antidiuretic hormone adh adh hypertonic interstitial fluid collecting duct h2oh2o urine
TRANSCRIPT
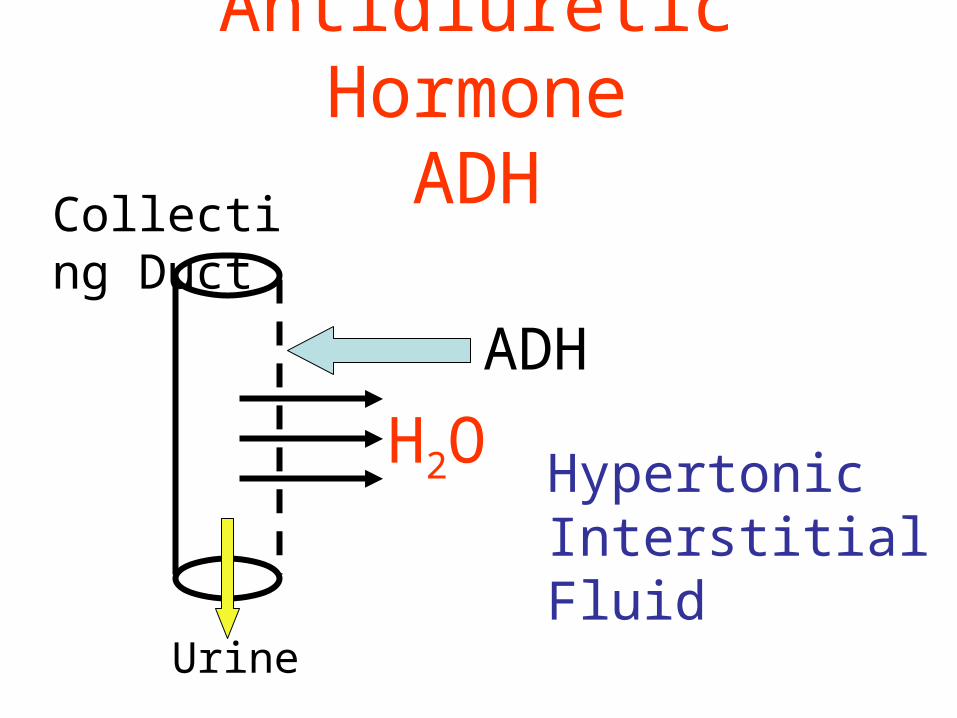
Antidiuretic HormoneADH
ADH
Hypertonic Interstitial Fluid
Collecting Duct
H2O
Urine
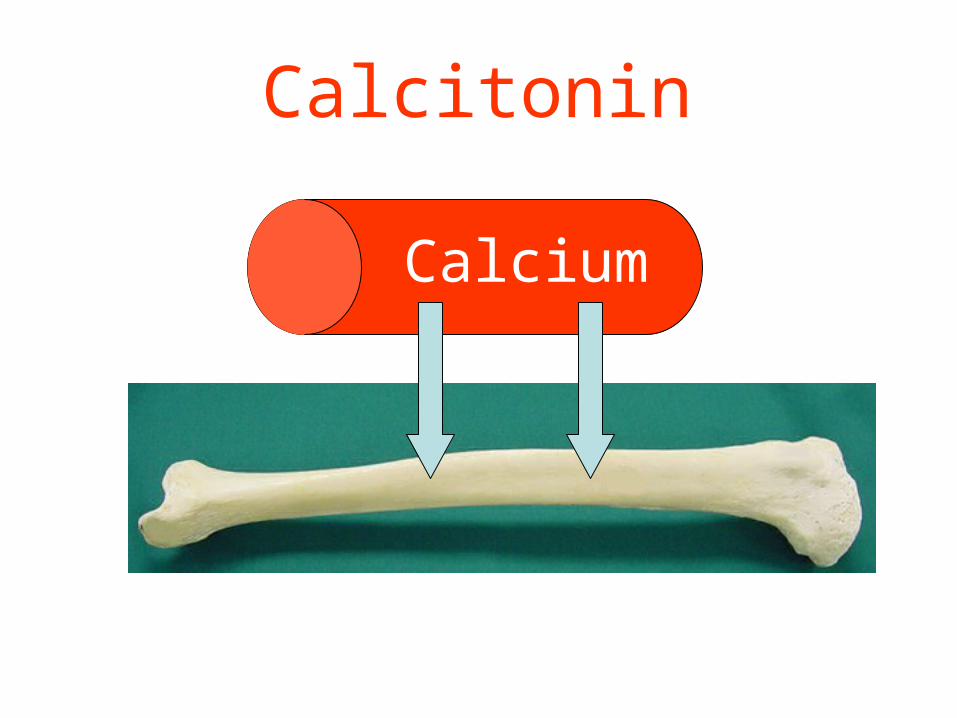
Calcitonin
Calcium
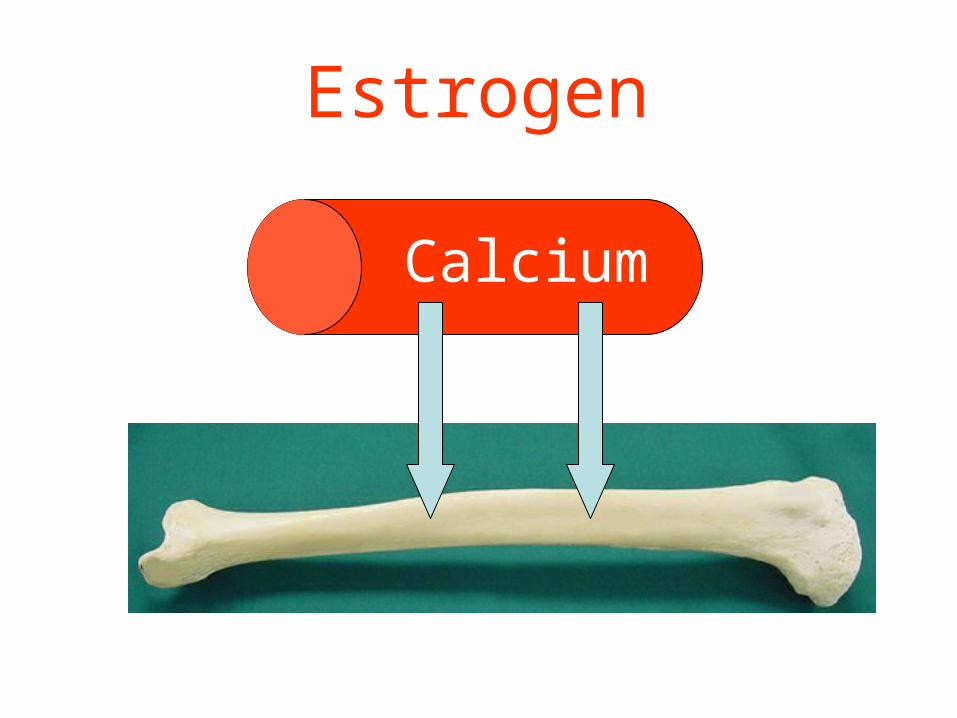
Estrogen
Calcium
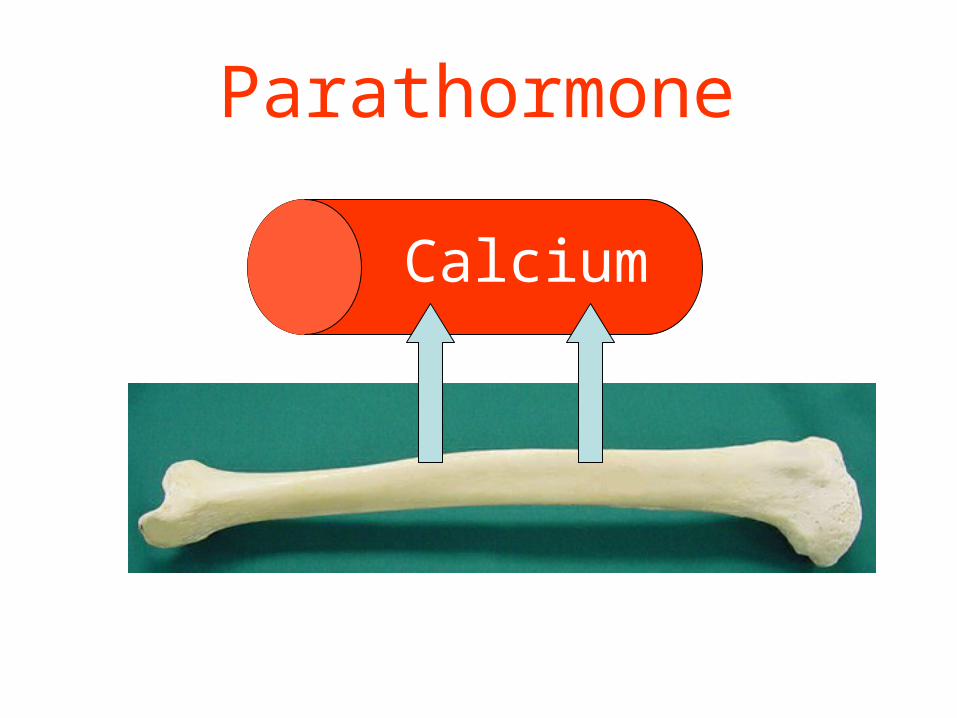
Parathormone
Calcium
Blood pH = 7.4(7.35-7.45)
Blood pH regulated by1. Kidneys2. Lungs
3. Buffers in blood
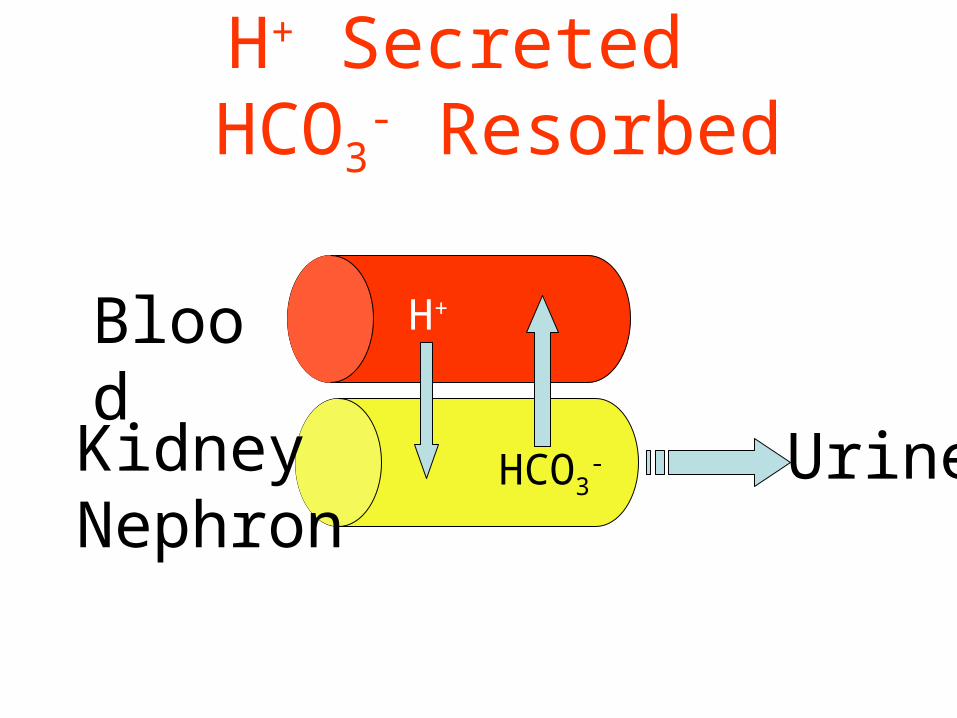
H+ Secreted HCO3
- Resorbed
Blood
Kidney Nephron
HCO3-
H+
Urine
Kidneys Regulate pH
• Excreting excess hydrogen ions, retain bicarbonate– if pH is too low
• Retaining hydrogen ions, excrete bicarbonate– if pH is too high
Lungs Regulate pH
• Breathe faster to get rid of excess carbon dioxide if pH is too low– Carbon dioxide forms carbonic acid in the
blood
• Breathe slower to retain carbon dioxide if pH is too high
Carbon Dioxide and Acid
CO2 + H2O H2CO3 H+ + HCO3-
Carbonic Acid

More Carbon Dioxide = More Acid = Lower pH
• Breathing slower will retain CO2 , pH will– decrease (more acid)
• Breathing faster will eliminate more CO2 pH will– increase (less acid)
Blood pH Drops to 7.3How does the body compensate?
• Breathe faster to get rid of carbon dioxide– eliminates acid
Blood pH Increases to 7.45How does the body compensate?
• Breathe slower to retain more carbon dioxide– retains more acid

The role of ADH:
• ADH = urinary concentration• ADH = secreted in response to ⇑
osmolality;
= secreted in response to ⇓ vol;• ADH acts on DCT / CD to reabsorb water• Acts via V2 receptors & aquaporin 2• Acts only on WATER
PG
Calculation of osmolality
• Difficult: measure & add all active osmoles
• Easy = [ sodium x 2 ] + urea + glucose
• Normal = 280 - 290 mosm / kg
PG
Fluid shifts in disease
• Fluid loss:– GI: diarrhoea, vomiting, etc.– Renal: diuresis– Vascular: haemorrhage– Skin: burns,sweat
• Fluid gain:– Iatrogenic:– Heart / liver / kidney failure:
PG
Prescribing fluids:
• Crystalloids:– 0.9% saline - not “normal” !– 5% dextrose– 0.18% saline + 0.45% dextrose– Others
• Colloids:– Blood– Plasma / albumin– Synthetics eg gelofusion
PG
The rules of fluid replacement:
• Replace blood with blood• Replace plasma with colloid• Resuscitate with crystalloid or colloid• Replace ECF depletion with saline• Rehydrate with dextrose
PG
How much fluid to give ?
• What is your starting point ?– Euvolaemia ? ( normal )– Hypovolaemia ? ( dry )– Hypervolaemia ? ( wet )
• What are the expected losses ?• What are the expected gains ?
PG
Signs of hypo / hypervolaemia:
Signs of …Volume depletion Volume overloadPostural hypotension Hypertension
Tachycardia Tachycardia
Absence of JVP @ 45o Raised JVP / gallop rhythm
Decreased skin turgor Oedema
Dry mucosae Pleural effusions
Supine hypotension Pulmonary oedema
Oliguria Ascites
Organ failure Organ failure
PG
What are the expected losses ?
• Measurable:– urine ( measure hourly if necessary )– GI ( stool, stoma, drains, tubes )
• Insensible:– sweat– exhaled
PG
• Electrolyte (Na+, K+, Ca++) Steady State• Amount Ingested = Amount Excreted.• Normal entry: Mainly ingestion in food. • Clinical entry: Can include parenteral
administration.
Case 1:
• A 62 year old man is 2 days post-colectomy. He is euvolaemic, and is allowed to drink 500ml. His urine output is 63 ml/hour:
1. How much IV fluid does he need today ?
2. What type of IV fluid does he need ?
PG
Case 2:
• 3 days after her admission, a 43 year old woman with diabetic ketoacidosis has a blood pressure of 88/46 mmHg & pulse of 110 bpm. Her charts show that her urine output over the last 3 days was 26.5 litres, whilst her total intake was 18 litres:
1. How much fluid does she need to regain a normal BP ?
2. What fluids would you use ?
PG
Case 3:
• An 85 year old man receives IV fluids for 3 days following a stroke; he is not allowed to eat. He has ankle oedema and a JVP of +5 cms; his charts reveal a total input of 9 l and a urine output of 6 litres over these 3 days.
1. How much excess fluid does he carry ?
2. What would you do with his IV fluids ?
PG
Case 4:
• 5 days after a liver transplant, a 48 year old man has a pyrexia of 40.8oC. His charts for the last 24 hours reveal:
• urine output: 2.7 litres• drain output: 525 ml• nasogastric output: 1.475 litres• blood transfusion: 2 units (350 ml
each)• IV crystalloid: 2.5 litres• oral fluids: 500 ml
PG
Case 4 cont:
• On examination he is tachycardic; his supine BP is OK, but you can’t sit him up to check his erect BP. His serum [ Na+ ] is 140 mmol/l.
• How much IV fluid does he need ?• What fluid would you use ?
PG
Case 5
• 30yo girl• SOB, moist cough, chest pain• ESKD• Very little urine output• Has missed dialysis last 3 sessions
Case 5
• What next?
– Current weight 78kg– IBW 68kg– JVP twitching her ear– No peripheral oedema– Coarse crackles to mid zones– BP 240/110– P 100– Gallop rhythm– 4cm of liver in RUQ
Case 5
• Assessment– Acute significant overload– Probably about 10kg
Case 6
• 55yo lady• Presents to dialysis for her routine session• BP 78/30
• History of dizziness for the last 6 hours• Current weight 58kg• IBW 59kg
Case 6
• P 120• Chest clear• HS dual• No oedema• Admits to 24hours of diarrhoea• Thirsty• No JVP visible
Case 6
• Dehydrated• Volume constricted• Hypotensive due to decreased circulating
fluid volume• Resuscitation?

The EndThe End
Acknowledgements
• Paddy Gibson – 4th year teaching ppt 2009
• Robert Harris – Fluid Balance ppt 2009• Heather Laird-Fick – Fluid and electrolyte
disorders ppt 2009• JXZhang Lecture 14 – ppt 2009• Dennis Wormington – fundamentals of
fluid assessment ppt 2009