwise healthy woman, not pregnant Uncomplicated pyelonephritis:
• Urine Culture
• OPD management
All other patients Pyelonephritis:
• Urine Culture
• Blood Culture
Patients with non-localizing systemic symptoms like fever,
altered mental status along with leucocytosis:
Consider Complicated UTI or Pyelonephritis :-
Look for other potential etiologies
Urine Culture
Blood Culture

Case 3
30 year old second gravida lady in her third
trimester presented with a positive urine
culture in the absence of any symptom.
What should be her ideal management?

Diagnostic Approach
Patient profile Management
Pregnant or renal transplant
recipient or planned to undergo an
invasive urologic procedure
Asymptomatic Bacteriuria (ABU)
Screening and treatment
warranted
All other patients Consider ABU
No additional treatment and
workup needed
Patient with urinary catheter Consider CA-ABU
No additional treatment and
workup needed
Remove unnecessary catheters

Case 4
68 year old gentleman presented with
recurrent acute urinary symptoms.
Approach to management?

Diagnostic Approach
Patient Profile Management
Male Consider chronic bacterial prostatitis:
• Meares-Stamey 4-glass test
• Urology consultation
Otherwise healthy female not pregnant Consider reucurrent cystitis:
• Urine Culture
• Consider prophylaxis or patient
initiated management

QUIZ BUGS

Carrot no. 1
• A 10 year old male child presented with
hearing loss, dimness in vision and
persistent hematuria. Gene study showed
COL4A4 mutation.
What is your diagnosis?

Carrot no. 2
• 21 Year old female visited ophthalmology
clinic with complaints of pain in eyes and
difficulty in adjusting to dark. She was
found to have iliac horns and gave history
of passage of reddish urine.
What is your diagnosis?

Carrot no. 3
• 30 year old lady
presented with pain in
left lower quadrant
along with hematuria.
The figure beside
shows the etiology.
What is your diagnosis?
