antiplatelet therapy in cad minilecture. objectives indications for antiplatelet therapy in patients...
TRANSCRIPT
Antiplatelet therapy in CADMINILECTURE

Objectives Indications for Antiplatelet Therapy in patients with CAD and ACS
Antiplatelet Therapy in the role of primary and secondary prevention of cardiovascular events
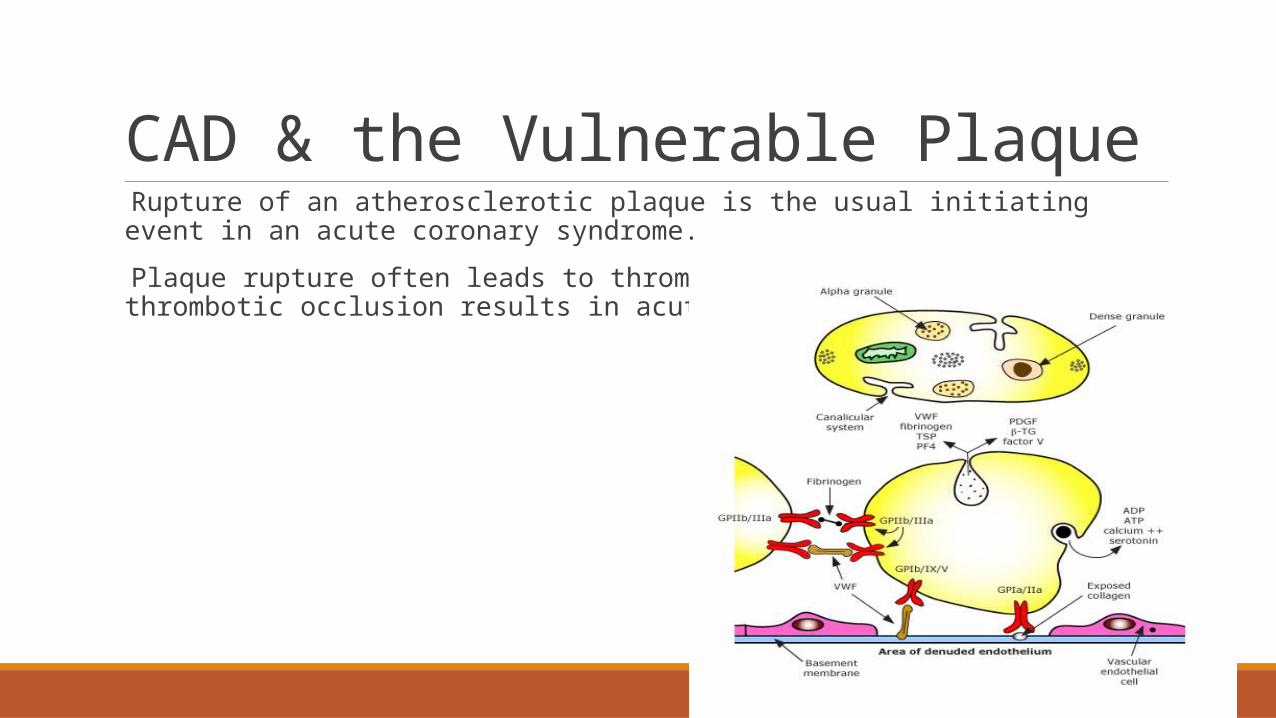
CAD & the Vulnerable Plaque Rupture of an atherosclerotic plaque is the usual initiating event in an acute coronary syndrome.
Plaque rupture often leads to thrombus formation and persistent thrombotic occlusion results in acute myocardial infarction.
Antiplatelet Mechanism of Action
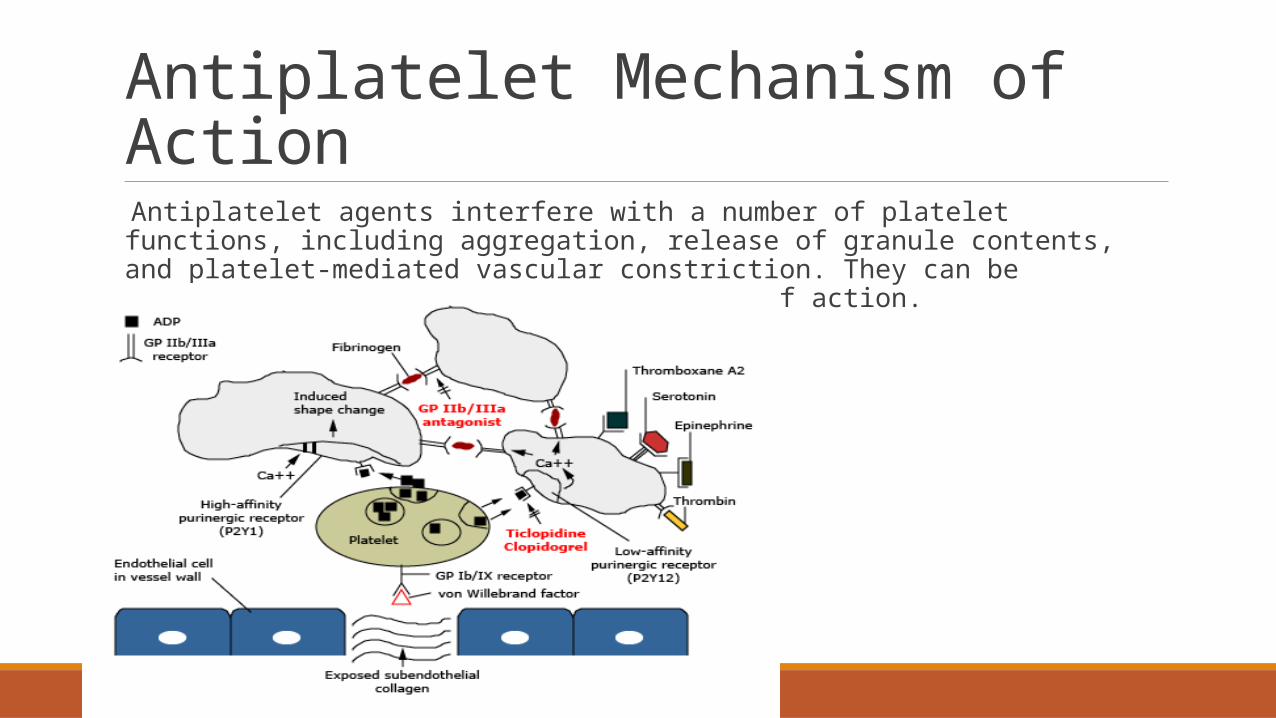
Antiplatelet agents interfere with a number of platelet functions, including aggregation, release of granule contents, and platelet-mediated vascular constriction. They can be classified according to their mechanism of action.
Antiplatelet Mechanism of Action
Aspirin blocks cyclooxygenase, the enzyme that mediates the first step in the biosynthesis of prostaglandins and thromboxanes from arachidonic acid, preventing platelet aggregation
The P2Y12 (ADP) receptor blockers (clopidogrel, etc.) block the binding of adenosine diphosphate (ADP) to a platelet receptor P2Y12, thereby inhibiting activation of the glycoprotein (GP) IIb/IIIa complex and platelet aggregation
Anti-GP IIb/IIIa antibodies and receptor antagonists inhibit the final common pathway of platelet aggregation (the cross-bridging of platelets by fibrinogen binding to the GP IIb/IIIa receptor)
Aspirin Platelets do not synthesize new enzymes functional defect induced by aspirin persists for the life of the platelet (nonreversible)
In ACS, including Unstable Angina and NSTEMI: reduction in the combined endpoints of subsequent nonfatal MI, nonfatal stroke, and vascular death
◦ Give first dose in ACS of 162-325mg, crushed or chewed, as soon as possible in ACS◦ ASA has rapid and immediate antithrombotic effect◦ Discharge patient on ASA 75-100mg daily and to be continued indefinitely for secondary preventionSide effects: GI intolerance, worsening of preexistent bleedingPrimary Prevention1. Benefit of ASA must be weighed against risk of bleeding
1. Risk of bleeding likely to outweigh benefits in patients w/ Framingham 10 year risk scores < 10%2. Consider in patients with DMII and those with CKD as well as patients w/ Framingham risk scores > 10%
Antiplatelet Therapy After Stenting
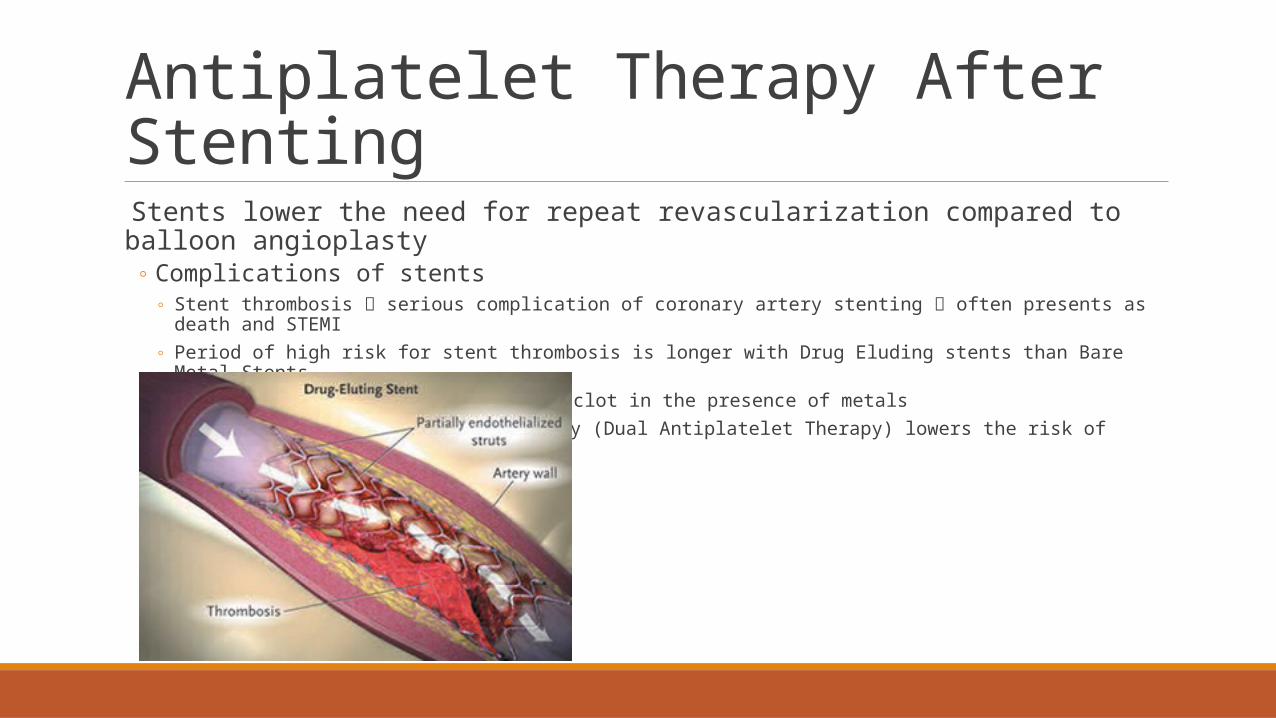
Stents lower the need for repeat revascularization compared to balloon angioplasty◦ Complications of stents
◦ Stent thrombosis serious complication of coronary artery stenting often presents as death and STEMI ◦ Period of high risk for stent thrombosis is longer with Drug Eluding stents than Bare Metal Stents
◦ Tendency for circulating blood to clot in the presence of metals◦ More intense antiplatelet therapy (Dual Antiplatelet Therapy) lowers the risk of stent thrombosis
Dual-Antiplatelet Therapy (DAPT) After Stenting
DURATION◦ For both Drug Eluting Stents and Bare Metal Stents optimal duration of dual platelet therapy is 1 year
◦ ASA indefinitely for both DES and BMS◦ BMS Clopidogrel or other ADP antagonist for a minimum of 1 month and preferably for 12 months, uninterrupted◦ DES Clopidogrel or other ADP antagonist for a minimum of 6 month and preferably for 12 months, uninterrupted◦ Balloon angioplasty ASA indefinitely and Clopidogrel for 1 month
Patient and Risk Factor Specific◦ Certain high risk groups for whom therapy > 12 months may be optimal (low bleeding risk factor profile)
◦ Left main or proximal LAD stent (consequences for stent thrombosis is catastrophic)◦ Complex PCI bifurcation, long lesions, or saphenous vein grafts
◦ Certain *high risk groups* for whom uninterrupted therapy < 12 months may be considered◦ Bleeding event during DAPT◦ Temporary discontinuation of DAPT due to need for urgent or time sensitive surgery
Dual-Antiplatelet Therapy (DAPT) After Stenting
Major Considerations◦ Warfarin + Dual Antiplatelet Treatment
◦ If warfarin is needed for Atrial Fibrillation, mechanical valves, DVT, etc. consider INR on the lower side of target range and in patients with stents, consider discontinuation of clopidogrel after the minimum duration of dual antiplatelet treatment to minimize the bleeding risk
◦ Management of bleeding risk for dual antiplatelet treatment◦ Patients with a history of GI bleeding or are at risk for GI bleed use PPI
◦ Elderly◦ Warfarin◦ Steroids◦ NSAIDs
◦ Determination of duration and ability to comply with dual antiplatelet therapy along with the risks of bleeding often plays a role in determining what type of stent a patient ultimately gets
Clopidogrel-PPI interactions Observations studies suggested PPIs decrease the efficacy of clopidogrel
Randomized control trial of clopidogrel + omeprazole showed that the combination decreased the rate of GI events compared to placebo with no difference in cardiovascular events
ADP receptor antagonists (P2Y12 receptor blockers)
Ticlopidine: rarely used anymore due to risk of thrombocytopenia, neutropenia, GI upset and TTP-HUS
Clopidogrel: DAPT with Clopidogrel and ASA was superior compared to ASA alone in patients w/ NSTEMI
◦ 3 limitations to the use of clopidogrel◦ Delayed onset of action◦ Large individual variability in platelet response due to mutation in CYP2C19 allele decreased platelet inhibition and increase in
ischemic events◦ Inhibitory effect on platelets is Irreversible
Prasugrel: more rapid onset of action and achieves higher degrees of platelet inhibition than clopidogrel
◦ Compared with Clopidogrel, 19% reduction in cardiovascular death/MI/stroke when given at time of planned PCI, however bleeding risk greatly increased (including life-threatening bleed)
◦ Contraindicated in patients w/ history of stroke, age > 75 years, or weight < 60 kg
Ticagrelor Binds reversibly to the P2Y12 platelet receptor
◦ More rapid onset of action than clopidogrel◦ More intense platelet inhibition than clopidogrel◦ Data reveals better *efficacy* than clopidogrel with reduction in cardiovascular death, MI, stroke in
patients with ACS
Antiplatelet Therapy after CABG Issue of whether Clopidogrel or other ADP receptor antagonist should be started after CABG in patients with ACS has not been adequately addressed
◦ Suggestion of benefit from long-term ADP receptor antagonists in ACS patients who undergo CABG◦ Non-significant decrease in CV death, MI, and stroke seen in the CURE trial
◦ 2011 American College of Cardiology Foundation and AHA guideline for CABG does not make a recommendation for or against the addition of clopidogrel◦ Surgeon Preference
Antiplatelet Therapy in STEMI I. For patients with planned PCI, Dual Antiplatelet Therapy is recommended with ASA and either Clopidogrel, Ticagrelor, or Prasugrel
II. If Clopidogrel is chosen then the initial loading dose recommended is 600mg
III. For patients receiving fibrinolytic therapy, Clopidogrel is recommended in preference to Ticagrelor or Prasugrel given the increased bleeding risk
◦ Initial loading dose is 300mg for patients < 75 years◦ For patients > 75 years, 75mg loading dose should be given
Question Question 1: A 55-year-old man with a history of coronary artery disease undergoes a routine eval. Six months ago, a bare metal stent was placed in the left anterior descending coronary artery. He has had no
On physical examination, temperature is normal, blood pressure is 115/80 mm Hg, pulse rate is 70/min, and respiration rate is 12/min. Jugular venous pulsations are normal, and normal S1 and S2 are heard without murmurs. Lung fields are clear, distal pulses are normal, and no peripheral edema is present. The patient is requesting information regarding how long he needs to be on ASA/Plavix.
A. Patient will need to be on ASA/Plavix for a minimum of 3 months
B. Patient will need to be on ASA/Plavix for a minimum of 6 months
C. Patient will need to be on ASA/Plavix for a minimum of 9 months
D. Patient will need to be on ASA/Plavix for a minimum of 12 months
Answer Correct answer: D
For patients treated with either DES or BMS who are not at high bleeding risk and who do not have planned noncardiac surgery within one year, continue DAPT for at least 12 months rather than a shorter treatment duration.
For patients treated with BMS at high bleeding risk or who have planned noncardiac surgery within one year, we recommend a minimum of one month of uninterrupted DAPT. For such patients treated with DES, we recommend uninterrupted DAPT for a minimum of six months.
Continue ASA indefinitely in all stented patients.