antibiotics presentation gpce brisbane1.ppt · patients with mild community-acquired pneumonia...
TRANSCRIPT
15 – 16 September 2012
Workshop W13M
Antibiotic Resistance
Speakers: Cathy Prest Ann Winkle

1
Speakers:
Antibiotic Resistance andRespiratory Tract Infections
Ann Winkle & Cathy Prest
Presented by NPS Better choices, Better health
Medicare Local – Metro North Brisbane
The History of Medicine(Anonymous, WHO, 2000):
2000 BC – Here, eat this root
1000 AD – that root is heathen; here, say this prayer
1850 AD – that prayer is superstition; here swallow this pill
1945 AD – that pill is ineffective; here take this penicillin
1960 -1999 AD – oops… bugs mutated; here take this more
powerful antibiotic
2000 AD – the bugs have won! Here, eat this root
The introduction of a new antibiotic followed by firstreports of acquired resistance
Total antibacterials approved for use byUSA FDA
From IDSA Capitol Hill talk by Brad Spellberg May 11 2010.www.idsociety.org/Content.aspx?id=4810
Resistance at the population level• Resistance genes are often transmissible from bacterium to
bacterium.
Eg: the ampicillin-resistance gene (TEM-1) commonly found in E.colihas spread to Haemophilus influenzae and is by farthe most common cause of ampicillin resistance in that species
Plasmid-acquired resistance
Collignon P. Antibiotic resistance. Med J Aust 2002 177: 325-329.
Resistance at the population level
• Resistances are accumulating
• Important resistances in community-acquired respiratorypathogens*
Amox AmClav Macros Tetras Co-tri
Streptococcus pneumoniae <1% <1% 17% 15% 26%
Haemophilus influenzae 27% 2% 100% 12% 20%
Moraxella catarrhalis 95% 0% 0% ~10% ~10%
*AGAR: http://www.agargroup.org/surveys
2
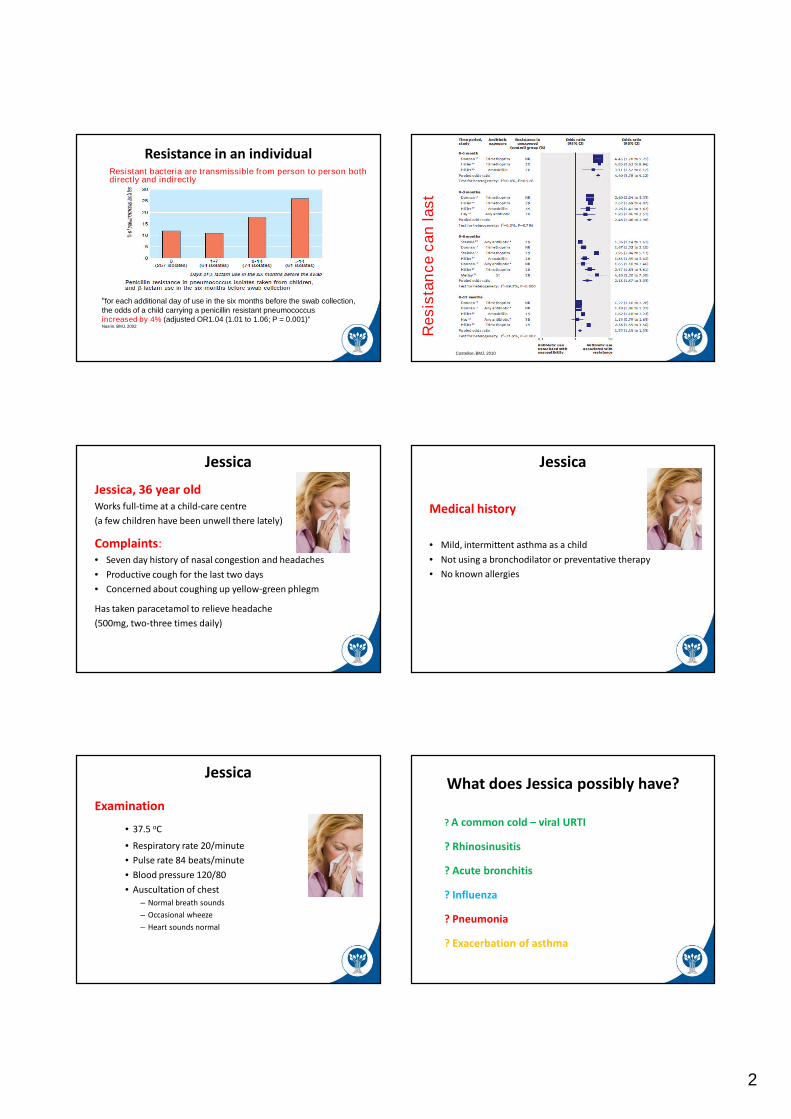
Resistance in an individual
“for each additional day of use in the six months before the swab collection,the odds of a child carrying a penicillin resistant pneumococcusincreased by 4% (adjusted OR1.04 (1.01 to 1.06; P = 0.001)”Nasrin, BMJ, 2002
Resistant bacteria are transmissible from person to person bothdirectly and indirectly
Resis
tan
ce
can
last
Costelloe, BMJ, 2010
Jessica
Jessica, 36 year oldWorks full-time at a child-care centre
(a few children have been unwell there lately)
Complaints:• Seven day history of nasal congestion and headaches
• Productive cough for the last two days
• Concerned about coughing up yellow-green phlegm
Has taken paracetamol to relieve headache
(500mg, two-three times daily)
Medical history
• Mild, intermittent asthma as a child
• Not using a bronchodilator or preventative therapy
• No known allergies
Jessica
Examination
• 37.5 oC
• Respiratory rate 20/minute
• Pulse rate 84 beats/minute
• Blood pressure 120/80
• Auscultation of chest– Normal breath sounds
– Occasional wheeze
– Heart sounds normal
JessicaWhat does Jessica possibly have?
? A common cold – viral URTI
? Rhinosinusitis
? Acute bronchitis
? Influenza
? Pneumonia
? Exacerbation of asthma
3
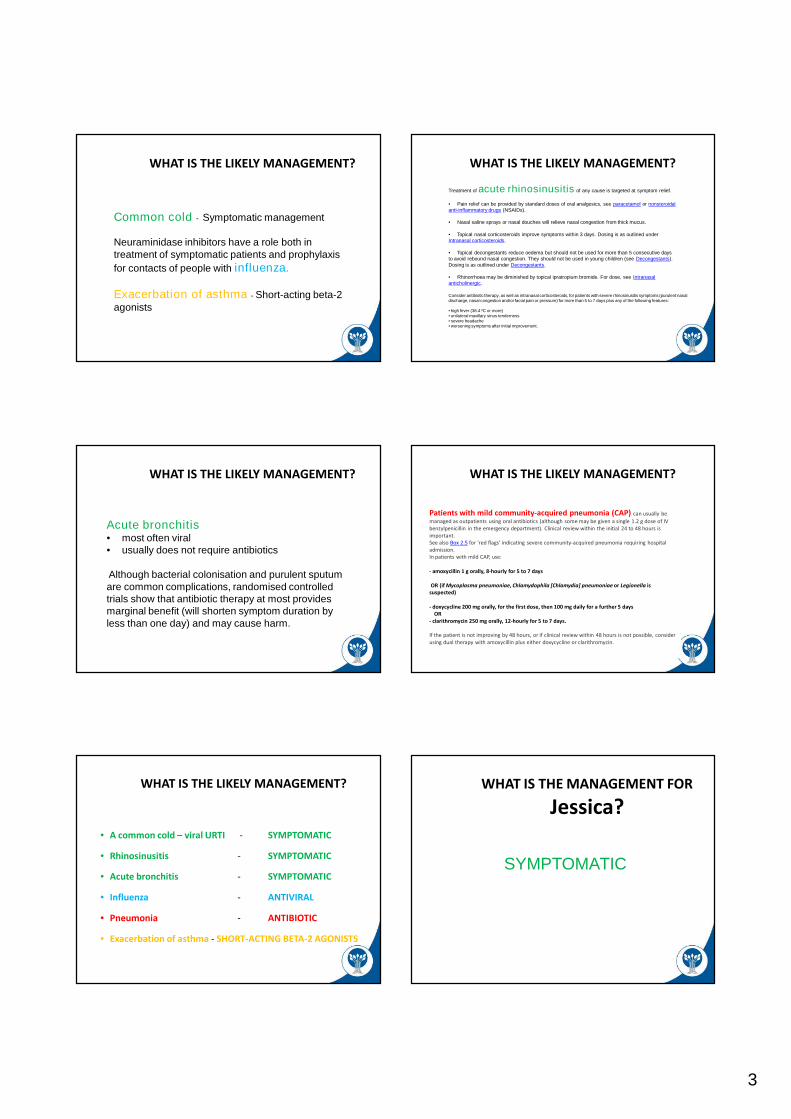
WHAT IS THE LIKELY MANAGEMENT?
Common cold - Symptomatic management
Neuraminidase inhibitors have a role both intreatment of symptomatic patients and prophylaxis
for contacts of people with influenza.
Exacerbation of asthma - Short-acting beta-2agonists
WHAT IS THE LIKELY MANAGEMENT?
Treatment of acute rhinosinusitis of any cause is targeted at symptom relief.
• Pain relief can be provided by standard doses of oral analgesics, see paracetamol or nonsteroidalanti-inflammatory drugs (NSAIDs).
• Nasal saline sprays or nasal douches will relieve nasal congestion from thick mucus.
• Topical nasal corticosteroids improve symptoms within 3 days. Dosing is as outlined underIntranasal corticosteroids.
• Topical decongestants reduce oedema but should not be used for more than 5 consecutive daysto avoid rebound nasal congestion. They should not be used in young children (see Decongestants).Dosing is as outlined under Decongestants.
• Rhinorrhoea may be diminished by topical ipratropium bromide. For dose, see Intranasalanticholinergic.
Consider antibiotic therapy, as well as intranasal corticosteroids, for patients with severe rhinosinusitis symptoms (purulent nasaldischarge, nasal congestion and/or facial pain or pressure) for more than 5 to 7 days plus any of the following features:
• high fever (38.4 ºC or more)• unilateral maxillary sinus tenderness• severe headache• worsening symptoms after initial improvement.
WHAT IS THE LIKELY MANAGEMENT?
Acute bronchitis• most often viral• usually does not require antibiotics
Although bacterial colonisation and purulent sputumare common complications, randomised controlledtrials show that antibiotic therapy at most providesmarginal benefit (will shorten symptom duration byless than one day) and may cause harm.
WHAT IS THE LIKELY MANAGEMENT?
Patients with mild community-acquired pneumonia (CAP) can usually be
managed as outpatients using oral antibiotics (although some may be given a single 1.2 g dose of IVbenzylpenicillin in the emergency department). Clinical review within the initial 24 to 48 hours isimportant.See also Box 2.5 for 'red flags' indicating severe community-acquired pneumonia requiring hospitaladmission.In patients with mild CAP, use:
- amoxycillin 1 g orally, 8-hourly for 5 to 7 days
OR (if Mycoplasma pneumoniae, Chlamydophila [Chlamydia] pneumoniae or Legionella issuspected)
- doxycycline 200 mg orally, for the first dose, then 100 mg daily for a further 5 daysOR
- clarithromycin 250 mg orally, 12-hourly for 5 to 7 days.
If the patient is not improving by 48 hours, or if clinical review within 48 hours is not possible, considerusing dual therapy with amoxycillin plus either doxycycline or clarithromycin.
WHAT IS THE LIKELY MANAGEMENT?
• A common cold – viral URTI - SYMPTOMATIC
• Rhinosinusitis - SYMPTOMATIC
• Acute bronchitis - SYMPTOMATIC
• Influenza - ANTIVIRAL
• Pneumonia - ANTIBIOTIC
• Exacerbation of asthma - SHORT-ACTING BETA-2 AGONISTS
WHAT IS THE MANAGEMENT FOR
Jessica?
SYMPTOMATIC

4
Doctor – Patient Communication Doctor – Patient Communication
Patient beliefs………. what are they?
Adults believed that:
• Antibiotics needed for bacterial infection 93.3%
• Antibiotics needed for sore throat 3%
But…if sick enough to see GP:
• Antibiotics required for sore throats, runny nose andcough when they had a fever 53%
Sydney 2008 survey
Australian community survey
Proportion of Australian adults believed thatantibiotics are always or nearly always appropriatefor managing a cold/flu (by age groups), 2006
Patient expectations …..what are they?
Patients visiting GPs with acute RTIs:
• 50% expected antibiotics
• 90% expected information/reassurance*
*Welschen I, Clinical practice 2004
Patient expectations andprescriptions for antibiotics
Doctors’ perceptions stronger determinant of ABprescribing than pts’ actual preference:
• Likelihood is 10 times more for patient to receive amedication when GPs think that patient wants it*
• Receiving antibiotic in the past – expectation forantibiotic in the future
*Cockburn J, BMJ 1997
5
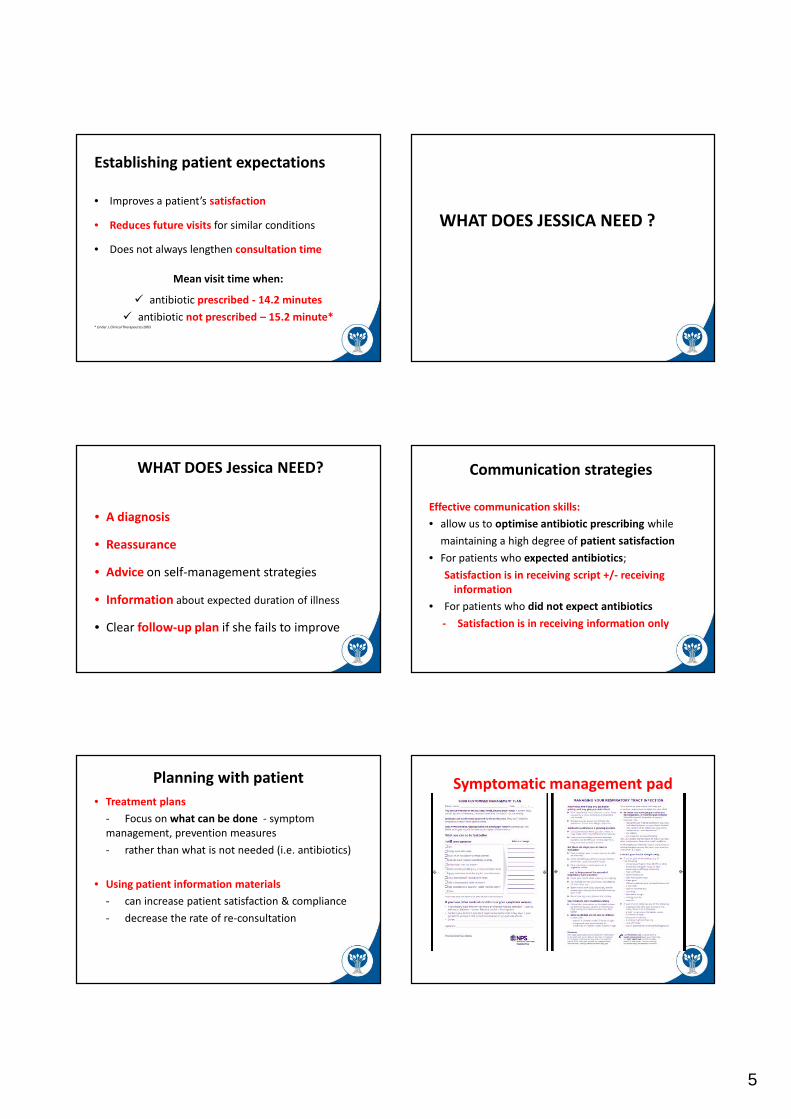
Establishing patient expectations
• Improves a patient’s satisfaction
• Reduces future visits for similar conditions
• Does not always lengthen consultation time
Mean visit time when:
antibiotic prescribed - 14.2 minutes
antibiotic not prescribed – 15.2 minute** Linder J, Clinical Therapeutics2003
WHAT DOES JESSICA NEED ?
WHAT DOES Jessica NEED?
• A diagnosis
• Reassurance
• Advice on self-management strategies
• Information about expected duration of illness
• Clear follow-up plan if she fails to improve
Communication strategies
Effective communication skills:
• allow us to optimise antibiotic prescribing while
maintaining a high degree of patient satisfaction
• For patients who expected antibiotics;
Satisfaction is in receiving script +/- receivinginformation
• For patients who did not expect antibiotics
- Satisfaction is in receiving information only
Planning with patient
• Treatment plans
- Focus on what can be done - symptommanagement, prevention measures
- rather than what is not needed (i.e. antibiotics)
• Using patient information materials
- can increase patient satisfaction & compliance
- decrease the rate of re-consultation
Symptomatic management pad
6
Doctor – Patient CommunicationIssues of resistance when
prescribing
• After the antibiotic stops, resistant bacterialeave the body slowly
they may have the opportunity to ‘invade’later and cause disease
they can continue to be spread to otherpeople over a long period of time
• The longer the exposure, the more likely it willbe that resistant bacteria are spread to others
THE ANTIBIOTIC CREED
M microbiology guides therapy wherever possible
I indications should be evidence-based
N narrowest spectrum required
D dosage appropriate to the site and type of infection
M minimise duration of therapy
E ensure monotherapy in most situations
Sullivan and Nicolaides Respiratory pathogen antibiogram
Alfred Hospital, MELBOURNE 1994
(Fuller A, et al ANZ J Med 1995;25:572)
228 patients, 130 etiology determined (56%)
C pneumoniae 14.5%
S pneumoniae 8.8%
P jiroveci 8.8%
Haemophilus sp. 7.0%
Ps aeruginosa 3.9%
Legionella 3.9%
S aureus 3.1%
Klebsiella 2.6%
M tuberculosis 2.6%
M catarrhalis 2.2%
Etiology of pneumonia, 1994 Etiology of pneumonia, 2006

7
% SUSCEPTIBLE
Freq(%)
P G E/R CTR TIM AUG
Pneumococcus 50 97 0 85 99 97 97
C pneumoniae 10 0 0 100 0 0 0
H influenzae 8 85 0 - 100 100 100
M pneumoniae 6 0 0 100 0 0 0
Gram negatives 5 0 100 0 90 90 90
Legionella 3 0 0 100 0 0 0
Tuberculosis 3 0 0 0 0 0 0
Viruses and others 15 - - - - - -
D Looke 1995
CAP antibiogramCAP antibiogram
based on ACAPS study Aust 2006Organism Freq(%) Pen Aug Rox Dox Zin Cro Tim
Unknown 54 ? ? ? ? ? ? ?
S pneum 14 95 95 73 72 95 95 68
M pneum 9 0 0 100 100 0 0 0
Influenza 8 0 0 0 0 0 0 0
Picorna 5 0 0 0 0 0 0 0
H flu 5 72 99 ? ? 99 99 99
Legion 3 0 0 100 100 0 0 0
RSV 2 0 0 0 0 0 0 0
Chlam 2 0 0 100 100 0 0 0
Ps aerug 1 0 0 0 0 0 0 98
GNBs 1 0 85 0 0 90 95 95
S aureus 1 5 85 80 80 85 50 85
M catarrh 1 0 100 ? ? 100 100 100
Other 2 ? ? ? ? ? ? ?
David Looke 2012
Key messages• Antibiotic resistance requires consideration at both a
population and individual level
• Establish a patient’s beliefs and expectations about
antibiotics for acute RTIs and tailor communication
strategies accordingly
• Encourage self-management of acute RTIs and explain why
antibiotics may not be appropriate
• Consider the issue of resistance when prescribing antibiotics
Diagnostic imaging pathways: Measurement of radiation dose
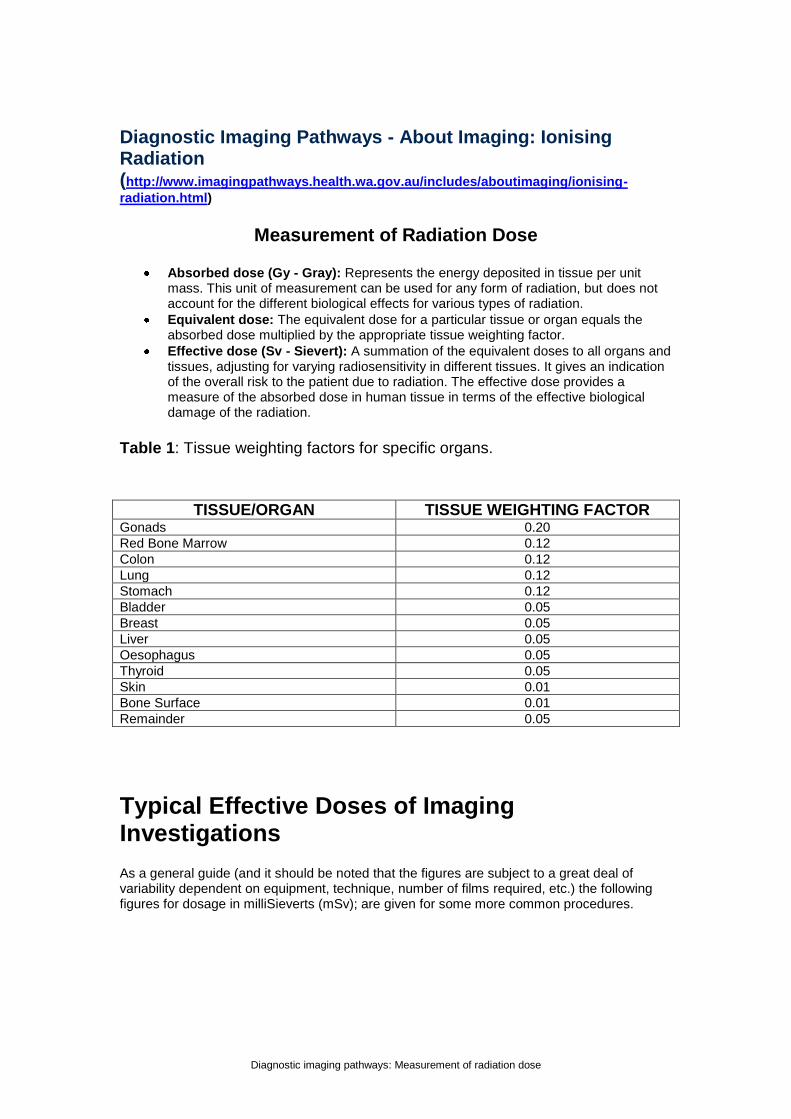
Diagnostic Imaging Pathways - About Imaging: Ionising Radiation (http://www.imagingpathways.health.wa.gov.au/includes/aboutimaging/ionising-
radiation.html)
Measurement of Radiation Dose
Absorbed dose (Gy - Gray): Represents the energy deposited in tissue per unit mass. This unit of measurement can be used for any form of radiation, but does not account for the different biological effects for various types of radiation.
Equivalent dose: The equivalent dose for a particular tissue or organ equals the absorbed dose multiplied by the appropriate tissue weighting factor.
Effective dose (Sv - Sievert): A summation of the equivalent doses to all organs and tissues, adjusting for varying radiosensitivity in different tissues. It gives an indication of the overall risk to the patient due to radiation. The effective dose provides a measure of the absorbed dose in human tissue in terms of the effective biological damage of the radiation.
Table 1: Tissue weighting factors for specific organs.
TISSUE/ORGAN TISSUE WEIGHTING FACTOR Gonads 0.20
Red Bone Marrow 0.12
Colon 0.12
Lung 0.12
Stomach 0.12
Bladder 0.05
Breast 0.05
Liver 0.05
Oesophagus 0.05
Thyroid 0.05
Skin 0.01
Bone Surface 0.01
Remainder 0.05
Typical Effective Doses of Imaging Investigations
As a general guide (and it should be noted that the figures are subject to a great deal of variability dependent on equipment, technique, number of films required, etc.) the following figures for dosage in milliSieverts (mSv); are given for some more common procedures.

Diagnostic imaging pathways: Measurement of radiation dose
Table 2: Typical effective doses for common procedures.
IMAGING INVESTIGATION
EFFECTIVE DOSE (mSv)
EQUIVALENT NUMBER OF CHEST XRAYS
EQUIVALENT PERIOD OF NATURAL
RADIATION
PLAIN RADIOGRAPHY
Extremities 0.01 0.50 1.5 days
Chest 0.02 1.00 3 days
Skull 0.07 3.50 11 days
Cervical Spine 0.10 5.00 15 days
Thoracic Spine 0.70 35.0 4 months
Lumbar Spine 1.30 65.0 7 months
Hip 0.30 15.0 7 weeks
Pelvis 0.70 35.0 4 months
Abdomen 1.00 50.0 6 months
IVP 2.50 125 14 months
Barium Swallow 1.50 75.0 8 months
Barium Meal 3.00 150 16 months
Barium Follow through 3.00 150 16 months
Barium Enema 7.00 350 3.2 years
COMPUTED TOMOGRAPHY
Head 2.30 115 1 year
Cervical Spine 1.50 75.0 8 months
Thoracic Spine 6.00 300 2.5 years
Chest 8.00 400 3.6 years
Lumbar Spine 3.30 165 1.4 years
Abdomen 10.0 500 4.5 years
Pelvis 10.0 500 4.5 years
NUCLEAR MEDICINE
Bone Imaging (Tc-99m) 4.00 200 1.6 years
Cerebral Perfusion (Tc-99m)
5.00 250 2.0 years
Lung Ventilation (Xe-133) 0.30 15.0 7 weeks
Lung Perfusion (Tc-99m) 1.00 50.0 6 months
Myocardial Perfusion (Tc-99m)
6.00 300 2.5 years
Myocardial Imaging (FDG-PET)
10.0 500 4.0 years
Thyroid Imaging (Tc-99m) 1.00 50.0 6 months
DTPA Renogram 2.00 100 10 months
DMSA Renogram 0.70 35.0 3.5 months
HIDA Hepatobilliary Imaging
2.30 115 1.0years
Diagnostic imaging pathways: Measurement of radiation dose
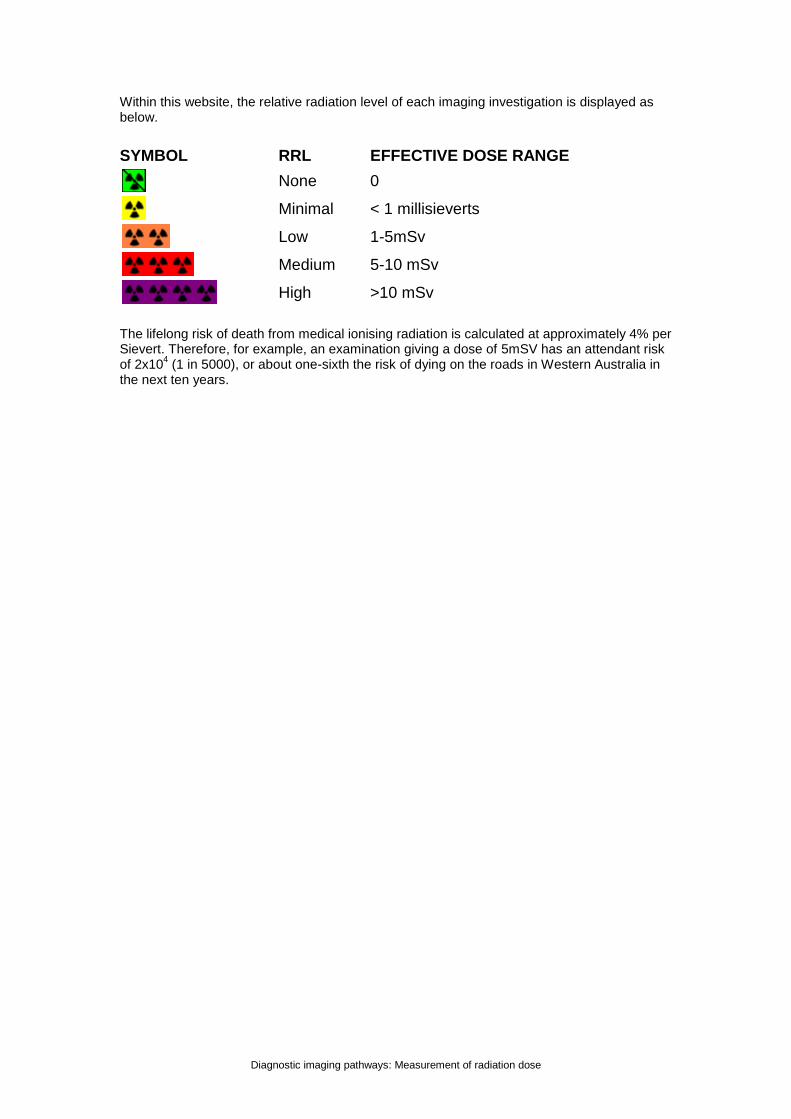
Within this website, the relative radiation level of each imaging investigation is displayed as below.
SYMBOL RRL EFFECTIVE DOSE RANGE
None 0
Minimal < 1 millisieverts
Low 1-5mSv
Medium 5-10 mSv
High >10 mSv
The lifelong risk of death from medical ionising radiation is calculated at approximately 4% per Sievert. Therefore, for example, an examination giving a dose of 5mSV has an attendant risk of 2x10
4 (1 in 5000), or about one-sixth the risk of dying on the roads in Western Australia in
the next ten years.
bulletinSNP Antibiogram – Respiratory Pathogens 2004 – 2010 comparison Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis
The trend for nonsusceptibility (Intermediate + Resistant) to penicillin for S pneumoniae has increased since 2004. 9.4% of isolates are resistant i.e. the minimum inhibitory concentration (MIC) is ≥ 2 mg/L, compared to 2.4% in 2004. Approximately 23.4% of isolates have intermediate susceptibility, i.e. MIC. of 0.12mg/L to 1 mg/L. Although infections with isolates of intermediate susceptibility will generally respond to higher doses of conventional beta-lactam antibiotics (penicillin, amoxycillin), treatment failures have occurred when such organisms have caused meningitis. Pneumonia caused by S pneumoniae can generally be successfully treated with parenteral pencillin when the penicillin MIC is as high as 2 mg/L (see Table 1). Susceptibility testing of the third generation cephalosporins (ceftriaxone, cefotaxime) is only routinely performed on penicillin intermediate or resistant S pneumoniae. The 10.2% resistance and 26.9% intermediate susceptibility for ceftriaxone refers to this subset of isolates only. The few multiresistant S pneumoniae isolates tested against the newer generation quinolone, moxifloxacin, (n = 26) were all susceptible. Macrolide resistance (erythromycin, clarithromycin) for S pneumoniae has also increased from 19% to 27.4%. The corresponding resistance rates for clindamycin in 2004 and 2010 are 14.5% and 24% respectively. Clindamycin resistance is only slightly less than that of erythromycin, indicating that most erythromycin/clindamycin resistance is mediated by the same erm gene that encodes for erythromycin ribosome methylase, rather than an independent efflux method. Erythromycin is unsuitable for treatment of H influenzae infections. There are proponents for treatment of H influenzae with the related macrolides (roxithromycin, clarithromycin). In this series, 88.4% tested susceptible. This has been an increase since 2004. Most M catarrhalis are susceptible in vitro to the macrolides, erythromycin and clarithromycin (99.1%), and these can be used effectively to treat these infections.
Cotrimoxazole is not recommended for treatment of respiratory tract infections. 26.6% of S pneumoniae isolates (n = 1296), 30.9% of H influenzae (n = 3932) and 1.9% of M catarrhalis isolates (n = 976) are resistant. Tetracycline (including doxycycline) is generally not effective for empiric therapy of S pneumoniae (n = 1296) showing 21.8% resistance and increase from 2004 when the rate was 12.8%. H influenzae (n = 3932) resistance rates for tetracycline are 0.2% (a suprising decrease from 14.6% in 2004), and 0.3% for M catarrhalis isolates (n = 976) which is not significantly different from resistance rates of 0.9% in 2004. Beta-lactamase production by H influenzae (n = 3932), and consequent resistance to amoxycillin/ampicillin, occurs in 23.2% of isolates in 2010, in contrast to 21.4% in 2004. Alternative treatment is co-amoxyclav, although there is a small number of beta-lactamase negative amoxicillin/ampicillin resistant isolates (BLNAR). 1.0% of a total number of 3893 H influenzae isolates would not be effectively treated by the addition of clavulanate as in co-amoxyclav in 2010. In contrast, in 2004 the rate was 2.6%. Beta-lactamase production is very common in M catarrhalis isolates (96.95%). Infections with this organism can be effectively treated with co-amoxyclav. Fluoroquinolone resistance (moxifloxacin) remains rare and is the treatment of choice for multidrug resistant pneumococcus.
Table 1 Penicillin susceptibility definitions for S pneumoniae
Susceptible Intermediate Resistant Penicillin parenteral(Meningitis) ≤ 0.06 mg/L - ≥ 0.12 mg/L
Penicillin parenteral(non Meningitis) ≤ 2 mg/L 4 mg/L ≥ 8 mg/L
Penicillin oral ≤ 0.06 mg/L ≥ 0.12 – 1 mg/L ≥ 2 mg/L

SULLIVAN NICOLAIDES PTY LTD • ABN 38 078 202 196 134 WHITMORE STREET • TARINGA • QLD 4068 • AUSTRALIA
TEL (07) 3377 8666 • FAX (07) 3870 0549 MAIL ADDRESS • P O BOX 344 • INDOOROOPILLY • QLD 4068 • AUSTRALIA
www.snp.com.au
Item 05816Correct at time of printing – reviewed July 2011For further information visit our website www.snp.com.au
Dr Jenny Robson FRCPA FRACP FACTMDr Jenny Robson graduated from The University of Queensland and has worked at Sullivan Nicolaides Pathology since 1989. She is interested in all things infectious, but particularly zoonoses, immunisation, tropical and travel medicine, antibiotic resistance, infection control, and the molecular diagnosis of infectious diseases.Dr Robson is available for consultation.T: (07) 3377 8506E: [email protected] Sarah Cherian FRCPADr Sarah Cherian graduated from The University of Queensland and worked with the Brisbane Southside Public Health Unit before joining Sullivan Nicolaides Pathology in 2001. Sarah’s interests include public health, microbiology, hepatitis testing, and molecular diagnosis of infectious diseases.Dr Cherian is available for consultation.T: (07) 3377 8628E: [email protected]
SNP Antibiogram – Respiratory Pathogens 2004 – 2010 comparison Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis cont...
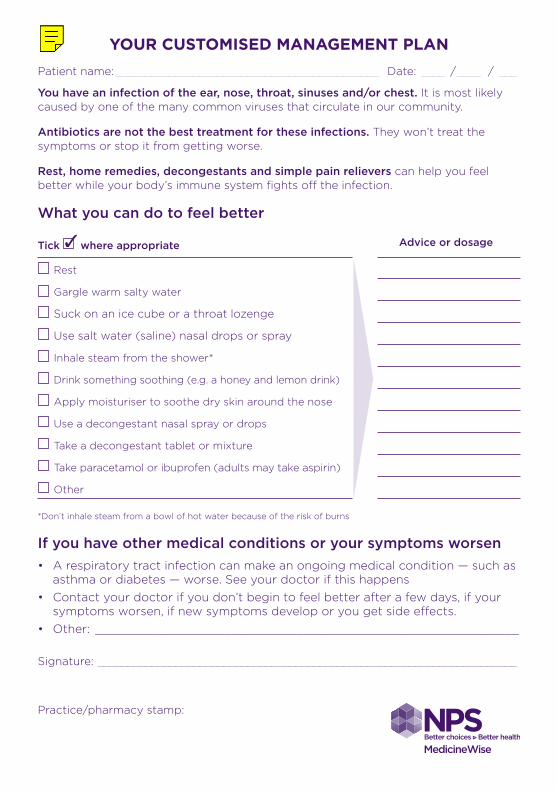
YOUR CUSTOMISED MANAGEMENT PLANPatient name: ____________________________________________ Date: ____ / ____ / ___
You have an infection of the ear, nose, throat, sinuses and/or chest. It is most likely caused by one of the many common viruses that circulate in our community.
Antibiotics are not the best treatment for these infections. They won’t treat the symptoms or stop it from getting worse.
Rest, home remedies, decongestants and simple pain relievers can help you feel better while your body’s immune system fights off the infection.
What you can do to feel better
Tick where appropriate Advice or dosage
Rest
Gargle warm salty water
Suck on an ice cube or a throat lozenge
Use salt water (saline) nasal drops or spray
Inhale steam from the shower*
Drink something soothing (e.g. a honey and lemon drink)
Apply moisturiser to soothe dry skin around the nose
Use a decongestant nasal spray or drops
Take a decongestant tablet or mixture
Take paracetamol or ibuprofen (adults may take aspirin)
Other
*Don’t inhale steam from a bowl of hot water because of the risk of burns
If you have other medical conditions or your symptoms worsen• A respiratory tract infection can make an ongoing medical condition — such as
asthma or diabetes — worse. See your doctor if this happens• Contact your doctor if you don’t begin to feel better after a few days, if your
symptoms worsen, if new symptoms develop or you get side effects. • Other: ___________________________________________________________
Signature: ______________________________________________________________________
Practice/pharmacy stamp:
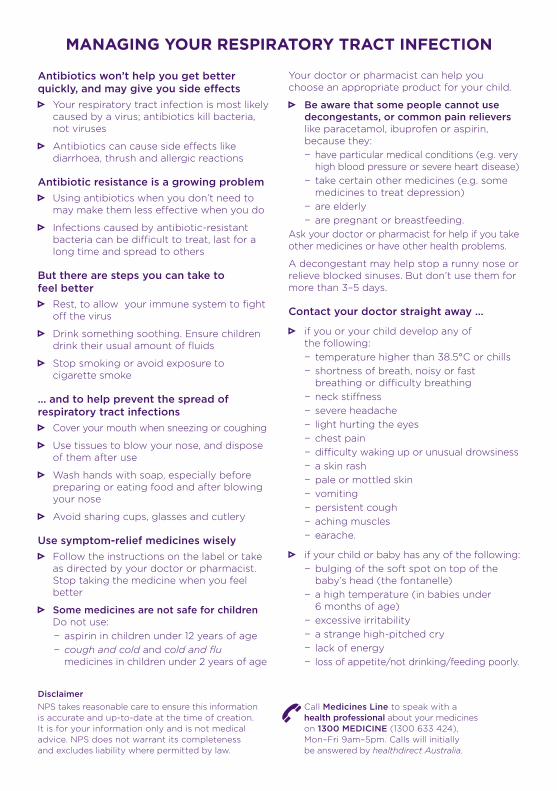
MANAGING YOUR RESPIRATORY TRACT INFECTION
Antibiotics won’t help you get better quickly, and may give you side effects
Your respiratory tract infection is most likely caused by a virus; antibiotics kill bacteria, not viruses
Antibiotics can cause side effects like diarrhoea, thrush and allergic reactions
Antibiotic resistance is a growing problem Using antibiotics when you don’t need to
may make them less effective when you do
Infections caused by antibiotic-resistant bacteria can be difficult to treat, last for a long time and spread to others
But there are steps you can take to feel better
Rest, to allow your immune system to fight off the virus
Drink something soothing. Ensure children drink their usual amount of fluids
Stop smoking or avoid exposure to cigarette smoke
… and to help prevent the spread of respiratory tract infections
Cover your mouth when sneezing or coughing
Use tissues to blow your nose, and dispose of them after use
Wash hands with soap, especially before preparing or eating food and after blowing your nose
Avoid sharing cups, glasses and cutlery
Use symptom-relief medicines wisely Follow the instructions on the label or take
as directed by your doctor or pharmacist. Stop taking the medicine when you feel better
Some medicines are not safe for children Do not use:
− aspirin in children under 12 years of age − cough and cold and cold and flu medicines in children under 2 years of age
Your doctor or pharmacist can help you choose an appropriate product for your child.
Be aware that some people cannot use decongestants, or common pain relievers like paracetamol, ibuprofen or aspirin, because they:
− have particular medical conditions (e.g. very high blood pressure or severe heart disease)
− take certain other medicines (e.g. some medicines to treat depression)
− are elderly − are pregnant or breastfeeding.
Ask your doctor or pharmacist for help if you take other medicines or have other health problems.
A decongestant may help stop a runny nose or relieve blocked sinuses. But don’t use them for more than 3–5 days.
Contact your doctor straight away …
if you or your child develop any of the following:
− temperature higher than 38.5°C or chills − shortness of breath, noisy or fast breathing or difficulty breathing
− neck stiffness − severe headache − light hurting the eyes − chest pain − difficulty waking up or unusual drowsiness − a skin rash − pale or mottled skin − vomiting − persistent cough − aching muscles − earache.
if your child or baby has any of the following: − bulging of the soft spot on top of the baby’s head (the fontanelle)
− a high temperature (in babies under 6 months of age)
− excessive irritability − a strange high-pitched cry − lack of energy − loss of appetite/not drinking/feeding poorly.
DisclaimerNPS takes reasonable care to ensure this information is accurate and up-to-date at the time of creation. It is for your information only and is not medical advice. NPS does not warrant its completeness and excludes liability where permitted by law.
Call Medicines Line to speak with a health professional about your medicines on 1300 MEDICINE (1300 633 424), Mon–Fri 9am–5pm. Calls will initially be answered by healthdirect Australia.
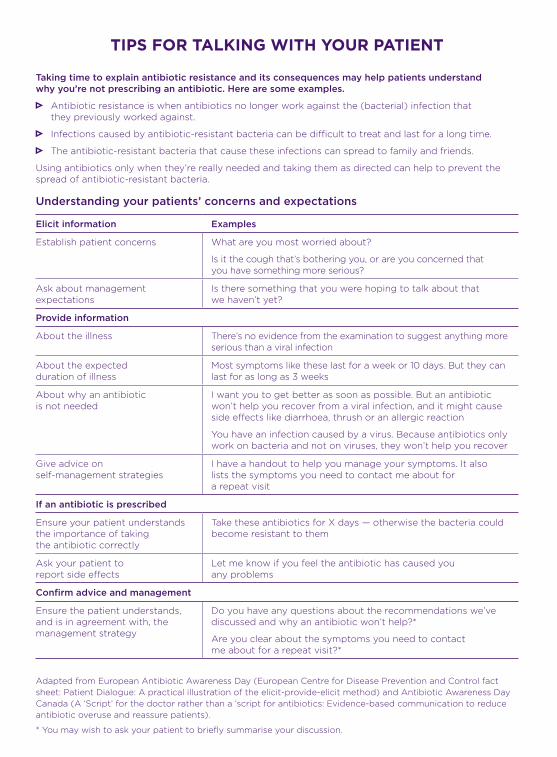
tips for tAlking with your pAtient
Taking time to explain antibiotic resistance and its consequences may help patients understand why you’re not prescribing an antibiotic. Here are some examples.
Antibiotic resistance is when antibiotics no longer work against the (bacterial) infection that they previously worked against.
Infections caused by antibiotic-resistant bacteria can be difficult to treat and last for a long time.
The antibiotic-resistant bacteria that cause these infections can spread to family and friends.
Using antibiotics only when they’re really needed and taking them as directed can help to prevent the spread of antibiotic-resistant bacteria.
Understanding your patients’ concerns and expectations
Elicit information Examples
Establish patient concerns What are you most worried about?
Is it the cough that’s bothering you, or are you concerned that you have something more serious?
Ask about management expectations
Is there something that you were hoping to talk about that we haven’t yet?
Provide information
About the illness There’s no evidence from the examination to suggest anything more serious than a viral infection
About the expected duration of illness
Most symptoms like these last for a week or 10 days. But they can last for as long as 3 weeks
About why an antibiotic is not needed
I want you to get better as soon as possible. But an antibiotic won’t help you recover from a viral infection, and it might cause side effects like diarrhoea, thrush or an allergic reaction
You have an infection caused by a virus. Because antibiotics only work on bacteria and not on viruses, they won’t help you recover
Give advice on self-management strategies
I have a handout to help you manage your symptoms. It also lists the symptoms you need to contact me about for a repeat visit
If an antibiotic is prescribed
Ensure your patient understands the importance of taking the antibiotic correctly
Take these antibiotics for X days — otherwise the bacteria could become resistant to them
Ask your patient to report side effects
Let me know if you feel the antibiotic has caused you any problems
Confirm advice and management
Ensure the patient understands, and is in agreement with, the management strategy
Do you have any questions about the recommendations we’ve discussed and why an antibiotic won’t help?*
Are you clear about the symptoms you need to contact me about for a repeat visit?*
Adapted from European Antibiotic Awareness Day (European Centre for Disease Prevention and Control fact sheet: Patient Dialogue: A practical illustration of the elicit-provide-elicit method) and Antibiotic Awareness Day Canada (A ‘Script’ for the doctor rather than a ‘script for antibiotics: Evidence-based communication to reduce antibiotic overuse and reassure patients).
* You may wish to ask your patient to briefly summarise your discussion.