antisaccades elicited by visual and acoustic cues – an
TRANSCRIPT

Antisaccades elicited by visual and acoustic cues –
an investigation of children with and without attention deficit hyperactivity disorder
Dissertation
zur Erlangung des akademischen Grades
des Doktors der Naturwissenschaften (Dr. rer. nat.)
an der Universität Konstanz
Mathematisch-Naturwissenschaftliche Sektion
Fachbereich Psychologie
vorgelegt von Johanna Goepel
Konstanz, 2010
Tag der mündlichen Prüfung: 29.03.2011
1. Referentin: Prof. Dr. Brigitte Rockstroh
2. Referentin: Dr. Isabella Paul - Jordanov

Acknowledgment
-i-
ACKNOWLEDGMENT
Thank you for supporting and accompaning me through
the maze dissertation.

Contents
-ii-
CONTENTS
ACKNOWLEDGMENT..................................... ........................................................................................ I
CONTENTS............................................................................................................................................. II
ABBREVIATIONS...................................... ............................................................................................ III
CONDUCTED STUDIES & OWN RESEARCH CONTRIBUTIONS..... ..................................................V
ZUSAMMENFASSUNG .................................... .....................................................................................VI
SUMMARY ...........................................................................................................................................VIII
I. GENERAL INTRODUCTION ............................ ............................................................................... - 1 -
1.1 ATTENTION DEFICIT HYPERACTIVITY DISORDER.............................................................................. - 1 - 1.1.1 Phenotype and diagnostics................................................................................................ - 1 - 1.1.2 Epidemiology ..................................................................................................................... - 2 - 1.1.3 Aetiology ............................................................................................................................ - 3 - 1.1.4 ADHD and (central) auditory processing disorder ............................................................. - 6 -
1.2 SACCADES ................................................................................................................................ - 10 - 1.2.1 Influences on saccades ................................................................................................... - 13 - 1.2.2 Models of saccade generation: Race model & LATER model ........................................ - 17 - 1.2.3 Neurophysiology of saccades.......................................................................................... - 18 - 1.2.4 Saccades & ADHD .......................................................................................................... - 21 -
1.3 CONCLUSION............................................................................................................................. - 23 -
II. THREE ANTISACCADE STUDIES ...................... ........................................................................ - 26 -
2.1 PRO- AND ANTISACCADES IN CHILDREN ELICITED BY VISUAL AND ACOUSTIC CUES – DOES MODALITY MATTER?......................................................................................................................................... - 26 -
2.1.1 Abstract............................................................................................................................ - 26 - 2.1.2 Introduction ...................................................................................................................... - 26 - 2.1.3 Methods ........................................................................................................................... - 29 - 2.1.4 Results ............................................................................................................................. - 32 - 2.1.5 Discussion........................................................................................................................ - 35 - 2.1.6 Conclusion ....................................................................................................................... - 37 -
2.2 MEDIO-FRONTAL AND ANTERIOR TEMPORAL ABNORMALITIES IN CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) DURING AN ACOUSTIC ANTISACCADE TASK AS REVEALED BY ELECTRO-CORTICAL SOURCE RECONSTRUCTION .............................................................................................. - 39 -
2.2.1 Abstract............................................................................................................................ - 39 - 2.2.2 Introduction ...................................................................................................................... - 39 - 2.2.3 Methods ........................................................................................................................... - 41 - 2.2.4 Results ............................................................................................................................. - 46 - 2.2.5 Discussion........................................................................................................................ - 48 - 2.2.6 Conclusion ....................................................................................................................... - 52 -
2.3 BRAIN ACTIVATION DIFFERENCES DURING THE GENERATION OF VISUALLY AND ACOUSTICALLY GUIDED ANTISACCADES BETWEEN CHILDREN WITH AND WITHOUT ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD).......................................................................................................................................... - 53 -
2.3.1 Abstract............................................................................................................................ - 53 - 2.3.2 Introduction ...................................................................................................................... - 53 - 2.3.3 Methods ........................................................................................................................... - 56 - 2.3.4 Results ............................................................................................................................. - 60 - 2.3.5 Discussion........................................................................................................................ - 68 -
III. GENERAL DISCUSSION............................ ................................................................................. - 76 -
LIST OF TABLES AND FIGURES......................... ........................................................................... - 86 -
REFERENCES .................................................................................................................................. - 88 -

Abbreviations
-iii-
ABBREVIATIONS
ACC Anterior cingulate cortex
ADHD Attention deficit hyperactivity disorder
ADHS Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung
ANOVA Analysis of variance
approx. Approximately
BESA Brain electrical analysis software
(C)APD (Central) auditory processing disorder
ca Circa
CAPT Continuous Attention Performance Test
C-DT Choice-Delay tasks
cm Centimetre
CPM Coloured Progressive Matrices
CPT Continuous Performance Test
dB Dezibel
df Degrees of freedom
DPFC Dorsolateral prefrontal cortex
DSM IV Diagnostic and Statistical Manual of Mental Disorders IV
e.g. For example (Latin: exempli gratia)
ed. Edition
Eds. Editors
EEG Electroencephalography, Electroencephalogram, Elektroenzephalografie
ERN Error related negativity
ERP Event - related potential
et al. And others (Latin: et alii)
etc. Et cetera
FD Frequency discrimination
FEF Frontal eye fields
FM Frequency modulation
fMRI Functional Magnetic Resonance Imaging
Hz Hertz (1/sec)
i.e. That is (Latin: id est)
ICD 10 International Classification of Diseases 10
kOhm Kiloohm

Abbreviations
-iv-
LATER Model Linear Approach to Threshold with Ergodic Rate Model
MFC Medio-frontal cortex
mm Millimetre
MPH Methylphenidate
ms Milliseconds
nAm Nano ampermeter
P300 Positive ERP-component at approximately 300 ms
PEF Parietal eye fields
PN Processing negativity
PPC Posterior parietal cortex
RD Reading disability
RT Reaction time
SC Superior colliculus
SD Standard deviation
sec Seconds
SEF Supplementary eye fields
SPECT Single Photon Emission Computed Tomography
SRT Saccadic reaction time
SST Stop-Signal Test
STC Supplemental temporal cortex
TAC Temporal anterior cortex
TPC Temporal parietal cortex
vs. Versus
WMA World Medical Association
µs Micro seconds
µV Micro volt
Conducted studies & own research contributions
-v-
CONDUCTED STUDIES & OWN RESEARCH CONTRIBUTIONS
The studies presented in this work were supported by a number of colleagues. Listed
below are the three different studies and my own research contributions.
Study I:
Pro- and antisaccades in children elicited by visual and acoustic cues – does modality
matter?
Authors: Johanna Goepel1, Stefanie Biehl2, Johanna Kissler1 and Isabella Paul-
Jordanov1
Submitted to BMC Pediatrics
Own Contributions: Research on the theoretical background, running the Eye Tracker
experiments, data analyses, and drafting the manuscript.
Study II:
Medio-frontal and anterior temporal abnormalities in children with attention deficit
hyperactivity disorder (ADHD) during an acoustic antisaccade task as revealed by
electro-cortical source reconstruction
Authors: Johanna Goepel1, Johanna Kissler1, Brigitte Rockstroh1 and Isabella Paul-
Jordanov1
Published in BMC Psychiatry
Own Contributions: Research on the theoretical background, running the EEG-
experiments, data analyses, and drafting the manuscript.
Study III:
Brain activation differences during the generation of visually and acoustically guided
antisaccades between children with and without attention deficit hyperactivity disorder
(ADHD)
Authors: Johanna Goepel1, Johanna Kissler1, Brigitte Rockstroh1 and Isabella Paul-
Jordanov1
Submitted to ADHD Attention Deficit and Hyperactivity Disorders
Own Contributions: Research on the theoretical background, planning the study,
development and programming of the basic design, running the EEG-experiments, data
analyses, and drafting the manuscript.
1 Department of Clinical Psychology, University of Konstanz, 78457 Konstanz 2 Clinic for Psychiatry and Psychotherapy, University of Würzburg, 97080 Würzburg

Zusammenfassung
-vi-
ZUSAMMENFASSUNG
Impulsivität und damit unzureichende Inhibitionskontrolle ist eine der
Kernsymptome der Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS) – eine der
häufigsten chronischen psychiatrischen Störungen im Kindes- und Jugendalter. Eine
Möglichkeit inhibitorische Mechanismen zu untersuchen ist die Antisakkadenaufgabe –
eine Aufgabe, bei der ein Proband aufgefordert wird eine Sakkade in Richtung eines
plötzlich erscheinenden Reizes (Prosakkade) zu unterdrücken und stattdessen eine
willentliche Sakkade gleicher Größe auf die gegenüberliegende Seite zu generieren.
Ziel der vorliegenden Doktorarbeit war es zu erforschen, ob Kinder mit ADHS
nicht nur in der Inhibition auf plötzlich erscheinende visuelle, sondern auch auf plötzlich
erscheinende akustische Stimuli eingeschränkt sind, um eine Grundlage für bessere
Differentialdiagnostik zu legen.
Studie I – eine Eye Tracker Pilotstudie – untersuchte Kontrollkinder mit einer
randomisierten Anti-/Prosakkadenaufgabe und deckte vergleichbare
Inhibitionsleistungen in der visuellen und akustischen Bedingung auf: mehr Fehler in der
Anti- als in der Prosakkadenbedingung. Zusätzlich wurden modalitätsabhängige
Unterschiede gefunden: Der „Greif-Reflex“ war für die akustisch hervorgerufenen
Sakkaden schwächer und sie schienen weniger stark durch Impulsivität beeinflussbar,
da ihre Latenzen länger waren, was wiederum in weniger Antisakkadenfehlern
resultierte.
Während Studie II wurde das gleiche Paradigma bei Kindern mit und ohne ADHS
in einem Elektroenzephalografie (EEG) Experiment getestet. Auf der Verhaltensebene
wurden keine Gruppenunterschiede gefunden, jedoch wurden bei der 23-Quellen-Modell
Analyse Gruppenunterschiede in den akustisch ausgelösten und richtig ausgeführten
Antisakkaden sichtbar: Kinder mit ADHS zeigten im anterioren temporalen Lappen und
im medio-frontalen Cortex (für die Inhibition wichtige Strukturen) mehr Aktivität um
insgesamt die gleichen Verhaltensleistungen wie Kinder ohne ADHS zu erzeugen.
Möglichweise kann diese erhöhte Aktivität als ein kompensatorischer Mechanismus
gesehen werden.
In Studie III wurden Kinder mit und ohne ADHS während einer geblockten
Sakkadenaufgabe in einem EEG Experiment getestet. In der visuellen Bedingung waren
Kinder mit ADHS auf der Verhaltensebene (mehr Fehler und verlängerte Latenzen in der
Antisakkadenbedingung) als auch auf der physiologischen Ebene eingeschränkt. Die
Befunde weisen auf eine frontale Unteraktivität und ein parietal-cerebellares
kompensatorisches Netzwerk bei ADHS hin. Während des akustischen Experimentes

Zusammenfassung
-vii-
schienen Kinder mit ADHS größere Schwierigkeiten bei der Generierung von Sakkaden
zu haben, nicht aber bei der Inhibition.
Letztendlich ist anzunehmen, dass Kinder mit ADHS durchaus unterschiedlich
bezüglich der Inhibitonskontrolle eingeschränkt sind. Dies scheint von der
Aufgabenkomplexität und nicht von der Stimulus Modalität per se abzuhängen.
Summary
-viii-
SUMMARY
Impulsivity and with it deficient inhibition control is one of the core symptoms of
attention deficit hyperactivity disorder (ADHD) – one of the most prevalent chronic
psychiatric disorders in childhood and adolescence. One possibility to investigate
inhibitory mechanisms is the antisaccade task – a task, in which a subject is required to
suppress a saccade towards a suddenly appearing cue (prosaccade) and to generate a
voluntary saccade of equal size towards the opposite direction instead.
Aim of the present thesis was to investigate if children with ADHD are constricted
in their inhibition of not only suddenly arising visual but also suddenly arising acoustic
cues in order to establish a basis for a better differential diagnostic.
Study I – an eye tracker pilot study – investigated control children in a random
anti-/prosaccade task and revealed similar inhibition performance in visual and acoustic
conditions: more errors in the anti- compared to the prosaccade condition. Additionally,
modality dependant differences were found: the “grasp-reflex” was weaker for
acoustically elicited saccades and they seemed less prone to be influenced by
impulsivity as their latency was longer which in turn resulted in fewer antisaccade errors.
During Study II the same paradigm was tested with children with and without
ADHD in an Electroencephalography (EEG) experiment. On the behavioural level no
group differences were found but in a 23-source-model analysis group differences were
observable in acoustically elicited and correct performed antisaccades: children with
ADHD showed more activity in the anterior temporal lobe and medio-frontal cortex
(structures important for inhibition) to achieve the same behavioural output than children
without ADHD. The heightened activation could possibly be seen as a compensatory
mechanism.
In Study III children with and without ADHD were compared during a blocked
saccade task in an EEG experiment. In the visual condition children with ADHD were
impaired on the behavioural level (more errors and elongated latency in the antisaccade
condition) as well as on the physiological level. The findings suggest a frontal
hypoactivation and a parietal-cerebellar compensatory network in ADHD. During the
acoustic experiment children with ADHD seemed to have greater difficulties generating
saccades but not inhibiting.
Finally, it is to assume that children with ADHD are probably impaired quite
differently concerning inhibition control. This seems to depend on task complexity and
not on cue modality per se.

General introduction
- 1 -
I. GENERAL INTRODUCTION
1.1 Attention deficit hyperactivity disorder
1.1.1 Phenotype and diagnostics
Attention deficit hyperactivity disorder (ADHD) with a worldwide prevalence in
children of about 5-10% (Biederman & Faraone, 2005; Faraone, Sergeant, Gillberg, &
Biederman, 2003; Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007; Scahill &
Schwab-Stone, 2000) is one of the most frequent chronic psychiatric disorders in
childhood and adolescence with substantial lifelong implications on social und personally
functioning, academic performance and quality of life in general (Danckaerts, et al.,
2010; Harpin, 2005). In Germany with a prevalence of 7.7%, boys are affected to a
greater extent than girls with 1.8% (Huss, Holling, Kurth, & Schlack, 2008). The
male/female ratio of 3:1 in the community constitutes an under-identification of girls with
ADHD because they run a lower risk to develop a disruptive behaviour disorder – a
disorder which increases the referral rate (Biederman, 2005). Prevalence estimates
predictably vary according to the methodology (including diagnostic criteria, source of
information etc.) of the studies (Faraone, et al., 2003; Polanczyk, et al., 2007).
Core deficits of ADHD are cross-situational impairments in attention
(distractibility), impulse control (impulsivity) and activity (hyperactivity). The Diagnostic
and Statistical Manual of Mental Disorders IV (DSM IV; American Psychiatric
Association, 2000) and the International Classification of Diseases 10 (ICD 10; World
Health Organization, 1993) distinguish between three different disorder types: a
predominantly hyperactive type (codes 314.01 and F90.1), a predominantly inattentive
type (codes 314.00 and F98.8) and a combined type (codes 314.01 and F90.0). A
common diagnostic criterion of all three subtypes is that core deficits have to be
persistent in more than one setting (e.g. school and home) over six months and have to
develop before the age of seven. For a diagnostic in addition to a multitude of parents
and teacher behaviour questionnaires (e.g. Conners Scale, Diagnose-Checklists ADHD;
Döpfner, Görtz-Dorten, Lehmkuhl, Breuer, & Goletz, 2008; Lauth & Schlottke, 2002),
several neuropsychological measurements are applied in which children with ADHD
perform worse (Nichols & Waschbusch, 2004). Patients with ADHD show deficits in tests
of executive functions (Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005) especially
while performing tests of inhibition (Nigg, 2001). Frequently used tests are the
Continuous Performance Test (CPT, a Go/Nogo paradigm requiring response inhibition
for specific stimulus combinations; Rosvold, Mirsky, Sarason, Bransome, & Beck, 1956)
and the Stop-Signal Test (SST, where primary response has to be made following a
visual stimulus unless there is a signal indicating to stop the response for one trial;

General introduction
- 2 -
Logan, Cowan, & Davis, 1984). In such tests children with ADHD show higher error rates
and elongated reaction times (RTs) as well as altered brain activities (e.g. Fallgatter, et
al., 2004; Liotti, Pliszka, Perez, Kothmann, & Woldorff, 2005; Overtoom, et al., 2002;
Pliszka, Liotti, & Woldorff, 2000; Russell Schachar & Logan, 1990; Schachar, Mota,
Logan, Tannock, & Klim, 2000; Tamm, Menon, Ringel, & Reiss, 2004). Additionally,
children with ADHD select the shorter delay in a higher rate compared to control children
in Choice-Delay Tasks (C-DT, children have to choose between a large delayed reward
and a smaller immediate reward; e.g. Marco, et al., 2009). These findings support the
hypothesis that one underlying aetiological factor in ADHD might be a behavioural
disinhibition, a dysfunctional executive system and a delay aversion.
1.1.2 Epidemiology
ADHD which develops in early childhood is a chronical disorder (Harpin, 2005)
which persists in 4-78% (Biederman, Petty, Evans, Small, & Faraone, 2010; Mannuzza,
Klein, Bessler, Malloy, & LaPadula, 1998) of children into adulthood.
In infancy more than half of the children have problems related to sleep and
eating. In addition, children with ADHD have gross and fine motor or hearing problems
(Thompson, et al., 2004). As a consequence of lacking social functions, these children
have fewer friends and fewer outside activities. Children with ADHD often are made the
scapegoat resulting in low self-esteem, aggression, low empathy, sadness, isolation, etc.
up to depression (Spencer, Biederman, & Mick, 2007; Thompson, et al., 2004). Thus,
children with ADHD suffer from additional psychiatric disorders to a high degree (Angold,
Costello, & Erkanli, 1999). Comorbid diagnoses include oppositional defiant disorders,
conduct disorders, mood disorders (unipolar and bipolar), anxiety disorders, tic disorders,
substance use disorders and learning disorders (Biederman & Faraone, 2005;
Biederman, et al., 2010; Scahill & Schwab-Stone, 2000; Spencer, et al., 2007;
Thompson, et al., 2004).
During adolescence symptoms of inattention decline at a very modest rate,
whereas those of hyperactivity and impulsivity remit much more abruptly (Biederman,
Mick, & Faraone, 2000). However, when coming into the teenage years new problems
can arise. As a result patients with ADHD run a higher risk for academic failure
(Biederman, et al., 2004), criminal conduct (Fletcher & Wolfe, 2009), risky sexual
behaviour associated with unwanted pregnancy (Flory, Molina, Pelham, Gnagy, & Smith,
2006), high-risk driveability (Barkley, Murphy, Dupaul, & Bush, 2002) and further
additional psychiatric problems, such as antisocial personality disorder and nonalcohol
substance abuse (Mannuzza, et al., 1998). However, there is a wide range of teenagers

General introduction
- 3 -
that have the ability to adjust their behaviour. Therefore, the persistence of ADHD is not
associated with a uniform dysfunctional outcome, but instead leads to a range of
emotional, educational and social progression that can be partially predicted by maternal
psychopathology, lager family size, psychiatric comorbidity and impulsive symptoms
(Biederman, Mick, & Faraone, 1998). Thus, it is obvious that symptoms do not disappear
but rather change in the course of life. The current prevalence of adult ADHD is between
2 and 3% (Steinhausen, 2003). The failure of an appropriate symptom description may
reduce the true prevalence of ADHD in adulthood (Spencer, et al., 2007). Inattention in
adulthood is characterised by a poor self and task management, difficulty in initiating,
completing and changing tasks, trouble with multitasking, procrastination and avoiding of
activities that demand attention. The aimless restlessness in childhood changes in
purposeful restlessness in adulthood like working in more than one job, working long
hours or working in active jobs (Adler, 2008).
1.1.3 Aetiology
To date, there is no monocausal explanation for genesis of ADHD. Rather a
multifactor model is assumed with genetic, biologic, and psychosocial interactions
(Biederman & Faraone, 2005).
Studies have shown that ADHD is transmitted in families. According to family
studies, it seems that parents and siblings of children with ADHD have a two- to eightfold
increase to run a risk for developing ADHD (Biederman, 2005). Sprich and colleagues
(2000) reported that the rate of ADHD was similar in the adoptive relatives (6%) of
adopted children with ADHD and the biological relatives (3%) of non-ADHD control
children. Compared to this rate the percentage of ADHD was higher in the relatives of
biological ADHD probands (18%). Based on 20 twin studies from the United States,
Australia, Scandinavia, and the European Union the heritability is up to 76% (Faraone, et
al., 2005).
On the molecular genetics level, genes responsible for expression of
catecholamines (dopamine, serotonin, and noradrenalin) have been the initial
candidates. This was based (1) on results of imaging studies that comprised brain
structures with dopamine innervations (e.g. the fronto-striatal and the fronto-parietal
circuits, which are believed to be critical for executive functioning and regulation of
behavioural responses such as arousal, attention, and inhibition; Dickstein, Bannon,
Castellanos, & Milham, 2006) and (2) on the fact that stimulant medications act as
dopaminergic and noradrenergic agonists (Pliszka, 2005; Pliszka, McCracken, & Maas,
1996) which influence the anterior (dopamine- and noradrenergic) and posterior

General introduction
- 4 -
(noradrenergic) attention systems (Himelstein, Newcorn, & Halperin, 2000).
Methylphenidate (MPH), which is until now the primary pharmacological treatment for
ADHD, prevents dopamine reuptake by blocking the dopamine transporters (DAT). DATs
were found in higher density in patients with ADHD (Dougherty, et al., 1999; Krause,
Dresel, Krause, la Fougere, & Ackenheil, 2003) which decreases the level of dopamine
in the synaptic cleft. Recent studies, however, failed to verify the DAT hypothesis (see for
review Swanson, et al., 2007). The gene that encodes the DAT protein – located on
human 10-repeat allele of chromosome 5p15.3 – is associated with ADHD (Friedel, et
al., 2007; Yang, et al., 2007). It occurs in a higher concentration in ADHD samples rather
than in those of the control groups (Swanson, et al., 2000). Finally, DAT is connected to
dopamine receptors. Although the results of studies are inconsistent (Faraone, et al.,
2005) it seems that the 7-repeat allele on chromosome 11p15.5, which coded dopamine
receptors D4, also occurs more frequently in children with ADHD than in controls
(Swanson, et al., 2000).
Swanson and colleagues (2000) pointed out that three changes of the systems
are possible: a sub sensitive dopamine receptor D4 (combined with lesser signal
transfer), a hyper efficient DAT (associated with a hyper dopamine reuptake) or both,
which may result in underactivity of brain regions that are involved in attention and
behaviour.
However, more than the mentioned neurotransmitters and genes are involved in
ADHD (Faraone, et al., 2005). To date, findings of genetic studies in ADHD are still
inconsistent and disappointing (Banaschewski, Becker, Scherag, Franke, & Coghill,
2010).
Neuroimaging studies suggested anatomical abnormalities in ADHD individuals,
consisting in smaller sizes than the normal one of several brain regions: e.g. frontal
cortex (Seidman, Valera, & Makris, 2005), cerebellum (Castellanos, et al., 2002), and
subcortical structures, like the anterior cingulate cortex (ACC) (Seidman, et al., 2006),
caudatus nucleus, globus pallidus and corpus callosum (Seidman, et al., 2005). These
subcortical structures are part of the neural circuits underlying motor control, executive
functions, inhibition of behaviour and the modulation of reward (Biederman, 2005).
Additionally, the volume reductions are related to measures of symptom severity in
ADHD samples (Casey, et al., 1997; Castellanos, et al., 2002).
Furthermore, functional studies referred to a “lazy frontal lobe”: the fronto-striatal
regions of patients with ADHD are hypoperfused, hypometabolic, and functionally
disrupted in comparison to control subjects (Hale, Hariri, & McCracken, 2000).

General introduction
- 5 -
Therefore, functional imaging studies of ADHD, using Single Photon Emission
Computed Tomography (SPECT) showed a reduced blood flow in the frontal lobe and
the basal ganglia but an increased blood flow to the occipital lobe (Lou, Henriksen, &
Bruhn, 1990).
Elevated theta power (slow wave activity) as well as reduced alpha and beta
power during electrophysical studies are interpreted as cortical underarousal (Barry,
Clarke, & Johnstone, 2003). Niedermeyer (2001) postulated that this frontal hypoarousal
results in a deficient inhibition of the motor cortex followed by an excess of motor activity.
One possibility for increasing beta band activity is the prescription of MPH, which
correlates positively with attention performances (Clarke, et al., 2003; Wienbruch, Paul,
Bauer, & Kivelitz, 2005).
The P300 component, an event - related potential (ERP), is also related to
attention. Besides poorer performance in tests of sustained and/or selective attention
children with ADHD showed an altered P300: smaller amplitudes and longer latencies
compared to controls were found (see for review Tannock, 1998) referring to problems in
signal identification and processing. In healthy adults an increased P300 with longer
latency was observed in Nogo stimuli compared to Go stimuli (Bokura, Yamaguchi, &
Kobayashi, 2001; Fallgatter, Bartsch, & Herrmann, 2002). Children with ADHD showed a
diminished Nogo - P300 in such tasks (Fallgatter, et al., 2004; Paul-Jordanov, Bechtold,
& Gawrilow, 2010) which could be increased with MPH or self-regulation strategies
(Paul-Jordanov, et al., 2010; Paul, et al., 2007).
Furthermore, in children with ADHD a reduced N200 – associated with inhibitory
processes – was found during SSTs (Dimoska, Johnstone, Barry, & Clarke, 2003;
Pliszka, et al., 2000). The error related negativity (ERN) – a negative component
observed following errors – is also reduced in children with ADHD compared to control
children reflecting impaired error monitoring (Liotti, et al., 2005).
Finally, environmental factors such as nicotine, lead or foetal adaptation in
response to stress are discussed to influence the risk for ADHD also in interaction with
genes (see for review Swanson, et al., 2007). Fundamentally, the reciprocal influence
between the behaviour of children and that of parents or of other attachment figures and
with that the developing of a vicious circle is considered in the epidemiology (Harpin,
2005), i.e. the intensity of ADHD symptoms is influenced by the behaviour of the
environment.
Different models of aetiology were assumed in order to summarize the results.
Presently, the following important models are discussed: (1) the Executive Attention
Model postulated by Barkley (1997). In this model, patients with ADHD exhibit deficits in

General introduction
- 6 -
three sub-processes of inhibition (inhibition of prepotent responses, stopping an ongoing
response and interference control). (2) The Delay Aversion Model of Sonuga-Barke
(1994; 1992), which suggests that children’s inattention, hyperactivity and impulsiveness
are situation specific attempts to minimize delay. Finally, there are ambitions to combine
both models to a dual pathway model. This idea assumes that delay aversion (linked to
the fronto-ventral-striatal reward network) and poor inhibition control (associated with the
fronto-dorsal-striatal system) are independently coexisting characteristics of the
combined type of ADHD (Sonuga-Barke, 2002, 2003). To date, a triple pathway model is
discussed including deficits in the domains inhibitory control, delay aversion and
temporal processing (Sonuga-Barke, Bitsakou, & Thompson, 2010).
Although these models try to explain the underlying deficits in children with ADHD,
deficits in executive functions and delay aversion are neither necessary nor sufficient to
cause the group heterogeneity of ADHD occurrences (Nigg, 2005; Willcutt, et al., 2005).
Thus, it is still an open question which multilevel factors are responsible for the diversity
of ADHD symptoms.
1.1.4 ADHD and (central) auditory processing disorder
In recent years, questions arose concerning the coherence between ADHD and
the (central) auditory processing disorder ((C)APD). Musiek described auditory
processing as "How well the ear talks to the brain and how well the brain understands
what the ear tells it” (Paul-Brown, 2003). Thus APD (ICD-10 code F80.20) – compared to
ADHD a relative “new” disorder – is characterised by disturbed hearing despite of a
normally functioning auditory periphery. Typical symptoms are difficulties in sound
localization and lateralization, auditory discrimination and auditory pattern recognition.
Patients are handicapped in temporal aspects of audition, including temporal integration,
temporal discrimination (e.g. temporal gap detection), temporal ordering, and temporal
masking. Children with APD show a poor auditory performance in competing acoustic
signals (including dichotic listening) and a reduced auditory performance with degraded
acoustic signals (American Speech-Language-Hearing Association, 2005; British Society
of Audiology Steering Group, 2007). These symptoms are related to poor performance in
confusing environments, difficulties in following oral instructions or rapid/degraded
speech and difficulties in background noise. Children with APD appear to be inattentive
and distractible. Most of them have academic difficulties as well as language, reading
and spelling disorders (Bamiou, Musiek, & Luxon, 2001). The prevalence ranges
between 2 and 7% (Bamiou, et al., 2001; Chermak, Hall, & Musiek, 1999) with a 2:1
male/female ratio (Nickisch, et al., 2007) and the aetiology is similar heterogeneous to

General introduction
- 7 -
those of other developmental disorders (Bamiou, et al., 2001; Dawes, Bishop, Sirimanna,
& Bamiou, 2008; Witton, 2010). The heterogeneity of APD itself is accepted as
evidenced by the appearance of symptom-profiling schemas: the Buffalo Model and the
Bellis/Ferre Model (Dawes & Bishop, 2009). These models describe four and five APD
categories, respectively, but must refine their classification for clinical utility (Jutras, et al.,
2007). Three factors seem to make the diagnostic of APD complicate: (1) other types of
childhood feature similar behaviour patterns, (2) some of the audiological tests fail in
differentiating children with APD from children with other problems because there is only
a behavioural performance required of the children and (3) there is always a likelihood
for an encounter with other confounding processes like the lack of motivation, sustained
attention, cooperation or understanding (Jerger & Musiek, 2000).
However, efforts for testing diagnostic manuals are available. For example, Bellis
and colleagues (2008) investigated the dichotic listening task and found a lager right ear
advantage for children with APD compared to control children, and a reversed
asymmetry for a corresponding visual analogous task (left visual field advantage for
control children and right visual field advantage for children with APD). Parallel
questionnaires were tested (e.g. Meister, von Wedel, & Walger, 2004) but up to now
there is no standard diagnostic test set for APD (Dawes, et al., 2008).
An overlap between symptoms of ADHD and APD is described very well in the
literature (e.g. Cacace & McFarland, 2005b; Dawes & Bishop, 2009; Keller & Tillery,
2002) and a comorbidity of both disorders seems to be the rule rather than the exception.
Riccio and colleagues (1994) found that in 30 children diagnosed with APD, 50% would
also conform to a diagnosis of ADHD based on formal evaluation. The other way around
29-79% ADHD was diagnosed in APD children (see for review Keller & Tillery, 2002).
Additionally, rankings by audiologists and paediatricians of symptoms associated with
APD and ADHD correlated very high (Cacace & McFarland, 2005b; McFarland &
Cacace, 2003).
Both, children with APD and children with ADHD, have difficulties in paying
attention and remembering information presented orally, are easily distracted, have
difficulties in following complex acoustic directions or commands, and show low
academic performance.
Anecdotally children with APD show behaviour patterns associated with ADHD
criteria, including among others short attention spans, impulsivity, distractibility,
daydreaming, hypoactivity or hyperactivity, whereas children with ADHD have difficulty
with specific types of dichotic listening tasks, verbal memory measures, and word finding
or rapid naming tasks (see for review Riccio & Hynd, 1996). For example children with

General introduction
- 8 -
ADHD showed poorer speech discrimination in noise than control children (Geffner,
Lucker, & Koch, 1996), interpreted as worse figure-ground capabilities in children with
ADHD. Furthermore, patients perceived speech as comfortable or tolerable at lesser
loudness levels as control children (Lucker, Geffner, & Koch, 1996).
In addition to deviations in the auditory modality on behavioural levels, differences
between children with and without ADHD were also found in brainstem evoked potentials
or ERPs. For example Lahat and colleagues (1995) identified prolonged latencies of
early brainstem auditory evoked potentials in children with ADHD, pointing out an
additional dysfunction of early acoustic stimuli perception. Furthermore, during auditory
selective attention tasks the processing negativity (PN) of the ERPs – generated in the
auditory cortex – seemed to be smaller and more anterior located in children with ADHD
(Kemner, et al., 2004). The P300 frontal activity seemed to be higher whereas a reduced
activity in parietal regions was found compared to control subjects (Johnstone & Barry,
1996). At the same time, the reduced parietal activation was interpreted as attention
deficit and the frontal activity as compensatory mechanism. Additionally, imaging studies
provided a neuroanatomical basis through findings of morphologic and structural
differences in auditory brain areas (see for review Chermak, et al., 1999; Riccio & Hynd,
1996).
The overlap between both disorders could be confirmed by the high comorbidity
rate of learning disabilities in both. Thus, according to Barkley (1991a), approximately
25-40% of children with ADHD suffer from a learning disability. And Sharma and
colleagues (2009) reported that 67% of a sample of children with APD additionally had
language or reading problems, or both. Inversely it seems that children with nonverbal
learning disabilities run a risk to develop APD because a study showed that 61% of the
group of children with a nonverbal learning disorder was diagnosed with APD (Keller,
Tillery, & McFadden, 2006).
The results of these studies refer to an association between attention deficits and
performance on central auditory tests. Thus, three hypotheses arise: (1) APD and ADHD
may be distinct but comorbid, (2) one disorder causes the other or (3) both labels are
compatible and are assigned in dependency of the specialisation of the diagnostician
(Dawes & Bishop, 2009).
As a result, a range of authors (Cacace & McFarland, 2005a; Jerger & Musiek,
2000) challenged to improve the differential diagnosis with tests of multiple sensory
modalities because it has to be expected that APD is frequently comorbid showing
symptoms of other disorders (Witton, 2010). Following the theoretical framework, it was
assumed that children with APD perform poorly on auditory tasks, while children with

General introduction
- 9 -
ADHD might perform poorly on auditory and visual tasks (Dawes & Bishop, 2009; Jerger
& Musiek, 2000).
A first step for upgrading the diagnostic tools was the development of the
Continuous Attention Performance Test (CAPT) (Starzacher, Nubel, Grohmann, Gaupp,
& Pfeiffer, 2007) based on CPT test versions with visual and/or acoustic stimuli
(Jonkman, et al., 1997a, 1997b; Keith & Engineer, 1991; Klorman, et al., 1990; Mahone,
Pillion, Hoffman, Hiemenz, & Denckla, 2005; Morgan, Hynd, Riccio, & Hall, 1996; Tillery,
Katz, & Keller, 2000). Riccio and colleagues (1996) showed that it was not possible to
separate children with ADHD or ADHD and APD with an auditory CPT. Mahone and
colleagues (2005) found that children with ADHD performed worse in the auditory CPT
compared to control children - but only within very young children. Jonkam and
colleagues (1997b) revealed in both modality conditions higher error rates and reduced
event-related potentials for children with ADHD compared to control children. Starzacher
(2006) showed in 20 children with APD and 31 control children that children with APD
had a weaker performance compared to control children in the whole CAPT. Additionally,
she pointed out that within the control group no differences were found between visual
and auditory subtests – with reservations that high individual differences in performance
between both subtests exist. Children with APD exhibited a lower attention performance
in the acoustic than in the visual test. But an experiment with another integrated visual
and auditory CPT showed in 68 children with suspected APD that more children had
problems with both attention types than with auditory or visual attention alone.
Additionally, the authors suggested that 30% of the children had a normal auditory
attention and a diagnosis of APD, whereas 8% had a poor auditory attention but no APD
diagnosis (Sharma, et al., 2009). Furthermore, the attempts to differentiate APD children
with and without ADHD using electro physical measures have not been successful (Ptok,
Blachnik, & Schonweiler, 2004). These partly conflicting findings demonstrate that the
strict definition which identifies the deficits of children with APD as being restricted to the
auditory modality does not apply.
In summing up, ADHD (and its subtypes) and APD (including possible subtypes)
are very heterogenic and an overlap between behavioural symptomatology is evident.
Thus, there is a high possibility for misdiagnosis and comorbidity or a causal conjunction
(Cacace & McFarland, 2005b). Identifying an objective instrument for modality specific
perceptual malfunction would help to clarify criteria and diagnostic (Cacace & McFarland,
2005b). Thus, more research in this domain is necessary to upgrade diagnostic and
treatment in order to help people with the described disturbances.

General introduction
- 10 -
1.2 Saccades
Saccades are quick, simultaneous movements of both eyes in the same direction
serving as mechanism to new readjust our gaze over and over again to the particular
scene of interest to position this target on the fovea for a high definition vision (Leigh &
Zee, 1999). Thus, the function of voluntary saccades in primates is directly related to the
existence of a fovea. Saccades include both voluntary and involuntary changes of
fixation, the quick phase of vestibular and optokinetic nystagmus and the rapid eye
movements during sleep.
According to Leigh and Zee’s hierarchy classification (1999, 2006) there are nine
saccade classes from higher to lower order: (1) volitional saccades, (2) predictive,
anticipatory saccades, (3) memory-guided saccades, (4) antisaccades, (5) saccades to
command, (6) reflexives saccades, (7) express saccades, (8) spontaneous saccades
and (9) quick phases. In the context of inhibition investigation, two kind of saccades are
important for research: (i) reflexive saccades (called prosaccades) are saccades
triggered by sudden onset (visual, acoustic or tactile) stimuli and (ii) antisaccades which
are saccades generated towards the mirror image location of a sudden appearance of a
target (Hallett, 1978). Antisaccades as a task of response inhibition consists of two
processes: (1) the capacity to suppress a prepotent response before or after its initiation
and (2) the protection of this response delay and the goal-directed behaviour from the
interference of competing processes (Barkley, 1991a). The understanding of the
cognitive processes that underlie pro- and antisaccades – also described as exo- and
endogenous saccades – is of fundamental importance because there is considerable
evidence suggesting that antisaccade in contrast to prosaccades performance is mostly
impaired in psychiatric patients (Everling & Fischer, 1998; Hutton & Ettinger, 2006;
Karatekin, 2007; Rommelse, Van der Stigchel, & Sergeant, 2008). In the laboratory,
saccades are elicited by instructing the participants to look away from a central fixation
point towards (prosaccades) – which usually serve as control task – or to look to the
mirror image (antisaccades) of a sudden onset periphery target.
In doing so, different parameters are used to characterise saccades (see figure 1):

General introduction
- 11 -
Figure 1: The parameters of eye movement
Saccades amplitude: The amplitude is the size of the saccade, usually measured
in degrees of arc. The amplitude determines the saccade accuracy. This is commonly
denoted by the term "gain". The gain is the ratio of the actual saccade amplitude and the
desired saccade amplitude. The degree of dysmetria is usually relatively small (i.e. 10-
20% of the amplitude of the saccade; Leigh & Zee, 2006). Also, there is the
differentiation between hypometria (gains of <1) – i.e. the undershooting of saccades –
and hypermetria (gains of >1) – i.e. the overshooting of saccades.
Saccadic velocity: Saccades are the fastest movements produced by the human
body. After reaction initiation, velocity usually increases to a peak and then either
declines slightly or oscillates around the target velocity. This peak velocity can be used to
determine a value for the gain parameter (peak velocity/target velocity). It is usually
approximately equal to the velocity of the stimuli. The peak angular speed of the eye
during a saccade achieves 400 to 800°/sec (Irving, Steinbach, Lillakas, Babu, &
Hutchings, 2006; Leigh & Zee, 1999; Sparks, 2002).
Saccadic acceleration: The rate of change of the eye velocity is called
acceleration. Maximal acceleration of visual triggered saccades is 20000°/sec 2
(Haarmeier, in press).
Saccadic duration: Saccadic duration is the time taken to complete the saccade.
This is most easily measured from the velocity profile. Most saccades are completed
within 100ms (Leigh & Zee, 2006).
Saccadic latency: The latency is the processing time needed between stimulus
and response onset (conventionally when eye speed exceeds some threshold, such as

General introduction
- 12 -
30°/sec; Leigh & Zee, 2006). Saccadic latencies can be viewed as decision time because
this time is more than a pure signal transmission. The more saccades made, the less
time there is for fixations so it has to be determined whether the costs of a saccade are
justified. Saccades beginning -300 to +80ms relative to the onset of the cue are defined
as anticipatory responses (Klein, 2001). Reactions with latencies from 81 to 130ms post
stimuli are defined as express saccades – considered to be the most reflexive type of
eye movement – whereas regular saccades latencies are generated between 131 and
700ms (Klein, 2001; Klein, Foerster, Hartnegg, & Fischer, 2005). The typical latency of a
“reflexive” saccade in adults is around 200ms, and the variability around this average is
large. Antisaccades are associated with a higher effort and therefore antisaccades
latencies are typically elongated about 70-80ms in contrast to prosaccades (Everling &
Fischer, 1998; Forbes & Klein, 1996; Ford, Goltz, Brown, & Everling, 2005; Klein,
Raschke & Brandenbusch, 2003; Munoz, Broughton, Goldring, & Armstrong, 1998)
whereas the latency of erroneous antisaccades are generally in the range of standard
prosaccades (Evdokimidis, et al., 2002). The latency is highly dependant upon the nature
of the stimulus (Leigh & Zee, 1999). Modality and temporal properties of cue
presentation and their influence on saccade performance are explained in detail in
section 1.2.1.
Saccadic error rate: During the saccade task, errors occur when a prosaccade is
generated instead of an antisaccade or vice versa. Error rates during antisaccade tasks
reflect the ability to inhibit a response. Errors are usually followed by corrective saccades
to the suitable direction, indicating that the instruction was understood but the reflexive
response could not be suppressed. Thus, in contrast to prosaccades, higher error rates
were found in the antisaccade condition (Klein, et al., 2003; Munoz, et al., 1998). In
healthy adults, the antisaccade error rate is typically around 20% (Evdokimidis, et al.,
2002; Hutton, 2008; Leigh & Zee, 2006) – but the range both across participants and
studies depends to a major extent on the different task parameters.
Relationship between saccades parameters: The negative correlation between
percentage of error and mean latency is well established (Evdokimidis, et al., 2002;
Smyrnis, et al., 2002): the faster the response the higher the error rate. The relationships
between saccade amplitude, duration and velocity are specified, so that it is possible to
use them to characterise an observed eye movement as a normal or deviant saccade.
Thus, there is a linear relationship between saccadic amplitude and peak velocity; called
main sequence (Leigh & Zee, 1999): the bigger the gaze jump, the greater the maximum
speed. Similarly, a linear relation between amplitude and duration is characteristically for

General introduction
- 13 -
saccades: a saccade of 30° evinces saccade duration of circa 100ms (Leigh & Zee,
1999).
1.2.1 Influences on saccades
There are several cognitive factors (Hutton, 2008), task manipulation parameters
and at least individual properties that may influence the execution of saccades. In the
following paragraph a short overview of the relevant factors is given.
Gap/overlap effects: One of the most common manipulations in saccade tasks is
the relationship between offset of the central fixation stimulus and the onset of the
peripheral target stimulus. In “step” trials the fixation offset conforms to the onset of the
target. Whereas during “gap” trials the fixation offset precedes the target onset. And
during “overlap” trials the target onset takes place while the fixation stimulus is still
visible. The duration for both gap and overlap periods is typically 200ms. A large number
of studies supports the basic finding that the prosaccade latency is reduced in gap trials
and increased in overlap trials compared to step trials (Leigh & Zee, 2006; Saslow,
1967). The same effect was found in the antisaccade condition even though to a reduced
extent (Forbes & Klein, 1996; Klein, et al., 2003; Reuter-Lorenz, Oonk, Barnes, &
Hughes, 1995). Additionally, the delay of the stimulus onset interferes with the error rate:
during a gap condition more errors are generated (Klein, 2001; Klein & Foerster, 2001;
Klein, et al., 2003). These findings are explained by assuming that the disappearance of
the fixation stimulus in gap trials allows attention disengagement before the target arises
(resulting in faster saccade latencies and higher error rates), whereas during overlap
trials visual attention is engaged and saccades are inhibited (resulting in slower
latencies; Leigh & Zee, 2006). But the gap effect is more than a “fixation release”
component. It seems to involve an additional warning component which was found in
experiments with warning signals (Reuter-Lorenz, et al., 1995): fixation offset itself can
speed performance by increasing response readiness.
Eccentricity: Studies in the visual domain show that both the number of directional
errors to visual targets and the saccadic reaction time (SRT) rise with increasing stimulus
eccentricity (Jay & Sparks, 1990; Yao & Peck, 1997; Zambarbieri, Beltrami, & Versino,
1995). Additionally, hypometria is usually more prominent for saccades directed toward
the periphery whereas in normal individuals hypermetria – i.e. the overshooting of
saccades – is observed when the saccade is directed towards the centre (Leigh & Zee,
1999).

General introduction
- 14 -
Modality: Eye movements can be elicited by both visual and acoustic stimuli.
Prosaccades to acoustically triggered cues are slower (Goldring, Dorris, Corneil,
Ballantyne, & Munoz, 1996; Zambarbieri, Schmid, Magenes, & Prablanc, 1982;
Zambarbieri, Schmid, Prablanc, & Magenes, 1981) and have a lower peak velocity and
longer duration (Jay & Sparks, 1990; Zambarbieri, et al., 1982; Zambarbieri, et al., 1981).
Effects of eccentricity are dissociable for the acoustic versus the visual
experiment: an increasing distance between cue and fixation centre is associated with a
decreasing latency for acoustic stimuli and an increasing latency for visual cues (Frens &
Van Opstal, 1995; Jay & Sparks, 1990; Yao & Peck, 1997; Zambarbieri, 2002;
Zambarbieri, et al., 1995). But the findings are inconsistent. One study related any
effects on both visually and acoustically elicited saccades latencies (Zambarbieri, et al.,
1982) and another on acoustically triggered saccades only (Zambarbieri, et al., 1981). In
these studies, different presentation times were chosen – a hypothetical explanation for
absence of eccentricity influence. Concerning the accuracy, the eccentricity is not of high
importance: the accuracy rises with increasing eccentricity in both visually and
acoustically triggered saccades (Jay & Sparks, 1990; Yao & Peck, 1997). For target
eccentricity of ±20° and ±30°, acoustically trigger ed saccades were less accurate than
visually elicited reactions, but there were no significant differences in accuracy when
stimuli eccentricity was 10° (Yao & Peck, 1997).
Investigations related to the latency in the gap condition reported a reduction in
the gap effect in saccades elicited by acoustic stimuli compared to the effect in visual
conditions (Fendrich, Hughes, & Reuter-Lorenz, 1991; Shafiq, Stuart, Sandbach, Maruff,
& Currie, 1998; Taylor, Klein, & Munoz, 1999; Zambarbieri, 2002). Thus, it seems that
the gap effect is not modality specific. This is consistent with the interpretation that deep
layers of the superior colliculus (SC) appear as a likely candidate for the source of
premotor facilitation given that this structure receives convergent visual and acoustic
input (Jay & Sparks, 1990; Taylor, et al., 1999). Thus, findings from neurophysiological
studies investigating the SC in awake animals suggest that visual and acoustic signals
employ a final common pathway for the generation of saccades (Jay & Sparks, 1987a,
1987b). However, there is at least one critical difference: the superficial layer of the SC
receives direct visual input from the retina via the retinotectal pathway whereas acoustic
signals reach the SC via multisynaptic pathways that include the inferior colliculus.
Studies concerning the control of reflexive saccades elicited by acoustic stimuli
are rare. To date, only two studies investigated auditory antisaccades. One study
compared pro- and antisaccade performance in response to visual and acoustic cues in
healthy young adults and schizophrenia patients (Schooler, Roberts, & Cohen, 2008).

General introduction
- 15 -
The authors found a higher error rate for acoustically than visually triggered antisaccades
in healthy young adults, but the reverse pattern identifying more errors for visually than
for acoustically elicited antisaccades in schizophrenia patients. The authors attributed the
higher error rate for acoustically evoked antisaccades (as well as prosaccades) in
healthy adults to additional demands of the remapping process between the craniotopic
and the retinotopic system. Schizophrenia patients, by contrast, who generated overall
more errors than the healthy controls, produced relatively fewer errors on the acoustic
than the visual version of the task. This reverse pattern in schizophrenia patients is
assumed to be due to the fact that the remapping process reduces immediate inhibitory
demands on the system, making the stimulus ‘less preemptive’. Therefore, people with
reduced executive system capacities may experience a relative benefit from different
modality cues on tasks requiring response inhibition. The second study compared pro- to
antisaccade performance in response to acoustic cues in healthy adults and patients with
a hemispherectomy (Reuter-Lorenz, Herter, & Guitton, in press). The authors elicited
saccades by acoustic stimuli because of permanent hemianopia, which limits visually
evoked contralesional saccades. Patients generated more direction errors contralesional
than the control participants, whereas the rate of ipsilesional errors was approximately
equivalent to the error rate of the control group. Additionally, patients were slower in
initiating antisaccades than controls. Thus, the authors assumed that a single
hemisphere is not able to suppress reflexive saccades bilaterally but is capable to
generate antisaccades in response to acoustic stimuli. Finally, they hypothesised
alterations in the SC in the intact hemisphere.
Furthermore, Yao and Peck (1997) assumed that the motor coordinate system
used by humans in generating saccades to acoustic targets is identical to that used in
making saccades to visual cues. The only difference may be that the information about
the location of auditory targets must be transformed from craniotopic, i.e. head-related,
into retinocentric coordinates prior accessing the burst generators.
Age: Naturally, age is one of the cardinal factors of influence on saccadic
performance. During adolescence, the brain undergoes specialization that enables the
individual to adapt to their environment. This developmental maturation is related to brain
myelination, which progresses from dorsal to ventral brain regions and supports the
cognitive control of behaviour. Frontal and posterior parietal cortices involved in visually
guided saccades handling, continue to acquire myelin throughout childhood (Gogtay, et
al., 2004). Thus, many studies showed that the saccade latency itself as well as their
variability are relatively high in children (circa 210ms), decrease curvilinear from
childhood to adolescence (circa 170ms; Fischer, Biscaldi, & Gezeck, 1997; Fukushima,

General introduction
- 16 -
Hatta, & Fukushima, 2000; Irving, et al., 2006; Klein & Foerster, 2001; Klein, et al., 2005;
Munoz, et al., 1998; Salman, et al., 2006) and increases in a linear fashion in later years
(circa 210ms; Abel, Troost, & Dell'Osso, 1983; Fischer, et al., 1997; Klein, Fischer,
Hartnegg, Heiss, & Roth, 2000; Klein, et al., 2005; Munoz, et al., 1998). The change in
saccadic latencies in adolescents may reflect a shorter saccadic processing time as a
function of brain development. Longer saccadic latencies in children and elderly people
may reflect the immaturity and decomposition of several saccadic relevant processes,
respectively. Age also influences the gap effect in regard to latency – i.e. the SRT
reduction under the gap as compared to the overlap condition. This effect becomes
smaller with an increasing age (Klein, 2001).
Along with a decrease in latency there is only a weak relationship between age
and express saccades (Fischer, et al., 1997; Klein, et al., 2005). This lack of age-related
changes in express saccades suggests that the fixation system supported by subcortical
structures matures earlier than the cognitive processes needed for voluntary saccades
(Luna, Velanova, & Geier, 2008).
Findings in the domain of developmental changes of velocity have not been
consistent. A number of studies concluded that the peak velocity is not influenced by age
(Abel, et al., 1983; Fukushima, et al., 2000; Munoz, et al., 1998; Salman, et al., 2006)
while others reported a velocity increase in adolescence (from 446°/sec to 610°/sec) and
a gradual decline with age (345°/sec; Fioravanti, I nchingolo, Pensiero, & Spanio, 1995;
Irving, et al., 2006). Because of differences in task parameters it is difficult to compare
the studies with one another, but Luna and colleagues (2008) concluded that age
appears to have an effect, at least. Hypometria seems to be evident among the youngest
children (Munoz, et al., 1998), but stabilizes in childhood so that age effects are no
longer predominant (Luna, et al., 2008). Thus, no differences in the amplitude between
children and adults (Salman, et al., 2006) or adults and elderly (Abel, et al., 1983) were
found. One study pointed out that duration increased significantly across age groups
(Munoz, et al., 1998).
Finally, development looms large in response inhibition and working memory.
Both aspects develop on a different time course and influence performance in complex
executive tasks (Luna, Garver, Urban, Lazar, & Sweeney, 2004). In addition, there is
evidence that these two processes may be affected differentially in psychiatric disorders
like schizophrenia or ADHD (Ross, Harris, Olincy, & Radant, 2000). Both adult patients
groups are impaired in inhibition control, but only schizophrenic subjects demonstrate an
impaired working memory.

General introduction
- 17 -
The error rate during antisaccades tends to decrease from 60 to 13% as a
function of age (Fischer, et al., 1997; Fukushima, et al., 2000; Klein & Foerster, 2001;
Munoz, et al., 1998) and increases to 20% with higher age (Fischer, et al., 1997; Klein, et
al., 2000). Most of the participants correct their errors, indicating that all subjects,
independent of age, have the ability of generating post-inhibition voluntary saccades
(Luna, et al., 2008). During development there is also a reduction of intra-subject
variability (Klein, et al., 2005). At younger ages, a wide distribution of performances is
observed: some individuals mature earlier than others. Furthermore, the error gap effect
decreases from childhood to adulthood (Klein, 2001; Klein & Foerster, 2001). The same
pattern was found for the latency. It decreases curvilinear with age through childhood to
adolescence age (from approx. 350ms to 220ms; Fischer, et al., 1997; Fukushima, et al.,
2000; Irving, et al., 2006; Klein & Foerster, 2001; Klein, et al., 2005; Munoz, et al., 1998;
Salman, et al., 2006) and increases linearly again in later years (approx. 280ms; Abel, et
al., 1983; Fischer, et al., 1997; Klein, et al., 2000; Klein, et al., 2005; Munoz, et al., 1998).
Thus, studies have consistently demonstrated improvement of antisaccade performance
from childhood to adolescence.
1.2.2 Models of saccade generation: Race model & LATER model
Many authors (Hutton & Ettinger, 2006; Massen, 2004; Munoz & Everling, 2004)
argue that with stimulus onset a “competition” between the exogenously triggered pro-
and the endogenously initiated antisaccade starts. This rivalry is described by the Horse-
Race Model (Logan, et al., 1984) which proposes that the two processes – ongoing and
stop process – race against each other. If the stopping process wins (e.g. reaches some
threshold for activation), the reflexive saccade is cancelled. If the ongoing process wins
the competition, an erroneous prosaccade is made, sometimes followed by a corrective
antisaccade. Two interpretations of error generation have been developed: (1) errors will
occur if processes related to the initiation of the reflexive saccades are inadequately
interrupted, resulting in an increased likelihood of reaching the threshold for saccade
generation (Munoz & Everling, 2004). This describes two processes: an active inhibition
mechanism and an antisaccade generation (Everling & Fischer, 1998; Hutton, 2008). (2)
An alternative interpretation is that antisaccade errors result from a failure of adequate
activation of the correct response (Hutton, 2008; Nieuwenhuis, Broerse, Nielen, & de
Jong, 2004), which requires a single process: the generation of the antisaccade (Hutton,
2008). This view is also supported by Carpenter’s LATER model (Linear Approach to
Threshold with Ergodic Rate model; Cutsuridis, Smyrnis, Evdokimidis, & Perantonis,
2007) of neural decision-making. This model tries to explain the long and surprisingly

General introduction
- 18 -
variable latencies (approx. 200ms). Consequentially, in effect there has to be only a
delay around 60ms between stimulus and response because humans need 40ms to
transfer a visual signal to the SC and additional 20ms to trigger a saccade in the
brainstem (Carpenter, 1981) – the shortest neural circuit between retina and oculomotor
muscles. Carpenter proposes that the delay reflects an intentional “procrastination” that
allows a more elaborated processing of saccade cues than simply their location. It is a
kind of cost-benefit analysis to ensure that the processing resources are directed
towards the most relevant part of the scene. With the onset of the cue a decision signal
starts to rise linearly at a constant rate (r) from an initial level (S0) until it reaches a
threshold (ST), at which a saccade is initiated. The rate of rise varies randomly from trial
to trial in a Gaussian way (with a mean µ and a variance σ2), establishing the skewed
distribution of latencies (Carpenter & McDonald, 2007). Thus, despite their ubiquity and
apparent lightness, saccadic eye movements involve a wide variety of different cognitive
processes.
1.2.3 Neurophysiology of saccades
Saccadic generation includes a trade-off between “bottom up” signals that
concern basic stimulus properties, e.g. stimulus position and size, and “top down” signals
reflecting the current goal and ambitions of the person (Hutton, 2008). Reflexive
saccades seem to be controlled by subcortical systems while voluntary saccades appear
to be induced by a cortically dominated network (see figure 2).
Information about a visual target of interest enters through the retina and reaches
(1) via retinotectal pathway the SC and (2) via the geniculostrate pathway the visual
cortex. This brain region shows a higher activation in pro- than in antisaccades
(Clementz, et al., 2010; Dyckman, Camchong, Clementz, & McDowell, 2007; McDowell,
Dyckman, Austin, & Clementz, 2008), indicating that in this early state task-dependant
activation modulation is available (McDowell, et al., 2008). The visual cortex (including
striate and extrastriate visual areas) sends target information to the SC and to the
posterior parietal cortex (PPC with the parietal eye fields (PEF)). The PPC is also
connected to the SC and the frontal motor regions (McDowell, et al., 2008). It is primarily
involved in visuo-spatial integration and attention – a process which accompanies
saccade generation – whereas the PEF are directly involved in saccade programming via
the SC (Leigh & Zee, 2006; Pierrot-Deseilligny, et al., 2004). The activity in the PPC is
higher during voluntary than reflexive saccades (Dyckman, et al., 2007; Ettinger, et al.,
2008; Ford, et al., 2005; McDowell, et al., 2008).

General introduction
- 19 -
Figure 2: Cortical areas involved in saccade generation and execution. After processing visual information in the visual cortex and after integration of visuo-spatial integration in the PPC, reflexive saccades are triggered by the PEF. In contrast, intentionally saccades are elicited by the FEF. If a saccade is inhibited the DLPFC will play a primary role. Furthermore, the SEF are responsible for the control of motor programming, whereas the CEF inherit a motivational role for areas controlling intentional saccades. ACC: anterior cingulate cortex; CEF: cingulate eye fields; DLPFC: dorsolateral prefrontal cortex; FEF: frontal eye fields; PEF: parietal eye fields; PPC: posterior parietal cortex; SC: superior colliculus; SEF: supplementary eye field Modified to Pierrot-Deseilligny, Milea, & Muri, 2004; Pierrot-Deseilligny, Muri, Nyffeler, & Milea, 2005
The frontal cortex is important for motor control. The frontal eye fields (FEF) are
involved in planning and triggering of voluntary saccades (Reuter, Kaufmann, Bender,
Pinkpank, & Kathmann, 2009). Thus, lesions or transcranial stimulation of the FEF lead
to longer latencies of correct antisaccades and to inaccurate memory guided saccades
(Gaymard, Ploner, Rivaud, Vermersch, & Pierrot-Deseilligny, 1998; Muri, Hess, &
Meienberg, 1991; Nyffeler, et al., 2006). As early as during the instruction phase higher
activity was found in the FEF for voluntary saccades compared to reflexives saccade
tasks (Connolly, Goodale, Menon, & Munoz, 2002; Ford, et al., 2005). In sum, the FEF
influence the variation of RT within individuals and across different saccade tasks
(McDowell, et al., 2008) – probably via the direct connection to the SC. Also, strong
reciprocal connections exist between FEF and supplementary eye fields (SEF). It seems
that elicitation of antisaccades requires the suppression of saccade neurons in the FEF
and SC (Everling, Dorris, & Munoz, 1998; Everling & Munoz, 2000) before stimulus
General introduction
- 20 -
presentation. This inhibition seems to be caused by the SEF. Movement-related neurons
of the SEF discharge with a higher rate before anti- than prosaccades (Dyckman, et al.,
2007; Ford, et al., 2005; McDowell, et al., 2005). Finally, the dorsolateral prefrontal
cortex (DLPFC) as part of a prefrontal network is involved in the generation of
antisaccades, memory guided saccades and in decisional processes (Pierrot-Deseilligny,
et al., 2004). Several lesion studies showed that the percentage of errors in the
antisaccade task is increased after DLPFC lesion (Pierrot-Deseilligny, et al., 2003;
Pierrot-Deseilligny, Rivaud, Gaymard, & Agid, 1991; Ploner, Gaymard, Rivaud-Pechoux,
& Pierrot-Deseilligny, 2005). Therefore, it is assumed that the DLPFC is involved in
inhibition of reflexive eye movements (Gaymard, Ploner, et al., 1998; Pierrot-Deseilligny,
et al., 2004; Pierrot-Deseilligny, et al., 2005; Pierrot-Deseilligny, et al., 2003; Pierrot-
Deseilligny, et al., 1991; Ploner, et al., 2005). However, recent studies indicated that
DLPFC activation is more likely to reflect greater demands in the activation and
maintenance of task rules or in response selection (Dyckman, et al., 2007; Ettinger, et
al., 2008).
The role of subcortical structures during saccadic control has not yet been
clarified. Studies reporting saccade-related activity showed activation in ACC,
cerebellum, striatum, thalamus and SC. The ACC, including the cingulate eye fields
(CEF), seems to be involved in motivation of intentional saccades via preparation of FEF,
SEF and DLPFC (Gaymard, Rivaud, et al., 1998; Pierrot-Deseilligny, et al., 2003) and in
evaluation of the error response (Brown & Braver, 2005), as higher activation during
erroneous compared to correct antisaccades was found in this region (Ford, et al., 2005;
Polli, et al., 2005). The cerebellum has an influence on saccade steering and stopping –
i.e. determining the accuracy of saccades (Jenkinson & Miall, 2010; Ramat, Leigh, Zee,
& Optican, 2007). The striatum is involved in saccade initiation (Watanabe, Lauwereyns,
& Hikosaka, 2003) and inhibition (Hikosaka, Takikawa, & Kawagoe, 2000). The SC,
besides FEF and SEF, is a structure with projections directly to the reticular formation
(Munoz & Everling, 2004). It is a structure with seven layers of neurons responding to
visual, acoustic and somatosensory stimuli (Sparks, 2002). It receives projections from
FEF, SEF, DLPFC, PPC and the cerebellum (Munoz & Everling, 2004). Some of these
pathways are direct and some continue via basal ganglia (Leigh & Zee, 2006). The
neurons of the SC include saccade neurons, which increase their discharging before and
during the saccade, and fixation neurons, which are inactive during saccades but fire
during visual fixation (Munoz & Everling, 2004). Thus, the SC is basically involved in the
saccade generation. Disinhibition and inhibition of the SC are inherit by the SEF and

General introduction
- 21 -
additionally by the basal ganglia which are strongly modulated depending on behavioural
context, reflecting working memory, expectation or attention (Hikosaka, et al., 2000).
As mentioned above there are three parallel pathways to the brainstem neurons,
generating saccades: the SC, the FEF and the cerebellum directly influence the saccade
generation in the reticular formation (Munoz & Everling, 2004) where three cranial nerves
(Oculomotor nerve, Trochlear nerve and Abducens nerve) arise, innervating motor
neurons of three extraocular muscles pairs. These muscles are responsible for the final
control of the eye (Sparks, 2002).
1.2.4 Saccades & ADHD
Eye movement tasks are a unique neuroscientific tool which allows examining the
relationship between brain and behaviour and its development because it is very well
investigated. According to this it builds an important tool to explore the neurobiological
basis of psychiatric illness.
Moreover, this tool is particularly useful when studying children with
developmental disorders for numerous reasons. First, the saccade task is simple and
can be successfully performed on children. Second, the performance is less likely to be
facilitated by verbal or learning strategies like other neurophysiological tests. As a
consequence, the antisaccade task allows to investigate the inhibitory control with
minimal working memory demands except for remembering the instruction (Luna, et al.,
2008). Third, whether conducting with an eye tracker or Electroencephalography (EEG)
these systems are non-invasive. Fourth, the well described neural circuitry underlying the
control of eye movements is based on years of electrophysiological and lesion
experiments in monkeys and humans. Fifth, normal and abnormal eye movement
performances are unique. This allows drawing connections between performance,
development, disease, anatomical sources or drug interference. Sixth, oculomotor
methods – especially tasks with voluntary control of saccades – have proven to be
sensitive for impaired executive function in psychiatric disorders that are believed to have
a neurodevelopmental basis such as schizophrenia, autism and ADHD (Everling &
Fischer, 1998; Karatekin, 2007; Rommelse, et al., 2008; Sweeney, Takarae, Macmillan,
Luna, & Minshew, 2004).
Thus, antisaccade tasks may establish an objective and sensitive measure of
brain (dys-) function in children with and without ADHD and may also provide a basis for
differentiating these two groups.
There is a growing body of literature on saccade experiments comparing children
with ADHD to control children (Karatekin, 2007; Rommelse, et al., 2008). Despite some

General introduction
- 22 -
inconsistencies, the general finding is altered performance in pro- and antisaccade tasks
in children with ADHD compared to typically developed children. The majority of studies
on prosaccades revealed that children with ADHD compared with control children show
an increased variability of the SRT (Mostofsky, Lasker, Cutting, Denckla, & Zee, 2001;
Mostofsky, Lasker, Singer, Denckla, & Zee, 2001; Munoz, Armstrong, Hampton, &
Moore, 2003). Additionally, some studies revealed longer latencies itself for children with
ADHD (Klein, et al., 2003; Mahone, Mostofsky, Lasker, Zee, & Denckla, 2009;
Mostofsky, Lasker, Singer, et al., 2001; Munoz, et al., 2003). However, some
investigators did not find differences in the latency (Goto, et al., 2010; Hanisch, Radach,
Holtkamp, Herpertz-Dahlmann, & Konrad, 2006; Karatekin, 2006; Loe, Feldman, Yasui,
& Luna, 2009; Mostofsky, Lasker, Singer, et al., 2001; O'Driscoll, et al., 2005; Rothlind,
Posner, & Schaughency, 1991). It is assumed that the latency of prosaccades is more
variable and possibly slower in children with ADHD. This might be an indicator for ADHD
childrens’ difficulty in saccade generation (Rommelse, et al., 2008).
During antisaccade tasks some studies found slower antisaccade latencies (Goto,
et al., 2010; Karatekin, 2006; Klein, et al., 2003; Munoz, et al., 2003) and a higher
variability in children with ADHD compared with control children (Karatekin, Bingham, &
White, 2009). Other studies revealed no group differences in antisaccade latencies
(Karatekin, et al., 2009; O'Driscoll, et al., 2005; Rothlind, et al., 1991). The majority of
studies found elevated error rates in antisaccade tasks (Goto, et al., 2010; Karatekin,
2006; Klein, et al., 2003; Loe, et al., 2009; Mahone, et al., 2009; Mostofsky, Lasker,
Cutting, et al., 2001; Mostofsky, Lasker, Singer, et al., 2001; Munoz, et al., 2003;
O'Driscoll, et al., 2005) and a fewer correction in children with ADHD compared with
control children (Karatekin, et al., 2009; Klein, et al., 2003), whereas no effects were
discovered in a number of other studies (Aman, Roberts, & Pennington, 1998; Hanisch,
et al., 2006; Karatekin, et al., 2009; Rothlind, et al., 1991). The lack of the antisaccade
effect in these studies might be explained by a lack of statistical power and task
parameters (Rommelse, et al., 2008). One study – in which the different tasks are
presented in a mixed way – reported a statistical trend of p=.16 towards more directional
errors in the patient group (Hanisch, et al., 2006). In the second study – with an immense
age range – each participant performed only ten trials in each condition, possibly
resulting in low statistical power (Rothlind, et al., 1991). In a third study a different kind of
antisaccade task was used where an additional detection task was presented (Aman, et
al., 1998).
Finally, it seems that children with ADHD are impaired in inhibition of erroneous
prosaccades. This is in line with clinical evidence demonstrating that patients with ADHD

General introduction
- 23 -
are challenged by executive functions like response inhibition, vigilance, working
memory, and planning (Willcutt, et al., 2005).
Variables such as development, subtype of ADHD and medication additionally
influence the performance of children with ADHD. Thus, elongated latencies und
increased error rates in children with ADHD could be reduced by medication application
(Klein, Jr Fischer, Fischer, & Hartnegg, 2002; O'Driscoll, et al., 2005). This indicates that
the mechanisms responsible for the deficits in antisaccade performance are related to
the cortical structures influenced by methylphenidate (Rommelse, et al., 2008). Children
with ADHD show not the age-related latency pattern of control children: higher increase
in antisaccade compared to prosaccade latencies (Klein, et al., 2003). Furthermore, the
influence of different ADHD subtypes has not yet been investigated very well. It was
found that children with an ADHD combined subtype but no participants with an ADHD
inattentive subtype generated more errors than control children during antisaccade tasks.
Whereas the proportion of subjects with impaired antisaccade performance was higher in
the combined than in the inattentive subtype (O'Driscoll, et al., 2005). Additionally, it was
shown that there are no differences between the subtypes concerning the error rate
(Loe, et al., 2009; O'Driscoll, et al., 2005). One study pointed out that with training or
reduced working memory demands the performance of adolescents with ADHD can
reach the level of control subjects indicating that elevated SRTs during antisaccades in
this disorder may be related to regulating arousal on a novel task (Karatekin, 2006). It
was also found that participants with ADHD made more premature saccades and fewer
corrective saccades than both, the age-matched and younger groups. This suggests
difficulties with impulsivity and goal neglect or poor working memory for task instructions
(Karatekin, 2006).
1.3 Conclusion
One of the core deficits of ADHD is a disturbed response inhibition, manifested in
the difficulty in delaying responses, in blurting out answers to questions before they have
been completed, in difficulty in awaiting one´s turn in games or in group situations and in
interrupting or intruding on others (American Psychiatric Association, 2000). Inhibitory
deficits were verified in more than one study with responding to visual stimuli. But the
question arises if inhibitory deficits are restricted to the visual modality.
Inhibition of reaction on acoustic cues has a high practical relevance. Thus, a
child on a bike, for example, has to pay his or her full attention to the traffic in the
moment of crossing a road instead to a person calling his or her name. Or else, children
in the classroom having the motivation to listen to the teacher have to inhibit knee-jerk,

General introduction
- 24 -
focusing on whispering neighbours or siren sounds from outside. Thus, children and, of
course, adults need to be able to inhibit reflexive responses to acoustic stimuli.
It has to question if children with ADHD also impaired in this kind of inhibition
performance. This question immediately suggest itself due to impairments in range of
acoustic tasks (Riccio & Hynd, 1996), the large degree of overlaps between ADHD and
APD (although there are some behaviours more often associated with one disorder than
the other; Chermak, Tucker, & Seikel, 2002; Ptok, Buller, Schwemmle, Bergmann, &
Luerssen, 2006) and the up to 70% high comorbidity rate of learning disabilities (Mayes,
Calhoun, & Crowell, 2000), which enclose deficits in recording, integration, storing and
retrieving of visual as well as acoustic information.
In order to answer the core question whether children with ADHD are impaired in their
inhibitory control of reflexive reactions to visual as well as to acoustic cues and thereby
to promote the needed differential diagnostic, it is important to develop tests with
comparable performance measurements in different modalities. Thus, it is possible to
gain assumptions in which modality systems deficits are prior-ranking.
To enlarge the already existing multimodal diagnostic approach the idea of the
present thesis was to investigate the impulsivity in antisaccade experiments with different
modality inputs. Saccades triggered by visual stimuli are well investigated in children with
and without ADHD (Rommelse, et al., 2008). Some studies investigated also
prosaccades elicited by acoustic stimuli in adults (Fendrich, et al., 1991; Frens & Van
Opstal, 1995; Shafiq, et al., 1998; Yao & Peck, 1997; Zambarbieri, 2002; Zambarbieri, et
al., 1995; Zambarbieri, et al., 1982; Zambarbieri, et al., 1981). However, to date there are
only two studies that investigated antisaccades elicited by acoustic cues in the context of
schizophrenia and hemispherectomy, respectively (Reuter-Lorenz, et al., in press;
Schooler, et al., 2008) and none had investigated the antisaccade performance on
acoustic stimuli in children.
The aim of Study I was to test the practicability of the designed experiment and to
investigate the comparability of pro- and antisaccades elicited by visual and acoustic
stimuli in a control group. Based on primary interest in the behavioural performance an
eye tracker system was used. Because of the transformation from craniotopic into
retinocentric coordinates it was assumed to extend prior results of slower acoustically
compared to visually triggered prosaccades (Goldring, et al., 1996; Zambarbieri, et al.,
1982; Zambarbieri, et al., 1981) to antisaccades and to children. Additionally, eccentricity
effects were investigated during antisaccades and in children in order to compare the
results to the described effects in prosaccades (SRTs decreasing of acoustically
triggered saccades and SRTs increasing of visually triggered saccades with larger

General introduction
- 25 -
stimulus eccentricities; Frens & Van Opstal, 1995; Yao & Peck, 1997; Zambarbieri, 2002;
Zambarbieri, et al., 1995). Finally, the gap effect regarding SRTs, which appears less
pronounced for acoustically than for visually elicited prosaccades (Fendrich, et al., 1991;
Shafiq, et al., 1998; Taylor, et al., 1999; Zambarbieri, 2002), was investigated also for the
first time in acoustically triggered antisaccades.
Constructively based on the results on Study I the same experiment was carried
out with children with and without ADHD. One constriction of behavioural tests is that the
measurement of the performance is the end product of information processing. EEG
permits the measurement of brain activity – induced by task stimuli – before the
performance takes place, e.g. an answer will be observable. Therefore, Study II
measured along with the behavioural performance the brain activity. Functional brain
imaging studies have shown that a distributed fronto-parietal network is more active
when subjects perform antisaccades compared with prosaccades (McDowell, et al.,
2008). The DLPFC activity seems to provide an inhibitory signal that precedes a correct
antisaccade performance (Clementz, McDowell, & Stewart, 2001; Fitzgerald, et al., 2008;
McDowell, et al., 2005). Additionally, the ACC is relevant for the visual antisaccade
performance (Brown, Goltz, Vilis, Ford, & Everling, 2006; Ford, et al., 2005; Gaymard,
Ploner, et al., 1998; Polli, et al., 2005). Given that children with ADHD showed structural
and functional changes in a fronto-subcortical network (Bush, Valera, & Seidman, 2005;
Dickstein, et al., 2006; Seidman, et al., 2005) it was anticipated that children with ADHD
will generate more errors and altered brain activities in the antisaccade task compared to
control subjects.
Finally, children have difficulties to generate a prosaccade with a preceding
antisaccade (Hanisch, et al., 2006) or more generally, they have difficulties when mixed-
saccade tasks were applied (O'Driscoll, et al., 2005). In adults a context effect was also
detected on the behavioural (Barton, Greenzang, Hefter, Edelman, & Manoach, 2006;
Barton, Raoof, Jameel, & Manoach, 2006; Ethridge, Brahmbhatt, Gao, McDowell, &
Clementz, 2009) as well as on cortical level (Dyckman, et al., 2007). Blocked conditions
are easier and do not add a third step to the inhibition of prepotent response and the
execution of the appropriate eye movement: interpretation of the cue (Irving, Tajik-
Parvinchi, Lillakas, Gonzalez, & Steinbach, 2009). In order to simplify the experiment for
Study III a block design of the experiment was developed. It was assumed that through
this design it will be possible to differentiate children with and without ADHD on the
behavioural as well as on cortical level and, in doing so, to gain a differentiated view on
damages of children with ADHD in the different modalities.

Three antisaccade studies – Study I
- 26 -
II. THREE ANTISACCADE STUDIES
2.1 Pro- and antisaccades in children elicited by v isual and acoustic cues – does
modality matter?
2.1.1 Abstract
Background
Children are able to inhibit a prepotent reaction to suddenly arising visual stimuli,
although this skill is not yet as pronounced as it is in adulthood. However, up to now no
study investigated the inhibition mechanism to acoustic stimuli.
Methods
Reflexive (prosaccade) and inhibitory (antisaccade) responses to visual and
acoustic cues were examined with an eye tracker system in 31 children between seven
and twelve years of age using a gap-overlap task and two cue eccentricities.
Results
Acoustically cued saccades had longer reaction times than visually cued
saccades. A gap effect (i.e. shorter reaction time in the gap than the overlap condition)
was only found for visually elicited saccades, whereas an eccentricity effect (i.e. faster
saccades to more laterally presented cues) was only present in the acoustic condition.
Longer reaction times of antisaccades compared to prosaccades were found only in the
visual task. Across both tasks the typical pattern of elevated error rates in the
antisaccade condition was found. Antisaccade errors were declining with age, indicating
an ongoing development of inhibitory functions.
Conclusions
The present results lay the ground for further studies of acoustically triggered
saccades in typically as well as atypically developing children.
2.1.2 Introduction
It is a reflex-like feature of human behaviour to look towards sudden changes in
our visual field. This enables us to respond adequately to changes in our environment.
Scientifically, this reflexive behaviour is studied with prosaccade tasks. Here, participants
are required to generate a saccade to a suddenly appearing peripheral visual cue – also
called “visual grasp reflex”. Parameters such as accuracy and saccadic reaction time
(SRT) can be measured (Leigh & Zee, 1999). In order to not look towards a suddenly
appearing peripheral cue, volitional inhibition of the visual grasp reflex is required.
Scientifically, this can be investigated with antisaccade tasks (Hallett, 1978). Here,
participants are asked to suppress a prosaccade towards a visual cue and to look at its

Three antisaccade studies – Study I
- 27 -
mirror position in the opposite visual field instead. As antisaccades require active
inhibition of an already initiated motor response, more direction errors are made and
SRTs are longer compared to prosaccade tasks (Forbes & Klein, 1996; Ford, et al.,
2005; Fukushima, et al., 2000; Klein & Foerster, 2001; Munoz, et al., 1998; Munoz &
Everling, 2004). The timing of peripheral cue onset affects direction error rate and SRT of
both pro- and antisaccades. When the central fixation cross disappears before the onset
of the peripheral cue (gap condition), more errors are produced than when the peripheral
cue appears while central fixation is still on (overlap condition). At the same time, SRT in
gap conditions is reduced compared to overlap conditions. This “gap effect” is probably
due to the reduction in firing rate of fixation neurons in the superior colliculus and frontal
eye fields with gap onset (Munoz, et al., 1998; Munoz & Everling, 2004; Saslow, 1967).
This causes faster responses as saccade neurons in these structures start firing earlier.
The SRT gap effect is bigger for prosaccades than antisaccades (Forbes & Klein, 1996)
and more pronounced in children than in young adults (Klein, 2001; Klein & Foerster,
2001; Munoz, et al., 1998). Another factor affecting direction errors and SRT is the
peripheral position (eccentricity) of the target. Both, the number of direction errors in
response to visual targets and SRT increase with larger stimulus eccentricity (Yao &
Peck, 1997; Zambarbieri, et al., 1995). Studies of ocular motor performance in children
have shown that SRT decreases with age (Salman, et al., 2006) as does the proportion
of direction errors, although at a different pace (Fukushima, et al., 2000; Klein, 2001;
Klein & Foerster, 2001; Klein, et al., 2003; Munoz, et al., 1998).
Humans not only look towards visual stimuli, they also direct their gaze to locate
the origin of a suddenly appearing sound. This reaction is already present in babies (Muir
& Field, 1979). Although saccades towards acoustic cues are scientifically less well
investigated than saccades towards visual cues, a recent study delineated an “acoustic-
evoked ocular grasp reflex” in adults (Reuter-Lorenz, et al., in press).
Both children and adults also need to be able to inhibit reflexive visual responses
to acoustic stimuli. A child, for example, will automatically look at the person who calls
his name. But standing in the middle of a busy street it might be better to not look at the
person but to focus on the traffic coming from the opposite direction to avoid an accident.
An important difference between the visual and auditory modality is the reference
system. While input to the visual field is thought to be processed in relation to a
retinotopic reference system, acoustic cues are related to a craniotopic, i.e. head-related,
reference system (Zambarbieri, et al., 1995). The craniotopic reference system is by
definition wider than the retinotopic reference system, this being caused by the position
of the ears on the sides of our head, while the eyes face forward. The craniotopic

Three antisaccade studies – Study I
- 28 -
reference system is more accurate and sensitive to lateral stimuli, while the retinotopic
system is most accurate for stimuli directly in front of us. When sounds trigger a saccadic
response, it is assumed that sound representation needs to be remapped from the
craniotopic into the retinotopic reference system, in order to produce spatially correct
saccades (Yao and Peck, 1997).
Animal studies with nonhuman primates as well as experimental studies with
adults have revealed lower accuracy and longer SRTs of prosaccades towards acoustic
cues than towards visual cues (Jay & Sparks, 1990; Zambarbieri, et al., 1982;
Zambarbieri, et al., 1981). This is probably caused by the additional demand of
remapping from the craniotopic to the retinotopic reference system. Considering target
eccentricity, a reverse relationship between SRTs and target position has been found in
the auditory compared to the visual modality: SRTs of acoustically triggered saccades
decrease for larger stimulus eccentricities, but SRTs of visually triggered saccades
increase with larger stimulus eccentricities (Frens & Van Opstal, 1995; Yao & Peck,
1997; Zambarbieri, 2002; Zambarbieri, et al., 1995). Ostensibly at least in adults, a
processing advantage for centrally presented visual stimuli and a disadvantage for
centrally presented acoustic stimuli exists (Zambarbieri, et al., 1982). In adults, the gap
effect also interacts with target modality. The gap effect regarding SRTs of prosaccades
appears less pronounced for acoustic than for visual cues (Fendrich, et al., 1991; Shafiq,
et al., 1998; Taylor, et al., 1999; Zambarbieri, 2002).
The vast majority of studies on saccades triggered by acoustic cues only
investigated prosaccades. Until now there are only two studies, which investigated
acoustically triggered antisaccades in adults (Reuter-Lorenz, et al., in press; Schooler, et
al., 2008). One of these studies (Reuter-Lorenz, et al., in press) studied acoustic
antisaccades in three patients with hemispherectomy and a control group. They revealed
that patients generated more errors and showed longer SRTs than control participants.
Schooler and colleagues (2008) investigated adults with and without schizophrenia and
compared performance in antisaccade tasks using visual and acoustic cues. They found
a higher error rate for acoustically than visually triggered antisaccades in healthy young
adults while patients generated the reverse pattern of more errors during visually than
during acoustically elicited antisaccades.
The present study is – to the best of our knowledge – the first to compare SRTs
and error rates of pro- and antisaccades elicited by visual and acoustic cues in typically
developing children. We investigated children between seven and twelve years regarding
the impact of central fixation engagement (gap, overlap) as well as target eccentricity on
pro- and antisaccades elicited by visual and acoustic peripheral cues.

Three antisaccade studies – Study I
- 29 -
This is of relevance as studies on pro- and antisaccades triggered by acoustic and
visual cues in children will further our understanding of modality differences in ocular
motor responses and the development of basic, ecologically as well as clinically relevant
sensory-motor processing.
2.1.3 Methods
Participants
31 children between seven and twelve years participated in this study. They were
recruited at primary schools in the Konstanz area. Six children had to be excluded
because they were too small for the eye-tracker, too restless, had a partial hearing loss,
low scores on a questionnaire on auditory processing and perception, or because they
decided to not to continue after the half-time break in the experiment. The 25 remaining
children (18 girls and seven boys) had a mean age of 9.31 ±0.24 years. 24 children were
right-handed, one child was left-handed. None of the children fulfilled criteria for attention
deficit hyperactivity (ADHD) or auditory processing disorder (APD). Neither did parents
report any other neurological, psychiatric, or physiologic problems.
Procedure
The families were shown the laboratory equipment and the task was explained to
them. Children and parents then signed informed consent forms (according to the
Helsinki declaration (WMA, 2004)). Parents were asked to fill in a general information
questionnaire about their child, an ADHD symptom checklist (Lauth & Schlottke, 2002),
and an auditory processing disorder checklist (DGPP, 2002) while children completed
the Edinburgh-Handedness-Inventory (Oldfield, 1971). To ensure within-normal hearing
levels, children’s hearing thresholds were determined for frequencies 500, 1000, 2000
and 4000Hz in an acoustically shielded room. Children were then shown a computerised,
animated explanation of the task, which included examples and four training trials. For
additional motivation, children were told that they would be able to collect four “cartoon
dogs” on the computer screen if they performed well (although the dogs always
appeared after fixed intervals) which would then allow the children to pick a small gift
from a “treasure chest” after the experiment. Thus, it was ensured that all children were
motivated and perceived themselves as successful. Children were additionally
compensated with 10 Euros at the end of the experimental session.
For the eye-tracker experiment, children were comfortably seated on a height-
adjustable chair, their heads resting on a chin rest 518mm away from the computer
monitor. Brightness and contrast of the eye tracker-camera were adapted, headphones

Three antisaccade studies – Study I
- 30 -
were put on and the 30min - experiment was started after calibration of the eye tracker
(11 standard positions distributed over the screen).
Task
Participants were instructed to generate saccades in response to visual or
acoustic cues. The nature of the required saccade depended on the instruction.
Saccades could either be directed towards the cue (prosaccade) or away from the cue
(antisaccade). Visual cues consisting of yellow dots that that filled one of four empty
circles could appear “near” (6°) or “far” (12°) lef t or right of the fixation cross for 1000ms.
Acoustic cues were 1000Hz sine tones presented for 1000ms that were perceived either
“far” left/right (90°) or “near” left/right (45°, s ee the description below). Children were
instructed that in response to “near” acoustic cues they should generate saccades
towards the 6° circle, and upon “far” to make sacca des towards the 12° circle. Cues
could either appear 200ms after extinction of the fixation cross (gap) or with a 200ms
overlap with the fixation cross. Random combinations of the following within-group
factors were presented throughout the experiment: cue modality (visual vs. acoustic),
direction (right vs. left), type (anti- vs. prosaccade), distance (near (6° visual, 45°
acoustic) vs. far (12° visual, 90° acoustic)), dela y (gap vs. overlap). Nine runs of each
combination resulted in a total of 288 trials.
After trials 96, 129, 259 and 288 children were shown a motivation picture with 1,
2, 3 and 4 dogs, respectively. A pause-signal appeared after 144 trials indicating that
children could take a short break. The length of the break was determined by the
children.
Each trial began with a 1000ms instruction slide depicting the nature of the
required saccade by a prominent symbol the meaning of which had been explained to
the children beforehand (see procedure above). Each trial lasted 6500ms (see figure 3
for a schematic overview).

Three antisaccade studies – Study I
- 31 -
Figure 3: Example trial (visual prosaccade); top: overlap-condition and bottom: gap-condition
Equipment and Oculomotor Recordings
Cues were presented with the software Presentation (Neurobehavioral Systems,
Inc.). Visual cues were generated within Presentation. Sine tones were generated with
Adobe Audition 2.0®. The effect of sound lateralisation was created by intensity and
phase differences between the left and right channel. The impression of a 90°
lateralisation to either direction was created by attenuating the contra-lateral channel by
3.62dB and shifting its onset by 6.5µs. The impression of a 45° lateralisation was created
by attenuating the contralateral channel by 2.8dB and delaying its onset by 1µs.
Stimuli were presented with a PC (Intel (R) Pentium (R) 4, CPU 3.00GHz
processor, 522.928 RAM) running a Windows 2000® operating system on a monitor with
640 x 480pixels resolution (22”/51cm viewable; Iivama MA203DT; Vision Master Pro
513) and via stereo headphones (Sony Digital Reference Dynamic MDR-CD470). The
recording computer had the same specifications as the stimulus computer.
Eye movements were measured with a high-speed camera system (iView Hi-
Speed-Eye Tracker, SensoMotoric Instruments, Teltow, Germany). The eye-tracker had
a temporal resolution of 240Hz and a spatial resolution <0.01°. Data were stored for
offline analysis. During testing, eye movements were visualised on the recording
computer to enable on-line monitoring and re-calibration, if necessary.
Data analysis
SRTs and direction of saccades were analysed. Saccade onset was defined semi-
automatically with the software BeGaze® Version 1.02.0076 (SensoMotoric Instruments,
http://www.smivision.com). Individual saccades were cross-checked manually and
onsets were corrected if necessary.
Direction error rate and SRT were analysed statistically using Statistica version
6.1 (StatSoft, Inc., 2003, http://www.statsoft.de). Univariate repeated measures analyses

Three antisaccade studies – Study I
- 32 -
of variance (ANOVAs), using within-subject factors modality (visual/acoustic), type (anti-
/prosaccade), distance (near/far), and delay (gap/overlap) were computed. Significant
interactions were investigated further with a post hoc test (Tukey’s Honest Significant
Difference-Test). Correlations between age (in months) and dependant variables were
tested using the Bravais Pearson correlation test and Spearman Rank test. Correlations
of dependant variables in the visual and acoustic condition were tested with the Bravais
Pearson correlation test, Spearman Rank test and the partial correlation test.
2.1.4 Results
Saccadic Reaction Times
Results will be restricted to correct trials, since incorrect trials were rare in some
conditions (i.e. visual prosaccades), potentially skewing latency results. There were no
significant correlations between age and SRTs in either condition.
Therefore, it was not necessary to use age as a covariate of no interest in the
ANOVAs. Mean SRT for correct reactions was 620.76 ±163.08ms. Saccades triggered
by visual cues had shorter SRTs than saccades after acoustic cues (main effect modality
F(1,23)=97.370, p<.001, acoustic: 791.08 ±202.16ms, visual: 449.36 ±160.11ms). SRTs
of prosaccades were shorter than SRTs of antisaccades (main effect type
F(1,23)=20.488 p<.001, pro: 567.09 ±144.30ms, anti: 674.88 ±195.80ms). An interaction
between modality and type was found (F(1,23)=18.606, p<.001, see figure 4a).
Acoustically triggered pro- and antisaccades did not differ in SRTs (acoustic-pro: 769.21
±190.59ms, acoustic-anti: 812.95 ±236.44ms, p=.198). In contrast, SRTs of visual
prosaccades were significantly shorter than SRTs of visual antisaccades (visual-pro:
364.97 ±136.24ms, visual-anti: 535.01 ±196.47ms, p<.001).
SRTs in gap conditions were shorter than in overlap conditions (main effect delay:
F(1,23)=29.986, p<.001, gap: 587.68 ±165.70ms, overlap: 653.52 ±165.33ms). The
interaction modality*delay (F(1,23)=16.402, p<.001, see figure 4b) showed no SRT
difference between gap and overlap for saccades triggered by acoustic stimuli (acoustic-
gap: 776.48 ±208.02ms, acoustic-overlap: 805.68 ±209.06ms, p=.610), whereas SRTs in
gap-conditions were shorter than in overlap conditions for visually evoked saccades
(visual-gap: 397.36 ±162.49ms, visual-overlap: 501.37 ±163.45ms, p<.001, figure 4b).
Investigating SRT as a function of stimulus eccentricity showed that SRTs after
cues near the fixation cross were longer than SRTs after cues that were further away
(main effect distance F(1,23)=7.747, p<.05, near: 645.42 ±161.74ms, far: 595.74
±174.02ms). A significant interaction modality*distance was also found (F(1,23)=19.224,
p<.001, see figure 4c). Near and far stimulus cues led to equally long SRTs within

Three antisaccade studies – Study I
- 33 -
visually triggered conditions (visual-near: 437.59 ±167.03ms, visual-far: 460.81
±171.11ms, p=.676), whereas for acoustically evoked saccades SRTs were shorter after
cues that were further away from the fixation cross compared to near cues (acoustic-
near: 853.24 ±197.55ms, acoustic-far: 728.92 ±222.56ms, p<.001).
There was a positive correlation between SRTs in the visual and the acoustic
condition (r=.515, p<.01) across saccade type and for pro- and antisaccades,
respectively (antisaccades: r=.497, p<.05; prosaccades: r=.484, p<.05, see figure 4d).
Figure 4: a: Interaction modality*type for the dependant variable latency; b: interaction modality*delay for the dependant variable latency; c: interaction modality*distance for the dependant variable latency; d: correlation between latencies in visually and acoustically cued saccades; filed circle: antisaccades, empty circles: prosaccades
Error Rates
As there was a correlation between age and overall-error rate (age/error r=-.459,
p<.05), as well as age and antisaccade errors (see table 1), age was used as continuous
predictor in the ANOVAs.
Table 1 : Correlation of errors with age [in month] Age [in month] correlation with r(X.Y) p All -0.459 0.021 Antisaccades All -0.490 0.013 Visual -0.467 0.019 Acoustic -0.355 0.081 Prosaccades All -0.150 0.473 Visual -0.009 0.965 Acoustic -0.235 0.259

Three antisaccade studies – Study I
- 34 -
Across all conditions a mean of 27.38 ±9.22% direction errors were generated,
whereof 69.05 ±12.31% were corrected. The main effect type revealed that children
made more direction errors during anti- than prosaccades (antisaccades: 20.27 ±7.42%,
prosaccades: 7.11 ±3.61, F(1,23)=12.428, p<.01). The interaction type*modality was
marginally significant (F(1,23)=3.378, p=.079; visually cued antisaccades: 25.58 ±9.29%,
acoustically cued antisaccades 14.88 ±8.34%, visually cued prosaccades: 3.93 ±2.35%,
acoustically cued prosaccades 10.35 ±6.25% (see figure 5a). This result showed in the
post hoc test significant higher error rates in the anti- than in the prosaccades within in
the visual condition (p<.001) but none in the acoustic condition (p=.121) and additionally
significant higher error rates during saccades towards acoustic than visual cues within
the prosaccade condition (p<.05) and a significant opposite result within the antisaccade
condition (p<.001).
The interaction modality*distance (F(1,23)=4.616, p<.05, see figure 5b) revealed
that groups only differed in the 8° condition ( p<.05). Error rates were higher during
visually than during acoustically elicited saccades (visual condition: 15.67 ±5.58%,
acoustic condition: 12.74 ±5.38%). No further post-hoc tests were significant.
There was a positive correlation between errors in the visual and the acoustic
condition (r=.663, p<.001, see figure 5c) across saccade type, whichever is still
significant in a partial correlation corrected for age (r=.594, p<.01). However, further
inspection revealed that error rates only correlated between modalities for antisaccades
without controlling for age, not for prosaccades (antisaccades: r=.400, p<.05, partial
correlation: r=.314, p=.126; prosaccades: r=.282, p=.172).

Three antisaccade studies – Study I
- 35 -
Figure 5: a: Interaction modality*type for the dependant variable error rate; b: interaction modality*distance for the dependant variable error rate; c: correlation between errors in visually and acoustically cued saccades
2.1.5 Discussion
The present study is the first to investigate pro- and antisaccades following visual
and acoustic cues in children.
Using visual cues, the present study replicates a number of previous findings:
SRTs were longer for antisaccades than for prosaccades (Everling & Fischer, 1998;
Forbes & Klein, 1996; Ford, et al., 2005; Klein, et al., 2003; Munoz, et al., 1998) and
shorter for gap than for overlap trials (Everling & Fischer, 1998; Klein, et al., 2003;
Munoz, et al., 1998). More direction errors were made on antisaccade than on
prosaccade trials (Ford, et al., 2005; Fukushima, et al., 2000; Munoz, et al., 1998; Munoz
& Everling, 2004). Target eccentricity affected neither RT nor error rate. This
corresponds with findings in a study with children that used similar eccentricities as the
present one, namely 8°, 12° and 24° (Fukushima, et al., 2000), but differs from other
studies with adults (Yao & Peck, 1997; Zambarbieri, et al., 1995), suggesting that
developmental effects may account for the null finding in children. Alternatively, effects of
target eccentricity may appear only with larger visual angles.
Using acoustic cues revealed that SRTs did not differ between pro- and
antisaccades. An explanation might be that as the remapping process from the
craniotopic to the retinotopic reference system takes more time (as reflected in over-all
longer SRTs for acoustically triggered saccades), the salience of the acoustic cue

Three antisaccade studies – Study I
- 36 -
becomes obscured and thus the immediate “grasp-reflex” less strong. This is somewhat
supported by the findings regarding error rates. Although the main effect condition
suggests that across modalities more antisaccade errors were made than prosaccade
errors, the interaction condition*modality was marginally significant. Thus, although there
is a tendency for more errors in the anti- than in the prosaccade condition, the anti/pro-
difference is smaller than in the visual condition. This is due to more prosaccade and
fewer antisaccade errors in the acoustic than the visual condition. Correct acoustic
prosaccade generation appears to be more difficult than visual prosaccade generation in
children. In line with this finding a lower error rate on acoustically than on visually cued
antisaccades was observed by Schooler and colleagues (2008) in adult schizophrenia
patients but not in healthy adults. The authors offered the explanation that the remapping
process reduces immediate inhibitory demands on the system, making the acoustic
stimulus ‘less preemptive’. Therefore, people with reduced executive system capacities
may experience a relative benefit from different modality cues on tasks requiring
response inhibition. Children’s executive system is also less developed, as frontal lobe
maturity is only reached in adulthood (Gogtay, et al., 2004). Therefore their lower error
rate in the acoustic antisaccade task might result from their presumably less developed
executive system, which may benefit from the extra time gained in the re-mapping
process.
No auditory gap effect was found for SRTs nor error rates. In contrast to this,
previous findings in adults have described a smaller, but still significant gap effect for
acoustically cued saccades (Fendrich, et al., 1991; Reuter-Lorenz, et al., in press;
Shafiq, et al., 1998; Taylor, et al., 1999). It might be the case for children that although
mean SRTs indicate a gap-effect, it is obscured by a relatively high SRT variablity
(208.02ms gap, 209.06ms overlap condition). Alternatively, Fendrich and colleagues
(1991) suggest that a reduction (or absence) of the gap effect for acoustic cues might be
due to the fact that gap durations are usually chosen to be optimal for visual but not
necessarily for auditory saccades. In line with this notion and the present findings
Reuter-Lorenz and colleagues (in press) neither found a gap effect for error rates when
antisaccades were elicited by acoustic cues.
Target eccentricity had an effect on SRTs of acoustically cued saccades,
saccades to more peripheral targets being generated more quickly than saccades to the
nearer targets. This extends previous results in adults (Yao & Peck, 1997; Zambarbieri,
2002; Zambarbieri, et al., 1995; Zambarbieri, et al., 1982; Zambarbieri, et al., 1981) to
children between the ages of seven and twelve.
Three antisaccade studies – Study I
- 37 -
Comparing results across modalities showed that SRTs to acoustic targets were
generally longer than to visual targets. This finding replicates previous results for
prosaccades in adults (Fendrich, et al., 1991; Jay & Sparks, 1990; Shafiq, et al., 1998;
Zambarbieri, 2002; Zambarbieri, et al., 1995; Zambarbieri, et al., 1982; Zambarbieri, et
al., 1981) and extends them to children and to antisaccades. It shows that extra
processing time is needed to switch between references systems. Target eccentricity
affected SRTs to acoustic, but not visual cues, saccades to more distant acoustic cues
being generated more quickly than to closer cues. Presumably, within a craniotopic
reference system more lateral cues are easier to locate than nearer cues (Yao & Peck,
1997). Modality differences were found in the near condition: more errors for visually
than acoustically triggered saccades were made. One possible explanation might be the
different stimulus presentation degree between modalities. While visual cues were
presented 8° or 12° lateral of the fixation cross, acoustic stimuli represented a 45° and
90° angle. Thus, it might have been easier to disti nguish between the sides in the
acoustic condition.
Correlations between age (in months) and SRTs revealed no developmental
effects of age on saccadic RT within the age range studied. Yet, across all conditions the
slope of the regression line was negative, still indicating a small reduction of SRTs with
age until young adulthood, which, in line with other previous reports, may reach
significance for wider age ranges (Klein, 2001; Klein & Foerster, 2001; Munoz, et al.,
1998). For direction errors, significant negative correlations between age in months and
error percentage were observed for both visual and acoustic antisaccades, but not for
prosaccades, indicating a significant improvement in antisaccade performance between
the ages of seven and twelve years in both modalities. These results extend the findings
of developmental visual saccade performance (Klein, 2001; Klein & Foerster, 2001) to
the auditory modality. Thus, it can be assumed that developmental effects are
comparable for the visual and the acoustic condition.
The correlation between latencies in visual and acoustic conditions indicates that
both tasks are to some degree comparable. Children with slower latencies in visual
condition also had slower latencies in the acoustic condition. The same was true for error
rate.
2.1.6 Conclusion
The present study was the first study to investigate pro- and antisaccades elicited
by visual and acoustic stimuli in children. While many similarities between cue
presentation modalities arose, there were important differences: the “grasp-reflex” was

Three antisaccade studies – Study I
- 38 -
weaker for auditory saccades and they seemed less prone to be influenced by impulsivity
as their latency was longer resulting in fewer antisaccade errors. Studying different input
modalities in the context of response inhibition might be of interest for investigating
populations with disorders, such as auditory processing disorder (APD) and attention-
deficit/hyperactivity disorder (ADHD), as these diagnoses tend to overlap, although APD
should by definition be restricted to difficulties in the auditory domain. The present results
would predict that children with ADHD and children with APD should show dissociated
error and latency patterns.

Three antisaccade studies – Study II
- 39 -
2.2 Medio-frontal and anterior temporal abnormaliti es in children with attention
deficit hyperactivity disorder (ADHD) during an aco ustic antisaccade task as
revealed by electro-cortical source reconstruction
2.2.1 Abstract
Background
Attention deficit hyperactivity disorder (ADHD) is one of the most prevalent
disorders in children and adolescence. Impulsivity is one of three core symptoms and
likely associated with inhibition difficulties. To date the neural correlate of the
antisaccade task, a test of response inhibition, has not been studied in children with (or
without) ADHD.
Methods
Antisaccade responses to visual and acoustic cues were examined in nine
unmedicated boys with ADHD (mean age 122.44 ±20.81 months) and 14 healthy control
children (mean age 115.64 ±22.87 months, three girls) while an Electroencephalogram
(EEG) was recorded. Brain activity before saccade onset was reconstructed using a 23-
source-montage.
Results
When cues were acoustic, children with ADHD had a higher source activity than
control children in medio-frontal cortex (MFC) between -230 and -120ms and in the left-
hemispheric temporal anterior cortex (TAC) between -112 and 0ms before saccade
onset, despite both groups performing similarly behaviourally (antisaccades errors and
saccade latency). When visual cues were used EEG-activity preceding antisaccades did
not differ between groups.
Conclusion
Children with ADHD exhibit altered functioning of the TAC and MFC during an
antisaccade task elicited by acoustic cues. Children with ADHD need more source
activation to reach the same behavioural level as control children.
2.2.2 Introduction
Children with ADHD have difficulties with cognitive control, working memory and
response inhibition (Willcutt, et al., 2005). Response inhibition consists of two processes:
(i) the capacity to suppress a prepotent response before or after its initiation, and (ii) the
goal-directed behaviour from the interference of competing processes (Barkley, 1991b).
Antisaccades are one way to examine inhibition, as antisaccade tasks require the
suppression of the automatic response to look towards a peripheral cue and to generate

Three antisaccade studies – Study II
- 40 -
a saccade in the opposition direction instead (Everling & Fischer, 1998). Error rates
during antisaccade tasks reflect the ability to inhibit a response, while saccadic reaction
times (SRT) during correct trials reflect the duration of the underlying cognitive and motor
processes. There is a growing body of literature on eye movement experiments
comparing children with ADHD with control subjects (Rommelse, et al., 2008). Despite
some inconsistencies, the general finding is that subjects with ADHD have an elevated
number of direction errors during antisaccade tasks (Goto, et al., 2010; Karatekin, 2006;
Klein, et al., 2003; Loe, et al., 2009; Mahone, et al., 2009; Mostofsky, Lasker, Cutting, et
al., 2001; Mostofsky, Lasker, Singer, et al., 2001; Munoz, et al., 2003; O'Driscoll, et al.,
2005). However, until now, no study has examined brain function during antisaccade
tasks in ADHD, although this might lead to important new insight into the cortical
mechanisms of behavioural inhibition and its dysfunction in ADHD.
Inhibition difficulties are not only relevant in the visual domain, where they have
mostly been studied. Humans also redirect their gaze to locate the origin of a suddenly
appearing noise, a tendency, which is already present in babies (Muir & Field, 1979).
Still, until now, there is no study, which investigates pro- or antisaccades elicited by
acoustic cues in children. Accordingly, it is unclear, which neuronal network underlies
antisaccades following acoustic cues. There is a particular interest in analysing inhibition
deficits following acoustic cues in children with ADHD as a high number of children with
ADHD have difficulties with acoustic tasks (Breier, Fletcher, Foorman, Klaas, & Gray,
2003; Sutcliffe, Bishop, Houghton, & Taylor, 2006; Tillery, et al., 2000).
Electrophysiological and functional brain imaging studies have given insight into
which cerebral areas are active during visual saccadic tasks. The frontal eye fields
(FEF), the supplementary eye fields (SEF) and the parietal eye fields (PEF) in the
posterior parietal cortex (PPC) are active when saccades are initiated. The dorsolateral
prefrontal cortex (DLPFC) and the anterior cingulate cortex (ACC) with the Cingulate Eye
Field are associated with “higher level”, volitional and cognitive aspects of saccade
control, specifically during antisaccades (Connolly, et al., 2002; Ford, et al., 2005;
Kulubekova & McDowell, 2008; Munoz & Everling, 2004; Pierrot-Deseilligny, et al., 2004;
Pierrot-Deseilligny, et al., 2005; Pierrot-Deseilligny, et al., 2003; Pierrot-Deseilligny, et
al., 1991; Ploner, et al., 2005). DLPFC shows activity during antisaccades that is not
present during prosaccades (Clementz, et al., 2010). Its activity seems to provide an
inhibitory signal that precedes correct antisaccade performance (Clementz, et al., 2001;
Fitzgerald, et al., 2008; McDowell, et al., 2005). Directional errors are therefore generally
linked to frontal dysfunctions. The ACC is involved in the executive control of attention
and plays an important role in visual antisaccade performance (Brown, et al., 2006; Ford,

Three antisaccade studies – Study II
- 41 -
et al., 2005; Gaymard, Ploner, et al., 1998; Polli, et al., 2005). Given that children with
ADHD have difficulties with response inhibition and make more antisaccade errors than
children without ADHD, one might assume that activity of frontal structures involved in
the generation of antisaccades is altered. Disturbed functioning of prefrontal cortex,
ACC, and striatum are also thought to underlie other executive function deficits in ADHD
(Bush, et al., 2005). This is in line with the aetiological theory that ADHD results from
structural and functional changes in a fronto-subcortical network (Bush, et al., 2005;
Dickstein, et al., 2006; Seidman, et al., 2005).
The first aim of the present study was to investigate how children with and without
ADHD differ in brain activation during an antisaccade task. The second aim was to
investigate, whether children with ADHD have comparable inhibition difficulties when
cues are visual and acoustic.
2.2.3 Methods
Participants
Sixteen children with ADHD and sixteen children without ADHD were investigated.
Children with ADHD were recruited at two child psychiatric outpatient clinics, diagnoses
being made by the head psychiatrist and his/her team of psychologists based on
questionnaires, anamnestic biographical interviews and psychometric tests. Control
children were recruited at a local school. However, data of seven children with ADHD
and data of two control children had to be discarded due to insufficient data quality (too
many movement artefacts). Data of nine children with ADHD (mean age 122.44 ±20.81
months, boys only) and 14 healthy control children (mean age 115.64 ±22.87 months,
three girls) were further analysed. All but one child with ADHD were diagnosed with
ADHD combined type; the remaining child was diagnosed with ADHD primarily
inattentive type. All children were investigated off medication. Three children with ADHD
who were prescribed with methylphenidate refrained from taking it at least 24 hours
before the experiment in concordance with their respective psychiatrist and their parents.
All children with ADHD had at least one comorbid disorder (mostly specific
developmental disorder of motor function) and 44% had at least two comorbid disorders
(mostly specific developmental disorders of scholastic skills). Control children did not
have any clinically relevant diagnoses or took any medication as reported by the parents.
Procedure
Children and parents were shown the laboratory equipment and the task was
explained to them. They then signed informed consent forms (according to the Helsinki

Three antisaccade studies – Study II
- 42 -
declaration (WMA, 2004)). Parents were asked to fill in an ADHD symptom checklist
(Lauth & Schlottke, 2002), an auditory processing disorder (APD) checklist (DGPP,
2002) and a routine questionnaire while children completed the Edinburgh-Handedness-
Inventory (Oldfield, 1971). To ensure within-normal hearing levels, children’s hearing
thresholds were determined for frequencies 500, 1000, 2000 and 4000Hz in an
acoustically shielded room. Children were then shown a computerised, animated
explanation of the task, which included examples and four training trials. To ensure that
all children were motivated and perceived themselves as successful, children were told
that they would be able to collect four “cartoon dogs” on the computer screen if they
performed well (the dogs always appeared after fixed intervals) which would then allow
the children to pick a small gift from a “treasure chest” after the experiment. Children
were additionally compensated with 20 Euros at the end of the experimental session.
For the EEG experiment, children were comfortably seated in a chair, their heads
resting on a chin rest 500mm away from the computer monitor. Headphones were put on
and the 30min - experiment was started after impedance measurement. After the EEG
experiment intelligence was assessed by the Coloured Progressive Matrices (CPM;
Raven, Raven, & Court, 2002).
Task
Participants were instructed to generate saccades in response to visual or
acoustic cues. The nature of the required saccade depended on the instruction.
Saccades could either be directed towards the cue (prosaccade) or away from the cue
(antisaccade). Visual cues, consisting of yellow dots that filled one of four empty circles,
could appear “near” (6°) or “far” (12°) and left or right of the fixation cross for 1000ms.
Acoustic cues were 1000Hz sine tones presented for 1000ms that were perceived either
“far” left/right (90°) or “near” left/right (45°, s ee the description below). Children were
explained that in response to “near” acoustic cues they should generate saccades
towards the 6° circle, and upon “far” to make sacca des towards the 12° circle. Cues
could either appear 200ms after extinction of the fixation cross (gap) or with a 200ms
overlap with the fixation cross. Random combinations of the following within-group
factors were presented throughout the experiment: cue modality (visual vs. acoustic),
direction (right vs. left), type (anti- vs. prosaccade), distance (near (6° visual, 45°
acoustic) vs. far (12° visual, 90° acoustic)) and d elay (gap vs. overlap). Nine runs of each
combination resulted in a total of 288 trials. This random design was chosen to avoid
ceiling effects and enable better group differentiation.

Three antisaccade studies – Study II
- 43 -
After trial 96, 129, 259 and 288 children were shown a motivation picture with 1, 2,
3 and 4 dogs, respectively. A pause-signal appeared after 144 trials indicating that
children could take a short break. The length of the break was determined by the
children.
Each trial began with a 1000ms instruction slide depicting the nature of the
required saccade by a prominent symbol the meaning of which had been explained to
the children beforehand (see procedure above). Each trial lasted 6500ms (see figure 6
for a schematic overview).
Figure 6: Temporal structure of an exemplary trial (visual prosaccade); top: overlap-condition and
bottom: gap-condition
Equipment and Recordings
Cues were presented with the software Presentation (Neurobehavioral Systems,
Inc.). Visual cues were generated within Presentation. Sine tones were generated with
Adobe Audition 2.0®. The effect of sound lateralisation was created by intensity and
phase differences between the left and right channel. The impression of a 90°
lateralisation to either direction was created by attenuating the contra-lateral channel by
3.62dB and shifting its onset by 6.5µs. The impression of a 45° lateralisation was created
by attenuating the contralateral channel by 2.8dB and delaying its onset by 1µs.
Stimuli were presented with a PC Dell precision 390 with Intel ® Core ™ 2CPU
2.13Hz-processor with 2GB Ram operating system on a monitor with 365 x 270mm
resolution (Samtron 96 BDF) and via stereo headphones (Sennheiser HD 280 pro
(64Ω)).
Electrical brain activity was measured using EEG. Recording was done with a 257
channel system from EGI Electrical Geodesics Inc. using NetStaionTM12 on a Mac OSX
with 1,25GHz PowerPC G4 processor and 1GB DDR SD RQM. Sample rate was 250Hz
and an online filter of 100Hz lowpass and 0.1Hz highpass were applied.

Three antisaccade studies – Study II
- 44 -
Data analysis
Data were analysed with BESA software (Brain Electrical Analysis, version
5.2.4.52, MEGIS Software GmbH, Graefelfing, Germany). Vertical and horizontal eye
movements artefacts (blinks and saccades) were systematically removed using an
algorithm implemented in BESA (Berg & Scherg, 1994; Lins, Picton, Berg, & Scherg,
1993). For each condition, data were segmented into epochs from 500ms pre to 2000ms
post stimulus (notch filter at 50Hz). For the identification of saccades, data were filtered
digitally from 0.01-8Hz (6dB/octave forward and 12dB/octave zerophase). The
percentage of correct saccades was determined and saccade latency was measured to
the nearest sampling point. Saccades with latencies <80ms were excluded, as they can
be classified as anticipations rather than responses (Klein, 2001). Next, unfiltered
response-locked averages of antisaccades (merged across direction, distance and delay
to gain higher statistical power and more averages for source reconstruction) were
generated i.e. epochs (500ms pre and 500ms post response) were exported, which were
centred at saccade onset. Source analysis was carried out with a 23-source-model
(generated on the basis of talairach coordinates of structures known to be involved in
saccade generation), data being filtered digitally from 0.1-30Hz (6dB/octave forward and
24dB/octave zerophase). The source montage was generated to cover activity of
structures relevant for the processing and production of saccades (SEF, FEF, DLPFC,
PPC – left and right, frontal midline and medio-frontal cortex (MFC)). Further, sources
were placed that covered activity of structures relevant for the processing of acoustic and
visual stimuli (supplemental temporal cortex (STC), temporal parietal cortex (TPC),
temporal anterior cortex (TAC) – left and right). Additional sources of no interest
(cerebellum – left and right) were placed to increase the sensitivity of the sources of
interest. The sensitivity of a source describes its ability to pick up the activity generated
by the brain volume of interest. Source sensitivity is dependant on the position of the
source in the brain model, the number of sources in the montage, as well as the distance
between the sources. The sensitivity of relevant sources was carefully tested with
sensitivity maps in BESA (see figure 7 for the sensitivity map). The output of a source
montage is each individual source’s activity over time. Source positions in space are
fixed.

Three antisaccade studies – Study II
- 45 -
Figure 7: Sensitivity map of the MFC (top) and the TAC left (bottom)
Statistical analysis
Only antisaccades were analysed, as the leading question of the present article
concerned response inhibition. SRTs and the percentage of correctly generated
antisaccades (merged across direction, distance and delay) were compared between
groups using Statistica (StatSoft, Inc., 2003). T-tests or Mann-Whitney-U tests were
computed after testing for normal distribution of the dependant variables using Shapiro-
Wilks-W-test. Scores of questionnaire data were analysed accordingly. In order to
objectively identify time-windows, throughout which the experimental groups differed in
activity of one or more sources, non-parametric cluster-based analysis of EEG source
data was performed using FieldTrip, an open-source signal processing toolbox for Matlab
(Donders Institute for Brain, Cognition and Behaviour, Radboud University Nijmegen,
The Netherlands. http://www.ru.nl/neuroimaging/fieldtrip). Groups were compared for
each sampling point and each source via independent t-tests. In order to prevent
chance-findings, data were re-shuffled 1000 times using a cluster-based Monte-Carlo
randomization.
This method effectively controls for multiple comparisons (Maris & Oostenveld,
2007). Clusters (here: clusters of sampling points) were defined as significant when the
probability of observing larger effects in the shuffled data was below 5%. As response
inhibition takes place before the onset of the saccade and in accord with already existing
findings (Clementz, et al., 2001; McDowell, et al., 2005), data analysis was carried out for
the time-windows -230ms until -120ms before response and -120ms until 20ms after
response.

Three antisaccade studies – Study II
- 46 -
2.2.4 Results
Sample characteristics
Groups did not differ in age (t(21)=0.689, p=.499) or gender distribution
(χ2(1)=2.22, p=.135). Children with and without ADHD had comparable intelligence
scores as measured by the CPM (ADHD: 71.00 ±29.97 percentile rank, Control: 66.15
±29.84 percentile rank; t(19)=0.361, p=.722). Children with and without ADHD had
hearing sensitivities of 20dB or better in each ear for all measured frequencies (American
Speech-Language-Hearing Association, 1997). Groups did not differ from each other
(see table 2).
Table 2: Results hearing levels ADHD (n=9) Control (n=14)
Side tested test Frequency (Hz)
Mean SD Mean SD t/Z- Value
df p
t-test 500 4.67 5.05 3.50 4.15 0.605 21 0.552 t-test 1000 1.56 4.98 0.21 3.93 0.721 21 0.479 t-test 2000 -0.89 4.83 -0.79 4.92 -0.049 21 0.961
Right
t-test 4000 0.33 5.36 -0.93 6.81 0.469 21 0.644 t-test 500 3.00 7.45 3.36 5.42 -0.133 21 0.895 MWU 1000 -1.33 8.02 -0.86 6.77 -0.031 21 0.975 MWU 2000 -2.67 5.55 0.07 8.40 -0.661 21 0.508
Left
MWU 4000 -2.00 6.08 -0.43 9.49 -0.504 21 0.614
Children with ADHD had higher values than control children for both subscales of
the ADHD questionnaire (see table 3). Groups also differed on the subscales Speech
Perception and Auditory Memory of the APD questionnaire (see table 3).

Three antisaccade studies – Study II
- 47 -
Table 3: Results parental ratings of ADHD/APD symptoms
ADHD Control
Symptoms Subscales Test n Mean SD n Mean SD t/Z-value
df p
Inattention MWU 9 34.00 7.38 14 14.71 2.40 3.874 21 0.000 ADHD
Hyperactivity/ Impulsivity
MWU 9 3.09 0.67 14 1.34 0.22 3.969 21 0.000
Speech Perception
t-test 9 1.89 0.73 13 1.29 0.25 2.767 20 0.012
Auditory Discrimination
MWU 9 1.38 0.72 14 1.14 0.23 0.787 21 0.380
Sound Localisation
MWU 9 1.27 0.53 14 1.01 0.05 1.134 21 0.086
Hearing in background noise
MWU 9 1.63 0.78 14 1.48 0.41 0.157 21 0.874
Auditory Memory
MWU 9 1.81 0.65 14 1.30 0.42 2.331 21 0.019
APD
Auditory Hypersensitivity
t-test 9 2.77 0.64 13 2.48 0.62 1.058 20 0.303
Saccadic reaction and latencies
Groups did not differ regarding correct antisaccade reactions in the visual
condition (ADHD 50.52 ±16.54% correct, Control 48.84 ±20.53% correct, t(21)=0.205,
p=.839) and in the acoustic condition (ADHD: 57.20 ±12.88% correct, Control: 65.38
±12.32% correct, t(21)=-1.527, p=.142).
There were neither group differences in antisaccade latency in the visual condition
(ADHD: 493.36 ±196.43ms, Control: 441.00 ±146.65ms, Z(21)=0.504, p=.614), nor in the
acoustic condition (Antisaccades: ADHD: 696.25 ±258.34ms, Control: 639.94
±226.71ms, t(21)=0.551, p=.588).
Pre-saccadic brain activity
A significant group difference was identified for the acoustic antisaccade condition
between 228 and 140ms before antisaccade onset (t(21)=74.707, p<.05) in the MFC
source and at 112-0ms before antisaccade onset (t(21)=76.294, p<.05) in the TAC left
source. Children with ADHD showed higher source activity than control children (MFC:
ADHD: 67.09 ±40.16nAm, Control. 34.59 ±13.49nAm, see figure 8; TAC left: ADHD:
61.83 ±31.80nAm, Control 31.34 ±20.18nAm, see figure 9).
In contrast, no significant group differences were revealed in the visual
antisaccade condition in either of these sources or any other source.

Three antisaccade studies – Study II
- 48 -
Figure 8: Group effect for the dependant variable source power of correct antisaccades in the MFC
Figure 9: Group effect for the dependant variable source power of correct antisaccades in the TAC left
2.2.5 Discussion
Aim of this study was to investigate differences in response inhibition and
corresponding brain activity between children with and without ADHD. Response
inhibition was measured in an antisaccade task where saccades were either elicited by
acoustic or visual cues.
The main finding of the study was that children with and without ADHD differed in
brain activity when saccades were elicited by acoustic cues. Children with ADHD had a
higher source activity than control children in the MFC source between -228 and -140ms
and in the left-hemispheric TAC source between -112 and 0ms before saccade onset.
These time windows overlap with the critical period for response inhibition in visual
antisaccade tasks (Clementz, Brahmbhatt, McDowell, Brown, & Sweeney, 2007;
Clementz, et al., 2001; McDowell, et al., 2005).
Three antisaccade studies – Study II
- 49 -
Behavioural data
No group differences regarding the correctness of saccade execution were found
in the present study. Other studies on antisaccades using only visual cues revealed an
elevated number of direction errors in children with ADHD (Rommelse, et al., 2008),
indicating that these children are less able than control children to inhibit inappropriate
responses. However, there are also studies in line with the present findings (Aman, et al.,
1998; Hanisch, et al., 2006; Rothlind, et al., 1991) without group differences. The random
design of experimental presentation in the present study was chosen to increase task
difficulty in order to differentiate between the groups. However, it might have been the
case that the task was equally more difficult for both, control children and children with
ADHD, as supplementary task switching between pro- and antisaccades is required
(Irving, et al., 2009; O'Driscoll, et al., 2005), thus concealing group effects.
Another explanation for the negative finding of behavioural group differences
might be related to the age range of the children in the present study. Rothlind and
colleagues (1991) investigated a group of children with a similar age range. The mean
age of their ADHD group was 10.5 ±2.4 years (range: 6.9 – 13.9 years), mean age of the
control group was 9.9 ±2.8 years (range: 6.8 – 14.4 years). As in the present study,
Rothlind and colleagues did not find any group differences in saccadic errors. Other
studies have used groups of children with a smaller age-range and were able to find
more errors in children with ADHD (Goto, et al., 2010; Karatekin, 2006; Klein, et al.,
2003; Mahone, et al., 2009; Munoz, et al., 2003; O'Driscoll, et al., 2005). A reason might
be that boys younger than 11 years have difficulty with oculomotor inhibition in general
(Fischer, et al., 1997; Klein & Foerster, 2001). However, a study with younger children
has also found differences between children with and without ADHD (Goto, et al., 2010)
and thus questions the assumption of a general oculomotor inhibition deficit in younger
children. Finally the subtype of ADHD might be an influencing factor on performance in
saccade tasks. Children with ADHD combined type made more antisaccade errors than
control children, while no group differences were found between children with ADHD
inattentive type and control children (O'Driscoll, et al., 2005). In the present study eight of
nine children with ADHD had the diagnose ADHD combined type. Thus, ADHD subtype
is not likely to have influenced the response pattern in the present study.
As for saccadic correctness, no group differences were found for SRTs in the
present study. The latency of correct antisaccades was not investigated in all saccade
studies and results are inconsistent. Some studies found slower antisaccade latencies in
children with ADHD compared with control children (Goto, et al., 2010; Karatekin, 2006;
Klein, et al., 2003; Mostofsky, Lasker, Cutting, et al., 2001; Mostofsky, Lasker, Singer, et

Three antisaccade studies – Study II
- 50 -
al., 2001; Munoz, et al., 2003). Other studies found no group differences in antisaccades
latencies (O'Driscoll, et al., 2005; Rothlind, et al., 1991), which is in line with the present
result.
Thus, it is still unclear why no group differences were found in the rate of correct
saccades and its latencies. The small sample size – which resulted from the fact that
only ADHD children off medication were included – and the relatively big age range
seem to be the most likely explanation. However, an absence of behavioural differences
reduces ambiguities in the interpretation of any effects in brain measures.
Pre-saccadic brain activity
Indeed, source activation differed between groups in the acoustic condition.
Children with ADHD had higher activation of the MFC and the left-hemispheric TAC
compared to control children during time-windows likely to reflect response inhibition.
MFC includes parts of the dorsal ACC, which is connected with the prefrontal cortex and
parietal cortex as well as the motor system and the frontal eye fields (Brown, Vilis, &
Everling, 2007; Ding, Powell, & Jiang, 2009; Wang, Matsuzaka, Shima, & Tanji, 2004). It
is crucially involved in the executive control of attention. The ACC plays an important role
in visual antisaccade performance (Brown, et al., 2006; Ford, et al., 2005; Gaymard,
Ploner, et al., 1998; Polli, et al., 2005) and ACC activity seems to be altered in patients
with ADHD (Bush, et al., 1999; Colla, et al., 2008; Fallgatter, et al., 2004; Paul-Jordanov,
et al., 2010). In the present study, children with ADHD had higher activity in the MFC
source than control children preceding an auditory antisaccade. Still, behavioural
performance, i.e. the percentage of correctly executed saccades did not differ between
the groups. It thus appears that children with ADHD needed more activation of the MFC
to reach the same level of response inhibition as control children. The present results
were found only when saccades were elicited by acoustic cues. Still, a comparable
pattern of brain activation results was found in studies investigating response inhibition in
a visual go/nogo task design (Dickstein, et al., 2006; Durston, et al., 2003; Vaidya, et al.,
1998). The present results are also in line with a meta - analysis (Dickstein, et al., 2006),
which concluded that there are two brain areas, in which ADHD patients have
significantly more activation than controls: the medial frontal gyrus and the right
secondary somatosensory area.
Activation of the left TAC source was higher in children with ADHD than in control
children preceding antisaccades. Results from other experiments regarding temporal
lobe activity during cognitive tasks are inconsistent. There seems to be some evidence of
dysfunction and also of compensatory use of the temporal lobes in ADHD (Cherkasova &

Three antisaccade studies – Study II
- 51 -
Hechtman, 2009). However, the current finding is in line with a go/nogo study in which
children with ADHD showed more activation than the control children in the
middle/inferior/superior temporal gyrus (Tamm, et al., 2004). This might be also related
to structural abnormalities in children with ADHD (Seidman, et al., 2005). Castellanos
and colleagues (2001; 2002) showed that children with ADHD have a reduced volume of
frontal and temporal gray matter, caudate, and cerebellum. These volume reductions
were related with measures of symptom severity in an ADHD sample (Casey, et al.,
1997; Castellanos, et al., 2002). Another study detected reduced brain volumes in the
lateral anterior and midtemporal cortices bilaterally (Sowell, et al., 2003). Lateral
temporal and parietal regions are part of the cross-modal association cortex, which also
includes the DLPFC. This system integrates information from lower order sensory
systems into higher order rules and functions. It is assumed that these regions together -
beside their anatomical interconnection - form a broadly distributed action-attention
system that supports the maintenance of attentional focus and successful inhibition
(Mesulam, 1998; Peterson, et al., 1999; Sowell, et al., 2003). It might be speculated that
because of the smaller volume of the temporal cortex, children with ADHD showed more
reflexive reaction to acoustic cues. Because of that, more frontal activation might have
been needed as well in order to control behavioural output.
Finally, group differences in brain activation during acoustically elicited
antisaccades are in line with auditory deficits (in Speech Perception and Auditory
Memory) as detected in the APD questionnaire in the present study. The results are also
in line with a suggested symptom overlap of children with ADHD and children with APD
(Cacace & McFarland, 2006; Dawes & Bishop, 2009; Keller & Tillery, 2002; Witton,
2010). APD is characterised by disturbed hearing despite a normally functioning
periphery. Typical symptoms are poor recognition, discrimination, separation, grouping,
localisation, ordering of non-speech sounds and difficulties with acoustic tasks when
competing acoustic signals are present (American Speech-Language-Hearing
Association, 2005; British Society of Audiology Steering Group, 2007). Both, children
with APD and children with ADHD, have difficulty paying attention and remembering
information presented orally, are easily distracted, have difficulty following complex
acoustic directions or commands, and show low academic performance. The present
results also demonstrate that acoustic processing should be a focus of interest in ADHD
research. Knowing more about alterations of the auditory systems and according
consequences might enable better differentiation of the ADHD/APD diagnosis.
Three antisaccade studies – Study II
- 52 -
In summary, both structures - MFC and the left-hemispheric TAC - are part of
functional brain areas involved in attention and response inhibition, and seem to be
functionally or structurally altered in children with ADHD.
Against expectations, no differences in brain activity were found in the visual
antisaccade condition. There might be many contributing factors such as sample size,
task design, and age range, as mentioned above. It is not possible to directly compare
the present results to previous findings, as no other studies have investigated brain
activation during antisaccades in children with ADHD. However, it should be noted that
there are inconsistent findings in imaging studies of other visual inhibition tasks. Some
studies reported that ADHD children exhibit a smaller P300 amplitude than control
children (Kemner, et al., 1996; Liotti, et al., 2005; Paul-Jordanov, et al., 2010; Paul, et al.,
2007), and showed lower activation of inferior prefrontal cortex and other brain regions
(Dickstein, et al., 2006; Rubia, et al., 1999; Rubia, Smith, Brammer, Toone, & Taylor,
2005). Other authors found increased activation in prefrontal brain regions (Durston, et
al., 2003; Vaidya, et al., 1998) and in the medial frontal gyrus respectively (Dickstein, et
al., 2006). Again, it is difficult to compare studies using different inhibition tasks. More
research with bigger sample sizes and a smaller age range are needed to answer to the
question if there are differences in brain activity between children with and without ADHD
during visually cued antisaccades.
2.2.6 Conclusion
In sum, the present study for the first time provides insight in the cortical network
underlying the production of antisaccades elicited by acoustic stimuli in children with and
without ADHD. While no group differences were found when visual cues were used,
results showed that functioning of the anterior temporal lobe and medio-frontal cortex is
altered in children with ADHD when acoustic cues are used to trigger antisaccades. The
present results support the hypothesis that cortical structures underlying response
inhibition are more active in children with ADHD to achieve the same behavioural output
as children without ADHD, possibly as a compensatory mechanism.

Three antisaccade studies – Study III
- 53 -
2.3 Brain activation differences during the generat ion of visually and acoustically
guided antisaccades between children with and witho ut attention deficit
hyperactivity disorder (ADHD)
2.3.1 Abstract
Background
Disinhibition is a symptom of ADHD. It can be investigated with the antisaccade
task, where the reflex to look towards an appearing stimulus needs to be suppressed.
Children with ADHD have difficulties with this task. Until now, only response inhibition
after visual cues has been explored in ADHD. However, research into the cross-modality
of disinhibition is necessary in order to better understand the executive function deficit in
ADHD and to distinguish ADHD from auditory processing disorder. The present study
investigated cross-modal response inhibition.
Methods
16 children with ADHD and 16 healthy control children participated in two
antisaccade experiments with visual and acoustic cues while an Electroencephalogram
(EEG) was recorded. Behavioural data (errors and latencies) as well as response-locked
EEG-activity were analysed. Source localisation (CLARA) was performed in time-
windows of significant effects between and within groups.
Results
Children with ADHD had an inhibition deficit only when cues were visual. Children
with ADHD made more saccadic errors than control children when cues were acoustic,
yet they were not specifically impaired with response inhibition. Groups differed in brain
activity in a time-window corresponding to response inhibition. Source reconstruction of
this effect implied frontal hypoactivation and a parietal-cerebellar compensatory network
in ADHD.
Conclusion
Although children with ADHD do seem to have greater difficulties generating
saccades when acoustic cues are used, they do not have an inhibition deficit. Children
with ADHD only had difficulties with response inhibition after visual cues. This supports
the idea that deficient response inhibition is not a cross-modal phenomenon.
2.3.2 Introduction
ADHD is characterised by inattention, hyperactivity and impulsivity (American
Psychiatric Association, 2000). One feature of impulsivity is disturbed response
inhibition, i.e. the ability to suppress prepotent responses. This has been demonstrated

Three antisaccade studies – Study III
- 54 -
in many experiments using different tasks like the Continuous Performance Test (CPT;
Losier, McGrath, & Klein, 1996) or a modified version of the Stop-Signal Task (Paul-
Jordanov, et al., 2010; Paul, et al., 2007; Willcutt, et al., 2005). One further possibility to
investigate response inhibition is the antisaccade task (Everling & Fischer, 1998). While
in the prosaccade condition subjects are required to direct their gaze at an appearing
stimulus as quickly as they can, they are asked to look at the mirror position of the
stimulus in the antisaccade condition. The generation of correct antisaccades involves at
least two processes: (i) the suppression of the reflexive saccade towards the stimulus
and (ii) the generation of the intentional antisaccade. The repression of the reflexive
saccade can be considered as impulse control or response inhibition. Thus, errors during
the antisaccade condition are an indicator for impulsivity.
Several studies investigating antisaccades elicited by visual stimuli in participants
with ADHD showed an elevated number of direction errors compared to control
participants (Goto, et al., 2010; Karatekin, 2006; Klein, et al., 2003; Loe, et al., 2009;
Mahone, et al., 2009; Mostofsky, Lasker, Cutting, et al., 2001; Mostofsky, Lasker, Singer,
et al., 2001; Munoz, et al., 2003; O'Driscoll, et al., 2005).
To the best of our knowledge, until now only one study from our group has
investigated antisaccades triggered by acoustic cues (Goepel, Kissler, Rockstroh, &
Paul-Jordanov, 2011). It was demonstrated that more cortical activation in the medial
frontal and anterior temporal areas is needed in children with ADHD to perform on the
same behavioural level as control children when antisaccades are elicited by acoustic
cues. Yet, impulse control in response to acoustic stimuli is behaviourally highly relevant.
An example might be a pupil in class listening to the teacher, while other sounds are
present (the neighbour whispering, noises from outside, etc.). In order to pay attention to
the teacher it is important to not respond to competing acoustic sounds.
The need for more research into cross-modality of symptoms in ADHD becomes
apparent when considering the diagnosis central auditory processing disorder ((C)APD).
APD is considered as a central disorder, i.e. children have difficulties with hearing and
psychoacoustic tasks despite the peripheral hearing system being fully functional
(American Speech-Language-Hearing Association, 2005; British Society of Audiology
Steering Group, 2007). However, there is much dispute about the nature of APD in the
literature. It has been suggested that ADHD and APD are the same disorder, the label
simply defined by the person who diagnoses the child (psychiatrist vs. audiologist), or
whether they are different disorders overlapping in phenotype (Cacace & McFarland,
2005b). The attempts to differentiate APD children with and without ADHD using electro-
physiological measures have not been successful (Ptok, et al., 2004). Both groups had

Three antisaccade studies – Study III
- 55 -
comparable late acoustic potentials. One difficulty is that multi-modal testing is necessary
to differentiate between ADHD and APD. It is assumed that children with APD show poor
performance only on acoustic tasks, while children with ADHD show poor performance
on auditory and visual attention tasks (Dawes & Bishop, 2009; Jerger & Musiek, 2000).
However, only few studies on APD have focused on more than one modality. For
example, Starzacher (2006) demonstrated in 20 children with APD and 31 control
children, that patients performed poorer than control children on all subtests of the
continuous performance attention test, i.e. on subtests involving the auditory and visual
modality. Another experiment using a visual and auditory CPT showed in 68 children with
suspected APD that a greater proportion of children had problems in both modalities than
with auditory or visual attention alone. Additionally, the authors suggested that 30% of
the children had normal auditory attention and a diagnosis of APD, whereas 8% had poor
auditory attention but no APD diagnosis (Sharma, et al., 2009). These findings
demonstrate that the strict definition that deficits of children with APD are restricted to the
auditory modality does not hold true.
Regarding ADHD, Jonkam and colleagues (1997b) showed that children with
ADHD indeed had higher error rates and amplitude-reduced event-related potentials
during a CPT compared to control children in both modality conditions (visual and
auditory). Further, Breier and colleagues (2003) used a task assessing the perception of
auditory temporal and nontemporal cues. Participants were children with (a) reading
disability (RD), (b) ADHD, (c) RD with ADHD and (d) control children. The presence of
ADHD was associated with a general reduction of performance across all
psychoacoustic tasks. Another study showed that children with ADHD have difficulties
with frequency discrimination (FD), but not with the detection of frequency modulation
(FM) (Sutcliffe, et al., 2006). The latter result is particularly interesting, as it shows that
poor performance on psychoacoustic tasks is not necessarily the result of inattention,
otherwise it should have affected both, performance on the FD and the FM task. These
results demonstrate that children with ADHD have difficulties with psychoacoustic tasks
that might be independent of an attention deficit.
In order to differentiate between ADHD and APD, a multi-modal approach is
nevertheless the only option. It is important to understand, whether typical ADHD
symptoms are restricted to one modality in order to be able to compare children with
ADHD and APD. We followed this idea and aimed at investigating response inhibition in
ADHD using an antisaccade task, where saccades were either triggered by visual or
acoustic cues. Previous studies (Rommelse, et al., 2008) suggest that children with
ADHD make more antisaccade errors when visual cues are used. Barely results exist

Three antisaccade studies – Study III
- 56 -
regarding acoustic cues. Thus the present study lays the ground for further comparison
of children with ADHD and children with APD.
2.3.3 Methods
Participants
16 children with ADHD and 16 healthy control children participated in the
experiment (see results section for demographic information). One child per group was
excluded from analysis of the visual experiment due to a high artefact level in the EEG
data. For the acoustic experiment two children per group were excluded. Control children
were recruited at a local school and did not have any clinically relevant diagnoses or took
any medication as reported by the parents. Children with ADHD were recruited at two
child psychiatric outpatient clinics, diagnoses being made by the head psychiatrist and
his/her team of psychologists based on questionnaires, anamnestic interviews and
psychometric tests. None of the children with ADHD took any kind of medication.
Procedure
The families were shown the laboratory equipment and the task was explained to
them. Children and parents then signed informed consent forms (according to the
Helsinki declaration (WMA, 2004)). Parents were asked to fill in a standardised ADHD
symptom checklist, a standardised conduct disorder symptom checklist (Diagnose-
Checkliste Aufmerksamkeitsdefizit-/ Hyperaktivitätsstörungen (DCL-ADHS), Diagnose-
Checkliste Störung des Sozialverhaltens (DCL-SSV); Döpfner, et al., 2008) and an
auditory processing disorder checklist (DGPP, 2002). Children completed the Edinburgh-
Handedness-Inventory (Oldfield, 1971) and their non-verbal intelligence was measured
by the Coloured Progressive Matrices (CPM; Raven, et al., 2002). To ensure within-
normal hearing levels children’s hearing thresholds were determined for frequencies 500,
1000, 2000 and 4000Hz in an acoustically shielded room. Children were then shown a
computerised, animated explanation of the task, which included examples and 16
training trials. For additional motivation, children were told that they would be able to
collect eight “cartoon mice” on the computer screen if they performed well (although the
mice always appeared after fixed intervals) which would then allow the children to pick a
small gift from a “treasure chest” after the experiment. Thus, it was ensured that all
children were motivated and perceived themselves as successful. Children were
additionally compensated with 20 Euros at the end of the experimental session.
For the EEG experiment, children were comfortably seated on a chair, their heads
resting on a chin rest 500mm away from the computer monitor. The 30min-experiment
Three antisaccade studies – Study III
- 57 -
(with a flexible break in the half of the session) was started after ensuring that
impedances were below 30kOhm.
After the experiment children rated the difficulty and their perceived success.
Groups found the experiment equally difficult (visual experiment: Z(27)=0.655, p=.513,
acoustic experiment: t(25)=.629, p=.535) and perceived themselves as equally
successful (visual experiment: Z(27)=0.655, p=.513, acoustic experiment: Z(25)=.946,
p=.344). Children with and without ADHD described the task as easy (visual experiment
mean: 32.07 ±22.46, acoustic experiment mean: 30.37 ±21.07, “0” representing very
easy, “100” representing very difficult) and assumed that they had made mistakes in
27.59 ±18.01% and 28.81 ±19.44% of trials, respectively.
Task
Four blocks with 60 trials each were presented in randomised order for each
experiment (visual, acoustic). Two blocks involved prosaccades, the other two blocks
involved antisaccades. Thus, a trial could either cue an anti- or a prosaccade, directed to
the left or the right of the screen. It was counter-balanced, whether a child started with
the visual or acoustic experiment. In the visual experiment, the cue was a cartoon owl; in
the acoustic experiment, the cue was the sound of an owl-call. For prosaccade trials
participants were asked to look towards the cue as quickly as possible, while they were
asked to look at the mirror-location of the cue for antisaccade trials. Each block started
with an instruction slide (anti- or prosaccade) of variable length as children were asked to
repeat the instruction to make sure they had understood the task. Each trial began with a
1300ms fixation time with a black fixation cross in the middle of a blue screen and two
black owl silhouettes to the left and right of the fixation cross (±30°). Then the cross
disappeared and after a 200ms gap period the cue (the visual cue filled one of the owl
silhouettes; the acoustic cue was played on one of the loudspeakers ±39° in front of the
participant) was presented for 1000ms. Subsequently, the fixation cross appeared again
for 500ms. After each block children were shown a picture of a clock for 5sec, which
graphically depicted how many blocks they had already finished (the clock was filled
subsequently). This was followed by a motivation picture (5sec) with 1 to 8 already
collected cartoon mice. A pause-signal appeared after 120 trials indicating that children
could take a short break. The length of the break was determined by the children.
Before the actual experiment, a calibration block was run, in which the children
were requested to look towards a visual cue left, right, above and below the fixation
cross. These calibration saccades were later used to build template eye-movements for
EEG data analysis.

Three antisaccade studies – Study III
- 58 -
Equipment and Oculomotor Recordings
Cues were presented with the software Presentation (Neurobehavioral Systems,
Inc.). The visual cue (picture of an owl) had been painted by hand and was (25 x 25mm).
The fixation cross was generated within Presentation and was (10 x 12mm).
Presentation was run on a PC (Dell precision 390 with Intel® Core™ 2CPU 2.13Hz-
Prozessor with 2GB Ram operating system) and the stimuli were presented on a monitor
with 27.5” (1920x1200 pixels) resolution (HANNS. G HG 281 DJ). The acoustic cue (owl
call) was downloaded from an open internet database (http://www.findsounds.com) and
modified with Adobe Audition 2.0® in order to last 1000ms. The sound was presented at
67dB through external loudspeakers (Creative Inspire 280 2.0) placed at an angle of 39°
before the participant.
EEG-recordings were made with a high-density 257-channel system from EGI
Electrical Geodesics Inc. using NetStaionTM12 (run on a Mac OSX with 1.25GHz
PowerPC G4 processor and 1GB DDR SD RQM). The sampling rate was 250Hz using
an online filter of 100Hz lowpass and 0.1Hz highpass.
Data and statistical analysis
Questionnaire values (Handedness in %, positive values indicating right-
handedness; CPM raw values with a maximum of 36; DCL-ADHS and DCL-SSV
questionnaire in stanine values; APD questionnaire in raw values ranging from 1 to 4,
where 1 represents “few problems” and 4 represents “many problems”) were compared
between groups using Statistica (StatSoft, Inc., 2003). T-tests, Mann-Whitney-U tests or
Chi2-Test were chosen after testing for normal distribution with the Kolmogorov Smirnov
Test (Lillifors adaption).
EEG data were analysed with the software package BESA (Brain Electrical
Analysis, version 5.3.4, MEGIS Software GmbH, Gräfelfing, Germany). Bad channels
were identified and interpolated for each individual EEG data set. For the identification of
eye movements, data were notch filtered at 50Hz, low-pass filtered at 8Hz (12dB/octave
zerophase) and high-pass filtered at 0.5Hz (6dB/octave forward). Data were manually
scored for saccade onset (saccadic reaction time, SRT) and correctness. Epochs
containing saccades with latencies <80ms or eye movements in the 100ms time window
before stimulus onset were discarded. Eye movement artefacts (blinks and saccades)
were then systematically removed using an algorithm implemented in BESA (Berg &
Scherg, 1994; Lins, et al., 1993).
Saccadic correctness and SRTs were statistically probed using analyses of
variance (ANOVAs), T-tests, Mann-Whitney-U tests or sign tests after testing for normal

Three antisaccade studies – Study III
- 59 -
distribution with the Kolmogorov Smirnov Test (Lillifors adaption) using Statistica. Post-
hoc testing of significant interactions was done using the Tukey test. Age was introduced
as a covariate in the ANOVA when the correlation between age and the dependant
variable (Bravais Pearson correlation test or Spearman Rank test) became significant.
In order to investigate inhibition skills in children with and without ADHD
response-locked averages of correct saccades (-500 until 900ms after response;
baseline -500 to -400ms) were generated for each condition with all filters turned off
except the notch filter. Averaged epochs were then filtered between 1Hz (6dB/octave
forward) and 30Hz (24dB/octave zerophase). In order to reduce the number of statistical
tests, data were resampled to 83.3Hz using Matlab (Version 7.5.0.342 (R2007b)). In
order to objectively identify time-windows of interest, non-parametric cluster-based
analyses of EEG sensor data were performed using FieldTrip, an open-source signal
processing toolbox for Matlab (Donders Institute for Brain, Cognition and Behaviour,
Radboud University Nijmegen, The Netherlands. http://www.ru.nl/neuroimaging/fieldtrip).
As response inhibition takes place before the onset of a saccade and in accord with
already existing findings (Clementz, et al., 2001; McDowell, et al., 2005), data analysis
was carried out for the time-windows -156ms until -24ms before response. In order to
objectively determine time-windows, during which brain activity of ADHD and control
children would differ, the difference waveforms anti- minus prosaccades waveforms were
compared between groups using independent t-tests. Cluster α was set at 0.1.
Additionally anti- and prosaccades were compared via dependant t-tests (cluster α=0.05)
within groups. In order to prevent chance-findings, data were re-shuffled 1000 times
using a cluster-based Monte-Carlo randomization. This method effectively controls for
multiple comparisons (Maris & Oostenveld, 2007). Clusters were defined as significant
when the probability of observing larger effects in the shuffled data was below 5%.
Significant interactions (i.e. in this case significant group difference of anti- minus
prosaccades equals an interaction group (ADHD, Control) x condition (anti-,
prosaccades)) were further probed with a post-hoc test, comparing mean amplitudes of
pro- and antisaccades within groups and individual conditions (anti-, prosaccades)
between groups for statistically significant electrode clusters. Additionally grand averages
of anti- minus prosaccade difference waveforms, as well as grand averages of individual
conditions (anti-, prosaccades) were computed per group. In time-windows of statistical
significance, the underlying brain activity of the grand average difference waveforms
(ADHD (anti- minus prosaccade) minus Control (anti- minus prosaccade)) was modelled
using CLARA (realistic head-model approximation for ages 10-12 years). The result of
the CLARA image only reveals brain regions that differ in activation between two groups.

Three antisaccade studies – Study III
- 60 -
They do not allow the interpretation of the direction of the effect, i.e. which condition
(anti- or prosaccades) led to more activity. Thus, source montages (regional dipoles)
were generated based on the CLARA results. These source montages were then applied
to the individual conditions (e.g. anti- minus prosaccades, antisaccades or prosaccades
within control children and children with ADHD) and the mean magnitude in the time-
windows of interest was extracted.
2.3.4 Results
Sample characteristics
Groups did not differ in age, gender distribution, handedness or intelligence
scores (table 4). Children with and without ADHD had hearing levels of 20dB or better in
each ear for all measured frequencies.
Table 4: Demographic characteristics ADHD (n=16) Control (n=16) test t/Z/χ2 FG p
Age [in month] 129.38 ±22.47 122.63 ±20.71 t-test 0.884 30 0.384 Gender (male : female) 14:2 13:3 Chi 0.240 1 0.626 Handedness [in %] 93.75 ±8.06 65 ±60.22 MWU 1.300 30 0.194 CPM [raw scores] 30.88 ±3.16 32.19 ±3.37 MWU -1.489 30 0.137
Children with ADHD had higher values than control children for all three subscales
of the ADHD questionnaire. Further, groups differed on the subscale oppositional
aggressive behaviour of the conduct disorder questionnaire (table 5).

Three antisaccade studies – Study III
- 61 -
Table 5: Parental ratings of ADHD/APD symptoms ADHD Control
Symptoms Subscale n n test Z FG p Inattention 15 7.33 ±0.98 16 4.56 ±1.67 MWU 4.091 29 0.000 Hyperactivity 15 7.20 ±1.21 16 4.06 ±2.93 MWU 3.320 29 0.001 ADHD Impulsivity 15 7.27 ±2.02 16 4.44 ±2.94 MWU 2.965 29 0.003 Oppositional aggressive behaviour 15 7.27 ±1.75 16 5.13 ±2.45 MWU 2.510 29 0.012
Conduct Disorder Dissocial
aggressive behaviour 15 6.53 ±2.45 16 5.06 ±2.62 MWU 1.957 29 0.050
Speech Perception 16 1.51 ±0.67 16 1.21 ±0.26 MWU 1.432 30 0.152 Auditory Discrimination 16 1.30 ±0.64 16 1.16 ±0.2 MWU 0.094 30 0.925 Sound Localisation 16 1.06 ±0.38 16 1.04 ±0.08 MWU 0.528 30 0.598 Hearing in background noise
16 1.71 ±0.77 16 1.22 ±0.2 MWU 2.506 30 0.012
Auditory Memory 16 1.70 ±0.74 16 1.29 ±0.3 MWU 2.205 30 0.027
APD
Auditory Hypersensitivity 16 2.40 ±0.87 15 2.34 ±0.82 MWU 0.217 29 0.828
Visual experiment
Correctness of saccades
As age and saccade correctness were correlated (table 6), age [in months] was
used as continuous predictor in the ANOVA. Besides the main effects group (more
correct saccades in control children than in children with ADHD: F(1,27)=19.159, p<.001)
and condition (more correct saccades in the pro- than in the antisaccade condition:
F(27)=29.761, p<.001) the interaction condition x group was significant (F(1,27)=6.542,
p<.05). Children with ADHD made fewer correct antisaccades than control children
(p<.01), while groups did not differ regarding prosaccades. Within groups more correct
prosaccades were generated than antisaccades (ADHD: p<.001; Controls: p<.001, table
7).
Table 6: Correlation of correct reactions [in %] with age [in months] in the visual experiment Age [in month] correlation with r(X.Y) p All Antisaccades 0.681 0.000 Prosaccades 0.586 0.001 ADHD Antisaccades 0.700 0.004 Prosaccades 0.518 0.048 Control Antisaccades 0.891 0.000 Prosaccades 0.570 0.026
Table 7: Mean ± standard deviation [in %] of correct saccades in the visual experiment All children (n=30) ADHD (n=15) Control (n=15)
All 82.61 ±9.20 79.36 ±8.02 85.87 ±9.39 Antisaccades 72.55 ±14.61 67.42 ±12.70 77.68 ±14.99 Prosaccades 93.67 ±5.71 92.56 ±5.27 94.78 ±6.08

Three antisaccade studies – Study III
- 62 -
Latency
Latency of antisaccades also correlated with age (table 8). Therefore, age was
used as continuous predictor in the ANOVA.
Table 8: Correlation of latency [in ms] with age [in months] in the visual experiment Age [in month] correlation with r(X.Y) p All Antisaccades -0.482 0.007 Prosaccades -0.118 0.534 ADHD Antisaccades -0.531 0.042 Prosaccades 0.152 0.590 Control Antisaccades -0.687 0.005 Prosaccades -0.067 0.813
The main effect group (F(1,27)=6.182 p<.05) revealed that saccade onset was
later in children with ADHD than in control children. The main effect condition was found
(F(1,27)=44.877, p<.001). Antisaccade onset was later than prosaccade onset. The
interaction condition x group did not reach significance (table 9).
Table 9: Mean ± standard deviation [in ms] of correct saccades in the visual experiment
All children (n=30) ADHD (n=15) Control (n=15)
All Antisaccades
268.64 ±59.67 335.22 ±90.32
289.8 ±71.17 362.63 ±110.88
247.49 ±36.73 307.8 ±54.70
Prosaccades 202.07 ±44.12 216.97 ±52.37 187.17 ±28.55
Brain activity
Group-comparison of the difference waveform anti- minus prosaccades revealed
a negative cluster of 76 electrodes (t(14)=-763.029, p<.05) and a positive cluster of 88
electrodes (t(14)=881.185, p<.05, table 10 and figure 10). Here, a negative cluster
represents a more negative difference anti- minus prosaccades in children with ADHD,
while a positive cluster represents a more positive difference anti- minus prosaccades in
the ADHD compared to the control group.
Table 10 : Mean amplitudes and standard deviations [in µV] in the time window -156 to -24ms before response onset in the visual experiment
Antisaccade Prosaccade Mean SD Mean SD
ADHD -2.00 0.60 -0.46 0.72 Negative Cluster Control -1.54 0.65 -1.51 0.88 ADHD 2.22 0.66 0.51 0.84 Positive Cluster Control 1.19 0.74 1.46 1.01
Post hoc mean amplitudes were compared between and within groups. This
comparison revealed that control children had higher negative amplitudes in the

Three antisaccade studies – Study III
- 63 -
prosaccade condition than children with ADHD (t(28)=3.091, p<.01). Groups did not differ
for the positive cluster after bonferroni correction. Additionally, higher activity in the
antisaccade than in the prosaccade condition in both clusters (negative cluster:
Z(15)=3.098, p<.01, positive cluster: Z(15)=3.615, p<.001) within the ADHD group was
found (table 11). Source reconstruction of the difference ADHD minus Control revealed
activity of the sources described in table 12 and displayed in figure 10.
Table 11: Post-hoc results of the interaction group x condition in the visual experiment Negative Cluster
Group Condition test t/Z FG p ADHD vs. Control Antisaccades MWU -0.809 28 0.419 ADHD vs. Control Prosaccades t-test 3.091 28 0.004 ADHD Anti- vs. Prosaccades Sign test 3.098 15 0.002 Control Anti- vs. Prosaccades t-test -0.078 14 0.939
Positive Cluster ADHD vs. Control Antisaccades MWU 0.809 28 0.419 ADHD vs. Control Prosaccades t-test -2.132 28 0.042 ADHD Anti- vs. Prosaccades Sign test 3.615 15 0.000 Control Anti- vs. Prosaccades t-test -0.395 14 0.699
Note: Bold p-values are significant after Bonferroni correction.
Table 12: Sources underlying the difference (ADHD (anti- minus prosaccades) minus control group (anti- minus prosaccades)) in the visual experiment
Talairach
coordinates Mean Amplitude
[in nAm]
x y z Val
[in nAm/cm3] % ADHD Control ADHD vs. Control
Right anterior cingulate cortex 3.5 46.1 2.7 2.3400 100 13.25 16.56 Right insula 31.5 11.1 -4.3 2.0000 85.6 11.39 24.22 Left inferior frontal lobe -24.5 18.1 2.7 0.8628 36.9 4.72 17.31 Right cerebellum anterior lobe 3.5 -58.9 -25.3 0.8620 36.8 21.12 10.72 Right parietal lobe 17.5 -44.9 37.7 0.2465 10.5 15.02 11.69

Three antisaccade studies – Study III
- 64 -
Figure 10: Children with ADHD (anti- minus prosaccades) vs. control children (anti- minus prosaccades) during the visual experiment: from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude of the significant electrode cluster for anti- (dashed line) and prosaccades (continuous line) and for children with ADHD (red) and control children (black), (3) sources of the anti- minus prosaccade group-difference: (a) right anterior cingulate cortex, (b) right insula, (c) left inferior frontal lobe, (d) right cerebellum anterior lobe, (e) right parietal lobe
In the time window -156 to -24ms before response onset a negative cluster
(higher negative amplitudes during anti- than prosaccades) of 104 electrodes (t(14)=-
3035.000, p<.001) and a positive cluster (higher positive amplitudes during anti- than
prosaccades) of 92 electrodes (t(14)=2689.800, p<.001, table 13 and figure 11) were
found in the group of children with ADHD. For control children, a negative cluster of 60
electrodes was also found (t(14)=-637.806, p<.01, table 13 and figure 12), while no
positive cluster reached significance. Source reconstruction of the difference anti- minus
prosaccades within groups revealed activity of the sources described in table 14 and
displayed in figure 11 and 12.
Table 13: Mean amplitudes and standard deviations [in µV] in the time window -156 to -24ms before response onset in the visual experiment
Antisaccade Prosaccade Mean SD Mean SD
ADHD Negative Cluster -1.97 0.59 -0.48 0.73 Positive Cluster 2.29 0.67 0.57 0.85
Control Negative Cluster -1.78 0.84 -1.26 0.72

Three antisaccade studies – Study III
- 65 -
Table 14: Sources underlying the difference antisaccades minus prosaccades in the visual experiment
Talairach
coordinates Mean Amplitude
[in nAm]
X y z Val
[in nAm/cm3] % Antisaccades Prosaccades ADHD
Right medial frontal gyrus 3.5 46.1 9.7 1.1500 100 7.23 8.87 Left cerebellum posterior lobe -10.5 -58.9 -32.3 0.7491 65.1 15.55 10.33 Left paracentral lobule -3.5 -23.9 44.7 0.4668 40.6 25.84 11.20 Right medial temporal lobe 31.5 -2.9 -11.3 0.2597 22.6 6.64 5.65
Control Right insula 31.5 11.1 -4.3 1.9500 100.0 32.58 12.87 Left insula -31.5 11.1 -4.3 0.7118 36.5 30.75 16.89 Right cerebellum posterior lobe 24.5 -58.9 -32.3 0.6944 35.6 20.01 17.04 Right anterior cingulate cortex 3.5 46.1 2.7 0.5616 28.8 16.87 4.91 Right cuneus 3.5 -72.9 16.7 0.2429 12.4 17.92 17.93
Figure 11: Children with ADHD during the visual experiment; from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude for significant electrode clusters for anti- (dashed line) and prosaccades (continuous line) (3) sources of the anti- minus prosaccade difference: (a) right medial frontal gyrus, (b) left cerebellum posterior lobe, (c) left paracentral lobule, (d) right medial temporal lobe
Figure 12: Control children during the visual experiment; from left to right: (1) topoplot: negative cluster, (2) mean amplitude for significant electrodes for anti- (dashed line) and prosaccades (continuous line), (3) sources of the anti- minus prosaccade subtraction: (a) right insula, (b) left insula, (c) right cerebellum posterior lobe, (d) right anterior cingulate cortex, (e) right cuneus
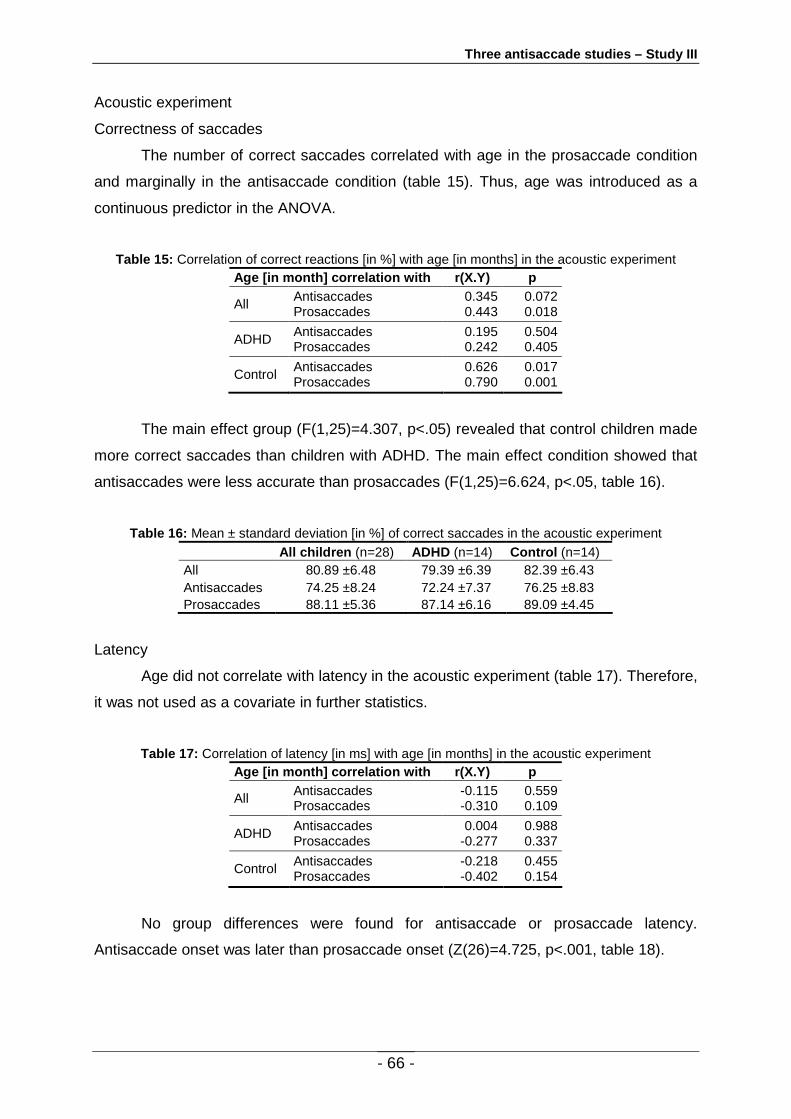
Three antisaccade studies – Study III
- 66 -
Acoustic experiment
Correctness of saccades
The number of correct saccades correlated with age in the prosaccade condition
and marginally in the antisaccade condition (table 15). Thus, age was introduced as a
continuous predictor in the ANOVA.
Table 15: Correlation of correct reactions [in %] with age [in months] in the acoustic experiment Age [in month] correlation with r(X.Y) p
All Antisaccades Prosaccades
0.345 0.443
0.072 0.018
ADHD Antisaccades Prosaccades
0.195 0.242
0.504 0.405
Control Antisaccades Prosaccades
0.626 0.790
0.017 0.001
The main effect group (F(1,25)=4.307, p<.05) revealed that control children made
more correct saccades than children with ADHD. The main effect condition showed that
antisaccades were less accurate than prosaccades (F(1,25)=6.624, p<.05, table 16).
Table 16: Mean ± standard deviation [in %] of correct saccades in the acoustic experiment
All children (n=28) ADHD (n=14) Control (n=14) All 80.89 ±6.48 79.39 ±6.39 82.39 ±6.43 Antisaccades 74.25 ±8.24 72.24 ±7.37 76.25 ±8.83 Prosaccades 88.11 ±5.36 87.14 ±6.16 89.09 ±4.45
Latency
Age did not correlate with latency in the acoustic experiment (table 17). Therefore,
it was not used as a covariate in further statistics.
Table 17: Correlation of latency [in ms] with age [in months] in the acoustic experiment Age [in month] correlation with r(X.Y) p
All Antisaccades Prosaccades
-0.115 -0.310
0.559 0.109
ADHD Antisaccades Prosaccades
0.004 -0.277
0.988 0.337
Control Antisaccades Prosaccades
-0.218 -0.402
0.455 0.154
No group differences were found for antisaccade or prosaccade latency.
Antisaccade onset was later than prosaccade onset (Z(26)=4.725, p<.001, table 18).

Three antisaccade studies – Study III
- 67 -
Table 18: Values represent mean ± standard deviation [in ms] of correct saccade latencies
All children (n=28) ADHD (n=14) Control (n=14) All 369.42 ±137.45 358.17 ±83.73 380.66 ±178.76 Antisaccades 427.20 ±170.10 412.66 ±108.84 441.74 ±218.61 Prosaccades 311.63 ±111.78 303.68 ±65.98 319.57 ±146.50
Brain activity
In the acoustic experiment the group comparison of the difference waveform anti-
minus prosaccades did not result in any significant clusters (figure 13).
Figure 13: Topoplot (t-Values) difference antisaccades minus prosaccades per group elicited by acoustic stimuli – no interaction was found in the time window -156 to -24ms before response onset
In the time window -156 to -24ms before response onset a marginally significant
negative cluster (higher negative amplitudes for anti- than prosaccades, t(13)=-544.286,
p=.064) of 57 electrodes and a significant positive cluster (higher positive amplitudes for
anti- than prosaccades, t(13)=953.064, p<.05, table 19) of 68 electrodes were found in
the group of children with ADHD. Source reconstruction of the difference anti- minus
prosaccades revealed the sources listed in table 20 and displayed in figure 14. In the
control group no significant clusters were found.
Table 19: Mean amplitudes and standard deviations for the positive and negative cluster within the group of children with ADHD in the acoustic experiment
Antisaccade Prosaccade Mean SD Mean SD Negative Cluster -2.44 0.89 -1.18 0.88 Positive Cluster 2.22 0.90 1.05 0.71

Three antisaccade studies – Study III
- 68 -
Table 20 : Sources underlying the difference antisaccades minus prosaccades within the group of children with ADHD in the acoustic experiment
Talairach
coordinates Mean Amplitude
[in nAm]
x y z Val
[in Am/cm3x10-3] % Antisaccades Prosaccades ADHD Right cerebellum posterior lobe 24.5 -58.9 -32.3 0.4505 100 15.76 21.19 Left precuneus -3.5 -44.9 44.7 0.4412 97.9 31.20 17.37 Left medial temporal lobe -31.5 -2.9 -4.3 0.2943 65.3 11.97 7.19 Right medial temporal lobe 31.5 -16.9 -11.3 0.2549 56.6 22.93 28.21 Right medial frontal gyrus 10.5 46.1 16.7 0.2413 53.6 5.42 6.46
Figure 14: Children with ADHD during the acoustic experiment; from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude for significant electrode clusters for anti- (dashed line) and prosaccades (continuous line) (3) sources of the anti- minus prosaccade difference: (a) right cerebellum posterior lobe, (b) left precuneus, (c) left medial temporal lobe, (d) right medial temporal lobe and (e) right medial frontal gyrus
2.3.5 Discussion
The present study aimed at investigating, whether response inhibition in children
with ADHD is equally disturbed when it is triggered by visual and acoustic cues. Another
goal was to uncover brain activity underlying differences in performance between
children with and without ADHD. Results of the present study suggest that children with
ADHD are more impaired when response inhibition is cued by visual stimuli than after
acoustic stimuli on the behavioural level. Likewise, groups only differed in brain activity
after visual stimuli. This shall be discussed in more detail in the following.
Behavioural data
Behavioural data of the visual experiment are in line with previous findings on
antisaccade tasks comparing children with and without ADHD (Karatekin, 2007;
Rommelse, et al., 2008). More errors were made during the anti- than the prosaccade
condition, indicating that more errors were made, when reflexive behaviour was to be

Three antisaccade studies – Study III
- 69 -
inhibited and a volitional antipodal response needed to be generated. This was true for
the control group and for children with ADHD. The interaction group x condition revealed
that children with ADHD made fewer correct antisaccades than control children (Goto, et
al., 2010; Karatekin, 2006; Klein, et al., 2003; Loe, et al., 2009; Mahone, et al., 2009;
Munoz, et al., 2003; O'Driscoll, et al., 2005), whereas no group differences were found
during the prosaccade condition (e.g. O'Driscoll, et al., 2005). This shows that children
with ADHD have more difficulties with response inhibition than control children (Willcutt,
et al., 2005). No group differences in performance were found in a previous antisaccade
study of our group (Goepel, et al., 2011). However, the main difference was that trials
were not presented block-wise as in the present study, but randomly. I.e. with every trial,
children did not know whether to expect a prosaccade or an antisaccade and whether it
would be triggered by a visual or an acoustic cue. Task difficulty in a random
presentation design is thus much higher. This might be the reason, why group
differences were not found in the previous study. They might have been obscured by a
ceiling effect.
Antisaccade latencies were longer than prosaccade latencies. This also reflects
the greater difficulty of the antisaccade task and the fact that more processes are
involved and more actions need to be executed in the antisaccade condition compared to
the control condition (Everling & Fischer, 1998; Forbes & Klein, 1996; Ford, et al., 2005;
Klein, et al., 2003; Munoz, et al., 1998). Further, children with ADHD had longer latencies
than control children. A comparable finding was reported by Munoz and colleagues
(2003) and Klein and colleagues (2003) and has been interpreted as an indicator that
children with ADHD have difficulty in saccade initiation (Rommelse, et al., 2008).
However, no group differences in saccade latency have also been found (O'Driscoll, et
al., 2005; Rothlind, et al., 1991). One reason for this discrepancy might be that latencies
of children with ADHD are more variable and less consistent, which can lead to group
effects in one or the other direction.
During the acoustic experiment both groups made more errors on antisaccade
trials than on prosaccade trials. This demonstrates that acoustic cues – like visual cues –
have a “grasping” effect. As in the visual experiment, children made more errors when
they were asked to inhibit their automatic reaction to look towards the cue. Children with
ADHD made more errors than control children across conditions. However, no group x
condition interaction was found. It thus appears that although children with ADHD have
more difficulties with the acoustic task than control children, they do not specifically have
greater difficulties with behavioural inhibition. In line with the results on visually triggered
saccades, latencies of antisaccades were longer than after prosaccades. No group

Three antisaccade studies – Study III
- 70 -
effects were found. The higher error rate in children with ADHD on acoustic trials might
be a consequence of their deficit in auditory processing (Riccio & Hynd, 1996). Data of
the APD questionnaire indeed revealed lower scores in children with ADHD for auditory
memory and hearing in background noise.
In conclusion, behavioural results of the visual experiment in the present study
show that children with ADHD are less able than control children to suppress
inappropriate responses and need a longer time to initiate their saccades. When
saccades are cued by acoustic stimuli, children with ADHD make more errors than
control children, but are not specifically more impaired regarding behavioural inhibition.
EEG data
EEG data after visual cues
Groups differed in brain activation of the difference correct anti- minus
prosaccades after visual stimulation. This is equal to an interaction group x condition.
The group difference occurred between -156 and -24ms before saccade onset. This
overlaps with the time-range usually connected to response inhibition (Clementz, et al.,
2001; McDowell, et al., 2005). Post-hoc testing revealed that the interaction on the
sensor level mainly stemmed from activation differences in the prosaccade condition.
Here, control children had higher amplitudes in the prosaccade condition than children
with ADHD, effectively making the difference anti- minus prosaccades smaller in the
control group than in the ADHD group. Accordingly amplitudes of anti- and prosaccades
differed significantly in children with ADHD for both sensor clusters, while no differences
were found for control children. As only correct saccades were analysed, this means that
brain activation in children with ADHD was higher for correct anti- than correct
prosaccades, while brain activation did not differ for control children. Taking into account
that control children performed better than children with ADHD, i.e. they made less
antisaccade/inhibition errors, the EEG sensor space results imply that children with
ADHD needed a clearer distinction between anti- and prosaccades in terms of brain
activation, i.e. higher activation for anti- than prosaccades in order to perform correct
saccades. In control children, smaller activation differences, which did not lead to
statistically significant differences between conditions, seem to have been sufficient. In
other words, children with ADHD had greater activation for response inhibition than
control children for the correct execution of saccades. This could be interpreted as a
compensatory mechanism in children with ADHD. In control children, the neural network
underlying response inhibition seems to be more efficient, thus resulting in less
activation.

Three antisaccade studies – Study III
- 71 -
Looking at the source reconstruction of the interaction ((ADHD: anti-pro) minus
(Control: anti-pro)) revealed that five brain regions were involved. The anterior cingulate
cortex (ACC) was most active followed by the insula, the inferior frontal lobe, the
cerebellum and the parietal lobe. Functional Magnetic Resonance Imaging (fMRI) studies
have shown that the ACC is involved in antisaccade tasks (Brown, et al., 2006;
Gaymard, Ploner, et al., 1998; Pierrot-Deseilligny, et al., 2005; Polli, et al., 2005). Activity
in the ACC was higher before correct than before incorrect antisaccades, whereas higher
activity for incorrect antisaccades than prosaccades was found during the response
period. Therefore, the ACC was interpreted to be involved in the signalling of an error
and error monitoring during the antisaccade task (Ford, et al., 2005). The ACC has also
been found to be the relevant structure in studies investigating response inhibition with a
Go/Nogo task (Bokura, et al., 2001), a modified stop-paradigm (Paul-Jordanov, et al.,
2010; Paul, et al., 2007), and a continuous performance task (Fallgatter, et al., 2004).
Thus, the ACC seems to be robustly activated when response inhibition is involved.
Along with the ACC Lerner and colleagues (2009) found the insula to be active in a study
on blinking suppression. The authors concluded that both structures mediate the control
and suppression of physiological urges and play a role in behavioural inhibition. In a
meta-analysis of studies on response inhibition, Dickstein and colleagues (2006) also
revealed the inferior frontal lobe to be active in various studies on response inhibition and
reduced activation in this structure was found in children with ADHD (Rubia, et al., 2005).
Further, it has been shown that patients with inferior frontal lesions have specific deficits
with response inhibition and working memory (Aron, Fletcher, Bullmore, Sahakian, &
Robbins, 2003; Clark, et al., 2007). The cerebellum is classically linked to motor fine-
tuning and timing of motor actions (Ivry, Spencer, Zelaznik, & Diedrichsen, 2002). In the
context of saccades it seems to be important for steering and stopping saccades, thus
determining their accuracy (Jenkinson & Miall, 2010). The relative volume of the vermis
was related to saccadic accuracy in humans. Larger volumes were associated with
greater accuracy during a prosaccade task (Ettinger, et al., 2002). The cerebellum is also
increasingly becoming of interest in ADHD research (Schneider, Retz, Coogan, Thome,
& Rosler, 2006) because of its connection to the frontal lobe. In mice it was shown that
the cerebellum can influence the dopamine outflow in the frontal cortex (Mittleman,
Goldowitz, Heck, & Blaha, 2008). The parietal lobe also has connections to frontal motor
regions (Kulubekova & McDowell, 2008) and is more active during voluntary than
reflexives saccades (Dyckman, et al., 2007; Ettinger, et al., 2008; Ford, et al., 2005;
Kulubekova & McDowell, 2008). Thus, the parietal lobe also seems to be involved in the
voluntary control of actions.

Three antisaccade studies – Study III
- 72 -
Looking at activation differences between groups in these structures, it appears
that control children had more activity in the ACC, in the insula and in the inferior frontal
lobe. These structures seem to be responsible for better inhibition performance in control
children. This finding also goes in line with the hypothesis that children with ADHD have
a frontal hypoactivation (Dickstein, et al., 2006). In contrast, children with ADHD had
higher activity in the cerebellum and in the parietal lobe. This could again reflect a
compensatory mechanism. The absolute values should not be interpreted, as the source
models were computed on grand average waveforms across the children within each
group. Still, they give an idea of how the activity pattern differs between groups. It should
be noted at this point that the source structure as described above underlies the
interaction on sensor level. Thus, although on sensor level only children with ADHD had
higher activation for anti- than prosaccades, and although the group-difference was only
significant for prosaccades, the underlying activity pattern leading to this interaction on
sensor level suggests stronger activation during inhibition in frontal regions in control
children, while children with ADHD show stronger activation in the cerebellum and the
parietal cortex.
Looking for inhibition within group (without the requisite that groups need to differ)
revealed two sensor cluster with higher activity for anti- than prosaccades in the ADHD
group and one sensor cluster in the control group. Source reconstruction of this effect
within the ADHD group revealed four active sources. The medial frontal gyrus was most
active, followed by the posterior lobe of the cerebellum, the paracentral lobule and the
medial temporal lobe. In control children, also four structures were involved. Bilateral
insulae were most active, followed by the posterior lobe of the cerebellum, the ACC and
the cuneus. The medial frontal gyrus was more active during prosaccades than during
antisaccades in children with ADHD. The ACC is in close proximity to the medial frontal
gyrus and was clearly more active during antisaccades than during prosaccades in
control children. This is in line with the notion that the ACC is strongly involved in
successful response inhibition in control children. The frontal lobe in general (more
specifically the dorsolateral prefrontal cortex (DLPFC), the frontal eye fields (FEF) and
the supplementary eye fields (SEF)) is involved in the control of voluntary saccades. The
DLPFC is involved in the inhibition of prosaccades and the generation and of
antisaccades, memory-guided saccades and in decision processes (Pierrot-Deseilligny,
et al., 2004). Several lesion studies showed that error percentage in the antisaccade task
is increased after DLPFC lesion (Pierrot-Deseilligny, et al., 2003; Pierrot-Deseilligny, et
al., 1991; Ploner, et al., 2005). Further, it was shown that children with ADHD have
reduced brain activation in the right inferior prefrontal cortex reaching deep into the

Three antisaccade studies – Study III
- 73 -
insula during successful motor response inhibition compared to control subjects (Rubia,
et al., 2005). Thus, the fact that activation in the medial frontal cortex was bigger during
pro- than antisaccades in children with ADHD is in line with the notion of a hypoactivation
in structures relevant for inhibition (Rubia, et al., 1999).
Both groups had higher activation during anti- than prosaccades in the
cerebellum. Analogue to the source reconstruction of the group interaction, children with
ADHD had a slightly larger activation in the cerebellum than control children. This might
be part of a compensatory mechanism to increase saccadic accuracy. Only children with
ADHD had greater activation in the paracentral lobule during anti- than during
prosaccades. The paracentral lobule includes the medial part of the superior frontal
gyrus. The posterior part is part of the parietal lobe, whereas the anterior section is part
of the frontal lobe and is often described as the supplementary motor area. Successful
antisaccades are linked to activity in the pre-supplementary motor area (Fitzgerald, et al.,
2008). Tamm and colleagues (2004) also revealed activation in the supplementary motor
area in a Go/Nogo task in children with ADHD. The authors concluded that this is
probably related to motor planning and response execution. Similarly, in the meta-
analysis of neuroimaging studies on response inhibition it was demonstrated that in
children with ADHD the paracentral lobule was active (Dickstein, et al., 2006). As this
area was not activated in control children and as only correct saccades were analysed,
one might assume that the present activation pattern in children with ADHD reflects a
compensatory mechanism to overcome difficulties in response inhibition.
According to the source reconstruction of the group interaction, the insula was
found to be more active during anti- than prosaccades only in control children. As
mentioned above, the insula has been shown to be active in a study on blinking
suppression in control children (Lerner, et al., 2009) and also in the meta analysis on
response inhibition (Dickstein, et al., 2006). Thus, in control children, the insula seems to
be part of a cortical network responsible for response inhibition. In contrast, children with
ADHD had higher activation in the right medial temporal lobe during anti- than
prosaccades. As the right temporal lobe has been linked to spatial memory (Nunn,
Graydon, Polkey, & Morris, 1999), it is conceivable that the antisaccade task places a
higher demand on spatial memory in children with ADHD. This might compensating for
the lack of activity in the frontal inhibition system.
The cuneus was also activated in control children. However, its activation was
nearly equal for anti- and prosaccades. Thus, it is unlikely that it plays a relevant role for
response inhibition.

Three antisaccade studies – Study III
- 74 -
EEG data after acoustic cues
No group effects were found in brain activation after acoustic cues. This is in line
with behavioural findings, where control children and children with ADHD also did not
differ in response inhibition performance. Neither were there any significant brain
activation differences between anti- and prosaccades within the control group. It might
have been the case that the task was easier for control children. This is supported by
lower error rates compared to children with ADHD. Consequently, it might have been the
case that activation of structures involved in saccade generation and response inhibition
were not activated as strongly by antisaccades as in the visual experiment.
Consequently, the comparison of EEG data during anti- and prosaccades did not reach
statistical significance. Within the ADHD group, two electrode clusters with higher
amplitudes for anti- than prosaccades were found. Source reconstruction of this effect
revealed four underlying brain-regions: the cerebellum was most active, followed by the
precuneus, the medial temporal lobe and the medial frontal gyrus. Similar to the visual
experiment higher activity in pro- compared to antisaccades was found in the medial
frontal gyrus. Therefore the theory of frontal hypoactivity during inhibition may extend to
auditory modality, as well. Also comparable to the visual experiment was the finding of
higher activity during anti- than prosaccades in the precuneus, which borders with the
paracentral lobule. This activation pattern in the parietal cortex in children with ADHD
might compensate for the frontal under-activation. However, the direction of the effect in
the other structures was reversed compared to the visual experiment, although the
structures themselves were the same. In the acoustic experiment, activity in the
cerebellum was higher during pro- than antisaccades. In the visual experiment it was
higher during anti- than prosaccades. The same was true for the right medial temporal
lobe.
Taken together, the cerebellum and the right medial temporal lobe do not seem to
be part of a compensatory inhibition network when acoustic stimuli trigger saccades as
seen in the visual experiment. It is more likely that task demand is different when
saccades are triggered by acoustic cues compared to visual cues. Latencies of saccades
were approximately 100ms longer when saccades were triggered by acoustic cues. This
was true for both, anti- and prosaccades. Thus, it appears that the task was more
demanding when acoustic cues were used resulting in a longer reaction time to initiate
pro- and antisaccades. This is conceivable, as for the correct execution of saccades the
position of the acoustic cue, which is believed to be represented in a craniotopic, i.e.
head-related reference system needs to be re-mapped to a retinotopic reference system
before the generation of acoustically triggered saccades (Jay & Sparks, 1990;

Three antisaccade studies – Study III
- 75 -
Zambarbieri, et al., 1982). Given that also the execution of prosaccades is more difficult
when cues are acoustic, this could explain, why in the same structures that were more
active during antisaccades in the visual experiment were more active during
prosaccades in the acoustic experiment. Interestingly, the left medial temporal lobe was
more active during anti- than prosaccades. In the study of Tamm and colleagues (2004)
children with ADHD had higher activity in Nogo than in Go stimuli in the left
middle/inferior temporal gyrus. The authors suggested that this may reflect the adoption
of verbally mediated strategies to rehearse or hold the instruction in mind to enhance
task performance. Thus, this could again reflect a compensatory mechanism in children
with ADHD to enhance inhibition performance by internal rehearsal rather than the
activation of a control-like inhibition network. Thus it appears that the medial temporal
lobes fulfil different purposes in the context of visually and acoustically triggered
saccades.
In summary, interpreting the behavioural results together with the source-
reconstruction results implies that children with ADHD have a deficit in response
inhibition when it is cued by visual cues. This is accompanied by frontal hypoactivation
and activation of a compensatory posterior-cerebellar network. Children with ADHD do
not seem to have an inhibition deficit when acoustic cues are used. However, the
underlying source structure of response inhibition in ADHD suggests that the same
structures are involved when acoustic and visual cues are used, while the functionality of
the structures is not always the same. The present study was the first to investigate
response inhibition in a cross-modal block-design. Although children with ADHD do seem
to have greater difficulties generating saccades when acoustic cues are used, they do
not have an inhibition deficit. Children with ADHD only had difficulties with response
inhibition after visual cues. This supports the idea that deficient response inhibition is not
a cross-modal phenomenon.
General discussion
- 76 -
III. General discussion
Inhibition is an evolutionary-biological principle to prevent situations inadequate
reactions, in order to activate operation relevant responses, which is linked to structural
and functional brain maturation. Patients with ADHD often are conspicuous due to
inappropriate behaviour. Their impulsivity – one of the three core deficits – is manifested
as difficulty in delaying responses, blurting out answers, having difficulties to wait,
interrupting others or grabbing objects from others (American Psychiatric Association,
2000).
Inhibition control is measured with SST, CPT and other Go/Nogo paradigms and
the majority of functional image studies identified reduced activation in frontal regions,
ACC and striatum in children with ADHD compared to control participants (Cherkasova &
Hechtman, 2009). This hypo-frontality was found in fMRI studies applying prior Go/Nogo
tasks (e.g. Booth, et al., 2005; Durston, et al., 2003; Rubia, et al., 1999; Smith, Taylor,
Brammer, Toone, & Rubia, 2006; Tamm, et al., 2004). The typical Go/Nogo task makes
use of visual stimuli and disregards acoustic cues and their everyday life relevance.
Thus, aim of the thesis was to delineate possible brain areas – involved in
inhibition control of reactions to visual and acoustic suddenly arising stimuli – revealing
altered activity patterns in children with ADHD and, thus, to answer the question whether
children with ADHD are handicapped in suppression of reflexive responds to acoustic
cues in order to advance the basics for a differential diagnostic. As a measuring
instrument the antisaccade task was chosen because the task as well as the underlying
brain activity are well investigated.
Bringing together the results of these saccade studies presented here indicate
that the degree to which children with ADHD are impaired in inhibition control depends
on the complexity of the task. This was varied by the amount of stimulus x response
compatibility (one versus two modalities) and the kind of design (blocked versus
random). In doing so, the integration of two modalities alleviated whereas the random
design increased the task demand. Judging the complexity by the mean error rate of
both groups (as far as possible) – on the behavioural level, children with ADHD showed
inhibition impairment only at the second least complexity experiment, i.e. during the
blocked visual experiment (Study III). On the physiological level group differences were
apparent in the previously mentioned condition and at the second highest extensive
condition, i.e. during the randomly presented acoustic experiment (Study II). Thus, it is
assumed that in the two other conditions (visual random and acoustic blocked condition)
floor and ceiling effects caused the missing incidence of group differences: one condition

General discussion
- 77 -
was too difficult and the other too easy. This and further consideration shall be discussed
in more detail below.
To make sure that the severity of the mono modality condition (visual condition) is
comparable to the cross-modality condition (acoustic condition), the eye tracker Study I
(a pilot study) tested the experiment with a control group of children comparing pro- and
antisaccade performance elicited by visual and acoustic stimuli, something that has
never been done before. The results showed that the saccade performances are
comparable: in both conditions the typical anti-/prosaccade pattern emerged (increased
error rate in anti- compared to prosaccades). Additionally, the correlations between the
two conditions within the error rate and within latency have strengthened the similarity.
Based on these findings it was assumed that both modality conditions measured
inhibition control and the comparability of both conditions could be embraced.
Furthermore, important differences between both conditions were found: primary,
acoustically cued saccades had elongated SRTs compared with visually triggered
saccades, which could have been caused by the remapping from the craniotopic, i.e.
head-related reference system to the retinotopic reference system (Yao & Peck, 1997).
In the visual condition, a gap effect (i.e. shorter reaction time in the gap than the overlap
condition) and longer reaction times in anti- compared to prosaccades were found but
not so in the acoustic condition, whereas an eccentricity effect (i.e. faster saccades to
more laterally presented cues) was only presented in the acoustic experiment. That is,
the influence of different task conditions on the behavioural performance depended on
the cue modality.
The interaction condition x modality was marginally significant and showed that
the anti-/prosaccade difference was smaller pronounced in the acoustic than in the visual
condition due to more pro- and fewer antisaccade errors during acoustically rather than
during visually elicited responses. The advantage in the acoustic antisaccade condition
compared with the visually triggered antisaccades was explained by a relative benefit
from the remapping process, reducing the immediate inhibitory demand on the system
for children, whose executive system is not completely developed yet. It seems that
acoustically elicited saccades were less prone to be influenced by impulsivity. This
interpretation was deduced from the same behavioural pattern, which Schooler and
colleagues (2008) found in adult schizophrenia patients during a blocked antisaccade
task.
As a second step, Study II was carried out – the comparison of children with and
without ADHD. The measuring instrument of Study I (eye tracker) was replaced by an

General discussion
- 78 -
EEG because neural activity shows a higher sensitivity than pure behavioural data. Due
to the interest in inhibition control in particular, only the antisaccade performance was
analyzed. It was hypothesized that children with ADHD – described to have difficulties in
acoustic tasks (Riccio & Hynd, 1996) – have, compared to control subjects, a higher
error rate not only in the visual but also in the acoustic antisaccade experiment. Study II,
however, revealed a completely different pattern: although children with ADHD
generated slightly fewer correct antisaccades than control subjects in the acoustic
condition, no significant differences were found between the children groups in the
antisaccade task performance. The high difficulty of the task might be an explanation for
this – the demand of the task was too high for both groups. On the physiological level,
children with ADHD generated a higher brain activity in the MFC between -230 and -
120ms and in the left-hemispheric TAC between -112 and 0ms before saccade onset
(time windows in which inhibition processes were found; McDowell, et al., 2005) during
the acoustic condition. I.e. because of the slightly higher error rate in children with ADHD
during the acoustic antisaccade task it was assumed that this task is more difficult for
them compared to the control children. Therefore, group differences in the brain activity
were not surprising in the task that seems to have differential demands for the children
groups.
This increased activity on the physiological level has to be explained. Based on
functional studies, Johnston and Everling (2008) assumed that the preparation for an
antisaccade leads to a suppression of preparatory and stimulus-related activities in the
FEF and SC. Top-down signals required for this could be elicited in the DLPFC, the ACC
or the SEF, whereas the ACC is recruited when task demands increase (Johnston,
Levin, Koval, & Everling, 2007). Due to the random experimental design, in which
supplementary task switching between pro- and antisaccades is needed (O'Driscoll, et
al., 2005), the task is very demanding. Thus, it was assumed that both, control subjects
and children with ADHD, had the ability to suppress the activity in FEF and SC. However,
in children with ADHD this suppression required a higher activity of the ACC – mapped in
higher activity of the MFC compared to control children. The ACC – involved in
antisaccade tasks (Brown, et al., 2006; Gaymard, Ploner, et al., 1998; Pierrot-
Deseilligny, et al., 2005; Polli, et al., 2005) – seems to be responsible for error monitoring
and signalling (higher activity before correct than incorrect antisaccades; Ford, et al.,
2005). Supposed the task was more difficult for children with than without ADHD, the
higher activity in the MFC is necessary to generate correct demanding cross-modal
antisaccades. Similarly the higher activity in the left TAC was interpreted as a
compensatory mechanism in children with ADHD, suggesting the possibility of an internal

General discussion
- 79 -
rehearsal of the instruction mechanism (Tamm, et al., 2004), although the underlying
mechanisms are not fully understood.
Summing it up to this point – children with ADHD presented the same behavioural
inhibition pattern in a random task design as control subjects but in the acoustic condition
it seemed only possible because of a higher fronto-temporal activity – interpretable as a
compensatory mechanism.
Based on the results of Study II, it was assumed that the random design was very
difficult for both children groups. Therefore, for Study III a new paradigm which should
differentiate adequately between the groups was created in a – compared to the random
paradigm easier – block design. This design change was motivated by former studies
with blocked designs, which revealed group differences in visual inhibition tasks (e.g.
Klein, et al., 2003; Munoz, et al., 2003). Additionally, the conditions were diminished – no
overlap condition and no different eccentricity conditions were inserted – to include more
trials per condition, given that error rates are the key measure of inhibitory skill on this
task and that RTs are confounded with the number of trials on which they are based in
comparisons between groups with widely different accuracy rates (Everling & Fischer,
1998). Finally, in order to make the experiment more attractive for children, stimuli were
changed to owl calls and cartoons. The visual experiment results of Study III next to the
condition main effects in error rate and latency (more correct saccades and longer
latencies in the pro- than in the antisaccade condition) revealed that children with ADHD
made fewer correct antisaccades than control children and showed elongated latency in
pro- as well as antisaccades – a result that confirms the inhibition deficit in children with
ADHD and replicates results of former studies (Rommelse, et al., 2008).
Looking at the source reconstruction, several brain areas were active during a
time window between -156 and -24ms before response onset, in which inhibition
processes take place. The group x condition interaction showed higher activation
differences (anti- minus prosaccades) for control children in the ACC, the insula and the
inferior frontal lobe, whereas smaller activity was found in the cerebellum anterior lobe
and the parietal lobe. Thus, it seems that children with ADHD exhibited a frontal
hypoactivation but were able to reach a correct saccade reaction with the support of a
compensatory posterior-cerebellar network. This assumption was enhanced by findings
in the within-group comparisons: here, children with ADHD showed less medial frontal
activations and a higher activation in the cerebellum, the parietal and temporal lobe in
the anti- compared to the prosaccade condition, whereas in control children higher

General discussion
- 80 -
frontal-cerebellar activation in the anti- than in the prosaccade condition was found,
strengthening the assumption of frontal inhibition mechanism.
In the acoustic experiment next to the simplification through the block design the
remapping process provided additional time resulting in no differences between children
groups. Children with ADHD did not seem to benefit from this additional time, because it
was revealed that children with ADHD made more errors than control children in both
conditions – interpreted as a consequence of their deficit in auditory processing (Riccio,
et al., 1996), although both children groups were constricted by higher error rates and
elongates latencies in the anti- compared to the prosaccade condition. In other words,
both groups showed inhibition deficits but the expected enhanced handicap in children
with ADHD during antisaccades was lacking, rather a general deficit in both conditions
was apparent. Thus, it seemed that the task was easier for children in the control group.
In line with the behavioural results on source level no group x condition interaction
was found and also no condition effect within the control group. Because of the easiness
of the task it might have been the case that activation of structures involved in volitional
saccade generation and response inhibition were not activated as strongly by
antisaccades as in the visual experiment. Children with ADHD, however, showed higher
activation in the medial frontal gyrus during pro- compared to antisaccade, extending the
theory of frontal hypoactivity to the auditory modality. Higher and therefore compensatory
activity was found in the precuneus and left medial temporal lobe during anti- compared
to prosaccades. Not expected was the antisaccade related higher activity in the right
cerebellum and the right temporal lobe because of an opposite pattern in the visual
experiment.
Summing it up to this point – children with ADHD presented in the visual
experiment compared to control children an inhibition deficit which was accompanied by
frontal hypoactivation and activation of a compensatory posterior-cerebellar network. In
contrast when cues were acoustic, children with ADHD did not seem to have an inhibition
deficit whereas the underlying structures resembled the structures of the visual
experiment, while the functionality of the structures was not always the same.
To compare the findings of Study II and III it has to be mentioned that design and
data analyses in both studies were different: both, Study II and III investigated pro- and
antisaccades but first in a random (very difficult) and second in a blocked (more easy)
design, perhaps causing different influences of attention and motivation. The cue
property in Study II was compared to Study III very simplistic (pure sinus tone and yellow

General discussion
- 81 -
dot vs. owl call and owl cartoon) and perhaps responsible for different brain area
activations. Furthermore, the angle of visual and acoustic cue was more comparable in
Study III than in Study II. Study II included gap and overlap conditions, whereas in Study
III only gap conditions were presented. Study II compared both groups in the antisaccade
conditions whereas Study III considered anti- as well as prosaccades; therefore, direct
group comparisons within the different conditions were not considered anymore in order
to accomplish an interaction analysis. Source reconstruction was done in Study II with an
established 23-source-model and in Study III sources were searched with CLARA,
perhaps resulting in different sensitivity dispersions.
In the following section both studies are compared also with regard to implications
for further research – based on the previously described background the analogy of both
findings should be considered carefully.
On the behavioural level it was illustrated that more correct antisaccades could be
generated in the blocked design compared to the random design – confirming the
facilitation by lapse of task switching. A further group differentiation was possible in the
visual antisaccade performance when the task was presented in a blocked manner:
children with ADHD made more errors and were slower during correct antisaccades,
inferring that the visual blocked experiment is the most differentiating condition.
Although it was not analysed, it seems that in Study II the simplification by a less
strong stimulus x response compatibility (acoustic condition) was higher for control
children than for children with ADHD. When comparing the correct response rate per
condition, children with ADHD showed in the visual condition 50.52 ±16.54% and in the
acoustic condition 57.20 ±12.88% correct antisaccades, whereas control children
generated 48.84 ±20.53% visual and 65.38 ±12.32% acoustic correct antisaccades –
replicating the pattern of Study I.
However, considering the behavioural performance in Study III it seems that here
children with ADHD compared to control subjects benefited more from the additional time
(slightly higher correct performance in the acoustic than in the visual condition while
there was no difference in the control group) – which means that results were contrary to
those of Study II. In comparison to the study of Schooler and colleagues (2008) –
mentioning that two blocked studies were matched now – children with ADHD and adult
patients with schizophrenia were similar. This resemblance is eminent because patients
with schizophrenia reveal comparable performance patterns in visual elicited saccades
like patients with ADHD (Hutton & Ettinger, 2006). It seems that the advantage in the
control children group in the acoustic over the visual antisaccade condition – seen in the
random design – was lacking in the blocked design. Perhaps this benefit reverts in

General discussion
- 82 -
adulthood in support of a better performance in the visual condition (Schooler, et al.,
2008).
The comparison between performance in visual, acoustic and also combined
tasks during different designs in further investigations is worthwhile due to accentuating
loss-making and compensatory mechanisms in patient groups: thus, at nearly no time in
life an inhibition is requires on a pure stimulus. A siren for example triggers always a
visual search for an ambulance parallel to the auditory orientation. Combined tasks are
necessary for finding an adequate treatment for children with ADHD to adjust their
performance in the different modalities to that of normally developed children.
However, it seems that in the random design comparable behavioural
performances were generated during the acoustic condition based on fronto-
hyperactivation whereas in the blocked design a fronto-hypoactivity was present in both
modality conditions. Below structures which overlapped in both studies and their
functions are discussed.
The frontal lobe: Study II revealed a frontal hyperactivation in children with ADHD
compared to control subjects differing from previous reports of reduced activation during
Go/Nogo tasks, SSTs, CPTs or Stroop tests (Cherkasova & Hechtman, 2009) and also
from the results of Study III. Although it seems that there is consistence in current ADHD
literature about frontal hypoactivity reflecting a decrease in the intensity of activation in
this region, authors indicated to be cautious in making rapid inferences. For example,
Dickstein and colleagues (2006) pointed out that the altered activity pattern could also
reflect decreases in the spatial extent of activations, more spatial dispersion of
activations, decreases in functional connectivity or more statistical noise. This noise is
perhaps conditional on factors such as more variable responses in or greater motions in
patients. Additionally, it has to be mentioned that some regions show a greater activation
for patients compared to controls as seen in Study III, suggesting that ADHD is not
purely constituted by hypofunction and accentuating compensatory mechanism
(Dickstein, et al., 2006).
Furthermore, some studies conform to results of Study II (Schulz, et al., 2004;
Schulz, et al., 2005; Vaidya, et al., 1998), therefore, indicating that the participants of
Schulz and colleagues (2004; 2005) were older compared to the other studies, which
could have had an influence on the results. In a Go/Nogo task Schulz and colleagues
(2004) investigated adolescents with a history of ADHD with fMRI design and found
compared to control subjects higher frontal activations. Additionally an inverse relation
was found between the anterior cingulate gyrus activity and the performance on the
Go/Nogo task of both groups and between the frontopolar activation and the behavioural

General discussion
- 83 -
performance of the control group: the more difficult in inhibiting the prepotent response
the greater the brain activation. Vaidya and colleagues (1998) assumed that the
inhibition task including selection, online maintenance of stimuli in working memory, and
switching attentional sets (Go and Nogo trials) and therefore the widespread and greater
activation in children with ADHD may reflect greater inhibitory efforts.
While results of Study III are in line with the hypothesis of frontal hypoactivation in
children with ADHD, the findings of Study II are conflictive to the state of inhibition
research (established on Go/Nogo tasks). Therefore, the question arises whether a
comparison between inhibition performances and their underlying brain activity during
Go/Nogo and antisaccade tasks should be allowed. Both tasks involve an inhibition effort
but the antisaccade task requests an additional volitional eye movement. Recent studies
tend to investigate both conflicting responses separately (Brown, et al., 2007; Ettinger, et
al., 2008; Reuter, et al., 2009) but without any consistent findings. Thus, further research
is essential to clarify the nature of both findings of decreased and increased activities
associated with ADHD.
The temporal lobe – as a second overlapping structure – is a region that is
involved in more complex and integrative tasks and develops later (Gogtay, et al., 2004).
Independent of the design in children with ADHD higher activity was found in the left
temporal lobe during acoustically elicited antisaccades. It was assumed that this activity
reflects a kind of compensatory mechanism. This mechanism could be an instruction
holding in mind (Tamm, et al., 2004) i.e. to strengthen the working memory. This is in line
with Barkley’s (1997) theory, hypothesizing that the primary deficit in ADHD is a
behavioural disinhibition, and that deficits in working memory, self-regulation,
reconstitution and internalization of speech are secondary to the behavioural inhibition
deficit. Therefore, both studies strengthen the assumption that in inhibition tasks also the
working memory is involved and should be respected. Children with ADHD seem to
benefit from the temporal activity and further research should consider the temporal lobe
beside the frontostriatal circuitry in investigations of ADHD.
Concluding, advantages and limitations of the present studies with implications of
further research – if not mentioned until now – are presented in the following section.
Study III replicated the well investigated fact that children with ADHD are impaired
in oculomotor inhibition control compared to normal developed children. And at the first
time this differences could be demonstrated on a physiological level during the visual
experiment. To a large extent, physiological inhibition control investigations make use of
fMRI as a method containing significant motion artefacts, resulting in up to 50% of data

General discussion
- 84 -
loss in some cases (Yerys, et al., 2009). Thus, the advantage of the used EEG system in
the present studies is that this method is also applicable in groups of children with
psychiatric disorders, who are often restless. This advantage should be maintained in
further research, also because of the low cost and the related possibility for diagnostic
initiation.
Due to the findings of the pilot study, it was assumed that both modality conditions
are equivalent. This seems not be confirmed. The acoustic experiment has a higher
complexity than the pure visual task. Therefore, children with ADHD showed a higher
error rate in this condition than control children, whereas no group differentiation
between the inhibition and the control task was possible. Additionally, it seems that in all
three studies acoustically elicited saccades were less prone to be influenced by
impulsivity – possibly due to the remapping process. Consequently, the question, which
arises, is whether the present task is the right method for investigating inhibition control
in the auditory modality. Or if the obvious conclusion can be drawn from the present
experiment that children with ADHD are impaired in the visual but not in the cross-modal
inhibition. Higher comparable tasks have to be designed – for example an experiment
including visual and acoustic stimuli with a key press as response. This kind of
experiment would resemble the CAPT, measuring attention. It was shown that children
with ADHD are more impaired in a response inhibition network than in the selective
attention network (Booth, et al., 2005), thus, the considered task could be described as a
helpful completive diagnostic tool to investigate impaired fields of inhibition control
children with ADHD.
The present studies provided insight in the cortical network underlying the
production of antisaccades elicited by acoustic stimuli in children with and without ADHD
for the first time. It was shown that conclusions regarding functional roles of the
prefrontal cortex regions in adults may not be directly applicable to children (Hwang,
Velanova, & Luna, 2010; Tamm, Menon, & Reiss, 2002). Additionally, up to now little is
known about the inhibition control of acoustic cues and also nothing about the
development of this skill over the life time. Therefore, further developmental studies –
comparable to studies investigating visual inhibition development (Luna & Sweeney,
2004) – as well as complementary longitudinal investigations should investigate this
question in control participants in order to develop templates or growth curves to which
children with an atypical development, cognition or behaviour can be compared.
Although disinhibition in children with ADHD may result from discrete dysfunction in
specific brain regions, the possibility of a developmental dysmaturation (Tamm, et al.,

General discussion
- 85 -
2002) or late development of frontal lobe (Gogtay, et al., 2004) as a contributing factor
should not be forgotten.
Due to the small participant number in the present studies, further investigations
should give more priority to the sample size – the bigger the sample the higher the
generalization. Approaches for modifications of the design – only to mention the high
relevant alterations – should be a random fixation time so that the predictability of the
stimulus will be reduced to enhance the complexity of the task minimal in order to
heightening the differentiability in turn. Furthermore, the aspect of correction of
erroneous saccades seems to be important because children with ADHD correct less
than control subjects (Klein, et al., 2003). An analysis of the EEG data of the erroneous
saccades in comparison to the correct reaction is equally important, in order to
understand the underlying brain physiological mechanism in deficits.
Thus, it should not be forgotten that all the major, developmental disorders –
inclusive ADHD – are closely linked to one another (Witton, 2010). It is not important to
find the correct label for the symptoms of a patient but an appropriate description of the
patient’s symptoms to be able to develop the most adapted therapy. The results of the
present thesis show: a multi-professional approach to diagnosis and management is
critically indispensable.

List of tables and figures
- 86 -
LIST OF TABLES AND FIGURES
Tables
Table 1: Correlation of errors with age [in month] ............................................................................- 33 -
Table 2: Results hearing levels ........................................................................................................- 46 -
Table 3: Results parental ratings of ADHD/APD symptoms ............................................................- 47 -
Table 4: Demographic characteristics ..............................................................................................- 60 -
Table 5: Parental ratings of ADHD/APD symptoms .........................................................................- 61 -
Table 6: Correlation of correct reactions [in %] with age [in months] in the visual experiment........- 61 -
Table 7: Mean ± standard deviation [in %] of correct saccades in the visual experiment................- 61 -
Table 8: Correlation of latency [in ms] with age [in months] in the visual experiment......................- 62 -
Table 9: Mean ± standard deviation [in ms] of correct saccades in the visual experiment ..............- 62 -
Table 10: Mean amplitudes and standard deviations [in µV] in the time window -156 to -24ms before response onset in the visual experiment.....................................................................- 62 -
Table 11: Post-hoc results of the interaction group x condition in the visual experiment ................- 63 -
Table 12: Sources underlying the difference (ADHD (anti- minus prosaccades) minus control group (anti- minus prosaccades)) in the visual experiment..................................................- 63 -
Table 13: Mean amplitudes and standard deviations [in µV] in the time window -156 to -24ms before response onset in the visual experiment.....................................................................- 64 -
Table 14: Sources underlying the difference antisaccades minus prosaccades in the visual experiment ........................................................................................................................................- 65 -
Table 15: Correlation of correct reactions [in %] with age [in months] in the acoustic experiment ........................................................................................................................................- 66 -
Table 16: Mean ± standard deviation [in %] of correct saccades in the acoustic experiment .........- 66 -
Table 17: Correlation of latency [in ms] with age [in months] in the acoustic experiment ...............- 66 -
Table 18: Values represent mean ± standard deviation [in ms] of correct saccade latencies .........- 67 -
Table 19: Mean amplitudes and standard deviations for the positive and negative cluster within the group of children with ADHD in the acoustic experiment.................................................- 67 -
Table 20: Sources underlying the difference antisaccades minus prosaccades within the group of children with ADHD in the acoustic experiment .................................................................- 68 -
Figures
Figure 1: The parameters of eye movement ....................................................................................- 11 -
Figure 2: Cortical areas involved in saccade generation and execution. After processing visual information in the visual cortex and after integration of visuo-spatial integration in the PPC, reflexive saccades are triggered by the PEF. In contrast, intentionally saccades are elicited by the FEF. If a saccade is inhibited the DLPFC will play a primary role. Furthermore, the SEF are responsible for the control of motor programming, whereas the CEF inherit a motivational role for areas controlling intentional saccades. ACC: anterior cingulate cortex; CEF: cingulate eye fields; DLPFC: dorsolateral prefrontal cortex; FEF: frontal eye fields; PEF: parietal eye fields; PPC: posterior parietal cortex; SC: superior colliculus; SEF: supplementary eye field Modified to Pierrot-Deseilligny, Milea, & Muri, 2004; Pierrot-Deseilligny, Muri, Nyffeler, & Milea, 2005 .......................................................................................................................................- 19 -
Figure 3: Example trial (visual prosaccade); top: overlap-condition and bottom: gap-condition ...........................................................................................................................................- 31 -

List of tables and figures
- 87 -
Figure 4: a: Interaction modality*type for the dependant variable latency; b: interaction modality*delay for the dependant variable latency; c: interaction modality*distance for the dependant variable latency; d: correlation between latencies in visually and acoustically cued saccades; filed circle: antisaccades, empty circles: prosaccades...........................................- 33 -
Figure 5: a: Interaction modality*type for the dependant variable error rate; b: interaction modality*distance for the dependant variable error rate; c: correlation between errors in visually and acoustically cued saccades ..........................................................................................- 35 -
Figure 6: Temporal structure of an exemplary trial (visual prosaccade); top: overlap-condition and bottom: gap-condition ................................................................................................- 43 -
Figure 7: Sensitivity map of the MFC (top) and the TAC left (bottom) .............................................- 45 -
Figure 8: Group effect for the dependant variable source power of correct antisaccades in the MFC............................................................................................................................................- 48 -
Figure 9: Group effect for the dependant variable source power of correct antisaccades in the TAC left.......................................................................................................................................- 48 -
Figure 10: Children with ADHD (anti- minus prosaccades) vs. control children (anti- minus prosaccades) during the visual experiment: from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude of the significant electrode cluster for anti- (dashed line) and prosaccades (continuous line) and for children with ADHD (red) and control children (black), (3) sources of the anti- minus prosaccade group-difference: (a) right anterior cingulate cortex, (b) right insula, (c) left inferior frontal lobe, (d) right cerebellum anterior lobe, (e) right parietal lobe................................................................................- 64 -
Figure 11: Children with ADHD during the visual experiment; from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude for significant electrode clusters for anti- (dashed line) and prosaccades (continuous line) (3) sources of the anti- minus prosaccade difference: (a) right medial frontal gyrus, (b) left cerebellum posterior lobe, (c) left paracentral lobule, (d) right medial temporal lobe ........................................................- 65 -
Figure 12: Control children during the visual experiment; from left to right: (1) topoplot: negative cluster, (2) mean amplitude for significant electrodes for anti- (dashed line) and prosaccades (continuous line), (3) sources of the anti- minus prosaccade subtraction: (a) right insula, (b) left insula, (c) right cerebellum posterior lobe, (d) right anterior cingulate cortex, (e) right cuneus.....................................................................................................................- 65 -
Figure 13: Topoplot (t-Values) difference antisaccades minus prosaccades per group elicited by acoustic stimuli – no interaction was found in the time window -156 to -24ms before response onset......................................................................................................................- 67 -
Figure 14: Children with ADHD during the acoustic experiment; from left to right: (1) topoplot: top: negative cluster, bottom: positive cluster, (2) mean amplitude for significant electrode clusters for anti- (dashed line) and prosaccades (continuous line) (3) sources of the anti- minus prosaccade difference: (a) right cerebellum posterior lobe, (b) left precuneus, (c) left medial temporal lobe, (d) right medial temporal lobe and (e) right medial frontal gyrus ......................................................................................................................................- 68 -

References
- 88 -
REFERENCES
Abel, L. A., Troost, B. T., & Dell'Osso, L. F. (1983). The effects of age on normal saccadic characteristics and their variability. Vision Res, 23(1), 33-37.
Adler, L. A. (2008). Epidemiology, impairments, and differential diagnosis in adult ADHD: introduction. CNS Spectr, 13(8 Suppl 12), 4-5.
Aman, C. J., Roberts, R. J., Jr., & Pennington, B. F. (1998). A neuropsychological examination of the underlying deficit in attention deficit hyperactivity disorder: frontal lobe versus right parietal lobe theories. Dev Psychol, 34(5), 956-969.
American Psychiatric Association, APA (2000). Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR (Vol. 4). Washington, DC: Author.
American Speech-Language-Hearing Association, ASHA (2005). (Central) Auditory Processing Disorders [Technical Report]. Retrieved from www.asha.org/policy
Angold, A., Costello, E. J., & Erkanli, A. (1999). Comorbidity. J Child Psychol Psychiatry, 40(1), 57-87.
Aron, A. R., Fletcher, P. C., Bullmore, E. T., Sahakian, B. J., & Robbins, T. W. (2003). Stopsignal inhibition disrupted by damage to right inferior frontal gyrus in humans. Nat Neurosci 6, 115-116.
American Speech-Language-Hearing Association, ASHA (1997). Guidelines for Audiologic Screening [Guidelines]. Retrieved from www.asha.org/policy
American Speech-Language-Hearing Association, ASHA (2005). (Central) Auditory Processing Disorders [Technical Report]. Retrieved from www.asha.org/policy
Bamiou, D. E., Musiek, F. E., & Luxon, L. M. (2001). Aetiology and clinical presentations of auditory processing disorders--a review. Arch Dis Child, 85(5), 361-365.
Banaschewski, T., Becker, K., Scherag, S., Franke, B., & Coghill, D. (2010). Molecular genetics of attention-deficit/hyperactivity disorder: an overview. Eur Child Adolesc Psychiatry, 19(3), 237-257.
Barkley, R. A. (1991a). The ecological validity of laboratory and analogue assessment methods of ADHD symptoms. J Abnorm Child Psychol, 19(2), 149-178.
Barkley, R. A. (1991b). Attention-Deficit/Hyperactivity Disorder Attention-Deficit Disoder: A Handbook For Diagnosis And Treatment (Vol. 3, pp. 75 - 143). New York: The Guildford Press.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull, 121(1), 65-94.
Barkley, R. A., Murphy, K. R., Dupaul, G. I., & Bush, T. (2002). Driving in young adults with attention deficit hyperactivity disorder: knowledge, performance, adverse outcomes, and the role of executive functioning. J Int Neuropsychol Soc, 8(5), 655-672.
Barry, R. J., Clarke, A. R., & Johnstone, S. J. (2003). A review of electrophysiology in attention-deficit/hyperactivity disorder: I. Qualitative and quantitative electroencephalography. Clin Neurophysiol, 114(2), 171-183.
Barton, J. J., Greenzang, C., Hefter, R., Edelman, J., & Manoach, D. S. (2006). Switching, plasticity, and prediction in a saccadic task-switch paradigm. Exp Brain Res, 168(1-2), 76-87.
Barton, J. J., Raoof, M., Jameel, O., & Manoach, D. S. (2006). Task-switching with antisaccades versus no-go trials: a comparison of inter-trial effects. Exp Brain Res, 172(1), 114-119.
Bellis, T. J., Billiet, C., & Ross, J. (2008). Hemispheric lateralization of bilaterally presented homologous visual and auditory stimuli in normal adults, normal children, and children with central auditory dysfunction. Brain Cogn, 66(3), 280-289.
Berg, P., & Scherg, M. (1994). A multiple source approach to the correction of eye artifacts. Electroencephalogr Clin Neurophysiol, 90(3), 229-241.
Biederman, J. (2005). Attention-deficit/hyperactivity disorder: a selective overview. Biol Psychiatry, 57(11), 1215-1220.

References
- 89 -
Biederman, J., & Faraone, S. V. (2005). Attention-deficit hyperactivity disorder. Lancet, 366(9481), 237-248.
Biederman, J., Mick, E., & Faraone, S. V. (1998). Normalized functioning in youths with persistent attention-deficit/hyperactivity disorder. J Pediatr, 133(4), 544-551.
Biederman, J., Mick, E., & Faraone, S. V. (2000). Age-dependent decline of symptoms of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry, 157(5), 816-818.
Biederman, J., Monuteaux, M. C., Doyle, A. E., Seidman, L. J., Wilens, T. E., Ferrero, F., et al. (2004). Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. J Consult Clin Psychol, 72(5), 757-766.
Biederman, J., Petty, C. R., Evans, M., Small, J., & Faraone, S. V. (2010). How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Research, 177(3), 299-304.
Bokura, H., Yamaguchi, S., & Kobayashi, S. (2001). Electrophysiological correlates for response inhibition in a Go/NoGo task. Clin Neurophysiol, 112(12), 2224-2232.
Booth, J. R., Burman, D. D., Meyer, J. R., Lei, Z., Trommer, B. L., Davenport, N. D., et al. (2005). Larger deficits in brain networks for response inhibition than for visual selective attention in attention deficit hyperactivity disorder (ADHD). J Child Psychol Psychiatry, 46(1), 94-111.
Breier, J. I., Fletcher, J. M., Foorman, B. R., Klaas, P., & Gray, L. C. (2003). Auditory temporal processing in children with specific reading disability with and without attention deficit/hyperactivity disorder. J Speech Lang Hear Res, 46(1), 31-42.
British Society of Audiology Steering Group, BSA (2007). Auditory Processing Disoder. Retrieved from http://www.thebsa.org.uk/apd/Home.htm#working%20def
Brown, J. W., & Braver, T. S. (2005). Learned predictions of error likelihood in the anterior cingulate cortex. Science, 307(5712), 1118-1121.
Brown, M. R., Goltz, H. C., Vilis, T., Ford, K. A., & Everling, S. (2006). Inhibition and generation of saccades: rapid event-related fMRI of prosaccades, antisaccades, and nogo trials. Neuroimage, 33(2), 644-659.
Brown, M. R., Vilis, T., & Everling, S. (2007). Frontoparietal activation with preparation for antisaccades. J Neurophysiol, 98(3), 1751-1762.
Bush, G., Frazier, J. A., Rauch, S. L., Seidman, L. J., Whalen, P. J., Jenike, M. A., et al. (1999). Anterior cingulate cortex dysfunction in attention-deficit/hyperactivity disorder revealed by fMRI and the Counting Stroop. Biol Psychiatry, 45(12), 1542-1552.
Bush, G., Valera, E. M., & Seidman, L. J. (2005). Functional neuroimaging of attention-deficit/hyperactivity disorder: a review and suggested future directions. Biol Psychiatry, 57(11), 1273-1284.
Cacace, A. T., & McFarland, D. J. (2005a). The importance of modality specificity in diagnosing central auditory processing disorder. Am J Audiol, 14(2), 112-123.
Cacace, A. T., & McFarland, D. J. (2005b). Delineating Auditory Processing Disorder (APD) and Attention Deficit Hyperactivity Disorder (ADHD): A Conceptual, Theoretical, and Practical Framework. In T. K. Parthasarathy (Ed.), An Introduction to Auditory Processing Disorders in Children (1 ed., pp. 39-61). Mahwah: Lawrence Erlbaum Associates Inc.
Cacace, A. T., & McFarland, D. J. (2006). Delineating Auditory Processing Disorder (APD) and Attention Deficit Hyperactivity Disorder (ADHD): A Conceptual, Theoretical, and Practical Framework. In T. K. Parthasarathy (Ed.), An introduction to auditory processing disorders in children (pp. 39 - 61 ). New Jersey: Lawrence Erlbaum Associates, Inc. .
Carpenter, R. H. (1981). Oculomotor Procrastination. In D. F. Fisher, R. A. Monty & J. W. Senders (Eds.), Eye Movements: Cognition and Visual Perception (pp. 237-246). Hillsdale: Lawrence Erlbaum.
Carpenter, R. H., & McDonald, S. A. (2007). LATER predicts saccade latency distributions in reading. Exp Brain Res, 177(2), 176-183.

References
- 90 -
Casey, B. J., Castellanos, F. X., Giedd, J. N., Marsh, W. L., Hamburger, S. D., Schubert, A. B., et al. (1997). Implication of right frontostriatal circuitry in response inhibition and attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry, 36(3), 374-383.
Castellanos, F. X., Giedd, J. N., Berquin, P. C., Walter, J. M., Sharp, W., Tran, T., et al. (2001). Quantitative brain magnetic resonance imaging in girls with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry, 58(3), 289-295.
Castellanos, F. X., Lee, P. P., Sharp, W., Jeffries, N. O., Greenstein, D. K., Clasen, L. S., et al. (2002). Developmental trajectories of brain volume abnormalities in children and adolescents with attention-deficit/hyperactivity disorder. JAMA, 288(14), 1740-1748.
Cherkasova, M. V., & Hechtman, L. (2009). Neuroimaging in attention-deficit hyperactivity disorder: beyond the frontostriatal circuitry. Can J Psychiatry, 54(10), 651-664.
Chermak, G. D., Hall, J. W., 3rd, & Musiek, F. E. (1999). Differential diagnosis and management of central auditory processing disorder and attention deficit hyperactivity disorder. J Am Acad Audiol, 10(6), 289-303.
Chermak, G. D., Tucker, E., & Seikel, J. A. (2002). Behavioral characteristics of auditory processing disorder and attention-deficit hyperactivity disorder: predominantly inattentive type. J Am Acad Audiol, 13(6), 332-338.
Clark, L., Blackwell, A. D., Aron, A. R., Turner, D. C., Dowson, J., Robbins, T. W., et al. (2007). Association between response inhibition and working memory in adult ADHD: A link to right frontal cortex pathology? Biological Psychiatry, 61(12), 1395-1401.
Clarke, A. R., Barry, R. J., McCarthy, R., Selikowitz, M., Clarke, D. C., & Croft, R. J. (2003). Effects of stimulant medications on children with attention-deficit/hyperactivity disorder and excessive beta activity in their EEG. Clin Neurophysiol, 114(9), 1729-1737.
Clementz, B. A., Brahmbhatt, S. B., McDowell, J. E., Brown, R., & Sweeney, J. A. (2007). When does the brain inform the eyes whether and where to move? An EEG study in humans. Cereb Cortex, 17(11), 2634-2643.
Clementz, B. A., Gao, Y., McDowell, J. E., Moratti, S., Keedy, S. K., & Sweeney, J. A. (2010). Top-down control of visual sensory processing during an ocular motor response inhibition task. Psychophysiology.
Clementz, B. A., McDowell, J. E., & Stewart, S. E. (2001). Timing and magnitude of frontal activity differentiates refixation and anti-saccade performance. Neuroreport, 12(9), 1863-1868.
Colla, M., Ende, G., Alm, B., Deuschle, M., Heuser, I., & Kronenberg, G. (2008). Cognitive MR spectroscopy of anterior cingulate cortex in ADHD: elevated choline signal correlates with slowed hit reaction times. J Psychiatr Res, 42(7), 587-595.
Connolly, J. D., Goodale, M. A., Menon, R. S., & Munoz, D. P. (2002). Human fMRI evidence for the neural correlates of preparatory set. Nat Neurosci, 5(12), 1345-1352.
Cutsuridis, V., Smyrnis, N., Evdokimidis, I., & Perantonis, S. (2007). A neural model of decision-making by the superior colicullus in an antisaccade task. Neural Netw, 20(6), 690-704.
Danckaerts, M., Sonuga-Barke, E. J., Banaschewski, T., Buitelaar, J., Dopfner, M., Hollis, C., et al. (2010). The quality of life of children with attention deficit/hyperactivity disorder: a systematic review. Eur Child Adolesc Psychiatry, 19(2), 83-105.
Dawes, P., & Bishop, D. (2009). Auditory processing disorder in relation to developmental disorders of language, communication and attention: a review and critique. Int J Lang Commun Disord, 44(4), 440-465.
Dawes, P., Bishop, D. V., Sirimanna, T., & Bamiou, D. E. (2008). Profile and aetiology of children diagnosed with auditory processing disorder (APD). Int J Pediatr Otorhinolaryngol, 72(4), 483-489.
DGPP (2002, 19.09.2002). Anamnesebogen zur Erfassung Auditiver Verarbeitungs- und Wahrnehmungsstörungen (AVWS) Retrieved 22.07.2008, 2008, from http://www.dgpp.de/Profi/index_Profi.htm

References
- 91 -
Dickstein, S. G., Bannon, K., Castellanos, F. X., & Milham, M. P. (2006). The neural correlates of attention deficit hyperactivity disorder: an ALE meta-analysis. J Child Psychol Psychiatry, 47(10), 1051-1062.
Dimoska, A., Johnstone, S. J., Barry, R. J., & Clarke, A. R. (2003). Inhibitory motor control in children with attention-deficit/hyperactivity disorder: event-related potentials in the stop-signal paradigm. Biol Psychiatry, 54(12), 1345-1354.
Ding, J., Powell, D., & Jiang, Y. (2009). Dissociable frontal controls during visible and memory-guided eye-tracking of moving targets. Hum Brain Mapp, 30(11), 3541-3552.
Döpfner, M., Görtz-Dorten, A., Lehmkuhl, G., Breuer, D., & Goletz, H. (2008). Diagnostik - System für psychische Störungen nach ICD-10 und DSM-IV für Kinder und Jugendliche - II (DISYPS - II) (1 ed.). Göttingen: Verlag Hans Huber, Hogrefe AG.
Dougherty, D. D., Bonab, A. A., Spencer, T. J., Rauch, S. L., Madras, B. K., & Fischman, A. J. (1999). Dopamine transporter density in patients with attention deficit hyperactivity disorder. Lancet, 354(9196), 2132-2133.
Durston, S., Tottenham, N. T., Thomas, K. M., Davidson, M. C., Eigsti, I. M., Yang, Y., et al. (2003). Differential patterns of striatal activation in young children with and without ADHD. Biol Psychiatry, 53(10), 871-878.
Dyckman, K. A., Camchong, J., Clementz, B. A., & McDowell, J. E. (2007). An effect of context on saccade-related behavior and brain activity. Neuroimage, 36(3), 774-784.
Ethridge, L. E., Brahmbhatt, S., Gao, Y., McDowell, J. E., & Clementz, B. A. (2009). Consider the context: blocked versus interleaved presentation of antisaccade trials. Psychophysiology, 46(5), 1100-1107.
Ettinger, U., Ffytche, D. H., Kumari, V., Kathmann, N., Reuter, B., Zelaya, F., et al. (2008). Decomposing the neural correlates of antisaccade eye movements using event-related FMRI. Cereb Cortex, 18(5), 1148-1159.
Ettinger, U., Kumari, V., Chitnis, X. A., Corr, P. J., Sumich, A. L., Rabe-Hesketh, S., et al. (2002). Relationship between brain structure and saccadic eye movements in healthy humans. Neurosci Lett, 328(3), 225-228.
Evdokimidis, I., Smyrnis, N., Constantinidis, T. S., Stefanis, N. C., Avramopoulos, D., Paximadis, C., et al. (2002). The antisaccade task in a sample of 2,006 young men. I. Normal population characteristics. Exp Brain Res, 147(1), 45-52.
Everling, S., Dorris, M. C., & Munoz, D. P. (1998). Reflex suppression in the anti-saccade task is dependent on prestimulus neural processes. J Neurophysiol, 80(3), 1584-1589.
Everling, S., & Fischer, B. (1998). The antisaccade: a review of basic research and clinical studies. Neuropsychologia, 36(9), 885-899.
Everling, S., & Munoz, D. P. (2000). Neuronal correlates for preparatory set associated with pro-saccades and anti-saccades in the primate frontal eye field. J Neurosci, 20(1), 387-400.
Fallgatter, A. J., Bartsch, A. J., & Herrmann, M. J. (2002). Electrophysiological measurements of anterior cingulate function. J Neural Transm, 109(5-6), 977-988.
Fallgatter, A. J., Ehlis, A. C., Seifert, J., Strik, W. K., Scheuerpflug, P., Zillessen, K. E., et al. (2004). Altered response control and anterior cingulate function in attention-deficit/hyperactivity disorder boys. Clin Neurophysiol, 115(4), 973-981.
Faraone, S. V., Perlis, R. H., Doyle, A. E., Smoller, J. W., Goralnick, J. J., Holmgren, M. A., et al. (2005). Molecular genetics of attention-deficit/hyperactivity disorder. Biol Psychiatry, 57(11), 1313-1323.
Faraone, S. V., Sergeant, J., Gillberg, C., & Biederman, J. (2003). The worldwide prevalence of ADHD: is it an American condition? World Psychiatry, 2(2), 104-113.
Fendrich, R., Hughes, H. C., & Reuter-Lorenz, P. A. (1991). Fixation-point offsets reduce the latency of saccades to acoustic targets. Percept Psychophys, 50(4), 383-387.
Fioravanti, F., Inchingolo, P., Pensiero, S., & Spanio, M. (1995). Saccadic eye movement conjugation in children. Vision Res, 35(23-24), 3217-3228.

References
- 92 -
Fischer, B., Biscaldi, M., & Gezeck, S. (1997). On the development of voluntary and reflexive components in human saccade generation. Brain Res, 754(1-2), 285-297.
Fitzgerald, K. D., Zbrozek, C. D., Welsh, R. C., Britton, J. C., Liberzon, I., & Taylor, S. F. (2008). Pilot study of response inhibition and error processing in the posterior medial prefrontal cortex in healthy youth. J Child Psychol Psychiatry, 49(9), 986-994.
Fletcher, J., & Wolfe, B. (2009). Long-term consequences of childhood ADHD on criminal activities. J Ment Health Policy Econ, 12(3), 119-138.
Flory, K., Molina, B. S., Pelham, W. E., Jr., Gnagy, E., & Smith, B. (2006). Childhood ADHD predicts risky sexual behavior in young adulthood. J Clin Child Adolesc Psychol, 35(4), 571-577.
Forbes, K., & Klein, R. M. (1996). The Magnitude of the Fixation Offset Effect with Endogenously and Exogenously Controlled Saccades. Journal of Cognitive Neuroscience, 8(4), 344-352.
Ford, K. A., Goltz, H. C., Brown, M. R., & Everling, S. (2005). Neural processes associated with antisaccade task performance investigated with event-related FMRI. J Neurophysiol, 94(1), 429-440.
Frens, M. A., & Van Opstal, A. J. (1995). A quantitative study of auditory-evoked saccadic eye movements in two dimensions. Exp Brain Res, 107(1), 103-117.
Friedel, S., Saar, K., Sauer, S., Dempfle, A., Walitza, S., Renner, T., et al. (2007). Association and linkage of allelic variants of the dopamine transporter gene in ADHD. Mol Psychiatry, 12(10), 923-933.
Fukushima, J., Hatta, T., & Fukushima, K. (2000). Development of voluntary control of saccadic eye movements. I. Age-related changes in normal children. Brain Dev, 22(3), 173-180.
Gaymard, B., Ploner, C. J., Rivaud, S., Vermersch, A. I., & Pierrot-Deseilligny, C. (1998). Cortical control of saccades. Exp Brain Res, 123(1-2), 159-163.
Gaymard, B., Rivaud, S., Cassarini, J. F., Dubard, T., Rancurel, G., Agid, Y., et al. (1998). Effects of anterior cingulate cortex lesions on ocular saccades in humans. Exp Brain Res, 120(2), 173-183.
Geffner, D., Lucker, J. R., & Koch, W. (1996). Evaluation of auditory discrimination in children with ADD and without ADD. Child Psychiatry Hum Dev, 26(3), 169-179.
Goepel, J., Kissler, J. M., Rockstroh, B., & Paul-Jordanov, I. (2011). Medio-Frontal and Anterior Temporal abnormalities in children with attention deficit hyperactivity disorder (ADHD) during an acoustic antisaccade task as revealed by electro-cortical source reconstruction. BMC Psychiatry, 11, 7.
Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein, D., Vaituzis, A. C., et al. (2004). Dynamic mapping of human cortical development during childhood through early adulthood. Proc Natl Acad Sci U S A, 101(21), 8174-8179.
Goldring, J. E., Dorris, M. C., Corneil, B. D., Ballantyne, P. A., & Munoz, D. P. (1996). Combined eye-head gaze shifts to visual and auditory targets in humans. Exp Brain Res, 111(1), 68-78.
Goto, Y., Hatakeyama, K., Kitama, T., Sato, Y., Kanemura, H., Aoyagi, K., et al. (2010). Saccade eye movements as a quantitative measure of frontostriatal network in children with ADHD. Brain Dev.
Haarmeier, T. (in press). Sakkadische Augenbewegungen in der neurologischen Diagnostik. Neurophysiol. Lab.
Hale, T. S., Hariri, A. R., & McCracken, J. T. (2000). Attention-deficit/hyperactivity disorder: perspectives from neuroimaging. Ment Retard Dev Disabil Res Rev, 6(3), 214-219.
Hallett, P. E. (1978). Primary and secondary saccades to goals defined by instructions. Vision Res, 18(10), 1279-1296.
Hanisch, C., Radach, R., Holtkamp, K., Herpertz-Dahlmann, B., & Konrad, K. (2006). Oculomotor inhibition in children with and without attention-deficit hyperactivity disorder (ADHD). J Neural Transm, 113(5), 671-684.
Harpin, V. A. (2005). The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child, 90 Suppl 1, i2-7.

References
- 93 -
Hikosaka, O., Takikawa, Y., & Kawagoe, R. (2000). Role of the basal ganglia in the control of purposive saccadic eye movements. Physiol Rev, 80(3), 953-978.
Himelstein, J., Newcorn, J. H., & Halperin, J. M. (2000). The neurobiology of attention-deficit hyperactivity disorder. Front Biosci, 5, D461-478.
Huss, M., Holling, H., Kurth, B. M., & Schlack, R. (2008). How often are German children and adolescents diagnosed with ADHD? Prevalence based on the judgment of health care professionals: results of the German health and examination survey (KiGGS). Eur Child Adolesc Psychiatry, 17 Suppl 1, 52-58.
Hutton, S. B. (2008). Cognitive control of saccadic eye movements. Brain Cogn, 68(3), 327-340.
Hutton, S. B., & Ettinger, U. (2006). The antisaccade task as a research tool in psychopathology: a critical review. Psychophysiology, 43(3), 302-313.
Hwang, K., Velanova, K., & Luna, B. (2010). Strengthening of top-down frontal cognitive control networks underlying the development of inhibitory control: a functional magnetic resonance imaging effective connectivity study. J Neurosci, 30(46), 15535-15545.
Irving, E. L., Steinbach, M. J., Lillakas, L., Babu, R. J., & Hutchings, N. (2006). Horizontal saccade dynamics across the human life span. Invest Ophthalmol Vis Sci, 47(6), 2478-2484.
Irving, E. L., Tajik-Parvinchi, D. J., Lillakas, L., Gonzalez, E. G., & Steinbach, M. J. (2009). Mixed pro and antisaccade performance in children and adults. Brain Res, 1255, 67-74.
Ivry, R. B., Spencer, R. M., Zelaznik, H. N., & Diedrichsen, J. (2002). The cerebellum and event timing. Ann N Y Acad Sci, 978, 302-317.
Jay, M. F., & Sparks, D. L. (1987a). Sensorimotor integration in the primate superior colliculus. I. Motor convergence. J Neurophysiol, 57(1), 22-34.
Jay, M. F., & Sparks, D. L. (1987b). Sensorimotor integration in the primate superior colliculus. II. Coordinates of auditory signals. J Neurophysiol, 57(1), 35-55.
Jay, M. F., & Sparks, D. L. (1990). Localization of auditory and visual targets for the initation of saccadic eye movements. In M. A. Berkley & W. C. Stebbins (Eds.), Comperative perception, Vol. 1: Basic mechanisms (pp. 351-374). New York: John Wiley & Sons.
Jenkinson, N., & Miall, R. (2010). Disruption of Saccadic Adaptation with Repetitive Transcranial Magnetic Stimulation of the Posterior Cerebellum in Humans. The Cerebellum, 1-8.
Jerger, J., & Musiek, F. (2000). Report of the Consensus Conference on the Diagnosis of Auditory Processing Disorders in School-Aged Children. J Am Acad Audiol, 11(9), 467-474.
Johnston, K., & Everling, S. (2008). Neurophysiology and neuroanatomy of reflexive and voluntary saccades in non-human primates. Brain Cogn, 68(3), 271-283.
Johnston, K., Levin, H. M., Koval, M. J., & Everling, S. (2007). Top-down control-signal dynamics in anterior cingulate and prefrontal cortex neurons following task switching. Neuron, 53(3), 453-462.
Johnstone, S. J., & Barry, R. J. (1996). Auditory event-related potentials to a two-tone discrimination paradigm in attention deficit hyperactivity disorder. Psychiatry Res, 64(3), 179-192.
Jonkman, L. M., Kemner, C., Verbaten, M. N., Koelega, H. S., Camfferman, G., vd Gaag, R. J., et al. (1997a). Effects of methylphenidate on event-related potentials and performance of attention-deficit hyperactivity disorder children in auditory and visual selective attention tasks. Biol Psychiatry, 41(6), 690-702.
Jonkman, L. M., Kemner, C., Verbaten, M. N., Koelega, H. S., Camfferman, G., vd Gaag, R. J., et al. (1997b). Event-related potentials and performance of attention-deficit hyperactivity disorder: children and normal controls in auditory and visual selective attention tasks. Biol Psychiatry, 41(5), 595-611.
Jutras, B., Loubert, M., Dupuis, J. L., Marcoux, C., Dumont, V., & Baril, M. (2007). Applicability of central auditory processing disorder models. Am J Audiol, 16(2), 100-106.
Karatekin, C. (2006). Improving antisaccade performance in adolescents with attention-deficit/hyperactivity disorder (ADHD). Exp Brain Res, 174(2), 324-341.

References
- 94 -
Karatekin, C. (2007). Eye tracking studies of normative and atypical development. Developmental Review, 27(3), 283-348.
Karatekin, C., Bingham, C., & White, T. (2009). Oculomotor and Pupillometric Indices of Pro- and Antisaccade Performance in Youth-Onset Psychosis and Attention Deficit/Hyperactivity Disorder. Schizophr Bull.
Keith, R. W., & Engineer, P. (1991). Effects of methylphenidate on the auditory processing abilities of children with attention deficit-hyperactivity disorder. J Learn Disabil, 24(10), 630-636.
Keller, W. D., & Tillery, K. L. (2002). Reliable Differential Diagnosis and Effective Management of Auditory Processing and Attention Deficit Hyperactivity Disorders. Semin Hear, 23(4), 337 - 348.
Keller, W. D., Tillery, K. L., & McFadden, S. L. (2006). Auditory processing disorder in children diagnosed with nonverbal learning disability. Am J Audiol, 15(2), 108-113.
Kemner, C., Jonkman, L. M., Kenemans, J. L., Bocker, K. B., Verbaten, M. N., & Van Engeland, H. (2004). Sources of auditory selective attention and the effects of methylphenidate in children with attention-deficit/hyperactivity disorder. Biol Psychiatry, 55(7), 776-778.
Kemner, C., Verbaten, M. N., Koelega, H. S., Buitelaar, J. K., van der Gaag, R. J., Camfferman, G., et al. (1996). Event-related brain potentials in children with attention-deficit and hyperactivity disorder: effects of stimulus deviancy and task relevance in the visual and auditory modality. Biol Psychiatry, 40(6), 522-534.
Klein, C. (2001). Developmental functions for saccadic eye movement parameters derived from pro- and antisaccade tasks. Exp Brain Res, 139(1), 1-17.
Klein, C., Fischer, B., Hartnegg, K., Heiss, W. H., & Roth, M. (2000). Optomotor and neuropsychological performance in old age. Exp Brain Res, 135(2), 141-154.
Klein, C., & Foerster, F. (2001). Development of prosaccade and antisaccade task performance in participants aged 6 to 26 years. Psychophysiology, 38(2), 179-189.
Klein, C., Foerster, F., Hartnegg, K., & Fischer, B. (2005). Lifespan development of pro- and anti-saccades: multiple regression models for point estimates. Brain Res Dev Brain Res, 160(2), 113-123.
Klein, C., Jr Fischer, B., Fischer, B., & Hartnegg, K. (2002). Effects of methylphenidate on saccadic responses in patients with ADHD. Exp Brain Res, 145(1), 121-125.
Klein, C., Raschke, A., & Brandenbusch, A. (2003). Development of pro- and antisaccades in children with attention-deficit hyperactivity disorder (ADHD) and healthy controls. Psychophysiology, 40(1), 17-28.
Klorman, R., Brumaghim, J. T., Salzman, L. F., Strauss, J., Borgstedt, A. D., McBride, M. C., et al. (1990). Effects of methylphenidate on processing negativities in patients with attention-deficit hyperactivity disorder. Psychophysiology, 27(3), 328-337.
Krause, K. H., Dresel, S. H., Krause, J., la Fougere, C., & Ackenheil, M. (2003). The dopamine transporter and neuroimaging in attention deficit hyperactivity disorder. Neurosci Biobehav Rev, 27(7), 605-613.
Kulubekova, S., & McDowell, J. J. (2008). A computational model of selection by consequences: log survivor plots. Behav Processes, 78(2), 291-296.
Lahat, E., Avital, E., Barr, J., Berkovitch, M., Arlazoroff, A., & Aladjem, M. (1995). BAEP studies in children with attention deficit disorder. Dev Med Child Neurol, 37(2), 119-123.
Lauth, G. W., & Schlottke, P. F. (2002). Training mit aufmerksamkeitsgestörten Kindern. Diagnostik & Therapie. (5 ed.). Weinheim: Beltz, PsychologieVerlagsUnion.
Leigh, R. J., & Zee, D. S. (1999). The saccadic system. In R. J. Leigh & D. S. Zee (Eds.), The neurology of eye movements (pp. 90 - 134). New York: Oxford University Press Inc.
Leigh, R. J., & Zee, D. S. (2006). The Saccadic System. In R. J. Leigh & D. S. Zee (Eds.), The neurology of eye movements (4 ed., pp. 108 - 187). New York: Oxford Universtiy Press, Inc.
References
- 95 -
Lerner, A., Bagic, A., Hanakawa, T., Boudreau, E. A., Pagan, F., Mari, Z., et al. (2009). Involvement of insula and cingulate cortices in control and suppression of natural urges. Cereb Cortex, 19(1), 218-223.
Lins, O. G., Picton, T. W., Berg, P., & Scherg, M. (1993). Ocular artifacts in EEG and event-related potentials. I: Scalp topography. Brain Topogr, 6(1), 51-63.
Liotti, M., Pliszka, S. R., Perez, R., Kothmann, D., & Woldorff, M. G. (2005). Abnormal brain activity related to performance monitoring and error detection in children with ADHD. Cortex, 41(3), 377-388.
Loe, I. M., Feldman, H. M., Yasui, E., & Luna, B. (2009). Oculomotor performance identifies underlying cognitive deficits in attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry, 48(4), 431-440.
Logan, G. D., Cowan, W. B., & Davis, K. A. (1984). On the ability to inhibit simple and choice reaction time responses: a model and a method. J Exp Psychol Hum Percept Perform, 10(2), 276-291.
Losier, B. J., McGrath, P. J., & Klein, R. M. (1996). Error patterns on the continuous performance test in non-medicated and medicated samples of children with and without ADHD: a meta-analytic review. J Child Psychol Psychiatry, 37(8), 971-987.
Lou, H. C., Henriksen, L., & Bruhn, P. (1990). Focal cerebral dysfunction in developmental learning disabilities. Lancet, 335(8680), 8-11.
Lucker, J. R., Geffner, D., & Koch, W. (1996). Perception of loudness in children with ADD and without ADD. Child Psychiatry Hum Dev, 26(3), 181-190.
Luna, B., Garver, K. E., Urban, T. A., Lazar, N. A., & Sweeney, J. A. (2004). Maturation of cognitive processes from late childhood to adulthood. Child Dev, 75(5), 1357-1372.
Luna, B., & Sweeney, J. A. (2004). The emergence of collaborative brain function: FMRI studies of the development of response inhibition. Ann N Y Acad Sci, 1021, 296-309.
Luna, B., Velanova, K., & Geier, C. F. (2008). Development of eye-movement control. Brain Cogn, 68(3), 293-308.
Mahone, E. M., Mostofsky, S. H., Lasker, A. G., Zee, D., & Denckla, M. B. (2009). Oculomotor anomalies in attention-deficit/hyperactivity disorder: evidence for deficits in response preparation and inhibition. J Am Acad Child Adolesc Psychiatry, 48(7), 749-756.
Mahone, E. M., Pillion, J. P., Hoffman, J., Hiemenz, J. R., & Denckla, M. B. (2005). Construct validity of the auditory continuous performance test for preschoolers. Dev Neuropsychol, 27(1), 11-33.
Mannuzza, S., Klein, R. G., Bessler, A., Malloy, P., & LaPadula, M. (1998). Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry, 155(4), 493-498.
Marco, R., Miranda, A., Schlotz, W., Melia, A., Mulligan, A., Muller, U., et al. (2009). Delay and reward choice in ADHD: an experimental test of the role of delay aversion. Neuropsychology, 23(3), 367-380.
Maris, E., & Oostenveld, R. (2007). Nonparametric statistical testing of EEG- and MEG-data. J Neurosci Methods, 164(1), 177-190.
Massen, C. (2004). Parallel programming of exogenous and endogenous components in the antisaccade task. Q J Exp Psychol A, 57(3), 475-498.
Mayes, S. D., Calhoun, S. L., & Crowell, E. W. (2000). Learning disabilities and ADHD: overlapping spectrumn disorders. J Learn Disabil, 33(5), 417-424.
McDowell, J. E., Dyckman, K. A., Austin, B. P., & Clementz, B. A. (2008). Neurophysiology and neuroanatomy of reflexive and volitional saccades: evidence from studies of humans. Brain Cogn, 68(3), 255-270.
McDowell, J. E., Kissler, J. M., Berg, P., Dyckman, K. A., Gao, Y., Rockstroh, B., et al. (2005). Electroencephalography/magnetoencephalography study of cortical activities preceding prosaccades and antisaccades. Neuroreport, 16(7), 663-668.
McFarland, D. J., & Cacace, A. T. (2003). Potential problems in the differential diagnosis of (central) auditory processing disorder (CAPD or APD) and attention-deficit hyperactivity disorder (ADHD). Journal of the American Academy of Audiology, 14(5), 278-280.

References
- 96 -
Meister, H., von Wedel, H., & Walger, M. (2004). Psychometric evaluation of children with suspected auditory processing disorders (APDs) using a parent-answered survey. Int J Audiol, 43(8), 431-437.
Mesulam, M. M. (1998). From sensation to cognition. Brain, 121 ( Pt 6), 1013-1052.
Mittleman, G., Goldowitz, D., Heck, D. H., & Blaha, C. D. (2008). Cerebellar modulation of frontal cortex dopamine efflux in mice: relevance to autism and schizophrenia. Synapse, 62(7), 544-550.
Morgan, A. E., Hynd, G. W., Riccio, C. A., & Hall, J. (1996). Validity of DSM-IV ADHD predominantly inattentive and combined types: relationship to previous DSM diagnoses/subtype differences. J Am Acad Child Adolesc Psychiatry, 35(3), 325-333.
Mostofsky, S. H., Lasker, A. G., Cutting, L. E., Denckla, M. B., & Zee, D. S. (2001). Oculomotor abnormalities in attention deficit hyperactivity disorder: a preliminary study. Neurology, 57(3), 423-430.
Mostofsky, S. H., Lasker, A. G., Singer, H. S., Denckla, M. B., & Zee, D. S. (2001). Oculomotor abnormalities in boys with tourette syndrome with and without ADHD. J Am Acad Child Adolesc Psychiatry, 40(12), 1464-1472.
Muir, D., & Field, J. (1979). Newborn infants orient to sounds. Child Dev, 50(2), 431-436.
Munoz, D. P., Armstrong, I. T., Hampton, K. A., & Moore, K. D. (2003). Altered control of visual fixation and saccadic eye movements in attention-deficit hyperactivity disorder. J Neurophysiol, 90(1), 503-514.
Munoz, D. P., Broughton, J. R., Goldring, J. E., & Armstrong, I. T. (1998). Age-related performance of human subjects on saccadic eye movement tasks. Exp Brain Res, 121(4), 391-400.
Munoz, D. P., & Everling, S. (2004). Look away: the anti-saccade task and the voluntary control of eye movement. Nat Rev Neurosci, 5(3), 218-228.
Muri, R. M., Hess, C. W., & Meienberg, O. (1991). Transcranial stimulation of the human frontal eye field by magnetic pulses. Exp Brain Res, 86(1), 219-223.
Nichols, S. L., & Waschbusch, D. A. (2004). A review of the validity of laboratory cognitive tasks used to assess symptoms of ADHD. Child Psychiatry Hum Dev, 34(4), 297-315.
Nickisch, A., Gross, M., Schonweiler, R., Uttenweiler, V., am Zehnhoff-Dinnesen, A., Berger, R., et al. (2007). [Auditory processing disorders : Consensus statement by the German Society for Phoniatry and Paedaudiology.]. HNO, 55(1), 61-72.
Niedermeyer, E. (2001). Frontal lobe disinhibition, Rett syndrome and attention deficit hyperactivity disorder. Clin Electroencephalogr, 32(1), 20-23.
Nieuwenhuis, S., Broerse, A., Nielen, M. M., & de Jong, R. (2004). A goal activation approach to the study of executive function: an application to antisaccade tasks. Brain Cogn, 56(2), 198-214.
Nigg, J. T. (2001). Is ADHD a disinhibitory disorder? Psychol Bull, 127(5), 571-598.
Nigg, J. T. (2005). Neuropsychologic theory and findings in attention-deficit/hyperactivity disorder: the state of the field and salient challenges for the coming decade. Biol Psychiatry, 57(11), 1424-1435.
Nunn, J. A., Graydon, F. J., Polkey, C. E., & Morris, R. G. (1999). Differential spatial memory impairment after right temporal lobectomy demonstrated using temporal titration. Brain, 122 ( Pt 1), 47-59.
Nyffeler, T., Wurtz, P., Pflugshaupt, T., von Wartburg, R., Luthi, M., Hess, C. W., et al. (2006). One-Hertz transcranial magnetic stimulation over the frontal eye field induces lasting inhibition of saccade triggering. Neuroreport, 17(3), 273-275.
O'Driscoll, G. A., Depatie, L., Holahan, A. L., Savion-Lemieux, T., Barr, R. G., Jolicoeur, C., et al. (2005). Executive functions and methylphenidate response in subtypes of attention-deficit/hyperactivity disorder. Biol Psychiatry, 57(11), 1452-1460.
Oldfield, R. C. (1971). The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia, 9(1), 97-113.
References
- 97 -
Overtoom, C. C., Kenemans, J. L., Verbaten, M. N., Kemner, C., van der Molen, M. W., van Engeland, H., et al. (2002). Inhibition in children with attention-deficit/hyperactivity disorder: a psychophysiological study of the stop task. Biol Psychiatry, 51(8), 668-676.
Paul-Brown, D. (2003). Let's talk Retrieved 25.10.2010, from http://www.asha.org/uploadedFiles/aud/LetsTalkAuditoryProcessing.pdf
Paul-Jordanov, I., Bechtold, M., & Gawrilow, C. (2010). Methylphenidate and if-then plans are comparable in modulating the P300 and increasing response inhibition in children with ADHD. ADHD Attention Deficit and Hyperactivity Disorders.
Paul, I., Gawrilow, C., Zech, F., Gollwitzer, P., Rockstroh, B., Odenthal, G., et al. (2007). If-then planning modulates the P300 in children with attention deficit hyperactivity disorder. Neuroreport, 18(7), 653-657.
Peterson, B. S., Skudlarski, P., Gatenby, J. C., Zhang, H., Anderson, A. W., & Gore, J. C. (1999). An fMRI study of Stroop word-color interference: evidence for cingulate subregions subserving multiple distributed attentional systems. Biol Psychiatry, 45(10), 1237-1258.
Pierrot-Deseilligny, C., Milea, D., & Muri, R. M. (2004). Eye movement control by the cerebral cortex. Curr Opin Neurol, 17(1), 17-25.
Pierrot-Deseilligny, C., Muri, R. M., Nyffeler, T., & Milea, D. (2005). The role of the human dorsolateral prefrontal cortex in ocular motor behavior. Ann N Y Acad Sci, 1039, 239-251.
Pierrot-Deseilligny, C., Muri, R. M., Ploner, C. J., Gaymard, B., Demeret, S., & Rivaud-Pechoux, S. (2003). Decisional role of the dorsolateral prefrontal cortex in ocular motor behaviour. Brain, 126(Pt 6), 1460-1473.
Pierrot-Deseilligny, C., Rivaud, S., Gaymard, B., & Agid, Y. (1991). Cortical control of reflexive visually-guided saccades. Brain, 114 ( Pt 3), 1473-1485.
Pliszka, S. R. (2005). The neuropsychopharmacology of attention-deficit/hyperactivity disorder. Biol Psychiatry, 57(11), 1385-1390.
Pliszka, S. R., Liotti, M., & Woldorff, M. G. (2000). Inhibitory control in children with attention-deficit/hyperactivity disorder: event-related potentials identify the processing component and timing of an impaired right-frontal response-inhibition mechanism. Biol Psychiatry, 48(3), 238-246.
Pliszka, S. R., McCracken, J. T., & Maas, J. W. (1996). Catecholamines in attention-deficit hyperactivity disorder: current perspectives. J Am Acad Child Adolesc Psychiatry, 35(3), 264-272.
Ploner, C. J., Gaymard, B. M., Rivaud-Pechoux, S., & Pierrot-Deseilligny, C. (2005). The prefrontal substrate of reflexive saccade inhibition in humans. Biol Psychiatry, 57(10), 1159-1165.
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry, 164(6), 942-948.
Polli, F. E., Barton, J. J., Cain, M. S., Thakkar, K. N., Rauch, S. L., & Manoach, D. S. (2005). Rostral and dorsal anterior cingulate cortex make dissociable contributions during antisaccade error commission. Proc Natl Acad Sci U S A, 102(43), 15700-15705.
Ptok, M., Blachnik, P., & Schonweiler, R. (2004). [Late auditory potentials (NC-ERP) in children with symptoms of auditory processing and perception disorder. With and without attention deficit disorder]. HNO, 52(1), 67-75.
Ptok, M., Buller, N., Schwemmle, C., Bergmann, C., & Luerssen, K. (2006). [Auditory processing disorder versus attention deficit/hyperactivity disorder. A dysfunction complex or different entities?]. HNO, 54(5), 405-408, 410-404.
Ramat, S., Leigh, R. J., Zee, D. S., & Optican, L. M. (2007). What clinical disorders tell us about the neural control of saccadic eye movements. Brain, 130(Pt 1), 10-35.
Raven, J. C., Raven, J., & Court, J. H. (2002). Coloured Progressive Matrices (S. Bulheller & H. Häcker, Trans.). Frankfurt: Swets & Zeitlinger B.V., Swets Test Services.
Reuter-Lorenz, P. A., Herter, T. M., & Guitton, D. (in press). Control of Reflexive Saccades following Hemispherectomy. J Cogn Neurosci.

References
- 98 -
Reuter-Lorenz, P. A., Oonk, H. M., Barnes, L. L., & Hughes, H. C. (1995). Effects of warning signals and fixation point offsets on the latencies of pro- versus antisaccades: implications for an interpretation of the gap effect. Exp Brain Res, 103(2), 287-293.
Reuter, B., Kaufmann, C., Bender, J., Pinkpank, T., & Kathmann, N. (2009). Distinct Neural Correlates for Volitional Generation and Inhibition of Saccades. J Cogn Neurosci.
Riccio, C. A., Cohen, M. J., Hynd, G. W., & Keith, R. W. (1996). Validity of the Auditory Continuous Performance Test in differentiating central processing auditory disorders with and without ADHD. J Learn Disabil, 29(5), 561-566.
Riccio, C. A., & Hynd, G. W. (1996). Relationship between ADHD and central auditory processing disorder. School Psychology International, 17(3), 235-252.
Riccio, C. A., Hynd, G. W., Cohen, M. J., Hall, J., & Molt, L. (1994). Comorbidity of central auditory processing disorder and attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry, 33(6), 849-857.
Rommelse, N. N., Van der Stigchel, S., & Sergeant, J. A. (2008). A review on eye movement studies in childhood and adolescent psychiatry. Brain Cogn, 68(3), 391-414.
Ross, R. G., Harris, J. G., Olincy, A., & Radant, A. (2000). Eye movement task measures inhibition and spatial working memory in adults with schizophrenia, ADHD, and a normal comparison group. Psychiatry Res, 95(1), 35-42.
Rosvold, H. E., Mirsky, A. F., Sarason, I., Bransome, J., E. D., , & Beck, L. H. (1956). A Continuous Performance Test of Brain Damage. Journal of Consulting Psychology, 20, 343-350.
Rothlind, J. C., Posner, M. I., & Schaughency, E. A. (1991). Lateralized control of eye movements in attention deficit hyperactivity disorder. Journal of Cognitive Neuroscience, 3(4), 377-381.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C., Simmons, A., et al. (1999). Hypofrontality in attention deficit hyperactivity disorder during higher-order motor control: a study with functional MRI. Am J Psychiatry, 156(6), 891-896.
Rubia, K., Smith, A. B., Brammer, M. J., Toone, B., & Taylor, E. (2005). Abnormal brain activation during inhibition and error detection in medication-naive adolescents with ADHD. Am J Psychiatry, 162(6), 1067-1075.
Salman, M. S., Sharpe, J. A., Eizenman, M., Lillakas, L., Westall, C., To, T., et al. (2006). Saccades in children. Vision Res, 46(8-9), 1432-1439.
Saslow, M. G. (1967). Effects of components of displacement-step stimuli upon latency for saccadic eye movement. J Opt Soc Am, 57(8), 1024-1029.
Scahill, L., & Schwab-Stone, M. (2000). Epidemiology of ADHD in school-age children. Child Adolesc Psychiatr Clin N Am, 9(3), 541-555, vii.
Schachar, R., & Logan, G. D. (1990). Impulsivity and Inhibitory Control in Normal Development and Childhood Psychopathology. Developmental Psychology, 26(5), 710-720.
Schachar, R., Mota, V. L., Logan, G. D., Tannock, R., & Klim, P. (2000). Confirmation of an inhibitory control deficit in attention-deficit/hyperactivity disorder. J Abnorm Child Psychol, 28(3), 227-235.
Schneider, M., Retz, W., Coogan, A., Thome, J., & Rosler, M. (2006). Anatomical and functional brain imaging in adult attention-deficit/hyperactivity disorder (ADHD)--a neurological view. Eur Arch Psychiatry Clin Neurosci, 256 Suppl 1, i32-41.
Schooler, C., Roberts, B., & Cohen, R. (2008). Context, complexity, and cognitive processing in schizophrenia. Cogn Neuropsychiatry, 13(3), 250-266.
Schulz, K. P., Fan, J., Tang, C. Y., Newcorn, J. H., Buchsbaum, M. S., Cheung, A. M., et al. (2004). Response inhibition in adolescents diagnosed with attention deficit hyperactivity disorder during childhood: an event-related FMRI study. Am J Psychiatry, 161(9), 1650-1657.
Schulz, K. P., Tang, C. Y., Fan, J., Marks, D. J., Newcorn, J. H., Cheung, A. M., et al. (2005). Differential prefrontal cortex activation during inhibitory control in adolescents with and without childhood attention-deficit/hyperactivity disorder. Neuropsychology, 19(3), 390-402.

References
- 99 -
Seidman, L. J., Valera, E. M., & Makris, N. (2005). Structural brain imaging of attention-deficit/hyperactivity disorder. Biol Psychiatry, 57(11), 1263-1272.
Seidman, L. J., Valera, E. M., Makris, N., Monuteaux, M. C., Boriel, D. L., Kelkar, K., et al. (2006). Dorsolateral prefrontal and anterior cingulate cortex volumetric abnormalities in adults with attention-deficit/hyperactivity disorder identified by magnetic resonance imaging. Biol Psychiatry, 60(10), 1071-1080.
Shafiq, R., Stuart, G. W., Sandbach, J., Maruff, P., & Currie, J. (1998). The gap effect and express saccades in the auditory modality. Exp Brain Res, 118(2), 221-229.
Sharma, M., Purdy, S. C., & Kelly, A. S. (2009). Comorbidity of auditory processing, language, and reading disorders. J Speech Lang Hear Res, 52(3), 706-722.
Smith, A. B., Taylor, E., Brammer, M., Toone, B., & Rubia, K. (2006). Task-specific hypoactivation in prefrontal and temporoparietal brain regions during motor inhibition and task switching in medication-naive children and adolescents with attention deficit hyperactivity disorder. Am J Psychiatry, 163(6), 1044-1051.
Smyrnis, N., Evdokimidis, I., Stefanis, N. C., Constantinidis, T. S., Avramopoulos, D., Theleritis, C., et al. (2002). The antisaccade task in a sample of 2,006 young males. II. Effects of task parameters. Exp Brain Res, 147(1), 53-63.
Sonuga-Barke, E. J. (1994). On dysfunction and function in psychological theories of childhood disorder. J Child Psychol Psychiatry, 35(5), 801-815.
Sonuga-Barke, E. J. (2002). Psychological heterogeneity in AD/HD--a dual pathway model of behaviour and cognition. Behav Brain Res, 130(1-2), 29-36.
Sonuga-Barke, E. J. (2003). The dual pathway model of AD/HD: an elaboration of neuro-developmental characteristics. Neurosci Biobehav Rev, 27(7), 593-604.
Sonuga-Barke, E. J., Bitsakou, P., & Thompson, M. (2010). Beyond the dual pathway model: evidence for the dissociation of timing, inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry, 49(4), 345-355.
Sonuga-Barke, E. J., Taylor, E., Sembi, S., & Smith, J. (1992). Hyperactivity and delay aversion--I. The effect of delay on choice. J Child Psychol Psychiatry, 33(2), 387-398.
Sowell, E. R., Thompson, P. M., Welcome, S. E., Henkenius, A. L., Toga, A. W., & Peterson, B. S. (2003). Cortical abnormalities in children and adolescents with attention-deficit hyperactivity disorder. Lancet, 362(9397), 1699-1707.
Sparks, D. L. (2002). The brainstem control of saccadic eye movements. Nat Rev Neurosci, 3(12), 952-964.
Spencer, T. J., Biederman, J., & Mick, E. (2007). Attention-deficit/hyperactivity disorder: diagnosis, lifespan, comorbidities, and neurobiology. J Pediatr Psychol, 32(6), 631-642.
Sprich, S., Biederman, J., Crawford, M. H., Mundy, E., & Faraone, S. V. (2000). Adoptive and biological families of children and adolescents with ADHD. J Am Acad Child Adolesc Psychiatry, 39(11), 1432-1437.
Starzacher, E. (2006). Investigation of modality-specific attention skills in children with and without auditory processing disorder using the Continous Attention Performance Test. Freie Universität Berlin, Berlin.
Starzacher, E., Nubel, K., Grohmann, G., Gaupp, K., & Pfeiffer, Y. (2007). Continuous Attention Performance Test (CAPT) (Vol. 1). Göttingen: Hogrefe.
Steinhausen, H. C. (2003). Attention-deficit hyperactivity disorder in a life perspective. Acta Psychiatr Scand, 107(5), 321-322.
Sutcliffe, P. A., Bishop, D. V., Houghton, S., & Taylor, M. (2006). Effect of attentional state on frequency discrimination: a comparison of children with ADHD on and off medication. J Speech Lang Hear Res, 49(5), 1072-1084.
Swanson, J. M., Flodman, P., Kennedy, J., Spence, M. A., Moyzis, R., Schuck, S., et al. (2000). Dopamine genes and ADHD. Neurosci Biobehav Rev, 24(1), 21-25.

References
- 100 -
Swanson, J. M., Kinsbourne, M., Nigg, J., Lanphear, B., Stefanatos, G. A., Volkow, N., et al. (2007). Etiologic subtypes of attention-deficit/hyperactivity disorder: brain imaging, molecular genetic and environmental factors and the dopamine hypothesis. Neuropsychol Rev, 17(1), 39-59.
Sweeney, J. A., Takarae, Y., Macmillan, C., Luna, B., & Minshew, N. J. (2004). Eye movements in neurodevelopmental disorders. Curr Opin Neurol, 17(1), 37-42.
Tamm, L., Menon, V., & Reiss, A. L. (2002). Maturation of brain function associated with response inhibition. J Am Acad Child Adolesc Psychiatry, 41(10), 1231-1238.
Tamm, L., Menon, V., Ringel, J., & Reiss, A. L. (2004). Event-related FMRI evidence of frontotemporal involvement in aberrant response inhibition and task switching in attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry, 43(11), 1430-1440.
Tannock, R. (1998). Attention deficit hyperactivity disorder: advances in cognitive, neurobiological, and genetic research. J Child Psychol Psychiatry, 39(1), 65-99.
Taylor, T. L., Klein, R. M., & Munoz, D. P. (1999). Saccadic performance as a function of the presence and disappearance of auditory and visual fixation stimuli. J Cogn Neurosci, 11(2), 206-213.
Thompson, M. J., Brooke, X. M., West, C. A., Johnson, H. R., Bumby, E. J., Brodrick, P., et al. (2004). Profiles, co-morbidity and their relationship to treatment of 191 children with AD/HD and their families. Eur Child Adolesc Psychiatry, 13(4), 234-242.
Tillery, K. L., Katz, J., & Keller, W. D. (2000). Effects of methylphenidate (Ritalin) on auditory performance in children with attention and auditory processing disorders. J Speech Lang Hear Res, 43(4), 893-901.
Vaidya, C. J., Austin, G., Kirkorian, G., Ridlehuber, H. W., Desmond, J. E., Glover, G. H., et al. (1998). Selective effects of methylphenidate in attention deficit hyperactivity disorder: a functional magnetic resonance study. Proc Natl Acad Sci U S A, 95(24), 14494-14499.
Wang, Y., Matsuzaka, Y., Shima, K., & Tanji, J. (2004). Cingulate cortical cells projecting to monkey frontal eye field and primary motor cortex. Neuroreport, 15(10), 1559-1563.
Watanabe, K., Lauwereyns, J., & Hikosaka, O. (2003). Neural correlates of rewarded and unrewarded eye movements in the primate caudate nucleus. J Neurosci, 23(31), 10052-10057.
Wienbruch, C., Paul, I., Bauer, S., & Kivelitz, H. (2005). The influence of methylphenidate on the power spectrum of ADHD children - an MEG study. BMC Psychiatry, 5, 29.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry, 57(11), 1336-1346.
Witton, C. (2010). Childhood auditory processing disorder as a developmental disorder: the case for a multi-professional approach to diagnosis and management. Int J Audiol, 49(2), 83-87.
WMA (2004). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Int Bioethique, 15(1), 124-129.
World Health Organization, WHO (1993). The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic criteria for research Geneva.
Yang, B., Chan, R. C. K., Jing, J., Li, T., Sham, P., & Chen, R. Y. L. (2007). A meta-analysis of association studies between the 10-repeat allele of a VNTR polymorphism in the 3′-UTR of dopamine transporter gene and attention deficit hyperactivity disorder. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 144B(4), 541-550.
Yao, L., & Peck, C. K. (1997). Saccadic eye movements to visual and auditory targets. Exp Brain Res, 115(1), 25-34.
Yerys, B. E., Jankowski, K. F., Shook, D., Rosenberger, L. R., Barnes, K. A., Berl, M. M., et al. (2009). The fMRI success rate of children and adolescents: typical development, epilepsy, attention deficit/hyperactivity disorder, and autism spectrum disorders. Hum Brain Mapp, 30(10), 3426-3435.
Zambarbieri, D. (2002). The latency of saccades toward auditory targets in humans. Prog Brain Res, 140, 51-59.

References
- 101 -
Zambarbieri, D., Beltrami, G., & Versino, M. (1995). Saccade latency toward auditory targets depends on the relative position of the sound source with respect to the eyes. Vision Res, 35(23-24), 3305-3312.
Zambarbieri, D., Schmid, R., Magenes, G., & Prablanc, C. (1982). Saccadic responses evoked by presentation of visual and auditory targets. Exp Brain Res, 47(3), 417-427.
Zambarbieri, D., Schmid, R., Prablanc, C., & Magenes, G. (1981). Characteristics of eye movements evoked by the presentation of acoustic targets. In A. Fuchs & W. Becker (Eds.), Progress in oculmotor research (pp. 559-566). Amsterdam: Elsevier North Holland.