antibiotic prophylaxis
DESCRIPTION
A presentation on the antibiotic prophylaxis in dental patientsTRANSCRIPT


Review of Antibiotics
and Indications forProphylaxis
Dent Clin N Am 56 (2012) 235–244
INFECTIVE ENDOCARDITIS
• IE is an uncommon, but life-threatening infection of the inner lining of the heart (endocardium)
• It is characterized by the presence of vegetations composed of– Platelets– Fibrin– Microorganisms– Inflammatory cells
• Endothelial damage caused by turbulent blood flow normally seen in congenital or acquired heart disease causes platelets and fibrin deposition leading to formation of nonbacterial thrombotic endocarditis (NBTE)

INFECTIVE ENDOCARDITIS
• In this environment, an incidence of bacteremia could result in bacterial adherence to NBTE, bacterial proliferation within the NBTE, and formation of vegetations
• IE most commonly occurs in conjunction with – Invasive dental – Gastrointestinal (GI)– Genitourinary (GU) tract procedures
INFECTIVE ENDOCARDITIS
• Certain underlying cardiac conditions may predispose an individual to developing endocarditis, such as artificial heart valves
• If left untreated, endocarditis can damage or destroy heart valves and can lead to life-threatening complications
• Often patients with IE have substantial morbidity and mortality despite technological and medical advancements

WHY WERE THE PREVIOUS GUIDELINES CHANGED?
• AHA guidelines (1997) separated cardiac conditions into high-, moderate and low-risk (negligible risk) categories, with prophylaxis not advised for the low risk group
• A detailed list (of dental, respiratory, GI and GU, tract procedures for which prophylaxis was and was not recommended) was included
• It was found that the basis for recommendations for IE prophylaxis was not well-established, and the quality of evidence was not adequate
WHY WERE THE PREVIOUS GUIDELINES CHANGED?
• Number of cases of IE that could be prevented by antibiotic prophylaxis, even if 100% effective, is very small
• Most endocarditis cases caused by oral microflora are the result of bacteremia caused by routine daily activities (eg, tooth brushing and flossing)
• Thus, the current AHA guidelines shift the emphasis away from antibiotic prophylaxis for dental procedures and toward improved access to dental care and oral health for patients, especially those with underlying cardiac risk factors
WHY WERE THE PREVIOUS GUIDELINES CHANGED?
• Many authorities and advisory bodies have questioned the efficacy of antimicrobial prophylaxis to prevent endocarditis in patients who undergo a dental, GI, or GU tract procedure and have pushed for alterations to the 1997 AHA guidelines

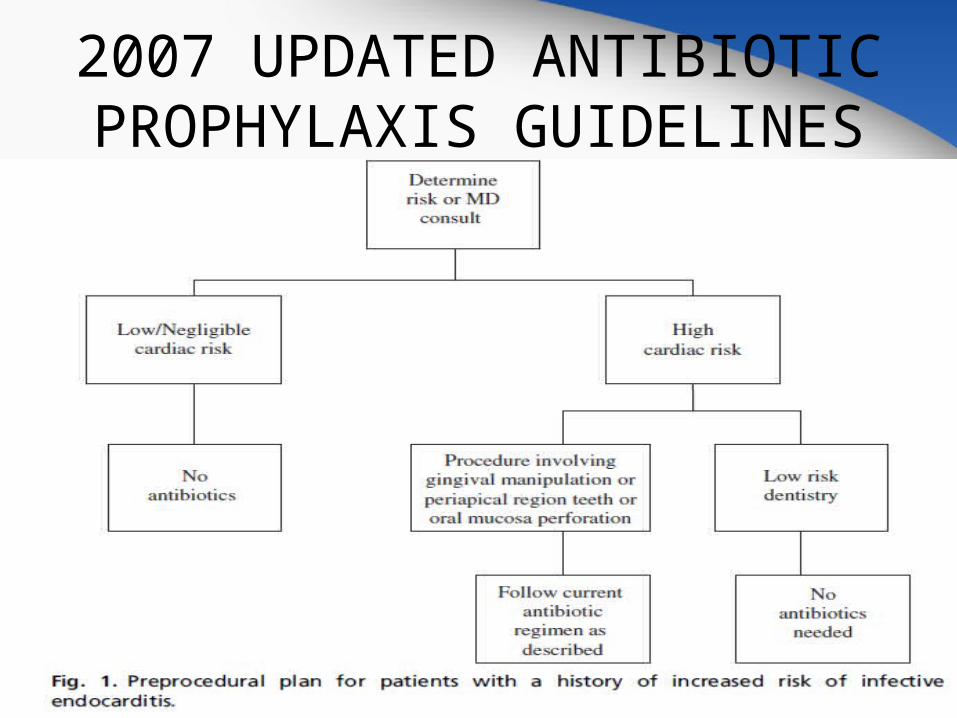
2007 UPDATED ANTIBIOTIC PROPHYLAXIS GUIDELINES
• AHA (2007) new guidelines suggest that antibiotic prophylaxis is reasonable for all dental procedures that involve manipulation of gingival tissues or the periapical region of teeth or perforation of oral mucosa only for patients with underlying cardiac conditions associated with the highest risk of adverse outcome from IE
• However, certain procedures do not require antibiotic prophylaxis, including the routine anesthetic injections through noninfected tissue, the taking of dental radiographs, the placement of removable prosthodontic or orthodontic appliances, and the adjustment of orthodontic appliances

2007 UPDATED ANTIBIOTIC PROPHYLAXIS GUIDELINES
• Cardiac conditions associated with the highest risk of adverse outcome from endocarditis for which prophylaxis with dental procedures is reasonable
1. Prosthetic cardiac valve or prosthetic material used for cardiac valve repair
2. Previous infective endocarditis
3. Congenital heart disease (CHD)a) Unrepaired cyanotic CHD, including palliative shunts and conduits
b) Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure
c) Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)
4. Cardiac transplantation recipients who develop cardiac valvulopathy
2007 UPDATED ANTIBIOTIC PROPHYLAXIS GUIDELINES
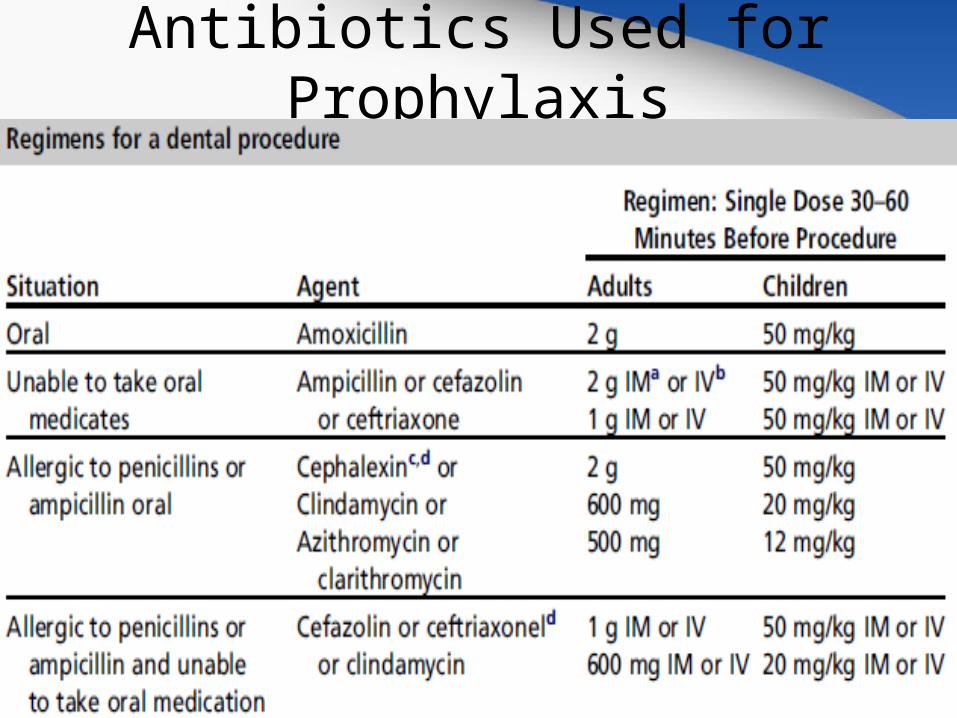
Antibiotics Used for Prophylaxis
Antibiotics Used for Prophylaxis
• Antibiotics should be given 30 to 60 minutes before starting the indicated procedure
• According to the AHA, if the drug is inadvertently omitted before the procedure, it may be administrated up to 2 hours after the procedure with some protective benefit

Antibiotics Used for Prophylaxis
• Penicillins
• Ampicillin and amoxicillin are aminopenicillins that have identical coverage as penicillin against the same non–beta-lactamase containing gram-positive pathogens
• This group has additional coverage against non–beta-lactamase producing strains of Haemophilus influenzae, Escherichia coli, Proteus mirabilis, Salmonella, and Shigella but lacks coverage against Pseudomonas aeruginosa
• Aminopenicillins have an increased incidence of drug hypersensitivity reactions with rashes as compared with other penicillins

Antibiotics Used for Prophylaxis
• Cephalosporins
• They can often be used in place of penicillins when patients have a history of mild rashes associated with penicillin use
• However, cephalosporins should not be used in patients who describe anaphylaxis, angioedema, urticaria, or asthma when using penicillin
Antibiotics Used for Prophylaxis
• Cephalosporins
• Cefazolin-----intravenous first-generation cephalosporin-----recommended for patients who those patients who are allergic to penicillin
• It has similar activity against most gram-positive cocci including Staphylococcus aureus, group A beta-hemolytic Streptococcus (Streptococcus pyogenes), and penicillin-susceptible Streptococcus pneumonia
Antibiotics Used for Prophylaxis
• Cephalosporins
• Cephalexin is also a first-generation oral cephalosporin and is most effective against Streptococcus pyogenes
• Ceftriaxone is a third-generation cephalosporin that covers many important infections because of its broad coverage, high potency etc.
• However, this agent has less activity against gram-positive pathogens compared with the first-generation cephalosporins
Antibiotics Used for Prophylaxis
• Macrolides
• Clarithromycin and azithromycin are commonly used to treat infections caused by gram-positive bacteria, Streptococcus pneumoniae, and Haemophilus influenzae infections such as respiratory tract and soft-tissue infections
• The antimicrobial spectrum of macrolides is slightly wider than that of penicillin, and, therefore, macrolides remain a common alternative for patients with a penicillin allergy
• Concerns with macrolide antibiotics include GI distress, drug–drug interactions, and QT prolongation

Antibiotics Used for Prophylaxis
• Lincosamides
• Clindamycin is a semisynthetic derivative of lincomycin
• It is bacteriostatic by inhibiting protein synthesis
• Clindamycin is an excellent agent for the treatment of infections of the oral cavity and is effective against most pneumococci and streptococci and most penicillin-resistant staphylococci including some methicillin-resistant Staphylococcus aureus (MRSA) isolates
Antibiotics Used for Prophylaxis
• Lincosamides
• Clostridium difficile pseudomembranous colitis is a complication that may occur after all antibacterial agents but has been linked most often with clindamycin
• Treatment includes discontinuation of the antibiotic and treatment with oral metronidazole, vancomycin, or nitazoxanide

Antibiotic Prophylaxis for Full Joint Replacement
• Joint guidelines were published in 2003 by the American Dental Association (ADA) and the American Academy of Orthopedic Surgeons (AAOS) regarding antibiotic prophylaxis for dental patients with total joint replacements
• They stated: “The risk/benefit and cost/effectiveness ratios fail to justify the administration of routine antibiotic prophylaxis” for individuals with joint replacements
• However, these guidelines also suggest that patients at greater risk because of specific medical conditions should be considered for prophylaxis
Antibiotic Prophylaxis for Full Joint Replacement
• These include patients
– whose prostheses are less than 2 years old– those who have high-risk conditions such as
• inflammatory arthropathies (rheumatoid arthritis, systemic lupus erythematosus)
• drug-induced or radiation-induced immunosuppression• previous joint infection• malnourishment• hemophilia• human immunodeficiency virus infection • insulin-dependent diabetes • Malignancy
Antibiotic Prophylaxis for Full Joint Replacement
• In February 2009, without a joint effort with organized dentistry or nonorthopedic physician specialties, the AAOS published what it called an “Information Statement” entitled “Antibiotic Prophylaxis for Bacteremia in Patients With Joint Replacements.”
• It stated: “Given the potential adverse outcomes and cost of treating an infected joint replacement, the AAOS recommends that clinicians consider antibiotic prophylaxis for all total joint replacement patients before any invasive procedure thatmay cause bacteremia.”

Antibiotic Prophylaxis for Full Joint Replacement
• In a position paper from the American Academy of Oral Medicine (AAOM), it was suggested that the statement issued by the AAOS was made with little or no scientific data to suggest a link between late prosthetic joint infections and organisms specific to the mouth
• Currently, the ADA and the AAOS are working together to develop evidence-based, clinical practice guidelines for antibiotic prophylaxis for dental patients with total joint replacement
Antibiotic Prophylaxis for Nonvalvular Cardiovascular
Devices
• Dental patients with nonvalvular cardiovascular devices (prosthetic valves, pacemakers, defibrillators, ventriculoatrial shunts, closure devices, patches, stents, vascular grafts, dacron grafts or patches, vena caval filters, vascular closure devices, total artificial hearts, and L ventricular assist devices) do not require antibiotic prophylaxis for dental treatment
• An exception involves patients with nonvalvular cardiovascular devices that undergo extraction or incision and drainage for infection, or to replace an infected device

Antibiotic Prophylaxis for Renal Dialysis Shunt
• The AHA does not recommend antibiotic prophylaxis for patients undergoing hemodialysis when they are receiving invasive dental procedures

Antibiotic Prophylaxis for Patients with
Immunosuppression secondary to cancer and cancer
chemotherapy
• The National Cancer Institute Web site suggests that patients with indwelling venous access lines and neutrophil counts between 1000 and 2000 mm3 receive the AHA-recommended regimen for antibiotics, with consideration given to a more aggressive antibiotic therapy in the presence of infection
Antibiotic Prophylaxis for Insulin-dependent diabetes
• Some articles and opinion papers suggest that patients with unstable, insulindependent diabetes should receive coverage with prophylactic antibiotics for invasive dental procedures
• Others, however, suggest prophylaxis only in the presence of an acute oral infection
Antibiotic Prophylaxis for Vascular Grafts
• Some texts and narrative review papers recommend and stress the importance of antibiotic prophylaxis
• In contrast, other authors have suggested that there is no indication for antibiotic prophylaxis.
Antibiotic Prophylaxis for Organ Transplants
• The new AHA IE prevention guidelines state that there is lack of evidence to support prophylaxis in heart transplant patients; however, the AHA did recommend it for those patients who developed cardiac valvulopathy
• As a general guideline, antibiotic prophylaxis for invasive dental procedures should be considered for patients with a suppressed immune response, regardless of the cause that is, neutropenia (<1000/mm3) or a low CD4 count (<200/mm3)
• The clinician and the patient’s physician should decide together whether antibiotic prophylaxis is required or not
Antibiotic Resistance
• Widespread use of antibiotic therapy promotes the emergence of resistant microorganisms most likely to cause endocarditis, such as viridans groupstreptococci and enterococci
• This increased resistance has reduced the efficacy and number of antibiotics available for the treatment of IE

Antibiotic Resistance
• Antibiotic resistance has also contributed to the rise of methicillin-resistant MRSA
• MRSA refers to Staphylococcus aureus that is resistant to all currently available b-lactam antimicrobial agents, including antistaphylococcal penicillins (methicillin, oxacillin, nafcillin) and cephalosporins
• Controlled use of antibiotics may be the key adjustable factor for the primary prevention of MRSA colonization
