appendies - college of medicine · week #2 didactics at com, 1pm 1st case write-up due by this...
TRANSCRIPT

Appendix A: Sample Psychiatry evaluation template
Psychiatry Evaluation
Patient Name_____________________________________Patient # ____________ Unit ______ Date___________
Identifying information and reason for evaluation______________________________________________________
The purpose of this evaluation was explained to the patient, who then agreed to proceed: YES _________________
HISTORY OF PRESENT ILLNESS _______________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
PAST PSYCHIATRIC HISTORY ____________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
MEDICAL HISTORY: 1. Major Medical Problems _______________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
2. Current Medications _____________________________________________________________________________________
________________________________________________________________________________________________________
3. Allergies_______________________________________________________________________________________________
4. Tobacco Use____________________________________________________________________________________________
5. Alcohol Use____________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
Illicit Drug Use ___________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
Alcohol and/or Drug Complications: Legal________________________________Medical_______________________________
Job _______________________________Social_________________________Family __________________________________
Alcohol blackouts_______________________________Withdrawal symptoms_________________________________________
Chemical Dependency Tx ___________________________________________________________________________________
MEDICAL REVIEW OF SYMPTOMS ________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
FAMILY MEDICAL AND PSYCHIATRIC HlSTORY ___________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
SOCIAL HISTORY: 1. Devclopment. _________________________________________________________________________
2. Education ______________________________________________________________________________________________
3. Military History _________________________________________________________________________________________
4. Legal History ___________________________________________________________________________________________
5. Marital History __________________________________________________________________________________________
APPENDICES

2
6. Vocational History ___________________________________________________________________________
7. Current stressors______________________________________________________________________________
VITAL SIGNS: TEMP__________ BP_____________ PULSE_________ RESP _____ Sa02= ______ %
MENTAL STATUS EXAMINATION
Appearance ________________________________ Behavior ___________________________________________
Affect_____________________________________ Mood _____________________________________________
Speech____________________________________ Gait/Station _________________________________________
Muscle Strength & tone_______________________ Psychomotor functioning_ _____________________________
Perception, e.g., hallucinations_____________________________________________________________________
Thought content, e.g., delusions or obsessions_________________________________________________________
Thoughts of harming self or others__________________________________________________________________
Thought processes, e.g., associations_________________________________________________________________
Expressive & Receptive Language, e.g., naming objects__________________________________________________
Cognitive ft: level of consciousness____________________ Orientation____________________________________
Attention/conc.: Serial 7's____________________________ Spells world backwards: Yes ______ No _______
Memory: Remote__________________________Recent:____________________ Recalls __ /3 words after 3min
Fund of knowledge (e.g., current events; vocabulary) __________________________________________________
Abstract thinking _______________________________________________________________________________
Judgment______________________________________________________________________________________
Insight________________________________________________________________________________________
CURRENT LAB & RADIOLOGIC STUDIES________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
ASSESSMENT: DSM-5 DIAGNOSES:
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
RECOMMENDATIONS: 1. Further evaluation : _____________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
2. Psychopharmacological treatment: ______________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
3. Psychotherapeutic interventions: _______________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
4. Social/Family interventions: ___________________________________________________________________________
____________________________________________________________________________________________________
____________________________________________________________________________________________________
5. Is Chemical Dependency treatment indicated? _____________________________________________________________
6. Disposition:_________________________________________________________________________________________
Psychiatry assessment done by: _____________________________________________________ Date __________

3
Appendix B: For more information on absences, attendance expectations, dress code, protection from
mistreatment, blood-borne pathogens exposure, Counseling Services, UCF COM grading, etc., see the UCF
COM Student Handbook at http://med.ucf.edu/students/affairs/documents/student_handbook_2010.pdf
Appendix C: Website for “Five Minute Preceptor”:
http://www.oucom.ohiou.edu/fd/monographs/microskills.htm

4
Appendix D: Community Resources:

5
Appendix D: (continued)

6
APPENDIX E: Basis of Final Grade for the Psychiatry Clerkship The UCF COM utilizes a letter system: A (90-100); B (80-90); C (70-80); and F (below 70). The Clerkship Director determines the final grade based upon: 1. Preceptor Evaluations 50% 2. NBME shelf exam 20% 3. Clinical Skills Evaluations 10% 4. IRATs 10% 5. Case Write-Ups 10% 1. Preceptor Evaluations including narratives (see form) will be completed at the end of the clerkship by the pri-mary preceptors who have worked with the student at his/her clinical sites. The Clerkship Student Performance Evaluation form is used to determine a score from 1 to 8 (determined by which box is checked) in each of twelve different clinical areas. A final mean score is calculated for each evaluation using a scale of 1 to 8; scores falling between integers are rounded to the closest integer.
2. NBME Shelf Exam, which assesses students’ Medical Knowledge . The UCF COM has a NBME Shelf Exam Score Conversion Chart to allow conversion of NBME Scaled Scores to a COM grade/score. Also, a national listserv re-view among members of the Association of Directors of Medical Student Education in Psychiatry in January 2011 revealed the pattern utilized by medical schools to determine cutoff scores for determining grades based upon percentile score obtained on the NBME shelf exam in Psychiatry. These practices across the country were taken into consideration in determining that a percentile score at or above the 70th percentile MUST be obtained in order to be eligible to receive HONORS in the UCF COM Psychiatry Clerkship. Additionally, students must score at or above the 5th percentile in order to be eligible to pass the Clerkship. 3. Clinical Skills Evaluations (CSE): each student must complete at least two Psychiatry Clinical Skills Evaluations during the clerkship, utilizing a preceptor as the Examiner (see evaluation form in handbook). The Psychiatry Clinical Skills Evaluation Form is used to determine a score from 1 to 8 (determined by which box is checked) in each of ten different clinical areas. A final mean score is calculated for each evaluation using a scale of 1 to 8; scores falling between integers are rounded to the closest integer.
Evaluation Mean Score Grade %
Mean score of 8 100%
Mean score of 7 93%
Mean score of 6 87%
Mean score of 5 82%
Mean score of 4 77%
Mean score of 3 72%
Mean score of 2 67%
Mean score of 1 62%
Evaluation Mean Score Grade %
Mean score of 8 100%
Mean score of 7 93%
Mean score of 6 87%
Mean score of 5 82%
Mean score of 4 77%
Mean score of 3 72%
Mean score of 2 67%
Mean score of 1 62%
7
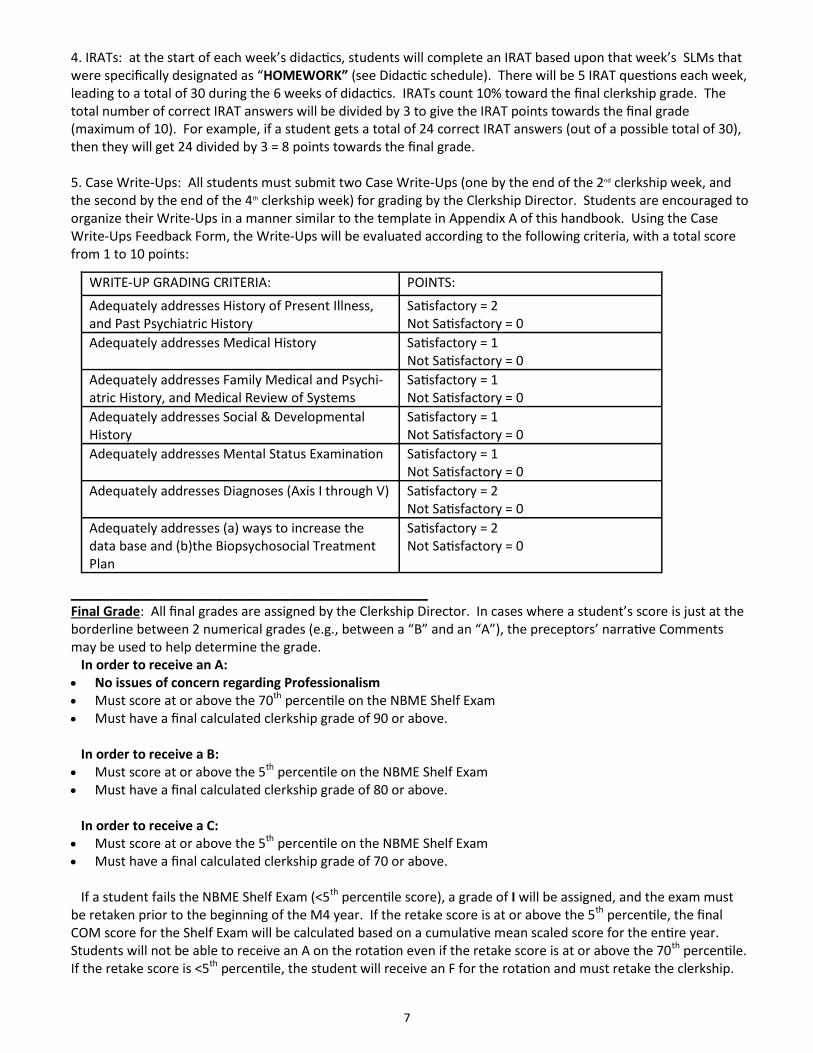
4. IRATs: at the start of each week’s didactics, students will complete an IRAT based upon that week’s SLMs that were specifically designated as “HOMEWORK” (see Didactic schedule). There will be 5 IRAT questions each week, leading to a total of 30 during the 6 weeks of didactics. IRATs count 10% toward the final clerkship grade. The total number of correct IRAT answers will be divided by 3 to give the IRAT points towards the final grade (maximum of 10). For example, if a student gets a total of 24 correct IRAT answers (out of a possible total of 30), then they will get 24 divided by 3 = 8 points towards the final grade. 5. Case Write-Ups: All students must submit two Case Write-Ups (one by the end of the 2nd clerkship week, and the second by the end of the 4th clerkship week) for grading by the Clerkship Director. Students are encouraged to organize their Write-Ups in a manner similar to the template in Appendix A of this handbook. Using the Case Write-Ups Feedback Form, the Write-Ups will be evaluated according to the following criteria, with a total score from 1 to 10 points:
_________________________________________________ Final Grade: All final grades are assigned by the Clerkship Director. In cases where a student’s score is just at the borderline between 2 numerical grades (e.g., between a “B” and an “A”), the preceptors’ narrative Comments may be used to help determine the grade. In order to receive an A: No issues of concern regarding Professionalism Must score at or above the 70th percentile on the NBME Shelf Exam Must have a final calculated clerkship grade of 90 or above. In order to receive a B: Must score at or above the 5th percentile on the NBME Shelf Exam Must have a final calculated clerkship grade of 80 or above. In order to receive a C: Must score at or above the 5th percentile on the NBME Shelf Exam Must have a final calculated clerkship grade of 70 or above. If a student fails the NBME Shelf Exam (<5th percentile score), a grade of I will be assigned, and the exam must be retaken prior to the beginning of the M4 year. If the retake score is at or above the 5th percentile, the final COM score for the Shelf Exam will be calculated based on a cumulative mean scaled score for the entire year. Students will not be able to receive an A on the rotation even if the retake score is at or above the 70th percentile. If the retake score is <5th percentile, the student will receive an F for the rotation and must retake the clerkship.
WRITE-UP GRADING CRITERIA: POINTS:
Adequately addresses History of Present Illness, and Past Psychiatric History
Satisfactory = 2
Not Satisfactory = 0
Adequately addresses Medical History Satisfactory = 1
Not Satisfactory = 0
Adequately addresses Family Medical and Psychi-atric History, and Medical Review of Systems
Satisfactory = 1
Not Satisfactory = 0
Adequately addresses Social & Developmental History
Satisfactory = 1
Not Satisfactory = 0
Adequately addresses Mental Status Examination Satisfactory = 1
Not Satisfactory = 0
Adequately addresses Diagnoses (Axis I through V) Satisfactory = 2
Not Satisfactory = 0
Adequately addresses (a) ways to increase the data base and (b)the Biopsychosocial Treatment Plan
Satisfactory = 2
Not Satisfactory = 0

8
APPENDIX F: PSYCHIATRY CLERKSHIP 6-WEEK TIMELINE/DUE DATES
Monday Tuesday Wednesday Thursday Friday
Week
#1
DIDACTICS at
COM, 1PM
Week
#2
DIDACTICS at
COM, 1PM
1st Case Write-up due
by this weekend
Week
#3
Students to complete
mid-clerkship self-
assessment and up-
date their clinical logs
& duty hours, in prepa-
ration for meeting with
Dr. Klapheke
DIDACTICS at
COM, 1PM
Mid-clerkship
meetings with
Dr. Klapheke
at COM.
1)Preceptors to sub-
mit Mid-Clerkship
Evaluations
Week
#4
DIDACTICS at
COM, 1PM
Mid-clerkship
meetings with
Dr. Klapheke
at COM
2nd Case Write-up
due by this weekend
Week
#5
DIDACTICS at
COM, 1PM
Remind students to
complete the clinical
log, Clinical Skills Eval-
uations & other
“passport” require-
ments (see page 32)
in order to sit for
NBME exam next
Friday
Week
#6
DIDACTICS at
COM, 1PM
1)Students be sure all
NBME “passport” re-
quirements are fulfilled.
2) Priceptors to submit
final evaluations of stu-
dents
3) Students to com-
plete and submit Clerk-
ship Evaluation and
Preceptor Evaluation
NBME shelf exam at
COM for students

9
Name Address Office Number Email
Department of Veterans Affairs
Paul A. Deci, MD Chief, Mental Health Services
5201 Raymond Street Orlando, FL 32803
321-397-6288 [email protected]
Silvana Montautti, MD Chief of Psychiatry & Site Director
5201 Raymond Street Orlando, FL 32803
407-621-2638 [email protected]
Lakeside Behavioral Healthcare
Jesse Tan, MD Medical Director & Site Director
434 W. Kennedy Blvd Orlando, FL 32810
407-875-3700 [email protected]
Thomas Greenman, LMHC Outpatient Clin-ical Director
1800 Mercy Drive, Suite 100 Orlando, FL 32808
407-875-3700 x 6140
Life Care Center
Eduardo Diaz, MD Site Director
989 Orienta Avenue Altamonte Springs, FL
32701 407-831-3446 [email protected]
Mark Williams, MD
989 Orienta Avenue Altamonte Springs, FL
32701 407-831-3446 [email protected] Pasadena Villa
Myrtho Mompoint-Branch, MD Medical Director & Site Director
625 Virginia Avenue Orlando, FL 32803
877-845-5235 [email protected]
Brandee Baldwin, HR Specialist 625 Virginia Avenue Orlando, FL 32803
407-896-2636 [email protected]
Central Florida BHC
Nasreen Malik, MD Site Director
6601 Central Florida Pkwy Orlando, FL 32821
407-370-0111 [email protected]
Park Place BH
Garrett Griffin, Psy.D Site Director
208 Park Place Blvd. Kissimmee, FL 34741
407-846-0023 EXT 1302
Steven Speiser, M.D 208 Park Place Blvd. Kissimmee, FL 34741
407-846-0023 EXT 1116
Coastal Mental Health Cen-
ter
Christine Grissom, MD 197 Bouganvillea Drive,
Suite A Rockledge, FL 32955
321-633-2398 (office)
407-342-1255 (cell)
Psychiatric Group of Orlan-
do
Ali El-Menshawi, MD, Ph.D 422 S. Alafaya Trail, Suite 17
Orlando, FL 32828 407-275-0745 [email protected]
Circles of Care
Kazi Ahmad, MD Harbour Pines—880 Airport Blvd. Melbourne, FL 32901
321-557-0105 [email protected]
UCF College of Medicine
Martin Klapheke, MD Clerkship Director Lake Nona Campus
407-266-1183 (office)
407-284-0724 (cell)
APPENDIX G: Clerkship Site Contact List

10
APPENDIX H: The following web address will direct you to the UCF College of medicine
Volunteer and Affiliated Faculty Handbook, as well as other pertinent
information regarding volunteer faculty appointments.
http://www.med.ucf.edu/faculty/affairs/va_faculty.asp
APPENDIX I:
The American Psychiatric Association (APA) offers free membership to medical students.
Their association’s mission is listed as the following:
To promote the highest quality care for individuals with mental disorders (including intel-
lectual developmental disorders and substance use disorders) and their families;
To promote psychiatric education and research; advance and represent the profession of
psychiatry; and
To serve the professional needs of its membership.
They have over 36,000 member physicians and the APA website offers numerous valuable
resources for healthcare workers in the psychiatric field, including list-servs, discussion
boards, newsletters, and discounted journals.
If interested in joining, you will find the online membership application for medical
students here:
http://apps.psychiatry.org/membershipapplications/MedStudentMemshipApp.aspx