aortic root replacement - professional · chapter 33 aortic root replacement 527 the ascending...
TRANSCRIPT
525
33 Aortic Root Replacement Kaushik MandalDuke E. Cameron
KEY CONCEPTS
• Epidemiology • Aortic aneurysms were the 15th most common cause
of death in the United States in the year 2000. Among patients who die of thoracic aortic aneurysms (TAAs), rupture is the cause of death in about 80 percent of cases. Approximately 50 percent of thoracic aneurysms involve the root and the ascending aorta. The estimated growth rate for TAAs has been calculated to be 1.2 to 4.2 mm/year. Aneurysms that are larger than 6 cm can be associated with a yearly rate of rupture or dissection of at least 6.9 percent and a death rate of 11.8 percent.
• Pathophysiology • Annuloaortic ectasia is a term used to describe an
increase in diameter of the aortic annulus coupled with an increase in the diameter of the aortic root. This type of situation is seen in patients with Marfan syndrome, Ehlers–Danlos syndrome, Loeys–Deitz syndrome, osteogenesis imperfecta, and pseudoxanthoma elasticum. Annuloaortic ectasia may have familial origins or may be idiopathic. Recently, a significant body of research has focused on the involvement of endogenous extracellular matrix-degrading enzymes in aneurysms and aortic remodeling. Of greatest interest are the matrix metalloproteinases (MMPs), particularly those of the gelatinase class (MMP-2, MMP-9). Similarly ARB2 receptor blockade with Losartan has shown to slow the dilatation of aorta in animal model studies. Another important cause of aortic root destruction is acute infective endocarditis with aggressive organisms such as Staphylococcus aureus. A central common theme in the development of aortic root aneurysms is cystic medial degeneration, in which gradual disruption of the media of the aorta occurs, with the creation of small acellular spaces within it. This process weakens the aortic wall, and a slow remodeling of the aortic root and ascending aorta results in aneurysm formation.
• Clinical features • Most patients with aortic root pathology are
asymptomatic, with the exception of patients who present with endocarditis (sepsis, congestive heart
failure) or aortic root destruction secondary to acute type A aortic dissection (severe chest pains, asymmetric pulses, congestive heart failure). The age range of presentation is very broad (twenties to eighties) and is dependent on the underlying pathology. Certain patients will have characteristic stigmata of connective tissue diseases such as Marfan syndrome.
• Diagnostics • The workup for candidates for aortic root replacement
includes echocardiography to estimate ventricular function and assess for the possibility of aortic valve preservation. Coronary catheterization is usually necessary to rule out coronary artery disease. Thin-slice computed tomography (CT) or magnetic resonance imaging (MRI) scanning will provide the necessary information about the anatomy of the aneurysm. A careful oral examination or dental consultation is very important to prevent postoperative prosthetic valve infection.
• Treatment • Aortic root replacement options include composite
valve-graft, separate valve-graft, xenograft tissue, homograft, pulmonary autograft (Ross procedure), and valve-sparing aortic root replacement. The decision to use each one of these options is dependent on patient age and valve preference, comorbid conditions, the condition of the native aortic valve, and contraindications to the use of anticoagulants.
• Outcomes • Operative (30-day) mortality runs in the range of 0 to
10 percent. Reoperation for mediastinal hemorrhage should be required in less than 10 percent of cases. Complete heart block requiring pacemaker insertion occurs in about 1 to 2 percent in most series. Stroke occurs in approximately 1 to 4 percent of these patients. Approximately 30 percent of patients who present for aortic root replacement are candidates for a valve-sparing procedure that offers improved freedom from bleeding and thromboembolic complications and obviates the need for oral anticoagulation.

526 Part II Adult Cardiac Surgery
BACKGROUND
The first thoracic aortic replacements were performed with homograft tissue primarily in the descending thoracic aorta. Continuing efforts at developing an artificial fabric graft for use for aortic replacement, culminated with Michael DeBakey’s discovery of Dacron. 1 During the late 1950s, the Houston group led by Michael DeBakey systematically developed operations for resection and graft replacement of the ascending aorta, followed by the descending and thora-coabdominal aorta. In 1968, Bentall and DeBono published a landmark article on replacement of the entire aortic root with anastomoses of the coronary ostia to the replacement graft. 2 The description of this technique included side-to-side anastomoses of the coronary arteries to the graft. The aneurysm sac then was closed completely around the graft. A common complication of this operation was pseudoa-neurysmal development at the level of the coronary ostia, presumably caused by the tension placed on the coronary anastomoses. A subsequent modification of this technique by Kouchoukos and coworkers 3 included complete excision of the aneurysm and aortic root, leaving both coronary arter-ies suspended by only a small “button-shaped” circular por-tion of aorta that then would be anastomosed directly into a hole created in the side of the Dacron graft, thus eliminating pseudoaneurysm formation. An extended ascending aortic replacement was described by Wheat and associates, effec-tively excluding most of the ascending aorta but leaving the coronary arteries attached to the remaining aortic root tissue in continuity. 4
In 1979, acting on the observation that many patients pre-senting for aortic root replacement have normal aortic valve morphology, Sir Magdi Yacoub and colleagues at Harefield Hospital in the United Kingdom developed a strategy for aortic root replacement in which the aortic valve was pre-served. 5 In 1988, Tirone David introduced a different tech-nique for valve-sparing aortic root replacement. 6
Interest in homograft aortic root replacement began in the 1950s. At that time, Norman Shumway and colleagues at Stanford University were experimenting with excision of the right ventricular outflow tract, the pulmonary valve, and the proximal portions of the pulmonary artery in continuity in dogs and translocating this to the aortic root, with subse-quent reconstruction of the pulmonary artery with homo-graft or tube graft material. 7 The operation in this iteration ultimately would be doomed to failure because of right ventricular failure resulting from the lack of a pulmonary valve, but Donald Ross, building on that experience, later performed the first pulmonary autograft aortic root replace-ments in humans. 8
DEVELOPMENTAL ANATOMY
The aortic root and the ascending aorta develop as part of a common truncus arteriosus that partitions itself into the ascending aorta and the aortic root and the pulmonary
artery at approximately the fifth and sixth weeks of develop-ment. The aortic root is a tripartite structure owing to the presence of coronary sinuses. The aortic valve proper has no true fibrous annulus, although surgeons use the term aortic annulus to describe the junction of the aorta and the ven-tricle. The noncoronary sinus of the aortic valve tends to be the largest of the three sinuses, and therefore the size of the aortic valve leaflets reflects this, with the noncoronary leaflet generally being the largest. The length of the distance from the basal attachment of each aortic valve leaflet to the aorta is approximately 1.5 times the length of the free margin of the leaflet ( Fig. 33-1 ). The commissures of each of the aortic valves extend right to or just below the sinotubular junction that marks the anatomic ridge between the end of the aortic root and the beginning of the ascending aorta. In general, the sinotubular ridge is approximately 10 to 15 percent smaller in diameter than the aortic annulus ( Fig. 33-1 ). Anatomic dis-ease states that cause dilatation of the sinotubular junction or dilatation of the aortic annulus will cause insufficiency of the aortic valve. There is an aortic–mitral continuity, which is a fibrous tissue attachment between the aorta and the mitral valves that constitutes approximately 55 percent of the cir-cumference of the aortic root. The left side of the aortic root toward the pulmonary artery is attached to the ventricular muscle, corresponding to approximately 45 percent of the circumference.
EPIDEMIOLOGY
The exact extent of occurrence of thoracic aortic aneu-rysms (TAAs) is unknown. Bickerstaff and associates 9 found the prevalence of TAAs to be 5.9 per 100,000 per year in the Rochester, MN, area. Among a total of 72 patients with TAAs studied by Bickerstaff and colleagues, 51 per-cent, or 37 of the aneurysms in those patients, involved
A B
FM
H
B
ST
AA
FIGURE 33-1 Anatomic features of the aortic root. A . Normal aortic valve leaflet. B . Aortic root demonstrating the smaller diameter of the sinotubular junction compared with the aortic annulus. (Reproduced with permission from David TE. Complex operations of the aortic root. In: Edmunds LH (ed). Cardiac Surgery in the Adult . New York: McGraw-Hill, 1997:939–957.)

Chapter 33 Aortic Root Replacement 527
the ascending aorta, 8 (11 percent) the aortic arch, and 27 (38 percent) the descending thoracic aorta.
According to the National Center for Health Statistics, aortic aneurysms (AAs) were the 15th most common cause of death in the United States in the year 2000; approximately 0.6 percent of all females and 1.1 percent of all males die of aortic aneurys-mal disease. TAA deaths occur in about 0.7 per 100,000 popu-lation per year. 10 Among patients who die of TAAs, rupture is the cause of death in about 80 percent of cases.
The estimated growth rate for TAAs has been calculated to be 1.2 to 4.2 mm/year, and enlargement accelerates as an aneurysm gets larger. 11 Risk factors for accelerated growth include the presence of dissection in the enlarged segment, synchronous arch or abdominal AA, smoking, no β-blocker therapy, renal failure, and diastolic hypertension. Rupture is much more likely to occur when the aneurysm exceeds 5 cm in diameter, and the risk of rupture increases as the aneu-rysm increases in size. Aneurysms larger than 6 cm can be associated with a yearly rate of rupture or dissection of at least 6.9 percent and a death rate of 11.8 percent. 12
PATHOPHYSIOLOGY
Annuloaortic ectasia is a term used to describe an increase in the diameter of the aortic annulus coupled with an increase in the diameter of the aortic root. This ectasia tends to occur along the fibrous tissue of the ventricle, with the ventricular muscular portion of the aortic root generally preserved. This type of situation is seen in patients with Marfan syndrome (characterized by defect in the fibrilin gene), Ehlers–Danlos syndrome (characterized by a defect in type 3 collagen syn-thesis), Loeys–Dietz syndrome (characterized by a defect in Transforming Growth Factor beta gene), osteogenesis imperfecta, and pseudoxanthoma elasticum. It may have other familial origins or may be idiopathic. In these syn-dromes, the aortic sinuses become thinner and dilated and the sinotubular junction increases in diameter. When this happens, the aortic valve leaflets are not allowed to coapt properly because of separation of the commissures. These patients develop central jets of aortic insufficiency on echo-cardiographic assessment. Degenerative diseases of the aorta may cause dilatation of the ascending aorta and aortic sinuses with minimal or no dilatation of the aortic annu-lus. The aortic root also may be destroyed in the setting of acute or chronic aortic dissection and other congenital syn-dromes, such as those associated with bicuspid aortic valves. Recently, a significant body of research has focused on the involvement of endogenous extracellular matrix degrading enzymes in the involvement of aneurysms and aortic remod-eling. Of greatest interest are the matrix metalloproteinases (MMPs), particularly those of the gelatinase class (MMP-2, MMP-9). 13,14 Another important cause of aortic root destruc-tion is acute infective endocarditis with aggressive organisms such as Staphylococcus aureus.
A central common theme in the development of aortic root aneurysms is a condition referred to as cystic medial
degeneration or simply medial degeneration. Histologically, the aorta is made up of three layers. The adventitia is com-posed primarily of a collagen-rich network. The tunica media, or media, is composed of alternating layers of vas-cular smooth muscle and elastin. Each successive pairing of smooth muscle cells and elastin is referred to as a lamellar unit. In humans, the media of the aortic root is composed of approximately 50 lamellar units. The third layer of the aorta is referred to as the intima and is composed of a single layer of epithelial cells. In many cases of AA, one sees gradual dis-ruption of the media of the aorta, with the creation of small acellular spaces within it. This process of medial degenera-tion results ultimately in weakening of the aortic wall and inability to sustain the normal shear stresses associated with systole. As a result, a slow remodeling of the aortic root and ascending aorta occurs, leading to aneurysm formation.
CLINICAL PRESENTATION AND DIAGNOSTIC MODALITIES
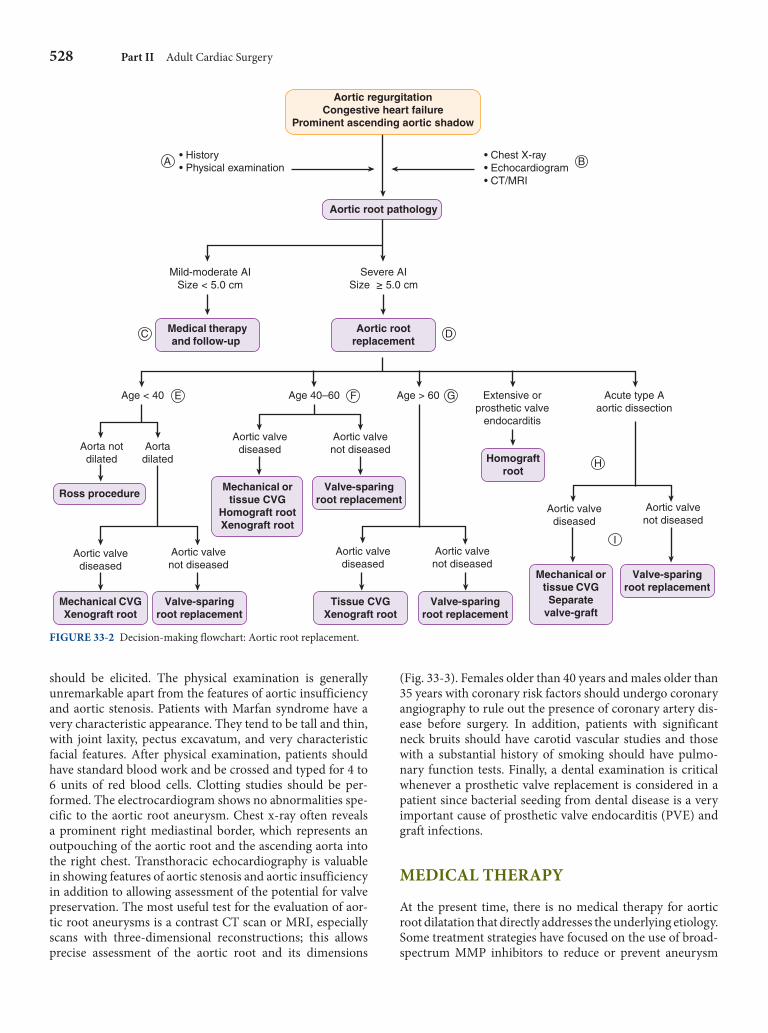
Patients present for aortic root replacement in a num-ber of circumstances (see the decision-making flowchart; Fig. 33-2 ). The most acute circumstance is a patient with a Stanford type A aortic dissection in whom the aortic root is virtually destroyed by the proximal extent of the dissection. The condition of these patients constitutes a surgical emer-gency, and as a result, aortic root replacement in these cir-cumstances is associated with more morbidity and a higher mortality than is standard aortic root replacement. A second acute situation occurs with infective endocarditis. The most common situation in which patients present for aortic root replacement is an aortic root aneurysm. The age range of presentation is wide and starts in the 20s and 30s in patients with hereditary connective tissue disorders and extends into the 70s and even 80s in those with degenerative aneurysms. Other than a family history of AAs and connective tissue disorders, risk factors for AAs include hypertension and atherosclerosis. Patients with isolated aortic root aneurysms are usually asymptomatic. Those conditions are identi-fied as a result of a workup for another disease process, such as a respiratory tract infection, that results in a chest x-ray. The chest x-ray may identify an abnormality in the medi-astinum, resulting in a computed tomography (CT) scan or a magnetic resonance imaging (MRI) scan that illustrates the aortic root aneurysm. Alternatively, other patients with AAs have significant aortic valve pathology, such as stenosis or insufficiency. Symptoms from these conditions result in referral to a physician. An echocardiogram is performed and shows evidence of aortic stenosis or insufficiency, and often a dilated aortic root is identified. This often leads to a fur-ther imaging study, such as a CT scan or an MRI scan, which shows the aortic root aneurysm.
The workup in patients with an aortic root aneurysm involves a careful history and physical examination, assess-ing for a history of bleeding problems and a history of sig-nificant dental work. In addition, a family history of AA
528 Part II Adult Cardiac Surgery
should be elicited. The physical examination is generally unremarkable apart from the features of aortic insufficiency and aortic stenosis. Patients with Marfan syndrome have a very characteristic appearance. They tend to be tall and thin, with joint laxity, pectus excavatum, and very characteristic facial features. After physical examination, patients should have standard blood work and be crossed and typed for 4 to 6 units of red blood cells. Clotting studies should be per-formed. The electrocardiogram shows no abnormalities spe-cific to the aortic root aneurysm. Chest x-ray often reveals a prominent right mediastinal border, which represents an outpouching of the aortic root and the ascending aorta into the right chest. Transthoracic echocardiography is valuable in showing features of aortic stenosis and aortic insufficiency in addition to allowing assessment of the potential for valve preservation. The most useful test for the evaluation of aor-tic root aneurysms is a contrast CT scan or MRI, especially scans with three-dimensional reconstructions; this allows precise assessment of the aortic root and its dimensions
FIGURE 33-2 Decision-making flowchart: Aortic root replacement.
Medical therapyand follow-up
Aortic rootreplacement
• History• Physical examination
• Chest X-ray• Echocardiogram• CT/MRI
Aortic regurgitationCongestive heart failure
Prominent ascending aortic shadow
Aortic root pathology
Ross procedure
Mild-moderate AISize < 5.0 cm
Age < 40
Severe AISize ≥ 5.0 cm
Aorta notdilated
Aortadilated
Aortic valvediseased
Mechanical CVGXenograft root
Aortic valvenot diseased
Valve-sparingroot replacement
Age 40–60
Aortic valvediseased
Mechanical ortissue CVG
Homograft rootXenograft root
Aortic valvenot diseased
Valve-sparingroot replacement
Age > 60
Aortic valvediseased
Tissue CVGXenograft root
Aortic valvenot diseased
Valve-sparingroot replacement
Extensive orprosthetic valve
endocarditis
Homograftroot
Acute type Aaortic dissection
Aortic valvediseased
Mechanical ortissue CVGSeparate
valve-graft
Aortic valvenot diseased
Valve-sparingroot replacement
E F G
H
I
A
C D
B
( Fig. 33-3 ). Females older than 40 years and males older than 35 years with coronary risk factors should undergo coronary angiography to rule out the presence of coronary artery dis-ease before surgery. In addition, patients with significant neck bruits should have carotid vascular studies and those with a substantial history of smoking should have pulmo-nary function tests. Finally, a dental examination is critical whenever a prosthetic valve replacement is considered in a patient since bacterial seeding from dental disease is a very important cause of prosthetic valve endocarditis (PVE) and graft infections.
MEDICAL THERAPY
At the present time, there is no medical therapy for aortic root dilatation that directly addresses the underlying etiology. Some treatment strategies have focused on the use of broad-spectrum MMP inhibitors to reduce or prevent aneurysm
Chapter 33 Aortic Root Replacement 529
expansion. Thompson and Baxter gave doxycycline 100 mg twice a day for 7 days to five patients before abdominal AA repair, and aneurysm biopsy showed a three-fold reduction in MMP-2 and a four-fold reduction in MMP-9 expression compared with nontreated controls in whom those two enzymes were expressed abundantly. 15 After this, a multi-institutional phase II prospective randomized trial was undertaken to assess the safety and potential efficacy of long-term doxycycline administration in 36 patients. Thirty-three patients completed the study, and significant treatment-related side effects occurred in five, or 13.9 percent, of those patients. There was no significant increase in aneurysm size at 6 months, and plasma MMP-9 levels dropped so that only 21 percent of the patients in the drug arm had MMP-9 that was considered to be elevated compared with 47 percent in the control arm. 16 Recent work from our institution has simi-larly suggested a role for ARB2 blocker Losartan, in slowing the growth of thoracic aneurysms associated with Loeys–Dietz Syndrome. 17 Hence, at present, the mainstays of man-agement of aortic root aneurysms are judicious hypertension control using a combination of β-blockers and ARB2 recep-tor blockers in conjunction with regular follow-up with CT scans and transthoracic echocardiography to assess for inter-val changes in aortic diameter and follow the characteristics of the aortic valve.
INDICATIONS FOR SURGERY
Generally, resection of an aortic root aneurysm is indicated in patients in whom the aortic root diameter exceeds 5 to 5.5 or becomes twice the size of a comparable normal aortic segment. 11 In addition, a patient with an aortic root aneu-rysm that is seen to grow more than 0.5 cm in a 6-month period also should be considered for operation. Some lati-tude is given for patients with connective tissue disorders in whom it is known that the aorta is inherently weak and more susceptible to rapid dilatation, especially in patients with Loeys–Dietz syndrome (ascending aortic diameter cutoff 4 cm), those with bicuspid aortic valve (ascend-ing aortic diameter cutoff 4.5 cm), and those with Marfan (ascending aortic diameter cutoff 5 cm). The clinical situa-tion often also arises when patients have significant aortic valve pathology in association with an AA that does not quite meet the size criteria for resection. In these circum-stances, aortic root replacement is indicated, since isolated replacement of the aortic valve in patients with a large aor-tic root and ascending aorta can pose technical difficulties in terms of closing the aorta after the aortic valve proce-dure and may predispose those patients to aortic dissec-tions. In addition, a complicated redo operation for aortic root replacement may be necessary, since the ascending
A
B
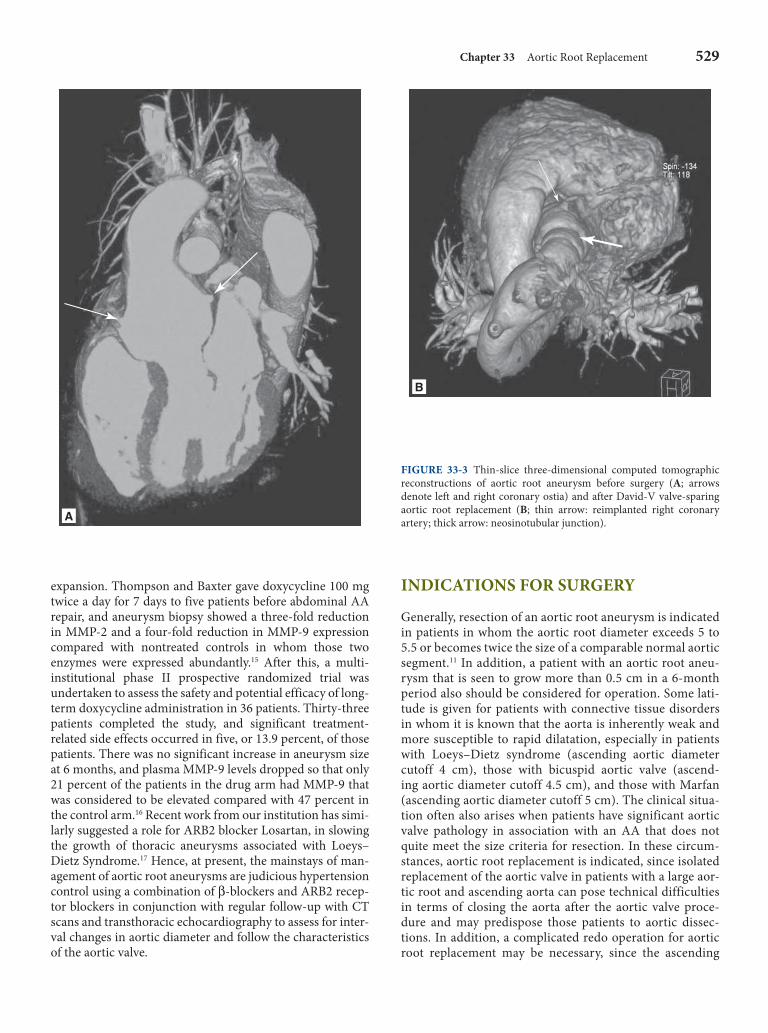
FIGURE 33-3 Thin-slice three-dimensional computed tomographic reconstructions of aortic root aneurysm before surgery ( A ; arrows denote left and right coronary ostia) and after David-V valve-sparing aortic root replacement ( B ; thin arrow: reimplanted right coronary artery; thick arrow: neosinotubular junction) .

530 Part II Adult Cardiac Surgery
aorta continues to dilate. As was stated earlier, aortic root replacement occasionally is indicated in patients with type A aortic dissections with destruction of the aortic root and also in younger patients with significant aortic valve pathol-ogy who have a normal aortic root and ascending aorta and who are undergoing homograft root replacement or a Ross procedure to benefit from the increased durability of the aortic valve associated with this operation. Finally, severe aortic valve endocarditis with abscess or PVE may be best treated with homograft aortic root replacement.
SURGICAL THERAPY
Conduct of the Operation
The patient is placed in the supine position under gen-eral anesthesia. The chest, abdomen, perineum, and lower extremities are prepped and draped in sterile fashion. Standard median sternotomy and exposure of the heart are performed. The orientation of the aortic root is visual-ized more easily if only the right side of the pericardium is tacked upward. This rotates the heart counterclockwise and allows the apex of the heart to sink into the left chest, thus improving the exposure of the aortic root. Arterial and venous cannulation is undertaken, and appropriate connec-tions are made to the pump oxygenator. If the patient has no significant aortic insufficiency, an antegrade cardiople-gia tack is placed, and in all cases a retrograde cardioplegia cannula also is placed. When everything is in readiness for the initiation of cardiopulmonary bypass, careful dissection is undertaken to separate as much of the aortic root from the pulmonary artery and right ventricular outflow tract as possible. Care must be taken in dissecting anteriorly to avoid injury to the right coronary artery. A careful dissection at this point can result in significant exposure of the aortic root and therefore decrease the amount of time needed to perform the aortic root replacement when the aorta is cross-clamped. After confirmation of an activated clotting time (ACT) longer than 400 s, cardiopulmonary bypass is per-formed and the aorta is cross-clamped. Whenever possible, the heart should be arrested with antegrade cardioplegia to promote better and faster distribution of the cardioplegia. A switch to retrograde cold blood cardioplegia may be consid-ered especially in the presence of significant aortic regurgi-tation. The authors give intermittent shots of 250 mL every 20 min during the cross-clamp period. This is supplemented with a cold saline-infused cooling jacket placed around the left ventricle. A right superior pulmonary vein vent is placed to keep the heart decompressed.
The ascending aorta is transected approximately 3 to 4 cm above the right coronary ostium. The aortic valve is inspected at this point, and if the situation is appropriate for valve preservation, the valve is not excised. If the valve is diseased so that its successful preservation is not possible, it is excised and debridement of the annulus is carried out if necessary. At this point, both the left and the right coronary
buttons are dissected free, taking care not to mobilize them significantly. Significant mobilization may result in disori-entation and kinking of the button after anastomosis to the Dacron graft. Specific techniques and choices for aortic root replacement are discussed below.
Systemic rewarming is begun at an appropriate point in the implantation procedure to avoid imposing extra time wait-ing for the patient to reach normothermia before separation from cardiopulmonary bypass. After root replacement, the vent is removed, and it is useful to give the final shot of car-dioplegia antegrade to inspect for significant bleeding points that can be repaired before removal of the cross-clamp and also as an initial test of valve competence. The cross-clamp is removed with the patient placed in the Trendelenburg posi-tion and with an ascending aortic vent on. Ventricular and atrial pacing wires are placed, and mechanical ventilation is resumed. De-airing maneuvers such as lung hyperinfla-tion, side-to-side shaking of the chest, and manual agitation of the heart are performed with the heart partially ejecting. Transesophageal echocardiography is very helpful in the assessment of de-airing and also in the interrogation of the valve for correct leaflet function. The patient is weaned from bypass at a systemic temperature of 36.5 to 37°C with good ventilation parameters. Protamine is given slowly, and the patient is decannulated. Meticulous hemostasis is obtained, a midline mediastinal drain (36F thoracostomy tube) is placed, and the patient is closed in the standard fashion.
Aortic Root Replacement: Choices and Results
COMPOSITE VALVE-GRAFT The current gold standard for aortic root replacement is the composite valve-graft replacement. Typically this consists of a mechanical valve that is annealed to a double-velour woven Dacron graft at the factory. The most commonly used version is the St. Jude composite valve-graft, although other brands are available. The operation consists of removal of the aortic root in its entirety except for the coronary ostia that are left surrounded by a small circular rim of native aorta. The aor-tic valve also is excised. After appropriate sizing, pledgeted horizontal mattress nonabsorbable sutures are placed across the annulus in everting fashion (i.e., from aorta to ventricle) and are placed across the sewing ring of the composite valve-graft. The composite valve-graft is seated, and the sutures are tied and cut. For an extra measure of hemostasis, it is useful to suture the remaining rim of the aortic root directly to the sewing ring of the composite valve-graft in running fashion with 3-0 polypropylene sutures. Small holes are made just above the valve in the graft with ophthalmic cautery to allow suture implantation of the right and left coronary buttons. The authors use a small amount of albumin–glutaraldehyde biological glue to seal the interstices of these suture lines to aid in achieving hemostasis, but with the understanding that this step is not a substitute for meticulous surgical technique. A distal anastomosis of the Dacron graft to the ascending
Chapter 33 Aortic Root Replacement 531
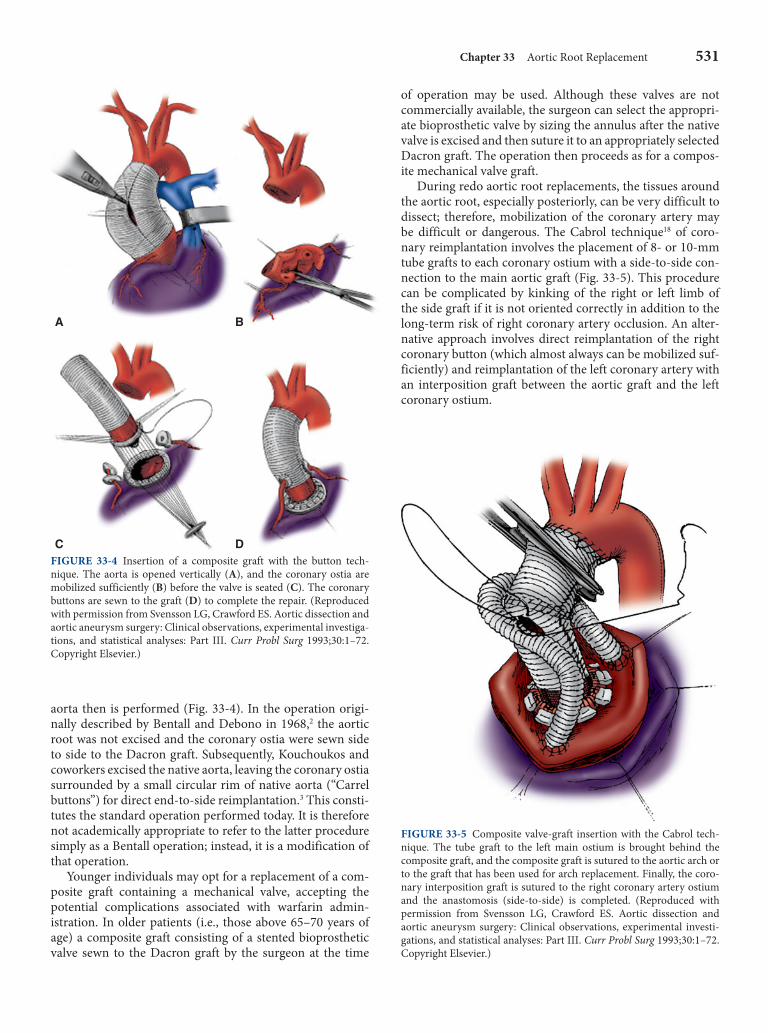
aorta then is performed ( Fig. 33-4 ). In the operation origi-nally described by Bentall and Debono in 1968, 2 the aortic root was not excised and the coronary ostia were sewn side to side to the Dacron graft. Subsequently, Kouchoukos and coworkers excised the native aorta, leaving the coronary ostia surrounded by a small circular rim of native aorta (“Carrel buttons”) for direct end-to-side reimplantation. 3 This consti-tutes the standard operation performed today. It is therefore not academically appropriate to refer to the latter procedure simply as a Bentall operation; instead, it is a modification of that operation.
Younger individuals may opt for a replacement of a com-posite graft containing a mechanical valve, accepting the potential complications associated with warfarin admin-istration. In older patients (i.e., those above 65–70 years of age) a composite graft consisting of a stented bioprosthetic valve sewn to the Dacron graft by the surgeon at the time
of operation may be used. Although these valves are not commercially available, the surgeon can select the appropri-ate bioprosthetic valve by sizing the annulus after the native valve is excised and then suture it to an appropriately selected Dacron graft. The operation then proceeds as for a compos-ite mechanical valve graft.
During redo aortic root replacements, the tissues around the aortic root, especially posteriorly, can be very difficult to dissect; therefore, mobilization of the coronary artery may be difficult or dangerous. The Cabrol technique 18 of coro-nary reimplantation involves the placement of 8- or 10-mm tube grafts to each coronary ostium with a side-to-side con-nection to the main aortic graft ( Fig. 33-5 ). This procedure can be complicated by kinking of the right or left limb of the side graft if it is not oriented correctly in addition to the long-term risk of right coronary artery occlusion. An alter-native approach involves direct reimplantation of the right coronary button (which almost always can be mobilized suf-ficiently) and reimplantation of the left coronary artery with an interposition graft between the aortic graft and the left coronary ostium.
A B
C D FIGURE 33-4 Insertion of a composite graft with the button tech-nique. The aorta is opened vertically ( A ), and the coronary ostia are mobilized sufficiently ( B ) before the valve is seated ( C ). The coronary buttons are sewn to the graft ( D ) to complete the repair. (Reproduced with permission from Svensson LG, Crawford ES. Aortic dissection and aortic aneurysm surgery: Clinical observations, experimental investiga-tions, and statistical analyses: Part III. Curr Probl Surg 1993;30:1–72. Copyright Elsevier.)
FIGURE 33-5 Composite valve-graft insertion with the Cabrol tech-nique. The tube graft to the left main ostium is brought behind the composite graft, and the composite graft is sutured to the aortic arch or to the graft that has been used for arch replacement. Finally, the coro-nary interposition graft is sutured to the right coronary artery ostium and the anastomosis (side-to-side) is completed. (Reproduced with permission from Svensson LG, Crawford ES. Aortic dissection and aortic aneurysm surgery: Clinical observations, experimental investi-gations, and statistical analyses: Part III. Curr Probl Surg 1993;30:1–72. Copyright Elsevier.)

532 Part II Adult Cardiac Surgery
The results of composite valve-graft aortic root replace-ment operations are generally very good but are depen-dent on the indication for operation. Gott and associates reviewed the extensive experience at Johns Hopkins with aortic root replacement in Marfan syndrome patients over a 24-year period. 19 Two hundred thirty-five Marfan patients underwent elective aortic root replacement with no 30-day mortality. The actuarial freedom from thromboembolism, endocarditis, and reoperation on the residual aorta 20 years postoperatively was 93 percent, 90 percent, and 74 per-cent, respectively. Lai and associates reviewed the Stanford experience with composite valve-graft (CVG) replacement for acute type A aortic dissection. 20 Thirty-day, 1-year, and 6-year survival estimates of 86 ± 8, 81 ± 9, and 65 ± 16 per-cent were seen with composite valve-graft replacement, with a 6-year freedom from reoperation of 100 percent. Ehrlich and coworkers 21 reported on 84 patients older than 65 years of age (median age was 74 years with a range of 66 to 89 years) who underwent CVG aortic root replacement over an 11-year period. Hospital mortality was 8.3 percent (7 of 84), with 16 late deaths (19 percent) noted during a median follow-up of 3.2 years (range 0 to 10 years). The authors concluded that composite valve-graft replacement in elderly patients results in low operative mortality, has excellent long-term survival, and averts fatal aneurysm rupture even in that higher-risk population.
THE COMPOSITE VALVE-GRAFT VERSUS SEPARATE VALVE-GRAFT CONTROVERSY In many cases an acceptable alternative to full CVG aortic root replacement is ascending aortic replacement starting at the sinotubular junction in association with separate aortic valve replacement [separate valve-graft (SVG)], leaving an intervening segment of the patient’s own aortic root from which the coronary ostia originate. The SVG procedure is less technically demanding and is useful when the sinotubu-lar junction is not effaced and the aortic root is not dilated. It is useful in elderly patients in whom a shorter cross-clamp time may limit morbidity, especially those with acute type A without significant annuloaortic ectasia. A relatively common problem is significant ascending aortic dilatation associated with aortic valve replacement for a bicuspid aor-tic valve. It is well known that patients with bicuspid aor-tic valves are predisposed to the development of ascending and root aneurysm. The cause is multifactorial and includes hemodynamic factors and heredity. 22
McCready and associates 23 observed an approximately 15 percent incidence of significant root dilatation an aver-age of 6.5 years after the SVG procedure. Houel and cowork-ers 24 found mortality rates of 7.7 percent with CVG versus 11 percent with SVG ( p = not significant). Actuarial sur-vival at 10 years postoperatively in these groups was 77.7 ± 5.6 versus 75.8 ± 6.9 percent ( p = not significant). However, freedom from late complications of the ascending aorta was significantly different (97.3 ± 1.9 percent CVG versus 68.3 ± 9.0 percent SVG at 10 years postoperatively). The
SVG technique was identified as a risk factor for late com-plications of the ascending aorta by multivariate analysis ( p = 0.01; odds ratio 9). In light of these data, an aggres-sive approach to CVG replacement in this population is recommended in patients with acceptable risk. 25 When the sinotubular junction and aortic root are intact so that SVG is considered appropriate, the procedure first described by Wheat and associates 4 may be useful to maximize exclusion of as much native aortic root tissue as possible without incur-ring the extra technical challenge of a full CVG implanta-tion. The decision to pursue CVG replacement to exclude all potentially diseased aortic root tissue should be tempered by an increased operative mortality rate compared with an isolated aortic valve replacement. The SVG technique may provide a reasonable compromise between these two proce-dural extremes, especially if concomitant procedures must be performed in the same setting; however, there is a risk of aneurysmal dilatation of the intervening aorta over time.
STENTLESS VALVE AS AN ALTERNATIVE FOR AORTIC ROOT REPLACEMENT The Freestyle aortic root bioprosthesis (Medtronic, Inc., Minneapolis, MN) is a stentless porcine aortic root prepared with low-pressure and zero-pressure fixation processes and α-aminooleic acid leaflet anticalcification treatment, with the aim of optimizing both hemodynamics and bioprosthesis durability. The device can be implanted as a subcoronary or modified subcoronary valve replacement, as a complete aor-tic root replacement (total root), or as a root inclusion. Initial implantations in human subjects began in 1992, and the device has been approved for clinical use in the United States since 1997. The implantation technique of this prosthesis is similar to that for CVG replacement described above. Bach and colleagues 26 reported the 8-year results of a multi-center cohort of 700 patients (of whom 93 percent were over 60 years of age) followed prospectively who received various configurations of this prosthesis. A total root replacement was performed in 162 of those patients, with actuarial free-dom from valve-related death of 92.3 percent, freedom from structural deterioration of 100 percent, and freedom from moderate or more aortic regurgitation of 98.7 percent. Oral anticoagulation is not required postoperatively.
HOMOGRAFT AORTIC ROOT REPLACEMENT Aortic root replacement can be performed with a cryopre-served homograft aortic root. This operation is more tech-nically demanding because of the less rigid nature of the tissue used. The operative technique is similar to the tech-niques described above except that many authors advocate a continuous running suture for the implantation of the left ventricular outflow tract side to the annulus. In addition, this proximal suture line must be planar; that is, it should not follow the scallops of the aortic annulus but should run somewhat under the commissures. This operation is particu-larly well suited for patients in the age range of 40 to 60 years
Chapter 33 Aortic Root Replacement 533
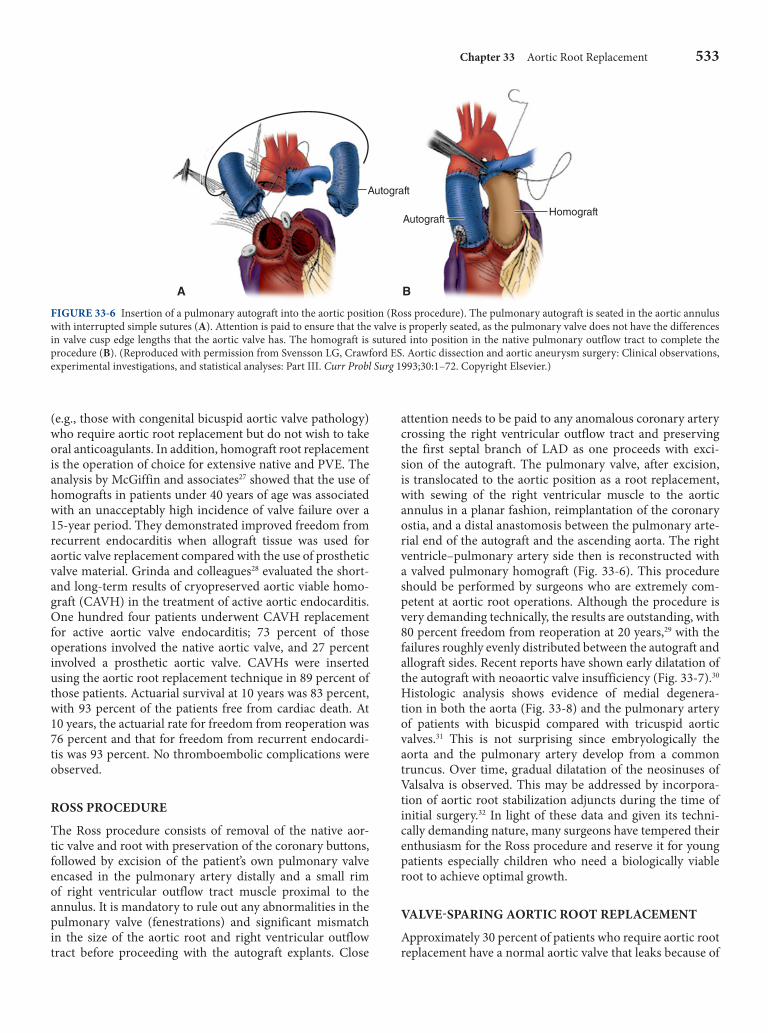
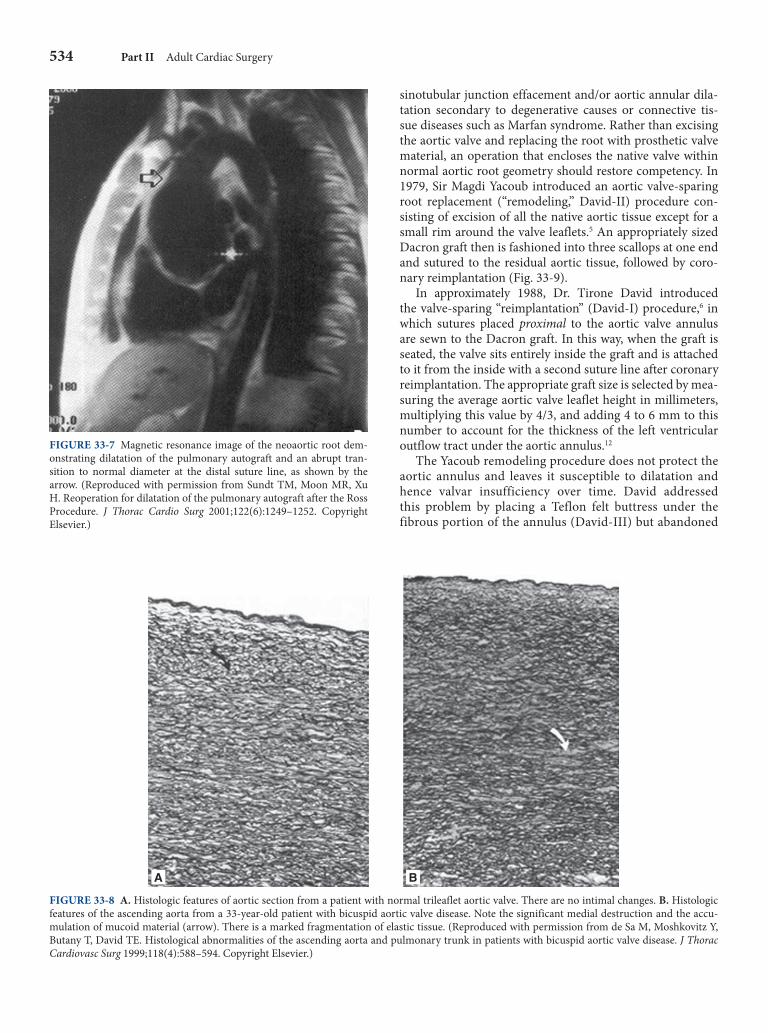
attention needs to be paid to any anomalous coronary artery crossing the right ventricular outflow tract and preserving the first septal branch of LAD as one proceeds with exci-sion of the autograft. The pulmonary valve, after excision, is translocated to the aortic position as a root replacement, with sewing of the right ventricular muscle to the aortic annulus in a planar fashion, reimplantation of the coronary ostia, and a distal anastomosis between the pulmonary arte-rial end of the autograft and the ascending aorta. The right ventricle–pulmonary artery side then is reconstructed with a valved pulmonary homograft ( Fig. 33-6 ). This procedure should be performed by surgeons who are extremely com-petent at aortic root operations. Although the procedure is very demanding technically, the results are outstanding, with 80 percent freedom from reoperation at 20 years, 29 with the failures roughly evenly distributed between the autograft and allograft sides. Recent reports have shown early dilatation of the autograft with neoaortic valve insufficiency ( Fig. 33-7 ). 30 Histologic analysis shows evidence of medial degenera-tion in both the aorta ( Fig. 33-8 ) and the pulmonary artery of patients with bicuspid compared with tricuspid aortic valves. 31 This is not surprising since embryologically the aorta and the pulmonary artery develop from a common truncus. Over time, gradual dilatation of the neosinuses of Valsalva is observed. This may be addressed by incorpora-tion of aortic root stabilization adjuncts during the time of initial surgery. 32 In light of these data and given its techni-cally demanding nature, many surgeons have tempered their enthusiasm for the Ross procedure and reserve it for young patients especially children who need a biologically viable root to achieve optimal growth.
VALVE-SPARING AORTIC ROOT REPLACEMENT Approximately 30 percent of patients who require aortic root replacement have a normal aortic valve that leaks because of
A B
Autograft
AutograftHomograft
FIGURE 33-6 Insertion of a pulmonary autograft into the aortic position (Ross procedure). The pulmonary autograft is seated in the aortic annulus with interrupted simple sutures ( A ). Attention is paid to ensure that the valve is properly seated, as the pulmonary valve does not have the differences in valve cusp edge lengths that the aortic valve has. The homograft is sutured into position in the native pulmonary outflow tract to complete the procedure ( B ). (Reproduced with permission from Svensson LG, Crawford ES. Aortic dissection and aortic aneurysm surgery: Clinical observations, experimental investigations, and statistical analyses: Part III. Curr Probl Surg 1993;30:1–72. Copyright Elsevier.)
(e.g., those with congenital bicuspid aortic valve pathology) who require aortic root replacement but do not wish to take oral anticoagulants. In addition, homograft root replacement is the operation of choice for extensive native and PVE. The analysis by McGiffin and associates 27 showed that the use of homografts in patients under 40 years of age was associated with an unacceptably high incidence of valve failure over a 15-year period. They demonstrated improved freedom from recurrent endocarditis when allograft tissue was used for aortic valve replacement compared with the use of prosthetic valve material. Grinda and colleagues 28 evaluated the short- and long-term results of cryopreserved aortic viable homo-graft (CAVH) in the treatment of active aortic endocarditis. One hundred four patients underwent CAVH replacement for active aortic valve endocarditis; 73 percent of those operations involved the native aortic valve, and 27 percent involved a prosthetic aortic valve. CAVHs were inserted using the aortic root replacement technique in 89 percent of those patients. Actuarial survival at 10 years was 83 percent, with 93 percent of the patients free from cardiac death. At 10 years, the actuarial rate for freedom from reoperation was 76 percent and that for freedom from recurrent endocardi-tis was 93 percent. No thromboembolic complications were observed.
ROSS PROCEDURE The Ross procedure consists of removal of the native aor-tic valve and root with preservation of the coronary buttons, followed by excision of the patient’s own pulmonary valve encased in the pulmonary artery distally and a small rim of right ventricular outflow tract muscle proximal to the annulus. It is mandatory to rule out any abnormalities in the pulmonary valve (fenestrations) and significant mismatch in the size of the aortic root and right ventricular outflow tract before proceeding with the autograft explants. Close
534 Part II Adult Cardiac Surgery
FIGURE 33-7 Magnetic resonance image of the neoaortic root dem-onstrating dilatation of the pulmonary autograft and an abrupt tran-sition to normal diameter at the distal suture line, as shown by the arrow. (Reproduced with permission from Sundt TM, Moon MR, Xu H. Reoperation for dilatation of the pulmonary autograft after the Ross Procedure. J Thorac Cardio Surg 2001;122(6):1249–1252. Copyright Elsevier.)
FIGURE 33-8 A . Histologic features of aortic section from a patient with normal trileaflet aortic valve. There are no intimal changes. B . Histologic features of the ascending aorta from a 33-year-old patient with bicuspid aortic valve disease. Note the significant medial destruction and the accu-mulation of mucoid material (arrow). There is a marked fragmentation of elastic tissue. (Reproduced with permission from de Sa M, Moshkovitz Y, Butany T, David TE. Histological abnormalities of the ascending aorta and pulmonary trunk in patients with bicuspid aortic valve disease. J Thorac Cardiovasc Surg 1999;118(4):588–594. Copyright Elsevier.)
A B
sinotubular junction effacement and/or aortic annular dila-tation secondary to degenerative causes or connective tis-sue diseases such as Marfan syndrome. Rather than excising the aortic valve and replacing the root with prosthetic valve material, an operation that encloses the native valve within normal aortic root geometry should restore competency. In 1979, Sir Magdi Yacoub introduced an aortic valve-sparing root replacement (“remodeling,” David-II) procedure con-sisting of excision of all the native aortic tissue except for a small rim around the valve leaflets. 5 An appropriately sized Dacron graft then is fashioned into three scallops at one end and sutured to the residual aortic tissue, followed by coro-nary reimplantation ( Fig. 33-9 ).
In approximately 1988, Dr. Tirone David introduced the valve-sparing “reimplantation” (David-I) procedure, 6 in which sutures placed proximal to the aortic valve annulus are sewn to the Dacron graft. In this way, when the graft is seated, the valve sits entirely inside the graft and is attached to it from the inside with a second suture line after coronary reimplantation. The appropriate graft size is selected by mea-suring the average aortic valve leaflet height in millimeters, multiplying this value by 4/3, and adding 4 to 6 mm to this number to account for the thickness of the left ventricular outflow tract under the aortic annulus. 12
The Yacoub remodeling procedure does not protect the aortic annulus and leaves it susceptible to dilatation and hence valvar insufficiency over time. David addressed this problem by placing a Teflon felt buttress under the fibrous portion of the annulus (David-III) but abandoned

Chapter 33 Aortic Root Replacement 535
that modification in favor of the reimplantation proce-dure. If reoperation is required because of valvar incom-petence after the remodeling procedure, a full aortic root replacement is necessary because of the persistence of unprotected native aortic root tissue. In contrast, with the David reimplantation procedure, the entire aortic root and annulus are enclosed in graft material, preventing dilata-tion over time. If reoperation is required, the graft can be opened, the native valve can be excised, and a stented or stentless valve of choice may be sutured directly into the graft, obviating the need for a much more difficult root re-replacement.
With the original David operation, isolated case reports described native valve failure with fibrotic, retracted aortic leaflets seen at reoperation, perhaps consistent with repeated trauma to the leaflets secondary to the lack of “neosinuses” produced with the Yacoub procedure. 33 The David pro-cedure has undergone two iterations to address this issue. The first (David-IV) involved the selection of a graft 4 to 6 mm larger in diameter than the calculation dictates and plication of the neosinotubular junction down to the correct
size. With the current (David-V) modification, the Dacron graft used for the aortic root replacement is oversized by 6 to 8 mm in diameter and then pleated at the annular and new sinotubular junction. 34 The graft will billow outward when it is subjected to arterial pressure, thus creating neo-sinuses. At Hopkins ( Fig. 33-10 ), we use a modified David I reimplantation procedure using the Valsalva graft, which has prefashioned pseudosinuses. 35 Our procedure differs from the original David I reimplantation technique in that only three subannular sutures are placed. The subannu-lar sutures serve only to anchor the base of the graft below the annulus, holding the entire aortic valve complex within the graft and are not hemostatic. We believe that use of the Valsalva graft in a reimplantation procedure provides both annular stabilization and preservation of sinuses. The size of the graft is based on optimal sinotubular junction sizing using valve sizers, determined intraoperatively after tran-section of aorta. A graft that is 2 to 3 mm larger is chosen as the graft will sit outside the aortic valve complex. Most patients in our experience 35 have had optimal sinotubular junction diameters of 28 to 30 mm and end up receiving a 30- to 32-mm graft. We have not found that measurement of leaflet dimension and formulas for graft selection are useful. The Valsalva graft is available in sizes 24 to 34 mm, which can accommodate majority of aortic roots encountered in clinical practice. Although patients with annular diameters greater than 34 mm may undergo valve sparing root sur-gery, in our experience, these patients typically have thin, stretched out abnormal leaflets and often have severe val-vular regurgitation. Surgeon experience and patient selec-tion are important factors for good outcomes after VSRR. Modified Bentall operation still remains the procedure of choice in patients with severe regurgitation, leaflet asymme-try, and fenestrations and those having bicuspid valves with significant thickening or prolapsed.
The results of the David operation have been excellent, with 100 percent freedom from reoperation in Dr. David’s hands. 36 Similar excellent results have been reported by other investigators. 35 Patients benefit from the long-term durabil-ity associated with preservation of their own valves, and anti-coagulation is not required postoperatively. 35,36
Postoperative Care and Surgical Results
Immediate postoperative care should focus on control of hypertension (for which intravenous sodium nitroprusside is used most commonly) and maintenance of adequate filling pressures (central venous pressure 10–15 mm Hg, pulmonary capillary wedge pressures in the range of 15–18 mm Hg). Dual-chamber pacing is required in a small proportion of patients who leave the operating room in conduction block. Often this resolves within 24 to 48 h. If conduction block persists longer than 4 to 5 days, permanent pacemaker inser-tion should be considered. In patients with no conduction disturbances, pacemaker wires can be removed on the third or fourth postoperative day. The patient should be placed
FIGURE 33-9 Operative technique of the remodeling (Yacoub) valve-sparing aortic root replacement. (Reproduced with permis-sion from Yacoub MH, Gehle P, Chandrasekaran V. Late results of a valve-preserving operation in patients with aneurysms of the ascend-ing aorta and root. J Thorac Cardiovasc Surg 1998:115(5);1080–1089. Copyright Elsevier.)
536 Part II Adult Cardiac Surgery
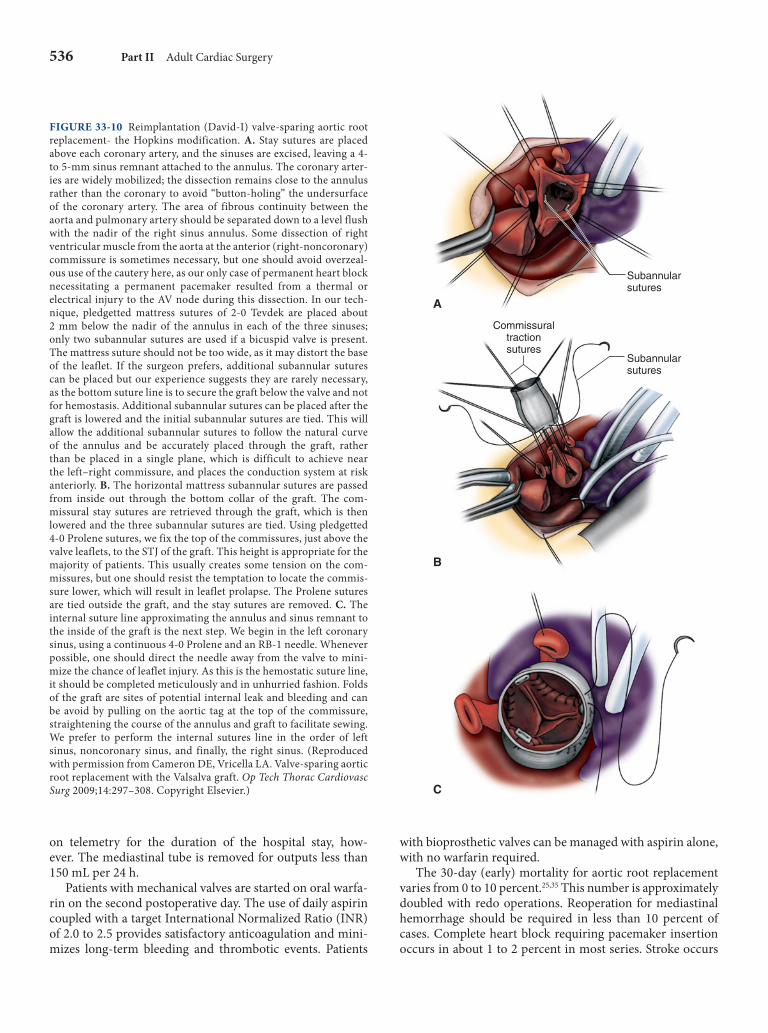
FIGURE 33-10 Reimplantation (David-I) valve-sparing aortic root replacement- the Hopkins modification. A . Stay sutures are placed above each coronary artery, and the sinuses are excised, leaving a 4- to 5-mm sinus remnant attached to the annulus. The coronary arter-ies are widely mobilized; the dissection remains close to the annulus rather than the coronary to avoid “button-holing” the undersurface of the coronary artery. The area of fibrous continuity between the aorta and pulmonary artery should be separated down to a level flush with the nadir of the right sinus annulus. Some dissection of right ventricular muscle from the aorta at the anterior (right- noncoronary) commissure is sometimes necessary, but one should avoid overzeal-ous use of the cautery here, as our only case of permanent heart block necessitating a permanent pacemaker resulted from a thermal or electrical injury to the AV node during this dissection. In our tech-nique, pledgetted mattress sutures of 2-0 Tevdek are placed about 2 mm below the nadir of the annulus in each of the three sinuses; only two subannular sutures are used if a bicuspid valve is present. The mattress suture should not be too wide, as it may distort the base of the leaflet. If the surgeon prefers, additional subannular sutures can be placed but our experience suggests they are rarely necessary, as the bottom suture line is to secure the graft below the valve and not for hemostasis. Additional subannular sutures can be placed after the graft is lowered and the initial subannular sutures are tied. This will allow the additional subannular sutures to follow the natural curve of the annulus and be accurately placed through the graft, rather than be placed in a single plane, which is difficult to achieve near the left–right commissure, and places the conduction system at risk anteriorly. B . The horizontal mattress subannular sutures are passed from inside out through the bottom collar of the graft. The com-missural stay sutures are retrieved through the graft, which is then lowered and the three subannular sutures are tied. Using pledgetted 4-0 Prolene sutures, we fix the top of the commissures, just above the valve leaflets, to the STJ of the graft. This height is appropriate for the majority of patients. This usually creates some tension on the com-missures, but one should resist the temptation to locate the commis-sure lower, which will result in leaflet prolapse. The Prolene sutures are tied outside the graft, and the stay sutures are removed. C . The internal suture line approximating the annulus and sinus remnant to the inside of the graft is the next step. We begin in the left coronary sinus, using a continuous 4-0 Prolene and an RB-1 needle. Whenever possible, one should direct the needle away from the valve to mini-mize the chance of leaflet injury. As this is the hemostatic suture line, it should be completed meticulously and in unhurried fashion. Folds of the graft are sites of potential internal leak and bleeding and can be avoid by pulling on the aortic tag at the top of the commissure, straightening the course of the annulus and graft to facilitate sewing. We prefer to perform the internal sutures line in the order of left sinus, noncoronary sinus, and finally, the right sinus. (Reproduced with permission from Cameron DE, Vricella LA. Valve-sparing aortic root replacement with the Valsalva graft. Op Tech Thorac Cardiovasc Surg 2009;14:297–308. Copyright Elsevier.)
A
B
C
Commissuraltractionsutures
Subannularsutures
Subannularsutures
on telemetry for the duration of the hospital stay, how-ever. The mediastinal tube is removed for outputs less than 150 mL per 24 h.
Patients with mechanical valves are started on oral warfa-rin on the second postoperative day. The use of daily aspirin coupled with a target International Normalized Ratio (INR) of 2.0 to 2.5 provides satisfactory anticoagulation and mini-mizes long-term bleeding and thrombotic events. Patients
with bioprosthetic valves can be managed with aspirin alone, with no warfarin required.
The 30-day (early) mortality for aortic root replacement varies from 0 to 10 percent. 25,35 This number is approximately doubled with redo operations. Reoperation for mediastinal hemorrhage should be required in less than 10 percent of cases. Complete heart block requiring pacemaker insertion occurs in about 1 to 2 percent in most series. Stroke occurs

Chapter 33 Aortic Root Replacement 537
in approximately 1 to 4 percent of these patients. There is no practical pharmacologic strategy for the prevention of post-operative atrial fibrillation, which occurs up to one-third of the time (in patients with no previous history). Careful correction of electrolytes and chemical cardioversion with intravenous and oral amiodarone are preferred and are suc-cessful 90 to 95 percent of the time. Patients should be main-tained on oral amiodarone for approximately 1 month, by which time the threat of recurrent atrial fibrillation should be resolved. In patients who require warfarin, the use of amiodarone makes it very difficult to manage the INR, and consideration should be given to alternative antiarrhythmics such as sotalol and procainamide. Patients with persistent atrial fibrillation despite attempts at chemical and electrical cardioversion should be maintained on oral warfarin until the arrhythmia resolves.
SUMMARY
Improvements in surgical technique, modifications of the procedure, and the development of specialized graft materi-als have improved the outcomes of aortic root replacement significantly.
Risk factors for the development or accelerated growth of ascending AAs include aortic dissection, aneurysmal disease elsewhere in the aortic wall, smoking, renal failure, and dia-stolic hypertension. Ascending aortic dilatation can result from genetic conditions such as Marfan syndrome, congeni-tal bicuspid aortic valve, and osteogenesis imperfecta as well as from excessive extracellular matrix degradation caused by unregulated activity of enzymes such as MMPs, as seen in inflammatory conditions. Aneurysmal enlargement of the aortic root can occur with an increase in the diameter of the aortic annulus (annuloaorticectasia) or without dilatation of the aortic annulus (degenerative disease).
Although certain patients may present with associated symptoms such as onset of pain from acute aortic dissection, the majority of these patients do not present with any specific physical abnormality, and many ascending AAs are detected as an incidental finding. Contrasted CT scans or MRIs, par-ticularly those with three-dimensional reconstructions, have become the most useful diagnostic tests for evaluating the aortic root. There is no medical therapy for ascending aor-tic root aneurysms, and beyond therapy for blood pressure reduction and careful follow-up, including frequent radio-logic imaging, surgical replacement of the aortic root is the only treatment.
For patients in whom surgical replacement of the aor-tic root is indicated, the surgeon must choose the appro-priate ascending aortic root replacement device. Current options for aortic root replacement include composite synthetic xenograft valve-conduit prostheses and homo-graft replacement. Additional options include using the patient’s own pulmonary valve after transposition to the aortic position (Ross procedure) and valve-sparing aortic root replacement.
REFERENCES 1. De Bakey ME, Cooley DA, Crawford ES, Morris GC, Jr. Clinical appli-
cation of a new flexible knitted dacron arterial substitute. Am Surg 1958;24(12):862–869.
2. Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax 1968;23(4):338–339.
3. Kouchoukos NT, Marshall WG Jr, Wedige-Stecher TA. Eleven-year experience with composite graft replacement of the ascending aorta and aortic valve. J Thorac Cardiovasc Surg 1986;92(4):691–705.
4. Wheat MW Jr, Wilson JR, Bartley TD. Successful replacement of the entire ascending aorta and aortic valve. JAMA 1964;188:717–719.
5. Yacoub MH, Gehle P, Chandrasekaran V, Birks EJ, Child A, Radley-Smith R. Late results of a valve-preserving operation in patients with aneurysms of the ascending aorta and root. J Thorac Cardiovasc Surg 1998;115(5):1080–1090.
6. David TE, Feindel CM. An aortic valve-sparing operation for patients with aortic incompetence and aneurysm of the ascending aorta. J Thorac Cardiovasc Surg 1992;103(4):617–621; discussion 622.
7. Pillsbury RC, Shumway NE. Replacement of the aortic valve with the autologous pulmonic valve. Surg Forum 1966;17:176–177.
8. Ross DN. Replacement of aortic and mitral valves with a pulmonary autograft. Lancet 1967;2(7523):956–958.
9. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneu-rysms: A population-based study. Surgery 1982;92(6):1103–1108.
10. Lilienfeld DE, Gunderson PD, Sprafka JM, Vargas C. Epidemiology of aortic aneurysms: I. Mortality trends in the United States, 1951 to 1981. Arteriosclerosis 1987;7(6):637–643.
11. Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J Am Coll Cardiol 2010;55(9):841–857.
12. Davies RR, Goldstein LJ, Coady MA, et al. Yearly rupture or dissection rates for thoracic aortic aneurysms: Simple prediction based on size. Ann Thorac Surg 2002;73(1):17–27; discussion 27-18.
13. Absi TS, Sundt TM 3rd, Tung WS, Moon M, Lee JK, Damiano RR Jr, Thompson RW. Altered patterns of gene expression distinguish-ing ascending aortic aneurysms from abdominal aortic aneurysms: Complementary DNA expression profiling in the molecular char-acterization of aortic disease. J Thorac Cardiovasc Surg 2003;126(2):344–357; discussion 357.
14. Boyum J, Fellinger EK, Schmoker JD, et al. Matrix metalloproteinase activity in thoracic aortic aneurysms associated with bicuspid and tri-cuspid aortic valves. J Thorac Cardiovasc Surg 2004;127(3):686–691.
15. Thompson RW, Baxter BT. MMP inhibition in abdominal aortic aneu-rysms. Rationale for a prospective randomized clinical trial. Ann N Y Acad Sci 1999;878:159–178.
16. Baxter BT, Pearce WH, Waltke EA, et al. Prolonged administration of doxycycline in patients with small asymptomatic abdominal aortic aneurysms: Report of a prospective (Phase II) multicenter study. J Vasc Surg 2002;36(1):1–12.
17. Habashi JP, Judge DP, Holm TM, et al. Losartan, an AT1 antagonist, prevents aortic aneurysm in a mouse model of Marfan syndrome. Science 2006;312(5770):117–121.
18. Cabrol C, Pavie A, Gandjbakhch I, et al. Complete replacement of the ascending aorta with reimplantation of the coronary arteries: New sur-gical approach. J Thorac Cardiovasc Surg 1981;81(2):309–315.
19. Gott VL, Cameron DE, Alejo DE, et al. Aortic root replacement in 271 Marfan patients: A 24-year experience. Ann Thorac Surg 2002;73(2):438–443.
20. Lai DT, Miller DC, Mitchell RS, et al. Acute type A aortic dissection complicated by aortic regurgitation: Composite valve graft versus sep-arate valve graft versus conservative valve repair. J Thorac Cardiovasc Surg 2003;126(6):1978–1986.
21. Ehrlich MP, Ergin MA, McCullough JN, et al. Favorable outcome after composite valve-graft replacement in patients older than 65 years. Ann Thorac Surg 2001;71(5):1454–1459.
22. Fedak PW, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation 2002;106(8):900–904.
23. McCready RA, Pluth JR. Surgical treatment of ascending aortic aneu-rysms associated with aortic valve insufficiency. Ann Thorac Surg 1979;28(4):307–316.

538 Part II Adult Cardiac Surgery
24. Houel R, Soustelle C, Kirsch M, Hillion ML, Renaut C, Loisance DY. Long-term results of the bentall operation versus separate replace-ment of the ascending aorta and aortic valve. J Heart Valve Dis 2002;11(4):485–491.
25. Yun KL, Miller DC, Fann JI, et al. Composite valve graft versus separate aortic valve and ascending aortic replacement: Is there still a role for the separate procedure? Circulation 1997;96(9 Suppl):II-368–II-375.
26. Bach DS, Kon ND, Dumesnil JG, Sintek CF, Doty DB. Eight-year results after aortic valve replacement with the Freestyle stentless bio-prosthesis. J Thorac Cardiovasc Surg 2004;127(6):1657–1663.
27. McGiffin DC, Galbraith AJ, O’Brien MF, et al. An analysis of valve re-replacement after aortic valve replacement with biologic devices. J Thorac Cardiovasc Surg 1997;113(2):311–318.
28. Grinda JM, Mainardi JL, D’Attellis N, et al. Cryopreserved aortic viable homograft for active aortic endocarditis. Ann Thorac Surg 2005;79(3):767–771.
29. Oury JH, Hiro SP, Maxwell JM, Lamberti JJ, Duran CM. The Ross Procedure: Current registry results. Ann Thorac Surg 1998;66(6 Suppl):S162–S165.
30. Sundt TM, Moon MR, Xu H. Reoperation for dilatation of the pul-monary autograft after the Ross procedure. J Thorac Cardiovasc Surg 2001;122(6):1249–1252.
31. de Sa M, Moshkovitz Y, Butany J, David TE. Histologic abnormalities of the ascending aorta and pulmonary trunk in patients with bicuspid aortic valve disease: Clinical relevance to the Ross procedure. J Thorac Cardiovasc Surg 1999;118(4):588–594.
32. Charitos EI, Hanke T, Stierle U, et al. Autograft reinforcement to preserve autograft function after the Ross procedure: A report from the german-dutch ross registry. Circulation 2009;120(11 Suppl):S146–S154.
33. Leyh RG, Fischer S, Kallenbach K, et al. High failure rate after valve-sparing aortic root replacement using the “remodeling technique” in acute type A aortic dissection. Circulation 2002;106(12 Suppl 1):I229–I233.
34. Miller DC. Valve-sparing aortic root replacement in patients with the Marfan syndrome. J Thorac Cardiovasc Surg 2003;125(4):773–778.
35. Cameron DE, Alejo DE, Patel ND, et al. Aortic root replacement in 372 Marfan patients: Evolution of operative repair over 30 years. Ann Thorac Surg 2009;87(5):1344–1349; discussion 1349–1350.
36. de Oliveira NC, David TE, Ivanov J, et al. Results of surgery for aortic root aneurysm in patients with Marfan syndrome. J Thorac Cardiovasc Surg 2003;125(4):789–796.
AORTIC ROOT REPLACEMENT BOARD REVIEW QUESTIONS (CHAPTER 33)
1. Which of the following is correct regarding the modi-fied Bentall procedure? A. Originally proposed by Kouchoukos B. Involves separate reimplantation of the coronary
buttons C. Is the current preferred technique for aortic root
replacement D. Prevents pseudoaneurysm developed at the coronary
ostia E. All of the above
2. Which is correct concerning valve-sparing root replace-ment with the David I technique? A. Recreates the sinuses of Valsalva B. Precedes the Yacoub technique C. Stabilizes the aortic root with sutures placed distal to
the aortic annulus
D. Utilizes a straight tube graft E. The incidence of aortic insufficiency is higher than
with the remodeling technique
3. Which has been shown to reduce aneurysm growth in Loeys–Dietz syndrome? A. Doxycycline B. ARB2 inhibitors C. β-Blockers D. Diuretics E. ACE inhibitors
4. Which dimension is correct for consideration of surgery to replace the ascending aorta? A. No history of connective tissue disorder—5.5 cm B. Marfan syndrome—5.0 cm C. Bicuspid aortic valve—4.5 cm D. Loeys–Dietz syndrome—4.0 cm E. All of the above
5. Which is not a common complication of the Ross procedure? A. Bleeding B. Injury to the first septal perforator C. Heart block D. Dilation of the autograft E. Thrombosis of the pulmonary homograft
ANSWERS
1. Answer: E. The current preferred technique for aortic root replacement is the modified Bentall procedure, which requires reimplantation of the coronary arteries. This modification was proposed by Kouchoukos as a solution to the problem of coronary ostia pseudoaneu-rysm that occurred after other operations.
2. Answer: D . The David I operation uses a straight tube graft and does not recreate the sinuses of Valsalva. It was introduced after the Yacoub remodeling technique and stabilizes the root with sutures placed proximal to the aortic annulus. The incidence of aortic insufficiency is lower when compared to the remodeling technique.
3. Answer: B . Losartan has been shown to slow growth of aneurysms associated with Loeys–Dietz syndrome.
4. Answer: E . These are the generally accepted dimensions for surgical intervention for aneurysm of the ascending aorta.
5. Answer: E . Stenosis and/or insufficiency occurs in the pulmonary homograft in up to 20 percent of patients, but thrombosis is rare. The combined use of the autolo-gous pulmonary valve and the homograft pulmonary valve is suitable for young, active patients that desire to avoid anticoagulation.