antenatal care provider personas
TRANSCRIPT
IntroductionThis set of two user personas was developed to inform product development of new preeclampsia diagnostic tools, including new tests and digital tools, and explore perceptions related to taskshifting to self-monitoring. Preeclampsia is a dangerous complication in pregnancy characterized by hypertension and high levels of protein in urine (proteinuria). Danger signs of preeclampsia include frontal headaches, blurred vision, inflammation, abdominal pain, and shortness of breath. Preeclampsia can be life-threatening to both the mother and child if care is delayed or complications advance to eclampsia; however, the condition can be managed and prevented with adequate diagnosis and care.
In Ghana, community health nurses (CHNs) and midwives are currently responsible for diagnosis of preeclampsia and other pregnancy complications at the community level. For this reason, these personas focus on CHNs and midwives, who have complementary roles and challenges in providing antenatal care (ANC) to their communities.
Personas are a human-centered design method that communicate user needs and inform product design and delivery strategies. They typically capture characteristics and goals of the user group, including common behaviors, constraints, and motivations. Personas also represent the environment where the user group operates. Personas thus build a common understanding within multidisciplinary teams that can provide focus throughout the product development process, from defining functional product requirements to designing effective delivery strategies.
These personas were developed in a two-phased process. First, draft personas were created based on a usability study conducted by PATH and the Kintampo Health Research Centre in 2016. Observational and interview data were collected from midwives (n=8) and CHNs (n=10) from 11 different health facilities in the Kintampo North and South districts of the Brong-Ahafo Region. Results were validated and refined through secondary research and a follow-on study in 2020 that engaged additional midwives (n=15) and CHNs (n=5) from 19 facilities in the same two districts in focus group discussions and interviews.
Antenatal care provider personas
ContextThese user personas were developed to represent CHNs and midwives who work in ANC in Brong-Ahafo Region, Ghana.
Brong-Ahafo was the second-largest region in Ghana. It was made up of 27 districts and located in the midwestern part of the country (Figure 1). At least 21 different languages were spoken in the area. In 2014, it was home to more than 2.5 million people. The region had a total of 689 health facilities in 2014: 29 hospitals, 82 health centers, 112 clinics, 43 private maternity homes, and 423 functional community-based health planning and services (CHPS) compounds.1 Many facilities did not have access to technological tools such as computers, tablets, and mobile phones. (Note: Subsequent to our 2016 study, Brong-Ahafo was divided into three regions, Bono, Bono-East, and Ahafo. Kintampo North and South districts are located in Bono-East.)
Accra
Brong-Ahafo Region
Ghana
Figure 1. Brong-Ahafo Region in Ghana.
These personas were developed in collaboration with the Kintampo Health Research Centre, which
played a critical role in data collection, analysis, and write-up and dissemination of results for this
study. Special thanks to Charlotte Tawiah, Dennis Adu-Gyasi, Kwaku Poku Asante, and Sam Newton
for their guidance in the study and reviews of the personas to ensure they are representative of
the populations we work with. We would like to express our appreciation to the midwives and
community health nurses who participated in the study for sharing their experiences with us.
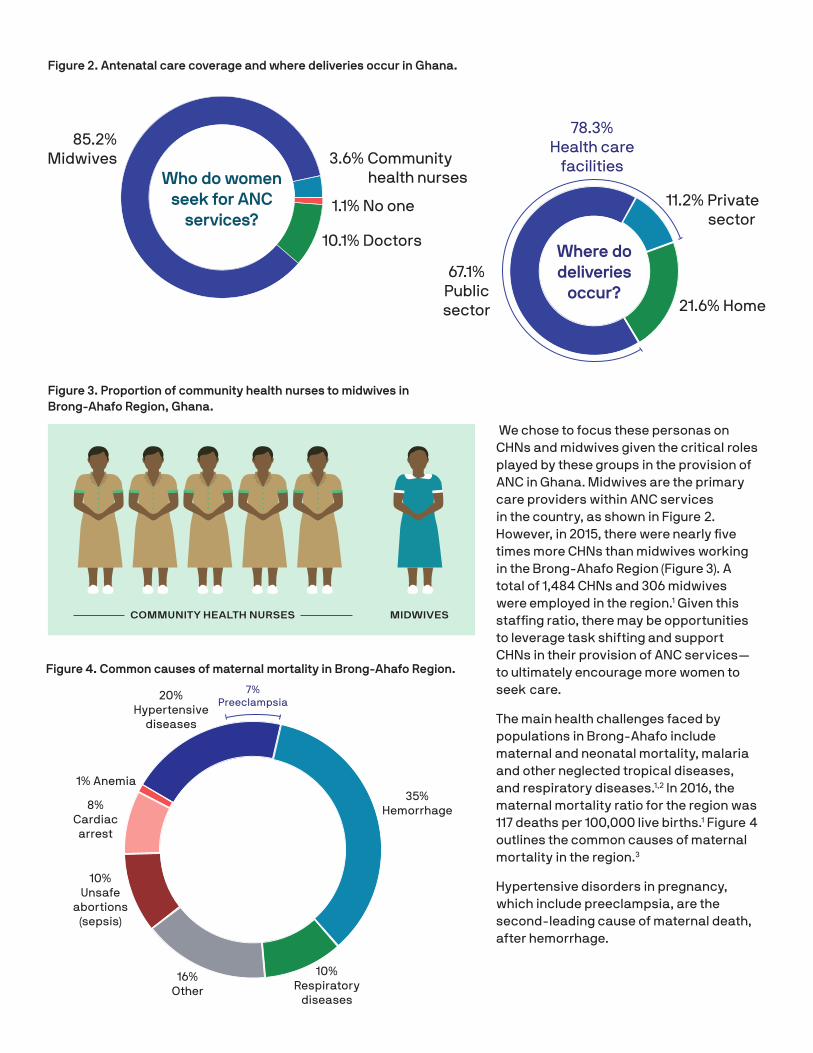
We chose to focus these personas on CHNs and midwives given the critical roles played by these groups in the provision of ANC in Ghana. Midwives are the primary care providers within ANC services in the country, as shown in Figure 2. However, in 2015, there were nearly five times more CHNs than midwives working in the Brong-Ahafo Region (Figure 3). A total of 1,484 CHNs and 306 midwives were employed in the region.1 Given this staffing ratio, there may be opportunities to leverage task shifting and support CHNs in their provision of ANC services—to ultimately encourage more women to seek care.
The main health challenges faced by populations in Brong-Ahafo include maternal and neonatal mortality, malaria and other neglected tropical diseases, and respiratory diseases.1,2 In 2016, the maternal mortality ratio for the region was 117 deaths per 100,000 live births.1 Figure 4 outlines the common causes of maternal mortality in the region.3
Hypertensive disorders in pregnancy, which include preeclampsia, are the second-leading cause of maternal death, after hemorrhage.
Figure 3. Proportion of community health nurses to midwives in Brong-Ahafo Region, Ghana.
Figure 2. Antenatal care coverage and where deliveries occur in Ghana.
Figure 4. Common causes of maternal mortality in Brong-Ahafo Region.
COMMUNITY HEALTH NURSES MIDWIVES
35% Hemorrhage
10% Respiratory
diseases
16% Other
10% Unsafe
abortions (sepsis)
8% Cardiac
arrest
1% Anemia
20% Hypertensive
diseases
7% Preeclampsia
10.1% Doctors
1.1% No one
3.6% Community health nursesWho do women
seek for ANC services?
85.2% Midwives
67.1% Public sector
11.2% Private sector
21.6% Home
78.3% Health care
facilities
Where do deliveries
occur?
Antenatal care provider persona
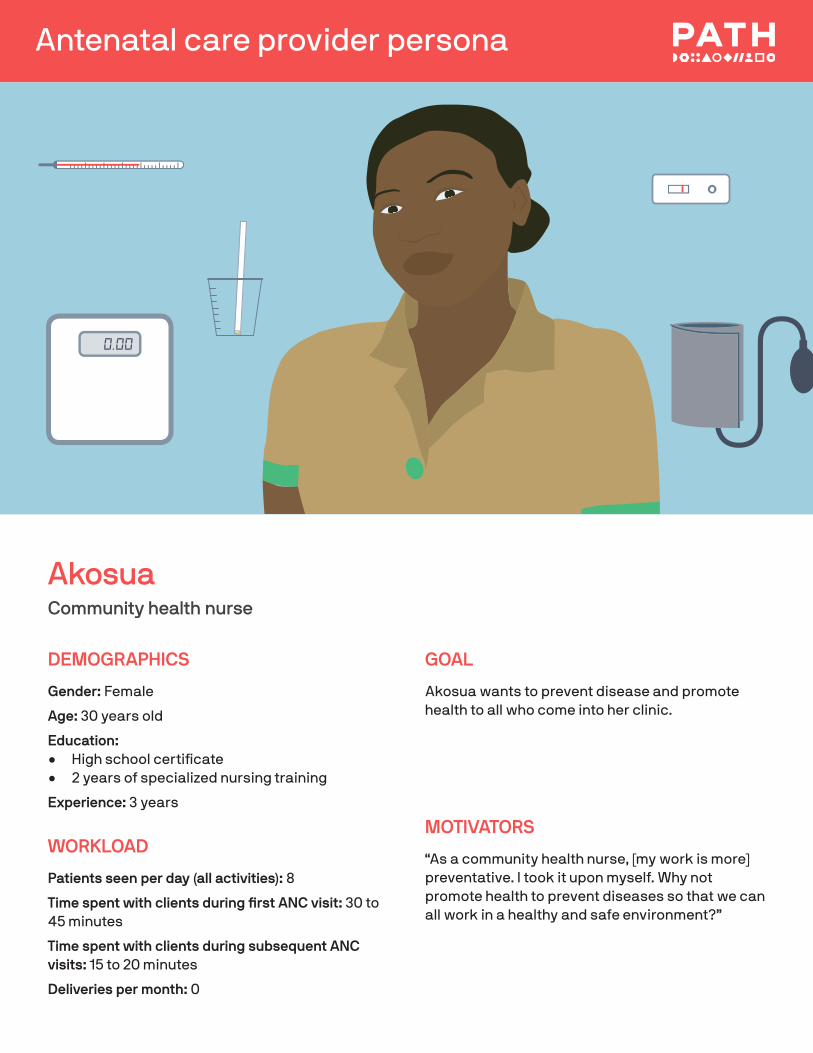
AkosuaCommunity health nurse
DEMOGRAPHICS
Gender: Female
Age: 30 years old
Education: • High school certificate• 2 years of specialized nursing training
Experience: 3 years
WORKLOAD
Patients seen per day (all activities): 8
Time spent with clients during first ANC visit: 30 to 45 minutes
Time spent with clients during subsequent ANC visits: 15 to 20 minutes
Deliveries per month: 0
GOAL
Akosua wants to prevent disease and promote health to all who come into her clinic.
MOTIVATORS
“As a community health nurse, [my work is more] preventative. I took it upon myself. Why not promote health to prevent diseases so that we can all work in a healthy and safe environment?”
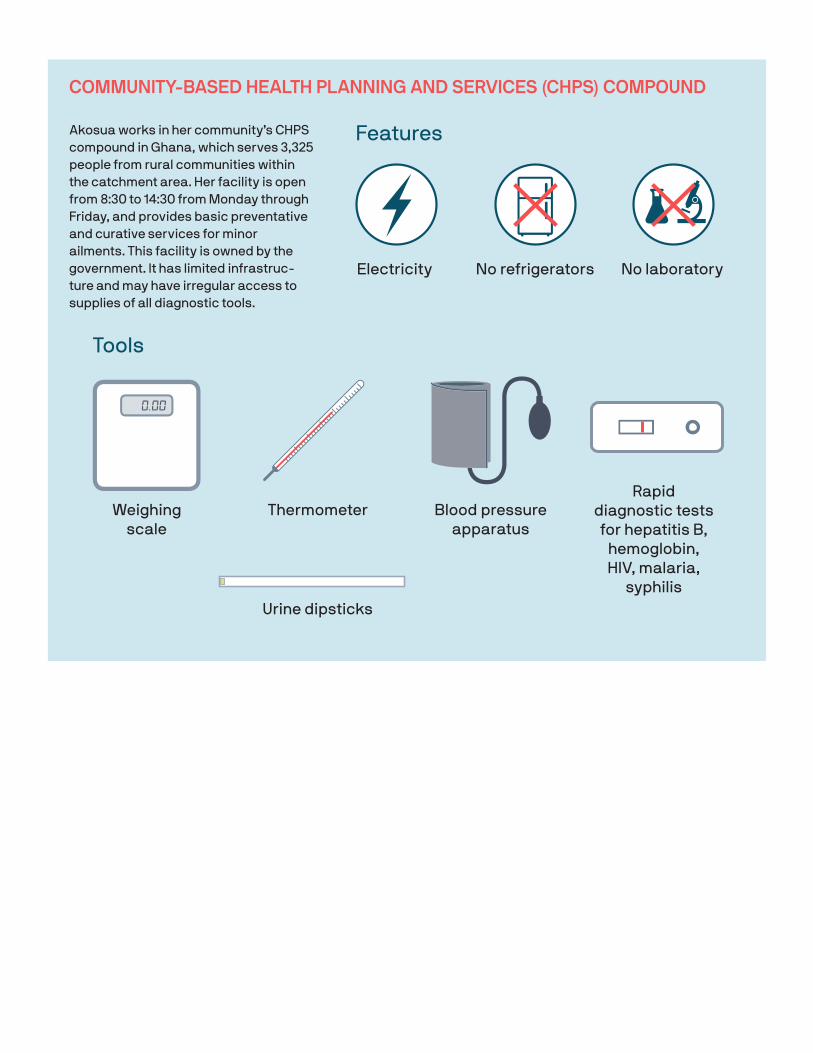
Tools
Weighing scale
Thermometer Blood pressure apparatus
Rapid diagnostic tests for hepatitis B,
hemoglobin, HIV, malaria,
syphilisUrine dipsticks
COMMUNITY-BASED HEALTH PLANNING AND SERVICES (CHPS) COMPOUND
Akosua works in her community’s CHPS compound in Ghana, which serves 3,325 people from rural communities within the catchment area. Her facility is open from 8:30 to 14:30 from Monday through Friday, and provides basic preventative and curative services for minor ailments. This facility is owned by the government. It has limited infrastruc-ture and may have irregular access to supplies of all diagnostic tools.
No refrigeratorsElectricity No laboratory
Features
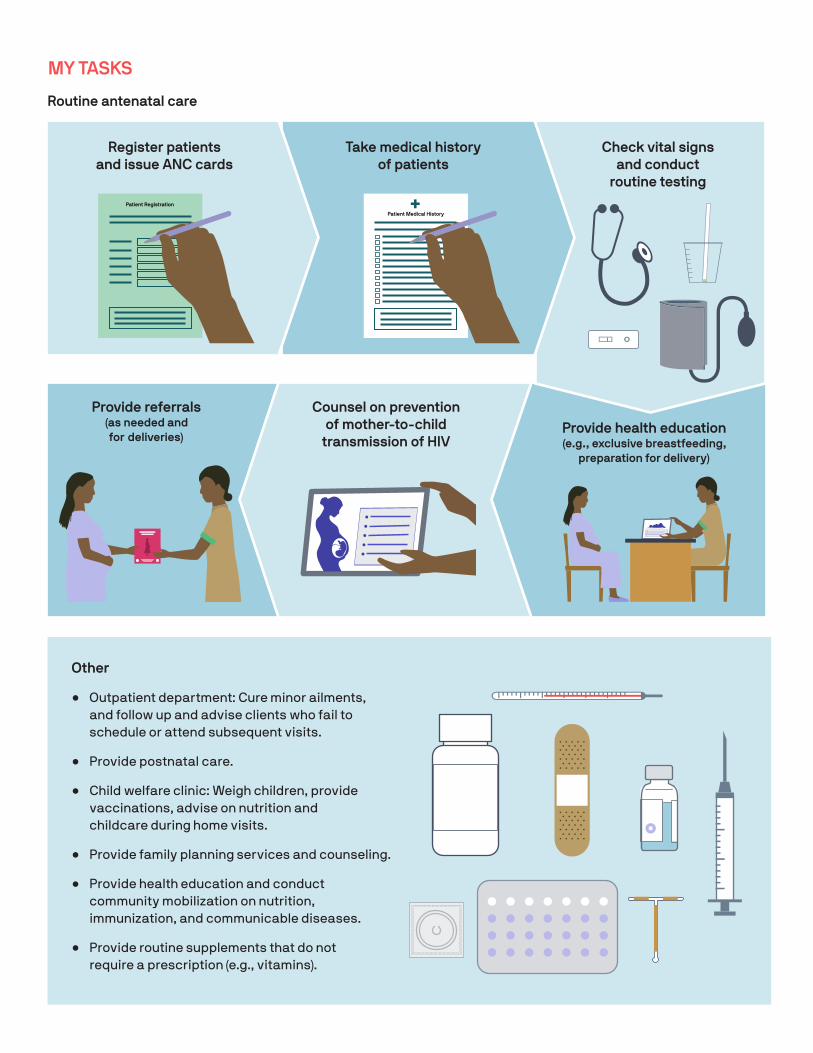
Other
• Outpatient department: Cure minor ailments, and follow up and advise clients who fail to schedule or attend subsequent visits.
• Provide postnatal care.
• Child welfare clinic: Weigh children, provide vaccinations, advise on nutrition and childcare during home visits.
• Provide family planning services and counseling.
• Provide health education and conduct community mobilization on nutrition, immunization, and communicable diseases.
• Provide routine supplements that do not require a prescription (e.g., vitamins).
Routine antenatal care
MY TASKS
Patient Registration
Patient Medical History
Register patients and issue ANC cards
Take medical history of patients
Check vital signs and conduct
routine testing
Provide health education (e.g., exclusive breastfeeding,
preparation for delivery)
Counsel on prevention of mother-to-child
transmission of HIV
Provide referrals (as needed and for deliveries)
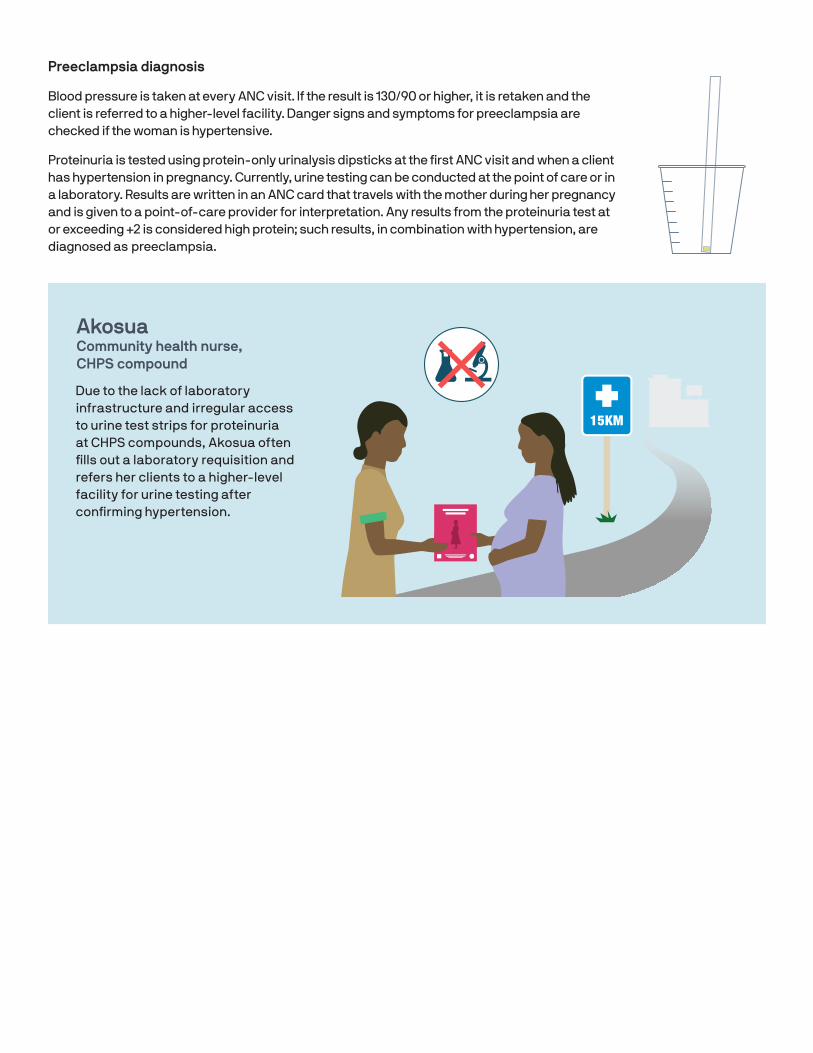
Preeclampsia diagnosis
Blood pressure is taken at every ANC visit. If the result is 130/90 or higher, it is retaken and the client is referred to a higher-level facility. Danger signs and symptoms for preeclampsia are checked if the woman is hypertensive.
Proteinuria is tested using protein-only urinalysis dipsticks at the first ANC visit and when a client has hypertension in pregnancy. Currently, urine testing can be conducted at the point of care or in a laboratory. Results are written in an ANC card that travels with the mother during her pregnancy and is given to a point-of-care provider for interpretation. Any results from the proteinuria test at or exceeding +2 is considered high protein; such results, in combination with hypertension, are diagnosed as preeclampsia.
?
~40MIN
15KM
Akosua Community health nurse, CHPS compound
Due to the lack of laboratory infrastructure and irregular access to urine test strips for proteinuria at CHPS compounds, Akosua often fills out a laboratory requisition and refers her clients to a higher-level facility for urine testing after confirming hypertension.
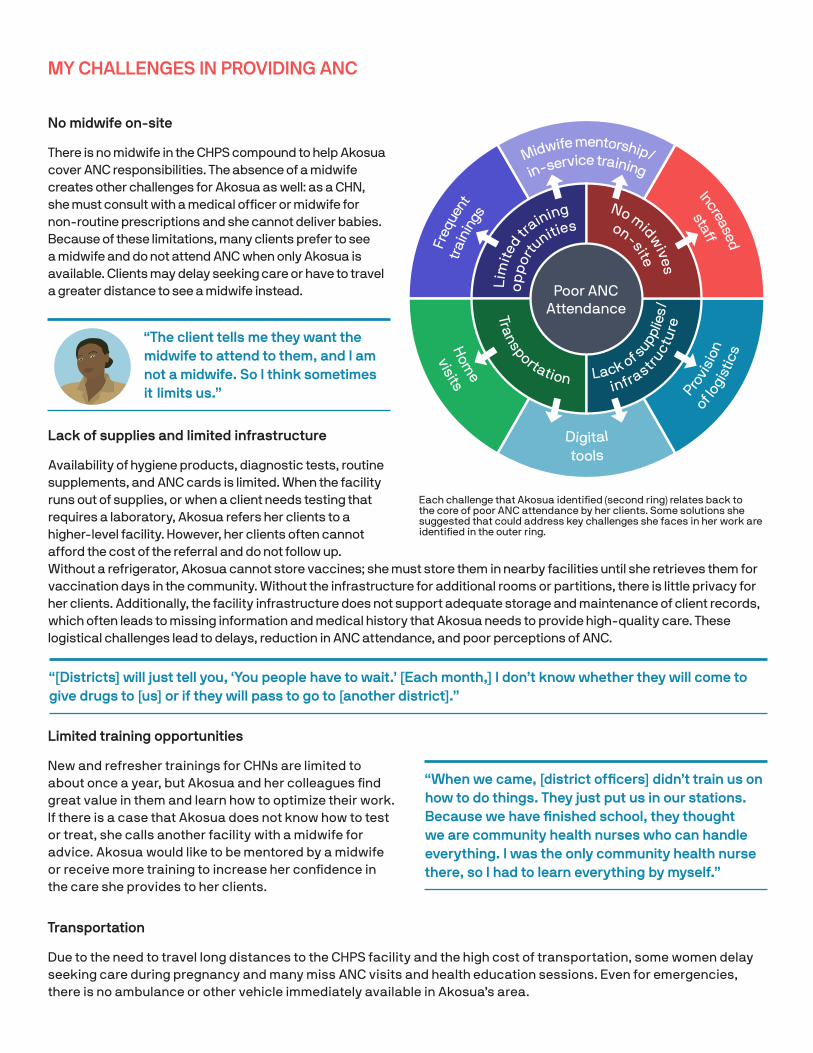
MY CHALLENGES IN PROVIDING ANC
No midwife on-site
There is no midwife in the CHPS compound to help Akosua cover ANC responsibilities. The absence of a midwife creates other challenges for Akosua as well: as a CHN, she must consult with a medical officer or midwife for non-routine prescriptions and she cannot deliver babies. Because of these limitations, many clients prefer to see a midwife and do not attend ANC when only Akosua is available. Clients may delay seeking care or have to travel a greater distance to see a midwife instead.
Lack of supplies and limited infrastructure
Availability of hygiene products, diagnostic tests, routine supplements, and ANC cards is limited. When the facility runs out of supplies, or when a client needs testing that requires a laboratory, Akosua refers her clients to a higher-level facility. However, her clients often cannot afford the cost of the referral and do not follow up. Without a refrigerator, Akosua cannot store vaccines; she must store them in nearby facilities until she retrieves them for vaccination days in the community. Without the infrastructure for additional rooms or partitions, there is little privacy for her clients. Additionally, the facility infrastructure does not support adequate storage and maintenance of client records, which often leads to missing information and medical history that Akosua needs to provide high-quality care. These logistical challenges lead to delays, reduction in ANC attendance, and poor perceptions of ANC.
Limited training opportunities
New and refresher trainings for CHNs are limited to about once a year, but Akosua and her colleagues find great value in them and learn how to optimize their work. If there is a case that Akosua does not know how to test or treat, she calls another facility with a midwife for advice. Akosua would like to be mentored by a midwife or receive more training to increase her confidence in the care she provides to her clients.
Transportation
Due to the need to travel long distances to the CHPS facility and the high cost of transportation, some women delay seeking care during pregnancy and many miss ANC visits and health education sessions. Even for emergencies, there is no ambulance or other vehicle immediately available in Akosua’s area.
in-service trainingMidwife mentorship/
Increased
staff
Freq
uent
trai
ning
s
of logis
tics
Provi
sion
toolsDigital
visitsH
ome
Poor ANC AttendanceTra
nsportation
Lim
ited
training
op
por
tunities
infrastructu
re
Lack of s
upplie
s/
No midwives
on-site
“[Districts] will just tell you, ‘You people have to wait.’ [Each month,] I don’t know whether they will come to give drugs to [us] or if they will pass to go to [another district].”
“The client tells me they want the midwife to attend to them, and I am not a midwife. So I think sometimes it limits us.”
Each challenge that Akosua identified (second ring) relates back to the core of poor ANC attendance by her clients. Some solutions she suggested that could address key challenges she faces in her work are identified in the outer ring.
“When we came, [district officers] didn’t train us on how to do things. They just put us in our stations. Because we have finished school, they thought we are community health nurses who can handle everything. I was the only community health nurse there, so I had to learn everything by myself.”
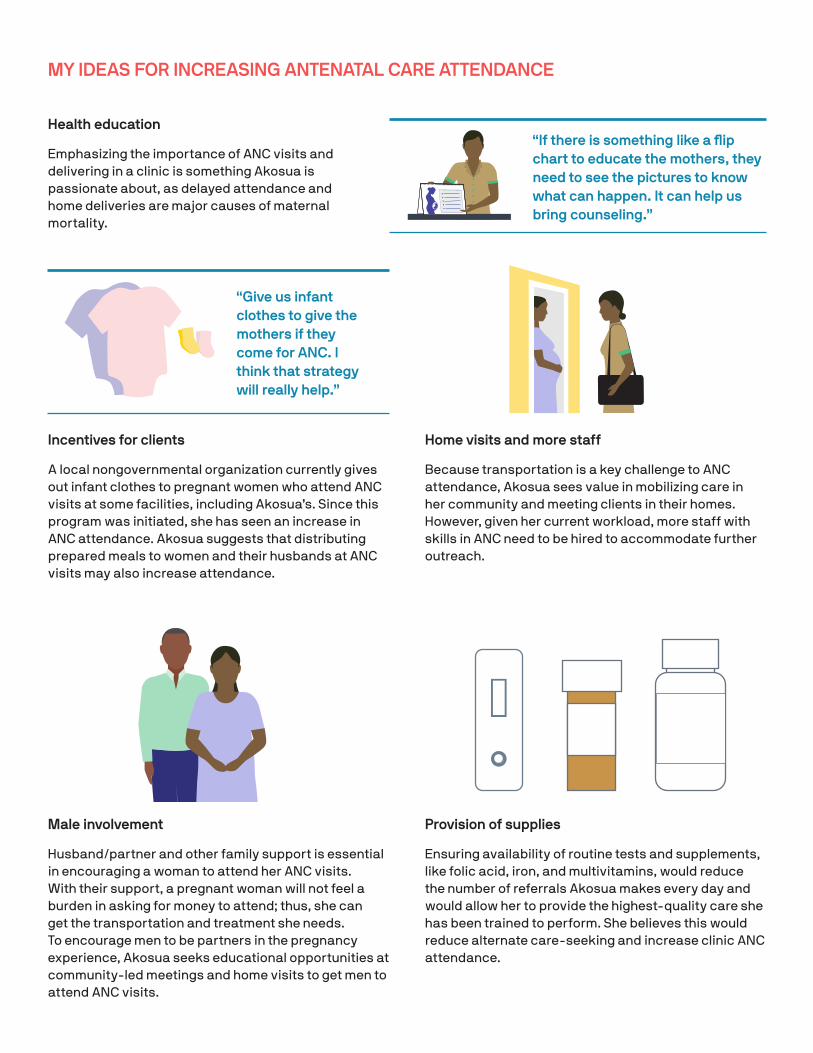
MY IDEAS FOR INCREASING ANTENATAL CARE ATTENDANCE
Health education
Emphasizing the importance of ANC visits and delivering in a clinic is something Akosua is passionate about, as delayed attendance and home deliveries are major causes of maternal mortality.
“If there is something like a flip chart to educate the mothers, they need to see the pictures to know what can happen. It can help us bring counseling.”
Incentives for clients
A local nongovernmental organization currently gives out infant clothes to pregnant women who attend ANC visits at some facilities, including Akosua’s. Since this program was initiated, she has seen an increase in ANC attendance. Akosua suggests that distributing prepared meals to women and their husbands at ANC visits may also increase attendance.
Home visits and more staff
Because transportation is a key challenge to ANC attendance, Akosua sees value in mobilizing care in her community and meeting clients in their homes. However, given her current workload, more staff with skills in ANC need to be hired to accommodate further outreach.
Male involvement
Husband/partner and other family support is essential in encouraging a woman to attend her ANC visits. With their support, a pregnant woman will not feel a burden in asking for money to attend; thus, she can get the transportation and treatment she needs. To encourage men to be partners in the pregnancy experience, Akosua seeks educational opportunities at community-led meetings and home visits to get men to attend ANC visits.
Provision of supplies
Ensuring availability of routine tests and supplements, like folic acid, iron, and multivitamins, would reduce the number of referrals Akosua makes every day and would allow her to provide the highest-quality care she has been trained to perform. She believes this would reduce alternate care-seeking and increase clinic ANC attendance.
“Give us infant clothes to give the mothers if they come for ANC. I think that strategy will really help.”
Antenatal care provider persona
RukayaMidwife
DEMOGRAPHICS
Gender: Female
Age: 36 years old
Education: • High school certificate• 2 years of specialized nursing training (CHN)• 2 years of midwifery training
Experience: 5 years
WORKLOAD
Patients seen per day: 15
Time spent with clients during first ANC visit: 30 to 45 minutes
Time spent with clients during subsequent ANC visits: 15 to 20 minutes
Deliveries per month: 26
GOAL
Rukaya wants her clients to be happy and healthy. She tries to reduce maternal and neonatal mortality through ANC and safe deliveries.
“I enjoy it when I see a healthy baby and a healthy mother. Being the first to see somebody on earth gives me joy.”
MOTIVATOR
“I just had that passion to go into midwifery so that I will be able to empower these women to know more about themselves, pregnancies, and how to care for themselves.”
102
Tools
Weighing scale
Thermometer
Blood pressure apparatus
Glucometer
Rapid diagnostic tests for hepatitis B,
hemoglobin, HIV, malaria,
syphilisUrine dipsticks
HEALTH CENTER
Rukaya is the only midwife in her community’s health center in Ghana, which serves 6,421 people from urban and rural communities within the catchment area. Her facility is open 24 hours a day, 7 days a week, and provides preventative and curative services, as well as outreach programs to her community. Refrigerator Electricity Laboratory
Features
(no backup generator)
102

Other
• Attend deliveries.
• Refer hypertensive and complex cases.
• Prescribe drugs (antimalarials, PrEP, HIV treatment).
• Provide postnatal care.
• Supervise the health center.
• Provide in-service training of CHNs and junior midwives.
MY TASKS
Routine antenatal care
Patient Registration
Register patients Check vital signs
Provide health education (e.g., exclusive breastfeeding,
preparation for delivery)Request lab tests
(including urine dipstick and rapid diagnostic tests)
Counsel on prevention of mother-to-child
transmission of HIV
Administer tetanus vaccines
Treat minor ailments
Prescribe routine drugs (e.g., folic acid, SP, iron, vitamins, hypertension
medication)
Provide referrals (as needed)
Perform physical exam (palpations and fetal
development monitoring)
PrEP: pre-exposure prophylaxis. SP: sulfadoxine-pyrimethamine.

Preeclampsia diagnosis
Blood pressure is taken at every ANC visit. If the result is 130/90 or higher, it is retaken and the client is referred to a higher-level facility. Danger signs and symptoms for preeclampsia are checked if the woman is hypertensive.
Proteinuria is tested using protein-only urinalysis dipsticks at the first ANC visit and when a client has hypertension in pregnancy. Currently, urine testing can be conducted at the point of care or in a laboratory, along with any other testing the client may need during her ANC visit. Results are written in an ANC card that travels with the mother during her pregnancy and is given to a point-of-care provider for interpretation. Any results from the proteinuria test at or exceeding +2 is considered high protein; such results, in combination with hypertension, is diagnosed as preeclampsia.
The laboratory technicians and point-of-care providers who currently run the tests face challenges with urine dipsticks when the results are between color blocks on the colorimetric scale. When test operators have a heavy workload, the target of reading the dipsticks at exactly 60 seconds is often missed, which can produce faulty results. Results may also be affected by women in this region needing to purchase their own urine collection containers and tending to reuse them when urine testing is required; without proper cleaning, this can cross-contaminate samples and produce faulty results. Rukaya thus has low confidence in the results she interprets, which affects her suggested course of treatment for her clients.
RukayaMidwife, health center
Health centers have laboratories and greater access to urine test strips for proteinuria than many CHPS compounds. Rukaya sends her clients to the lab for testing when symptoms suggest complications in pregnancy, where they wait for an average of 40 minutes to be seen.4 They return with the numeric results written in their ANC cards. Rukaya interprets the results and counsels her clients accordingly. When tests are unavailable, Rukaya focuses on blood pressure and danger signs to determine if a woman is likely preeclamptic and provides appropriate treatment (including magnesium sulphate).
?
~40MIN
15KM
MY CHALLENGES IN PROVIDING ANC
In-service
training
Increased staff
of logis
tics
Provisio
n
Maleinvolvement
Digital tools
Poor ANC Attendance
Lack of supp
lies
with c
lients
Only m
idwife
availableLanguage
barr
iers
cu
ltural beliefs
Perceptions &
Relatio
nship
s
Only midwife
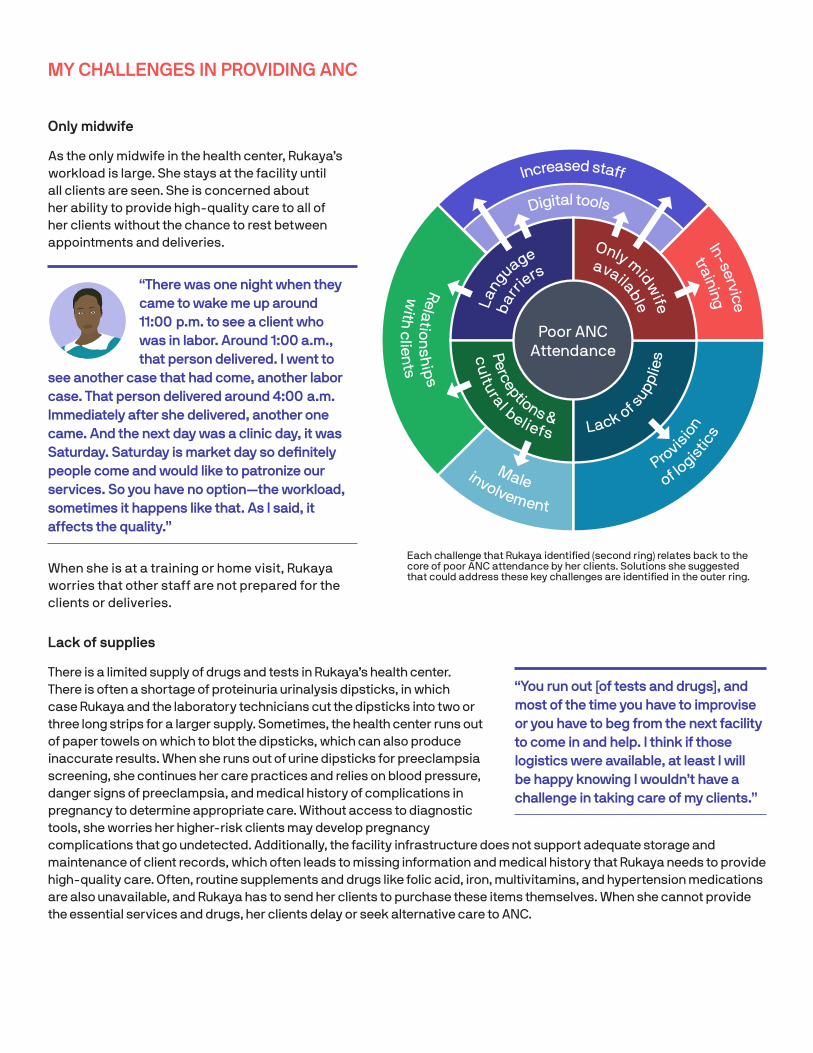
As the only midwife in the health center, Rukaya’s workload is large. She stays at the facility until all clients are seen. She is concerned about her ability to provide high-quality care to all of her clients without the chance to rest between appointments and deliveries.
“There was one night when they came to wake me up around 11:00 p.m. to see a client who was in labor. Around 1:00 a.m., that person delivered. I went to
see another case that had come, another labor case. That person delivered around 4:00 a.m. Immediately after she delivered, another one came. And the next day was a clinic day, it was Saturday. Saturday is market day so definitely people come and would like to patronize our services. So you have no option—the workload, sometimes it happens like that. As I said, it affects the quality.”
When she is at a training or home visit, Rukaya worries that other staff are not prepared for the clients or deliveries.
Lack of supplies
There is a limited supply of drugs and tests in Rukaya’s health center. There is often a shortage of proteinuria urinalysis dipsticks, in which case Rukaya and the laboratory technicians cut the dipsticks into two or three long strips for a larger supply. Sometimes, the health center runs out of paper towels on which to blot the dipsticks, which can also produce inaccurate results. When she runs out of urine dipsticks for preeclampsia screening, she continues her care practices and relies on blood pressure, danger signs of preeclampsia, and medical history of complications in pregnancy to determine appropriate care. Without access to diagnostic tools, she worries her higher-risk clients may develop pregnancy complications that go undetected. Additionally, the facility infrastructure does not support adequate storage and maintenance of client records, which often leads to missing information and medical history that Rukaya needs to provide high-quality care. Often, routine supplements and drugs like folic acid, iron, multivitamins, and hypertension medications are also unavailable, and Rukaya has to send her clients to purchase these items themselves. When she cannot provide the essential services and drugs, her clients delay or seek alternative care to ANC.
“You run out [of tests and drugs], and most of the time you have to improvise or you have to beg from the next facility to come in and help. I think if those logistics were available, at least I will be happy knowing I wouldn’t have a challenge in taking care of my clients.”
Each challenge that Rukaya identified (second ring) relates back to the core of poor ANC attendance by her clients. Solutions she suggested that could address these key challenges are identified in the outer ring.
Language barriers
Because Rukaya serves a culturally diverse population with 21 languages spoken, she struggles to communicate with all of her clients. She is concerned with their ability to understand her health education and counseling. Clients who do not understand her often do not complete their referrals or follow their care plan. Usually there is not an option for an interpreter, so Rukaya seeks support from fellow health care workers and other clients. She worries about client anonymity and privacy when someone helps interpret for her.
Limitations in seeking care due to perceptions and cultural beliefs
In Rukaya’s community, women need approval from their family, church, or husband/partner to attend ANC visits. Without their support, Rukaya’s clients do not have the money for transportation to the health center or to purchase the routine drugs needed. Some churches discourage ANC attendance, fearing witchcraft or abortions.
“[Poor ANC attendance] is a challenge because, most of the time, you give [a client the] date of the next visit and they don’t comply. They come back at their own time. When you try to find out why, it all boils down to financial difficulty. They say: ‘I didn’t get money to pick a vehicle.’ Or it boils down to cultural beliefs. They say: ‘I need to inform my mother-in-law before I leave home. Without the consent of my mother-in-law I can’t leave home.’
Another is religious beliefs: The person tells you that she went to a church and the pastor told her that for this and that reason, the day she was asked to go, don’t go. [She was told to instead go] on this other path on another day… A perception they have in coming to antenatal care early, or seeking care early, is that if you make reports that say she is at the early stage of pregnancy, somebody might look at her with an evil eye, which will abort/spoil the pregnancy. So they delay coming to the facility to seek care.”
A client’s family support is also influential in whether a client will deliver at home or in a clinic.
“[Some women and some community members] believe delivering in a hospital makes you not a strong woman. It makes our [clinic] deliveries drop.”
MY IDEAS FOR INCREASING ANC ATTENDANCE
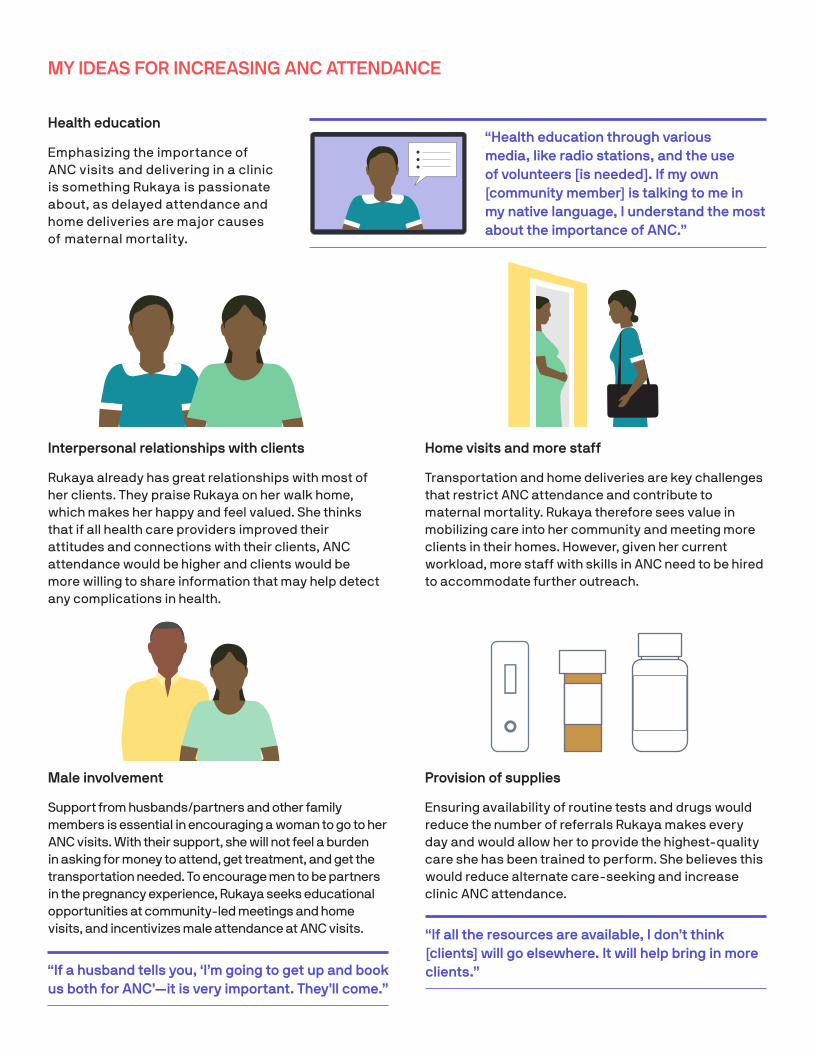
Health education
Emphasizing the importance of ANC visits and delivering in a clinic is something Rukaya is passionate about, as delayed attendance and home deliveries are major causes of maternal mortality.
“Health education through various media, like radio stations, and the use of volunteers [is needed]. If my own [community member] is talking to me in my native language, I understand the most about the importance of ANC.”
“If a husband tells you, ‘I’m going to get up and book us both for ANC’—it is very important. They’ll come.”
“If all the resources are available, I don’t think [clients] will go elsewhere. It will help bring in more clients.”
Interpersonal relationships with clients
Rukaya already has great relationships with most of her clients. They praise Rukaya on her walk home, which makes her happy and feel valued. She thinks that if all health care providers improved their attitudes and connections with their clients, ANC attendance would be higher and clients would be more willing to share information that may help detect any complications in health.
Home visits and more staff
Transportation and home deliveries are key challenges that restrict ANC attendance and contribute to maternal mortality. Rukaya therefore sees value in mobilizing care into her community and meeting more clients in their homes. However, given her current workload, more staff with skills in ANC need to be hired to accommodate further outreach.
Male involvement
Support from husbands/partners and other family members is essential in encouraging a woman to go to her ANC visits. With their support, she will not feel a burden in asking for money to attend, get treatment, and get the transportation needed. To encourage men to be partners in the pregnancy experience, Rukaya seeks educational opportunities at community-led meetings and home visits, and incentivizes male attendance at ANC visits.
Provision of supplies
Ensuring availability of routine tests and drugs would reduce the number of referrals Rukaya makes every day and would allow her to provide the highest-quality care she has been trained to perform. She believes this would reduce alternate care-seeking and increase clinic ANC attendance.
Case study: Perspectives on digital tools
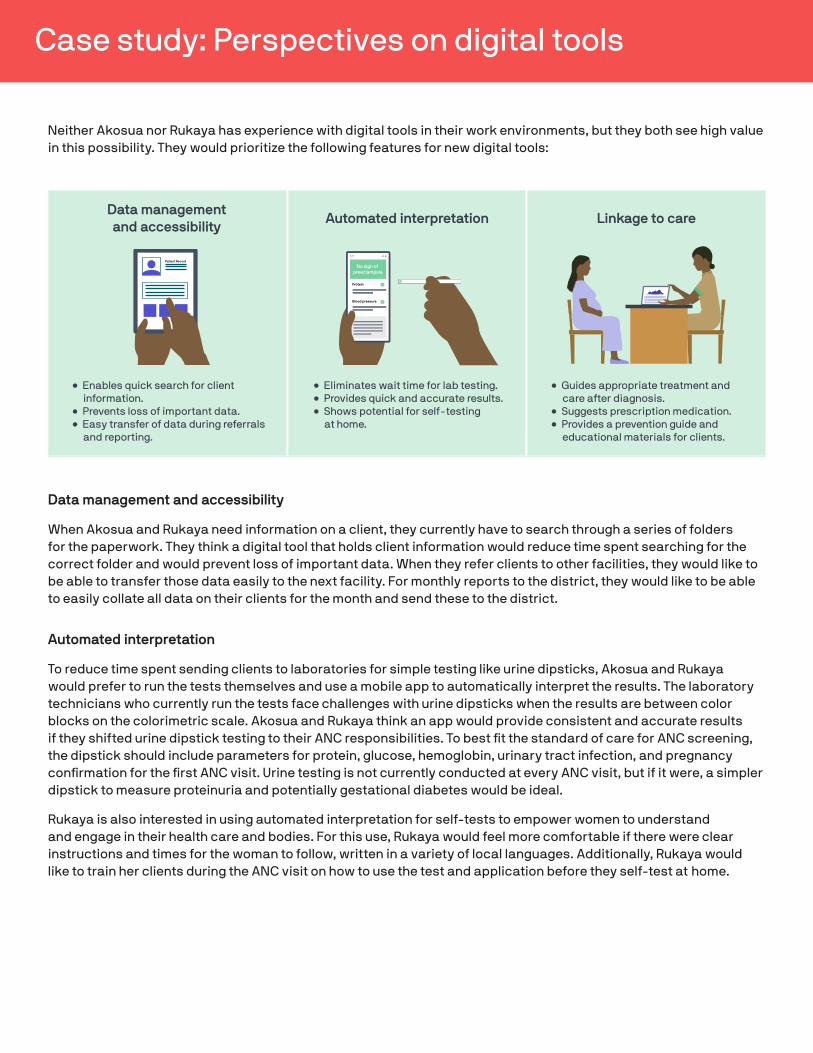
Neither Akosua nor Rukaya has experience with digital tools in their work environments, but they both see high value in this possibility. They would prioritize the following features for new digital tools:
Data management and accessibility
When Akosua and Rukaya need information on a client, they currently have to search through a series of folders for the paperwork. They think a digital tool that holds client information would reduce time spent searching for the correct folder and would prevent loss of important data. When they refer clients to other facilities, they would like to be able to transfer those data easily to the next facility. For monthly reports to the district, they would like to be able to easily collate all data on their clients for the month and send these to the district.
Automated interpretation
To reduce time spent sending clients to laboratories for simple testing like urine dipsticks, Akosua and Rukaya would prefer to run the tests themselves and use a mobile app to automatically interpret the results. The laboratory technicians who currently run the tests face challenges with urine dipsticks when the results are between color blocks on the colorimetric scale. Akosua and Rukaya think an app would provide consistent and accurate results if they shifted urine dipstick testing to their ANC responsibilities. To best fit the standard of care for ANC screening, the dipstick should include parameters for protein, glucose, hemoglobin, urinary tract infection, and pregnancy confirmation for the first ANC visit. Urine testing is not currently conducted at every ANC visit, but if it were, a simpler dipstick to measure proteinuria and potentially gestational diabetes would be ideal.
Rukaya is also interested in using automated interpretation for self-tests to empower women to understand and engage in their health care and bodies. For this use, Rukaya would feel more comfortable if there were clear instructions and times for the woman to follow, written in a variety of local languages. Additionally, Rukaya would like to train her clients during the ANC visit on how to use the test and application before they self-test at home.
Patient Record
Data management and accessibility
Automated interpretation
• Eliminates wait time for lab testing.• Provides quick and accurate results.• Shows potential for self-testing
at home.
• Guides appropriate treatment and care after diagnosis.
• Suggests prescription medication.• Provides a prevention guide and
educational materials for clients.
Linkage to care
• Enables quick search for client information.
• Prevents loss of important data.• Easy transfer of data during referrals
and reporting.
Protein
Blood pressure
No sign of preeclampsia
Kintampo Health Research CentreNo. 2 Hospital LoopMinistry of Health/Ghana Health ServicePO Box 200Kintampo, Bono-East Region
www.kintampo-hrc.org
© 2020 PATH. The material in this document may be freely used for educational or noncommercial purposes, provided that the material is accompanied by an ac-knowledgment. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
International License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/. All other rights reserved.
References1. Ghana Health Service (GHS), Regional Health Directorate Brong-Ahafo Region. 2015 Annual Report. GHS; 2016:143. https://www.
ghanahealthservice.org/downloads/BA_Annual_Report_2015_EDITED_VERSION.pdf.
2. Institute for Health Metrics and Evaluation website. GBD Compare | Viz Hub Ghana-level data page. https://vizhub.healthdata.org/gbd-compare/. Accessed August 20, 2020.
3. Ghana Health Service website. Brong-Ahafo Region - Regional Health Directorate: Supervised delivery page. https://www.ghanahealthservice.org/rhdsubcategory.php?ghsrid=6&cid=55&ghsscid=60. Accessed July 13, 2020.
4. Goodman DM, Srofenyoh EK, Olufolabi AJ, Kim SM, Owen MD. The third delay: understanding waiting time for obstetric referrals at a large regional hospital in Ghana. BMC Pregnancy and Childbirth. 2017;17:216. https://doi.org/10.1186/s12884-017-1407-4.
Additional resources1. World Health Organization (WHO). WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: WHO; 2016. https://
www.who.int/reproductivehealth/publications/maternal_perinatal_health/anc-positive-pregnancy-experience/en/.
2. World Health Organization (WHO). WHO Recommendations for Prevention and Treatment of Pre-eclampsia and Eclampsia. Geneva: WHO; 2011. https://www.who.int/reproductivehealth/publications/maternal_perinatal_health/9789241548335/en/.
3. World Health Organization (WHO), United Nations Children’s Fund, United Nations Population Fund. Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors. 2nd ed. Geneva: WHO; 2017. https://www.who.int/maternal_child_adolescent/documents/managing-complications-pregnancy-childbirth/en/.
4. Brown MA, Magee LA, Kenny LC, et al. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72(1):24–43. https://doi.org/10.1161/HYPERTENSIONAHA.117.10803.
5. National Institute for Health and Care Excellence (NICE). Hypertension in Pregnancy: Diagnosis and Management. NICE Guideline 133. London: NICE; 2019. https://www.nice.org.uk/guidance/ng133.
6. Magee LA, von Dadelszen P, Stones W, Mathai M, eds. The FIGO Textbook of Pregnancy Hypertension: An Evidence-Based Guide to Monitoring, Prevention and Management. London: The Global Library of Women’s Medicine; 2016. http://www.safemotherhood.ucsf.edu/wp-content/uploads/2013/01/FIGO-Pregnancy_Hypertension-Final.pdf.
7. Ghana Statistical Service (GSS), Ghana Health Service (GHS), ICF. Ghana 2017 Maternal Health Survey Key Findings. Rockville, MD: GSS, GHS, and ICF; 2018. https://www.dhsprogram.com/pubs/pdf/SR251/SR251.pdf.
Linkage to care
When results from testing come back from the laboratory or an app, Akosua and Rukaya would like a digital tool to support them in guiding clients to appropriate treatment and care. They suggest that recommendations for care, prescriptions to the pharmacy, a prevention guide, and other educational materials to share with clients be included in this design function.
Key features of an effective digital tool
Offline use
Compatibility with Android devices
Instructional videos (optional)
Alerts and timers to prompt next steps
Mailing AddressPO Box 900922Seattle, WA 98109 USA
Street Address2201 Westlake AvenueSuite 200Seattle, WA 98121 USA
www.path.org