applications of cbt in group therapies
DESCRIPTION
TRANSCRIPT
Applications of Cognitive-Behavioral Group Therapy
(CBGT)
Kevin J. Drab, M.A., M.Ed., LPC, NBCCH, CACD, EMDRT
Behavioral Counseling & Training, 418 Stump Road, Suite #208, Montgomeryville, PA 18936 Tel: (215) 527-2904
e-mail: [email protected] website: http://BCTPRO.com
The Third Wave of Behavior Therapies The Third Wave of Behavior Therapies
First Wave - traditional behavior therapy, which works to replace harmful behaviors with constructive ones through a learning principle called conditioning.
Second Wave - cognitive therapy seeks to change problem behaviors by changing the thoughts that cause and perpetuate them.
Third Wave – movement away from cognitivism, toward new forms of behaviorism, including functional analysis, and traditionally nonclinical treatment techniques like acceptance, mindfulness, cognitive defusion, dialectics, values, spirituality, and relationship development.
These therapies reexamine the causes and diagnoses of psychological problems, the treatment goals of psychotherapy, and even the definition of mental illness itself.
2

Cognitive-behavioral therapy does not exist as a distinct therapeutic technique. The term "cognitive-behavioral therapy (CBT)" is a very general term for a classification of therapies with similarities.
There are many approaches labeled as cognitive-behavioral therapy, including:•Rational Emotive Behavior Therapy•Cognitive-Behavioral Modification Therapy•Reality Therapy (now known as Control Theory)•Cognitive Restructuring Therapy •Cognitive Therapy•Dialectic Behavior Therapy•Behavioral Activation Therapy•Mindfulness-Based Cognitive Therapy•Acceptance and Commitment Therapy•Schema-Focused Cognitive Therapy

A Wide Variety of Resources and Approaches
CBT is based on behaviorism, social learning theory, and generally covert cognitive structures.
While recognizing that there may be various genetic and psychophysiogic susceptibilities contributing to the development of various mental health problems and substance use disorders, it is assumed that the primary mechanism is through learning, occurring mostly out of awareness, via social modeling, operant and classical conditioning, and adaptive biological changes in the body.
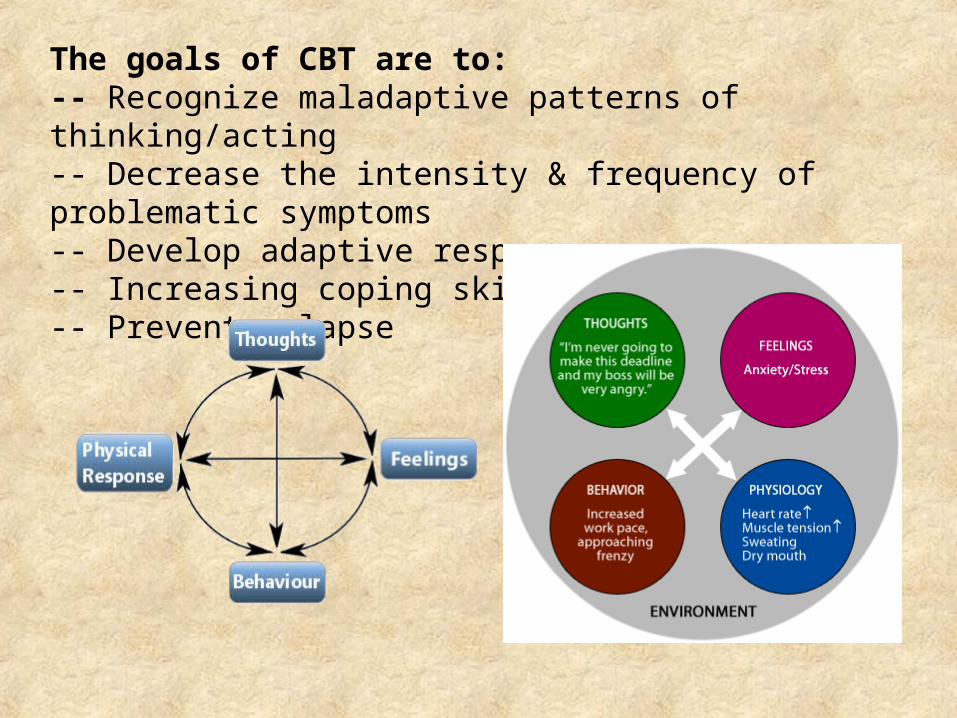
The goals of CBT are to:-- Recognize maladaptive patterns of thinking/acting-- Decrease the intensity & frequency of problematic symptoms-- Develop adaptive responses-- Increasing coping skills-- Prevent relapse
Fundamental to a CBT approach is an understanding of the cognitive model.
That thoughts, feelings and behaviors are interrelated and multidirectional.
CBT is not a logical, intellectual approach. It is a collaborative exploration of the client’s phenomenological world: memories, thoughts, emotions, experiences, and patterns and structures of responding. In group therapy this involves both the therapist, and group clients.
The focus at first is usually on identifying and challenging dysfunctional/irrational Automatic Thoughts which lead to self-defeating emotional and behavioral responses.
Automatic thoughts coexist with a more manifest stream of thoughts, arise spontaneously, are negative, are usually very brief, and are not based on reflection or deliberation. e.g., I’m a total failure; Everybody is laughing at me; I can’t stand this; This will just get worse; I am losing control; etc.
Beck’s favorite clinical question which he called the clinical probe was: “What is going through your mind right now?”
Underlying the immediate automatic thoughts are the individual’s conditional or intermediate beliefs – the if-then statements by which an individual makes sense of the cause-and-effect relations in the world.
The cognitive model holds that everyone has an array of conditional beliefs that have been learned and accumulated over a lifetime, and seem unquestionably true and obvious to them.
Therapy helps the individual explore those conditional beliefs which are not helping them, are not true, and causing them troubles.

Beneath these conditional beliefs, the cognitive model locates what are called core beliefs or schemas. These are the deep, fundamental ways that a person regards him or herself. Individuals usually hold a combination of positive and core beliefs as to their lovability and competence in facing life’s challenges.
Examples of negative schemas:I am helplessI am powerlessI am not safeI am out of controlI am weakI am vulnerableI can’t trust anyoneI am responsibleIt will always be taken away from me
I am inadequateI am ineffectiveI am stupidI am incompetentI will always failI am defective (i.e., I do not measure up to others)I am not good enough (in terms of achievement)I am shameful
I am unworthyI am nothingI am differentI am undesirableI am unattractiveI am unwantedI am uncared forI am badI don’t deserve anythingI can’t trust myself

The key active ingredients that distinguish CBT from other therapies and that must be delivered for adequate exposure to CBT include the following:
The key active ingredients that distinguish CBT from other therapies and that must be delivered for adequate exposure to CBT include the following:
• Functional analyses of relationships between thoughts, emotional problems, behaviors, substance use, and environmental influences
• Individualized training in recognizing and coping with dysfunctional cognitions and physiologic responses causing problems.
• Recognizing risk-factors, triggers, seemingly irrelevant decisions, and how to deal with impulses and urges (such as with depression or substance abuse)
• Identification and debriefing of past and future high-risk situations
• Encouragement and review of extra-session implementation of skills
• Practice of skills within sessions
• Functional analyses of relationships between thoughts, emotional problems, behaviors, substance use, and environmental influences
• Individualized training in recognizing and coping with dysfunctional cognitions and physiologic responses causing problems.
• Recognizing risk-factors, triggers, seemingly irrelevant decisions, and how to deal with impulses and urges (such as with depression or substance abuse)
• Identification and debriefing of past and future high-risk situations
• Encouragement and review of extra-session implementation of skills
• Practice of skills within sessions

Essential Techniques:1. Connection between thoughts, situational triggers, and elicitation of negative affect, including depression and anxiety.2. Use of evidence gathering and thought distortions to become more objective about one’s thoughts.3. Use of experiments.4. Exploration of underlying beliefs and assumptions.
Adaptive response: the primary therapeutic mechanism of CBT in which an individual learns to make effective changes in how they think, feel, act and adapt.

Examples of Various Techniques Used in CBT
Cognitive reconstructionSelf-monitoring (e.g. Thought Record)Descending Arrow TechniqueSocratic Questioning TechniquesAdvantages and disadvantagesRational-emotional role-playRelaxationActing “as if”Behavioral experimentsHomeworkExposureSkills developmentReconstructing personal historyBalcony methodResponse Prevention
PsychoeducationCognitive continuumAcceptanceBehavioral ActivationRelapse PreventionMindfulnessSelf-disclosureCore Belief worksheetExtreme contrastsDeveloping metaphorsHistorical testsRestructuring early memoriesCoping cardsProblem-solvingPie Chart
The notion that the patient’s everyday experiences could be used as a testing ground for checking the accuracy of various beliefs crystalized into the general concept of “Collaborative Empiricism” which became the cornerstone of cognitive-behavioral therapy.

Core Therapeutic Principles
1. Collaborative Empiricism in which the therapist and client “join forces to investigate thoughts and experiences in a manner that is reminiscent of the scientific method. This requires developing hypotheses about thoughts and testing these through logical analysis and collection of factual evidence.”
2. Socratic Dialogue, involves “a series of interconnected questions that lead to a more logical, objective conclusion about one’s experiences” and is also a common theme for all cognitive techniques.”
3. Guided Discovery in which the therapist helps to illuminate meaning of thoughts and problems in logic, or helps to create situations from which the patient learns new information and different ways of thinking, acting and feeling.”
Examples of Socratic Dialogue QuestionsClarifying questions What do you mean by ______? What is your main point? How does ____ relate to ____? Could you put that another way? Let me see if I understand you; do you mean _____ or _____? Could you give me an example? Could you explain that further? Could you expand upon that?
Assumption questions
What are you assuming? What could we assume instead? You seem to be assuming ____. Do I understand you correctly? You seem to be assuming ____. How would you justify taking this for granted? Is it always the case? Why do you think the assumption holds here? Why would someone make this assumption?
Reason and evidence questions
How do you know? Why do you think that is true? Do you have any evidence for that? What difference does that make? What are your reasons for saying that? Can you explain how you logically got from ____ to ____? Do you see any difficulties with your reasoning here? What would change your mind? What would you say to someone who said ____? Can someone else give evidence to support that response? By what reasoning did you come to that conclusion? How could we find out whether that is true?




Why Cognitive-Behavioral Group Therapy?• Cost effective• Variety of resources and viewpoints
– Members profit by hearing other members talk about their problems.
– Group members are able to identify cognitive distortions.– Understand, confront and identify with more than one person.
• Sense of belonging – Decreases the feeling that the client is unique and encourages
the client to talk about his/her problems.• Clients can explore the way they behave and communicate in a safe
environment.• Conditional beliefs naturally rise to the surface, providing multiple
opportunities to identify, test and revise these underlying rules that govern social behavior.
• Learn problem solving techniques from other members, especially developing adaptive responses.
• Social Modeling and learning about functional roles of individuals.• Practice in a real life approximation of society.

Features of Good CBGTFeatures of Good CBGT• Effective CBT groups do not contain random self-disclosure,
emotional confrontation among group members, or straying into deep affective expressions in the absence of a CBT strategy, or technique.
• Supporting and enhancing effective group process leads to better outcomes.
• Knowledge and ability to conduct individual CBT sessions is a prerequisite to conducting groups, due to the complex demands involved in tracking and facilitating group process issues.
• Involve individual in intervention, then expand to group, then back to client; involving other clients in what is going on.

Features of Good CBGTFeatures of Good CBGTCollaborative relationship involves continually developing a therapeutic alliance in which clients are actively involved in process and tasks, asking questions, providing inputs, and working with therapist to achieve goals. Facilitating group members to develop adaptive responses.
The following are elements of a collaborative relationship in CBGT:•Agenda – usually arrived at by consensus.•Feedback – relevant according to each client’s treatment goals.•Goal Setting – therapist guides discussion of goals, but goals originate from group members themselves.•Homework – behavioral experimentation, helping clients to find homework that they are motivated to do; group pressure.•Socratic Questioning – clients begin to learn how to use this in their interactions with each other.

Task Focus CBT and related
therapeutic activities
Client working and actively benefiting from therapeutic
components
Group Leader. Facilitating, focusing, directing, modeling, etc.
Client working and actively benefiting from therapeutic
components
Group Leader. Facilitating, focusing, directing, modeling, etc.
Clients’ Involvement in providing feedback, advice,
applying CBT ideas and methods, relating to their own
experiences/beliefs.
Process - the way, or how, members react and interact, while focused on the content. Nonverbal behavior and patterns of content are examples of dynamics that are skillfully tracked by the leader to ensure he or she effectively manages the group.
Components of Effective Cognitive-Behavioral Group Therapy -- Kevin J. Drab
Task Focus CBT and related
therapeutic activities
Client working and actively benefiting from therapeutic
components
Group Leader. Facilitating, focusing, directing, modeling, etc.
Ten Commonly Used Methods in CBGT
• Automatic Thought Record• Challenging the Thoughts• Mood Monitoring• Arousal Hierarchy• Anxiety Monitoring• Problem Solving• Relaxation• Risk Assessment• Treatment Protocols• Relapse Prevention

Some examples of client psychoeducation
Directly – therapist provides mini-lectures, handouts, descriptions.Indirectly – exercises to explore an idea or method, therapist modeling, client’s sharing their experiences, watching other clients work and change.Homework – clients learn ideas and approaches from assignments, e.g., doing cognitive distortions form, DTR, monitoring triggers.Phenomenological explorations – “how do you…? Depress yourself. Cross Low Frustration Threshold.Extratherapeutic experiences – client’s observing other people, media, teaching CBT methods to others.