annual report and summary accounts 2007-2008 · pdf file · 2014-05-15annual report...
TRANSCRIPT

Pennine CareNHS Trust
Annual Report andSummary Accounts
2007-2008Specialist Mental Health Service
for Bury, Rochdale, Oldham,Stockport, Tameside and Glossop

2
ContentsIntroduction Page 3
Key developments Page 4
Our staff Page 7
Improving standards Page 9
An estate fit for purpose Page 13
Involving service users and carers Page 15
Challenging inequality Page 17
Foundation Trust application Page 19
Priorities for the future Page 20
The Trust Board Page 24
Statement of internal control Page 27
Report from the Director of Finance/Deputy Chief Executive: Page 31
Operating and financial review
Statement of the Chief Executive’s responsibilities as the Accountable Officer of the Trust
Statement of the Directors’ responsibilities in respect of the accounts
Independent Auditors’ Report to the Directors of the Board of Pennine Care NHS Trust
Income and expenditure account
Balance sheet
Statement of total recognised gains and losses
Cash flow statement
Remuneration report
Salary and pension entitlements of senior managers 2007/08
Obtaining further information Page 42
Glossary Page 43

Welcome.
We are delighted to welcome you to the 2007/08Annual Report of Pennine Care NHS Trust.
This has been a year of progress and significantchange for the Trust, as we have continued todevelop excellent services for local people whilstmaking big strides in organisational developmentand our Foundation Trust bid. The Trust’s progresshas been recognised externally this year – theHealthcare Commission officially rated Pennine Careas providing ‘Excellent’ services and ‘Good’ use ofresources. We have continued to improve the waywe work, introducing new ways of working whichmake our services better able to respond to theneeds of service users.
This year, the Trust has taken major steps towardsFoundation Trust status. We have recruited over10,000 members, including nearly 8,000 membersof the public from across our footprint. The Trustreceived Department of Health approval to proceedtowards Foundation Trust status and the process ofelecting a Council of Members is underway. This willbe a revolution in the way the Trust develops servicesfor local people.
The Trust has again achieved all of its statutoryfinancial duties. During the year our CapitalInvestment Programme was again a major challengeas we continue to work towards improving ourfacilities and building an estate fit for the twenty first century.
The work of the Trust’s staff has once again beenexemplary. Their efforts in improving services andproviding effective and efficient mental healthservices for all of our diverse clients are muchappreciated. We thank them for their continuinghard work.
This year we must pay tribute to our formerChairman Terry McCabe, who retired after leadingthe Trust since its creation in 2002. His leadershipand guidance made an enormous difference tomental health service provision across our Boroughs,and his years of service are to be commended. TheTrust’s new Chairman joins us at a hugely excitingtime as we move towards Foundation Trust status.The Chairman can make an enormous positivedifference to the Trust, building productive andwarm relationships with Directors and staff. A newChairman with a wealth of experience of the privatesector, and business and management expertise, willundoubtedly be of benefit to the organisation.
During the year the Trust has undertaken asignificant amount of Board development, equippingthe Board to carry out its oversight and advisoryroles as effectively as possible. At the same time, wehave become much more effective in driving forwardimprovements to services and our ambitious capitalprogramme by rearranging how we structure ourwork programmes. We are confident that our Boardand senior management team will continue toprovide the right skills and experience to makeprogress with our agenda and ensure we remainsuccessful and lead us to Foundation Trust status.
The coming year will be an exciting time for theTrust, and we look forward to making furtherprogress for our service users as we become aFoundation Trust and providing ever more effectiveservices across our footprint.
Introduction
Annual Report and Summary Accounts 2007-20083
John SchofieldChairman
John ArcherChief Executive

4
Key developmentsAchieving high levels of performanceThe Trust achieved higher performance againstthe ratings in last year’s Annual Report,obtaining a Healthcare Commission score of‘Excellent’ for service quality, increasing from‘Good’ last year. In addition, the HealthcareCommission gave the Trust a score of ‘Good’ forthe Auditor’s Local Evaluation and the way wemanage our finances. This is anotherimprovement from last year, and we are proudto have met our targets in this regard.
These scores confirm that the Trust is amongst thehighest performing Trusts in the country, and this is atribute to the excellent work of our staff.
The Trust has in place a robust and rigorousPerformance Assessment Framework which ensureswe will continue to improve our services by meetingall our standards as set out in ‘Standards for BetterHealth’, the Auditor’s Local Evaluation, and nationaland local targets.
Foundation Trust applicationThis year the Trust has made significant progress onthe journey towards Foundation Trust status. Wereceived Department of Health approval to proceedwith our application in March 2008. Following aperiod of assessment by Monitor, the government’sagency which oversees Foundation Trusts, we hopeto be confirmed as a Foundation Trust later on in 2008.
As part of preparing for Foundation Trust status, wehave recruited over 10,000 Trust members. We areon course to meet the target of 1% of the totalpopulation of our footprint, and we confidentlyexpect to exceed this during next year. A Council ofMembers will be elected, drawn up from ourmembership and allowing members to have muchmore of a say in how services are provided acrossthe Trust.
Business PlanningBuilding on work done last year in creating the firstIntegrated Business Plan (IBP) for the Trust, this yearhas seen further embedding of good practice around business planning. The IBP has beensubstantially refreshed, and business plans have beencreated for both the North and South Division, allDirectorates and support services. These follow aspecific template designed to link the Trust’scorporate objectives to the individual roles of staffwithin teams.
Work Programme Groups and theService Development StrategyLast year, the Trust developed a Service DevelopmentStrategy (SDS). This strategy sets out a five year planfor how we intend to continue developing andimproving our services. Work has continued towardsrealising the SDS this year, and the way that theTrust manages its services has changed as a result.
The SDS sets the Trust three main priority areas:l providing care closer to home
l fewer inpatient beds
l the development of specialist services
Work Programme Groups have been established tohelp realise the SDS. They will cover Adult AcuteServices, Adult Community Services, Older People’sServices, Child and Adolescent Mental HealthServices (CAMHS), Forensics, Substance MisuseServices, and Psychological Services. They arecharged with making sure that projects arecompleted and work carried out to a high standard.These new groups align services in a more effectiveway, ensuring that good practice can be sharedacross the organisation.
Developing new servicesThis year has seen a number of new servicesdeveloping for patients across the Trust.
Service users in crisis now benefit from improvedCrisis Resolution and Home Treatment (CRHT) teams,which have been developed this year to act asgatekeeper for all admissions into inpatient beds,and to provide a more appropriate response tocrises. The CRHT teams can provide intensive homebased treatment for service users, allowing them tomaintain a 24/7 level of independence even at timesof greatest need.

In Oldham, New Ways of Working have beenpiloted, with our Consultants changing the way thatthey work, and becoming based either in communityor inpatient teams. Once again, this change toworking practices has led to a more effective use ofour resources to provide a better service to patients.
The way that admissions are handled out-of-hourshas changed with the introduction of the ‘Hospitalat Night’ project. This has seen the creation ofspecialist teams able to handle liaison with hospitalsout-of-hours, reducing the burdens on juniordoctors, ensuring Trust compliance with theEuropean Working Time Directive, and providing aconsistent service across the Trust.
The Trust continued on its ambitious programme ofservice development. We successfully won a tenderfor the provision of new low secure services and are on course to open a new Young Person’s Unitnext year.
Engagement strategiesThe Trust has undertaken wide consultation withPrimary Care Trusts, Local Authorities, Joint Overviewand Scrutiny Committees, Joint Consultation andNegotiation Committee (JCNC/staff side/unions) ondeveloping our service over the next few years. A full consultation strategy was developed by theTrust to support implementation of the ServiceDevelopment Strategy.
This consultation began in September 2007 to gainsupport for service changes (ward closures, dayservice changes etc.) to deliver services for 2008/09.Meetings continue with all our partners to ensurecontinuing support for the Trust’s overall direction.
The Trust continues to work to strengthen the veryvaluable relationships we have with our partners.Partnership working is vital to continually improveservices, and the maintenance and development ofour work with partners will remain at the forefrontof our endeavours in the future.
Improving the patient environmentIn 2007/08, the Trust invested over £12 million toimprove inpatient and community facilities.
This year the Trust was proud to formally open theIrwell Unit in Bury, and the newly refurbishedservices in Rochdale.
In addition, we have made significant progressimplementing standards around privacy and dignity,and improving gender separation on inpatient wards.
We believe our service users should receive care inthe most dignified and comfortable settings andduring 2007/08, we commissioned a number ofschemes to improve the inpatient environment inStockport, Tameside and Bury and invested in anumber of projects to improve ward and communitypremises across the Trust.
Key developments
Annual Report and Summary Accounts 2007-20085
The new Irwell Unit in Bury
The new CAMHS reception at Birch Hill Hospital

6
Key developmentsDevelopment of CAMHS and SMS DirectoratesWork has continued to provide more specialistservices in a more effective way. With this in mind,the Trust has established directorates for SubstanceMisuse Services (SMS) and Child and AdolescentMental Health Services (CAMHS). This newarrangement will allow the services to grow anddevelop their own specialisms whilst still retainingthe support and expertise of the Trust.
Better information, better servicesWe have continued to build on the successfulimplementation of the National Care Records System(NCRS) across the Trust, and are building onproviding ever more useful information on theservices which we provide. The Trust is delighted tohave been chosen as a pilot for the implementationof the next stage of the National Programme for ITand it is hoped that this will provide even moreinformative data to help plan future services andstrengthen relationships with commissioners.
In addition to this, the Trust has beenundertaking a project with our five maincommissioners to develop a mental healthcurrency for future contracts. This work is using15 care groups to describe the range of servicescommissioners want and the Trust provides. Theaim of developing these care groups andproviding evidenced-based pathways of careleading to better outcomes for patients.
Karen Tipping, the Drug Liaison Midwife at theRochdale Community Drug Team

Consulting with staffThe last year has proved to be another yearwhere the time, skill and commitment of ourworkforce have contributed to the Trust’s manyachievements. Throughout the early part of theyear, discussions with staff as well as manystakeholders began, to think about how wecould improve the organisation.
In July, we held a major consultation event, whichtook place with staff to explore views and listen totheir ideas of what Pennine Care should stand forand what sort of organisation we should be. Over150 staff joined together to develop a range of ideasand principles that will help build our vision for theTrust and its Organisational Development (OD).
The outcomes of those discussions included thefollowing organisational promises: l A promise that the Trust would be a listening
organisation, involving and supporting all staff and investing in them to be successful, making Pennine Care a great place to work
l A promise to our commissioners to always deliver the most effective services possible, highly competitive in both quality and efficiency and to always involve commissioners in the development of the organisational goals
l A promise to our service users and carers to provide the best patient care experience possible, deliver consistently and always preserving dignity and promoting choice of recovery
l An investment of over £1 million over the next two years to support the staff development agenda
Consultation with staff has continued with thedevelopment of focus groups to build on these key promises.
New skills and investmentWe have established an Organisational DevelopmentSteering Group which led to the construction of ourWorkforce and People Strategy. This work includedthe development of staff focus groups, a refreshedtraining strategy for clinical and managementtraining more explicitly related to the ServiceDevelopment Strategy.
As part of the OD Strategy, investment in today’sleadership and tomorrow’s ‘Rising Stars’ is essentialto drive forward the Trust’s Business Plan. Thisinvestment began with a number of programmesincluding:l Individual coaching for associate directors and
other senior staff
l A coaching skills programme for senior managerial staff so that they would also be able to support and guide other staff
l The commissioning of a highly successful team leaders’ and managers’ development programme to provide intense development time for all team leaders in Pennine Care
l Five Leadership Bursaries which anyone across the Trust could apply for to improve their leadership skills and provide a positive benefit back into services for the Trust, Service Users and/or our Partner Commissioners
Our staff
Annual Report and Summary Accounts 2007-20087
Staff at the Organisational Development day‘Rising Stars’ bursary winners

8
Our staffA Great Place to WorkAs part of this goal, the Trust held its third annualAwards Ceremony in November 2007. The ceremonywas the biggest to date. All Trust staff were asked tonominate a colleague or colleagues who in theiropinion had shown commitment to their role in avariety of areas and ways. There were 11 categoriesranging from Nursing Excellence (The Claire HodgsonAwards) to individual excellence, equality anddiversity, social inclusion, work above and beyond,lifetime achievement award and team of the year.This year saw a record 289 nominations.
The Trust recognises both the excellence andcommitment of its staff. To that end, Long ServiceAwards were held at a separate event in February2008. Staff were recognised for 25 years service withPennine Care and its predecessor Trusts, and werethanked for their service to the Trust and the NHS.
Improving Human Resources in the Business HubsDuring 2007/08, members from the HumanResources Department began working as part of theBusiness Hubs established in the North, South andForensics Division. Other members of the hubsinclude Finance and Information and Performance.This has proved to be very successful in identifyingand aligning strategic issues with Boroughobjectives. In particular, there has been a significantimprovement in ensuring workforce issues are an integral part of the business planning and delivery processes.
As a way of strengthening management informationand ensuring the impact of changes are understoodand acted upon, Key Performance Indicators (KPI)continue to be developed and shared within the hubs.
Investment in trainingTraining and Development of staff has been a majorfocus this year. The Trust has in place a robustmandatory training programme. This focuses onhealth and safety legislation, employment andclinical practice. As well as this, there are trainingand development opportunities available forAdvanced Practitioners and Assistant Practitioners.
Whilst there has been much success in supportingindividual staff to develop, the Trust is committed tomaking further improvements in 2008/09 to ensurethat training and development opportunities reachand benefit more staff.
Work has commenced this year to review learningand development, and a new Learning andDevelopment Strategy will be launched in Summer 2008.
National developments and our staffAction continues to realise the benefits of a range ofnational initiatives to modernise our workforce andincrease productivity. These include the furthertraining and introduction of Assistant and AdvancedPractitioner roles and the roll out of the Hospital atNight teams. We have also made improvements tothe recruitment and selection of nurses to our nursebank, refined our job evaluation processes andstrengthened the equality and diversity team in orderto support embedding and implementation ofequality legislation at Borough and service level.Human Resources policies have been reviewed totake into account employment legislation,particularly in relation to the care of vulnerableadults and children and the amendments to theMental Health Act.
The Trust is particularly fortunate in having thesupport and advice of Staff Side Representatives whohave actively contributed to the shaping of bothpolicies and service development.
Celebrations at the Trust Awards

Our governance systems work to continuouslyimprove quality and safety for service users andstaff. All areas of the Trust work in anintegrated way in order to ensure learning inone area is incorporated across the organisation.
Standards for Better Health core standards set by theHealthcare Commission (HCC) contribute tostrengthening our governance framework andquality improvements. This year, the Trust was fullycompliant with these standards for the secondconsecutive year.
This year, the Trust further improved its rating underthe Healthcare Commission Annual Health Check.Having scored ‘Good’ for Quality of Services and‘Fair‘ for Use of Resources in 2006/07, we improvedto ‘Excellent’ Quality of Services and ‘Good’ Use ofResources in 2007/08.
The Trust’s framework for monitoring quality isoverseen by the Risk and Clinical GovernanceCommittee, which has full multi-disciplinaryrepresentation from across the organisation. This isstrongly linked with Borough governance groups andother Trust forums to ensure governance is fullyintegrated across all areas.
Patient safety Patient safety continues to be at the centre of theTrust’s governance arrangements.
During the past year Professor Paul Rogers, Professorin Forensic Nursing, University of Glamorgan andBroadmoor Hospital, and colleagues visited the Trustand co-ordinated focus groups.
Following on from the focus groups, training wasdeveloped focusing on the evidence base for riskassessment. A wide range of clinical staff attendedthis from all services across the Trust. This work isintended to continue with a review of riskassessment procedures and processes using theDepartment of Health Best Practice in Managing Risk (2007).
The Trust continues to look at upgrading clinicalequipment across the organisation. New ECGmachines were purchased in 2007 to ensure safetyand standardisation within units. This will supportconsistency in training and promoting use of routinemonitoring in relation to physical health.
The Trust continues to implement the CSIP suicideprevention audit to ensure that the standards areembedded into clinical practice.
An extensive programme of window replacement hasbeen completed in all acute inpatient areas across theTrust. The new design of windows will have reducedligature fixtures and improve ventilation.
The Trust has also invested in a new secure vehicle totransfer patients in a safe, dignified way acrossBoroughs and other areas with trained drivers.
The Trust has continued to report all safety incidentsto the National Patient Safety Agency (NPSA),through the electronic National Reporting andLearning System (NRLS). The national data on patientsafety incidents allows NHS organisations tobenchmark their incident data with other Trusts.
Through the NRLS in 2007, the NPSA published areport on slips, trips and falls in hospital to improveunderstanding of the scale and impact of falls withinthe NHS. The Trust used the best practice identifiedin the report to develop a falls prevention strategy. In addition, a number of clinical staff were funded toattend the Falls Prevention National Conference inMarch 2008 to ensure the Trust continues to buildinternal expertise around falls prevention. This willcontinue to be a priority for 2008.
Improving standards
Annual Report and Summary Accounts 2007-20089
The secure vehicle service ensures safe transferof service users

10
Improving standardsSeven steps to Patient Safety (NPSA NHS 2004) hascontinued to be implemented with an on-goingaction plan to ensure we promote patient safety.There is a quarterly Integrated Governance Reportand publication ‘Governance Matters’ that identifieskey learning themes for staff.
Training continues for all new staff promotingpatient safety and a positive reporting culture. Riskawareness is included in induction and mental healthpractitioners training.
The Trust provided Root Cause Analysis training forstaff to improve awareness into investigations ofserious and untoward incidents.
Mandatory training continues to be provided inrelation to life support skills, infection control,medicines management, patient moving andhandling, and management of violence andaggression.
During 2007 we have continued to activelyparticipate in establishing and developing the LocalSafeguarding Children Boards across the PennineCare footprint and continuing to undertake training to all staff groups. We have seen majorimprovements to the child visiting facilities across theTrust and this work will continue as part of theTrust’s service developments. The Trust has fulfilledits responsibilities for safeguarding children as part ofour inter-agency work, whilst responding to national,regional and local requirements.
Infection Control and Physical HealthThe Trust is striving to prevent and control healthcareassociated infections by embedding high standardsof infection prevention and control into everydayPractice. A range of initiatives are in place to enableus to achieve this.
The Training Department ensures that all new staffundertake mandatory hand hygiene training as partof their induction and then annually thereafter. The‘glow and tell’ machine is used as a teaching toolwithin the clinical areas, ensuring staff use thecorrect hand-washing techniques.
All staff are undertaking the e-learning InfectionControl package to increase their knowledgeregarding infection prevention and control.
There is also a resource file for staff in order todevelop their knowledge in relation to infectioncontrol and physical healthcare.
The Trust has signed up to the NPSA ‘Clean YourHands Campaign’, which will provide educationalresources for staff and posters for wards to increasethe awareness of the need for good hand hygiene.
The Trust is compliant with the Health Act and hasachieved a score of 92.9% in the Essential Steps toSafe, Clean Care Self-Assessment.
Clinical EffectivenessNICENational Institute for Health and Clinical Excellence(NICE) guidance continues to be a priority. This year has seen the establishment of the NICEImplementation Group, which will improve the wayin which NICE guidance is managed andimplemented across the Trust whilst helping the Trustto maintain its core and developmental standards.This group will look forward to promoting anddeveloping evidence-based practice and monitoringthe implementation of national guidance through avariety of quality improvement projects.
Dr Sudhir Kaligotla, Medical Director and David Curtis, Director of Nursing and IntegratedGovernance, try out the ‘glow and tell’ machine
with Catherine Forman, CNS InfectionControl/Physical Health Lead

Physical health projects The Clinical Nurse Specialist for Infection Control andPhysical Health Lead appointed last year hascoordinated a review of the physical wellbeing ofservice users in key areas including Obesity and HandHygiene. These quality improvement projects havehighlighted areas for implementing and sharing bestpractice including the dissemination of learningmaterials and training across the Trust.
Suicide PreventionDuring 2007/08, the Trust has continued to auditand monitor the standards on Suicide Preventionfrom the Care Services Improvement Partnership(CSIP). We have sustained our efforts to reduce thenumber of suicides by people who are in contactwith mental health services and in turn promotemental health among vulnerable groups. Thequarterly results continue to help form and advisepart of the Trust’s Suicide Prevention Work Plan, byhighlighting the areas where improvements can bemade and by sharing learning outcomes. Thisprocess has been instrumental in demonstrating ourongoing compliance with the CSIP standards.
Quality mattersThis year, we welcomed the launch of ‘QualityMatters’, a Clinical Governance awareness event thattook place on 4th March 2008. The event was wellattended and presentations focused upon qualitywithin clinical effectiveness from a diverse range ofprofessional perspectives. The events will continuetwice yearly as staff conduct a range of significantquality improvement projects, share learning andpromote evidence-based practice.
Implementing Best PracticeAs part of the progress with our ServiceDevelopment Strategy, we have reviewed ourprocedures for promoting and implementingevidence-based practice and incorporating values ofrecovery and social inclusion. In particular we havesought to streamline the introduction of nationalguidance by ensuring robust clinical and professionalengagement. A new Clinical and Social Care Boardhas been established to facilitate this. Its initial focushas been on the review of action plans andprocesses based on guidance from the NationalInstitute for Health and Clinical Excellence.
Linking different areas of governance is key toensuring improvements in quality. As part of ourongoing clinical review and learning process forserious incidents we have now linked a concurrentreview of Suicide Prevention standards. This is aunique approach, which promotes full clinical teaminvolvement in both the timely review of incidentsand in the audit of standards for suicide prevention.Results are monitored quarterly with learningdisseminated to staff and this informs the Trust’sSuicide Prevention Strategy.
Central to governance for evidence-basedpractice is the dissemination of relevant guidanceand policies to staff supported by relevanttraining programmes. A number of key areashave been considered this year including manymedication-related protocols/policies, riskassessment, self-harm, falls prevention,complementary therapy and physical healthcare.
Comments and complaints
We aim to provide the highest possible standard ofcare and want everyone who uses our services, orcares for someone who uses our services, to haveconfidence in them and feel safe. The Trustrecognises that, however diligent and skillful ourstaff are, there will inevitably be circumstanceswhere service users’ expectations have not been metand they will need to voice their feelings.
The Trust takes all complaints seriously and they arefully investigated following national guidance.Actions are taken to address the issues of concernand to provide an explanation. Last year (2007/08),the Trust received 130 formal complaints, which is asmall decrease on the previous year (2006/07). Ofthese, 96% were responded to within the targetresponse time of 25 working days.
This response rate has been achieved due to anumber of factors, including the streamlining of ITsystems, the development of new investigationguidance and training and the commitment and hard work of all staff involved in complaints handling.
We have also dealt with a total of 112 furtherconcerns informally. These are still taken veryseriously, and investigated and responded topromptly, but have been resolved by local servicemanagers working with the complainant to try toaddress and resolve the issues directly.
Improving standards
Annual Report and Summary Accounts 2007-200811
12
Improving standardsLearning from complaints
We are keen to ensure that complaints areinvestigated as fully as possible and makerecommendations where needed to prevent thedifficulties being repeated.
The following are examples of how services havebeen improved following receipt of complaints:l Development of a protocol in partnership with
local Acute Trusts regarding liaison around shared care and the transfer of patients
l Development and implementation of a policy on using bed rails safely and effectively
l Clarification of the patient property procedure to ensure items taken into safe keeping are properly documented and witnessed
The NHS Complaints Procedure is currently underreview and this is likely to lead to some changes in2009. At this point, the Complaints HandlingTraining will be updated and disseminated to staffacross the Trust.
Compliments
The Complaints Department continues to receivecopies of compliments from service users and carerswho have taken time to express their positivecomments about the care and treatment provided byPennine Care NHS Trust staff. During 2007/08, 249such compliments were received by the Trust.
It is important for staff to be recognised for theirachievements and line managers are reminded toencourage staff to share any positive feedback theyhave received. Each compliment is personallyacknowledged by the Chief Executive and reportedto the relevant Trust forums.

Transforming our facilitiesIn 2007/08, the Trust carried out an extensiveprogramme of improvements to the Estate,investing £12 million to deliver new andimproved facilities for our services and staff.Improvements were seen in each Borough andthe main schemes were:
Section 136 Schemes in each Borough
Section 136 facilities were completed in eachBorough. This work commenced in 2006/07, inconjunction with the police and in line with newnational guidance for the use of Section 136 (thepolice power to remove persons believed to besuffering from mental disorder from a public place toa place of safety to facilitate a mental healthassessment). New facilities are now operating ateach main site.
Patient Environment Action Team
A number of schemes were delivered during2007/08 in the patient environment, including newfurniture and new activity equipment for patients inall Boroughs.
Maintenance
2007/08 saw the first full year of operation of theTrust’s in-house maintenance team. The serviceincludes a maintenance assistant based on eachmain hospital site supported by a central team ofskilled staff who provide planned and responsiveservice across all Boroughs. The service also includesa helpdesk function and a 24-hour on-call service.
Capital investment
Four major capital schemes were completed during2007/08.
In September, Ivan Lewis, MP for Bury South andMinister for Social Care officially opened the newlybuilt Irwell Unit at Fairfield General Hospital. The unitprovides two new adult wards in significantlyimproved accommodation.
In October, the Trust opened the new ward 21 atTameside Hospital, a 17-bed Older People’s wardbased on the ground floor of the Mental HealthUnit. The ward provides interim accommodationpending the move to the new 48-bed Older People’sMental Health Unit in 2009.
In November, a scheme to improve the MentalHealth Unit at Stockport was completed. The schemeprovided a garden area that had been developed inconjunction with the King’s Fund, a new café forservice users and staff, new reception facilities foroutpatients, and an extension that provided newconsulting offices.
An estate fit for purpose
Annual Report and Summary Accounts 2007-200813
Ivan Lewis MP, carer Lily Reid and John Archer,Chief Executive, unveil the plaque at the official
opening of the Irwell Unit
The Oasis Café is a welcome retreat at Stepping Hill Hospital
The therapeutic garden haven at Stepping Hill Hospital

14
An estate fit for purposeAlso in November, the refurbished adult inpatientunit at Birch Hill Hospital in Rochdale wascompleted. The refurbishment provides a wide rangeof improved facilities for patients.
In addition, this year saw the completion of theHealth Improvement in Tameside (HIT) scheme,providing a very large investment in new healthservice facilities for the people of Tameside.
The rest of the Trust also benefited from additionalcapital investment, including:l A series of schemes to improve the safety of
patients and staff at a number of locations. The Trust is committed to providing a safe and secure environment for our patients and staff and to support this, improvements were carried out that included improvements to CCTV, access control, staff alarm systems, external lighting and increased security patrols
l A programme of window replacement within inpatient areas in Bury, Tameside and Stockport providing safer windows that also improved air circulation
l The commencement of the following schemes that will complete during 2008/2009:• The development of a new 12-bed Young
Persons’ Inpatient Unit in Bury
• The development of a new 16-bed Older People’s ward in Bury
• The refurbishment of Moorside Ward, Rochdale
• The refurbishment and extension of Rowan Ward, Oldham
• The development of a new 15-bed Older People’s ward in Stockport
• The development of a new 20-bed Low Secure Unit in Tameside
• The development of secure garden areas for inpatients at Birch Hill Hospital
DDA ComplianceDuring 2007/08 the Trust made furtherimprovements to facilities for the disabled, includingthe installation of access ramps, automatic doors anddisabled car parking spaces.
Privacy and DignityThe Trust also carried out a series of improvementsto enhance gender segregation in inpatient areasand to develop multi-faith facilities and child visitingrooms at each main site.
The newly refurbished premises at Birch HillHospital in Rochdale were officially opened onthe 7th September by Paul Rowan MP (centre).Pictured left to right is Stephen Netherwood,
Head of Service, Adult Care Rochdale MBCAdult Care Service; Jean Ashworth, RochdaleMBC; Barry Windle RMBC and Terry McCabe,
Trust Chairman
An artist’s impression of the HealthImprovement in Tameside (HIT) scheme

The Service User and Carer Involvement Forumcontinues to improve consultation amongst theTrust and its service users. Two service users andtwo carer representatives are elected from eachBorough, and the Forum has continued to meetmonthly during the course of 2007. This yearhas seen some important consultation with theForum, including updates regarding the Trust’sapplication to become a Foundation Trust, andupdating the Trust’s Patient and PublicInvolvement (PPI) strategy.
The Trust recognises that effective engagement andinvolvement is essential to the delivery of excellentservices, in particular through learning from theexperiences of service users and carers. It alsorecognises that, to be effective, public and patientinvolvement takes a variety of forms. We haveincreased investment into our Patient Advice andLiaison Service (PALS). The Public and PatientInvolvement Forum (PPIF) is represented on the TrustBoard. In addition, the Trust now supports localinvolvement networks (LINks), which havesuperseded the PPIF.
Consultation has led to some significantimprovements this year. For instance, following aconsultation event, a training package focusing oncustomer care and values was developed by serviceusers and carers and will be delivered by them at theinduction of all new staff. Service users and carersare also involved in training our Support, Time andRecovery (STaR) workers.
To support effective involvement, the Trust hasdeveloped a policy that details the areas in which it expects its staff to involve service users and carersand the payments that will be made to reward that involvement.
Volunteering
Volunteering is another effective way of involvingservice users, carers and the public. Following thedevelopment of the volunteering policy, work hascontinued to establish an infrastructure to supportvolunteering across the Trust’s footprint. There isnow a volunteer coordinator in each of theBoroughs, and placements have been established formore than sixty volunteers.
Each volunteer has an identified placementsupervisor, and the coordinator offers an annualpersonal development planning opportunity. Peoplewho wish to can then move on to volunteer workplacements to help them identify their readiness toapply for paid employment.
The Trust continues to offer places on the accreditedvolunteer training scheme and also offers acomprehensive induction training day. The Trustrecognises the immense benefits that volunteersbring to the organisation, and continues to paytribute to the hard work of our selfless volunteers.
As well as offering practical support to volunteers,the Trust has decided to offer its own thanks withthe introduction of an annual Volunteers’ Lunch.
In recognition of the contribution volunteers make tothe Trust by enhancing the services it offers, thelunch is attended by volunteers, service users andthe Board.
Involving service users and carers
Annual Report and Summary Accounts 2007-200815
Members of the Trust Board presented certificates to volunteers

Oldham Stockport Rochdale
Bury Tameside
The artwork on this page was created byservice users on Wards 35 and 36 during OTSessions. Each piece had a photograph as astarting point and different techniqueswere utilised.
Oldham – This image was created directlyfrom the original photograph which wastransferred to computer. The final pieceillustrates the fact that the market has beenan integral part of Oldham Town Centre formany years.
Stockport – The viaduct in Stockport, hasalways been a key visual feature of thetown centre, this bold, uncomplicatedwater-colour, emphasises the structure,uncluttered by modern architecture.
Rochdale – An original pencil drawingwas transferred to computer andenhanced with blocks of colour, whilstretaining the artist's original pencildrawing.
Bury – The design of the building suggestedan Art Deco approach. This wasexaggerated in the stylised reflection of thesky in the plate glass windows.
Tameside – The artist worked in pen and inkon the original colour photograph. Thistechnique, whilst effective as a piece ofartwork, gives the suggestion of anarchitectural drawing.
Thank you to all who contributed theirartwork and to Neil Smith, TechnicalInstructor, for co-ordinating the project.
16

Over the last year, awareness of the importanceof challenging inequalities faced by peoplewith mental health problems has steadilyincreased within Pennine Care. Numerouspositive developments have occurred as a resultof a focused approach to challenging inequalitythat includes:l Involvement of diverse service users and staff
l Training and development
l Wider equality monitoring
l A firm commitment to developing a central Equality and Diversity team
l Improved structures for reporting on equality and diversity
Equality SchemesThe Trust has Equality Schemes and action plans fordisability, gender and race. As a specialist mentalhealth Trust, Pennine Care is committed toembracing national agendas that challengeinequalities experienced by users of mental healthservices and also support diverse staff. As such, theRace Action Plan specifically incorporates actionpoints related to the national Delivering RaceEquality in Mental Health Strategy (DRE), and theTrust continues to produce an annual ‘Count Me in’Census report where the equality profile ofinpatients is recorded and analysed for informationto improve the Trust response to service user needs.
Additionally, the Trust’s Gender Equality Schememakes specific reference to the nationalimplementation guidance ‘Mainstreaming Gender & Women’s Mental Health’.
Equality and Diversity TrainingOver the past 12 months, Trust staff have accessedEquality and Diversity training that includes the e-learning package ‘Respect for People’, drama-based Managing Diversity Sessions. CAMHScultural competency training and Equality Impactassessment training have also taken place.
Staff have introduced the learning from thesesessions into everyday practice and interaction withothers. In the recent staff survey, more staff told usthat they were benefitting from this equality anddiversity training.
Diversity support within the TrustThe Trust Black and Minority Ethnic Staff Networkhas gone from strength to strength. In October2007, the formal launch of the network took placeat Dukinfield Town Hall. The keynote speaker wasJulie-Jaye Charles, Ministerial Adviser and CEO of theEqualities National Council. The launch was wellreceived and involved a range of staff and partnersas attendees and presenters. The outcomes of thisday will influence future actions for staffdevelopment and improvements to service.
Equality and Diversity training
BME Staff Network launch. David Curtis, Director of Nursing and Integrated Governance,
Julie-Jaye Charles and Mansoor Shah
Challenging inequality
Annual Report and Summary Accounts 2007-200817

18
Challenging inequalityActive membership of the Trust-wide Equality andDiversity steering group has increased to incorporatethe full range of the Trust’s clinical divisions, medical staff and corporate services. This ensures awhole organisation commitment to challenginginequality and aids with embedding equality anddiversity as a mainstream vision for all services andorganisational functions.
Involving service users and staffThe Trust has actively sought the opinions of serviceusers and staff through involvement that includesgender equality and staff network surveys.Additionally, equality monitoring has improved.Incidents and complaints are now monitored acrossthe equality groups. Equality information collectedby HR has also improved. Such involvement,monitoring and analysis enables the Trust to see where gaps exist in service delivery andemployment issues.
Supporting diversity in servicesThe Trust is committed to developing services thatrespond to diverse needs. This sometimes meansthat targeted services are required. In line with this,the Trust has gender and ethnic specific services,such as Asian men’s and Asian women’s sessions inRochdale and a Women’s Unit in Forensic and HighSupport Services. Furthermore, the Trust has made anumber of improvements to our premises to improvefacilities for disabled access. A scheme to providemulti-faith rooms at each main site has also commenced.
Communicating progress in challenging inequalitiesis important. To this end the Trust has an equalityand diversity section on its website, and each editionof the Trust newsletter includes an equality anddiversity-focussed article. In the past twelve monthsthis has included information on the Black andMinority Ethnic staff network, a wall hangingcreated by service users and donated to the multi-faith room at Tameside Hospital, DisabilityAwareness Day, increased work with South Asianolder women, and Delivering Gender Equality.
Whilst we have not eliminated problems related toinequality, within Pennine Care clear improvementshave been made. We are proud of this progress andall achievements but also acknowledge that thereare still issues to be addressed around inequality andaccess to appropriate services based aroundcharacteristics such as diagnosis, race, gender(including transgender), language, sexual orientation,age, ethnicity, disability, religion and belief. The Trustis committed to continuously addressing andpreventing inequalities where they exist so thatservice users and staff can experience equality ofopportunity in access to and experience of servicesand employment.
Wall hanging donated to Tameside Multi-Faith Prayer Room
Following a successful diagnostic assessment, theTrust has been actively progressing itsFoundation Trust (FT) application, and is aimingto become a Foundation Trust in 2008. Monitor,the government agency charged with overseeingFoundation Trusts, is visiting the Trust betweenApril and June 2008, with the aim of beingauthorised as a Foundation Trust on 1st July.
Becoming a Foundation Trust will provide a numberof benefits. It will:l Enable greater involvement of the local community
and staff in the development of services
l Allow the Trust to respond to what local people want and need from their local health services
l Give freedom to develop improved mental health services
l Offer the opportunity for greater financial flexibility
l Offer access to additional funding sources
l Generate greater organisational freedom to fulfil local priorities
l Reduce the burden and bureaucracy of central monitoring while still ensuring high service standards are maintained
Membership is centralto the ‘mutual’ modelon which FoundationTrusts are based. By giving staff,
patients, partners and the public a real stake in theTrust, the organisation has been set the challengeof transforming itself into an outward facing,locally owned organisation, which can deliverbetter services to its communitiesas a result.
Membership is free andprovides the opportunity to:l Become actively involved in
the work of the Trust and shape future plans
l Get better understanding of mental health and substance misuse services
l Help stamp out stigma and discrimination
l Elect member councillors
l Make sure the views of local communities are heard
l Receive information about the Trust and how it is performing
Becoming a member of the Foundation Trust wouldprovide our service users, carers, local residents andstaff with the opportunity to influence how wedevelop mental health services locally, as well asenable them to be involved in decisions regardingthe future direction of the Trust. Further informationon how to become a member of the FoundationTrust may be obtained from the Trust website atwww.penninecare.nhs.uk or alternatively from:Membership OfficePennine Care NHS TrustTrust HQ225 Old StreetAshton-under-LyneLancashireOL6 7SR
Telephone: 0161 604 3374
Work is underway for the first elections to theCouncil of Members, which will allow electedmembers of the Trust to have a much greater levelof involvement with our services. This has involvedworkshops across our footprint for membersinterested in playing a greater part and becomingMember Councillors. Elections have been scheduled,and will allow all members to vote for representativeMember Councillors in their Boroughs or staffgroups. The Council of Members will be in place bythe time the Trust is authorised as an FT and will playa valuable role in overseeing the Trust’s activities anddriving forward the future direction of our work.
Lisa Howarth dresses upat an FT membership
recruitment event
Karen Byrne (middle) and Nicola Grimleyparticipate at an FT membership
recruitment event
The Trust’s anti-stigma logo
Foundation Trust application
Annual Report and Summary Accounts 2007-200819

20
Priorities for the futureOur Strategic GoalsThe Trust is clear about its priorities for thefuture. We have a vision, ‘making people feelbetter’ that is simple and well understood byeveryone. Our main aim and corporate objectivesand priorities for 2008/09 flow from this.
To achieve this vision, the Trust’s Board and seniormanagement team developed five key strategic goalsin January 2008, which are driving and shaping thebusiness of the Trust.
These strategic goals recognise the importance of awide range of factors necessary to develop theTrust’s services.
Service ExcellenceThe Trust has made significant strides towards thisgoal, and the high quality of our services wasrecognised by the Healthcare Commission, whichawarded the Trust a rating of ‘Excellent’ for servicequality in late 2007.
In the year ahead, the Trust will continue with itsambitious programme of service development.
After successfully bidding to provide 20-bed lowsecure service, we will deliver this facility by June2009 by redesigning our current service provision at Tameside.
In addition, a new Young Persons’ Inpatient Unit forchildren and adolescents will open in Bury in May2008, giving local people the chance to benefit fromthis type of facility for the very first time.
We will also deliver a new Specialist Step Down Unitfor older people in Stockport.
During the coming year, the Trust will also developits Early Intervention Service, creating a Trust-wideapproach to this vital and often overlooked elementof mental healthcare.
The Trust has completely redesigned Crisis and HomeTreatment services, to manage admission to the
acute wards and drive efficiency in the inpatientsystem, including reducing occupancy by providing a more effective alternative to inpatient care in acrisis situation.
The Trust is developing a range of Care Pathways toset down ideal standards of care and outcomes forall patients entering the Trust’s services. Not only willthis provide a clear framework of care for patients,but it will also show commissioners the ideal level ofservice required.
Crucial to the realisation of the business plans will bethe implementation of Work Programme Groups todrive forward changes and service developments.These Work Programme Groups will be organised ona Trust-wide basis to implement improvements toservices within their remit, such as older people’sservices and adult community services.
The Trust has developed CAMHS and SMSdirectorates this year, including broadening what theTrust offers to attract new business, and in terms ofproviding a better service to those patients already inthe care of the Trust. This will be particularly evidentwith the new facilities due to come on-line duringthe year, such as the new Young Persons’ InpatientUnit due to open in Bury in May.
An objective of the Trust for the coming year will beto implement our Psychological Services strategy andincrease capacity in line with NICE guidelines.
Strategic Goal High level measure
ServiceExcellence
Achieving ‘excellent’ for theAnnual Health Check from theHealthcare Commission
Retain andexpand highquality services forcommissioners
Achieving the next three yearsigned contracts and contracts forYoung Persons’ Unit and LowSecure service
To be a greatplace to work
Achieving the outcomes in theOrganisational DevelopmentStrategy related to Trust Promise,Learning and Development,Engagement and Celebration andSustainable Leadership
Effective use ofresources
Achieving at least ‘good’ in theAuditor’s Local Evaluation as partof the Annual Health Check
To become aFoundationTrust
Passing through Department ofHealth and Monitor assessmentprocesses and becoming alicensed Foundation Trust in2008/09

Priorities for the future
Annual Report and Summary Accounts 2007-200821
We will increase capacity and capability of ourcommunity services and see a reduction in demandfor inpatient care for working age adults and olderpeople. In addition, the Trust will continue to striveto develop more home-based care for older people,and to empower service users in choices anddecisions over their treatment and recovery plans,including advanced directives.
All changes that have been made to services acrossthe Trust have been undertaken after full andsuccessful consultation with stakeholders includingstaff and service users.
The Trust remains committed to achieving serviceexcellence and has involved staff from all servicesand at all levels in identifying key areas fordevelopment in the future.
Retain and expand high quality services for commissioners97% of the Trust’s clinical income comes from ourfive main commissioners. As a result, the Truststrives to provide excellent services and to expandthe range of services we provide. We have signedthree year contracts (2007/08 – 2009/10) and willreceive a 1% quality payment each year from2007/08 until 2009/10.
In 2008/09, we will continue to work with our PCTand Local Authority commissioners to continue toattract new investment to improve services. Further improvements will be made to CrisisResolution and Home Treatment Teams and EarlyIntervention Services.
The Trust will continue to manage positive andeffective relationships with our workforce, staffside, PCT commissioners and Local Authorityofficers, along with our Joint Overview andScrutiny Committee.
Although we already market our existing forensicservices we have recognised the need to bring inadditional marketing experience to the organisationand development of a Marketing Strategy.
We believe we already have a strong performanceand quality focus, but recognise that as an FT wewill need to improve all our main functions (finance,HR, performance, governance and information) tobegin to deliver service line management.
To be a Great Place to WorkThe Trust will continue to progress the areas outlinedin our Organisation Development Strategy. We willlaunch the Learning and Development Strategy inSummer 2008 to ensure that our service and trainingstrategies work to create a well trained, expert andconfident workforce for the future.
We will continue to ensure that staff benefit fromflexible working, and continue regular consultationwith staff groups, focus groups and Trade Unions toensure that opportunities for workforce developmentare maximised.
We will continue to strengthen engagement andinvolvement of all our clinicians to build plans thatare achievable and effective.
Another staff engagement and development event is planned for July 2008, to continue to achieve our goal of making Pennine Care ‘A Great Place To Work’.
In addition to this, the Trust is working to create anEstate Investment Strategy, working with the EstatesTeam and external consultants from a companycalled Community Solutions to deliver a strategy formanaging the estate and achieve value for moneypremises, including investigating the possibility ofrationalising the estate.
The Organisational Development event
22
Priorities for the futureEffective use of resourcesPennine Care has always been efficient in meeting itsfinancial duties. The Trust has managed significantservice changes over the past few years, and is nowin recurrent surplus. At the same time, our referencecost is low and our service quality is high, indicatingthat we are achieving a large amount at a relativelylow cost.
The Healthcare Commission recently awarded theTrust a rating of ‘Good’ for Use of Resources, andwe are confident that we will continue to deliverexcellent value for service users and commissioners.
We will continue work with our commissioners ondelivering a local currency for mental health andwork as part of the Department of Health’s ‘Paymentby Results’ pilot to shape the national agenda.
When the Trust becomes a Foundation Trust,reinvestment of the surplus that we will make will go towards improving the Trust’s organisationalobjectives.
Becoming a Foundation TrustThe Trust is confident that we will become aFoundation Trust in 2008/09. However, securing thetitle of a Foundation Trust is just one aspect of thisobjective. Our ambitions as a FT are much broader,and we intend to use the greater freedoms that FTstatus will bring to enhance services, userinvolvement, and the reach of our business.
The Trust is conscious of its role in serving thecommunity, particularly vulnerable people withmental health needs. To this end we recognise that our objectives will hold significantly more valueif they represent the needs of the communities we serve.
One of the key drivers for moving towards FT statusis the opportunity to liaise more with service users.We have a good track record of service userinvolvement with service users/carers and the Publicand Patient Involvement Forum sitting on our TrustBoard. We will build on this experience as we recruitour members and develop the Council of Members,and fully involve all stakeholders in setting andreviewing corporate objectives moving forward.
Being an efficient and effective organisation withinthe new regime is equally as important. Thereforewe are planning to progress both our applicationand our long term plans for the future with thesupport of over 10,000 local members with anincreased say over the direction of the Trust, and theCouncil of Members to represent the widermembership body.
The external validation by Monitor, the inspectors ofFoundation Trusts, will give us further confidencethat as a FT we will be a well managed andfinancially sound body.
The FT will work within a legally binding constitutionthat is based on a government recommended modelconstitution for Foundation Trusts, as amended to fitPennine Care’s unique make-up. The constitutionand the entire governance framework for theFoundation Trust fits with the Monitor ComplianceFramework.

Priorities for the future
Annual Report and Summary Accounts 2007-200823
Looking back on our achievements since last yearThe Trust set itself some ambitious objectives in 2007/08, and has achieved an enormous amount. The Trust is proud of its achievements in the last year and hopesthat it can continue to develop its services and meet its objectives in the future as it has done in the past year.
Our record of achievement against our objectives in the last year is strong, and includes:
We said... We did...
“We will establish two newdirectorates for CAMHS andSMS”
The two directorates have been established and are now performing more strongly. Business is growing and services are beingprovided in a more improved way.
In the coming year we hope to build on this success and grow a more full range of services for our clients.
“We intend to establishBusiness Hubs for our Northand South Divisions and theHigh Support and ForensicsDirectorate”
Business Hubs are now operational in all of these areas. The Hubs bring together finance, HR and business planning expertisealongside clinical and managerial personnel from the Divisions and Directorate concerned, to allow focused decision making anddedicated resources. They also build relationships with PCTs and Local Authorities to better serve the Trust here too.
The Hubs have been very successful in providing what they were designed to do, and Hub staff are now being made available forthe newly established SMS and CAMHS directorates.
“We will continue to developour implementation plans tomeet NICE guidance… and wewill for the first time clarify thecost, quality and quantity of theservices we provide”
The Trust has set up and continues to work on a project to develop a ‘Care Pathways’ approach to service delivery, making it clearto the Trust and its commissioners the quality, quantity and cost of services.
The Care Pathways that are developed are being created not only with NICE guidance in mind, but other nationally recognisedgood practice guidance, and the clinical expertise of the relevant parts of the Trust.
“We will increaseOrganisational Activity to reachout widely across theworkforce”
Over £1 million has been identified for the Trust’s Organisational Development strategy, which has been distributed Trust-wide.
Enhanced development opportunities include coaching and leadership development for managers, and a greater scope for thecreation of Assistant and Advanced practitioners for clinical staff.
“We will continue to becomemore efficient and still deliversustained improvement to meetthe expectations of those whouse our services”
The Trust has once again met all of its statutory financial obligations, whilst improving service quality.
The Healthcare Commission has improved its rating of the Trust to ‘Excellent’ for service quality and ‘Good’ for Use of Resources –an improvement in both scores.
At the same time as we make significant efficiency savings and meet challenging financial targets, we continue to improve servicequality across the board.

24
The Trust BoardThe Trust Board is responsible for setting thestrategic direction for the organisation, monitoringservices and financial performance and ensuringpublic accountability and probity.
The Trust is committed to applying the principles ofthe Codes of Conduct and Accountability publishedby the Department of Health.
Meetings of the Trust Board are held on the lastWednesday of each month and in February 2008 itwas agreed to open these to the public four timesper year. Membership of the Board includes theChairman and five Non-Executives who bring anindependent external view to the organisation, alongwith the Chief Executive and four ExecutiveDirectors. Additionally, invitations to the public Boardmeetings are extended to six Associate Directorswho bring a Local Authority view, plus Service Userand Carer representatives. Additionally, in November2007, the Board appointed Katy Calvin-Thomas asDirector of Planning, Performance and Information.
Remuneration of Board Members is agreed by theRemuneration Sub-Committee. As part of ensuringprobity and overseeing performance, the Trust hasestablished Trust Board sub-committees plus aSteering Group for service user and carerinvolvement. Membership of these committees isshown against each name by the following numbers:
Remuneration (1)Finance (2) until 14.05.07Audit (3) Workforce and Organisational Development (4) until 12.04.07Governance (5) until 23.08.07Integrated Governance (6) from 24.10.07IM&T Strategy (7) until 27.03.08Service Development Board (8) from 12.07.08Service Users and Carers Steering Group (9)
ChairmanTerence McCabe (until 31.10.07)John Schofield (from 01.11.07)
Non-Executive DirectorsRex CharltonAlan MoranMansoor ShahAnne SykesChristine Webb (until 30.09.07)Robert Ainsworth (from 01.01.08)
DirectorsJohn Archer Chief Executive
David Curtis Director of Nursing & Integrated Governance
Dr Di James Medical Director (until 30.09.07)
Dr Sudhir Kaligotla Medical Director (from 01.10.07)
Michael McCourt Director of Operations
Martin Roe Director of Finance/ Deputy Chief Executive
Katy Calvin-Thomas Director of Planning Performance and Information
Associate DirectorsCllr. Tim ChamberlainCllr. Maggie Clay until 06.11.07Cllr. Irene Davidson until 15.05.07Cllr. Philip HarrisonCllr. Wendy Meikle from 07.11.07Cllr. Dale Mulgrew from 16.05.07Cllr. Jackie LaneCllr. Roger Wilkinson
Service User RepresentativesToni Goodhew and Steven Watson
Carer RepresentativeJean Prest
The Trust Board
Annual Report and Summary Accounts 2007-200825
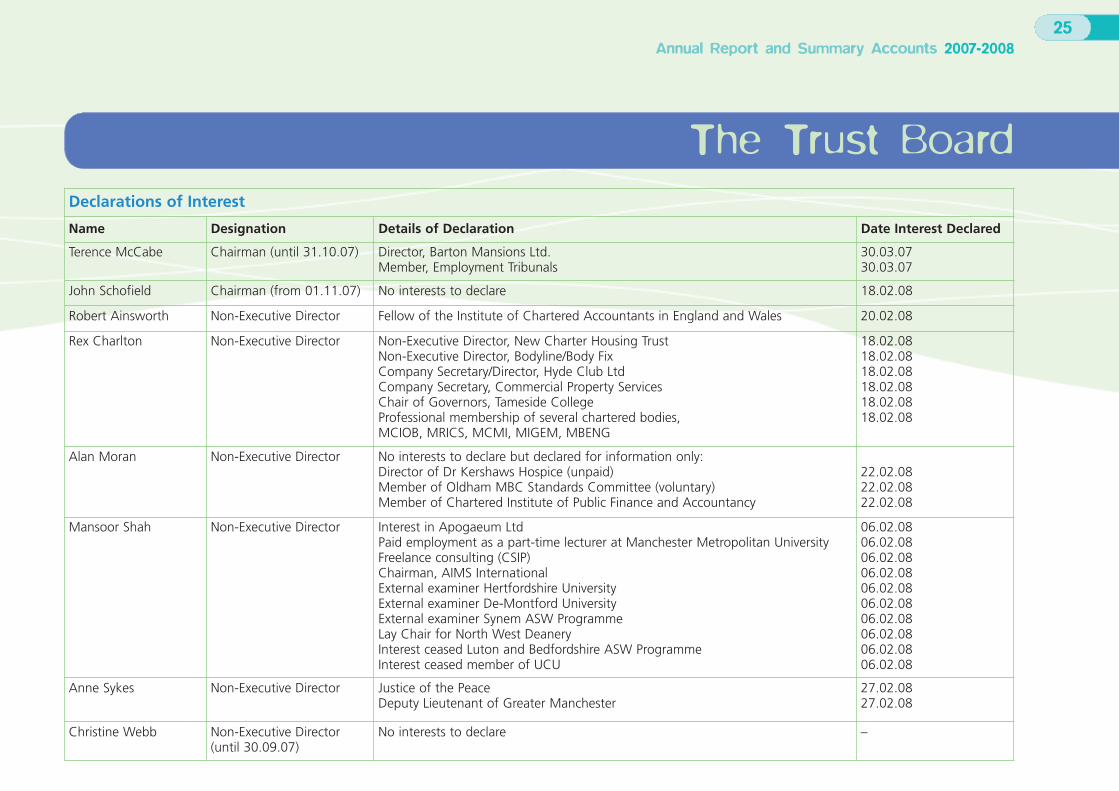
Declarations of Interest
Name Designation Details of Declaration Date Interest Declared
Terence McCabe Chairman (until 31.10.07) Director, Barton Mansions Ltd.Member, Employment Tribunals
30.03.0730.03.07
John Schofield Chairman (from 01.11.07) No interests to declare 18.02.08
Robert Ainsworth Non-Executive Director Fellow of the Institute of Chartered Accountants in England and Wales 20.02.08
Rex Charlton Non-Executive Director Non-Executive Director, New Charter Housing TrustNon-Executive Director, Bodyline/Body FixCompany Secretary/Director, Hyde Club LtdCompany Secretary, Commercial Property ServicesChair of Governors, Tameside CollegeProfessional membership of several chartered bodies, MCIOB, MRICS, MCMI, MIGEM, MBENG
18.02.0818.02.0818.02.0818.02.0818.02.0818.02.08
Alan Moran Non-Executive Director No interests to declare but declared for information only:Director of Dr Kershaws Hospice (unpaid)Member of Oldham MBC Standards Committee (voluntary)Member of Chartered Institute of Public Finance and Accountancy
22.02.0822.02.0822.02.08
Mansoor Shah Non-Executive Director Interest in Apogaeum LtdPaid employment as a part-time lecturer at Manchester Metropolitan UniversityFreelance consulting (CSIP)Chairman, AIMS InternationalExternal examiner Hertfordshire UniversityExternal examiner De-Montford UniversityExternal examiner Synem ASW ProgrammeLay Chair for North West DeaneryInterest ceased Luton and Bedfordshire ASW ProgrammeInterest ceased member of UCU
06.02.0806.02.0806.02.0806.02.0806.02.0806.02.0806.02.0806.02.0806.02.0806.02.08
Anne Sykes Non-Executive Director Justice of the PeaceDeputy Lieutenant of Greater Manchester
27.02.0827.02.08
Christine Webb Non-Executive Director(until 30.09.07)
No interests to declare –

26
The Trust Board
In line with our work on becoming a Foundation Trust, the Trust has simplified its committee structures during 2007/08. We now have four sub-committees of the Board:
Declarations of Interest (continued)
Name Designation Details of Declaration Date Interest Declared
John Archer Chief Executive No interests to declare 18.02.08
David Curtis Director of Nursing & Integrated Governance No interests to declare 03.03.08
Dr Di James Medical Director (until 30.09.07) No interests to declare 09.02.07
Dr Sudhir Kaligotla Medical Director (from 01.10.07) No interests to declare 03.03.08
Michael McCourt Director of Operations No interests to declare 18.03.08
Martin Roe Director of Finance/Deputy Chief Executive No interests to declare 22.02.08
Katy Calvin-Thomas Director of Planning, Performance & Information (from 01.11.07) No interests to declare 15.02.08
Committee name Function Membership
Audit Committee Scrutiny and testing of organisational process and procedures Non-Executive Director ChairAll Non-ExecutivesDirector of FinanceOther Directors and Managers as required
Remuneration Sub-Committee Remuneration of Board Members and senior managers Chairman
Executive IntegratedGovernance Group
Management of integrated governance including risk, complaints andcompliance
Director of Nursing and Integrated Governance (Chair)Executive Directors including Medical DirectorSenior Managers from Clinical and Corporate GovernanceDeputy Director of Finance
Service Development Board Management of the Trust’s Strategic Goals and Business Plan Chief Executive (Chair)All Executive DirectorsService Directors and Deputy Director of Finance

11.1 Scope of responsibilityThe Board is accountable for internal control. As Accountable Officer, and Chief Executive ofthis Board, I have responsibility for maintaininga sound system of internal control that supportsthe achievement of the organisation’s policies,aims and objectives. I also have responsibility forsafeguarding the public funds and theorganisation’s assets for which I am personallyresponsible as set out in the Accountable OfficerMemorandum.
The responsibility of the Trust Chief Executive
The Chief Executive has overall responsibility forhaving an effective Risk Management system inplace within the Trust and for meeting all statutoryrequirements and adhering to guidance issued bythe Department of Health in respect of riskmanagement. Responsibility for core standard C9under the Trust’s Annual Health Check 2007/08,Standards for Better Health AccountabilityFramework also falls within this role.
The responsibility of the Director ofFinance/Deputy Chief Executive
The Director of Finance has overall responsibility forFinancial Management and statutory requirementsrelated to financial risk and reporting. For corestandards C7b and C7d under the Trust’s AnnualHealth Check 2007/08, Standards for Better HealthAccountability Framework.
The responsibility of the Director of Nursingand Integrated Governance
The Director of Nursing & Integrated Governance isthe lead Director for Governance and Risk. This postis also the Executive lead for Health and Safety. Forcore standards C1a, C1b, C2, C4a, C4b, C4c, C4e,C7a, C7e, C10b, C12, C14a, C14b, C14c, C15a,C16, C18, C20a, C20b, C21, C23 under the Trust’sAnnual Health Check 2007/08, Standards for BetterHealth Accountability Framework.
The responsibility of the Director of Operationsand Organisational Development
The Director of Operations as a member of CLIG isresponsible for the management of all seriousuntoward incidents investigation reviews and themanagement and Trust-wide implementation ofrecommendations for core standards C5b, C5c, C6,C7f, C8a, C8b, C10a, C11a, C11b, C11c, C13a,C15b, C17, C19, C22a, C22b, C24 under the Trust’sAnnual Health Check 2007/08, Standards for BetterHealth Accountability Framework. This post is alsoExecutive lead for the Whistle Blowing Policysupported by the Head of Human Resources.
The responsibility of the Medical Director
The Medical Director is the lead executive directorfor Clinical Effectiveness including Drugs &Therapeutics. For core standards C4d, C5a, C5d,C13b, C13c under the Trust’s Annual Health Check2007/08, Standards for Better Health AccountabilityFramework.
The responsibility of Director of Planning,Performance and Information
The Director of Planning, Performance andInformation has delegated responsibility for businessplanning and business planning risks, developmentand monitoring of the Performance AssessmentFramework as a key organisational control and forensuring the completion of the Core Standards final declaration.
The responsibility of the Associate Director ofClinical Governance
The Associate Director of Clinical Governance hasdelegated responsibility for clinical risk. This postholder chairs the Risk & Clinical GovernanceCommittee, the Health and Safety Committee andthe Complaints Litigation and Incident Review Group (CLIG).
The purpose of the system of internal control
The system of internal control is designed to managerisk to a reasonable level rather than to eliminate allrisk of failure to achieve policies, aims and objectives.It can therefore only provide reasonable and notabsolute assurance of effectiveness. The system ofinternal control is based on an ongoing processdesigned to:l Identify and prioritise the risks to the achievement
of the organisation’s policies, aims and objectives,
l Evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically
Statement of internal control
Annual Report and Summary Accounts 2007-200827

28
Statement of internal controlThe system of internal control has been in place in Pennine Care NHS Trust for the year ended 31 March 2008 and up to the date of approval ofthe annual report and accounts.
11.2 Capacity to handle riskThe Trust has a Risk Management Strategy that isendorsed by the Board. The Board reviewed theStrategy in 2007/08. The Strategy is available to allstaff via both the intranet and internet and clearlyoutlines the risk management process.
In 2007/08 the Trust substantially refreshed itsIntegrated Business Plan as part of its FoundationTrust application. The plan details risk issues in meeting short, medium and long term business plans.
Training and education are key elements of theTrust’s risk management development process. Itprovides staff with the necessary knowledge andskills to work safely and to minimise risks at alllevels. The Trust provides training in all areas to staffand other agencies working within the Trust sites toensure the maintenance and continuousdevelopment of a risk management culture.
This process is started at induction. All staff arerequired to attend a corporate induction programmeon joining the Trust and this includes an introductionto risk management within Pennine Care NHS Trust,which requires staff to self-assess their personalresponsibilities and development needs in relation torisk management.
Staff are required to undertake further training asidentified in the mandatory training plan, which isdeveloped as part of the OrganisationalDevelopment strategy.
11.3 The risk and control frameworkThe purpose of the Trust’s Risk ManagementStrategy is to detail the Trust’s framework for settingobjectives, providing assurance and managing risk,which enables:l The Trust to maintain a risk register, that details
those risks that could prevent the achievement of Trust strategic and directorate objectives stated within the corporate plan
l The risk register to be reported through to the Trust Board via the Integrated Governance Executive Committee
l Risks to be reported to the Risk Department and entered onto the Risk Register (Safeguard system)
The Trust has a Corporate Governance team. Theteam is responsible for overall delivery of robuststandards of governance and assurance for therange of processes around corporate riskmanagement. During 2007/08 the team has beenfocused on Foundation Trust membership, and hasthis year held numerous events and consultativeexercises, achieving the Trust’s target of recruitingover 10,000 members of the local community. In2008/09 the team will begin its close workingrelationship with the Council of Members.
The Trust takes both pro-active and reactiveapproaches to the identification and management ofprincipal risks that may threaten the achievement ofstrategic and directorate objectives. This involvesboth strategic (Risk & Clinical GovernanceCommittee) and operational (Governance Forums)undertaking the following process:l Risk Identification (principal risk)
l Risk Identification (corporate risk)
l Evaluate the nature and extent of identified principal risks
l Confirming existing controls
l Assessing the level of risk
l Assessing residual risk
l Acceptable risk
l Unacceptable Risk
l Significant Risk
l Implementing an action plan
l Populating the risk register
The Trust risk register is reported monthly to theIntegrated Governance Executive Group.
Management of risk is embedded in the organisation by the development of systems andprocesses at all levels. At a Borough level riskmanagement is embedded by means of localgovernance and performance forums. At Trust levelthis is the responsibility of the Risk & ClinicalGovernance Committee.
The Risk & Clinical Governance Committee isresponsible for ensuring that all significant risks arereported to the Board via the Integrated GovernanceExecutive Group on a quarterly basis. The committee

co-ordinates the management of reported risks andsupervises the operation of the risk register and theprocesses that support it. The committee receivesminutes from the following subsidiary committeesand groups: l Health and Safety Committee
l Medical Devices Group
l Infection Control Committee
l Patient Information Review Group
l Resuscitation Committee
l Clinical Procedures Committee
l Borough Governance Groups (for all Boroughs)
l ECT Forum
l R&D and Audit Committee
l Forensic and High Support Directorate Governance Group
l Governance Managers Committee
l Psychotherapeutic Committee
l Essence of Care Steering Group
The Risk & Clinical Governance Committee isresponsible for the overall monitoring of risk andmonitoring of the Trust-wide risk register.
The Trust commissioned KPMG to audit revisedintegrated governance systems and reportingframeworks. The findings of this review will beimplemented in 2008/09.
The Assurance Framework was audited in 2007 bythe Trust’s internal audit service. It has now beenfully aligned to the Trust’s objectives. The Frameworkmeets all the Department of Health requirements
but has been developed to incorporate additionalfeatures recommended. These are: l Action Plan to address risk
l Responsible officer
l Applicable time frame
The assurance framework has also been developedto link objectives with core standards underStandards for Better Health and the four keyprincipal risks linked to objectives.
Public stakeholders are involved in managing riskswhich impact on them by means of regular interfacemeetings and consultations. The main liaison is with:l Joint Interface meetings between the Trust, PCTs
and Local Authorities
l Joint Overview and Scrutiny Committee
l Patient and Public Involvement forums
There have been no significant gaps in controlsduring 2007/08 and the Assurance Frameworksupported by the Performance AssessmentFramework and risk register has resulted in all corestandards being met. Good progress is being madeon developmental standards, with targets beingachieved against Standards for Better Health andnew and existing targets respectively.
As an employer with staff entitled to membership ofthe NHS pension scheme control measures are inplace to ensure all employer obligations containedwithin scheme regulations are complied with. Thisincludes ensuring that deductions from salary,employer’s contributions and payments in to thescheme are in accordance with the scheme’s rulesand that member pension scheme records are
accurately updated in accordance with the timescalesdetailed in the regulations.
11.4 Review of effectivenessAs Accountable Officer, I have responsibility forreviewing the effectiveness of the system of internalcontrol. My review is informed in a number of ways.
The Head of Internal Audit provides me with anopinion on the overall arrangements for gainingassurance through the Assurance Framework and onthe controls reviewed as part of the internal auditwork. Executive managers within the organisationwho have responsibility for the development andmaintenance of the system of internal control provideme with assurance. The Assurance Framework itselfprovides me with evidence that the effectiveness ofcontrols that manage the risks to the organisationachieving its principal objectives have been reviewed.
My review is also informed by the PerformanceAssessment Framework, which monitors progressagainst Standards for Better Health, Auditor’s LocalEvaluation achievement levels, existing and newMental Health targets, and Trust productivity targets.My review is also informed by the external auditors,Integrated Governance Reports, HealthcareCommission Improvement Reviews, and theHealthcare Commission’s core and developmentalstandards self-assessment declaration as part of theAnnual Health Check.
I have been advised on the implications of the resultof my review of the effectiveness of the system ofinternal control by the Board, Audit Committee,Executive Integrated Governance Group and theService Development Board.
Statement of internal control
Annual Report and Summary Accounts 2007-200829

30
Statement of internal controlA plan to address weaknesses and ensurecontinuous improvement of the system is in place.l The Board with support of the Audit Committee
and Integrated Governance Executive Group is responsible for the maintenance and review of internal control systems. This year has seen the introduction of Board development sessions focused on integrated governance and board reporting, the introduction of the performance assessment framework and exception reporting, to ensure the Board is kept fully informed of risks and progress for improvement, and in the development of the Standards for Better Health Accountability Framework.
l Reports and recommendations from external and internal audit are discussed in detail at the audit committee and inform the work of and priorities of the Integrated Governance Executive Group.
l In 2007/08 the Trust has worked with service user groups to develop audits that reflect what service users want to know and 24 hour spot visits to mental health facilities by the Patient and Public Involvement Forum (PPIF) to review service quality. The PPIF is also actively involved in Patient Environment assessments during this annual process.
l There have not been any significant internal control issues in 2007/08.
11.5 Key ways in which riskmanagement is embedded in theactivity of the organisationl Over the course of 2007/08 a number of specific
actions and projects were undertaken with regards to our commitment to Information Governance and managing the risks associated with safeguarding information (regarding
Gateway 9912 dated 20th May 2008 relating to paragraph v). All actions taken were in line with the Information Security Management: NHS Code of Practice, these include:
l Trust signed up to NHS Statement of Compliance – Part 1 SOC declaration
l Completed and signed internal assurance statements as part of the Department of Health Assurance Review
l Policy produced for electronic transfer of Person Identifiable Data
l Policy produced for disposal and destruction of electronic media
l Policy produced for use of removal media
l Introduced missing case notes procedure
l Information Governance Toolkit overall score for 2007/08 (version 5) was 84% (Green)
l Procured Safeboot device control software to manage encryption on portable removable computer media
l Auditing programme for information governance compliance recommended for 2008/09
l All corporate staff received updated Information Governance training
Significant achievements
With regards to our commitment to InformationGovernance (regarding Gateway 9912 dated 20th May 2008 relating to paragraph iv) the Trusthas had no serious incidents involving data loss during 2007/08.
Summary of serious untoward incidentsinvolving personal data as reported tothe information commissioner’s office in 2007/08
Date of Incident (Month) NilNature of IncidentNature of Data InvolvedNumber of People Potentially AffectedNotification Steps
Summary of other personal data relatedincidents in 2007/08
John ArcherChief Executive(Accountable Officer, on behalf of the Board)9 May 2008
Category Nature of Incident TotalI Loss of inadequately protected
electronic equipment, devices orpaper documents from securedNHS premises
Nil
II Loss of inadequately protectedelectronic equipment, devices orpaper documents from outsidesecured NHS premises
Nil
III Insecure disposal of inadequatelyprotected electronic equipment,devices or paper documents
Nil
IV Unauthorised disclosure Nil
V Other Nil

31
Report from the Director of Finance/Deputy Chief Executive
Operating and financial review
Introduction
The Operating and Financial Review (OFR)examines the current performance of theorganisation against the key policies and targetsit is required to achieve. The OFR provides acomprehensive analysis of the Trust’sdevelopment and analysis during the year and itsposition at the end of the year. It will also identifythe main trends and factors that have affectedthis position and will highlight any future impactthey may have on the Trust’s overall performance.
Trust Performance 2007/08
Despite facing significant financial pressures the Trustwas able to achieve its financial targets (without theneed for planned financial support) whilst continuingto deliver and develop services.
Capital Resource Limited (CRL)
Definition:The Trust is given a Capital Resource Limit (CRL)which it is not permitted to overspend againstPurpose:The CRL controls the amount of capital expenditurethat the Trust may incur in a financial yearSource of Data:Trust Audited Financial Statements Target: £11,842kResult: £11,797k – Achieved within permissible limits
External Financing Limit (EFL)
Definition:The EFL is the difference between the CapitalExpenditure incurred in year and the cash generatedfrom its operations to fund that expenditurePurpose:To limit the cash that will be provided by HMTreasury, minimising the Public Sector BorrowingrequirementSource of Data:Trust Audited Financial Statements Target: £7,295kResult: £7,270k – Achieved within permissible limits
Capital Cost Absorption Ratio
Definition:The Trust is required to absorb the cost of capital at3.5% of average relevant net assets, calculated asthe percentage that dividends paid on publicdividend capital bears to average relevant net assets Purpose:To reflect the cost of the money tied up in capitalassets and not available to use elsewhereSource of Data:Trust Audited Financial Statements Target: 3.5%Result: 3.3% – Achieved within permissible limits
Public Sector Payment Policy
Definition:Unless other terms are agreed, the Trust is requiredto pay its creditors within 30 days of the receipt ofgoods, or a valid invoice, whichever is the laterPurpose:To ensure that the Trust complies with the BetterPayment Practice CodeSource of Data:Trust Audited Financial Statements Target: 95%
Non NHS Creditors Number £000Total bills paid in the year 19,629 39,554Total bills paid within target 19,208 39,410
Percentage of bills paid within target 97.9% 99.6%
NHS Creditors Number £000Total bills paid in the year 1,220 15,921Total bills paid within target 1,196 15,901
Percentage of bills paid within target 98.0% 99.9%
Result: Achieved
Annual Report and Summary Accounts 2007-2008

32
BreakevenDefinition:The Trust should ensure that its revenue is not lessthan sufficient taking one year with another to meetits outgoingsPurpose:To ensure the Trust achieves a balanced position onthe income and expenditure account each yearSource of Data:Trust Audited Financial Statements Target: Minimum of £0kResult: Achieved with an in year £612k surplus. In line with Department of Health guidance Trustsare now expected to budget to achieve a smallsurplus.
Management CostsIn order to control the amount of NHS expenditurecommitted to the management of organisations, theNHS Executive requires organisations to report theirManagement Costs as a percentage of income.
Late Payment InterestLegislation is in force, which requires Trusts to payinterest to small companies if payment is not madewithin 30 days (Late Payment of Commercial Debts(Interest) Act 1996). The Trust’s performance againstthis criteria is:
£000Amounts included within Interest Payable arising from claims made by businesses under this legislation. 0
The Trust achieved all its financial targets in 2007/08and generated an overall surplus of £612k (0.6%) inline with Department of Health guidance. During theyear the Trust implemented and successfullydelivered a cost improvement programme of £4.5million, which enabled the Trust to achieve itsfinancial targets.
The management of cash, and the achievement ofthe External Financing Limit, was once againparticularly challenging in 2007/08 given the size ofthe capital programme with expenditure of £11.8million across 30 schemes.
The Trust had previously achieved ‘good’ for thequality of its services and ‘fair’ for the use ofresources under the Healthcare Commission’s AnnualHealthcheck. Since the publication of the last AnnualReport, the Trust has been successful in improving itsscores to ‘ excellent’ and ‘good’ respectively.
The Trust continued to pursue its application forFoundation Trust (FT) status throughout 2007/08. Aspart of its application the Trust has developed a fiveyear Business Plan, Financial Model, MembershipStrategy and Constitution. A key element of theBusiness Plan is the Service Development Strategy,which sets out the service strategy over the next fiveyears and is based on the developmental workcarried out in the Service Improvement Groups.
In March 2008 the Trust gained the support of theSecretary of State to progress with its application.The Trust is now able to move on the final stage ofthe application process, which involves a rigorousassessment of the Trust’s plans by Monitor, the FTRegulatory Body. The Trust anticipates receiving finalauthorisation to become an FT by 1st July 2008.
The Trust continues to develop its PerformanceAssessment Framework (PAF) which identifies all thekey national and local targets and monitors progress towards achieving them. The PAF helps theTrust deliver high quality services and meet thenational standards.
From a capital perspective, the Trust has completedthe Rochdale and Bury business, transforming theselocal services. A new outpatients department,sensory garden and main entrance has beencompleted at Stepping Hill Hospital, linking twoolder buildings to create a friendlier and morepractical environment for all. There has been a needto move and realign services in relation to the Healthin Tameside scheme, these moves enabling theTameside PFI to continue. Emphasis has also beenplaced on backlog maintenance and DDA in 2007/08to ensure a safe and pleasant environment forclients, staff and visitors and to ensure that there isno ‘high risk’ work outstanding.
Emergency PreparednessWe have built on our Major Incident Plan and nowhave a range of more specific plans including thePandemic Flu Plan, the Heatwave Plan, the MajorIncident Multiple Enquiry Plan and aCommunications Plan, all of which meet national guidance.
This year has seen substantial revision of the Trust’sEmergency Plan, and agreement by the Board of anaction plan to refresh the emergency preparednessof the Trust as a whole. In addition, the Board hasworked with external emergency responseprofessionals to ensure that the Trust furtherdevelops its plans in this area.
£0002006/07
£000Management Costs 5,640 5,000Income 103,916 95,151
Environmental PolicyDuring 2007/08 the Trust commenced a long-termprogramme of improvements to the environment, as follows: l Developed a new waste management policy and
through the introduction of this policy improved waste recycling measures will be introduced
l Introduced separate metering at all premises where this was achievable. This will give the Trust a clearer understanding of energy usage by site and from that we can develop measures to reduce our CO2 emissions
l Developed a bid for funding that has been submitted to the DH to install Combined Heat and Power units at the five main sites and through this we will achieve reduced CO2 emissions and reduced costs
Looking AheadThe Trust faces a series of significant financialchallenges over the next five years and beyondbut by having three year signed contracts in placewith its main commissioners, together withcommitments to an additional 1% qualitypayment for each of the next three years there ismore certainty about the level of income the Trustwill receive in the medium term.
The Trust is active in many ways to help deliver ourobjectives:l Implementing the business plan for 2008/09
This sets out the objectives that each Borough andcorporate service need to build upon its excellent performance in 2007/08 and to deliver in 2008/09, assisting the Trust to remain on track with its business plan
l Delivering an Organisational Development StrategyWe will continue to invest in our OD and training strategy to ensure our staff are supported and able to deliver better services as we become a FT
l Improving the contracting function and supporting work to deliver the CSIP ProjectWe continue to work with all our PCTs and LAs to develop better tools for contracting mental health services
l Service Line ManagementThe Trust has established two pilot sites to help develop Service Line Management (SLM). The SLM initiative will enable a clearer link to be made between the income that the Trust receives for services and the costs of providing those services, i.e. relative profitability/efficiency
l Investment StrategyThe Trust has already identified its areas of investment for 2008/09, designed specifically to assist in the achievement of the Trust’s five-year business plan. The Trust appreciates the important role that our Estate will play in achieving our objectives and will continue to refine its Estate Strategy. This in turn will enable the development of an Investment Strategy for our Estate over the next five years
l New Business developmentWe will continue with the structure and processes that demonstrates how and why we have taken decisions about new business, to ensure full transparency of decision making
l MarketingWe will continue to develop our Marketing Strategy. The Trust has already actively brought new business and marketing skills onto the Trust Board and will continue to do so
l Integrated GovernanceWe will continue work to improve integrated governance ensuring that the Board has the assurance it requires to take the organisation forward as an FT
l Achieving performance and governance targetsWe will continue to use our PAF to deliver improved levels of performance both nationally and locally
Annual Report and Summary Accounts 2007-200833

34
Overall assessment of the TrustThe Trust has continued to develop services andimprove the overall environment for service users. At the same time the Trust has made major progressin stabilising its financial position, 2007/08 is the firsttime that the Trust has started a new financial yearin recurrent financial balance. By securingFoundation Trust status the Trust will have access tofinancial freedoms and flexibilities, which will help tosecure its future financial viability.
The accounts shown on pages 37 to 39 are summaryfinancial statements and might not contain sufficient
information for a full understanding of the Trust’sfinancial position and performance. A copy of thefull accounts are included on the Trust’s internet siteor can be obtained by writing to:
Freedom of Information OfficerChief Executive’s DepartmentPennine Care NHS TrustTrust HQ225 Old StreetAshton-under-LyneLancashireOL6 7SR
There is, however, a series of risks associated with delivering the Business Plan and they, together with the strategy for managing them, are detailed in the tablebelow:
Risk Ongoing mitigation
SecuringContractIncome
Contracts are signed on a three year basis and the Trust is in the 2nd year of our three year contract.
Recent guidance has required PCTs to place all providers on a new Standard NHS Contract. For aspirant FTs, the guidance suggests that an interimcontract be issued from the point of authorisation for 18 months until March 2012. It will then be subject to re-negotiation. The Trust is already indiscussion with our Lead Commissioner (HMR PCT) about the development of rolling contracts.
The Trust is also working with commissioners on the MH Commissioning Project and is a PbR pilot to support the delivery of a mental health currency.
WorkforceDevelopment
This was recognised as a potential weakness in our SWOT analysis. We recognised that ensuring we have excellent staff and are able to attract andretain staff is key to our success as an FT.
We have engaged with an outside agency to work with us to improve our workforce and organisational development. Our overarching WorkforceAction Plan picks up the various workstreams.
The Trust continues to implement its OD strategy and has recently launched its new Learning and Development Directorate in May 2008.
EstateInvestmentPlan
The Trust has nine main sites and 44 community premises and it is recognised that the configuration and utilisation of our estate will play a majorrole in delivering the IBP. The Trust has already been able to address backlog maintenance to the extent that it can now report no high riskmaintenance issues. Work also continues on the business cases for the forensic unit and the young persons’ ward. The Trust is actively engagedwith Community Solutions (a LIFT company with experience of providing capital solutions across agencies) to support work on development of ourEstate Investment Plan.
Young Persons’Unit
The Trust decided to open an interim Young Persons’ Unit in May 2008. This was to ensure that we were an early entrant into this new market andto secure contracts with the Trust’s main commissioners. This Trust has already undertaken and been successful in contract negotiations but workcontinues to ensure the full occupancy of this unit.

Summary of Financial Statements
Statement of the Chief Executive’sresponsibilities as the AccountableOfficer of the TrustThe Secretary of State has directed that the ChiefExecutive should be the Accountable Officer to the Trust.
The relevant responsibilities of the AccountableOfficers, including their responsibility for thepropriety and regularity of the public finances forwhich they are answerable, and for the keeping ofproper records, are set out in the AccountableOfficers’ Memorandum issued by the Department of Health.
To the best of my knowledge and belief, I haveproperly discharged the responsibilities set out in myletter of appointment as an accountable officer.
John ArcherChief Executive OfficerMay 2008
Statement of the Directors’responsibilities in respect of the accountsThe Directors are required under the National HealthService Act 1977 to prepare accounts for eachfinancial year.
The Secretary of State, with the approval of theTreasury, directs that these accounts give a true andfair view of the state of affairs of the Trust and ofthe income and expenditure of the Trust for thatperiod. In preparing those accounts, the Directors arerequired to:l Apply on a consistent basis accounting policies
laid down by the Secretary of State with the approval of the Treasury
l Make judgments and estimates which are reasonable and prudent
l State whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts
The Directors are responsible for keeping properaccounting records, which disclose with reasonableaccuracy at any time the financial position of theTrust and to enable them to ensure that theaccounts comply with requirements outlined in theabove-mentioned direction of the Secretary of State.They are also responsible for safeguarding the assets of the Trust and hence for taking reasonablesteps for the prevention and detection of fraud andother irregularities.
The Directors confirm they have complied with theabove requirements in preparing the accounts.
By order of the Board:
John ArcherChief Executive OfficerMay 2008
Martin RoeDirector of Finance/Deputy Chief ExecutiveMay 2008
Annual Report and Summary Accounts 2007-200835

36
Independent Auditors’ Report tothe Directors of the Board ofPennine Care NHS TrustWe have examined the summary financial statementswhich comprise the Income and ExpenditureAccount, the Note to the Income and ExpenditureAccount, the Balance Sheet, the Statement of TotalRecognised Gains and Losses and the Cash Flow Statement.
This report is made solely to the Board of PennineCare NHS Trust in accordance with Section 2 of theAudit Commission Act 1998. Our audit work hasbeen undertaken so that we might state to theBoard of Pennine Care NHS Trust those matterswhich we are required to state to them in anauditor’s report and for no other purpose. To thefullest extent permitted by law, we do not accept orassume responsibility to anyone other than PennineCare NHS Trust and the Board of Pennine Care NHSTrust, as a body, for our audit work, for this report,of for the opinions we have formed.
Respective responsibilities of directors and auditorsThe directors are responsible for preparing theAnnual Report. Our responsibility is to report to youour opinion on the consistency of the summaryfinancial statement within the Annual Report withthe statutory financial statements.
We also read the other information contained in theAnnual Report and consider the implications for ourreport if we become aware of any mis-statements ormaterial inconsistencies with the summary financialstatement.
Basis of opinionWe conducted our work in accordance with Bulletin1999/6 ‘The auditors’ statement on the summaryfinancial statement’ issued by the Auditing PracticesBoard. Our report on the statutory financialstatements describes the basis of our audit opinionon those financial statements.
OpinionIn our opinion the summary financial statement isconsistent with the statutory financial statements ofthe Trust for the year ended 31 March 2008.
KPMG LLPManchester20th June 2008

Annual Report and Summary Accounts 2007-200837
Income and expenditure account for the year ending 31st March 2008
2007/08£000
2006/07£000
Income from activities 93,374 84,064
Other operating income 19,753 17,911
Total income 113,127 101,975
Operating expenses (110,437) (100,088)
OPERATING SURPLUS/(DEFICIT) 2,690 1,887
Profit/(loss) on disposal of fixed assets 0 402
SURPLUS/(DEFICIT) BEFOREINTEREST
2,690 2,289
Interest receivable 278 173
Interest payable 0 0
Other finance costs – unwinding ofdiscount
(3) (3)
Other finance costs – change indiscount rate on provisions
0 0
SURPLUS/(DEFICIT) FOR THEFINANCIAL YEAR
2,965 2,459
Public Dividend Capital dividendspayable
(2,353) (1,916)
RETAINED SURPLUS/(DEFICIT) FORTHE YEAR
612 543
Note to the income and expenditure account for the yearended 31st March 2008
2007/08£000
2006/07£000
Retained surplus/(deficit) for the year 612 543
Financial support included in retainedsurplus/(deficit) for the year – NHSBank
0 0
Financial support included in retainedsurplus/(deficit) for the year –Internally Generated
0 0
Retained surplus/(deficit) for the yearexcluding financial support
612 543
The Trust has not received any financial support during 2007/08.

38
Balance sheet as at 31st March 2008
Signed: (Director of Finance/Deputy Chief Executive) Date: 18th June 2008
31st March 2008£000
31st March 2007£000
FIXED ASSETS
Intangible assets 149 96
Tangible assets 79,751 68,528
79,900 68,624
CURRENT ASSETS
Stocks and work in progress 925 46
Debtors 5,057 4,804
Cash at bank and in hand 2,351 326
8,333 5,176
CREDITORS: Amounts falling duewithin one year
(8,614) (5,741)
NET CURRENTASSETS/(LIABILITIES)
(281) (565)
TOTAL ASSETS LESS CURRENTLIABILITIES
79,619 68,059
PROVISIONS FOR LIABILITIES ANDCHARGES
(191) (269)
TOTAL ASSETS EMPLOYED 79,428 67,790
FINANCED BY:
TAXPAYERS' EQUITY
Public dividend capital 69,542 60,247
Revaluation reserve 8,063 6,430
Government grant reserve 59 56
Income and expenditure reserve 1,764 1,057
TOTAL TAXPAYERS' EQUITY 79,428 67,790
Statement of total recognised gains and losses for the year ended 31st March 2008
2007/08£000
2006/07£000
Surplus/(deficit) for the financial yearbefore dividend payments
2,965 2,459
Fixed asset impairment losses (3,491) (6,286)
Unrealised surplus/(deficit) on fixedasset revaluations/indexation
5,224 4,764
Total recognised gains and lossesfor the financial year
4,698 937
Prior period adjustment 0 0
Total gains and losses recognisedin the financial year
4,698 937

Annual Report and Summary Accounts 2007-200839
Cash flow statement for the year ended31st March 2008
Remuneration report
The Trust has a Remuneration Sub-Committee (which is a full sub-Committee of the Board) whose membership consists of:l Chairman of the Trust
l Two Non-Executive Directors
In attendance (where relevant) are:l Chief Executive
l Director of Finance/Deputy Chief Executive
l Director of Operations
l Head of Human resources
The Remuneration Sub-Committee determines the remuneration of theExecutive Directors and the remuneration of Associate Directors is in linewith the Agenda for Change terms and conditions.
The Trust has an individual performance development review process in placefor Executive Directors led by the Chairman and Chief Executive.
Senior managers hold substantive contracts of employment with threemonth notice periods. Any termination payments (outside contractualentitlement) are determined by the Remuneration Sub-Committee.
All senior managers hold substantive contracts of employment and there isno provision in the contracts for early termination.
No significant awards (for early termination) have been made to seniormanagers during the financial year 2007/08.
The remuneration of the Board members (together with their pensionbenefits) is detailed in the following tables.
John ArcherChief Executive Officer Dated: May 2008
2007/08£000
2006/07£000
OPERATING ACTIVITIES
Net cash inflow/(outflow) fromoperating activities
5,984 2,030
RETURNS ON INVESTMENTS ANDSERVICING OF FINANCE:Interest received 278 173
Net cash inflow/(outflow) fromreturns on investments and servicingof finance
278 173
CAPITAL EXPENDITURE
(Payments) to acquire tangible fixedassets
(11,085) (32,169)
Receipts from sale of tangible fixed assets 0 570
(Payments) to acquire intangible assets (94) (45)
Net cash inflow/(outflow) fromcapital expenditure
(11,179) (31,644)
DIVIDENDS PAID (2,353) (1,916)
Net cash inflow/(outflow) beforemanagement of liquid resources andfinancing
(7,270) (31,357)
Net cash inflow/(outflow) frommanagement of liquid resources
0 0
Net cash inflow/(outflow) beforefinancing
(7,270) (31,357)
FINANCING
Public dividend capital received 9,295 31,399
Net cash inflow/(outflow) fromfinancing
9,295 31,399
Increase/(decrease) in cash 2,025 42

40
A) Remuneration 2007-08 2006-07Salary
(bands of £5,000)Other
Remuneration(bands of £5,000)
Benefits in Kind(nearest £100)
Salary (bands of £5,000)
OtherRemuneration
(bands of £5,000)
Benefits in Kind(nearest £100)
£000 £000 £00 £000 £000 £00
Executive Directors
Mr J Archer, Chief Executive 110 - 115 – – 105 - 110 – 34
Mr M Roe, Director of Finance 85 - 90 – 102 80 - 85 – 88
Mr D Curtis, Director of Nursing andIntegrated Governance
80 - 85 – 50 80 - 85 – 50
Mr M McCourt, Director of Operations 80 - 85 – 75 80 - 85 – 75
Dr D James, Medical Director (Leaver 13/10/07)
30 - 35 45 - 50 – 30 - 35 115 - 120 –
Dr S Kaligotla, Medical Director(Starter 15/10/07) *1
20 - 25 35 - 40 3 – – –
Ms K Calvin-Thomas, (Starter 01/11/07) *2
65 - 70 – – – – –
Chairman
Mr T McCabe, Chairman (Leaver 29/10/07)
10 - 15 – – 15 - 20 – 1
Mr J Schofield (Starter 01/11/07) 5 - 10 – – 0 – –
Non-Executive Directors
Mrs A Sykes, Vice Chairman 5 - 10 – – 5 - 10 – –
Mr R Charlton, Non-Executive Director 5 - 10 – – 5 - 10 – –
Mr A Moran, Non-Executive Director 5 - 10 – – 0 - 5 – –
Mr M Shah, Non-Executive Director 5 - 10 – – 5 - 10 – –
Mrs C Webb, Non-Executive Director(Leaver 30/09/07)
0 - 5 – – 5 - 10 – –
Mr R Ainsworth, Non-ExecutiveDirector (Starter 01/01/08)
0 - 5 – – 0 – –
*1 Dr Kaligotla was appointed to the post of Medical Director but was already a consultant within the Trust*2 Ms K Calvin-Thomas was appointed to the post of Director but was already an officer within the Trust
Salary and pension entitlements of senior managers 2007/08

Annual Report and Summary Accounts 2007-200841
B) Pension Benefits
Name Real increasein pension
and relatedlump sum
age 60
Real increasein pension
lump sum atage 60
Total accruedpension andrelated lump
sum at age 60at 31st March
2008
Lump sum atage 60 related
to accruedpension at31st March
2008
CashEquivalent
Transfer Valueat 31st March
2008
CashEquivalent
Transfer Valueat 31st March
2007
Real increasein Cash
EquivalentTransfer Value
EmployersContribution
toStakeholder
Pension
(bands of£2,500)
(bands of£2,500)
(bands of£5,000)
(bands of£5,000)
£000 £000 £000 £000 £000 £000 £000 £00
Mr J Archer, Chief Executive 0 - 2.5 2.5 - 5.0 55 - 60 165 - 170 888 819 49 344
Mr M Roe, Director of Finance 0 - 2.5 5 - 7.5 25 - 30 80 - 85 404 354 40 283
Mr D Curtis, Director of Nursing andIntegrated Governance
0 - 2.5 5 - 7.5 35 - 40 110 - 115 669 610 44 308
Mr M McCourt, Director of Operations
0 - 2.5 2.5 - 5 20 - 25 60 - 65 255 226 43 162
Dr D James, Medical Director 5 - 7.5 15 - 17.5 60 - 65 185 - 190 – 953 – –
Mr S Kaligotla, MedicalDirector
2.5 - 5.0 10.0 - 12.5 10 - 15 45 - 50 160 121 36 251
Ms K Calvin-Thomas, Director of Planning,Performance & Information
0.0 - 2.5 5.0 - 7.5 5 - 10 25 - 30 90 67 22 154
A Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valuedare the member’s accrued benefits and any contingent spouse’s pension payable from the scheme. A CETV is a payment made by a pension scheme, or arrangement to secure pensionbenefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shownrelate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which thedisclosure applies. The CETV figures, and from 2004/05 the other pension details, include the value of any pension benefits in another scheme or arrangement that the individual hastransferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in thescheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real Increase in CETV – This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid bythe employee (including the value of any benefits transferred from another pension scheme or arrangement) and uses common market valuation factors for the start and end of the period.

42
Obtaining further informationIf you need help to understand this document or you require it in another format such as large print, spoken (on CD), or Braille please contact us on the details below:
Telephone: 0161 234 4041Text Phone: 0161 234 3316 (This is a text phone minicom only)Email: patient [email protected]
Supported by M4 Translations
Arabic
Bangla
Chinese
Farsi
French
Gujarati
Pushto
Urdu
Polish

A&E Accident & Emergency
BME Black and Minority Ethnic
CAMHS Child and Adolescent Mental Health Service
CETV Cash Equivalent Transfer Value
CLIG Complaints Litigation and Incident Review Group
CPA Care Programme Approach
CRL Capital Resource Limit
CSIP Care Services Improvement Partnership
DDA Disability Discrimination Act
DH Department of Health
ECT Electro-Convulsive Therapy
EFL External Financing Limit
FBC Full Business case
FT Foundation Trust
HCC Healthcare Commission
HQ Headquarters
IBP Integrated Business Plan
ICAS Independent Complaints Advocacy Service
IM&T Information Management & Technology
LAs Local Authorities
NCRS National Care Records System
NICE National Institute of Clinical Excellence
NPSA National Patient Safety Agency
NRLS National Reporting and Learning System
OD Organisational Development
OFR Operating and Financial Review
PAF Performance Assessment Framework
PCT Primary Care Trust
PICU Psychiatric Intensive Care Unit
PPIF Patient and Public Involvement Forum
SBH Standards for Better Health
SDS Service Development Strategy
SHA Strategic Health Authority
SIC Statement of Internal Control
SIG Service Improvement Group
SMS Substance Misuse Services
STaR Support, Time and Recovery
Glossary
Annual Report and Summary Accounts 2007-200843

designed and produced by vega design www.vegadesign.co.uk