antipsychotic induced diabetes 6.23
TRANSCRIPT

Non-ketonic Hyperglycemia Hyperosmolar State Secondary to Clozapine TherapyMichael Nguyen, Pharm. D. Candidate 2017
MCPHS University

ObjectivesAfter this presentation, the audience should be able to 1. Appreciate the risks of metabolic effects (specifically
hyperglycemia) from antipsychotic medications2. Explain how to manage acute non-ketonic
hyperglycemia hyperosmolar state (HHS). 3. Make recommendations for patients with new onset
diabetes secondary to antipsychotic therapy
For the purposes of this discussion Atypical antipsychotics = AAPs = 2nd generation antipsychotics = SGA’sTypical antipsychotics = TAPs = 1st generation antipsychotics = FGA’s

Meet the patientAM is a 67 year old male who presents to Lahey ER with a CC of altered mental status and lethargy with increased thirst and urination.
Nurses at his locked psychiatric facility noticed he was behaving differently.
He became dizzy and fell, causing him to be brought in to Lahey. There was no documentation of head trauma.
Of note, he was recently treated for furunculosis with Keflex

PTA medicationsSchizoaffective disorder
HLD± HTN± INS± BPH± ANX± Smoking Cessation
Misc.
Clozapine 150 mg PO daily
Lithium 300 mg PO daily
Haloperidol 0.5 mg PO PRN agitation
Atorvastatin 20 mg PO daily
Metoprolol tartrate 175 mg by mouth BID
Melatonin 3 mg HS
Diphen** 25 mg tablet PO HS PRN for insomnia
Tamsulosin 0.4 mg PO daily
Lorazepam1 mg PO Q6H PRN for anxiety
Nicotine Polacrilex 4 mg lozenge PRN for smoking cessation
Maalox Advanced, 30 mL PO Q6H PRN
Clotrimazole 1% cream every morning and evening
Vit. D3 1ooo IU QD
B12 1000 mcg QD
Docusate 100 mg capsule every morning and evening
Milk of Magnesium 400 mg / 5 mL suspension, 30 mL PO QD PRN
Sennosides 8.6 mg PO daily
± HLD – Hyperlipidemia, HTN – Hypertension, INS – Insomnia, BPH – Benign prostate hyperplasia, ANX – Anxiety ** diphenhydramine
Medications Held on admission
New In-Patient Meds (3 day stay)
Maalox Advanced, 30 mL PO Q6H PRNDiphenhydramine 25 mg tablet, PO HS PRN for insomniaLithium 300 mg PO daily Lorazepam 1 mg PO Q6H PRN for anxietySennosides 8.6 mg PO daily
(6/5) Ceftriaxone (6/6) Cefazolin 1 g Q8h(6/6) Lithium CR 300 BIDNormal Saline IV bolus & Continuous Heparin 5000 u SC BID Insulin aspart and glargineSaccharomyces Boulardii BID

Schizoaffective disorder vs. Schizophrenia
• Diagnostic and Statistical Manual of Mental Disorders (DSM-5) definitions
• Schizophrenia – a serious mental illness characterized by at least 2 of the following symptoms for a minimum of 6 months and include at least one month of active symptoms. (which interfere with social/occupational function)▫Delusions▫Hallucinations▫Disorganized speech and behavior ▫Grossly disorganized or catatonic behavior▫Negative symptoms (diminished emotional expression)
ADD MOOD SWINGS (bipolar
disorder)
Schizoaffective
Disorder
DSM-5 2013;150(1):3-10DSM-5 2013;150(1):21-25

Hyperosmolar Hyperglycemia StateDiagnostic Criteria Diagnostic value Our Patient Blood Glucose > 600 mg / dL 813 mg / dLArterial pH > 7.3 7.38Bicarbonate > 15 mEq / L 24 mEq / LMild Ketonuria / Ketonemia
Positive Urine ketones negative
Effective Serum Osmolality
> 320 mOsm / kg H2O
303 mOsm / kg
Diabetes Care 2009;32(7):1335-1343
Effective serum osmolality = 2(Na) + (Glucose)/18

My Questions
How did the endocrinologist associate HHS with clozapine?
What is the nature of clozapine induced diabetes mellitus (DM)?
Did we properly treat AM’s HHS?
How do you manage a patient with diabetes induced by clozapine?
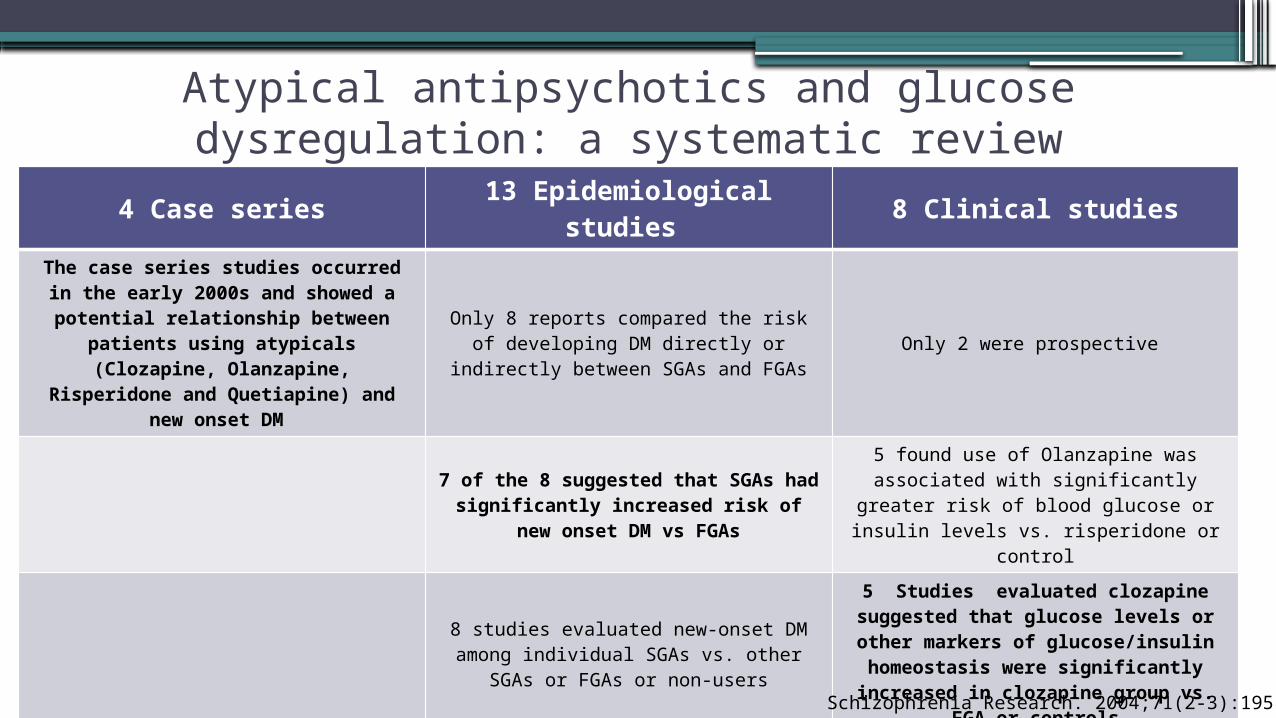
Atypical antipsychotics and glucose dysregulation: a systematic review
4 Case series 13 Epidemiological studies 8 Clinical studies
The case series studies occurred in the early 2000s and showed a potential relationship between
patients using atypicals (Clozapine, Olanzapine, Risperidone and
Quetiapine) and new onset DM
Only 8 reports compared the risk of developing DM directly or indirectly
between SGAs and FGAsOnly 2 were prospective
7 of the 8 suggested that SGAs had significantly increased risk of new
onset DM vs FGAs
5 found use of Olanzapine was associated with significantly greater risk
of blood glucose or insulin levels vs. risperidone or control
8 studies evaluated new-onset DM among individual SGAs vs. other SGAs
or FGAs or non-users
5 Studies evaluated clozapine suggested that glucose levels or other markers of glucose/insulin homeostasis were significantly
increased in clozapine group vs. FGA or controls
2 studies found no difference in risk of developing DM with clozapine while 2 other found greater risk Schizophrenia Research. 2004;71(2-3):195-212

Clozapine-associated DiabetesHyperglycemic events associated with Clozapine use were searched using
FDA Medwatch (Jan 1990 – Feb 2001)Medline (Jan 1985 – Feb 2001)
Koller E. et al. 2001
n = 384 cases

Clozapine-associated Diabetes cont. Koller E. et al. 2001

Association of Diabetes Mellitus with Use of Atypical Neuroleptics in the Treatment of Schizophrenia
•Retrospective study of ALL patients in VA database with a diagnosis of schizophrenia during fiscal year of 1999 (October 1, 1998 to September 30, 1999)
•Hypothesis – Prescription of atypical neuroleptics (SGA’s) is associated with an increased prevalence of diabetes.
AJP. 2002;159(4):561-566Sernyak, Leslie, Alarcon, et al.

Full of confounding?Patients with Dx of Schizophrenia(Oct 1998 – Sep 1999)
n = 38,632
15,984 (41.4%) Received typical antipsychotics
22648 (58.6%) received atypical antipsychotics
Baseline Characteristics
The groups were significantly different in all characteristics except for Hispanic or Degree of VA
compensation
Significantly • Younger • Have less income• More female • Incidence of another psychiatry
diagnosis• They also lived further from VA
hospital • Likely hood of being hospitalized
AJP. 2002;159(4):561-566
Association of Diabetes Mellitus with Use of Atypical Neuroleptics in the Treatment of Schizophrenia

What were the odds of DM with atypicals? • Younger age groups (<60) had higher
odds of DM diagnosis • For the entire group (all ages) All
atypicals had significantly greater odds of DM diagnosis except for risperidone
• Although there was no difference in older groups, look at the rate of diabetes in either group
AJP. 2002;159(4):561-566

Key Points of the articlesKoller et. al. Sernyak et. al.
• Most hyperglycemic events associated with clozapine occur within 6 months of therapy initiation.
• There are some cases where discontinuing clozapine therapy may reverse hyperglycemia / glucose dysregulation
• 15% of the new-onset diabetes patients developed blood sugars of > 700 mg/dL
• This study did not show any correlation with dose and severity of the hyperglycemic event.
• Patients receiving SGAs are 9% more likely to have DM than those on conventional antipsychotics (p = 0.002)
• Younger aged patients with schizophrenia who take atypicals have significantly greater odds of having DM diagnosis vs. those not taking atypicals. The odds are not significant in older patients (60+)
• This supports that older patients are more likely to get diabetes and metabolic dysregulation due to the nature of the disease.

Back to our patient…Diagnostic Criteria Diagnostic value Our Patient Blood Glucose > 600 mg / dL 813 mg / dLArterial pH > 7.3 7.38Bicarbonate > 15 mEq / L 24 mEq / LMild Ketonuria / Ketonemia
Positive Urine ketones negative
Effective Serum Osmolality
> 320 mOsm / kg H2O
303 mOsm / kg
Diabetes Care 2009;32(7):1335-1343
Effective serum osmolality = 2(Na) + (Glucose)/18

Treatment regimen for hyperosmolar hyperglycemia state
Diabetes Care 2009;32(7):1335-1343

So… what ever happened to our patient?
6/4/16 12:00 6/5/16 0:00 6/5/16 12:00 6/6/16 0:00 6/6/16 12:00 6/7/16 0:00 6/7/16 12:00 6/8/16 0:000
100
200
300
400
500
600
700
800
0
5
10
15
20
25
30
35
40AM’s 3 day Clinical Course
Glucose (g/dL) Potassium (mmol/L) Rapid/Short Insulin (units) Glargine (units)
IV bolus
SubQ

Review of outpatient monitoring with antipsychotics
Baseline 4 weeks 8 weeks 12 weeks Quarterly
Annually Every 5 years
Personal/Family Hx
X X
Weight (BMI) X X X X XWaist Circumf. X XBlood Pressure X X XFasting blood gluc.
X X X X
Fasting Lipid panel
X XDiabetes Care. 2004;27(2):596-601
“Consider switching to a less offensive agent if the patient develops a weight gain of 5% or more during any time of
treatment with SGA or those who develop worsening glycemia or dyslipidemia”

Patient discharge •AM was discharged on 6/7/16 (2 days inpatient) to
Bedford VA to be followed up with psychiatry and endocrinology
Schizoaffective disorder
HLD± HTN± INS± BPH± ANX± Smoking Cessation
Misc.
Clozapine 150 mg PO daily
Lithium 300 mg PO daily
Haloperidol 0.5 mg PO PRN agitation
Atorvastatin 20 mg PO daily
Metoprolol tartrate 175 mg by mouth BID
Melatonin 3 mg HS
Diphen** 25 mg tablet PO HS PRN for insomnia
Tamsulosin 0.4 mg PO daily
Lorazepam1 mg PO Q6H PRN for anxiety
Nicotine Polacrilex 4 mg lozenge PRN for smoking cessation
Maalox Advanced, 30 mL PO Q6H PRN
Clotrimazole 1% cream every morning and evening
Vit. D3 1ooo IU QD
B12 1000 mcg QD
Docusate 100 mg capsule every morning and evening
Milk of Magnesium 400 mg / 5 mL suspension, 30 mL PO QD PRN
Sennosides 8.6 mg PO daily
New Medication at D/C Insulin aspart sliding scale and insulin glargine 40 units SC HS
Continue with PTA medications

Any Questions ?References
• Malaspina D, Owen MJ, Heckers S, et al. Schizoaffective Disorder in the DSM-5. Schizophrenia Research. 2013;150(1):21-25. doi:10.1016/j.schres.2013.04.026. Accessed 6/18/2016
• Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophrenia Research. 2013;150(1):3-10. doi:10.1016/j.schres.2013.05.028.
• Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic Crises in Adult Patients With Diabetes. Diabetes Care. 2009;32(7):1335-1343. doi:10.2337/dc09-9032.
• Koller E, Schneider B, Bennett K, Dubitsky G. Clozapine-associated diabetes. The American Journal of Medicine. 2001;111(9):716-723. doi:10.1016/s0002-9343(01)01000-2.
• Taylor M, Perera U. NICE CG178 Psychosis and Schizophrenia in Adults: Treatment and Management - an evidence-based guideline. The British Journal of Psychiatry. 2015;206(5):357-359. doi:10.1192/bjp.bp.114.155945.
• Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. Diabetes Care. 2004;27(2):596-601. doi:10.2337/diacare.27.2.596.
• Jin H, Meyer JM, Jeste DV. Atypical antipsychotics and glucose dysregulation: a systematic review. Schizophrenia Research. 2004;71(2-3):195-212. doi:10.1016/j.schres.2004.03.024
• Clozapine and the Risk of Neutropenia: A Guide for Healthcare Providers. Clozapine REMS. https://www.clozapinerems.com/cpmgclozapineui/rems/pdf/resources/clozapine_rems_a_guide_for_healthcare_providers.pdf. Published September 2015. Accessed June 23, 2016.
• Sernyak MJ, Leslie DL, Alarcon RD, Losonczy MF, Rosenheck R. Association of Diabetes Mellitus With Use of Atypical Neuroleptics in the Treatment of Schizophrenia. American Journal of Psychiatry AJP. 2002;159(4):561-566. doi:10.1176/appi.ajp.159.4.561.