aortic stenosis and mitral regurgitation: gudelines ... · “absence of the aortic second sound is...
TRANSCRIPT
Aortic Stenosis and Mitral Regurgitation:
Gudelines Evolution
SYNERGY 2018Louis Heller, MD FACC FSCAI
Nothing Much Has Changed
Circulation. 2018;137:2099-2100
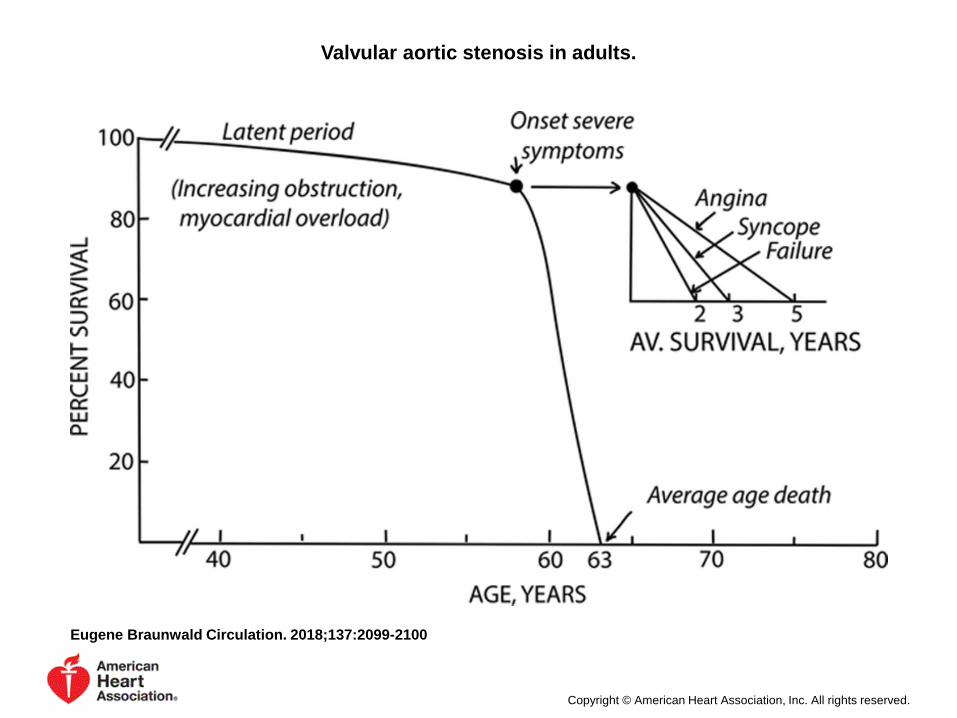
Valvular aortic stenosis in adults.
Eugene Braunwald Circulation. 2018;137:2099-2100
Copyright © American Heart Association, Inc. All rights reserved.
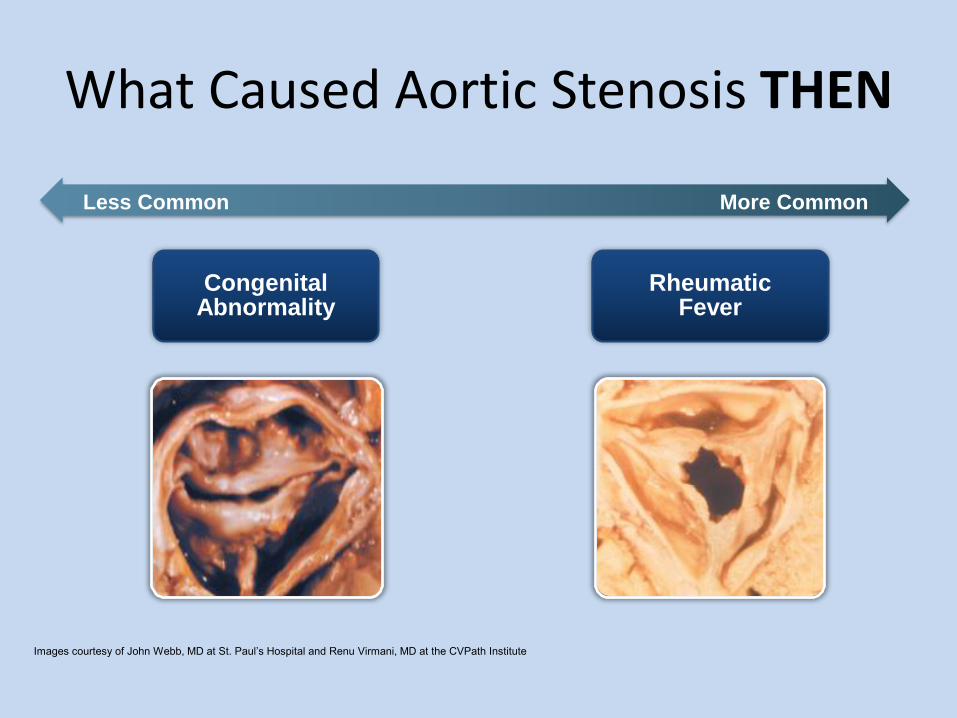
What Caused Aortic Stenosis THEN
More CommonLess Common
Images courtesy of John Webb, MD at St. Paul’s Hospital and Renu Virmani, MD at the CVPath Institute
Congenital Abnormality
RheumaticFever
“Absence of the aortic second sound is rare in aortic stenosis, and when so recorded usually implies ignorance of modern auscultatorytechniques and nomenclature”.
Wood P. Aortic stenosis. Am J Cardiol. 1958;1:553–571.
• “At the present time aortic valvotomy is too hazardous and too crude an operation to advise when it is most desirable (just before the onset of symptoms) and frequently too late when impending disaster makes it imperative “
Wood P. Aortic stenosis. Am J Cardiol. 1958;1:553–571.
Aortic Stenosis: Then
• Most cases rheumatic
• Circa 1960: No OHS or LHC
• No echo
• Diagnosis by auscultation
• 1970s: SAVR mortality 15%
• Only 2/3 had symptomatic improvement
• Remainder : irreversible myo damage + CHF
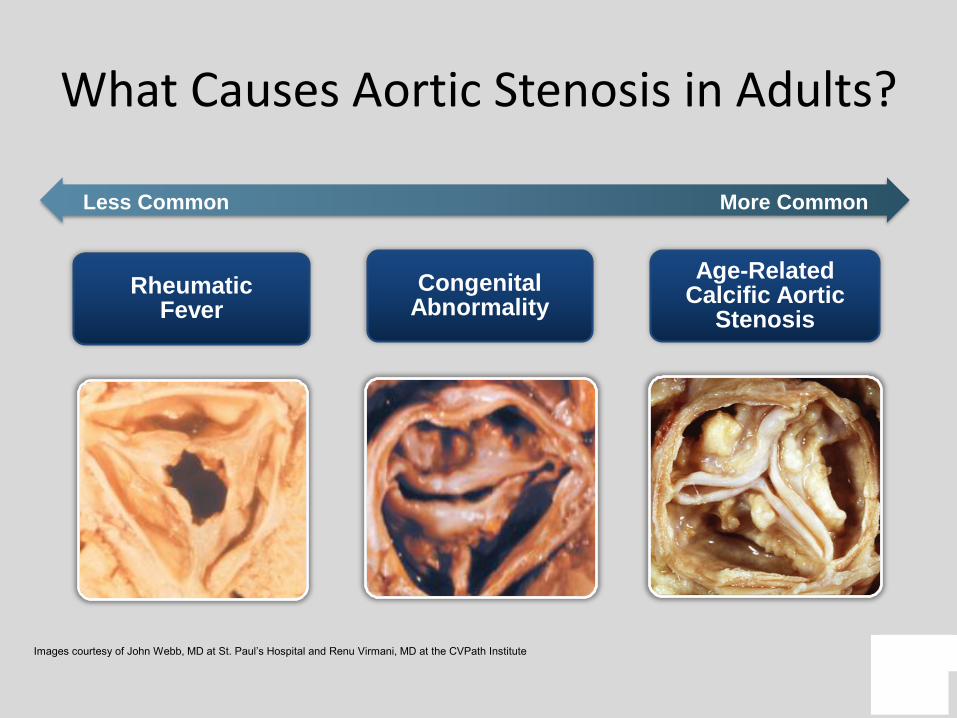
What Causes Aortic Stenosis in Adults?
More CommonLess Common
Images courtesy of John Webb, MD at St. Paul’s Hospital and Renu Virmani, MD at the CVPath Institute
Age-Related Calcific Aortic
Stenosis
Congenital Abnormality
RheumaticFever
Aortic Stenosis: NOW
• Most cases SENILE CALCIFIC
• Diagnosis by echo
• Retrograde LHC and coronary angiography
• CABG
• SAVR mortality 3% and widely available
• People live longer
13
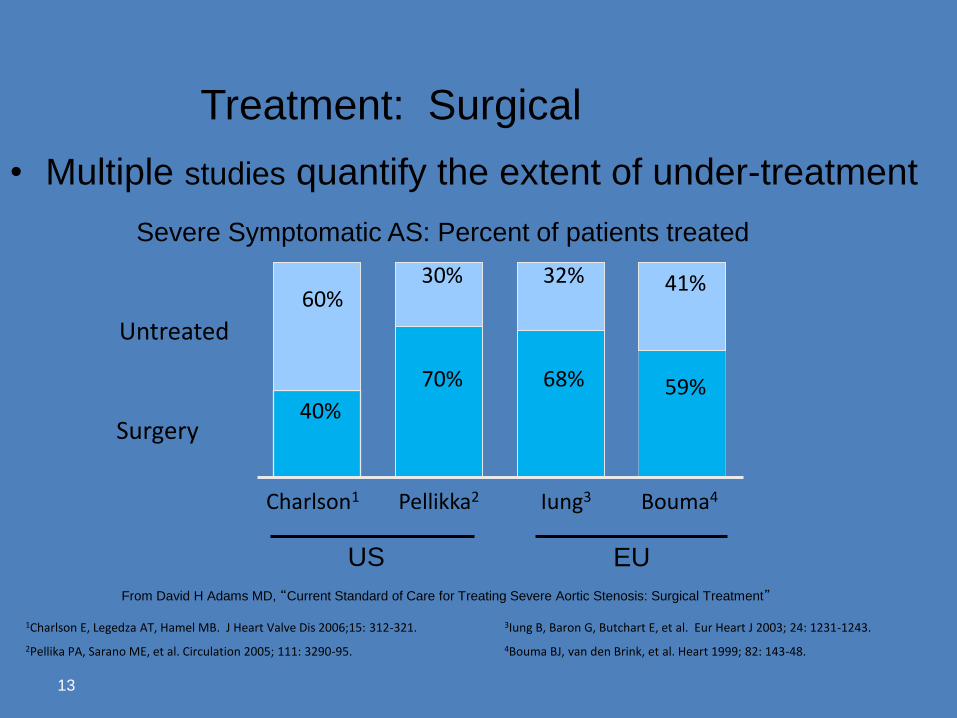
Severe Symptomatic AS: Percent of patients treated
EUUS
Untreated
Surgery
Pellikka2Charlson1 Iung3 Bouma4
59%68%70%
40%
41%32%30%60%
• Multiple studies quantify the extent of under-treatment
Treatment: Surgical
From David H Adams MD, “Current Standard of Care for Treating Severe Aortic Stenosis: Surgical Treatment”
1Charlson E, Legedza AT, Hamel MB. J Heart Valve Dis 2006;15: 312-321. 3Iung B, Baron G, Butchart E, et al. Eur Heart J 2003; 24: 1231-1243.
4Bouma BJ, van den Brink, et al. Heart 1999; 82: 143-48.2Pellika PA, Sarano ME, et al. Circulation 2005; 111: 3290-95.
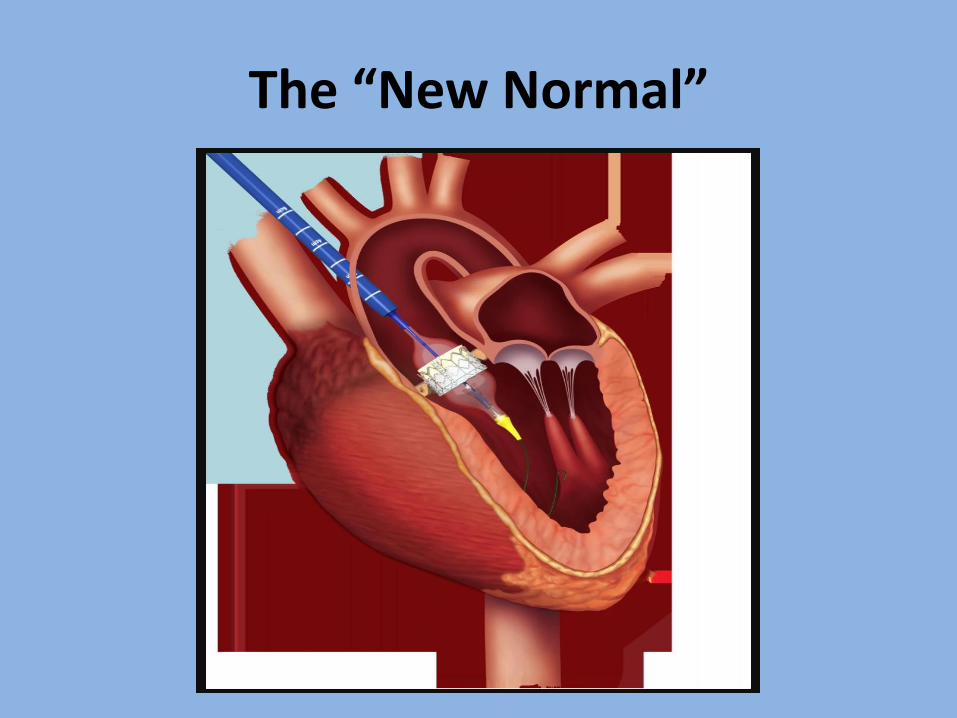
The “New Normal”
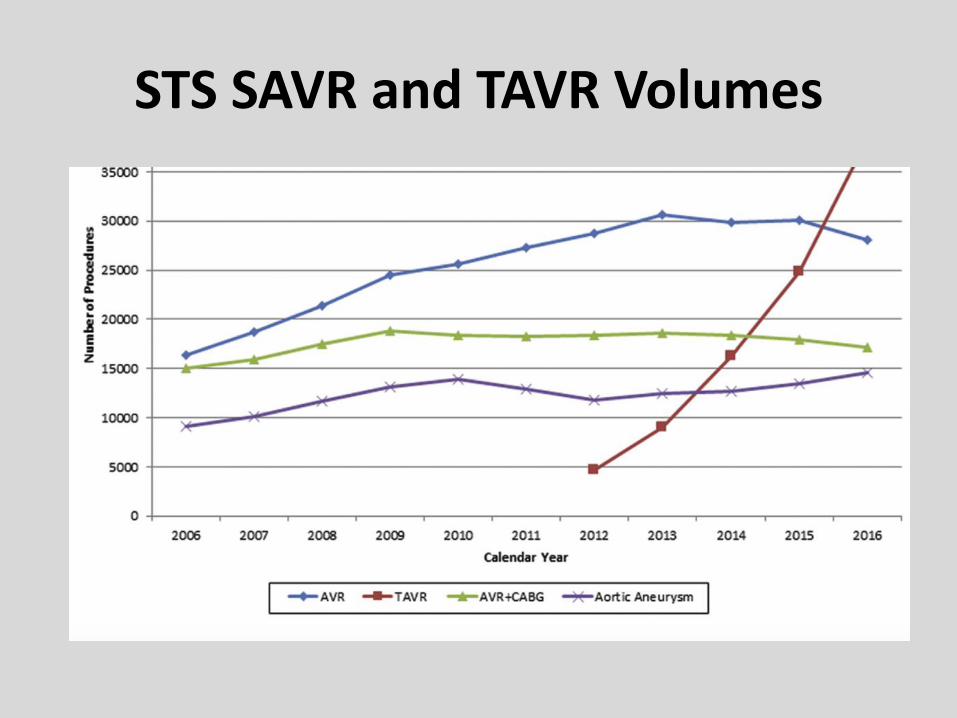
STS SAVR and TAVR Volumes
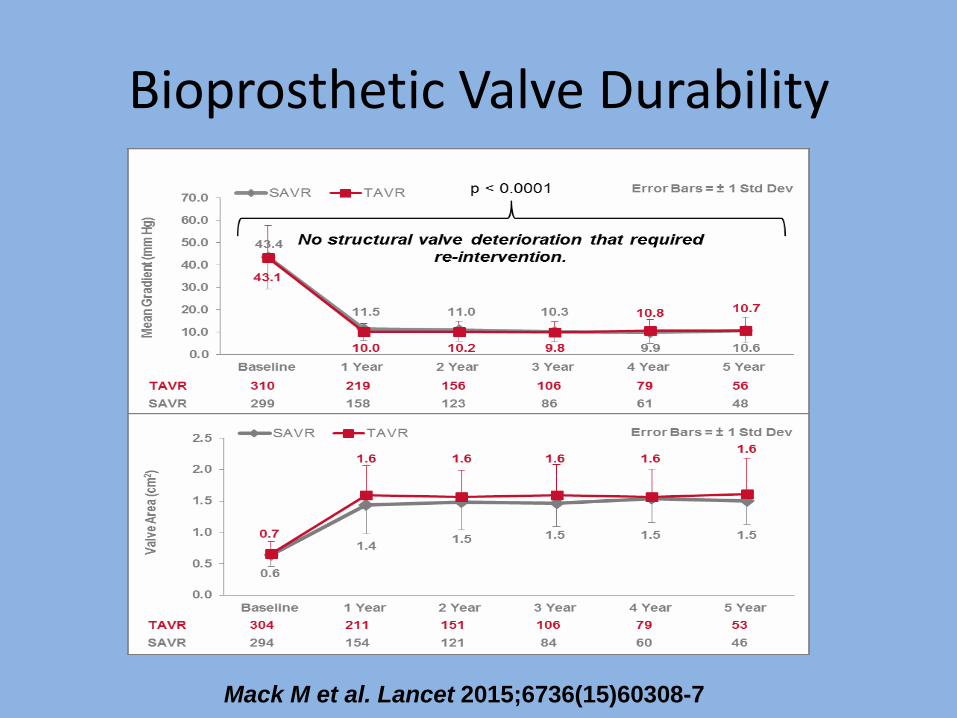
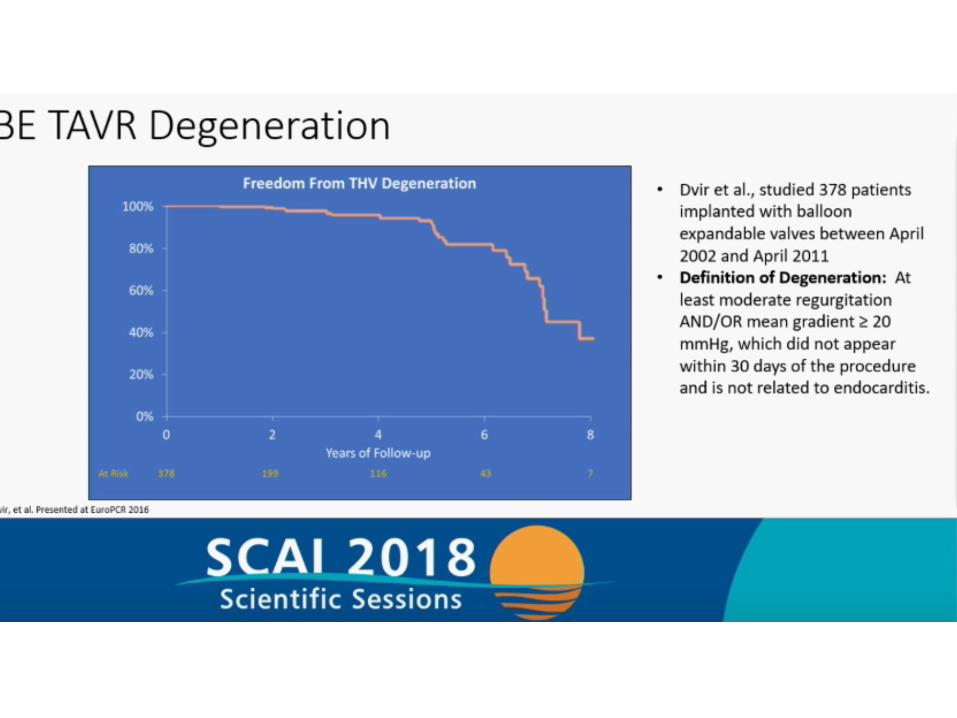
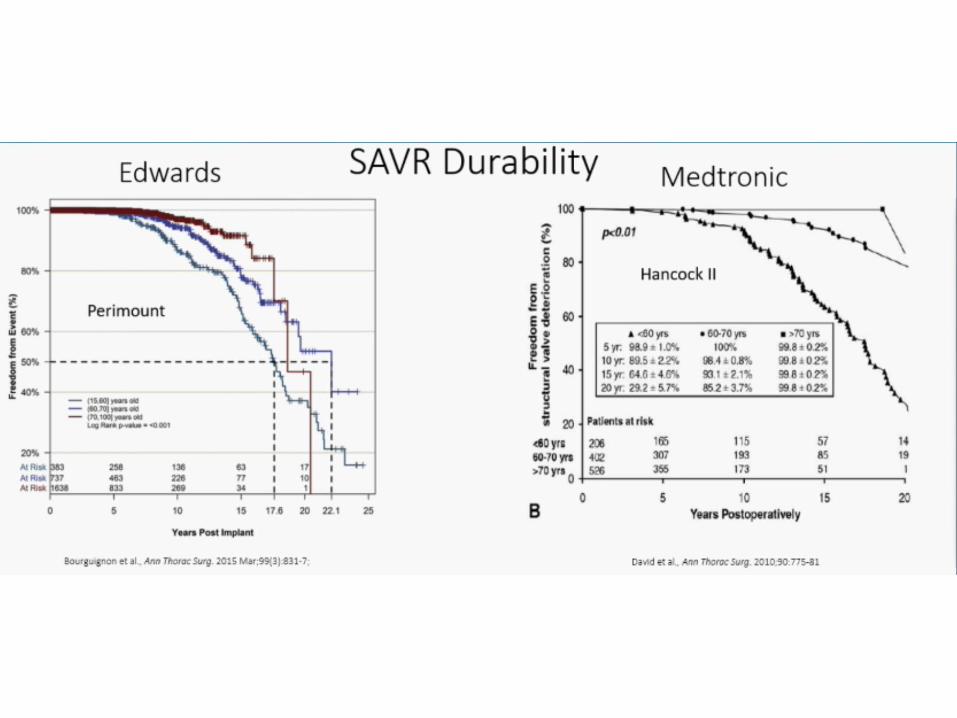
Bioprosthetic Valve Durability
Mack M et al. Lancet 2015;6736(15)60308-7
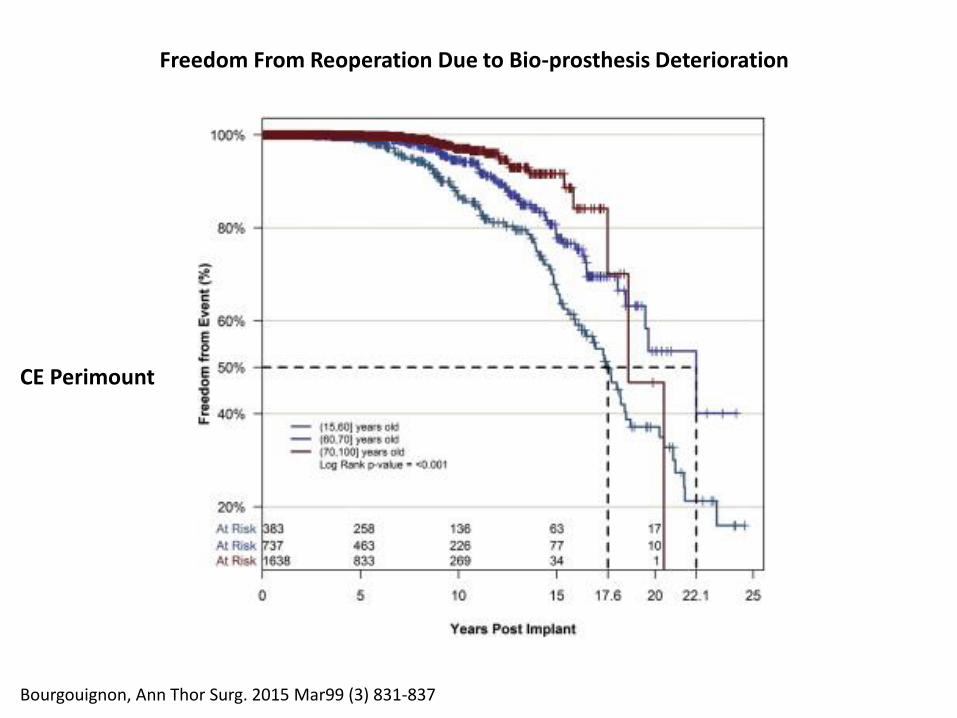
Fig 3
The Annals of Thoracic Surgery 2015 99, 831-837DOI: (10.1016/j.athoracsur.2014.09.030) Bourgouignon, Ann Thor Surg. 2015 Mar99 (3) 831-837
CE Perimount
Freedom From Reoperation Due to Bio-prosthesis Deterioration
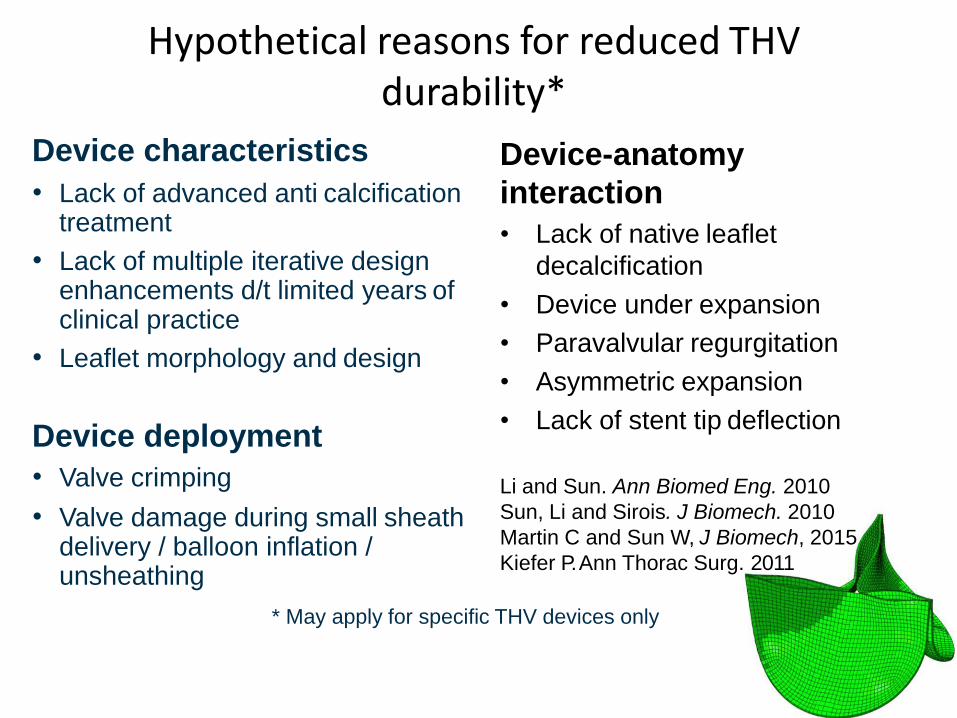
Hypothetical reasons for reduced THVdurability*
Device characteristics
• Lack of advanced anti calcification treatment
• Lack of multiple iterative design enhancements d/t limited years of clinical practice
• Leaflet morphology and design
Device deployment
• Valve crimping
• Valve damage during small sheath delivery / balloon inflation / unsheathing
Device-anatomy
interaction
• Lack of native leaflet
decalcification
• Device under expansion
• Paravalvular regurgitation
• Asymmetric expansion
• Lack of stent tip deflection
Li and Sun. Ann Biomed Eng. 2010
Sun, Li and Sirois. J Biomech. 2010
Martin C and Sun W, J Biomech, 2015
Kiefer P. Ann Thorac Surg. 2011
* May apply for specific THV devices only
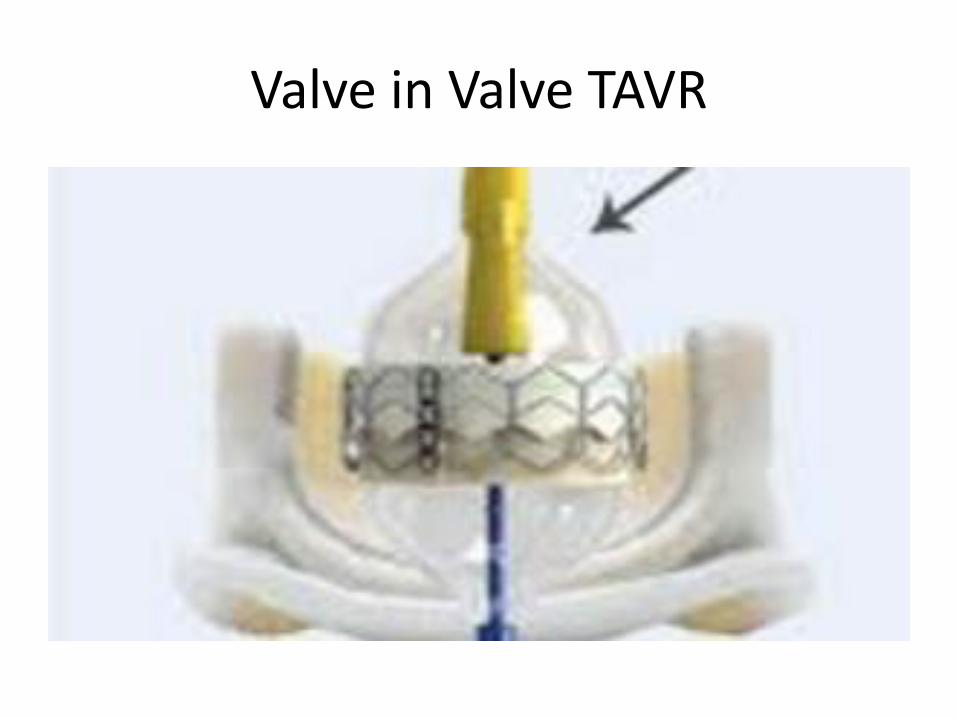
Valve in Valve TAVR
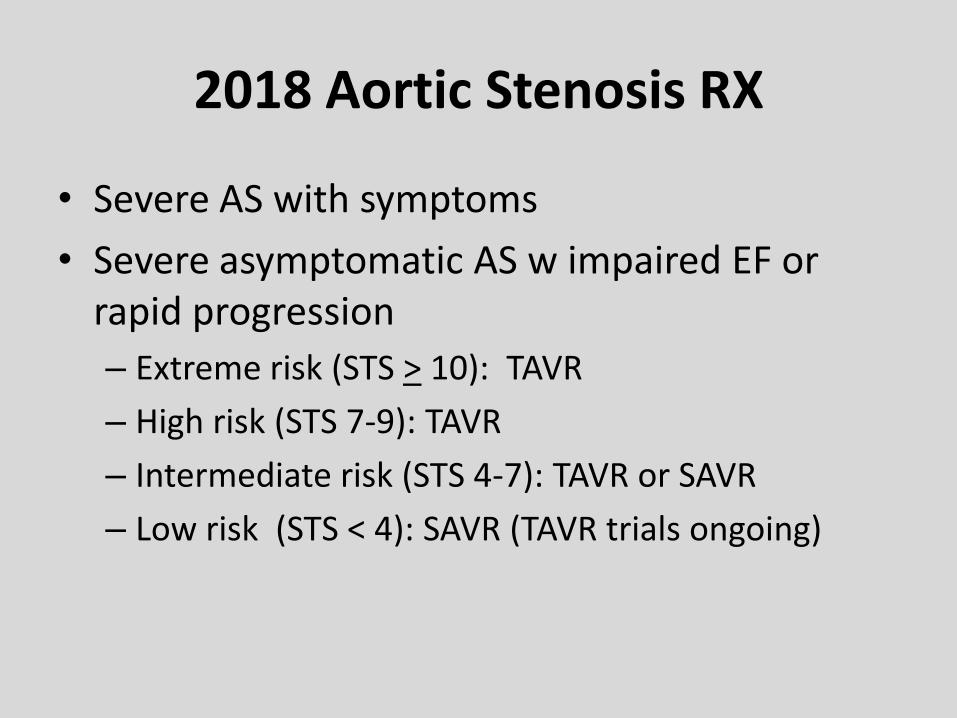
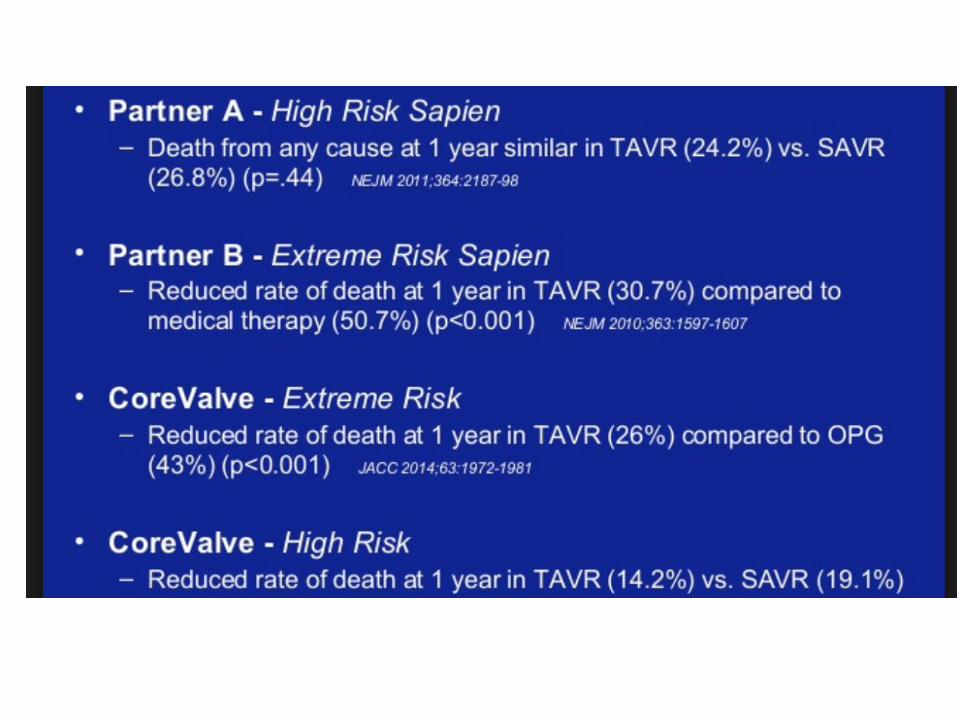
2018 Aortic Stenosis RX
• Severe AS with symptoms
• Severe asymptomatic AS w impaired EF or rapid progression
– Extreme risk (STS > 10): TAVR
– High risk (STS 7-9): TAVR
– Intermediate risk (STS 4-7): TAVR or SAVR
– Low risk (STS < 4): SAVR (TAVR trials ongoing)
TAVR : Future Challenges and Trends
• Bicuspid valves
• Valve durability
– Younger patients
– Limited long term data (>10 years)
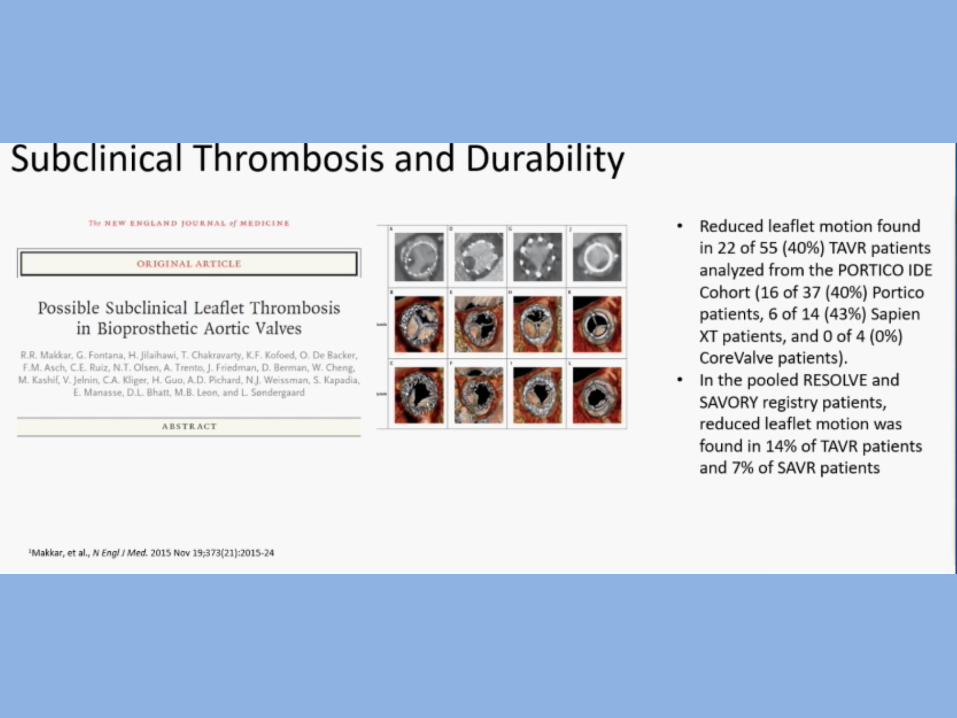
– Subclinical leaflet thrombosis
– Paravalvular leaks – assessment and Rx
– Increasing Valve-in-Valve procedures
• Cardiologists will be the gate keepers
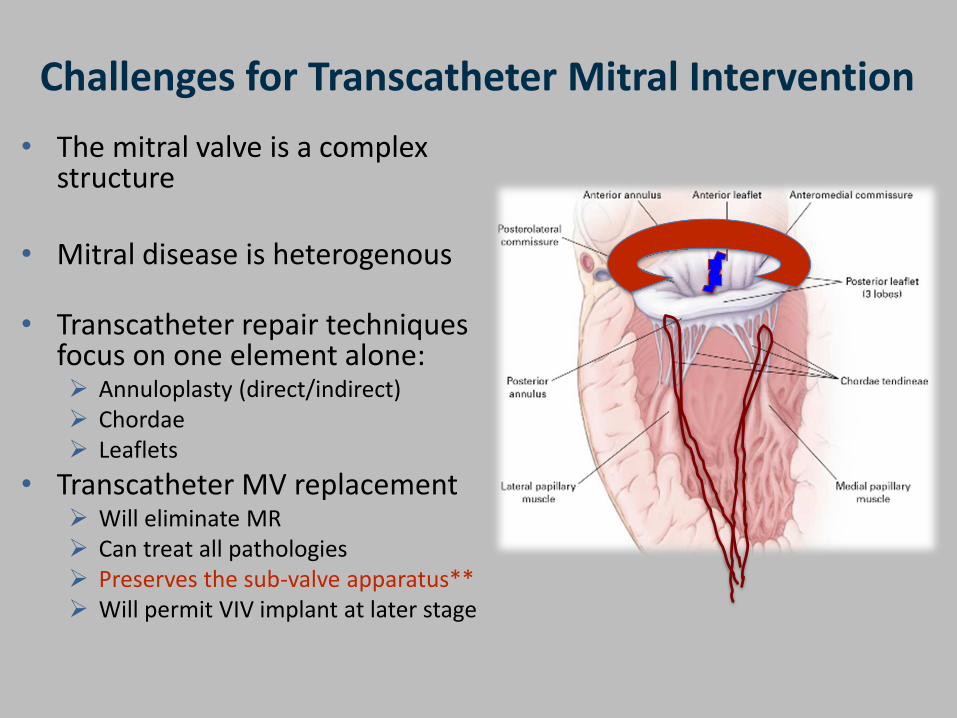
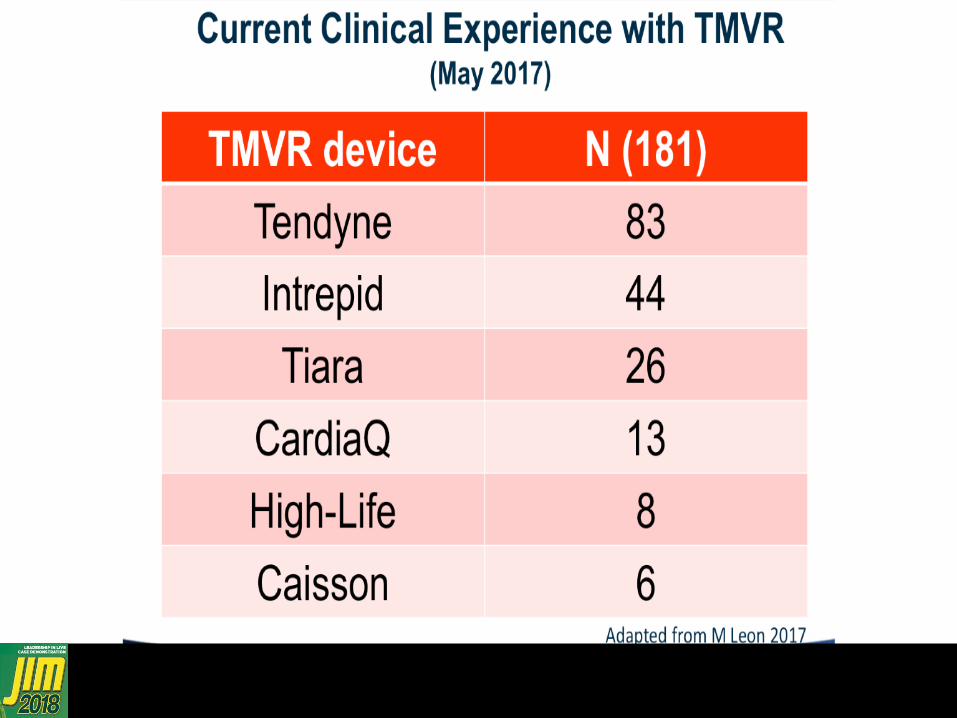
Challenges for Transcatheter Mitral Intervention
• The mitral valve is a complex structure
• Mitral disease is heterogenous
• Transcatheter repair techniques focus on one element alone: ➢ Annuloplasty (direct/indirect) ➢ Chordae ➢ Leaflets
• Transcatheter MV replacement➢ Will eliminate MR➢ Can treat all pathologies➢ Preserves the sub-valve apparatus**➢ Will permit VIV implant at later stage
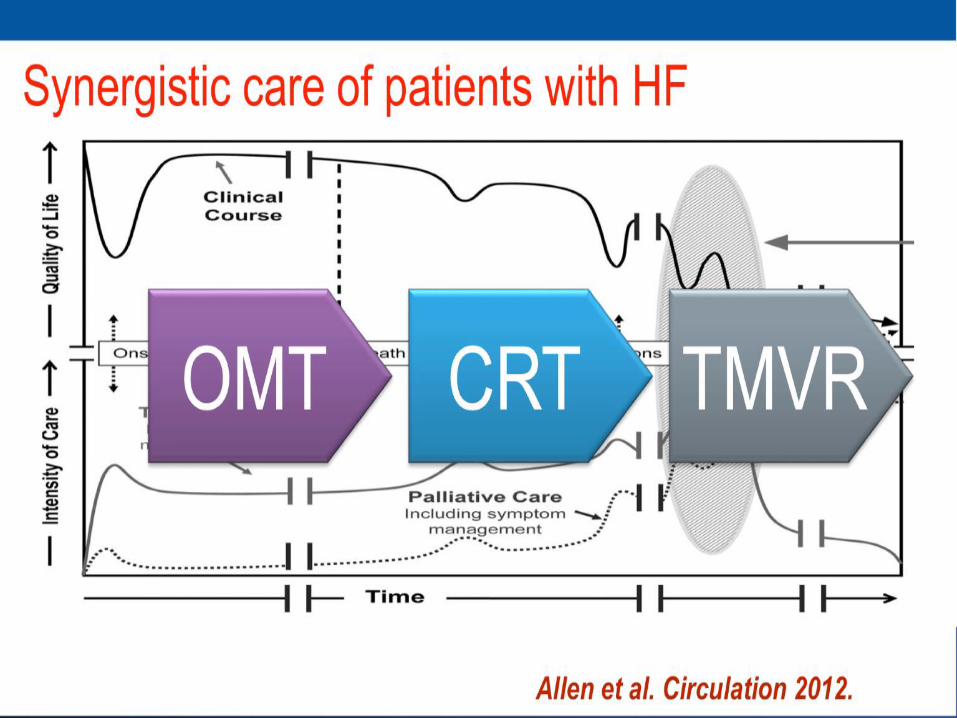
The Natural History of Mitral Regurgitation
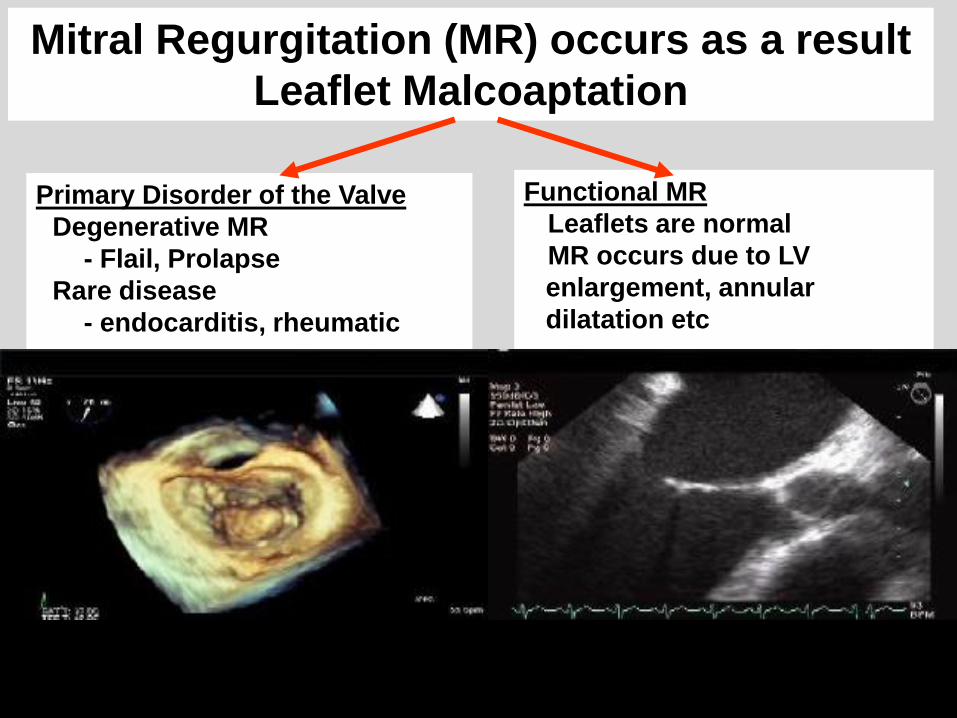
Mitral Regurgitation (MR) occurs as a result
Leaflet Malcoaptation
Primary Disorder of the Valve
• Degenerative MR
- Flail, Prolapse
• Rare disease
- endocarditis, rheumatic
Functional MR
• Leaflets are normal
• MR occurs due to LV
enlargement, annular
dilatation etc
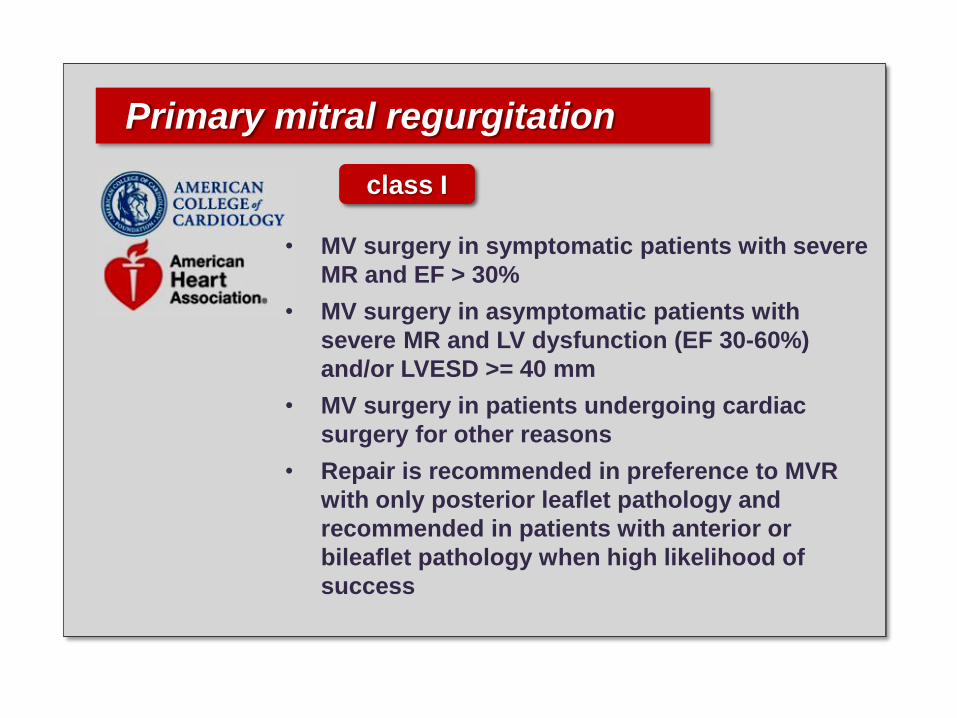
Primary mitral regurgitation
class I
• MV surgery in symptomatic patients with severe
MR and EF > 30%
• MV surgery in asymptomatic patients with
severe MR and LV dysfunction (EF 30-60%)
and/or LVESD >= 40 mm
• MV surgery in patients undergoing cardiac
surgery for other reasons
• Repair is recommended in preference to MVR
with only posterior leaflet pathology and
recommended in patients with anterior or
bileaflet pathology when high likelihood of
success
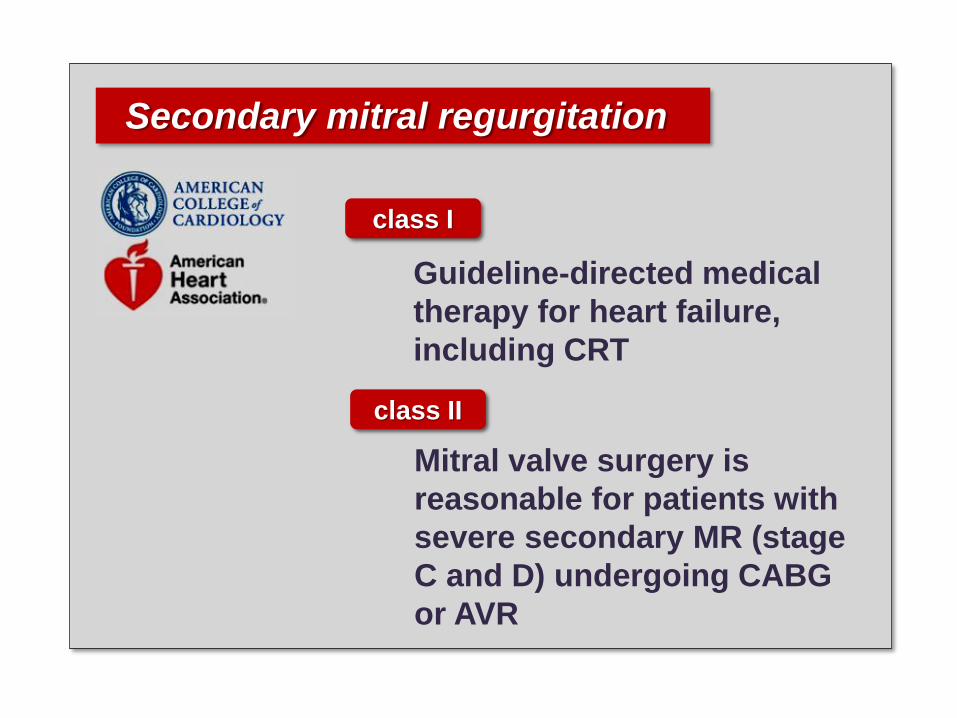
Secondary mitral regurgitation
class I
Guideline-directed medical
therapy for heart failure,
including CRT
class II
Mitral valve surgery is
reasonable for patients with
severe secondary MR (stage
C and D) undergoing CABG
or AVR
Basic Premise of Transcatheter Valve Therapy Development
➢Transcatheter devices mimic established surgical therapies
➢Therapies should demonstrate benefit (i.e. lower or equivalent mortality) when compared with “gold-standard” established therapies (presumably surgery)
Copyright ©2011 American College of Cardiology Foundation. Restrictions may apply.
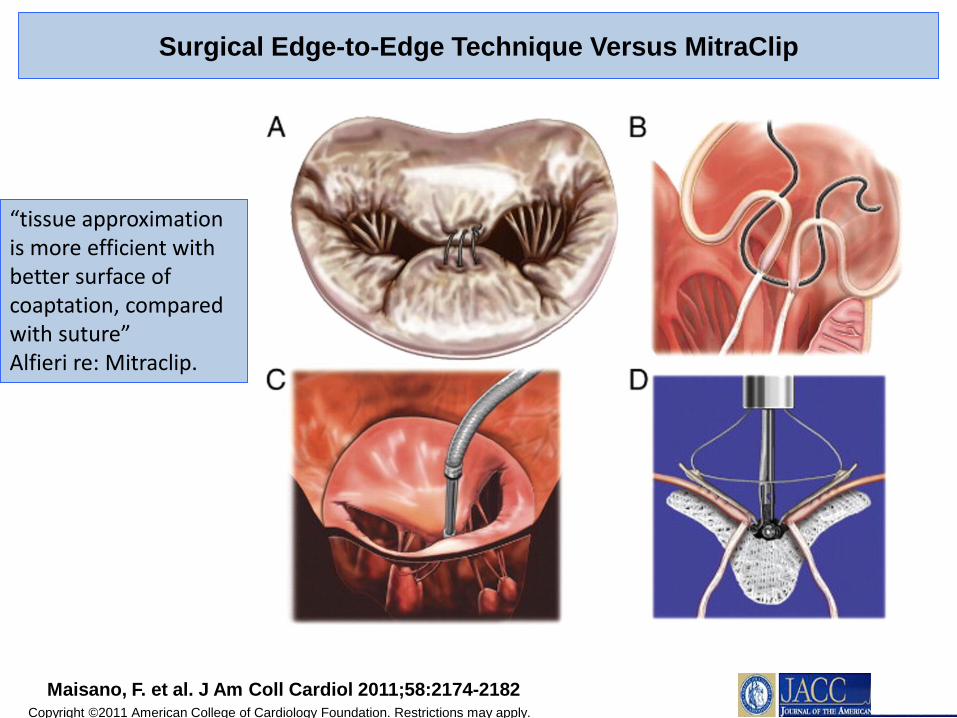
Maisano, F. et al. J Am Coll Cardiol 2011;58:2174-2182
Surgical Edge-to-Edge Technique Versus MitraClip
“tissue approximation is more efficient with better surface of coaptation, compared with suture” Alfieri re: Mitraclip.
34
0%
20%
40%
60%
80%
100%
Baseline 12 Months Baseline 12 Months
Device Group Control Group
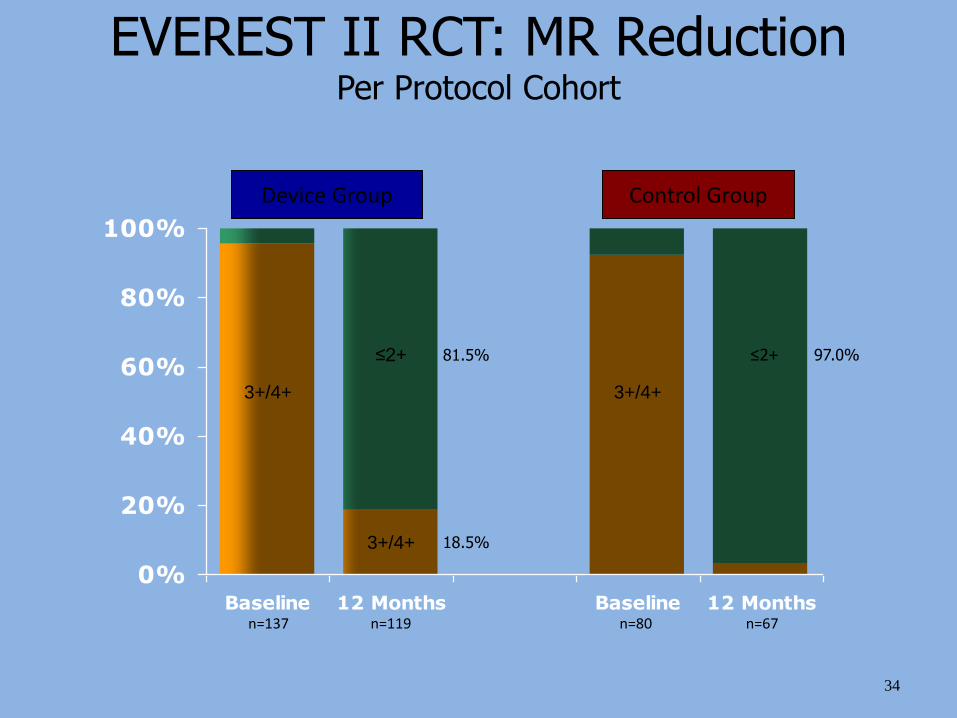
EVEREST II RCT: MR ReductionPer Protocol Cohort
≤2+
n=137 n=119 n=80 n=67
3+/4+
≤2+
3+/4+
81.5%
18.5%3+/4+
97.0%
0
20
40
60
80
100
Perc
ent
Patients
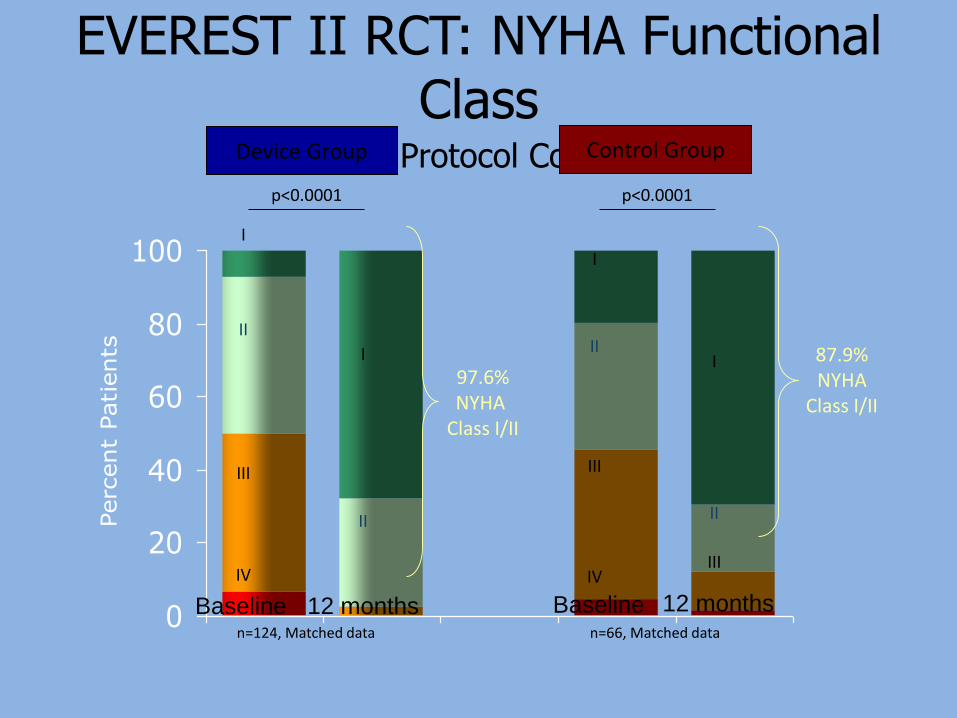
EVEREST II RCT: NYHA Functional Class
Per Protocol Cohort
97.6%NYHA
Class I/II
87.9%NYHA
Class I/II
n=124, Matched data n=66, Matched data
I
II
III
I
II
III
IVIV
III
II
I
II
I
Device Group Control Group
Baseline Baseline12 months 12 months
p<0.0001 p<0.0001
Transcatheter Mitral Valve Treatment
• The field is in it’s infancy and many technical challenges remain
• The runaway success of TAVR will be difficult to emulate.
• Treatment paradigms for functional MR remain uncertain
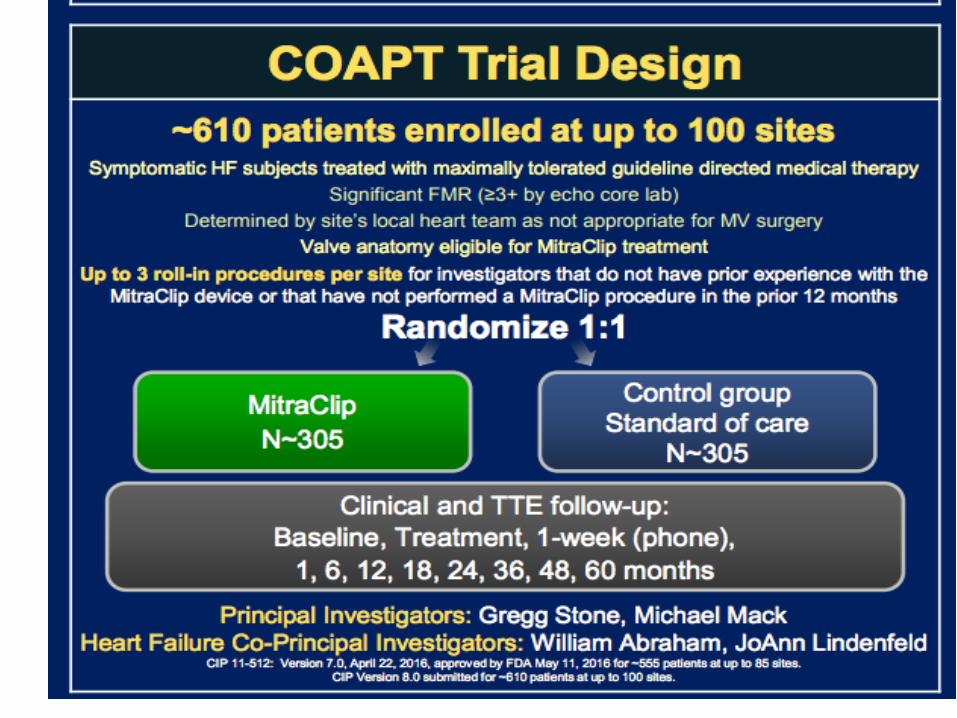
• Trial designs for transcatheter devices unclear– MR etiology – Functional vs Degenerative– Control arm – Surgical vs Medical Therapy– Primary endpoint ? – Stay tuned: COAPT and MITRA-FR
An 80 year old woman 16 years s/p surgical AVR with a mechanical valve presents with recurrent CHF. Echo reveals severe aortic insufficiency and an EF of 45%. Her home medications include furosemide, lisinopril, and carvedilol at home. EKG reveals and old IWMI. The best treatment option is :
(1) Adjust diuretics and add aldactone.
(2) CRT
(3) TAVR
(4) Re-do AVR
An 80 year old woman 16 years s/p surgical AVR with a mechanical valve presents with recurrent CHF. Echo reveals severe aortic insufficiency and an EF of 45%. Here home medications include furosemide, lisinopril, and carvedilol. EKG reveals and old IWMI. The best treatment option is :
(1) Adjust diuretics and add aldactone.
(2) CRT
(3) TAVR
(4) Re-do AVR
A 55 year old woman w known CM presents with recurrent CHF. EKG shows a new LBBB. She takes Entresto, furosemide and atenolol. Echo reveals moderate to severe MR and an EF = 40%. The best rxoption is:
(1) DC atenolol and titrate carvedilol.
(2) CRT
(3) Mitraclip
(4) Surgical MV replacement
(5) Surgical mitral valve repair
A 55 year old woman w a known CM presents with recurrent CHF. EKG shows a new LBBB. She takes Entresto, furosemide and atenolol at home. Echo reveals moderate to severe MR and an EF = 40%. The best rx option is:
(1) DC atenolol and titrate carvedilol.
(2) CRT
(3) Mitraclip
(4) Surgical MV replacement
(5) Surgical mitral valve repair
A 74 year old man presents with syncope. Cathreveals an 80% mid-RCA stenosis. PMH includes moderate COPD, prior CEA, and DM. Echo reveals severe AS and normal LV-EF. Acceptable treatment options are:
(1) AVR/CABG
(2) TAVR/PCI
(3) Evaluate for PPM.
(4) PCI and close f/u.
(5) #1 or #2
A 74 year old man presents with syncope. Cathreveals an 80% mid-RCA stenosis. PMH includes moderate COPD, prior CEA, and DM. Echo reveals severe AS and normal LV-EF. Acceptable treatment options are:
(1) AVR/CABG
(2) TAVR/PCI
(3) Evaluate for PPM.
(4) PCI and close f/u.
(5) #1 or #2

Thank you!
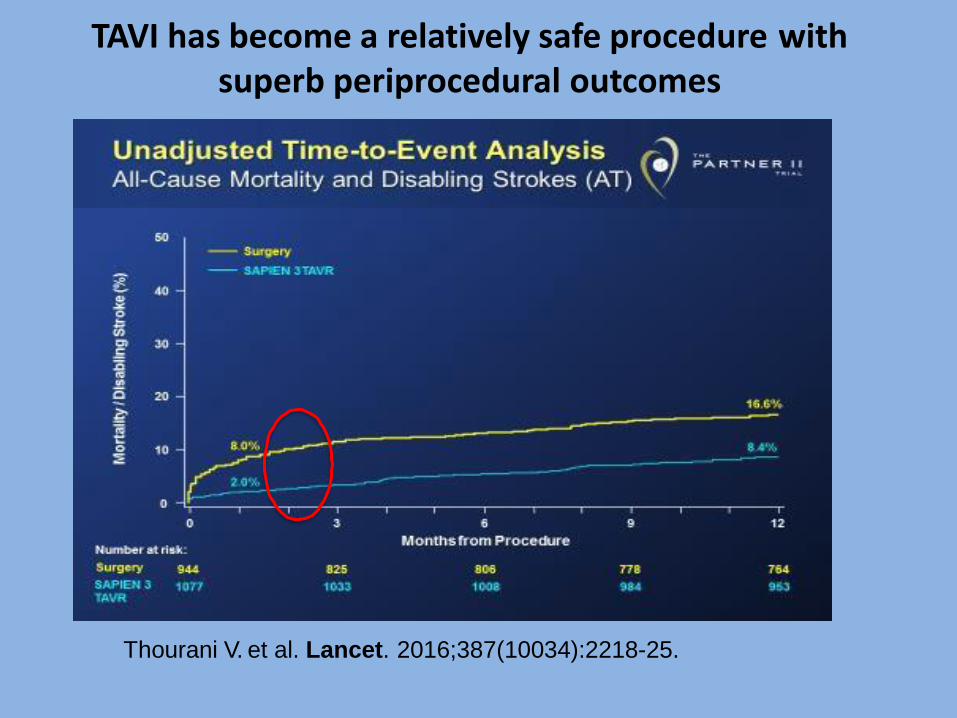
TAVI has become a relatively safe procedure withsuperb periprocedural outcomes
Thourani V. et al. Lancet. 2016;387(10034):2218-25.
5-YEAR SURVIVAL
(Distant Metastasis)8
Surv
ival, %
51
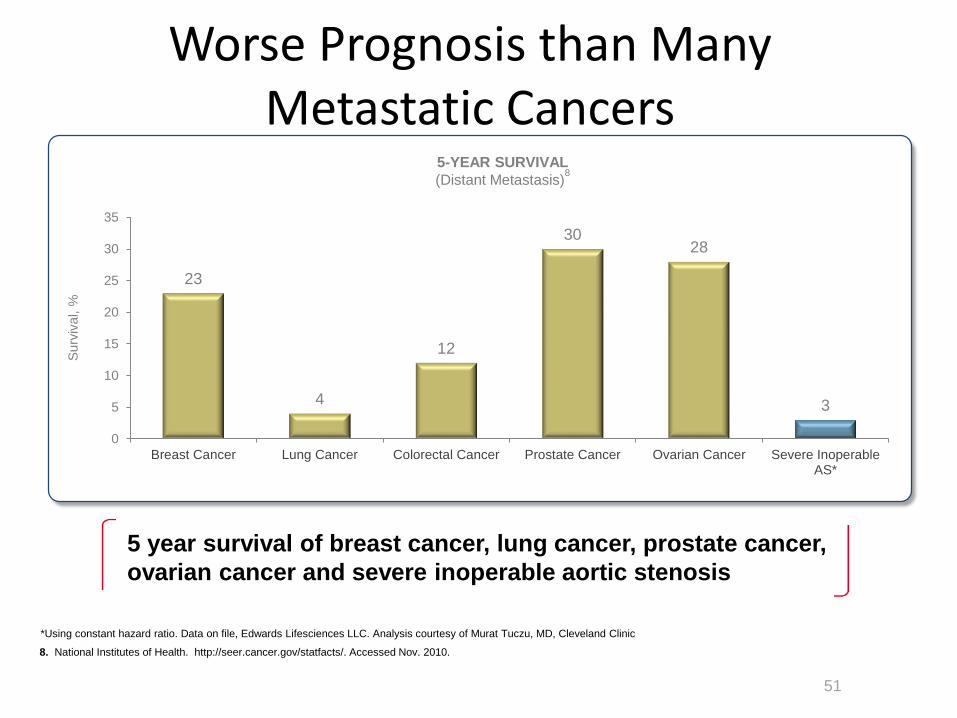
Worse Prognosis than Many Metastatic Cancers
5 year survival of breast cancer, lung cancer, prostate cancer,
ovarian cancer and severe inoperable aortic stenosis
23
4
12
3028
3
0
5
10
15
20
25
30
35
Breast Cancer Lung Cancer Colorectal Cancer Prostate Cancer Ovarian Cancer Severe InoperableAS*
*Using constant hazard ratio. Data on file, Edwards Lifesciences LLC. Analysis courtesy of Murat Tuczu, MD, Cleveland Clinic
8. National Institutes of Health. http://seer.cancer.gov/statfacts/. Accessed Nov. 2010.
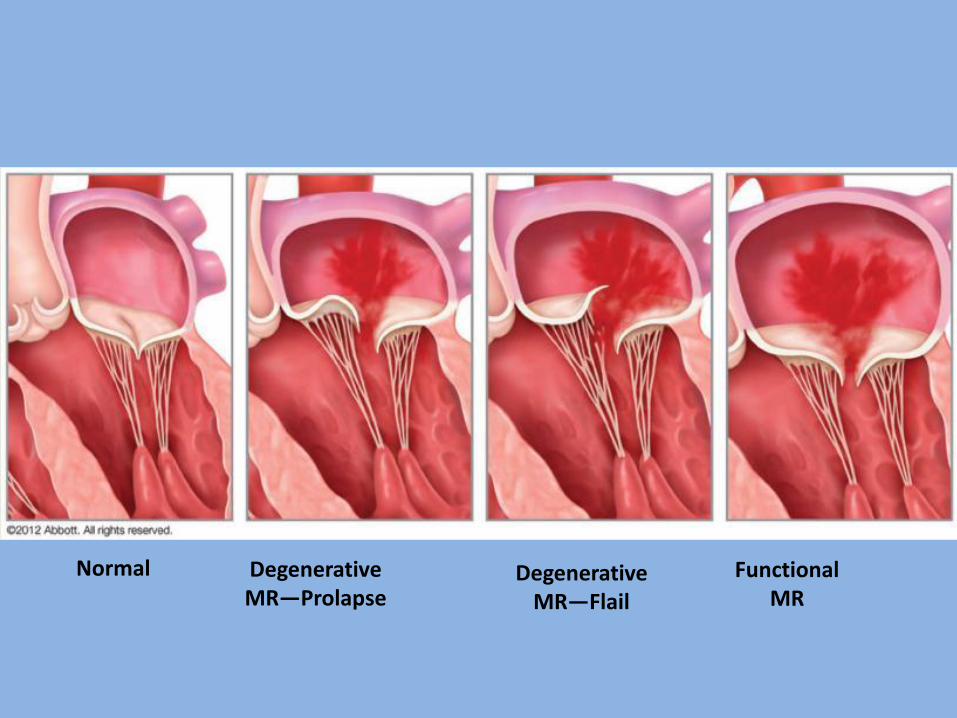
Normal Degenerative MR—Prolapse
Degenerative MR—Flail
Functional MR
What about Secondary Mitral
Regurgitation?
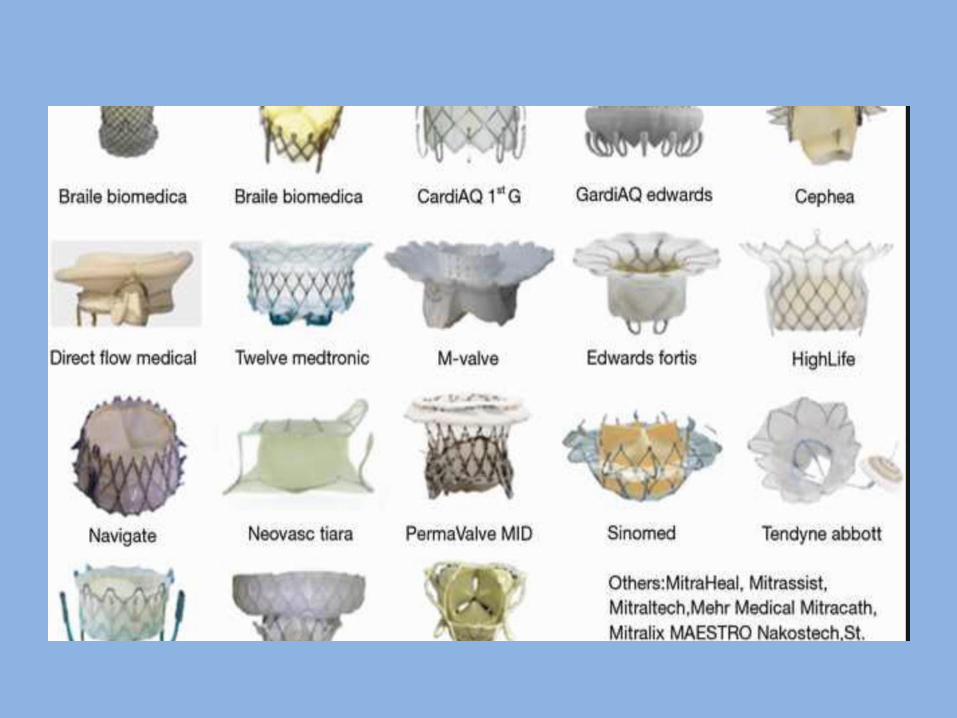
TAVR Devices Approved in the US
TMVR ≠ TAVR
❖Indications for Treatment
❖Comparator Population
❖Anatomic Challenges
Transcatheter Mitral Valve Repair Approaches
• Leaflet approach– Mitraclip– PASCAL
• Annuloplasty– Direct
• Edwards Cardioband• Millipede
– Indirect• MVRx Arto• GDS Accucinch• Carillon
As bioprosthetic SAVR and TAVR valves are indicated and implanted in younger patients, defining and understanding the durability of these valves will become increasingly important.
Shunk, SCAI 2018
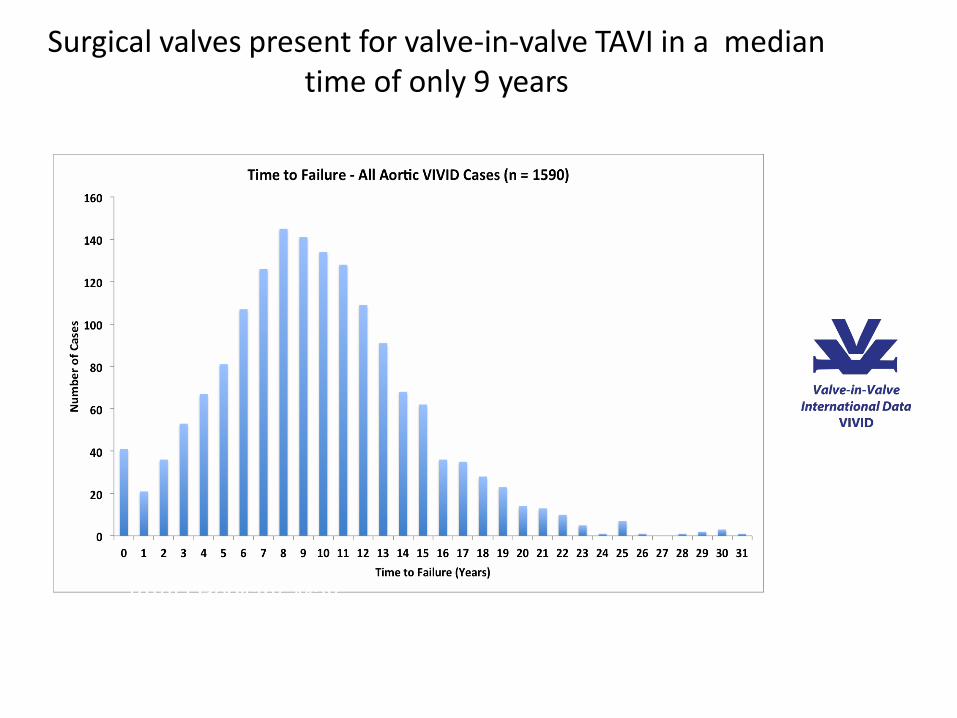
Surgical valves present for valve-in-valve TAVI in a median time of only 9 years
VIVID Registry. May
TAVR = TMVR because AS = MR
• TAVR: paradigm shift (a lot has happened)
– Emulates a surgical gold standard
– Natural history of AS well understood
• Transcatheter Rx for MR: a lot is happening
– Primary (degenerative) vs Secondary MR
– What is the gold standard for Secondary MR?
– Unlike AS, MR kills slowly