another introduction to tcd
DESCRIPTION
introduction to TCDTRANSCRIPT
TRANSCRANIAL DOPPLER ULTRASOUND
INTRODUCTION TO TCD
Nicolet Vascular, Inc.
A Division of
VIASYS HEALTHCARE
WHAT IS TCD?
• TCD (Transcranial Doppler) is a
non-invasive assessment of cerebral blood flow in the basal cerebral arteries
• Utilizes low frequency Doppler ultrasound
WHAT IS TCD?
• Uses 2 MHz pulsed Doppler ultrasound
• Passes through cranial “windows”
• Provides information regarding velocity and direction of cerebral blood flow
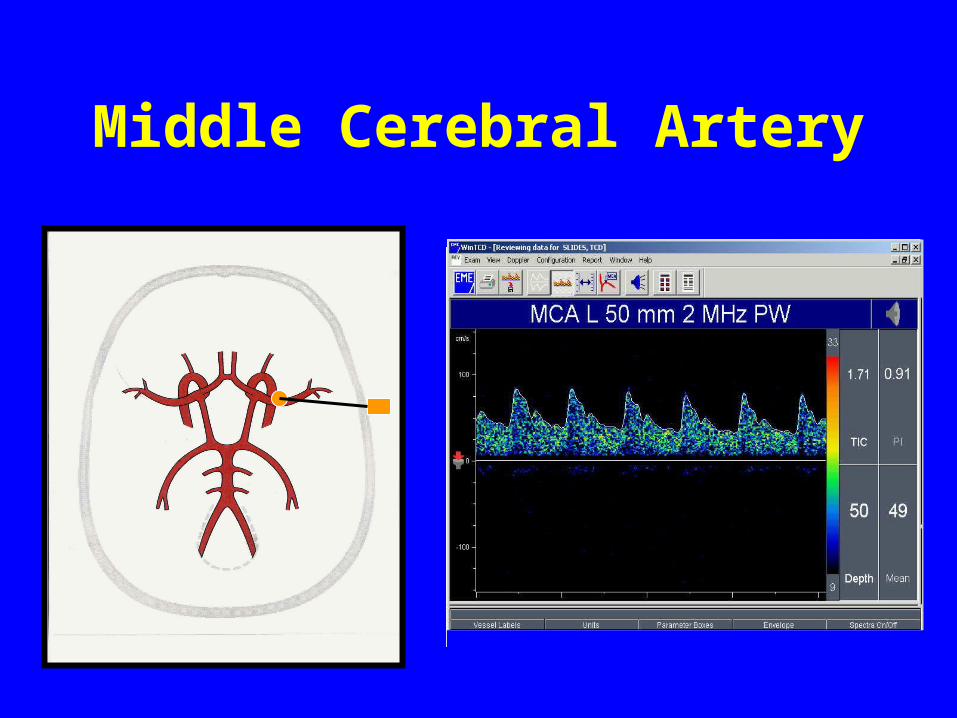
Middle Cerebral Artery

BLOOD FLOW VELOCITY
• Changes in flow velocity occur when:
• There is a change in vessel caliber• There is a change in volume flow
TRANSCRANIAL DOPPLER
• Non-invasive• Painless• Inexpensive• Can provide instantaneous and continuous
cerebral blood flow information • Can be used in any hospital environment• Safe
DEVELOPMENT OF TCD
• 1982 Dr. Rune Aaslid– First publication Transtemporal Approach
• 1984 Dr. Merrill Spencer– First publication Transorbital Approach
• 1986 Dr. M. Von Reutern– First publication Suboccipital Approach
• 1983 First commercial TCD unit (EME)
TCD APPLICATIONS
• Accepted applications *(AAN):
– Detect intracranial stenosis– Follow the time course of vasospasm– Confirm the diagnosis of brain death– Assist in the detection an management
of AVMs
*American Academy of Neurology
TCD APPLICATIONS
• Other reported uses:– Assess of collateral pathways– Assess autoregulation and vasomotor
reactivity– ICU monitoring (effects of ICP)– Surgical monitoring (CEA, CABG)– Detection of emboli (HITS)– Aid in classification of strokes
TCD APPLICATIONS
• Other reported uses:– Subclavian steal assessment– Assess mechanical compression of the
vertebral arteries– Evaluate Sickle Cell patients– Evaluate patients with carotid
dissections

TCD APPLICATIONS
• Assess the effects of pharmacological interventions
• Research applications
• Surgical monitoring

INTRAOPERATIVE MONITORING APPLICATIONS
• Carotid Endarterectomy
• Carotid Stenting
• Coronary Artery Bypass Surgery
• Cardiac Valve Surgery
• Abdominal Aortic Aneurysm
• Liver Transplants
• Orthopedic Surgery
TCD MONITORING
• Patent Foramen Ovale evaluation
• Implantable cardioverter defibrillator testing
• Any procedure where knowledge of the state of blood flow to the brain is of critical importance
TRANSCRANIAL DOPPLER
EXAMINATION TECHNIQUE
TCD - APPROACHES
• Transtemporal
• Transorbital
• Suboccipital (Transforaminal)
• Submandibular

TRANSCRANIAL DOPPLER ACCESS ROUTES
TRANSTEMPORAL APPROACH
• Middle Cerebral Artery MCA• Anterior Cerebral Artery ACA• Terminal Internal Carotid Artery T-ICA• Posterior Cerebral Artery PCA• Communicating Arteries
– Anterior Communicating Artery
ACoA– Posterior Communicating Artery PCoA
CRITERIA FOR VESSEL IDENTIFICATION
• Depth of the sample volume
• Direction of flow
• Traceability of the vessel
• Transducer angulation
• Spatial relationship of spectra
• Response to carotid or vertebral oscillations or compressions
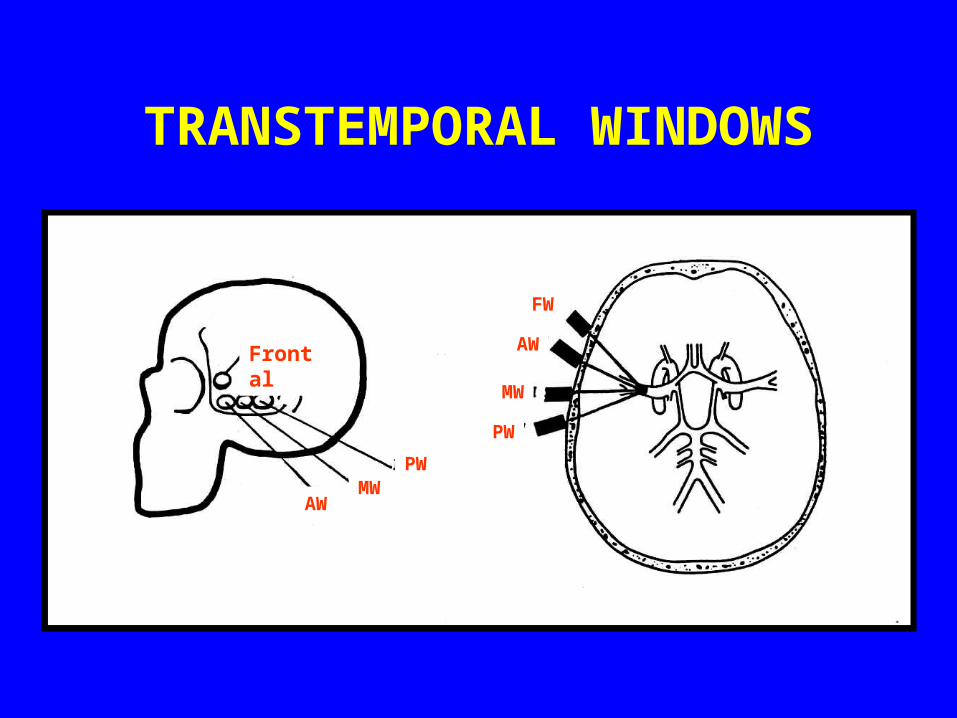
TRANSTEMPORAL WINDOWS
Frontal
AW
PW
MW
AW
MW
PW
FW
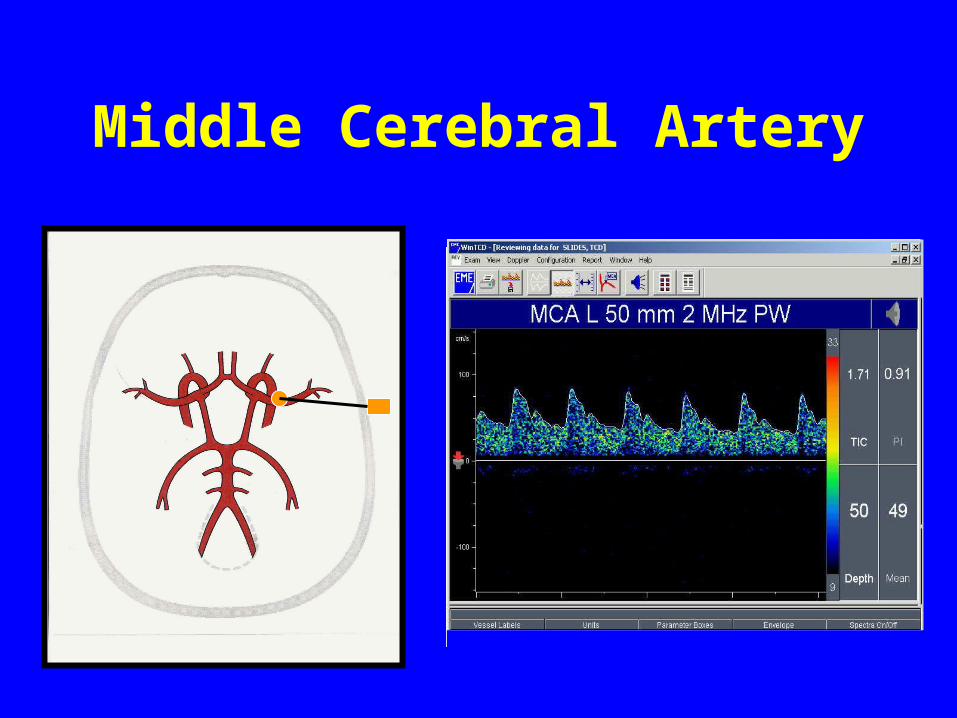
Middle Cerebral Artery
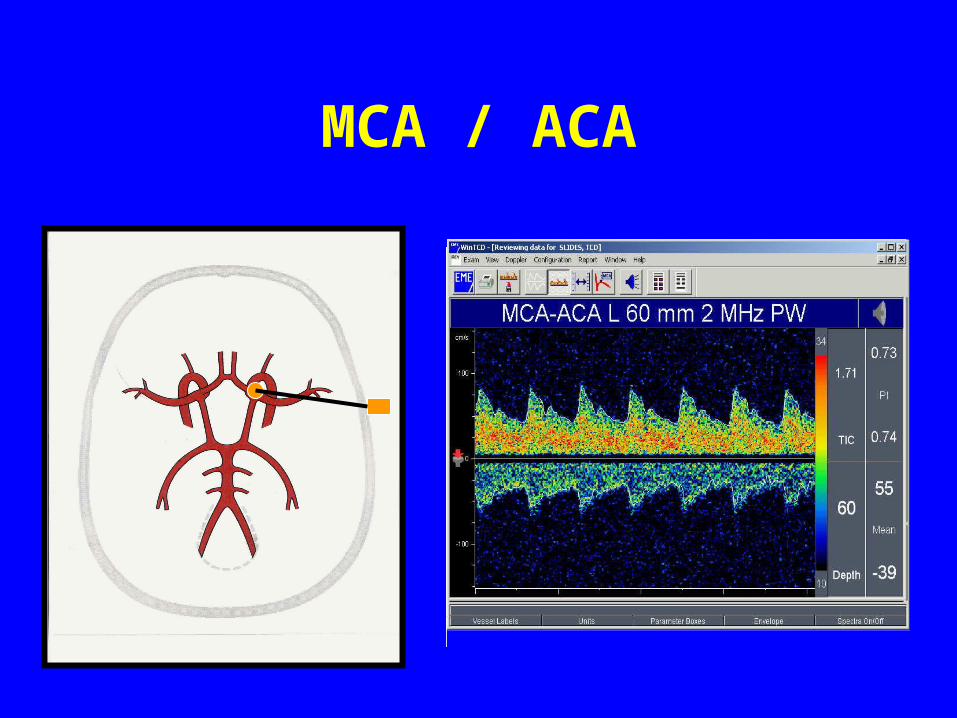
MCA / ACA
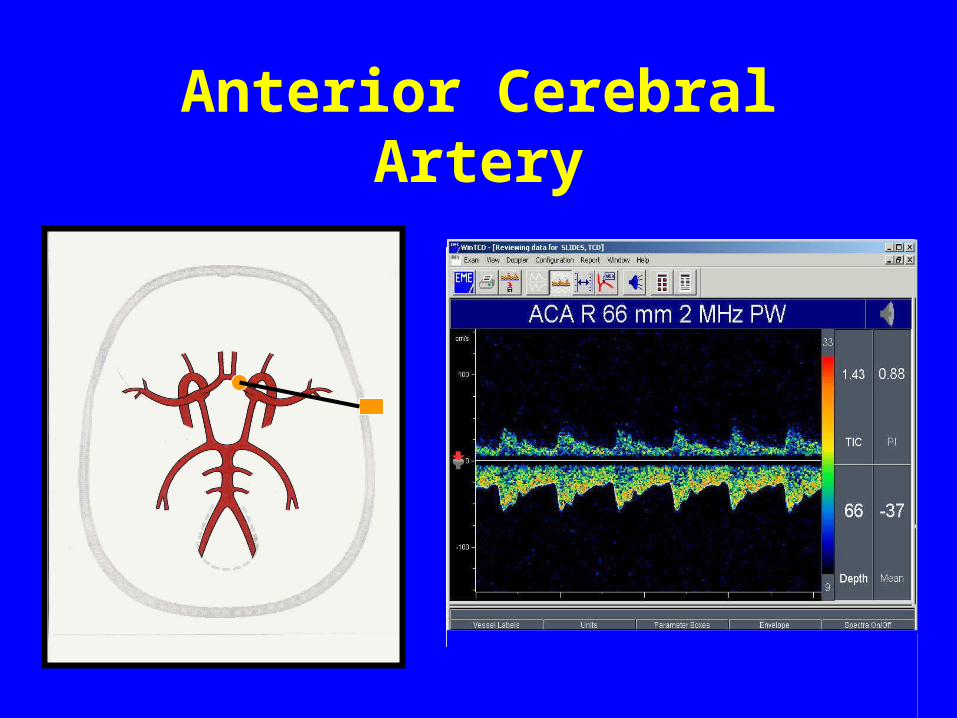
Anterior Cerebral Artery
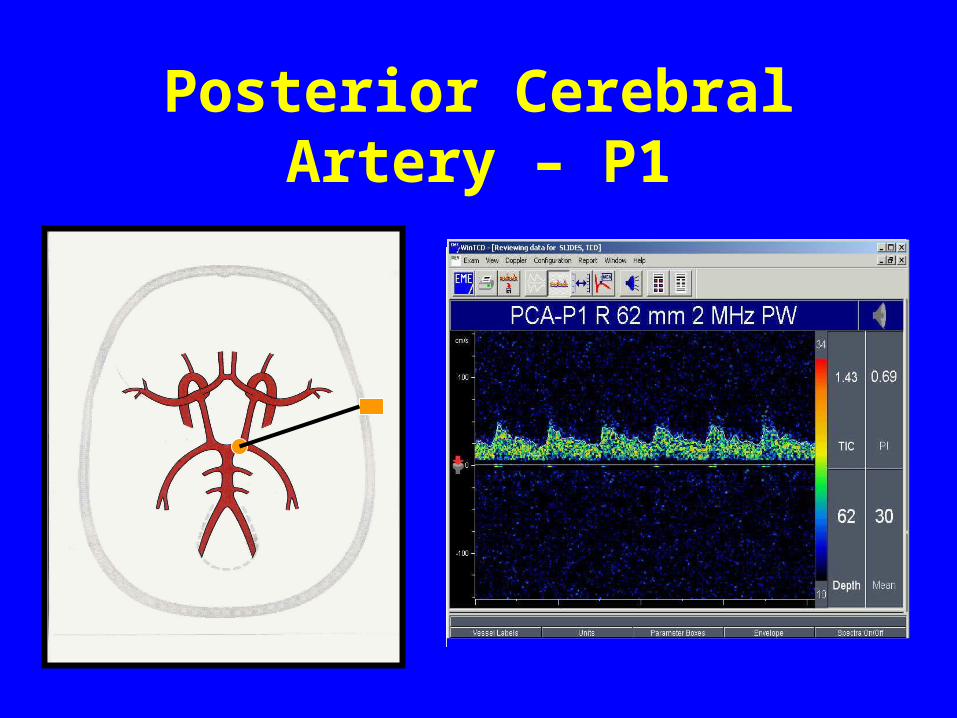
Posterior Cerebral Artery – P1
TRANSORBITAL APPROACH
• Ophthalmic Artery OA
• Internal Carotid Artery Siphon
– Parasellar
– Genu
– Supraclinoid
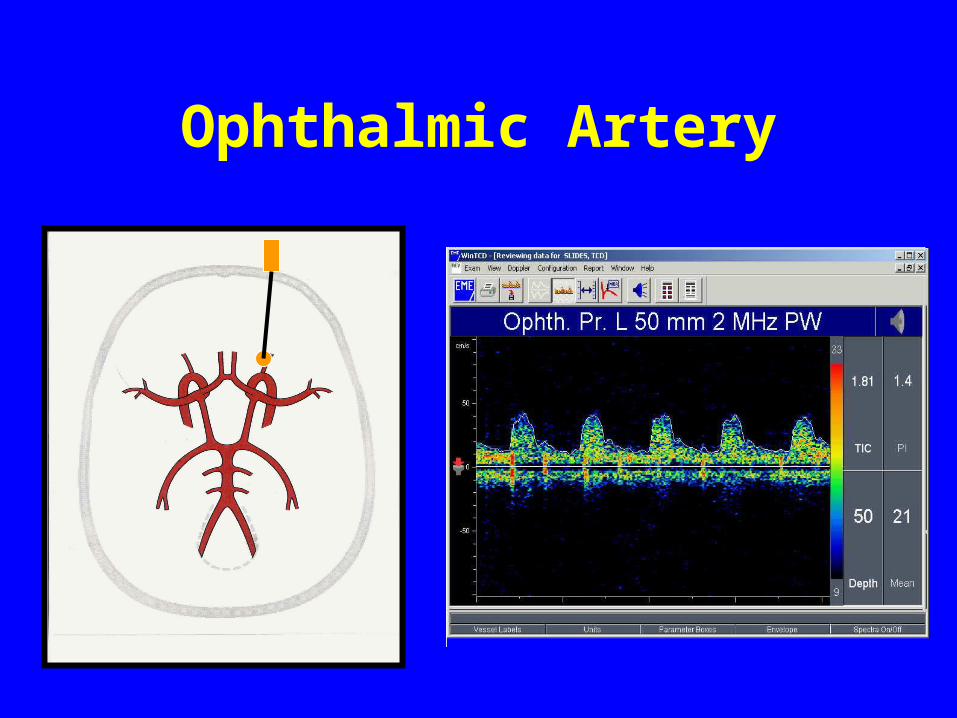
Ophthalmic Artery

Carotid Siphon - Genu
SUBOCCIPITAL APPROACH
• Vertebral Artery VA
• Basilar Artery BA

Vertebral Artery

Basilar Artery
NORMAL VELOCITY RELATIONSHIPS
MCA > ACA > PCAPCA ~ VA and BA
PRIMARY DIAGNOSTIC FEATURES
• Changes in velocity
• Changes in pulsatility
• Changes in systolic upstroke
• Changes in flow direction
• Side to side differences
• Embolic phenomena (HITS)
TRANSCRANIAL DOPPLER
COLLATERAL CIRCULATION
Effects of Extracranial Carotid Stenosis / Occlusion
• Factors affecting cerebral blood flow:
– Degree of proximal stenosis– Size and extent of collateral channels

EFFECTS OF CAROTID STENOSIS
• Mild to Moderate Stenosis (< +/- 75%)
– TCD exam: Essentially normal
• Severe Stenosis (> +/- 75%)
– TCD exam: Abnormal– Changes in Doppler spectral waveform shape– Changes in flow patterns (Collateral)

WAVEFORM CHANGES
• Decreased velocity
• Delayed systolic upstroke
• Decreased pulsatility
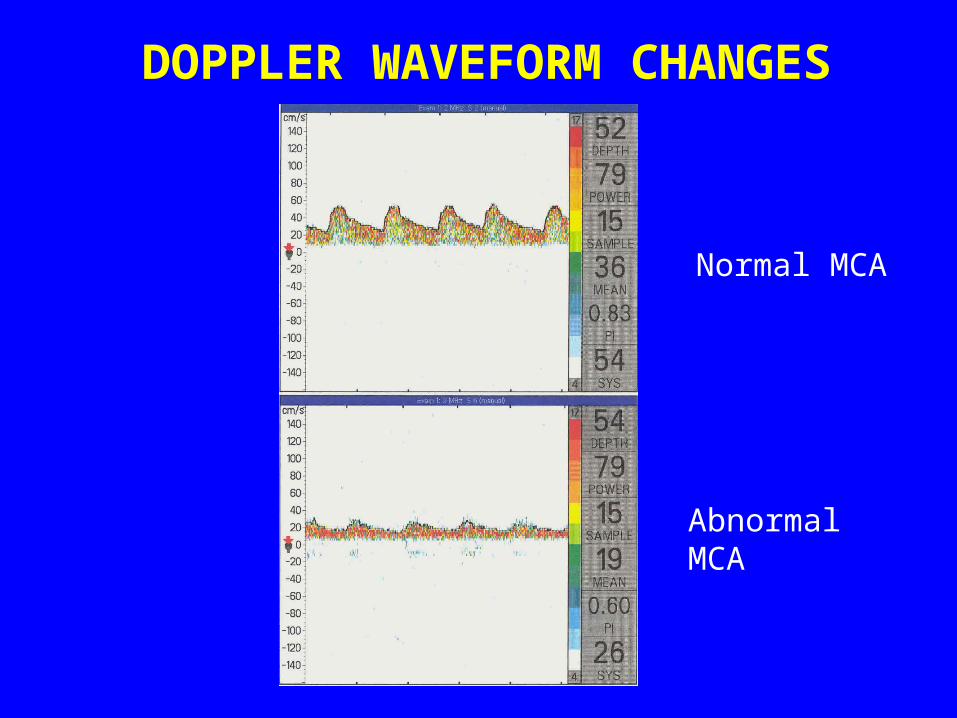
DOPPLER WAVEFORM CHANGES
Normal MCA
Abnormal MCA
COLLATERAL SOURCES
• Collateral detectable by TCD include:
– Circle of Willis, including the vertebrobasilar system
– ECA to ICA collateral via the ophthalmic artery
COLLATERAL SOURCES
• Collateral not detectable by TCD include:
– Branches of the ECA connecting to branches of the vertebral artery
– Leptomeningeal anastomoses

INTRACRANIAL STENOSIS
• Focal elevated velocities above adjacent segments
• Side to side differences exceeding normal variation (usually > 15% or 30 cm/sec between right and left MCA)
• Downstream effects: – Turbulence– Delayed systolic upstroke– Decreased velocity
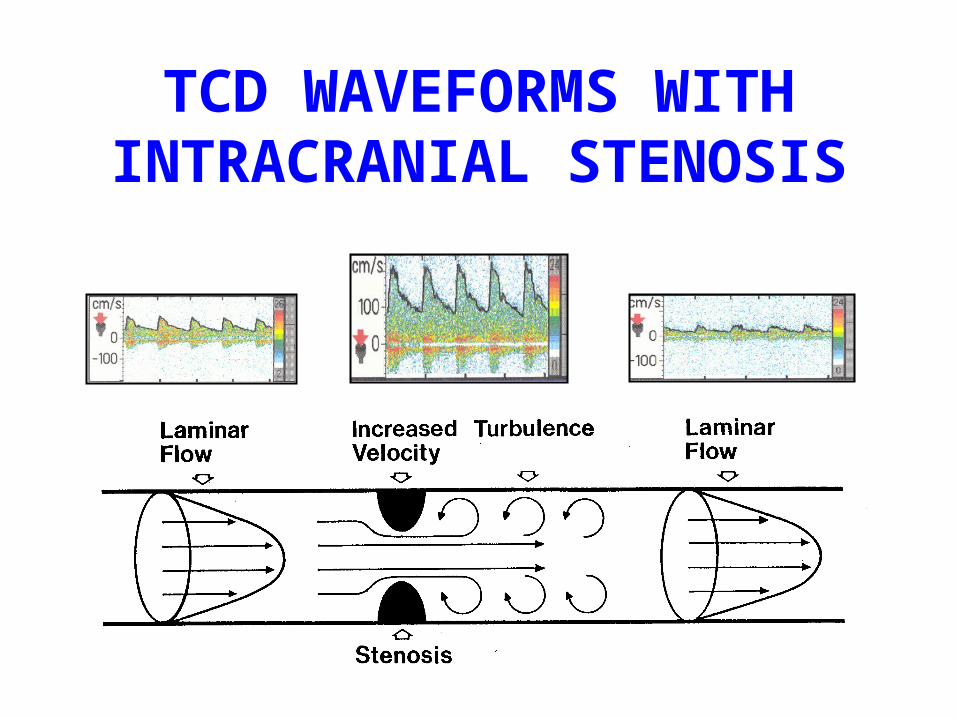
TCD WAVEFORMS WITH INTRACRANIAL STENOSIS
INTRACRANIAL STENOSISCauses
• Atherosclerosis
• Intraluminal thromboembolism
• Arterial dissection
• Moyamoya disease
• Vasculitis
• Vasospasm
• Extrinsic vessel compression
TRANSCRANIAL DOPPLER
EMBOLI DETECTION(HITS)
EMBOLIC EVENTS
• Foreign solids and / or gaseous materials within the blood stream
• Reflect sound waves more intensely than surrounding red blood cells
• Characterized by an audible “chirp” and simultaneous visual “HIT” on the screen

TCD - EMBOLI DETECTION
• Can detect the presence of embolic signals caused by the presence of a variety of materials, both gaseous and solid
• Cannot determine the size of an embolus
• Cannot determine the composition of an embolus
• Can detect particles as small as 50 microns
EMBOLI RECOGNITION International Consensus Committee
• Short < 0.1 second, 3-60 dB transients
• Unidirectional in spectra
• Occur randomly in cardiac cycles
• Change frequency within spectrum
• Audible sound: chirps, clicks, plunks
• Solid vs. air emboli distinguished by circumstance (solid designated when there is no invasion of vasculature)

EMBOLI DETECTION
• Carotid artery stenosis
• Arterial dissection
• Post endarterectomy
• Heart valve replacement
• Patent foramen ovale
• Atrial fibrillation
• Significant CHF
• Endocarditis
• Acute MI
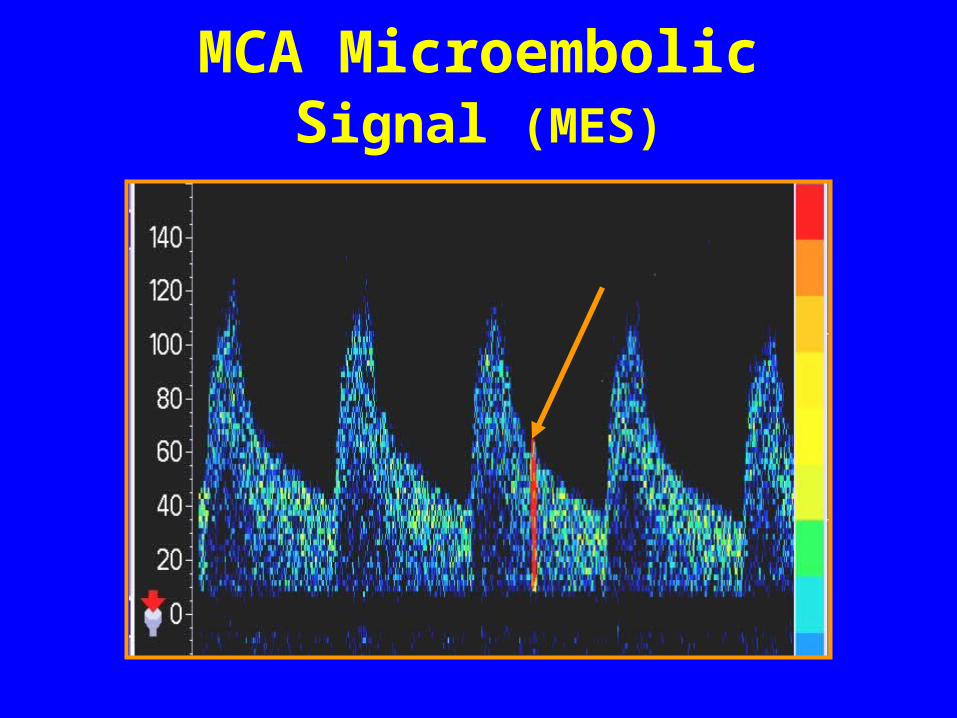
MCA Microembolic Signal (MES)

Transcranial Doppler
Paradoxical Stroke
and
PFO Evaluation

Ischemic Stroke
• Represents the third greatest cause of death in the western word
• Is the greatest cause of functional incapacity
• Origin is undetermined in 40% of cases according to conventional etiological criteria
Sacco R.L.,et al, Infarcts of undetermined cause: the
NINCDS Stroke Data Bank. Ann. Neurol. 1989:25:382-390

Cryptogenic Stroke
• Stroke of unknown etiology
• Suspicion of paradoxical brain emboli arising from the venous circulation
• Emboli from the venous system can pass to the arterial circulation through
a PFO (Patent foramen ovale)
Paradoxical Brain Emboli (PBE)
• Emboli whose source is not from an identifiable source in the arterial system
• Also referred to as venous-to-arterial emboli
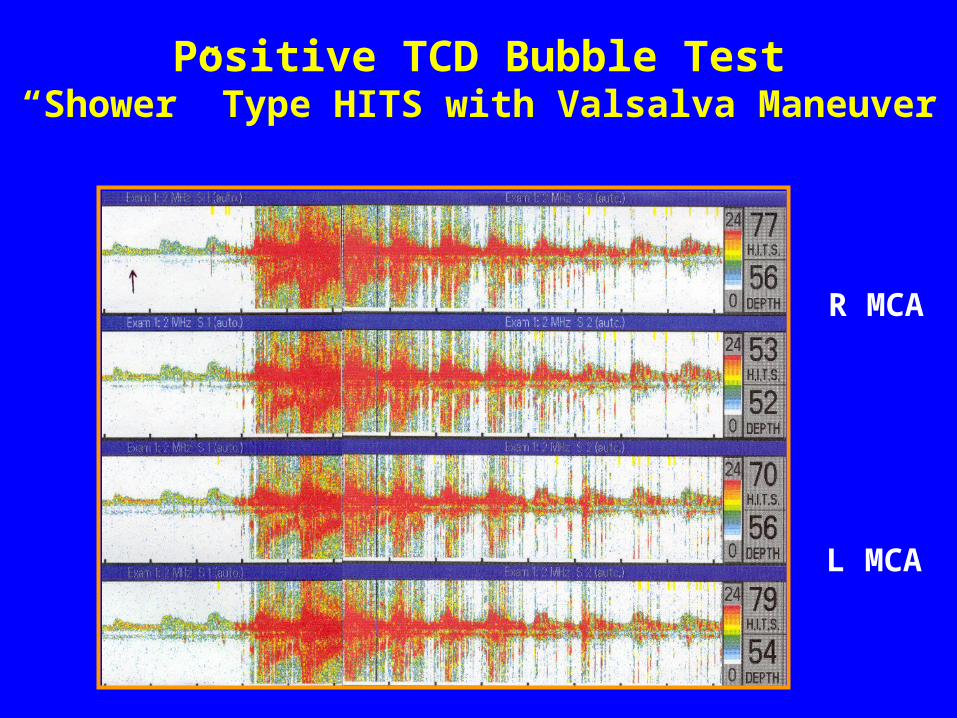
Positive TCD Bubble Test“Shower” Type HITS with Valsalva Maneuver
R MCA
L MCA
TRANSCRANIAL DOPPLER
Cerebral Circulatory Arrest
TCD - BRAIN DEATH
• Brain death is a clinical diagnosis
• TCD is a confirmatory test
• TCD can detect cerebral circulatory arrest

Transcranial Doppler
• Can aid in timing of other necessary tests
• Helpful in following potential organ donors
• Useful when patients are being treated with barbiturates which affect EEG
CEREBRAL CIRCULATORY ARRESTTCD Evaluation
• Bilateral study including posterior circulation
• Oscillating flow pattern persists over time (20 – 30 minutes minimum)
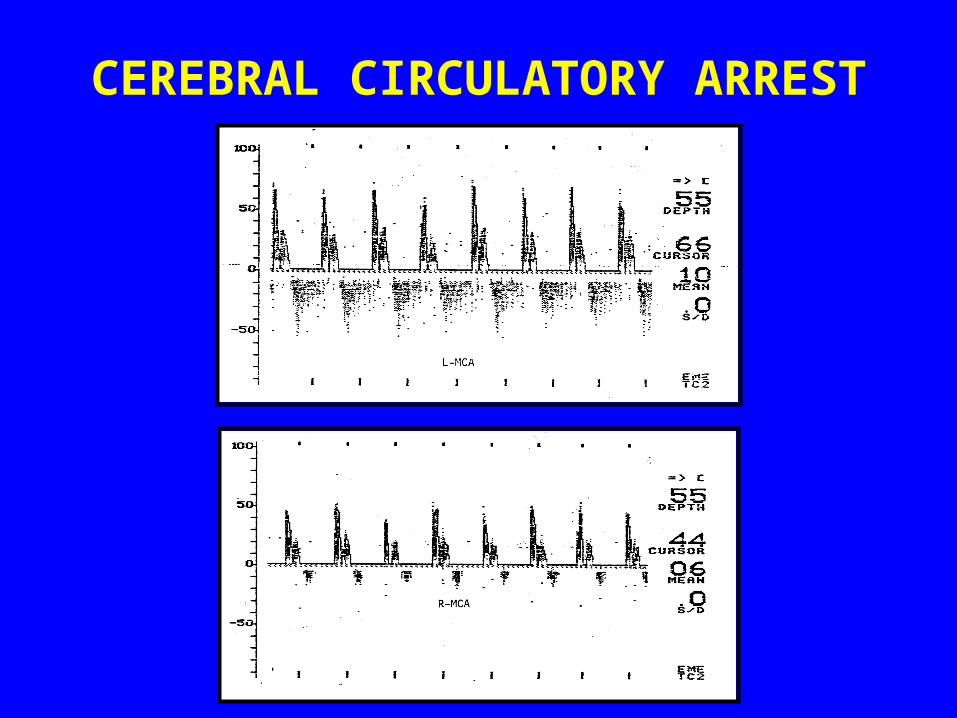
CEREBRAL CIRCULATORY ARREST